Contents
- What is inferior vena cava
- Inferior vena cava physiologic variants
- What does the inferior vena cava do?
- Inferior vena cava syndrome
- Inferior vena cava syndrome causes
- Inferior vena cava syndrome pathophysiology
- Inferior vena cava syndrome signs and symptoms
- Inferior vena cava syndrome complications
- Inferior vena cava syndrome diagnosis
- Inferior vena cava syndrome differential diagnosis
- Inferior vena cava syndrome treatment
- Inferior vena cava syndrome prognosis
- Inferior vena cava filter
What is inferior vena cava
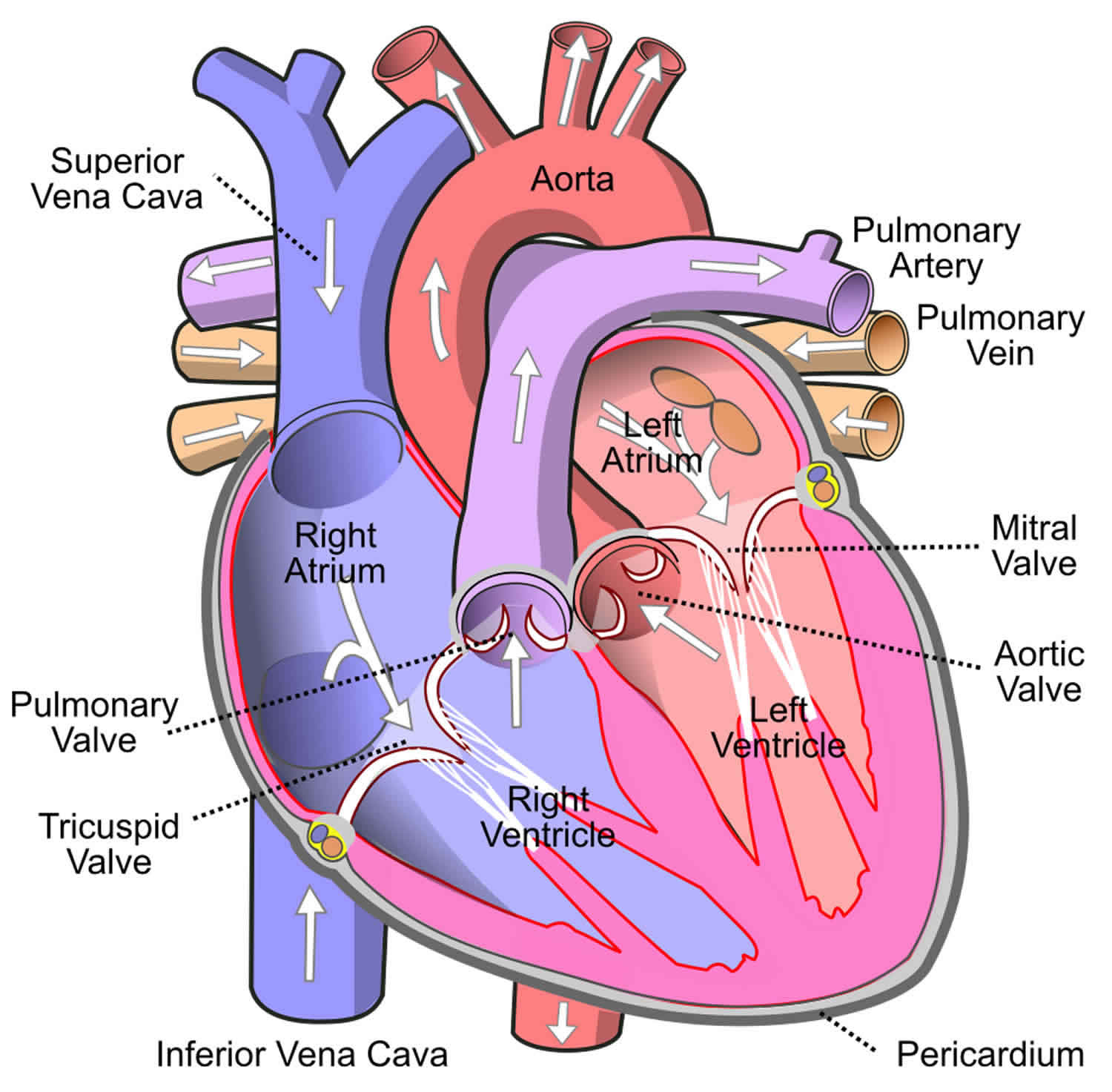
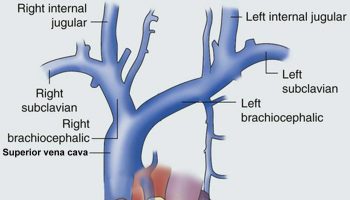
Inferior vena cava is a large retroperitoneal blood vessel formed by the confluence of the right and left common iliac veins (usually occurs at the L5 vertebral level) that is responsible for transporting deoxygenated blood from the body regions inferior to the diaphragm (lower extremities and abdomen) back to the right atrium of your heart. The inferior vena cava lies along the right anterolateral aspect of the vertebral column and passes through the central tendon of the diaphragm around the T8 vertebral level. Inferior vena cava has the largest diameter of the venous system and is a thin-walled vessel. These anatomic characteristics make it ideal for transporting large quantities of venous blood. Many veins contain one-way valves to ensure the forward flow of blood back toward the heart. The inferior vena cava, however, does not contain such valves, and forward flow to the heart is driven by the differential pressure created by normal respiration. As the diaphragm contracts and creates negative pressure in the chest for the lungs to fill with air, this pressure gradient pulls the venous blood from the abdominal inferior vena cava into the thoracic inferior vena cava and subsequently into the right heart. The inferior vena cava enters the right atrium of the heart after coursing through the diaphragm, entering the posterior inferior aspect of the atrium. The inferior vena cava enters the right atrium inferior to the entrance of the superior vena cava.
The inferior vena cava is a mostly symmetric vessel with a few exceptions. Due to the inferior vena cava residing on the right side of the vertebral column the vessels entering the inferior vena cava from the left side of the body, like the left renal vein, are longer than their anatomic counterparts on the right. Other left-sided veins, like the left adrenal and left gonadal vein, first join the left renal vein before joining the inferior vena cava and continuing as venous flow returning to the heart. This differs from the right side of the body where the right adrenal and right gonadal vein directly join the inferior vena cava without first joining the right renal vein. Anatomic variants venous of anatomy involving both right and left sides have been described 1.
Blood from the left and right femoral veins enters the inferior vena cava via the left and right common iliac veins, respectively. Blood from the abdominal viscera travels into the portal vein and enters the inferior vena cava via the hepatic veins after traversing the liver and its sinusoids. Venous blood from the abdominal wall reaches the inferior vena cava through lumbar veins. Ascending lumbar veins connect lumbar veins to the azygos vein and this provides some collateral circulation between the inferior vena cava and the superior vena cava 2. This potential for collateral flow could be critical if either of the larger veins becomes obstructed.
Below is a list of (most common) vertebral levels at which different veins enter the inferior vena cava:
- T8: Hepatic veins, inferior phrenic veins
- L1: Right suprarenal vein, renal veins
- L2: Right gonadal vein
- L1-L5: Lumbar vertebral veins
- L5: Right and left common iliac veins
Blood Supply and Lymphatics
Blood supply to the inferior vena cava is derived partially from the deoxygenated blood it carries towards the heart and partially supplied by the vasa vasorum that penetrate the tunica adventitia of the vessel 3.
Nerves
The inferior vena cava receives autonomic innervation from the splanchnic nerves 4. This innervation serves to alter the diameter of the inferior vena cava via interactions with alpha-1, alpha-2, and beta-2 receptors.
Muscles
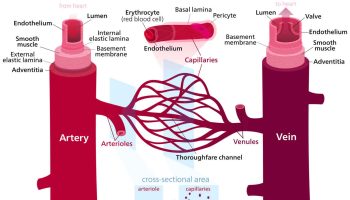
As in all vasculature, the inferior vena cava contains three layers: the tunica intima, the tunica media, and the tunica adventitia. The tunica media layer of the inferior vena cava contains smooth muscle responsive to the input from the nervous system 4. No other muscles are found in the inferior vena cava.
