
Contents
- What is breast pain
- Breast Awareness
- Types of breast pain
- Breast pain causes
- Breast pain reasons
- Breast pain diagnosis
- Breast pain treatment
What is breast pain
Breast pain also called mastalgia or mastodynia, is any discomfort or pain in the breast. However, breast pain is not a common symptom of breast cancer. Breast pain is thought to be present in up to 69% of women and is most common in women between the ages of 30 and 50.
There are many reasons why your breasts can be painful. Most likely breast pain is from hormonal fluctuations from your periods, pregnancy, puberty, menopause and breastfeeding. Breast pain can also be associated with fibrocystic breast disease. Breast cancer is rarely the cause of breast pain, only accounting for 1.2–6.7% of cases of this symptom.
Studies have shown that almost 50% of women have consulted a health care professional due to breast pain. It is also the most common breast-related symptom which prompted a visit to a health care professional. Amongst which, women who are under the age of 35 are most likely to have a mammogram (x-ray of both breasts) as part of ongoing investigations.
Knowing how your breasts normally look and feel is an important part of breast health.
Breast Awareness
It is important for all women to become aware of how their breasts usually look and feel, so that if there are any changes, you can see a health professional as soon as you notice a difference.
Most breast change are due to benign conditions, but it is of course important to exclude breast cancer, as it is the most commonly diagnosed cancer in women in United States. Breast cancer is the most common cancer in American women, except for skin cancers. Currently, the average risk of a woman in the United States developing breast cancer sometime in her life is about 12% 1. This means there is a 1 in 8 chance she will develop breast cancer. This also means there is a 7 in 8 chance a woman will never have the disease.
There are three steps to being breast aware:
- Get to know the normal look and feel of your breasts
- See your doctor if you notice any unusual changes
- If you are aged 45 to 54, have a mammogram every year
- If you are aged 55 or older, have a mammogram two years or you can choose to continue yearly mammograms
There is no right or wrong way to examine your breasts, but the following tips might help:
- Use a mirror to become familiar with the usual look and shape of your breasts.
- Become familiar with the normal feel of your breasts at different times of the month. You might find this easiest in the shower or bath, lying in bed or getting dressed.
- Feel all the breast tissue, from the collarbone to below the bra line and under the armpit
- Use the pads of your fingers to feel near the surface, and then press more firmly to feel deeper in the breast.
Women of all ages should be familiar with their breasts, but it is more important the older you get, as the risk of breast cancer increases with age.
Changes to look out for include:
- A lump or lumpiness, especially if it is in one breast
- A change to the shape or size of your breast
- Changes to the skin over the breast, such as thickening, dimpling or redness
- An unusual persistent pain, particularly if it is in one breast
- Changes to the nipple, such as inversion (turning inwards), crusting or redness
- Nipple discharge
If you notice any of these changes, or any other breast problems you are concerned about, you should see a doctor as soon as possible. Be reassured that most breast changes are not due to cancer, but it is important to detect breast cancer as early as possible if it is present.
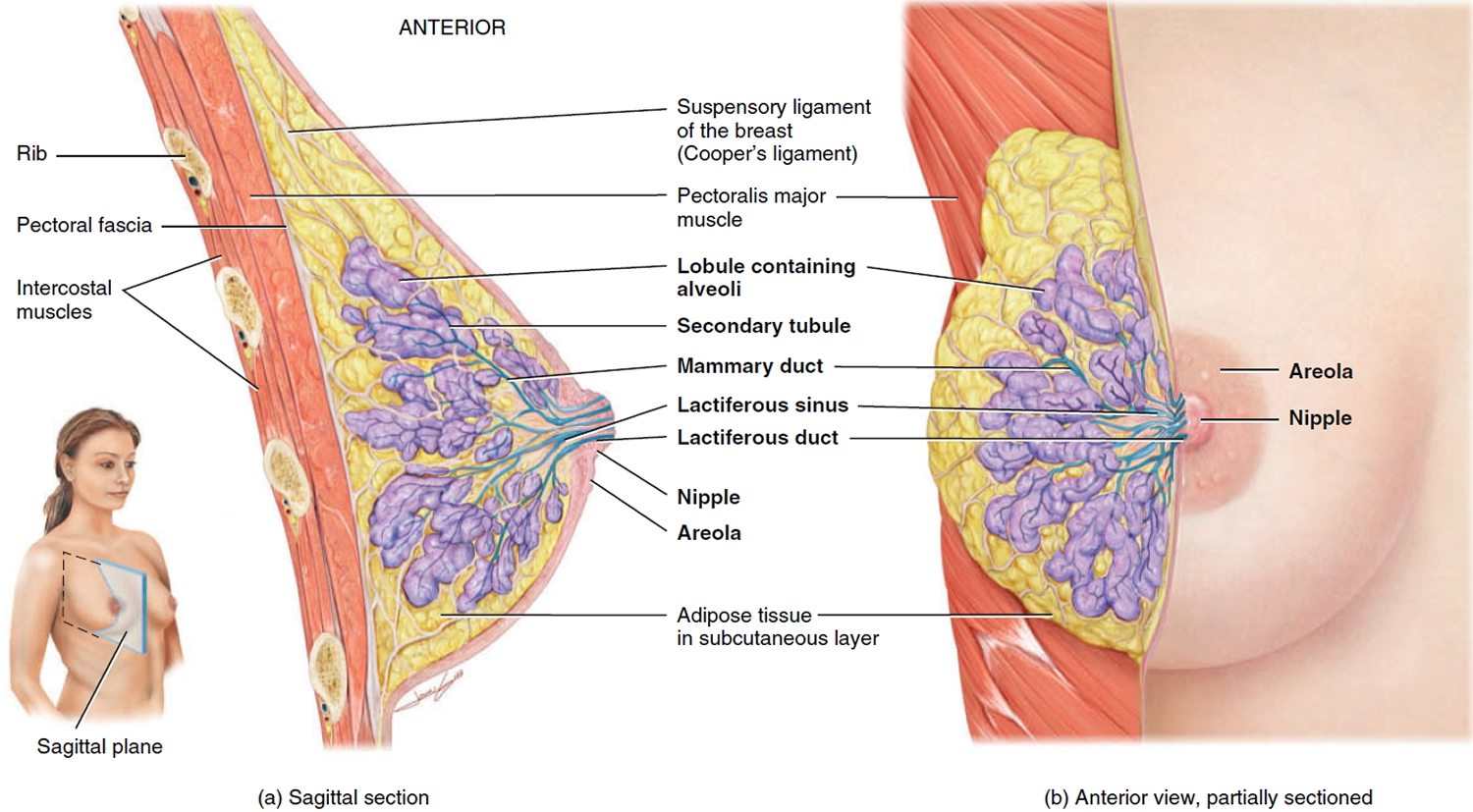
Figure 1. Normal breast (female)
American Cancer Society Recommendations for the Early Detection of Breast Cancer
The American Cancer Society has screening guidelines for women at average risk of breast cancer, and for those at high risk for breast cancer 2.
