
Contents
What is bladder pain
Interstitial cystitis also known as chronic inflammation of the bladder or severe chronic “painful bladder syndrome” 1, is a condition that causes discomfort or pain in the bladder and a need to urinate frequently and urgently 2. People who have interstitial cystitis have a bladder wall that is inflamed and irritated (red and sore). This inflammation can scar the bladder or make it stiff. A stiff bladder can’t expand as urine fills it. In some cases, the walls of the bladder may bleed slightly. A few people get sores in the bladder lining. More than 3 million American women and 1 million men have interstitial cystitis 3.
New research supports that interstitial cystitis is much more prevalent than originally thought 4.
- Women: 3 to 8 million women in the United States may have interstitial cystitis. That is about 3 to 6% of all women in the US.
- Men: 1 to 4 million men have interstitial cystitis as well, however, this number is likely lower than the true rate because IC in men may often be mistaken for another disorder, such as chronic prostatitis/chronic pelvic pain syndrome.
- Children: Many adults comment that their interstitial cystitis symptoms started in childhood. Pediatricians also diagnose children with this chronic condition. But, epidemiology studies have not yet been done to estimate the true prevalence of children with interstitial cystitis.
The symptoms vary from person to person. Some people may have pain without urgency or frequency. Others have urgency and frequency without pain. Women’s symptoms often get worse during their periods. They may also have pain with sexual intercourse.
Types of Interstitial cystitis
Researchers continue to study interstitial cystitis and investigate why interstitial cystitis symptoms can be different in different patients. Many believe that there may be additional subtypes, called phenotypes, of interstitial cystitis. This also helps to explain why there is such disparity in how interstitial cystitis patients respond to treatments. Of note is the national phenotyping initiative called the MAPP Research Network, part of the National Institutes of Health.
Currently there are two recognized subtypes of interstitial cystitis: non-ulcerative and ulcerative 5.
- Non-ulcerative: 90% of interstitial cystitis patients have the non-ulcerative form of interstitial cystitis. Non-ulcerative interstitial cystitis presents with pinpoint hemorrhages, also known as glomerulations, in the bladder wall. However, these are not specific for interstitial cystitis and any inflammation of the bladder can give that appearance.
- Ulcerative: 5 to 10% of interstitial cystitis patients have the ulcerative form of interstitial cystitis. These patients usually have Hunner’s ulcers or patches, which are red, bleeding areas on the bladder wall.
The above criteria were based mainly on cystoscopic findings of glomerulations and Hunner ulcers are now thought to represent severe disease 1.
About 5% of interstitial cystitis patients have persistent symptoms for more than 2 years and 5% of patients have end stage disease defined as very hard bladders with low capacity and terrible pain. Many of these patients also have Hunner’s ulcers.
What are the symptoms of interstitial cystitis ?
The symptoms of interstitial cystitis/painful bladder syndrome often mimic urinary tract infection, but cultures are negative 6.
People who have interstitial cystitis may have the following symptoms:
- An urgent need to urinate, both in the daytime and during the night (yet you may pass only very small amounts of urine each time)
- Pressure, pain and tenderness around the bladder, pelvis and perineum (the area between the anus and vagina or the anus and the scrotum). This pain and pressure may increase as the bladder fills and decrease as it empties in urination.
- A bladder that won’t hold as much urine as it used to
- Pain during sexual intercourse
- Painful urination
- In men, discomfort or pain in the penis or scrotum
For many women, the symptoms get worse before their menstrual period. Stress may also make the symptoms worse, but it doesn’t cause them.
