Contents
What is a blood transfusion
A blood transfusion is when you’re given blood from someone else (a donor) or from the patient’s own blood is transfused into the body to increase blood volume. Not all blood transfusions use blood donated from a stranger. If you’re going to have surgery, you may need a blood transfusion because of blood loss during the operation. If it’s surgery that you’re able to schedule months in advance, your doctor may ask whether you would like to use your own blood, rather than donated blood. If you choose to use your own blood, you will need to have blood drawn one or more times prior to the surgery. A blood bank will store your blood for your use.
A blood transfusion is a very safe and common procedure in which blood is given to you through an intravenous (IV) line in one of your blood vessels. A blood transfusion can be life-saving!
Blood volume varies with body size, percent adipose tissue, and changes in fluid and electrolyte concentrations. An average-size adult has a blood volume of about 5 liters (5.3 quarts), 4–5 liters in a female and 5–6 liters in a male.
Blood transfusions are done to replace blood lost during surgery or due to a serious injury. A transfusion also may be done if your body can’t make blood properly because of an illness.
Blood transfusions are very common. Each year, almost 5 million Americans need a blood transfusion. Most blood transfusions go well. Mild complications can occur. Very rarely, serious problems develop.
How long does a blood transfusion take?
During a blood transfusion, a small needle is used to insert an IV line into one of your blood vessels. Through this line, you receive healthy blood. The procedure usually takes 1 to 4 hours to receive 1 bag of blood. The time depends on how much blood you need and what part of the blood you receive.
What is autologous blood donation?
Autologous blood donation means to receive your own blood. This is normally the safest blood to receive. People of almost any age can donate for themselves, especially prior to surgery or a medical procedure. You may be able to donate for yourself, even if you are ineligible for allogeneic donation. Ask your physician if you are able to self-donate. Designated donation means to receive others’ blood, such as family or friends. Allogenic blood donation is available from the general blood supply (volunteer blood donation) and may be ordered for your needs by your physician. Various factors, such as donation constraints due to your medical condition, urgency, or lack of donors, may necessitate the use of this blood source.
Blood Banks
Blood banks collect, test, and store blood. They carefully screen all donated blood for possible infectious agents, such as viruses, that could make you sick.
Blood bank staff also screen each blood donation to find out whether it’s type A, B, AB, or O and whether it’s Rh-positive or Rh-negative. Getting a blood type that doesn’t work with your own blood type will make you very sick. That’s why blood banks are very careful when they test the blood.
To prepare blood for a transfusion, some blood banks remove white blood cells. This process is called white cell or leukocyte reduction. Although rare, some people are allergic to white blood cells in donated blood. Removing these cells makes allergic reactions less likely.
All blood transfused must meet the donor eligibility requirements established by the US Food and Drug Administration (FDA) and the American Association of Blood Banks. All donated units of blood are tested for evidence of viral or bacterial infections transmitted by blood:
- Hepatitis viruses B and C
- HIV-1 and HIV-2 viruses
- Human T-lymphotropic viruses (HTLV-1 and HTLV-2) — Rare viruses that cause diseases of the blood or nerves.
- Syphilis
- Chagas disease
- West Nile virus
What is Blood
Blood has many vital jobs. The heart pumps blood through a network of arteries and veins throughout the body. Blood transports a variety of materials between interior body cells and those that exchange substances with the external environment. Blood carries oxygen and other nutrients to your body’s organs and tissues. In this way, blood helps maintain stable internal environmental conditions. Having a healthy supply of blood is important to your overall health. Blood is composed of formed elements suspended in a fluid extracellular matrix called blood plasma. The “formed elements” include red blood cells, white blood cells, and cell fragments called platelets (Figure 2). Most blood cells form in red marrow within the hollow parts of certain long bones.
Blood is made up of various parts, most blood samples are about 45% red blood cells by volume. This percentage is called the hematocrit. The white blood cells and platelets account for less than 1% of blood volume. The remaining blood sample, about 55%, is the plasma, a clear, straw-colored liquid. Blood plasma is a complex mixture of water, gases, amino acids, proteins, carbohydrates, lipids, vitamins, hormones, electrolytes, and cellular wastes (see Figure 1).
Red blood cells carry oxygen to all parts of your body. They also remove carbon dioxide (a waste product) from your body’s cells and carry it to the lungs to be exhaled.
Red blood cells are made in your bone marrow—a sponge-like tissue inside the bones. White blood cells (WBCs) and platelets (thrombocytes) also are made in your bone marrow. White blood cells help fight infection. Platelets stick together to seal small cuts or breaks on blood vessel walls and stop bleeding.
Blood is transfused either as whole blood (with all its parts) or, more often, as individual parts.
- Red blood cells. These cells carry oxygen from your lungs to other body organs. They also carry carbon dioxide back to the lungs to be breathed out (exhaled). The body needs a certain number of these cells to work well. Bleeding due to injury, surgery, or disease may cause a low red blood cell count. This is the most common type of transfusion.
- White blood cells. These cells fight infections by destroying bacteria, viruses, and other germs. White blood cells are rarely transfused. They are often set aside as a short-term (temporary) treatment for people with a low white cell count and severe infection that has not responded to antibiotics.
- Platelets. These little pieces of blood cells help blood to clot. Your body may not make enough platelets. This might be due to bone marrow disorders, increased destruction of platelets, or medicines such as chemotherapy. Platelets may be transfused before a procedure that may cause a person with a low platelet count to bleed.
- Plasma. This fluid carries the blood cells all over the body. It contains proteins, vitamins, and minerals. Some of the proteins also help blood to clot. Plasma or fresh frozen plasma can be transfused in people who severely lack certain parts of the blood that help with clotting.
Figure 1. Blood composition


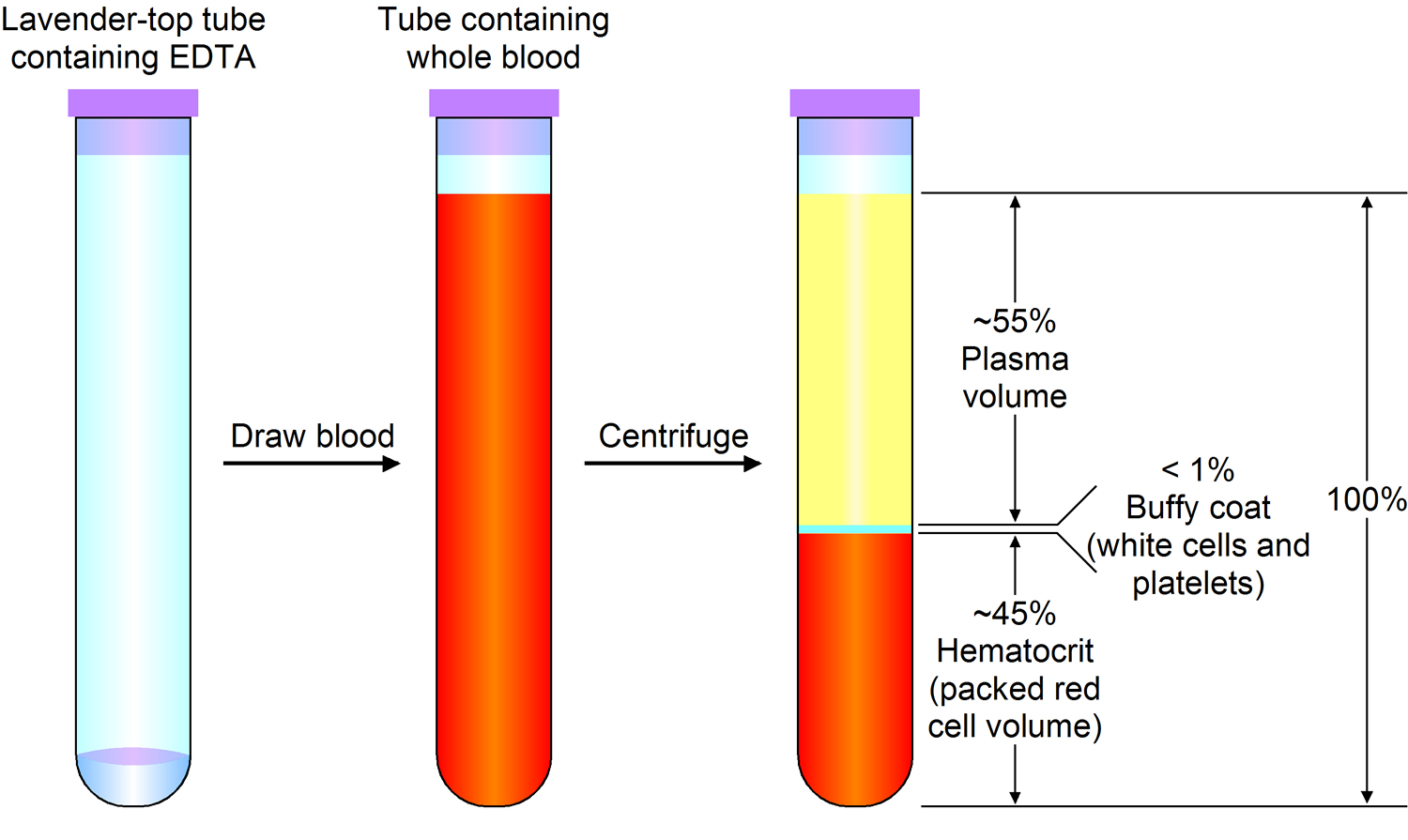
Note: Blood consists of a liquid portion called plasma and a solid portion (the formed elements) that includes red blood cells, white blood cells, and platelets. When blood components are separated by centrifugation, the white blood cells and platelets form a thin layer, called the “buffy coat,” between the plasma and the red blood cells, which accounts for about 1% of the total blood volume. Blood cells and platelets can be seen under a light microscope when a blood sample is smeared onto a glass slide.
