Contents
- What is cauda equina
What is cauda equina
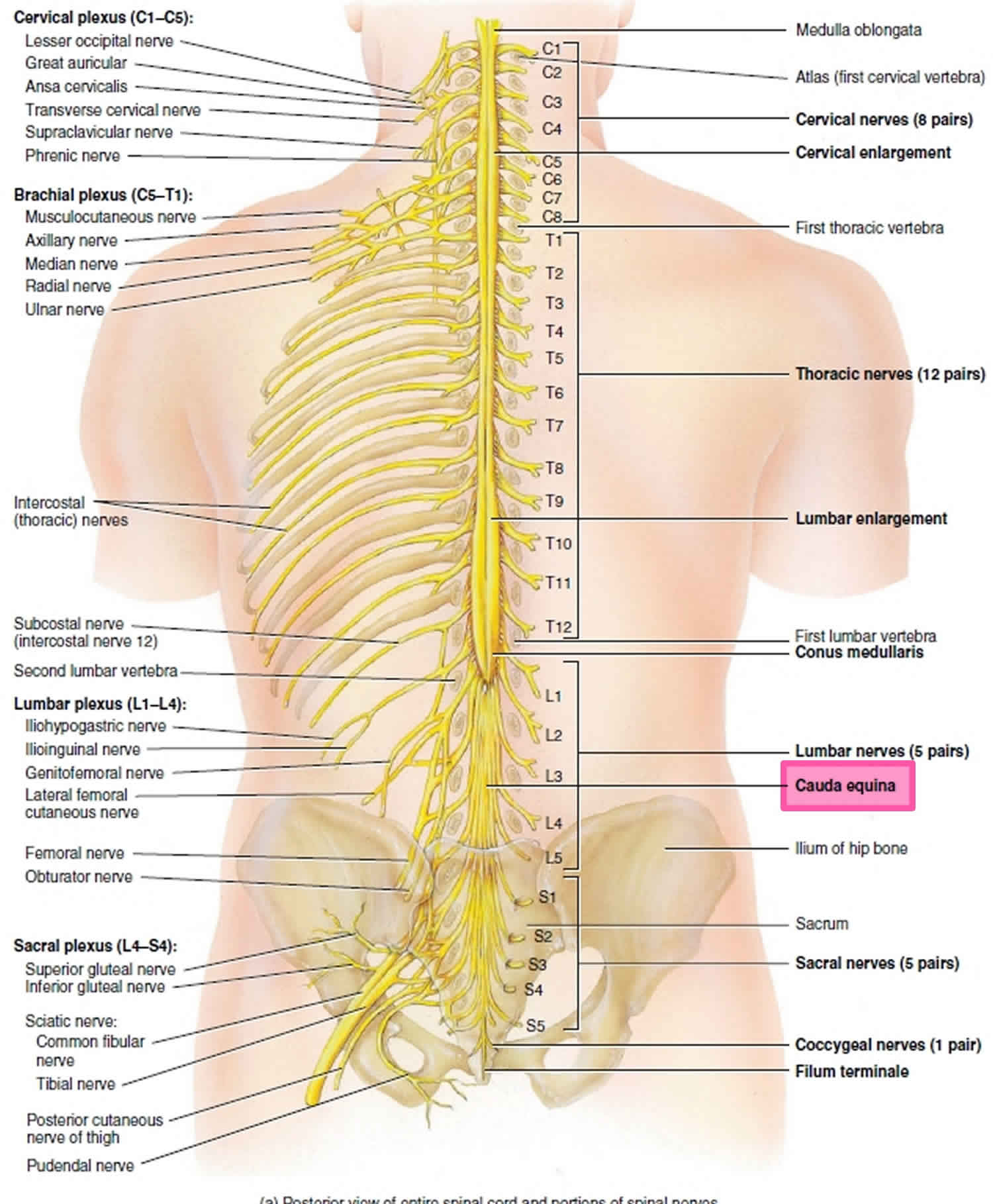
As spinal nerves branch from the spinal cord, they pass laterally to exit the vertebral canal through the intervertebral foramina between adjacent vertebrae. However, because the spinal cord is shorter than the vertebral column, nerves that arise from the lumbar, sacral, and coccygeal regions of the spinal cord do not leave the vertebral column at the same level they exit the spinal cord. The roots of these lower spinal nerves angle inferiorly alongside the filum terminale in
the vertebral canal like wisps of hair. Accordingly, a rope-like tail of nerve fibers at the caudal end of the spinal cord are collectively named the cauda equina, from the Latin translation meaning “horse’s tail”. The cauda equina is a group of nerves and nerve roots stemming from the distal end of the spinal cord, typically levels L1-L5 and contains axons of nerves that give both motor and sensory innervation to the legs, bladder, anus, and perineum 1. Cauda equina syndrome is a medical emergency that results from compression and disruption of the function of these nerves and can be inclusive of the conus medullaris or distal to it, and most often occurs when damage occurs to the L3-L5 nerve roots 2. Cauda equina syndrome can present with back pain radiating to the legs, motor and sensory dysfunction of the lower extremities, bladder and/or bowel dysfunction, sexual dysfunction and saddle anesthesia 3. Cauda equina syndrome also carry a high risk of litigation as delays in diagnosis and management can lead to devastating life-long impairment 4.
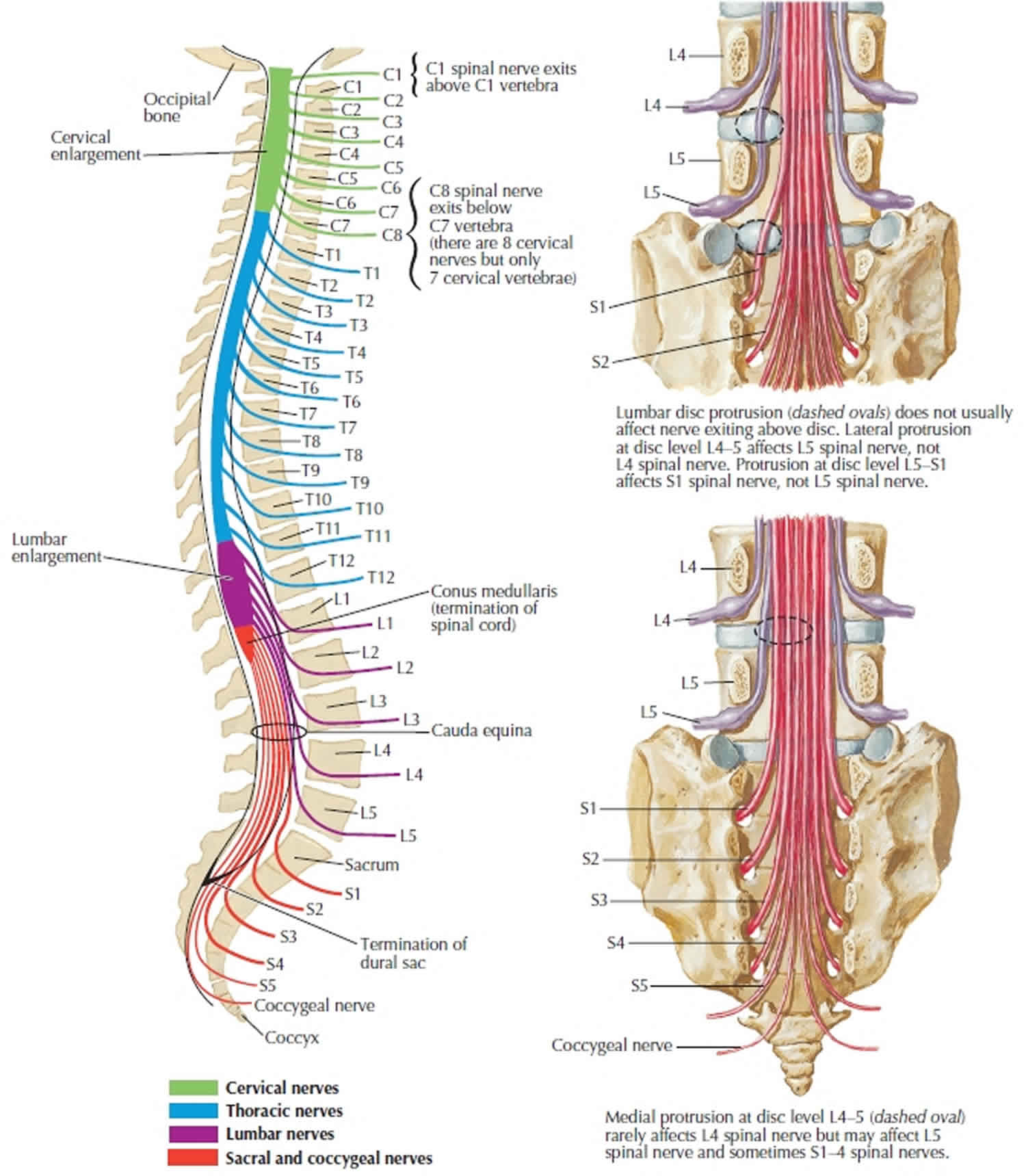
