Contents
- What causes blisters on tongue
- Can you get genital herpes from a fever blister on tongue (cold sore) ?
- What are the clinical features of herpes simplex infection ?
- Who gets herpes simplex ?
- How is herpes simplex diagnosed ?
- What are the complications of herpes simplex ?
- What is the treatment for blister on my tongue ?
- Episodic Oral Treatment for Primary Herpetic Gingivostomatitis (Gums)
- Episodic Oral Treatment for Recurrent Herpes Labialis (Lips)
- Episodic Topical Treatment for Recurrent Herpes Labialis (lips)
- Oral Treatment to Prevent Herpes Labialis (lips) Recurrences
- Home remedies for fever blisters
- Outlook (Prognosis) for fever blister
- Can fever blister on my tongue be prevented ?
What causes blisters on tongue
Blisters on your tongue are also known as cold sore or herpetic stomatitis, is caused by a contagious virus called herpes simplex virus (HSV) 1. There are two types of herpes simplex virus – Herpes Simplex Virus Type 1 (HSV-1) usually causes oral herpes or cold sores. Some people call them fever blisters, but you don’t have to have a fever to have one. Whilst others called them cold sores, you don’t need to have a cold to get one, either. Type 1 Herpes Simplex Virus infects more than half of the U.S. population by the time they reach their 20’s. Type 2 Herpes Simplex Virus usually affects the genital area, but could also infect the oral mucosa (your mouth, tongue and lips), though this is much less common and does not tend to become recurrent 2. People can catch HSV-1 by kissing a person with a cold sore or sharing a drinking glass or utensils, so it’s easy to see why there are so many cold sores around. If someone you know has a cold sore, don’t kiss him or her and don’t drink out of the same glass or use the same knife, fork, or spoon. Sharing towels, washcloths, or napkins is off-limits, too, because the virus may survive on the fabric.
- Both of these viruses can affect your mouth or genitals and can be spread by oral sex. Cold sores are contagious even if you don’t see the sores.
- There is no cure for fever blisters (cold sores). They normally go away on their own in a few weeks. Antiviral medicines can help them heal faster. They can also help to prevent fever blister in people who often get them. Other medicines can help with the pain and discomfort of the sores. These include ointments that numb the blisters, soften the crusts of the sores, or dry them out. Protecting your lips from the sun with sunblock lip balm can also help.
- A history of cold sores was reported in 25.6 percent of freshmen and 28 percent of fourth-year students. Significant predictors of HSV-1 antibodies in this population were female sex, sexual intercourse before 15 years of age, greater total years of sexual activity, history of a partner with oral sores, and personal history of a non-HSV sexually transmitted disease 3.
Fever blister is characterized by an eruption of small and usually painful blisters on the skin of the lips, mouth, gums, tongue or the skin around the mouth. A fever blister is highly contagious. On the other hand a canker sore is a benign, open sore in the mouth, which appears as a painful white or yellow sore (ulcer) surrounded by a bright red area, which is not contagious. A fever blister is very different from a canker sore, although they both develop in close proximity in area of the mouth.
Some people have no symptoms from the fever blister infection. But others develop painful and unsightly cold sores. Cold sores usually occur outside the mouth, on or around the lips. When they are inside the mouth, they are usually on the gums or the roof of the mouth. They are not the same as canker sores, which are not contagious.
Herpes viruses spread most easily from individuals with an active outbreak or sore. You can catch this virus if you:
- Have intimate or personal contact with someone who is infected
- Touch an open herpes sore or something that has been in contact with the herpes virus, such as infected razors, towels, dishes, and other shared items.
Young children commonly get it when they are first exposed to Herpes Simplex Virus (HSV). The first outbreak is usually the most severe. Herpes Simplex Virus (HSV) can easily be spread from one child to another. Parents may spread the virus to their children during regular daily activities. Kids who get infected with HSV-1 may get cold sores occasionally for the rest of their lives. That’s because even after the sores themselves dry up and go away, the virus stays in the body, waiting around for another time to come out and cause more sores. When a cold sore reappears, it is often in the same place as the previous one.
