






What is bergamot
Bergamot orange (Citrus bergamia Risso et Poiteau), is a fragrant citrus fruit the size of an orange, with a yellow or green color similar to a lime, depending on ripeness. Bergamot is a plant belonging to the Rutaceae family, defined as a hybrid of bitter orange and lemon 1). Other authors 2) considered bergamot a hybrid between a sour orange and lime (C. aurantifolia [Christm. and Panzer] Swingle). Bergamot an endemic plant of the Calabria region south of Italy – with more than 90% of the world production of bergamot comes from this region. However, small numbers of bergamot plants grow in other countries, such as Greece, Morocco, Iran and Ivory Coast, Argentina, and Brazil. Bergamot orange is primarily used for the extraction of its essential oil (bergamot essential oil).
Bergamot essential oil is a cold-pressed essential oil produced by cells inside the rind of a bergamot orange fruit. The scent of bergamot essential oil is similar to a sweet light orange peel oil with a floral note. Bergamot essential oil from the peel of this orange is used in perfume, to get rid of insects, in cosmetics, food, confectionery industries and to flavor tea 3). Bergamot oil is also used in aromatherapy for depression, anxiety and poor digestion. Several clinical studies on aromatherapy with bergamot essential oil, in combination with other essential oils, have shown promising results: anxiety and stress reduction, anti‐depression, pain relief, and blood pressure and heart rate reduction. Further human studies with bergamot essential oil inhalation alone have also shown significant effects on anxiety reduction 4), depression reduction 5) and blood pressure 6) and heart rate reduction 7). In addition, bergamot essential oil has minimal side effects, if any 8), suggesting bergamot essential oil inhalation may have potential therapeutic benefits including improving overall mental health and anxiety.
Bergamot juice, obtained from the endocarp after essential oils extraction, has long time been considered just a secondary and discarded product of the essential oil industry due to its bitter taste. Recently, bergamot juice gained attention because of its hypolipemic and hypoglycaemic activity 9), as well as its anti-inflammatory 10) and anti-cancer properties 11).
Figure 1. Bergamot orange

Bergamot essential oil
Bergamot essential oil is a greenish or brownish-yellow volatile oil (corresponding to the beginning and the end of the productive season) with a bitter aromatic taste and a characteristic pleasant odor.
The chemical composition of bergamot essential oil has been widely investigated and is well known 12). Bergamot essential oil contains several bioactive molecules with potential health benefits. It is composed of both a volatile (93–96% of total) and a non-volatile (4–7% of total) fraction. The first is mainly represented by monoterpene and sesquiterpene hydrocarbons, and their oxygenated derivatives, along with aliphatic aldehydes, alcohols, and esters 13). They include monoterpene limonene (25–53%) and high quantities of oxygenated compounds, such as linalool (2–20%), linalyl acetate (15–40%), γ-terpinene, and β-pinene 14). The non-volatile fraction (4–7% of total) contains pigments, waxes, coumarins, and psoralens (such as 5-methoxypsoralen, also known as bergapten or 5-MOP, contained in about 0.2%), as well as bergamottine [5-geranyloxypsoralen]) 15). Due to the well-known 5-MOP-induced photo-toxicity, a furocoumarins-free essential oil has been prepared for perfumery and cosmetic uses. The vacuum distillation of bergamot peels provides a high-quality bergamot essential oil totally devoid of 5-MOP that is chemically comparable to that of the cold-pressed oil 16).
The characteristic flavor of Citrus oils is mainly provided by linalool, citral, and linalyl acetate 17), whereas limonene and pinene are not much flavoring and they are relatively unstable compounds when exposed to heat and light. Thus, it is necessary to remove them to increase the shelf life of the products 18).
Bergamot essential oil uses
Bergamot essential oil is one of the main basic constituents for the manufacture of perfumes, due to its ability to fix the aromatic bouquet of aromas and harmonize all of the essences, enhancing the fragrance. Bergamot essential oil is also used by the pharmaceutical industry, both to absorb the unpleasant smells of medicinal products and for its antiseptic and antibacterial properties. Finally, bergamot essential oil is used in the food and confectionery industries as a flavoring.
