Contents
- Cervical cancer
- Types of cervical cancer
- Cervical cancer signs and symptoms
- Cervical cancer causes
- Cervical cancer risk factors
- Human papilloma virus (HPV) infection
- Smoking
- Having a weakened immune system
- Chlamydia infection
- Many sexual partners
- Early sexual activity
- Other sexually transmitted infections (STIs)
- A diet low in fruits and vegetables
- Being overweight
- Long-term use of oral contraceptives (birth control pills)
- Intrauterine device (IUD) use
- Having multiple full-term pregnancies
- Young age at first full-term pregnancy
- Economic status
- Diethylstilbestrol (DES)
- Having a family history of cervical cancer
- Cervical cancer risk factors
- Cervical cancer prevention
- Cervical cancer diagnosis
- Cervical cancer stages
- Treatment of cervical cancer
- Cervical cancer treatment by stage
- Cervical cancer during pregnancy
- Cervical cancer prognosis
- HPV and Cancer
- What is HPV?
- How do people get HPV ?
- Cancers linked to HPV infection
- Can HPV infection be prevented ?
- Testing for HPV
- Treatment for HPV or HPV-related diseases
- Things to remember about HPV
- HPV Vaccine Facts and Fears
- Fact 1: The vaccine is safe.
- Fact 2: The HPV vaccine causes no bad side effects.
- Fact 3: The HPV vaccine does not cause fertility problems.
- Fact 4: The HPV vaccine does not contain harmful ingredients.
- Fact 5: Getting the HPV vaccine is not opening the door to having sex.
- Fact 6: The HPV vaccine is for both males and females.
- Fact 7: The HPV vaccine works and can help prevent cervical cancer.
- Fact 8: The HPV vaccine lasts a long time – maybe forever.
Cervical cancer
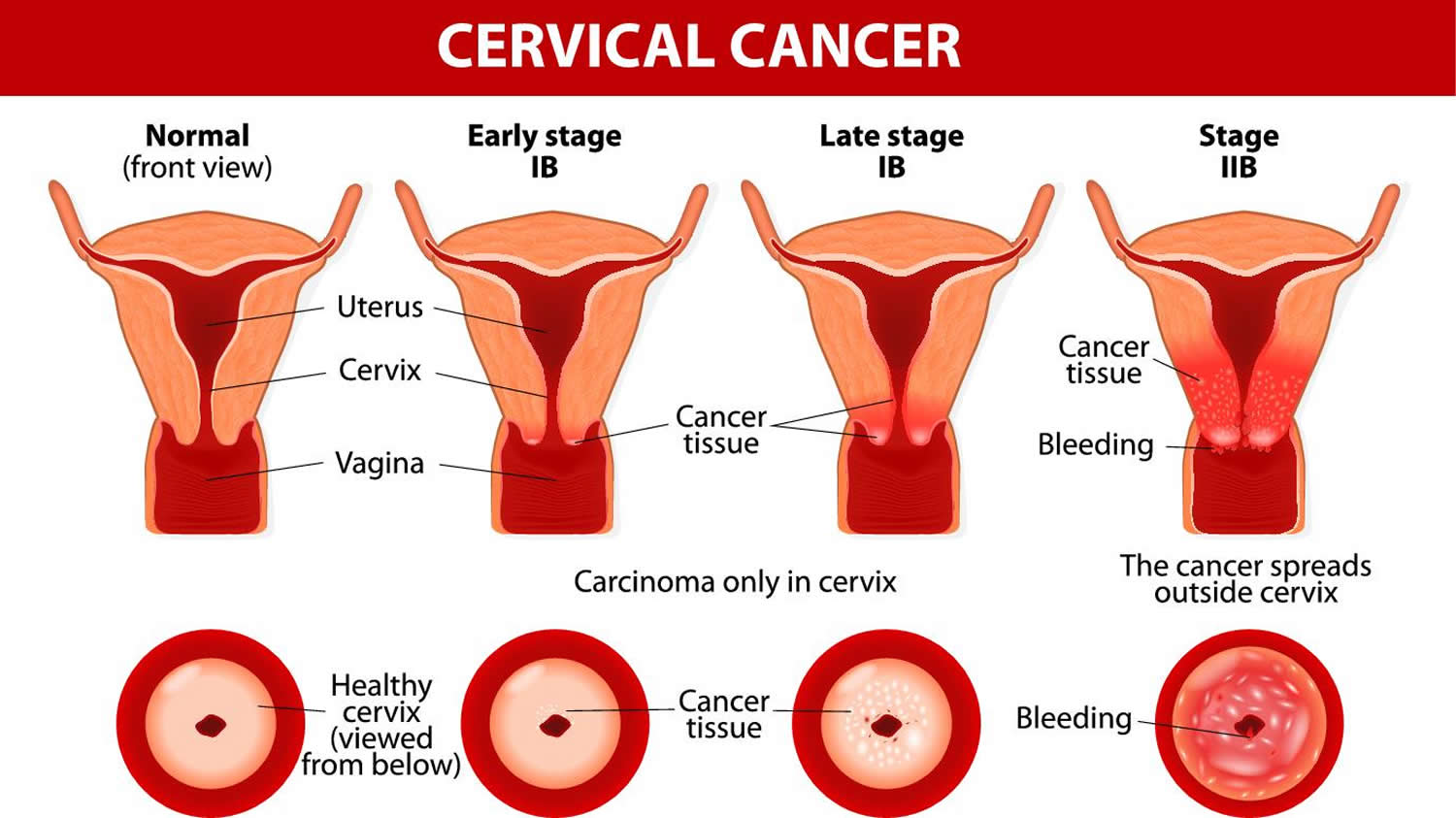
Cervical cancer is cancer that starts in the cells lining the cervix (the organ connecting the uterus and vagina) 1. Cervical cancer is usually a slow-growing cancer that may not have symptoms but can be found with regular Pap tests (a procedure in which cells are scraped from the cervix and looked at under a microscope). Cervical cancer is almost always caused by human papilloma virus (HPV) infection 1.
The cervix is the lowest part of the uterus (womb). The lumen (internal cavity) of the uterus communicates with the vagina by way of a narrow passage through the cervix called the cervical canal (see Figure 1 and 2).
Various strains of the human papilloma virus (HPV), a sexually transmitted infection, play a role in causing most cervical cancer. When exposed to HPV, a woman’s immune system typically prevents the virus from doing harm. In a small group of women, however, the virus survives for years, contributing to the process that causes some cells on the surface of the cervix to become cancer cells.
In many cases, cervical cancer can be prevented. You can reduce your risk of developing cervical cancer by avoiding getting HPV, get regular Pap tests and receiving a vaccine that protects against HPV infection. HPV vaccine can protect young people against the virus. The vaccine is FDA-approved for all boys and girls between 9 years and 26 years of age. HPV vaccine is most effective when you get it before you have been exposed to HPV. The Centers for Disease Control and Prevention (CDC) recommends that girls and boys who are 11 or 12 get the HPV vaccine. But anyone age 26 or younger should get the HPV vaccine, even if you’ve already had HPV.
Other ways to lower your risk of getting HPV include:
- Limit your number of sex partners.
- Don’t have sex with someone who has had a lot of partners.
- Use condoms anytime you have sex. Remember, condoms aren’t 100% effective. HPV is spread by skin-to-skin contact. This makes condoms less reliable for prevention.
Cervical Cancer Location
Cervical cancer starts in the cells lining the cervix — this is sometimes called the uterine cervix. The fetus grows in the body of the uterus (the upper part). The cervix connects the body of the uterus to the vagina (birth canal).
The cervix is made of two different parts and is covered with two different types of cells.
- The part of the cervix closest to the body of the uterus is called the endocervix and is covered with glandular cells. These glandular cells produce mucus. The glandular cells of the endocervix can become cancerous, leading to an adenocarcinoma of the cervix.
- The outer part of the cervix next to the vagina is the exocervix (or ectocervix) and is covered with a layer of skin-like cells on its outer surface called squamous cells. The skin-like cells of the ectocervix can become cancerous, leading to a squamous cell cervical cancer. This is the most common type of cervical cancer.
The place where these two cell types meet in the cervix is called the transformation zone (see Figure 3 and 4). The transformation zone is the area that your doctor checks during cervical screening. The exact location of the transformation zone changes as you age and if you give birth.
- Most cervical cancers begin in the cells in the transformation zone 2. These cells do not suddenly change into cancer. Instead, the normal cells of the cervix first gradually develop abnormal changes that are called pre-cancerous. Doctors use several terms to describe these pre-cancerous changes, including cervical intraepithelial neoplasia (CIN), squamous intraepithelial lesion (SIL), and dysplasia. These changes can be detected by the Pap test. Cervical pre-cancers are diagnosed far more often than invasive cervical cancer.
When the pre-cancerous changes are checked in the lab, they are graded on a scale of 1 to 3 based on how much of the cervical tissue looks abnormal.
- In CIN1 also called mild dysplasia or low grade squamous intraepithelial lesion (SIL), not much of the tissue looks abnormal, and it is considered the least serious cervical pre-cancer.
- In CIN2 or CIN3 also called moderate or severe dysplasia or high-grade squamous intraepithelial lesion (SIL), more of the tissue looks abnormal; high-grade SIL is the most serious pre-cancer.
Although cervical cancers start from cells with pre-cancerous changes (pre-cancers), only some of the women with pre-cancers of the cervix will develop cancer. It usually takes several years for cervical pre-cancer to change to cervical cancer, but it can happen in less than a year. For most women, pre-cancerous cells will go away without any treatment. Still, in some women pre-cancers turn into true (invasive) cancers. Treating all cervical pre-cancers can prevent almost all cervical cancers.
The American Cancer Society estimates for cervical cancer in the United States for 2023 are 3, 4:
- New cases: About 13,960 new cases of invasive cervical cancer will be diagnosed.
- Deaths: About 4,310 women will die from cervical cancer.
- 5-Year Relative Survival: 67.2%. Relative survival is an estimate of the percentage of patients who would be expected to survive the effects of their cancer. It excludes the risk of dying from other causes. Because survival statistics are based on large groups of people, they cannot be used to predict exactly what will happen to an individual patient. No two patients are entirely alike, and treatment and responses to treatment can vary greatly.
- Cervical cancer deaths as a percentage of All Cancer Deaths: 0.7%.
- Rate of New Cases and Deaths per 100,000: The rate of new cases of cervical cancer was 7.7 per 100,000 women per year. The death rate was 2.2 per 100,000 women per year. These rates are age-adjusted and based on 2016–2020 cases and deaths.
- Lifetime Risk of Developing cervical cancer: Approximately 0.7 percent of women will be diagnosed with cervical cancer at some point during their lifetime, based on 2017–2019 data.
- In 2020, there were an estimated 296,981 women living with cervical cancer in the United States.
Cervical cancer is most frequently diagnosed in women between the ages of 35 and 44 with the average age at diagnosis being 50. It rarely develops in women younger than 20. Many older women do not realize that the risk of developing cervical cancer is still present as they age. More than 20% of cases of cervical cancer are found in women over 65. However, these cancers rarely occur in women who have been getting regular tests to screen for cervical cancer before they were 65.
In its early stages, cervical cancer may not have any symptoms. In later stages, cervical cancer symptoms could include:
- Unusual vaginal bleeding (not during your menstrual cycle)
- Abnormal vaginal discharge
- Pelvic pain
- Pain during sex
If you experience any of these symptoms, see your doctor.
Cervical cancer was once one of the most common causes of cancer death for American women. The cervical cancer death rate dropped significantly with the increased use of the Pap test. During a Pap test, your doctor takes a sample of cells from your cervix. The sample is sent to a lab and checked under a microscope. This screening procedure can find changes in the cervix before cancer develops. It can also find cervical cancer early − when it’s small and easier to cure.
In recent years, the HPV test has been approved as another screening test for cervical cancer since almost all cervical cancers are caused by HPV (human papillomavirus). The HPV test looks for infection by high-risk types of HPV that are more likely to cause pre-cancers and cancers of the cervix. The HPV test can be used alone (primary HPV test) or at the same time as the Pap test (called a co-test).
If the results of your Pap test are abnormal, your doctor may repeat the test. He or she may also do a cervical HPV test. This test can show if you have one of the types of HPV that can cause cancer. Your doctor may want you to have a colposcopy. During this procedure, he or she will use a magnifying lens to look more closely at your cervix. They can also take a sample of tissue (biopsy) to test for cancer.
Cells of the cervix go through many changes before they turn into cancer. A Pap test can show if your cells are going through these changes. If caught and treated early, cervical cancer is not life threatening. This is why it is so important that you get regular Pap tests.
Invasive cervical cancer treatment options depend on the size of the tumor and how far the cancer has spread. They also may depend on your plans for having children in the future. The most common treatments include:
- Surgery — The cancerous tissue is removed in an operation.
- Radiation —High-energy rays like X-rays shrink or kill the cancerous cells.
- Chemotherapy — Powerful medicines, in pill form or injected into the veins, shrink or kill the cancer.
Treatment of invasive cancer often involves a team of specialists. This could include your family doctor, a gynecologist, and an oncologist (cancer specialist). You will all work together to develop the best treatment plan for you.
Figure 1. Cervix position
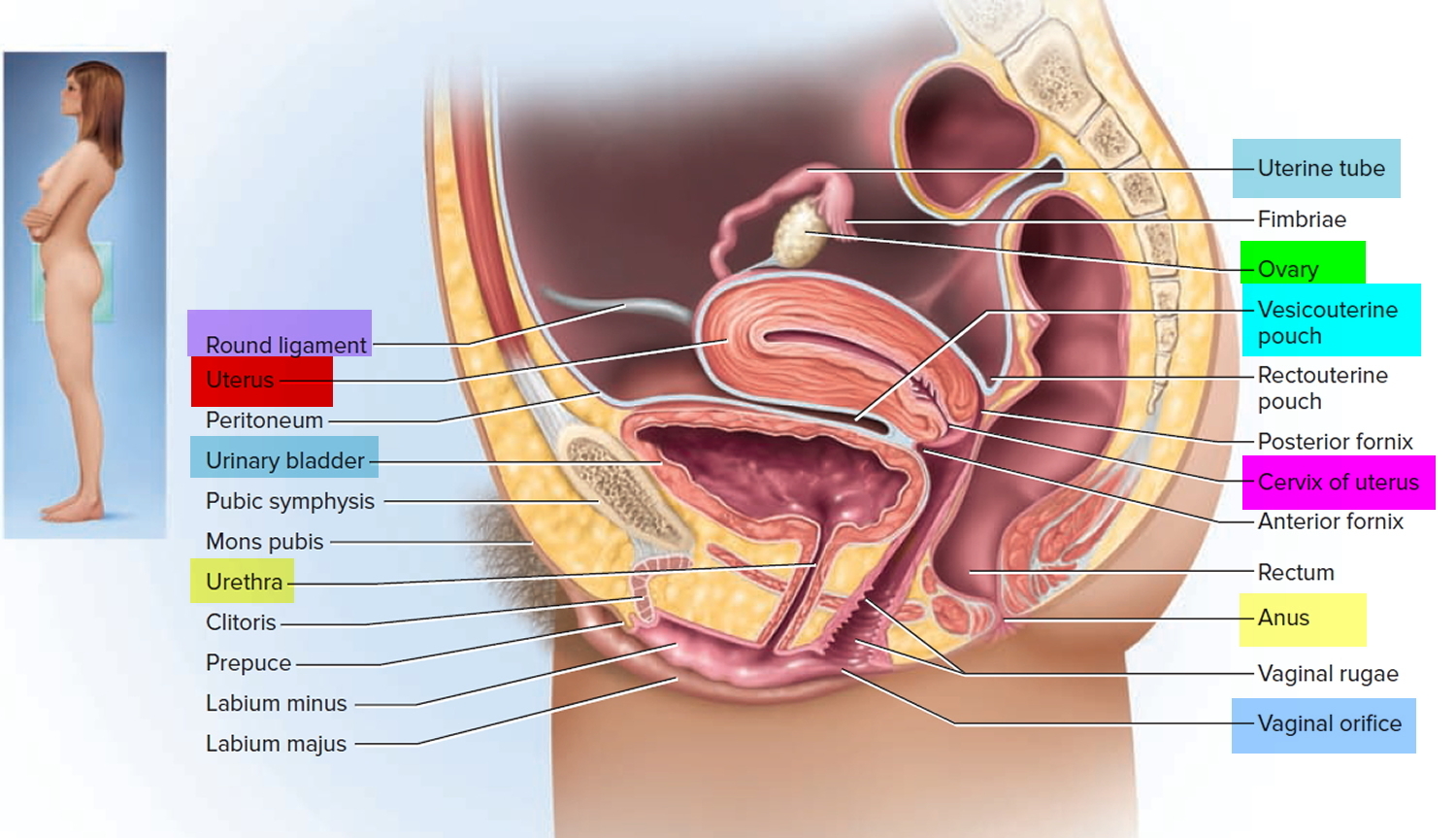
Figure 2. Cervix location
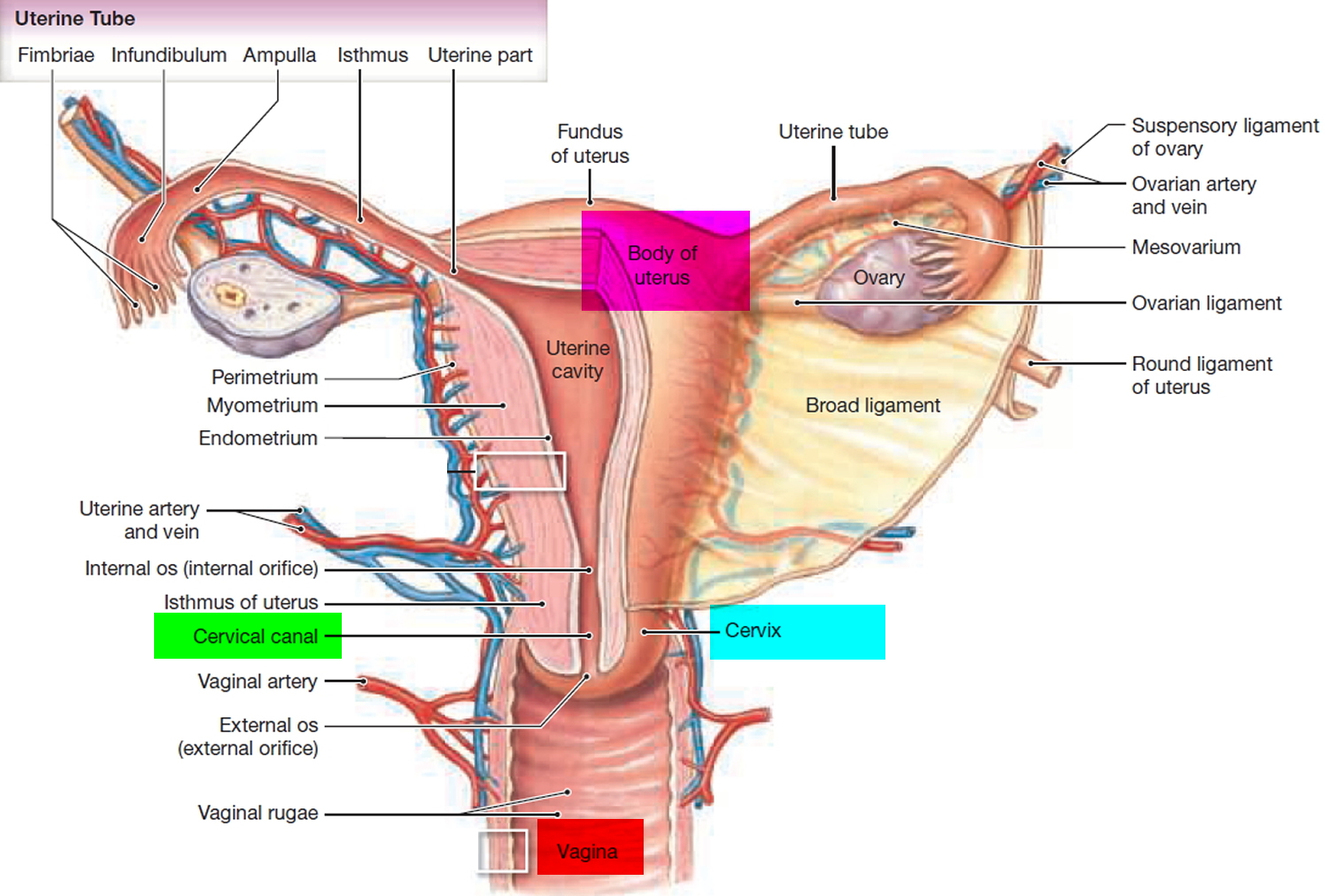
Figure 3. Transformation zone on the cervix
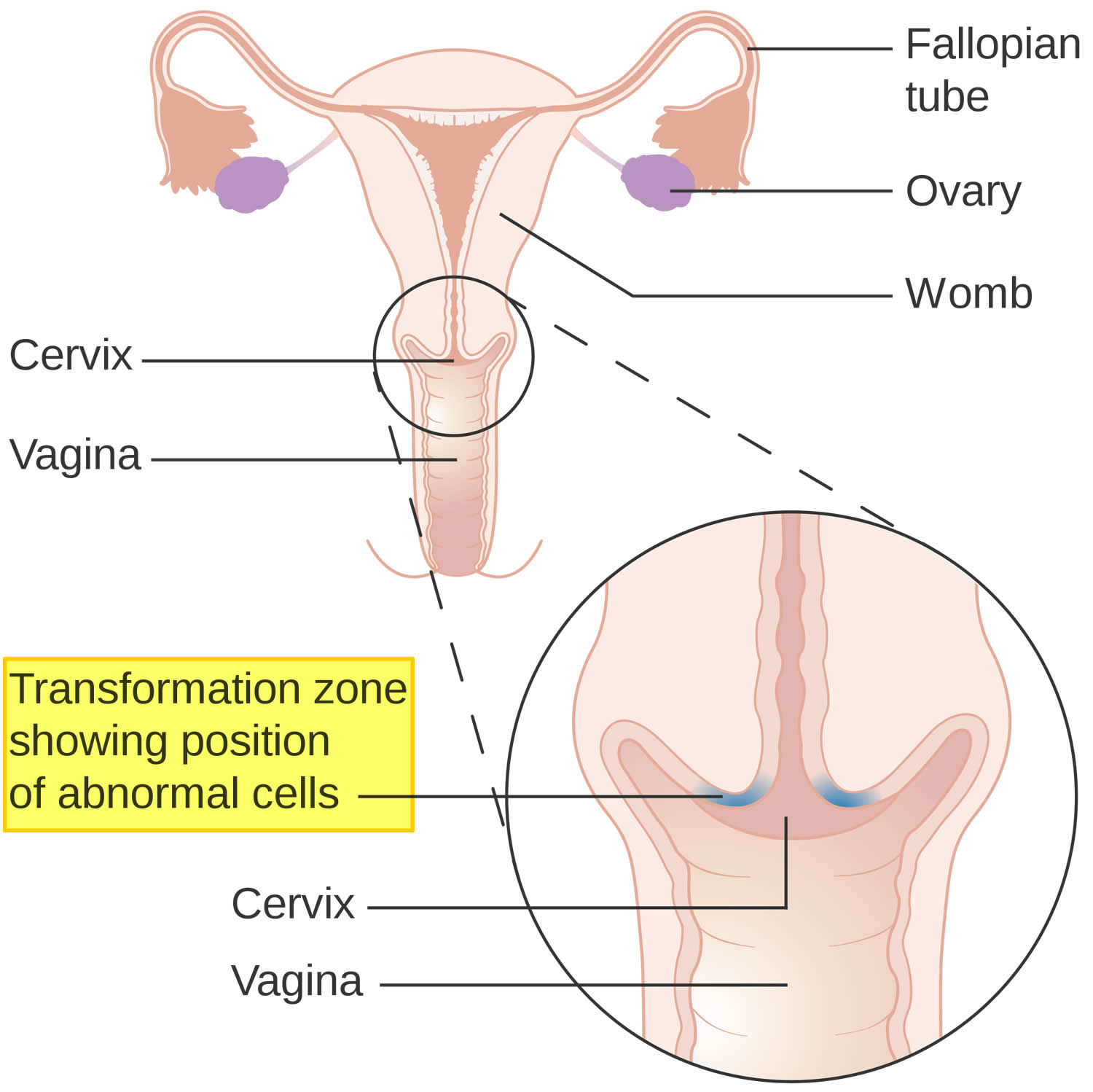
Figure 4. Cervical transformation zone
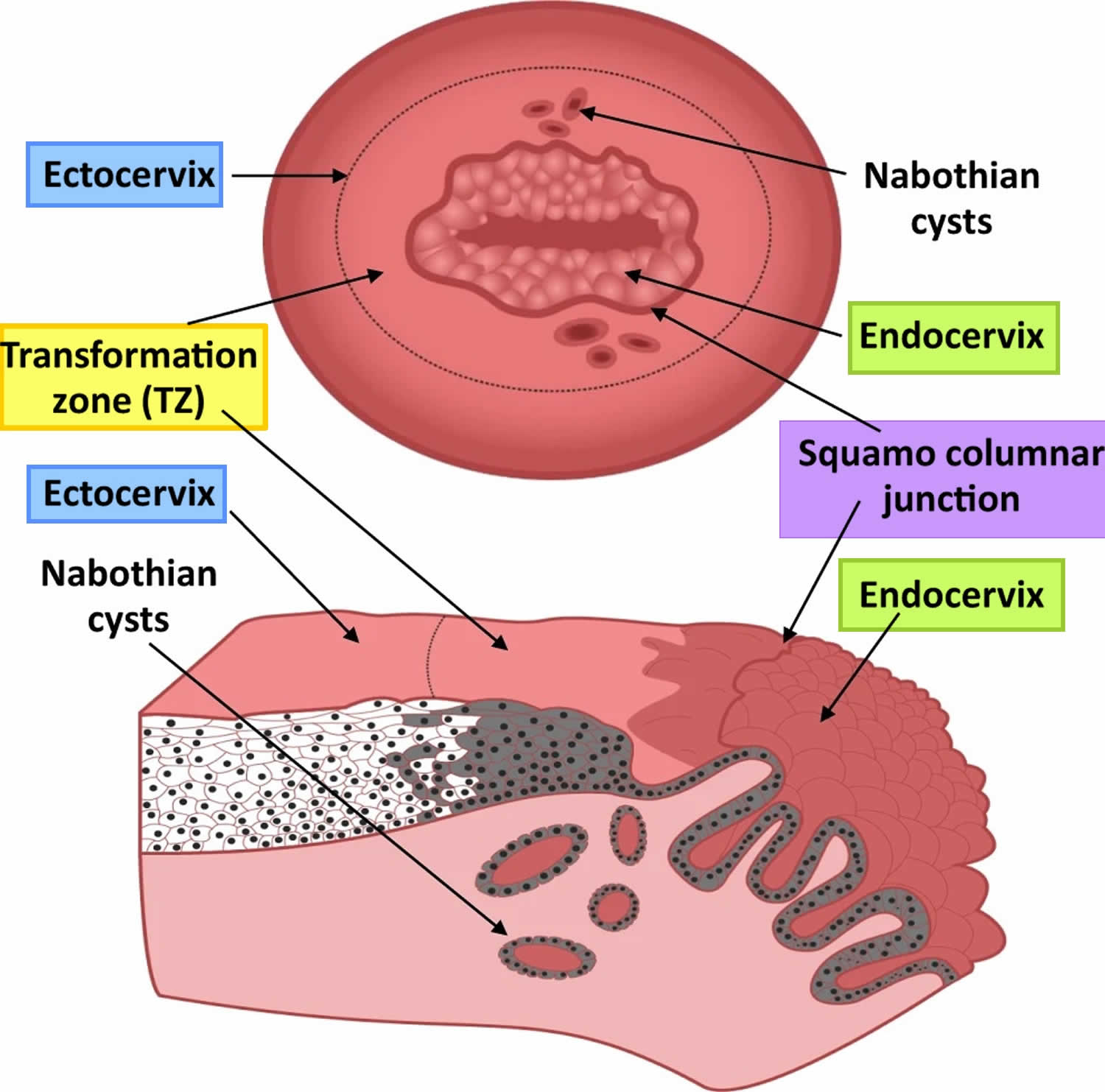
Footnotes: Schematic of the cervical transformation zone. (Top) View of cervix as seen through gynecologist’s speculum showing ectocervix, transformation zone with Nabothian cysts, and endocervix. (Bottom) Cross section of transformation zone showing columnar epithelium of endocervix and stratified squamous epithelium of transformation zone and ectocervix. Nabothian cysts form when mucous ducts of endocervix become occluded by overgrowth of stratified squamous epithelium from newly formed transformation zone. Brown shading illustrates cells derived from endocervical reserve cells.
[Source 5 ]Types of cervical cancer
Cervical cancers and cervical pre-cancers are classified by how they look under a microscope. There are different types of cervical cancer.
The main types of cervical cancers are:
- Squamous cell carcinoma