Figure 1. Inferior vena cava
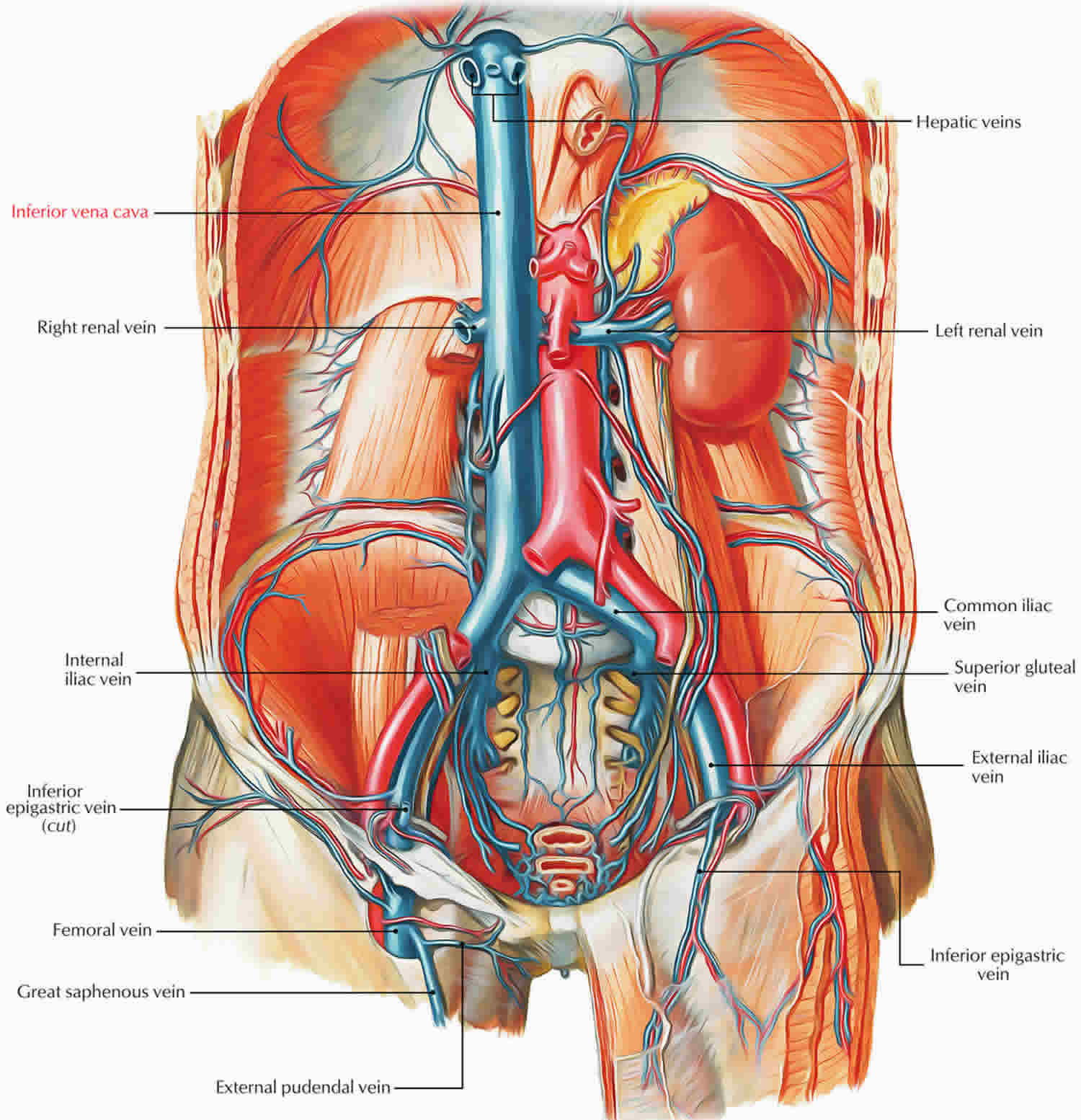
Figure 2. Heart
Inferior vena cava physiologic variants
There are many physiologic variants of the inferior vena cava 1. Compared to the arterial system the venous system is much more susceptible to congenital malformations, many of which remain asymptomatic throughout a patient’s life. If symptoms are present, they are often vague and include abdominal pain or low back pain. Some of the more clinically significant physiologic variants are listed below.
- Left Inferior Vena Cava: This anomaly is caused by regression of the right supracardinal vein and the persistence of the left supracardinal vein. The left inferior vena cava is joined by the left renal vein and then crosses anterior to the aorta before it joins the right atrium, forming a normal pre-renal inferior vena cava. This anomaly has a suspected prevalence of 0.2% to 0.5%.
- Double Inferior Vena Cava: This anomaly is caused by the persistence of both the left and right supracardinal veins. A prevalence of 0.2% to 0.3% is suspected.
- Intrahepatic Inferior Vena Cava Agenesis: Congenital anomaly resulting in the lack of the intrahepatic inferior vena cava. Intrahepatic venous supply bypasses the hepatic inferior vena cava through the azygous/hemiazygous venous system 2.
- Absent Infrarenal Inferior Vena Cava: This is the rarest of the physiologic caval anomalies. The suspected and currently accepted etiology of absent infrarenal inferior vena cava is intrauterine or perinatal thrombosis and resultant degeneration of the infrarenal inferior vena cava 5.
What does the inferior vena cava do?
Inferior vena cava is ultimately responsible for the transport of almost all venous blood (deoxygenated) from the abdomen and lower extremities back to the right side of your heart for oxygenation.
Inferior vena cava syndrome
Inferior vena cava syndrome (IVCS) also called inferior vena cava obstruction (IVCO) is a collection of clinical signs and symptoms resulting from either partial or complete obstruction of blood flow through the inferior vena cava (IVC) preventing blood from flowing normally from your abdomen and lower extremities back to the right side of your heart for oxygenation 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19. Inferior vena cava syndrome (IVCS) symptoms include swelling in your legs (pitting leg edema), shortness of breath, scrotal swelling (in males) and abdominal discomfort. There are many causes of inferior vena cava syndrome (IVCS) such as blood clot (thrombosis), tumor thrombosis, iatrogenic occlusion caused by liver transplantation, congenital abnormality such as Budd-Chiari syndrome (a rare disorder that occurs when blood flow out of your liver is obstructed causing serious complications, including liver damage and fluid build-up in your abdomen), compression by tumor outside the vein, liver abscess, retroperitoneal fibrosis, or uterus during the third trimester of pregnancy 20. A blood clot (thrombosis) in the inferior vena cava is a difficult clinical condition to diagnose. Although a blood clot (thrombosis) in the inferior vena cava can be asymptomatic, inferior vena cava thrombosis can also present with a myriad of symptoms. These are usually non-specific symptoms like abdominal or back pain, but may also include leg cramping, swelling, or pain. A blood clot (thrombosis) in the inferior vena cava treatment is based on patient condition/symptoms and can include anticoagulation, clot removal and/or filter (if present) removal via Interventional Radiology techniques or rarely open surgical technique. The most common cause of inferior vena cava thrombosis in a patient without anatomic variants is previous inferior vena cava filter placement.
The symptoms of inferior vena cava syndrome (inferior vena cava obstruction) are dependent upon the level of obstruction and they include intravascular hypovolemia, liver damage, kidney damage, edema of lower extremities, and ileus 21, 22. In rare occasions, intravascular hypovolemia caused by inferior vena cava obstruction induces circulation collapse and result in shock, a life-threatening condition 23.
The classic presentation of inferior vena cava thrombosis (IVCT) includes bilateral leg edema with dilated, visible superficial abdominal veins (caput medusae) 24. Intuitively, this collection of clinical signs and symptoms makes sense, though it is not universally found. In one study, almost 60% of patients did not have bilateral leg edema 24. In addition, if the thrombus (blood clot) is confined to the inferior vena cava and does not involve the iliac or femoral veins, the collateral pathways form along the posterior abdominal wall. This scenario may have significant impact on surgical procedures involving this anatomic region. Occlusive thrombus of the inferior vena cava (IVC) at the juxtarenal level can affect kidney function by altering kidney blood flow.
It is hypothesized that blood return with an absent inferior vena cava (IVC) is inadequate, despite adequate collaterals, resulting in chronic venous hypertension in the lower extremities and causing venous stasis that precipitates thrombosis.
Because patients with inferior vena cava syndrome (IVCS) or inferior vena cava obstruction (IVCO) may present with a variety of signs and symptoms, the diagnosis can be challenging 25. Inferior vena cava syndrome (IVCS) is less frequently found in comparison with the superior vena cava syndrome (SVCS) 7. Using a system to classify the symptoms (e.g, predominantly thrombotic in origin or predominantly embolic in nature) may aid in the diagnosis. However, only with your doctor’s awareness of the possibility of inferior vena cava syndrome (IVCS) or inferior vena cava obstruction (IVCO), you’re more likely to receive prompt diagnosis and subsequent treatment that minimizes ensuing complications.
The treatment of inferior vena cava syndrome (inferior vena cava obstruction) varies dependent on the underlying cause of inferior vena cava syndrome (inferior vena cava obstruction). For example, cancer requires surgical resection, chemotherapy, and radiation, whereas in case of thrombosis, anticoagulants form the mainstay of treatment 7, 22. Obstruction of inferior vena cava caused by extravascular compression from a malignant tumor can be treated by irradiation 26 or endovascular stent placement 27, 14.