In Italian folk medicine, it has been used primarily for fever and parasitic diseases, in addition to mouth, skin, respiratory and urinary tract infections, gonococcal infections, leucorrhoea, vaginal pruritus, tonsillitis, and sore throats 19). For its antiseptic and antibacterial proprieties, bergamot essential oil has been used as an antimicrobial agent to facilitate wound healing and has been included in preparations used to treat upper respiratory-tract disorders and hyperhidrosis. Moreover, bergamot essential oil’s use in magisterial, handcrafted, and homemade medicaments that were useful for skin disinfection, as well as use as an aid for healing minor wounds, has a long tradition in Italy. Currently, a furocoumarins-free bergamot essential oil is used in preparations for cutaneous use.
Bergamot essential oil is widely employed in aromatherapy, and has recently received renewed popularity in improving mood and mild symptoms of stress-induced disorders 20) and facilitating sleep induction 21). Aromatherapy massage has been shown to relieve symptoms of anxiety in patients with cancer 22).
Bergamot essential oil aromatherapy
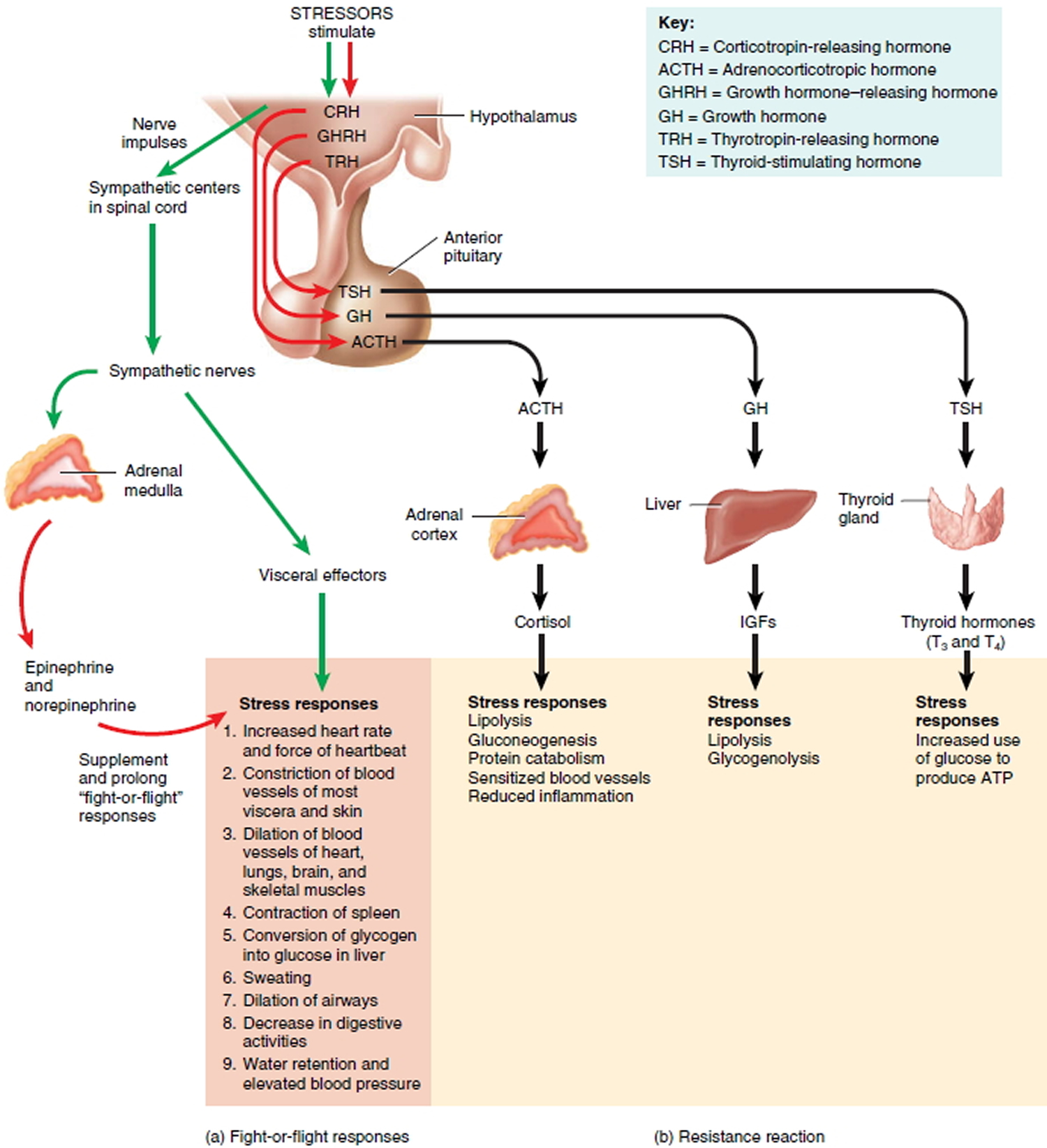
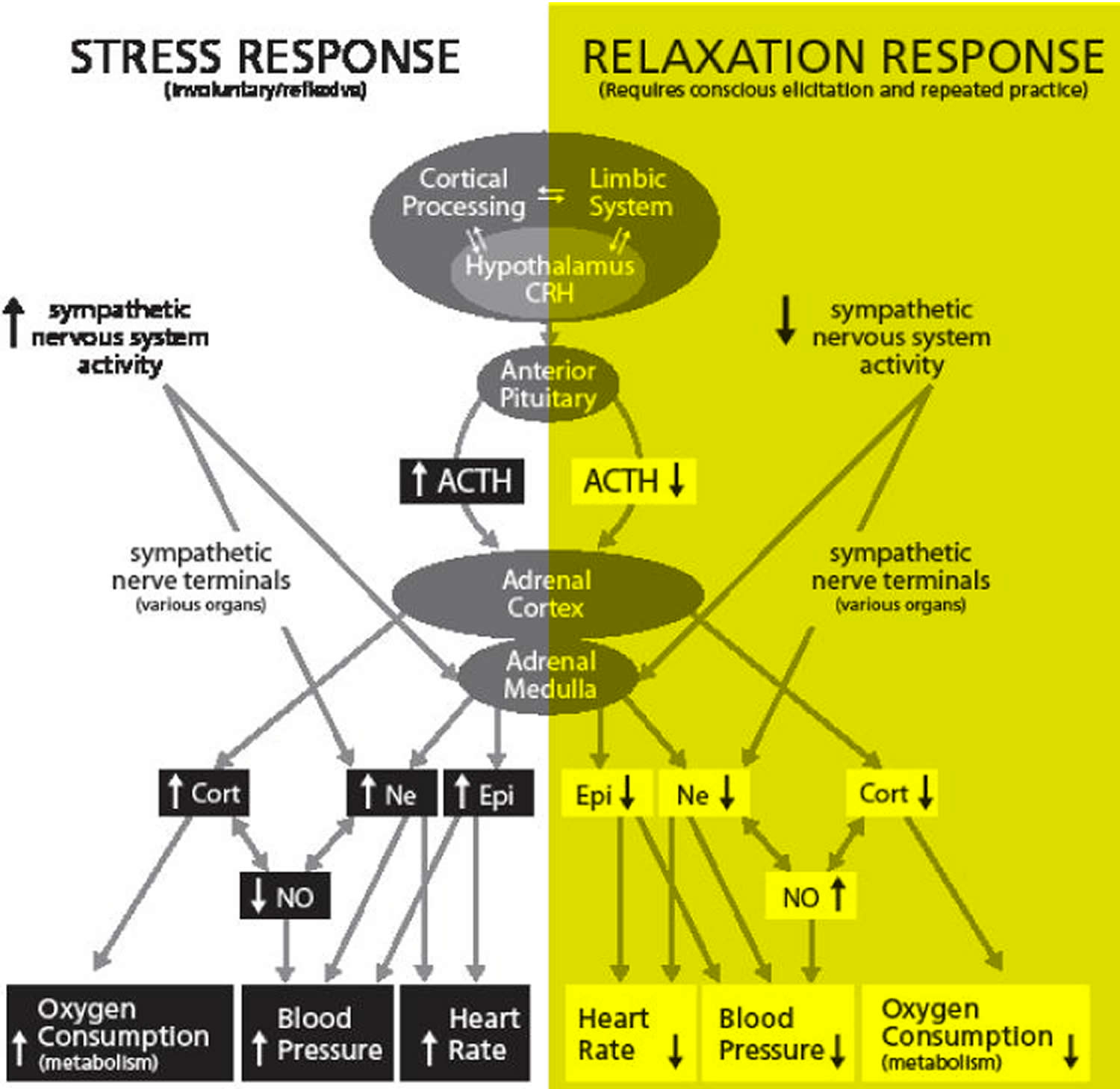
The scientific rationale of essential oils use in aromatherapy to improve mood and the mild symptoms of stress disorders, such as anxiety, depression, and chronic pain, is supported by both the physiological and psychological effects caused by the inhalation of volatile components that are believed to act via limbic system structures, such as the hippocampal formation, the hypothalamus and the pyriform cortex 23). Indeed, several clinical and experimental data indicate that aromatherapy can improve mood, alertness, and cognition. Specific EEG (electroencephalogram) changes associated with alertness and relaxation have been observed in some studies using essential oils. With regard to bergamot essential oil, these effects have been attributed to volatile components other than 5-MOP 24). Although the mechanisms by which bergamot essential oil induces its effects on the central nervous system have not yet been fully understood, it has been suggested that they could be mediated by the release of amino acids that interact with mechanisms that modulate synaptic plasticity.
