
Contents
What are blood vessels
Blood vessels are not rigid tubes that simply direct the flow of blood but rather are dynamic structures that pulsate, constrict and relax, and even proliferate, according to the changing needs of the body.
When the heart contracts, it forces blood into the large arteries that leave the ventricles. The blood then moves into successively smaller branches of arteries, finally reaching the smallest branches, the arterioles, which feed into the capillaries of the organs. Blood leaving the capillaries is collected by venules, small veins that merge to form larger veins that ultimately empty into the heart. This pattern of vessels applies to both the pulmonary and systemic circuits.
Altogether, the blood vessels in an adult human body stretch for 100,000 km or 60,000 miles, a distance equivalent to almost 2.5 times around the Earth. Notice that arteries are said to “branch,” “diverge,” or “fork” as they carry blood away from the heart. Veins, by contrast, are said to “join,” “merge,” “converge,” or “serve as tributaries” as they carry blood toward the heart.
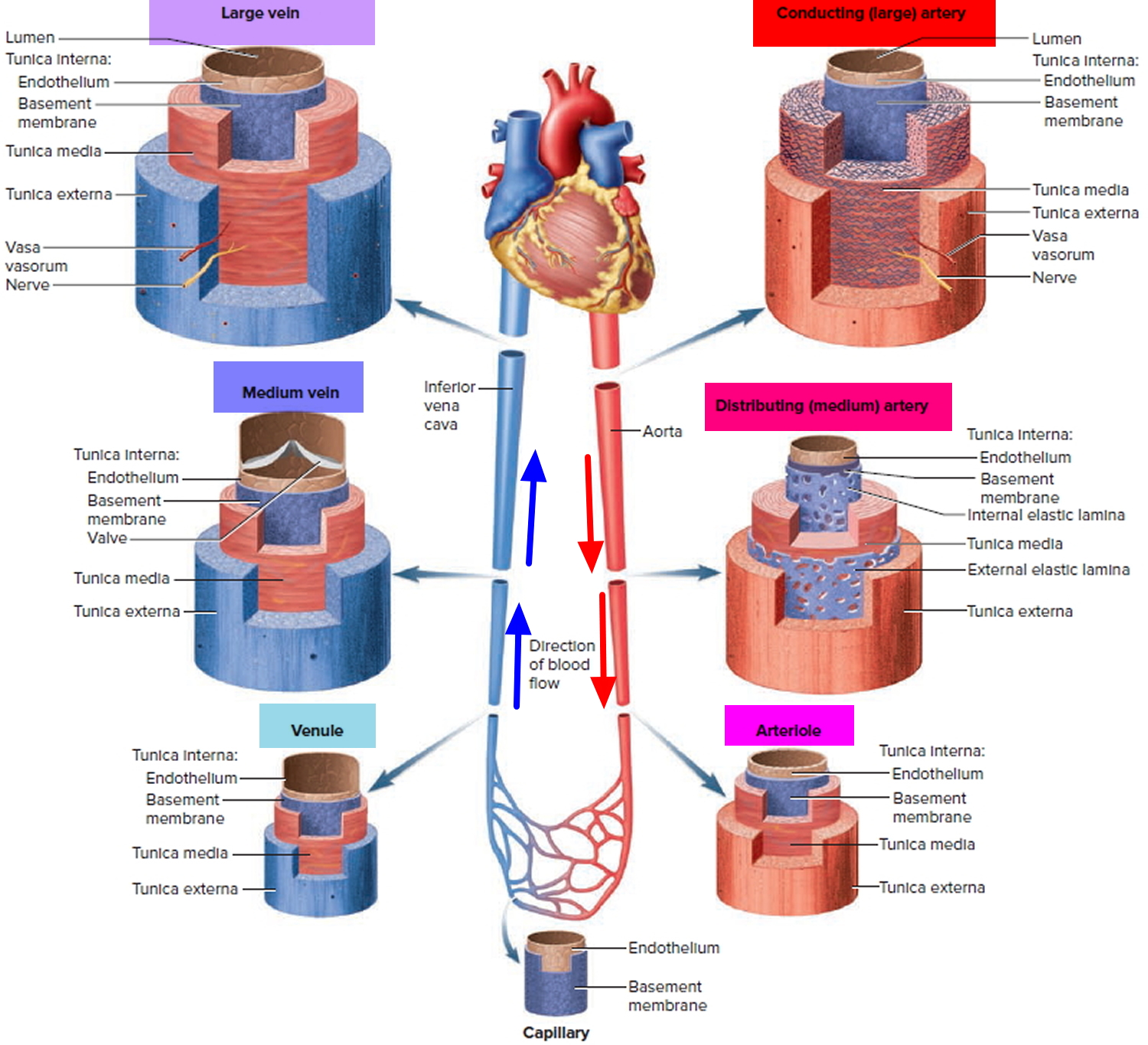
Figure 1. Blood vessels
The total blood volume is unevenly distributed among arteries, veins, and capillaries. The heart, arteries, and capillaries contain approximately 30–35 percent of the blood volume (about 1.5 Liter of whole blood), and the venous system contains the rest (65–70 percent, or about 3.5 Liters). Because the walls of veins are thinner and contain more elastic tissue and less smooth muscle than those of arteries, veins are much more distensible (stretchable) than arteries. For a given rise in blood pressure, a typical vein stretches about eight times as much as a corresponding artery.
The capacitance of a blood vessel is the relationship between the volume of blood it contains and the blood pressure, and veins are called capacitance vessels. Because veins have high capacitance, they act as blood reservoirs, which can accommodate large changes in blood volume. If the blood volume rises or falls, the elastic walls stretch or recoil, respectively, changing the volume of blood in the venous system. If serious hemorrhaging (blood loss) occurs, sympathetic nerves stimulate smooth muscle cells in the walls of medium-sized veins in the systemic system to constrict. This process, called venoconstriction reduces the volume of blood within the venous system, increasing the volume within the arterial system and capillaries. Reducing the amount of blood in the venous system maintains the blood volume within the arterial system at near-normal levels despite a significant blood loss. As a result, blood flow to active skeletal muscles and delicate organs, such as the brain, can be increased or maintained.
Layers of blood vessels
The wall of a blood vessel consists of three layers, or tunics, of different tissues:
- an epithelial inner lining,
- a middle layer consisting of smooth muscle and elastic connective tissue, and
- a connective tissue outer covering.
The three structural layers of a generalized blood vessel from innermost to outermost are the tunica interna (intima), tunica media, and tunica externa (adventitia) (Figure 2). Modifications of this basic design account for the five types of blood vessels and the structural and functional differences among the various vessel types. Always remember that structural variations correlate to the differences in function that occur throughout the cardiovascular system.
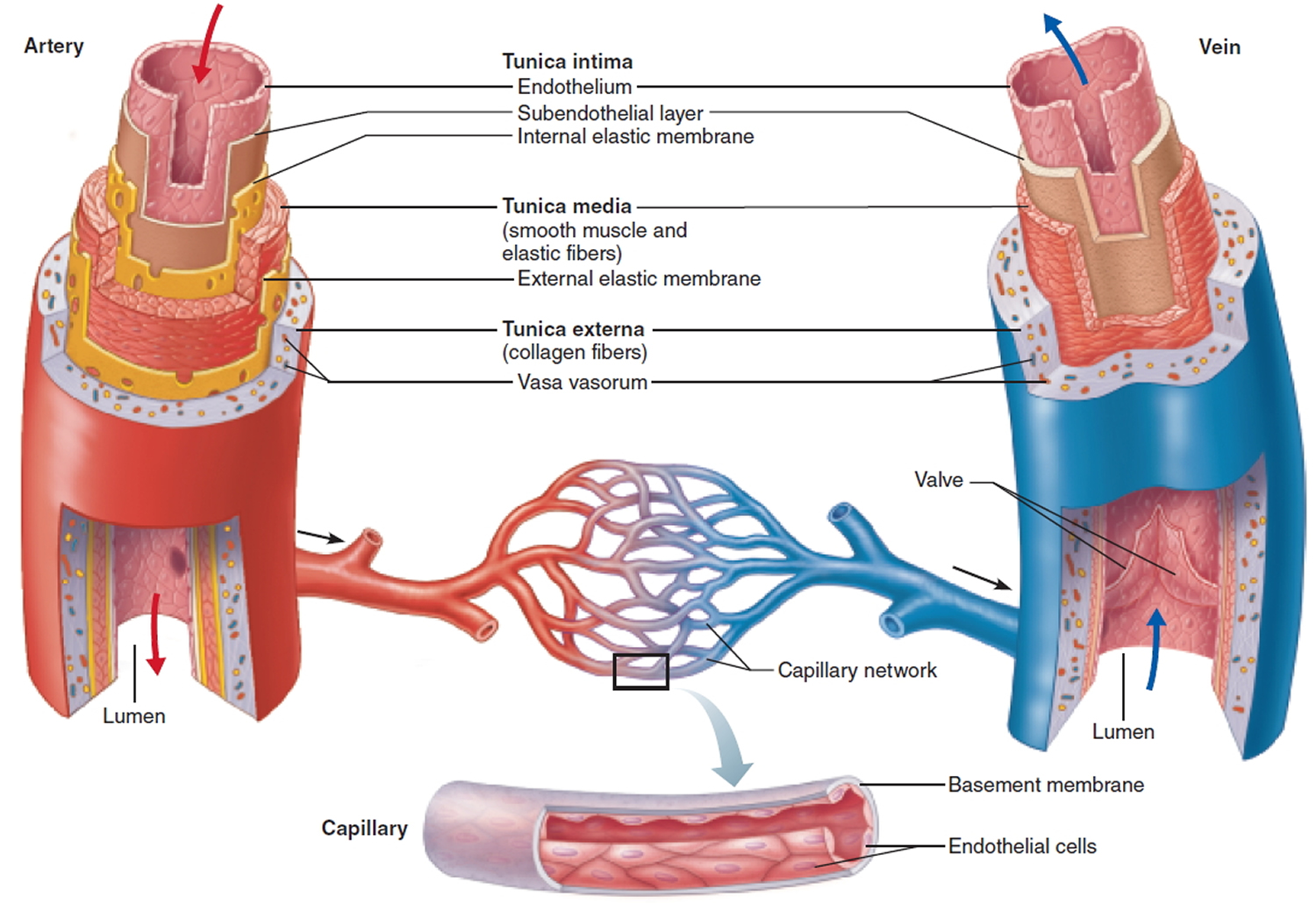
Figure 2. Layers of blood vessels
Tunica Interna
The tunica interna (intima) forms the inner lining of a blood vessel and is in direct contact with the blood as it flows through the lumen or interior opening, of the vessel. Although this layer has multiple parts, these tissue components contribute minimally to the thickness of the vessel wall. Its innermost layer is called endothelium, which is continuous with the endocardial lining of the heart. The endothelium is a thin layer of flattened cells that lines the inner surface of the entire cardiovascular system (heart and blood vessels). It is now known that endothelial cells are active participants in a variety of vessel-related activities, including physical influences on blood flow, secretion of locally acting chemical mediators that influence the contractile state of the vessel’s overlying smooth muscle, and assistance with capillary permeability. In addition, their smooth luminal surface facilitates eff icient blood flow by reducing surface friction.
