
Contents
What is brachial artery
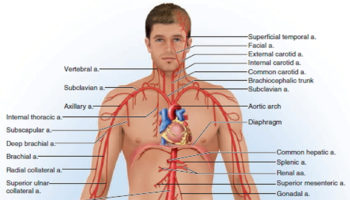
The brachial artery is a branch of a prominent artery – the subclavian artery that changes its name along its course. After leaving the thoracic cavity and passing over the first rib, each subclavian artery becomes an axillary artery. The axillary arteries supply blood to the muscles of the pectoral region and axilla. The axillary artery crosses the axilla and enters the arm, where it gives rise to the humeral circumflex arteries 1. These vessels supply structures near the head of the humerus. Beyond this loop, the axillary artery becomes the brachial artery, which supplies blood to the upper limb (see Figure 3).
The brachial artery continues down the medial and anterior sides of the humerus and ends just distal to the elbow, supplying the anterior flexor muscles of the brachium along the way. The brachial artery is the most common site of blood pressure measurement, using an inflatable cuff that encircles the arm and compresses the artery. The deep brachial artery arises from the proximal end of the brachial and supplies the humerus and triceps brachii muscle (see Figure 3). About midway down the arm, it continues as the radial collateral artery 2.
Locating the brachial artery in the arm
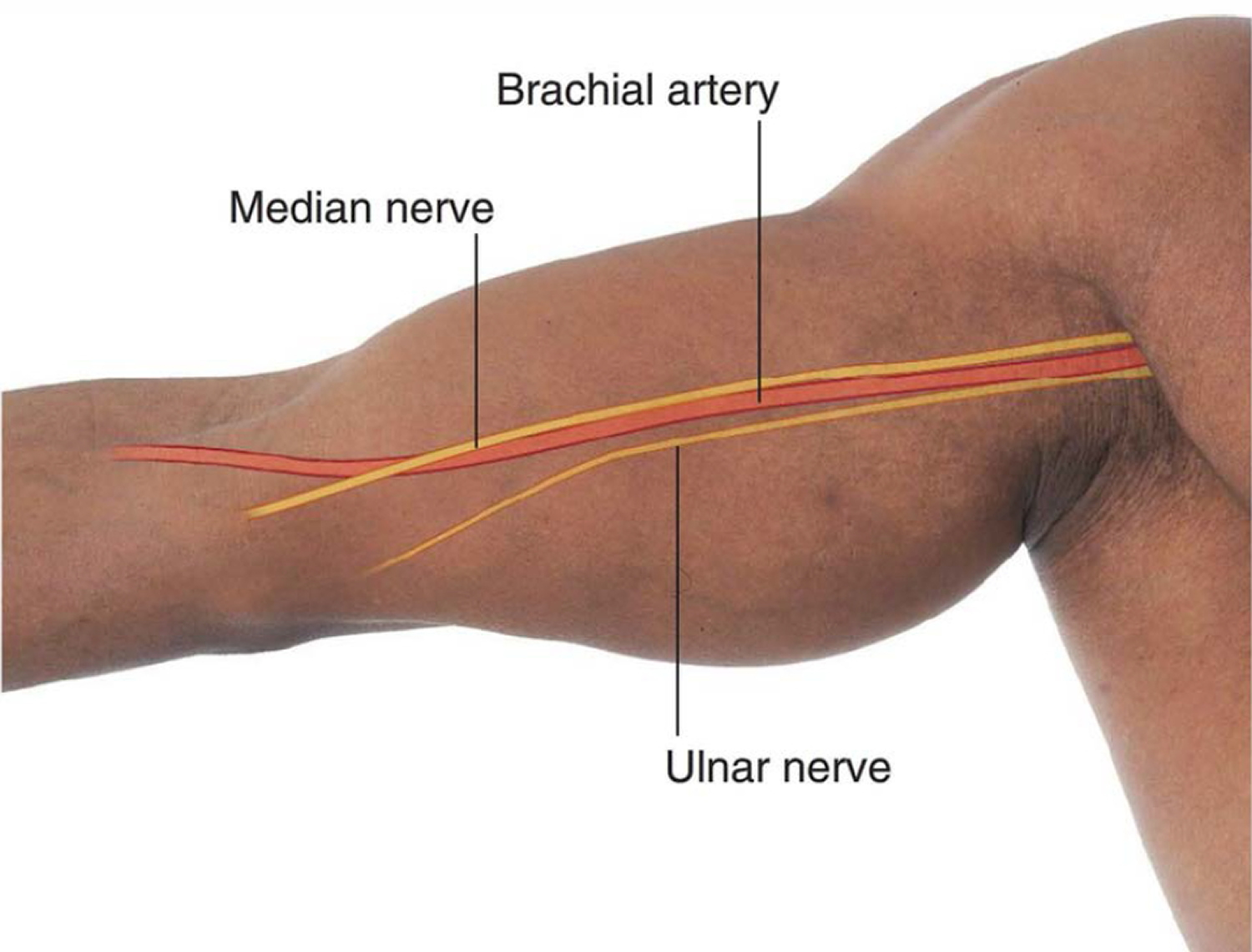
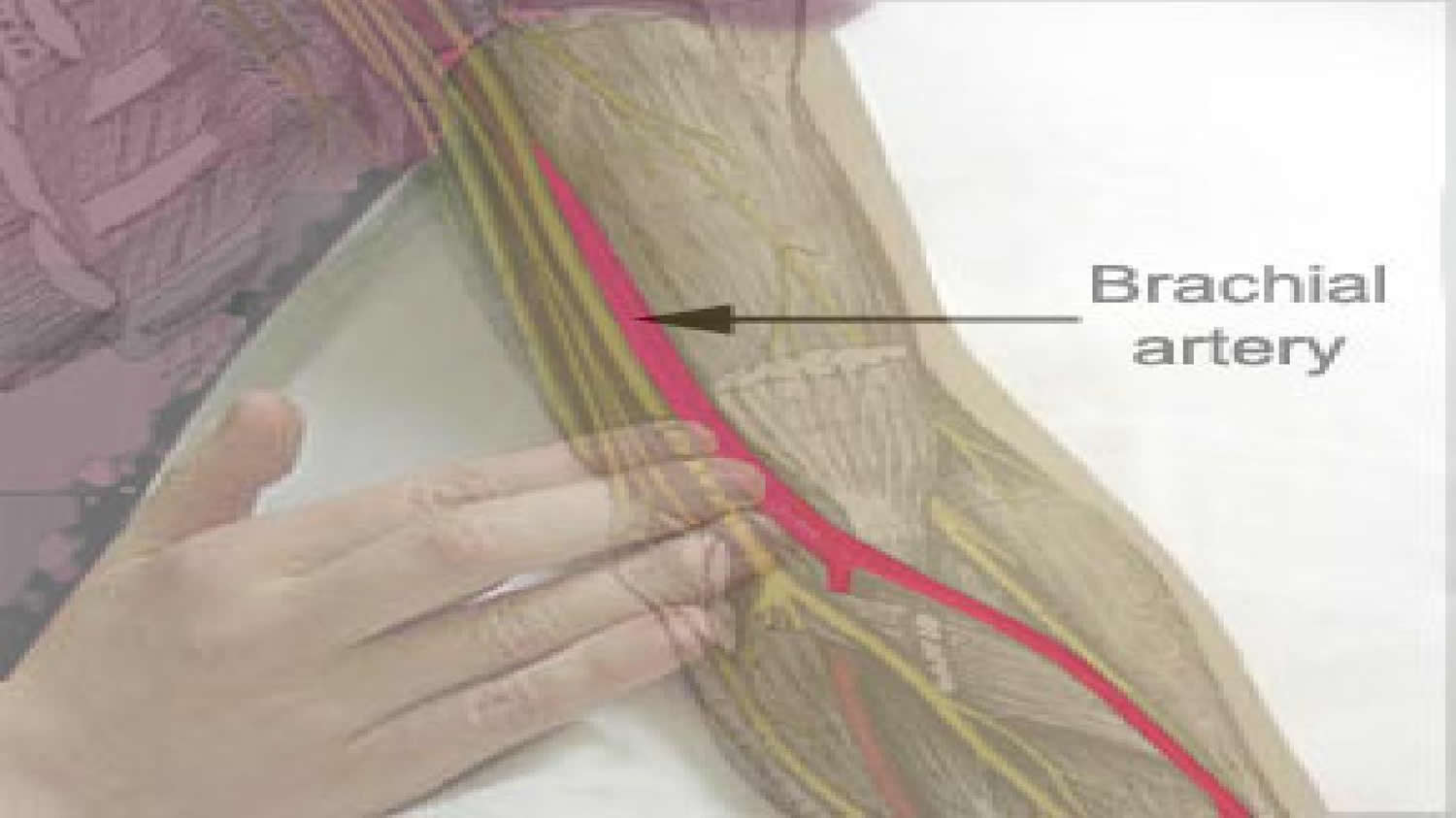
The brachial artery is on the medial side of the arm in the cleft between the biceps brachii and triceps brachii muscles (Figure 4) . The median nerve courses with the brachial artery, whereas the ulnar nerve deviates posteriorly from the vessel in distal regions.