Clinical research focused essentially on the therapeutic application of bergamot essential oil in aromatherapy, by inhalation or hand massage, on anxiety and stress responses. We reviewed the results of ten clinical studies in which only two reported negative results. Their principal data are reported in Table 1. Four studies evaluated the effects of different essential oil combinations, with bergamot essential oil being a constituent of the mixture associated with lavender (Lavandula angustifolia), cedarwood (Cedrus atlantica), ylang ylang (Cananga odorata) or frankincense 25). Among the studies with combinations, only Graham et al.’s (2003) study reported negative results. The other three studies showed positive effects based on the subjective responses to stress. The remaining six studies were all conducted using only bergamot essential oil. Five of these studies reported beneficial effects from bergamot essential oil, such as reduced heart rate, blood pressure and stress responses 26). One study investigating the effects of aromatherapy with bergamot essential oil on pain and nausea of children and adolescents undergoing stem cell transplantation, showed no benefit. Unfortunately, most of clinical trials did not report the quality parameters of the essential oils used. Even though these studies are not always satisfactory from a methodological point of view, they show that employment of bergamot essential oil in aromatherapy can be useful for reducing anxiety and stress responses, and it deserves further clinical investigation.
Table 1. Clinical studies on aromatherapy with bergamot essential oil (BEO), alone or in combination with other essential oils (lavender, cedarwood, ylang ylang, frankincense)
| Authors | Study type | Essential oils | Subjects | Principal endpoints | Outcome |
|---|---|---|---|---|---|
| Graham et al. 27) | Double-blind placebo-controlled randomized | Lavender, bergamot, and cedarwood by inhalation | 200 patients undergoing radiotherapy | Anxiety measured by HADS | Negative results |
| Hwang 28) | Placebo-controlled randomized | Lavender, ylang ylang, and bergamot by inhalation | 52 subjects affected by hypertension | Blood pressure, serum cortisol levels, catecholamine levels | Reduction of psychological stress responses, serum cortisol levels, blood pressure |
| Chang 29) | Controlled (non-equivalent control group) | Bergamot, Lavender, and Frankincense by hand massage | 58 hospice patients with terminal cancer | Pain, depression scales | Reduction of pain and depression |
| Peng et al. 30) | Open-label randomized controlled trial | Bergamot by inhalation | 114 healthy undergraduate students | Heart rate variability | Reduction of heart rate |
| Seo 31) | Placebo-controlled, cross-over | Bergamot by inhalation | 36 female high school students | Blood pressure, pulse rate, IgA levels | Reduction of blood pressure and heart rate, no effects on IgA levels |
| Hongratanaworakit 32) | Controlled, randomized | Bergamot, lavender cutaneous application | 40 healthy subjects | Blood pressure, pulse rate, breathing rate, and skin temperature, recorded as indicators of the arousal level of the ANS | Decrease of subjective behavioral arousal |
| Chang and Shen 33) | Not controlled | Bergamot by inhalation | 54 elementary school teachers | Blood pressure, heart rate | Decreases in blood pressure and heart rate |
| Ndao et al. 34) | Double-blind, placebo-controlled randomized | Bergamot by inhalation | 40 children/adolescents to undergo Stem cell transplantation | Pain and nausea scales | No benefit |
| Ni et al. 35) | Placebo-controlled, randomized | Bergamot by inhalation | 116 patients awaiting ambulatory surgery | Responses to the (STAI) score and vital signs | Reduction of anxiety, heart rate, variability and blood pressure |
| Liu et al. 36) | Placebo-controlled, no randomization | Bergamot by inhalation | 29 elementary work stressed schoolteachers | Blood pressure, heart rate | Reduction of heart rate |
Antimicrobial Activity
It has been reported that bergamot essential oil has both antibacterial and antifungal activity against Campylobacter jejuni, Escherichia coli O157, Listeria monocytogenes, Bacillus cereus, and Staphylococcus aureus and dermatophytes, respectively 38). The in vitro activity of bergamot essential oil against Candida species suggests bergamot essential oil’s potential role in the topical treatment of Candida infections 39). Bergamot essential oil is also active against dermatophytes in vitro 40). Additionally, chitosan-based films containing bergamot essential oil at 0.5, 1, 2, and 3% w/w showed a significant dose-dependent inhibitory effect on the growth of Penicillium italicum 41). Moreover, the in vitro effectiveness of the oil and vapors of bergamot and its components against common foodborne pathogens has been also investigated, and linalool was revealed to be the most effective anti-bacterial component 42).