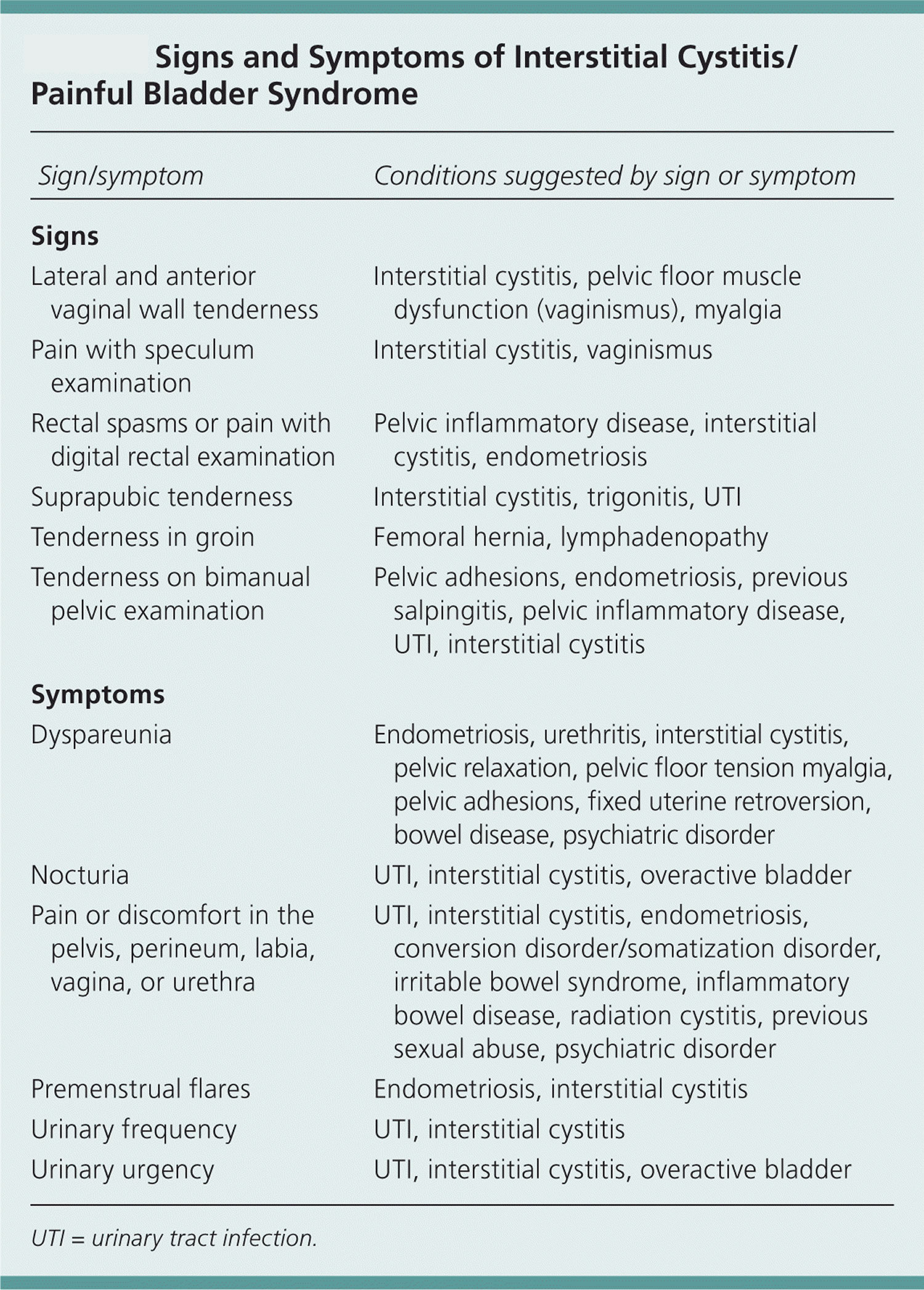
Table 1. Signs and Symptoms of Interstitial Cystitis/Painful Bladder Syndrome
| Sign/symptom | Conditions suggested by sign or symptom | |
|---|---|---|
Signs | ||
Lateral and anterior vaginal wall tenderness | Interstitial cystitis, pelvic floor muscle dysfunction (vaginismus), myalgia | |
Pain with speculum examination | Interstitial cystitis, vaginismus | |
Rectal spasms or pain with digital rectal examination | Pelvic inflammatory disease, interstitial cystitis, endometriosis | |
Suprapubic tenderness | Interstitial cystitis, trigonitis, UTI | |
Tenderness in groin | Femoral hernia, lymphadenopathy | |
Tenderness on bimanual pelvic examination | Pelvic adhesions, endometriosis, previous salpingitis, pelvic inflammatory disease, UTI, interstitial cystitis | |
Symptoms | ||
Dyspareunia (difficult or painful sexual intercourse) | Endometriosis, urethritis, interstitial cystitis, pelvic relaxation, pelvic floor tension myalgia, pelvic adhesions, fixed uterine retroversion, bowel disease, psychiatric disorder | |
Nocturia (excessive night time urination) | UTI, interstitial cystitis, overactive bladder | |
Pain or discomfort in the pelvis, perineum, labia, vagina, or urethra | UTI, interstitial cystitis, endometriosis, conversion disorder/somatization disorder, irritable bowel syndrome, inflammatory bowel disease, radiation cystitis, previous sexual abuse, psychiatric disorder | |
Premenstrual flares | Endometriosis, interstitial cystitis | |
Urinary frequency | UTI, interstitial cystitis | |
Urinary urgency | UTI, interstitial cystitis, overactive bladder | |
UTI = urinary tract infection.
There are two symptom screening questionnaires available for use in office practice11: the O’Leary-Sant Symptom and Problem Index 7 (Figure 1) and the Pelvic Pain and Urgency/Frequency Symptom Scale 6. The former has been evaluated in a sample of more than 1,000 unselected women presenting to their primary care physician; 1.1 percent had a score of 7 or higher, and 0.6 percent had a score of 12 or higher, consistent with severe interstitial cystitis/painful bladder syndrome 8. The Pelvic Pain and Urgency/Frequency Symptom Scale score correlates with a positive potassium sensitivity test in women and men 9. Because there is no reference standard test, the accuracy of these scores cannot be reported.
