Contents
- Cavernous malformation brain
- Cavernous malformation regional manifestations
- Cerebral cavernous malformation
- Cerebral cavernous venous malformation classification
- What are the chances of a cerebral cavernous malformation bleeding?
- Cerebral cavernous malformation prognosis
- Cavernous malformation brain stem
- Cerebral cavernous malformation causes
- Cerebral cavernous malformation complications
- Cavernous malformation symptoms
- Cavernous malformation diagnosis
- Cavernous malformation treatment
Cavernous malformation brain
Cerebral cavernous malformations are abnormal collections of small blood vessels (capillaries) in the brain and spinal cord that are enlarged and irregular in structure. These capillaries have abnormally thin walls, and they lack other support tissues, such as elastic fibers, which normally make them stretchy. As a result, the blood vessels are prone to leakage, which can cause the health problems related to this condition.
Cavernous malformation is sometimes known as cavernous angioma, cavernous hemangioma, or cerebral cavernous malformation. A typical cavernous malformation looks like a raspberry. It’s filled with blood that flows slowly through vessels that are like “caverns.” A cavernous malformation can vary in size from a few millimeters to several centimeters across. Histologically cavernous malformations are composed of a “mulberry-like” cluster of dilated thin-walled capillaries, with surrounding hemosiderin 1. Unlike arteriovenous malformations (AVMs), there is no normal brain between the interstices of these lesions. On occasion, cavernous malformations are intimately associated with a developmental venous anomaly, in which case they are known as mixed vascular malformation.
Cavernous malformations can occur anywhere in the body, but usually produce serious signs and symptoms only when they occur in the brain and spinal cord (which are described as cerebral cavernous malformation).
Cavernous malformation regional manifestations
Cavernous malformations are found throughout the body.
Central nervous system
- cerebral cavernous venous malformation
- spinal cord cavernous malformation
Head and neck
- cavernous sinus hemangioma
- orbital cavernous venous malformation
- skull vault hemangioma
Chest
- breast venous malformation (breast hemangioma)
- cardiac venous malformations
- mediastinal hemangioma
- pericardial hemangioma
Abdominal
- adrenal hemangioma
- hepatic venous malformation (hepatic hemangioma)
- splenic venous malformation (splenic hemangioma)
- retroperitoneal hemangioma
Musculoskeletal
- soft tissue hemangioma
- synovial hemangioma
- primary intraosseous hemangioma
- vertebral hemangioma
Cerebral cavernous malformation
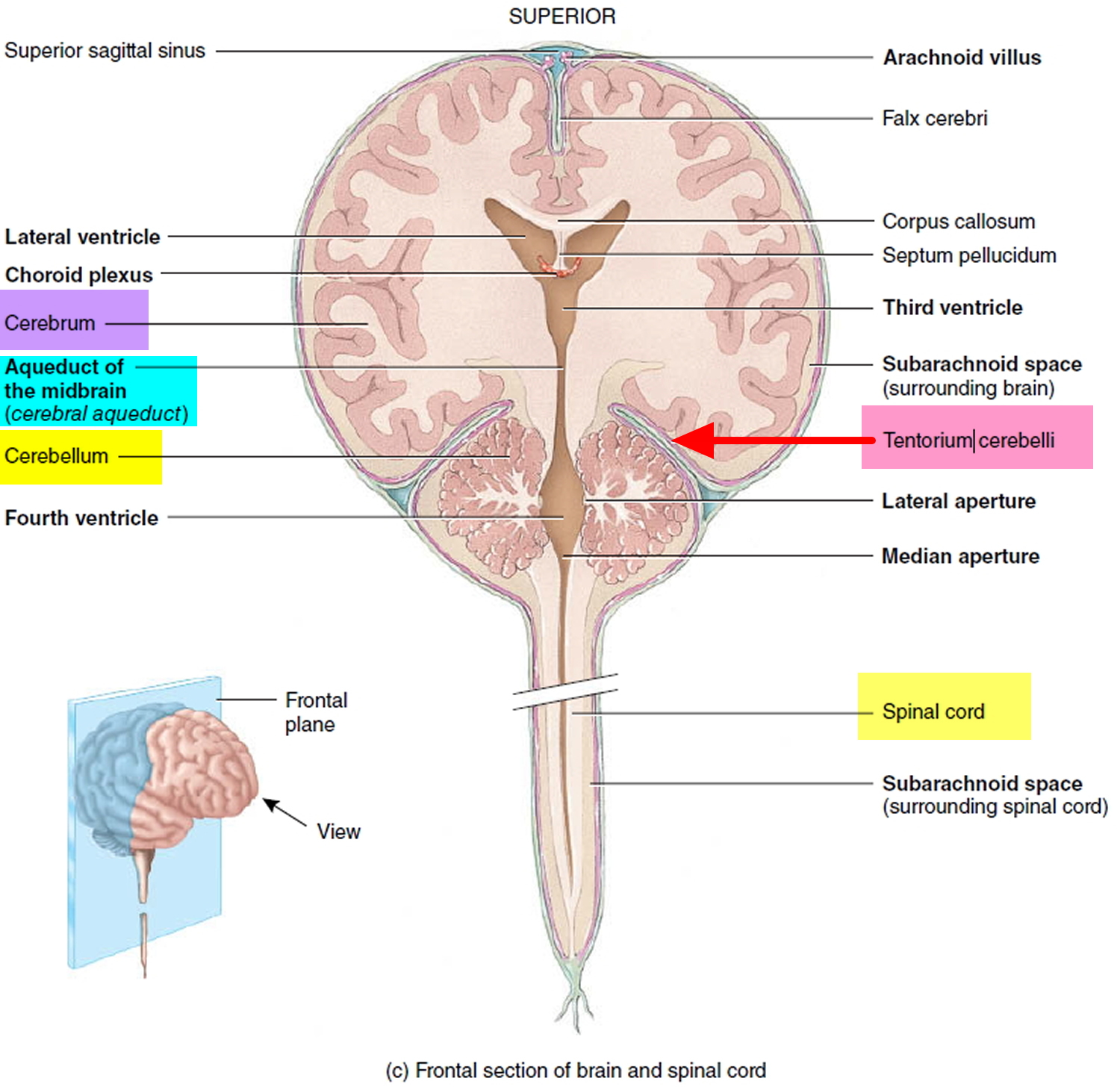
Cerebral cavernomas tend to be supratentorial (~80% cases) but can be found anywhere including the brainstem. Tentorium cerebelli is a transverse shelf of dura mater that forms a partition between the occipital lobe of the cerebral hemispheres and the cerebellum and that covers the cerebellum (see Figures 2 and 3). They are usually solitary, although up to one-third of patients with sporadic lesions have more than one 2.
Approximately 25 percent of individuals with cerebral cavernous malformations never experience any related health problems. Other people with cerebral cavernous malformation may experience serious signs and symptoms such as headaches, seizures, paralysis, hearing or vision loss, and bleeding in the brain (cerebral hemorrhage). The risk of hemorrhage is 1% per year for familial cerebral cavernous malformation and somewhat less for sporadic lesions. Severe brain hemorrhages can result in death. The location and number of cerebral cavernous malformations determine the severity of this disorder. These malformations can change in size and number over time.