Inferior vena cava syndrome causes
The cause of inferior vena cava syndrome (IVCS) depends on the interrupted blood flow location. The pathogenesis of inferior vena cava syndrome (IVCS) is divided into two events, including the vena cava obstruction and compression by adjacent structures. The obstruction of the inferior vena cava (IVCO) is mostly caused by a primary thrombotic event, either congenital (present at birth) or acquired 16. Congenital thrombosis of the inferior vena cava (IVC) is often asymptomatic which is caused by well-developed collaterals 28. In contrast, acquired causes include spontaneous thrombosis of the inferior vena cava (IVC) either due to external compression or pathological changes of the inferior vena cava (IVC) wall 16. Inferior vena cava thrombosis (IVCT) can be due to the spreading of a blood clot from deep venous thrombosis (DVT) or from the extension of a thrombus 16. In addition, conditions that increase the obstruction risk of inferior vena cava (IVC) are cancer, pregnancy, infection, obesity, or other intrinsic vein disease 7.
Cancer of organs near the inferior vena cava (IVC), such as renal cell carcinoma (the most common type of kidney cancer in adults) 29, gastric adenocarcinoma (the most common type of stomach cancer) 30, pancreatic adenocarcinoma (the most common type of pancreatic cancer) 31, primary or metastatic liver cancers or tumor of any organ surrounding the inferior vena cava (IVC) can compress the inferior vena cava (IVC) which leads to obstruction of venous return to your heart 7. Tumor compression of the inferior vena cava (IVC) results in blood clot formation (thrombosis) can sometimes lead to the development of superior vena syndrome (SVCS) in conjunction with inferior vena cava syndrome (IVCS) 32.
In pregnancy, the distended uterus can compress the inferior vena cava (IVC) which leads to obstruction of the blood flow to your heart and causes increased venous congestion or pooling 33.
Inferior vena cava syndrome (IVCS) can also be due to congenital malformations such as May-Thurner syndrome also called iliocaval compression syndrome (a rare condition that occurs when the right iliac artery compresses left common iliac vein in the pelvis, this compression disrupts blood flow and may lead to deep vein thrombosis [DVT]) or Budd-Chiari syndrome (a rare disorder that occurs when blood flow out of your liver is obstructed causing serious complications, including liver damage and fluid build-up in your abdomen). May-Thurner syndrome is a chronic condition in which anatomical variations of vessels in the iliocaval region cause blood flow obstruction 35, 36. Budd-Chiari syndrome is a rare disorder that occurs when blood flow out of your liver is obstructed causing serious complications, including liver damage and fluid build-up in your abdomen, can be classified as primary or secondary. The primary Budd-Chiari syndrome refers to any obstruction of the hepatic vein due to a primarily venous process such as thrombosis or phlebitis. In comparison, secondary Budd-Chiari syndrome relates to compression of the hepatic veins due to external lesions such as cancer 37.
Inferior vena cava syndrome (IVCS) can also be caused by iatrogenic processes such as inferior vena cava filter placement and venous catheterization, which promotes thrombosis 16. In addition, solid organ transplant or surgery, such as liver lobe resection can also increase the risk of thrombosis 38.
Other disease processes that can cause inferior vena cava syndrome (IVCS) include gallstones (cholelithiasis) 39 and retroperitoneal hemorrhage (a rare but serious condition that occurs when there is bleeding in the retroperitoneal space) 40, can cause obstruction or compression of the inferior vena cava (IVC). Hepatic vena cava syndrome, which is associated with poor-hygiene causing bacterial infection leading to thrombophlebitis of the hepatic veins near the inferior vena cava (IVC) outflow tract, is also recognized as a cause of inferior vena cava syndrome (IVCS) 41.
It has been observed that using Broviac central venous hyperalimentation catheters in children and teens who need IV therapy usually for an extended period can lead to the development inferior vena cava syndrome 42.
Inferior vena cava syndrome pathophysiology
The inferior vena cava (IVC) along with superior vena cava (SVC) returns venous blood (deoxygenated blood, blood that has lost oxygen and is rich in carbon dioxide) to your heart. The pathophysiology of inferior vena cava syndrome (IVCS) is similar to superior vena cava syndrome (SVCS) because of the presence of an underlying process that blocks venous return to the right atrium. Obstruction or compression to the inferior vena cava (IVC) reduces the venous return to your heart, causing an imbalance in the hemodynamic equilibrium. Decreased venous return causes hemodynamic instability in several ways. When there is a decrease in venous return, it will decrease the oxygenation of the blood, which results in hypoxia (low levels of oxygen in your body tissues to sustain bodily function) and subsequent tachycardia (fast heart rate). Furthermore, decreased venous return causes a decrease in heart preload, which leads to decreased cardiac output (the amount of blood pumped by your heart in 1 minute), and the heart compensates by beating rapidly to maintain adequate perfusion to end organs 43.
Thrombosis of the inferior vena cava (IVC) can be caused by either compression or physical obstruction of the inferior vena cava (IVC), which leads to venous stasis. Venous stasis is one of the three criteria of Virchow’s triad of thrombus formation; the other two: hypercoagulable state and endothelial damage 44. The impedance in blood flow causes stasis, which promotes thrombus formation 44.
Inferior vena cava syndrome signs and symptoms
Patients with inferior vena cava syndrome (IVCS) or inferior vena cava obstruction (IVCO) may present with a spectrum of signs and symptoms. Patients may be asymptomatic, or they may present only after complications occur 45. This variability is a significant part of the challenge of diagnosing inferior vena cava syndrome (IVCS). Some people with inferior vena cava syndrome (IVCS) or inferior vena cava obstruction (IVCO) may present with symptoms that are predominantly thrombotic (blood clot) in origin or predominantly embolic (obstruction of an artery or vein by a clot of blood) in nature. Additionally, the thrombotic findings are dependent on the degree of occlusion of the inferior vena cava and on the location between the iliac confluence and the right atrium.
Patients who have inferior vena cava thrombosis (IVCT) may present only after having pulmonary embolism (PE). The lack of uniform symptoms and the significant number of asymptomatic patients contribute to this feature of inferior vena cava thrombosis (IVCT). In one retrospective review of all patients who had cavography (a procedure in which a thin flexible tube called a catheter is inserted through a vein usually in the neck or groin which allows your doctor to take x-ray pictures of the large central vein) to document inferior vena cava thrombus, 20% had angiographically proven pulmonary embolism (PE) with no symptoms of deep vein thrombosis (DVT). Therefore, pulmonary embolism (PE) may be the first sign of inferior vena cava thrombosis (IVCT).
The decreased venous return in inferior vena cava syndrome (IVCS) mimics the presentation of hypovolemic shock and causes tachycardia (fast heart rate), sweating (diaphoresis), low blood pressure (hypotension), shortness of breath on exertion, dizziness, and cold extremities. Inferior vena cava congestion also causes pale skin, the accumulation of fluid in the peritoneal cavity causing abdominal swelling (ascites), lower extremity pitting peripheral edema, and hypoxia (low levels of oxygen in your body tissues to sustain bodily function).
Inferior vena cava syndrome (IVCS) can also presents with generalized symptoms such as nausea, headache, malaise, and fatigue. In extreme cases, the decreased blood, either through thrombotic or non-thrombotic mechanisms, can lead to altered mental status and even death 43.
Inferior vena cava syndrome (IVCS) may rarely cause low back pain mimicking a lumbar hernia and even cauda equina syndrome 46.
In patients with complete absence of the inferior vena cava, symptoms associated with severe venous hypertension (eg, bilateral leg edema, varicose veins, nonhealing venous ulcers, caput medusae [a network of swollen veins around the belly button] or other signs of collateral venous system hypertension/dilatation) may be varied in their manifestation and, in some cases, may not be apparent until later in life.
Inferior vena cava syndrome complications
Complications of inferior vena cava syndrome (IVCS) depend on the underlying comorbidity and patient’s risk factors for the following but include:
- Pulmonary embolism (PE) is a life-threatening blood clot that blocks an artery in your lungs. Pulmonary embolism (PE) occurs when a blood clot breaks off and travels from another part of your body to your lungs. This causes issues with blood flow and oxygen levels in your lungs. A PE is a medical emergency. You need a prompt diagnosis and treatment 47
- Deep vein thrombosis (DVT) is a blood clot (thrombus) that forms in one or more of the deep veins within your body, usually in your leg. Deep vein thrombosis (DVT) can cause leg pain or swelling. Sometimes there are no noticeable symptoms. Get treatment right away so you can prevent serious complications. Treatments include medicines, compression stockings and surgery. Be patient. You may need to take medicine for a few months and wear compression stockings for two years.
- Chronic venous insufficiency (CVI) happens when your leg veins become damaged and can’t work as they should. Normally, valves in your leg veins keep blood flowing back up to your heart. But chronic venous insufficiency damages those valves, causing blood to pool in your legs. This increases pressure in your leg veins and causes symptoms like swelling and ulcers.
