Contents
What is a bone marrow biopsy
Bone marrow biopsy and bone marrow aspiration are invasive medical procedures to collect and examine bone marrow — the spongy tissue inside some of your larger bones (see Figure 1). Bone marrow biopsy, also called trephination, is a procedure where a small sample of the bone marrow is withdrawn by inserting a needle that passing through the outside portion of the bone and into the middle of the bone where the marrow is located. The bone marrow plays an important role in the human body. Bone marrow manufactures blood stem cells like red blood cells, white blood cells, and the platelets. The blood stem cells, red blood cells, white blood cells, and the platelets have a very important job.
Stem cells are found in bone marrow, and they develop into the three types of blood cells that the body needs:
- Red blood cells, which carry oxygen to the tissues of the body;
- White blood cells, which fight infection by contributing to your immune system by protecting the body against infectious diseases or foreign substances that enters the body;
- Platelets, which help the blood clot preventing the body from bleeding.
Bone marrow biopsy and aspiration can show whether your bone marrow is healthy and making normal amounts of blood cells. Doctors use these procedures to diagnose and monitor blood and marrow diseases, including some cancers – such as lymphoma, leukemia, and metastasis to bone marrow, as well as fevers of unknown origin. The examination usually includes an aspiration and/or biopsy from the iliac crest (the top ridge of the rear hipbone or pelvic bone). For babies and young children, the sample will be taken on a part of the lower leg bone, just below the knee. When diagnosing Hodgkin’s lymphoma, an aspirate and biopsy are taken from both sides. Sometimes, aspiration from the sternum is appropriate. In special cases, the aspiration is performed with the help of image guidance in cooperation with the nuclear medicine department.
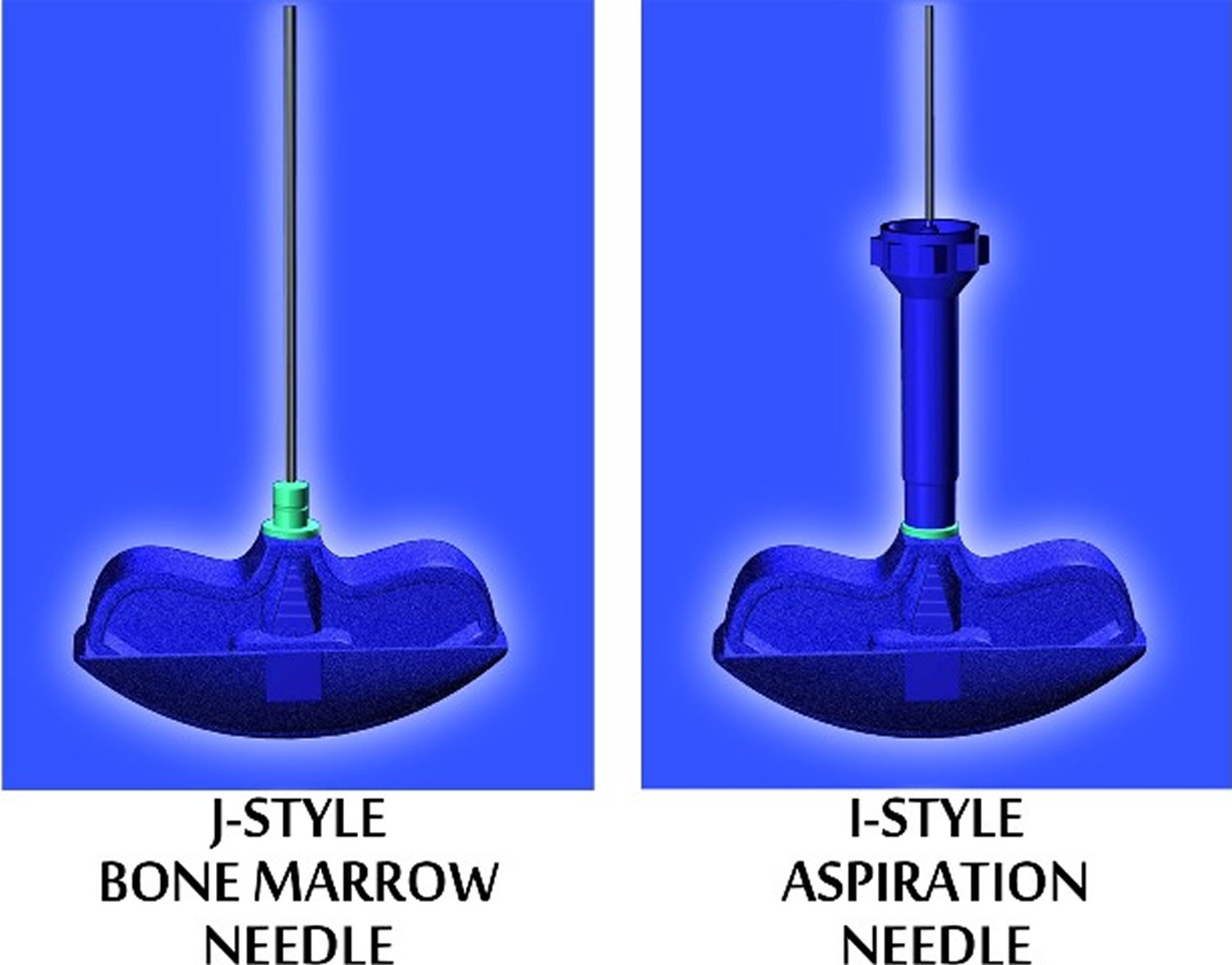
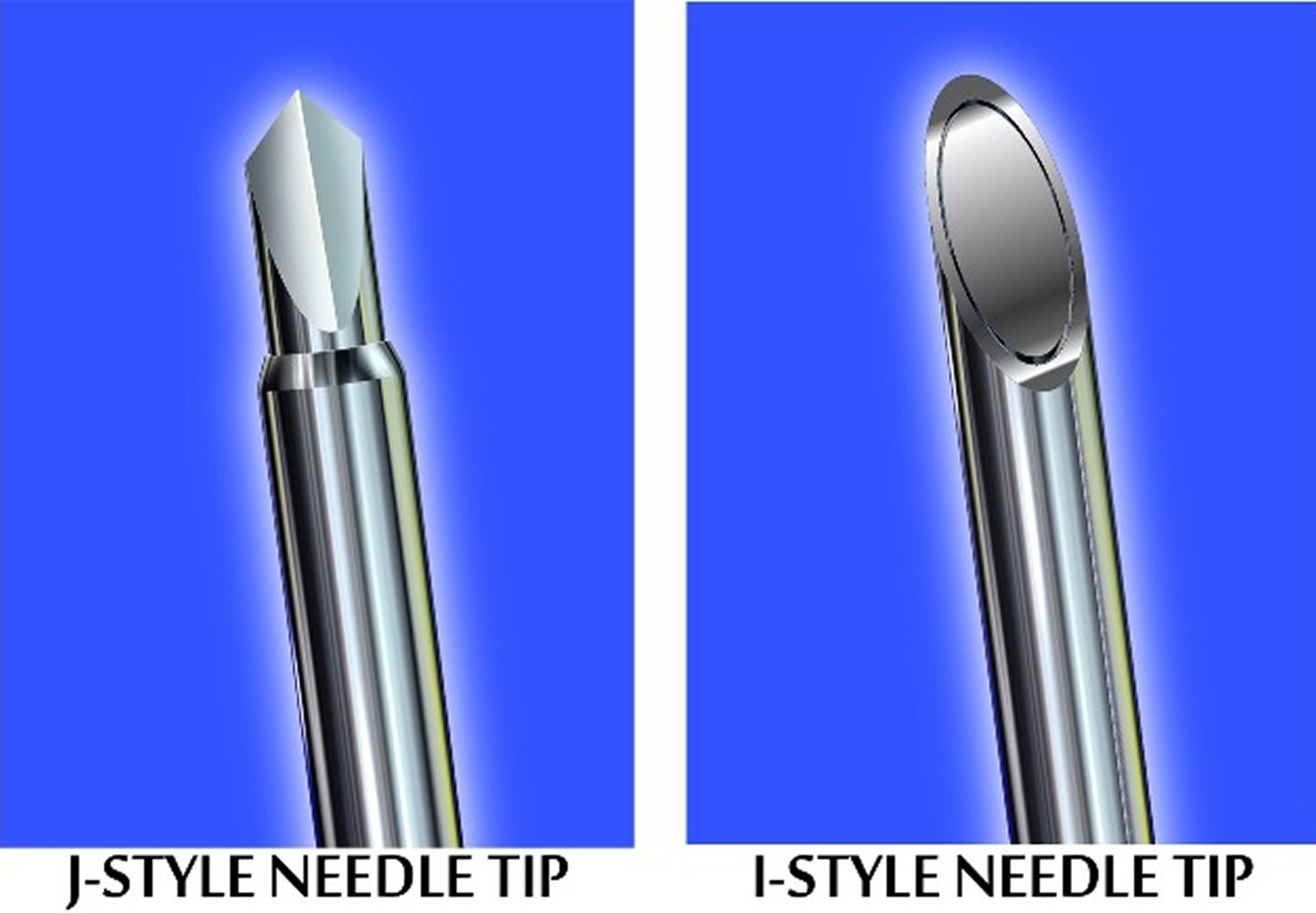
The type and caliber of the bone marrow biopsy needle is one of the main variables of the bone marrow aspiration and biopsy procedure and is selected on the basis of the age, gender and body mass of the patient.