Figure 1. Interstitial Cystitis/Painful Bladder Syndrome – Symptom screening questionnaires
What causes interstitial cystitis ?
The cause of interstitial cystitis isn’t known. However, doctors do know that it isn’t caused by bacterial or viral infections.
The common denominator in interstitial cystitis/painful bladder syndrome is a defect or damage to the urothelium (the lining of the bladder), which normally acts as a barrier against insults to the bladder 10, 11. Normally, the lining protects the bladder wall from the toxic effects of urine. In about 70% of the people who have interstitial cystitis, the protective layer of the bladder is “leaky.” This may let urine irritate the bladder wall, causing interstitial cystitis.
Various structural and molecular abnormalities can alter urothelial permeability and trigger the pathogenesis of interstitial cystitis/painful bladder syndrome 12. The mucous layer produced by the urothelium provides a shield against noxious solutes present in the urine. The anionic mucus regulates the permeation of cationic solutes into the bladder interstitium, especially potassium, which is normally present in urine at levels that are toxic to the bladder interstitium 13.
Damaged urothelium produces cytokines that activate mast cells in the interstitium 14, 15. The diffusion of excess potassium into the bladder interstitium through a defective urothelium also triggers mast cell activation 14. The activation of mast cells results in a cycle of neuronal hyperexcitability leading to secretion of neurotransmitters and triggering further mast cell stimulation and degranulation. This process appears to contribute to the chronic pain, urgency, and frequency experienced by patients 13.
Several painful pelvic processes in men and women have demonstrated relationships to abnormalities in the urothelium, including chronic urethritis, chronic prostatitis, and chronic pelvic pain. On this basis, one expert has proposed renaming the group of conditions as lower urinary dysfunctional epithelium 10.
Is there a connection between interstitial cystitis and urinary tract infections ?