Figure 1. Origin of brachial artery
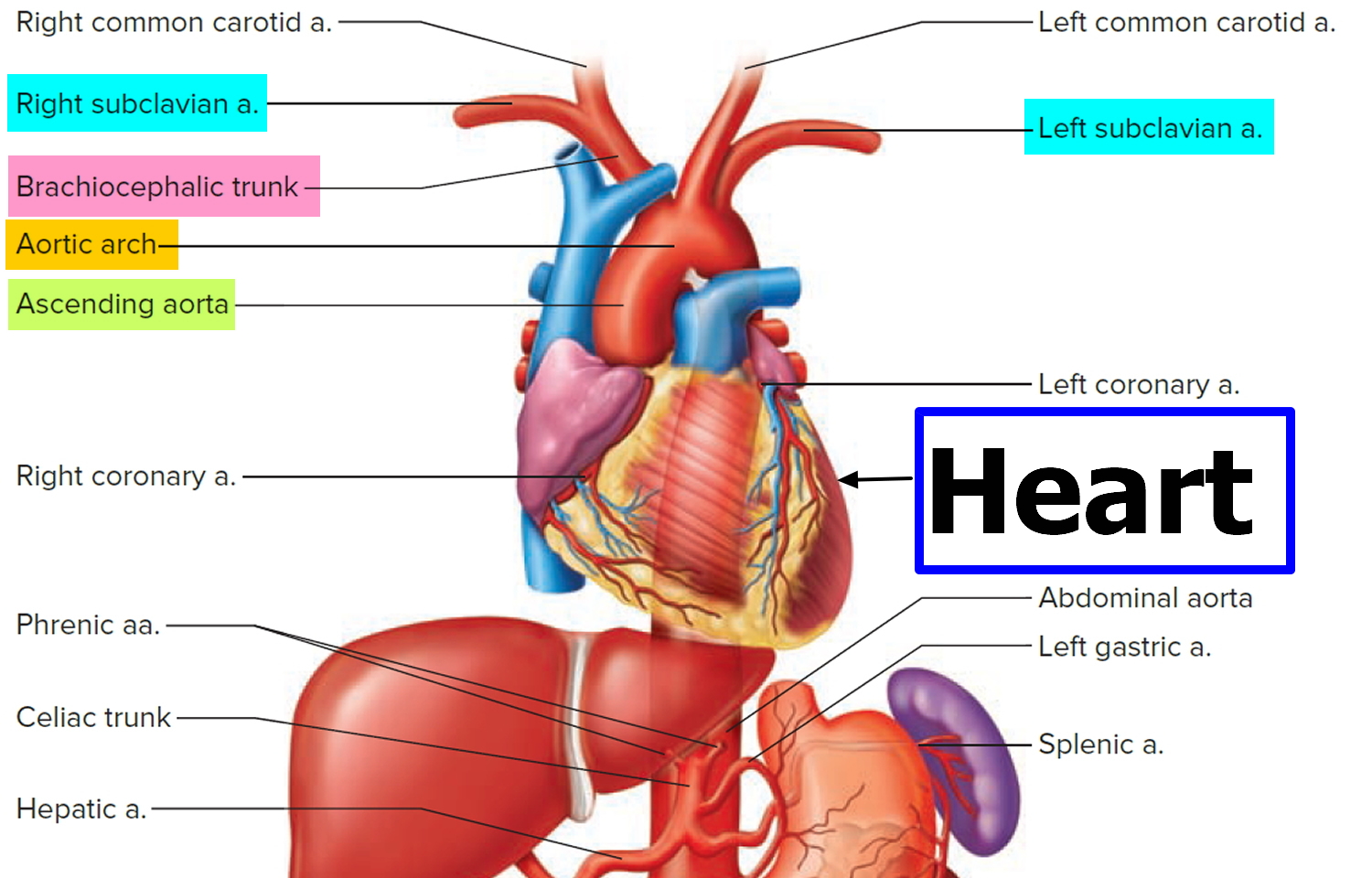
Figure 2. Brachial artery
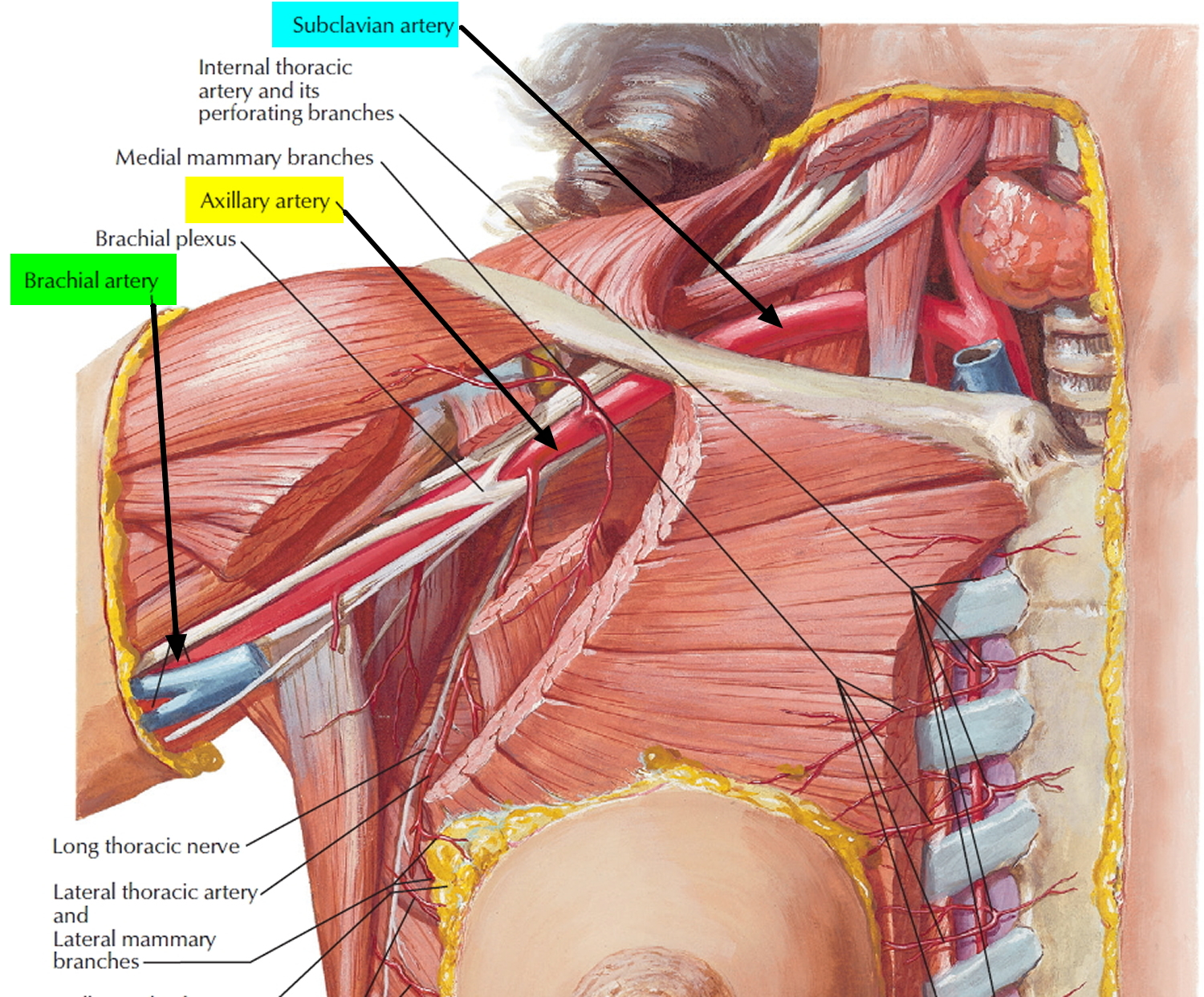
Figure 3. Brachial artery anatomy
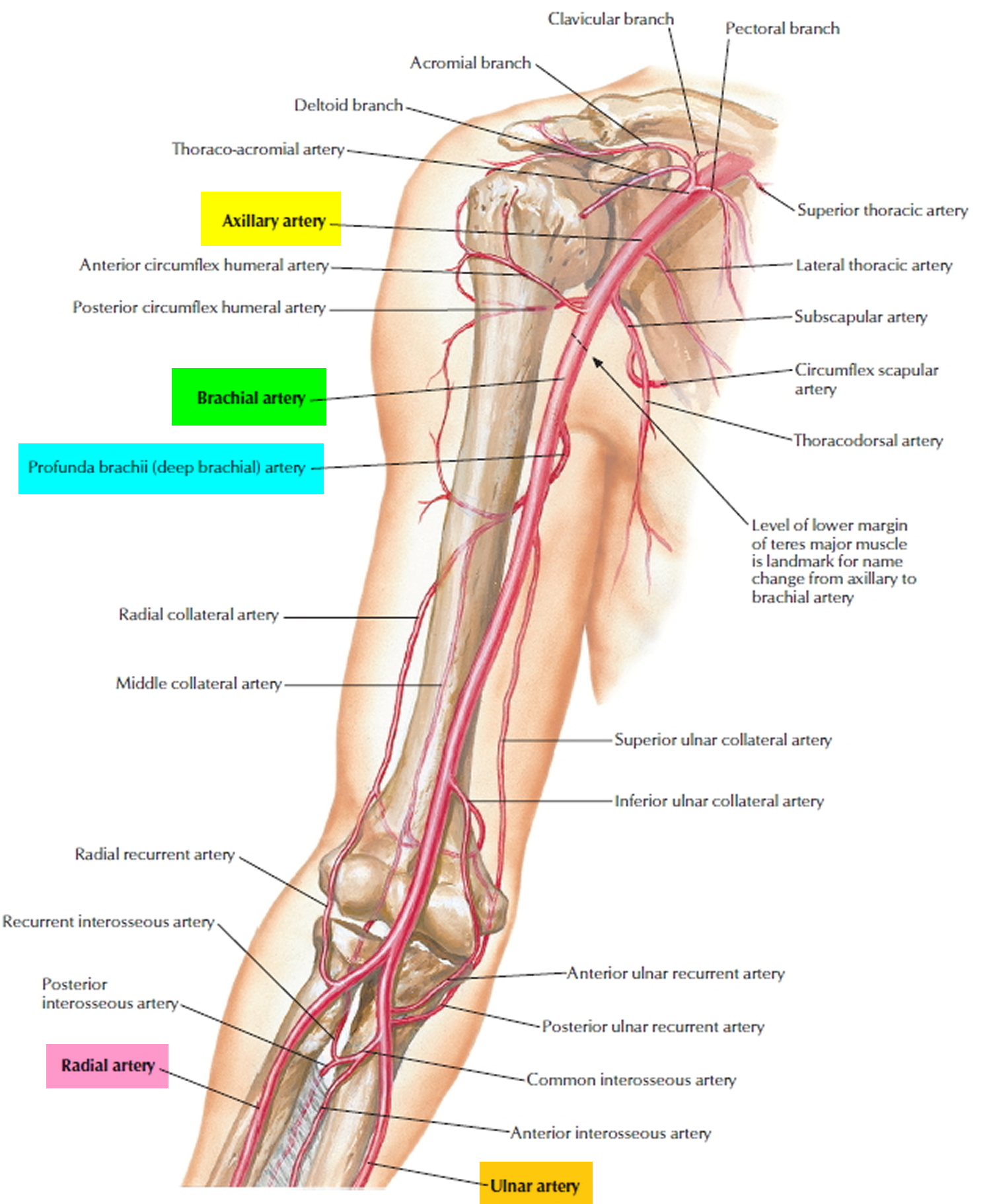
Figure 4. Brachial artery location in the arm
Brachial artery blood pressure
The heart is responsible for supplying the organs and tissues of the body with blood. To do this it pumps blood into the large vessels of the circulatory system with every beat. The blood that is pumped into these vessels puts pressure on the walls of the vessels. When the heart muscle contracts during each heartbeat, the pressure rises as well. When measuring blood pressure, there are two different values:
- Systolic blood pressure is taken while the heart muscle is contracting and pumping oxygen-rich blood into the blood vessels.