The second component of the tunica interna is a basement membrane deep to the endothelium. It provides a physical support base for the epithelial layer. Its framework of collagen fibers affords the basement membrane significant tensile strength, yet its properties also provide resilience for stretching and recoil. The basement membrane anchors the endothelium to the underlying connective tissue while also regulating molecular movement. It appears to play an important role in guiding cell movements during tissue repair of blood vessel walls.
The outermost part of the tunica interna, which forms the boundary between the tunica interna and tunica media, is the internal elastic lamina. The internal elastic lamina is a thin sheet of elastic fibers with a variable number of window like openings that give it the look of Swiss cheese. These openings facilitate diffusion of materials through the tunica interna to the thicker tunica media.
Tunica Media
The tunica media (media = middle) is a muscular and connective tissue layer that displays the greatest variation among the different vessel types. In most vessels, it is a relatively thick layer comprising mainly smooth muscle cells and substantial amounts of elastic fibers. The primary role of the smooth muscle cells, which extend circularly around the lumen like a ring encircles your finger, is to regulate the diameter of the lumen. An increase in sympathetic stimulation typically stimulates the smooth muscle to contract, squeezing the vessel wall and narrowing the lumen. Such a decrease in the diameter of the lumen of a blood vessel is called vasoconstriction. In contrast, when sympathetic stimulation decreases, or in the presence of certain chemicals (such as nitric oxide, H+, and lactic acid) or in response to blood pressure, smooth muscle fibers relax. The resulting increase in lumen diameter is called vasodilation.The rate of blood flow through different parts of the body is regulated by the extent of smooth muscle contraction in the walls of particular vessels. Furthermore, the extent of smooth muscle contraction in particular vessel types is crucial in the regulation of blood pressure.
In addition to regulating blood flow and blood pressure, smooth muscle contracts when a small artery or arteriole is damaged (vascular spasm) to help limit loss of blood through the injured vessel. Smooth muscle cells also help produce the elastic fibers within the tunica media that allow the vessels to stretch and recoil under the applied pressure of the blood.
The tunica media is the most variable of the tunics. Separating the tunica media from the tunica externa is a network of elastic fibers, the external elastic lamina, which is part of the tunica media.
Tunica Externa
The outer covering of a blood vessel, the tunica externa (externa = outermost), consists of elastic and collagen fibers. The tunica externa contains numerous nerves and especially in larger vessels, tiny blood vessels that supply the tissue of the vessel wall. These small vessels that supply blood to the tissues of the vessel are called vasa vasorum, or vessels to the vessels. They are easily seen on large vessels such as the aorta. In addition to the important role of supplying the vessel wall with nerves and self-vessels, the tunica externa helps anchor the vessels to surrounding tissues.
Types of blood vessels
The five main types of blood vessels are:
- Arteries,
- Arterioles,
- Capillaries,
- Venules,
- Veins.
Arteries carry blood away from the heart to other organs. Large, elastic arteries leave the heart and divide into medium-sized, muscular arteries that branch out into the various regions of the body.
Medium-sized arteries then divide into small arteries, which in turn divide into still smaller arteries called arterioles. As the arterioles enter a tissue, they branch into numerous tiny vessels called blood capillaries or simply capillaries.
The thin walls of capillaries allow the exchange of substances between the blood and body tissues. Groups of capillaries within a tissue re -unite to form small veins called venules (little veins). These in turn merge to form progressively larger blood vessels called veins.
Veins are the blood vessels that convey blood from the tissues back to the heart.
Circulatory Routes
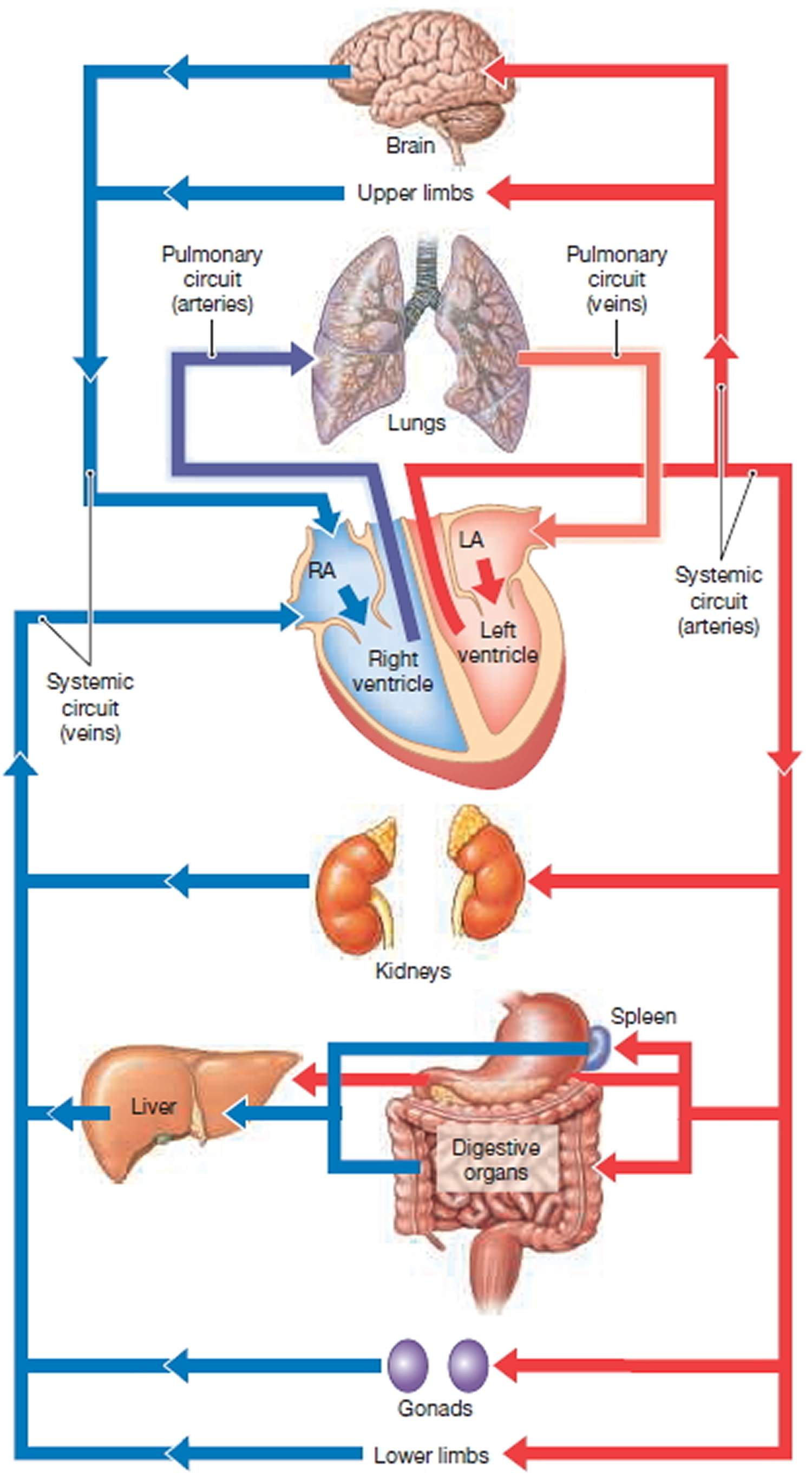
The simplest and most common route of blood flow is heart → arteries → capillaries → veins → heart. Blood usually passes through only one network of capillaries from the time it leaves the heart until the time it returns (Figure 3), but there are exceptions, notably portal systems and anastomoses.
Figure 3. Circulatory Routes
Arteries
Arteries are vessels that carry blood away from the heart. It is a common misconception that all arteries carry oxygen-rich blood, whereas all veins carry oxygen-poor blood. This statement is correct for the systemic circuit, but it is not correct for the pulmonary circuit, whose arteries carry oxygen-poor blood to the lungs for oxygenation.
The passage of blood through the arteries proceeds from elastic arteries, to muscular arteries, to arterioles.
Elastic Arteries
Elastic arteries are the largest arteries near the heart—the aorta and its major branches—with diameters ranging from 2.5 cm (about the width of the thumb) to 1 cm (slightly less than the width of the little finger). Their large lumen allows them to serve as low-resistance conduits for conducting blood between the heart and the medium-sized muscular arteries. For this reason, elastic arteries are sometimes called conducting arteries. More elastin occurs in the walls of these arteries than in any other type of vessel, and the sheets of elastin in the tunica media are remarkably thick. The high elastin content of conducting arteries dampens the surges of blood pressure resulting from the rhythmic contractions of the heart. When the heart forces blood into the arteries, the elastic elements in these vessels expand in response to increased blood pressure, in effect storing some of the energy of the flowing fluid; then, when the heart relaxes, the elastic elements recoil, propelling the blood onward. As the blood proceeds through smaller arteries, there is a marked decline both in its absolute pressure (due to resistance imparted by the arterial walls) and in the size of the pressure vacillations (due to the elastic recoil of the arteries just described). By the time the blood reaches the thin-walled capillaries, which are too fragile to withstand strong surges in blood pressure, the pressure of the blood is considerably lower and completely steady.
Muscular Arteries
Muscular (distributing) arteries lie distal to the elastic arteries and supply groups of organs, individual organs, and parts of organs. These “middle-sized” arteries constitute most of the named arteries seen in the anatomy laboratory. They range in diameter from about 1 cm to 0.3 mm.
The following features distinguish muscular arteries:
- The tunica media of muscular arteries is thicker relative to the size of the lumen than that of any other type of vessel. By actively changing the diameter of the artery, this muscular layer regulates the amount of blood flowing to an organ according to the specific needs of that organ.
- The smooth muscle of the tunica media of muscular arteries is sandwiched between two thick sheets of elastin: A wavy internal elastic membrane forms the outer layer of the tunica intima, and an external elastic membrane forms the outer layer of the tunica media. These elastic membranes, in addition to the thin sheets of elastin found within the tunica media, help to dampen the pulsatile pressure produced by the heartbeat.