Bone marrow has a fluid portion and a more solid portion. In bone marrow biopsy, your doctor uses a needle to withdraw a sample of the solid portion. In bone marrow aspiration, a needle is used to withdraw a sample of the fluid portion.
Bone marrow biopsy and bone marrow aspiration are often done at the same time. Together, these procedures may be called a bone marrow exam.
A bone marrow biopsy and aspiration can be done in a hospital, clinic or doctor’s office. The bone marrow biopsy and bone marrow aspiration procedures are usually done by a doctor who specializes in blood disorders (hematologist) or cancer (oncologist).
The bone marrow exam typically takes about 10 minutes. Extra time is needed for preparation and post-procedure care, especially if you receive intravenous (IV) sedation. The total time for the procedure is about 30 minutes.
The only contraindication for carrying out a bone marrow biopsy is serious hemophilia. This must be performed in cooperation with a hemophilia clinic.
Trepanning is one of the oldest surgical operations known to man dating from 6500 BC, of 120 prehistoric craniums 430 showed signs of trepanning. A trephine (from the Latin trypan) or auger is a cylindrical surgical instrument of varying size and shape. Trepans are specially designed to obtain cylindrical fragments of bone for analysis, or to drill through the cranium. In 1927, Anirkin, a Russian physician, obtained bone marrow from the sternum using a lumbar puncture