- Diastolic blood pressure is taken while the muscle is relaxing and refilling with blood.
In clinical use, the term blood pressure usually refers to the pressure in arteries generated by the left ventricle during systole and the pressure remaining in the arteries when the ventricle is in diastole. Blood pressure is usually measured in the brachial artery in the left arm. The device used to measure blood pressure is a
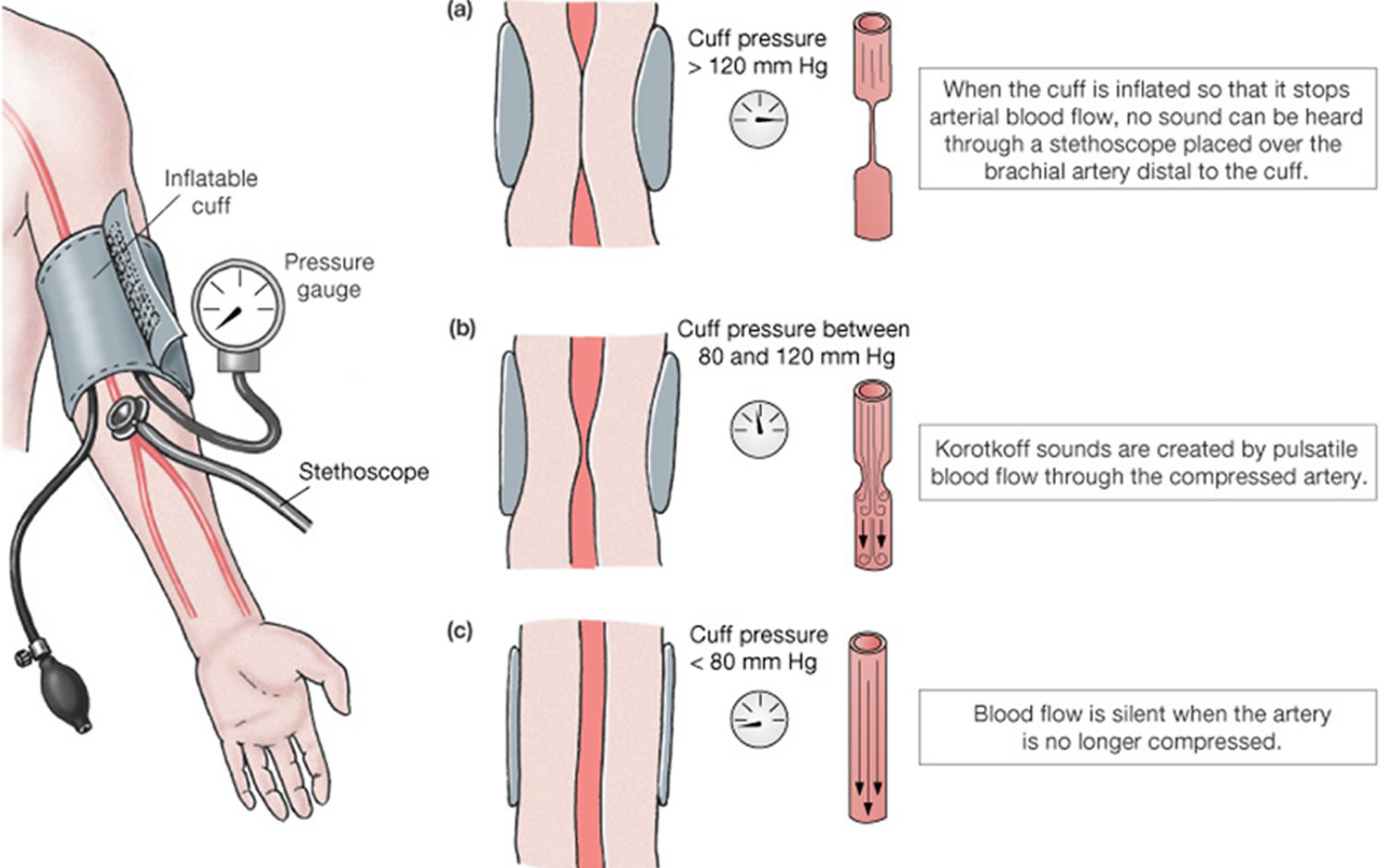
sphygmomanometer. It consists of a rubber cuff connected to a rubber bulb that is used to inflate the cuff and a meter that registers the pressure in the cuff. With the arm resting on a table so that it is about the same level as the heart, the cuff of the sphygmomanometer is wrapped around a bared arm. The cuff is inflated by squeezing the bulb until the brachial artery is compressed and blood flow stops, about 30 mmHg higher than the person’s usual systolic pressure. The technician places a stethoscope below the cuff on the brachial artery, and slowly deflates the cuff . When the cuff is deflated enough to allow the artery to open, a spurt of blood passes through, resulting in the first sound heard through the stethoscope. This sound corresponds to systolic blood pressure, the force of blood pressure on arterial walls just after ventricular contraction. As the cuff is deflated further, the sounds suddenly become too faint to be heard through the stethoscope. This level, called the diastolic blood pressure, represents the force exerted by the blood remaining in arteries during ventricular relaxation. At pressures below diastolic blood pressure, sounds disappear altogether. The various sounds that are heard while taking blood pressure are called Korotkoff sounds.