The goal of screening tests for breast cancer is to find it before it causes symptoms (like a lump that can be felt). Screening refers to tests and exams used to find a disease in people who don’t have any symptoms. Early detection means finding and diagnosing a disease earlier than if you’d waited for symptoms to start.
Breast cancers found during screening exams are more likely to be smaller and still confined to the breast. The size of a breast cancer and how far it has spread are some of the most important factors in predicting the prognosis (outlook) of a woman with this disease.
These guidelines are for women at average risk for breast cancer. For screening purposes, a woman is considered to be at average risk if she doesn’t have a personal history of breast cancer, a strong family history of breast cancer, or a genetic mutation known to increase risk of breast cancer (such as in a BRCA gene), and has not had chest radiation therapy before the age of 30. (See below for guidelines for women at high risk.)
- Women between 40 and 44 have the option to start screening with a mammogram every year.
- Women 45 to 54 should get mammograms every year.
- Women 55 and older can switch to a mammogram every other year, or they can choose to continue yearly mammograms. Screening should continue as long as a woman is in good health and is expected to live 10 more years or longer.
- All women should understand what to expect when getting a mammogram for breast cancer screening – what the test can and cannot do.
Mammograms
Regular mammograms can help find breast cancer at an early stage, when treatment is most successful. A mammogram can find breast changes that could be cancer years before physical symptoms develop. Results from many decades of research clearly show that women who have regular mammograms are more likely to have breast cancer found early, are less likely to need aggressive treatment like surgery to remove the breast (mastectomy) and chemotherapy, and are more likely to be cured.
Mammograms are not perfect. They miss some cancers. And sometimes a woman will need more tests to find out if something found on a mammogram is or is not cancer. There’s also a small possibility of being diagnosed with a cancer that never would have caused any problems had it not been found during screening. It’s important that women getting mammograms know what to expect and understand the benefits and limitations of screening.
Clinical breast exam and breast self-exam
Research has not shown a clear benefit of regular physical breast exams done by either a health professional (clinical breast exams) or by yourself (breast self-exams). There is very little evidence that these tests help find breast cancer early when women also get screening mammograms. Most often when breast cancer is detected because of symptoms (such as a lump), a woman discovers the symptom during usual activities such as bathing or dressing. Women should be familiar with how their breasts normally look and feel and report any changes to a health care provider right away.
American Cancer Society screening recommendations for women at high risk
Women who are at high risk for breast cancer based on certain factors should get an MRI and a mammogram every year, typically starting at age 30. This includes women who:
- Have a lifetime risk of breast cancer of about 20% to 25% or greater, according to risk assessment tools that are based mainly on family history (see below)
- Have a known BRCA1 or BRCA2 gene mutation (based on having had genetic testing)
- Have a first-degree relative (parent, brother, sister, or child) with a BRCA1 or BRCA2 gene mutation, and have not had genetic testing themselves
- Had radiation therapy to the chest when they were between the ages of 10 and 30 years
- Have Li-Fraumeni syndrome, Cowden syndrome, or Bannayan-Riley-Ruvalcaba syndrome, or have first-degree relatives with one of these syndromes
The American Cancer Society recommends against MRI screening for women whose lifetime risk of breast cancer is less than 15%.