Figure 2. Blood cells
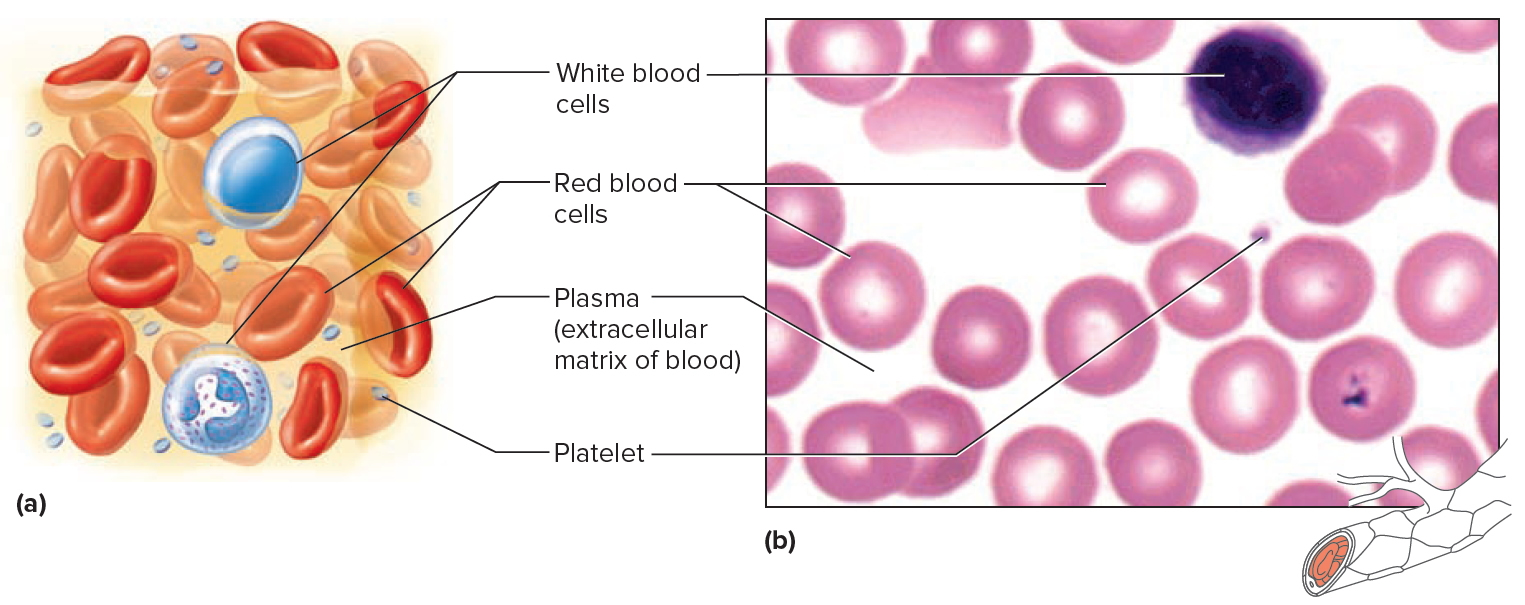
Note: Blood tissue consists of red blood cells, white blood cells, and platelets suspended in plasma. (a) Idealized representation of a sample of blood. (b) Micrograph of a sample of blood (1,000x).
Blood Antigens and Antibodies
An antigen, is any molecule that triggers an immune response, the body’s reaction to invasion by a foreign substance or organism. When the immune system encounters an antigen not found on the body’s own cells, it will attack, producing antibodies. In a transfusion reaction, antigens (agglutinogens) on the surface of the donated red blood cells react with antibodies (agglutinins) in the plasma of the recipient, resulting in the agglutination of the donated red blood cells.
A mismatched blood transfusion quickly produces telltale signs of agglutination—anxiety, breathing difficulty, facial flushing, headache, and severe pain in the neck, chest, and lumbar area. Red blood cells burst, releasing free hemoglobin. Liver cells and macrophages phagocytize the hemoglobin, converting it to bilirubin, which may sufficiently accumulate to cause the yellow skin of jaundice. Free hemoglobin reaching the kidneys may ultimately cause them to fail.
Only a few of the 32 known antigens on red blood cell membranes can produce serious transfusion reactions. These include the antigens of the ABO group and those of the Rh group. Avoiding the mixture of certain kinds of antigens and antibodies prevents adverse transfusion reactions.
Blood Types
Every person has one of the following blood types: A, B, AB, or O. Also, every person’s blood is either Rh-positive or Rh-negative. So, if you have type A blood, it’s either A positive or A negative.
- Each person has an ABO blood type – either A, B, AB, or O – which means antigen A, antigen B, both antigens (type AB), or neither antigen (type O) is found on their blood cells.
- Each person also is either Rh-positive or Rh-negative (you either have Rh or you don’t).
The blood used in a transfusion must work with your blood type. If it doesn’t, antibodies (proteins) in your blood attack the new blood and make you sick.
Type O blood is safe for almost everyone. About 40 percent of the population has type O blood. People who have this blood type are called universal donors. Type O blood is used for emergencies when there’s no time to test a person’s blood type.
People who have type AB blood are called universal recipients. This means they can get any type of blood.
If you have Rh-positive blood, you can get Rh-positive or Rh-negative blood. But if you have Rh-negative blood, you should only get Rh-negative blood. Rh-negative blood is used for emergencies when there’s no time to test a person’s Rh type.
ABO blood types
The ABO blood group is based on the presence (or absence) of two major antigens on red blood cell membranes—antigen A and antigen B. A and B antigens are carbohydrates attached to glycolipids projecting from the red blood cell surface. A person’s erythrocytes have on their surfaces one of four antigen combinations: only A, only B, both A and B, or neither A nor B.
A person with only antigen A has type A blood. A person with only antigen B has type B blood. An individual with both antigens A and B has type AB blood. A person with neither antigen A nor B has type O blood. Thus, all people have one of four possible ABO blood types—A, B, AB, or O. The resulting ABO blood type is inherited. It is the consequence of DNA encoding enzymes to synthesize A or B antigens on erythrocytes in one of these four combinations.
- In the United States, the most common ABO blood types are O (47%) and A (41%). Rarer are type B (9%) and type AB (3%). These percentages vary in subpopulations and over time, reflecting changes in the genetic structure of populations.
Antibodies that affect the ABO blood group antigens are present in the plasma about two to eight months following birth, as a result of exposure to foods or microorganisms containing the antigen(s) that are not present on the individual’s red blood cells. Specifically, whenever antigen A is absent in red blood cells, an antibody called anti-A is produced, and whenever antigen B is absent on cells, an antibody called anti-B is produced. Therefore, individuals with type A blood have anti-B antibody in their plasma; those with type B blood have anti-A antibody; those with type AB blood have neither antibody; and those with type O blood have both anti-A and anti-B antibodies (Figure 3 and Table 1). The antibodies anti-A and anti-B are large and do not cross the placenta. Thus, a pregnant woman and her fetus may be of different ABO blood types, but agglutination in the fetus will not occur.
An antibody of one type will react with an antigen of the same type and clump red blood cells; therefore, such combinations must be avoided. The major concern in blood transfusion procedures is that the cells in the donated blood not clump due to antibodies in the recipient’s plasma. For this reason, a person with type A (anti-B) blood must not receive blood of type B or AB, either of which would clump in the presence of anti-B in the recipient’s type A blood. Likewise, a person with type B (anti-A) blood must not receive type A or AB blood, and a person with type O (anti-A and anti-B) blood must not receive type A, B, or AB blood.
Type AB blood does not have anti-A or anti-B antibodies, so an AB person can receive a transfusion of blood of any other type. For this reason, individuals with type AB blood are called universal recipients. However, type A (anti-B) blood, type B (anti-A) blood, and type O (anti-A and anti-B) blood still contain antibodies (either anti-A and/or anti-B) that could agglutinate type AB cells if transfused rapidly.
Consequently, even for AB individuals, using donor blood of the same type as the recipient is best. Type O blood has neither antigen A nor antigen B. Therefore, theoretically this type could be transfused into persons with blood of any other type. Individuals with type O blood are called universal donors. Type O blood, however, does contain both anti-A and anti-B antibodies. If type O blood is given to a person with blood type A, B, or AB, it should be transfused slowly so that the recipient’s larger blood volume will dilute the donor blood, minimizing the chance of an adverse reaction.
- If you have type O blood, you can only get type O red blood cell transfusions. But you can give your red blood cells to people with type A, B, AB, or O blood, which is why you are sometimes called a universal donor. (Universal donor blood cells are typically only used in emergencies. For example, if a person is bleeding severely and nearing death, there may no time for testing. In everyday practice, people in the US are almost always given the exact same type of red blood cells that they have.)
- If you have type A blood, you cannot get either type B or AB red blood cells.
- If you have type B blood, you cannot get type A or AB red blood cells.
- If you have type AB blood, you can get transfusions of O, A, B, or AB red blood cells.
