Contents
What to do for a burn
A burn is damage to your body’s tissues caused by heat, chemicals, electricity, sunlight, or radiation. Scalds from hot liquids and steam, building fires and flammable liquids and gases are the most common causes of burns. Another kind is an inhalation injury, caused by breathing smoke.
People with severe burns often require treatment at specialized burn centers. They may need skin grafts to cover large wounds or to minimize scarring with deep wounds. And they may need emotional support and months of follow-up care, such as physical therapy.
Burn Statistics 2005-2014 1
- Survival Rate: 96.8%
- Gender: 68% Male, 32% Female
- Ethnicity: 59% Caucasian, 20% African-American, 14% Hispanic, 7% Other
- Admission Cause: 43% Fire/Flame, 34% Scald, 9% Contact, 4% Electrical, 3% Chemical, 7% Other
- Place of Occurrence: 73% Home, 8% Occupational, 5% Street/Highway, 5% Recreational/Sport, 9% Other
Each year in the United States, about a half-million people seek medical attention for burns and 40,000 are hospitalized 2 and approximately 4,000 people die each year from fire and burn injuries 3. Burns can be caused by scalding from hot liquids or cooking oils, contact with flames, or from overexposure to the sun. Burn also can be electrical (e.g., when a child bites an electrical cord) or chemical (e.g., resulting from swallowing or spilling bleach on your skin). Household burns lead to nearly 7 of 10 admissions to burn centers. The good news is that the number of deaths from severe burns has dropped by more than half over the past 4 decades, in large part because of treatments developed through research.
There are three degrees of burns:
- First-degree burns damage only the outer layer of skin (the epidermis). It may cause redness, swelling and pain. It usually heals with first-aid measures within several days to a week. Sunburn is a classic example.
- Second-degree burns: This type of burn affects both the epidermis and the second layer of skin (dermis). It may cause red, white or splotchy skin, pain, and swelling. And the wound often looks wet or moist. Blisters may develop, and pain can be severe. Deep second-degree burns can cause scarring (see Figure 3).
- Third-degree (most serious) burns damage or destroy the entire thickness of the skin, permanently destroying it and the tissue that’s underneath. This burn reaches into the fat layer beneath the skin (see Figure 4). Burned areas may be charred black or white. The skin may look waxy or leathery. Third-degree burns can destroy nerves, causing numbness. A person with this type of burn may also have difficulty breathing or experience smoke inhalation or carbon monoxide poisoning. Third-degree burns usually require skin grafts for wound closure.
- Fourth-Degree Burns: Fourth-degree burns destroy all skin layers and extend into muscle, tendon, or bone 4.
Anatomy and Skin Function
The skin’s three anatomic layers (i.e., epidermis, dermis, and subcutaneous tissue) have functions that are lost after burn injuries. The epidermis is a barrier to bacteria and moisture loss. After a burn injury, local wound care and fluid management are required. The dermis provides elasticity and protection from mechanical trauma, and it contains blood vessels that supply all skin layers. When the skin is damaged, epidermal cells regenerate from cells deep within the dermal appendages, which is why deep dermal injury causes significant scarring and permanent skin damage 5.
Figure 1. Skin structure

Figure 2. Structure and skin cells of the Epidermis
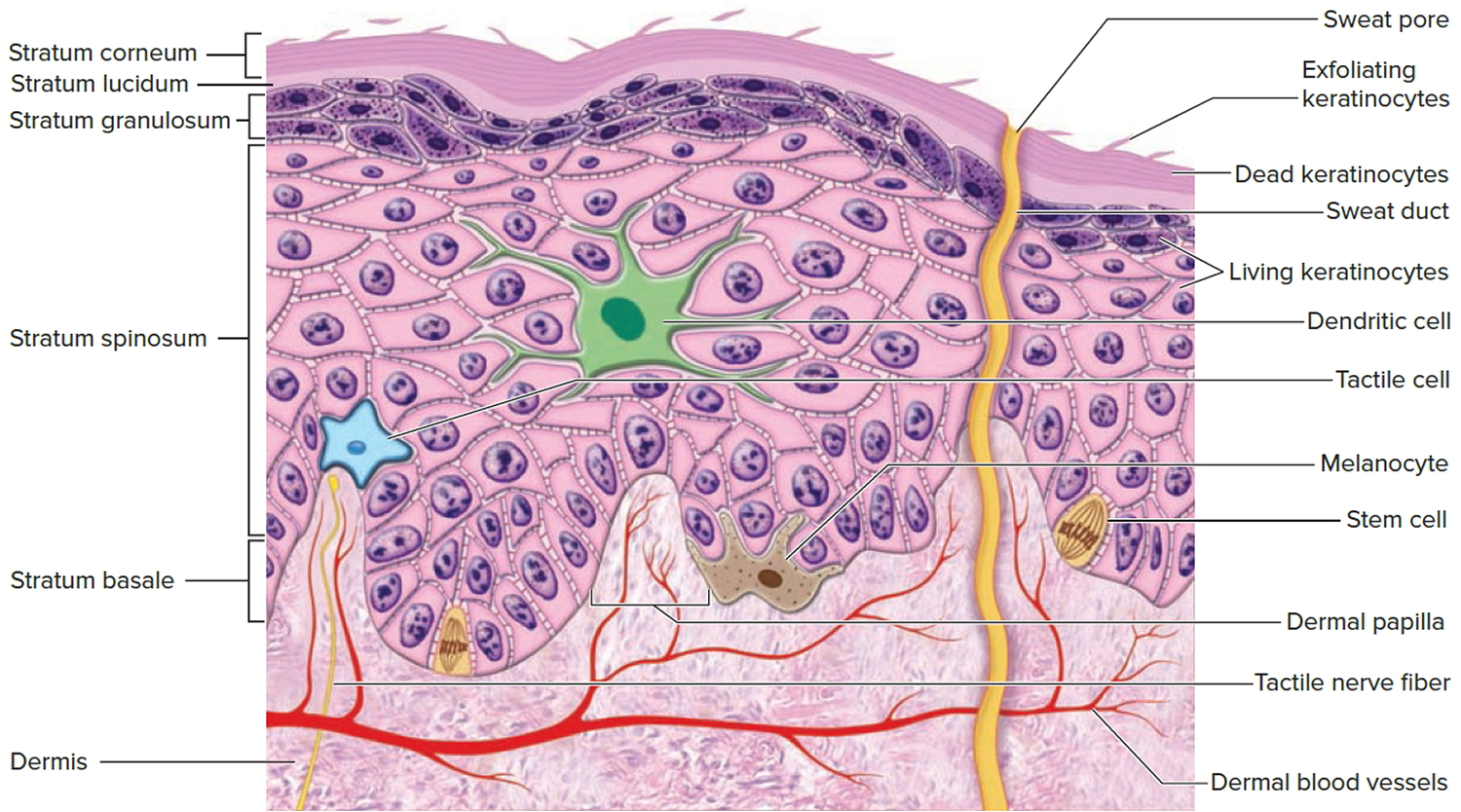
Figure 3. First degree burn

Figure 4. 2nd degree burn

Figure 5. Superficial Partial-Thickness (Superficial Second-Degree) Burns

Figure 6. Deep Partial-Thickness (Deep Second-Degree) Burn

Figure 7. Deep Partial-Thickness (Deep Second-Degree) Burn – face and neck region

Figure 8. 3rd degree burn

Burns can cause swelling, blistering, scarring and, in serious cases, shock, and even death. They also can lead to infections because they damage your skin’s protective barrier. Treatment for burns depends on the cause of the burn, how deep it is, and how much of the body it covers. Antibiotic creams can prevent or treat infections. For more serious burns, treatment may be needed to clean the wound, replace the skin, and make sure the patient has enough fluids and nutrition.
