Contents
- What is brain cancer
- The Brain
- Parts of the brain
- Brain cancer survival rate
- Types of brain cancer and spinal cord tumors in Adults
- What causes brain cancer in Adults
- Signs and Symptoms of Adult Brain and Spinal Cord Tumors
- How is Brain and Spinal Cord Cancers Diagnosed – Adults
- Brain cancer treatment in Adults
- Types of brain cancer in Children
- Gliomas
- Astrocytomas
- Oligodendrogliomas
- Ependymomas
- Mixed gliomas
- Brain stem gliomas
- Primitive neuroectodermal tumors (PNETs)
- Craniopharyngiomas
- Mixed glial and neuronal tumors
- Choroid plexus tumors
- Schwannomas (neurilemmomas)
- Other tumors that start in or near the brain
- Cancers that spread to the brain from other sites
- Survival rates for more common childhood brain and spinal cord tumors
- What causes brain cancer in Children
What is brain cancer
A brain cancer or malignant brain tumor, is a mass or growth of abnormal cells in your brain or close to your brain – that have grown out of control 1. A brain cancer (malignant brain tumor) is a fast-growing cancer that spreads to other areas of the brain and spine. The main concerns with brain and spinal cord cancer are how readily they spread through the rest of the brain or spinal cord and whether they can be removed and not come back.
Brain and spinal cord tumors tend to be different in adults and children. They often form in different areas, develop from different cell types, and may have a different outlook and treatment.
Brain cancers can egin in your brain (primary brain tumors), or cancer can begin in other parts of your body and spread to your brain (secondary, or metastatic, brain tumors).
The American Cancer Society’s estimates for brain and spinal cord tumors in the United States for 2017 include both adults and children.
- About 23,800 malignant tumors of the brain or spinal cord (13,450 in males and 10,350 in females) will be diagnosed. These numbers would be much higher if benign tumors were also included.
- About 16,700 people (9,620 males and 7,080 females) will die from brain and spinal cord tumors.
Overall, the chance that a person will develop a malignant tumor of the brain or spinal cord in his or her lifetime is less than 1%. The risk for men (about 1 in 140) is slightly higher than that for women (about 1 in 190), although certain types of tumors are more common in women.
Brain and spinal cord tumors are the second most common cancers in children (after leukemia). They account for about 1 out of 4 childhood cancers. More than 4,000 central nervous system tumors are diagnosed each year in children and teens. The incidence rate (number of tumors per 100,000 children) has not changed much in recent years.
Boys develop these tumors slightly more often than girls.
About 3 out of 4 children with brain tumors (all types combined) survive at least 5 years after being diagnosed. The outlook can vary a great deal based on the type of tumor, where it is, and other factors.
Survival rates for some of the more common types of brain and spinal cord tumors are discussed towards the bottoms of this article in Survival rates for more common childhood brain and spinal cord tumors.
Survival rates for brain and spinal cord tumors vary widely, depending on the type of tumor (and other factors). Rates for some of the more common types of brain and spinal cord tumors are discussed in Survival Rates for Selected Adult Brain and Spinal Cord Tumors.
How quickly a brain tumor grows can vary greatly. The growth rate as well as location of a brain tumor determines how it will affect the function of your nervous system.
Generally, brain cancers (tumors) are graded from 1 to 4, according to their behavior, such as how fast they grow and how likely they are to grow back after treatment. A malignant brain tumor is either grade 3 or 4, whereas grade 1 or 2 tumors are usually classed as benign or non-cancerous.
Most malignant tumors are secondary cancers, which means they started in another part of the body and spread to the brain. Primary brain tumors are those that started in the brain.
Brain tumor treatment options depend on the type of brain tumor you have, as well as its size and location.
The Brain
To understand brain cancers, it helps to know about the normal structure and function of the central nervous system (CNS), which is the medical name for the brain and spinal cord.
The brain is the center of thought, feeling, memory, speech, vision, hearing, movement, and much more. The spinal cord and special nerves in the head called cranial nerves help carry messages between the brain and the rest of the body. These messages tell our muscles how to move, transmit information gathered by our senses, and help coordinate the functions of our internal organs.
The brain is protected by the skull. Likewise, the spinal cord is protected by the bones (vertebrae) of the spinal column.
The brain and spinal cord are surrounded and cushioned by a special liquid, called cerebrospinal fluid (CSF). Cerebrospinal fluid is made by the choroid plexus, which is found in spaces within the brain called ventricles. The ventricles and the spaces around the brain and spinal cord are filled with CSF.
Figure 1. Human brain
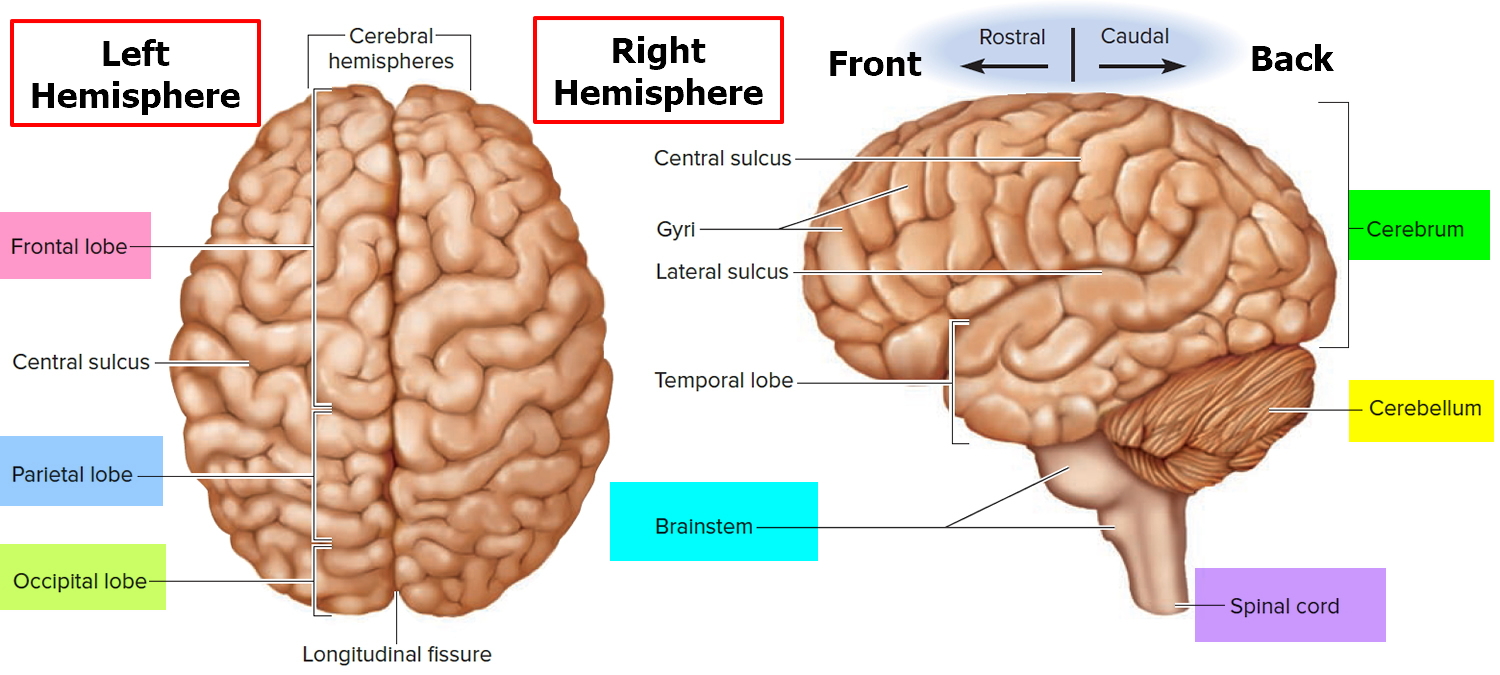
Figure 2. Medial aspect of the human brain
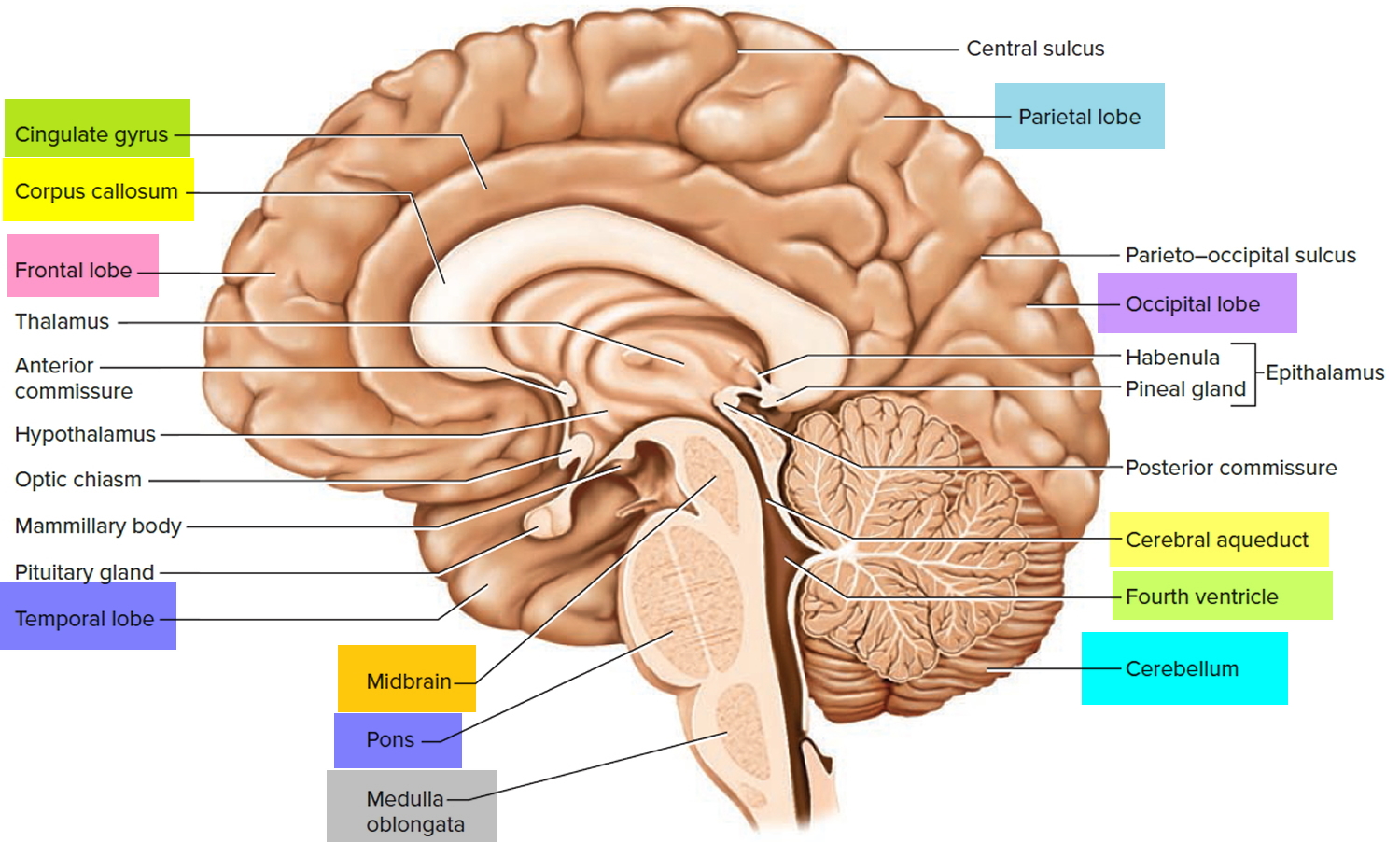
Figure 3. Diencephalon of the human brain
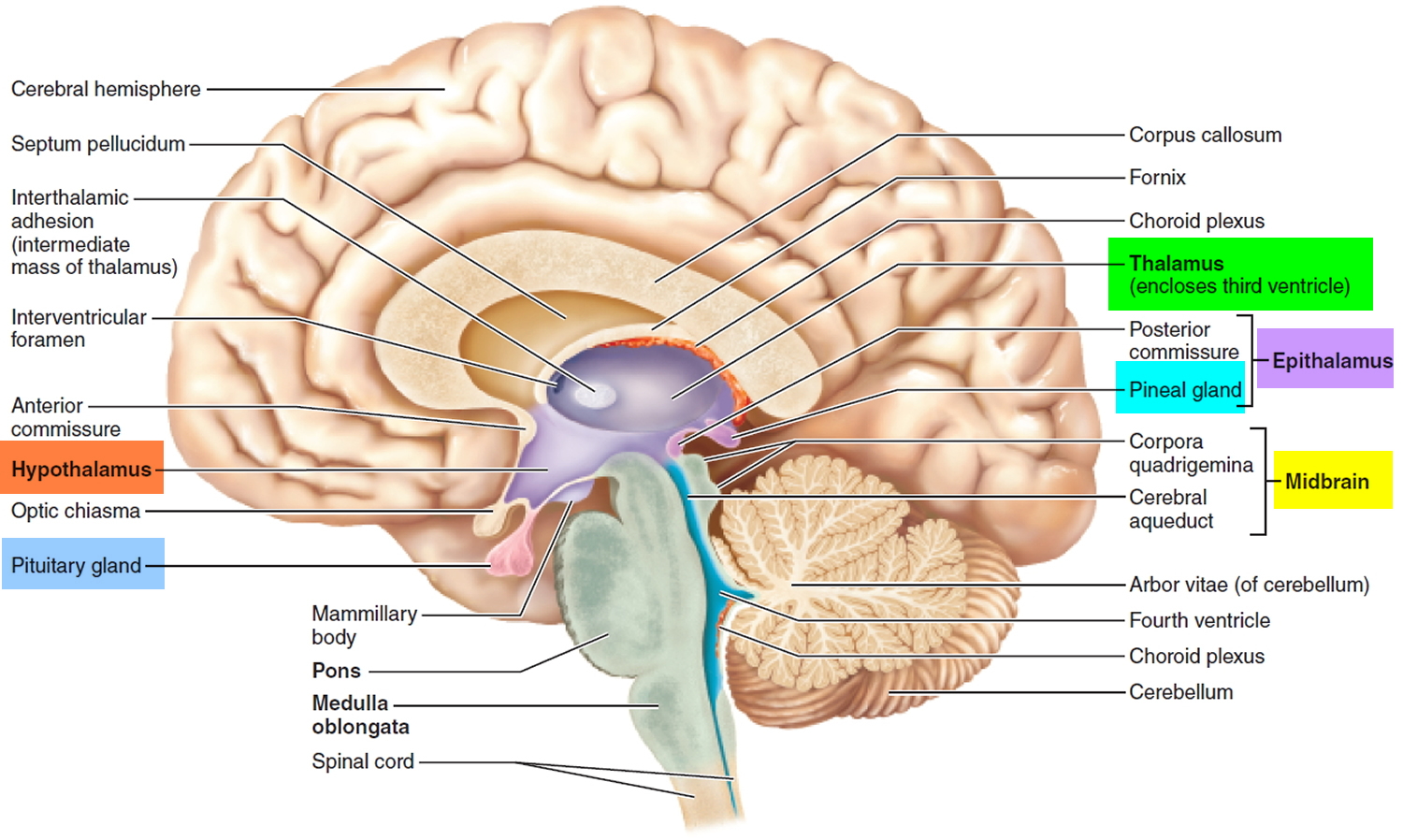
Figure 4. Spinal cord
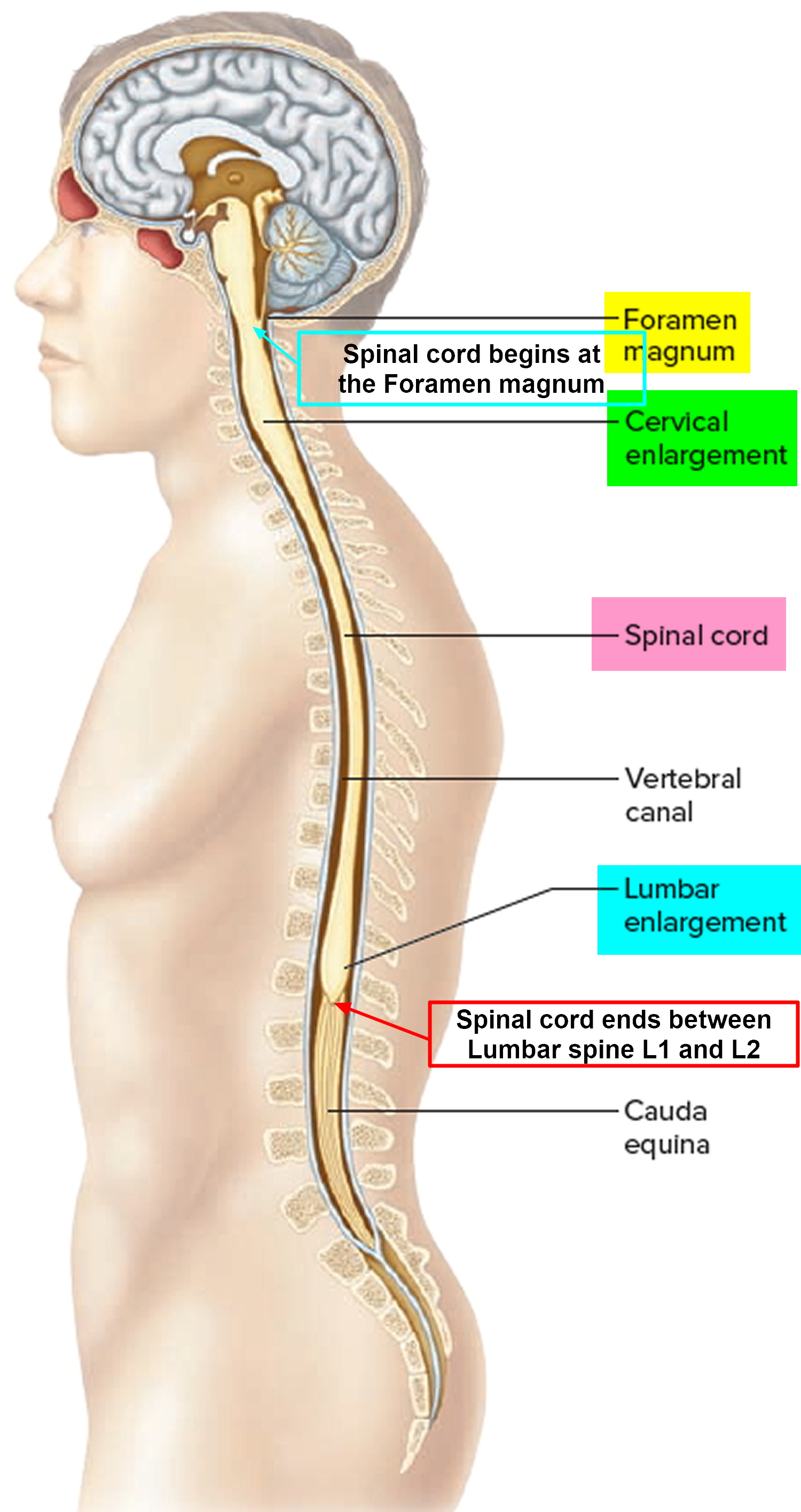
Figure 5. 12 Cranial nerves
 Parts of the brain
Parts of the brain
Anatomists conceptually divide the brain into four major parts. Each part has a special function.
- The Cerebrum.
- The Diencephalon (thalamus, hypothalamus, and epithalamus).
- The Cerebellum.
- The Brain stem.
Cerebrum
The cerebrum is the large, outer part of the brain. The cerebrum is about 83% of the brain’s volume and consists of a pair of half globes called the cerebral hemispheres. Each hemisphere is marked by thick folds called gyri (singular, gyrus) separated by shallow grooves called sulci (singular, sulcus). A very deep median groove, the longitudinal fissure, separates the right and left hemispheres from each other. At the bottom of this fissure, the hemispheres are connected by a thick bundle of nerve fibers called the corpus callosum—a prominent landmark for anatomical description with a distinctive C shape in sagittal section.