- Adenocarcinoma.
Most (up to 9 out of 10) cervical cancers are squamous cell carcinomas. These cancers form from cells in the ectocervix and the cancer cells have features of squamous cells under the microscope. Squamous cells are the flat, skin-like cells that cover the outer surface of the cervix (the ectocervix). Squamous cell carcinomas most often begin in the transformation zone (where the ectocervix joins the endocervix) (Figures 3 and 4).
Most of the other cervical cancers are adenocarcinomas. Adenocarcinomas are cancers that develop from gland cells. Cervical adenocarcinoma develops from the mucus-producing gland cells of the endocervix. Cervical adenocarcinomas seem to have become more common in the past 20 to 30 years.
Less commonly (5 to 6% of cervical cancer) , cervical cancers have features of both squamous cell carcinomas and adenocarcinomas. These are called adenosquamous carcinomas or mixed carcinomas.
Although almost all cervical cancers are either squamous cell carcinomas or adenocarcinomas, other types of cancer also can develop in the cervix.
Small cell cancer of the cervix is a very rare type of cervical cancer. Around 3 in every 100 women (3%) diagnosed with cervical cancer have this type. Small cell cancers tend to grow quickly and are treated in a different way to the more common types of cervical cancer.
Other rarer types of cervical cancer, such as melanoma, sarcoma, and lymphoma, occur more commonly in other parts of the body.
Cervical cancer signs and symptoms
Women with early cervical cancers and cervical pre-cancers usually have no symptoms. Symptoms often do not begin until the cancer becomes larger and grows into nearby tissue. When this happens, the most common symptoms are:
- Abnormal vaginal bleeding, such as bleeding after vaginal sex, bleeding after menopause, bleeding and spotting between periods, or having (menstrual) periods that are longer or heavier than usual. Bleeding after douching may also occur.
- An unusual discharge from the vagina − the discharge may contain some blood and may occur between your periods or after menopause.
- Pain during sex
- Pain in the pelvic region
Signs and symptoms seen with more advanced cervical cancer can include:
- Swelling of the legs
- Problems urinating or having a bowel movement
- Blood in the urine
These signs and symptoms can also be caused by conditions other than cervical cancer. Still, if you have any of these symptoms, see a health care professional right away. Ignoring symptoms may allow the cancer to grow to a more advanced stage and lower your chance for successful treatment.
Cervical cancer causes
Cervical cancer begins when healthy cells acquire a genetic change (mutation) that causes them to turn into abnormal cells. Healthy cells grow and multiply at a set rate, eventually dying at a set time. Cancer cells grow and multiply out of control, and they don’t die. The accumulating abnormal cells form a mass (tumor). Cancer cells invade nearby tissues and can break off from a tumor to spread (metastasize) elsewhere in the body.
It isn’t clear what causes cervical cancer, but it’s certain that long lasting (persistent) infection of certain types of the human papilloma virus (HPV) plays a role. HPV is very common, and in most cases your immune system clears the infection without any problems and most women with the virus never develop cervical cancer. This means other factors — such as your environment or your lifestyle choices — also determine whether you’ll develop cervical cancer. Other risk factors, like smoking and HIV infection, influence which women exposed to HPV are more likely to develop cervical cancer.
Human papillomaviruses (HPV) have two proteins known as E6 and E7 which turn off some tumor suppressor genes (genes that help keep cell growth under control or make cells die at the right time), such as p53 and Rb. This may allow the cells lining the cervix to grow too much and to develop changes in additional genes, which in some cases can lead to cancer.
Each year in the United States, about 46,143 new cases of cancer are found in parts of the body where human papillomavirus (HPV) is often found 6. HPV causes about 36,500 of these cancers.
Genital human papillomavirus (HPV) is the most common sexually transmitted infection in the United States 7. More than 40 HPV types can infect the genital areas of men and women, including the skin of the penis, vulva (area outside the vagina), and anus, and the linings of the vagina, cervix, and rectum. These types can also infect the lining of the mouth and throat.
Most people who become infected with HPV do not know they have it. Usually, the body’s immune system gets rid of the HPV infection naturally within two years. This is true of both oncogenic and non-oncogenic HPV types. By age 50, at least 4 out of every 5 women will have been infected with HPV at one point in their lives. HPV is also very common in men, and often has no symptoms.
Cervical cancer risk factors
A risk factor is anything that increases your chance of getting a disease such as cancer. Several risk factors can increase your chance of developing cervical cancer. People without any of these risk factors rarely develop cervical cancer. Although these risk factors can increase the odds of developing cervical cancer, many with these risks do not develop this disease.
When you think about risk factors, it helps to focus on those you can change or avoid (like smoking or human papillomavirus infection), rather than those you cannot (such as your age and family history). However, it is still important to know about risk factors that cannot be changed, because it’s even more important for women who have these factors to get regular Pap tests to detect cervical cancer early.
Cervical cancer risk factors include:
- Many sexual partners. The greater your number of sexual partners — and the greater your partner’s number of sexual partners — the greater your chance of acquiring HPV.
- Early sexual activity. Having sex at an early age increases your risk of HPV.
- Other sexually transmitted infections (STIs). Having other STIs — such as chlamydia, gonorrhea, syphilis and HIV/AIDS — increases your risk of HPV.
- A weakened immune system. You may be more likely to develop cervical cancer if your immune system is weakened by another health condition and you have HPV.
- Smoking. Smoking is associated with squamous cell cervical cancer.
- Exposure to miscarriage prevention drug. If your mother took a drug called diethylstilbestrol (DES) while pregnant in the 1950s, you may have an increased risk of a certain type of cervical cancer called clear cell adenocarcinoma.
Human papilloma virus (HPV) infection
The most important risk factor for cervical cancer is infection by the human papilloma virus (HPV). The human papillomavirus (HPV) is a non-enveloped, double-stranded, circular DNA virus that is the most prevalent sexually transmitted infection 8. HPV is a group of more than 200 related viruses, some of which cause a type of growth called papillomas, which are more commonly known as warts. Individuals with persistent HPV infection and those who have multiple sexual partners are at very high risk for acquiring more HPV subtypes 9.
- HPV can infect cells on the surface of the skin, and those lining the genitals, anus, mouth and throat, but not the blood or internal organs such as the heart or lungs.
- HPV can be spread from one person to another during skin-to-skin contact. One way HPV is spread is through sex, including vaginal, anal, and even oral sex.
- Different types of HPV cause warts on different parts of the body. Some cause common warts on the hands and feet; others tend to cause warts on the lips or tongue.
Certain types of HPV may cause warts on or around the female and male genital organs and in the anal area. These are called low-risk types of HPV or “non-oncogenic” (wart-causing) HPV because they are seldom linked to cancer.
Other types of HPV are called high-risk types or “oncogenic” (cancer-causing) HPV because they are strongly linked to cancers, including cancers of the cervix, vulva, and vagina in women, penile cancer in men, and cancers of the anus, mouth and throat in men and women. The International Agency for Research on Cancer found that 13 HPV types can cause cervical cancer, and at least one of these types can cause cancers of the vulva, vagina, penis, anus, and certain head and neck cancers (specifically, the oropharynx, which includes the back of the throat, base of the tongue and tonsils) 10. The types of HPV that can cause genital warts are not the same as the types that can cause cancer. The high-risk types include HPV 16, HPV 18, HPV 31, HPV 33, and HPV 45, as well as some others. There might be no visible signs of infection with a high-risk HPV until pre-cancerous changes or cancer develops.
About 10% of women with HPV infection on their cervix will develop long-lasting HPV infections that put them at risk for cervical cancer 7.
Doctors believe that a woman must be infected with HPV in order to develop cervical cancer. Although this can mean infection with any of the high-risk types, about two-thirds of all cervical cancers are caused by HPV 16 and 18.
Infection with HPV is common, and in most people the body can clear the infection by itself. Sometimes, however, the infection does not go away and becomes chronic. Chronic infection, especially when it is caused by certain high-risk HPV types, can eventually cause certain cancers, such as cervical cancer.
Although scientists believe that it’s necessary to have had HPV for cervical cancer to develop, most women with this virus do not develop cancer. Doctors believe that other factors must come into play for cancer to develop. Some of these known factors are listed below.
Smoking
When someone smokes, they and those around them are exposed to many cancer-causing chemicals that affect organs other than the lungs. These harmful substances are absorbed through the lungs and carried in the bloodstream throughout the body.
Women who smoke are about twice as likely as those who don’t smoke to get cervical cancer. Tobacco by-products have been found in the cervical mucus of women who smoke. Researchers believe that these substances damage the DNA of cervix cells and may contribute to the development of cervical cancer. Smoking also makes the immune system less effective in fighting HPV infections.
Having a weakened immune system
Human immunodeficiency virus (HIV), the virus that causes AIDS, damages the immune system and puts women at higher risk for HPV infections. This might explain why women with AIDS have a higher risk for cervical cancer. The immune system is important in destroying cancer cells and slowing their growth and spread. In women with HIV, a cervical pre-cancer might develop into an invasive cancer faster than it normally would.
Another group of women at risk for cervical cancer are those taking drugs to suppress their immune response, such as those being treated for an autoimmune disease (in which the immune system sees the body’s own tissues as foreign and attacks them, as it would a germ) or those who have had an organ transplant.
Chlamydia infection
Chlamydia is a relatively common kind of bacteria that can infect the reproductive system. It is spread by sexual contact. Women who are infected with chlamydia often have no symptoms and they may not know that they are infected at all unless they are tested during a pelvic exam. Chlamydia infection can cause pelvic inflammation, leading to infertility.
Some studies have seen a higher risk of cervical cancer in women whose blood tests and cervical mucus showed evidence of past or current chlamydia infection. Certain studies show that the Chlamydia bacteria may help HPV grow and live on in the cervix which may increase the risk of cervical cancer.