Urine cultures of interstitial cystitis patients are typically negative, meaning that bacteria cannot be found. Some theorize that interstitial cystitis may be triggered by an initial bacterial infection, or that bacteria are somehow connected with the disease. Some interstitial cystitis patients have a history of recurrent urinary tract infections prior to developing interstitial cystitis. However, many interstitial cystitis patients have no history of urinary tract infections. No evidence of bacteria or viruses in the urine cultures or bladder biopsies of interstitial cystitis patients has been found.
Interstitial cystitis patients can experience a urinary tract infection in addition to suffering from interstitial cystitis. This will require treatment with antibiotics. Patients who do experience occasional urinary tract infections may need further urological evaluation to seek a cause. Since urinary tract infections can have such a negative impact on the symptoms of interstitial cystitis, it is important to treat the urinary tract infection as soon as it is found. To prevent urinary tract infections, techniques such as antibiotic prophylaxis (taking low doses of a given antibiotic to prevent infection), and hormone replacement therapy (in post-menopausal women) can sometimes be helpful.
Diagnosis and tests for interstitial cystitis
There is no reference standard test for the diagnosis of interstitial cystitis/painful bladder syndrome. Adding to the complexity of diagnosis, numerous conditions have overlapping symptoms.
Your doctor will ask you questions about your medical history. He or she may also ask you to keep track of how much fluid you drink, how often your urinate and how much urine you pass.
Your doctor will rule out other diseases such as urinary tract infections, bladder cancer, endometriosis, kidney stones, sexually transmitted infections, chronic prostatitis in men and vaginal infections in women.
Your doctor may also refer you to a urologist (a doctor whose specialty is problems of the urinary tract). The urologist may use a special scope (called a cytoscope) to look inside your bladder for inflammation, pinpoint bleeding or ulcers. These things could indicate that you have interstitial cystitis.
Table 2. Differential Diagnosis of Interstitial Cystitis/Painful Bladder Syndrome
Carcinoma in situ | |
Infection | |
Common intestinal bacteria | |
Chlamydia trachomatis | |
Mycoplasma, Ureaplasma, Corynebacterium species | |
Candida species | |
Mycobacterium tuberculosis | |
Herpes simplex virus and human papillomavirus | |
Radiation and chemotherapy | |
Bladder neck obstruction | |
Bladder stone | |
Lower ureteral stone | |
Ureteral diverticulum | |
Urogenital prolapse | |
Genital cancers | |
Incomplete voiding | |
Overactive bladder | |
Pudendal nerve entrapment | |
Pelvic floor muscle–related pain | |
*—Listed in descending order of importance.
Physical Examination
The examination should include a bimanual pelvic examination in women and digital rectal examination in men. Examination of patients with interstitial cystitis/painful bladder syndrome may reveal pelvic floor spasms, rectal spasms, or suprapubic tenderness. In women, anterior vaginal wall and bladder base tenderness may be present.
Intravesical Potassium Sensitivity Test
The potassium sensitivity test is widely used to aid in the diagnosis of interstitial cystitis/painful bladder syndrome, although it is not universally accepted 6. It is based on the hypothesis that an abnormally permeable urothelium allows diffusion of potassium into the bladder wall, where it causes characteristic symptoms. The potassium sensitivity test is a relatively non-invasive office-based procedure and can be performed by physicians other than urologists 16. False-positive results are possible with other types of cystitis, such as bacterial and radiation cystitis 17. False-negative results may occur with use of pain medications, and in very severe or mild disease 18.
Anesthetic Bladder Challenge
An anesthetic solution such as buffered lidocaine (Xylocaine) can be instilled in a symptomatic patient. Pain relief suggests that the bladder is the source of the pain 7. An anesthetic solution also can be administered after a positive potassium sensitivity test to hasten pain resolution.