When to see a doctor
Cold sores generally clear up without treatment. See your doctor if:
- You have a weakened immune system
- The cold sores don’t heal within two weeks
- Symptoms are severe
- You have frequent recurrences of cold sores
- You experience irritation in your eyes.
A cold sore usually passes through several stages
Warning symptoms
- Tingling and itching. Many people feel an itching, burning or tingling sensation around their lips for a day or so before a small, hard, painful spot appears and blisters erupt.
- Itching of the lips or skin around the mouth
- Burning near the lips or mouth area
- Tingling near the lips or mouth area.
Before blisters appear, you may have:
- Sore throat
- Fever
- Swollen glands
- Painful swallowing
Blisters or a rash stage
Blisters. Small fluid-filled blisters typically break out along the border where the outside edge of the lips meets the skin of the face. Cold sores can also occur around the nose or on the cheeks.
Blisters or a rash may form on your:
- Gums
- Lips
- Mouth
- Throat
Many blisters are called an outbreak. You may have:
- Red blisters that break open and leak
- Small blisters filled with clear yellowish fluid
- Several smaller blisters that may grow together into a large blister
- Yellow and crusty blister as it heals, which eventually turns into pink skin.
Oozing and crusting stage
Oozing and crusting. The small blisters may merge and then burst, leaving shallow open sores that will ooze fluid and then crust over.
Can you get genital herpes from a fever blister on tongue (cold sore) ?
Yes — it is possible to get genital herpes from oral sex.
Genital herpes is caused by the herpes simplex virus (HSV). There are two types of herpes viruses — HSV-1 and HSV-2. Genital herpes is usually caused by HSV-2; oral herpes (cold sores) is usually caused by HSV-1.
However, genital herpes can also be caused by HSV-1. Someone with HSV-1 can transmit the virus through oral contact with another person’s genitals, anus, or mouth, even if they don’t have sores that are visible at the time.