Digital blood pressure meters are often used on the wrist, but they can also be placed on the finger or upper arm and only have to be activated by pressing a button. They read the blood pressure automatically from variations in the volume of the blood present in the arteries.
When measuring on the wrist it is important to keep the hand level with the heart. Otherwise you can get skewed results. Digital meters can also sometimes be inaccurate and produce unreliable readings – especially in people with certain heart rhythm problems or arteries hardened due to arteriosclerosis.
Blood pressure is measured in units of “millimeters of mercury”; written mmHg for short. Blood pressure measurements are always given in pairs, with the upper (systolic blood pressure) value first, followed by the lower (diastolic blood pressure) value. So someone who has a reading of 132/88 mmHg (often spoken “132 over 88”) has a systolic blood pressure of 132 mmHg and a diastolic blood pressure of 88 mmHg.
It is important to measure blood pressure more than once, because it fluctuates over the course of the day 3. Physical exertion, stress, pain or extreme heat or cold can affect blood pressure, for example. But if blood pressure changes due to any of these things, it is only temporarily high and will then fall back down to normal range quickly.
So, if blood pressure is measured just once and found to be high, it does not automatically mean that it is also permanently too high. A blood pressure reading taken at the doctor’s office can also be misleading: a visit to the doctor makes some people so nervous that their blood pressure rises.
All of this means that to get reliable results it is important to always take readings on different days and while the person is at rest. This means sitting back and relaxing on a chair and waiting about three minutes before taking a measurement so that the circulatory system comes to rest. The upper arm, which is commonly used to take the measurement, should lie on a table at about the same level as the heart while the reading is being done.
Which number is more important ?
Typically, more attention is given to systolic blood pressure (the top number) as a major risk factor for cardiovascular disease for people over 50 4. In most people, systolic blood pressure rises steadily with age due to the increasing stiffness of large arteries, long-term build-up of plaque and an increased incidence of cardiac and vascular disease.
However, elevated systolic or diastolic blood pressure alone may be used to make a diagnosis of high blood pressure. And, according to recent studies, the risk of death from ischemic heart disease and stroke doubles with every 20 mm Hg systolic or 10 mm Hg diastolic increase among people from age 40 to 89 4.
Figure 5. Blood pressure measurement over the brachial artery
What is normal blood pressure, and when is blood pressure considered to be high ?
Blood pressure is always measured on several days and when you are at rest 3. If several of these measurements are too high, you are said to have high blood pressure, even if only one of the two – either the systolic or the diastolic value – is high 3. The medical term for high blood pressure is hypertension. Normal blood pressure in adults is below 140 mmHg for systolic and below 90 mmHg for diastolic.
Normal blood pressure: systolic under 140 mmHg and diastolic under 90 mmHg. However, the normal (optimal) blood pressure range is 120/80 mm Hg. People who exercise regularly and are in good physical condition may have even lower blood pressures. Thus, blood pressure slightly lower than 120/80 may be a sign of good health and fitness.
A person has hypertension if the systolic value is over 140 mmHg, the diastolic value is over 90 mmHg, or if both are too high. High blood pressure itself usually goes unnoticed. Only if it is extremely high can it result in symptoms like dizziness or trouble seeing.
If hypertension remains undetected for a long time and is not treated, the risk of cardiovascular disease such as heart attacks, strokes and heart and kidney failure increases. So if you or your doctor think you have high blood pressure it is important to have your blood pressure checked regularly. If the readings are repeatedly abnormal, there are several different ways of lowering your blood pressure and thereby decreasing the risk of complications.
Table 1. Healthy and unhealthy blood pressure ranges
| Blood Pressure Category | Systolic mm Hg (upper #) | Diastolic mm Hg (lower #) | |
|---|---|---|---|
| Normal | less than 120 | and | less than 80 |
| Prehypertension | 120 – 139 | or | 80 – 89 |
| High Blood Pressure (Hypertension) Stage 1 | 140 – 159 | or | 90 – 99 |
| High Blood Pressure (Hypertension) Stage 2 | 160 or higher | or | 100 or higher |
| Hypertensive Crisis (Emergency care needed) | Higher than 180 | or | Higher than 110 |
Note: A diagnosis of high blood pressure must be confirmed with a medical professional. A doctor should also evaluate any unusually low blood pressure readings. Additionally, lower targets may be appropriate for some populations such as African-Americans, the elderly, or patients with underlying issues such as diabetes mellitus or chronic kidney disease.
[Source: American Heart Association 5]Prehypertension (early stage high blood pressure)
Prehypertension is when blood pressure is consistently ranging from 120-139/80-89 mm Hg. People with prehypertension are likely to develop high blood pressure unless steps are taken to control it.