The Cerebral hemispheres control reasoning, thought, emotion, and language. It is also responsible for planned (voluntary) muscle movements (throwing a ball, walking, chewing, etc.) and for taking in and interpreting sensory information such as vision, hearing, smell, touch, and pain.
The symptoms caused by a tumor in a cerebral hemisphere depend on where the tumor is. Common symptoms include:
- Seizures
- Trouble speaking
- A change of mood such as depression
- A change in personality
- Weakness or paralysis in part of the body
- Changes in vision, hearing, or other senses
Cerebellum
The cerebellum occupies the posterior cranial fossa inferior to the cerebrum, separated from it by the transverse cerebral fissure. It is also marked by fissures, sulci, and gyri (called folia in the cerebellum). The cerebellum is the second-largest region of the brain, constituting about 10% of its volume but containing over 50% of its neurons.
The cerebellum lies under the cerebrum at the back part of the brain. It helps coordinate movement. Tumors of the cerebellum can cause problems with coordination in walking, trouble with precise movements of hands, arms, feet, and legs, problems swallowing or synchronizing eye movements, and changes in speech rhythm.
Brain stem
The brain stem is the lower part of the brain that connects to the spinal cord. It contains bundles of very long nerve fibers that carry signals controlling muscles and sensation or feeling between the cerebrum and the rest the body. Special centers in the brain stem also help control breathing and the beating of the heart. Also, most cranial nerves (see Figures 1 and 2 above) start in the brain stem.
Tumors in this critical area of the brain can cause weakness, stiff muscles, or problems with sensation, facial or eye movement, hearing, or swallowing. Double vision is a common early symptom of brain stem tumors, as are problems with coordination in walking. Because the brain stem is a small area that is so essential for life, it might not be possible to surgically remove tumors in this area.
The Diencephalon (thalamus, hypothalamus, and epithalamus)
Deep in the core area of the brain, just above the top of the brainstem, is the diencephalon that consists largely of three paired structures—the thalamus, the hypothalamus and the epithalamus. The diencephalon are structures that have a great deal to do with perception, movement, and the body’s vital functions.
The thalamus consists of two oval masses that contain about a dozen major nuclei, each of which sends axons to a particular portion of the cerebral cortex (Figure 3). The thalamic masses contain nerve cell bodies that sort information from four of the senses—sight, hearing, taste, and touch—and relay it to the cerebral cortex. (Only the sense of smell sends signals directly to the cortex, bypassing the thalamus.) Sensations of pain, temperature, and pressure are also relayed through the thalamus, as are the nerve impulses from the cerebral hemispheres that initiate voluntary movement.
Sensory inputs are not the only type of information relayed through the thalamus. Every part of the brain that communicates with the cerebral cortex must relay its signals through a nucleus of the thalamus. The thalamus can therefore be thought of as the “gateway” to the cerebral cortex.
The thalamus not only relays information to the cerebral cortex but also processes the information as it passes through.
The thalamic nuclei organize and then either amplify or “tone down” the signals headed for the cerebral cortex. This is why, for example, you can focus on a conversation with a single person in large, noisy cafeteria.
The hypothalamus (“below the thalamus”) is the inferior portion of the diencephalon. Projecting inferiorly from the hypothalamus is the pituitary gland (Figure 1) and the hypothalamus occupies approximately 2 per cent of the brain volume. The hypothalamus is situated in a strategic position at the crossroad of four systems, neurovegetative, neuroendocrine, limbic, and optic 2.
The hypothalamus forms the inferolateral walls of the third ventricle. On the underside of the brain, the hypothalamus lies between the optic chiasma (point of crossover of cranial nerves II, the optic nerves) and the posterior border of the mammillary bodies, rounded bumps that bulge from the hypothalamic floor (mammillary = “little breast”).
The hypothalamus, like the thalamus, contains about a dozen brain nuclei of gray matter. Despite its relatively small size (roughly that of a thumbnail or an almond), functionally, the hypothalamus is the main visceral control center of the body, regulating many activities of the visceral organs.
The hypothalamus is the main point of interaction for the body’s two physical control systems: the nervous system, which transmits information in the form of minute electrical impulses, and the endocrine system, which brings about changes of state through the release of chemical factors. It is the hypothalamus that first detects crucial changes in the body and responds by stimulating various glands and organs to release hormones.
Cranial nerves
The cranial nerves extend directly out of the base of the brain (as opposed to coming out of the spinal cord). These nerves carry signals directly between the brain and the face, eyes, tongue, mouth, and some other areas.
Tumors starting in cranial nerves can cause vision problems, trouble swallowing, hearing loss in one or both ears, or facial paralysis, numbness, or pain.
Spinal cord
The spinal cord has bundles of very long nerve fibers that carry signals that control muscles, sensation or feeling, and bladder and bowel control.
Spinal cord tumors can cause weakness, paralysis, or numbness. The spinal cord is a narrow structure, so tumors within it usually cause symptoms on both sides of the body (for example, weakness or numbness of both legs). This is different from most brain tumors, which often affect only one side of the body.