Most patients who present symptomatically do so at 40-60 years of age. Most patients have single cerebral cavernous malformation lesion. Multiple cerebral cavernous malformation lesions may be familial and screening of family members may be indicated. Additionally, cavernous malformations, along with capillary telangiectasias, are commonly seen following cerebral radiotherapy 1.
There are two forms of cerebral cavernous malformation: familial and sporadic.
- The familial cerebral cavernous malformation is passed from parent to child, and affected individuals typically have multiple cerebral cavernous malformations.
- The sporadic cerebral cavernous malformation occurs in people with no family history of the disorder. These individuals typically have only one malformation.
Cerebral cavernous malformations affect about 0.5 percent of the population worldwide.
A cerebral cavernous malformation often doesn’t cause symptoms, but when symptoms do occur they can include:
- bleeding (hemorrhage)
- fits (seizures)
- headaches
- neurological problems, such as dizziness, slurred speech (dysarthria), double vision, balance problems and tremor
- weakness, numbness, tiredness, memory problems and difficulty concentrating
- a type of stroke called a hemorrhagic stroke
The severity and duration of symptoms can vary depending on the type of cavernous malformation and where it’s located.
Problems can occur if the cavernous malformation bleeds or presses on certain areas of the brain. The cells lining a cavernous malformation are often thinner than those that line normal blood vessels, which means they’re prone to leaking blood.
In most cases, bleeding is small – usually around half a teaspoonful of blood and may not cause other symptoms. But severe hemorrhages can be life threatening and may lead to longlasting problems.
You should seek medical help as soon as possible if you experience any of the above symptoms for the first time.
Figure 1. Human brain
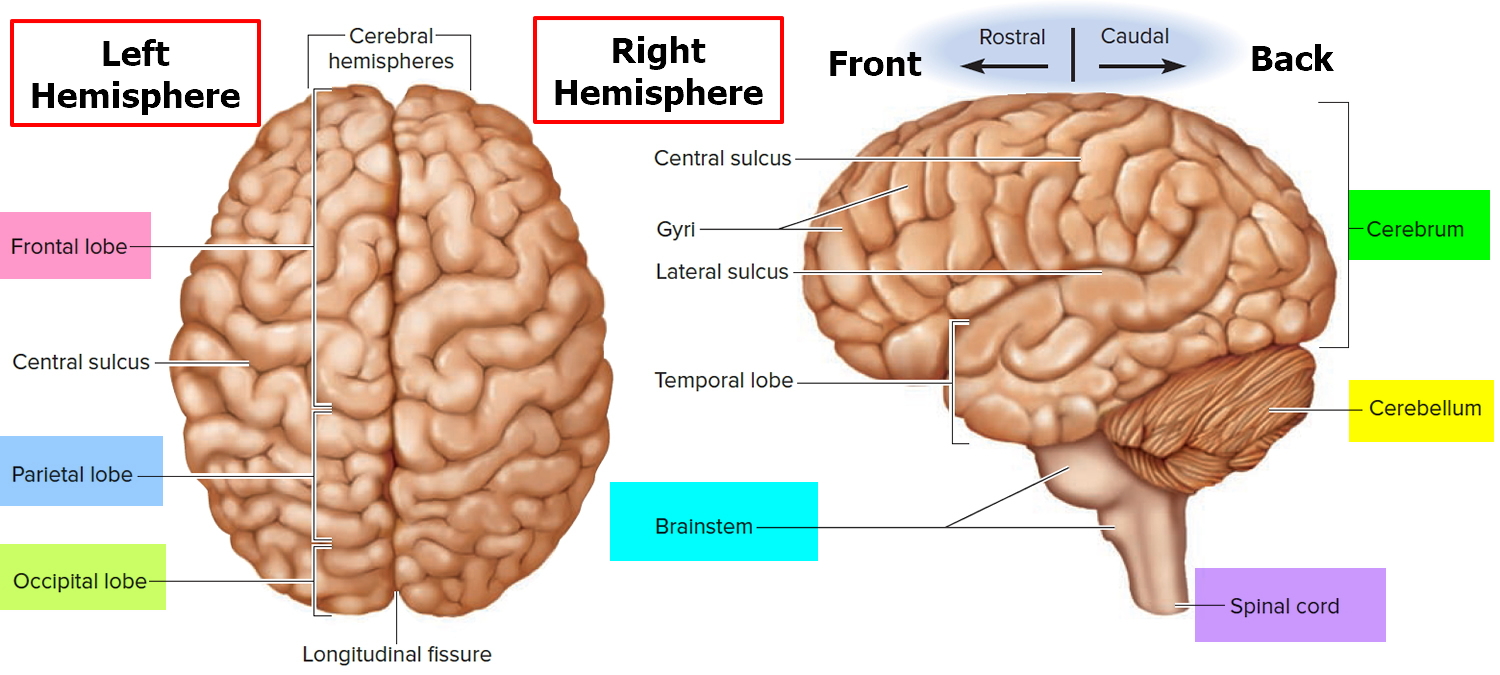
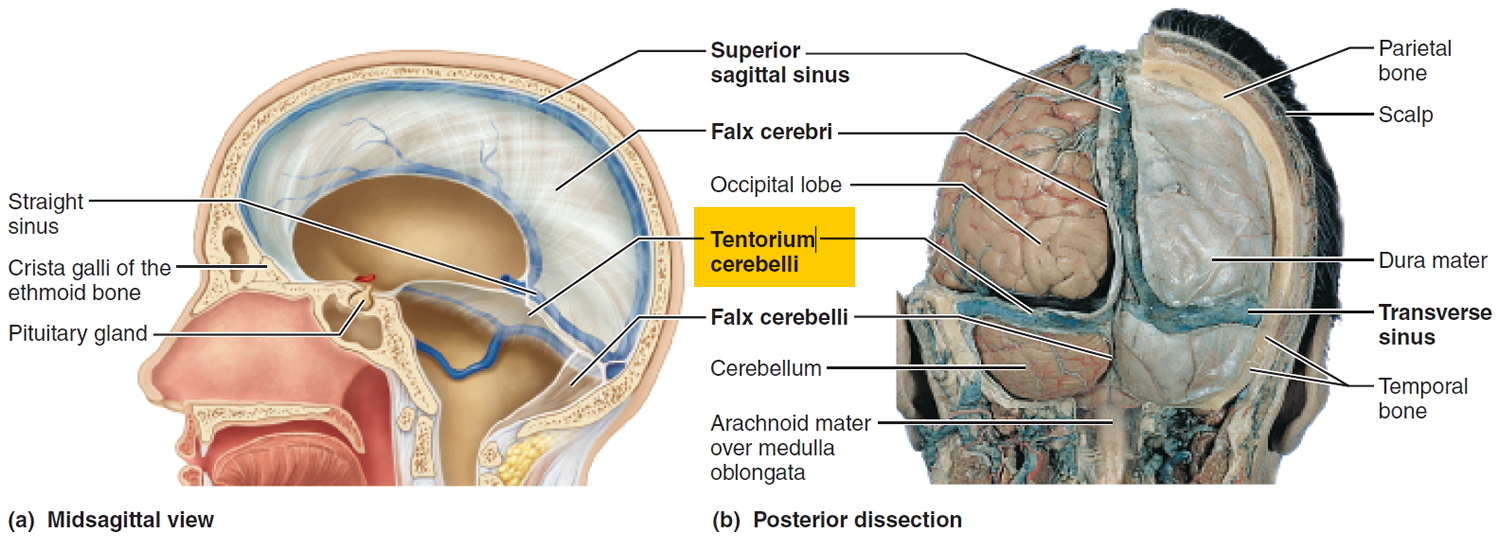
Figure 2. Tentorium cerebelli – resembling a tent over the cerebellum (tentorium means “tent”), this almost horizontal sheet lies in the transverse fissure between the cerebrum and cerebellum.