Other than abstinence (not having sex) the best way to help prevent herpes is to use a condom during any type of sex (oral, vaginal, or anal). Girls should have their partners use a dental dam every time they receive oral sex to help protect against genital herpes. And if either partner has a sore, it’s best to not have sex until the sore has cleared up.
Figure 1. Blister on tip of tongue

Figure 2. Herpes simplex infection on lips

Figure 3. Blisters under tongue
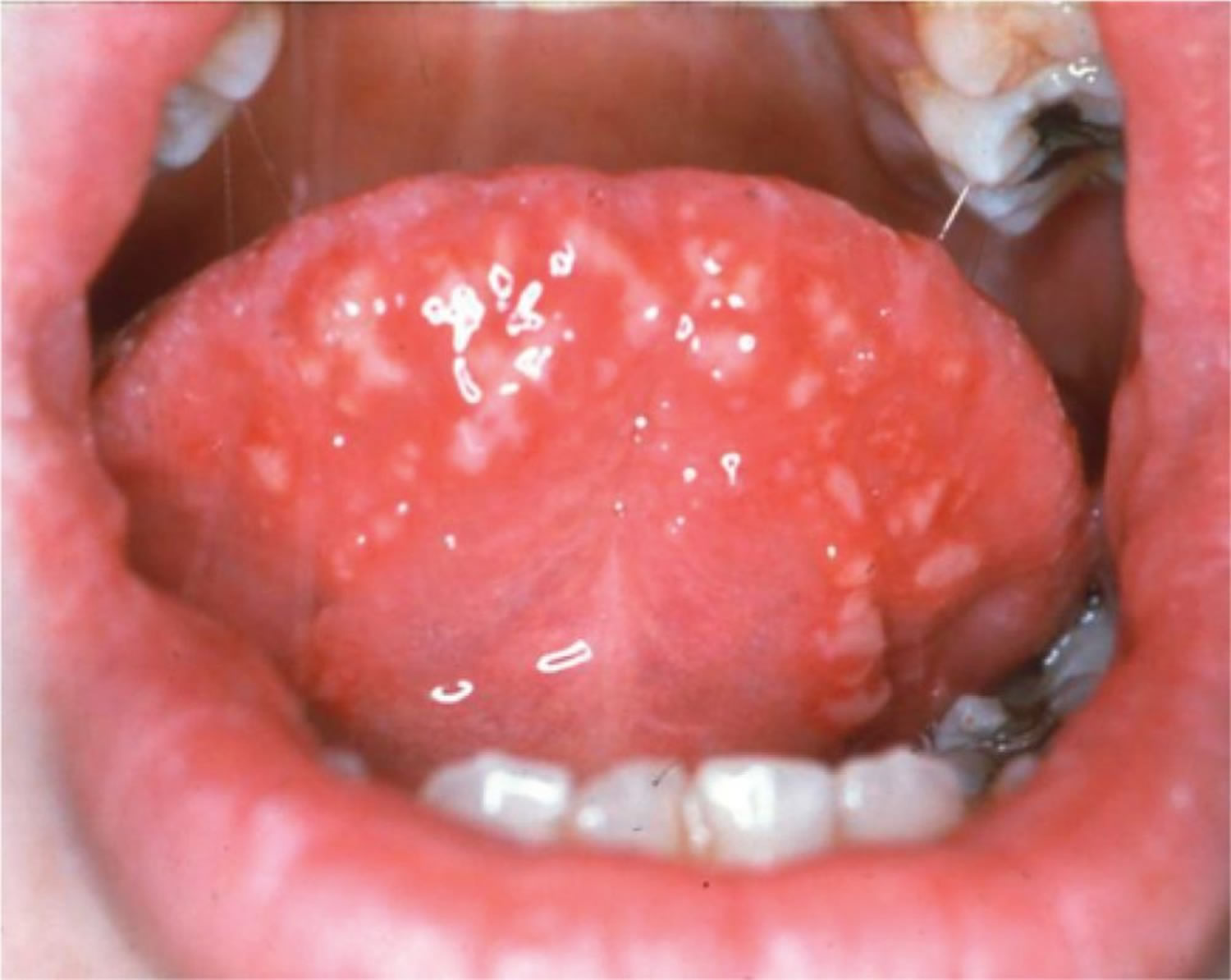
Figure 4. Fever blister on tongue and inside upper lip

What causes blisters on tongue (herpes simplex) ?
Herpes simplex is caused by one of two types of herpes simplex virus (HSV), members of the Herpesvirales family of double-stranded DNA viruses.
- Type 1 Herpes Simplex Virus is mainly associated with oral and facial infections
- Type 2 Herpes Simplex Virus is mainly associated with genital and rectal infections (anogenital herpes)
However, either virus can affect almost any area of skin or mucous membrane.
After the primary episode of infection, Herpes Simplex Virus (HSV) resides in a latent state in spinal dorsal root nerves that supply sensation to the skin. During a recurrence, the virus follows the nerves onto the skin or mucous membranes, where it multiplies, causing the clinical lesion. After each attack and lifelong, it enters the resting state.
During an attack, the virus can be inoculated into new sites of skin, which can then develop blisters as well as the original site of infection.
Risk factors of fever blister
About 90 percent of adults worldwide — even those who’ve never had symptoms of an infection — test positive for evidence of the virus that causes cold sores.
People who have weakened immune systems are at higher risk of complications from the virus. Medical conditions and treatments that increase your risk of complications include:
- HIV/AIDS
- Severe burns
- Eczema
- Cancer chemotherapy
- Anti-rejection drugs for organ transplants.
What are the clinical features of herpes simplex infection ?
Primary herpes simplex
Primary infection with HSV can be mild or subclinical, but symptomatic infection tends to be more severe than recurrences. Type 2 HSV is more often symptomatic than Type 1 HSV.