needle. Anirkin’s technique was used not only for the analysis of bone marrow, but also for diagnosis of typhoid and tuberculosis. The technique continued to improve throughout the 1940s and into the 1950s, when the pelvis was suggested as the collection site (Rubinstein 1950, Bierman 1952, Sacker and Nordin 1954) 1. In response to a 5% failure rate in obtaining samples, McFarland and Dameshek (1958) described a trephination technique using the Vim-Silverman biopsy needle (Silverman, 1938). These biopsies were performed using local anaesthesia, and several modifications were made to the needle (1959–1963) (Figure 3B and 3C). Up to this point, all biopsy procedures were performed in the outpatient setting. In 1971, Iranian hematologist Khosrow Jamshidi redesigned the needle so that the interior diameter of the distal portion was tapered, allowing tissue to freely enter the lumen without fracturing the core (Figure 3D). Some early attempts at designing electric drills were made between the 1960s and 1980s. However, due to the ease of use, efficacy and low cost of hand-held needles, these electric devices were discontinued. Modern needles are similar in design to those used in the 20th century, and the procedure is carried out under local anaesthetic to minimize patient discomfort 2.
Figure 1. Bone marrow biopsy
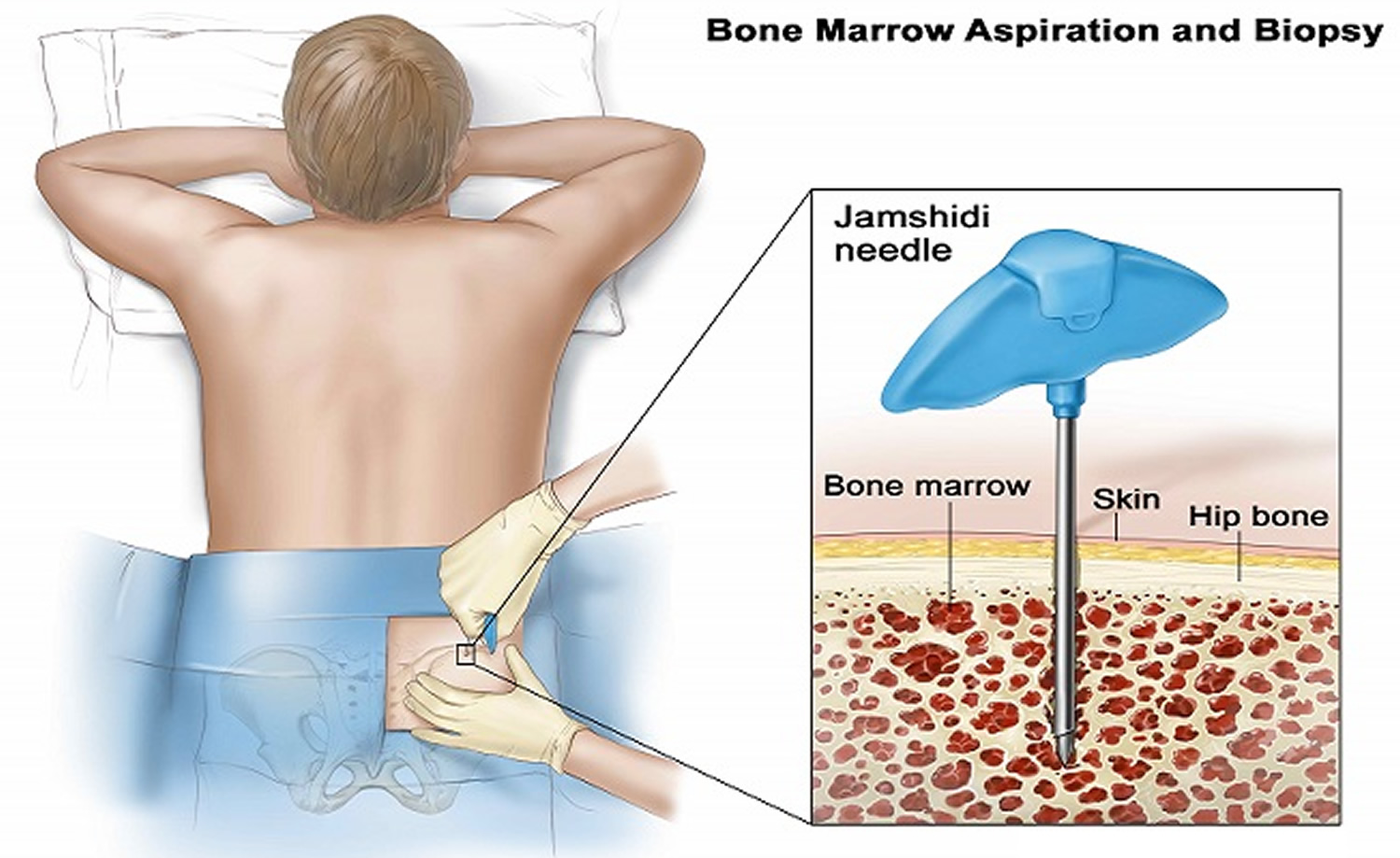
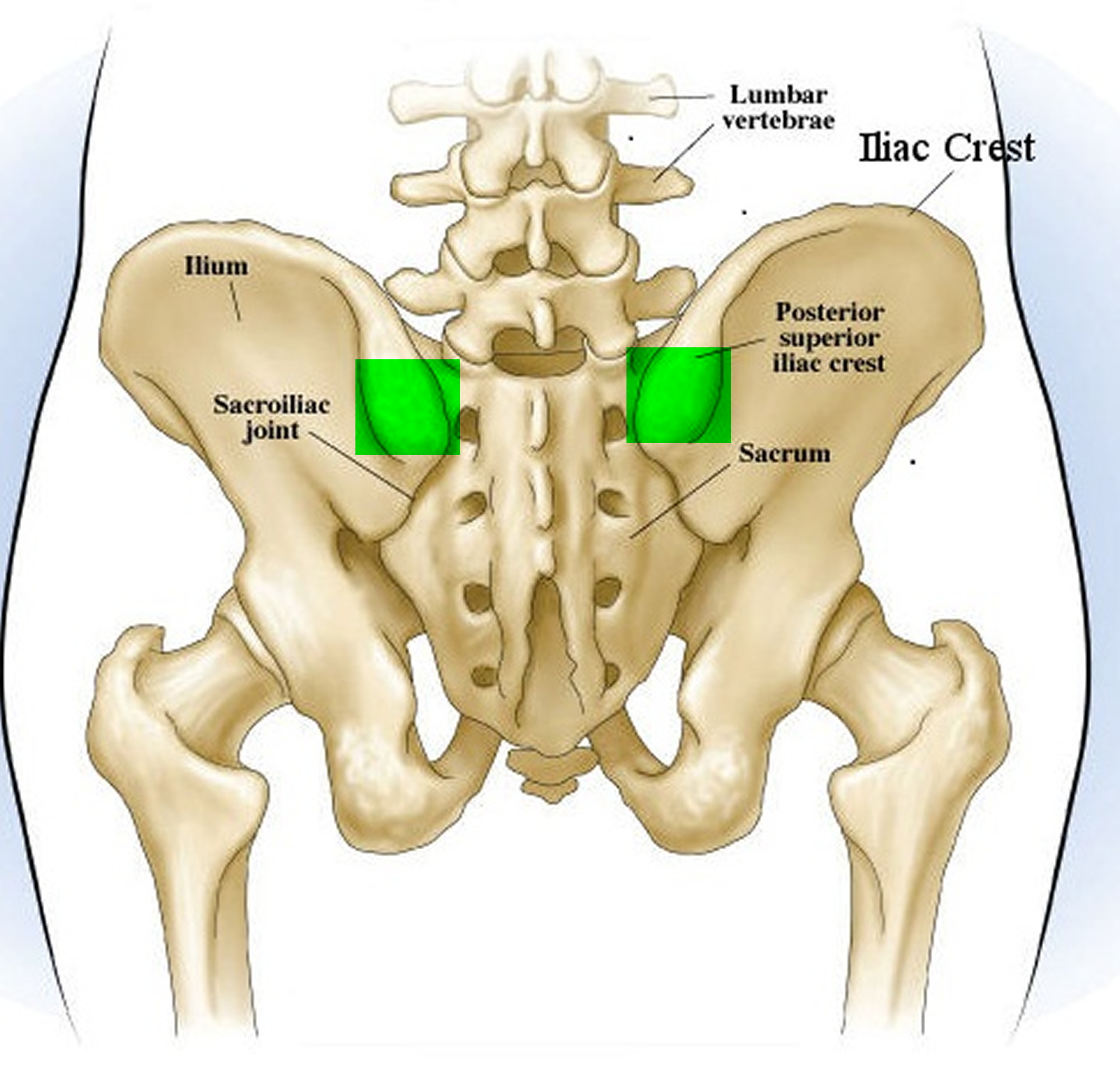 Figure 2. Site of bone marrow biopsy and bone marrow aspiration