Seek medical help immediately if you experience any symptoms of seizure, or signs and symptoms that suggest brain hemorrhage, such as:
- Sudden, severe headache
- Nausea
- Vomiting
- Weakness or numbness on one side of the body
- Difficulties in speaking or understanding speech
- Loss of vision
- Double vision
- Balance difficulties
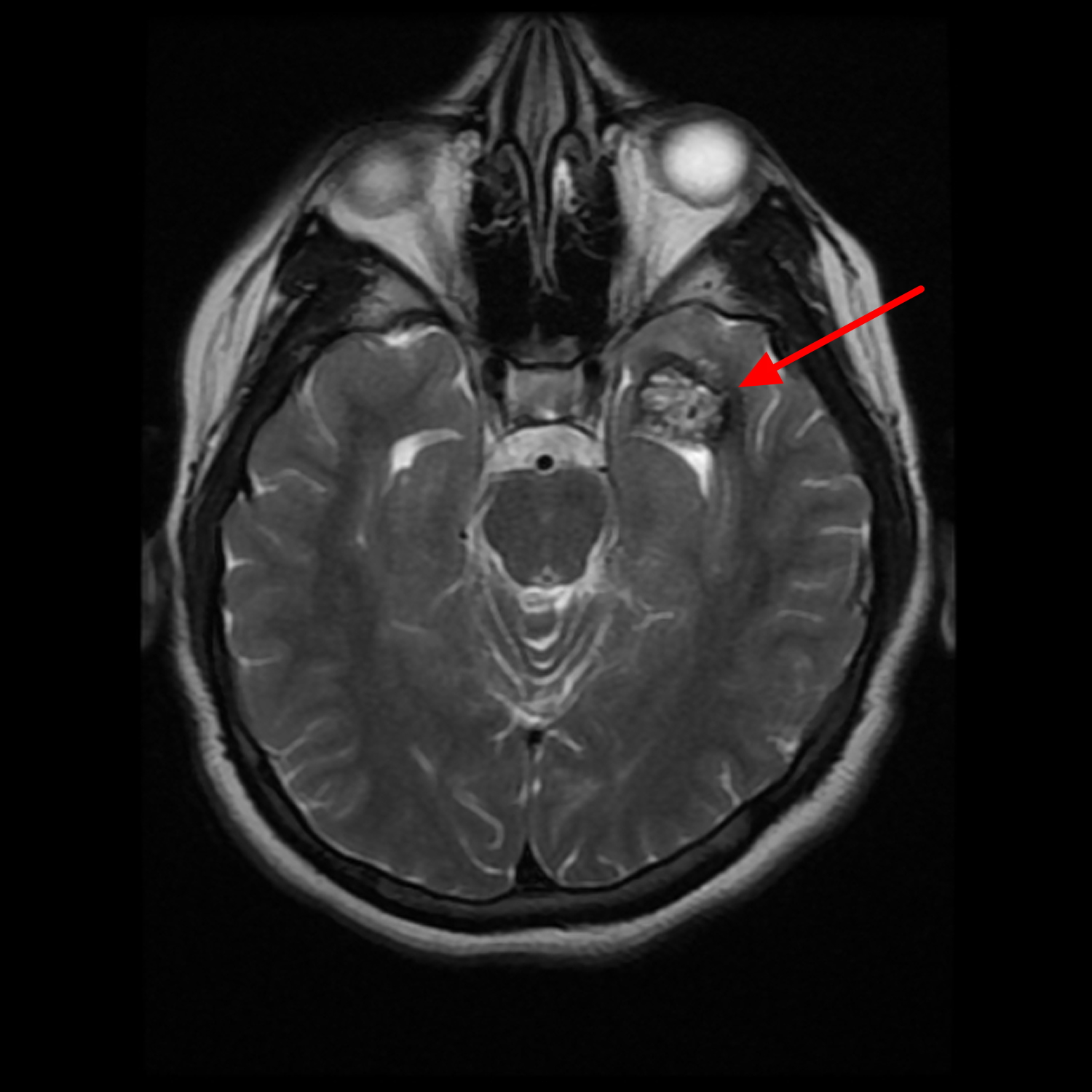
Figure 3. Cerebral cavernous malformation – left temporal intra axial space occupying lesion that displays typical popcorn appearance on MRI scan
Cerebral cavernous venous malformation classification
The Zabramski classification of cerebral cavernous malformation has been proposed as a way of classifying cerebral cavernous malformations, and although not used in clinical practice it is useful in scientific publications that seek to study cavernous malformations.
The classification was proposed in 1994 3, and remains the most commonly used classification of cavernous malformations in the literature.