Emergency treatment for third-degree and some second-degree burns may include a blood transfusion and/or extra fluids to help maintain blood pressure. Grafting—placing healthy skin on top of the burn wound—might help promote new skin growth.
Severe burns can lead to widespread inflammation, organ failure, and shock. This sometimes-deadly response can arise a week or two after the initial burn. But doctors can’t tell beforehand which patients might develop this extreme reaction.
You can care for most minor burns at home. If the burn is red and painful with mild swelling or little blistering, then it’s a first-degree or minor second-degree burn.
See a doctor if the burn is dark red and looks glossy with a lot of blistering. These are signs of a deep second-degree burn. Get immediate treatment if the burned skin is dry and leathery, perhaps with white, brown, or black patches. These are signs of third-degree burn.
Burns can become infected with bacteria or other germs if protective layers of skin are lost. Burns can also lead to painful inflammation, as your immune system shifts into gear.
Seek emergency medical assistance for:
- Burns that cover the hands, feet, face, groin, buttocks, a major joint or a large area of the body
- Deep burns, which means burns affecting all layers of the skin and even other tissues
- All burns caused by chemicals or electricity
- Burns that cause white or charred skin – any size
- Difficulty breathing or burns to the airway e.g. facial burns, coughing, a sore throat or difficulty breathing
People at greater risk from the effects of burns, such as children under five years old and pregnant women, should also get medical attention after a burn or scald.
The size and depth of the burn will be assessed and the affected area cleaned before a dressing is applied. In severe cases, skin graft surgery may be recommended.
Minor burns can be cared for at home, but call your doctor if you experience:
- Large blisters
- Signs of infection, such as oozing from the wound, increased pain, redness and swelling
- A burn or blister that doesn’t heal in several weeks
- New, unexplained symptoms
- Significant scarring
Types of burn
Burns are assessed by how seriously your skin is damaged and which layers of skin are affected.
Your skin has three layers:
- the epidermis – the outer layer of skin
- the dermis – the layer of tissue just beneath, which contains blood capillaries, nerve endings, sweat glands and hair follicles
- the subcutaneous fat, or subcutis – the deeper layer of fat and tissue.
There are four main types of burn, which tend to have a different appearance and different symptoms:
- Superficial epidermal burn – where the epidermis is damaged; your skin will be red, slightly swollen and painful, but not blistered
- Superficial partial-thickness (Superficial Second-Degree) burn – where the epidermis and part of the dermis are damaged; your skin will be pale pink and painful, and there may be small blisters
- Deep Partial-Thickness (Deep Second-Degree) Burn – where the epidermis and the dermis are damaged: this type of burn makes your skin turn red and blotchy; your skin may be dry or moist, and become swollen and blistered, and it may be very painful or painless
- Full thickness burn – where all three layers of skin (the epidermis, dermis and subcutis) are damaged; the skin is often burnt away and the tissue underneath may appear pale or blackened, while the remaining skin will be dry and white, brown or black with no blisters, and the texture of the skin may also be leathery or waxy.
- Fourth-Degree Burns: Fourth-degree burns destroy all skin layers and extend into muscle, tendon, or bone 4.
Classification of Burns
Burn depth and size are important factors in determining whether a burn can be classified as minor, and are crucial in dictating the initial steps of burn assessment and management 2. Superficial burns can often be managed on an outpatient basis, whereas full-thickness burns must be evaluated by a specialist for possible excision and grafting. Determination of burn depth can be complicated by the conversion of burns to a higher burn category within the first several days. Conversion occurs when the damaged skin continues to spread and burn depth increases because of thermal injury that did not fully present on initial assessment; therefore, frequent evaluation and reassessment are necessary for all categories of burns 6.
Minor Burn Classification Criteria 7
- Does not cross major joints
- Is not circumferential
- Isolated injury
- May not involve face, hands, perineum, genitalia, or feet
- Partial-thickness burns on less than 5 percent of total body surface area in patients younger than 10 years or older than 50 years
- Partial-thickness burns on less than 10 percent of total body surface area in patients 10 to 50 years of age
Burn size is determined by estimating the percentage of the patient’s body surface area that is covered by partial-thickness and full-thickness burns (Figure 9) 8. First-degree burns are not incorporated into formal estimations of burn size. The Lund-Browder classification can be used for initial assessment of burn size in adults or children. The “rule of nines” diagram is helpful for rapid assessment of burn size, but this method is less accurate than the Lund-Browder classification, especially in children. The hand is often used to measure small burn areas; it correlates to 1 percent of total body surface area. Studies have shown that the adult hand is closer to 0.8 percent of total body surface area, and that a child’s hand is about 1 percent 9.
Figure 9. Burn size estimation
Note: Diagrams to assess the extent of burns. (A) The “rule of nines” divides the body into areas of 9 or 18 percent of total body area. (B) The Lund-Browder classification is more accurate in estimating burn size, especially in children.