Arterioles
Arterioles are the smallest arteries, with diameters ranging from about 0.3 mm to 10 μm. Their tunica media contains only one or two layers of smooth muscle cells. Larger arterioles have all three tunics plus an internal elastic network in the tunica intima. Smaller arterioles, which lead into the capillary beds, are little more than a single layer of smooth muscle cells spiraling around an underlying endothelium.
The diameter of each arteriole is regulated in two ways:
- Local factors in the tissues signal the smooth muscle cells to contract or relax, thus regulating the amount of blood sent downstream to each capillary bed; and
- The sympathetic nervous system adjusts the diameter of arterioles throughout the body to regulate systemic blood pressure. For example, a widespread sympathetic vasoconstriction raises blood pressure during fight-or-flight responses.
Capillaries
Capillaries are the smallest blood vessels, with a diameter of 8–10 μm, just large enough to enable erythrocytes to pass through in single file. They are composed of only a single layer of endothelial cells surrounded by a basement membrane. They are the body’s most important blood vessels because they renew and refresh the surrounding tissue fluid (interstitial fluid) with which all body cells are in contact. Capillaries deliver to this fluid the oxygen and nutrients cells need, and they remove the carbon dioxide and nitrogenous wastes that cells deposit into the fluid. Along with these universal functions, some capillaries also perform site-specific functions. In the lungs, oxygen enters the blood (and carbon dioxide leaves it) through capillaries. Capillaries in the small intestine receive digested nutrients; those in the endocrine glands pick up hormones; and those in the kidneys remove nitrogenous wastes from the body. There are three types of capillaries: continuous, fenestrated, and sinusoids.
Types of Capillaries
There are three types of capillaries, distinguished by the ease with which they allow substances to pass through their walls and by structural differences that account for their greater or lesser permeability.
1)Continuous Capillaries
Continuous capillaries are the most common type of capillary, occurring in most organs of the body such as skeletal muscles, skin, and the central nervous system.
Tight junctions and occasional desmosomes hold the capillary endothelial cells together. These tight junctions block the passage of small molecules, but they do not surround the whole perimeter of the endothelial cells. There are gaps of unjoined membrane called intercellular clefts that allow small molecules to pass into and out of the capillary. External to the endothelial cells, the delicate capillary is strengthened and stabilized by scattered pericytes, spider-shaped contractile stem cells whose thin processes form a widely spaced network around the capillary. Pericytes help control capillary permeability and can give rise to new vessels.
2) Fenestrated Capillaries
Like continuous capillaries, the endothelial cells of fenestrated capillaries are joined by tight junctions and contain intercellular clefts. In addition, fenestrated capillaries have pores (fenestrations, or “windows”) spanning the endothelial cells. Fenestrated capillaries occur only where there are exceptionally high rates of exchange of small molecules between the blood and the surrounding tissue fluid. For example, capillaries in the small intestine, which receive the digested nutrients from food; capillaries in the glomeruli of the kidneys, which filter blood; capillaries in the endocrine glands, which pick up secreted hormones; and capillaries in the synovial membranes of joints, where many water molecules exit the blood to contribute to the synovial fluid.
3) Sinusoid Capillaries (Sinusoids)
Some organs contain wide, leaky capillaries called sinusoids or sinusoid capillaries. Each sinusoid follows a twisted path and has both expanded and narrowed regions. Sinusoids are usually fenestrated, and their endothelial cells have fewer cell junctions than do other capillaries. In some sinusoids, in fact, the intercellular clefts are wide open. Sinusoids occur wherever there is an extensive exchange of large materials, such as proteins or cells, between the blood and surrounding tissue. For example, they occur in the bone marrow and spleen, where many blood cells move through their walls. The large diameter and twisted course of sinusoids ensure that blood slows when flowing through these vessels, allowing time for the many exchanges that occur across their walls.
Capillary Permeability
Molecules pass into and out of capillaries through four routes.
- Direct diffusion through the endothelial cell membranes. Carbon dioxide and oxygen seem to be the only important molecules that diffuse directly through endothelial cells, because these uncharged molecules easily diffuse through the lipid-containing membranes of cells.
- Intercellular clefts. Most small molecules are exchanged through the intercellular clefts. In sinusoids, larger molecules and cells are exchanged through the wide intercellular clefts.
- Fenestrations. In fenestrated capillaries, the pores in the endothelial cells allow passage of many small molecules.
- Pinocytotic vesicles. Pinocytotic vesicles invaginate from the plasma membrane and migrate across the endothelial cells, transporting dissolved gases, nutrients, and waste products into the capillary.
Low-Permeability Capillaries: The Blood Brain Barrier
The blood brain barrier, which prevents all but the most vital molecules (and normally even leukocytes) from leaving the blood and entering brain tissue, derives from the structure of capillaries in the brain. These capillaries lack the structural features that account for capillary permeability: Brain capillaries are continuous capillaries with complete tight junctions; intercellular clefts are absent. The vital molecules, such as glucose, that must cross brain capillaries are “ushered through” by highly selective transport mechanisms in the plasma membranes of the endothelial cells. The blood brain barrier is not a barrier against uncharged and lipid-soluble molecules such as oxygen, carbon dioxide, and some anesthetics, which diffuse unhindered through the endothelial cells and freely enter brain tissue.
During prolonged emotional stress, the tight junctions between the endothelial cells of brain capillaries are opened, so that the blood brain barrier fails and toxic substances in the blood can enter brain tissue. Further study of the disruption of the blood brain barrier could one day help medical researchers who are seeking ways to deliver beneficial drugs—antibiotics and chemicals to kill brain tumors—into the brain.
Capillary Beds
Capillaries supply body tissues through structures called capillary beds. A capillary bed is a network of the body’s smallest vessels. Capillary beds run throughout almost all tissues, especially the loose connective tissues. A terminal arteriole leads to a metarteriole—a vessel that is structurally intermediate between an arteriole and a capillary—from which branch true capillaries. The metarteriole continues into a thoroughfare channel, a vessel structurally intermediate between a capillary and a venule. True capillaries merge into the thoroughfare channel, which then joins a venule. Smooth muscle cells called precapillary sphincters wrap around the root of each true capillary where it leaves the metarteriole.
The precapillary sphincters regulate the flow of blood to the tissue according to that tissue’s needs for oxygen and nutrients. When the tissue is functionally active, the sphincters are relaxed, enabling blood to flow through the wide-open capillaries and supply the surrounding tissue cells. When the tissue has lower demands (such as when nearby tissue cells already have adequate oxygen), the precapillary sphincters contract, closing off the true capillaries and forcing blood to flow straight from the metarteriole into the thoroughfare channel and venule—thereby bypassing the true capillaries. In this way, capillary beds precisely control the amount of blood supplying a tissue at any time.
Most tissues and organs have a rich capillary supply, but not all do. Tendons and ligaments are poorly vascularized. Epithelia and cartilage contain no capillaries; instead, they receive nutrients indirectly via diffusion from nearby vascularized connective tissues. The cornea and the lens have no capillary supply at all and are nourished by the aqueous humor and other sources.
Venous Vessels
Veins are the blood vessels that conduct blood from the capillaries toward the heart. Veins in the systemic circuit carry blood that is relatively oxygen-poor, but the pulmonary veins carry oxygen-rich blood returning from the lungs.
Venules
The smallest veins are called venules and are 8–100 μm in diameter. The smallest venules, called postcapillary venules, consist of an endothelium on which lie pericytes. These venules function very much like capillaries. In fact, during inflammatory responses, more fluid and leukocytes leave the circulation through postcapillary venules than through capillaries. Larger venules have a tunica media that consists of one or two layers of smooth muscle cells and a thin tunica externa.
Veins
Venules join to form veins. Structurally, veins differs from arteries in the following ways:
- The lumen of a vein is larger than that of an artery of comparable size. At any given time, veins hold fully 65% of the body’s blood.
- In a vein, the tunica externa is thicker than the tunica media. In an artery, the tunica media is the thicker layer. In the body’s largest veins—the venae cavae, which return systemic blood to the heart—longitudinal bands of smooth muscle further thicken the tunica externa.
- Veins have less elastin in their walls than do arteries because veins do not need to dampen any pulsations (all of which are smoothed out by arteries before the blood reaches the veins).
- The wall of a vein is thinner than that of a comparable artery. Blood pressure declines substantially while blood passes through the high-resistance arterioles and capillary beds; thus, blood pressure in the veins is much lower than in the arteries.
Several mechanisms counteract the low venous blood pressure and help move the blood back to the heart. One structural feature of some veins is valves that prevent the backflow of blood away from the heart. Each of these valves has several cusps formed from the tunica intima. The flow of blood toward the heart pushes the cusps apart, opening the valve, and any backflow pushes the cusps together, closing the valve. Valves are most abundant in veins of the limbs, where the superior direction of venous flow is most directly opposed by gravity. A few valves occur in the veins of the head and neck, but none are located in veins of the thoracic and abdominal cavities.
One functional mechanism that aids the return of venous blood to the heart is the normal movement of the body and limbs, for instance, during walking. Swinging a limb moves the blood in the limb, and the venous valves ensure that this blood moves only in the proper direction. Another mechanism aiding venous return is the skeletal muscular pump, in which contracting skeletal muscles press against the thin-walled veins, forcing valves proximal to the area of contraction to open and propelling blood toward the heart. Valves distal to the contracting muscles are closed by backflowing blood.
The effectiveness of venous valves in preventing the backflow of blood is easily demonstrated. Hang one hand by your side until the veins on its dorsal surface become distended with blood. Next, place two fingertips against one of the distended veins, and, pressing firmly, move the superior finger proximally along the vein, and then release that finger. The vein stays flat and collapsed despite the pull of gravity. Finally, remove the distal fingertip, and watch the vein refill rapidly with blood.
Anastomoses
Most tissues of the body receive blood from more than one artery. The union of the branches of two or more arteries supplying the same body region is called an anastomosis. Anastomoses between arteries provide alternative routes for blood to reach a tissue or organ. If blood flow stops for a short time when normal movements compress a vessel, or if a vessel is blocked by disease, injury, or surgery, then circulation to a part of the body is not necessarily stopped. The alternative route of blood flow to a body part through an anastomosis is known as collateral circulation. Anastomoses may also occur between veins and between arterioles and venules. Arteries that do not anastomose are known as end arteries. Obstruction of an end artery interrupts the blood supply to a whole segment of an organ, producing necrosis (death) of that segment. Alternative blood routes may also be provided by nonanastomosing vessels that supply the same region of the body.