The nerves that reach the arms begin in the spinal cord at the level of the neck (cervical spine). Nerves that branch off the spinal cord to the legs, bowel, and bladder arise in the back (thoracic and lumbar spine). Most tumors of the spinal cord start in the neck and can cause symptoms in the arms and legs, as well as affect bowel and bladder function. Spinal cord tumors below the neck only affect the legs and bowel and bladder function.
Types of cells and body tissues in the brain and spinal cord
The brain and spinal cord have many kinds of tissues and cells, which can develop into different types of tumors.
Neurons (nerve cells): These are the cells in the brain that help determine thought, memory, emotion, speech, muscle movement, sensation, and just about everything else that the brain and spinal cord do. They do this by transmitting chemical and electrical signals through their nerve fibers (axons). Axons in the brain tend to be short, while those in the spinal cord can be as long as several feet.
Unlike many other types of cells that can grow and divide to repair damage from injury or disease, neurons in the brain and spinal cord largely stop dividing about a year after birth (with a few exceptions). Neurons do not usually form tumors, but they are often damaged by tumors that start nearby.
Glial cells: Glial cells are the supporting cells of the brain. Most brain and spinal cord tumors develop from glial cells. These tumors are sometimes referred to as gliomas.
There are 3 types of glial cells – astrocytes, oligodendrocytes, and ependymal cells. A fourth cell type called microglia is part of the immune system and is not truly a glial cell.
- Astrocytes help support and nourish neurons. When the brain is injured, astrocytes form scar tissue that helps repair the damage. The main tumors starting in these cells are called astrocytomas or glioblastomas.
- Oligodendrocytes make myelin, a fatty substance that surrounds and insulates the nerve cell axons of the brain and spinal cord. This helps neurons send electric signals through the axons. Tumors starting in these cells are called oligodendrogliomas.
- Ependymal cells line the ventricles (fluid-filled areas) within the brain and form part of the pathway through which CSF flows. Tumors starting in these cells are called ependymomas.
- Microglia are the immune (infection-fighting) cells of the central nervous system.
Neuroectodermal cells: These are very early forms of nervous system cells that are probably involved in brain cell development. They are found throughout the brain, although they are not often seen in the adult central nervous system. The most common tumors that come from these cells develop in the cerebellum and are called medulloblastomas.
Meninges: These are layers of tissue that line and protect the brain and spinal cord. CSF travels through spaces formed by the meninges. The most common tumors that start in these tissues are called meningiomas.
Choroid plexus: The choroid plexus is the area of the brain within the ventricles that makes CSF, which nourishes and protects the brain.
Pituitary gland and hypothalamus: The pituitary is a small gland at the base of the brain. It is connected to a part of the brain called the hypothalamus. Both make hormones that help regulate the activity of several other glands in the body. For example, they control the amount of thyroid hormone made by the thyroid gland, breast milk production and release, and the amount of male or female hormones made by the testicles or ovaries. They also make growth hormone, which stimulates body growth, and vasopressin, which regulates water balance by the kidneys.
The growth of tumors in or near the pituitary or hypothalamus, as well as surgery and/or radiation therapy in this area, can affect these functions. For example, tumors starting in the pituitary gland sometimes make too much of a certain hormone, which can cause problems. On the other hand, a person may have low levels of one or more hormones after treatment and may need to take hormones to make up for this.
Pineal gland: The pineal gland is not really part of the brain. It is a small endocrine gland that sits between the cerebral hemispheres. It makes melatonin, a hormone that regulates sleep, in response to changes in light. The most common tumors of the pineal gland are called pineoblastomas.
Blood-brain barrier: The inner lining of the small blood vessels (capillaries) in the brain and spinal cord creates a very selective barrier between the blood and the tissues of the central nervous system. This barrier normally helps maintain the brain’s metabolic balance and keeps harmful toxins from getting into the brain. Unfortunately, it also keeps out most chemotherapy drugs that are used to kill cancer cells, which in some cases limits their usefulness.
Figure 6. Glial (neuroglial) cells in the brain (astrocytes, oligodendrocytes, and microglial cells)
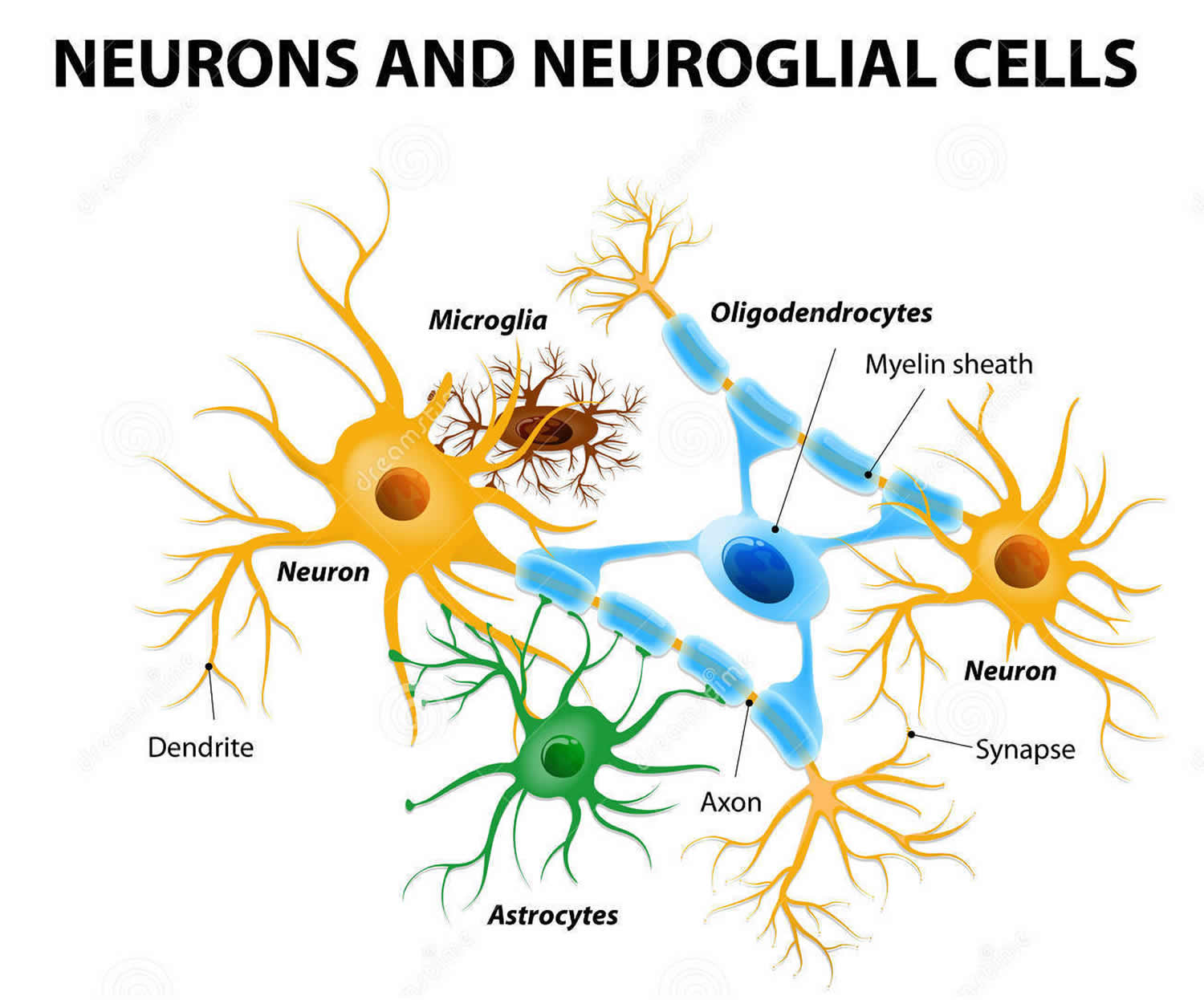
Note: Glial (Neuroglial) cells do not conduct nerve impulses, but, instead, support, nourish, and protect the neurons. Glial cells (glia) are far more numerous than neurons and, unlike neurons, are capable of mitosis. Glial roles that are well-established include maintaining the ionic milieu of nerve cells, modulating the rate of nerve signal propagation, modulating synaptic action by controlling the uptake of neurotransmitters, providing a scaffold for some aspects of neural development, and aiding in (or preventing, in some instances) recovery from neural injury 3.
Brain cancer survival rate
Survival rates are a way to get a general idea of the outlook (prognosis) for people with a certain type of tumor. They tell you what portion of people with the same type of tumor are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding about how likely it is that your treatment will be successful.
The 5-year survival rate is the percentage of people who live at least 5 years after being diagnosed. For example, a 5-year survival rate of 70% means that an estimated 70 out of 100 people who have that type of tumor are still alive 5 years after being diagnosed. Keep in mind, however, that many of these people live much longer than 5 years.
Relative survival rates (like the numbers below) are a more accurate way to estimate the effect of cancer on survival. These rates compare people with cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific type of tumor is 70%, it would mean that people who have that type of tumor are, on average, about 70% as likely as people who don’t have that tumor to live for at least 5 years after being diagnosed.
But remember, the 5-year relative survival rates are estimates – your outlook can vary based on a number of factors specific to you.
Survival rates don’t tell the whole story
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are some limitations to remember:
These numbers are among the most current available. But to get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. As treatments are improving over time, people who are now being diagnosed with brain or spinal cord tumors may have a better outlook than these statistics show.
The outlook for people with brain or spinal cord tumors varies by the type of tumor and the person’s age. But many other factors can also affect a person’s outlook, such as their age and overall health, where the tumor is located, and how well the tumor responds to treatment. The outlook for each person is specific to their circumstances.
Your doctor can tell you how these numbers may apply to you, as he or she is familiar with your situation.
Survival rates for more common adult brain and spinal cord tumors
The numbers in the table come from the Central Brain Tumor Registry of the United States 4 and are based on people who were treated between 2000 and 2014. As can be seen below, survival rates for brain and spinal cord tumors can vary widely by age, with younger people tending to have having better outlooks than older people. The survival rates for those 65 or older are generally lower than the rates for the ages listed below.
These numbers are for some of the more common types of brain and spinal cord tumors. Numbers are not readily available for all types of tumors, often because they are rare or are hard to classify.
| Type of Tumor | 5-Year Relative Survival Rate | ||
| Age | |||
| 20-44 | 45-54 | 55-64 | |
| Low-grade (diffuse) astrocytoma | 68% | 44% | 22% |
| Anaplastic astrocytoma | 54% | 32% | 14% |
| Glioblastoma | 19% | 8% | 5% |
| Oligodendroglioma | 88% | 81% | 68% |
| Anaplastic oligodendroglioma | 71% | 61% | 46% |
| Ependymoma/anaplastic ependymoma | 92% | 89% | 86% |
| Meningioma | 87% | 77% | 71% |
Remember, these survival rates are only estimates – they can’t predict what will happen to any individual. If you find these statistics are confusing and you have more questions, talk to your doctor to better understand your specific situation.
Prognostic Factors for brain and spinal cord cancers
For most types of cancer, the stage of the cancer — a measure of how far it has spread — is one of the most important factors in selecting treatment options and in determining a person’s outlook (prognosis).
But tumors of the brain and spinal cord differ in some important ways from cancers in other parts of the body. One of the main reasons other cancers are dangerous is that they can spread throughout the body. Tumors starting in the brain or spinal cord can spread to other parts of the central nervous system, but they almost never spread to other organs. These tumors are dangerous because they can interfere with essential brain functions.
Because tumors in the brain or spinal cord almost never spread to other parts of the body, they do not have a formal staging system like most other cancers. Some of the important factors that help determine a person’s outlook include:
- Their age
- Their functional level (whether the tumor is affecting normal brain functions and everyday activity)
- The type of tumor (such as astrocytoma, ependymoma, etc.)
- The grade of the tumor (how quickly the tumor is likely to grow, based on how the cells look under a microscope)
- If the tumor cells have certain gene mutations or other changes (For example, tumors with a mutation in the IDH1 or IDH2 gene, known as “IDH-mutant” tumors, tend to grow more slowly and have a better outlook than tumors without these mutations.)
- The location and size of the tumor
- How much of the tumor can be removed by surgery (if it can be done)
- Whether or not the tumor has spread through the cerebrospinal fluid to other parts of the brain or spinal cord
- Whether or not tumor cells have spread beyond the central nervous system
If you have a brain or spinal cord tumor, talk to your doctor to learn more about how these and other factors might affect your outlook and treatment options.