Figure 3. ABO Blood Types and Antibodies (different combinations of antigens and antibodies distinguish blood types)
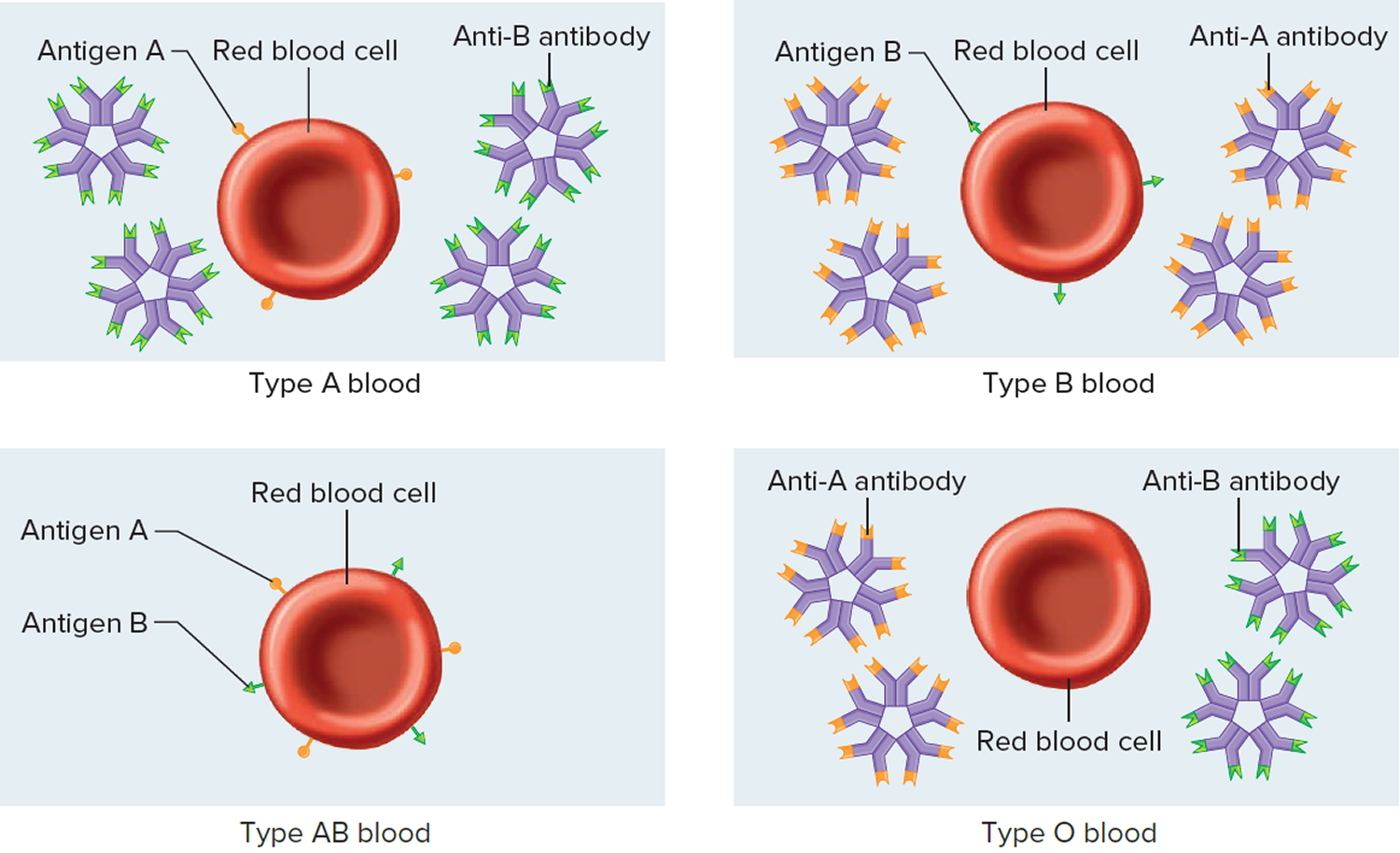
Table 1. Antigens and Antibodies of the ABO Blood Group
Blood Type | Antigen | Antibody |
A | A | Anti-B |
B | B | Anti-A |
AB | A and B | Neither anti-A nor anti-B |
O | Neither A nor B | Both anti-A and anti-B |
Table 2. Preferred and Permissible Blood Types for Transfusions
Blood Type of Recipient | Preferred Blood Type of Donor | If Preferred Blood Type Unavailable, Permissible Blood Type of Donor |
A | A | O |
B | B | O |
AB | AB | A, B, O |
O | O | No alternate types |
Rh (Rhesus) factor
The Rh (Rhesus) blood group was named after the rhesus monkey in which it was first studied. In humans, this group includes several Rh antigens (factors). The most prevalent of these is antigen D, a transmembrane protein.
If the Rh antigens are present on the red blood cell membranes, the blood is said to be Rh-positive. Conversely, if the red blood cells do not have Rh antigens, the blood is called Rh-negative. The presence (or absence) of Rh antigens is an inherited trait. Anti-Rh antibodies (anti-Rh) form only in Rh-negative individuals in response to the presence of red blood cells with Rh antigens. This happens, for example, if an individual with Rh-negative blood receives a transfusion of Rh-positive blood. The Rh antigens stimulate the recipient to begin producing anti-Rh antibodies. Generally, this initial transfusion has no serious consequences, but if an individual with Rh-negative blood—who is now sensitized to Rh-positive blood—receives another transfusion of Rh-positive blood some months later, the donated red cells are likely to agglutinate.
A similar situation of Rh incompatibility arises when an Rh-negative woman is pregnant with an Rh-positive fetus. Her first pregnancy with an Rh-positive fetus would probably be uneventful. However, if at the time of the infant’s birth (or if a miscarriage occurs) the placental membranes that separated the maternal blood from the fetal blood during the pregnancy tear, some of the infant’s Rh-positive blood cells may enter the maternal circulation. These Rh-positive cells may then stimulate the maternal tissues to produce anti-Rh antibodies. If a woman who has already developed anti-Rh antibodies becomes pregnant with a second Rh-positive fetus, these antibodies, called hemolysins, cross the placental membrane and destroy the fetal red blood cells. The fetus then develops a condition called erythroblastosis fetalis, or hemolytic disease of the fetus and newborn.
Erythroblastosis fetalis is extremely rare today because obstetricians carefully track Rh status. An Rh-negative woman who might carry an Rh-positive fetus is given an injection of a drug called RhoGAM at week 28 of her pregnancy and after delivery of an Rh-positive baby. Rhogam is a preparation of anti-Rh antibodies, which bind to and shield any Rh-positive fetal cells that might contact the woman’s cells and sensitize her immune system. RhoGAM must be given within 72 hours of possible contact with Rh-positive cells—including giving birth, terminating a pregnancy, miscarrying, or undergoing amniocentesis (a prenatal test in which a needle is inserted into the uterus).
Blood is either Rh-positive or Rh-negative, depending on whether the red blood cells have Rh antigens on their surface. A person who has type B, Rh-positive blood is called B positive, whereas a person with type B, Rh-negative blood is B negative.
If you have Rh-positive blood, you can get Rh-positive or Rh-negative red blood cell transfusions. But people with Rh-negative blood should only get Rh-negative red blood cells except in extreme emergencies. This is because an Rh-positive blood transfusion can cause a person with Rh negative blood to make antibodies against the Rh factor, causing a transfusion reaction (discussed below). If an Rh-negative woman makes antibodies like this, it can seriously harm any Rh-positive babies she may have in the future. Her anti-Rh antibodies can attack Rh-positive blood cells in the fetus.
Other antigens
There are other antigens on red blood cells that can lead to transfusion reactions. These are rare because people don’t make antibodies against them unless they have had transfusions before. Still, these antigens may become a factor in matching blood for a person who has had many transfusions in the past, as is the case for some people with cancer.
Plasma, platelets, cryo, and blood type
Blood types are also important for plasma transfusions, but the rules are different than the rules for red blood cells transfusions. For example, people with type AB blood are universal plasma donors, and they can only receive type AB plasma.
For platelet and cryoprecipitate transfusions, matching the blood type of the donor to the recipient is usually not critical, but labs still try to match them. This may become important for patients who have already had many transfusions or who have reacted to transfusions in the past.
Blood Cell Formation
The process of blood cell formation, called hematopoiesis, begins in the yolk sac, which lies outside the human embryo. Later in the fetal development, red blood cells are manufactured (erythropoiesis) in the liver and spleen, and still later they form in bone marrow. After birth, these cells are produced in the red bone marrow.
Bone marrow is a soft, netlike mass of connective tissue within the medullary cavities of long bones, in the irregular spaces of spongy bone, and in the larger central canals of compact bone tissue. It is of two kinds: red and yellow. Red bone marrow functions in the formation of red blood cells (erythrocytes), white blood cells (leukocytes), and blood platelets. The color comes from the oxygen-carrying pigment hemoglobin in the red blood cells.
In an infant, red marrow occupies the cavities of most bones. As a person ages, yellow bone marrow, which stores fat, replaces much of the red marrow. Yellow marrow is not active in blood cell production. In an adult, red marrow is primarily found in the spongy bone of the skull, ribs, breastbone (sternum), collarbones (clavicles), backbones (vertebrae), and hip bones. If the supply of blood cells is deficient, some yellow marrow may become red marrow, which then reverts to yellow marrow when the deficiency is corrected.
Figure 4 illustrates the stages in the formation of red blood cells from hematopoietic stem cells (blood-forming cells), which are also called hemocytoblasts.
Red blood cells have nuclei during their early stages of development but lose their nuclei as the cells mature. Losing the nuclei provides more space for hemoglobin. Because mature red blood cells do not have nuclei, they cannot divide. They use none of the oxygen they carry because they do not have mitochondria. Mature red blood cells produce ATP through glycolysis only.
The average life span of a red blood cell is 120 days. Many of these cells are removed from the circulation each day, and yet the number of cells in the circulating blood remains relatively stable. This observation suggests a homeostatic control of the rate of red blood cell production.
The hormone erythropoietin controls the rate of red blood cell formation through negative feedback. The kidneys, and to a lesser extent the liver, release erythropoietin in response to prolonged oxygen deficiency (Figure 6). At high altitudes, for example, where the amount of oxygen in the air is reduced, the blood oxygen level initially decreases. This drop in the blood oxygen level triggers the release of erythropoietin, which travels via the blood to the red bone marrow and stimulates red blood cell production.
After a few days of exposure to high altitudes, many newly formed red blood cells appear in the circulating blood. The increased rate of production continues until the number of erythrocytes in the circulation is sufficient to supply tissues with oxygen. When the availability of oxygen returns to normal, erythropoietin release decreases, and the rate of red blood cell production returns to normal as well. An excessive increase in red blood cells is called polycythemia. This condition increases blood viscosity, slowing blood flow and impairing circulation.