Arterial Sense Organs
Certain major arteries above the heart have sensory structures in their walls that monitor blood pressure and composition. These receptors transmit information to the brainstem that serves to regulate the heartbeat, blood vessel diameters, and respiration.
They are of three kinds:
- Carotid sinuses. These are baroreceptors—sensors that monitor blood pressure. Ascending the neck on each side is a common carotid artery, which branches near the angle of the mandible, forming the internal carotid artery to the brain and external carotid artery to the face. The carotid sinuses are located in the wall of the internal carotid artery just above the branch point. The carotid sinus has a relatively thin tunica media and an abundance of glossopharyngeal nerve fibers in the tunica externa. The role of the baroreceptors in adjusting blood pressure, called the baroreflex.
- Carotid bodies. Also located near the branch of the common carotid arteries, these are oval receptors about 3 × 5 mm in size, innervated by sensory fibers of the glossopharyngeal nerves. They are chemoreceptors—sensors that monitor changes in blood composition. They primarily transmit signals to the brainstem respiratory centers, which adjust breathing to stabilize the blood pH and its CO2 and O2 levels.
- Aortic bodies. These are one to three chemoreceptors located in the aortic arch near the arteries to the head and arms. They are structurally similar to the carotid bodies and have the same function, but transmit their signals to the brainstem via the vagus nerves.
Blood vessels function
Your heart and blood vessels make up your overall blood circulatory system. Your blood circulatory system is made up of four subsystems.
Arterial Circulation
Arterial circulation is the part of your circulatory system that involves arteries, like the aorta and pulmonary arteries. Arteries are blood vessels that carry blood away from your heart. (The exception is the coronary arteries, which supply your heart muscle with oxygen-rich blood.) The arteries carry oxygenated blood from the heart to the capillaries of organs throughout the body.
Healthy arteries are strong and elastic (stretchy). They become narrow between heartbeats, and they help keep your blood pressure consistent. This helps blood move through your body.
Arteries branch into smaller blood vessels called arterioles. Arteries and arterioles have strong, flexible walls that allow them to adjust the amount and rate of blood flowing to parts of your body.
Venous Circulation
Venous circulation is the part of your circulatory system that involves veins, like the vena cavae and pulmonary veins. Veins are blood vessels that carry blood to your heart.
Veins have thinner walls than arteries. Veins can widen as the amount of blood passing through them increases.
Capillary Circulation
Capillary circulation is the part of your circulatory system where oxygen, nutrients, and waste pass between your blood and parts of your body.
Capillaries are very small blood vessels. They connect the arterial and venous circulatory subsystems.
The importance of capillaries lies in their very thin walls. Oxygen and nutrients in your blood can pass through the walls of the capillaries to the parts of your body that need them to work normally.
Capillaries’ thin walls also allow waste products like carbon dioxide to pass from your body’s organs and tissues into the blood, where it’s taken away to your lungs.
Pulmonary Circulation
Blood entering the right atrium is returning from capillary beds in the peripheral tissues and myocardium where oxygen was released and carbon dioxide absorbed. After traveling through the right atrium and right ventricle, blood passes through the pulmonary valve and enters the pulmonary trunk, the start of the pulmonary circuit. This circuit, which contains approximately 9 percent of the total blood volume at any given moment, begins at the pulmonary valve and ends at the entrance to the left atrium. In the pulmonary circuit, oxygen is replenished and carbon dioxide is released. Compared with the systemic circuit, the pulmonary circuit is short: The base of the pulmonary trunk and the lungs are only about 15 cm (6 in.) apart.
The arteries of the pulmonary circuit carry deoxygenated (oxygen-poor) blood, which is different from the arteries of the systemic circuit. (For this reason, color-coded diagrams usually show the pulmonary arteries in blue, the same color as systemic veins.) The pulmonary trunk curves over the superior border of the heart, where it divides into the left and right pulmonary arteries. These large arteries enter the lungs before branching repeatedly, giving rise to smaller and smaller arteries. The smallest branches, the pulmonary arterioles, provide blood to capillary networks surrounding small air pockets, or alveoli, in the lungs. The walls of the alveoli are thin enough to allow gas exchange between the capillary blood and inspired air. As oxygenated (oxygen-rich) blood leaves the alveolar capillaries, it enters venules that merge to form larger and larger vessels carrying blood toward the pulmonary veins. These four veins, typically two from each lung, empty into the left atrium, to complete the pulmonary circuit.
Dilated blood vessels
Aneurysm
An aneurysm is a bulge or “ballooning” in the wall of an artery 1. Arteries have thick walls to withstand normal blood pressure. However, certain medical problems, genetic conditions, and trauma can damage or injure artery walls. The force of blood pushing against the weakened or injured walls can cause an aneurysm. If an aneurysm grows large, it can burst and cause dangerous bleeding or even death 2. About 13,000 Americans die each year from aortic aneurysms. Most of the deaths result from rupture or dissection.
An aneurysm can grow large and rupture (burst) or dissect. A rupture causes dangerous bleeding inside the body. A dissection is a split in one or more layers of the artery wall. The split causes bleeding into and along the layers of the artery wall.
Both rupture and dissection often are fatal.
Most aneurysms occur in the aorta, the main artery that runs from the heart through the chest and abdomen. An aneurysm that occurs in the chest portion of the aorta is called a thoracic aortic aneurysm. An aneurysm that occurs in the abdominal portion of the aorta is called an abdominal aortic aneurysm.
Aneurysms also can happen in arteries in the brain, heart and other parts of the body. If an aneurysm in the brain bursts, it causes a stroke.
Early diagnosis and treatment can help prevent rupture and dissection. However, aneurysms can develop and become large before causing any symptoms. Often doctors can stop aneurysms from bursting if they find and treat them early. They use imaging tests to find aneurysms. Often aneurysms are found by chance during tests done for other reasons. Medicines and surgery are the two main treatments for aneurysms.
Figure 5. Aortic Aneurysm
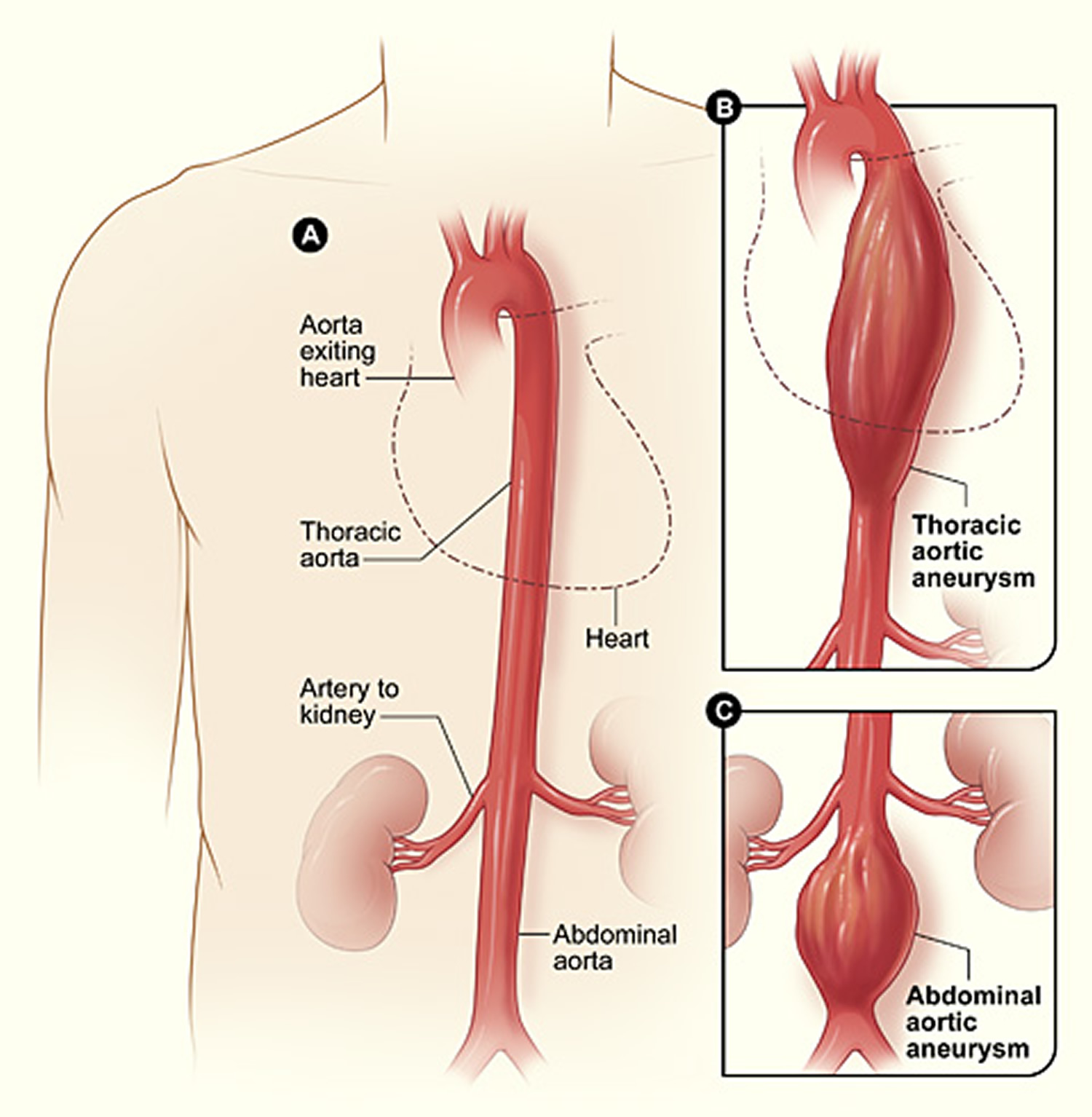
Note: (A) shows a normal aorta. Figure B shows a thoracic aortic aneurysm, which is located behind the heart. Figure C shows an abdominal aortic aneurysm, which is located below the arteries that supply blood to the kidneys.
Types of Aneurysms
Aortic Aneurysms
The two types of aortic aneurysm are abdominal aortic aneurysm and thoracic aortic aneurysm. Some people have both types.
Abdominal Aortic Aneurysms
An aneurysm that occurs in the abdominal portion of the aorta is called an abdominal aortic aneurysm. Most aortic aneurysms are abdominal aortic aneurysms.
These aneurysms are found more often now than in the past because of computed tomography scans, or CT scans, done for other medical problems.
Small abdominal aortic aneurysms rarely rupture. However, abdominal aortic aneurysms can grow very large without causing symptoms. Routine checkups and treatment for an abdominal aortic aneurysm can help prevent growth and rupture.
