
Contents
Blocked tear duct
A blocked tear duct is when the eye’s drainage system for tears is either partially or completely obstructed. Tears cannot drain normally, causing a watery, irritated or chronically infected eye.
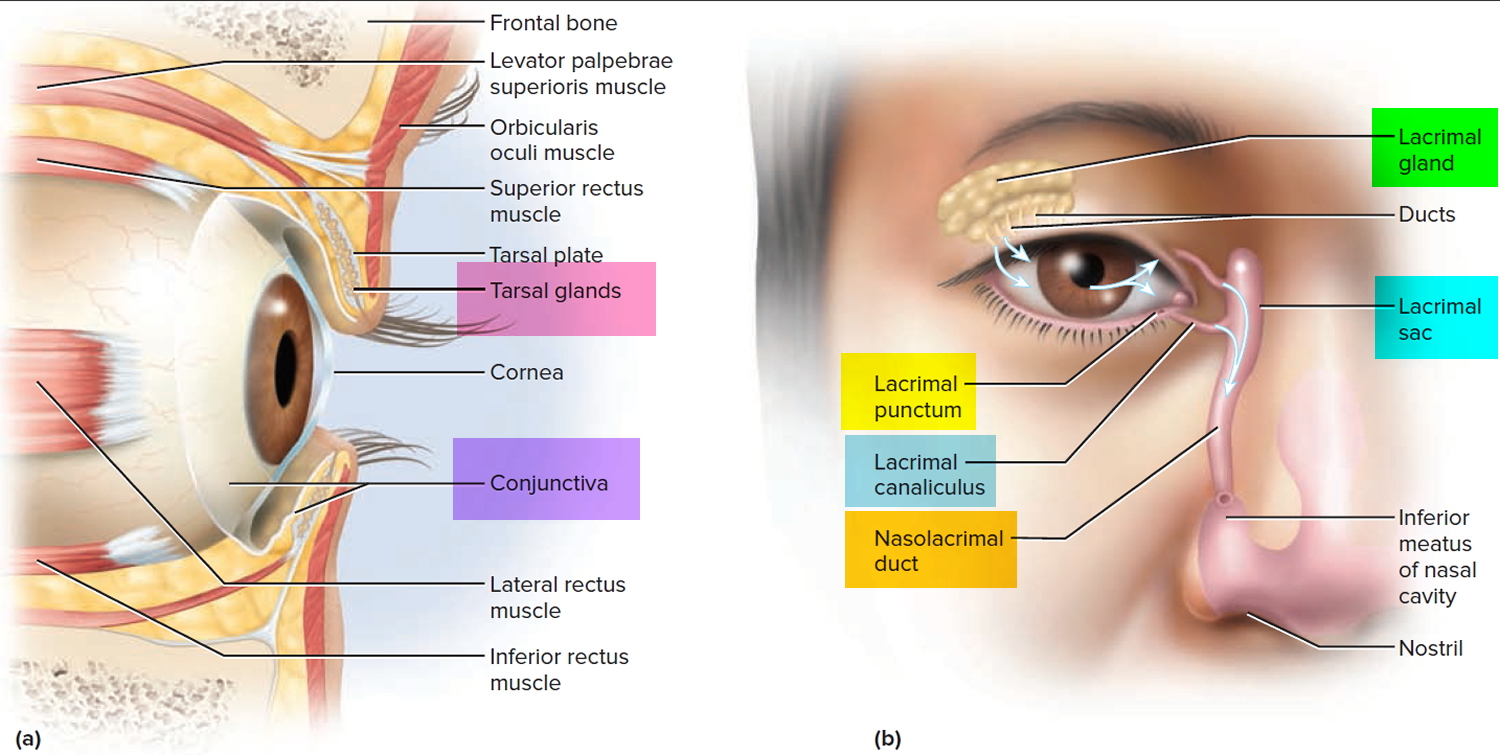
Most of your tears come from your lacrimal glands, which are located above each eye. The tears flow down the surface of your eye to lubricate and protect it, and then drain into tiny holes (puncta) in the corners of your upper and lower eyelids. The tears then travel through the small canals in the lids (canaliculi) to a sac where the lids are attached to the side of the nose (lacrimal sac), then down a duct (the nasolacrimal duct) before emptying into your nose, where they evaporate or are reabsorbed.
In adults, the tear duct obstruction can result from an eye infection, swelling, injury or a tumor.
Blocked tear duct newborn
A baby can be born with a blocked tear duct (a congenital blocked tear duct) and it affects almost 15-20 percent of normal newborns. It is estimated nearly 15-20 percent of newborns have a blocked tear duct, but the condition usually resolves on its own within four to six months. If the blockage persists past 4 to 6 months, the chances that it will open on its own are less than 20 percent and falling every day the child gets older. Most often, surgery is recommended before a year of age.