The human spinal cord terminates at the L1-L2 vertebral level in a conical structure called the conus medullaris, which lies just caudad to the anatomical landmark of the 12th rib. The cauda equina contains a bundle of nerves which project distally within the enclosed cavity of the lumbar cistern from the spinal cord and conus medullaris toward the coccyx. Each nerve exits at its respective vertebral level toward targets which are supplied by the L2-S5 spinal cord level. Nerves contained within the cauda equina provide somatic efferent innervation to muscles of the lower extremity and somatic afferent sensations such as vibration, proprioception, pain, and temperature. Parasympathetic nerves provide visceral efferent signals to the urinary bladder from the S2 to S4 spinal cord levels and are responsible for micturition, accomplished by stimulating the detrusor muscle to contract while simultaneously relaxing the internal urethral sphincter. Sympathetic fibers from T11 through L2 exert urinary bladder filling by relaxing the detrusor muscle and contracting the internal urethral sphincter 5.
The cauda equina is supplied by arteries of the same name, which are small and may not be visualized radiographically. Each spinal nerve root has a corresponding medullary artery. A vasocorona surrounding the conus medullaris and the high degree of arterial anastomoses among the nerve roots predispose the vasculature patterns to significant diversity. Lymphatic capillaries occur nearly everywhere in the body except for a small number of sites, including the central nervous system (CNS); consequently, immune surveillance occurs within the layers of the meninges in a medium of cerebrospinal fluid (CSF). Cerebrospinal fluid bathes the brain, spinal cord, and cauda equina and is thought to serve as a protective layer of lubrication which provides nutrients and removes waste.
Figure 1. Cauda equina
What is cauda equina syndrome
Cauda equina syndrome occurs when the bundle of nerve roots at the lower end of the spinal cord called the cauda equina are compressed and disrupt motor and sensory function to the lower extremities and bladder. Patients with cauda equina syndrome are often admitted to the hospital as a medical emergency. Cauda equina syndrome can lead to incontinence and even permanent paralysis.
If patients with cauda equina syndrome do not seek immediate treatment to relieve the pressure, it can result in permanent paralysis, impaired bladder and/or bowel control, loss of sexual sensation, and other problems. Even with immediate treatment, some patient may not recover complete function.
Although early treatment is required to prevent permanent problems, cauda equina syndrome may be difficult to diagnose.
Cauda equina syndrome and conus medullaris syndrome are rare, with an estimated prevalence of 1 in 30,000 to 100,000 people per year 6. Estimates of annual incidence are between 1.5 to 3.4 per million people.[5] It occurs in 3% of all disc herniations 6. Cauda equina syndrome and conus medullaris syndrome are most common in young men, possibly due to this population group being more likely to experience compressive thoracolumbar trauma 6. One study estimated that in the U.S. we would expect to see 1016 new causes of cauda equina syndrome and 449 new cases of conus medullaris per year 6.