Types of brain cancer and spinal cord tumors in Adults
Tumors that start in the brain (primary brain tumors) are not the same as tumors that start in other organs, such as the lung or breast, and then spread to the brain (metastatic or secondary brain tumors). In adults, metastatic tumors to the brain are actually more common than primary brain tumors. These tumors are not treated the same way. For example, breast or lung cancers that spread to the brain are treated differently from tumors that start in the brain.
Unlike cancers that start in other parts of the body, tumors that start in the brain or spinal cord rarely spread to distant organs. Even so, brain or spinal cord tumors are rarely considered benign (non-cancerous). They can still cause damage by growing and spreading into nearby areas, where they can destroy normal brain tissue. And unless they are completely removed or destroyed, most brain or spinal cord tumors will continue to grow and eventually be life-threatening.
Primary brain tumors can start in almost any type of tissue or cell in the brain or spinal cord. Some tumors have mixed cell types. Tumors in different areas of the central nervous system (CNS) may be treated differently and have a different prognosis (outlook).
Brain and spinal cord tumor grades
Some brain and spinal cord tumors are more likely to grow into nearby tissues (and to grow quickly) than are other tumors. The World Health Organization (WHO) divides brain and spinal cord tumors into 4 grades (using Roman numerals I to IV), based largely on how the cells look under the microscope:
- Grade I: These tumors typically grow slowly and do not grow into (invade or infiltrate) nearby tissues. They can often be cured with surgery.
- Grade II: These tumors also tend to grow slowly but they can grow into nearby brain tissue. They are more likely to come back after surgery than grade I tumors. They are also more likely to become faster-growing tumors over time.
- Grade III: These tumors look more abnormal under the microscope. They can grow into nearby brain tissue and are more likely to need other treatments in addition to surgery.
- Grade IV: These are the fastest growing tumors. They generally require the most aggressive treatment.
Gliomas
Gliomas are not a specific type of brain tumor. Glioma is a general term for tumors that start in glial cells. A number of tumors can be considered gliomas, including:
- Astrocytomas (which include glioblastomas)
- Oligodendrogliomas
- Ependymomas
About 3 out of 10 of all brain tumors are gliomas. Most fast-growing brain tumors are gliomas.
Astrocytomas
Astrocytomas are tumors that start in glial cells called astrocytes. About 2 out of 10 brain tumors are astrocytomas.
Most astrocytomas can spread widely throughout the brain and blend with the normal brain tissue, which can make them very hard to remove with surgery. Sometimes they spread along the cerebrospinal fluid (CSF) pathways. It is very rare for them to spread outside of the brain or spinal cord.
Astrocytomas (like other brain tumors) are classified into 4 grades.
- Non-infiltrating (grade I) astrocytomas do not usually grow into nearby tissues and tend to have a good prognosis. These include pilocytic astrocytomas and subependymal giant cell astrocytomas (SEGAs). They are more common in children than in adults.
- Low-grade (grade II) astrocytomas, such as diffuse astrocytomas, tend to be slow growing, but they can grow into nearby areas and can become more aggressive and fast growing over time.
- Anaplastic (grade III) astrocytomas grow more quickly.
- Glioblastomas (grade IV) are the fastest growing. These tumors make up more than half of all gliomas and are the most common malignant brain tumors in adults.
Oligodendrogliomas
These tumors start in brain glial cells called oligodendrocytes. These are grade II tumors that tend to grow slowly. Most of these can grow into (infiltrate) nearby brain tissue and cannot be removed completely by surgery. Oligodendrogliomas sometimes spread along the CSF pathways but rarely spread outside the brain or spinal cord. As with astrocytomas, they can become more aggressive over time. Very aggressive (grade III) forms of these tumors are known as anaplastic oligodendrogliomas. Only about 2% of brain tumors are oligodendrogliomas.
Ependymomas
These tumors start in ependymal cells, which line the ventricles. They can range from fairly low-grade (grade II) tumors to higher grade (grade III) tumors, which are called anaplastic ependymomas. Only about 2% of brain tumors are ependymomas.
Ependymomas are more likely to spread along the cerebrospinal fluid (CSF) pathways than other gliomas but do not spread outside the brain or spinal cord. Ependymomas may block the exit of CSF from the ventricles, causing the ventricles to become very large – a condition called hydrocephalus.
Unlike astrocytomas and oligodendrogliomas, ependymomas usually do not grow into normal brain tissue. As a result, some (but not all) ependymomas can be removed completely and cured by surgery. But because they can spread along ependymal surfaces and CSF pathways, treating them can sometimes be difficult. Spinal cord ependymomas have the greatest chance of being cured with surgery, but treatment can cause side effects related to nerve damage.
Meningiomas
Meningiomas begin in the meninges, the layers of tissue that surround the outer part of the brain and spinal cord. Meningiomas account for about 1 out of 3 primary brain and spinal cord tumors. They are the most common brain tumors in adults (although strictly speaking, they are not actually brain tumors).
The risk of these tumors increases with age. They occur about twice as often in women. Sometimes these tumors run in families, especially in those with neurofibromatosis, a syndrome in which people develop many benign tumors of nerve tissue.
Meningiomas are often assigned a grade, based on how the cells look under the microscope.
- Grade I (benign) meningiomas have cells that look the most like normal cells. They account for about 8 of 10 meningiomas. Most of these can be cured by surgery, but some grow very close to vital structures in the brain or cranial nerves and cannot be cured by surgery alone.
- Grade II (atypical or invasive) meningiomas usually have cells that look slightly more abnormal. They make up about 15% to 20% of meningiomas. They can grow directly into nearby brain tissue and bone and are more likely to come back (recur) after surgery.
- Grade III (anaplastic or malignant) meningiomas have cells that look the most abnormal. They make up only about 1% to 3% of meningiomas. They tend to grow quickly, can grow into nearby brain tissue and bone, and are the most likely to come back after treatment. Some may even spread to other parts of the body.
Medulloblastomas
Medulloblastomas develop from neuroectodermal cells (early forms of nerve cells) in the cerebellum. They are fast-growing (grade IV) tumors and often spread throughout the CSF pathways, but they can be treated by surgery, radiation therapy, and chemotherapy.
Medulloblastomas occur much more often in children than in adults. They are part of a class of tumors called embryonal tumors that can also start in other parts of the central nervous system. They are discussed in more detail in Brain and Spinal Cord Tumors in Children.
Gangliogliomas
Gangliogliomas contain both neurons and glial cells. These tumors are very uncommon in adults. They are typically slow growing (grade II) tumors and can usually be cured by surgery alone or surgery combined with radiation therapy.
Schwannomas (neurilemmomas)
Schwannomas develop from Schwann cells, which surround and insulate cranial nerves and other nerves. They make up about 8% of all CNS tumors.
Schwannomas are almost always benign (grade I) tumors. They can arise from any cranial nerve. When they form on the cranial nerve responsible for hearing and balance near the cerebellum they are called vestibular schwannomas or acoustic neuromas. They can also start on spinal nerves after the point where they have left the spinal cord. When this happens, they can press on the spinal cord, causing weakness, sensory loss, and bowel and bladder problems.
Craniopharyngiomas
These slow-growing (grade I) tumors start above the pituitary gland but below the brain itself. They may press on the pituitary gland and the hypothalamus, causing hormone problems. Because they start very close to the optic nerves, they can also cause vision problems. Their tendency to stick to these important structures can make them hard to remove completely without damaging vision or hormone balance. Craniopharyngiomas are more common in children, but they are sometimes seen in adults.
Other tumors that can start in or near the brain
Chordomas
These rare tumors start in the bone at the base of the skull or at the lower end of the spine. Chordomas don’t start in the central nervous system, but they can injure the nearby brain or spinal cord by pressing on it.
These tumors are treated with surgery if possible, often followed by radiation therapy, but they tend to come back in the same area after treatment, causing more damage. They usually do not spread to other organs.
Non-Hodgkin lymphomas
Lymphomas are cancers that start in white blood cells called lymphocytes (one of the main cell types of the immune system). Most lymphomas start in other parts of the body, but some start in the CNS, and are called primary CNS lymphomas. These lymphomas are more common in people with immune system problems, such as those infected with HIV, the virus that causes AIDS. Because of new treatments for AIDS, primary CNS lymphomas have become less common in recent years.
These lymphomas often grow quickly and can be hard to treat. Recent advances in chemotherapy, however, have improved the outlook for people with these cancers. For more information on primary CNS lymphomas (including treatment), see Non-Hodgkin Lymphoma.
Pituitary tumors
Tumors that start in the pituitary gland are almost always benign (non-cancerous). But they can still cause problems if they grow large enough to press on nearby structures or if they make too much of any kind of hormone.
What causes brain cancer in Adults
The cause of most brain and spinal cord tumors is not fully understood, and there are very few well-established risk factors. But researchers have found some of the changes that occur in normal brain cells that may lead them to form brain tumors.
Normal human cells grow and function based mainly on the information contained in each cell’s DNA. Brain and spinal cord tumors, like other tumors, are caused by changes in the DNA inside cells. DNA is the chemical that makes up our genes, which control how our cells function. We usually look like our parents because they are the source of our DNA. But DNA affects more than how we look.
Some genes control when our cells grow, divide into new cells, and die:
- Certain genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that help keep cell division under control, or make cells die at the right time, are called tumor suppressor genes.
Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes. These gene changes can be inherited from a parent, but more often they happen during a person’s lifetime.
Inherited gene changes
Researchers have found gene changes that cause some rare inherited syndromes (like neurofibromatosis, tuberous sclerosis, Li-Fraumeni syndrome, and von Hippel-Lindau syndrome) and increase the risk of developing some brain and spinal cord tumors. For example, the Li-Fraumeni syndrome is caused by changes in the TP53 tumor suppressor gene. Normally, this gene prevents cells with damaged DNA from growing. Changes in this gene increase the risk of developing brain tumors (particularly gliomas), as well as some other cancers.
Gene changes acquired during a person’s lifetime
Most often, it’s not known why people without inherited syndromes develop brain or spinal cord tumors. Most exposures that cause cancer somehow damage DNA. For example, tobacco smoke is a risk factor for lung cancer and several other cancers because it contains chemicals that can damage the genes inside cells. The brain is relatively protected from tobacco smoke and other cancer-causing chemicals that we might breathe in or eat, so these factors are not likely to play a major role in these cancers.
Several different gene changes usually occur in normal cells before they become cancerous. There are many kinds of brain tumors, each of which may have different sets of gene changes. A number of gene changes have been found in different brain tumor types, but there are probably many others that have not yet been found.
Researchers now understand some of the gene changes that occur in different types of brain tumors, but it’s still not clear what causes most of these changes. Some gene changes might be inherited, but most brain and spinal cord tumors are not the result of known inherited syndromes. Other than radiation, no known lifestyle-related or environmental factors are clearly linked to brain tumors. Most gene changes are probably just random events that sometimes happen inside a cell, without having an outside cause.
Risk Factors for Brain and Spinal Cord Tumors in Adults
A risk factor is anything that affects your chance of getting a disease such as a brain or spinal cord tumor. Different types of cancer have different risk factors. Some risk factors, like smoking, you can change. Others, like your age or family history, can’t be changed.
But having a risk factor, or even several, does not always mean that a person will get the disease, and many people get tumors without having any known risk factors.
Most brain tumors are not linked with any known risk factors and have no obvious cause. But there are a few factors that can raise the risk of brain tumors.
Radiation exposure
The best known environmental risk factor for brain tumors is radiation exposure, most often from radiation therapy to treat some other condition. For example, before the risks of radiation were known, children with ringworm of the scalp (a fungal infection) were sometimes treated with low-dose radiation therapy, which was later found to increase their risk of brain tumors as they got older.
Today, most radiation-induced brain tumors are caused by radiation to the head given to treat other cancers. They occur most often in people who received radiation to the brain as children as part of their treatment for leukemia. These brain tumors usually develop around 10 to 15 years after the radiation.
Radiation-induced tumors are still fairly rare, but because of the increased risk (as well as the other side effects), radiation therapy is only given to the head after carefully weighing the possible benefits and risks. For most patients with other cancers involving the brain or head, the benefits of radiation therapy far outweigh the risk of developing a brain tumor years later.
The possible risk from exposure to imaging tests that use radiation, such as x-rays or CT scans, is not known for sure. These tests use much lower levels of radiation than those used in radiation treatments, so if there is any increase in risk, it is likely to be very small. But to be safe, most doctors recommend that people (especially children and pregnant women) not get these tests unless they are clearly needed.