The lacrimal (tear) apparatus
The lacrimal (tear) apparatus (Figure 1) is a group of structures that produces and drains lacrimal fluid (tears) in a process called lacrimation. The lacrimal apparatus consists of the lacrimal (tear) gland and a series of ducts that drain the tears into the nasal cavity. The lacrimal gland, about the size and shape of an almond, is nestled in a shallow fossa of the frontal bone in the superolateral corner of the orbit. About 6-12 short ducts lead from the gland to the surface of the conjunctiva.
The lacrimal (tear) glands are supplied by parasympathetic fibers of the facial (VII) nerves. The lacrimal fluid produced by these glands is a watery solution containing salts, some mucus, and lysozyme, a protective bactericidal enzyme to prevent infection. Tear fluid protects, cleans, lubricates, moistens the eyeball and delivers oxygen and nutrients to the conjunctiva. After being secreted from the lacrimal gland, tear fluid is spread medially over the surface of the eyeball by the blinking of the eyelids. Each lacrimal gland produces about 1 mL of lacrimal fluid per day
After washing across the eye, tears collect near the medial commissure and flow into a tiny pore, the lacrimal punctum, on the margin of each eyelid. The punctum opens into a short lacrimal canaliculus, which leads to the lacrimal sac in the medial wall of the orbit. From this sac, a nasolacrimal duct carries the tears to the inferior meatus of the nasal cavity; thus an abundance of tears from crying or watery eyes can result in a runny nose. Once the tears enter the nasal cavity, they normally flow back to the throat and are swallowed.
An obstruction of the tear ducts may occur due to numerous reasons (aging, trauma, inflammatory conditions, medications and tumors) and cause numerous signs and symptoms ranging from wateriness or tearing to discharge, swelling, pain and infection. These signs and symptoms may result from the tear drainage system becoming obstructed at any point from the puncta to the nasal cavity.
Figure 1. Eyes tear glands and anatomy
Blocked tear duct complications
Because your tears aren’t draining the way they should, the tears that remain in the drainage system become stagnant. This promotes growth of bacteria, viruses and fungi, which can lead to recurrent eye infections and inflammation.
Any part of the tear drainage system, including the clear membrane over your eye surface (conjunctiva), can become infected or inflamed because of a blocked tear duct.
Blocked tear duct causes
A blockage can occur at any point in the tear drainage system. When that happens, your tears don’t drain properly, giving you watery eyes and increasing your risk of eye infections and inflammation.
Babies in utero have a thin membrane that seals the nasolacrimal duct. In newborns, a blocked tear duct may be the result of that membrane not opening as it should at birth.
Another cause of blocked tear duct may be chronic nose infections. Chronic sinusitis may irritate the tissues and form scars, which block the tear duct system.
Other causes of blocked tear duct:
- Abnormal development of the skull and face (craniofacial abnormalities), like those in Down syndrome or other disorders, increases the likelihood of blockage of the tear ducts.
- Age-related changes in older adults can cause blocked tear ducts, including narrowing of the punctal openings.
- Eyedrops. Rarely, long-term use of certain medications, such as eyedrops used to treat glaucoma, can cause a blocked tear duct.
- Nose trauma, such as a broken nose; scar tissue can block the tear duct.
- Injury or trauma. An injury to your face can cause bone damage or scarring near the drainage system, disrupting the normal flow of tears through the ducts. Even small particles of dirt or loose skin cells lodged in the duct can cause blockage.
- Nose polyps, a growth from the lining of the nose (affecting some people who have nasal allergies), can obstruct the tear duct system
- Conjunctivitis, infection and inflammation of the conjunctiva, the thin membrane covering the eye. In rare cases, the tear duct system may become infected and blocked, especially after some viral infections. Chronic infection or inflammation of your eyes, tear drainage system or nose can cause your tear ducts to become blocked.
- Tumor, a tumor in the nose or anywhere along the tear drainage system can cause blockage of the tear duct system and prevent drainage.
- Cancer treatments. A blocked tear duct is a possible side effect of chemotherapy medication and radiation treatment for cancer.
If your eye has been watery and leaking or is continually irritated or infected, you should see your ophthalmologist.
Risk factors for blocked tear duct
Certain factors increase your risk of developing a blocked tear duct:
- Age and sex. Older women are at highest risk of developing blocked tear ducts due to age-related changes.