- Post-thrombotic syndrome (PTS) is a group of signs and symptoms that develop as a complication of deep vein thrombosis (DVT) 48. Post-thrombotic syndrome occurs within two years of your deep vein thrombosis (DVT) diagnosis in the same affected limb (leg or arm). You may notice pain, heaviness, itching, swelling or redness in your limb progressing to venous ulceration, venous gangrene. Treatment includes compression therapy and lifestyle changes. is a chronic condition that can occur after a deep vein thrombosis (DVT).
- Hemodynamically instability leading to cardiac arrests and possibly death 16 .
Inferior vena cava syndrome diagnosis
Diagnosing inferior vena cava syndrome (IVCS) can be challenging and a high index of suspicion is needed. Inferior vena cava syndrome (IVCS) is not a primary diagnosis but is a consequence of any underlying pathology. The presentation of inferior vena cava syndrome (IVCS) is dependent on the patient’s comorbidities and underlying diseases. Accurate diagnosis is based on a thorough history taking and physical examination. The symptoms which a patient shows are in accordance with the pathophysiology of inferior vena cava syndrome (IVCS). The most reliable noninvasive methods for establishing a diagnosis of inferior vena cava syndrome (IVCS) are computed tomography (CT) with intravenous (IV) contrast and magnetic resonance imaging (MRI). CT, unlike ultrasound, is a good imaging modality for the retroperitoneal space 49. Another accurate, albeit more invasive, imaging modality is venography, which is particularly useful if any surgery is planned.
Patients with inferior vena cava syndrome (IVCS) or inferior vena cava obstruction (IVCO) may present with a spectrum of signs and symptoms. Therefore, it is important to inquire about other signs and symptoms, such as fatigue, dizziness, weight loss, abdominal pain, night sweats, anorexia, palpitations, diaphoresis, dizziness, shortness of breath on exertion. In addition, the history taking also has to get deep into previous illness history, including the history of abdominal surgeries, organ transplantation, lower extremity swelling and pain, family and past medical history of coagulopathy, prior deep venous thrombosis (DVT), as well as occupation and lifestyle.
A thorough physical examination will assist in the accurate diagnosis of IVCS. The vital signs will usually reveal hypotension, tachycardia, and possibly fast breathing (tachypnea) with hypoxia (low levels of oxygen in your body tissues to sustain bodily function). Signs of anemia, such as pale appearance or pale conjunctiva, might be the earlier sign of cancer, and with additional constitutional symptoms of cancer can lead to the diagnosis of IVCS.
While there are no specific tests with pathognomonic findings of inferior vena cava syndrome (IVCS), certain findings such as lower extremity edema, signs of DVT and pulmonary embolism (PE), cold and clammy extremities, abnormal neurological exam, enlarged liver (hepatomegaly), and abdominal swelling due to ascites, can lead to the decrease of venous return which then impair the perfusion of end organs.
Imaging studies and procedures
Duplex ultrasound is the first line of test can be used in a hemodynamically unstable patient. It is a rapid, accurate, and non-invasive modality to investigate the cause of inferior vena cava obstruction (IVCO). Duplex ultrasound is a painless test that uses sound waves to look at blood flow through the valves in the veins. Duplex ultrasound can help find a blood clot. However, interference like obesity, limits the use of ultrasound in identifying the cause of inferior vena cava obstruction (IVCO).
- Advantages of duplex ultrasound include the following:
- Noninvasiveness
- Portability
- Efficacy in helping diagnose deep vein thrombosis (DVT) at the femoral level and, to some extent, at the distal iliac level
- Possible ability to help in visualizing dilated collaterals
- Possibly more accurate assessment of the extent of thrombus than venography
- Disadvantages of duplex ultrasound include the following:
- Operator dependence
- Anatomic limitations
- Less reliable diagnosis within the abdomen because of greater difficulty in assessing venous compressibility
- Loss of respiratory phasicity above the renal veins because of retrograde transmission of the cardiac cycle through the valveless inferior vena cava (IVC)
Esophagogastroduodenoscopy can also be used to reveal esophageal, gastric, or duodenal pathologies, especially tumor which compresses the inferior vena cava (IVC) 30.
CT abdomen and pelvis can then be used as an alternate non-invasive diagnostic modality. CT scan, unlike ultrasound, is a good imaging modality for the retroperitoneal space 49. The very limited data from the literature suggest that, in cases of a congenital absence of inferior vena cava in young people (in some data, patients younger than 30 years; in other data, patients aged 20-40 years), an abdominal CT scan should be performed. False-positive study results sometimes occur.
Magnetic resonance (MR), a non-invasive but expensive diagnostic tool, can also be used to access obstruction of the inferior vena cava (IVC) in hemodynamically stable patients and is replacing CT scans. Underlying causes should be urgently obtained in hypotensive patients in order to prevent complications 16.
- Advantages of MRI include the following:
- Noninvasiveness
- Lack of any ionizing radiation
- Ability to help determine the proximal extent of thrombosis
- Disadvantages of MRI include the following:
- Cost (expensive)
- Less accessibility
- Possibility that turbulent flow may be read falsely as a clot.
Contrast venography, the gold standard for diagnosis, is used to assess the thrombotic obstructions of the abdomen in hemodynamically stable patients. Although it is an invasive procedure, it gives the most accurate finding of inferior vena cava obstruction (IVCO) and compression.
- Advantages of contrast venography include the following:
- Limited false-positive study results
- Access for therapy, thrombolytic agents, or caval interrupting device
- Access for pulmonary angiography (if indicated)
- Disadvantages of contrast venography include the following:
- Invasiveness
- Possible need for more than one puncture
- Possibility of postprocedural deep vein thrombosis (DVT).
Laboratory studies
Assessing the clotting and fibrinolytic systems may be helpful. Confounding factors include variations caused by heparin and warfarin therapy, and dynamic factors involved with acute thrombosis may also alter measured parameters because of the active consumption of factor by the thrombus 50. Gayer et al 51 recommended that all patients with an inferior vena cava (IVC) anomaly be screened for a thrombophilic disorder. In their series, seven of nine patients with an inferior vena cava (IVC) anomaly and deep vein thrombosis (DVT) had a positive thrombophilic screen 51. Therefore, protein C, protein S, antithrombin III, and anticardiolipin studies may all be helpful, but many of these assessments can only be made after the fact 51.
However, there have been three case reports in the English-language medical literature of thromboembolism due to an inferior vena cava (IVC) anomaly (congenital absence of inferior vena cava, absence of the infrarenal portion of the inferior vena cava (IVC), infrarenal IVC hypoplasia), in which the thrombophilic screen was negative in all cases 52, 53, 54. It was hypothesized that multiple emboli from deep vein thrombosis (DVT) in the common and superficial femoral veins migrated through the well-developed hemiazygos or azygos system to the pulmonary circulation.
Inferior vena cava syndrome differential diagnosis
The differential diagnosis of inferior vena cava syndrome (IVCS) is broad, mainly because it is rarely ever diagnosed as a primary disease process.
Inferior vena cava syndrome (IVCS) differential diagnosis are:
- Chronic venous insufficiency is a condition that occurs when blood pools in the veins of your legs. Chronic venous insufficiency happens when your leg veins become damaged and can’t work as they should. Normally, valves in your leg veins keep blood flowing back up to your heart. But chronic venous insufficiency damages those valves, causing blood to pool in your legs. This increases pressure in your leg veins and causes symptoms like swelling and ulcers. This can lead to pain, swelling, and other symptoms.
- Shock is a life-threatening condition that occurs when the body’s blood flow drops suddenly. It can be caused by trauma, heatstroke, blood loss, allergic reaction or other conditions.
- Cancer 31
- Deep vein thrombosis (DVT)
- May-Thurner syndrome also called iliocaval compression syndrome or Cockett’s syndrome is a rare condition that occurs when the right iliac artery compresses left common iliac vein in the pelvis, this compression disrupts blood flow and may lead to deep vein thrombosis (DVT) 35, 36.
- Aortocaval syndrome also known as supine hypotensive syndrome, occurs when the pregnant uterus compresses the aorta and inferior vena cava 33. This can reduce blood flow to the placenta and the mother, and can be life-threatening.
Inferior vena cava syndrome treatment
The guideline treatment of inferior vena cava syndrome (IVCS) has not been clearly described. Therefore, treatment and management are determined by the causative lesion and tailored to the patient’s condition. If the lesion is thrombotic, immediate treatment is focused on the prevention of growth of the blood clot, causing a pulmonary embolism (PE) and management of pain, edema, and the resulting hypotension. Either medical or surgical intervention can accomplish this. Medical treatments include anticoagulation using either low-molecular-weight heparin (LMWH), fondaparinux, or direct thrombin inhibitors. These medications reduce the buildup and growth of the thrombosis but do not eliminate the primary thrombosis.