Figure 2. Site of bone marrow biopsy and bone marrow aspiration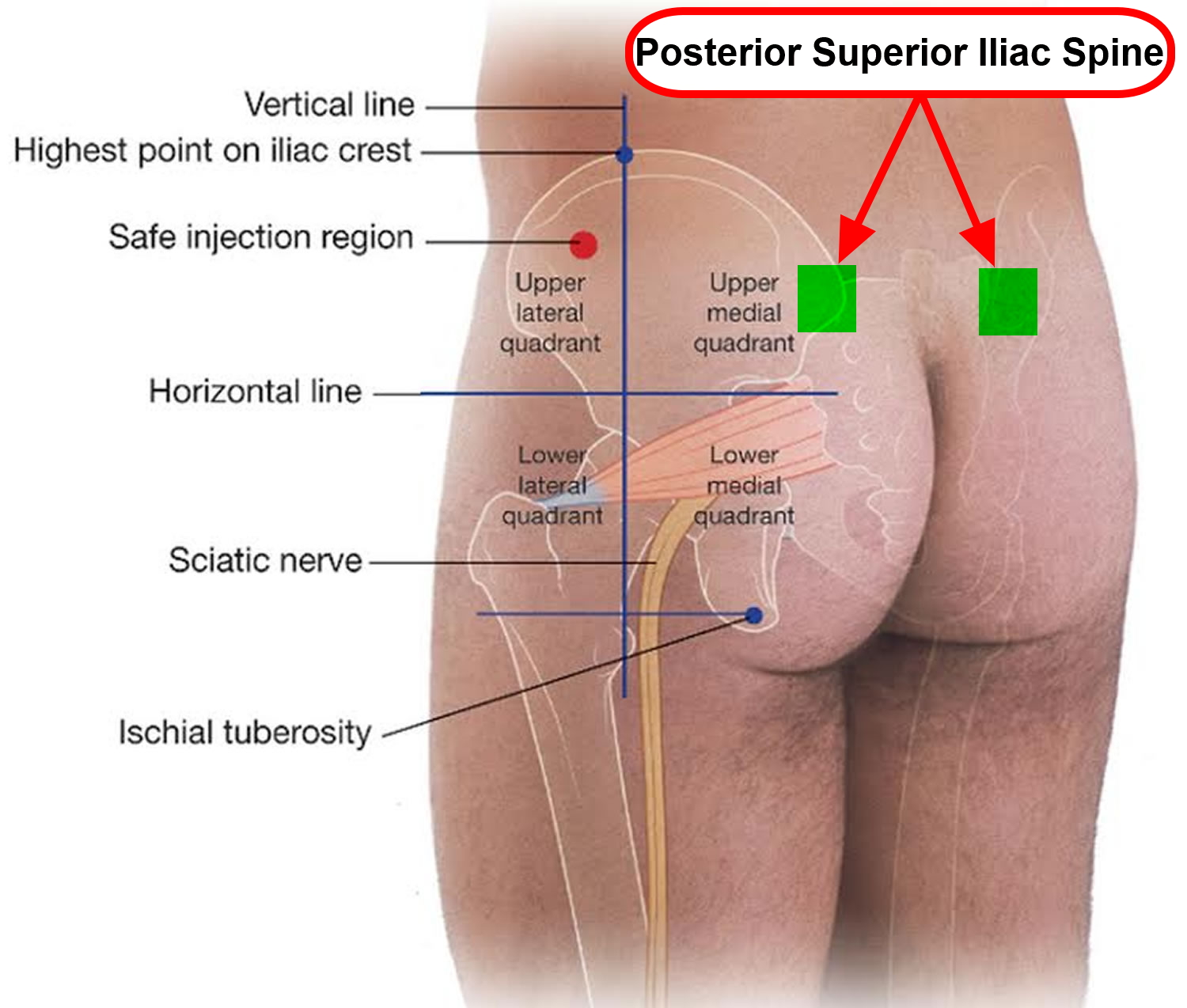
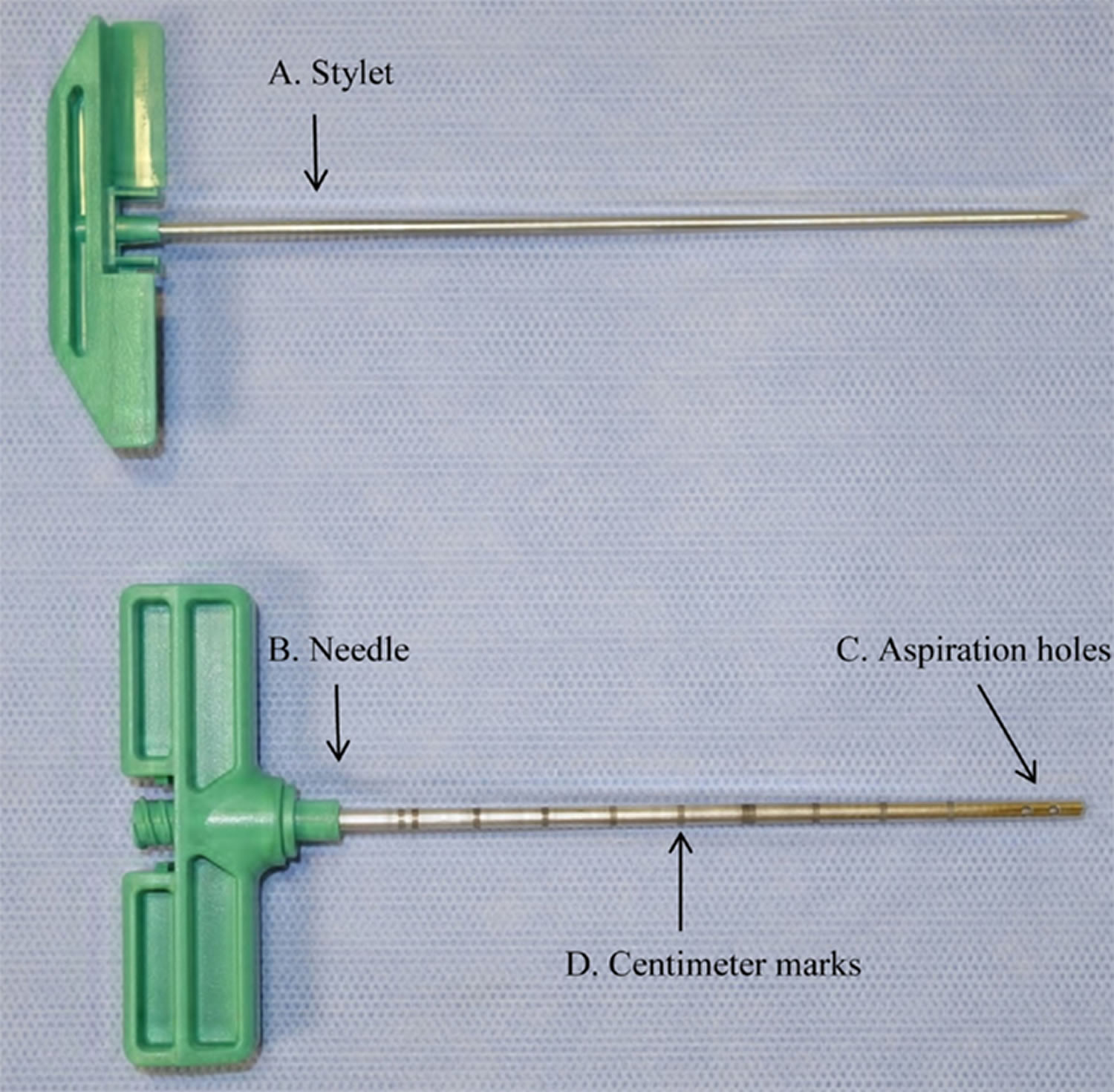
Bone marrow biopsy needle
Ideal size of bone marrow biopsy needles
Bone marrow biopsy complements the study of bone marrow smear specimens obtained by aspiration, thus facilitating the diagnostic process. Diagnosis will depend on the size of the sample obtained. According to Wintrobe, the ideal sample size is 2.0cm 3. Bishop et al. 4 at the Christie Hospital in Manchester, UK, evaluated the quality of 767 bone marrow trephines performed using 2 types of needles (the Jamshidi and the Islam). The average histology sample size was found to be 1.59cm, and 25% of the specimen was fractured and therefore not viable for the purpose of the study. The average, useful length of the biopsy specimen was 1.15cm (0.09cm soft tissue, 0.04cm of cortex, 0.26cm of disrupted marrow, and 0.74cm of interpretable marrow). The largest specimens were usually obtained using the Jamshidi needle 4.
Figure 3. Bone marrow biopsy needle – Note: Needles used in bone marrow biopsy or aspiration. (A) Klima sternal needle; (B) Salah bone marrow aspiration needle; (C) Watherfield iliac crest bone marrow aspiration needle; (D) Modern Jamshidi needle for bone marrow biopsy and aspiration.
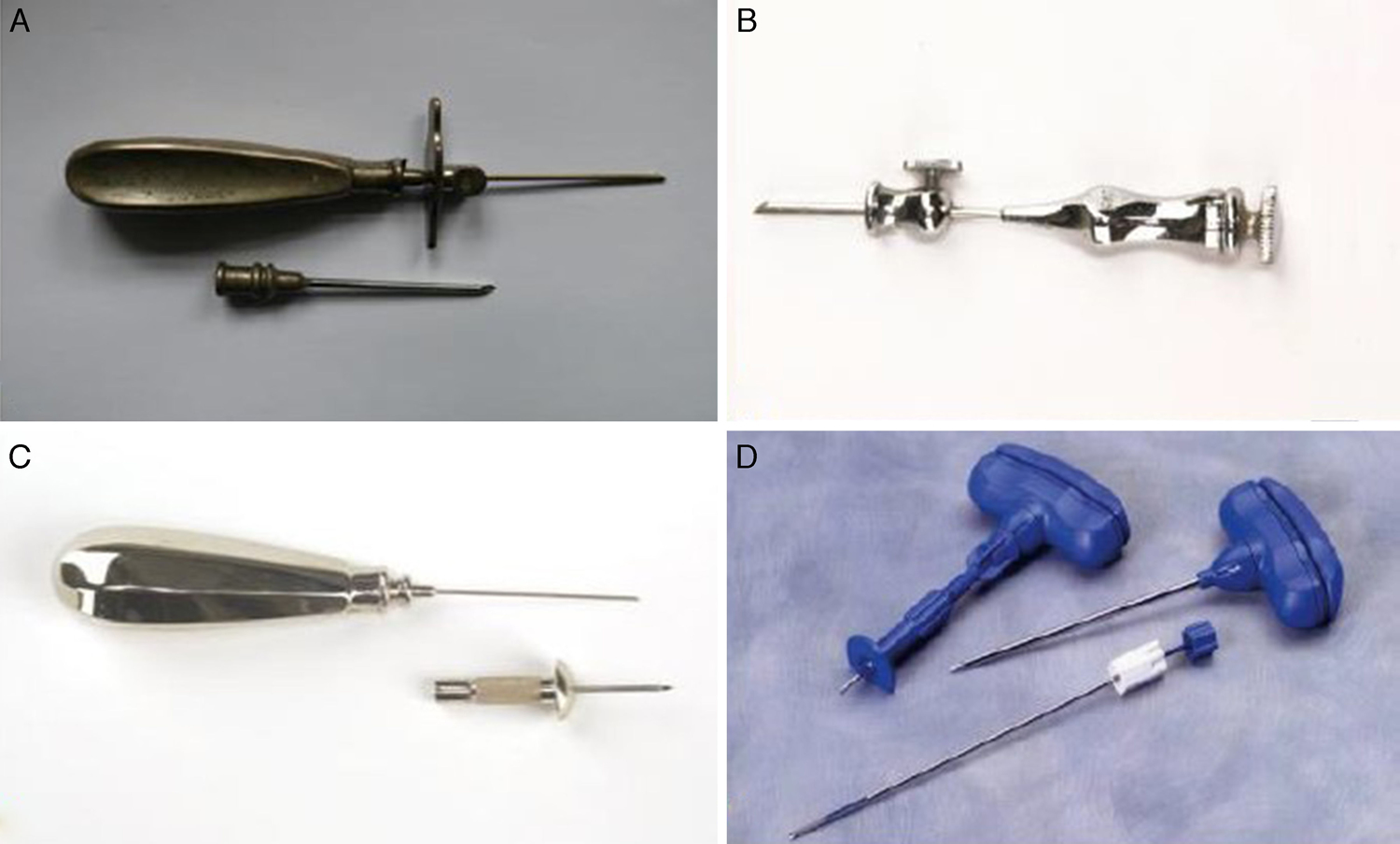
Figure 4. Bone marrow biopsy needle – From left: biopsy cannula, mandrin, plugs, retrieval spoon, and blunt mandrin.