- Chronic eye inflammation. If your eyes are continually irritated, red and inflamed (conjunctivitis), you’re at higher risk of developing a blocked tear duct.
- Previous surgery. Previous eye, eyelid, nasal or sinus surgery may have caused some scarring of the duct system, possibly resulting in a blocked tear duct later.
- Glaucoma. Anti-glaucoma medications are often used topically on the eye. If you’ve used these or other topical eye medications, you’re at higher risk of developing a blocked tear duct.
- Previous cancer treatment. If you’ve had radiation or chemotherapy to treat cancer, particularly if the radiation was focused on your face or head, you’re at higher risk of developing a blocked tear duct.
Prevention for blocked tear duct
To reduce your risk of developing a blocked tear duct later in life, get prompt treatment of eye inflammation or infections. Follow these tips to avoid eye infections in the first place:
- Wash your hands thoroughly and often.
- Try not to rub your eyes.
- Replace your eyeliner and mascara regularly. Never share these cosmetics with others.
- If you wear contact lenses, keep them clean according to recommendations provided by the manufacturer and your eye care specialist.
Blocked tear duct symptoms
If the tear passageways become blocked, tears cannot drain properly and may overflow from the eyelids onto the face as if you were crying. The symptoms of a blocked tear duct may get worse after a cold or sinus infection. Also, symptoms may be more noticeable after exposure to cold, wind or sunlight. In addition to excessive tearing you may also experience blurred vision, mucous discharge, eye irritation, and painful swelling in the inner corner of the eyelids. A thorough examination by an ophthalmic plastic surgeon can determine the cause of tearing and recommended treatment.
When tear ducts are blocked, trapped bacteria in the nasolacrimal sac can lead to infection (called dacryocystitis). Symptoms of infection include:
- Inflammation (swelling), tenderness and redness of the inside corner of the eye or around the eye and nose
- Recurrent eye infections or inflammation (pink eye)
- Eye mucus discharge
- Crusty eyelashes
- Blurred vision
- Blood-tinged tears
- Fever
Blocked tear duct diagnosis
To diagnosis your condition, your doctor talks with you about your symptoms, examines your eyes and does a few tests. He or she will also examine the inside of your nose to determine if any structural disorders of your nasal passages are causing an obstruction. If your doctor suspects a blocked tear duct, he or she may have you undergo other tests to find the location of the blockage.
Your eye doctor will also use certain tests to examine the tear drainage system for blockage. A special fluid is flushed into the affected tear duct opening and, if the fluid cannot be tasted in the throat, a blocked tear duct is diagnosed.
Other tests may include an X-ray or CT scan of the tear duct area (called a dacryocystogram).
Tests used to diagnose a blocked tear duct include:
- Tear drainage test. This test measures how quickly your tears are draining. One drop of a special dye is placed on the surface of each eye. You may have a blocked tear duct if after five minutes most of the dye is still on the surface of your eye.
- Irrigation and probing. Your doctor may flush a saline solution through your tear drainage system to check how well it’s draining. Or he or she may insert a slender instrument (probe) through the tiny drainage holes at the corner of your lid (puncta) to check for blockages. In some cases this probing may even fix the problem.
- Eye imaging tests. For these procedures, a contrast dye is passed from the puncta in the corner of your lid through your tear drainage system. Then X-ray, computerized tomography (CT) or magnetic resonance imaging (MRI) images are taken to find the location and cause of the blockage.
Blocked tear duct treatment
Depending on your symptoms and their severity, your specialist will suggest an appropriate course. In mild cases, a treatment of warm compresses and antibiotics may be recommended. In more severe cases, surgical intervention to bypass the tear duct obstruction (dacryocystorhinostomy surgery) may be recommended. A dacryocystorhinostomy is performed by creating a new tear passageway from the lacrimal sac to the nose, bypassing the obstruction. A small silicone tube called a stent may temporarily be placed in the new passageway to keep it open during the healing process. In a small percentage of cases, the obstruction is between the puncta and the lacrimal sac. In these cases, in addition to the dacryocystorhinostomy procedure, the surgeon will insert a tiny artificial tear drain called a Jones Tube. A Jones Tube is made of Pyrex glass and allows tears to drain directly from the eye to the lacrimal sac.
Dacryocystorhinostomy surgery is usually performed as an outpatient procedure. Patients usually have some bruising and swelling on the side of the nose that subsides in one to two weeks. In general, surgery has a greater than 90% success rate and most patients experience a resolution of their tearing and discharge problems once surgery and recovery are completed.
Blocked tear duct in adults treatment
In most cases of blocked tear ducts after a facial injury, the drainage system starts working again on its own a few months after the injury, and no additional treatment is necessary. Your ophthalmologist (eye doctor) may recommend waiting a few months after the injury before considering surgery to open the blocked tear duct.