Figure 3. Bone marrow anatomy

Anatomy of the bone. The bone is made up of compact bone, spongy bone, and bone marrow. Compact bone makes up the outer layer of the bone. Spongy bone is found mostly at the ends of bones and contains red marrow. Bone marrow is found in the center of most bones and has many blood vessels. There are two types of bone marrow: red and yellow. Red marrow contains blood stem cells that can become red blood cells, white blood cells, or platelets. Yellow marrow is made mostly of fat.
Dietary Factors Affecting Red Blood Cell Production
Availability of B-complex vitamins—vitamin B12 and folic acid—significantly influences red blood cell production. Because these vitamins are required for DNA synthesis, they are necessary for the growth and division of cells. Cell division is frequent in blood-forming (hematopoietic) tissue, so this tissue is especially vulnerable to a deficiency of either of these vitamins.
Hemoglobin synthesis and normal red blood cell production also require iron. The small intestine absorbs iron slowly from food. The body reuses much of the iron released by the decomposition of hemoglobin from damaged red blood cells. Nonetheless, insufficient dietary iron can reduce hemoglobin synthesis.
A deficiency of red blood cells or a reduction in the amount of hemoglobin they contain results in a condition called anemia. This reduces the oxygen-carrying capacity of the blood, and the affected person may appear pale and lack energy. A pregnant woman may have a normal number of red blood cells, but she develops a relative anemia because her plasma volume increases due to fluid retention. This shows up as a decreased hematocrit.
In contrast to anemia, the inherited disorder called hemochromatosis results in the absorption of iron in the small intestine at ten times the normal rate. Iron builds up in organs, to toxic levels. Treatment is periodic blood removal, as often as every week.
Figure 4. Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell

Figure 5. Blood cells
Note: Blood tissue consists of red blood cells, white blood cells, and platelets suspended in plasma. (a) Idealized representation of a sample of blood. (b) Micrograph of a sample of blood (1,000x).
Figure 6. Red blood cell formation
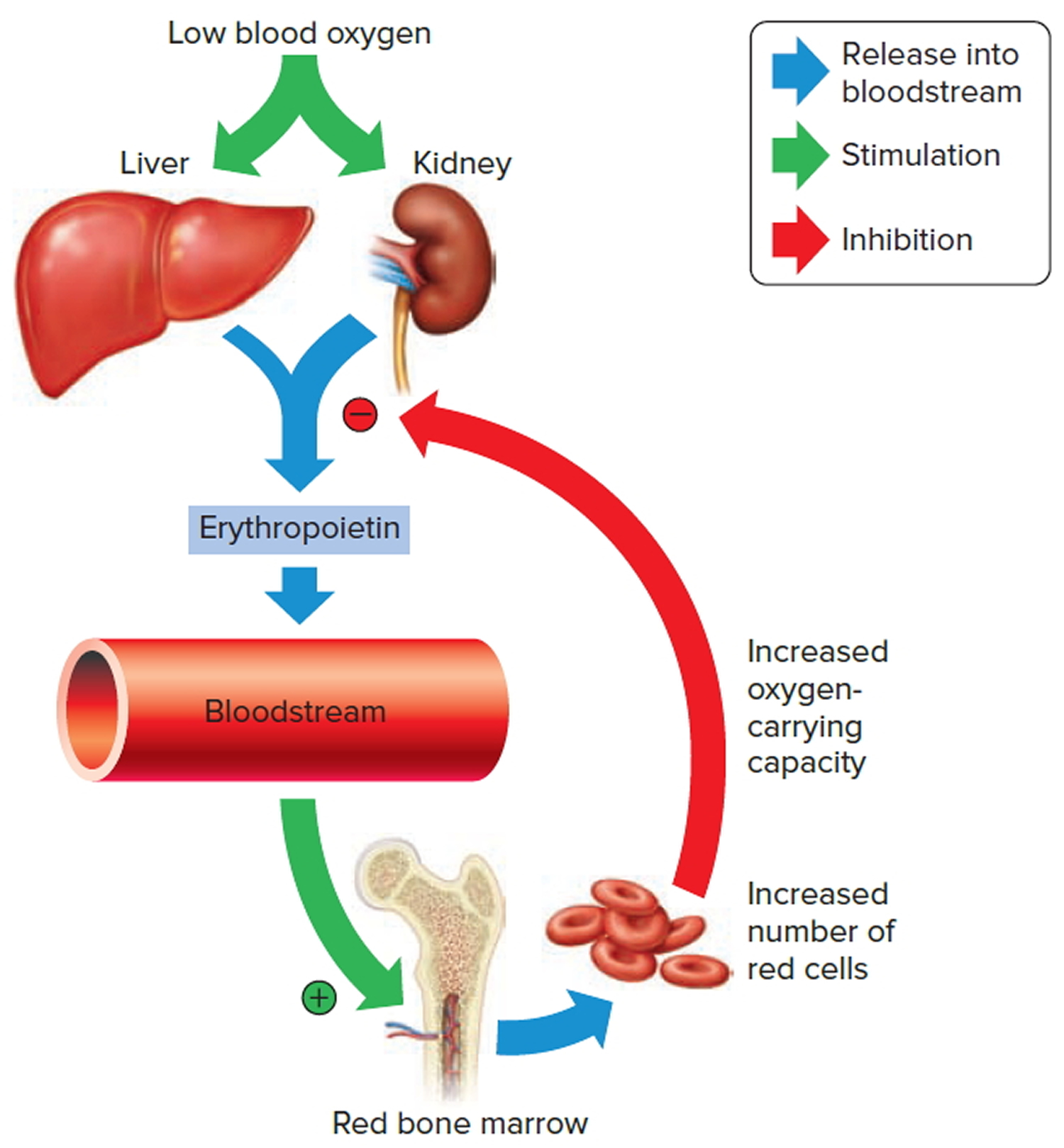
Note: Low blood oxygen causes the kidneys and to a lesser degree, the liver to release erythropoietin. Erythropoietin stimulates target cells in the red bone marrow to increase the production of red blood cells, which carry oxygen to tissues.
Sources of blood for blood transfusion
Blood From the Public (Volunteer Blood Donation)
The most common source of blood is from volunteers in the general public. This kind of donation is also called homologous blood donation.
Many communities have a blood bank at which any healthy person can donate blood. This blood is tested to see if it matches yours.
You may have read about the danger of becoming infected with hepatitis, HIV, or other viruses after a blood transfusion. Blood transfusions are not 100% safe. But the current blood supply is thought to be safer now than ever. Donated blood is tested for many different infections. Also, blood centers keep a list of unsafe donors.
Donors answer a detailed list of questions about their health before they are allowed to donate. Questions include risk factors for infections that can be passed on through their blood, such as sexual habits, drug use, and current and past travel history. This blood is then tested for infectious diseases before it is allowed to be used.
Directed Donor Blood From a Family Member or Friend
This method involves a family member or friend donating blood before a planned surgery. This blood is then set aside and held only for you, if you need a blood transfusion after surgery.
Blood from these donors must be collected at least a few days before it is needed. The blood is tested to see if it matches yours. It is also screened for infection.
Most of the time, you need to arrange with your hospital or local blood bank before your surgery to have directed donor blood.
It is important to note that there is no evidence that receiving blood from family members or friends is any safer than receiving blood from the general public. In very rare cases, though, blood from family members can cause a condition called graft-versus-host disease. For this reason, the blood needs to be treated with radiation before it can be transfused.
Autologous Blood Donation (Your own Blood)
Although blood donated by the general public and used for most people is thought to be very safe, some people choose a method called autologous blood donation.
Autologous blood is blood donated by you, which you later receive if you need a transfusion during or after surgery.
- You can have blood taken from 6 weeks to 5 days before your surgery.
- Your blood is stored and is good for a few weeks from the day it is collected.
- If your blood is not used during or after surgery, it will be thrown away.
Blood transfusion types
Blood is transfused either as whole blood (with all its parts) or, more often, as individual parts. The type of blood transfusion you need depends on your situation.
For example, if you have an illness that stops your body from properly making a part of your blood, you may need only that part to treat the illness.
Red Blood Cell Transfusions
Red blood cells are the most commonly transfused part of the blood. These cells carry oxygen from the lungs to your body’s organs and tissues. They also help your body get rid of carbon dioxide and other waste products.
You may need a transfusion of red blood cells if you’ve lost blood due to an injury or surgery. You also may need this type of transfusion if you have severe anemia due to disease or blood loss.
Anemia is a condition in which your blood has a lower than normal number of red blood cells. Anemia also can occur if your red blood cells don’t have enough hemoglobin.
Hemoglobin is an iron-rich protein that gives blood its red color. This protein carries oxygen from the lungs to the rest of the body.
Platelets and Clotting Factor Transfusions
Platelets and clotting factors help stop bleeding, including internal bleeding that you can’t see. Some illnesses may cause your body to not make enough platelets or clotting factors. You may need regular transfusions of these parts of your blood to stay healthy.
For example, if you have hemophilia, you may need a special clotting factor to replace the clotting factor you’re lacking. Hemophilia is a rare, inherited bleeding disorder in which your blood doesn’t clot normally.
If you have hemophilia, you may bleed for a longer time than others after an injury or accident. You also may bleed internally, especially in the joints (knees, ankles, and elbows).
Plasma Transfusions
Plasma is the liquid part of your blood. It’s mainly water, but also contains proteins, clotting factors, hormones, vitamins, cholesterol, sugar, sodium, potassium, calcium, and more.
If you have been badly burned or have liver failure or a severe infection, you may need a plasma transfusion.
Who Needs a Blood Transfusion?
Blood is a bodily fluid which carries oxygen, nutrients and wastes around the body via small vessels. Since blood serves such an important function, large losses of blood volume can be fatal. Some people may have conditions which affect certain components of their blood, such as the white blood cells, red blood cells and platelets.
Blood transfusions are very common. Each year, almost 5 million Americans need blood transfusions. This procedure is used for people of all ages.