[Source 8]Superficial First-Degree Burns
First-degree burns involve only the epidermis; like a sunburn, they are erythematous, painful, and dry (Figure 3). They are most often the result of severe ultraviolet exposure or minor thermal injury. First-degree burns usually heal in five to 10 days 9.
Superficial Partial-Thickness (Superficial Second-Degree) Burns
Second-degree burns involve all of the epidermis and part of the underlying dermis. Superficial partial-thickness burns damage the upper layers of the papillary dermis; they are identified by clear blisters and weeping, wet, erythematous skin, and they blanch painfully when touched (Figures 4 and 5). These burns heal within two weeks and generally do not cause scarring; however, scarring and pigment changes are possible.2,10
Deep Partial-Thickness (Deep Second-Degree) Burns
Deep second-degree burns involve the deeper layers of the dermis (i.e., reticular dermis). They appear white and do not blanch (Figures 6 and 7). These burns do not heal in less than three weeks and often result in scarring and contractures 10.
Full-Thickness (Third-Degree) Burns
Third-degree burns destroy all skin layers, including underlying subcutaneous fat.
- Entire thickness of skin destroyed (into fat)
- Any color (white, black, red, brown), dry, less painful (dermal plexus of nerves destroyed)
- Heal by contraction from wound edges and scar deposition (no epithelium left in middle of wound) over a protracted time course and subject to the following clinical sequelae if not grafted: severe scarring, wound infection and fragile repair prone to recurrent episodes of breakdown.
- Need specialized care to attain definitive wound closure via autologous skin grafting. When surface area of full thickness injury is extensive, special techniques are employed to expand skin grafts in order to achieve maximum wound coverage 10.
Fourth-Degree Burns
Fourth-degree burns destroy all skin layers and extend into muscle, tendon, or bone 4. Need specialized care (skin grafting alone is generally not sufficient).
First aid for burns
Appropriate first aid must be used to treat any burns or scalds as soon as possible. This will limit the amount of damage to your skin.
For minor burns:
- Stop the burning process as soon as possible. This may mean removing the person from the area, dousing flames with water, or smothering flames with a blanket. Don’t put yourself at risk of getting burnt as well.
- Remove the person from the heat source and remove any burned clothing, except clothing imbedded in the burn (don’t move anything that’s stuck to the skin as this could cause more damage).
- Run cool – not cold – running water for at least 10-20 minutes over the burn or hold a clean, cold compress on it until the pain subsides. Do not use ice or iced water. Do not use not butter, any creams or other types of grease.
- Remove jewelry or tight clothing from around burned areas.
- Cover the burn by placing a layer of cling film over it, rather than wrapping it around a limb. A clean plastic bag could also be used for burns on your hand.
- You can also apply antibiotic cream.
- Make sure the person keeps warm – by using a blanket, for example, but take care not to rub it against the burnt area. Keeping warm will prevent hypothermia, where a person’s body temperature drops below 35 °C (95 °F). This is a risk if you are cooling a large burnt area, particularly in young children and elderly people.
- Use painkillers such as paracetamol or ibuprofen to treat any pain
- If the face or eyes are burnt, sit up as much as possible, rather than lying down – this helps to reduce swelling
Seek emergency care for more serious burns and for any burns to the eyes, mouth, hands, and genital areas, even if mild. If the burn covers a large area, get medical attention immediately.
When to go to hospital
Once you have taken these steps, you’ll need to decide whether further medical treatment is necessary. Go to a hospital accident and emergency department for:
- large or deep burns – bigger than the affected person’s hand
- burns of any size that cause white or charred skin
- burns on the face, hands, arms, feet, legs or genitals that cause blisters
- all chemical and electrical burns
Also get medical help straight away if the person with the burn:
- has other injuries that need treating
- is going into shock – signs include cold, clammy skin, sweating, rapid, shallow breathing, and weakness or dizziness
- is pregnant
- is over the age of 60
- is under the age of five
- has a medical condition such as heart, lung or liver disease, or diabetes
- has a weakened immune system (the body’s defence system) – for example, because of HIV or AIDS, or because they’re having chemotherapy for cancer
If someone has breathed in smoke or fumes, they should also seek medical attention. Some symptoms may be delayed, and can include:
- coughing
- a sore throat
- difficulty breathing
- singed nasal hair
- facial burns
Get immediate medical attention if you have any of the following symptoms related to a burn:
- Fever
- Pus-like or foul-smelling drainage
- Excessive swelling
- Redness of the skin
- A blister filled with greenish or brownish fluid
- A burn that doesn’t heal in 10 days to two weeks
Never break blisters from a burn, and remember not to remove clothing stuck to burned skin. If you are helping someone with a serious burn, keep the burned areas elevated to reduce swelling.
In addition, know what to do in case you or your clothing catches fire: stop (don’t run), drop (to the floor, immediately), and roll (cover your face and hands while rolling over to smother the flames).
If you are helping someone else who has been burned, remove the person from danger first, unless doing so puts you in danger as well.
Electrical burns
- DO NOT approach a person who is connected to a high-voltage source (1,000 volts or more) – until you know the power source has been turned off.
Electrical burns may not look serious, but they can be very damaging. Someone who has an electrical burn should seek immediate medical attention at an emergency department.
If the person has been injured by a low-voltage source (up to 220-240 volts) such as a domestic electricity supply, safely switch off the power supply or remove the person from the electrical source using a material that doesn’t conduct electricity, such as a wooden stick or a wooden chair.
Minor electrical burns can be treated with cool (not cold or ice) compresses. After cleansing, a mild antibiotic ointment and bandage may be applied. A tetanus shot is also recommended, especially if the person has not had one in more than 10 years.
For more serious electrical burns:
- Check for breathing. If the person is not breathing, start rescue breathing if you know how.
- Raise burned arms and legs higher than the person’s heart.
- Cover the person with cool, wet cloths. Do not use butter, ointments or any other home remedy. Do not break the blisters or remove burned skin.
Chemical burns
Chemical burns can be very damaging and require immediate medical attention at an emergency department. If possible, find out what chemical caused the burn and tell the healthcare professionals at an emergency department.
If you’re helping someone else, put on appropriate protective clothing and then:
- remove any contaminated clothing on the person
- if the chemical is dry, brush it off their skin
- rinse chemicals off the skin by placing the person in a shower for 15 to 20 minutes. (Be careful to protect your eyes and the eyes of the injured person.)