Family history
Most people with brain tumors do not have a family history of the disease, but in rare cases brain and spinal cord cancers run in families. In general, patients with familial cancer syndromes tend to have many tumors that first occur when they are young. Some of these families have well-defined disorders, such as:
Neurofibromatosis type 1 (NF1)
This genetic disorder, also known as von Recklinghausen disease, is the most common syndrome linked to brain or spinal cord tumors. People with this condition have higher risks of schwannomas, meningiomas, and certain types of gliomas, as well as neurofibromas (benign tumors of peripheral nerves). Changes in the NF1 gene cause this disorder. These changes are inherited from a parent in about half of all cases. In the other half, the NF1 gene changes occur before birth in people whose parents did not have this condition.
Neurofibromatosis type 2 (NF2)
This condition, which is much less common than NF1, is associated with vestibular schwannomas (acoustic neuromas), which almost always occur on both sides of the head. It is also linked with an increased risk of meningiomas or spinal cord ependymomas. Changes in the NF2 gene are usually responsible for neurofibromatosis type 2. Like NF1, the gene changes are inherited in about half of cases. In the other half, they occur before birth in children without a family history.
Tuberous sclerosis
People with this condition may have subependymal giant cell astrocytomas (SEGAs), which are low-grade astrocytomas that develop beneath the ependymal cells of the ventricles. They may also have other benign tumors of the brain, skin, heart, kidneys, and other organs. This condition is caused by changes in either the TSC1 or the TSC2 gene. These gene changes can be inherited from a parent, but most often they develop in people without a family history.
Von Hippel-Lindau disease
People with this condition tend to develop benign or cancerous tumors in different parts of the body, including hemangioblastomas (benign blood vessel tumors) in the brain, spinal cord, or retina, as well as tumors of the inner ear, kidney, adrenal gland, and pancreas. It is caused by changes in the VHL gene. Most often the gene changes are inherited, but in some cases the changes happen before birth in people whose parents don’t have them.
Li-Fraumeni syndrome
People with this condition are at higher risk for developing gliomas, along with breast cancer, soft tissue sarcomas, leukemia, adrenal gland cancer, and certain other types of cancer. It is caused by changes in the TP53 gene.
Other syndromes
Other inherited conditions are also linked with increased risks of certain types of brain and spinal cord tumors, including:
- Gorlin syndrome (basal cell nevus syndrome)
- Turcot syndrome
- Cowden syndrome
Some families may have genetic disorders that are not well recognized or that may even be unique to a particular family.
Having a weakened immune system
People with weakened immune systems have an increased risk of developing lymphomas of the brain or spinal cord (known as primary CNS lymphomas). Lymphomas are cancers of lymphocytes, a type of white blood cell that fights disease. Primary CNS lymphoma is less common than lymphoma that develops outside the brain.
A weakened immune system can be congenital (present at birth), or it can be caused by treatments for other cancers, treatment to prevent rejection of transplanted organs, or diseases such as acquired immunodeficiency syndrome (AIDS).
Factors with uncertain, controversial, or unproven effects on brain tumor risk
Cell phone use
Cell phones give off radiofrequency (RF) rays, a form of energy on the electromagnetic spectrum between FM radio waves and those used in microwave ovens, radar, and satellite stations. Cell phones do not give off ionizing radiation, the type that can cause cancer by damaging the DNA inside cells. Still, there have been concerns that the phones, whose antennae are built-in and therefore are placed close to the head when being used, might somehow raise the risk of brain tumors.
Some studies have suggested a possible increased risk of brain tumors or of vestibular schwannomas (acoustic neuromas) with cell phone use, but most of the larger studies done so far have not found an increased risk, either overall or among specific types of tumors. Still, there are very few studies of long-term use (10 years or more), and cell phones haven’t been around long enough to determine the possible risks of lifetime use. The same is true of any possible higher risks in children, who are increasingly using cell phones. Cell phone technology also continues to change, and it’s not clear how this might affect any risk.
These risks are being studied, but it will probably be many years before firm conclusions can be made. In the meantime, for people concerned about the possible risks, there are ways to lower your exposure, such as using the phone’s speaker or an earpiece to move the phone itself away from the head.
Other factors
Other environmental factors such as exposure to vinyl chloride (a chemical used to manufacture plastics), petroleum products, and certain other chemicals have been linked with an increased risk of brain tumors in some studies but not in others.
Exposure to aspartame (a sugar substitute), exposure to electromagnetic fields from power lines and transformers, and infection with certain viruses have been suggested as possible risk factors, but most researchers agree that there is no convincing evidence to link these factors to brain tumors. Research on these and other possible risk factors continues.
Signs and Symptoms of Adult Brain and Spinal Cord Tumors
Signs and symptoms of brain or spinal cord tumors may occur gradually and become worse over time, or they can happen suddenly, such as with a seizure.
General symptoms
Tumors in any part of the brain might increase the pressure inside the skull (known as intracranial pressure). This can be caused by growth of the tumor itself, swelling in the brain, or blockage of the flow of cerebrospinal fluid. Increased pressure can lead to general symptoms such as:
- Headache
- Nausea
- Vomiting
- Blurred vision
- Balance problems
- Personality or behavior changes
- Seizures
- Drowsiness or even coma
Headaches that tend to get worse over time are a common symptom of brain tumors, occurring in about half of patients. (Of course, most headaches are not caused by tumors.)
As many as half of people with brain tumors will have seizures at some point. The type of seizure may depend on where the tumor is. Sometimes this is the first sign of a brain tumor, but fewer than 1 in 10 first seizures are caused by brain tumors.
Symptoms of tumors in different parts of the central nervous system
Brain and spinal cord tumors often cause problems with the specific functions of the region they develop in. But these symptoms can be caused by any disease in that particular location — they do not always mean a person has a brain or spinal cord tumor.
- Tumors in the parts of the cerebrum (the large, outer part of the brain) that control movement or sensation can cause weakness or numbness of part of the body, often on just one side.
- Tumors in or near the parts of the cerebrum responsible for language can cause problems with speech or even understanding words.
- Tumors in the front part of the cerebrum can sometimes affect thinking, personality, and language.
- If the tumor is in the cerebellum (the lower, back part of the brain that controls coordination), a person might have trouble walking, trouble with precise movements of hands, arms, feet, and legs, problems swallowing or synchronizing eye movements, and changes in speech rhythm.
- Tumors in the back part of the cerebrum, or around the pituitary gland, the optic nerve, or certain other cranial nerves can cause vision problems.
- Tumors in or near other cranial nerves might lead to hearing loss (in one or both ears), balance problems, weakness of some facial muscles, facial numbness or pain, or trouble swallowing.
- Spinal cord tumors can cause numbness, weakness, or lack of coordination in the arms and/or legs (usually on both sides of the body), as well as bladder or bowel problems.
The brain also controls functions of some other organs, including hormone production, so brain tumors can also cause many other symptoms not listed here.
Having one or more of the symptoms above does not necessarily mean that you have a brain or spinal cord tumor. All of these symptoms can have other causes. Still, if you have any of these symptoms, especially if they don’t go away or get worse over time, see your doctor so the cause can be found and treated, if needed.
How is Brain and Spinal Cord Cancers Diagnosed – Adults
Brain and spinal cord tumors are usually found because of signs or symptoms a person is having. If a tumor is suspected, tests will be needed to confirm the diagnosis.
Medical history and physical exam
If signs or symptoms suggest you might have a brain or spinal cord tumor, your doctor will get a complete medical history, focusing on your symptoms and when they began. The doctor will also do a neurologic exam to check your brain and spinal cord function. This exam tests reflexes, muscle strength, vision, eye and mouth movement, coordination, balance, alertness, and other functions.
If the results of the exam are abnormal, your doctor may refer you to a neurologist (a doctor who specializes in medical treatment of nervous system diseases) or a neurosurgeon (a doctor who specializes in surgical treatment of nervous system diseases), who will do a more detailed neurologic exam or other tests.
Imaging tests
Your doctor may order one or more imaging tests. These tests use x-rays, strong magnets, or radioactive substances to create pictures of the brain and spinal cord. The pictures may be looked at by doctors specializing in this field (neurosurgeons, neurologists, and neuroradiologists) as well as by your primary doctor.
Magnetic resonance imaging (MRI) and computed tomography (CT) scans are used most often to look for brain diseases. These scans will show a brain tumor, if one is present, in almost all cases. Doctors can often also get an idea about what type of tumor it might be, based on how it looks on the scan and where it is in the brain.
Magnetic resonance imaging (MRI) scan
MRI scans are very good for looking at the brain and spinal cord and are considered the best way to look for tumors in these areas. The images they provide are usually more detailed than those from CT scans (described below). But they do not image the bones of the skull as well as CT scans and therefore may not show the effects of tumors on the skull.
MRI scans use radio waves and strong magnets (instead of x-rays) to make pictures. A contrast material called gadolinium may be injected into a vein before the scan to help see details better.
Special types of MRI can be useful in some situations:
Magnetic resonance angiography (MRA) and magnetic resonance venography (MRV): These special types of MRI may be used to look at the blood vessels in the brain. This can be very useful before surgery to help the surgeon plan an operation.
Magnetic resonance spectroscopy (MRS): This test can be done as part of an MRI. It measures biochemical changes in an area of the brain (displayed in graph-like results called spectra, although basic images can also be created). By comparing the results for a tumor to that of normal brain tissue, it can sometimes help determine the type of tumor (or how quickly it is likely to grow), although a biopsy of the tumor is often still needed to get an accurate diagnosis. MRS can also be used after treatment to help determine if an area that still looks abnormal on another test is remaining tumor or if it is more likely to be scar tissue.
Magnetic resonance perfusion: For this test, also known as perfusion MRI, a contrast dye is injected quickly into a vein. A special type of MR image is then obtained to look at the amount of blood going through different parts of the brain and tumor. Tumors often have a bigger blood supply than normal areas of the brain. A faster growing tumor may need more blood.
Perfusion MRI can give doctors an idea of the best place to take a biopsy. It can also be used after treatment to help determine if an area that still looks abnormal is remaining tumor or if it is more likely to be scar tissue.
Functional MRI (fMRI): This test looks for tiny blood flow changes in an active part of the brain. It can be used to determine what part of the brain handles a function such as speech, thought, sensation, or movement. Doctors can use this to help determine which parts of the brain to avoid when planning surgery or radiation therapy.
This test is similar to a standard MRI, except that you will be asked to do specific tasks (such as answering simple questions or moving your fingers) while the scans are being done.
Computed tomography (CT) scan
A CT scan uses x-rays to make detailed cross-sectional images of your brain and spinal cord (or other parts of the body). Unlike a regular x-ray, a CT scan creates detailed images of the soft tissues in the body.
CT scans are not used as often as MRI scans when looking at brain or spinal cord tumors, but they can be useful in some cases. They may be used if MRI is not an option (such as in people who are very overweight or people who have a fear of enclosed spaces).CT scans also show greater detail of the bone structures near the tumor.
As with MRI, you may get an injection of a contrast dye through an IV (intravenous) line before the scan (although a different dye is used for CT scans). This helps better outline any tumors that are present.
CT angiography (CTA): For this test, you are injected with a contrast material through an IV line while you are in the CT scanner. The scan creates detailed images of the blood vessels in the brain, which can help doctors plan surgery. CT angiography can provide better details of the blood vessels in and around a tumor than MR angiography in some cases.
Positron emission tomography (PET) scan
For a PET scan, you are injected with a slightly radioactive substance (usually a type of sugar known as FDG) which collects mainly in tumor cells. A special camera is then used to create a picture of areas of radioactivity in the body. The picture is not as detailed as a CT or MRI scan, but it can provide helpful information about whether abnormal areas seen on other tests (such as MRIs) are likely to be tumors or not. This test is more likely to be helpful for fast-growing (high-grade tumors) than for slower-growing tumors.
This test is also useful after treatment to help determine if an area that still looks abnormal on an MRI scan is remaining tumor or if it is more likely to be scar tissue. Remaining tumor might show up on the PET scan, while scar tissue will not.
Chest x-ray
A chest x-ray might be done to look for tumors in the lungs if a tumor is found in the brain. This is because in adults, most tumors in the brain actually have started in another organ (most often the lung) and then spread to the brain. This test can be done in a doctor’s office, in an outpatient radiology center, or in a hospital.
Brain or spinal cord tumor biopsy
Imaging tests such as MRI and CT scans may show an abnormal area that is likely to be a brain or spinal cord tumor. But often these scans can’t tell exactly what type of tumor it is. This can only be done by removing some of the tumor tissue in a procedure called a biopsy. A biopsy may be done as a procedure on its own, or it may be part of surgery to treat the tumor.