Many sexual partners
The greater your number of sexual partners — and the greater your partner’s number of sexual partners — the greater your chance of acquiring HPV.
Early sexual activity
Having sex at an early age increases your risk of HPV.
Other sexually transmitted infections (STIs)
Having other STIs — such as chlamydia, gonorrhea, syphilis and HIV/AIDS — increases your risk of HPV.
A diet low in fruits and vegetables
Women whose diets don’t include enough fruits and vegetables may be at increased risk for cervical cancer.
Being overweight
Overweight women are more likely to develop adenocarcinoma of the cervix.
Long-term use of oral contraceptives (birth control pills)
There is evidence that taking oral contraceptives for a long time increases the risk of cancer of the cervix. Research suggests that the risk of cervical cancer goes up the longer a woman takes oral contraceptives, but the risk goes back down again after the oral contraceptives are stopped and returns to normal about 10 years after stopping.
A woman and her doctor should discuss whether the benefits of using oral contraceptives outweigh the potential risks.
Intrauterine device (IUD) use
Some research suggests that women who had ever used an intrauterine device (IUD) had a lower risk of cervical cancer. The effect on risk was seen even in women who had an IUD for less than a year, and the protective effect remained after the IUDs were removed.
Using an IUD might also lower the risk of endometrial (uterine) cancer. However, IUDs do have some risks. A woman interested in using an IUD should first discuss the potential risks and benefits with her doctor. Also, a woman with multiple sexual partners should use condoms to lower her risk of sexually transmitted illnesses no matter what other form of contraception she uses.
Having multiple full-term pregnancies
Women who have had 3 or more full-term pregnancies have an increased risk of developing cervical cancer. No one really knows why this is true. One theory is that these women had to have had unprotected intercourse to get pregnant, so they may have had more exposure to HPV. Also, studies have pointed to hormonal changes during pregnancy as possibly making women more susceptible to HPV infection or cancer growth. Another thought is that pregnant women might have weaker immune systems, allowing for HPV infection and cancer growth.
Young age at first full-term pregnancy
Women who were younger than 20 years when they had their first full-term pregnancy are more likely to get cervical cancer later in life than women who waited to get pregnant until they were 25 years or older.
Economic status
Many low-income women do not have easy access to adequate health care services, including Pap tests. This means they may not get screened or treated for cervical cancers pre-cancers.
Diethylstilbestrol (DES)
DES is a hormonal drug that was given to some women between 1940 and 1971 to prevent miscarriage. Women whose mothers took DES (when pregnant with them) develop clear cell adenocarcinoma of the vagina or cervix more often than would normally be expected. This type of cancer is extremely rare in women who haven’t been exposed to DES. There is about 1 case of this type of cancer in every 1,000 women whose mothers took DES during pregnancy. This means that about 99.9% of “DES daughters” do not develop these cancers.
DES-related clear cell adenocarcinoma is more common in the vagina than the cervix. The risk appears to be greatest in women whose mothers took the drug during their first 16 weeks of pregnancy. The average age of women diagnosed with DES-related clear-cell adenocarcinoma is 19 years. Since the use of DES during pregnancy was stopped by the FDA in 1971, even the youngest DES daughters are older than 40 − past the age of highest risk. Still, there is no age cut-off when these women are felt to be safe from DES-related cancer. Doctors do not know exactly how long women will remain at risk.
DES daughters may also be at increased risk of developing squamous cell cancers and pre-cancers of the cervix linked to HPV.
Having a family history of cervical cancer
Cervical cancer may run in some families. If your mother or sister had cervical cancer, your chances of developing the disease are 2 to 3 times higher than if no one in the family had it. Some researchers suspect some instances of this familial tendency are caused by an inherited condition that makes some women less able to fight off HPV infection than others. In other instances, women from the same family as a patient already diagnosed could be more likely to have one or more of the other non-genetic risk factors previously described in this section.
Cervical cancer prevention
The most common form of cervical cancer starts with pre-cancerous changes, and there are ways to stop this disease from developing. The first way is to find and treat pre-cancers before they become true cancers, and the second is to prevent the pre-cancers.
Finding cervical pre-cancers
A well-proven way to prevent cervix cancer is to have testing (screening) to find pre-cancers before they can turn into invasive cancer. The Pap test (or Pap smear) and the HPV (human papilloma virus) test are used for this. If a pre-cancer is found, it can be treated, stopping cervical cancer before it really starts. Most invasive cervical cancers are found in women who have not had regular Pap tests.
The Pap test is a procedure used to collect cells from the cervix so that they can be looked at under a microscope to find cancer and pre-cancer. A Pap test can be done during a pelvic exam, but not all pelvic exams include a Pap test.
An HPV test can be done on the same sample of cells collected from the Pap test.
Things you can do to prevent pre-cancers and cancers
To reduce your risk of cervical cancer:
- Get vaccinated against HPV. Vaccination is available for girls and women ages 9 to 26. The vaccine is most effective if given to girls before they become sexually active.
- Have routine Pap tests. Pap tests can detect precancerous conditions of the cervix, so they can be monitored or treated in order to prevent cervical cancer. Most medical organizations suggest women begin routine Pap tests at age 21 and repeat them every few years.
- Practice safe sex. Using a condom, having fewer sexual partners and delaying intercourse may reduce your risk of cervical cancer.
- Don’t smoke.
HPV is passed from one person to another during skin-to-skin contact with an infected area of the body. Although HPV can be spread during sexual activity − including vaginal, anal, and oral sex − sex doesn’t have to occur for the infection to spread. All that is needed is skin-to-skin contact with an area of the body infected with HPV. This means that the virus can be spread through genital-to-genital contact (without sex). It is even possible for a genital infection to spread through hand-to-genital contact.
Also, HPV infection seems to be able to be spread from one part of the body to another. This means that an infection may start in the cervix and then spread to the vagina and vulva.
It can be very hard not to be exposed to HPV. It may be possible to prevent HPV infection by not allowing others to have contact with your anal or genital area, but even then there might be other ways to become infected that aren’t yet clear.
Limiting the number of sex partners and avoiding sex with people who have had many other sex partners can help lower your risk of exposure to genital HPV. But again, HPV is very common, so having sex with even one other person can put you at risk. Remember that someone can have HPV for years and still have no symptoms. Someone can have the virus and pass it on without knowing it.
Use condoms
Condoms (“rubbers”) provide some protection against HPV but they don’t completely prevent infection. One reason that condoms cannot protect completely is because they don’t cover every possible HPV-infected area of the body, such as skin of the genital or anal area. Still, condoms provide some protection against HPV, and they also help protect against HIV and some other sexually transmitted infections.
Don’t smoke
Not smoking is another important way to reduce the risk of cervical pre-cancer and cancer.
Get an HPV vaccine
Vaccines are available that can protect young people against certain HPV infections. These vaccines protect against infection with the HPV subtypes most commonly linked to cancer, as well as some types that can cause anal and genital warts.
These vaccines only work to prevent HPV infection − they will not treat an infection that is already there. That is why, to be most effective, the HPV vaccines should be given before a person becomes exposed to HPV (such as through sexual activity).
These vaccines help prevent pre-cancers and cancers of the cervix. Some HPV vaccines are also approved to help prevent other types of cancers and anal and genital warts.
The vaccines require a series of injections (shots). Side effects are usually mild. The most common one is short-term redness, swelling, and soreness at the injection site. Rarely, a young person will faint shortly after the vaccine injection.
The American Cancer Society recommendations for HPV vaccine use are similar to those from the federal Advisory Committee on Immunization Practices and include the following (Can Cervical Cancer Be Prevented? https://www.cancer.org/cancer/cervical-cancer/causes-risks-prevention/prevention.html)), 11:
- HPV vaccination of children between the ages of 9 and 12.
- Children and young adults age 13 through 26 who have not been vaccinated, or who haven’t gotten all their doses, should get the vaccine as soon as possible.Vaccination of young adults will not prevent as many cancers as vaccination of children and teens.
- HPV vaccination is not recommended for everyone older than age 26 years. HPV vaccination in this age range provides less benefit, because most sexually active adults have already been exposed to HPV, although not necessarily all of the HPV types targeted by vaccination. Some adults age 27 through 45 years who are not already vaccinated may decide to get HPV vaccine after speaking with their doctor about their risk for new HPV infections and the possible benefits of vaccination for them.
It’s important to realize that no vaccine provides complete protection against all cancer-causing types of HPV, so routine cervical cancer screening is still necessary.
The American Cancer Society Guidelines for the Prevention and Early Detection of Cervical Cancer
The American Cancer Society recommends that women follow these guidelines to help find cervical cancer early 12. Following these guidelines can also find pre-cancers, which can be treated to keep cervical cancer from forming.
- Cervical cancer testing (screening) should begin at age 25.
- Those aged 25 to 65 should have a primary HPV test* every 5 years. If primary HPV testing is not available, screening may be done with either a co-test that combines an HPV test with a Papanicolaou (Pap) test every 5 years or a Pap test alone every 3 years. (*A primary HPV test is an HPV test that is done by itself for screening. The US Food and Drug Administration has approved certain tests to be primary HPV tests.) The most important thing to remember is to get screened regularly, no matter which test you get.
- Those over age 65 who have had regular screening in the past 10 years with normal results and no history of CIN2 or more serious diagnosis within the past 25 years should stop cervical cancer screening. Once stopped, it should not be started again.
- People who have had a total hysterectomy (removal of the uterus and cervix) should stop screening (such as Pap tests and HPV tests), unless the hysterectomy was done as a treatment for cervical cancer or serious pre-cancer. People who have had a hysterectomy without removal of the cervix (called a supra-cervical hysterectomy) should continue cervical cancer screening according to the guidelines above.
- People who have been vaccinated against HPV should still follow these guidelines for their age groups.
- Some people believe that they can stop cervical cancer screening once they have stopped having children. This is not true. They should continue to follow American Cancer Society guidelines.
- If you have a history of a serious pre-cancer, you should continue to have testing for at least 25 years after that condition was found, even if the testing goes past age 65.
- Those who are at high risk of cervical cancer because of a suppressed immune system (for example from HIV infection, organ transplant, or long-term steroid use) or because they were exposed to DES in utero may need to be screened more often. They should follow the recommendations of their health care team.
- Women over 65 years of age who have had regular screening in the previous 10 years should stop cervical cancer screening as long as they haven’t had any serious pre-cancers (like CIN2 or CIN3) found in the last 20 years (CIN stands for cervical intraepithelial neoplasia and is discussed later in the section).
- Women with a history of CIN2 or CIN3 should continue to have testing for at least 20 years after the abnormality was found.
- Women who have had a total hysterectomy (removal of the uterus and cervix) should stop screening (such as Pap tests and HPV tests), unless the hysterectomy was done as a treatment for cervical pre-cancer (or cancer). Women who have had a hysterectomy without removal of the cervix (called a supra-cervical hysterectomy) should continue cervical cancer screening according to the guidelines above.
Some women believe that they can stop cervical cancer screening once they have stopped having children. This is not true. They should continue to follow American Cancer Society guidelines.
Although annual (every year) screening should not be done, women who have abnormal screening results may need to have a follow-up Pap test (sometimes with a HPV test) done in 6 months or a year.
The American Cancer Society guidelines for early detection of cervical cancer do not apply to women who have been diagnosed with cervical cancer, cervical pre-cancer, or HIV infection. These women should have follow-up testing and cervical cancer screening as recommended by their health care team.
Importance of being screened for cervical cancer
Screening tests offer the best chance to have cervical cancer found early when successful treatment is likely. Screening can also actually prevent most cervical cancers by finding abnormal cervical cell changes (pre-cancers) so that they can be treated before they have a chance to turn into a cervical cancer.
If it’s found early, cervical cancer is one of the most successfully treatable cancers. In the United States, the cervical cancer death rate declined by more than 50% over the last 30 years. This is thought to be mainly due to the effectiveness of screening with the Pap test.
Despite the recognized benefits of cervical cancer screening, not all American women get screened. Most cervical cancers are found in women who have never had a Pap test or who have not had one recently. Women without health insurance and women who have recently immigrated are less likely to have cervical cancer screening.
Cervical cancer diagnosis
If cervical cancer is suspected, your doctor is likely to start with a thorough examination of your cervix. A special magnifying instrument (colposcope) is used to check for abnormal cells.
During the colposcopic examination, your doctor is likely to take a sample of cervical cells (biopsy) for laboratory testing.
To obtain tissue, your doctor may use:
- Punch biopsy, which involves using a sharp tool to pinch off small samples of cervical tissue.
- Endocervical curettage (endocervical scraping), which uses a small, spoon-shaped instrument (curet) or a thin brush to scrape a tissue sample from the cervix.
If the punch biopsy or endocervical curettage is worrisome, your doctor may perform one of the following tests:
- Electrical wire loop, which uses a thin, low-voltage electrical wire to obtain a small tissue sample. Generally this is done under local anesthesia in the office.
- Cone biopsy, which is a procedure that allows your doctor to obtain deeper layers of cervical cells for laboratory testing. A cone biopsy may be done in a hospital under general anesthesia.
The HPV DNA Test
The most important risk factor for developing cervical cancer is infection with HPV. Doctors can now test for the HPV (high-risk or carcinogenic types) that are most likely to cause cervical cancer by looking for pieces of their DNA in cervical cells. The test can be done at the same time as the Pap test, with the same swab or a second swab. You won’t notice a difference in your exam if you have both tests.
The HPV DNA test is most often used in 2 situations:
- The HPV gene test can be used in combination with the Pap test to screen for cervical cancer. The American Cancer Society recommends this combination for women 30 and older. The HPV DNA test is not recommended to screen for cervical cancer in women under 30. That is because women in their 20s who are sexually active are much more likely (than older women) to have an HPV infection that will go away on its own. For these younger women, results of this test are not as significant and may be more confusing. For more information, see the American Cancer Society document HPV and HPV Testing.
- The HPV DNA test can also be used in women who have slightly abnormal Pap test results (ASC-US) to find out if they might need more testing or treatment.
An HPV DNA test has been approved by the FDA to be used without a Pap test to screen for cervical cancer.
Follow-up of HPV testing
If your Pap test result is normal, but you test positive for HPV, the main options are:
- Repeat co-testing (with a Pap test and an HPV test) in one year
- Testing for HPV types 16 or 18 (this can often be done on the sample in the lab). If the test is positive for types 16 or 18, colposcopy would be recommended (colposcopy is discussed in the section, Work-up of abnormal Pap test results). If you test negative, you should get repeat co-testing in one year.
The Pap (Papanicolaou) Test
The Pap test is a procedure used to collect cells from the cervix so that they can be looked at under the microscope to find cancer and pre-cancer.
How the Pap test is done
The Pap test is a procedure used to collect cells from the cervix so that they can be looked at under the microscope to find cancer and pre-cancer.
The health care professional first places a speculum inside the vagina. The speculum is a metal or plastic instrument that keeps the vagina open so that the cervix can be seen clearly. Next, using a small spatula, a sample of cells and mucus is lightly scraped from the exocervix. A small brush or a cotton-tipped swab is then inserted into the opening of the cervix to take a sample from the endocervix (see illustration in What is cervical cancer? section). If your cervix has been removed (because you had a trachelectomy or hysterectomy) as a part of the treatment for a cervical cancer or pre-cancer, the cells will be sampled from the upper part of the vagina (known as the vaginal cuff). The samples are then prepared so that they can be looked at under a microscope in the lab.
Although the Pap test has been more successful than any other screening test in preventing a cancer, it’s not perfect. One of the limitations of the Pap test is that the results need to be examined by the human eye, so an accurate analysis of the hundreds of thousands of cells in each sample is not always possible. Engineers, scientists, and doctors are working together to improve this test. Because some abnormalities may be missed (even when samples are looked at in the best labs), it’s not a good idea to have this test less often than American Cancer Society guidelines recommend.
Making your Pap tests more accurate
You can do several things to make your Pap test as accurate as possible:
- Try not to schedule an appointment for a time during your menstrual period. The best time is at least 5 days after your menstrual period stops.
- Don’t use tampons, birth-control foams or jellies, other vaginal creams, moisturizers, or lubricants, or vaginal medicines for 2 to 3 days before the Pap test.
- Don’t douche for 2 to 3 days before the Pap test.
- Don’t have vaginal sex for 2 days before the Pap test.
A pelvic exam is not the same as a Pap test
Many people confuse pelvic exams with Pap tests. The pelvic exam is part of a woman’s routine health care. During a pelvic exam, the doctor looks at and feels the reproductive organs, including the uterus and the ovaries and may do tests for sexually transmitted disease. Pelvic exams may help find other types of cancers and reproductive problems. Pap tests are often done during pelvic exams after the speculum is placed. Sometimes a pelvic exam is done without having a Pap test, but a Pap test is needed to find early cervical cancer or pre-cancers. Ask your doctor if you had a Pap test with your pelvic exam.
How Pap test results are reported
The most widely used system for describing Pap test results is the Bethesda System (TBS).
There are 3 main categories, some of which have sub-categories:
- Negative for intraepithelial lesion or malignancy
- Epithelial cell abnormalities
- Other malignant neoplasms.
You may need further testing if your Pap test showed any of the abnormalities below. See Work-up of abnormal Pap test results.
Negative for intraepithelial lesion or malignancy
This category means that no signs of cancer, pre-cancer, or other significant abnormalities were found. There may be findings that are unrelated to cervical cancer, such as signs of infection with yeast, herpes, or Trichomonas vaginalis (a microscopic parasite), for example. Specimens from some women may also show “reactive cellular changes”, which is the way cervical cells appear when infection or other irritation is around.
Epithelial cell abnormalities
This means that the cells lining the cervix or vagina show changes that might be cancer or a pre-cancer condition. This category is divided into several groups for squamous cells and glandular cells.
Squamous cell abnormalities
Atypical squamous cells (ASCs) This category includes two types of abnormalities:
- Atypical squamous cells of uncertain significance (ASC-US) is a term used when there are cells that look abnormal, but it is not possible to tell if this is caused by infection, irritation, or a pre-cancer. Most of the time, cells labeled ASC-US are not pre-cancer, but more testing is needed to be sure.
- Atypical squamous cells where high-grade squamous intraepithelial lesion (HSIL) can’t be excluded (ASC-H) is a term used when the cells look abnormal but are more concerning for a possible pre-cancer that needs more testing and may need treatment.
Squamous intraepithelial lesions (SILs) These abnormalities are divided into two categories:
- In low-grade SIL (LSIL) the cells look mildly abnormal.
- In high-grade SIL (HSIL) the cells look severely abnormal and are less likely than the cells in LSIL to go away without treatment. They are also more likely to eventually develop into cancer if they are not treated.
Further tests are needed if SIL is seen on a Pap test. This is discussed in Work-up of abnormal Pap test results. If treatment is needed, it can cure most SILs and prevent true cancer from developing.
Squamous cell carcinoma: This result means that the woman is likely to have an invasive cancer. Further testing will be done to be sure of the diagnosis before treatment can be planned.
Glandular cell abnormalities
Atypical glandular cells: When the glandular cells do not look normal, but they have concerning features that could be cancerous, the term used is atypical glandular cells (AGC). In this case, the patient should have more testing done.
Adenocarcinoma: Cancers of the glandular cells are called adenocarcinomas. In some cases, the pathologist examining the cells can tell whether the adenocarcinoma started in the endocervix, in the uterus (endometrium), or elsewhere in the body.