Primary Type 1 HSV most often presents as gingivostomatitis (an inflammation of the oral mucosa and gingiva), in children between 1 and 5 years of age. Symptoms include fever, which may be high, restlessness and excessive dribbling. Drinking and eating are painful and the breath is foul. The gums are swollen and red and bleed easily. Whitish vesicles evolve to yellowish ulcers on the tongue, throat, palate and inside the cheeks. Local lymph glands are enlarged and tender.
The fever subsides after 3–5 days and recovery is usually complete within 2 weeks.
Primary Type 2 HSV usually presents as genital herpes after the onset of sexual activity. Painful vesicles, ulcers, redness and swelling last for 2 to 3 weeks, if untreated, and are often accompanied by fever and tender inguinal lymphadenopathy (swollen lymph nodes in your groin)..
In males, herpes most often affects the glans, foreskin and shaft of the penis. Anal herpes is more common in males who have sex with men than with heterosexual partners.
In females, herpes most often arises on the vulva and in the vagina. It is often painful or difficult to pass urine. Infection of the cervix may progress to severe ulceration.
Recurrent herpes simplex
After the initial infection, whether symptomatic or not, there may be no further clinical manifestations throughout life. Where viral immunity is insufficient, recurrent infections are common, particularly with Type 2 genital herpes.
Recurrences can be triggered by:
- Minor trauma, surgery or procedures to the affected area
- Upper respiratory tract infections
- Sun exposure
- Hormonal factors (in women, flares are not uncommon prior to menstruation)
- Emotional stress
In many cases, no reason for the eruption is evident.
The vesicles tend to be smaller and more closely grouped in recurrent herpes, compared to primary herpes. They usually return to roughly the same site as the primary infection.
- Recurrent Type 1 HSV can occur on any site, most frequently the face, particularly the lips (herpes simplex labialis).
- Recurrent Type 2 HSV may also occur on any site, but most often affects the genitals or buttocks.
Itching or burning is followed an hour or two later by an irregular cluster of small, closely grouped, often umbilicated vesicles on a red base. They normally heal in 7–10 days without scarring. The affected person may feel well or suffer from fever, pain and have enlarged local lymph nodes.
Herpetic vesicles are sometimes arranged in a line rather like shingles, and are said to have a zosteriform distribution, particularly when affecting the lower chest or lumbar region.
White patches or scars may occur at the site of recurrent HSV attacks, and are more obvious in those with skin of color.
Who gets herpes simplex ?
Primary attacks of Type 1 Herpes Simplex Virus infections occur mainly in infants and young children. In crowded, underdeveloped areas of the world, nearly all children have been infected by the age of 5. In less crowded places, the incidence is lower, for example less than half of university entrants in Britain have been infected. Type 2 HSV infections occur mainly after puberty, and are often transmitted sexually.
HSV is transmitted by direct or indirect contact with someone with active herpes simplex, which is infectious for 7–12 days. Asymptomatic shedding of the virus in saliva or genital secretions can also lead to transmission of Herpes Simplex Virus (HSV), but this is infrequent, as the amount shed from inactive lesions is 100 to 1000 times less than when it is active. The incubation period is 2–12 days.
Minor injury helps inoculate Herpes Simplex Virus into the skin. For example:
- A thumb sucker may transmit the virus from their mouth to their thumb.
- A health-care worker may develop herpetic whitlow (paronychia)
- A rugby player may get a cluster of blisters on one cheek (‘scrum pox’).
How is herpes simplex diagnosed ?
If there is clinical doubt, HSV can be confirmed by culture or PCR (polymerase chain reaction: a technique in molecular genetics that permits the analysis of any short sequence of DNA or RNA) of a viral swab taken from fresh vesicles. HSV serology is not very informative, as it’s positive in most individuals and thus not specific for the lesion with which they present.
What are the complications of herpes simplex ?
Eye infection
Herpes simplex may cause swollen eyelids and conjunctivitis with opacity and superficial ulceration of the cornea (dendritic ulcer).
Throat infection
Throat infections may be very painful and interfere with swallowing.