- wet chemicals should be flushed off affected areas with cool running water for 20 minutes or longer or until emergency help arrives.
- if you or someone else has swallowed a chemical substance or an object that could be harmful (e.g., watch battery) call poison control first and then your local emergency number. It is helpful to know what chemical product has been swallowed. Take it with you to the hospital.
Sunburn
In cases of sunburn, follow the advice below:
- If you notice any signs of sunburn, such as hot, red and painful skin, move into the shade or preferably inside.
- Take a cool bath or shower to cool down the burnt area of skin.
- Apply aftersun lotion to the affected area to moisturize, cool and soothe it. Don’t use greasy or oily products.
- If you have any pain, paracetamol or ibuprofen should help relieve it. Always read the manufacturer’s instructions and do not give aspirin to children under the age of 16.
- Stay hydrated by drinking plenty of water.
- Watch out for signs of heat exhaustion or heatstroke, where the temperature inside your body rises to 37-40 °C (98.6-104 °F) or above. Symptoms include dizziness, a rapid pulse or vomiting.
If a person with heat exhaustion is taken to a cool place quickly, given water to drink and has their clothing loosened, they should start to feel better within half an hour.
If they don’t, they could develop heatstroke. This is a medical emergency and you’ll need to call your local emergency number for an ambulance.
Heat exhaustion is not serious and usually gets better when you cool down.
The signs of heat exhaustion include:
- headache
- dizziness and confusion
- loss of appetite and feeling sick
- excessive sweating and pale, clammy skin
- cramps in the arms, legs and stomach
- fast breathing or pulse
- temperature of 38 °C (100.4 °F) or above
- intense thirst
The symptoms are often the same in adults and children, although children may become floppy and sleepy.
If someone is showing signs of heat exhaustion they need to be cooled down.
Things you can do to cool someone down
Follow these 4 steps:
- Move them to a cool place.
- Get them to lie down and raise their feet slightly.
- Get them to drink plenty of water. Sports or rehydration drinks are OK.
- Cool their skin – spray or sponge them with cool water and fan them. Cold packs around the armpits or neck are good too.
Stay with them until they are better.
They should start to cool down and feel better within 30 minutes.
Call your local emergency number if the person:
- is no better after 30 minutes
- feels hot and dry
- is not sweating even though they are too hot
- has a temperature that’s risen to 40 °C (104 °F) or above
- has rapid or shortness of breath
- is confused
- has a fit (seizure)
- loses consciousness
- is unresponsive
These can be signs of heat stroke.
While you wait for help, keep giving first aid and put them in the recovery position if they lose consciousness.
Preventing heat exhaustion and heat stroke
There is a high risk of heat exhaustion or heat stroke during hot weather or exercise.
To help prevent heat exhaustion or heat stroke:
- drink plenty of cold drinks, especially when exercising
- take cool baths or showers
- wear light-colored, loose clothing
- sprinkle water over skin or clothes
- avoid the sun between 11am and 3pm
- avoid excess alcohol
- avoid extreme exercise
This will also prevent dehydration and help your body keep itself cool.
Keep an eye on children, the elderly and people with long-term health conditions (like diabetes or heart problems) because they’re more at risk of heat exhaustion or heat stroke.
How to treat a burn
If your burn or scald is mild and treated at home, it normally heals without the need for further treatment.
While the skin heals, keep the area clean and don’t apply any creams or greasy substances. Don’t burst any blisters as this can lead to infection.
If you’ve scalded the inside of your mouth by drinking something hot, try to avoid things that can irritate the scalded area, such as hot and spicy food, alcohol and smoking, until the area heals.
Mild burns or scalds that only affect the uppermost layer of skin (superficial epidermal burns) usually heal in about a week without any scarring.
When to seek further medical advice
Whether your burn required medical attention or not, you should seek medical advice if:
- the wound becomes painful or smelly
- you develop a high temperature of 38 °C (100.4 °F) or higher
- the dressing becomes soaked with fluid leaking from the wound
- the wound hasn’t healed after two weeks
Blisters
Expert opinion is divided over the management of blisters that are caused by burns. However, it’s recommended that you shouldn’t burst any blisters yourself.
If your burn has caused a blister, you should seek medical attention. The blister will probably remain intact, although some burns units at hospitals follow a policy of deroofing blisters. Deroofing means removing the top layer of skin from the blister.
In some cases, a needle may be used to make a small hole in the blister to drain the fluid out. This is known as aspiration and may be carried out on large blisters or blisters that are likely to burst.
Your healthcare professional will advise you about the best way to care for your blister and what type of dressing you should use.
Exposure to the sun
During the first few years after a burn, you should try to avoid exposing the damaged skin to direct sunlight as this may cause it to blister. It’s especially sensitive during the first year after the injury. This also applies to a new area of skin after a skin graft.
It’s important to keep the area covered with cotton clothing. If the burn or scald is on your face, wear a peaked cap or wide-brimmed hat when you’re out in the sun. Total sun block – for example, one with a sun protection factor (SPF) of 50 + should be used on all affected areas.
The area can be exposed to sunshine again around three years after the injury, but it’s still very important to apply a high-factor sun cream (SPF 25 or above) and stay out of the midday sun.
Burns that need medical attention
If you have a burn or scald that requires medical treatment, it will be assessed to determine the level of care required.
The healthcare professional treating you will:
- assess the size and depth of the burn by examining the area
- clean the burn, being careful not to burst any blisters
- cover the burn with a sterile dressing – usually a pad and a gauze bandage to hold it in place
- offer you pain relief if necessary – usually paracetamol or ibuprofen
Burn severity is dictated by:
Percent total body surface area involvement (see Figure 9 above – Burn Size Estimation)
- Burns >20-25% total body surface area require IV fluid resuscitation
- Burns >30-40% total body surface area may be fatal without treatment
- In adults: “Rule of Nines” is used as a rough indicator of % total body surface area
- In children, adjust percents because they have proportionally larger heads (up to 20%) and smaller legs (13% in infants) than adults. Lund-Browder diagrams improve the accuracy of the % total body surface area for children.
Depending on how the burn happened, you may be advised to have an injection to prevent tetanus, a condition caused by bacteria entering a wound. For example, a tetanus injection may be recommended if there’s a chance soil got into the wound.
Your dressing will be checked after 24 hours to make sure there are no signs of infection. It will be changed after 48 hours, and then every three to five days until it’s completely healed.