Other malignant neoplasms
This category is for other types of cancer that hardly ever affect the cervix, such as malignant melanoma, sarcomas, and lymphoma.
Work-up of Abnormal Pap Test Results
The first step in finding cervical cancer is often an abnormal Pap test result. This will lead to further tests, which can diagnose cervical cancer.
Cervical cancer may also be suspected if you have symptoms like abnormal vaginal bleeding or pain during sex. Your primary doctor or gynecologist often can do the tests needed to diagnose pre-cancers and cancers and may also be able to treat a pre-cancer.
If there is a diagnosis of invasive cancer, your doctor should refer you to a gynecologic oncologist, a doctor who specializes in cancers of women’s reproductive systems.
Tests for women with symptoms of cervical cancer or abnormal Pap test results
Medical history and physical exam
First, the doctor will ask you about your personal and family medical history. This includes information related to risk factors and symptoms of cervical cancer. A complete physical exam will help evaluate your general state of health. The doctor will do a pelvic exam and may do a Pap test if one has not already been done. In addition, your lymph nodes will be felt for evidence of metastasis (cancer spread).
The Pap test is a screening test, not a diagnostic test. It cannot tell for certain if you have cervical cancer. An abnormal Pap test result may mean more testing, sometimes including tests to see if a cancer or a pre-cancer is actually present. The tests that are used include colposcopy (with biopsy), endocervical scraping and cone biopsies.
Colposcopy
If you have certain symptoms that are worrisome for cancer or if your Pap test shows abnormal cells, you will need to have a test called colposcopy. You will lie on the exam table as you do with a pelvic exam. A speculum will be placed in the vagina to help the doctor see the cervix. The doctor will use a colposcope to examine the cervix. The colposcope is an instrument that stays outside the body and has magnifying lenses. It lets the doctor see the surface of the cervix closely and clearly. Colposcopy itself usually causes no more discomfort than any other speculum exam. It can be done safely even if you are pregnant. Like the Pap test, it is better not to have it during your menstrual period.
At the time of the procedure, the doctor will apply a weak solution of acetic acid (similar to vinegar) to your cervix to make any abnormal areas easier to see. If an abnormal area is seen, a biopsy (removal of a small piece of tissue) will be done. The tissue is sent to a lab to be looked at under a microscope. A biopsy is the best way to tell for certain whether an abnormal area is a pre-cancer, a true cancer, or neither. Although the colposcopy procedure is usually not painful, the cervical biopsy can cause discomfort, cramping, bleeding, or even pain in some women.
Cervical biopsies
Several types of biopsies can be used to diagnose cervical pre-cancers and cancers. After these procedures, patients may feel mild cramping or pain and may also have some light bleeding.
Colposcopic biopsy
For this type of biopsy, the cervix is examined with a colposcope to find the abnormal areas. A local anesthetic may then be used to numb the cervix before the biopsy. Using biopsy forceps, a small section of the abnormal area is removed.
Endocervical curettage (endocervical scraping)
Sometimes the transformation zone (the area at risk for HPV infection and pre-cancer) cannot be seen with the colposcope, so something else must be done to check that area for cancer. This means taking a scraping of the endocervix by inserting a narrow instrument (called a curette) into the endocervical canal (the part of the cervix closest to the uterus). The curette is used to scrape the inside of the canal to remove some of the tissue, which is then sent to the lab for examination.
Cone biopsy
Cone biopsy also known as conization, the doctor removes a cone-shaped piece of tissue from the cervix. The tissue removed in the cone includes the transformation zone where cervical pre-cancers and cancers are most likely to start.
A cone biopsy is not only used to diagnose pre-cancers and cancers. It can also be used as a treatment since it can sometimes completely remove pre-cancers and some very early cancers.
The methods commonly used for cone biopsies are the loop electrosurgical excision procedure (LEEP), also called the large loop excision of the transformation zone (LLETZ), and the cold knife cone biopsy. With both procedures, you might have mild cramping and some bleeding for a few weeks.
- Loop electrosurgical procedure (LEEP or LLETZ): In this method, the tissue is removed with a thin wire loop that is heated by electricity and acts as a small knife. For this procedure, a local anesthetic is used, and it can be done in your doctor’s office.
- Cold knife cone biopsy: This method uses a surgical scalpel or a laser instead of a heated wire to remove tissue. · You will receive anesthesia during the operation (either a general anesthesia, where you are asleep, or a spinal or epidural anesthesia, where an injection into the area around the spinal cord makes you numb below the waist) and it is done in a hospital.
Possible complications of cone biopsies include bleeding, infection and narrowing of the cervix.
Having any type of cone biopsy will not prevent most women from getting pregnant, but if a large amount of tissue has been removed, women may have a higher risk of giving birth prematurely.
For women with cervical cancer
If a biopsy shows that cancer is present, your doctor may order certain tests to see if and how far the cancer has spread. Many of the tests described below are not necessary for every patient. Decisions about using these tests are based on the results of the physical exam and biopsy.
Cystoscopy, proctoscopy, and examination under anesthesia
These are most often done in women who have large tumors. They are not necessary if the cancer is caught early.
In a cystoscopy, a slender tube with a lens and a light is placed into the bladder through the urethra. This lets the doctor check your bladder and urethra to see if cancer is growing into these areas. Biopsy samples can be removed during cystoscopy for testing in the lab. Cystoscopy can be done under a local anesthetic, but some patients may need general anesthesia. Your doctor will let you know what to expect before and after the procedure.
Proctoscopy is a visual inspection of the rectum through a lighted tube to look for spread of cervical cancer into your rectum.