Other Urologic Testing
Cystoscopy with hydrodistension under anesthesia has been widely used for diagnosis of interstitial cystitis/painful bladder syndrome based on the 1987 National Institute of Diabetes and Digestive and Kidney Diseases diagnostic criteria 19. However, lack of evidence has led to consensus that it is not needed to confirm the diagnosis. Direct visualization of the urothelium may be useful to document bladder inflammation and disease severity. Hydrodistension can aid in the evaluation of maximal bladder capacity (about 1,150 mL in healthy adults). Small bladder capacity occurs in severe interstitial cystitis/painful bladder syndrome, but may be near normal in patients with mild to moderate cases. Cystoscopy with hydrodistension carries the risk of urethral tears and, rarely, bladder perforations.
Bladder biopsies
Bladder biopsies are not performed routinely in the United States, although they are widely used to diagnose interstitial cystitis/painful bladder syndrome in Europe 7. Biopsy may be useful to exclude a specific diagnosis such as carcinoma in situ 20. Urodynamics are not required but may help differentiate interstitial cystitis/painful bladder syndrome from detrusor overactivity.
How is interstitial cystitis treated ?
There is no cure for interstitial cystitis. A wide array of treatment options exist for interstitial cystitis/painful bladder syndrome, although well-designed clinical trials to evaluate effectiveness are largely lacking 21. Multimodal therapy that includes pentosan polysulfate sodium (Elmiron), a tricyclic antidepressant, and an antihistamine is a relatively new approach to symptom relief based on advances in understanding of the complementary pathophysiologic mechanisms, but it remains to be evaluated in well-designed clinical effectiveness trials 22. It is important to set realistic goals and expectations with patients because individual responses vary and the evidence base is weak.
You may need to try several treatments or a combination of treatments before you notice an improvement in your symptoms.
Table 3. Multimodal Therapy for Interstitial Cystitis
| Agent/dosage | Intended effect |
|---|---|
Pentosan polysulfate sodium (Elmiron), 300 to 400 mg per day divided into two to three doses | Restore epithelial function |
Hydroxyzine (Vistaril), 10 to 25 mg per day at bedtime | Control mast cell degranulation |
Amitriptyline or nortriptyline (Pamelor), 10 to 50 mg per day at bedtime | Inhibit neural activation |
Most people feel better after trying one or more of the following treatments:
- Diet. Your doctor may tell you to change what you eat. You may need to avoid alcohol, acidic foods and tobacco.
- Bladder distention. Under anesthesia, a doctor overfills your bladder with gas or fluid. This stretches the walls of the bladder. Doctors are not sure exactly why distension helps. It may make your bladder be able to hold more urine. It may also interfere with the pain signals sent by nerves in the bladder.
- Medicine. Your doctor may have you take an oral medicine called pentosan polysulfate. This medicine helps protect the lining of the bladder wall from the toxic parts of urine. Another oral medicine used to treat interstitial cystitis is an antihistamine called hydroxyzine. This medicine reduces the amount of histamine that is made in the bladder wall. Another medicine that may help is amitriptyline. It blocks pain and reduces bladder spasms. This medicine can make you sleepy, so it is usually taken at bedtime. Your doctor may also suggest that you take an over-the-counter pain medicine to ease pain.
- Bladder instillation. During a bladder instillation, a catheter (a thin tube) is used to fill your bladder with liquid medicine. You hold the medicine inside your bladder for a few seconds to 15 minutes. Then the liquid is released through urination. Treatments are given every one to two weeks for six to eight weeks. The treatment can be repeated as needed.
Oral Medicines
Pentosan polysulfate sodium is the only oral therapy approved by the U.S. Food and Drug Administration (FDA) for the treatment of interstitial cystitis 21. It was approved in 1996 and is thought to repair the urothelium. Amitriptyline and hydroxyzine (Vistaril) are inexpensive generic medications that also may be used 21. A small randomized controlled trial of four months’ duration supports the effectiveness of amitriptyline to reduce symptoms 22. Another small randomized controlled trial demonstrated that oral cimetidine (Tagamet) significantly improved symptoms of suprapubic pain and nocturia 23. Limited and uncontrolled studies show pain reduction associated with use of prednisone.