Eczema herpeticum
In patients with a history of atopic dermatitis or Darier disease, HSV may result in severe and widespread infection, known as eczema herpeticum. The skin disease can be active or historical. Numerous blisters erupt on the face or elsewhere, associated with swollen lymph glands and fever.
Erythema multiforme
A single episode or recurrent erythema multiforme is an uncommon reaction to herpes simplex. The rash of erythema multiforme appears as symmetrical plaques on hands, forearms, feet and lower legs. It is characterised by target lesions, which sometimes have central blisters. Mucosal lesions may be observed.
Nervous system
Cranial/facial nerves may be infected by HSV, producing temporary paralysis of the affected muscles. Rarely, neuralgic pain may precede each recurrence of herpes by 1 or 2 days (Maurice syndrome). Meningitis is rare.
Widespread infection
Disseminated infection and/or persistent ulceration due to HSV can be serious in debilitated or immune deficient patients, eg people with human immunodeficiency virus (HIV) infection.
What is the treatment for blister on my tongue ?
Mild uncomplicated eruptions of herpes simplex require no treatment. Blisters may be covered if desired, e.g. with a hydrocolloid patch. Severe infection may require treatment with an antiviral agent.
Antiviral drugs used for herpes simplex and their usual doses are:
- Aciclovir – 200 mg 5 times daily for 5 days
- Valaciclovir – 1 g 3 times daily for 7 days
- Famciclovir – as a single dose of 3 x 500 mg
Higher doses are used for eczema herpeticum or for disseminated herpes simplex.
Topical aciclovir or penciclovir may shorten attacks of recurrent herpes simplex, provided the cream is started early enough.
The following steps can also help make you feel better:
- Apply ice or a warm washcloth to the sores to help ease pain.
- Wash the blisters gently with germ-fighting (antiseptic) soap and water. This helps prevent spreading the virus to other body areas.
- Avoid hot beverages, spicy and salty foods, and citrus.
- Gargle with cool water or eat popsicles.
- Rinse with salt water.
- Take a pain reliever such as acetaminophen (Tylenol).
Episodic Oral Treatment for Primary Herpetic Gingivostomatitis (Gums)
Oral acyclovir suspension (Zovirax; 15 mg per kg five times per day for seven days) can be used to treat herpetic gingivostomatitis in young children. In one randomized controlled trial, children receiving acyclovir had oral lesions for a shorter time than children receiving placebo (median of four versus 10 days). The treatment group also had earlier resolution of the following signs and symptoms: fever (one versus three days); eating difficulties (four versus seven days); and drinking difficulties (three versus six days) 4. Viral shedding was significantly shorter in the group treated with acyclovir (one versus five days) 4. Children should be treated symptomatically with oral analgesics and cold, soothing foods such as ice pops and ice cream. Various concoctions of topical anesthetics and other medications have been used to numb the painful ulcers so that children can be kept well hydrated.
Episodic Oral Treatment for Recurrent Herpes Labialis (Lips)
In a Cochrane review on the treatment of herpes labialis in patients receiving cancer treatment, acyclovir was found to be effective with regard to viral shedding (median of 2.5 versus 17.0 days); time to first decrease in pain (median of three versus 16 days); complete resolution of pain (9.9 versus 13.6 days); and total healing (median of 13.9 versus 20.7 days) 5. The brief period of viral replication in recurrent herpes labialis lesions suggests short therapeutic regimens should produce good results. In one randomized controlled trial, 701 patients self-initiated therapy with famciclovir (Famvir; 1,500 mg once [single dose] or 750 mg twice per day for one day [single day]) or placebo within one hour of prodromal symptoms onset 6. Median healing times of primary (first to appear) vesicular lesions in the famciclovir single-dose, famciclovir single-day, and placebo groups were 4.4, 4.0, and 6.2 days, respectively 6. Famciclovir showed decreased healing times, with no significant difference between the divided- or single-dose famciclovir treatment groups 6.