Your doctor may also do a pelvic exam while you are under anesthesia to find out if the cancer has spread beyond the cervix.
Imaging studies
If your doctor finds that you have cervical cancer, certain imaging studies may be done to look inside the body. These tests can show if and where the cancer has spread, which will help you and your doctor decide on a treatment plan.
- Chest x-ray. Your chest may be x-rayed to see if cancer has spread to your lungs.
- Computed tomography (CT). CT scans are usually done if the tumor is larger or if there is concern about cancer spread.
- Magnetic resonance imaging (MRI). MRI scans look at the soft tissue parts of the body sometimes better than other imaging tests, like a CT scan. Your doctor will decide which imaging test is best to use in your situation.
- Positron emission tomography (PET scan). For a PET scan, a slightly radioactive form of sugar (known as FDG) is injected into the blood and collects mainly in cancer cells.
- PET/CT scan: Often a PET scan is combined with a CT scan using a special machine that can do both at the same time. This lets the doctor compare areas of higher radioactivity on the PET scan with a more detailed picture on the CT scan. This is the type of PET scan most often used in patients with cervical cancer. This test can help see if the cancer has spread to lymph nodes. PET scans can also be useful if your doctor thinks the cancer has spread but doesn’t know where.
- Intravenous urography also known as intravenous pyelogram (IVP) is an x-ray of the urinary system taken after a special dye is injected into a vein. This test can find abnormal areas in the urinary tract, caused by the spread of cervical cancer. The most common finding is that the cancer has blocked the ureters (tubes that connect the kidneys to the bladder). IVP is rarely used for patients with cervical cancer because CT and MRI are also good at finding abnormal areas in the urinary tract, as well as others not seen with an IVP.
Cervical cancer stages
If your doctor determines that you have cervical cancer, you’ll have further tests to find out if cancer cells have spread within the cervix or to other parts of the body. The process used to find out if cancer has spread within the cervix or to other parts of the body is called staging. Your cancer’s stage is one of the most important factors in deciding how to treat the cancer and determining how successful treatment might be.
To determine the cancer’s stage after a cervical cancer diagnosis, doctors try to answer these questions:
- How far has the cancer grown into the cervix?
- Has the cancer reached nearby structures?
- Has the cancer spread to the nearby lymph nodes or to distant organs?
Information from exams and tests is used to determine the size of the tumor, how deeply the tumor has invaded tissues in and around the cervix, and its spread to distant places (metastasis).
The FIGO (International Federation of Gynecology and Obstetrics) staging system is used most often for cancers of the female reproductive organs, including cervical cancer 13. For cervical cancer, the clinical stage is used and is based on the results of the doctor’s physical exam, biopsies, imaging tests, and a few other tests that are done in some cases, such as cystoscopy and proctoscopy. It is not based on what is found during surgery. If surgery is done, a pathologic stage can be determined from the findings at surgery, but it does not change your clinical stage. Your treatment plan is based on the clinical stage.
Cervical cancer stage ranges from stages I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means a more advanced cancer. And within a stage, an earlier letter means a lower stage. Cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
Cervical cancer staging can be complex. If you have any questions about your stage, please ask your doctor to explain it to you in a way you understand.
Table 1. Cervical cancer stages
| FIGO Stage | Stage description | |
|---|---|---|
| 1 | The cancer cells have grown from the surface of the cervix into deeper tissues of the cervix. Cancer has not spread to nearby lymph nodes. Cancer has not spread to distant sites. | |
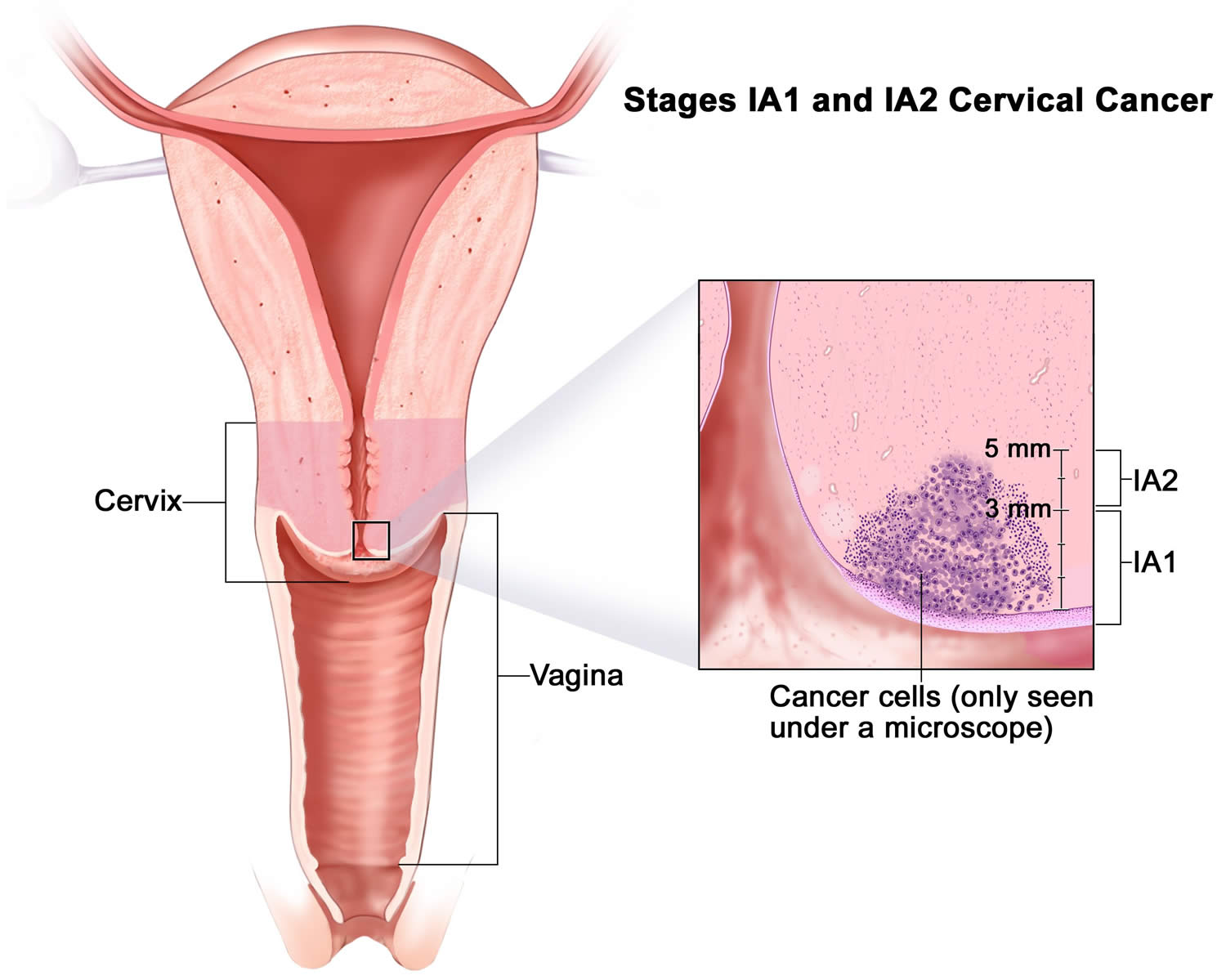
| 1A | There is a very small amount of cancer, and it can be seen only under a microscope, with maximum depth of invasion ≤5 mm It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
| 1A1 | The area of cancer can only be seen with a microscope and is less than 3 mm (about 1/8-inch) deep. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
| 1A2 | The area of cancer can only be seen with a microscope and is between 3 mm and 5 mm (about 1/5-inch) deep. It not has not spread to nearby lymph nodes. It has not spread to distant sites. | |
| 1B | This includes stage 1 cancer that has spread deeper than 5 mm (about 1/5 inch [greater than Stage 1A]) but is still limited to the cervix with size measured by maximum tumor diameter. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
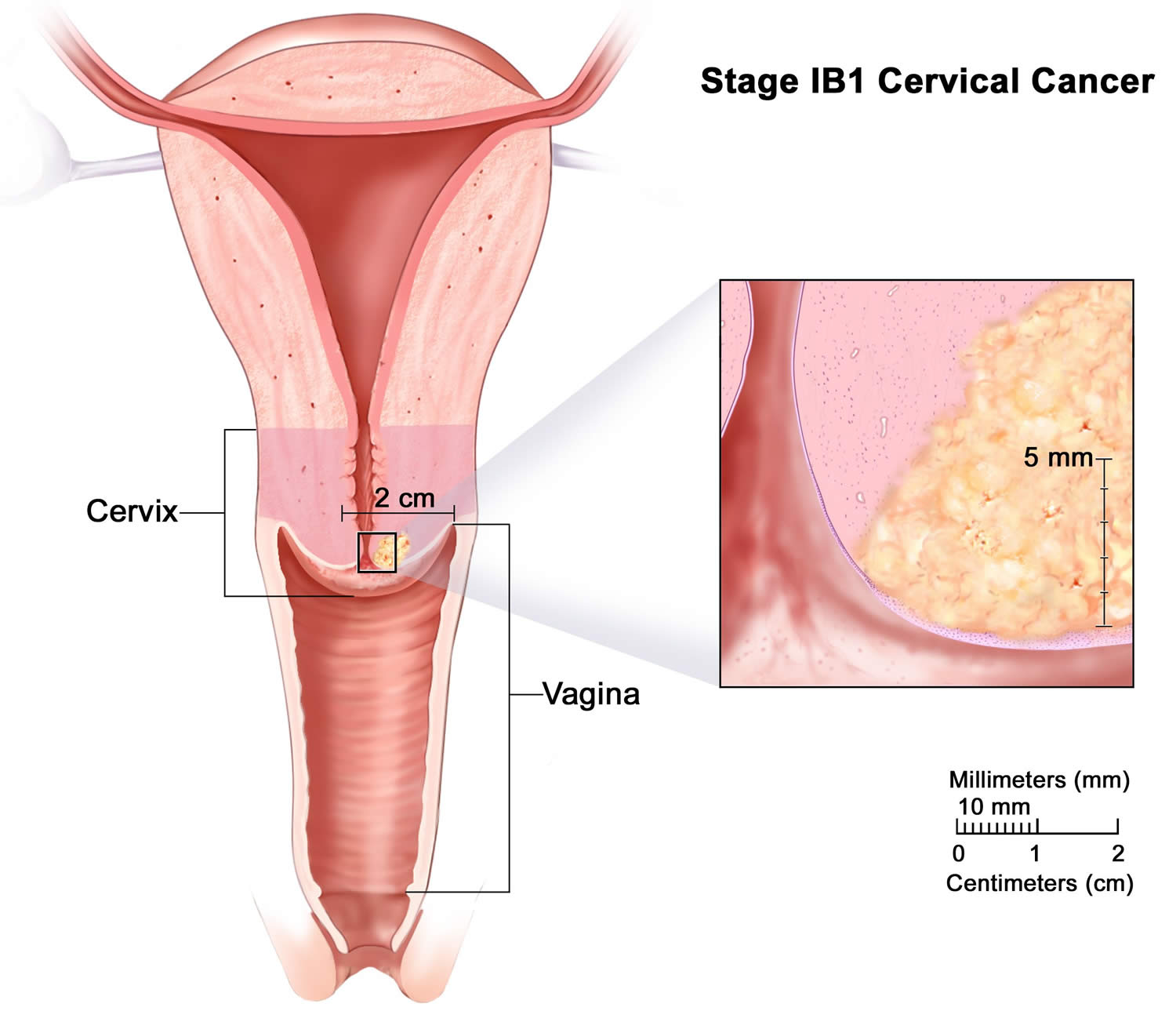
| 1B1 | The cancer is deeper than 5 mm (about 1/5-inch) but not more than 2 cm (about 4/5-inch) in size. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
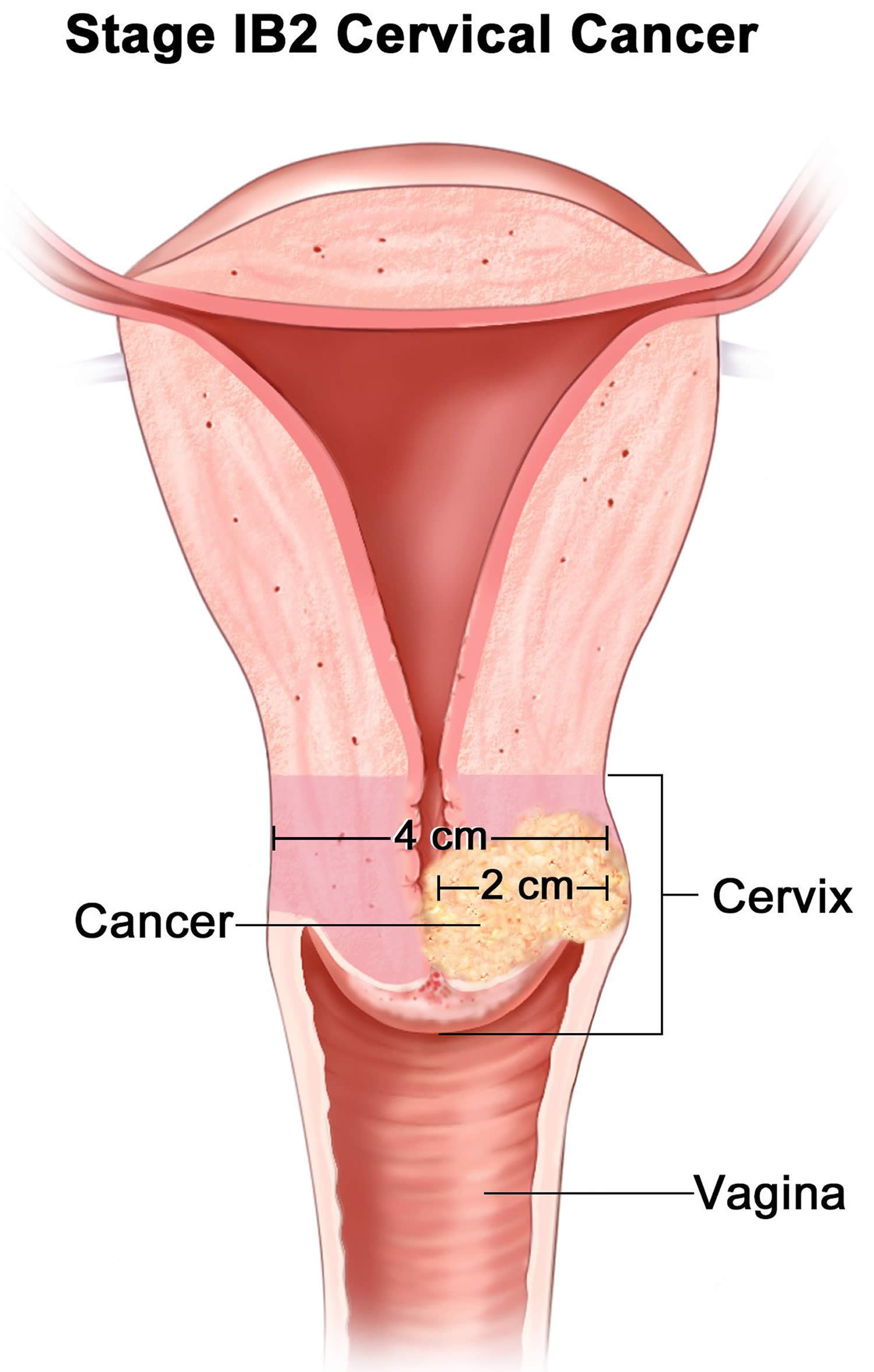
| 1B2 | The cancer is at least 2 cm in size but not larger than 4 cm. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
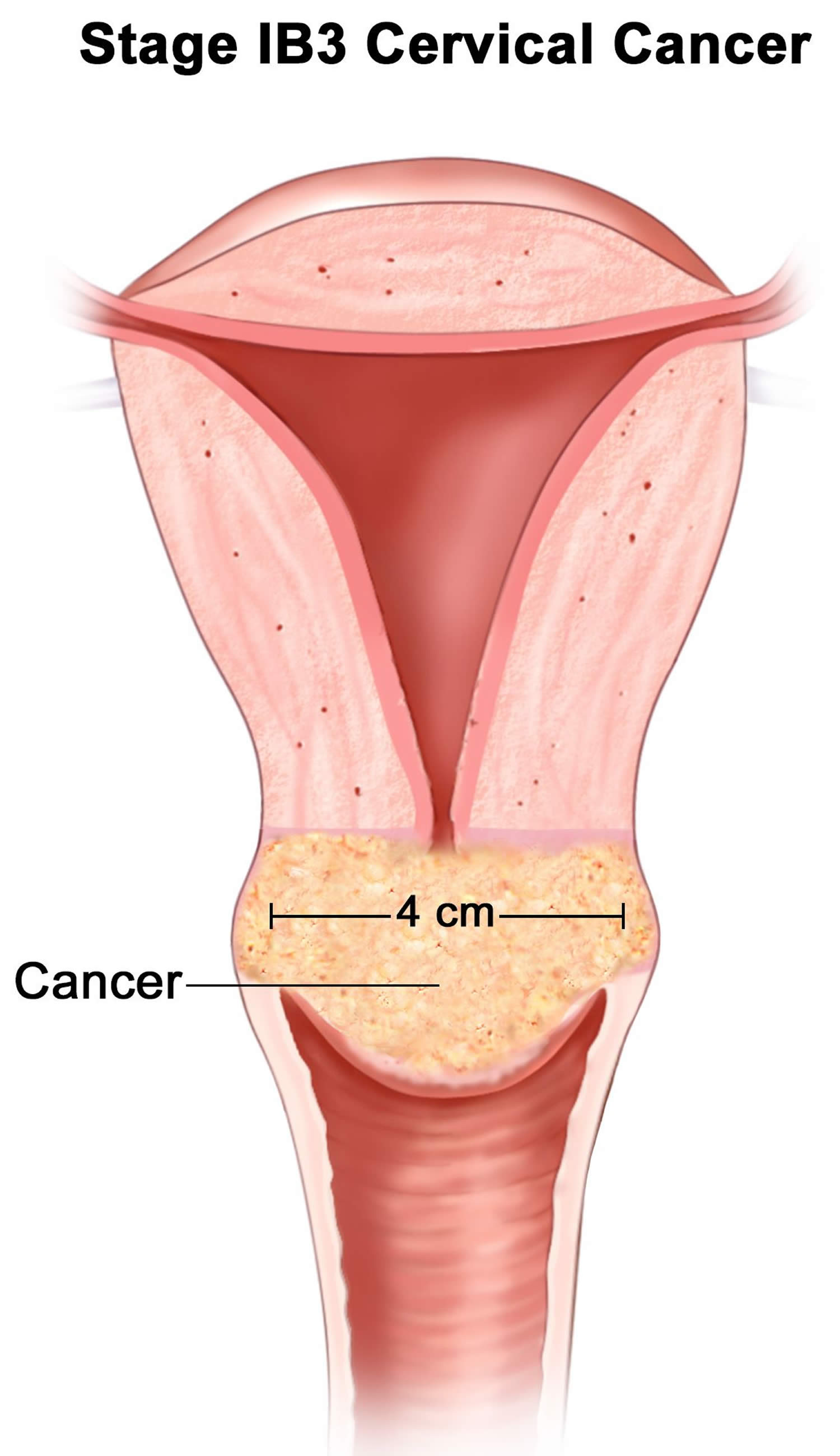
| 1B3 | The cancer is greater than 4 cm in size and limited to the cervix. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
| 2 | The cancer has grown beyond the cervix and uterus, but hasn’t spread to the walls of the pelvis or the lower third of the vagina. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
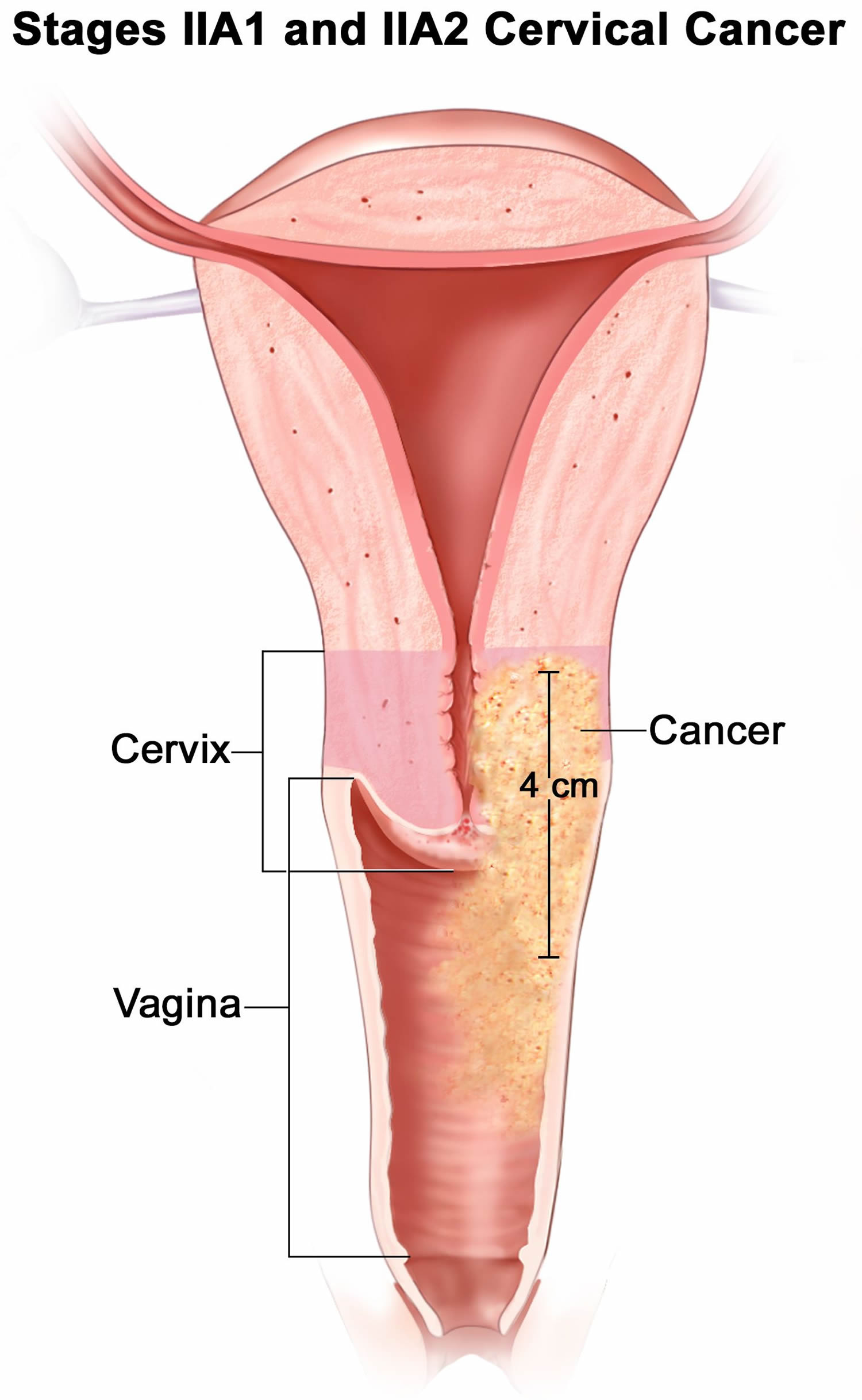
| 2A | The cancer has grown beyond the cervix and limited to the upper two-thirds of the vagina but has not spread into the tissues next to the cervix (called the parametria). It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
| 2A1 | The cancer is not larger than 4 cm (about 1 3/5 inches). It not has not spread to nearby lymph nodes. It has not spread to distant sites. | |
| 2A2 | The cancer is 4 cm or larger. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
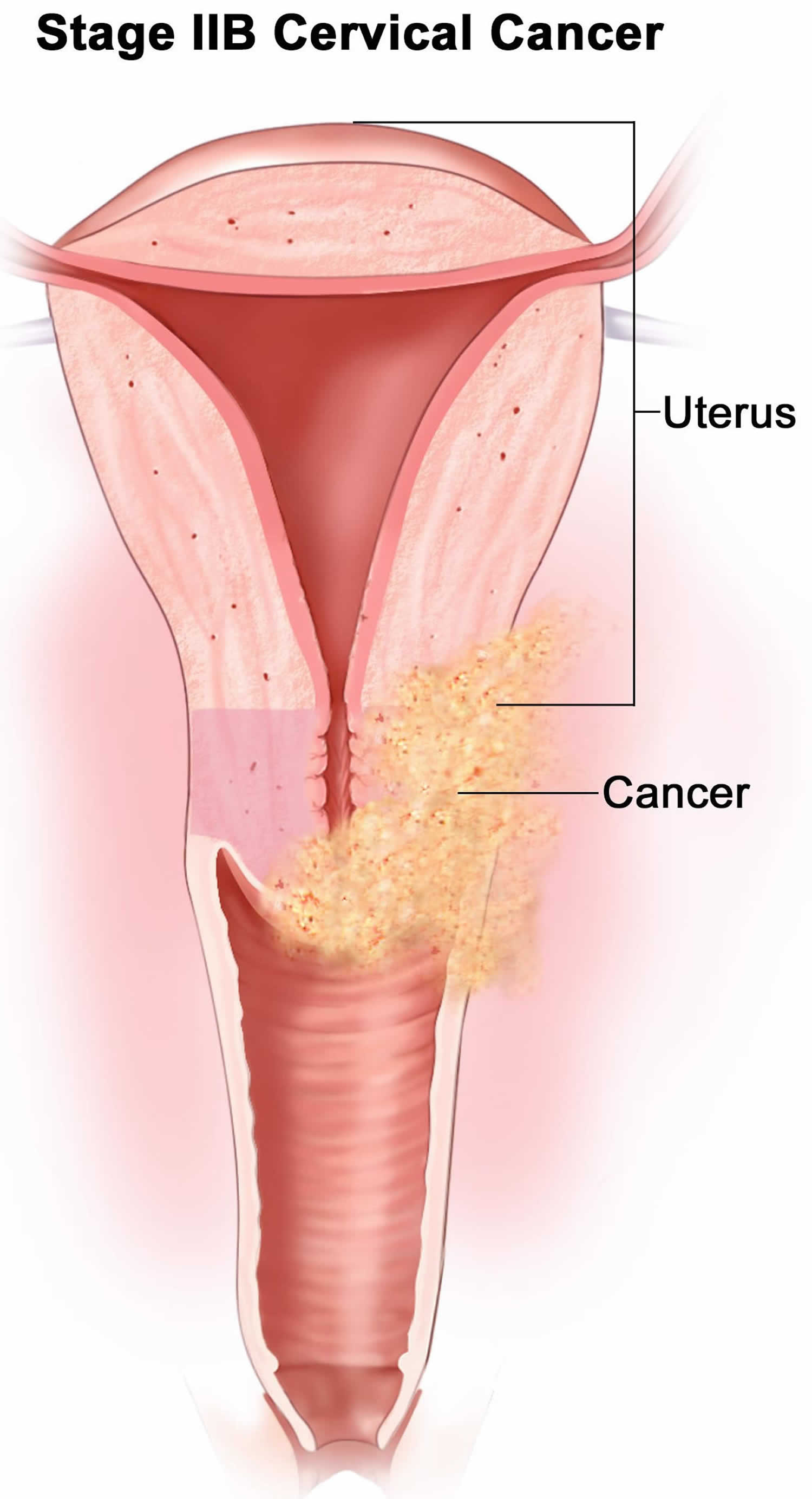
| 2B | The cancer has grown beyond the cervix and uterus and has spread into the tissues next to the cervix (the parametria) but not up to the pelvic wall. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
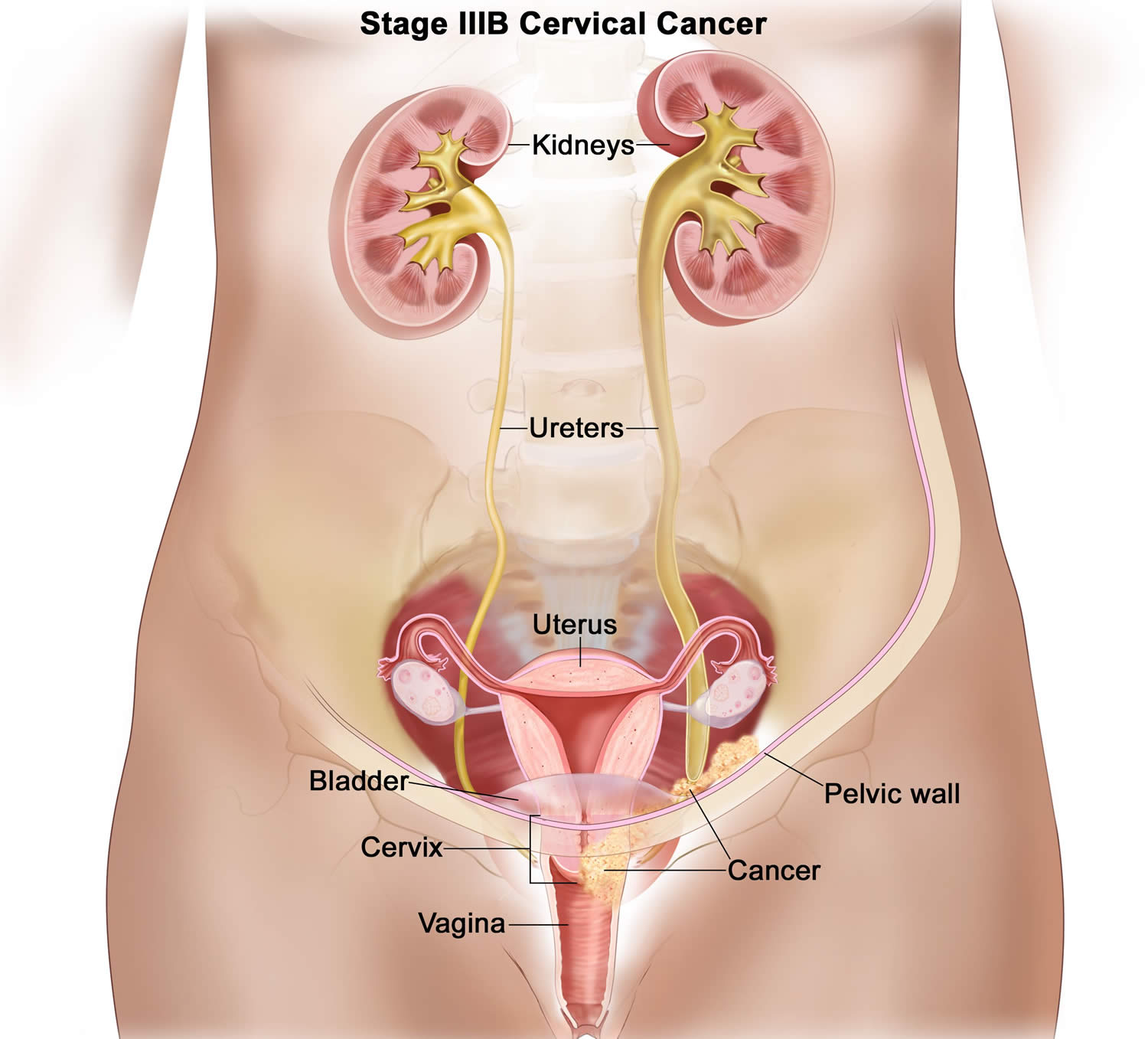
| 3 | The cancer has spread to the lower third of the vagina and/or the walls of the pelvis. The cancer may be blocking the ureters (tubes that carry urine from the kidneys to the bladder) causing hydronephrosis or nonfunctioning kidney. It might or might not have not spread to nearby lymph nodes (pelvic and/or para-aortic lymph nodes). It has not spread to distant sites. | |