Minor burns affecting the outer layer of skin and some of the underlying layer of tissue (superficial dermal burns) normally heal in around 14 days, leaving minimal scarring.
If the burn is severe, you may be referred to a specialist. In some cases, it may be necessary to have surgery to remove the burnt area of skin and replace it with a skin graft taken from another part of your body.
More severe and deeper burns can take months or even years to fully heal, and usually leave some visible scarring.
The American Burn Association has established criteria to help physicians determine when to refer patients to burn centers (Table 1) 11. One-half of patients treated at non-burn centers meet these criteria for transfer, and a higher percentage of patients treated at non-burn centers are discharged to a nursing home, resulting in a higher burden on the health care system when these criteria are not followed.
Table 1. American Burn Association Burn Center Referral Criteria
Any patient with burns and concomitant trauma (e.g., fractures) in whom the burn injury poses the greatest risk of morbidity or death |
Burns in children at hospitals without qualified personnel or equipment for the care of children |
Burns in patients who will require special social, emotional, or rehabilitative intervention |
Burns in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality |
Burns that involve the face, hands, feet, genitalia, perineum, or major joints |
Chemical burns |
Electrical burns, including lightning injury |
Inhalation injury |
Partial-thickness burns on more than 10 percent of the total body surface area |
Third-degree (full-thickness) burns in any age group |
Burn complications
Burns and scalds can sometimes lead to further problems, including shock, heat exhaustion, infection and scarring.
Shock
After a serious injury, it’s possible to go into shock. Shock is a life-threatening condition that occurs when there’s an insufficient supply of oxygen to the body. It’s possible to go into shock after a serious burn. Burns can damage blood vessels and cause fluid loss. This may result in low blood volume (hypovolemia). Severe blood and fluid loss prevents the heart from pumping enough blood to the body.
Signs and symptoms of shock include:
- a pale face
- cold or clammy skin
- a rapid pulse
- fast, shallow breathing
- yawning
- unconsciousness
Dial your local emergency number and ask for an ambulance if you think that someone who has been seriously injured is going into shock.
While you wait for the ambulance:
- lay the person down (if their injuries allow it) and raise and support their legs
- use a coat or blanket to keep them warm, but don’t cover their face or the burnt area
- don’t give them anything to eat or drink
Hypothermia
Dangerously low body temperature. The skin helps control the body’s temperature, so when a large portion of the skin is injured, you lose body heat. This increases your risk of a dangerously low body temperature (hypothermia). Hypothermia is a condition in which the body loses heat faster than it can produce heat.
Breathing problems
Breathing hot air or smoke can burn airways and cause breathing (respiratory) difficulties. Smoke inhalation damages the lungs and can cause respiratory failure.
Heat exhaustion and heatstroke
Heat exhaustion and heatstroke are two heat-related health conditions that happen when the temperature inside your body rises to 37-40 °C (98.6-104 °F) or above.
Both heat exhaustion and heatstroke can be very serious. They’re often caused by being exposed to too much sunlight or heat.
Symptoms of heat exhaustion and heatstroke include:
- extreme tiredness and lack of energy
- dizziness or fainting
- feeling sick or vomiting
- rapid pulse
- headache
- muscle pain
- irritability
- confusion
If a person with heat exhaustion is taken quickly to a cool place, given water to drink and has their clothing loosened, they should start to feel better within half an hour. If they don’t, they could develop heatstroke. This is a medical emergency and you’ll need to call for an ambulance.
Infection
Wounds can become infected if bacteria get into them. If your burn or scald has a blister that has burst, it may become infected if it’s not kept clean. Seek medical attention for any burn that causes a blister.
Your wound may be infected if:
- it’s uncomfortable, painful or smelly
- you have a high temperature of 38 °C (100.4 °F) or higher
- you have signs of cellulitis, a bacterial infection that causes redness and swelling of the skin
Seek immediate medical attention if you think your burn has become infected. An infection can usually be treated with antibiotics and painkilling medication, if necessary.
In rare cases, an infected burn can cause blood poisoning (sepsis) or toxic shock syndrome. These serious conditions can be fatal if not treated.
Signs of sepsis and toxic shock syndrome include:
- a high temperature
- dizziness
- vomiting
Scarring
A scar is a patch or line of tissue that remains after a wound has healed. Most minor burns only leave minimal scarring. You can try to reduce the risk of scarring after the wound has healed by:
- applying an emollient, such as aqueous cream or emulsifying ointment, two or three times a day
- using sunscreen with a high sun protection factor (SPF) 50+ to protect the healing area from the sun when you are outside.
Bone and joint problems
Deep burns can limit movement of the bones and joints. Scar tissue can form and cause shortening and tightening of skin, muscles or tendons (contractures). This condition may permanently pull joints out of position.
Burn Prevention
Many severe burns and scalds affect babies and young children. The following advice can help reduce the likelihood of your child having a serious accident.
In the kitchen
- it’s best to keep your toddler out of the kitchen, well away from kettles, saucepans and hot oven doors – you could put a safety gate across the doorway to stop them getting in
- use a kettle with a short or curly cord to stop it hanging over the edge of the work surface, where it could be grabbed
- when cooking, use the rings at the back of the cooker and turn saucepan handles towards the back so your child can’t grab them
In the bathroom
- never leave a child under five alone in the bath, even for a moment
- fit a thermostatic mixing valve to your bath’s hot tap to control the temperature
- put cold water into the bath first, then add the hot water – use your elbow to test the temperature of the water before you put your baby or toddler in the bath
Throughout the home
- put your iron, hair straighteners or curling tongs out of reach while they cool down after you’ve finished using them
- fit fireguards to all fires and heaters
- keep matches, lighters and lit candles out of young children’s sight and reach
Hot drinks
- keep hot drinks well away from young children – a hot drink can still scald 20 minutes after it was made
- put hot drinks down before you hold your baby
- after warming a bottle of milk, shake the bottle well and test the temperature of the milk by placing a few drops on the inside of your wrist before feeding – it should feel lukewarm, not hot
- don’t let your child drink a hot drink through a straw
Preventing sunburn
- encourage your child to play in the shade – under trees, for example – especially between 11am and 3pm, when the sun is at its strongest
- keep babies under the age of six months out of direct sunlight, especially around midday
- cover your child up in loose, baggy cotton clothes, such as an oversized T-shirt with sleeves
- get your child to wear a floppy hat with a wide brim that shades their face and neck
- cover exposed parts of your child’s skin with sunscreen, even on cloudy or overcast days – use a broadspectrum sunscreen that has a sun protection factor (SPF) of 30+ or above and is effective against UVA and UVB
- reapply sunscreen often throughout the day – even water-resistant sunscreens should be reapplied after you come out of the water.