Anti-inflammatory activity
Bergamot essential oil anti-inflammatory activity was demonstrated using the carrageenan-induced rat paw oedema test. The highest level of bergamot essential oil anti-inflammatory activity was obtained with a 0.10 ml/kg dosage. The median effective dose of bergamot essential oil was found to be 0.079 ml/kg 43).
Antiproliferative Activity
Bergamot essential oil has also been found to inhibit the survival and proliferation of SH-SY5Y neuroblastoma cells, 44) through the activation of multiple pathways leading to both necrotic and apoptotic cell death 45). Moreover, Russo et al. 46) showed that association of limonene and linalyl acetate, but not the exposure to the single compounds, caused significant cytotoxicity, suggesting for a major role of the combined action of these monoterpenes in cancer cell death induced by bergamot essential oil.
Neuroprotective Activities
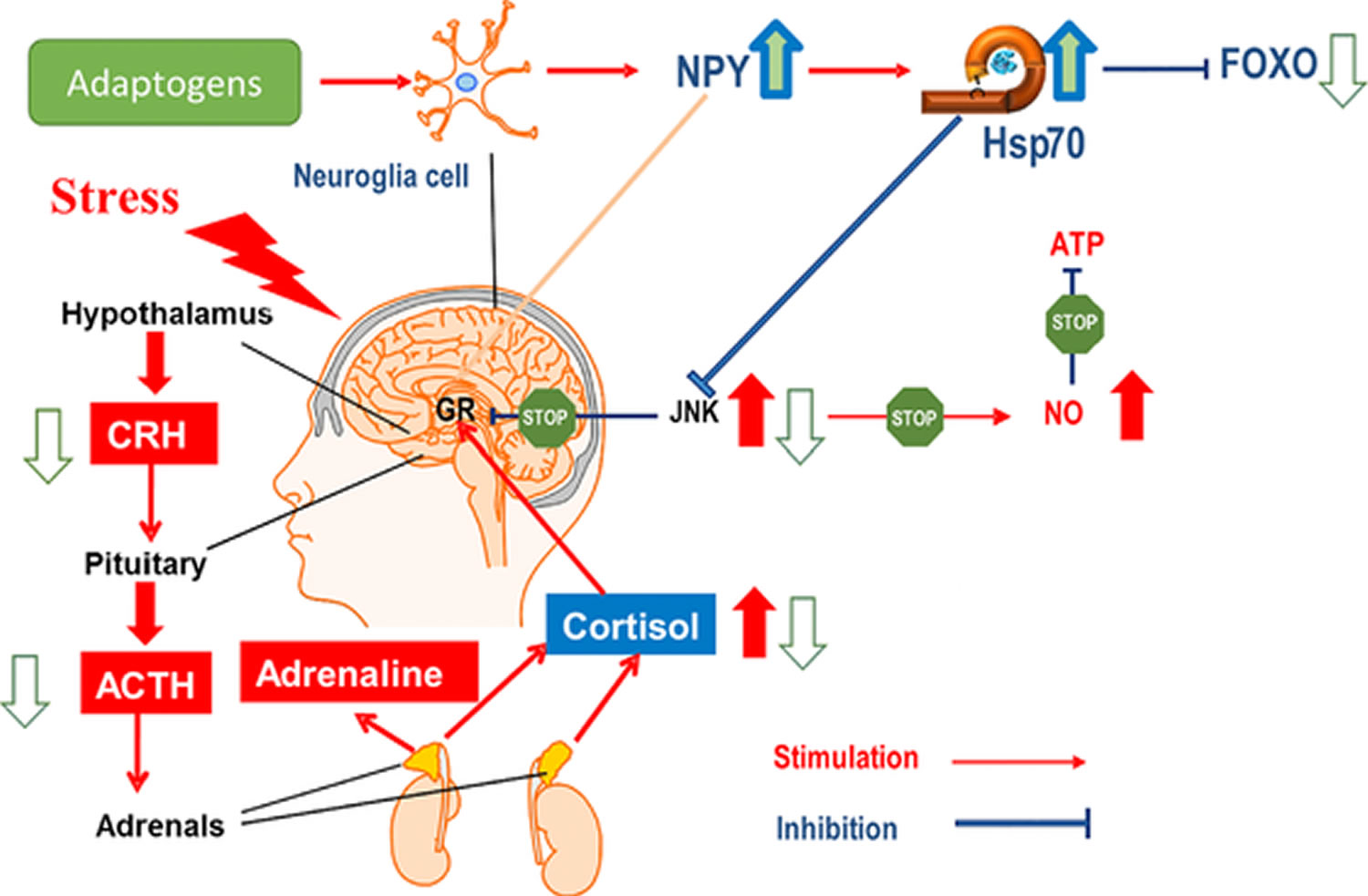
Anxiolytic effects of bergamot essential oil (1.0, 2.5, and 5.0% w/w) were studied by administering it to rats subjected to anxiety-related behaviors, the elevated plus-maze and the hole-board tests, and then measuring the stress-induced levels of plasma corticosterone in comparison with the effects of diazepam. Bergamot essential oil (2.5%) and diazepam exhibited anxiolytic-like effects and attenuated the corticosterone response to acute stress 47).