Cauda equina syndrome causes
Cauda equina syndrome (and conus medullaris syndrome) result from compression of the spinal cord and nerves/nerve roots arising from L1-L5 levels. The most common cause of compression in 45% of cauda equina syndrome is a herniated lumbar intervertebral disc 3. Other causes include epidural abscess, spinal epidural hematoma, diskitis, tumor (either metastatic or a primary CNS cancer), trauma (particularly when there is retropulsion of bone fracture fragments), spinal stenosis and aortic obstruction 7. Rare reported cases exist in which cauda equina syndrome was associated with chiropractic manipulation, placement of interspinous devices, and thrombosis of the inferior vena cava 7.
Causes of cauda equina syndrome include:
- Spinal canal stenosis with a smaller disc prolapse
- Trauma to the spine
- Rare causes include infection in and around the vertebral bones (osteomyelitis), cancer in the spine, after injections into the spine or spine surgery.
Risk factors for developing cauda equina syndrome
Risk factors for developing cauda equina syndrome include:
- A history of low back pain with sciatica, especially sciatica in both legs.
- Instability or deformity of the spine
- Trauma to the spine, often following a car accident
- Recent lumbar spine surgery
- A history of cancer
- Recent severe infection
- Cauda equina syndrome can develop suddenly even without these risk factors.
Cauda equina syndrome prevention
Prevention of cauda equina syndrome is focused on early diagnosis by identifying the symptoms described (below). While low back pain with leg pain and/or weakness is a common complaint that affects many people, cauda equina syndrome is a rare complication. Your doctors should be vigilant in identifying these cases. You should familiarize yourself with the signs and symptoms that could suggest possible cauda equina syndrome, including change in bowel or bladder function and loss of sensation in the groin.
Cauda equina syndrome symptoms
Cauda equina symptoms can vary in intensity and may evolve slowly over time.
See your doctor immediately if you have:
- Bladder and/or bowel dysfunction, causing you to retain urine or be unable to hold it.
- Severe or progressive problems in the lower extremities, including loss of or altered sensation between the legs, over the buttocks, the inner thighs and back of the legs (saddle area), and feet/heels.
The symptoms of cauda equina syndrome can vary, but the key signs doctors look for are:
- Severe low back pain and sciatica
- Pain may be sudden and severe or gradually develop over weeks
- Motor weakness, sensory loss, or pain in one, or more commonly both legs
- Difficulty to pass urine or use the bowels. Prolonged inability to pass urine can result in urine leaking uncontrollably
- Numbness or tingling in the groin (“saddle region”)
- Sexual dysfunction
Cauda equina syndrome complications
Cauda equina syndrome complications are increasingly likely if diagnosis and appropriate management is delayed, and include residual:
- Paralysis
- Sensory abnormalities
- Bladder, bowel, and sexual dysfunction
One study looked at 63-day outcomes on micturition, defecation, saddle anesthesia, sexual function, and sciatica in cauda equina syndrome. The data indicate that a large percentage of patients still experience residual symptoms irrespective of their time to surgical decompression 3. Micturition deficits such as retention requiring self-catheterization or presence of suprapubic or indwelling catheters and incontinence still presented in 47.7% of patients 3. Dysfunction with defecation decreased post-operatively significantly, but 41.8% of patients still had problems at 63 days post-operatively 3. Sexual dysfunction persisted in 53.3% of patients, and saddle anesthesia in 56.6% 3. Sciatica was present in 47.5% of patients 3. The best predictors of outcome are neurological status at presentation and degree of injury. Incomplete injuries tend to have better outcomes 3.
Cauda equina syndrome diagnosis
To diagnose cauda equina syndrome, your doctor will evaluate your medical history, give you a physical examination, and order multiple diagnostic imaging studies.