Burns diagnosis
During the physical exam, your doctor will examine your burned skin and determine what percentage of your total body surface area is involved. In general, an area of skin roughly equal to the size of your palm equals 1 percent of your total body surface area. For people ages 10 to 40, the American Burn Association defines a severe burn as one that involves 25 percent total body surface area or any burn involving the eyes, ears, face, hands, feet or groin.
You’ll also be examined for other injuries and to determine whether the burn has affected the rest of your body. You may need lab tests, X-rays or other diagnostic procedures.
Burn treatment
Treatment of burns depends on the type and extent of the injuries. Most minor burns can be treated at home using over-the-counter products or aloe. They usually heal within a few weeks.
For serious burns, after appropriate first aid care and wound assessment, your treatment may involve medications, wound dressings, therapy and surgery. The goals of treatment are to control pain, remove dead tissue, prevent infection, reduce scarring, regain function and address emotional needs.
You may need months of additional treatments and therapy. This may be done during a hospital stay, on an outpatient basis or at home. Factors affecting this choice include your wishes, other conditions and abilities, such as whether you’re able to change bandages.
Medications and wound healing products
Topical burn care is the topic of many studies and discussions. Burn wounds heal best in moist—not wet—environments that promote reepithelialization and prevent cellular dehydration. This environment is best created by applying a topical agent or occlusive dressing to reduce fluid loss (Table 2). Topical agents provide pain control, promote healing, and prevent wound infection and desiccation 7.
Superficial burns can be treated successfully with topical application of lotion, honey, aloe vera, or antibiotic ointment 13. The lipid component of these treatments accelerates the repair of damaged skin and reduces drying 14. Although there are no medication requirements for patients with superficial burns, evidence has shown that topical nonsteroidal anti-inflammatory drugs and aloe vera reduce pain 15. Topical corticosteroids have not been shown to reduce the inflammatory reaction; therefore, they should not be used to treat superficial thermal burns or sunburns 16. Partial-thickness burns should be treated with a topical antimicrobial agent or an absorptive occlusive dressing to reduce pain, promote healing, and prevent wound desiccation. Topical silver sulfadiazine (Silvadene) is the standard antimicrobial treatment for partial-thickness burns; however, it is relatively contraindicated in patients with sulfa allergy, pregnant and lactating women, and newborns 17.
Numerous small studies have compared newer occlusive dressings with silver sulfadiazine 18. However, a 2008 Cochrane review found only minimal evidence to guide physicians because the included studies were flawed 19. The authors concluded that the use of newer occlusive dressings should be considered instead of silver sulfadiazine because they resulted in faster healing, decreased pain, fewer dressing changes, and improved patient satisfaction. Some newer occlusive dressings are more cost-effective than silver sulfadiazine 20. Physicians must educate patients on the proper method for changing dressings at home.
A systematic review showed that prophylactic systemic antibiotics administered in the hospital setting did not improve mortality 21; therefore, they generally are not recommended for burns.
For major burns, various medications and products are used to encourage healing.
- Water-based treatments. Your care team may use techniques such as ultrasound mist therapy to clean and stimulate the wound tissue.
- Fluids to prevent dehydration. You may need intravenous (IV) fluids to prevent dehydration and organ failure.
- Pain and anxiety medications. Healing burns can be incredibly painful. You may need morphine and anti-anxiety medications — particularly for dressing changes.
- Burn creams and ointments. Your care team can select from a variety of topical products for wound healing. These help keep the wound moist, reduce pain, prevent infection and speed healing.
- Dressings. Your care team may also use various specialty wound dressings. These create a moist environment that fights infection and helps the burn heal.
- Drugs that fight infection. If you develop an infection, you may need IV antibiotics.
- Tetanus shot. Your doctor might recommend a tetanus shot after a burn injury.
Table 2. Commonly Used Topical Medications and Wound Membranes
| Name | Type of therapy | Characteristics |
|---|---|---|
Bacitracin | Topical | Narrow antimicrobial coverage; inexpensive; painless; requires frequent dressing changes; can be used on face or near mucous membranes |
Mafenide acetate (Sulfamylon) | Topical | Broad-spectrum antimicrobial coverage; penetrates eschar; may delay healing or cause metabolic acidosis; used for deep burns |
Mupirocin (Bactroban) | Topical | Good gram-positive antimicrobial coverage; expensive; painless; requires frequent dressing changes; can be used on face |
SSD (Silvadene) | Topical | Broad-spectrum antimicrobial coverage; painless; requires frequent dressing changes; delays healing; stains tissue; used in deeper partial-thickness burns; relatively contraindicated in pregnant women, newborns, nursing mothers, and patients with glucose-6-phosphate dehydrogenase deficiency or sulfa allergy |
Aquacel Ag | Absorptive dressing | Silver impregnated; broad-spectrum antimicrobial coverage; decreases dressing changes; reduces pain; decreases use of pain medications; faster wound closure than with standard therapies; decreased total cost compared with silver sulfadiazine |
Biobrane | Biocomposite dressing | Less pain and shorter time to healing than with silver sulfadiazine; expensive but lower total treatment cost compared with silver sulfadiazine; one study showed effectiveness in superficial burns, but high failure rates with mid-dermal depth burns |
Hydrocolloids (Duoderm, Urgotul) | Absorptive dressing | Less pain and shorter time to wound closure than with silver sulfadiazine; good for weeping burns; malodorous; opaque |
Impregnated nonadherent gauze (Xeroform, Vaseline gauze) | Nonabsorptive dressing | No antimicrobial activity; messy; provides a nonadherent barrier over the burn for absorptive dressings; used for superficial burns1 |
Silicone (Mepitel) | Nonabsorptive dressing | Expensive; painless; allows seepage of exudates to secondary bandage1 |
Silver-impregnated dressing (Acticoat) | Nonabsorptive dressing | Delivers low concentrations of silver; broad-spectrum antimicrobial coverage; nonadherent; reduces pain; expensive |
SSD = silver sulfadiazine.