Cerebral cavernous malformation classification
- Type I: subacute hemorrhage
- T1: hyperintense
- T2: hypo or hyperintense
- Type II: most common type – classic “popcorn” lesion
- T1: mixed signal intensity centrally
- T2: mixed signal intensity centrally
- low signal rim with blooming on T2* sequences
- Type III: chronic hemorrhage
- T1: hypointense to isointense centrally
- T2: hypointense centrally
- low signal rim with blooming on T2* sequences
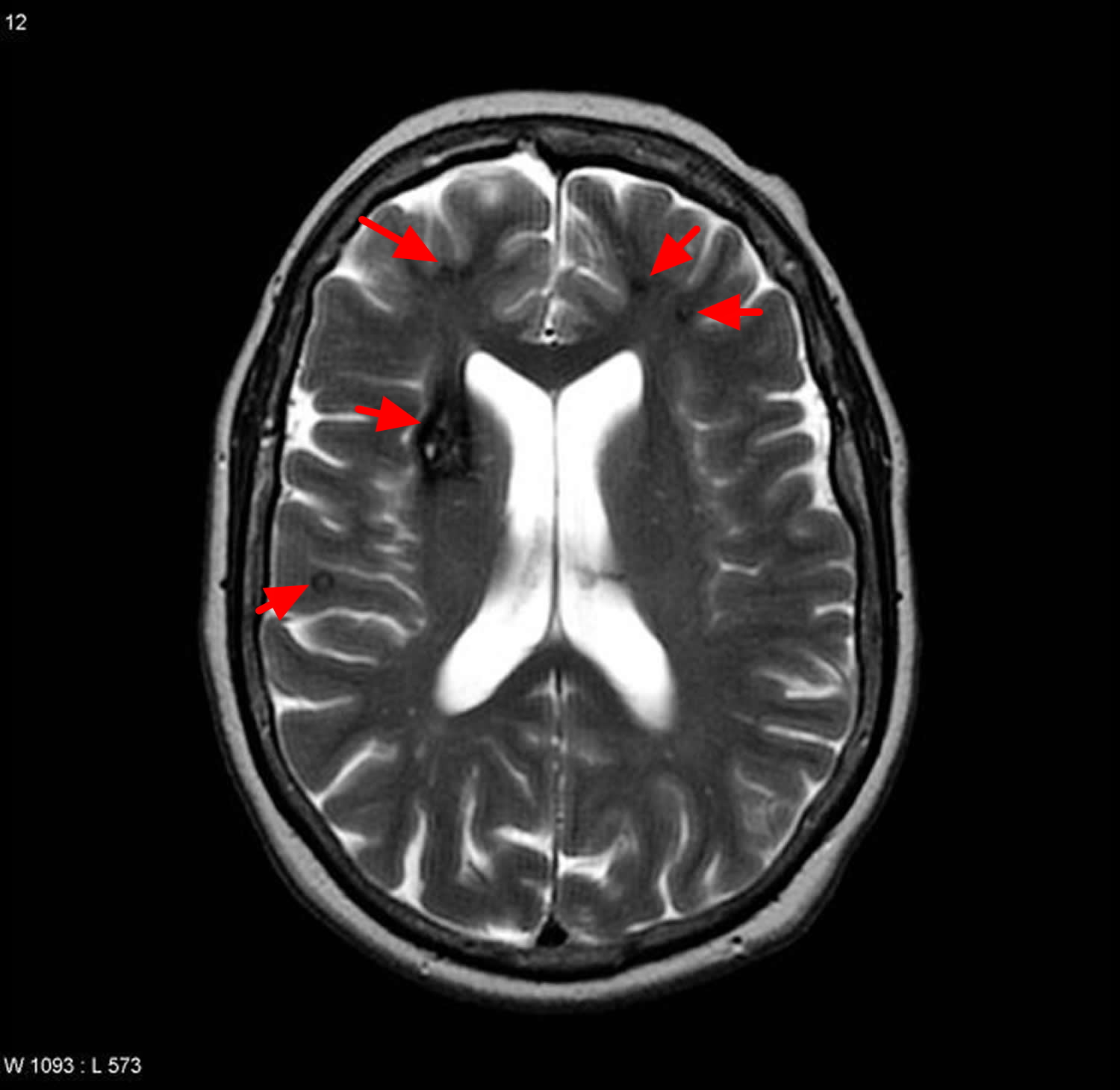
- Type IV: multiple punctate microhaemorrhages
- T1: difficult to identify
- T2: difficult to identify
- T2* Gradient Echo: “black dots” with blooming
- difficult to distinguish from small capillary telangiectasias
Figure 4. Cerebral cavernous malformation Zabramski classification
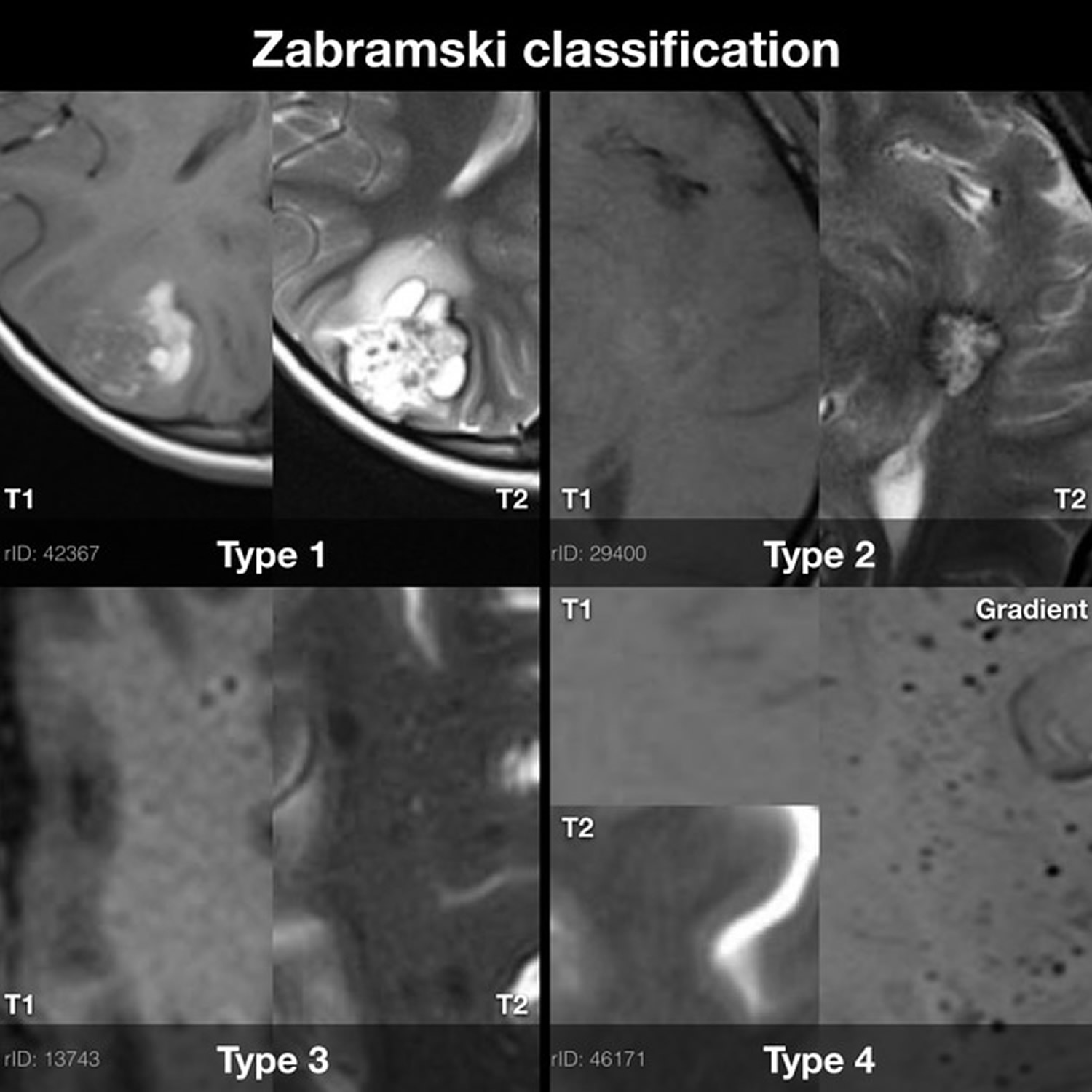
It is worth noting a couple of point about type IV cavernous malformations.
Firstly, the classification proposed in 1994 by Zabramski predates susceptibility weighted imaging (SWI) and as such some authors have suggested that care should be taken in assuming that lesions only seen on susceptibility weighted imaging (SWI) (but not on T2* sequences) are type 4 cavernous malformations 4.