Other medications that have been tried in the treatment of interstitial cystitis/painful bladder syndrome include cyclosporine A (Sandimmune), doxycycline, urinary anesthetic (phenazopyridine [Pyridium]), alpha blockers, benzodiazepines, muscle relaxants, and narcotics 24. Oral cyclosporine has been used to treat interstitial cystitis/painful bladder syndrome based on the finding of autoantibodies to the urothelium in some patients. Clinically significant improvements were observed, including increased bladder capacity and consequently decreased urinary frequency, but these were in an uncontrolled study 24.
Intra-Bladder Therapies
A Cochrane review 29 of intravesical therapies identified nine randomized controlled trials using six agents and including 616 participants. The therapies identified were dimethyl sulfoxide, pentosan polysulfate sodium, oxybutynin (Ditropan XL), bacille Calmette-Guérin (BCG), resiniferatoxin, and alkalinization of the urine. The authors concluded that the evidence was too limited to draw any firm conclusions. They noted that BCG and oxybutynin seemed most promising and were fairly well tolerated, whereas resiniferatoxin was associated with increased pain. Despite limited clinical trial data, dimethyl sulfoxide is the only FDA-approved intravesical agent to treat painful symptoms of interstitial cystitis/painful bladder syndrome. It is a weakly acidic solvent with anti-inflammatory, analgesic, muscle-relaxant, collagen-degrading, and bacteriostatic properties 25. Traditionally, irrigation with 50% dimethyl sulfoxide solution is used for six to eight weeks to relieve moderate to severe painful symptoms of interstitial cystitis/painful bladder syndrome 26. Women can be taught to self-catheterize and instill premixed solutions at home.
Pentosan polysulfate sodium can also be used in bladder instillations. A small double-blind, placebo-controlled trial including 41 women demonstrated that the combination of oral and intravesical pentosan polysulfate sodium resulted in significant improvement in moderate to severe interstitial cystitis/painful bladder syndrome versus placebo as measured by the O’Leary-Sant Symptom and Problem Index and health-related quality-of-life measures 25. Alternatively, some experts recommend intravesical heparin 21.
Intravesical hyaluronic acid is a natural proteoglycan used in Europe and Canada for the treatment of interstitial cystitis/painful bladder syndrome, but it is not approved for this use in the United States because supporting clinical trial data were lacking 27. An uncontrolled European trial demonstrated that intravesical hyaluronic acid treatments in combination with chondroitin sulfate led to markedly decreased pain and urgency at 12 weeks 28.
OTHER ADJUNCTIVE THERAPIES
Sacral nerve stimulation may be effective in addressing the frequency associated with interstitial cystitis/painful bladder syndrome, but not for pain relief, and it is not FDA-approved for this purpose 11. A small randomized crossover trial demonstrated better symptom relief with pudendal nerve stimulation than with sacral nerve stimulation 29.
Certain dietary products including, but not limited to, coffee, alcoholic beverages, citrus fruits, tomatoes, carbonated drinks, and spicy food have been associated with exacerbation of symptoms of interstitial cystitis/painful bladder syndrome by patient survey 30. A trial of elimination of such foods may be worthwhile, but this has not been rigorously studied 21.
Physical therapy may be used in select cases of interstitial cystitis/painful bladder syndrome, especially for treatment of associated pelvic floor muscle spasm. Chondroitin sulfate and quercetin are postulated to inhibit mast cell degranulation and were associated with symptom reduction when used together in an open-label study 31. However, randomized controlled trial data are needed to verify this finding. They are available over the counter as dietary supplements alone and in combination. Cystectomy with urinary diversion is a treatment of last resort 32.
What else can you do to help with your symptoms ?
- Diet. Alcohol, tomatoes, spices, carbonated drinks, chocolate, caffeine, citrus fruits and drinks, pickled foods, artificial sweeteners and acidic foods may irritate your bladder. That makes symptoms worse. Try removing these things from your diet for a couple of weeks. Then try eating one food at a time to see if it makes your symptoms worse.