There’s not enough evidence to make a recommendation for or against yearly MRI screening for women who have a higher lifetime risk based on certain factors , such as:
- Having a personal history of breast cancer, ductal carcinoma in situ (DCIS), lobular carcinoma in situ (LCIS), atypical ductal hyperplasia (ADH), or atypical lobular hyperplasia (ALH)
- Having “extremely” or “heterogeneously” dense breasts as seen on a mammogram
If MRI is used, it should be in addition to, not instead of, a screening mammogram. This is because although an MRI is more likely to detect cancer than a mammogram, it may still miss some cancers that a mammogram would detect.
Most women at high risk should begin screening with MRI and mammograms when they are 30 and continue for as long as they are in good health. But a woman at high risk should make the decision to start with her health care providers, taking into account her personal circumstances and preferences.
Types of breast pain
There are two main types of true breast pain – cyclical and non-cyclical breast pain. Pain that is felt in the breast can also originate from elsewhere in the body, for example the chest wall. This causes referred pain which is felt in the breast. If you are experiencing any sort of breast pain talk to a health professional about it, especially if it is severe or affecting your daily life. For example, if it is interfering with physical, sexual, social or work-related activities.
Breast pain is usually linked to your periods (cyclical breast pain)
Cyclical breast pain is linked to the menstrual cycle and fluctuating hormone levels during the cycle. Many women have some breast discomfort for a few days before their period. However for some women this can be more severe and/or prolonged where the pain develops for one to two weeks before a period. This then lessens and settles during the period. Approximately two thirds of women with breast pain have this type of pain.
Symptoms of breast pain caused by periods (cyclical breast pain):
- dull, heavy or aching pain – from mild to very bad
- pain that begins up to 2 weeks before a period, gets worse and then goes away when the period ends
- usually (but not always) affects both breasts and usually involves the upper outer breast area radiating to the armpit
- occurs in premenopausal women
- typically affects women in their 30s-40s
- can be spread over both breasts, but may be more severe in one breast
- is often described as ‘dull’, ‘heavy’ and ‘achy’
- usually settles during pregnancy and menopause.
How to ease the pain yourself
You can:
- Take acetaminophen or ibuprofen, or rub painkilling gel on your breasts
- There is also evidence that topical NSAIDs (such as diclofenac gel) are of benefit in both types of breast pain as well as chest wall pain and have very few side effects.
- Use heat or ice on the breast
- Wear a properly fitted bra during the day and a soft bra to sleep in
There is no good evidence to show that reducing the amount of fat, caffeine, or chocolate in your diet helps reduce breast pain. Vitamin E, thiamine, magnesium, and evening primrose oil are not harmful, but most studies have not shown any benefit. Talk to your doctor or nurse before starting any medicine or supplement.
Certain birth control pills may help ease breast pain. Ask your health care provider if this therapy is right for you.
Breast pain not linked to periods (non-cyclical breast pain)
Non-cyclical breast pain:
- is not associated with the menstrual cycle
- can be either constant or intermittent (comes and goes)
- affects approximately one third of women with breast pain
- usually affects women in their 40s-50s
- tends to be one-sided and localized within one section of the breast
- is often described as ‘burning’, ‘drawing’, ‘achy’ and ‘sore’.
Sometimes breast pain is caused by:
- injuries or sprains to the neck, shoulder or back – these can also be felt as breast pain
- medicines like the contraceptive pill and some antidepressants – check the side effects in the packet’s information leaflet
- conditions like mastitis or a breast abscess – these can cause breast pain along with other symptoms
- pregnancy – breast pain can be an early sign
Chest wall/musculoskeletal pain
The nerves that supply sensation to the breast leave the spinal cord at the upper part of the thoracic spine, run around the outside of the chest wall and then up into the breasts. Therefore irritation of these nerves anywhere along their course can lead to pain that is felt in the breast or nipple. Causes include shingles, costochondritis, and pneumonia.
Chest wall pain tends to be:
- one-sided
- brought on by activity
- experienced at the extremities of the breast
- reproduced by pressure on a specific area of the chest wall.
Breast pain menopause
Hormone changes during the menopause can cause breast pain. Once the menopause is over (you’ve had 12 months without a period) the pain should not return.
Breast pain during pregnancy
For women who have a regular monthly menstrual cycle, the earliest and most reliable sign of pregnancy is a missed period. Women who are pregnant sometimes have a very light period, losing only a little blood.
A positive pregnancy test result is almost certainly correct. A negative result is less reliable. If you get a negative pregnancy test result and still think that you may be pregnant, wait a week and try again. See your doctor if you get a negative result after a second pregnancy test but your period hasn’t arrived.