Secondly, how these differ from micro hemorrhages from other causes (e.g. cerebral amyloid angiopathy) is unclear in the absence of genetic evidence of familial multiple cavernous malformation syndrome, as the absence of central T1 / T2 abnormality makes a definite diagnosis of cavernous malformation (in the absence of histology) difficult 5.
What are the chances of a cerebral cavernous malformation bleeding?
The risk of having a hemorrhage varies from person to person, depending on whether you have experienced any bleeding before.
If you haven’t had any bleeding before, it’s estimated you have a less than 1% chance of experiencing a hemorrhage each year.
If your cavernous malformation has bled previously, your risk of having another hemorrhage is somewhere between 4% and 25% each year.
However, this risk decreases progressively over time if you don’t experience any further bleeds, and eventually returns to the same level as that of people who haven’t had any bleeding before.
Your level of risk will be one of the main factors taken into consideration when deciding if you would benefit from treatment.
Hemorrhage Types
Since cerebral cavernous malformation are low pressure, low flow lesions, there is no clearly understood forcing mechanism which would result in a hemorrhage. Most of the bleeding can be divided into three groups:
- “Slow ooze”: blood slowly seeps through the cavern “walls” inside the cavernous malformation itself. Since the internal cavern walls are very weak, it doesn’t take much for blood cells to penetrate them. Normally this does not result in noticeable symptoms, but over time, the lesion’s shape or size can change. Almost all cavernous malformation experience this type of oozing.
- Thrombosis: due to the stagnant nature of the blood in the cavernous malformation caverns, a thrombus (locally developed blockage/clot) can develop which can cause re-routing of the slow internal blood flow as well as growth inside the lesion. Much like 1) above, most times this is not clinically significant unless the lesion reaches a large enough size to impact surrounding brain tissue.
- Gross hemorrhage: blood escapes the confines of the lesion resulting in the deposit of blood products in normal brain tissue around the lesion. It is this hemorrhage type that is most commonly associated with clinical symptoms. Fortunately, the frequency of this hemorrhage type is lower than either 1) or 2). Symptoms primarily depend upon the exact hemorrhage location in the brain.
Preventative Measures and Other Considerations
So if you are diagnosed with a brain cavernous malformation, what precautions should you take? What should or shouldn’t you do?
General consensus among neurosurgeons most familiar and experienced with cerebral cavernous malformations is that patients harboring a lesion should 6:
- Maintain blood pressure as low in the normal range as possible
- Avoid blood thinning or anti-clot medications including aspirin, when possible. This is especially critical for patients whose lesions have demonstrated recent growth or hemorrhage. According to Dr. Issam Awad, chair of the Angioma Alliance scientific board, specific thinners to avoid include Coumadin and aspirin, but also common nonsteroidal antiinflammatory medications such as Advil and Motrin. While many patients take these medications without problem, it is likely that hemorrhage risk is increased; this could be serious with Coumadin. Pros and cons should be discussed between your doctor and the neurospecialist watching the cerebral cavernous malformation. In contrast to the above medications, Tylenol (acetaminophen) is a common pain killer that does not cause bleeding tendency. This is recommended for cerebral cavernous malformation patients.
- Stay away from roller coasters or any activity inducing strong gravitational force
- Stay stress free. Of course, this is much easier said than done! Dr. Awad notes that stress can alter neurological symptoms after a stroke, and can account for fluctuations of symptoms. There is no known physiologic or hormonal basis for this. However, stress can increase blood pressure, which could be a problem in hypertensive patients with increased hemorrhage risk.
Patients with cerebral cavernous malformations can:
- Exercise moderately, but avoid strenuous activities such as heavy weightlifting that can cause acute spikes in blood pressure
- Give birth vaginally as long as the cerebral cavernous malformation is closely managed during the term of pregnancy
- Fly in commercial aircraft with normal cabin pressures
- Consume alcohol and caffeinated beverages in moderation
Dr. Awad notes that there has been some relation shown between diet pills, certain stimulants, and nasal decongestants containing phenylpropranolamine and intracranial hemorrhage in young patients, including possibly cases with cerebral cavernous malformation. These items have been taken off the shelves by the FDA, but it is possible that other excessive stimulants might cause bleeds.
He explains that stimulants may increase blood pressure in hypertensive patients and this could contribute to predisposition to hemorrhagic stroke. Extreme stimulants such as cocaine and other illicit drugs have been shown to cause brain hemorrhages among patients without prior history of high blood pressure, including cases pre-existing vascular malformations.
Hemorrhage and Pregnancy
It has not yet been determined whether there is an increased risk of cavernous malformation hemorrhage during pregnancy. Some researchers believe that increased estrogen during pregnancy causes changes in the walls of cavernous malformation in such a way that they are more likely to leak. However, there are no clear statistics from large scale studies on whether hemorrhages occur more frequently in pregnant women than in others with cavernous malformations. The vast majority of women complete a pregnancy without a hemorrhage or need for surgical removal of a cavernous malformation. However, pregnancy is a time of intense physiologic changes for mother and baby, and the consequences of hemorrhage or seizure may be more complicated than in the non-pregnant state. Any patient with neurovascular problems and/or epilepsy is urged to have their pregnancy overseen by a high risk obstetrician. Your obstetrician should work in close coordination with a neurologist or neurosurgeon that is familiar with your neurological history and who is knowledgeable about cavernous malformations and about epilepsy in pregnancy.
Cerebral cavernous malformation prognosis
Receiving a cavernous angioma diagnosis upon experiencing symptoms is not a death sentence. The majority of lesions don’t bleed and the ones that do normally don’t explode like bombs. They may leak slowly, but this leakage can be enough to cause symptoms in the tight confines of the brain. There simply isn’t enough room to accommodate foreign material such as excess blood. The result is compression or destruction of fragile nerve cells, resulting in symptoms.
The impact of a hemorrhage depends on its location in the brain. For example, the biggest problem faced by patients who have lesions in the temporal lobe is one of seizures. Hemosiderin, a type of aged blood product that can be deposited in adjacent brain tissue after an overt hemorrhage, is a known irritant. It is enough to cause seizures when found in this location.
Those who have brainstem lesions normally suffer multiple and diverse symptoms (“focal neurological deficits”) ranging from double vision, nausea, balance problems, swallowing inability, and respiration difficultly among others.
Surgery is normally considered for those patients who have had more than one bleed in conjunction with worsening symptoms. Lesions such as these are normally considered “aggressive” and need to be removed, assuming the lesion is surgically accessible. While recovery from a hemorrhagic event normally occurs, many times a full recovery is not made. Each hemorrhage brings with it additional symptoms which may not resolve.
When considering surgery, pre-surgical patient condition is very important. The better the person’s physical condition prior to surgery, the better the chances of a successful lesion removal and recovery. Neurosurgeons recommend scheduling surgery within a few months after a bleed. This allows time for excess blood absorption, unmasking the lesion’s boundary relative to healthy brain tissue; however, if surgery is contemplated, it should not be delayed so long after a bleed that the lesion begins to shrink, making extraction more difficult.