Endovascular procedures can subsequently be utilized to facilitate the introduction of thrombolytics to lyse the clot. These can include catheter-directed thrombolysis, pulse-spray pharmaco-mechanical thrombolysis, and then angioplasty with or without inserting stents, which increases patency of the inferior vena cava. Performing such procedures is required within a short period (within 14 days) of the onset of symptoms to minimize complications and decrease mortality rates 7. Surgical modalities such as thrombectomy, bypass, reconstruction/replacement, and ligation are used as a last resort due to the high invasive and significant intervention nature 16.
If the stent placing is not advisable, placing inferior vena cava filters can alleviate symptoms for some time 32. Recently, the use of inferior vena cava filters has increased, especially in advanced-stage cancer patients, in order to prevent the pulmonary embolus, although there is no explicit evidence of improved survival rate 55. Temporary inferior vena cava filters are usually used in cancer patients during systemic chemotherapy 56.
If lesions are due to non-thrombotic causes such as cancer, then the treatment is directed to manage the underlying cause of the compression. This may include surgery, chemotherapy, radiation, or combination. Surgery to remove the tumor is a surgical option to remove tumor compression. However, resection is not possible to be done in unstable patients, thus, palliative care is provided. Another option is to place an intravascular stent or surgical bypass grafting, which increases the patency of the inferior vena cava (IVC) to alleviate symptoms 57. Recanalization of the occluded veins is usually done by implanting the metallic stents into the inferior vena cava (IVC) from the superior vena cava (SVC) via the right atrium 58.
Inferior vena cava syndrome (IVCS) patients with intrahepatic obstruction due to advanced cancer causing metastatic liver involvement and enlarged liver (hepatomegaly) are usually treated using strip radiotherapy to the intrahepatic inferior vena cava (IVC), with or without a hepatic arterial infusion of chemotherapy 59. The IVC obstruction is generally managed by crossing the tumorous lesion with either a guidewire or Brockenbrough needle along with a Mullins sheath assembly, and then a balloon dilatation was done with the help of Inoue or Mansfield balloon 60.
In some mild compression causes like pregnancy, physical maneuvers such as simply placing the patient in the left lateral position, therefore, shifting the uterus to the left, and removing pressure of the gravid uterus away from the the inferior vena cava can be applied 33.
Inferior vena cava syndrome prognosis
Prognosis of inferior vena cava syndrome (IVCS) depends on the underlying condition that initially caused the inferior vena cava obstruction, including the hemodynamic status of the patient, the severity of compression or vein obstruction, the stage of the cancer, and previous comorbidities 7. The prognosis (outcome) of patients who have inferior vena cava thrombosis (blood clot) overall relates to the embolic risk associated with deep vein thrombosis (DVT). If the inferior vena cava (IVC) is occluded, pulmonary embolism does not present a significant risk. However, if the inferior vena cava (IVC) lumen remains, embolization may occur.
Generally speaking, the impact and outcome (prognosis) of inferior vena cava syndrome (IVCS) or inferior vena cava obstruction (IVCO) are as variable as the clinical presentation 61. In one study, only one third of patients had a correct diagnosis before venography. Adult patients with ligation (surgical procedure that tie a blood vessel to shut it off) of their inferior vena cava reportedly have either no symptoms or mild edema after ligation 62.
A report on children who had inferior vena cava thrombosis (IVCT) unrelated to catheterization revealed that 50% had persistent inferior vena cava thrombosis (IVCT) 61. Symptoms of chronic limb pain and chronic abdominal pain were observed. Another series of pediatric patients with inferior vena cava thrombosis (IVCT) secondary to central venous access identified no complications unless concurrent superior vena cava thrombosis was present 61.
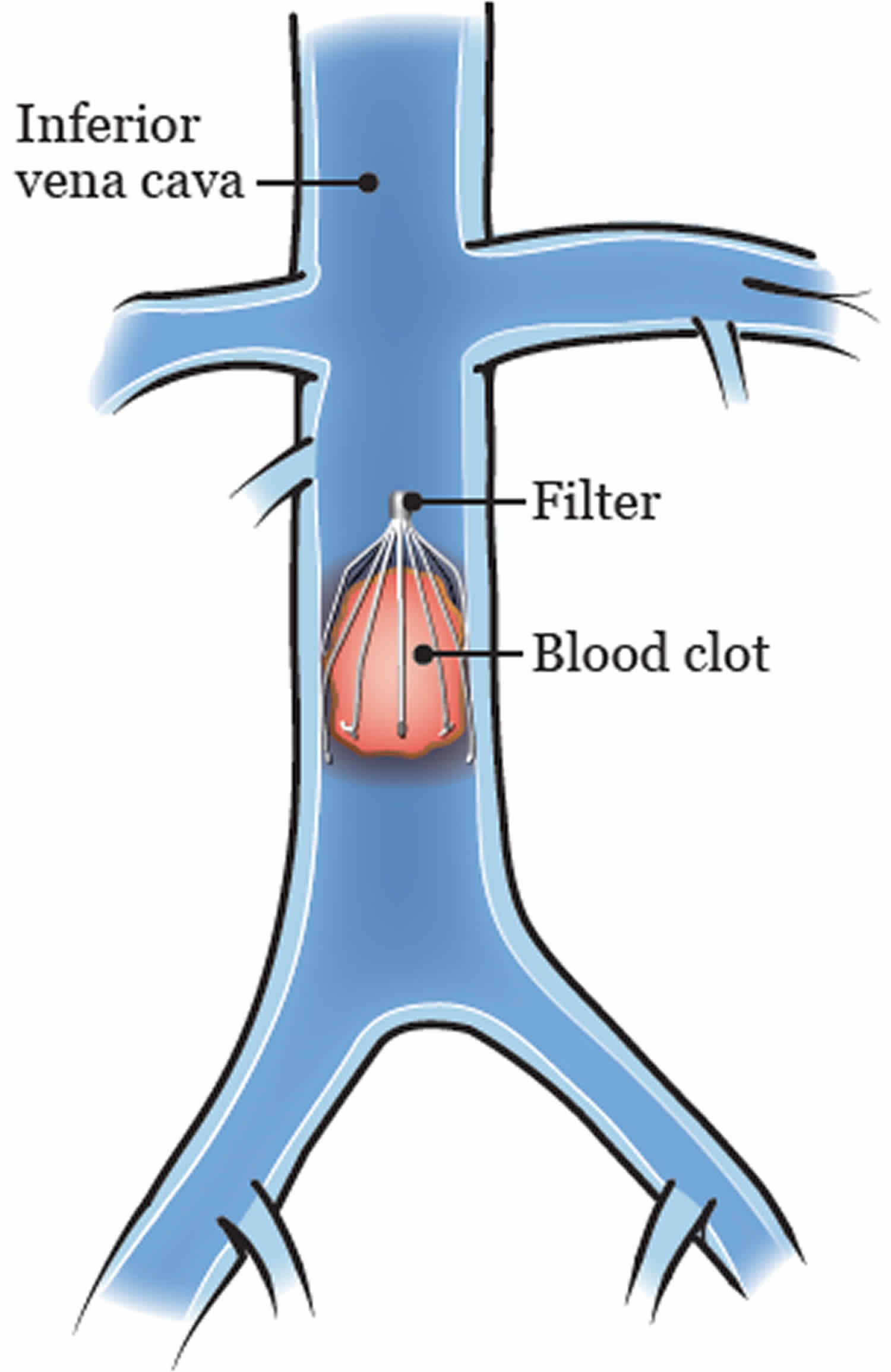
Inferior vena cava filter
An inferior vena cava filter is a small device that is placed in your inferior vena cava to prevent blood clots from moving through your blood into your lungs (pulmonary embolus) (see Figure 3). Although there is some controversy over inferior vena cava filter indications, recurrent deep venous thromboses and consequent pulmonary emboli refractory to treatment with anticoagulation may require placement of an inferior vena cava filter 63. Certain institutions also advocate for inferior vena cava filter placement for high risk trauma patients (even without documented clot). Inferior vena cava filters may be permanent or retrivable, although data suggests that only a fraction of the retrievable filters are later removed. Anatomic variations from the norm require careful attention to detail and understanding of their manifestations and potential complications during procedures. A pulmonary embolus is a blockage in the main artery of a lung. Inferior vena cava filters can be used to prevent or manage pulmonary emboli and deep vein thrombosis (DVT), and can be temporary or permanent. The shape of an inferior vena cava filter resembles that of an umbrella, and it functions in a similar way.
Your inferior vena cava filter will be placed by your interventional radiologist or vascular surgeon or cardiologist 64. An interventional radiologist is a doctor who specializes in image-guided procedures. The interventional radiologist will insert a 3 mm plastic tube (called a sheath) by going through a vein in your neck or groin. Your doctor will position the filter in the vein using a fluoroscopy (real-time x-rays). Your doctor will guide the sheath to the blood clot in the inferior cava vein, which is where the inferior vena cava filter will be placed.
The procedure will take about 30 minutes, but you should expect to be in the procedure room for about an hour. You will have a follow-up appointment 4 to 6 weeks after placement to see when your inferior vena cava filter can be removed.