Pain management strategies
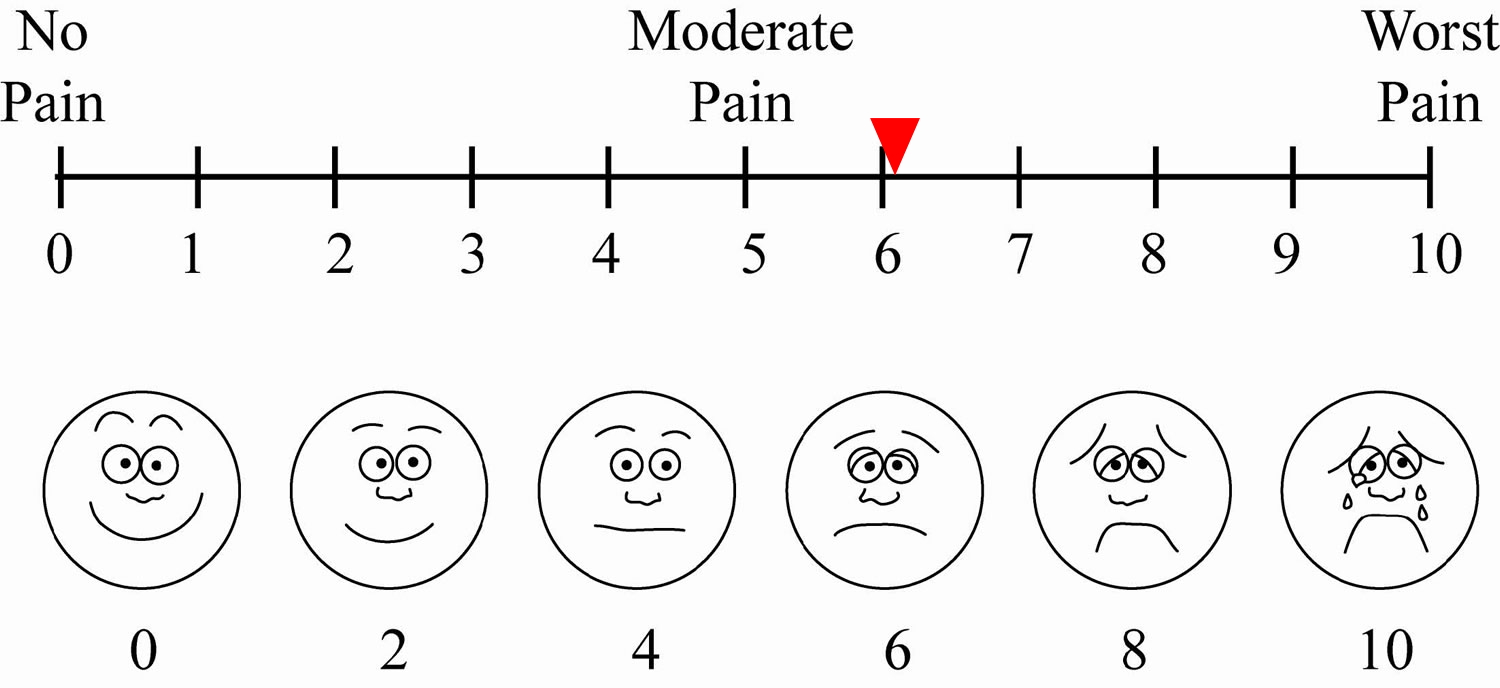
Needle aspiration and bone marrow biopsy are usually performed at the same time 5. Few studies have been published to date on pain management during the procedure. Park et al. 6 evaluated the use of low-dose lorazepam in a double-blind, placebo controlled trial that measured pain on a visual analogue pain scale. Scores were similar for both lorazepam (6.0) and placebo (6.2), although patients in the lorazepam groups showed greater willingness to repeat the procedure. Recently, Kuivalainen et al. 7 evaluated the use of sublingual fentanyl. They found no improvement over placebo, but observed a greater number of adverse effects. Other strategies have included nitrous oxide/oxygen (N2O/O2) administration prior to bone marrow biopsy, a low-cost, easily administered technique that can be used in the outpatient setting 8, 9. Other factors that influence the sensation of pain are patient anxiety, gender, age, body mass index and level of education, along with adequate information given prior to the procedure, history of previous biopsy, extent of the operator’s experience in the technique, and the duration and technical difficulty of the procedure 9. In clinical experience, the pain associated with the procedure has been reduced by a combination of factors: waiting for the lidocaine to take effect, continuous communication with the patient, and music therapy. Ultimately, however, bone marrow biopsy is still a painful procedure despite these strategies.
Figure 5. Bone marrow biopsy pain scale
Does a bone marrow biopsy hurt?
Yes, bone marrow biopsy is a painful procedure. You may feel a brief sharp pain or stinging. Factors that influence the sensation of pain are patient anxiety, gender, age, body mass index and level of education, along with adequate information given prior to the procedure, history of previous biopsy, extent of the operator’s experience in the technique, and the duration and technical difficulty of the procedure 9. In clinical experience, the pain associated with the procedure has been reduced by a combination of factors: waiting for the lidocaine to take effect, continuous communication with the patient, and music therapy.
Bone marrow biopsy and bone marrow aspiration is usually performed under local anesthesia. General anesthesia is reserved for children and/or very anxious patients.
How long does a bone marrow biopsy take?
The bone marrow biopsy and bone marrow aspiration typically takes about 10 minutes. Extra time is needed for preparation and post-procedure care, especially if you receive intravenous (IV) sedation. The total time for the procedure is about 30 minutes.
Reasons for bone marrow biopsy
Bone marrow biopsy and bone marrow aspiration offer detailed information about the condition of your bone marrow and blood cells.
Your doctor may order a bone marrow exam if blood tests are abnormal or don’t provide enough information about a suspected problem.
Your doctor may perform a bone marrow exam to:
- Diagnose a disease or condition involving the bone marrow or blood cells
- Determine the stage or progression of a disease
- Check iron levels and metabolism
- Monitor treatment of a disease
- Investigate a fever of unknown origin
Bone marrow biopsy and aspiration may be used for many conditions. These include:
- Anemia
- Blood cell conditions in which too few or too many of certain types of blood cells are produced, such as leukopenia, leukocytosis, thrombocytopenia, thrombocytosis, pancytopenia and polycythemia
- Cancers of the blood or bone marrow, including leukemias, lymphomas and multiple myeloma
- To diagnose lymphoma patients
- Diagnosis of lymphoma infiltration of bone marrow
- Diagnosis of hematological diseases
- To check the effect of radiation/chemotherapy on bone marrow if there are problems with long-term cytopenia
- To diagnose metastatic tumors in bone marrow. Cancers that have spread from another area, such as breast, into the bone marrow.
- Hemochromatosis
- Fevers of unknown origin
A bone marrow biopsy and a bone marrow aspiration offer different, but complementary, information about your bone marrow cells. The two procedures are usually performed together.
Bone marrow biopsy procedure
Bone marrow aspiration has gained momentum due to the possibility of obtaining hematopoietic stem cells. These are useful not only in the treatment of hematological and non-hematological diseases, but also for the purpose of tissue reconstruction 10.
The following describes the general technique used in sternal bone marrow aspiration. The technique used in iliac spine sampling is described in connection with bone marrow biopsy.
How you prepare for a bone marrow biopsy and bone marrow aspiration
Bone marrow biopsy and bone marrow aspiration are often performed on an outpatient basis in a hospital, clinic or doctor’s office. Special preparation usually isn’t needed. However, you may want to:
- Tell your doctor about medications and supplements you take. Certain medications and supplements may increase your risk of bleeding after a bone marrow biopsy and aspiration.
- Tell your doctor if you’re nervous about your procedure. Discuss your worries about the exam with your doctor. In some cases, your doctor may give you a sedative medication before your exam, in addition to a numbing agent (local anesthesia) at the site where the needle is inserted.
Before the bone marrow biopsy procedure
Your blood pressure and heart rate will be checked, and you’ll be given some form of anesthesia to keep you comfortable.
Most people need only local anesthesia, as bone marrow aspiration, in particular, can cause brief, but sharp, pain. You’ll be fully awake during the procedure, but the aspiration and biopsy site will be numbed to reduce pain.
- Bone marrow biopsy and bone marrow aspiration is usually performed under local anesthesia. General anesthesia is reserved for children and/or very anxious patients.
If you feel anxious about pain, you may be given an IV medication so that you’re either completely or partially sedated during the bone marrow exam.