Hypertension Stage 1
Hypertension Stage 1 is when blood pressure is consistently ranging from 140-159/90-99 mm Hg. At this stage of high blood pressure, doctors are likely to prescribe lifestyle changes and may consider adding blood pressure medication.
Hypertension Stage 2
Hypertension Stage 2 is when blood pressure is consistently ranging at levels greater than 160/100 mm Hg. At this stage of high blood pressure, doctors are likely to prescribe a combination of blood pressure medications along with lifestyle changes.
Hypertensive crisis
This is when high blood pressure requires emergency medical attention. If your blood pressure is higher than 180/110 mm Hg and you are NOT experiencing symptoms such as chest pain, shortness of breath, back pain, numbness/weakness, changes in vision or difficulty speaking, wait about five minutes and take it again. If the reading is still at or above that level, you should CALL your local emergency number and get help immediately.
A hypertensive (high blood pressure) crisis is when blood pressure rises quickly and severely. There are two types of hypertensive crises — both require immediate medical attention 5.
- Hypertensive Urgency
If you get a blood pressure reading of 180/110 or greater, wait about five minutes and try again. If the second reading is just as high, seek immediate medical help. Early evaluation of organ function is critical to determine an appropriate course of action. Your elevated reading may or may not be accompanied by one or more of the following symptoms 5:
- Severe headache
- Shortness of breath
- Nosebleeds
- Severe anxiety
Treatment of hypertensive urgency may involve adjusting or adding medications, but rarely requires hospitalization.
- Hypertensive Emergency
Hypertensive emergencies generally occur at blood pressure levels exceeding 180 systolic OR 120 diastolic, but organ damage can occur at even lower levels in patients whose blood pressure had not been previously high.
The consequences of uncontrolled blood pressure in this range can be severe and include 5:
- Stroke
- Loss of consciousness
- Memory loss
- Heart attack
- Damage to the eyes and kidneys
- Loss of kidney function
- Aortic dissection
- Angina (unstable chest pain)
- Pulmonary edema (fluid backup in the lungs)
- Eclampsia
Brachial artery injury
Vascular injuries of the upper extremity represent approximately 30% to 50% of all peripheral vascular injuries. The majority of injuries are to the brachial artery, and 90% of injuries are due to penetrating trauma 6. The morbidity and mortality rates associated with brachial artery injuries depend on the cause of the injury itself, which vein or tendon is injured, and whether musculoskeletal and nerve injuries are also present. In recent years, the limb salvage rate has reached nearly 100% because of early transport of patients to the hospital, early diagnosis, increased surgical experience, and developments in the treatment of hypovolemic shock and the use of antibiotic therapy 7.
Patients with obvious clinical symptoms of brachial artery injuries as detected by physical examination and those in whom Doppler ultrasonography demonstrates a substantial difference in pressure between the right and left brachial arteries should undergo surgical repair without further angiographic examination. Doppler ultrasonography of the upper extremity has been shown to be as specific and sensitive as arteriography in detecting brachial artery injuries 8. Normally, the average brachial–brachial Doppler pressure index between the 2 upper extremities is approximately 0.95; it is rarely less than 0.85 9. If uncertainty remains regarding vascular injuries after physical examination and Doppler ultrasonography, angiography may be used to confirm the vascular injury.