If you receive a temporary inferior vena cava filter, the interventional radiologist will remove the filter after the necessary period of time has passed. To remove the inferior vena cava filter, the interventional radiologist will insert a long plastic tube and a goose-neck system (like a miniature lasso) as before and use this to remove the inferior vena cava filter.
Figure 3. Inferior vena cava filter
Inferior vena cava filter indications
There are a number of treatments available to manage or prevent pulmonary emboli and DVT, including conservative (medical) therapy, inferior vena cava filters, intravenous systemic thrombolysis, catheter thrombolysis and a surgical operation.
Your suitability for this treatment depends on a number of factors, including how stable your blood pressure is and how well your heart is working. Other factors which will be taken into consideration are the type of inferior vena cava filter and your clinical situation, as permanent placement means you will need to take medication to prevent blood clotting for the rest of your life.
People who have a new deep vein thrombosis (DVT) in the large veins of the pelvis or thigh and are not able to safely take blood thinners because of current major bleeding or a high risk of bleeding should have an IVC filter inserted. Once it is safe to start blood thinners, after a few days or weeks, the filter should be removed.
There are a number of situations in which IVC filter placement is sometimes considered by physicians. However, it is less clear whether they really should be placed in these situations. Because filters by themselves, being foreign bodies in the vascular system, increase the risk for deep vein thrombosis (DVT) and because they can lead to the complications discussed above, the risk of placing a IVC filter in these situation may be higher than the potential benefit 64:
- Trauma: People who sustain a trauma, especially if it will require them to be immobilized for long periods of time, are at a higher risk of developing a blood clot. Many of these patients also cannot use blood thinners to prevent blood clots because of a high risk of bleeding or the need for surgery. It is unclear whether trauma patients should get an IVC filter if they do not have a new blood clot, but most probably should not.
- Orthopedic surgery: People undergoing orthopedic surgeries (hip or knee replacement; major pelvic, leg, or back surgeries) have a higher risk of blood clots. Most patients should be on blood thinners after surgery to prevent blood clots from forming. It is unclear whether people at high risk for blood clots should have an IVC filter in addition to using a blood thinner, but most probably should not.
- Pregnancy: Patients who are pregnant are at increased risk for blood clots as a result of increased estrogen levels and pressure of the pregnant uterus onto the big veins in the pelvis. It is not clear whether pregnant women at particularly high risk for deep vein thrombosis (DVT) should get a filter. The pressure of the overlying pregnant uterus can potentially damage filters. There are likely few, if any, situations in which a filter is needed and beneficial.
- Weight loss surgery (bariatric surgery): People undergoing obesity surgery are at increased risk of blood clots because of the surgery and the obesity itself. Small studies show that placing an IVC filter before surgery in a person who does not have a blood clot does not decrease the risk of a pulmonary embolism (PE) after surgery.
- Recurrent deep vein thrombosis (recurrent DVT): Although filters are sometimes considered in patients who have a second (recurrent) deep vein thrombosis (DVT) despite having been on blood thinners, that is, patients with anticoagulant failure, no data exist that filters in this situation are beneficial.
- Severe lung or heart disease: In patients with severe lung or heart disease, even a small to medium-sized PE can be detrimental. If such patients have a deep vein thrombosis (DVT), filters are sometimes considered to protect the lung from clots.
- Clot busters or mechanical deep vein thrombosis (DVT) removal (thrombectomy): Deep vein thrombosis (DVTs) are sometimes treated with strong clot-dissolving medications, called clot busters or fibrinolytic drugs, or by putting a catheter into the clot and sucking it out, referred to as mechanical thrombectomy. Because of a concern that parts of the clot may break loose during the procedure, an IVC filter is sometimes placed temporarily.
The American College of Chest Physicians 65 and the Society of Interventional Radiology 66 recommend that IVC filters be placed in someone with a known DVT in the pelvis or thigh who cannot be on blood thinners because of bleeding. Other guidelines, recommend the placement of retrievable (temporary) inferior vena cava filters whenever reversible contraindications to anticoagulation are present 67. These contraindications include recent hemorrhage, surgery, major trauma, etc.). Other circumstances include embolic prophylaxis during the mechanical removal of a thrombus, and in the setting of a massive or submassive pulmonary embolus. In each of these cases, the filter may be retrieved after anticoagulation is resumed. Alternatively, permanent filters may be deployed in individuals who are not anticipated to be candidates for systemic anticoagulation. Occasionally, patients with reversible contraindications to anticoagulation will not have their temporary inferior vena cava filter retrieved and it will become permanent. Regardless of the indication for placement.
The following additional recommendation have been made:
- The American College of Chest Physicians recommends that people do not get an IVC filter if they are able to use blood thinner medications 65.
- The Society of Interventional Radiology recommends IVC filters in patients who have a new or worsening clot while on blood thinners, whereas the American College of Chest Physicians does not recommend an IVC filter in this situation 65, 66. The Society of Interventional Radiology also recommends an IVC filter in people with a large pulmonary embolism (PE) who still have evidence of a DVT 66. In addition, the Society of Interventional Radiology recommends an IVC filter in patients with DVT who have severe heart or lung disease 66.
- Recognizing the potential side effects of IVC filters, the US Food and Drug Administration (FDA) recommends that IVC filters be considered for removal as soon as protection from pulmonary embolism (PE) is no longer needed 68.
In summary, patients with inferior vena cava filters (IVC filters) – particularly permanent filters – are at increased risk for recurrent deep vein thrombosis (DVT). Judicious use of inferior vena cava filters, as well as prompt retrieval of inferior vena cava filters that are intended to be temporary, substantially reduces the risk of inferior vena cava thrombosis 67. IVC filters should generally be reserved for patients with a new, acute, fresh blood clot in the pelvis or thigh who cannot safely use blood thinner medications. How long to keep someone on blood thinners if an IVC filter is not removed depends on a number of factors, mostly the reasons why the DVT or PE formed in the first place.
Inferior vena cava filter risks
There are some minor risks, including infection and bruising at the puncture site in your neck or groin. Major risks include the filter moving to another part of your body, the development of another thrombus, or a leg of the inferior vena cava filter breaking through the wall of the vein, which can be painful.
If you have a permanent inferior vena cava filter, the medication preventing blood clots that you will need to take carries further risks.
After your inferior vena cava filter procedure
In the recovery room
You will be taken to the recovery room or hospital bed.
Your nurse will explain your discharge instructions to you and your caregiver before you go home. They will also give you a wallet card with information about your inferior vena cava filter to keep with you.
Wearing a seatbelt may put pressure on your incisions. You may want to place small pillow or folded towel between the strap and your body when you go home.
At home
Caring for yourself
- Leave the bandage on the insertion site for 24 hours. After 24 hours, you can take it off.
- Your incision may feel sore. This should get better within a day or 2. You can take over-the-counter pain medication, such as acetaminophen (Tylenol®) or ibuprofen (Advil®), if you need it.
- You can shower 24 hours after your procedure.
Activities
- For the first few days, you should avoid certain activities, such as exercises that involve stretching.
- You can still have a magnetic resonance imaging (MRI) while you have an inferior vena cava filter, but it’s important to tell the healthcare provider at the radiology facility each time to be safe. Show them the wallet card your nurse gave to you.
- Your inferior vena cava filter will not set off metal detectors.
Call your doctor if you have:
- A temperature of 100.4° F (38° C) or higher
- Pain around your insertion site that doesn’t go away after taking medication
- Drainage around the incision site
- Redness and swelling around your insertion site.
Do I need to stay on anticoagulation if I have an IVC filter?
Blood thinners should be restarted when the bleeding has resolved even if an IVC filter was placed. It is important to start anticoagulation as soon as possible because an IVC filter does not prevent the formation of new blood clots. Once a patient is safely on blood thinners, the filter should be removed. The duration of treatment with blood thinners depends on what caused the DVT or PE in the first place. Although people with an IVC filter are at a slightly higher risk for a clot in the future once blood thinners are stopped, most people should not continue taking anticoagulation just because an IVC filter is in place. How long to treat with a blood thinner is an individualized decision that should be discussed with your doctor.
How is an IVC filter removed?
A radiologist or vascular surgeon can remove a filter by inserting a catheter into one of the neck veins, the same way as when the filter was placed. The catheter hooks around a hook at the top of the filter, which can then be pulled out. This is typically an outpatient procedure. Removing a filter is most successful if attempted within 3 months of placement. The filter becomes more difficult to remove the longer it has been in because its feet (struts) become embedded in the wall of the IVC. Sometimes, filters cannot be removed, even within the first few months after their placement. Some radiologists or vascular surgeons feel comfortable removing the filter while the patient is on a blood thinner; others want the patient to discontinue the blood thinner before the removal.