In one randomized controlled trial of recurrent herpes labialis, treatment with oral valacyclovir (Valtrex) plus topical clobetasol (Temovate) was compared with placebo 7. The patients took oral valacyclovir (2 g twice for one day) and applied clobetasol 0.05% gel (twice per day for three days) at onset of symptoms. There were more aborted lesions in the valacyclovirclobetasol group compared with the placebo-placebo group (50 versus 15.8 percent). Combination therapy reduced the mean maximum lesion size (9.7 versus 54 mm) and the mean healing time (5.8 versus 9.3 days) of classic lesions 7.
Episodic Topical Treatment for Recurrent Herpes Labialis (lips)
Topical treatment for herpes labialis is less effective than oral treatment. An randomized controlled trial of treatment with topical penciclovir 1% cream (Denavir) showed healing was marginally faster in the penciclovir group compared with placebo (4.8 versus 5.5 days) 8. The participants were adults in otherwise good health who had at least three episodes of herpes labialis per year. They applied penciclovir cream or placebo within one hour of the first sign or symptom of a recurrence, and then every two hours while awake for four days. Resolution of symptoms occurred more rapidly in the penciclovir group regardless of whether the medication was applied in the early or late stage. Penciclovir cream applied every two hours while awake reduced median duration of pain from 4.1 to 3.5 days, sped up the healing of classic lesions (e.g., vesicles, ulcers, crusts) from 5.5 to 4.8 days, and did not change median time of viral shedding (median of three versus three days) 8.
Docosanol cream (Abreva) is a saturated, 22-carbon, aliphatic alcohol with antiviral activity. It is available without prescription. One randomized controlled trial of 743 patients with herpes labialis showed a faster healing time in patients treated with docosanol 10% cream compared with placebo cream (4.1 versus 4.8 days), as well as reduced duration of pain symptoms (2.2 versus 2.7 days) 9. More than 90 percent of patients in both groups healed completely within 10 days 10. Treatment with docosanol cream, when applied five times per day and within 12 hours of episode onset, is safe and somewhat effective.
An randomized controlled trial of healthy adults with a history of frequent herpes labialis recurrences evaluated treatment with 5% acyclovir cream versus a vehicle control 11. Participants were told to self-initiate treatment five times per day for four days, beginning within one hour of the onset of a recurrent episode. In study 1, the mean duration of episodes was 4.3 days for patients treated with acyclovir cream and 4.8 days for those treated with the vehicle control 11. In study 2, the mean duration of episodes was 4.6 days for patients treated with acyclovir and 5.2 days for those treated with the vehicle control 11.
Oral Treatment to Prevent Herpes Labialis (lips) Recurrences
Oral acyclovir is effective in suppressing herpes labialis in immunocompetent adults with frequent recurrences. In one randomized controlled trial, treatment with oral acyclovir (400 mg twice per day) resulted in a 53 percent reduction in the number of clinical recurrences and a 71 percent reduction in virus culture-positive recurrences compared with placebo 12. The median time to first clinically documented recurrence was 46 days for placebo courses and 118 days for acyclovir courses 12. The mean number of recurrences per four-month treatment period was 1.80 episodes per patient during placebo treatment and 0.85 episodes per patient during acyclovir treatment 12.
Treatment with oral valacyclovir (500 mg per day) for 16 weeks was compared with placebo in the suppression of herpes labialis in patients with a history of four or more recurrent lesions in the previous year 13. Results showed 60 percent of persons in the valacyclovir group were recurrence-free throughout the study period compared with 38 percent in the placebo group. The mean time to first recurrence was longer with valacyclovir (13.1 weeks) compared with placebo (9.6 weeks) 13.
In a Cochrane review of herpes labialis prevention in patients receiving treatment for cancer, acyclovir was found to be effective in the prevention of HSV infections, as measured by oral lesions or viral isolates (relative risk = 0.16 and 0.17, respectively) 5. There also was no evidence that valacyclovir is more effective than acyclovir. In another study, daily valacyclovir (500 mg per day) and acyclovir (400 mg twice per day) were equally effective in the prevention of recurrent HSV eye disease 14.