Compartmental edema or contusion can impair venous drainage and arterial flow and can cause pressure injuries to the nerves 10.
Major venous injuries, fractures, and widespread tissue destruction may also influence the long-term function of the extremity 11. Whether primary and secondary nerve repair procedures are helpful is a point of controversy 12. The rate of functional disability ranges from 27% to 44% when injury to the upper extremity includes nerve injuries 13.
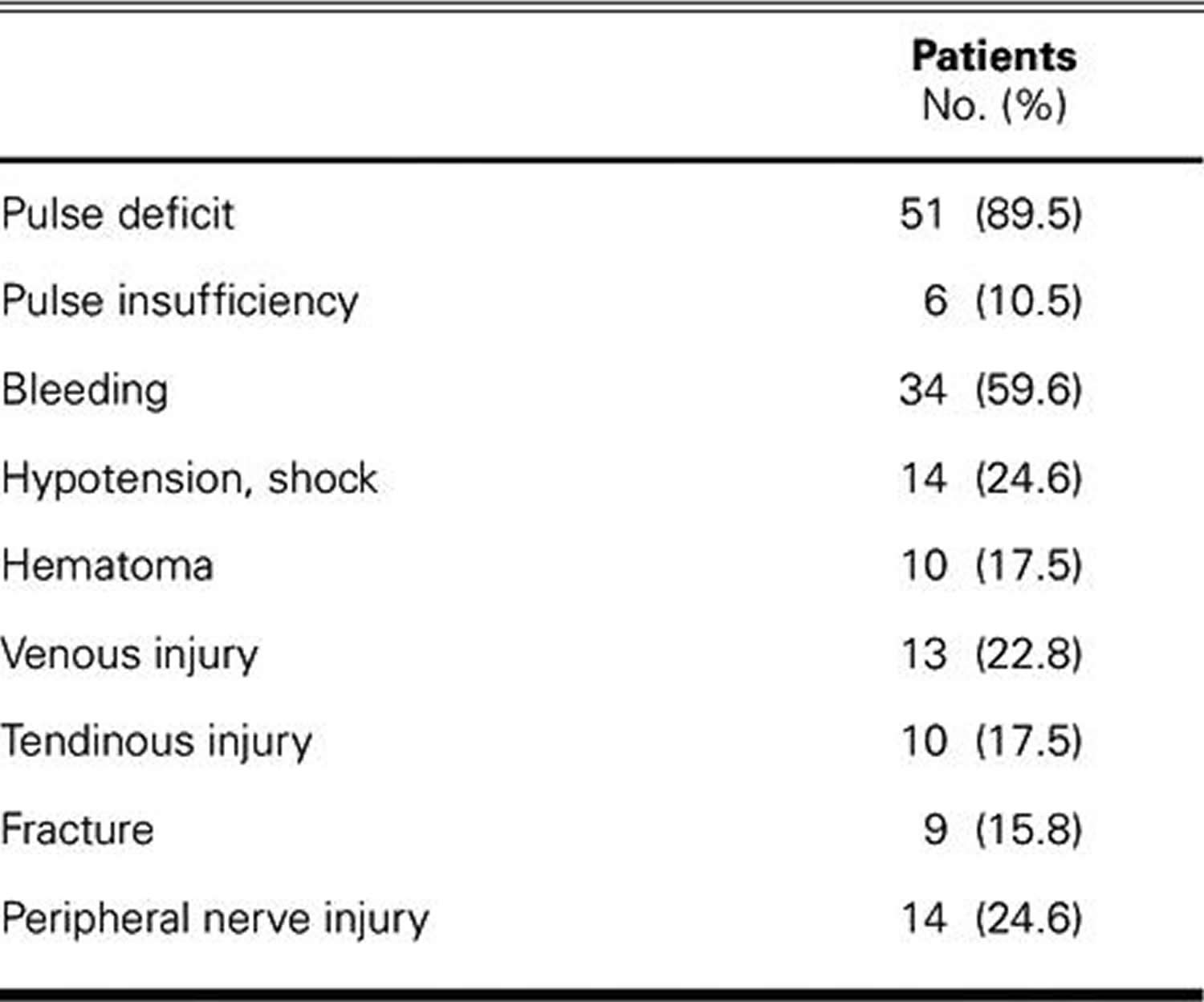
Table 2. Signs and Symptoms of Arterial Ischemia among Patients with Traumatic Brachial Artery Injury
- Human Anatomy 9th Edition. Frederic H. Martini, Inc., Robert B. Tallitsch, and Judi Nath. Published by Pearson Education, Inc., publishing as Pearson Benjamin Cummings.[↩]
- Human Anatomy 5th Edition. Kenneth S. Saladin. Georgia College & State University McGraw-Hill Education, 2 Penn Plaza, New York, NY 10121.[↩]
- What is blood pressure and how can I measure it ? National Center for Biotechnology Information, U.S. National Library of Medicine. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072435/[↩][↩][↩]
- American Heart Association. Understanding Blood Pressure Readings. http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/KnowYourNumbers/Understanding-Blood-Pressure-Readings_UCM_301764_Article.jsp[↩][↩]
- Understanding Blood Pressure Readings. American Heart Association. http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/KnowYourNumbers/Understanding-Blood-Pressure-Readings_UCM_301764_Article.jsp[↩][↩][↩][↩]
- Hunt CA, Kingsley JR. Vascular injuries of the upper extremity. South Med J 2000;93:466–8. https://www.ncbi.nlm.nih.gov/pubmed/10832942[↩]
- Shanmugam V, Velu RB, Subramaniyan SR, Hussain SA, Sekar N. Management of upper limb arterial injury without angiography–Chennai experience. Injury 2004;35:61–4. https://www.ncbi.nlm.nih.gov/pubmed/14728956[↩]
- Meissner M, Paun M, Johansen K. Duplex scanning for arterial trauma. Am J Surg 1991;161:552–5. https://www.ncbi.nlm.nih.gov/pubmed/2031535[↩]
- Johnston KW. Upper extremity ischemia. In: Rutherford RB, editor. Vascular surgery. 5th ed. Philadelphia: WB Saunders; 2000. p. 1111–39.[↩]
- Velmahos GC, Theodorou D, Demetriades D, Chan L, Berne TV, Asensio J, et al. Complications and nonclosure rates of fasciotomy for trauma and related risk factors. World J Surg 1997;21:247–53. https://www.ncbi.nlm.nih.gov/pubmed/9015166[↩]
- Visser PA, Hermreck AS, Pierce GE, Thomas JH, Hardin CA. Prognosis of nerve injuries incurred during acute trauma to peripheral arteries. Am J Surg 1980;140:596–9. https://www.ncbi.nlm.nih.gov/pubmed/7435813[↩]
- Rich NM, Spencer FC. Vascular trauma. Philadelphia: WB Saunders; 1978. p. 125–56[↩]
- Hardin WD Jr, O’Connell RC, Adinolfi MF, Kerstein MD. Traumatic arterial injuries of the upper extremity: determinants of disability. Am J Surg 1985;150:266–70. https://www.ncbi.nlm.nih.gov/pubmed/4025709[↩]
- Ergunes K, Yilik L, Ozsoyler I, Kestelli M, Ozbek C, Gurbuz A. Traumatic Brachial Artery Injuries. Texas Heart Institute Journal. 2006;33(1):31-34. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1413600/[↩]
{kind=link}