The area where the doctor will insert the biopsy needle is marked and cleaned. The bone marrow fluid (aspirate) and tissue sample (biopsy) are usually collected from the top ridge of the back of a hipbone (posterior superior iliac spine or crest). Sometimes, the front of the hip may be used.
Bone marrow aspiration — but not biopsy — is occasionally collected from the breastbone or, in children under the age of 12 to 18 months, from the lower leg bone.
You’ll be asked to lie on your abdomen or side, and your body will be draped with cloth so that only the exam site is showing.
Bone marrow biopsy technique
The best site for bone marrow biopsy is the posterior superior iliac spine. The biopsy is usually performed using a Jamshidi size 8–11 needle. The first step is to identify the parts of the needle, and then locate the sampling site.
- The bone marrow aspiration is usually done first.
- Correct injection of local anesthesia is crucial for the patient’s experience of the procedure. Inject 5–10 ml Xylocain® 10 mg/ml with adrenaline to reduce bleeding in the area. Inject a minimal amount intracutaneously. The patient will feel when the needle apex meets the periosteum. Rotate the syringe 180° to distribute the local anesthesia in the area. Allow the anesthesia to work before expanding the area by angling the cannula in four directions. To keep the cannula from simply turning in the same area, the cannula should be pulled back slightly each time before changing directions.
- The doctor makes a small incision with the scalpel before the biopsy to avoid unnecessary trauma of the skin, then inserts a hollow needle through the bone and into the bone marrow. The incision will heal better. Using a syringe attached to the needle, the doctor withdraws a sample of the liquid portion of the bone marrow. You may feel a brief sharp pain or stinging. The aspiration takes only a few minutes. Several samples may be taken.
- The health care team checks the sample to make sure it’s adequate. Rarely, fluid can’t be withdrawn and the needle is moved for another attempt.
- Your doctor uses a larger needle to withdraw a sample of solid bone marrow tissue. The biopsy needle is specially designed to collect a core (cylindrical sample) of bone marrow.
- The bone marrow biopsy can be collected from several different sites (anterior or posterosuperior iliac crest). Mark the preferred sampling site.
- Administer anaesthesia as described for bone marrow needle aspiration. When the trephine needle is assembled, it is inserted into the sampling site either directly, or after making a small (0.2cm) incision to facilitate access to the bone. The needle is pushed into the bone by rotating it on its axis.
- When the desired depth is reached, the stylet is withdrawn and the needle is advanced using the same rotating movement.
- The depth of the needle is measured using a stylet. A specimen measuring approximately 2cm in length should be collected.
- When the correct depth has been ascertained, the needle is rotated in the opposite direction to help loosen the specimen. The needle, with the specimen, is then withdrawn using a rotational movement.
New sampling methods
Bone marrow aspiration is less sensitive than bone marrow biopsy for detecting metastasis or lymphoid infiltration 11. Generally speaking, bone marrow biopsy does not give false positives, and is 100% consistent when performed bilaterally 12. The rate of positive diagnosis for lymphoid infiltration correlates with the length of the biopsy specimen (increasing by 35% in specimens measuring ≥20mm) 13. Bone marrow biopsy is a blind sampling technique, and as such it is difficult to accurately determine the length of the specimen collected. Recently, Islam, in the Buffalo General Hospital (USA), published a study on the use of ultrasound to gauge bone marrow biopsy specimen size 14.
Sternal puncture technique
- With the patient in the supine position, locate the sternal angle using gentle digital palpation. Use the needle cover to locate the intersection between the sternal angle and the midsternal line (Figure 6A and 6B). To facilitate the procedure, you will be asked to extend your neck (Figure 6C). The area will be sterilized and cover it with a surgical aperture drape.
- Administer local anaesthetic with 1% lidocaine, using 3 ml to anaesthetise the skin and subcutaneous tissue. Then, gently inject lidocaine at various points on the cortical bone, administering 1 ml anaesthetic with each injection.
- After a waiting time of between 3 and 5 min, start the procedure. First, identify the parts of the bone marrow needle (Figure 6D). Hematologists usually use size 16 and 18 needles.
- Insert the needle at the previously marked site, through the skin and subcutaneous tissue until it abuts the bone.
- Push the needle through the bony cortex, rotating it on its axis until it is fixed in place at the desired depth (Figure 6A and 6B).
- Withdraw the stylet (Figure 7C), attach a 20ml syringe, and aspirate gently (Figure 7D).
- For a smear sample, aspirate only 1ml of fluid.
- The smear technique used will usually vary from one hospital to another. Figure 8 shows the steps involved to prepare the smear.
Figure 6. Sternal puncture technique – Note: Sternal puncture. (A) Location of the sternal puncture site. The sternal angle, formed by the junction of the manubrium and the body of the sternum, lies 2cm below the sternal notch. (B) Gently mark the puncture site. (C) Inject 10ml lidocaine, initially at the level of the skin, and then in the periosteum. (D). Identify the parts of the Osgood needle before performing aspiration.

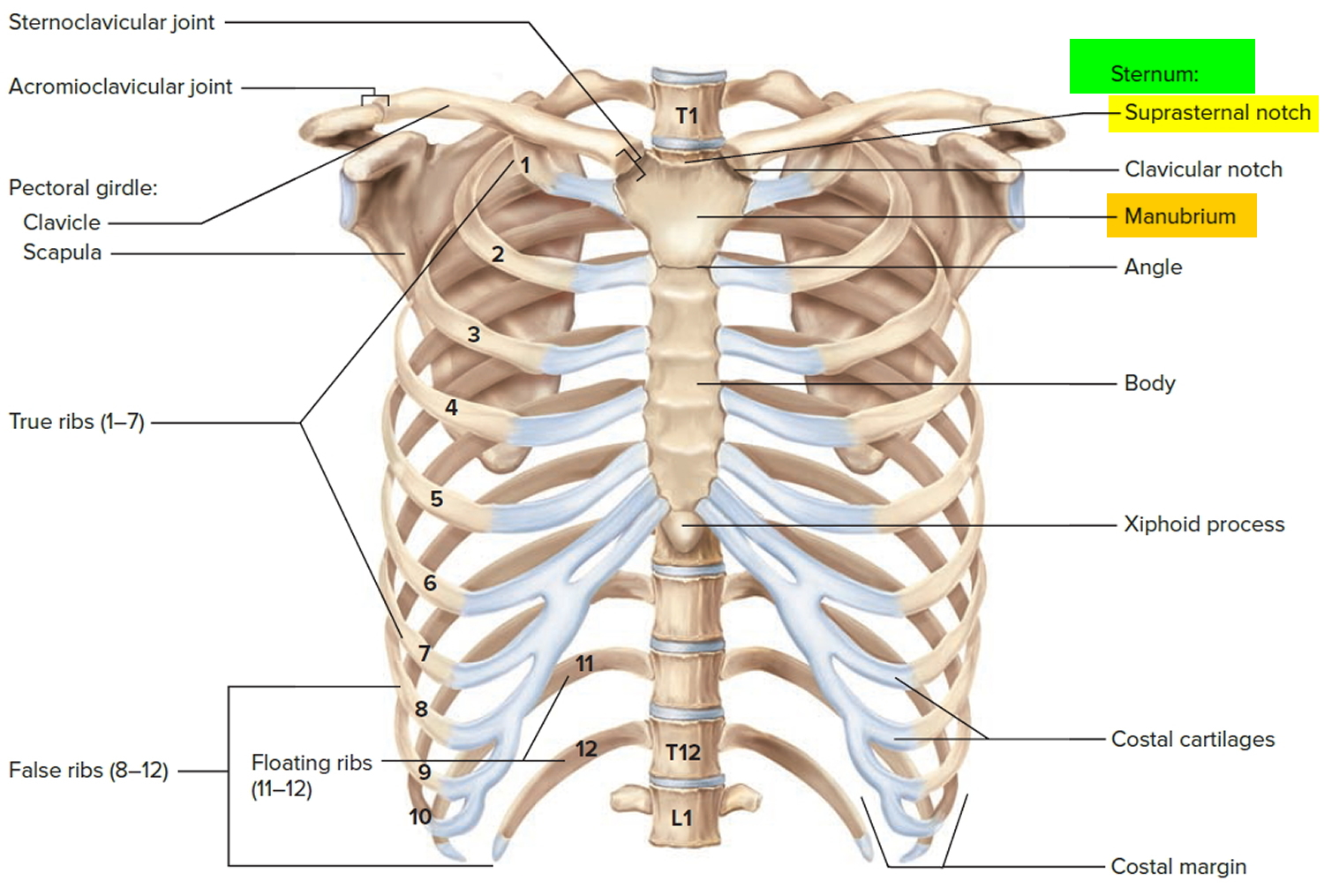 Figure 7. Sternal puncture technique – Note: (A) Introduce the needle by rotating it on its axis. (B) Continue until the needle is fixed in place. (C) Remove the stylet. (D) Draw the aspirate using a 20ml syringe. Only 1ml will be needed for the smear.