All pregnancy tests detect the hormone human chorionic gonadotrophin (hCG), which starts to be produced around six days after fertilisation.
Most pregnancy tests come in a box that contains one or two long sticks. You pee on the stick and the result appears on the stick after a few minutes. All tests are slightly different, so always check the instructions.
When you can do a pregnancy test
You can carry out most pregnancy tests from the first day of a missed period. If you don’t know when your next period is due, do the test at least 21 days after you last had unprotected sex.
Some very sensitive pregnancy tests can be used even before you miss a period, from as early as eight days after conception.
You can do a pregnancy test on a sample of urine collected at any time of the day. It doesn’t have to be in the morning.
Some of the other early pregnancy signs and symptoms are listed below. Every woman is different and not all women will notice all of these symptoms.
Breast pain or breast soreness in early pregnancy
Your breasts may become larger and feel tender, just as they might do before your period. They may also tingle. The veins may be more visible, and the nipples may darken and stand out.
Feeling sick during pregnancy
You may feel sick and nauseous, and/or vomit. This is commonly known as morning sickness, but it can happen at any time of the day or night.
For most women who have morning sickness, the symptoms start around six weeks after their last period.
If you’re being sick all the time and can’t keep anything down, contact your doctor. The pregnancy condition hyperemesis gravidarum is a serious condition that causes severe vomiting and needs treatment.
Peeing more often suggests pregnancy
You may feel the need to pee (urinate) more often than usual, including during the night.
Other signs of pregnancy that you may notice are:
- constipation
- an increased vaginal discharge without any soreness or irritation
Strange tastes, smells and cravings
During early pregnancy, you may find that your senses are heightened and that some foods or drinks you previously enjoyed become repellent. You might notice:
- a strange taste in your mouth, which many women describe as metallic
- that you crave new foods
- that you lose interest in certain foods or drinks that you previously enjoyed – such as tea, coffee or fatty food
- that you lose interest in tobacco
- that you have a more sensitive sense of smell than usual – for example, to the smell of food or cooking
Breast cancer symptoms pain
Early breast cancer usually does not cause symptoms. This is why regular breast exams are important.
The most common symptom of breast cancer is a new lump or mass. A painless, hard mass that has irregular edges is more likely to be cancer, but breast cancers can be tender, soft, or rounded. They can even be painful. For this reason, it is important to have any new breast mass, lump, or breast change checked by a health care professional experienced in diagnosing breast diseases.
As the cancer grows, symptoms may include:
- Swelling of all or part of a breast (even if no distinct lump is felt)
- Skin irritation or dimpling (sometimes looking like an orange peel)
- Breast or nipple pain
- Nipple retraction (turning inward)
- Redness, scaliness, or thickening of the nipple or breast skin — for example, you may have redness, dimpling, or puckering that looks like the skin of an orange
- Nipple discharge (other than breast milk) — may be bloody, clear to yellow, green, and look like pus
Men can get breast cancer, too. Symptoms include breast lump and breast pain and tenderness.
Symptoms of advanced breast cancer may include:
- Bone pain
- Breast pain or discomfort
- Skin ulcers
- Swelling of in the armpit (next to the breast with cancer)
- Weight loss
Sometimes a breast cancer can spread to lymph nodes under the arm or around the collar bone and cause a lump or swelling there, even before the original tumor in the breast is large enough to be felt. Swollen lymph nodes should also be checked by a health care provider.
Although any of these symptoms can be caused by things other than breast cancer, if you have them, they should be reported to a health care professional so that the cause can be found.
Because mammograms do not find every breast cancer, it is important for you to be aware of changes in your breasts and to know the signs and symptoms of breast cancer.
See a doctor about breast pain if:
- it’s not improving or painkillers aren’t helping
- you have persistent, unexplained breast pain
- you have a very high temperature or feel hot and shivery
- any part of your breast is red, hot or swollen
- you have signs of a breast infection, including local redness, pus, or fever
- there’s a history of breast cancer in your family
- you have any signs of pregnancy – you could do a pregnancy test first
Ask for an urgent appointment if:
- there’s a hard lump in your breast that doesn’t move around
- you noticed a new lump with the pain that does not go away after your menstrual period
- you get nipple discharge, which may be streaked with blood
- one or both breasts change shape
- the skin on your breast is dimpled (like orange peel)
- you have a rash on or around the nipple, or the nipple has sunk into the breast
These can be signs of something more serious.
Breast pain causes
Some amount of breast tenderness is normal. The discomfort may be caused by hormone changes from:
- Menopause (unless a woman is taking hormone replacement therapy)
- Menstruation and premenstrual syndrome (PMS)
- Pregnancy — breast tenderness tends to be more common during the first trimester and in women who become pregnant at a young age
- Puberty in both girls and boys
Soon after having a baby, a woman’s breasts may become swollen with milk. This can be very painful. If you also have an area of redness, call your health care provider.
Breastfeeding itself may also cause breast pain.