Cavernous malformation brain stem
Brainstem cavernous malformations have recently received a great deal of attention due to enhanced imaging techniques and the realization that even small hemorrhagic events can cause significant neurological deficits. While the majority (approx. 75%) of cavernous malformations occur in the upper (“supratentorial”) region of the brain, about 1 in 5 are located in the brainstem or in highly sensitive (“eloquent”), lower (“infratentorial “) areas of the brain 7. The most common symptom for brainstem lesions is focal neurological deficit as opposed to seizure or headache for lesions located in surpratentorial regions.
While people with brainstem cavernous malformations don’t have to worry about seizures, they may have serious vision problems, difficulty coordinating movement, numbness, tingling, neuropathic pain, headaches, balance problems and other cognitive and physical deficits.
While the underlying cause, the cavernous malformation is the same in any part of the brain, the effects and everyday problems are poles apart. In addition, people with multiple cerebral cavernous malformations can have them in both the brain and the brainstem, as well as, possibly, the spinal column.
Figure 5. Cavernous malformation brain stem
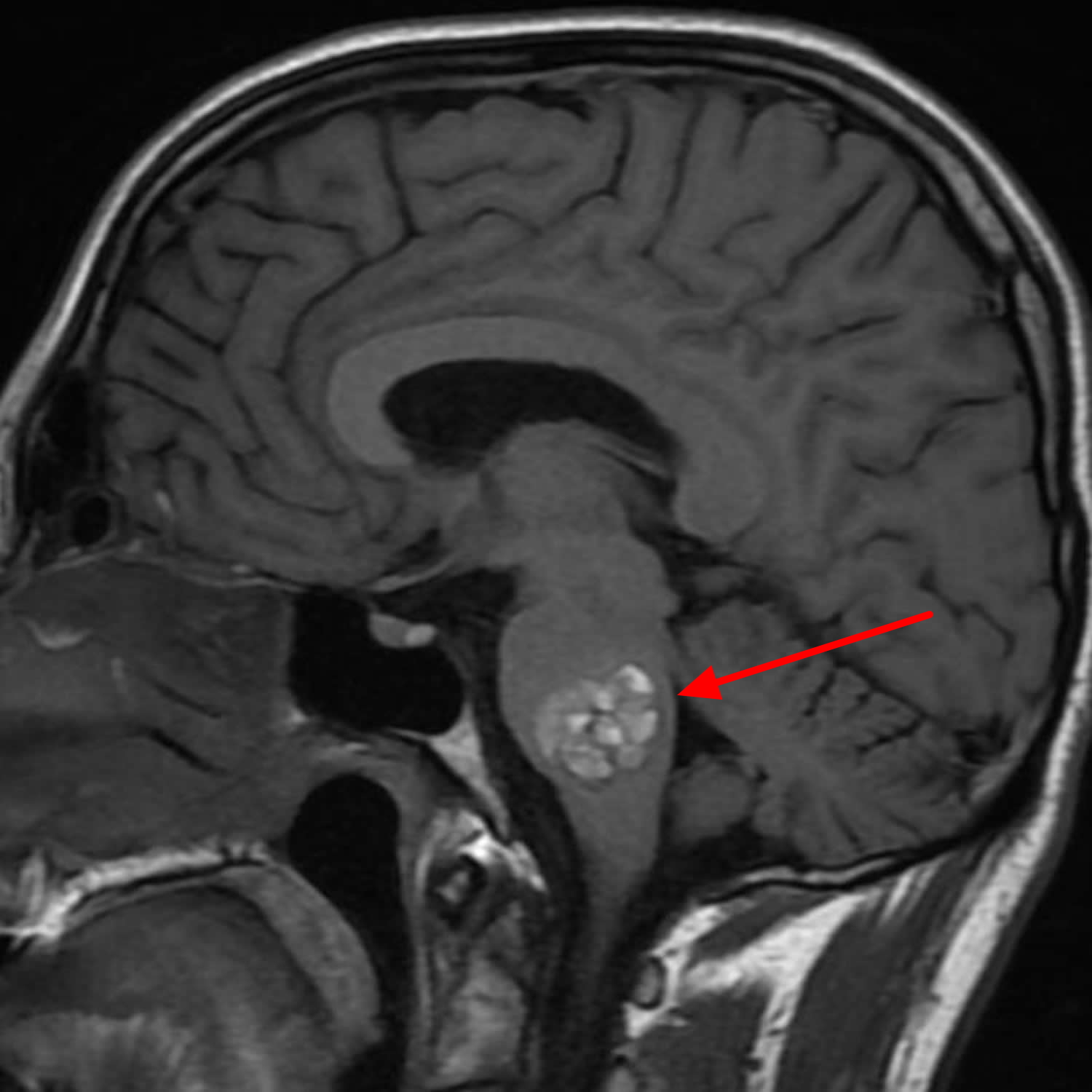
Cavernous malformations of the brainstem present particular problems to both the affected individual as well as the neurosurgeon. Tightly packed nuclei inhabit the narrow conduit of the brainstem. Any additional mass or introduction of fluid, such as blood products from a bleed, can compress or crush important nerve fibers 8. In other words, the smallest of intrusions can result in significant, and potentially life-threatening, symptoms. The nerves that transverse the brainstem control basic, involuntary functions such as respiration, gag reflex, heartbeat regulation, body temperature, pain and heat sensation, and hiccupping as well as other voluntary functions including eye movement, swallowing, facial muscle control, walking, and speech. Both cranial and “long tract” (whole body) nerves can be affected. For the individual, a brainstem cavernous malformation can manifest a disparate range of symptoms making diagnosis difficult. The neurosurgeon must worry about how to manage the case and whether the inherent risks of brainstem surgery are worth the potential beneficial rewards.
While the root cause of a cavernous malformation hemorrhage is not yet understood, there are some consensus guidelines relating specifically to brainstem cavernous malformation case management:
- Watch and wait (“conservative” case management). This consists of routine, periodic MRIs to monitor the changes in the lesion. As long as the lesion appears stable and there are no additional symptoms or evidence of hemorrhage, this is usually the most prudent course of action.
- Surgical removal (“resection”) may be considered if at least one of the following is true 9:
- The lesion abuts the surface of the brainstem that abuts the pia mater, the outer covering of the brain. This type of lesion is called “exophytic”.
- Repeated hemorrhages result in progressively worse deficits
- Acute hemorrhage is external to the “capsule” of the lesion. In other words, blood from a hemorrhage is entering brain tissue surrounding the cavernous malformation.
- The cavernous malformation has grown to a point where it is pressing upon surrounding brain tissue in a way that causes a visible compression of the surrounding tissue.
One study measured re-hemorrhaging rates as high as 30% per person per year 9. Other studies show varying rates of re-bleeding.
Venous anomalies are frequently associated with cavernous malformations of the brainstem. One study found that all 86 patients met this criterion. It is important to note that any associated venous anomalies should remain undisturbed during surgical resection of cavernous malformations, as they provide functional drainage 9. Elimination of these anomalies can result in infarction and death.