Thoracic Aortic Aneurysms
An aneurysm that occurs in the chest portion of the aorta (above the diaphragm, a muscle that helps you breathe) is called a thoracic aortic aneurysm.
Thoracic aortic aneurysms don’t always cause symptoms, even when they’re large. Only half of all people who have thoracic aortic aneurysms notice any symptoms. Thoracic aortic aneurysms are found more often now than in the past because of chest CT scans done for other medical problems.
With a common type of thoracic aortic aneurysm, the walls of the aorta weaken and a section close to the heart enlarges. As a result, the valve between the heart and the aorta can’t close properly. This allows blood to leak back into the heart.
A less common type of thoracic aortic aneurysm can develop in the upper back, away from the heart. A thoracic aortic aneurysm in this location may result from an injury to the chest, such as from a car crash.
Other Types of Aneurysms
Brain Aneurysms
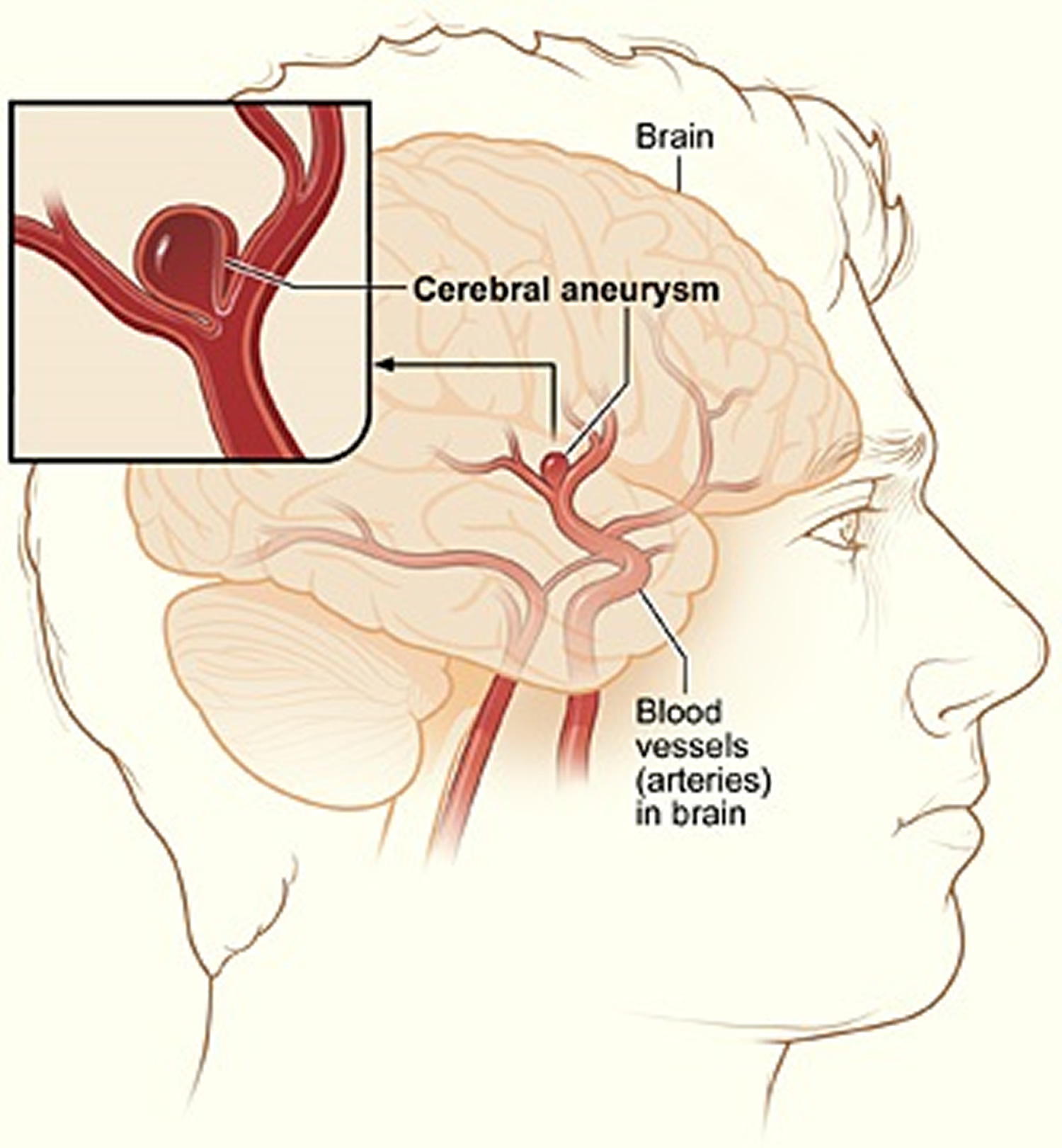
Aneurysms in the arteries of the brain are called cerebral aneurysms or brain aneurysms. Brain aneurysms also are called berry aneurysms because they’re often the size of a small berry.
Most brain aneurysms cause no symptoms until they become large, begin to leak blood, or rupture (burst). A ruptured brain aneurysm can cause a stroke.
Figure 6. Brain aneurysm
Peripheral Aneurysms
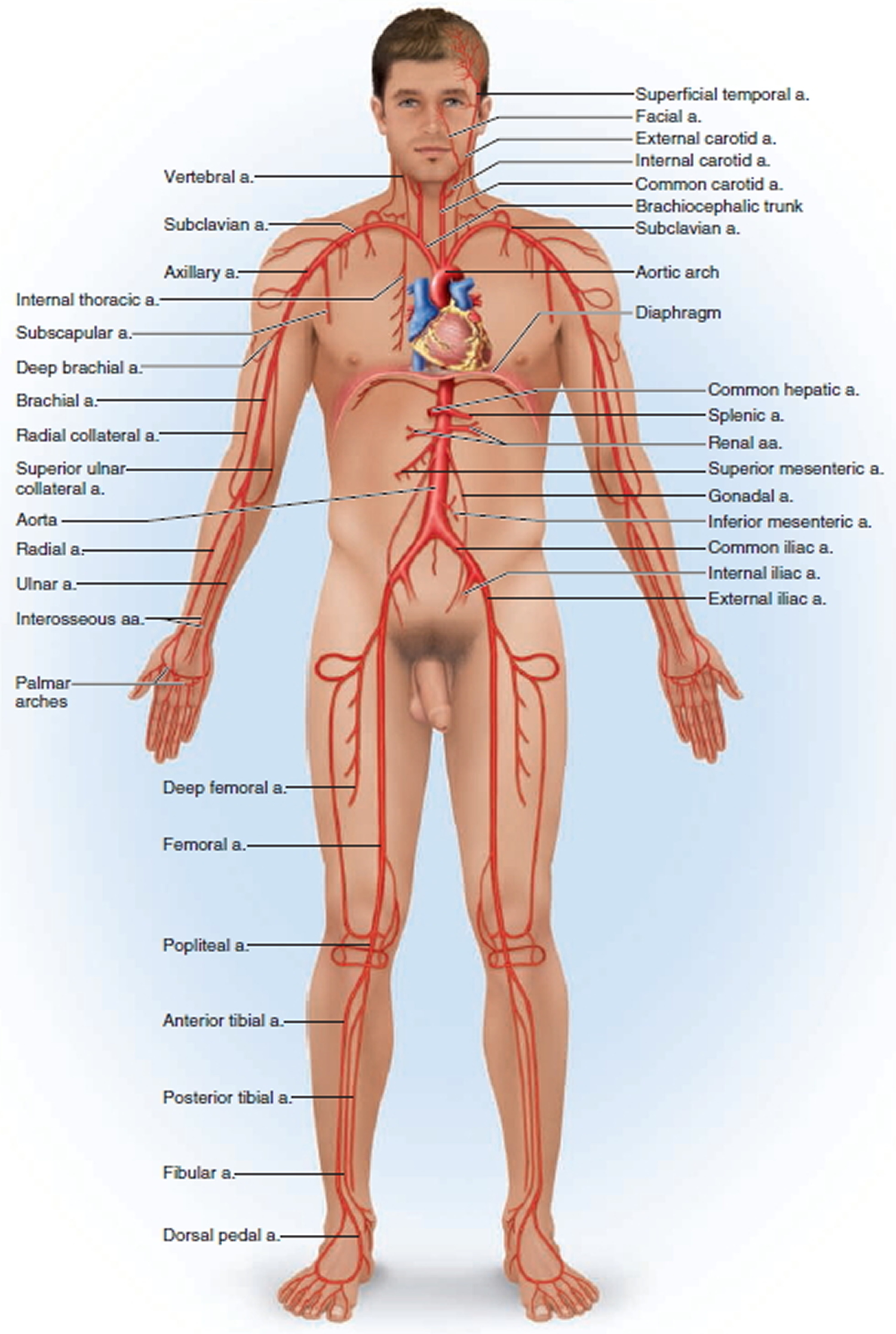
Aneurysms that occur in arteries other than the aorta and the brain arteries are called peripheral aneurysms. Common locations for peripheral aneurysms include the popliteal, femoral and carotid arteries.
The popliteal arteries run down the back of the thighs, behind the knees. The femoral arteries are the main arteries in the groin. The carotid arteries are the two main arteries on each side of your neck.
Peripheral aneurysms aren’t as likely to rupture or dissect as aortic aneurysms. However, blood clots can form in peripheral aneurysms. If a blood clot breaks away from the aneurysm, it can block blood flow through the artery.
If a peripheral aneurysm is large, it can press on a nearby nerve or vein and cause pain, numbness, or swelling.
What Causes an Aneurysm ?
The force of blood pushing against the walls of an artery combined with damage or injury to the artery’s walls can cause an aneurysm.
Many conditions and factors can damage and weaken the walls of the aorta and cause aortic aneurysms. Examples include aging, smoking, high blood pressure, and atherosclerosis. Atherosclerosis is the hardening and narrowing of the arteries due to the buildup of a waxy substance called plaque.
Rarely, infections—such as untreated syphilis (a sexually transmitted infection)—can cause aortic aneurysms. Aortic aneurysms also can occur as a result of diseases that inflame the blood vessels, such as vasculitis.
A family history of aneurysms also may play a role in causing aortic aneurysms.
In addition to the factors above, certain genetic conditions may cause thoracic aortic aneurysms. Examples of these conditions include Marfan syndrome, Loeys-Dietz syndrome, Ehlers-Danlos syndrome (the vascular type), and Turner syndrome.
These genetic conditions can weaken the body’s connective tissues and damage the aorta. People who have these conditions tend to develop aneurysms at a younger age than other people. They’re also at higher risk for rupture and dissection.