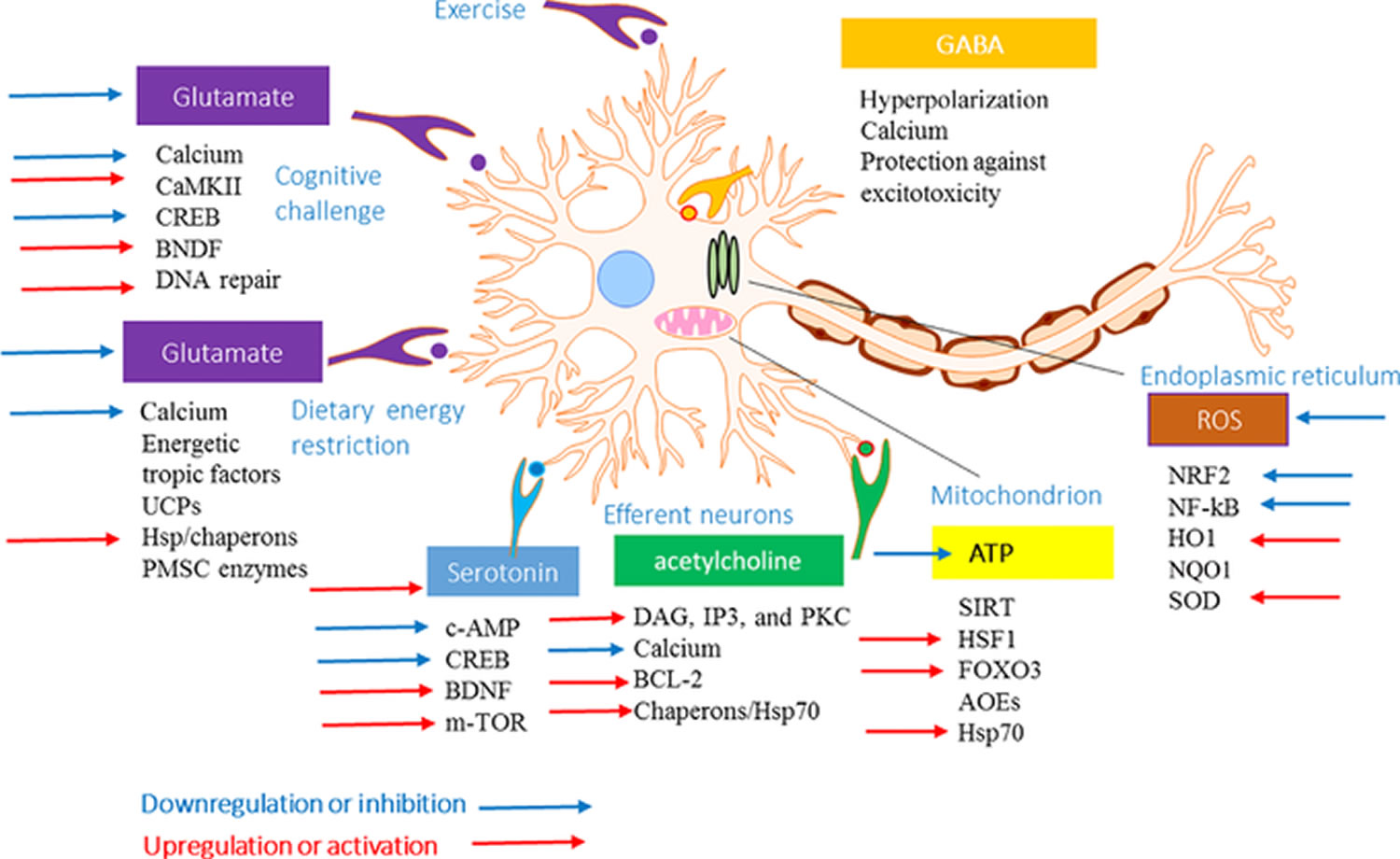
After perfusion into the hippocampus via the dialysis probe (20 μl/20 min), bergamot essential oil produced a dose-dependent and Ca2+-independent increase of extracellular aspartate, glycine, taurine, GABA, and glutamate 48). Moreover, bergamot essential oil (0.5 ml/kg) given intraperitoneally 1 h before experimental occlusion of the middle cerebral artery, significantly reduced infarct size after 24 h, especially in the medial striatum and the motor cortex, as revealed by 2,3,5-triphenyl-2H-tetrazolium chloride staining of tissue slices 49).
Finally, in the human SH-SY5Y neuroblastoma cell line exposed to N-methyl-D-aspartate (NMDA), bergamot essential oil (0.0005–0.01%) reduced the death of SH-SY5Y cells caused by 1 mM NMDA in a concentration dependent manner. In addition, 0.01% bergamot essential oil counteracted the deactivation of Akt (a serine/threonine-specific protein kinase) and the consequent activation of glycogen synthase kinase 3 beta (GSK-3B) induced by NMDA. Results obtained with specific fractions of bergamot essential oil, suggested that monoterpene hydrocarbons could be important for neuroprotection 50).
Analgesic Effects
Capsaicin-induced nociceptive responses in the plantar surface of the hindpaw were significantly reduced by intraplantar injection of bergamot essential oil. Further experiments addressed the importance of linalool in bergamot essential oil oil-induced antinociception 51). In another study, injection into the hindpaw of both the linalool and linalyl acetate compounds showed a significant reduction of nociceptive responses, which was much more potent than that induced by bergamot essential oil. The enhanced effect of the association of bergamot essential oil or linalool with morphine was antagonized by pretreatment with the opioid antagonist naloxone 52). The analgesic effect was also investigated using intraplantar injection of bergamot essential oil or linalool in mice with neuropathic hypersensitivity induced by partial sciatic nerve ligation. The results suggested that both bergamot essential oil and linalool reduced partial sciatic nerve ligation-induced mechanical allodynia in a dose-dependent manner through a local effect. Moreover, the analgesic effect was associated with a reduction of spinal extracellular signal-regulated protein kinase activation 53).
Cardiovascular Properties
Bergamottine significantly decreased the electrocardiographic changes that are typical of coronary arterial spasms and the occurrence of experimental cardiac arrhythmias provoked by pitressin in guinea pigs. Bergamottine also increased the dose of ouabain required to cause ventricular premature beats, ventricular tachyarrhythmias, and death. These results indicate that bergamottine possesses potential antianginal and antiarrhythmic properties 54).