Surgical approaches involving cutting through the floor of the 4th ventricle should be avoided at all costs 9. This does not preclude surgery as an option should the cavernous malformation abut the 4th ventricle floor; rather, the neurosurgeon must steer clear of approaching the lesion through the floor of this ventricle.
Stereotactic radiosurgery (“gamma knife”) is generally not an accepted method of treatment for brainstem cavernous malformations 10. Relatively high morbidity rates can result, although one study noted reduced hemorrhage rates after radiosurgery 11. Unlike radiotherapy for arteriovenous malformations (AVMs), stereotactic radiosurgery does not result in obliteration of the malformation 12. At a minimum, radiosurgery treatment for brainstem cavernous malformation is controversial.
Given the advancement in minimally invasive surgical techniques, more and more neurosurgeons are becoming comfortable with surgical removal of cavernous malformations from the brainstem; however, the potential for significant functional deficits from surgical complications is still significant. This risk must not be taken lightly. The decision to proceed with surgery should be weighed very carefully and implemented only on a case-by-case basis. Assuming one meets the criteria established in part 2 above, one may wish to ask some additional lifestyle questions to help arrive at a decision:
- Can I still drive?
- Can I work?
- Can I take care of the family?
- Can I… (whatever else is important in your life)?
- Are the symptoms becoming progressively worse?
- Am I in decent physical condition to survive the rigors of brain surgery?
- Am I young enough such that the odds of having another hemorrhage are greater than if I were much older?
- Do I have enough of a support network to help me transcend the potentially arduous recovery process?
Finally, here is a word about diagnostics and imaging. Smaller cavernous malformations are somewhat difficult to detect. Insist that one of your MRI sequences consists of “gradient-echo” or T2 sequences MRI (as opposed to spin-echo or proton beam) imaging. Gradient echo or T2* sequences are able to delineate these lesions better than T1 or T2 weighted images. In patients with familial or multiple cavernous angiomas GRE T2* sequences are very important in identifying the number of lesions missed by conventional Spin echo sequences. Gradient-echo MRI is most efficient at detecting small, or even punctate (point sized), cavernous malformations 13. Even though a spin-echo MRI may have detected a lesion, it’s always prudent to ensure that there are not additional, smaller lesions which might become a problem later in life.
Cerebral cavernous malformation causes
In most cerebral cavernous malformations occur as a single formation, without an apparent cause and without any family history. However, in a small percentage, cerebral cavernous malformation can sometimes run in families – roughly 20 percent of cases are thought to be genetic and most often with multiple malformations. Mutations in at least three genes, KRIT1 (also known as CCM1), CCM2, and PDCD10 (also known as CCM3), cause familial cerebral cavernous malformations. Genetic testing can be carried out to determine whether a cavernous malformation is genetic or whether it’s occurred randomly or sporadic.
Some cerebral cavernous malformation cases have also been linked to radiation exposure, such as previously having radiotherapy to the brain, usually as a child.
The precise functions of these genes are not fully understood. Studies show that the proteins produced from these genes are found in the junctions connecting neighboring blood vessel cells. The proteins interact with each other as part of a complex that strengthens the interactions between cells and limits leakage from the blood vessels. Mutations in any of the three genes impair the function of the protein complex, resulting in weakened cell-to-cell junctions and increased leakage from vessels as seen in cerebral cavernous malformations.
Mutations in these three genes account for 85 to 95 percent of all cases of familial cerebral cavernous malformations. The remaining 5 to 15 percent of cases may be due to mutations in unidentified genes or to other unknown causes. Mutations in the KRIT1, CCM2, and PDCD10 genes are not involved in sporadic cerebral cavernous malformations. The cause of this form of the condition is unknown.
Familial cerebral cavernous malformation has an autosomal dominant pattern of inheritance, which means one copy of the altered gene in each cell is sufficient to cause the disorder. In the familial cerebral cavernous malformation, an affected person inherits the mutation from one affected parent.
Risk factors for cavernous malformation brain
As mentioned above, while most cavernous malformations in the brain occur with no clear cause, the genetic (inherited familial) form of the condition can cause multiple cavernous malformations, both initially and over time.
To date, research has identified three genetic variants responsible for familial cavernous malformations, to which almost all familial cases of cavernous malformations have been traced.
Cerebral cavernous malformation complications
The most concerning complications of cerebral cavernous malformations stem from recurrent bleeding (hemorrhage), which may lead to progressive neurological damage.
Hemorrhages are more likely to recur in people with prior diagnosed hemorrhages. They’re also more likely to reoccur with malformations located in the brainstem.
Cavernous malformation symptoms
Cerebral cavernous malformations may exist without apparent symptoms. Any symptoms you have may come and go as the cavernous malformation bleeds and then reabsorbs blood. It’s important to closely monitor your symptoms, as any new symptoms might be a sign of a hemorrhage.
Obvious symptoms tend to occur when recurrent episodes of bleeding or blood clot formation lead either to seizures, for upper lobe cerebral cavernous malformations, or to focal or vision issues, for cerebral cavernous malformations in the brainstem, basal ganglia and spinal cord.
Generally, signs and symptoms of cerebral cavernous malformations, may include weakness, numbness, difficulty speaking, difficulty understanding others, unsteadiness, vision changes or severe headache. Seizures also can occur, and neurological issues can progressively worsen over time with recurrent bleeding (hemorrhage). Repeat bleeding can occur soon after an initial bleed or much later, or a repeat bleed may never occur.
Your doctor can advise you about what to do if you experience any new or worsening symptoms. They may also recommend having a further brain scan.
Magnetic resonance imaging (MRI) and computerized tomography (CT) scans can be used to detect bleeding on the brain, although they can’t necessarily identify cavernous malformations that are at an increased risk of bleeding.
This is because the features of a cavernous malformation that can be seen on a brain scan, such as an increase in size, don’t appear to be directly linked to the likelihood of bleeding.
Although cavernous malformations can get bigger, large cavernous malformations aren’t any more likely to bleed than smaller ones.
Cavernous malformation diagnosis
Magnetic resonance imaging (MRI) scans are mainly used to diagnose cavernous malformations. As symptoms aren’t always evident, many people are only diagnosed with a cavernous malformation after having an MRI scan for another reason.
A computerized tomography (CT) scan or angiography can also be used to diagnose cavernous malformation, but they’re not as reliable as an MRI scan.
Genetic testing. If you have a family history of the condition, genetic counseling and tests are helpful to identify changes associated with cerebral cavernous malformations in genes or chromosomes.
MRI
MRI is the modality of choice, demonstrating a characteristic “popcorn” or “berry” appearance with a rim of signal loss due to hemosiderin, which demonstrates prominent blooming on susceptibility weighted sequences.
T1 and T2 signal is varied internally depending on the age of the blood products and small fluid-fluid levels may be evident.
Gradient echo or T2* sequences are able to delineate these lesions better than T1 or T2 weighted images. In patients with familial or multiple cavernous angiomas GRE T2* sequences are very important in identifying the number of lesions missed by conventional Spin echo sequences.
Susceptibility weighted imaging (SWI) may have sensitivity equal to that of GRE in detecting these capillary telangiectasias in the brain. SWI is also highly sensitive in detecting calcification as compared to T1 and T2 images 14.