Figure 7. Sternal puncture technique – Note: (A) Introduce the needle by rotating it on its axis. (B) Continue until the needle is fixed in place. (C) Remove the stylet. (D) Draw the aspirate using a 20ml syringe. Only 1ml will be needed for the smear.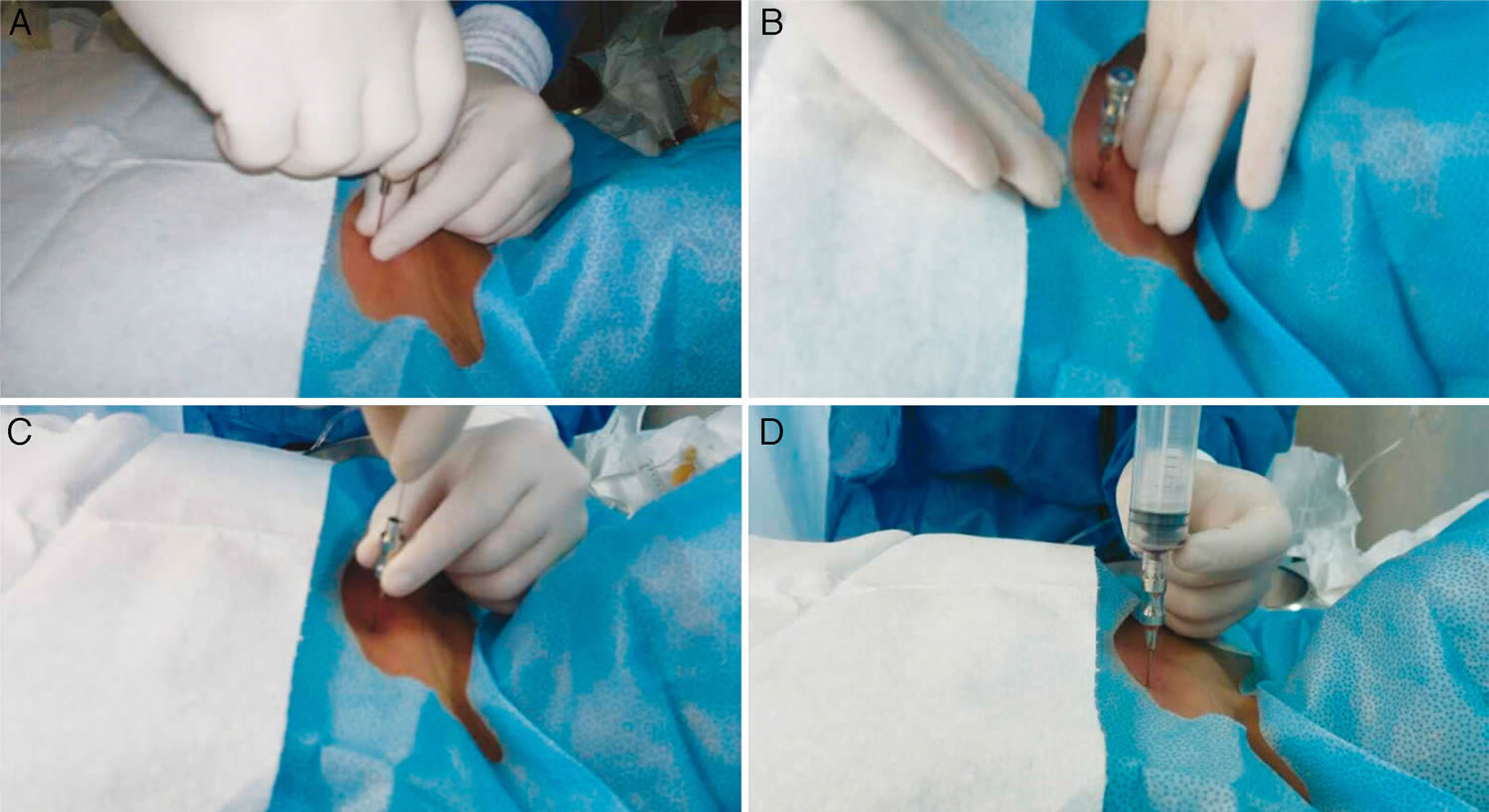
After the bone marrow biopsy and bone marrow aspiration procedure
Pressure will be applied to the area where the needle was inserted to stop the bleeding. Then a bandage will be placed on the site.
If you had local anesthesia, you’ll be asked to lie on your back for 10 to 15 minutes and apply pressure to the biopsy site. You can then leave and go about your day, returning to normal activity as soon as you feel up to it.
If you had IV sedation, you’ll be taken to a recovery area. Plan to have someone drive you home, and take it easy for 24 hours.
You may feel some tenderness for a week or more after your bone marrow exam. Ask your doctor about taking a pain reliever, such as acetaminophen (Tylenol, others).
Site care
Wear the bandage and keep it dry for 24 hours. Don’t shower, bathe, swim or use a hot tub. After 24 hours you can get the aspiration and biopsy area wet.
Contact your doctor if you have:
- Bleeding that soaks through the bandage or doesn’t stop with direct pressure
- A persistent fever
- Worsening pain or discomfort
- Swelling at the procedure site
- Increasing redness or drainage at the procedure site
To help minimize bleeding and discomfort, avoid rigorous activity or exercise for a day or two.
Bone marrow biopsy results
The bone marrow samples are sent to a laboratory for analysis. Your doctor generally gives you the results within a few days, but it may take longer.
At the lab, a hematologist or a specialist in analyzing biopsies (pathologist) will evaluate the samples to determine if your bone marrow is making enough healthy blood cells and to look for abnormal cells. The information can help your doctor:
- Confirm or rule out a diagnosis
- Determine how advanced a disease is
- Evaluate whether treatment is working
Depending on your exam results, you may need follow-up tests.
As mentioned above, specimen size is one the main problems encountered in the interpretation of bone marrow biopsy specimens. In the case of bone marrow aspirate, the main problem is the quality of the smear. Interpretation of a bone marrow smear will be unsafe if the sample is hemodiluted 15. The smear technique has been described in Figure 8 below, and initially requires about 0.5ml of aspirate. The greater the volume collected, the higher the risk of a haemodiluted sample. Bone marrow smears must be performed immediately following collection; 5 or 6 smears are usually sufficient. If the smears cannot be prepared immediately, the aspirate should be placed into a tube containing ethylene diamine tetra-acetic acid (EDTA) at a concentration of 1.5±0.25mg/ml of blood. For immunophenotyping, karyotyping or molecular studies, sample collection should follow the recommendations of the respective laboratories 16.