Table 1. Treatments for Oral Herpes (lips and oral mucosa) – Summary
| Drug | Dose or dosage | Cost of generic (brand)* | Evidence rating† | References |
|---|---|---|---|---|
Episodic oral treatment for recurrences‡ | ||||
Acyclovir (Zovirax) | 200 mg five times per day or 400 mg three times per day for five days | 200 mg: $23 ($154)§ 400 mg: $13 ($87) | A | |
Famciclovir (Famvir) | 1,500 mg once for one day | $173 ($158) | B | |
Valacyclovir (Valtrex) | 2 g twice for one day | $56 ($74) | B | |
Episodic topical treatment for recurrences‡ | ||||
Acyclovir cream | Apply five times per day for four days | 2-g tube: NA ($69) | B | |
Docosanol cream (Abreva) | Apply five times per day until healed | 2-g tube: NA ($15)∥ | B | |
Penciclovir cream (Denavir) | Apply every two hours while awake for four days | 1.5-g tube: NA ($54) | B | |
Treatment to prevent recurrences | ||||
Acyclovir | 400 mg twice per day (ongoing) | 30-day supply: $29 ($345) | A | |
Valacyclovir | 500 mg once per day (ongoing) | 30-day supply: $186 ($234) | B | |
NA = not available.
*—Estimated retail price of treatment based on information obtained at http://www.drugstore.com. Generic price listed first; brand price listed in parentheses.
†—A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series.
‡—Most effective if treatment is started at the onset of symptoms.
§—In retail discount program (200 mg only): may be available at discounted price ($10 or less) at one or more national retail chains.
∥—Available as brand product without a prescription.
Home remedies for fever blisters
To ease the discomfort of a cold sore, you may want to try the following tips:
- Apply a cold sore ointment. Docosanol (Abreva) is an over-the-counter cream for cold sores. It must be applied frequently and may shorten an outbreak by a few hours or a day.
- Try other cold sore remedies. Some over-the-counter preparations contain a drying agent, such as alcohol, that may speed healing.
- Use lip balms and cream. Protect your lips from the sun with a zinc oxide cream or lip balm with sunblock. If your lips become dry, apply a moisturizing cream.
- Apply a cool compress. A cool, damp cloth may reduce redness, help remove crusting and promote healing.
- Apply pain-relieving creams. Over-the-counter creams with lidocaine or benzocaine may offer some pain relief.
- Stress reduction. If your cold sores are triggered by stress, you might want to try relaxation techniques, such as deep-breathing exercises and meditation.
Alternative medicine
Although study results have been mixed, alternative medicine treatments for cold sores include:
- Lysine. An amino acid, lysine is available as an oral supplement and as a cream.
- Propolis. Also known as synthetic beeswax, this is available as a 3 percent ointment. When applied early and often, it may shorten the duration of the breakout.
- Rhubarb and sage. A cream combining rhubarb and sage may be about as effective as acyclovir (Zovirax) cream.
Outlook (Prognosis) for fever blister
Oral herpes most often goes away by itself in 1 to 2 weeks. However, it may come back.
Herpes infection may be severe and dangerous if:
- It occurs in or near the eye.
- You have a weakened immune system due to certain diseases and medicines.
Can fever blister on my tongue be prevented ?
As sun exposure often triggers facial herpes simplex, sun protection using high protection factor sunscreens and other measures are important.
Antiviral drugs will stop HSV multiplying once it reaches the skin or mucous membranes but cannot eradicate the virus from its resting stage within the nerve cells. They can therefore shorten and prevent attacks but a single course cannot prevent future attacks. Repeated courses may be prescribed or the medication may be taken continuously to prevent frequent attacks.
Here are some tips to prevent mouth sores:
- Apply sunblock or lip balm containing zinc oxide to your lips before you go outside.
- Apply a moisturizing balm to prevent the lips from becoming too dry.
- Avoid direct contact with herpes sores.
- Wash items such as towels and linens in boiling hot water after each use.
- Keep your hands clean. When you have a cold sore, wash your hands carefully before touching yourself and other people, especially babies.