- Smoking. Many people who have interstitial cystitis find that smoking makes their symptoms worse. Because smoking is also a main cause of bladder cancer, people who have interstitial cystitis have another good reason to quit smoking.
- Bladder training. Many people can train their bladder to urinate less often. You can train your bladder by going to the bathroom at scheduled times and using relaxation techniques.
- Physical therapy and biofeedback. People who have interstitial cystitis may have painful spasms of pelvic floor muscles. If you have muscle spasms, you can learn exercises to help strengthen and relax your pelvic floor muscles.
- TENS (transcutaneous electrical nerve stimulation). You can use a TENS machine to put mild electrical pulses into your body through special wires. Some doctors think that electrical pulses increase blood flow to the bladder. The increased blood flow strengthens the muscles that help control the bladder. It also releases hormones that block pain.
- Support group. You might consider joining a support group. The support of family, friends and other people who have interstitial cystitis can help you cope. People who learn about interstitial cystitis and participate in their own care do better than people who do not. A support group can provide you and your family with helpful tips and additional information.
- Interstitial Cystitis/Painful Bladder Syndrome. Am Fam Physician. 2011 May 15;83(10):1175-1181. http://www.aafp.org/afp/2011/0515/p1175.html[↩][↩][↩][↩][↩][↩]
- Interstitial Cystitis. Medline Plus. https://medlineplus.gov/interstitialcystitis.html [↩]
- Interstitial Cystitis. American Academy of Family Physicians. https://familydoctor.org/condition/interstitial-cystitis[↩]
- 4 to 12 Million May Have IC. Interstitial Cystitis Association. https://www.ichelp.org/about-ic/what-is-interstitial-cystitis/4-to-12-million-may-have-ic/[↩]
- What is Interstitial Cystitis (IC)? Interstitial Cystitis Association. https://www.ichelp.org/about-ic/what-is-interstitial-cystitis/[↩]
- Sant GR. Etiology, pathogenesis, and diagnosis of interstitial cystitis. Rev Urol. 2002;4 (suppl 1):S9–S15.[↩][↩][↩]
- Evans RJ, Sant GR. Current diagnosis of interstitial cystitis: an evolving paradigm. Urology. 2007;69(4 suppl):64–72.[↩][↩][↩]
- Rosenberg MT, Hazzard M. Prevalence of interstitial cystitis symptoms in women: a population based study in the primary care office. J Urol. 2005;174(6):2231–2234.[↩]
- Parsons CL, Dell J, Stanford EJ, et al. Increased prevalence of interstitial cystitis: previously unrecognized urologic and gynecologic cases identified using a new symptom questionnaire and intravesical potassium sensitivity. Urology. 2002;60(4):573–578.[↩]
- Parsons CL. The role of the urinary epithelium in the pathogenesis of interstitial cystitis/prostatitis/urethritis. Urology. 2007;69(4 suppl):9–16.[↩][↩]
- Parsons CL. Prostatitis, interstitial cystitis, chronic pelvic pain, and urethral syndrome share a common pathophysiology: lower urinary dysfunctional epithelium and potassium recycling. Urology. 2003;62(6):976–982.[↩][↩]
- Hurst RE, Moldwin RM, Mulholland SG. Bladder defense molecules, urothelial differentiation, urinary biomarkers, and interstitial cystitis. Urology. 2007;69(4 suppl):17–23.[↩]
- Parsons CL, Greene RA, Chung M, Stanford EJ, Singh G. Abnormal urinary potassium metabolism in patients with interstitial cystitis. J Urol. 2005;173(4):1182–1185.[↩][↩]