Blocked tear duct infant treatment
Many babies with congenital blocked tear duct improve on their own in the first several months of life, after the drainage system matures or the extra membrane involving the nasolacrimal duct opens up. In some cases, your ophthalmologist (eye doctor) may recommend that you use a special massage technique to help open up the membrane covering the lower opening into your baby’s nose. He or she will demonstrate how to correctly do this massage.
The purpose of massage is to put pressure on the lacrimal sac to pop open the membrane at the bottom of the tear duct. This is most easily accomplished by placing your hands on each side of the baby’s face with your index finger(s) between the inner corner of the eye and the side of the nose, pressing in and down over the lacrimal sac for a few seconds. The massage should be done once in the morning and once in the evening, and each massage should be ten strokes each. It is best to do the massage during a diaper change.
Dilation, probing and flushing
For infants and toddlers whose blocked tear ducts aren’t opening on their own, or for adults who have a partially blocked duct or a partial narrowing of the puncta, a technique using dilation, probing and irrigation may be used. An instrument is used to enlarge (dilate) the punctal openings and a narrow probe is guided through the puncta, into the tear drainage system, then through the nasal opening and removed. The tear drainage system is flushed with a saline solution to clear out any residual blockage.
Balloon catheter dilation
A balloon catheter dilation procedure opens tear drainage passages that are narrowed or blocked by scarring or inflammation. General anesthesia is used. A narrow catheter (tube) with a deflated balloon on the tip is guided through the lower nasolacrimal duct. The doctor then uses a pump to inflate and deflate the balloon along the drainage system.
Stenting or intubation
With a procedure called stenting or intubation, tiny tubes are used to open up blockages and narrowing within the tear drainage system. Again, general anesthesia is usually used. Your ophthalmologist (eye doctor) threads a very thin tube through one or both puncta in the corner of your eye, all the way through the tear drainage system and out through your nose. A tiny loop of tubing remains at the corner of your eye, but while it is visible, it’s usually not bothersome. These tubes are generally left in for three to four months, and then removed.
Blocked tear duct surgery
Surgery is usually the preferred option for people who develop blocked tear ducts. It is also effective in babies and toddlers with congenital blocked tear ducts, though usually an option only after other treatments have been tried.
Dacryocystorhinostomy is the surgical procedure usually used to treat most cases of blocked tear ducts in adults and rarely in children. This technique creates a new route for tears to drain out through your nose normally again by developing a new connection between your lacrimal sac and your nose. First you’re given a general anesthetic, or a local anesthetic if it’s performed as an outpatient procedure. This new route bypasses the duct that empties into your nose (nasolacrimal duct), which is typically the blockage site. Stents or intubation typically are placed in the new route while it heals, and then removed three or four months after surgery. The steps in this procedure will vary depending on your particular tear duct blockage.
Depending on the type of blockage, your surgeon may recommend creating an entirely new route from the inside corner of your eyes (puncta) to your nose, bypassing the tear drainage system altogether. This reconstruction of your entire tear drainage system is called conjunctivodacryocystorhinostomy.
To prevent postoperative infection and inflammation, you will need to use a nasal decongestant spray and eye drops. After about three to six months, your ophthalmologist (eye doctor) will remove any stents that were put in place to keep the new channel open while healing.
If a tumor is causing your blocked tear duct, surgery may be performed to remove the tumor, or other treatments may be used to shrink it.
The steps in this procedure vary, depending on the exact location and extent of your blockage, as well as your surgeon’s experience and preferences.
- External. With external dacryocystorhinostomy, your surgeon makes an incision on the side of your nose, near where the lacrimal sac is located. After connecting the lacrimal sac to your nasal cavity and placing a stent in the new passageway, the surgeon closes up the skin incision with a few stitches.
- Endoscopic or endonasal. With this method, your surgeon uses a microscopic camera and other tiny instruments inserted through the nasal opening to your duct system. This method requires no incision so leaves no scar. But the success rates aren’t as high as with the external procedure.
Following surgery you’ll use a nasal decongestant spray and eyedrops to prevent infection and reduce inflammation. After three to six months, you’ll return to your doctor’s office for removal of any stents used to keep the new channel open during the healing process.
Surgery side effects
The main risks of tear duct surgery are recurrence of the blockage (in about 10 percent of cases), infection (which is extremely rare), and blood from the eye or the nose. The bleeding usually subsides in a few hours from surgery and is only a few drops of blood mixing with the tears.





{kind=link}