Trauma, such as a car accident, also can damage the walls of the aorta and lead to thoracic aortic aneurysms.
Researchers continue to look for other causes of aortic aneurysms. For example, they’re looking for genetic mutations (changes in the genes) that may contribute to or cause aneurysms.
Who Is at Risk for an Aneurysm ?
Certain factors put you at higher risk for an aortic aneurysm. These factors include:
- Male gender. Men are more likely than women to have aortic aneurysms.
- Age. The risk for abdominal aortic aneurysms increases as you get older. These aneurysms are more likely to occur in people who are aged 65 or older.
- Smoking. Smoking can damage and weaken the walls of the aorta.
- A family history of aortic aneurysms. People who have family histories of aortic aneurysms are at higher risk for the condition, and they may have aneurysms before the age of 65.
- A history of aneurysms in the arteries of the legs.
- Certain diseases and conditions that weaken the walls of the aorta. Examples include high blood pressure and atherosclerosis.
Having a bicuspid aortic valve can raise the risk of having a thoracic aortic aneurysm. A bicuspid aortic valve has two leaflets instead of the typical three.
Car accidents or trauma also can injure the arteries and increase the risk for aneurysms.
If you have any of these risk factors, talk with your doctor about whether you need screening for aneurysms.
What Are the Signs and Symptoms of an Aneurysm ?
The signs and symptoms of an aortic aneurysm depend on the type and location of the aneurysm. Signs and symptoms also depend on whether the aneurysm has ruptured (burst) or is affecting other parts of the body.
Aneurysms can develop and grow for years without causing any signs or symptoms. They often don’t cause signs or symptoms until they rupture, grow large enough to press on nearby body parts, or block blood flow.
Abdominal Aortic Aneurysms
Most abdominal aortic aneurysms develop slowly over years. They often don’t cause signs or symptoms unless they rupture. If you have an abdominal aortic aneurysm, your doctor may feel a throbbing mass while checking your abdomen.
When symptoms are present, they can include:
- A throbbing feeling in the abdomen
- Deep pain in your back or the side of your abdomen
- Steady, gnawing pain in your abdomen that lasts for hours or days
If an abdominal aortic aneurysm ruptures, symptoms may include sudden, severe pain in your lower abdomen and back; nausea (feeling sick to your stomach) and vomiting; constipation and problems with urination; clammy, sweaty skin; light-headedness; and a rapid heart rate when standing up.
Internal bleeding from a ruptured abdominal aortic aneurysm can send you into shock. Shock is a life-threatening condition in which blood pressure drops so low that the brain, kidneys, and other vital organs can’t get enough blood to work well. Shock can be fatal if it’s not treated right away.
Thoracic Aortic Aneurysms
A thoracic aortic aneurysm may not cause symptoms until it dissects or grows large. If you have symptoms, they may include:
- Pain in your jaw, neck, back, or chest
- Coughing and/or hoarseness
- Shortness of breath and/or trouble breathing or swallowing
A dissection is a split in one or more layers of the artery wall. The split causes bleeding into and along the layers of the artery wall.
If a thoracic aortic aneurysm ruptures or dissects, you may feel sudden, severe, sharp or stabbing pain starting in your upper back and moving down into your abdomen. You may have pain in your chest and arms, and you can quickly go into shock.
If you have any symptoms of thoracic aortic aneurysm or aortic dissection, call your local emergency number. If left untreated, these conditions may lead to organ damage or death.
How Is an Aneurysm Diagnosed ?
If you have an aortic aneurysm but no symptoms, your doctor may find it by chance during a routine physical exam. More often, doctors find aneurysms during tests done for other reasons, such as chest or abdominal pain.
If you have an abdominal aortic aneurysm, your doctor may feel a throbbing mass in your abdomen. A rapidly growing aneurysm about to rupture (burst) can be tender and very painful when pressed. If you’re overweight or obese, it may be hard for your doctor to feel even a large abdominal aortic aneurysm.
If you have an abdominal aortic aneurysm, your doctor may hear rushing blood flow instead of the normal whooshing sound when listening to your abdomen with a stethoscope.
Specialists Involved
Your primary care doctor may refer you to a cardiothoracic or vascular surgeon for diagnosis and treatment of an aortic aneurysm.
A cardiothoracic surgeon does surgery on the heart, lungs, and other organs and structures in the chest, including the aorta. A vascular surgeon does surgery on the aorta and other blood vessels, except those of the heart and brain.
Diagnostic Tests and Procedures
To diagnose and study an aneurysm, your doctor may recommend one or more of the following tests.
- Ultrasound and Echocardiography
Ultrasound and echocardiography (echo) are simple, painless tests that use sound waves to create pictures of the structures inside your body. These tests can show the size of an aortic aneurysm, if one is found.
- Computed Tomography Scan
A computed tomography scan, or CT scan, is a painless test that uses x rays to take clear, detailed pictures of your organs.
During the test, your doctor will inject dye into a vein in your arm. The dye makes your arteries, including your aorta, visible on the CT scan pictures.
Your doctor may recommend this test if he or she thinks you have an abdominal aortic aneurysm or a thoracic aortic aneurysm. A CT scan can show the size and shape of an aneurysm. This test provides more detailed pictures than an ultrasound or echo.
- Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) uses magnets and radio waves to create pictures of the organs and structures in your body. This test works well for detecting aneurysms and pinpointing their size and exact location.
- Angiography
Angiography is a test that uses dye and special x rays to show the insides of your arteries. This test shows the amount of damage and blockage in blood vessels.
Aortic angiography shows the inside of your aorta. The test may show the location and size of an aortic aneurysm.
How Is an Aneurysm Treated ?
Aortic aneurysms are treated with medicines and surgery. Small aneurysms that are found early and aren’t causing symptoms may not need treatment. Other aneurysms need to be treated.
The goals of treatment may include:
- Preventing the aneurysm from growing
- Preventing or reversing damage to other body structures
- Preventing or treating a rupture or dissection
- Allowing you to continue doing your normal daily activities
Treatment for an aortic aneurysm is based on its size. Your doctor may recommend routine testing to make sure an aneurysm isn’t getting bigger. This method usually is used for aneurysms that are smaller than 5 centimeters (about 2 inches) across.
How often you need testing (for example, every few months or every year) is based on the size of the aneurysm and how fast it’s growing. The larger it is and the faster it’s growing, the more often you may need to be checked.
Medicines
If you have an aortic aneurysm, your doctor may prescribe medicines before surgery or instead of surgery. Medicines are used to lower blood pressure, relax blood vessels, and lower the risk that the aneurysm will rupture (burst). Beta blockers and calcium channel blockers are the medicines most commonly used.
Surgery
Your doctor may recommend surgery if your aneurysm is growing quickly or is at risk of rupture or dissection.
The two main types of surgery to repair aortic aneurysms are open abdominal or open chest repair and endovascular repair.
Open Abdominal or Open Chest Repair
The standard and most common type of surgery for aortic aneurysms is open abdominal or open chest repair. This surgery involves a major incision (cut) in the abdomen or chest.
General anesthesia is used during this procedure. The term “anesthesia” refers to a loss of feeling and awareness. General anesthesia temporarily puts you to sleep.
During the surgery, the aneurysm is removed. Then, the section of aorta is replaced with a graft made of material such as Dacron® or Teflon.® The surgery takes 3 to 6 hours; you’ll remain in the hospital for 5 to 8 days.
If needed, repair of the aortic heart valve also may be done during open abdominal or open chest surgery.
It often takes a month to recover from open abdominal or open chest surgery and return to full activity. Most patients make a full recovery.
Endovascular Repair
In endovascular repair, the aneurysm isn’t removed. Instead, a graft is inserted into the aorta to strengthen it. Surgeons do this type of surgery using catheters (tubes) inserted into the arteries; it doesn’t require surgically opening the chest or abdomen. General anesthesia is used during this procedure.
The surgeon first inserts a catheter into an artery in the groin (upper thigh) and threads it to the aneurysm. Then, using an x ray to see the artery, the surgeon threads the graft (also called a stent graft) into the aorta to the aneurysm.
The graft is then expanded inside the aorta and fastened in place to form a stable channel for blood flow. The graft reinforces the weakened section of the aorta. This helps prevent the aneurysm from rupturing.
The recovery time for endovascular repair is less than the recovery time for open abdominal or open chest repair. However, doctors can’t repair all aortic aneurysms with endovascular repair. The location or size of an aneurysm may prevent the use of a stent graft.
Figure 7. Endovascular repair
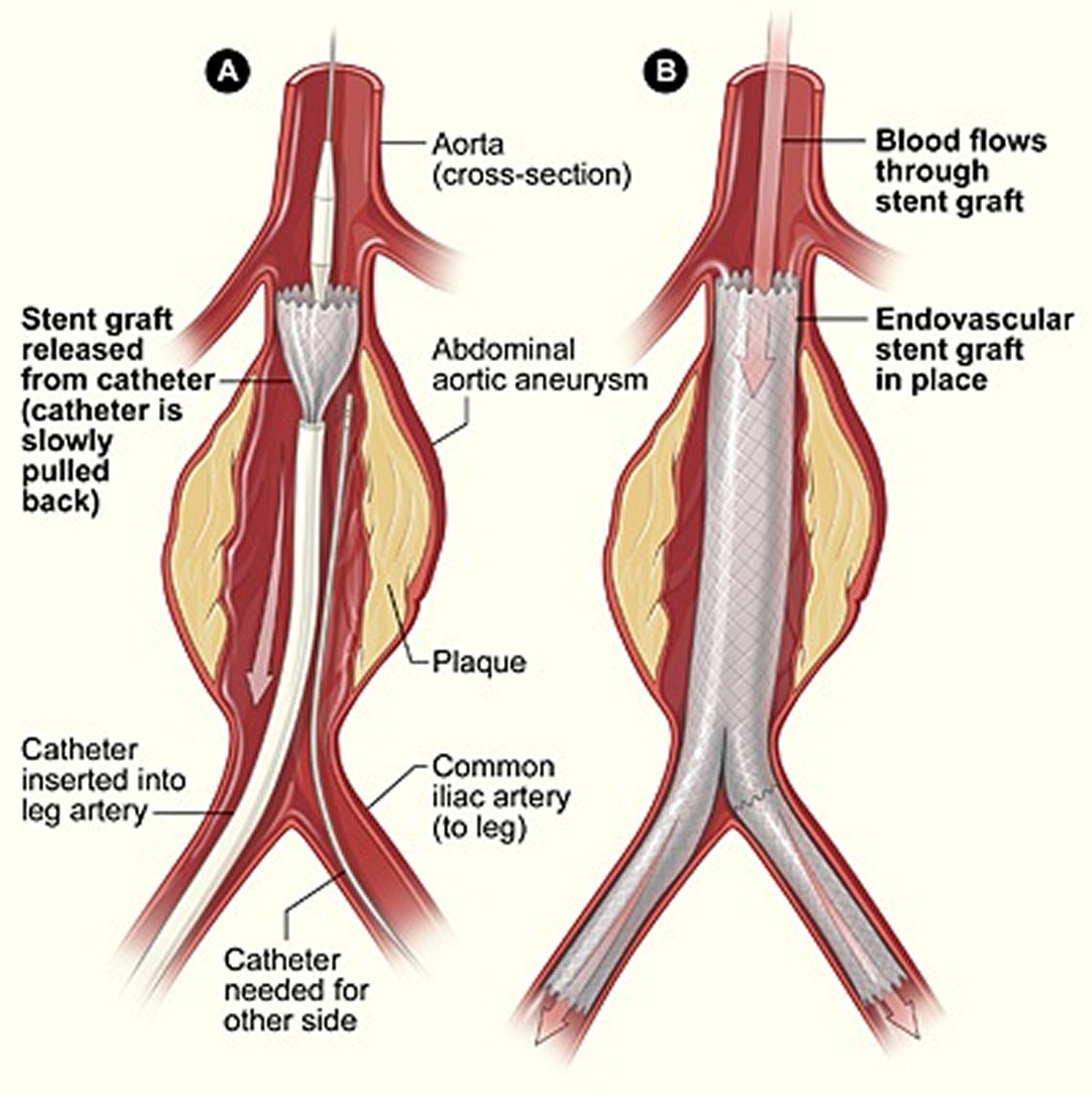
Note: The illustration shows the placement of a stent graft in an aortic aneurysm. In figure A, a catheter is inserted into an artery in the groin (upper thigh). The catheter is threaded to the abdominal aorta, and the stent graft is released from the catheter. In figure B, the stent graft allows blood to flow through the aneurysm.