Figure 8. Preparing the bone marrow smear
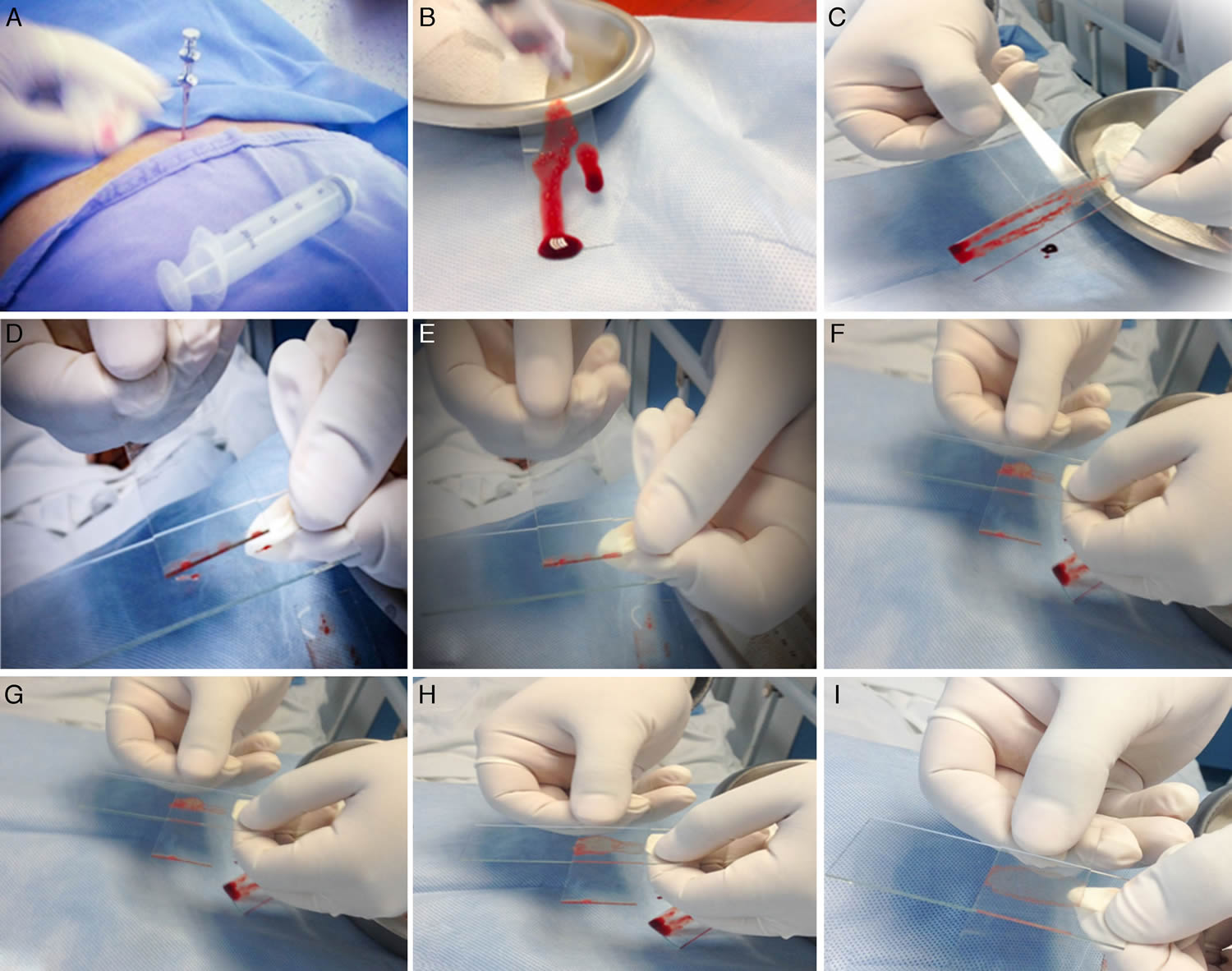
Note: (A) When the bone marrow aspiration needle is in place, use a 20ml syringe to draw 1ml of aspirate. (B) Place a few drops of aspirate on a slide held vertically to facilitate visualisation of the bone marrow spicules. (C) Using the edge of a second slide, separate and isolate a few bone marrow spicules from the rest of the sample. (D) Transfer these to a third slide. (E) Without applying pressure, distribute the spicules in the center of the slide. (F) Place the second slide across the third slide to form a cross with the spicules in the center. (G) Gently but quickly slide the second slide over the third slide to extend the spicules along its length. (H) Make sure the aspirate is spread evenly over the entire slide. (I) Allow to dry for 5min, and then send it to the lab for tincture.
A bone marrow examination involves:
- Smear for primary examination, otherwise for special indications
- Imprint of biopsy – the biopsy is placed on the slide glass and rolled out. This can be done if there are problems with the aspirate.
- Peripheral blood smear is taken if there is suspicion of leukemization (malignant cells in the blood circulation)
An expanded examination may include
- Flow cytometry immunphenotyping (marker testing)
- Cytogenetics (chromosome testing)
- Other molecular testing (For example PCR: polymerase chain reaction, FISH: fluorescence in situ hybridization)
- Special examinations associated with studies
Bone marrow biopsy complications
Bone marrow exams are generally safe procedures. Complications are rare but can include:
- Excessive bleeding, particularly in people with low numbers of a certain type of blood cell (platelets)
- Infection, especially in people with weakened immune systems
- Long-lasting discomfort at the biopsy site
- Penetration of the breastbone (sternum) during sternal aspirations, which can cause heart or lung problems
- Bone marrow aspiration and biopsy. Technique and considerations. Rev Med Hosp Gen Mex 2015;78:196-201 – DOI: 10.1016/j.hgmx.2015.06.006 http://www.elsevier.es/en-revista-revista-medica-del-hospital-general-325-articulo-bone-marrow-aspiration-biopsy-technique-S0185106315000700[↩]
- Trepanning or trephines: a history of bone marrow biopsy. Br J Haematol, 139 (2007), pp. 14-19 http://dx.doi.org/10.1111/j.1365-2141.2007.06749.x[↩]
- Disorders of iron metabolism. E. Beutler. Williams hematology, 8th ed.[↩]
- P.W. Bishop,K. McNally,M. Harris. Audit of bone marrow trephines. J Clin Pathol, 45 (1992), pp. 1105-1108 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC495006/pdf/jclinpath00426-0065.pdf[↩][↩]
- Bone marrow examination: techniques and interpretation. Hematol Oncol Clin N Am, 2 (1988), pp. 513-523[↩]
- A randomized double-blind placebo-controlled study of low-dose intravenous Lorazepam to reduce procedural pain during bone marrow aspiration and biopsy. Pain Med, 9 (2008), pp. 249-252 http://dx.doi.org/10.1111/j.1526-4637.2006.00284.x https://www.ncbi.nlm.nih.gov/pubmed/18298709[↩]
- A.-M. Kuivalainen,F. Ebeling,P.H. Rosenberg. Pre-medication with sublingual fentanyl did not relieve pain associated with bone marrow aspiration and biopsy: a randomized feasibility trial. Eur J Pain, 17 (2013), pp. 1357-1360 http://dx.doi.org/10.1002/j.1532-2149.2013.00303.x[↩]
- N. Hjortholm,E. Jaddini,K. Hałaburda. Strategies of pain reduction during the bone marrow biopsy. Ann Hematol, 92 (2013), pp. 145-149 http://dx.doi.org/10.1007/s00277-012-1641-9[↩]
- S.A. Kanagasundaram,L.J. Lane,B.P. Cavalletto. Efficacy and safety of nitrous oxide in alleviating pain and anxiety during painful procedures. Arch Dis Child, 84 (2001), pp. 492-495 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1718795/[↩][↩][↩]
- Bone marrow aspiration: technique, grafts, and reports. D. Smiler,M. Soltan. Implant Dent, 15 (2006), pp. 229-235 http://dx.doi.org/10.1097/01.id.0000236125.70742.86[↩]
- Comparison of bone marrow aspiration and bone marrow biopsy in neoplastic diseases. Gulf J Oncol, (2009), pp. 41-44[↩]
- Evaluation of bone marrow in 143 lymphomas: the relative frequency and pattern of involvement, secondary myelopathies, pitfalls and diagnostic validity. J Egypt Natl Cancer Inst, 20 (2008), pp. 17-30[↩]
- Optimum trephine length in the assessment of bone marrow involvement in patients with diffuse large cell lymphoma. Ann Oncol, 14 (2003), pp. 273-276 https://www.ncbi.nlm.nih.gov/pubmed/12562655[↩]
- Ultrasound: a new tool for precisely locating posterior iliac crests to obtain adequate bone marrow trephine biopsy specimen. J Clin Pathol, 66 (2013), pp. 718-720 http://dx.doi.org/10.1136/jclinpath-2013-201463[↩]
- B.J. Bain,K. Bailey. Pitfalls in obtaining and interpreting bone marrow aspirates: to err is human. J Clin Pathol, 64 (2011), pp. 373-379 http://dx.doi.org/10.1136/jcp.2010.080820[↩]
- S.-H. Lee,W.N. Erber,A. Porwit. ICSH guidelines for the standardization of bone marrow specimens and reports. Int J Lab Hematol, 30 (2008), pp. 349-364 http://dx.doi.org/10.1111/j.1751-553X.2008.01100.x[↩]





{kind=link}