Fibrocystic breast changes are a common cause of breast pain. Fibrocystic breast tissue contains lumps that tend to be more tender just before your menstrual period.
Certain medications may also cause breast pain, including:
- Anadrol
- Chlorpromazine
- Diuretics
- Digitalis preparations
- Methyldopa (Aldomet)
- Spironolactone (Aldactone)
Shingles can lead to pain in the breast if the painful blistering rash appears on the skin over one of your breasts.
Breast pain reasons
Breast pain caused by cyclical hormonal changes due to menstrual cycle
Breast pain associated with the hormonal changes of the menstrual cycle is usually cyclical in nature and varies with the time of the month. One third of women may, however, have noncyclical pain (not related to the menstrual cycle) which is less responsive to treatment.
Physiological breast pain typically presents in the premenstrual period (usually 1 week prior to onset of menses). It most frequently affects both breasts and is usually worse in the upper outer quadrant of the breasts. This type of breast pain is also typically associated with fibrocystic changes. Fibrocystic changes of the breast are non-cancerous tumours caused by hormonal changes during the menstrual cycle and usually resolve after menopause (the cessation of periods for 2 years or more occurring at an average age of 51).
Breast pain caused by hormonal therapies/drug side effects
Breast pain is one of the most frequently encountered side effects of hormonal therapies such as the oral contraceptive pill in women of reproductive age and hormonal replacement therapy in menopausal women. Other commonly encountered side effects of hormonal therapy include unwanted bleeding, headaches, pimple break-outs, decrease in sex drive and weight changes.
Theophylline (sold, for example, as Aminophylline and Nuelin), a drug sometimes used for the treatment of long-term asthma, may also rarely cause breast discomfort/pain. In addition, spironolactone (for example, sold under the trade names Aldactone and Spiractin), which is a drug used in people suffering from heart failure, can also cause gynaecomastia (breast enlargement) in males and breast pain in females.
Breast pain caused by breast diseases
Mammary duct ectasia
Mammary duct ectasia is a condition caused by enlargement of the milk ducts present in breasts (see Lactiferous duct in Figure 1 above). It may cause you to experience fever, breast pain/ tenderness and nipple discharge.
Mammary duct ectasia is most common amongst women between 40 and 50 years of age and may sometimes not cause any symptoms. Mammary duct ectasia usually requires no treatment and is not a risk factor for breast cancer.
Mastitis
Mastitis refers to inflammation of the breast which is caused mainly by milk stasis (stagnant milk) or infections. Milk being stagnant is usually the initial cause of mastitis which can then progress to an infection. Infections of the breast such as mastitis and formation of abscesses (collections of pus) within breast tissue are common among mothers who are breastfeeding. It is most common in the first month of breastfeeding and is usually caused by obstruction of the milk ducts leading to milk stasis and hence increasing the risk of infections occurring.
During the process of lactation (production of milk by the breasts), the nipple and surrounding skin often swell up until the nipple is conditioned to frequent suckling by the baby. This swelling may block milk flow and thus increasing the risk of infection by bacteria such as Staphylococcus aureus which is normally present on the skin. Candida (a type of fungus) infections may also cause mastitis following the use of antibiotics. Mastitis usually causes fever as well as pain, redness and swelling of the affected breast. The presence of a lump indicates abscess formation which would normally require surgical drainage. The treatment of mastitis usually involves antibiotics with surgical drainage of abscesses if they are present.
Breast cancer
The frequency of breast cancer in women presenting with breast pain is very low (1.2–6.7%). However, breast cancer is a serious condition which should always be ruled out.
In particular, inflammatory breast cancer (a sub-type of breast cancer) may present with a red, inflamed and painful breast. The skin may also appear dimpled or pitted like an orange peel (peau d’orange). Inflammatory breast cancer is a rare form of aggressive breast cancer that spreads along and blocks the lymph vessels in the skin of the breast. When the lymph vessels become blocked, the breast becomes red and inflamed. If there is any suspicion of breast cancer, you should consult a doctor so that he or she can carry out further investigations such as a mammogram, breast ultrasound or breast tissue biopsy (small sample of tissue removed to be studied under a microscope).
Male breast cancer is very rare and makes up less than 1% of all breast cancers. The most common symptom of male breast cancer is a breast lump, followed by breast pain and nipple discharge. Men who suffer from breast pain (mastalgia) should always consult a doctor to rule out the possibility of breast cancer.
Breast pain caused by other medical conditions
Muscular, skeletal and mechanical problems
Muscular strain or injury may cause pain in the chest wall which can mimic breast pain. This is most commonly due to strain or injury to the pectoralis major muscle (muscle in the front of the chest) which is related to repeated use in activities such as boat-rowing or shoveling.
Spinal injury, especially in the neck and thoracic (part of body between neck and abdomen) regions, may also result in referred pain to the chest wall and mimic breast pain. In addition, a disease known as ankylosing spondylitis, a chronic inflammatory disease of the skeleton typically affecting people between 20 and 30 years of age, may also involve the chest wall and present like breast pain.