How Can an Aneurysm Be Prevented ?
The best way to prevent an aortic aneurysm is to avoid the factors that put you at higher risk for one. You can’t control all aortic aneurysm risk factors, but lifestyle changes can help you lower some risks.
For example, if you smoke, try to quit. Talk with your doctor about programs and products that can help you quit smoking. Also, try to avoid secondhand smoke. For more information about how to quit smoking, go to the Diseases and Conditions Index (DCI) Smoking and Your Heart article.
Another important lifestyle change is following a healthy diet. A healthy diet includes a variety of fruits, vegetables, and whole grains. It also includes lean meats, poultry, fish, beans, and fat-free or low-fat milk or milk products. A healthy diet is low in saturated fat, trans fat, cholesterol, sodium (salt), and added sugar.
Be as physically active as you can. Talk with your doctor about the amounts and types of physical activity that are safe for you.
Work with your doctor to control medical conditions such as high blood pressure and high blood cholesterol. Follow your treatment plans and take all of your medicines as your doctor prescribes.
Screening for Aneurysms
Although you may not be able to prevent an aneurysm, early diagnosis and treatment can help prevent rupture and dissection.
Aneurysms can develop and grow large before causing any signs or symptoms. Thus, people who are at high risk for aneurysms may benefit from early, routine screening.
Your doctor may recommend routine screening if you’re:
- A man between the ages of 65 and 75 who has ever smoked
- A man or woman between the ages of 65 and 75 who has a family history of aneurysms
If you’re at risk, but not in one of these high-risk groups, ask your doctor whether screening will benefit you.
Varicose Veins
Varicose veins are swollen, twisted veins that you can see just under the surface of the skin 3. These veins usually occur in the legs, but they also can form in other parts of the body.
Veins have one-way valves that help keep blood flowing toward your heart. If the valves are weak or damaged, blood can back up and pool in your veins. This causes the veins to swell, which can lead to varicose veins.
Many factors can raise your risk for varicose veins. Examples of these factors include family history, older age, gender, pregnancy, overweight or obesity, lack of movement, and leg trauma.
Varicose veins are a common condition. They usually cause few signs and symptoms. Sometimes varicose veins cause mild to moderate pain, blood clots, skin ulcers (sores), or other problems.
Varicose veins are treated with lifestyle changes and medical procedures. The goals of treatment are to relieve symptoms, prevent complications, and improve appearance.
What Causes Varicose Veins ?
Weak or damaged valves in the veins can cause varicose veins. After your arteries and capillaries deliver oxygen-rich blood to your body, your veins return the blood to your heart. The veins in your legs must work against gravity to do this.
One-way valves inside the veins open to let blood flow through, and then they shut to keep blood from flowing backward. If the valves are weak or damaged, blood can back up and pool in your veins. This causes the veins to swell.
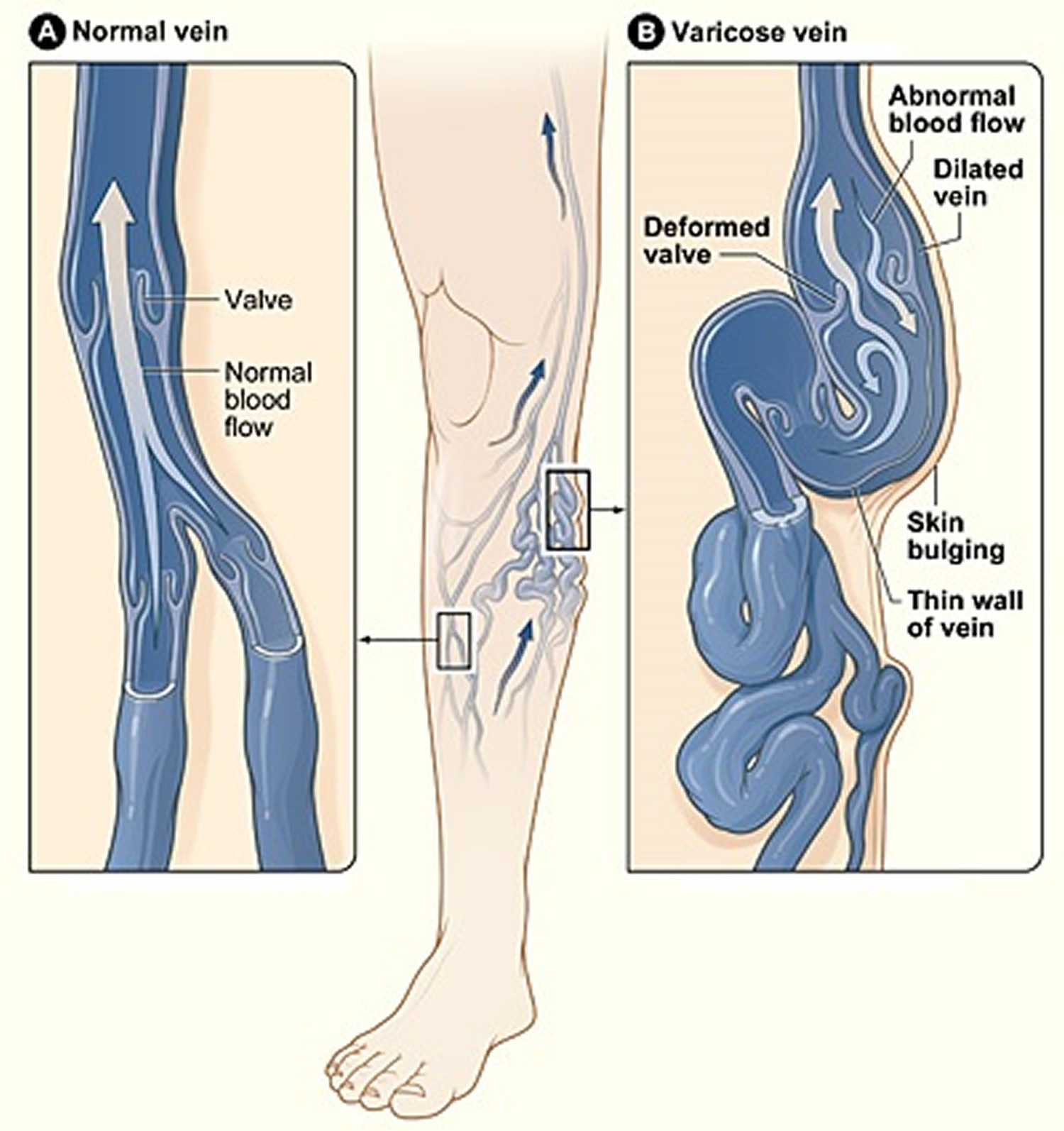
Weak vein walls may cause weak valves. Normally, the walls of the veins are elastic (stretchy). If these walls become weak, they lose their normal elasticity. They become like an overstretched rubber band. This makes the walls of the veins longer and wider, and it causes the flaps of the valves to separate.
When the valve flaps separate, blood can flow backward through the valves. The backflow of blood fills the veins and stretches the walls even more. As a result, the veins get bigger, swell, and often twist as they try to squeeze into their normal space. These are varicose veins.
Older age or a family history of varicose veins may raise your risk for weak vein walls. You also may be at higher risk if you have increased pressure in your veins due to overweight or obesity or pregnancy.
Figure 8. Varicose veins

Vein Problems Related to Varicose Veins
Many vein problems are related to varicose veins, such as telangiectasias, spider veins, varicoceles and other vein problems.
Telangiectasias
Telangiectasias are small clusters of blood vessels. They’re usually found on the upper body, including the face.
These blood vessels appear red. They may form during pregnancy, and often they develop in people who have certain genetic disorders, viral infections, or other conditions, such as liver disease.
Because telangiectasias can be a sign of a more serious condition, see your doctor if you think you have them.
Figure 9. Telangiectasias

Spider Veins
Spider veins are a smaller version of varicose veins and a less serious type of telangiectasias. Spider veins involve the capillaries, the smallest blood vessels in the body.
Spider veins often appear on the legs and face. They’re red or blue and usually look like a spider web or tree branch. These veins usually aren’t a medical concern.
Figure 10. Spider veins

Varicoceles
Varicoceles are varicose veins in the scrotum (the skin over the testicles). Varicoceles may be linked to male infertility. If you think you have varicoceles, see your doctor.
Other Related Vein Problems
Other types of varicose veins include venous lakes, reticular veins, and hemorrhoids. Venous lakes are varicose veins that appear on the face and neck. Reticular veins are flat blue veins often seen behind the knees. Hemorrhoids are varicose veins in and around the anus.
How Are Varicose Veins Treated ?
Varicose veins are treated with lifestyle changes and medical procedures. The goals of treatment are to relieve symptoms, prevent complications, and improve appearance.