Many people who have surgery need blood transfusions because they lose blood during their operations. For example, about one-third of all heart surgery patients have a transfusion.
Some people who have serious injuries—such as from car crashes, war, or natural disasters—need blood transfusions to replace blood lost during the injury.
Some people need extra blood or parts of blood because of illnesses. You may need a blood transfusion if you have the following conditions:
- A severe infection or liver disease that stops your body from properly making blood or some parts of blood.
- An illness that causes anemia, such as kidney disease or cancer. Medicines or radiation used to treat a medical condition also can cause anemia. There are many types of anemia, including aplastic anemia, Fanconi anemia, hemolytic anemia, iron-deficiency anemia, and sickle cell anemia and thalassemia.
- A bleeding disorder, such as hemophilia or thrombocytopenia.
- Serious bleeding due to trauma or accident
- Bleeding during surgery
- Hemophilia (a blood clotting disorder)
- Cancer or cancer treatment that can affect blood cells – including chemotherapy or stem cell transplants
- Pregnant women whose baby is at risk of Hemolytic Disease of the Newborn
- Premature babies
- Heart disease
A blood transfusion can replace blood you’ve lost, or just replace the liquid or cells found in blood (such as red blood cells, plasma or cells called platelets).
Ask your doctor or nurse why they think you might need a transfusion if you’re not sure.
How does a blood transfusion work
Red Blood Cells
Packed red blood cells (RBCs) are prepared from whole blood by removing approximately 250 mL of plasma. One unit of packed red blood cells (RBCs) should increase levels of hemoglobin by 1 g per dL (10 g per L) and hematocrit by 3 percent. In most areas, packed red blood cell units are filtered to reduce leukocytes before storage, which limits febrile nonhemolytic transfusion reactions (FNHTRs), and are considered cytomegalovirus safe 1.
Red blood cell (RBC) transfusions are used to treat hemorrhage and to improve oxygen delivery to tissues. Transfusion of red blood cells (RBCs) should be based on the patient’s clinical condition. Indications for red blood cell (RBC) transfusion include acute sickle cell crisis (for stroke prevention), or acute blood loss of greater than 1,500 mL or 30 percent of blood volume 2. Patients with symptomatic anemia should be transfused if they cannot function without treating the anemia 2. Symptoms of anemia may include fatigue, weakness, dizziness, reduced exercise tolerance, shortness of breath, changes in mental status, muscle cramps, and angina or severe congestive heart failure. The 10/30 rule—transfusion when a patient has a hemoglobin level less than or equal to 10 g per dL (100 g per L) and a hematocrit level less than or equal to 30 percent—was used until the 1980s as the trigger to transfuse, regardless of the patient’s clinical presentation 2.
In 1999, a randomized, multicenter, controlled clinical trial evaluated a restrictive transfusion trigger (hemoglobin level of 7 to 9 g per dL [70 to 90 g per L]) versus a liberal transfusion trigger (hemoglobin level of 10 to 12 g per dL [100 to 120 g per L]) in patients who were critically ill 3. Restrictive transfusion practices resulted in a 54 percent relative decrease in the number of units transfused and a reduction in the 30-day mortality rate. The authors recommended transfusion when hemoglobin is less than 7 g per dL, and maintenance of a hemoglobin level between 7 to 9 g per dL 3. A recently updated Cochrane review supports the use of restrictive transfusion triggers in patients who do not have cardiac disease 4.
A similar study was carried out in critically ill children 5. The restrictive transfusion trigger was a hemoglobin level of 7 g per dL, with a target level of 8.5 to 9.5 g per dL (85 to 95 g per L). The liberal transfusion trigger was a hemoglobin level of 9.5 g per dL, with a target level of 11 to 12 g per dL (110 to 120 g per L). Patients in the restrictive group received 44 percent fewer blood transfusions, with no difference in rates of multiple organ dysfunction syndrome or death. The restrictive transfusion strategy is useful for children who are stable patients in intensive care. It should not be used in preterm neonates or in children with severe hypoxemia, active blood loss, hemodynamic instability, or cyanotic heart disease 5.
Blood Plasma
Plasma products available in the United States include fresh frozen plasma and thawed plasma that may be stored at 33.8 to 42.8°F (1 to 6°C) for up to five days. Plasma contains all of the coagulation factors. Fresh frozen plasma infusion can be used for reversal of anticoagulant effects. Thawed plasma has lower levels of factors V and VIII and is not indicated in patients with consumption coagulopathy (diffuse intravascular coagulation) 1.
Plasma transfusion is recommended in patients with active bleeding and an International Normalized Ratio (INR) greater than 1.6, or before an invasive procedure or surgery if a patient has been anticoagulated 6. Plasma is often inappropriately transfused for correction of a high INR when there is no bleeding. Supportive care can decrease high-normal to slightly elevated INRs (1.3 to 1.6) without transfusion of plasma. Table 3 gives indications for plasma transfusion 7.
Table 3. Indications for Transfusion of Plasma Products
| Indication | Associated condition/additional information |
|---|---|
International Normalized Ratio > 1.6 | Inherited deficiency of single clotting factors with no virus-safe or recombinant factor available—anticoagulant factors II, V, X, or XI |
Prevent active bleeding in patient on anticoagulant therapy before a procedure | |
Active bleeding | |
Emergent reversal of warfarin (Coumadin) | Major or intracranial hemorrhage |
Prophylactic transfusion in a surgical procedure that cannot be delayed | |
Acute disseminated intravascular coagulopathy | With active bleeding and correction of underlying condition |
Microvascular bleeding during massive transfusion | ≥ 1 blood volume (replacing approximately 5,000 mL in an adult who weighs 155.56 lb [70 kg]) |
Replacement fluid for apheresis in thrombotic microangiopathies | Thrombotic thrombocytopenic purpura; hemolytic uremic syndrome |
Hereditary angioedema | When C1 esterase inhibitor is unavailable |
[Source 8]
Platelets
Platelet transfusion may be indicated to prevent hemorrhage in patients with thrombocytopenia or platelet function defects. Contraindications to platelet transfusion include thrombotic thrombocytopenic purpura and heparin-induced thrombocytopenia. Transfusion of platelets in these conditions can result in further thrombosis 9. One unit of apheresis platelets should increase the platelet count in adults by 30 to 60 × 103 per μL (30 to 60 × 109 per L) 1. In neonates, transfusing 5 to 10 mL per kg of platelets should increase the platelet count by 50 to 100 × 103 per μL (50 to 100 × 109 per L).12 One apheresis platelet collection is equivalent to six pooled random donor platelet concentrates 10.
Spontaneous bleeding through intact endothelium does not occur unless the platelet count is no greater than 5 × 103 per μL (5 × 109 per L) 7. One randomized controlled trial evaluated a threshold for prophylactic platelet transfusion in patients with acute myeloid leukemia 11. Patients were randomized based on platelet transfusion triggers of 10 × 103 per μL (10 × 109 per L) or 20 × 103 per μL (20 × 109 per L). Patients in the lower trigger group received 21.5 percent fewer transfusions than the higher trigger group. Gastrointestinal bleeding was more common in the lower trigger group; however, there was no difference in blood transfusions between groups. Tables 4 and Table 5 give indications for platelet transfusion in adults and neonates, respectively.
Table 4. Indications for Transfusion of Platelets in Adults
| Prophylactic transfusion indications | Platelet count (× 103 per μL) |
|---|---|
Major surgery or invasive procedure, no active bleeding | ≤ 50 |
Ocular surgery or neurosurgery, no active bleeding | ≤ 100 |
Surgery with active bleeding | < 50 (usually) |
> 100 (rarely) | |
Stable, nonbleeding | < 10 |
Stable, nonbleeding, and body temperature > 100.4°F (38°C) or undergoing invasive procedure | < 20 |
Table 5. Indications for Transfusion of Platelets in Neonates
| Platelet count (× 103 per μL) | Indications |
|---|---|
< 20 | Always transfuse |
20 to < 30 | Consider transfusion; transfuse for clinical reasons (e.g., active bleeding, lumbar puncture) |
30 to 50 | Transfuse if any of the following indications exist: |
First week of life with birth weight < 1,000 g (2 lb, 4 oz) | |
Intraventricular or intraparenchymal cerebral hemorrhage | |
Coagulation disorder | |
Sepsis or fluctuating arterial venous pressures | |
Invasive procedure | |
Alloimmune neonatal thrombocytopenia* |
*—Select a donor (possibly the mother) whose platelets lack the causative antigen. If the mother’s platelets are used, unit must be washed, irradiated, and resuspended in plasma that is ABO compatible with the neonate.
Cryoprecipitate
Cryoprecipitate is prepared by thawing fresh frozen plasma and collecting the precipitate. Cryoprecipitate contains high concentrations of factor VIII and fibrinogen. Cryoprecipitate is used in cases of hypofibrinogenemia, which most often occurs in the setting of massive hemorrhage or consumptive coagulopathy. Indications for cryoprecipitate transfusion are listed in Table 6. Each unit will raise the fibrinogen level by 5 to 10 mg per dL (0.15 to 0.29 μmol per L), with the goal of maintaining a fibrinogen level of at least 100 mg per dL (2.94 μmol per L) 12. The usual dose in adults is 10 units of pooled cryoprecipitate 1. Recommendations for dosing regimens in neonates vary, ranging from 2 mL of cryoprecipitate per kg to 1 unit of cryoprecipitate (15 to 20 mL) per 7 kg 13.
Table 6. Indications for Transfusion of Cryoprecipitate
Adults |
Hemorrhage after cardiac surgery |
Massive hemorrhage or transfusion |
Surgical bleeding |
Neonates |
Anticoagulant factor VIII deficiency* |
Anticoagulant factor XIII deficiency |
Congenital dysfibrinogenemia |
Congenital fibrinogen deficiency |
von Willebrand disease* |
*—Use when recombinant factors are not available.