Tietze’s syndrome is another condition which can be mistaken for breast pain. It can cause sudden or long term pain and a swelling about 4 cm from the edge of the breast bone. It is due to enlargement of the cartilage around the breast bone.
Mechanical problems such as bra problems, weight changes and having large breasts may also result in breast pain.
Chest wall/musculoskeletal pain
The nerves that supply sensation to the breast leave the spinal cord at the upper part of the thoracic spine, run around the outside of the chest wall and then up into the breasts. Therefore irritation of these nerves anywhere along their course can lead to pain that is felt in the breast or nipple. Causes include shingles, costochondritis, and pneumonia.
Chest wall pain tends to be:
- one-sided
- brought on by activity
- experienced at the extremities of the breast
- reproduced by pressure on a specific area of the chest wall.
Cardiovascular conditions
It is also possible to mistake a heart attack for breast pain. The symptoms which may be experienced by an individual suffering from a heart attack include sudden central chest pain which may spread to the left arm, increased sweating, shortness of breath and racing heart beat. This is a serious condition which requires urgent treatment. A doctor should be consulted urgently if you experience sudden central chest pain.
- If you have new or unexplained chest pain or suspect you’re having a heart attack, call for emergency medical help immediately.
- The warning signs of heart attack can be varied and may not always be sudden or severe.
- All chest pain is considered to be heart-related until proven otherwise!
If you have any of the symptoms above, call your local emergency number immediately and ask for an ambulance.
If you feel chest pain but don’t have any of the symptoms above, it’s still a good idea to see a doctor as soon as possible, so your heart health can be checked.
It’s better to be safe than sorry.
People having a heart attack may have just one of these symptoms, or a combination of them. They can come on suddenly or develop over minutes and get progressively worse. Symptoms usually last for at least 10 minutes.
Warning signs of a heart attack could include:
- discomfort or pain in the center of your chest – a heaviness, tightness or pressure, like an elephant sitting on your chest, or a belt tightening around your chest, or a bad case of indigestion
- discomfort in the arms, shoulder, neck, jaw or back
- other problems such as:
- a choking feeling in your throat
- your arms feeling heavy or useless
- feeling short of breath
- feeling nauseated
- having a cold sweat
- feeling dizzy or light-headed.
Chest pain symptoms can range from a mild sensation, to a severe pain. All chest pain is considered to be heart-related until proven otherwise.
Heart attacks are more common in older people than younger people, but they can occur in people of any age.
Approximately 1 percent of primary care office visits are for chest pain, and 1.5 percent of these patients will have unstable angina or acute myocardial infarction (heart attack) 3.
Cardiac disease is the leading cause of death in the United States, yet only 1.5 percent of patients presenting to a primary care office with chest pain will have unstable angina or an acute myocardial infarction (heart attack) 4.
The most common causes of chest pain in the primary care population include 4:
- Chest wall pain (20 percent);
- Reflux esophagitis (13 percent);
- Costochondritis (13 percent).
Although in practice, costochondritis is often included in the chest wall pain category. Other considerations include pulmonary (e.g., pneumonia, pulmonary embolism), gastrointestinal (e.g., gastroesophageal reflux disease [GERD]), and psychological (e.g., anxiety, panic disorder) etiologies, and cardiovascular disorders (e.g., acute congestive heart failure, acute thoracic aortic dissection). Table 1 lists the differential diagnosis of chest pain.
Table 1. Differential Diagnosis of Chest Pain
| Diagnosis | Clinical findings |
| Acute myocardial infarction | Chest pain radiates to both arms |
| Third heart sound on auscultation | |
| Hypotension | |
| Chest wall pain | At least two of the following findings: localized muscle tension; stinging pain; pain reproducible by palpation; absence of cough |
| Gastroesophageal reflux disease | Burning retrosternal pain, acid regurgitation, sour or bitter taste in the mouth; one-week trial of high-dose proton pump inhibitor relieves symptoms |
| Panic disorder/anxiety state | Single question: In the past four weeks, have you had an anxiety attack (suddenly feeling fear or panic)? |
| Pericarditis | Clinical triad of pleuritic chest pain (increases with inspiration or when reclining, and is lessened by leaning forward), pericardial friction rub, and electrocardiographic changes (diffuse ST segment elevation and PR interval depression without T wave inversion) |
| Pneumonia | Egophony |
| Dullness to percussion | |
| Fever | |
| Clinical impression | |
| Heart failure | Pulmonary edema on chest radiography |
| Clinical impression/judgment | |
| History of heart failure | |
| History of acute myocardial infarction | |
| Pulmonary embolism | High pretest probability based on Wells criteria |
| Moderate pretest probability based on Wells criteria | |
| Low pretest probability based on Wells criteria | |
| Acute thoracic aortic dissection | Acute chest or back pain and a pulse differential in the upper extremities |
Abdominal/gastrointestinal conditions
Gastrointestinal conditions such as gallbladder disease, stomach ulcers and pancreatitis (inflammation of the pancreas), among others, may cause chest pain and be mistaken for breast pain. At your doctor’s office, additional investigations such as abdominal ultrasound or gastro-oesophageal endoscopy may be carried out if gastrointestinal diseases are suspected.