If varicose veins cause few symptoms, your doctor may simply suggest making lifestyle changes. If your symptoms are more severe, your doctor may recommend one or more medical procedures. For example, you may need a medical procedure if you have a lot of pain, blood clots, or skin disorders caused by your varicose veins.
Some people who have varicose veins choose to have procedures to improve how their veins look.
Although treatment can help existing varicose veins, it can’t keep new varicose veins from forming.
Lifestyle Changes
Lifestyle changes often are the first treatment for varicose veins. These changes can prevent varicose veins from getting worse, reduce pain, and delay other varicose veins from forming. Lifestyle changes include the following:
- Avoid standing or sitting for long periods without taking a break. When sitting, avoid crossing your legs. Keep your legs raised when sitting, resting, or sleeping. When you can, raise your legs above the level of your heart.
- Do physical activities to get your legs moving and improve muscle tone. This helps blood move through your veins.
- If you’re overweight or obese, try to lose weight. This will improve blood flow and ease the pressure on your veins.
- Avoid wearing tight clothes, especially those that are tight around your waist, groin (upper thighs), and legs. Tight clothes can make varicose veins worse.
- Avoid wearing high heels for long periods. Lower heeled shoes can help tone your calf muscles. Toned muscles help blood move through the veins.
Your doctor may recommend compression stockings. These stockings create gentle pressure up the leg. This pressure keeps blood from pooling and decreases swelling in the legs.
There are three types of compression stockings. One type is support pantyhose. These offer the least amount of pressure. A second type is over-the-counter compression hose. These stockings give a little more pressure than support pantyhose. Over-the-counter compression hose are sold in medical supply stores and pharmacies.
Prescription-strength compression hose are the third type of compression stockings. These stockings offer the greatest amount of pressure. They also are sold in medical supply stores and pharmacies. However, you need to be fitted for them in the store by a specially trained person.
Medical Procedures
Medical procedures are done either to remove varicose veins or to close them. Removing or closing varicose veins usually doesn’t cause problems with blood flow because the blood starts moving through other veins.
You may be treated with one or more of the procedures described below. Common side effects right after most of these procedures include bruising, swelling, skin discoloration, and slight pain.
The side effects are most severe with vein stripping and ligation. Rarely, this procedure can cause severe pain, infections, blood clots, and scarring.
Sclerotherapy
Sclerotherapy uses a liquid chemical to close off a varicose vein. The chemical is injected into the vein to cause irritation and scarring inside the vein. The irritation and scarring cause the vein to close off, and it fades away.
This procedure often is used to treat smaller varicose veins and spider veins. It can be done in your doctor’s office, while you stand. You may need several treatments to completely close off a vein.
Treatments typically are done every 4 to 6 weeks. Following treatments, your legs will be wrapped in elastic bandaging to help with healing and decrease swelling.
Microsclerotherapy
Microsclerotherapy is used to treat spider veins and other very small varicose veins.
A small amount of liquid chemical is injected into a vein using a very fine needle. The chemical scars the inner lining of the vein, causing it to close off.
Laser Surgery
This procedure applies light energy from a laser onto a varicose vein. The laser light makes the vein fade away.
Laser surgery mostly is used to treat smaller varicose veins. No cutting or injection of chemicals is involved.
Endovenous Ablation Therapy
Endovenous ablation therapy uses lasers or radiowaves to create heat to close off a varicose vein.
Your doctor makes a tiny cut in your skin near the varicose vein. He or she then inserts a small tube called a catheter into the vein. A device at the tip of the tube heats up the inside of the vein and closes it off.
You’ll be awake during this procedure, but your doctor will numb the area around the vein. You usually can go home the same day as the procedure.
Endoscopic Vein Surgery
For endoscopic vein surgery, your doctor will make a small cut in your skin near a varicose vein. He or she then uses a tiny camera at the end of a thin tube to move through the vein. A surgical device at the end of the camera is used to close the vein.
Endoscopic vein surgery usually is used only in severe cases when varicose veins are causing skin ulcers (sores). After the procedure, you usually can return to your normal activities within a few weeks.
Ambulatory Phlebectomy
For ambulatory phlebectomy, your doctor will make small cuts in your skin to remove small varicose veins. This procedure usually is done to remove the varicose veins closest to the surface of your skin.
You’ll be awake during the procedure, but your doctor will numb the area around the vein. Usually, you can go home the same day that the procedure is done.
Vein Stripping and Ligation
Vein stripping and ligation typically is done only for severe cases of varicose veins. The procedure involves tying shut and removing the veins through small cuts in your skin.
You’ll be given medicine to temporarily put you to sleep so you don’t feel any pain during the procedure.
Vein stripping and ligation usually is done as an outpatient procedure. The recovery time from the procedure is about 1 to 4 weeks.
How Can Varicose Veins Be Prevented ?
You can’t prevent varicose veins from forming. However, you can prevent the ones you have from getting worse. You also can take steps to delay other varicose veins from forming.
Avoid standing or sitting for long periods without taking a break. When sitting, avoid crossing your legs. Keep your legs raised when sitting, resting, or sleeping. When you can, raise your legs above the level of your heart.
Do physical activities to get your legs moving and improve muscle tone. This helps blood move through your veins.
If you’re overweight or obese, try to lose weight. This will improve blood flow and ease the pressure on your veins.
Avoid wearing tight clothes, especially those that are tight around your waist, groin (upper thighs), and legs. Tight clothes can make varicose veins worse.
Avoid wearing high heels for long periods. Lower heeled shoes can help tone your calf muscles. Toned muscles help blood move through the veins.
Wear compression stockings if your doctor recommends them. These stockings create gentle pressure up the leg. This pressure keeps blood from pooling in the veins and decreases swelling in the legs.
Blood Vessels to the Brain
Although the brain is only 2% of the adult body weight, it receives 15% of the blood (about 750 mL/min.) and consumes 20% of its oxygen and glucose. Because neurons have such a high demand for ATP (adenosine triphosphate is a high-energy molecule found in every cell, its job is to store and supply the cell with needed energy) and therefore glucose and oxygen, the constancy of blood supply is especially critical to the nervous system. A mere 10-second interruption in blood flow can cause loss of consciousness; an interruption of 1 to 2 minutes can significantly impair neural function; and 4 minutes without blood usually causes
irreversible brain damage.
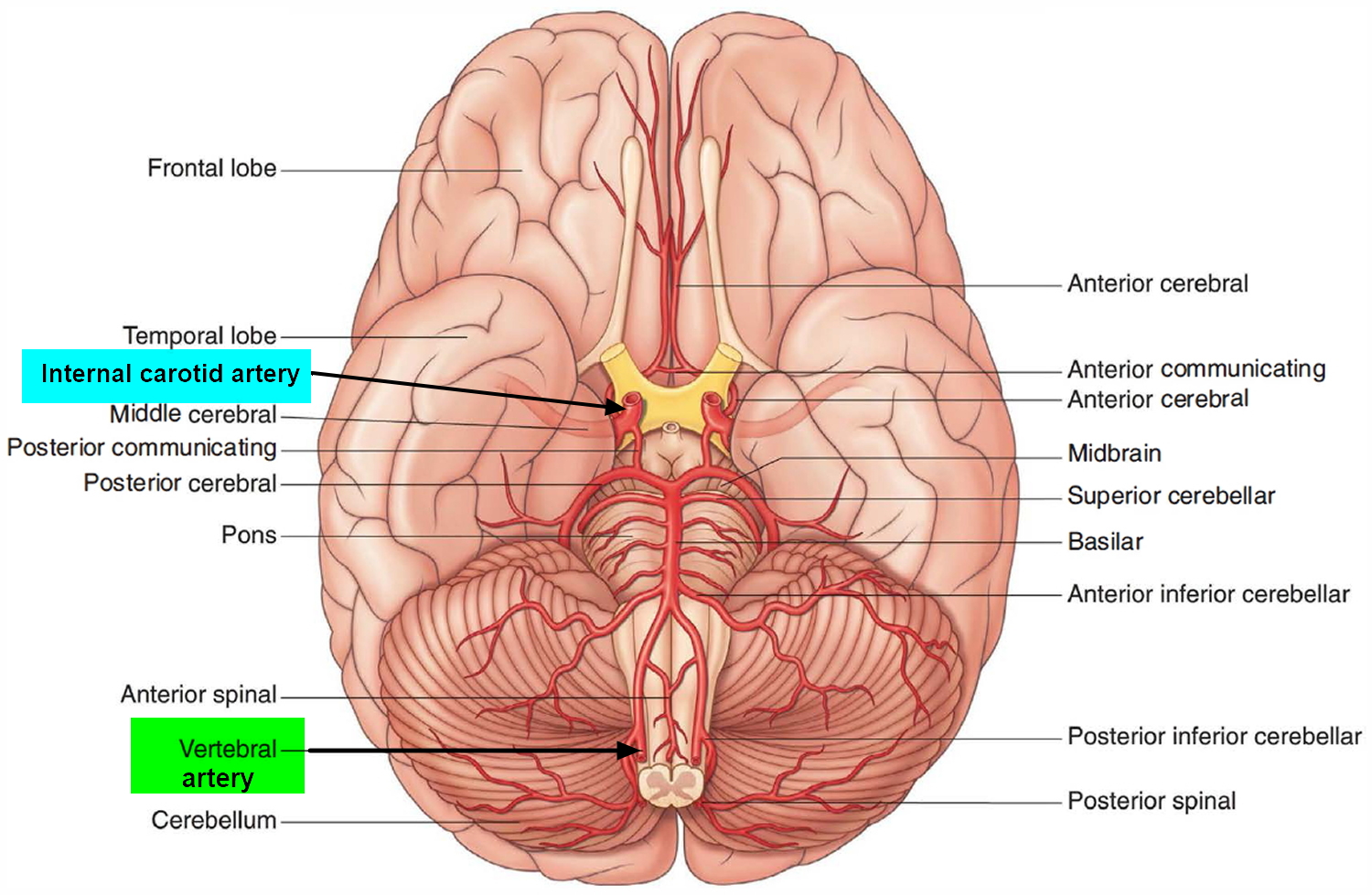
The brain receives its arterial supply from two pairs of vessels, the vertebral and internal carotid arteries, which are interconnected in the cranial cavity to produce a cerebral arterial circle (of Willis). The two vertebral arteries enter the cranial cavity through the foramen magnum and just inferior to the pons fuse to form the basilar artery. The two internal carotid arteries enter the cranial cavity through the carotid canals on either side.
Figure 11. Brain blood supply

{kind=link}