Long-term Management and Referral
Although cellulitis is not common in burns, it can cause the skin to become severely erythematous, exudative, painful, and swollen. This is a difficult process to assess because wounds generally are erythematous, painful, and swollen as they heal. Infections can progress rapidly; some of the most common pathogens found in burn wounds include Staphylococcus aureus, Streptococcus pyogenes, Pseudomonas aeruginosa, and Acinetobacter and Klebsiella species 7. Antibiotic treatment depends on local drug resistance and should be tailored toward broad coverage of gram-negative and gram-positive bacteria.
Pruritus and neuropathic pain are common postburn complications. Histamine H1 receptor antagonists such as cetirizine (Zyrtec) are the safest pharmacologic treatment for postburn pruritus 22. Topical doxepin, a tricyclic antidepressant with potent antihistamine properties, reduces postburn pruritus and erythema.47,48 Small studies have shown that pulsed dye laser treatment is effective for postburn pruritus46,49; however, more research is necessary. A recent retrospective review found that pregabalin (Lyrica) reduced postburn neuropathic pain in 69 percent of patients 23.
Patients with burns that extend over a joint should be referred for occupational and physical therapy while the wound is healing if loss of function or range of motion is anticipated. Because of the pain associated with burns, patients often restrict their activity, which results in stiffness and weakness of the surrounding joints 24. Referral to a burn specialist is indicated in patients with full-thickness burns; burns to the hands, feet, perineum, or genital areas (because of the anatomy and function of these areas) 9; and circumferential burns (because of the risk of compartment syndrome). Patients with burns to the face also should be referred, because these burns can result in significant psychological trauma and identity issues.
Referral to a surgeon or burn specialist should be considered for patients with wounds that worsen over the first 72 hours or that begin to cause significant scarring or any degree of contracture 9. If there is uncertainty about burn management at any time during outpatient treatment, a consultation should be obtained.
Physical and occupational therapy
If the burned area is large, especially if it covers any joints, you may need physical therapy exercises. These can help stretch the skin so the joints can remain flexible. Other types of exercises can improve muscle strength and coordination. And occupational therapy may help if you have difficulty doing your normal daily activities.
Breathing assistance
If you’ve been burned on the face or neck, your throat may swell shut. If that appears likely, your doctor may insert a tube down your windpipe (trachea) to keep oxygen supplied to your lungs.
Tube feeding
Your metabolism goes into overdrive when your body starts trying to heal your burns. To provide adequate nutrition for this task, you doctor may thread a feeding tube through your nose to your stomach.
Easing blood flow around the wound
If a burn scab (eschar) goes completely around a limb, it can tighten and cut off the blood circulation. A scab (eschar) that goes completely around the chest can make it difficult to breathe. Your doctor may cut the eschar in several places to relieve this pressure. This procedure is called decompression.
Plastic surgery
Plastic surgery can involve a number of different techniques to move and manipulate body tissue.
Before having plastic surgery, you should have a consultation with a plastic surgeon. They will explain in detail what will happen before, during and after surgery. You may also be given a psychological assessment.
Plastic surgery used to be confined to a procedure called a skin graft, but newer techniques such as tissue expansion and flap surgery are often used these days. These techniques are discussed in more detail below.
Skin grafts
A skin graft is a surgical procedure where healthy skin is removed from an unaffected area of the body and used to cover lost or damaged skin.
Skin grafts may be used for bone fractures that break the skin (open fractures), large wounds, surgical removal of an area of the skin (for example, because of cancer) and burns.
There are two main types of skin graft:
- a full thickness skin graft – the top layer of skin (epidermis) and all the layers of skin underneath (dermis) are removed and the area is closed with stitches; only a small area of skin will be removed, usually from the neck, behind the ear or the inner side of the upper arm
- a partial or split thickness skin graft – the epidermis and a smaller part of the dermis are removed, and the area is left to heal without being closed by stitches; the skin is usually taken from the thigh, buttock or upper arm
Before the procedure, you’ll be given a general anesthetic or a local anesthetic. This will depend on the size and location of the affected area.
The skin graft will usually be held in place using stitches, staples, clips or special glue. The area will be covered with a sterile dressing until it has connected with the surrounding blood supply, which usually takes around five to seven days.
A dressing will also be placed over the area where the skin has been taken from (the donor site) to help protect it from infection. The donor area of partial thickness skin grafts will usually take about two weeks to heal. For full thickness skin grafts, the donor area only takes about 5 to 10 days to heal, because it’s normally quite small and closed with stitches.
At first, the grafted area will appear reddish-purple, but it should fade over time. It can take a year or two for the appearance of the skin to settle down completely. The final color may be slightly different to the surrounding skin, and the area may be slightly indented.
Tissue expansion
Tissue expansion is a procedure that encourages the body to “grow” extra skin by stretching surrounding tissue. This extra skin can then be used to help reconstruct the nearby area.
Examples of when tissue expansion may be used include breast reconstruction and repairing large wounds.
The technique involves inserting a balloon-like device called an expander under the skin near the area to be repaired. This is then gradually filled with salt water over time, causing the skin to gradually stretch and grow.
The operation to insert the expander is usually carried out under general anaesthetic.
The time involved in tissue expansion can vary, and largely depends on the size of the area to be repaired. If a large area of skin is involved, it can take as long as three or four months for the skin to grow enough. During this time, the expander will create a bulge in the skin.
Once the skin has expanded sufficiently, a second operation is needed to remove the expander and reposition the new tissue.
This technique ensures that the repaired area of skin has a similar colour and texture to the surrounding area. There is also a lower chance of the repair failing because the blood supply to the skin remains connected.
Flap surgery
Flap surgery involves the transfer of a living piece of tissue from one part of the body to another, along with the blood vessels that keep it alive.
Flap surgery may be used for a variety of reasons, including breast reconstruction, open fractures, large wounds and improving cleft lip and palates.
In most cases, the skin remains partially attached to the body, creating a “flap”. The flap is then repositioned and stitched over the damaged area.
Occasionally, a technique called a free flap is used. This is where a piece of skin, and the blood vessels supplying it, are entirely disconnected from the original blood supply and then reconnected at a new site. A technique called microsurgery (surgery using a microscope) is used to connect the tiny blood vessels at the new site.
Depending on the location and size of the flap, the operation can be carried out under general or local anesthetic.
As flap surgery allows the blood supply to the repaired area to be maintained, there is a lower risk of the repair failing compared to a skin graft.