Breast pain diagnosis
Your doctor may ask you a series of questions to determine the cause of your breast pain, including:
- Location of the pain;
- When the pain started;
- What is the pain like (sharp, dull, throbbing, radiating);
- How bad is the pain;
- What are the factors which relieve or worsen the pain;
- Timing of the pain (cyclical vs. non-cyclical, relationship with menstrual cycle);
- Associated breast symptoms (lump, nipple discharge, redness);
- Other symptoms which you may experience including fever, weight loss and loss of appetite;
- History of injury to the chest or repetitive use of the chest wall muscles;
- Menstrual history (last normal menstrual period, regularity of menstrual cycle, length of your cycle, painful periods, bleeding in between periods and pre-menstrual symptoms);
- Drug history (use of hormonal therapy, theophylline or other drugs which can cause breast pain); and
- Family history (breast cancer in particular).
Your health care provider will perform a breast examination
It is also likely that your doctor will need to examine your breasts and the surrounding areas including the axilla (under the arms). He/she would be looking for signs such as:
- Skin changes (symmetry and contour, scars, skin retraction, dimpling, swellings, presence of ulcers and redness);
- Enlarged axillary (under the arms) or supraclavicular (above the collar bones) lymph nodes;
- Breast lumps; or
- Nipple discharge.
Investigations
At the doctor’s office, additional investigations such as mammogram or ultrasound and blood tests may be required to determine the cause of breast pain or determine the type of treatment required.
Your health care provider may schedule a follow-up visit if your symptoms have not gone away in a given period of time. You may be referred to a specialist.
Mammography
Most women who present with breast pain are under the age of 35 and therefore the role of mammography is limited. This is because mammography is less accurate in women under the age of 35 due to the breast tissue being denser in young women.
- Mammography is usually useful in certain groups of women who suffer from breast pain:
- Women older than 35 years who have not had a recent screening mammogram;
- Women younger than 35 years with abnormal findings on physical examination; or
- Women with a strong family history of breast cancer.
Ultrasound
Ultrasound is useful in detecting lumps at the site of the pain if present. It may also be used in locating abscesses if surgical drainage is required.
Breast pain treatment
Before commencing treatment for breast pain, breast diseases and other general medical conditions should be ruled out. It is important to let the doctor know about your current medications to rule out drug side effects as a cause of breast pain.
If it is found that your breast pain is due to a medication you are taking, hormonal therapy (oral contraceptive pill or hormone replacement therapy) should be decreased or discontinued if possible.
Should there be normal findings on clinical and imaging studies (that is, the breast pain is due to normal menstrual hormonal changes), the following measures may be adopted to manage physiological breast pain.
Conservative treatment
Reassurance
Simple reassurance by the doctor that the pain is unlikely to be due to breast cancer has been proven to provide adequate relief for most women. You should, however, consult your doctor again in 6 months time should the pain persist.
Mechanical support
Precise fitting of a brassiere will provide added support for women who have large breasts and may provide pain relief. The use of a sports bra during exercise or excessive activity has been shown to provide pain reduction and superior support for the breast as measured in a study conducted by the Institute of Sport.
Nutritional modifications
A low-fat diet has also been found to significantly reduce breast pain in various studies but it is thought that to derive benefit from a low-fat diet, women must decrease fat intake to less than 20% of their total daily caloric intake.
Caffeine restriction or elimination may also result in relief of breast pain. This includes avoidance of caffeine containing foods such as coffee, tea, colas and chocolate. Although the effectiveness of caffeine restriction has not been proven to be effective, it is worth considering if you have high intake of caffeine or are suffering from cyclical breast pain. It may, however, take up to 6 months before relief of symptoms are experienced after caffeine is eliminated from your diet.
These treatments are not recommended due to lack of evidence:
- evening primrose oil
- vitamin A, B6 or E
- narcotics such as codeine, morphine
- diuretics
Medications
Paracetamol or non-steroidal inflammatory drug (NSAID)
Simple pain-relievers such as paracetamol and NSAIDs such as ibuprofen may be considered for pain relief although there are limited studies which investigate their effectiveness. The common side effects of oral NSAIDs include inflammation of the stomach wall, worsening of pre-existing asthma and sudden kidney failure.
Topical NSAIDs such as diclofenac gel (used on the skin of affected areas) have also been shown to result in significant pain reduction in both cyclical and non-cyclical types of breast pain as well as chest wall pain with minimal side effects in a study.
If you have ongoing pain despite these measures you should consult your health professional again to discuss referral to a specialist. There are other hormonal medications which have been found to be effective in the treatment of breast pain, but they also have some significant side effects so are only prescribed by specialists (see below).