Blood transfusion procedure
First, blood tests such as a complete blood count (CBC) are done to find out if the patient’s symptoms are likely to be helped by a transfusion. A CBC measures the levels of components within the blood such as red blood cells, white blood cells, and platelets. Tests of clotting (coagulation) may also be done if abnormal bleeding is a problem.
If a transfusion is needed, it must be prescribed by a health care provider. At that point, more blood tests must be done to find a donated blood component that closely matches the patient.
Before having a blood transfusion, the procedure will be explained to you and you’ll be asked to sign a consent form.
Blood types
Before a blood transfusion, a technician tests your blood to find out what blood type you have (that is, A, B, AB, or O and Rh-positive or Rh-negative). He or she pricks your finger with a needle to get a few drops of blood or draws blood from one of your veins.
Blood types are important when it comes to transfusions. The blood type used in your transfusion must work with your blood type. You’ll only be given blood that’s safe for someone with your blood group. If it doesn’t, your body’s immune system (antibodies) in your blood attack the new blood and make you sick. This can cause a serious or even life-threatening transfusion reaction.
To be sure no mistakes are made, donated blood is carefully tested to find out what type it is. This is done when it’s taken from the donor and again once it’s received by the hospital lab. The blood bag is labeled with the type of blood it contains. When a person needs a blood transfusion, a blood sample is drawn from them and tested the same way.
All blood has the same components, but not all blood is the same. People have different blood types, which are based on substances called antigens on a person’s blood cells. The 2 most important antigens in blood typing are called A, B, O, and Rh.
- Each person has an ABO blood type – either A, B, AB, or O – which means antigen A, antigen B, both antigens (type AB), or neither antigen (type O) is found on their blood cells.
- Each person also is either Rh-positive or Rh-negative (you either have Rh or you don’t).
These 2 factors can be combined into 8 possible blood types:
| A positive | B positive | AB positive | O positive |
| A negative | B negative | AB negative | O negative |
Some people have allergic reactions even when the blood given does work with their own blood type. To prevent this, your doctor may prescribe a medicine to stop allergic reactions. For more information, see Blood Transfusion Risks and Side Effects below.
If you have allergies or have had an allergic reaction during a past transfusion, your doctor will make every effort to make sure you’re safe.
Most people don’t need to change their diets or activities before or after a blood transfusion. Your doctor will let you know whether you need to make any lifestyle changes prior to the procedure.
Antibodies and cross-matching
After blood is typed, a test called an antibody screen is done to see if a patient’s plasma contains other antibodies besides those against A, B, and Rh. If there are extra antibodies, the cross-matching may take longer. This is because some units of donor blood may not fully match the recipient’s, even though they have the same ABO and Rh types.
Before a person can get a transfusion of red blood cells, another lab test called a cross-match must be done to make sure that the donor blood is compatible with the recipient’s.
A unit of the right ABO and Rh type blood is selected, and a drop of donor red cells from the unit is mixed with a drop of plasma from the patient. The mixture is watched to see if the patient’s plasma causes the donor blood cells to clump. This may happen if the patient has extra antibodies to a protein in the donor unit. If there are no problems (no clumping), a cross-match takes about 30 minutes.
A cross-match is usually not needed for a platelet or plasma transfusion unless the platelets look like they could contain some red blood cells.
How does a blood transfusion work
Blood transfusions can take place in either a doctor’s office or a hospital. Sometimes they’re done at a person’s home, but this is less common. Blood transfusions also are done during surgery and in emergency rooms. The blood transfusion procedure usually takes 1 to 4 hours to receive 1 bag of blood, but it’s usually faster than this. The time depends on how much blood you need and what part of the blood you receive.
- You sit or lie down in a chair or bed.
- A needle is inserted into a vein in your arm or hand. You might feel a sharp prick when the needle is first inserted into your vein, but you shouldn’t feel anything during the blood transfusion.
- The needle is connected to a tube and a bag of blood.
- The blood runs through the tube into your vein.
Red blood cell transfusions are usually started slowly while the patient is watched closely for the signs and symptoms of a transfusion reaction. The patient’s vital signs (such as temperature, heart rate, and blood pressure) are checked often. If there are no problems, the infusion rate will slowly be increased (so the blood goes in faster). Each unit of red blood cells is usually given over a couple of hours, and should be completed within 4 hours. Other blood products, like plasma and platelets, go in much faster.
During the blood transfusion, a nurse carefully watches you, especially for the first 15 minutes. This is when allergic reactions are most likely to occur. The nurse continues to watch you during the rest of the procedure as well.
Tell a member of staff if you feel unwell or uncomfortable.
Some people develop a temperature, chills or a rash. This is usually treated with paracetamol or by slowing down the blood transfusion.
Your arm or hand may ache and have a bruise for a few days after.
You can normally go home soon after, unless you are seriously unwell or needed a lot of blood.
Contact your doctor if you feel unwell within 24 hours of having a blood transfusion, especially if you have difficulty breathing or pain in your chest or back.
After a Blood Transfusion
After a blood transfusion, your vital signs are checked (such as your temperature, blood pressure, and heart rate). The intravenous (IV) line is taken out. You may have some bruising or soreness for a few days at the site where the IV was inserted.
You may need blood tests that show how your body is reacting to the transfusion. Your doctor will let you know about signs and symptoms to watch for and report.
Blood transfusion risks and side effects
Blood transfusions are common and very safe procedures. However, mild problems and, very rarely, serious problems can occur.
All donor blood is checked before it’s used to make sure it doesn’t contain serious infections such as hepatitis or HIV.
There is a very small risk of complications such as:
- an allergic reaction to the donor blood
- a problem with your heart, lungs or immune system (the body’s defence against illness and infection)
The risks will be explained before having a transfusion, unless this isn’t possible – for example, if you need an emergency transfusion. Speak to your doctor or nurse if you have any concerns.
Table 7. Noninfectious Serious Hazards of Transfusion
Acute |
Acute hemolytic reaction |
Allergic reaction |
Anaphylactic reaction |
Coagulation problems in massive transfusion |
Febrile nonhemolytic reaction |
Metabolic derangements |
Mistransfusion (transfusion of the incorrect product to the incorrect recipient) |
Septic or bacterial contamination |
Transfusion-associated circulatory overload |
Transfusion-related acute lung injury |
Urticarial reaction |
Delayed |
Delayed hemolytic reaction |
Iron overload |
Microchimerism |
Overtransfusion or undertransfusion |
Post-transfusion purpura |
Transfusion-associated graft-versus-host disease |
Transfusion-related immunomodulation |
Complications of blood transfusion
Most patients who receive a transfusion don’t suffer any adverse reactions. However, it’s still possible for reactions to occur with any blood component. A reaction can occur at the time of the transfusion or not until weeks or months later.
Side effects that may occur during or soon after blood transfusion may include symptoms of an allergic reaction such as:
- Fever (called febrile reactions, these are the most common complications and usually aren’t serious)
- A skin rash or hives (called uriticaria, these are the second most common reaction)
- Chills
- Nausea
- Pain at the transfusion site (arm vein)
- Back pain
- Shortness of breath
- A drop in blood pressure
- Dark or red urine
If you notice any of these changes during a transfusion, however slight, alert the nursing staff promptly. Serious complications can be prevented by recognizing a reaction early, stopping the transfusion and limiting the amount of blood given. Although rare, a hemolytic transfusion reaction can occur when transfused red cells are damaged or destroyed. This can result in a drop in blood pressure, bleeding or kidney damage that may be life-threatening.
Febrile reaction
The person gets a sudden fever during or within 24 hours of the transfusion. Headache, nausea, chills, or a general feeling of discomfort may come with the fever. Acetaminophen (Tylenol) may help these symptoms.
These reactions are often the body’s response to white blood cells in the donated blood. They are more common in people who have had transfusions before and in women who have been pregnant several times. Other types of reaction can also cause fever, and further testing may be needed to be sure that the reaction is only febrile and not something more serious.
Patients who have had febrile reactions or who are at risk for them are usually given blood products that are leukoreduced. This means that the white blood cells have been removed by filters or other means. People with cancer often get leukoreduced blood products.
Allergic Reactions
Some people have allergic reactions to the blood given during transfusions. This can happen even when the blood given is the right blood type.
Allergic reactions can be mild or severe. Symptoms can include:
- Anxiety
- Chest and/or back pain
- Trouble breathing
- Fever, chills, flushing, and clammy skin
- A quick pulse or low blood pressure
- Nausea (feeling sick to the stomach)
A nurse or doctor will stop the transfusion at the first signs of an allergic reaction. The health care team determines how mild or severe the reaction is, what treatments are needed, and whether the transfusion can safely be restarted.
Allergic reactions range from mild (urticarial) to life threatening (anaphylactic). Urticarial allergic reactions are defined by hives or pruritus 14. Patients experiencing allergic transfusion reactions have been sensitized to the antigens in the donor unit. These antigens are soluble, and the associated reaction is dose-dependent. Allergic transfusion reactions occur in 1 to 3 percent of transfusions 15.
Patients with anaphylactic transfusion reactions, like those with urticarial reactions, may present with hives, but they are distinct in that they also develop hypotension, bronchospasm, stridor, and gastrointestinal symptoms 15. Anaphylaxis occurs in response to a recipient’s presensitization to a variety of proteins in donor plasma. For example, anaphylaxis occurs because of donor IgA being infused into a recipient who is IgA deficient and has preexisting circulating anti-IgA 16. In addition, anti–human leukocyte antigen (HLA) antibodies and anticomplement antibodies have been linked to anaphylactic reactions, which are estimated to occur in one in 20,000 to 50,000 transfusions 17.
Prevention of anaphylactic transfusion reactions includes avoiding plasma transfusions with IgA in patients known to be IgA deficient. Cellular products (e.g., RBCs, platelets) may be washed to remove plasma in patients with an IgA deficiency 15. The best precaution is observation of the patient during the initial 15 minutes of transfusion.