- Sant GR, Kempuraj D, Marchand JE, Theoharides TC. The mast cell in interstitial cystitis: role in pathophysiology and pathogenesis. Urology. 2007;69(4 suppl):34–40.[↩][↩]
- Theoharides TC, Kempuraj D, Sant GR. Mast cell involvement in interstitial cystitis: a review of human and experimental evidence. Urology. 2001;57(6 suppl 1):47–55.[↩]
- Parsons CL. Argument for the use of the potassium sensitivity test in the diagnosis of interstitial cystitis. For. Int Urogynecol J Pelvic Floor Dysfunct. 2005;16(6):430–431.[↩]
- Parsons CL, Stein PC, Bidair M, Lebow D. Abnormal sensitivity to intravesical potassium in interstitial cystitis and radiation cystitis. Neurourol Urodyn. 1994;13(5):515–520.[↩]
- Parsons CL. Interstitial cystitis and lower urinary tract symptoms in males and females–the combined role of potassium and epithelial dysfunction. Rev Urol. 2002;4 (suppl 1):S49–S55.[↩]
- Gillenwater JY, Wein AJ. Summary of the National Institute of Arthritis, Diabetes, Digestive and Kidney Diseases Workshop on Interstitial Cystitis, National Institutes of Health, Bethesda, Maryland, August 28–29, 1987. J Urol. 1988;140(1):203–206.[↩]
- van de Merwe JP, Nordling J, Bouchelouche P, et al. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: an ESSIC proposal. Eur Urol. 2008;53(1):60–67.[↩]
- Moldwin RM, Evans RJ, Stanford EJ, Rosenberg MT. Rational approaches to the treatment of patients with interstitial cystitis. Urology. 2007;69(4 suppl):73–81.[↩][↩][↩][↩][↩]
- van Ophoven A, Pokupic S, Heinecke A, Hertle L. A prospective, randomized, placebo controlled, double-blind study of amitriptyline for the treatment of interstitial cystitis. J Urol. 2004;172(2):533–536.[↩][↩]
- Thilagarajah R, Witherow RO, Walker MM. Oral cimetidine gives effective symptom relief in painful bladder disease: a prospective, randomized, double-blind placebo-controlled trial. BJU Int. 2001;87(3):207–212.[↩]
- Sairanen J, Tammela TL, Leppilahti M, et al. Cyclosporine A and pentosan polysulfate sodium for the treatment of interstitial cystitis: a randomized comparative study. J Urol. 2005;174(6):2235–2238.[↩][↩]
- Davis EL, El Khoudary SR, Talbott EO, Davis J, Regan LJ. Safety and efficacy of the use of intravesical and oral pentosan polysulfate sodium for interstitial cystitis: a randomized double-blind clinical trial. J Urol. 2008;179(1):177–185.[↩][↩]
- Kelada E, Jones A. Interstitial cystitis. Arch Gynecol Obstet. 2007;275(4):223–229.[↩]
- Dawson TE, Jamison J. Intravesical treatments for painful bladder syndrome/interstitial cystitis. Cochrane Database Syst Rev. 2007;(4):CD006113.[↩]
- Riedl CR, Engelhardt PF, Daha KL, Morakis N, Pflüger H. Hyaluronan treatment of interstitial cystitis/painful bladder syndrome. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):717–721.[↩]
- Peters KM, Feber KM, Bennett RC. A prospective, single-blind, randomized crossover trial of sacral vs pudendal nerve stimulation for interstitial cystitis. BJU Int. 2007;100(4):835–839.[↩]
- Shorter B, Lesser M, Moldwin RM, Kushner L. Effect of comestibles on symptoms of interstitial cystitis. J Urol. 2007;178(1):145–152.[↩]
- Theoharides TC, Sant GR. A pilot open label study of Cystoprotek in interstitial cystitis. Int J Immunopathol Pharmacol. 2005;18(1):183–188.[↩]
- Yong SM, Dublin N, Pickard R, Cody DJ, Neal DE, N’Dow J. Urinary diversion and bladder reconstruction/replacement using intestinal segments for intractable incontinence or following cystectomy. Cochrane Database Syst Rev. 2003;(1):CD003306.[↩]





{kind=link}