Sometimes, a tumor may look so much like an astrocytoma on an MRI scan that a biopsy is not needed, especially if the tumor is in a part of the brain that would make it hard to biopsy (such as the brain stem). In rare cases a PET scan or MR spectroscopy may give enough information so that a biopsy is not needed.
The 2 main types of biopsies for brain tumors are:
Stereotactic (needle) biopsy
This type of biopsy may be used if, based on imaging tests, the risks of surgery to remove the tumor might be too high (such as with some tumors in vital areas, those deep within the brain, or other tumors that probably can’t be treated with surgery) but a sample is still needed to make a diagnosis.
The patient may be asleep (under general anesthesia) or awake during the biopsy. If the patient is awake, the neurosurgeon injects a local anesthetic into areas of skin above the skull to numb them. (The skull and brain do not feel pain.)
The biopsy itself can be done in two main ways:
- One approach is to get an MRI or CT, and then use either markers (each about the size of a nickel) placed on different parts of the scalp, or facial and scalp contours, to create a map of the inside of the head. An incision (cut) is then made in the scalp, and a small hole is drilled in the skull. An image-guidance system is then used to direct a hollow needle into the tumor to remove small pieces of tissue.
- In an approach that’s being used less often, a rigid frame is attached to the head. An MRI or CT scan is often used along with the frame to help the neurosurgeon guide a hollow needle into the tumor. This also requires an incision in the scalp and a small hole in the skull.
The removed tissue is sent to a pathologist (a doctor specializing in diagnosis of diseases by lab tests). Sometimes it might need to be looked at by a neuropathologist, a pathologist who specializes in nervous system diseases. The pathologist looks at it under a microscope (and might do other lab tests) to determine if the tumor is benign or malignant (cancerous) and exactly what type of tumor it is. This is very important in determining a person’s prognosis (outlook) and the best course of treatment. A preliminary diagnosis might be available the same day, although it often takes at least a few days to get a final diagnosis.
Surgical or open biopsy (craniotomy)
If imaging tests show the tumor can likely be treated with surgery, the neurosurgeon may not do a needle biopsy. Instead, he or she may do an operation called a craniotomy to remove all or most of the tumor. (Removing most of the tumor is known as debulking.)
For a preliminary diagnosis, small samples of the tumor are looked at right away by the pathologist while the patient is still in the operating room. This can help guide treatment, including whether further surgery should be done at that time. A final diagnosis is made within a few days in most cases.
Lab tests of biopsy specimens
Finding out which type of tumor someone has is very important in helping to determine their outlook (prognosis) and treatment options. But in recent years, doctors have found that changes in certain genes, chromosomes, or proteins within the cancer cells can also be important. Some tumors are now tested for these types of changes. For example:
- Gliomas that are found to have IDH1 or IDH2 gene mutations tend to have a better outlook than gliomas without these gene mutations.
- Oligodendrogliomas whose cells are missing parts of certain chromosomes (known as a 1p19q co-deletion) are much more likely to be helped by chemotherapy than tumors that do not.
- In high-grade gliomas, MGMT promoter methylation is linked with better outcomes and a higher likelihood of responding to chemotherapy, so it can sometimes be used to help guide treatment.
Lumbar puncture (spinal tap)
This test is used mainly to look for cancer cells in the cerebrospinal fluid (CSF), the liquid that surrounds the brain and spinal cord. For this test, you lie on your side on a bed or exam table with your knees up near your chest. The doctor first numbs an area in the lower part of the back near the spine. A small, hollow needle is then placed between the bones of the spine to withdraw some of the fluid.
This fluid is sent to a lab to be looked at for cancer cells. Other tests may be done on the fluid as well.
Lumbar punctures are usually very safe, but doctors have to make sure the test does not result in a large drop in pressure in the fluid, which could possibly cause serious problems. For this reason, imaging tests such as CT or MRI scans are done first.
Lumbar punctures usually aren’t done to diagnose brain tumors, but they may be done to help determine the extent of a tumor by looking for cancer cells in the CSF. They are often used if a tumor has already been diagnosed as a type that can commonly spread through the CSF, such as an ependymoma. Lumbar punctures are particularly important in people with suspected brain lymphomas because often the lymphoma cells spread into the CSF.
Blood and urine tests
These lab tests rarely are part of the actual diagnosis of brain and spinal cord tumors, but they may be done to check how well the liver, kidneys, and some other organs are working. This is especially important before any planned surgery. If you are getting chemotherapy, blood tests will be done routinely to check blood counts and to see if the treatment is affecting other parts of your body.
Brain cancer treatment in Adults
Several types of treatment can be used to treat brain and spinal cord tumors, including:
- Surgery
- Radiation therapy
- Chemotherapy
- Targeted therapy
- Other types of drugs
Treatment is based on the type of tumor and other factors, and often more than one type of treatment is used. Typically a team of doctors plan each person’s treatment individually to give them the best chance of treating the tumor while limiting the side effects as much as possible.
Which doctors treat brain and spinal cord tumors?
Brain and spinal cord tumors can often be hard to treat and require care from a team of different types of doctors. This team is often led by a neurosurgeon, a doctor who operates on brain and nervous system tumors. Other doctors on the team might include:
- Neurologist: a doctor who diagnoses brain and nervous system diseases and treats them with medicines
- Radiation oncologist: a doctor who uses radiation to treat cancer
- Medical oncologist: a doctor who uses chemotherapy and other medicines to treat cancers
- Endocrinologist: a doctor who treats diseases in glands that secrete hormones
You might have many other specialists on your treatment team as well, including physician assistants, nurse practitioners, nurses, psychologists, social workers, rehabilitation specialists, and other health professionals. See Health Professionals Associated With Cancer Care for more on this.
Making treatment decisions
It’s important to discuss all of your treatment options, including their goals and possible side effects, with your treatment team to help make the decision that best fits your needs. Some important things to consider include:
- Your age and overall health
- The type and location of your tumor
- The likelihood that treatment will cure your tumor (or help in some other way)
- Your feelings about the possible side effects from treatment
You may feel that you need to decide quickly, but it’s important to give yourself time to think about the information you have learned. It’s also very important to ask questions if there is anything you’re not sure about.
Getting a second opinion
If time permits, getting a second opinion from a doctor experienced with your type of tumor is often a good idea. This can give you more information and help you feel more confident about the treatment plan you choose. If you aren’t sure where to go for a second opinion, ask your doctor for help.
Thinking about taking part in a clinical trial
Clinical trials are carefully controlled research studies that are done to get a closer look at promising new treatments or procedures. Clinical trials are one way to get state-of-the art cancer treatment. Sometimes they may be the only way to get access to newer treatments. They are also the best way for doctors to learn better methods to treat brain and spinal cord tumors. Still, they are not right for everyone.
If you would like to learn more about clinical trials that might be right for you, start by asking your doctor if your clinic or hospital conducts clinical trials.
Considering complementary and alternative methods
You may hear about alternative or complementary methods that your doctor hasn’t mentioned to treat your cancer or relieve symptoms. These methods can include vitamins, herbs, and special diets, or other methods such as acupuncture or massage, to name a few.
Complementary methods refer to treatments that are used along with your regular medical care. Alternative treatments are used instead of a doctor’s medical treatment. Although some of these methods might be helpful in relieving symptoms or helping you feel better, many have not been proven to work. Some might even be dangerous.
Be sure to talk to your treatment team about any method you are thinking about using. They can help you learn what is known (or not known) about the method, which can help you make an informed decision.
Help getting through treatment
Your treatment team will be your first source of information and support, but there are other resources for help when you need it. Hospital- or clinic-based support services are an important part of your care. These might include nursing or social work services, financial aid, nutritional advice, rehab, or spiritual help.
Choosing to stop treatment or choosing no treatment at all
For some people, when treatments have been tried and are no longer controlling the tumor, it could be time to weigh the benefits and risks of continuing to try new treatments. Whether or not you continue treatment, there are still things you can do to help maintain or improve your quality of life.
Some people, especially if the tumor is advanced, might not want to be treated at all. There are many reasons you might decide not to get treatment, but it’s important to talk this through with your doctors before you make this decision. Remember that even if you choose not to treat the tumor, you can still get supportive care to help with pain or other symptoms.
Types of brain cancer in Children
Tumors can form in almost any type of tissue or cell in the brain or spinal cord. Some tumors have a mixture of cell types. Tumors in different areas of the central nervous system may be treated differently and have a different prognosis (outlook).
Brain tumors in children are more likely to start in the lower parts of the brain, such as the cerebellum and brain stem, than they are in adults. But they can start in the upper parts of the brain as well.
Gliomas
Gliomas are not a specific type of tumor. Glioma is a general term for a group of tumors that start in glial cells. A number of tumors can be considered gliomas, including glioblastoma (also known as glioblastoma multiforme), anaplastic astrocytoma, astrocytoma, oligodendroglioma, ependymoma, brain stem glioma, and optic glioma. About half of all brain and spinal cord tumors in children are gliomas.
Astrocytomas
- Astrocytomas are tumors that start in cells called astrocytes, a kind of glial cell.
- Most astrocytomas can spread widely throughout the brain and blend with the normal brain tissue, which can make them very hard to remove by surgery. Sometimes they spread along the cerebrospinal fluid (CSF) pathways. It is very rare for them to spread outside of the brain or spinal cord.
- Astrocytomas are often grouped as high grade, intermediate grade, or low grade, based largely on how the cells look under the microscope.
Intermediate- and high-grade astrocytomas: These tumors tend to grow quickly and spread into the surrounding normal brain tissue. The highest-grade astrocytoma, known as glioblastoma, is the fastest growing. Anaplastic astrocytomas are also in this group.
Low-grade astrocytomas: These tumors tend to grow slowly and are the most common type in children. Some special types, known as non-infiltrating astrocytomas, tend to grow very slowly and do not grow into (infiltrate) nearby tissues, so they often have a good prognosis.
- Pilocytic astrocytomas are slow growing and rarely infiltrate nearby tissues. They most commonly occur in the cerebellum but can also begin in the optic nerve, hypothalamus, brain stem, or other areas. They account for nearly 1 out of 5 brain tumors in children.
- Subependymal giant cell astrocytomas (SEGAs) occur in the ventricles. They are also slow growing and rarely infiltrate nearby tissues. These tumors are almost always linked with an inherited condition called tuberous sclerosis.
- Fibrillary (diffuse) astrocytomas are also slow-growing tumors, but with the important characteristic of growing into nearby tissues, which makes them hard to remove with surgery. Though these tumors are thought of as low grade, they tend to become more aggressive and fast growing over time.
- Optic gliomas are low-grade astrocytomas that start in the optic nerves (the nerves leading from the eyes to the brain). They are often linked with an inherited condition called neurofibromatosis type 1. These tumors are rarely fatal, but they may cause vision loss and injury to nearby brain tissue.
Oligodendrogliomas
These tumors start in brain glial cells called oligodendrocytes. These tumors tend to grow slowly, but like astrocytomas, most of them can grow into nearby brain tissue and can’t be removed completely by surgery. Oligodendrogliomas rarely spread along the CSF pathways and even less frequently spread outside the brain or spinal cord. Only about 1% of brain tumors in children are oligodendrogliomas. As with astrocytomas, they can become more aggressive over time.
Ependymomas
- About 5% of brain tumors in children are ependymomas. These tumors start in the ependymal cells that line the ventricles or central canal of the spinal cord. They can range from fairly low-grade (slow growing) tumors to higher grade ones, which are called anaplastic ependymomas.
- Ependymomas may spread along the CSF pathways but do not spread outside the brain or spinal cord. These tumors can block the flow of CSF out of the ventricles, causing the ventricles to become very large – a condition called hydrocephalus.
- Unlike astrocytomas and oligodendrogliomas, ependymomas usually do not grow into normal brain tissue. As a result, some (but not all) ependymomas can be removed and cured by surgery. But because they can spread along ependymal surfaces and CSF pathways, treating them can sometimes be difficult.
Mixed gliomas
These tumors contain more than one cell type. For example, oligoastrocytomas have some of the same types of cells as both oligodendrogliomas and astrocytomas. Treatment is typically based on the fastest-growing component of the tumor.
Brain stem gliomas
This term refers to the location of the tumor, rather than the type of cell it starts in. A small number of brain stem gliomas occur as a tumor with very distinct edges (called a focal brain stem glioma). More often, brain stem gliomas grow diffusely throughout the brain stem, rather than growing as a focal tumor. These tumors often start in the pons, where they are called diffuse intrinsic pontine gliomas (DIPGs).