Danazol
Danazol (sold as, for example, Danocrine) is an androgen (male sex hormone) that is effective in relieving breast pain in more than 90% of cases and is the only US FDA (Food and Drug Administration) approved drug for the treatment of cyclical breast pain secondary to hormonal changes as a result of the menstrual cycle. Side effects of danazol include increased hair growth, weight gain, voice change, increased sex drive, pain during sexual intercourse, headaches, nausea, menstrual irregularities, decreased breast size and pimple break-outs.
Selective oestrogen receptor modulators
Tamoxifen (sold as Tamosin, Genox and others) belongs to the drug class known as selective oestrogen receptor modulators which may be used for patients with severe breast pain or breast pain that is not responsive to other treatments. Tamoxifen is a drug which is more regularly used as treatment for people suffering from certain types of breast cancer.
However, tamoxifen has potentially serious side effects which includes deep venous thrombosis (blood clots developing in veins of the body most commonly in the legs and pelvic region) and an increased risk for endometrial cancer (cancer of the womb lining). Common less severe side effects include hot flushes, nausea, menstrual irregularity, dryness of the vaginal walls and weight gain.
Other agents
Bromocriptine (sold as, for example, Parlodel and Cycloset) is a long-acting dopaminergic drug that reduces prolactin (a hormone in the body which controls breast milk production) secretion by the pituitary gland (an important gland present in the brain that releases many hormones). It has been proven to improve breast pain in many women but is not as effective as danazol.
Goserelin (sold as Zoladex and other trade names) which belongs to the class of drugs known as gonadotropin-releasing hormone agonists has also been reported to be effective in up to 80% of women suffering from cyclical breast pain but may cause reduced bone density thus increasing the risk of osteoporosis with long-term use.
- How Common Is Breast Cancer? https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html[↩]
- American Cancer Society Recommendations for the Early Detection of Breast Cancer. https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html[↩]
- Hsiao CJ, Cherry DK, Beatty PC, Rechtsteiner EA. National ambulatory medical care survey: 2007 summary. Natl Health Stat Report. 2010;(27):1–32.[↩]
- Klinkman MS, Stevens D, Gorenflo DW; Michigan Research Network. Episodes of care for chest pain: a preliminary report from MIRNET. J Fam Pract. 1994;38(4):345–352.[↩][↩]
- Outpatient Diagnosis of Acute Chest Pain in Adults. Am Fam Physician. 2013 Feb 1;87(3):177-182. https://www.aafp.org/afp/2013/0201/p177.html[↩]
- Panju AA, Hemmelgarn BR, Guyatt GH, Simel DL. The rational clinical examination. Is this patient having a myocardial infarction? JAMA. 1998;280(14):1256–1263.[↩]
- Bösner S, Becker A, Hani MA, et al. Chest wall syndrome in primary care patients with chest pain: presentation, associated features and diagnosis. Fam Pract. 2010;27(4):363–369.[↩]
- Zimmerman J. Validation of a brief inventory for diagnosis and monitoring of symptomatic gastrooesophageal reflux. Scand J Gastroenterol. 2004;39(3):212–216.[↩]
- Wang WH, Huang JQ, Zheng GF, et al. Is proton pump inhibitor testing an effective approach to diagnose gastroesophageal reflux disease in patients with noncardiac chest pain?: a meta-analysis. Arch Intern Med. 2005;165(11):1222–1228.[↩]
- Löwe B, Gräfe K, Zipfel S, et al. Detecting panic disorder in medical and psychosomatic outpatients: comparative validation of the Hospital Anxiety and Depression Scale, the Patient Health Questionnaire, a screening question, and physicians’ diagnosis. J Psychosom Res. 2003;55(6):515–519.[↩]
- Imazio M, Brucato A, Cemin R, et al.; CORP (COlchicine for Recurrent Pericarditis) Investigators. Colchicine for recurrent pericarditis (CORP): a randomized trial. Ann Intern Med. 2011;155(7):409–414.[↩]
- Maisch B, Seferović PM, Ristić AD, et al.; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases executive summary. Eur Heart J. 2004;25(7):587–610.[↩]
- Diehr P, Wood RW, Bushyhead J, Krueger L, Wolcott B, Tompkins RK. Prediction of pneumonia in outpatients with acute cough–a statistical approach. J Chronic Dis. 1984;37(3):215–225.[↩]
- Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 1997;278(17):1440–1445.[↩]
- Wang CS, FitzGerald JM, Schulzer M, Mak E, Ayas NT. Does this dyspneic patient in the emergency department have congestive heart failure? JAMA. 2005;294(15):1944–1956.[↩]
- Wells PS, Anderson DR, Rodger M, et al. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001;135(2):98–107.[↩]
- Tamariz LJ, Eng J, Segal JB, et al. Usefulness of clinical prediction rules for the diagnosis of venous thromboembolism: a systematic review. Am J Med. 2004;117(9):676–684.[↩]
- von Kodolitsch Y, Schwartz AG, Nienaber CA. Clinical prediction of acute aortic dissection. Arch Intern Med. 2000;160(19):2977–2982.[↩]





{kind=link}