Medical history
A thorough history is necessary, with detailed questions regarding recent falls, trauma or injuries, use of anticoagulation, presented spinal instrumentation, intravenous drug use, history of malignancy, chiropractic manipulation, and constitutional symptoms like fevers/chills 3.
Patients can present with:
- Back pain and sciatica (seen in as many as 97% of patients)
- Weakness and changes in sensation in the lower extremities
- Bladder dysfunction (disruption of autonomic fibers results in either retention or incontinence in up to 92% of patients)
- Bowel dysfunction (retention or incontinence in up to 72% of patients)
- Saddle anesthesia or decreased sensation in the perineum (in up to 93% of patients)
- Sexual dysfunction (impotence in men) 3
The symptoms above when presenting in isolation, are neither specific nor sensitive for cauda equina syndrome. However, several of the signs and symptoms mentioned above taken as a constellation should raise clinical suspicion 1. These symptoms also lack significant positive predictive value for the syndromes, especially early on 8. However, the onset of perineal anesthesia associated with bladder dysfunction is typical of the start of cauda equina syndrome and the time at which the clock starts on diagnosis and management 1. It is important also to note that painless urinary retention often has the greatest predictive value as a stand-alone symptom, but it is unfortunately indicative of late, often irreversible cauda equina syndrome 9.
Once clinical suspicion is established based on history, a thorough neurological examination is paramount. Findings to watch for include:
- Motor or sensory deficits in the legs – usually bilateral but can also be unilateral and asymmetrical (particularly in cases with an incomplete injury)
- Lower motor neuron signs in the legs – areflexia, hypotonia, atrophy (in cases of chronic cord compression resulting in cauda equina syndrome)
- Saddle anesthesia
- Absent or decreased rectal tone
- Absent or decreased bulbocavernosus reflex
- Palpable bladder indicating urinary retention 3
It is important to note that in the case of isolated conus medullaris syndrome, deficits of the lower extremities are more often bilateral and symmetric. Also, upper motor neuron signs can be present, such as spasticity and hyperreflexia 2.
Physical examination
Your doctor assesses stability, sensation, strength, reflexes, alignment and motion. He or she may ask you to stand, sit, walk on your heels and toes, bend forward, backward and to the sides, and lift your legs while lying down. Your doctor might check the tone and numbness of anal muscles. You may need blood tests.
Diagnostic imaging
Your doctor may order x-rays, magnetic resonance imaging (MRI) scans, and computed tomography (CT) scans to help assess the problem.
The following tests may be helpful in diagnosing cauda equina syndrome:
- Magnetic resonance imaging (MRI): A diagnostic test that produces three-dimensional images of body structures using magnetic fields and computer technology. MRI produces images of the spinal cord, nerve roots, and surrounding areas.
- Myleogram: An x-ray of the spinal canal following injection of a contrast material into the surrounding cerebrospinal fluid spaces; can show displacement on the spinal cord or spinal nerves due to herniated discs, bone spurs, tumors, etc.
The gold standard method of evaluation for cauda equina syndrome is obtaining urgent MRI imaging with sagittal and axial T1 and T2 sequences 1. There has not been a specific timeframe established for “door to MRI time” in the ED, but early MRI and neurosurgical or orthopedic consultation is imperative. An ideal goal for MRI is one hour from the patient presentation 1. For patients with contraindications to MRI, such as those with metal implants, a CT myelogram is a viable option 1. This imaging modality has limited utility as it requires injecting contrast through a spinal tap to visualize the spinal cord and its associated structures. A bladder scan checking for a post-void residual volume should also be obtained to evaluate for urinary retention 1.
Cauda equina syndrome treatment
If you have cauda equina syndrome, you may need urgent surgery to remove the material that is pressing on the nerves. The goal is to reverse the symptoms of neural dysfunction. The surgery may prevent pressure on the nerves from reaching the point at which damage is irreversible.