About 10% to 20% of brain tumors in children are brain stem gliomas. Nearly all of these tumors are some type of astrocytoma.
Primitive neuroectodermal tumors (PNETs)
These tumors start in primitive (immature) cells of the central nervous system called neuroectodermal cells. About 1 out of 5 brain tumors in children are PNETs. They are more common in younger children than older ones, and are rare in adults. PNETs tend to grow quickly and often spread throughout the CSF pathways.
- Medulloblastomas: PNETs that start in the cerebellum are called medulloblastomas. Most PNETs in children are medulloblastomas. These tumors can often be treated effectively and tend to have a better outlook than PNETs in other parts of the brain.
- Pineoblastomas: PNETs that occur in the pineal gland are called pineoblastomas. These tumors are usually harder to treat than medulloblastomas.
- Other PNETs: Other, less common types of central nervous system PNETs include medulloepitheliomas, ependymoblastomas, and neuroblastomas that start in the brain or spinal cord.
Craniopharyngiomas
These slow-growing tumors start above the pituitary gland but below the brain itself. They account for about 4% of brain tumors in children. These tumors may press on the pituitary gland and the hypothalamus, causing hormone problems. Because craniopharyngiomas start very close to the optic nerves, they can also cause vision problems. This makes them hard to remove completely without damaging the child’s vision or hormone balance.
Mixed glial and neuronal tumors
Certain tumors that develop in children and young adults (and rarely in older adults) have both glial and neuronal cell components. They tend to have a fairly good prognosis.
- Pleomorphic xanthoastrocytoma (PXA) and dysembryoplastic neuroepithelial tumors (DNETs) look as if they could grow quickly when seen under the microscope, but these tumors tend to be fairly benign, and most are cured by surgery alone.
- Ganglioglioma is a type of tumor that has both mature neurons and glial cells. Most can be cured by surgery alone or surgery combined with radiation therapy.
Choroid plexus tumors
These rare tumors start in the choroid plexus within the ventricles of the brain. Most are benign (choroid plexus papillomas) and are cured by surgery. However, some are malignant (choroid plexus carcinomas).
Schwannomas (neurilemmomas)
This type of tumor starts in Schwann cells that surround and insulate cranial nerves and other nerves. Schwannomas are usually benign tumors. They often form near the cerebellum on the cranial nerve responsible for hearing and balance, in which case they are called vestibular schwannomas or acoustic neuromas. They may also develop on spinal nerves past the point where the nerves have left the spinal cord. When this is the case, the tumor can press on the spinal cord, causing weakness, sensory loss, and bowel and bladder problems.
These tumors are rare in children. When schwannomas are found in a child, particularly if there are tumors on both sides of the head, it often means the child has an inherited tumor syndrome such as neurofibromatosis type 2.
Other tumors that start in or near the brain
Meningiomas
These tumors begin in the meninges, the layers of tissue that surround the outer part of the brain and spinal cord. Meningiomas cause symptoms by pressing on the brain or spinal cord. They are much less common in children than in adults.
Meningiomas are almost always benign and are usually cured by surgery. Some, however, are located very close to vital structures in the brain and can’t be cured by surgery alone.
Meningiomas are often assigned a grade based on how the tumor cells look.
- Grade I tumors, which look most like normal cells, make up about 80% to 90% of meningiomas.
- Grade II (atypical) meningiomas look slightly more abnormal.
- Grade III (anaplastic) meningiomas, which look the most abnormal, make up only about 1% to 3% of meningiomas.
Higher-grade meningiomas are more likely to come back after treatment, and some grade III meningiomas can spread to other parts of the body.
Chordomas
These tumors start in the bone at the base of the skull or at the lower end of the spine. These tumors don’t start in the central nervous system, but they can injure nearby parts of the brain or spinal cord by pressing on them. Chordomas tend to come back after treatment, if they are not removed completely, causing more damage. They usually do not spread to other organs. Chordomas are much more common in adults than in children.
Germ cell tumors
These rare tumors develop from germ cells, which normally form eggs in women and sperm in men. During normal development before birth, germ cells travel to the ovaries or testicles and develop into eggs or sperm cells. But sometimes some germ cells don’t move where they should and end up in abnormal locations such as the brain. They may then develop into germ cell tumors, similar to those that can form in the ovaries or testicles.
Germ cell tumors of the nervous system usually occur in children, most often in the pineal gland or above the pituitary gland. These tumors can sometimes be diagnosed without a biopsy by measuring certain chemicals in the cerebrospinal fluid (CSF) or blood.
The most common germ cell tumor of the nervous system is the germinoma. Other tumors that start in germ cells include choriocarcinomas, embryonal carcinomas, teratomas, and yolk sac tumors (endodermal sinus tumors).
Neuroblastomas
These nerve cell tumors are the third most common cancer in children. Neuroblastomas rarely develop in the brain or spinal cord; most develop from nerve cells inside the abdomen or chest. This type of cancer is most common during early infancy.
Lymphomas
Lymphomas are cancers that start in cells called lymphocytes (one of the main cell types of the immune system). Most lymphomas start in other parts of the body, but a small portion start in the central nervous system (CNS). CNS lymphomas are rare in children. For more on childhood lymphomas, see Non-Hodgkin Lymphoma.
Pituitary tumors
Tumors that start in the pituitary gland are almost always benign (non-cancerous). But they can still cause problems if they grow large enough to press on nearby structures or if they make too much of any kind of hormone. These tumors are more common in teens than in younger children.
Cancers that spread to the brain from other sites
Sometimes brain tumors are found not to have started in the brain but rather to have metastasized (spread) there from some other part of the body. Tumors that start in other organs and then spread to the brain are called metastatic or secondary brain tumors (as opposed to primary brain tumors, which start in the brain). This is important because metastatic and primary brain tumors are often treated differently.
In children, metastatic brain tumors are much less common than primary brain tumors. Childhood leukemias can sometimes spread to the CSF around the brain and spinal cord. When this happens, the cancer is still considered a leukemia (the cancer cells in the CSF are leukemia cells), so doctors use treatments directed at the leukemia.
Survival rates for more common childhood brain and spinal cord tumors
The numbers below come from the Central Brain Tumor Registry of the United States 4 and are based on children aged 19 or younger who were treated between 1995 and 2010. There are some important points to note about these numbers:
- These numbers are for some of the more common types of tumors. Numbers are not readily available for all types of tumors that occur in children, often because they are rare or are hard to classify.
- In some cases, the numbers include a wide range of different types of tumors that can have different outlooks. For example, the survival rate for primitive neuroectodermal tumors (PNETs) below includes medulloblastomas, pineoblastomas, and primitive neuroectodermal tumors (PNETs) in other parts of the brain. Medulloblastomas tend to have a better outlook than the other primitive neuroectodermal tumors (PNETs). Therefore the actual survival rate for medulloblastomas would be expected to be higher than the number below, while the number for other primitive neuroectodermal tumors (PNETs) would likely be lower.
| Type of Tumor | 5-Year Survival Rate |
| Pilocytic astrocytoma | About 95% |
| Fibrillary (diffuse) astrocytoma | About 80% to 85% |
| Anaplastic astrocytoma | About 30% |
| Glioblastoma | About 20% |
| Oligodendroglioma | About 90% to 95% |
| Ependymoma/anaplastic ependymoma | About 75% |
| PNETs (includes medulloblastoma and pineoblastoma) | About 60% to 65% |
Survival rates are often based on previous outcomes of large numbers of children who had the disease, but they can’t predict what will happen in any particular child’s case. Knowing the type of a child’s brain tumor is important in estimating their outlook. But many other factors can also affect a child’s outlook, such as the location and extent of the tumor and how well it responds to treatment. Even taking these other factors into account, survival rates are at best rough estimates. Your child’s doctor knows your child’s situation and is your best source of information on this topic.
What causes brain cancer in Children
The cause of most brain and spinal cord tumors is not fully understood. But researchers have found some of the changes that occur in normal brain cells that may lead them to form tumors.
Normal human cells grow and function based mainly on the information contained in each cell’s chromosomes. Chromosomes are long strands of DNA in each cell. Brain and spinal cord tumors, like other tumors, are usually caused by changes (mutations) in the DNA inside cells. DNA is the chemical that makes up our genes – the instructions for how our cells function. We usually look like our parents because they are the source of our DNA. But DNA affects more than how we look.
Some genes control when our cells grow, divide into new cells, and die. Certain genes that help cells grow, divide, and stay alive are called oncogenes. Others that slow down cell division, or cause cells to die at the right time, are called tumor suppressor genes. Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes. These gene changes can be inherited from a parent (as is sometimes the case with childhood cancers), but more often they happen spontaneously during a person’s lifetime.
In recent years, researchers have found the gene changes that cause some rare inherited syndromes (like neurofibromatosis, tuberous sclerosis, Li-Fraumeni syndrome, and von Hippel-Lindau syndrome) and increase the risk of developing some brain and spinal cord tumors. For example, the Li-Fraumeni syndrome is caused by changes in the TP53 tumor suppressor gene. Normally, this gene prevents cells with damaged DNA from growing. Changes in this gene increase the risk of developing brain tumors (particularly gliomas), as well as some other cancers.
In most cases, it is not known why people without inherited syndromes develop brain or spinal cord tumors. Most risk factors for cancer somehow damage genes. For example, tobacco smoke is a risk factor for lung cancer and several other cancers because it contains chemicals that can damage genes. The brain is relatively protected from tobacco smoke and other cancer-causing chemicals that we might breathe in or eat, so these factors are not likely to play a major role in these cancers.
Several different gene changes must usually occur in normal cells before they become cancerous. There are many kinds of brain tumors, each of which may have different sets of gene changes. A number of gene or chromosome changes have been found in different brain tumor types, but there are probably many others that have not yet been found.
Researchers now understand some of the gene changes that occur in different types of brain tumors, but it’s still not clear what causes these changes. Some gene changes might be inherited, but most brain and spinal cord tumors in children are not the result of known inherited syndromes. Most gene changes are probably just random events that sometimes happen inside a cell, without having an outside cause.
Other than radiation, there are no known lifestyle-related or environmental causes of childhood brain tumors, so it is important to remember that there is nothing these children or their parents could have done to prevent these cancers.
Risk Factors for Brain and Spinal Cord Tumors in Children
A risk factor is anything that affects a person’s chance of getting a disease such as a brain or spinal cord tumor. Different types of cancer have different risk factors.
Lifestyle-related risk factors such as diet, body weight, physical activity, and tobacco use play a major role in many adult cancers. But these factors usually take many years to influence cancer risk, and they are not thought to play much of a role in childhood cancers, including brain tumors.
Very few risk factors have been found for brain and spinal cord tumors. There is no clear cause for most of these tumors.
Radiation exposure
The only well-established environmental risk factor for brain tumors is radiation exposure to the head, which most often comes from the treatment of other conditions.
For example, before the risks of radiation were well known (more than 50 years ago), children with ringworm of the scalp (a fungal infection) often received low-dose radiation therapy. This was later found to increase their risk of brain tumors as they got older.
Today, most radiation-induced brain tumors are caused by radiation given to the head to treat other cancers, such as leukemia. These brain tumors usually develop around 10 to 15 years after the radiation.
Radiation-induced tumors are still fairly rare, but because of the increased risk (as well as the other side effects), radiation therapy is only given to the head after carefully weighing the possible benefits and risks. For most patients with cancer in or near the brain, the benefits of getting radiation therapy as part of their treatment far outweigh the small risk of developing a brain tumor years later.
The possible risk from fetal or childhood exposure to imaging tests that use radiation, such as x-rays or CT scans, is not known for sure. These tests use much lower levels of radiation than those used in radiation treatments, so if there is any increase in risk, it is likely to be very small. But to be safe, most doctors recommend that pregnant women and children not get these tests unless they are absolutely needed.
Inherited and genetic conditions
In rare cases (less than 5% of brain tumors), children have inherited abnormal genes from a parent that put them at increased risk for certain types of brain tumors. In other cases, these abnormal genes are not inherited but occur as a result of changes (mutations) in the gene before birth.
People with inherited tumor syndromes often have many tumors that start when they are young. Some of the more well-known syndromes include:
Neurofibromatosis type 1 (von Recklinghausen disease)
This is the most common syndrome linked to brain or spinal cord tumors. It is often inherited from a parent, but it can also start in some children whose parents don’t have it. Children with this syndrome may have optic gliomas or other gliomas of the brain or spinal cord, or neurofibromas (benign tumors of peripheral nerves). Changes in the NF1 gene cause this disorder.