- Do not share utensils, straws, glasses, or other items if someone has oral herpes.
Do not have oral sex if you have oral herpes, especially if you have blisters. You can spread the virus to the genitals. Both oral and genital herpes viruses can sometimes be spread, even when you do not have mouth sores or blisters.
- Fever blister. Medline Plus. https://medlineplus.gov/ency/imagepages/9325.htm[↩]
- Nongenital Herpes Simplex Virus. Am Fam Physician. 2010 Nov 1;82(9):1075-1082. http://www.aafp.org/afp/2010/1101/p1075.html[↩][↩]
- Gibson JJ, Hornung CA, Alexander GR, Lee FK, Potts WA, Nahmias AJ. A cross-sectional study of herpes simplex virus types 1 and 2 in college students: occurrence and determinants of infection. J Infect Dis. 1990;162(2):306–312.[↩]
- Amir J, Harel L, Smetana Z, Varsano I. Treatment of herpes simplex gingivostomatitis with aciclovir in children: a randomised double blind placebo controlled study. BMJ. 1997;314(7097):1800–1803.[↩][↩]
- Glenny AM, Fernandez Mauleffinch LM, Pavitt S, Walsh T. Interventions for the prevention and treatment of herpes simplex virus in patients being treated for cancer. Cochrane Database Syst Rev. 2009;(1):CD006706.[↩][↩][↩]
- Spruance SL, Bodsworth N, Resnick H, et al. Single-dose, patient-initiated famciclovir: a randomized, double-blind, placebo-controlled trial for episodic treatment of herpes labialis. J Am Acad Dermatol. 2006;55(1):47–53.[↩][↩][↩][↩]
- Hull C, McKeough M, Sebastian K, Kriesel J, Spruance S. Valacyclovir and topical clobetasol gel for the episodic treatment of herpes labialis: a patient-initiated, double-blind, placebo-controlled pilot trial. J Eur Acad Dermatol Venereol. 2009;23(3):263–267.[↩][↩][↩]
- Spruance SL, Rea TL, Thoming C, Tucker R, Saltzman R, Boon R. Penciclovir cream for the treatment of herpes simplex labialis. A randomized, multicenter, double-blind, placebo-controlled trial. Topical Penciclovir Collaborative Study Group. JAMA. 1997;277(17):1374–1379.[↩][↩][↩]
- Sacks SL, Thisted RA, Jones TM, et al.; Docosanol 10% Cream Study Group. Clinical efficacy of topical docosanol 10% cream for herpes simplex labialis: a multi-center, randomized, placebo-controlled trial. J Am Acad Dermatol. 2001;45(2):222–230[↩]
- Sacks SL, Thisted RA, Jones TM, et al.; Docosanol 10% Cream Study Group. Clinical efficacy of topical docosanol 10% cream for herpes simplex labialis: a multi-center, randomized, placebo-controlled trial. J Am Acad Dermatol. 2001;45(2):222–230.[↩][↩]
- Spruance SL, Nett R, Marbury T, Wolff R, Johnson J, Spaulding T. Acyclovir cream for treatment of herpes simplex labialis: results of two randomized, double-blind, vehicle-controlled, multicenter clinical trials. Antimicrob Agents Chemother. 2002;46(7):2238–2243.[↩][↩][↩][↩]
- Rooney JF, Straus SE, Mannix ML, et al. Oral acyclovir to suppress frequently recurrent herpes labialis. A double-blind, placebo-controlled trial. Ann Intern Med. 1993;118(4):268–272.[↩][↩][↩][↩]
- Baker D, Eisen D. Valacyclovir for prevention of recurrent herpes labialis: 2 double-blind, placebo-controlled studies. Cutis. 2003;71(3):239–242.[↩][↩][↩]
- Miserocchi E, Modorati G, Galli L, Rama P. Efficacy of valacyclovir vs acyclovir for the prevention of recurrent herpes simplex virus eye disease: a pilot study. Am J Ophthalmol. 2007;144(4):547–551.[↩]





{kind=link}