Plastic surgery complications
Complications from plastic surgery can include:
- pain and discomfort – which may require painkillers for a few days
- bleeding – which may require a blood transfusion if severe
- infection – which may require antibiotics or further surgery
- scars – you will have scars where incisions were made during surgery, although these will usually fade over time
- implant failure – if an implant is used during plastic surgery, there is a chance that this could leak and change shape, in which case further surgery may be needed to replace it
- skin graft or flap failure – a skin graft or flap can die if the blood supply to the area is restricted; if this happens, further surgery will be needed to remove it before you can have reconstructive surgery again
You should discuss with your surgeon the risks associated with your particular type of plastic surgery.
If you have any concerns regarding your recovery from a surgical procedure, such as pain, swelling, discharge or any other unexpected side effects, speak to your surgeon or healthcare team immediately.
How to heal a burn – home remedies
To treat minor burns, follow these steps:
- Cool the burn. Run cool (not cold) tap water over the burn for 10 to 20 minutes or until the pain eases. Or apply a clean towel dampened with cool tap water. Don’t use ice. Putting ice directly on a burn can cause further damage to the tissue.
- Remove rings or other tight items from the burned area. Try to do this quickly and gently, before the area swells.
- Don’t break small blisters (no bigger than your little fingernail). If blisters break, gently clean the area with mild soap and water, apply an antibiotic ointment, and cover it with a nonstick gauze bandage.
- Apply moisturizer or aloe vera lotion or gel. This may soothe the area and prevent dryness as the wound heals.
- If needed, take an over-the-counter pain reliever. Nonprescription products include ibuprofen (Advil, Motrin IB, others), naproxen (Aleve) and acetaminophen (Tylenol, others).
- Consider a tetanus shot. Make sure that your tetanus booster is up to date. Doctors recommend people get a tetanus shot at least every 10 years.
Whether your burn was minor or serious, use sunscreen and moisturizer regularly once the wound is healed.
Coping and support
Coping with a serious burn injury can be a challenge, especially if it covers large areas of your body or is in places readily seen by other people, such as your face or hands. Potential scarring, reduced mobility and possible surgeries add to the burden.
Consider joining a support group of other people who have had serious burns and know what you’re going through. You may find comfort in sharing your experience and struggles and meeting people who face similar challenges. Ask your doctor for information on support groups in your area or online.
- Burn Incidence and Treatment in the United States: 2016. http://ameriburn.org/who-we-are/media/burn-incidence-fact-sheet/[↩]
- Singer AJ, Dagum AB. Current management of acute cutaneous wounds. N Engl J Med. 2008;359(10):1037–1046.[↩][↩]
- Burns. http://www.emergencycareforyou.org/Emergency-101/Emergencies-A-Z/Burns/[↩]
- U.S. Department of Health and Human Services. Burn triage and treatment: thermal injuries. https://www.remm.nlm.gov/burns.htm[↩][↩][↩]
- Grunwald TB, Garner WL. Acute burns. Plast Reconstr Surg. 2008;121(5):311e–319e[↩]
- Singh V, Devgan L, Bhat S, Milner SM. The pathogenesis of burn wound conversion. Ann Plast Surg. 2007;59(1):109–115.[↩]
- Sheridan R. Outpatient burn care in the emergency department. Pediatr Emerg Care. 2005;21(7):449–456.[↩][↩][↩]
- Artz CP, Moncrief JA. General immediate care. In: Artz CP, Moncrief JA, eds. The Treatment of Burns. 2nd ed. Philadelphia, Pa.: W.B. Saunders; 1969:91–92.[↩][↩]
- Grunwald TB, Garner WL. Acute burns. Plast Reconstr Surg. 2008;121(5):311e–319e.[↩][↩][↩][↩]
- Pauldine R, Gibson BR, Gerold KB, Milner SM. Considerations in burn critical care. Contemp Crit Care. 2008;6(3):1–11.[↩][↩]
- Carter JE, Neff LP, Holmes JH IV. Adherence to burn center referral criteria: are patients appropriately being referred? J Burn Care Res. 2010;31(1):26–30.[↩]
- American Burn Association. Guidelines for the operation of burn centers. http://ameriburn.org/wp-content/uploads/2017/05/acs-resources-burn-chapter-14.pdf[↩]
- Jull AB, Rodgers A, Walker N. Honey as a topical treatment for wounds. Cochrane Database Syst Rev. 2008;(4):CD005083.[↩]
- Proksch E, Jensen JM, Crichton-Smith A, Fowler A, Clitherow J. Rational treatment of first-degree burns [in German]. Hautarzt. 2007;58(7):604–610.[↩]
- Maenthaisong R, Chaiyakunapruk N, Niruntraporn S, Kongkaew C. The efficacy of aloe vera used for burn wound healing: a systematic review. Burns. 2007;33(6):713–718.[↩]
- Faurschou A, Wulf HC. Topical corticosteroids in the treatment of acute sunburn: a randomized, double-blind clinical trial. Arch Dermatol. 2008;144(5):620–624.[↩]
- Rajan V, Bartlett N, Harvey JG, et al. Delayed cooling of an acute scald contact burn injury in a porcine model: is it worthwhile? J Burn Care Res. 2009;30(4):729–734.[↩]
- Chung JY, Herbert ME. Myth: silver sulfadiazine is the best treatment for minor burns. West J Med. 2001;175(3):205–206.[↩]
- Wasiak J, Cleland H, Campbell F. Dressings for superficial and partial thickness burns. Cochrane Database Syst Rev. 2008;(4):CD002106.[↩]
- Thomas S. Hydrocolloid dressings in the management of acute wounds: a review of the literature. Int Wound J. 2008;5(5):602–613.[↩]
- Avni T, Levcovich A, Ad-El DD, Leibovici L, Paul M. Prophylactic antibiotics for burns patients: systematic review and meta-analysis. BMJ. 2010;340:c241.[↩]
- Bell PL, Gabriel V. Evidence based review for the treatment of post-burn pruritus. J Burn Care Res. 2009;30(1):55–61.[↩]
- Wong L, Turner L. Treatment of post-burn neuropathic pain: evaluation of pregabalin. Burns. 2010;36(6):769–772.[↩]
- O’Brien SP, Billmire DA. Prevention and management of outpatient pediatric burns. J Craniofac Surg. 2008;19(4):1034–1039.[↩]





{kind=link}