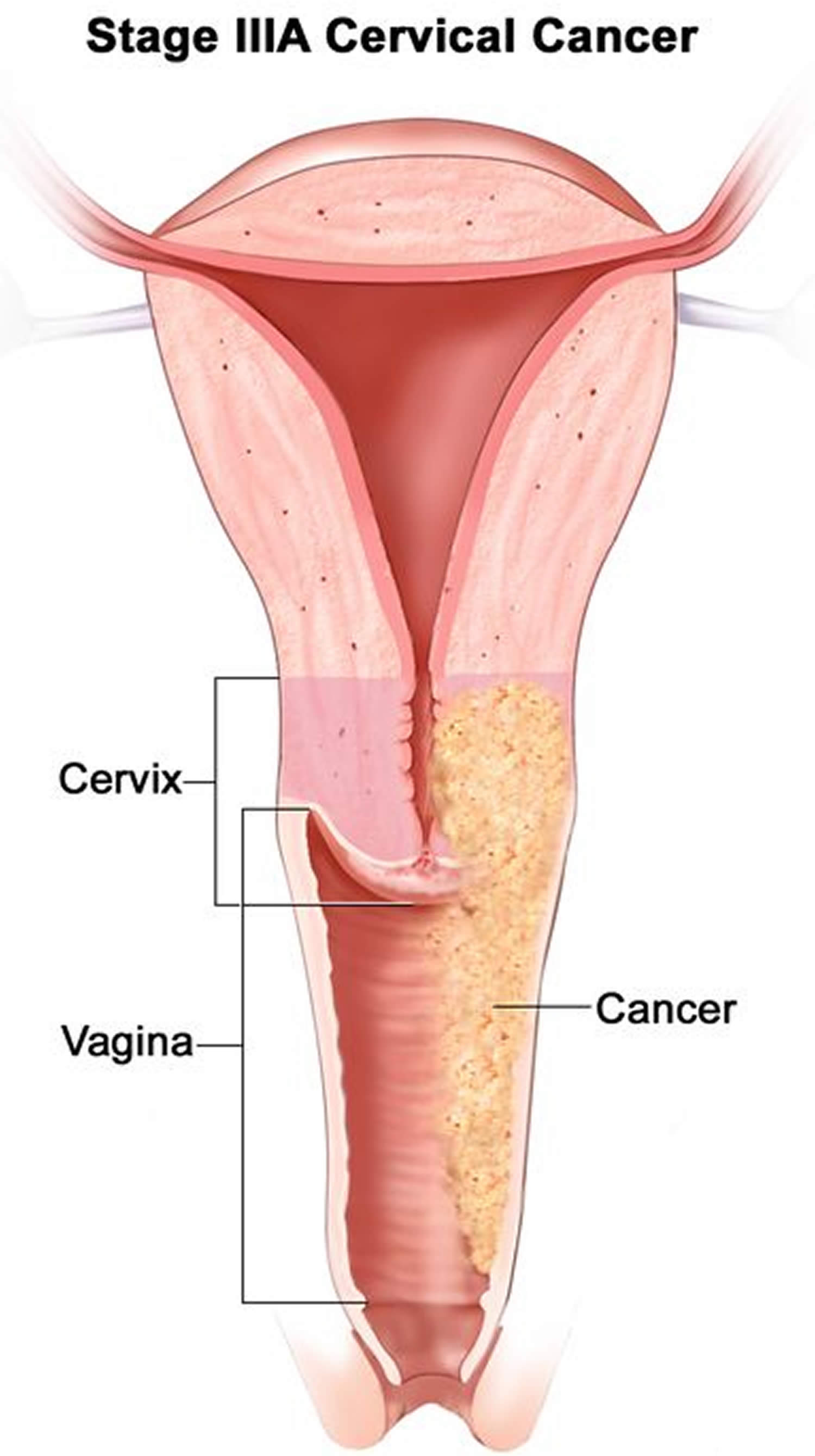
| 3A | The cancer has spread to the lower third of the vagina but not the walls of the pelvis. It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
| 3B | The cancer has grown into the walls of the pelvis and/or is blocking one or both ureters causing kidney problems (called hydronephrosis). It has not spread to nearby lymph nodes. It has not spread to distant sites. | |
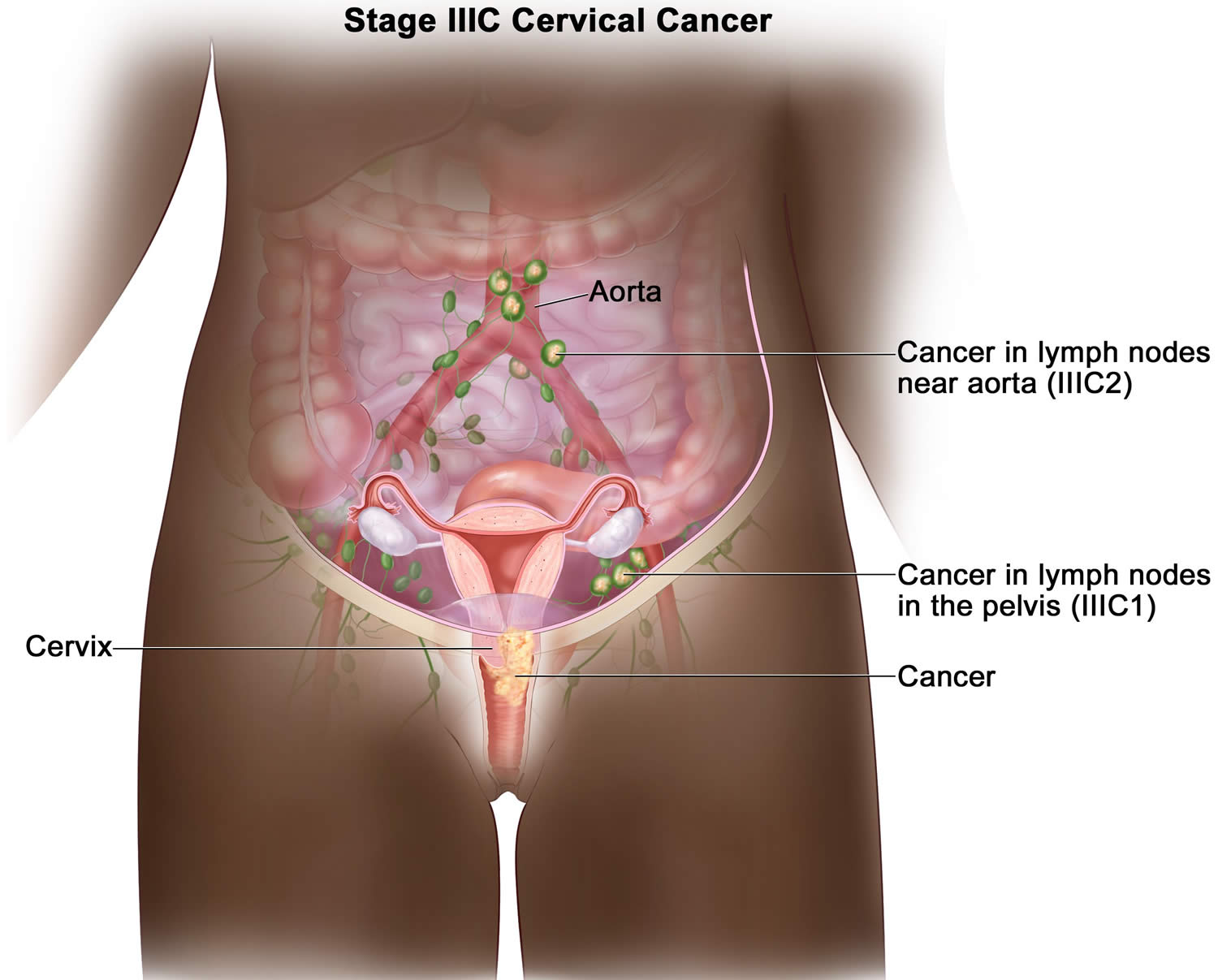
| 3C | The cancer can be any size. Imaging tests or a biopsy show the cancer has spread to nearby pelvic lymph nodes (3C1) or para-aortic lymph nodes (3C2). It has not spread to distant sites. | |
| 4 | The cancer has grown into the bladder or rectum or to far away organs like the lungs or bones. | |
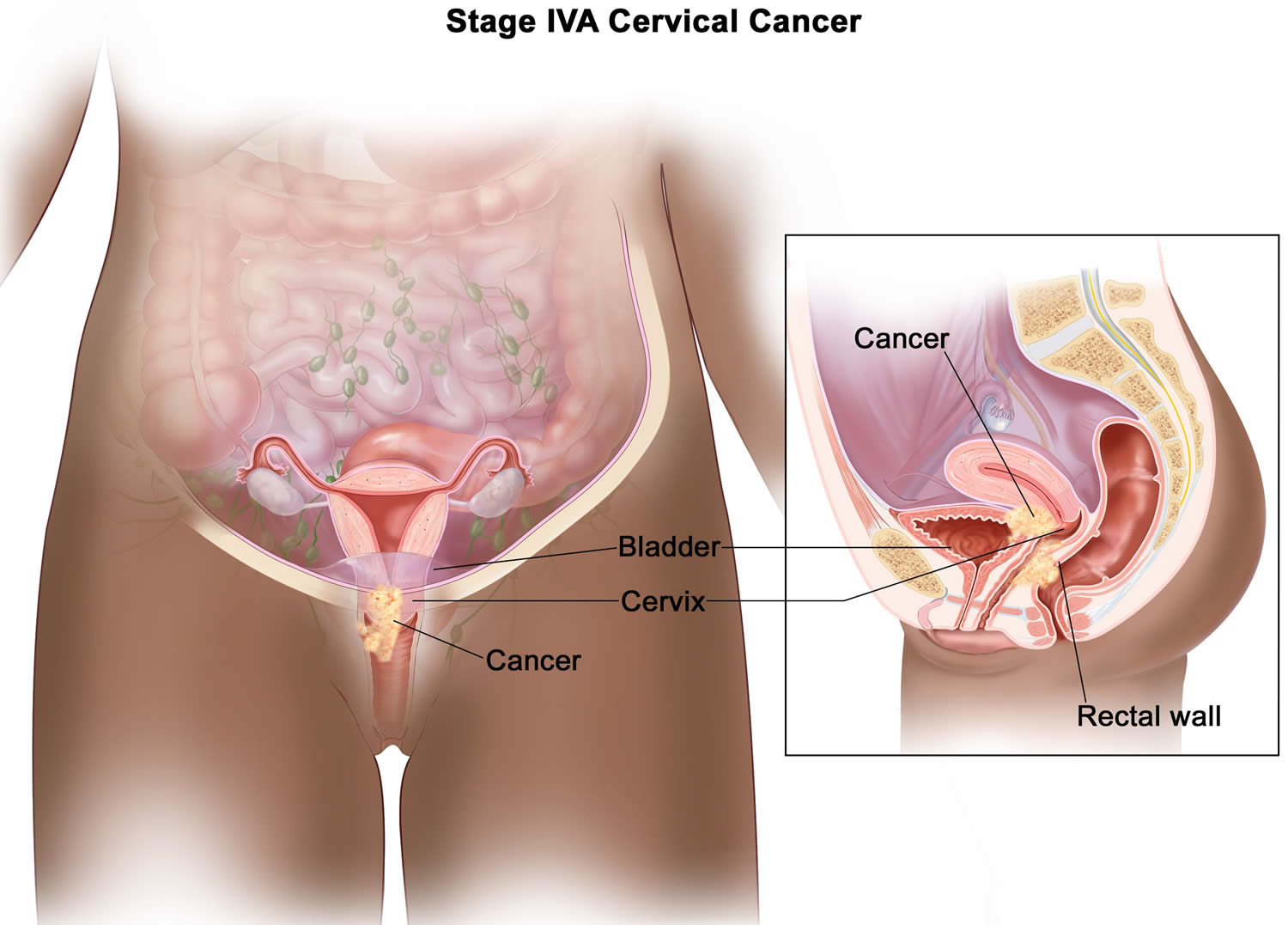
| 4A | The cancer has spread to the bladder or rectum or it is growing out of the pelvis. | |
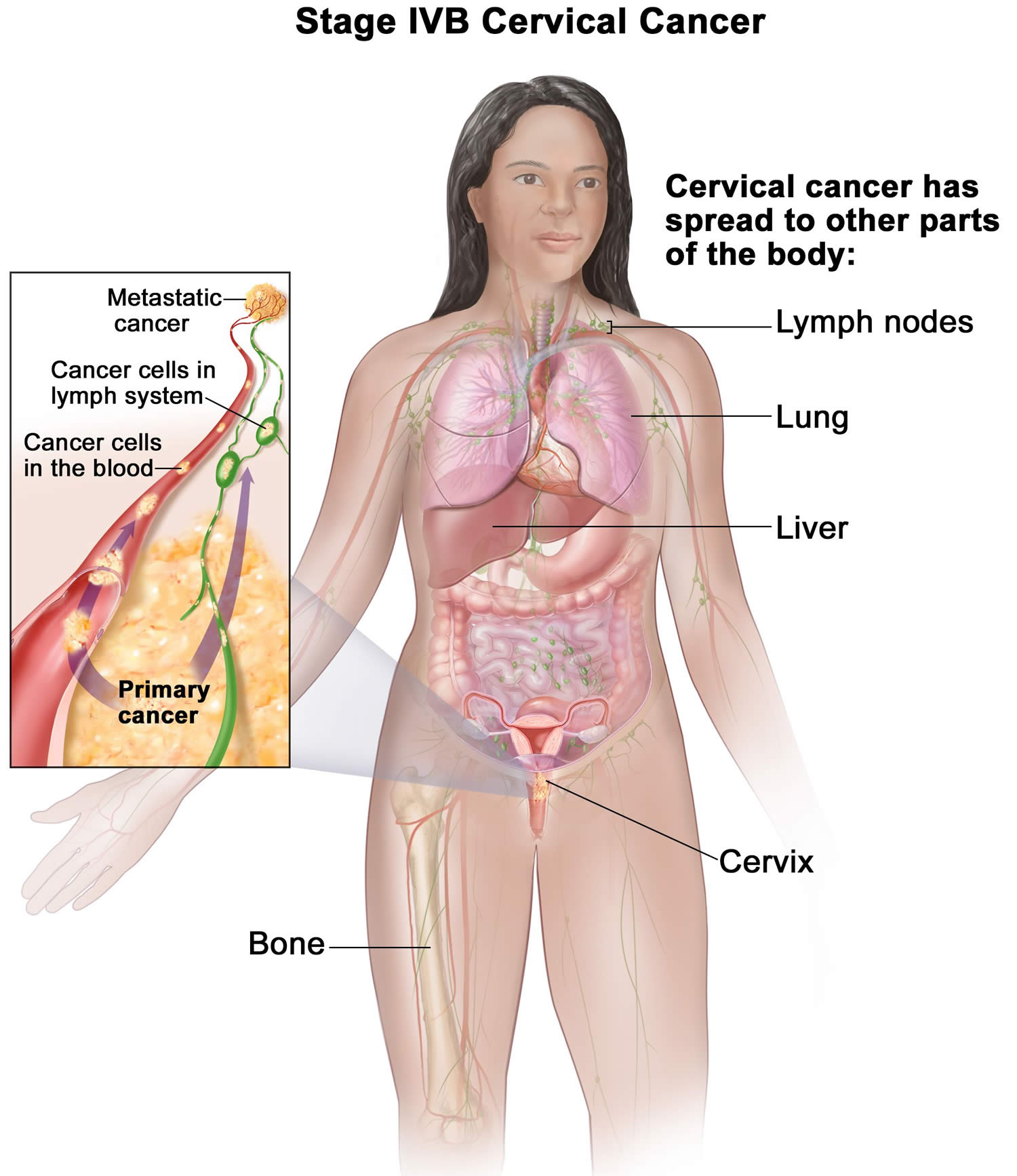
| 4B | The cancer has spread to distant organs outside the pelvic area, such as distant lymph nodes, lungs or bones. | |
The following tests and procedures may be used in the staging process:
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This picture can be printed to be looked at later.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Cystoscopy : A procedure to look inside the bladder and urethra to check for abnormal areas. A cystoscope is inserted through the urethra into the bladder. A cystoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
- Laparoscopy : A surgical procedure to look at the organs inside the abdomen to check for signs of disease. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope (a thin, lighted tube) is inserted into one of the incisions. Other instruments may be inserted through the same or other incisions to perform procedures such as removing organs or taking tissue samples to be checked under a microscope for signs of disease.
- Pretreatment surgical staging: Surgery (an operation) is done to find out if the cancer has spread within the cervix or to other parts of the body. In some cases, the cervical cancer can be removed at the same time. Pretreatment surgical staging is usually done only as part of a clinical trial.
The results of these tests are viewed together with the results of the original tumor biopsy to determine the cervical cancer stage.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if cervical cancer spreads to the lung, the cancer cells in the lung are actually cervical cancer cells. The disease is metastatic cervical cancer, not lung cancer.
Stage 1 cervical cancer
Stage 1 cervical cancer means that the cancer is only in the neck of the uterus (cervix). The cancer hasn’t spread to nearby tissues or other organs.
Stage 1 cervical cancer is often divided into:
- Stage 1A cervical cancer. In stage 1A the growth is so small that it can only be seen with a microscope or colposcope. It can be divided into 2 smaller groups:
- Stage 1A1 cervical cancer. Stage 1A1 means the cancer has grown less than 3 millimeters (mm) into the tissues of the cervix.
- Stage 1A2 cervical cancer. Stage 1A2 means the cancer has grown between 3 and 5 mm into the cervical tissues.
- Stage 1B cervical cancer. In stage 1B the cancerous areas are larger, but the cancer is still only in the tissues of the cervix and has not spread. It can usually be seen without a microscope, but not always. It can be divided into 3 groups:
- Stage 1B1 cervical cancer. In stage 1B1 the cancer is deeper than 5 mm but no more than 2cm in size.
- Stage 1B2 cervical cancer. In stage 1B2 the cancer is at least 2 cm but not bigger than 4cm in size.
- Stage 1B3 cervical cancer. In stage 1B3 the cancer is at least 4 cm but is still only in the cervix.
Stage 2 cervical cancer
Stage 2 cervical cancer means the cancer has spread outside the cervix, into the surrounding tissues. But it has not grown into the muscles or ligaments that line the pelvis (the area between the hip bones), or to the lower part of the vagina.
Stage 2 cervical cancer can be divided into:
- Stage 2A cervical cancer. In stage 2A the cancer has spread down into the top of the vagina. It can be divided into:
- Stage 2A1 cervical cancer. Stage 2A1 means the cancer is 4 cm or less.
- Stage 2A2 cervical cancer. Stage 2A2 means the cancer is more than 4 cm.
- Stage 2B cervical cancer. In stage 2B the cancer has spread up into the tissues around the cervix.
Stage 3 cervical cancer
Stage 3 cervical cancer means the cancer has spread from where it started in the cervix into the surrounding tissue or into the lymph nodes in the pelvis or abdomen. Stage 3 cervical cancer is divided into 3A, 3B and 3C, the stage you have depends on how far it has spread.
- Stage 3A cervical cancer. Stage 3A is when the cancer has spread to the lower third of the vagina but not the pelvic wall.
- Stage 3B cervical cancer. Stage 3B means the tumor has grown through to the pelvic wall or is blocking 1 or both of the tubes that drain the kidneys (the ureters).
- Stage 3C cervical cancer. Stage 3C means the cancer can be any size in the pelvis but has not spread to distant sites in the body. Stage 3C is then further divided into stage 3C1 and 3C2 if scans show cancer has spread to the lymph nodes.
- Stage 3C1 means cancer is in the nearby pelvic lymph nodes.
- Stage 3C2 means cancer is in the para-aortic lymph nodes (in the abdomen).
Stage 4 cervical cancer
Stage 4 cervical cancer means the cancer has spread to the bladder or rectum or further away. It can be divided into stage 4A and stage 4B.
- Stage 4A cervical cancer. Stage 4A is when the cancer has spread to nearby organs such as the bladder or rectum.
- Stage 4B cervical cancer. Stage 4B is when the cancer has spread to organs further away, such as the lungs. Your doctor might call this secondary or metastatic cancer.
Treatment of cervical cancer
Treatment for cervical cancer depends on several factors, such as the stage of the cancer, other health problems you may have and your preferences. Your doctor will talk to you about what the most suitable treatment options are and their possible side effects, and what the aim of treatment is. Surgery, radiation, chemotherapy or a combination of the three may be used.
Surgery for cervical cancer
Early-stage cervical cancer is typically treated with surgery to remove the uterus (hysterectomy). A hysterectomy can cure early-stage cervical cancer and prevent recurrence. But removing the uterus makes it impossible to become pregnant.