It is known that lectin-like oxyLDL receptor-1 (LOX-1) is involved in smooth muscle cell proliferation and neo-intima formation occurring in injured blood vessels. Interestingly, in an experimental model of rat angioplasty, pretreatment with the non-volatile fraction of bergamot essential oil, reduced the neointima proliferation in a dose-dependent manner, together with free radical formation and LOX-1 expression 55). Moreover, it has been suggested that bergamot essential oil induces vasorelaxation of the mouse aorta by activating K+ channels and inhibiting Ca2+ influx 56), which differentially modulates intracellular Ca2+ levels in vascular endothelial and smooth muscle cells 57). These findings indicate that bergamot essential oil could be further studied for its potential role as a vasodilator agent in cardiovascular diseases.
Bergamot Essential Oil Side Effects
Bergamot essential oil is a widely used aromatic ingredient in cosmetics that may be applied on sun-exposed skin areas, although components such as bergapten, citropten, bergamotene, and other furocoumarins may cause phototoxic effects 58). There are only a few reports of phototoxic reactions caused by aromatherapy with bergamot essential oil. Freund, in 1916, was the first to describe a series of four cases of intense pigmentation in irregular areas after the use of Eau de Cologne before exposure to sunshine. He observed the same phenomenon after experimental use of bergamot essential oil, one of the constituents of Eau de Cologne. Rosenthal first used the term “Berloque dermatitis” because of the form of the resulting pigmentation 59). Hyperpigmentation of the neck, face, arms, or trunk that have been exposed to light has been attributed to psoralens in the bergamot essential oil. Cases have become much more rare since the introduction of psoralen-free bergamot essential oil.
Bergamot essential oil rich in 5-MOP has been used as sun tanning products for many years. In 1995, this use was banned and limited to the treatment of certain skin disorders. Toxic reactions can occur due to psoralen or UVA overdosing or due to accidental exposure to additional UVA, including sunlight exposure. Skin application of psoralens is more likely to induce photosensitivity reactions. To avoid the phototoxic and photocarcinogenic harm, the International Fragrance Association recommended that products that are applied in areas of skin exposed to the sun not have to contain more than 0.4% of bergamot essential oil. The occurrence of second-degree skin burns was found in two women after PUVA exposure 60).
The cases of the two patients were described as having localized and disseminated bullous phototoxic skin reactions that developed 48–72 h after ultraviolet exposure subsequent to aromatherapy with bergamot essential oil. The first case was of a woman that had used a bergamot aromatherapy oil preparation 3 days earlier and subsequently stayed exposed to the sun for several hours. In the second case, the woman visited a sauna 2 days before, where she was exposed to aromatherapy with bergamot essential oil before being exposed to UVA radiation while tanning. Cutaneous lesions developed gradually within 48–72 h. In both cases, the patients did not use other creams and/or medications at the same time 61).
In another case, a 44-year-old man drank up to 4 L of black tea every day for 25 years. When he changed his brand because of occasional gastric pain, he began to drink the same daily quantity of Earl Gray tea. One week after the change, he noticed repeated muscle cramps. After 5 weeks of drinking the tea, the muscle cramps continued. Occasionally, he observed fasciculations, distal paraesthesia, and feelings of pressure in his eyes that were associated with blurred vision. Neurological examination confirmed reduced visual acuity and fasciculations. After 5 months, suspecting a relation between his symptoms and his tea intake, he stopped drinking Earl Gray, going back to black tea. Within 1 week, the symptoms completely disappeared. Successively, he observed that the symptoms did not appear if he ingested no more than 1 L of Earl Gray tea each day. Earl Gray tea is composed of black tea and bergamot essential oil. The adverse effects of bergamot essential oil in this patient could be explained by the potential effects of bergapten as a selective axolemmal potassium channel blocker, reducing potassium permeability at the nodes of Ranvier in a time-dependent manner. This may provoke hyperexcitability of the axonal membrane and phase alterations of potassium currents, producing fasciculation and muscle cramps. Impairment of the potassium channel function plays a pathogenic role in other disorders characterized by the occurrence of fasciculation. Prolonged opening of voltage-gated sodium channels caused by bergapten may enhance neuronal hyperexcitability 62).
Summary
Bergamot essential oil is generally well tolerated, but it possesses photosensitive properties because of the presence of furocoumarins, especially 5-MOP. Therefore, in topical preparations, psoralen-free essential oil was used in recent decades. As a consequence of this and because of safety concerns related to furocoumarins, the use of high quality controlled psoralen-free bergamot essential oil is recommended as a general precaution. However, although bergamot essential oil has been used extensively for many years, there have only been a few reports of phototoxic reactions to bergamot essential oil aromatherapy oil.
References [ + ]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}