Usually the only symptoms are hives and itching, which can be treated with antihistamines like diphenhydramine (Benadryl). In rare cases these reactions can be more serious.
Viruses and Infectious Diseases
Some infectious agents, such as HIV, can survive in blood and infect the person receiving the blood transfusion. To keep blood safe, blood banks carefully screen donated blood.
The risk of catching a virus from a blood transfusion is very low.
- HIV. Your risk of getting HIV from a blood transfusion is lower than your risk of getting killed by lightning. Only about 1 in 2 million donations might carry HIV and transmit HIV if given to a patient.
- Hepatitis B and C. The risk of having a donation that carries hepatitis B is about 1 in 350,000 to 1 in 1 million. The risk for hepatitis C is 1 in 2 million. If you receive blood during a transfusion that contains hepatitis, you’ll likely develop the virus.
- Human T-lymphotropic virus 1 or 2: The risk is 1 in 2 million
- Variant Creutzfeldt-Jakob disease (vCJD). This disease is the human version of Mad Cow Disease. It’s a very rare, yet fatal brain disorder. There is a possible risk of getting Variant Creutzfeldt-Jakob disease from a blood transfusion, although the risk is very low. Because of this, people who may have been exposed to Variant Creutzfeldt-Jakob disease aren’t eligible blood donors. Variant Creutzfeldt-Jakob disease is likely to be caused by consuming meat from a cow that had bovine spongiform encephalopathy (BSE or ‘mad cow disease’), a similar prion disease to Creutzfeldt-Jakob disease. Since the link between variant Creutzfeldt-Jakob disease and bovine spongiform encephalopathy (mad cow disease) was discovered in 1996, strict controls have proved very effective in preventing meat from infected cattle from entering the food chain. However, the average time it takes for the symptoms of variant Creutzfeldt-Jakob disease to occur after initial infection (the incubation period) is still unclear. The incubation period could be very long (over 10 years) in some people, so those exposed to infected meat before the food controls were introduced can still develop variant Creutzfeldt-Jakob disease.
- Cytomegalovirus (CMV) transmission. Cytomegalovirus is a common virus up to 3 in 4 people have this infection by the age of 40, but in patients undergoing blood or marrow stem cell transplantation, it can cause serious problems, such as pneumonia. If you haven’t had CMV and you need a transfusion, your cancer team might choose to give you CMV-negative blood products, which come from CMV-negative donors. Or they might use blood products prepared with fewer white blood cells in which the virus lives. Either of these measures greatly reduces the risk of getting CMV if your immune system is weak.
- Bacterial infection transmission. A bacterial infection is extremely rare with red cell transfusions, occurring once in every million transfusions. Infection following platelet transfusions are more common than with red cell transfusions, but special precautions are taken at all U.S. blood centers to prevent this from happening.
The Australian Red Cross Blood Service Transfusion Medicine Manual states the approximate risk for the following viruses, excluding bacterial sepsis 18:
- HIV: less than 1 in 1 million
- Hepatitis C: less than 1 in 1 million
- Hepatitis B: less than 1 in 1 million
- Variant Creutzfeld-Jacob Disease: Possible. Not yet reported in Australia
- Malaria: between 1 in 1 million
The Calman Chart for Explaining Risk
| Classification | Risk range | Example |
| Negligible | <1,000,000 | Death from a lightning strike |
| Minimal | 1:100,000–1:1,000,000 | Death from a train accident |
| Very low | 1:10,000–1:100,000 | Death from an accident at work |
| Low | 1:1,000–1:10,000 | Death from a road accident |
| Moderate | 1:100–1:1,000 | Death from smoking 10 cigarettes per day |
| High | >1:100 | Transmission of chickenpox to susceptible household contacts |
Fever
A Febrile Nonhemolytic Transfusion Reaction is defined as a rise in body temperature of at least 1.8°F (1°C) above 98.6°F (37°C) within 24 hours after a transfusion; it may involve rigors, chills, and discomfort 9. The fever occurs more often in patients who have been transfused repeatedly and in patients who have been pregnant 19. Leukoreduction, which is the removal or filtration of white blood cells from donor blood, has decreased Febrile Nonhemolytic Transfusion Reaction rates 20. Febrile Nonhemolytic Transfusion Reactions are caused by platelet transfusions more often than RBC transfusions and have an incidence that ranges from less than 1 percent to more than 35 percent 15.
You may get a sudden fever during or within a day of your blood transfusion. This is usually your body’s normal response to white blood cells in the donated blood. Over-the-counter fever medicine usually will treat the fever.
Two mechanisms have been proposed to explain Febrile Nonhemolytic Transfusion Reactions: a release of antibody-mediated endogenous pyrogen, and a release of cytokines. Common cytokines that may be associated with Febrile Nonhemolytic Transfusion Reactions include interleukin-1, interleukin-6, interleukin-8, and tumor necrosis factor 19. Febrile Nonhemolytic Transfusion Reaction is a diagnosis of exclusion that can be made only after ruling out other causes of fever (e.g., hemolysis, sepsis).
Some blood banks remove white blood cells from whole blood or different parts of the blood. This makes it less likely that you will have a reaction after the transfusion.
Iron Overload
Getting many blood transfusions can cause too much iron to build up in your blood (iron overload). People who have a blood disorder like thalassemia, which requires multiple transfusions, are at risk for iron overload. Iron overload can damage your liver, heart, and other parts of your body.
If you have iron overload, you may need iron chelation therapy. For this therapy, medicine is given through an injection or as a pill to remove the extra iron from your body.
Transfusion-Related Acute Lung Injury (TRALI)
Although it’s unlikely, blood transfusions can damage your lungs, making it hard to breathe. This usually occurs within about 6 hours of the blood transfusion procedure. Transfusion-related acute lung injury (TRALI) can happen with any type of transfusion, but is much more likely in people who are already seriously ill. Transfusions that contain more plasma, such as fresh frozen plasma or platelets, seem more likely to result in TRALI. It often starts within 1 to 2 hours of starting the transfusion, but can happen anytime up to 6 hours after a transfusion. There’s also a delayed transfusion-related acute lung injury (TRALI) syndrome, which can begin up to 72 hours after the transfusion is given.
The main symptom of TRALI is trouble breathing, which can become life-threatening. If TRALI is suspected during a transfusion, the transfusion should be stopped right away.
Most patients recover. However, 5 to 25 percent of patients who develop lung injuries die from the injuries. These people usually were very ill before their blood transfusion.
Doctors aren’t completely sure why blood transfusions damage the lungs. Antibodies (proteins) that are more likely to be found in the plasma of women who have been pregnant may disrupt the normal way that lung cells work. Antineutrophil cytoplasmic antibodies or anti-HLA antibodies activate the recipient’s immune system, resulting in massive pulmonary edema 16. Activated neutrophils in the lungs may also secrete proteolytic enzymes, leading to more tissue damage 21. Optimal methods for detecting these antibodies in donated products have yet to be determined 15. Because of this risk, hospitals are starting to use men’s and women’s plasma differently. Mortality in the United Kingdom decreased significantly after donor plasma from men was used exclusively 16. In 2006, TRALI was the leading cause of transfusion-related mortality, contributing to 50.7 percent of transfusion-related deaths 15. The TRALI working group of the AABB recommends using male-predominant plasma for transfusions 16. Because this policy excludes a large number of female donors, maintaining an adequate supply of plasma and platelets is a concern.
Doctors believe that several factors are involved in this illness. Many of the patients who get TRALI have had recent surgery, trauma, cancer treatment, transfusions, or have an active infection. Most of the time, TRALI goes away within 2 or 3 days if the person is helped with oxygen, fluids, and sometimes a breathing machine. Even with this kind of treatment, it’s deadly in 5% to 10% of cases. TRALI is more likely to be fatal if the patient was already very ill before the transfusion.
Delayed TRALI has been observed in people who are already critically ill or seriously injured. These patients have a higher risk of death. If a patient who has had TRALI in the past needs red blood cells, doctors may try to prevent it by removing most of the plasma from the red blood cells or by taking other measures. Researchers are working on other ways to reduce the risk of TRALI.
Transfusion Associated Circulatory Overload
Transfusion-associated circulatory overload is the result of a rapid transfusion of a blood volume that is more than what the recipient’s circulatory system can handle. It is not associated with an antibody-mediated reaction. Those at highest risk are recipients with underlying cardiopulmonary compromise, renal failure, or chronic anemia, and infants or older patients 16. Signs and symptoms include tachycardia, cough, dyspnea, hypertension, elevated central venous pressure, elevated pulmonary wedge pressure, and widened pulse pressure. Cardiomegaly and pulmonary edema are often seen on chest radiography 22.
The diagnosis is made clinically, but may be assisted by measuring brain natriuretic peptide levels, which are elevated in response to an increase in filling pressure 23. A study comparing patients who have transfusion-associated circulatory overload with patients who have TRALI found significantly greater levels of brain natriuretic peptide in those with transfusion-associated circulatory overload 23. Transfusion of lower volumes or at a slower rate may help prevent it 15. The treatment is diuresis to decrease volume overload.
Acute Immune Hemolytic Reaction
Acute immune hemolytic reaction is the most serious type of transfusion reaction, but also very rare. It occurs if the blood type you get during a transfusion doesn’t match or work with your blood type. Your body’s antibodies attack the transfused red blood cells, causing them to break open (hemolyze) and release harmful substances into the bloodstream that harm your kidneys.
Hemolytic transfusion reactions are caused by immune destruction of transfused RBCs, which are attacked by the recipient’s antibodies. The antibodies to the antigens of the ABO blood group or alloantibodies to other RBC antigens are produced after immunization through a previous transfusion or pregnancy. There are two categories of hemolytic transfusion reactions: acute and delayed. Nonimmune causes of acute reactions include bacterial overgrowth, improper storing, infusion with incompatible medications, and infusion of blood through lines containing hypotonic solutions or small-bore intravenous tubes 15.