Your doctor may recommend:
- Simple hysterectomy. The cervix and uterus are removed along with the cancer. Simple hysterectomy is usually an option only in very early-stage cervical cancer.
- Radical hysterectomy. The cervix, uterus, part of the vagina and lymph nodes in the area are removed with the cancer.
- Trachelectomy. A trachelectomy is removal of the cervix, upper part of the vagina and parametrium (tissue surrounding the cervix). Pelvic lymph nodes may also be removed.
Minimally invasive surgery may be an option for early-stage cervical cancer.
Surgery that preserves the possibility of becoming pregnant also may be an option, if you have very early-stage cervical cancer without lymph node involvement.
Simple hysterectomy
A simple hysterectomy removes the uterus (both the body of the uterus and the cervix) but not the structures next to the uterus (parametria and uterosacral ligaments). The vagina and pelvic lymph nodes are not removed. The ovaries are usually left in place unless there is another reason to remove them.
Simple hysterectomy can be used to treat certain types of severe CIN or certain types of very early cervical cancer.
There are different ways to do a hysterectomy:
- Abdominal hysterectomy: The uterus is removed through a surgical incision in the front of the abdomen.
- Vaginal hysterectomy: The uterus is removed through the vagina.
- Laparoscopic hysterectomy: The uterus is removed using laparoscopy. First, a thin tube with a tiny video camera at the end (the laparoscope) is inserted into one or more very small surgical incisions made on the abdominal wall to see inside the abdomen and pelvis. Small instruments can be controlled through the tube(s), so the surgeon can cut around the uterus without making a large cut in the abdomen. The uterus is then removed through a cut in the vagina.
- Robotic-assisted surgery: In this approach, the laparoscopy is done with special tools attached to robotic arms that are controlled by the doctor to help perform precise surgery.
General anesthesia is used for all of these operations.
For a laparoscopic or vaginal hysterectomy, the hospital stay is usually 1 to 2 days, followed by a 2- to 3-week recovery period. A hospital stay of 3 to 5 days is common for an abdominal hysterectomy, and complete recovery takes about 4 to 6 weeks.
Possible side effects: Any type of hysterectomy results in infertility (inability to have children). Complications are unusual but could include bleeding, infection, or damage to the urinary or intestinal systems such as the bladder or colon.
Hysterectomy does not change a woman’s ability to feel sexual pleasure. A woman does not need a uterus or cervix to reach orgasm. The area around the clitoris and the lining of the vagina remain as sensitive as before a hysterectomy.
Radical hysterectomy
For this operation, the surgeon removes the uterus along with the tissues next to the uterus (the parametria and the uterosacral ligaments), the cervix, and the upper part (about 1 inch [2-3cm]) of the vagina next to the cervix. The ovaries are not removed unless there is some other medical reason to do so. More tissue is removed in a radical hysterectomy than in a simple one, so the hospital stay can be longer. Some lymph nodes will also be removed and checked for cancer at this time.
This surgery is usually done through a large abdominal incision (also known as open surgery). Often, some pelvic lymph nodes are removed as well. This procedure is known as lymph node dissection.
A radical hysterectomy can also be done using laparoscopy or robot-assistance. These techniques are also referred to as minimally invasive surgery. Laparoscopic (or robotic) surgery can result in less pain, less blood loss during the operation, and a shorter hospital stay compared to open surgery. However, it is very important to note that recent studies have shown that women who have minimally invasive radical hysterectomies for cervical cancer have a higher chance of the cancer recurring and a higher risk of dying from the cancer than those who have surgery through an abdominal incision (open surgery). Having a radical hysterectomy through an abdominal cut is the preferred type of surgery in most cases. Laparoscopic surgery may still be an option for a small specific group of women with early stage cancer, but you should discuss your options carefully with your doctor.
A modified radical hysterectomy is similar to a radical hysterectomy but does not remove as much of the vagina and tissues next to the uterus (the parametria and the uterosacral ligaments) and lymph nodes are usually not removed.
Possible side effects: Because the uterus is removed, this surgery results in infertility. Because some of the nerves to the bladder are removed, some women have problems emptying their bladder after this operation and may need a catheter for a time. Complications are unusual but could include bleeding, infection, or damage to the urinary and intestinal systems such as the bladder or colon.
Removal of some of the lymph nodes to check for cancer may sometimes result in lymphedema (leg swelling). This is not common, but may happen after surgery and treated with different methods.
Radical hysterectomy does not change a woman’s ability to feel sexual pleasure. Although the vagina is shortened, the area around the clitoris and the lining of the vagina is as sensitive as before. A woman does not need a uterus or cervix to reach orgasm. When cancer has caused pain or bleeding with intercourse, the hysterectomy may actually improve a woman’s sex life by stopping these symptoms.
Trachelectomy
A trachelectomy is removal of the cervix, upper part of the vagina and parametrium (tissue surrounding the cervix). Pelvic lymph nodes may also be removed. It can be used to treat some cases of early stage cervical cancer in women who wish to keep their fertility and ability to carry a child.
This procedure removes the cervix and the upper part of the vagina but not the body of the uterus. The surgeon then places a permanent “purse-string” stitch inside the uterine cavity to keep the opening of the uterus closed, the way the cervix normally would.
The nearby lymph nodes are also removed using laparoscopy which may require another incision (cut). The operation is done either through the vagina or the abdomen.
After trachelectomy, some women are able to carry a pregnancy to term and deliver a healthy baby by cesarean section, although women who have had this surgery might have a higher risk of miscarriage.
Pelvic exenteration
This operation is done for very specific cases of recurrent cervical cancer. In this surgery, all of the same organs and tissues are removed as in a radical hysterectomy with pelvic lymph node dissection. In addition, the bladder, vagina, rectum, and part of the colon is also removed, depending on where the cancer has spread.
If your bladder is removed, you will need a new way to store and get rid of urine. This usually means using a short piece of intestine to function as a new bladder. The new bladder may be connected to the abdominal wall so that urine is drained periodically when the patient places a catheter into a urostomy (a small opening). Or urine drains continuously into a small plastic bag attached to the front of the abdomen.
If the rectum and part of the colon are removed, a new way to get rid of solid waste must be created. This is done by attaching the remaining intestine to the abdominal wall so that fecal material can pass through a small opening (stoma) into a small plastic bag worn on the front of the abdomen. In some cases, it may be possible to remove the cancerous part of the colon (next to the cervix) and reconnect the colon ends so that no bags or external appliances are needed.
If the vagina is removed, a new vagina can be surgically made out of skin, intestinal tissue, or muscle and skin (myocutaneous) grafts.
Sexual impact of pelvic exenteration
Recovery from total pelvic exenteration takes a long time. Most women don’t begin to feel like themselves again for about 6 months after surgery. Some say it takes a year or two to adjust completely.
Nevertheless, these women can lead happy and productive lives. With practice, they can also have sexual desire, pleasure, and orgasms.
Surgery to remove nearby lymph nodes
Para-aortic lymph node sampling
Usually during surgery for a radical hysterectomy, the lymph nodes next to the aorta (the large artery in the abdomen) are removed. This is called para-aortic lymph node sampling. The lymph nodes may be sent to the lab during the operation for quick testing. If the para-aortic lymph nodes show cancer, the surgery may be stopped, and radiation and chemotherapy given instead. If the lymph nodes do not show cancer, then pelvic lymph nodes (see below) are usually removed and the radical hysterectomy completed. Any tissue removed during surgery will be tested to see if the cancer has spread there. If so, radiation therapy with or without chemotherapy might be recommended.
Pelvic lymph node dissection
Cancer that starts in the cervix can spread to lymph nodes (pea-sized collections of immune system cells) in the pelvis. To check for lymph node spread, the surgeon might remove some of these lymph nodes. This procedure is known as a pelvic lymph node dissection or lymph node sampling. It is done at the same time as a hysterectomy or trachelectomy.
Removing lymph nodes can lead to fluid drainage problems in the legs. This can cause severe leg swelling, a condition called lymphedema.
Sentinel lymph node mapping and biopsy
Sentinel lymph node mapping and biopsy is a procedure in which the surgeon finds and removes only the lymph node(s) where the cancer would likely spread first. To do this, the surgeon injects a radioactive substance and/or a blue dye into the cervix at the beginning of the surgery. Lymphatic vessels will carry these substances along the same path that the cancer would likely take. The first lymph node(s) the dye or radioactive substance travels to will be the sentinel node(s). Removing only one or a few lymph nodes lowers the risk of side effects from the surgery, such as leg swelling that is also known as lymphedema.
After the substance has been injected, the sentinel node(s) can be found either by using a special machine to detect radioactivity in the nodes, or by looking for nodes that have turned blue. To double check, both methods are often used. The surgeon then removes the node(s) containing the dye or radioactivity.
Sentinel lymph node mapping may be considered for certain cases of stage 1 cervical cancer. It is best used for tumors that are less than 2 cm in size. If your surgeon is planning sentinel lymph node biopsies, you should discuss if this procedure is appropriate for you.
Even if sentinel lymph node mapping does not show any lymph nodes to biopsy, the surgeon will most likely still remove the lymph nodes on that side of the pelvis to make sure cancer is not missed. Also, any enlarged or suspicious lymph nodes need to be removed at the time of surgery, even if they do not map with dye.
Radiation therapy for cervical cancer
Radiation therapy uses high-powered energy beams, such as X-rays or protons, to kill cancer cells. Depending on the stage of the cervical cancer, radiation therapy may be used:
- As a part of the main treatment. For some stages of cervical cancer, the preferred treatment is radiation alone or surgery followed by radiation. For other stages, radiation and chemo given together called concurrent chemoradiation is the preferred treatment as the chemo helps the radiation work better.
- To treat cervical cancer that has spread or that has come back after treatment. Radiation therapy may be used to treat cervical cancers that have spread to other organs and tissues.
Radiation therapy can be given:
- Externally, by directing a radiation beam at the affected area of the body (external beam radiation therapy)
- Internally, by placing a device filled with radioactive material inside your vagina, usually for only a few minutes (brachytherapy)
- Both externally and internally
Premenopausal women may stop menstruating and begin menopause as a result of radiation therapy. If you might want to get pregnant after radiation treatment, ask your doctor about ways to preserve your eggs before treatment starts.
It is important to know that smoking increases the side effects from radiation and can make treatment less effective. If you smoke, you should stop.
Women can experience side effects related to radiation months to years after treatment.
- Vaginal stenosis: Both external beam radiation therapy (EBRT) and brachytherapy (internal radiation therapy) can cause scar tissue to form in the vagina. The scar tissue can make the vagina narrower (called vaginal stenosis), less able to stretch, or even shorter, which can make vaginal sex painful. A woman can help prevent this problem by stretching the walls of her vagina several times a week, either by having sex or by using a vaginal dilator (a plastic or rubber tube used to stretch out the vagina).
- Vaginal dryness: Vaginal dryness and painful sex can be long-term side effects from radiation (both brachytherapy and external beam radiation therapy). Estrogens used locally may help with vaginal dryness and changes to the vaginal lining, especially if radiation to the pelvis damaged the ovaries, and caused early menopause. These hormones are typically applied in the vagina and absorbed into the genital area, rather than taken by mouth. They come in gel, cream, ring, and tablet forms.
- Rectal bleeding/rectal stenosis: Radiation to the rectal wall can cause chronic inflammation of the area which can lead to bleeding and sometimes stenosis (narrowing) of the rectum which can be painful. An abnormal opening (called a fistula) also may form between the rectum and vagina, causing stool to come out of the vagina. These problems typically happen during the first 3 years after radiation treatment. Additional treatments, such as surgery, may be needed to fix these complications.
- Urinary problems: Radiation to the pelvis can cause chronic radiation cystitis (as mentioned above), blood in the urine, or an abnormal opening between the bladder and vagina (called a fistula). These side effects can be seen many years after radiation therapy.
- Weakened bones: Radiation to the pelvis can weaken the bones, leading to fractures. Hip fractures are the most common, and might occur 2 to 4 years after radiation. Bone density tests are recommended to monitor the risk of fracture.
- Swelling of the leg(s): If pelvic lymph nodes are treated with radiation, it can lead to fluid drainage problems in the leg. This can cause the leg to swell severely , a condition called lymphedema.
If you are having side effects from radiation treatment, discuss them with your cancer care team.
External beam radiation
External beam radiation therapy (EBRT) aims x-rays at the cancer from a machine outside the body. Treatment is much like getting a regular x-ray, but the radiation dose is stronger. Each radiation treatment lasts only a few minutes, but getting you into place for treatment usually takes longer. The procedure itself is painless.
When external beam radiation therapy is used as the main treatment for cervical cancer, it is usually combined with chemotherapy called concurrent chemoradiation. Often, a low dose of the chemo drug called cisplatin is used. Other chemo drugs can be used as well. The radiation treatments are given 5 days a week for about 5 weeks. The chemotherapy is given at scheduled times during the radiation. The schedule is determined by which drug is used. If the cancer has not spread to distant areas, brachytherapy, which is discussed below, may also be given after the concurrent chemoradiation is complete.
External beam radiation therapy can also be used as the main treatment of cervical cancer in patients who can’t tolerate chemoradiation, can’t safely have surgery, or choose not to have surgery. It can also be used by itself to treat areas of cancer spread.
Short-term side effects of external beam radiation therapy for cervical cancer can include:
- Fatigue (tiredness)
- Upset stomach
- Diarrhea or loose stools (if radiation is given to the pelvis or abdomen)
- Nausea and vomiting
- Skin changes (mild redness to peeling or flaking)
- Radiation cystitis: Radiation to the pelvis can irritate the bladder (radiation cystitis), causing discomfort, an urge to urinate often, and sometimes blood in the urine.
- Vaginal pain: Radiation can make the vulva and vagina more sensitive and sore, and sometimes causes a discharge.
- Menstrual changes: Pelvic radiation can affect the ovaries, leading to menstrual changes and even early menopause
- Low blood counts: Anemia (low levels of red blood cells) can make you feel tired. Neutropenia (low levels of white blood cells) increases the risks of serious infection. Thrombocytopenia (low levels of platelet counts) increases the risk of bleeding.
When chemotherapy is given with radiation, the blood counts tend to be lower and fatigue and nausea tend to be worse. These side effects typically improve in the weeks after treatment is stopped.
Brachytherapy (internal radiation therapy)
Brachytherapy, or internal radiation therapy, puts a source of radiation in or near the cancer. This type of radiation only travels a short distance. The type of brachytherapy used most often to treat cervical cancer is known as intracavitary brachytherapy. The radiation source is placed in a device in the vagina (and sometimes in the cervix). Brachytherapy is mainly used in addition to EBRT as a part of the main treatment for cervical cancer. Rarely, it might be used alone in very specific cases of early-stage cervical cancers.
There are two types of brachytherapy:
- Low-dose rate (LDR) brachytherapy is completed over a few days. During this time, the patient stays in bed in a private room in the hospital with instruments holding the radioactive material in place. While the radiation therapy is being given, the hospital staff will care for you, but will also take precautions to avoid being exposed to radiation themselves.
- High-dose rate (HDR) brachytherapy is done as an outpatient over several treatments (often at least a week apart). For each high-dose treatment, the radioactive material is inserted for a few minutes and then removed. The advantage of high-dose rate (HDR) treatment is that you do not have to stay in the hospital or stay still for long periods of time.
To treat cervical cancer in women who have had a hysterectomy, the radioactive material is placed in a tube in the vagina.
To treat a woman who still has a uterus, the radioactive material can be placed in a small metal tube (called a tandem) that goes in the uterus, along with small round metal holders (ovoids) placed near the cervix. This is sometimes called tandem and ovoid treatment.
Another option is called tandem and ring. For this, a round holder (like a disc) is placed close to the uterus. The choice of which one to use depends on what type of brachytherapy is planned.
Possible short-term side effects of brachytherapy
Since the radiation only travels a short distance with brachytherapy, the main effects of the radiation are on the cervix and the walls of the vagina. The most common side effect is irritation of the vagina. It may become red and sore, and there may be a discharge. The vulva may become irritated as well.
Brachytherapy can also cause many of the same side effects as external beam radiation therapy (EBRT), such as fatigue, diarrhea, nausea, irritation of the bladder, and low blood counts. Often brachytherapy is given right after external beam radiation (before the side effects can go away), so it can be hard to know which type of treatment is causing the side effect.
Chemotherapy for cervical cancer
Chemotherapy (chemo) uses anti-cancer drugs that are injected into a vein or given by mouth. These drugs enter the bloodstream and can reach almost all areas of the body, making this treatment useful for killing cancer cells in most parts of the body. Not all women with cervical cancer will need chemo, but there are a few situations in which chemo may be recommended:
- As part of the main treatment for cervical cancer. For some stages of cervical cancer, the preferred treatment is radiation and chemo given together called concurrent chemoradiation. The chemo helps the radiation work better. Options for concurrent chemoradiation include:
- Cisplatin given weekly during radiation. This drug is given into a vein (IV) before the radiation appointment. If cisplatin is not a good option, carboplatin may be used instead.
- Cisplatin plus 5-fluorouracil (5-FU) given every 3 weeks during radiation.
- For cervical cancer that has spread or come back after treatment. Chemo may be used to treat cervical cancer that has spread to other organs and tissues (advanced cervical cancer). It can also be helpful when cervical cancer comes back after treatment with chemoradiation (recurrent cervical cancer). The chemo drugs most often used to treat cervical cancer that has come back or spread to other areas include:
- Cisplatin
- Carboplatin
- Paclitaxel (Taxol)
- Topotecan
- Combinations of these drugs are often used.
- Some other drugs can be used as well, such as docetaxel (Taxotere), ifosfamide (Ifex), 5-fluorouracil (5-FU), irinotecan (Camptosar), gemcitabine (Gemzar) and mitomycin.
- Bevacizumab (Avastin), a targeted drug, may be added to chemo.
Chemo drugs for cervical cancer are typically given into a vein (IV), either as an injection over a few minutes or as an infusion in a vein over a longer period of time. This can be done in a doctor’s office, infusion center, or in a hospital setting.
Chemo is given in cycles, followed by a rest period to give you time to recover from the effects of the drugs. Cycles are most often weekly or 3 weeks long. The schedule varies depending on the drugs used. For example, with some drugs, the chemo is given only on the first day of the cycle. With others, it is given for a few days in a row, or once a week. Then, at the end of the cycle, the chemo schedule repeats to start the next cycle.
Sometimes, a slightly larger and sturdier IV is required to give chemo. These are known as central venous catheters (CVCs), central venous access devices (CVADs), or central lines. They are used to put medicines, blood products, nutrients, or fluids right into your blood. They can also be used to take blood for testing.
There are many different kinds of central venous catheters (CVCs). The most common types are the port and the PICC line.
Chemo drugs kill cancer cells but also damage some normal cells, which can lead to certain side effects. Side effects depend on the type and dose of the drugs and the length of time you are treated. Many side effects are short-term and go away after treatment is finished, but some can last a long time or even be permanent. It’s important to tell your health care team if you have any side effects, as there are often ways to lessen them.
Common short term side effects of chemotherapy can include:
- Nausea and vomiting
- Loss of appetite
- Hair loss
- Mouth sores
- Fatigue (tiredness)
Because chemotherapy can damage the blood-producing cells of the bone marrow, the blood cell counts might become low. This can result in:
- An increased chance of infection from a shortage of white blood cells (called neutropenia)
- Bleeding or bruising after minor cuts or injuries because of a shortage of blood platelets (called thrombocytopenia)
- Shortness of breath or fatigue due to low red blood cell counts (called anemia)
When chemo is given with radiation, the side effects are often more severe. The nausea, fatigue, diarrhea, and problems with low blood counts are often worse.