- Petik B. Inferior vena cava anomalies and variations: imaging and rare clinical findings. Insights Imaging. 2015 Dec;6(6):631-9.[↩][↩]
- Piciucchi S, Barone D, Sanna S, Dubini A, Goodman LR, Oboldi D, Bertocco M, Ciccotosto C, Gavelli G, Carloni A, Poletti V. The azygos vein pathway: an overview from anatomical variations to pathological changes. Insights Imaging. 2014 Oct;5(5):619-28[↩][↩]
- Heistad DD, Armstrong ML, Amundsen S. Blood flow through vasa vasorum in arteries and veins: effects of luminal PO2. Am. J. Physiol. 1986 Mar;250(3 Pt 2):H434-42[↩]
- Nakazato Y, Ohga A, Shigei T, Uematsu T. Extrinsic innervation of the canine abdominal vena cava and the origin of cholinergic vasoconstrictor nerves. J. Physiol. (Lond.). 1982 Jul;328:191-203[↩][↩]
- Paddock M, Robson N. The curious case of the disappearing IVC: a case report and review of the aetiology of inferior vena cava agenesis. J Radiol Case Rep. 2014 Apr;8(4):38-47[↩]
- Klein-Weigel PF, Elitok S, Ruttloff A, Reinhold S, Nielitz J, Steindl J, Lutfi P, Rehmenklau-Bremer L, Hillner B, Fuchs H, Wrase C, Herold T, Beyer L. Inferior vena cava-syndrome. Vasa. 2021 Jul;50(4):250-264. https://www.vascular-medicine.org/wp-content/uploads/2021/08/Klein-Weigel_Editors-Pick.pdf[↩]
- Lawrensia S, Khan YS. Inferior Vena Cava Syndrome. [Updated 2023 May 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560885[↩][↩][↩][↩][↩][↩][↩]
- Joshi A, Law J, Shah N, Ghnaima H, Akanbi M, Tikaria R. Superior and inferior vena cava syndrome caused by a rare lung cancer: A case report. Clin Case Rep. 2024 Aug 30;12(9):e9391. doi: 10.1002/ccr3.9391[↩]
- Murakami N, Arai Y, Takagawa Y, Okuma K, Takahashi K, Inaba K, Igaki H, Nakayama Y, Itami J. Inferior vena cava syndrome caused by retroperitoneal fibrosis after pelvic irradiation: A case report. Gynecol Oncol Rep. 2018 Dec 4;27:19-21. doi: 10.1016/j.gore.2018.12.002[↩]
- Morita S, Sugawara S, Suda T, Prasetyo D, Kobayashi Y, Hoshi T, Abe S, Yagi K, Terai S. Stent Placement for Malignant Inferior Vena Cava Syndrome in a Patient with Recurrent Colon Cancer. Intern Med. 2020 Nov 15;59(22):2885-2890. doi: 10.2169/internalmedicine.5033-20[↩]
- Lofroth J, Pourghadiri A, Hadjivassiliou A, Heran M, Legiehn G, Ho S, Dhatt R. Total Iliocaval Reconstruction in a Complex Palliative Patient with Malignant Inferior Vena Cava Syndrome. Curr Oncol. 2024 Jul 9;31(7):3978-3984. doi: 10.3390/curroncol31070294[↩]
- Gantes Padrão T, Casimiro M, Gaspar A, Raimundo A. Inferior Vena Cava Syndrome: A Rare Complication. Eur J Case Rep Intern Med. 2020 Oct 15;7(12):001628. doi: 10.12890/2020_001628[↩]
- Tesemma A, Adane M, Bekele K, Debebe B, Rosso E, Zenbaba D, Gomora D, Beressa G. Giant pedunculated liver hydatid cyst causing inferior vena cava syndrome: a case report. J Med Case Rep. 2024 Oct 7;18(1):464. doi: 10.1186/s13256-024-04772-0[↩]
- Makusha LP, Kulon M, Pucar D, Young CR. Inferior vena cava syndrome on skeletal scintigraphy secondary to metastatic prostate cancer. World J Nucl Med. 2020 Jul 2;19(3):324-326. doi: 10.4103/wjnm.WJNM_53_19[↩][↩]
- Wei W, Gong C, Wei R, Luo X, Liu Y, Chen G, Ran R, Liu F. Metastatic prostate cancer presenting as generalized lymphadenopathy and progressing with inferior vena cava syndrome: A case report and literature review. Oncol Lett. 2024 Sep 19;28(6):557. doi: 10.3892/ol.2024.14690[↩]
- McAree BJ, O’Donnell ME, Fitzmaurice GJ, Reid JA, Spence RA, Lee B. Inferior vena cava thrombosis: a review of current practice. Vasc Med. 2013 Feb;18(1):32-43. doi: 10.1177/1358863X12471967[↩][↩][↩][↩][↩][↩][↩][↩]
- Sonin AH, Mazer MJ, Powers TA. Obstruction of the inferior vena cava: a multiple-modality demonstration of causes, manifestations, and collateral pathways. Radiographics. 1992 Mar;12(2):309-22. doi: 10.1148/radiographics.12.2.1561419[↩]
- Missal ME, Robinson JA, Tatum W. Inferior vena cava obstruction: clinical manifestations, diagnostic methods, and related problems. Ann Intern Med. 1965;62:133–61. doi: 10.7326/0003-4819-62-1-133[↩]
- Kasimis BS, Spiers AS. Inferior vena cava obstruction. A complication of prostate cancer. Arch Intern Med. 1979;139:1056–1057. doi: 10.1001/archinte.1979.03630460086026[↩]
- Harris R.D. The etiology of inferior vena caval obstruction and compression. CRC Crit. Rev. Clin. Radiol. Nucl. Med. 1976;8(1):57–86[↩]
- Murakami N, Arai Y, Takagawa Y, et al. Inferior vena cava syndrome caused by retroperitoneal fibrosis after pelvic irradiation: A case report. Gynecol Oncol Rep. 2018;27:19–21. Published 2018 Dec 4. doi:10.1016/j.gore.2018.12.002 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6289939[↩]
- Raju S, Hollis K, Neglen P. Obstructive lesions of the inferior vena cava: clinical features and endovenous treatment. J Vasc Surg. 2006 Oct;44(4):820-7. doi: 10.1016/j.jvs.2006.05.054[↩][↩]
- Mohammed M., Elhamdani S., Abusnina W., Majdi A., Yousef S. Inferior vena cava obstruction and shock. J. Emerg. Trauma Shock. 2018;11(2):146–148.[↩]
- Inferior Vena Caval Thrombosis Clinical Presentation. https://emedicine.medscape.com/article/1933035-clinical#b3[↩][↩]
- Giordano P, Weber K, Davis M, Carter E. Acute thrombosis of the inferior vena cava. Am J Emerg Med. 2006 Sep;24(5):640-2. doi: 10.1016/j.ajem.2005.12.018[↩]
- Armstrong B.A., Perez C.A., Simpson J.R., Hederman M.A. Role of irradiation in the management of superior vena cava syndrome. Int. J. Radiat. Oncol. Biol. Phys. 1987;13(4):531–539[↩]
- Takeuchi Y., Arai Y., Sone M., Sugawara S., Aramaki T., Sato R., Kichikawa K., Tanaka T., Morishita H., Ito T. Evaluation of stent placement for vena cava syndrome: phase II trial and phase III randomized controlled trial. Support Care Cancer. 2018[↩]
- Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH Jr. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000 May-Jun;20(3):639-52. doi: 10.1148/radiographics.20.3.g00ma09639[↩]
- Beck AD. Renal cell carcinoma involving the inferior vena cava: radiologic evaluation and surgical management. J Urol. 1977 Oct;118(4):533-7. doi: 10.1016/s0022-5347(17)58098-2[↩]
- Patel SA. The inferior vena cava (IVC) syndrome as the initial manifestation of newly diagnosed gastric adenocarcinoma: a case report. J Med Case Rep. 2015 Sep 28;9:204. doi: 10.1186/s13256-015-0696-3[↩][↩]
- Goto T, Yamasaki T, Kawashima R, Koide T, Yasuda T, Sendo H, Muramatsu S, Miyashita M, Ku Y. [A Case of Pancreatic Adenocarcinoma with Inferior Vena Cava Invasion]. Gan To Kagaku Ryoho. 2020 Apr;47(4):634-636. Japanese.[↩][↩]
- Sauter A, Triller J, Schmidt F, Kickuth R. Treatment of superior vena cava (SVC) syndrome and inferior vena cava (IVC) thrombosis in a patient with colorectal cancer: combination of SVC stenting and IVC filter placement to palliate symptoms and pave the way for port implantation. Cardiovasc Intervent Radiol. 2008 Jul;31 Suppl 2:S144-8. doi: 10.1007/s00270-007-9113-7[↩][↩]
- Krywko DM, King KC. Aortocaval Compression Syndrome. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430759[↩][↩][↩]