Treating patients within 48 hours after the onset of the cauda equina syndrome provides a significant advantage in improving sensory and motor deficits as well as urinary and rectal function 8. But even patients who undergo surgery after the 48-hour ideal timeframe may experience considerable improvement.
Although short-term recovery of bladder function may lag behind reversal of lower extremity motor deficits, the function may continue to improve years after surgery. Following surgery, drug therapy coupled with intermittent self-catheterization can help lead to slow, but steady recovery of bladder and bowel function.
Cauda equina syndrome recovery
Surgery will not repair permanent nerve damage. If this occurs as a result of cauda equina syndrome, you can learn how to improve your quality of life.
Some suggestions:
- In addition to medical personnel, you may want to get help from an occupational therapist, social worker, continence advisor, or sex therapist.
- Involve your family in your care.
- To learn all you can about managing the condition, you may want to join a cauda equina syndrome support group.
Several studies have looked at prognosis and outcomes based on the timing of surgical decompression. Early intervention by surgical decompression in patients with conus medullaris and cauda equina syndromes is associated with a better prognosis, particularly when surgery occurs within 48 hours of initial presentation 8. The longer the compression continues, the worse the permanent structural and functional impairment, and the poorer the prognosis 1. It is important to note that the presence of bladder dysfunction prior to surgery has been linked to poorer outcomes regardless of the timing of decompression, although early decompression is still the recommendation for a better prognosis irrespective of clinical status at initial presentation 1.
Managing bladder and bowel function
Some bladder and bowel function is automatic, but the parts under voluntary control may be lost if you have cauda equina syndrome. This means you may not know when you need to urinate or move your bowels, and/or you may not be able to eliminate waste normally.
Some general recommendations for managing bladder and bowel dysfunction:
- Empty the bladder completely with a catheter 3 to 4 times each day. Drink plenty of fluids and practice regular personal hygiene to prevent urinary tract infection.
- Check for the presence of waste regularly and clear the bowels with gloved hands. You may want to use glycerin suppositories or enemas to help empty the bowels. Use protective pads and pants to prevent leaks.
- Quaile A. Cauda equina syndrome-the questions. Int Orthop. 2018 Oct 29[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Brouwers E, van de Meent H, Curt A, Starremans B, Hosman A, Bartels R. Definitions of traumatic conus medullaris and cauda equina syndrome: a systematic literature review. Spinal Cord. 2017 Oct;55(10):886-890[↩][↩]
- Korse NS, Pijpers JA, van Zwet E, Elzevier HW, Vleggeert-Lankamp CLA. Cauda Equina Syndrome: presentation, outcome, and predictors with focus on micturition, defecation, and sexual dysfunction. Eur Spine J. 2017 Mar;26(3):894-904[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Rider IS, Marra EM. Cauda Equina And Conus Medullaris Syndromes. [Updated 2019 Jan 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537200[↩]
- Ridley LJ, Han J, Ridley WE, Xiang H. Cauda equina: Normal anatomy. J Med Imaging Radiat Oncol. 2018 Oct;62 Suppl 1:123[↩]
- Podnar S. Epidemiology of cauda equina and conus medullaris lesions. Muscle Nerve. 2007 Apr;35(4):529-31.[↩][↩][↩][↩]
- Lavy C, James A, Wilson-MacDonald J, Fairbank J. Cauda equina syndrome. BMJ. 2009 Mar 31;338:b936.[↩][↩]
- Thakur JD, Storey C, Kalakoti P, Ahmed O, Dossani RH, Menger RP, Sharma K, Sun H, Nanda A. Early intervention in cauda equina syndrome associated with better outcomes: a myth or reality? Insights from the Nationwide Inpatient Sample database (2005-2011). Spine J. 2017 Oct;17(10):1435-1448[↩][↩][↩]
- Todd NV. Guidelines for cauda equina syndrome. Red flags and white flags. Systematic review and implications for triage. Br J Neurosurg. 2017 Jun;31(3):336-339.[↩]





{kind=link}