The incidence of acute hemolytic reactions is approximately one to five per 50,000 transfusions 24. From 1996 to 2007, there were 213 ABO-incompatible red blood cell (RBC) transfusions with 24 deaths 16. Systems using bar codes for blood and patient identification have decreased errors 16.
The symptoms include chills, fever, chest and lower back pain, and nausea. The kidneys may be badly damaged, and dialysis may be needed. A hemolytic reaction can be deadly if the transfusion is not stopped as soon as the reaction starts.
The doctor will stop the transfusion at the first sign of this reaction.
Delayed Hemolytic Reaction
This type of reaction happens when the body slowly attacks antigens (other than ABO antigens) on the transfused blood cells. The blood cells are broken down days or weeks after the transfusion. There are usually no symptoms, but the transfused red blood cells are destroyed and the patient’s red blood cell count falls. In rare cases, the kidneys may be affected, and treatment may be needed.
People don’t usually have this type of reaction unless they have had many transfusions in the past. Those who do have this reaction need special blood tests before any more blood can be transfused. Units of blood that do not have the antigen that the body is attacking must be used.
Both acute and delayed hemolytic reactions are most common in patients who have had a previous transfusion.
Graft-Versus-Host Disease
Graft-versus-host disease (GVHD) is a condition in which donor’s lymphocytes proliferating and causing an immune attack against the recipient’s tissues and organs. Graft-versus-host disease is fatal in more than 90 percent of cases 15. People who have weakened immune systems are the most likely to get Graft-Versus-Host Disease. Risk factors include a history of fludarabine (Oforta) treatment, Hodgkin disease, stem cell transplant, intensive chemotherapy, intrauterine transfusion, or erythroblastosis fetalis. Other probable risk factors include a history of solid tumors treated with cytotoxic drugs, transfusion in premature infants, and recipient-donor pairs from homogenous populations 25.
Symptoms start within a month of the blood transfusion. They include fever, rash, and diarrhea. To protect against Graft-Versus-Host Disease, people who have weakened immune systems should receive blood that has been treated so the white blood cells can’t cause Graft-Versus-Host Disease.
To prevent white blood cells from causing GVHD, donated blood can be treated with radiation before transfusion. Radiation stops white blood cells from working but does not affect red blood cells. These are called irradiated blood products. They are often used for people with cancer.
Alternatives to Blood Transfusions
Researchers are trying to find ways to make blood. There’s currently no man-made alternative to human blood. However, researchers have developed medicines that may help do the job of some blood parts.
For example, some people who have kidney problems can now take a medicine called erythropoietin that helps their bodies make more red blood cells. This means they may need fewer blood transfusions.
Surgeons try to reduce the amount of blood lost during surgery so that fewer patients need blood transfusions. Sometimes they can collect and reuse the blood for the patient.
A blood transfusion will only be recommended if it’s needed and other treatments won’t help.
If it’s possible that you’ll need a transfusion – for example, if you’re due to have surgery or you have anemia – you may sometimes be given medicine to:
- lower your risk of bleeding, such as tranexamic acid
- boost your number of red blood cells, such as iron tablets or injections
These can reduce your chances of needing a blood transfusion.
Volume expanders
When a patient has lost a lot of fluids, the body can go into a type of shock. This may be treated or prevented by giving solutions to expand fluid volume in order to keep blood circulating through vital organs. The solutions are put right into the bloodstream through a vein. They boost fluid volume and help with circulation, but don’t carry oxygen or raise the number of blood cells.
Growth factors
The body naturally makes hormone-like substances called hematopoietic growth factors that cause the bone marrow to make more blood cells. Man-made versions of some of these growth factors are available to help people with low blood cell counts. Growth factors can be used to boost red blood cell, white blood cell, or platelet counts.
Growth factors may help patients who would otherwise need transfusions. But they have some drawbacks that may limit their use in some cases:
- Unlike transfusions, growth factors often take many days or weeks to raise blood counts, so they may not be useful in people who need their blood cell levels raised quickly, such as those who are actively bleeding.
- People who have severe bone marrow disease may not respond to the growth factors because they don’t have enough blood-producing cells in their bone marrow.
- Some growth factors might cause certain types of cancer cells (such as lymphocytic leukemia, multiple myeloma, head and neck cancer, breast cancer, cervical cancer, and some kinds of lung cancer cells) to grow more quickly.
- Growth factors generally cost a lot more than transfusions.
Because of these drawbacks, certain growth factors are not used in people whose treatment is expected to cure their cancer. And when they are used, they are given for as short a time as possible.
Intra-operative or post-operative blood salvage
Patients getting surgery sometimes need transfusions to replace blood lost during or after the operation. Sometimes this lost blood can be “salvaged” or saved by collecting it with a special machine and giving it back into the patient.
Giving a person back his or her own blood is called an autologous transfusion. It cuts down on the need for transfusions from other donors. But some studies have found tumor cells in blood salvaged during cancer operations, and this isn’t something that can be done for all patients.
- King KE, Bandarenko N. Blood Transfusion Therapy: A Physician’s Handbook. 9th ed. Bethesda, Md.: American Association of Blood Banks; 2008:236.[↩][↩][↩][↩]
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415–426.[↩][↩][↩]
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group [published correction appears in N Engl J Med. 1999;340(13):1056]. N Engl J Med. 1999;340(6):409–417.[↩][↩]
- Carless PA, Henry DA, Carson JL, Hebert PP, McClelland B, Ker K. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2010;(10):CD002042.[↩]
- Lacroix J, Hébert PC, Hutchison JS, et al.; TRIPICU Investigators; Canadian Critical Care Trials Group; Pediatric Acute Lung Injury and Sepsis Investigators Network. Transfusion strategies for patients in pediatric intensive care units. N Engl J Med. 2007;356(16):1609–1619.[↩][↩]
- Practice parameter for the use of fresh-frozen plasma, cryoprecipitate, and platelets. Fresh-Frozen Plasma, Cryoprecipitate, and Platelets Administration Practice Guidelines Development Task Force of the College of American Pathologists. JAMA. 1994;271(10):777–781.[↩]
- Liumbruno G, Bennardello F, Lattanzio A, Piccoli P, Rossetti G; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI) Work Group. Recommendations for the transfusion of plasma and platelets. Blood Transfus. 2009;7(2):132–150.[↩][↩]
- Transfusion of Blood and Blood Products: Indications and Complications. Am Fam Physician. 2011 Mar 15;83(6):719-724. https://www.aafp.org/afp/2011/0315/p719.html[↩][↩][↩][↩][↩]
- British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of platelet transfusions. Br J Haematol. 2003;122(1):10–23.[↩][↩]
- Slichter SJ. Platelet transfusion therapy. Hematol Oncol Clin North Am. 2007;21(4):697–729, vii.[↩]
- Rebulla P, Finazzi G, Marangoni F, et al. The threshold for prophylactic platelet transfusions in adults with acute myeloid leukemia. Gruppo Italiano Malattie Ematologiche Maligne dell’Adulto. N Engl J Med. 1997;337(26):1870–1875.[↩]
- Callum JL, Karkouti K, Lin Y. Cryoprecipitate: the current state of knowledge. Transfus Med Rev. 2009;23(3):177–188.[↩]
- Poterjoy BS, Josephson CD. Platelets, frozen plasma, and cryoprecipitate: what is the clinical evidence for their use in the neonatal intensive care unit? Semin Perinatol. 2009;33(1):66–74.[↩]
- Reutter JC, Sanders KF, Brecher ME, Jones HG, Bandarenko N. Incidence of allergic reactions with fresh frozen plasma or cryo-supernatant plasma in the treatment of thrombotic thrombocytopenic purpura. J Clin Apher. 2001;16(3):134–138.[↩]
- Hendrickson JE, Hillyer CD. Noninfectious serious hazards of transfusion. Anesth Analg. 2009;108(3):759–769.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Vamvakas EC, Blajchman MA. Transfusion-related mortality: the ongoing risks of allogeneic blood transfusion and the available strategies for their prevention. Blood. 2009;113(15):3406–3417.[↩][↩][↩][↩][↩][↩][↩]
- Pineda AA, Taswell HF. Transfusion reactions associated with anti-IgA antibodies: report of four cases and review of the literature. Transfusion. 1975;15(1):10–15.[↩]
- http://resources.transfusion.com.au/cdm/singleitem/collection/p16691coll1/id/120/rec/3[↩]
- Addas-Carvalho M, Salles TS, Saad ST. The association of cytokine gene polymorphisms with febrile non-hemolytic transfusion reaction in multitransfused patients. Transfus Med. 2006;16(3):184–191.[↩][↩]
- King KE, Shirey RS, Thoman SK, Bensen-Kennedy D, Tanz WS, Ness PM. Universal leukoreduction decreases the incidence of febrile nonhemolytic transfusion reactions to RBCs (red blood cells). Transfusion. 2004;44(1):25–29.[↩]
- Stack G, Tormey CA. alpha1-Antitrypsin deficiency is a possible first event in the two-event model of transfusion-related acute lung injury: a proposal and case report. Transfusion. 2008;48(11):2477–2478.[↩]
- Popovsky MA. Transfusion-associated circulatory overload: the plot thickens. Transfusion. 2009;49(1):2–4.[↩]
- Zhou L, Giacherio D, Cooling L, Davenport RD. Use of B-natriuretic peptide as a diagnostic marker in the differential diagnosis of transfusion-associated circulatory overload. Transfusion. 2005;45(7):1056–1063.[↩][↩]
- Lichtiger B, Perry-Thornton E. Hemolytic transfusion reactions in oncology patients: experience in a large cancer center. J Clin Oncol. 1984;2(5):438–442.[↩]
- Webb I, Anderson KC. TA-GVHD. In: Anderson KC, ed. Scientific Basis of Transfusion Medicine: Implications for Clinical Practice. 2nd ed. Philadelphia, Pa.: Saunders; 2000:420–426.[↩]





{kind=link}