Neurofibromatosis type 2
Less common than von Recklinghausen disease, this condition can also either be inherited or may start in children without a family history. It is associated with cranial or spinal nerve schwannomas, especially vestibular schwannomas (acoustic neuromas), which almost always occur on both sides of the head. It is also linked to an increased risk of meningiomas, as well as spinal cord gliomas or ependymomas. Changes in the NF2 gene are responsible for neurofibromatosis type 2.
Tuberous sclerosis
Children with this condition may develop subependymal giant cell astrocytomas (SEGAs), as well as other benign tumors of the brain, skin, heart, kidneys, or other organs. This condition is caused by changes in either the TSC1 or the TSC2 gene.
Von Hippel-Lindau disease
Children with this disease tend to develop blood vessel tumors (hemangioblastomas) of the cerebellum, spinal cord, or retina, as well as tumors in the kidney, pancreas, and some other parts of the body. It is caused by changes in the VHL gene.
Li-Fraumeni syndrome
People with this syndrome have an increased risk of gliomas, as well as breast cancer, soft tissue sarcomas, leukemia, adrenal gland cancer, and some other types of cancer. It is caused by changes in the TP53 gene.
Other syndromes
Other inherited conditions linked with increased risks of certain types of brain and spinal cord tumors include:
- Gorlin syndrome (basal cell nevus syndrome)
- Turcot syndrome
- Cowden syndrome
- Hereditary retinoblastoma
- Rubinstein-Taybi syndrome
Some families may have genetic disorders that are not well recognized or that could even be unique to a particular family.
Factors with uncertain, controversial, or unproven effects on brain tumor risk
Cell phone use
Cell phones give off radiofrequency (RF) rays, a form of electromagnetic energy on the spectrum between FM radio waves and those used in microwave ovens, radar, and satellite stations. Cell phones do not give off ionizing radiation, the type that can cause cancer by damaging the DNA inside cells. Still, there have been concerns that the phones, whose antennae are built-in and therefore are placed close to the head when being used, might somehow raise the risk of brain tumors.
Some studies have suggested a possible increased risk of brain tumors or of vestibular schwannomas in adults with cell phone use, but most of the larger studies done so far have not found an increased risk, either overall or among specific types of tumors. Still, there are very few studies of long-term use (10 years or more), and cell phones haven’t been around long enough to determine the possible risks of lifetime use. The same is true of any possible higher risks in children, who are increasingly using cell phones. Cell phone technology also continues to change, and it’s not clear how this might affect any risk.
These risks are being studied, but it will likely be many years before firm conclusions can be made. In the meantime, for people concerned about the possible risks, there are ways to lower their (and their children’s) exposure, such as using the speaker function or an earpiece to move the phone itself away from the head when used.
Other factors
Exposure to aspartame (a sugar substitute), exposure to electromagnetic fields from power lines and transformers, and infection with certain viruses have been suggested as possible risk factors, but most researchers agree that there is no convincing evidence to link these factors to brain tumors. Research on these and other potential risk factors continues.
Signs and Symptoms of Brain and Spinal Cord Tumors in Children
Signs and symptoms from brain and spinal cord tumors might occur gradually and become worse over time, or they can happen suddenly, such as with a seizure.
General symptoms
Tumors in any part of the brain might raise the pressure inside the skull (known as intracranial pressure). This can be caused by growth of the tumor, swelling in the brain, or blocked flow of cerebrospinal fluid. Increased pressure can lead to general symptoms such as:
- Headache
- Nausea
- Vomiting
- Crossed eyes or blurred vision
- Balance problems
- Behavior changes
- Seizures
- Drowsiness or even coma
Headaches that get worse over time are a common symptom of brain tumors. But not all brain tumors cause headaches, and most headaches are not caused by tumors.
In some children, seizures are the first symptom of a brain tumor. Most seizures in children are not caused by brain tumors, but if your child has a seizure, your child’s doctor may refer you to a neurologist (a doctor who specializes in brain and nervous system problems) to make sure it wasn’t caused by a brain tumor or other serious disease.
In the first few years of life, other symptoms of tumors can include irritability, loss of appetite, developmental delay, and a drop in intellectual and physical abilities. In very young children who can’t complain of symptoms, a parent may notice an increase in head size, sometimes along with bulging of the soft spots of the skull (fontanelles). This happens because the bones of the skull haven’t grown together yet, and increased pressure from a tumor can push them apart.
In the school-aged child, other general symptoms of tumors can include poor school performance, fatigue, and personality changes.
If the child can cooperate, the doctor can sometimes tell if pressure inside the skull is increased by looking inside the child’s eyes for swelling of the optic nerve (known as papilledema).
Symptoms of tumors in different parts of the central nervous system
Tumors in different parts of the brain or spinal cord can cause different symptoms. But these symptoms can be caused by any disease in that particular location – they don’t always mean a child has a brain or spinal cord tumor.
Brain and spinal cord tumors often cause problems with the specific functions of the region they develop in. For example:
- Tumors in the parts of the cerebrum (the large, outer part of the brain) that control movement or sensation can cause weakness or numbness in a part of the body, often on just one side.
- Tumors in or near the parts of the cerebrum responsible for language can cause problems with speech or even understanding words.
- Tumors in the front part of the cerebrum can sometimes affect thinking, personality, and language skills.
- Tumors in an area of the brain called the basal ganglia typically cause abnormal movements and body positions.
- Tumors in the cerebellum, which controls coordination, can cause trouble walking or with other normal functions, even eating.
- Tumors in the back part of the cerebrum, or around the pituitary gland, the optic nerves, or certain other cranial nerves can cause vision problems.
- Tumors in or near other cranial nerves might lead to loss of hearing, balance problems, weakness of some facial muscles, or trouble swallowing.
- Spinal cord tumors may cause numbness, weakness, or lack of coordination in the arms and/or legs (usually on both sides of the body), as well as bladder or bowel problems.
Having one or more of the symptoms above does not mean that your child definitely has a brain or spinal cord tumor. All of these symptoms can have other causes. Still, if your child has any of these symptoms, especially if they don’t go away or get worse over time, see your child’s doctor so that the cause can be found and treated, if needed.
How Are Brain and Spinal Cord Tumors Diagnosed in Children?
See diagnosis of brain and spinal cord tumors diganosis in adults above.
How Are Brain and Spinal Cord Tumors in Children Staged?
The stage of a cancer is a measure of how far it has spread. The extent of spread is based on the results of imaging tests (see How are brain and spinal cord tumors in children diagnosed?) and any other tests that have been done.
For most types of cancer, the stage is one of the most important factors in selecting treatment options and in determining the outlook (prognosis). But tumors of the brain and spinal cord differ in some important ways from cancers in other parts of the body. One of the main reasons other cancers are dangerous is that they can spread throughout the body. Tumors starting in the brain or spinal cord can spread to other parts of the central nervous system, but they almost never spread to other organs. These tumors are dangerous because when they grow, it can interfere with essential functions of the brain.
Because most tumors in the brain or spinal cord do not usually spread, they are not formally staged. Some of the most important factors that determine your child’s prognosis include:
- The type of tumor (such as astrocytoma, ependymoma, etc.)
- The grade of the tumor (how quickly the tumor is likely to grow, based on how the cells look under a microscope)
- The location and size of the tumor
- How much of the tumor can be removed by surgery (if it can be done)
- Your child’s age
- Your child’s functional level (whether the tumor is affecting normal brain functions and everyday activities)
- Whether or not the tumor has spread through the cerebrospinal fluid (CSF) to other parts of the brain or spinal cord
- Whether or not tumor cells have spread beyond the central nervous system
Medulloblastoma risk groups
A staging system is a standard way for the cancer care team to describe the extent of tumor spread. Formal staging systems have been proposed for some childhood brain tumors.
For example, many clinical trials for treating medulloblastoma use a system that places children into either standard-risk or high-risk groups. Children are placed in the high-risk group if any of these apply:
- The child is younger than 3
- A lot of the tumor can’t be removed during surgery
- Tumor cells are in the CSF or have spread to other parts of the brain or elsewhere
Doctors are still refining this system to make it as accurate as possible.
- Recent research has shown that medulloblastomas can be divided into 4 types, based on the major gene changes found in the cancer cells. Each type of medulloblastoma has a different outlook, so doctors may be able to use this to better tailor the treatment each child gets.
Brain cancer treatment in Children
Children and teens with brain and spinal cord tumors and their families have special needs that can be met best by cancer centers for children and teens, working closely with the child’s primary care doctor. These centers offer the advantage of being treated by teams of specialists who know the differences between cancers in adults and those in children and teens, as well as the unique needs of younger people with cancer.
For childhood brain and spinal cord tumors, this team is often led by a pediatric neurosurgeon, a doctor who uses surgery to treat brain and nervous system tumors in children. Other doctors on the team may include:
- Pediatric neurologist: a doctor who treats brain and nervous system diseases in children
- Radiation oncologist: a doctor who uses radiation to treat cancer
- Pediatric oncologist: a doctor who uses chemotherapy and other medicines to treat children’s cancers
- Endocrinologist: a doctor who treats diseases in glands that secrete hormones
Many other specialists may be involved in your child’s care as well, including physician assistants (PAs), nurse practitioners (NPs), nurses, psychologists, social workers, rehabilitation specialists, and other health professionals.
Going through cancer treatment with a child often means meeting lots of specialists and learning about parts of the medical system you probably haven’t had contact with before.
Before treatment, the doctors and other members of the team will help you, as a parent, understand the tests that will need to be done. The team’s social worker will also counsel you about the problems you and your child might have during and after treatments such as surgery, and might be able to help you find housing and financial aid if needed.
Other team members, such as a psychologist and specialists in rehabilitation, may also see your child before treatment begins. For example, if the tumor is slow growing and your child’s condition is stable, he or she may be seen by a psychologist before treatment to assess any damage the tumor may have caused. Most of the work of these specialists takes place after treatment.
The main treatments for children with brain and spinal cord tumors are:
- Surgery
- Radiation therapy
- Chemotherapy
- Targeted therapy
- Other drug treatments
In many cases children will get some combination of these treatments. Treatment is based on the type of tumor and other factors. Doctors plan each child’s treatment individually to give them the best chance of a cure while limiting side effects as much as possible.
It’s important to discuss your child’s treatment options as well as their possible side effects with the treatment team to help make the decision that’s the best fit for your child. If there is anything you don’t understand, ask to have it explained.
If time allows, getting a second opinion from another doctor experienced with your child’s type of tumor is often a good idea. It can give you more information and help you feel more confident about the treatment plan you choose.
Taking part in a clinical trial
Clinical trials are carefully controlled research studies that are done to get a closer look at promising new treatments or procedures. Clinical trials are one way to get state-of-the art cancer treatment. In some cases they may be the only way to get access to newer treatments. They are also the best way for doctors to learn better methods to treat cancer. Still, they are not right for everyone.
If you would like to learn more about clinical trials that might be right for you, start by asking your doctor if your clinic or hospital conducts clinical trials.
Considering complementary and alternative methods
You may hear about alternative or complementary methods that your doctor hasn’t mentioned to treat your cancer or relieve symptoms. These methods can include vitamins, herbs, and special diets, or other methods such as acupuncture or massage, to name a few.
Complementary methods refer to treatments that are used along with your regular medical care. Alternative treatments are used instead of a doctor’s medical treatment. Although some of these methods might be helpful in relieving symptoms or helping you feel better, many have not been proven to work. Some might even be dangerous.
Be sure to talk to your cancer care team about any method you are thinking about using. They can help you learn what is known (or not known) about the method, which can help you make an informed decision.
Help getting through cancer treatment
Your cancer care team will be your first source of information and support, but there are other resources for help when you need it. Hospital- or clinic-based support services are an important part of your care. These might include nursing or social work services, financial aid, nutritional advice, rehab, or spiritual help.
- What Are Adult Brain and Spinal Cord Tumors? https://www.cancer.org/cancer/brain-spinal-cord-tumors-adults/about/what-are-brain-spinal-tumors.html[↩]
- Lemaire J-J, Nezzar H, Sakka L, et al. Maps of the adult human hypothalamus. Surgical Neurology International. 2013;4(Suppl 3):S156-S163. doi:10.4103/2152-7806.110667. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3654779/[↩]
- Purves D, Augustine GJ, Fitzpatrick D, et al., editors. Neuroscience. 2nd edition. Sunderland (MA): Sinauer Associates; 2001. Neuroglial Cells. Available from: https://www.ncbi.nlm.nih.gov/books/NBK10869/[↩]
- Central Brain Tumor Registry of the United States. http://www.cbtrus.org/[↩][↩]





{kind=link}