If a recent bleed has occurred then surrounding edema may be present.
The lesions generally do not enhance, although enhancement is possible 15.
Cavernous malformations can be grouped into four types based on MRI appearances using the Zabramski classification 16.
Cavernous malformation treatment
The recommended treatment for cavernous malformation will vary depending on an individual’s circumstances and factors such as size, location and number.
Some cavernous malformation symptoms, such as headaches and seizures, can be controlled with medication.
However, more invasive treatment may sometimes be offered to reduce the risk of future hemorrhages. The decision to have such treatment is made on a case-by-case basis in discussion with your doctors. Doctors trained in brain and nervous system conditions (neurologists and cerebrovascular neurologists), brain and nervous system surgery (neurosurgeons), brain imaging (neuroradiologists), and other specialties work with you to treat cerebral cavernous malformations as well as other neurological conditions.
Observation
If you’re not experiencing symptoms, your doctor may initially decide to monitor your cavernous malformation, especially since risk is generally lower for those who are non-symptomatic. Sometimes intermittent testing such as magnetic resonance imaging (MRI) is recommended to watch for any changes in the malformation. Let your doctor know right away about any changes in your symptoms.
Medications
If you have seizures related to a cavernous malformation, you may be prescribed medications to stop the seizures.
Surgery
If you’re experiencing symptoms related to a cavernous malformation that can be reached surgically, your doctor may recommend surgery to remove the malformation.
Types of treatment offered in the US to reduce the risk of hemorrhages include:
- neurosurgery – carried out under general anaesthetic to remove the cavernous malformation
- stereotactic radiosurgery – where a single, concentrated dose of radiation is aimed directly at the cavernous malformation, causing it to become thickened and scarred
In most cases, neurosurgery is preferred to stereotactic radiosurgery because the effectiveness of radiosurgery in preventing haemorrhages is unknown.
Stereotactic radiosurgery is usually only considered if the position of the cavernous malformation makes neurosurgery too difficult or dangerous.
Risks of invasive treatment include stroke and death, although the exact risks depend on the location of the cavernous malformation. You should discuss the possible risks of treatment with your doctor beforehand.
Potential future treatments
Several imaging technology areas hold promise for both improving predictions of the course of disease in some specific contexts and for enhancing the level of information available about a particular individual’s disease state, including potential advances in imaging through quantitative susceptibility mapping (QSM), permeability imaging using dynamic contrast-enhanced MRI, and the use of alternative MRI contrast agents such as ferumoxytol. While still under investigation, such developments hold promise for enhanced imaging that may lead to more precise and effective clinical care in the future.
- Jain R, Robertson PL, Gandhi D et-al. Radiation-induced cavernomas of the brain. AJNR Am J Neuroradiol. 2005;26 (5): 1158-62. AJNR Am J Neuroradiol. http://www.ajnr.org/content/26/5/1158.full[↩][↩]
- Blitstein MK, Tung GA. MRI of cerebral microhemorrhages. AJR Am J Roentgenol. 2007;189 (3): 720-5. doi:10.2214/AJR.07.2249 https://www.ncbi.nlm.nih.gov/pubmed/17715122[↩]
- Zabramski JM, Wascher TM, Spetzler RF et-al. The natural history of familial cavernous malformations: results of an ongoing study. J. Neurosurg. 1994;80 (3): 422-32. doi:10.3171/jns.1994.80.3.0422 http://thejns.org/doi/abs/10.3171/jns.1994.80.3.0422[↩]
- de Souza JM, Domingues RC, Cruz LC et-al. Susceptibility-weighted imaging for the evaluation of patients with familial cerebral cavernous malformations: a comparison with t2-weighted fast spin-echo and gradient-echo sequences. AJNR Am J Neuroradiol. 2008;29 (1): 154-8. doi:10.3174/ajnr.A0748 http://www.ajnr.org/content/29/1/154.long[↩]
- Greenberg SM, Vernooij MW, Cordonnier C et-al. Cerebral microbleeds: a guide to detection and interpretation. Lancet Neurol. 2009;8 (2): 165-74. doi:10.1016/S1474-4422(09)70013-4 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3414436/[↩]
- Cerebral Cavernous Angioma and Hemorrhage. http://www.angiomaalliance.org/pages.aspx?content=69&id=60[↩]
- Samii M, Eghbal R, Carvalho GA, Matthies C. Surgical management of brainstem cavernomas. J Neurosurg. 2001 Nov;95(5):825-32.[↩]
- Fritschi JA, Reulen HJ, Spetzler RF, Zabramski JM. Cavernous malformations of the brain stem. A review of 139 cases. Acta Neurochir (Wien). 1994;130(1-4):35-46. Review.[↩]
- Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, Zabramski JM. Cavernous malformations of the brainstem: experience with 100 patients. J Neurosurg. 1999 Jan;90(1):50-8.[↩][↩][↩][↩]
- Seo Y, Fukuoka S, Takanashi M, Nakagawara J, Suematsu K, Nakamura J, Nagashima K. Gamma Knife surgery for angiographically occult vascular malformations. Stereotact Funct Neurosurg. 1995;64 Suppl 1:98-109.[↩]
- Kondziolka D, Lunsford LD, Flickinger JC, Kestle JR. Reduction of hemorrhage risk after stereotactic radiosurgery for cavernous malformations. J Neurosurg. 1995 Nov;83(5):825-31.[↩]
- Amin-Hanjani S, Ogilvy CS, Candia GJ, Lyons S, Chapman PH. Stereotactic radiosurgery for cavernous malformations: Kjellberg’s experience with proton beam therapy in 98 cases at the Harvard Cyclotron. Neurosurgery. 1998 Jun;42(6):1229-36; discussion 1236-8.[↩]
- Clatterbuck RE, Moriarity JL, Elmaci I, Lee RR, Breiter SN, Rigamonti D. Dynamic nature of cavernous malformations: a prospective magnetic resonance imaging study with volumetric analysis. J Neurosurg. 2000 Dec;93(6):981-6.[↩]
- Zhu WZ, Qi JP, Zhan CJ et-al. Magnetic resonance susceptibility weighted imaging in detecting intracranial calcification and hemorrhage. Chin. Med. J. 2008;121 (20): 2021-5. Chin. Med. J. https://www.ncbi.nlm.nih.gov/pubmed/19080268[↩]
- Pinker K, Stavrou I, Knosp E et-al. Are cerebral cavernomas truly nonenhancing lesions and thereby distinguishable from arteriovenous malformations? MRI findings and histopathological correlation. Magn Reson Imaging. 2006;24 (5): 631-7. doi:10.1016/j.mri.2005.10.037 https://www.ncbi.nlm.nih.gov/pubmed/16735186[↩]
- Zabramski JM, Wascher TM, Spetzler RF et-al. The natural history of familial cavernous malformations: results of an ongoing study. J. Neurosurg. 1994;80 (3): 422-32. doi:10.3171/jns.1994.80.3.0422 http://thejns.org/doi/abs/10.3171/jns.1994.80.3.042[↩]





{kind=link}