- Linicus Y, Kindermann I, Cremers B, Maack C, Schirmer S, Böhm M. Vena cava compression syndrome in patients with obesity presenting with edema and thrombosis. Obesity (Silver Spring). 2016 Aug;24(8):1648-52. doi: 10.1002/oby.21506[↩]
- Taheri SA, Williams J, Powell S, Cullen J, Peer R, Nowakowski P, Boman L, Pisano S. Iliocaval compression syndrome. Am J Surg. 1987 Aug;154(2):169-72. doi: 10.1016/0002-9610(87)90172-3[↩][↩]
- Liddell RP, Evans NS. May-Thurner syndrome. Vasc Med. 2018 Oct;23(5):493-496. doi: 10.1177/1358863X18794276[↩][↩]
- DeLeve LD, Valla DC, Garcia-Tsao G; American Association for the Study Liver Diseases. Vascular disorders of the liver. Hepatology. 2009 May;49(5):1729-64. doi: 10.1002/hep.22772[↩]
- Van Ha TG, Tullius TG Jr, Navuluri R, Millis JM, Leef JA. Percutaneous treatment of IVC obstruction due to post-resection hepatic torsion associated with IVC thrombosis. CVIR Endovasc. 2019 Apr 25;2(1):14. doi: 10.1186/s42155-019-0056-2[↩]
- Ishikura Y, Shimazu A, Odagiri S, Yoshimatsu H, Kadoya C, Okuma R. [A case of inferior vena cava thrombosis associated with cholelithiasis demonstrated by ultrasonic examination]. Nihon Geka Gakkai Zasshi. 1986 Jul;87(7):813-7. Japanese.[↩]
- Fontaine E, Garneau G, Lemieux S. Management of retroperitoneal hemorrhage compressing the inferior vena cava in a patient with a renal transplant: A case report. Radiol Case Rep. 2020 Jan 8;15(3):241-245. doi: 10.1016/j.radcr.2019.12.003[↩]
- Shrestha SM, Kage M, Lee BB. Hepatic vena cava syndrome: New concept of pathogenesis. Hepatol Res. 2017 Jun;47(7):603-615. doi: 10.1111/hepr.12869[↩]
- Mulvihill SJ, Fonkalsrud EW. Complications of superior versus inferior vena cava occlusion in infants receiving central total parenteral nutrition. J Pediatr Surg. 1984 Dec;19(6):752-7. doi: 10.1016/s0022-3468(84)80363-2[↩]
- Lier H, Bernhard M, Hossfeld B. Hypovolämisch-hämorrhagischer Schock [Hypovolemic and hemorrhagic shock]. Anaesthesist. 2018 Mar;67(3):225-244. German. doi: 10.1007/s00101-018-0411-z[↩][↩]
- Kushner A, West WP, Khan Suheb MZ, et al. Virchow Triad. [Updated 2024 Jun 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539697[↩][↩]
- Inferior Vena Caval Thrombosis Clinical Presentation. https://emedicine.medscape.com/article/1933035-clinical[↩]
- Alkhouli M, Morad M, Narins CR, Raza F, Bashir R. Inferior vena cava thrombosis. JACC Cardiovasc Interv. 2016;9(7):629–643. doi: 10.1016/j.jcin.2015.12.268[↩]
- Sharma V, McGuire BB, Nadler RB. Implications of a 5-liter urinary bladder: inferior vena cava syndrome leading to bilateral pulmonary artery emboli. Urology. 2014 Jun;83(6):e11-2. doi: 10.1016/j.urology.2014.02.025[↩]
- Post-Thrombotic Syndrome. https://my.clevelandclinic.org/health/diseases/24936-post-thrombotic-syndrome[↩]
- Ueda J, Hara K, Kobayashi Y, Ohue S, Uchida H. Anomaly of the inferior vena cava observed by CT. Comput Radiol. 1983 May-Jun;7(3):145-54. doi: 10.1016/0730-4862(83)90089-6[↩][↩]
- Inferior Vena Caval Thrombosis Workup. https://emedicine.medscape.com/article/1933035-workup#c2[↩]
- Gayer G, Luboshitz J, Hertz M, Zissin R, Thaler M, Lubetsky A, Bass A, Korat A, Apter S. Congenital anomalies of the inferior vena cava revealed on CT in patients with deep vein thrombosis. AJR Am J Roentgenol. 2003 Mar;180(3):729-32. doi: 10.2214/ajr.180.3.1800729[↩][↩][↩]
- Cho BC, Choi HJ, Kang SM, Chang J, Lee SM, Yang DG, Hong YK, Lee DH, Lee YW, Kim SK. Congenital absence of inferior vena cava as a rare cause of pulmonary thromboembolism. Yonsei Med J. 2004 Oct 31;45(5):947-51. doi: 10.3349/ymj.2004.45.5.947[↩]
- D’Aloia A, Faggiano P, Fiorina C, Vizzardi E, Bontempi L, Grazioli L, Dei Cas L. Absence of inferior vena cava as a rare cause of deep venous thrombosis complicated by liver and lung embolism. Int J Cardiol. 2003 Apr;88(2-3):327-9. doi: 10.1016/s0167-5273(02)00404-7[↩]
- Takehara N, Hasebe N, Enomoto S, Takeuchi T, Takahashi F, Ota T, Kawamura Y, Kikuchi K. Multiple and recurrent systemic thrombotic events associated with congenital anomaly of inferior vena cava. J Thromb Thrombolysis. 2005 Apr;19(2):101-3. doi: 10.1007/s11239-005-1380-z[↩]
- Schunn C, Schunn GB, Hobbs G, Vona-Davis LC, Waheed U. Inferior vena cava filter placement in late-stage cancer. Vasc Endovascular Surg. 2006 Aug-Sep;40(4):287-94. doi: 10.1177/1538574406291821[↩]
- Masui S, Onishi T, Arima K, Sugimura Y. Successful management of inferior vena cava thrombus complicating advanced germ cell testicular tumor with temporary inferior vena cava filter. Int J Urol. 2005 May;12(5):513-5. doi: 10.1111/j.1442-2042.2005.01073.x[↩]
- Gong ZH, Yan LJ, Sun JG. Postoperative radiotherapy to stabilize a tumor embolus in clear cell renal cell carcinoma: A case report. Oncol Lett. 2014 Oct;8(4):1856-1858. doi: 10.3892/ol.2014.2421[↩]
- Sato Y, Inaba Y, Yamaura H, Takaki H, Arai Y. Malignant inferior vena cava syndrome and congestive hepatic failure treated by venous stent placement. J Vasc Interv Radiol. 2012 Oct;23(10):1377-80. doi: 10.1016/j.jvir.2012.06.035[↩]
- Hartley JW, Awrich AE, Wong J, Stevens K, Fletcher WS. Diagnosis and treatment of the inferior vena cava syndrome in advanced malignant disease. Am J Surg. 1986 Jul;152(1):70-4. doi: 10.1016/0002-9610(86)90145-5[↩]
- Srinivas BC, Dattatreya PV, Srinivasa KH, Prabhavathi, Manjunath CN. Inferior vena cava obstruction: long-term results of endovascular management. Indian Heart J. 2012 Mar-Apr;64(2):162-9. doi: 10.1016/S0019-4832(12)60054-6[↩]
- Inferior Vena Caval Thrombosis Prognosis. https://emedicine.medscape.com/article/1933035-overview#a8[↩][↩][↩]
- Perhoniemi V, Salmenkivi K, Vorne M. Venous haemodynamics in the legs after ligation of the inferior vena cava. Acta Chir Scand. 1986 Jan;152:23-7.[↩]
- Congenital absence of inferior vena cava as a rare cause of pulmonary thromboembolism. Cho BC, Choi HJ, Kang SM, Chang J, Lee SM, Yang DG, Hong YK, Lee DH, Lee YW, Kim SK. Yonsei Med J. 2004 Oct 31; 45(5):947-51.[↩]
- Carroll S, Moll S. Inferior Vena Cava Filters, May-Thurner Syndrome, and Vein Stents. Circulation. 2016 Feb 9;133(6):e383-7. doi: 10.1161/CIRCULATIONAHA.115.019944[↩][↩]
- Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, Nelson ME, Wells PS, Gould MK, Dentali F, Crowther M, Kahn SR. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e419S-e496S. doi: 10.1378/chest.11-2301. Erratum in: Chest. 2012 Dec;142(6):1698-1704[↩][↩][↩]
- Caplin DM, Nikolic B, Kalva SP, Ganguli S, Saad WE, Zuckerman DA; Society of Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for the performance of inferior vena cava filter placement for the prevention of pulmonary embolism. J Vasc Interv Radiol. 2011 Nov;22(11):1499-506. doi: 10.1016/j.jvir.2011.07.012[↩][↩][↩][↩]
- Byrne M, Mannis GN, Nair J, Andreadis C. Inferior vena cava filter thrombosis. Clin Case Rep. 2015;4(2):162–164. Published 2015 Dec 16. doi:10.1002/ccr3.418 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4736520[↩][↩]
- Safety Communications. https://www.fda.gov/medical-devices/medical-device-safety/safety-communications[↩]
{kind=link}