Your health care team will watch for side effects and can give you medicines to help prevent them or treat them to help you feel better. For example, you can be given drugs to help prevent or reduce nausea and vomiting.
Long-term side effects of chemotherapy can include:
- Menstrual changes: For younger women who have not had their uterus removed as a part of treatment, changes in menstrual periods are a common side effect of chemo. But even if your periods stop while you are on chemo, you might still be able to get pregnant. Getting pregnant while receiving chemo is not safe, as it could lead to birth defects and interfere with treatment. This is why it’s important that women who are pre-menopausal before treatment and are sexually active discuss with their doctor the options for birth control. Patients who have finished treatment (like chemo) can often go on to have children, but it’s important to talk to your doctor about when it is safe to do so.
- Premature menopause (not having any more menstrual periods) and infertility (not being able to become pregnant) may occur and may be permanent. Some chemo drugs are more likely to cause this than others. The older a woman is when she gets chemo, the more likely it is that she will become infertile or go through menopause as a result. If this happens, there is an increased risk of bone loss and osteoporosis. Medicines that can treat or help prevent problems with bone loss are available.
- Neuropathy: Some drugs used to treat cervical cancer, including paclitaxel and cisplatin, can damage nerves outside of the brain and spinal cord. The injury can sometimes lead to symptoms like numbness, pain, burning or tingling sensations, sensitivity to cold or heat, or weakness, mainly in the hands and feet. This called peripheral neuropathy. In most cases this gets better or even goes away once treatment stops, but it might last a long time in some women.
- Nephrotoxicity: Cisplatin, the main chemo drug used to treat cervical cancer, can damage the kidneys (also called nephrotoxicity). Many times the damage is preventable and reversible, but sometimes the damage may be long-lasting. Often, there are no symptoms, but the damage can be seen on bloodwork done routinely while chemo is given. If kidney damage happens, the cisplatin is usually stopped and carboplatin may be used instead.
Other side effects are also possible. Some of these are more common with certain chemo drugs. Ask your cancer care team to tell you about the possible side effects of the specific drugs you are getting.
Immunotherapy for cervical cancer
Immunotherapy is the use of medicines to boost a person’s own immune system to recognize and destroy cancer cells more effectively. Immunotherapy typically works on specific proteins involved in the immune system to enhance the immune response. They have different and sometimes less severe side effects than chemotherapy. Immunotherapy can sometimes be used to treat cervical cancer.
Immune checkpoint inhibitors
An important part of the immune system is its ability to keep itself from attacking the body’s normal cells. To do this, it uses “checkpoints” – proteins on immune cells that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoints to avoid being attacked by the immune system. Newer drugs that target these checkpoints are being used as cancer treatments.
Pembrolizumab (Keytruda) targets PD-1, a protein on immune system cells called T cells that normally helps keep these cells from attacking other cells in the body. By blocking PD-1, these drugs boost the immune response against cancer cells. This can shrink some tumors or slow their growth.
Before pembrolizumab can be used, a lab test might need to be done on the cancer cells to show they have at least a certain amount of the PD-L1 protein.
If enough PD-L1 protein is detected, pembrolizumab can be used:
- By itself for cervical cancer that has come back or that has spread while getting chemotherapy or after chemotherapy.
- As a first treatment, along with chemotherapy, with or without bevacizumab, for cervical cancer that is not shrinking with current treatment, has come back, or has spread to distant sites.
This immunotherapy drug is given as an intravenous (IV) infusion every 3 or 6 weeks.
Side effects of immunotherapy drugs can include fatigue, fever, nausea, headache, skin rash, loss of appetite, constipation, joint/muscle pain, and diarrhea.
Other, more serious side effects occur less often. These drugs work by basically removing the brakes on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, kidneys, or other organs.
It’s very important to report any new side effects to your health care team right away. If you do have a serious side effect, treatment may need to be stopped and you may be given high doses of corticosteroids to suppress your immune system.
Targeted drug therapy for cervical cancer
Targeted drug therapy is the use of medicines that target or are directed at proteins on cervical cancer cells that help them grow, spread, or live longer. Targeted drugs work to destroy cancer cells or slow down their growth. They have different side effects than chemotherapy. Different types of targeted drug therapy can be used to treat cervical cancer.
Angiogenesis inhibitors
Vascular endothelial growth factor (VEGF) is a protein that helps tumors form new blood vessels a process known as angiogenesis to get nutrients they need to grow. Some targeted drugs called angiogenesis inhibitors stop VEGF from working and block this new blood vessel growth.
Bevacizumab (Avastin®) is an angiogenesis inhibitor that can be used to treat advanced cervical cancer. It is a monoclonal antibody (a man-made version of a specific immune system protein) that targets vascular endothelial growth factor (VEGF).
This drug is often used with chemo for a time. Then, if the cancer responds, the chemo may be stopped and the bevacizumab given by itself until the cancer starts growing again.
The possible side effects of bevacizumab can include:
- High blood pressure
- Feeling tired
- Nausea
Less common but more serious side effects can include:
- Problems with bleeding
- Blood clots
- Wound healing
- Heart failure or a heart attack
Other rare but serious side effects are the formation of an abnormal opening (called a fistula) between the vagina and part of the colon or intestine or the formation of a hole in the bowel.
Antibody-drug conjugates
An antibody-drug conjugate (ADC) is a monoclonal antibody linked to a chemotherapy drug.
Tisotumab vedotin-tftv (Tivdak) is an antibody-drug conjugate (ADC) that has an antibody that targets tissue-factor (TF) protein on cancer cells. It acts like a homing signal by attaching to the TF protein bringing the chemo directly to the cancer cell. It can be used to treat cervical cancer that has spread (metastasized) to another part of the body or come back after initial treatment (recurred), typically after at least 2 other drug treatments have been tried. This drug is given in a vein (IV).
Common side effects of tisotumab vedotin-tftv (Tivdak) can include feeling tired, nausea, hair loss, vomiting, bleeding, diarrhea, rash, and nerve damage (peripheral neuropathy).
Common lab abnormalities that might be seen with this drug include low red blood cell counts (anemia), low white blood cell counts, and abnormal kidney function.
Tisotumab vedotin-tftv (Tivdak) can have major side effects involving the eyes. People taking this drug can have dry eye, changes in vision, vision loss, or ulceration of the cornea. They should have regular eye exams while on this drug and tell their healthcare team right away if they have any eye symptoms.
Follow-up care
After you complete treatment, your doctor will recommend regular checkups. Ask your doctor how often you should have follow-up exams.
Supportive (palliative) care
Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care.
When palliative care is used along with all of the other appropriate treatments, people with cancer may feel better and live longer.
Palliative care is provided by a team of doctors, nurses and other specially trained professionals. Palliative care teams aim to improve the quality of life for people with cancer and their families. This form of care is offered alongside curative or other treatments you may be receiving.
Cervical cancer treatment by stage
The stage of a cervical cancer is the most important factor in choosing treatment. But other factors can also affect your treatment options, including the exact location of the cancer within the cervix, the type of cancer (squamous cell or adenocarcinoma), your age and overall health, and whether you want to have children.
Stage 1A1 cervical cancer treatment
Stage 1A1 means cervical cancer has grown less than 3 millimeters (mm) into the tissues of the cervix. Treatment for this stage depends on whether or not you want to be able to have children (maintain fertility) and whether or not the cancer has grown into blood or lymph vessels (called lymphovascular invasion).
Treatment options for women who want to maintain fertility
A cone biopsy is the preferred procedure for women who want to have children after the cancer is treated.
- If the edges of the cone don’t contain cancer cells (called negative margins), the woman can be watched closely without further treatment as long as the cancer doesn’t come back.
- If the edges of the cone biopsy have cancer cells (called positive margins), then cancer may have been left behind. This can be treated with a repeat cone biopsy or a radical trachelectomy.
- If the cancer has grown into blood or lymph vessels, one treatment option is a cone biopsy (with negative margins) with removal of pelvic lymph nodes. Another option is a radical trachelectomy along with removal of the pelvic lymph nodes.
Treatment options for women who don’t want to maintain fertility
- A simple hysterectomy may be an option if the cancer shows no lymphovascular invasion and the edges of the biopsy have no cancer cells. If the edges of the biopsy have cancer cells present, a repeat cone biopsy or a radical hysterectomy with removal of the pelvic lymph nodes might be an option.
- If the cancer has grown into blood or lymph vessels, you might need a radical hysterectomy along with removal of the pelvic lymph nodes. Sometimes, surgery is not done and external beam radiation to the pelvis followed by brachytherapy is used.
If none of the lymph nodes are found to have cancer, radiation may still be discussed as an option if the tumor is large, if the tumor has grown into blood or lymph vessels, or if the tumor is invading the surrounding connective tissue that supports organs such as the uterus, bladder, vagina (the stroma).
If the cancer has spread to the tissues next to the uterus (called the parametria) or to any lymph nodes, or if the tissue removed has positive margins, radiation (EBRT) with chemotherapy is usually recommended. The doctor may also advise brachytherapy after the combined chemo and radiation are done.
Stage 1A2 cervical cancer
Stage 1A2 means the cancer has grown between 3 and 5 mm into the cervical tissues. Treatment for this stage depends in part on whether or not you want to continue to be able to have children (maintain fertility).
Treatment options for women who want to maintain fertility
- Cone biopsy with removal of pelvic lymph nodes (pelvic lymph node dissection)
- Radical trachelectomy with pelvic lymph node dissection
Treatment options for women who don’t want to maintain fertility
- External beam radiation therapy (EBRT) to the pelvis plus brachytherapy
- Radical hysterectomy with removal of pelvic lymph nodes
If none of the lymph nodes have cancer cells, radiation may still be an option if the tumor is large, if the tumor has grown into blood or lymph vessels, or if the tumor is invading the surrounding connective tissue that supports organs such as the uterus, bladder, vagina (the stroma).
If the cancer has spread to the tissues next to the uterus (called the parametria) or to any lymph nodes, or if the tissue removed has positive margins, radiation (EBRT) with chemotherapy is usually recommended. The doctor may also advise brachytherapy after the combined chemo and radiation are done.
Stages 1B1 and 1B2 cervical cancer
- In stage 1B1 the cancer is deeper than 5mm but no more than 2cm in size.
- In stage 1B2 the cancer is at least 2cm but not bigger than 4cm in size.
Treatment options for women who want to maintain fertility
Radical trachelectomy with pelvic lymph node dissection and sometimes removal of the para-aortic lymph nodes
Treatment options for women who don’t want to maintain fertility
- Radical hysterectomy with removal of lymph nodes in the pelvis and sometimes lymph nodes from the para-aortic area. If none of the lymph nodes are found to have cancer, radiation may still be discussed as an option if the tumor is large, if the tumor has grown into blood or lymph vessels, or if the tumor is invading the surrounding connective tissue that supports organs such as the uterus, bladder, vagina (the stroma). If the cancer has spread to the tissues next to the uterus (called the parametria) or to any lymph nodes, or if the tissue removed has positive margins, radiation (EBRT) with chemotherapy is usually recommended. The doctor may also advise brachytherapy after the combined chemo and radiation are done.
- Radiation using both brachytherapy and external beam radiation therapy may be an option if a woman is not healthy enough for surgery or if she decides she does not want surgery. Chemotherapy (chemo) may be given with the radiation (concurrent chemoradiation).
Stages 1B3 and 2A2 cervical cancer
- Stage 1 means that your cancer is within the neck of the uterus (cervix). It hasn’t spread to nearby tissues or other organs. In stage 1B the cancerous areas are larger, but the cancer is still only in the tissues of the cervix and has not spread. It can usually be seen without a microscope, but not always. In stage 1B3 the cancer is at least 4cm but is still only in the cervix.
- Stage 2 means the cancer has spread outside the cervix, into the surrounding tissues. But it has not grown into the muscles or ligaments that line the pelvis (the area between the hip bones), or to the lower part of the vagina. In stage 2A the cancer has spread down into the top of the vagina. Stage 2A2 means the cancer is more than 4 cm.
Treatment options
- Chemoradiation: The chemo may be cisplatin, carboplatin, or cisplatin plus fluorouracil. The radiation therapy includes both external beam radiation and brachytherapy.
- Radical hysterectomy with pelvic lymph node dissection and para-aortic lymph node sampling: If cancer cells are found in the removed lymph nodes, or in the edges of the tissue removed (positive margins), surgery may be followed by radiation therapy, which is often given with chemo (concurrent chemoradiation).
- Chemoradiation followed by a hysterectomy
Stage 2A1 cervical cancer
Stage 2 means the cancer has spread outside the cervix, into the surrounding tissues. But it has not grown into the muscles or ligaments that line the pelvis (the area between the hip bones), or to the lower part of the vagina. In stage 2A the cancer has spread down into the top of the vagina. Stage 2A1 means the cancer is 4 cm or less.
Treatment options
- Radical hysterectomy with pelvic lymph node dissection and para-aortic lymph node sampling: If cancer cells are found in the removed lymph nodes, or in the edges of the tissue removed (positive margins), surgery may be followed by radiation therapy, which is often given with chemo (concurrent chemoradiation).
- Radiation with or without chemotherapy: The radiation therapy includes both external beam radiation and brachytherapy. The chemo may be cisplatin, carboplatin, or cisplatin plus fluorouracil.
Stages 2B, 3 and 4A cervical cancer
- Stage 2B cervical cancer means the cancer has spread up into the tissues around the cervix.
- Stage 3 cervical cancer means the cancer has spread from where it started in the cervix into the surrounding tissue or into the lymph nodes in the pelvis or abdomen. It might have grown down into the lower part of the vagina and the muscles and ligaments that line the pelvis (pelvic wall). Or it might have grown up to block the tubes that drain the kidneys (the ureters).
- Stage 4 means the cancer has spread to the bladder or rectum or further away. Stage 4A is when the cancer has spread to nearby organs such as the bladder or the rectum.
Treatment options
- Chemoradiation: The chemo may be cisplatin, carboplatin, or cisplatin plus fluorouracil. The radiation therapy includes both external beam radiation and brachytherapy.
Stage 4B cervical cancer
Stage 4B is when the cancer has spread to organs further away, such as the lungs. Your doctor might call this secondary or metastatic cancer. Stage 4B cervical cancer is not usually considered curable. Treatment options include radiation therapy with or without chemo to try to slow the growth of the cancer or help relieve symptoms. Most standard chemo regimens include a platinum drug (cisplatin or carboplatin) along with another drug such as paclitaxel (Taxol), gemcitabine (Gemzar), or topotecan. The targeted drug bevacizumab (Avastin) with chemo, immunotherapy alone with pembrolizumab (Keytruda), the targeted drug tisotumab vedotin-tftv (Tivdak), or pembrolizumab (Keytruda) with chemo (with or without bevacizumab [Avastin]), may also be options.
Clinical trials are testing other combinations of chemo drugs, as well as some other experimental treatments.
Recurrent cervical cancer
Cancer that comes back after treatment is called recurrent cancer. Cancer can come back locally (in or near where it first started, such as the cervix, uterus or nearby the pelvic organs), or it can come back in distant areas (such as the lungs or bone).
If the cancer has recurred in the center of the pelvis only, extensive surgery (such as pelvic exenteration) may be an option for some patients, and offers the best chance for possibly curing the cancer (although it can have major side effects). Radiation therapy (sometimes along with chemo) might be another option. If not, chemo, immunotherapy, or targeted therapy may be used to slow the growth of the cancer or help relieve symptoms, but they aren’t expected to cure the cancer.
No matter which type of treatment your doctor recommends, it’s important that you understand the goal of treatment (to try to cure the cancer, control its growth, or relieve symptoms), as well as its possible side effects and limitations. For example, sometimes chemo can improve your quality of life, and other times it might diminish it. You need to discuss this with your doctor.
New treatments that may benefit patients who have distant recurrence of cervical cancer are being evaluated in clinical trials.
Cervical cancer during pregnancy
A small number of cervical cancers are found in pregnant women. Treatment of cervical cancer during pregnancy depends on the stage of the cancer and how long the patient has been pregnant. A biopsy and imaging tests may be done to determine the stage of the disease. To avoid exposing the fetus to radiation, MRI (magnetic resonance imaging) is used. Most of cervical cancers during pregnancy (70%) are stage 1 cancers. The treatment plan during pregnancy is determined by:
- Tumor size
- If nearby lymph nodes have cancer
- How far along the pregnancy is
- The specific type of cervical cancer
If the cancer is at a very early stage, such as stage 1A, most doctors believe it is safe to continue the pregnancy to term and have treatment several weeks after birth. Surgery options after birth for early-stage cancers include a hysterectomy, radical trachelectomy, or a cone biopsy.
If the cancer is stage IB or higher, then you and your doctor must decide whether to continue the pregnancy. If not, treatment would be radical hysterectomy and/or radiation. Sometimes chemotherapy can be given during the pregnancy (in the second or third trimester) to shrink the tumor.
If you decide to continue the pregnancy, the baby should be delivered by cesarean section (C-section) as soon as it is able to survive outside the womb. More advanced cancers typically need be treated immediately.
Treatment Options for Cervical Cancer During Pregnancy
Carcinoma in Situ (Stage 0) during pregnancy
Usually, no treatment is needed for carcinoma in situ (stage 0) during pregnancy. A colposcopy may be done to check for invasive cancer.
Stage 1 cervical cancer during pregnancy
Pregnant women with slow-growing stage I cervical cancer may be able to delay treatment until the second trimester of pregnancy or after delivery.
Pregnant women with fast-growing stage I cervical cancer may need immediate treatment. Treatment may include:
- Conization.
- Radical trachelectomy.
Women should be tested to find out if the cancer has spread to the lymph nodes. If cancer has spread to the lymph nodes, immediate treatment may be needed.
Stage 2, 3, and 4 cervical cancer during pregnancy
Treatment for stage II, stage III, and stage IV cervical cancer during pregnancy may include the following:
- Chemotherapy to shrink the tumor in the second or third trimester of pregnancy. Surgery or radiation therapy may be done after delivery.
- Radiation therapy plus chemotherapy. Talk with your doctor about the effects of radiation on the fetus. It may be necessary to end the pregnancy before treatment begins.
Cervical cancer prognosis
Survival rates can give you an idea of what percentage of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding of how likely it is that your treatment will be successful. Keep in mind that survival rates are estimates and are often based on previous outcomes of large numbers of people who had a specific cancer, but they can’t predict what will happen in any particular person’s case. These statistics can be confusing and may lead you to have more questions. Your doctor is familiar with your situation; ask how these numbers may apply to you.
A relative survival rate compares women with the same type and stage of cervical cancer to women in the overall population. For example, if the 5-year relative survival rate for a specific stage of cervical cancer is 91.8%, it means that women who have that cancer are, on average, about 91.8% as likely as women who don’t have that cancer to live for at least 5 years after being diagnosed.
The National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database tracks 5-year relative survival rates for cervical cancer in the United States, based on how far the cancer has spread. The SEER database, however, does not group cancers by FIGO stages (stage 1, stage 2, stage 3, etc.). Instead, it groups cancers into localized, regional, and distant stages 4:
- Localized: There is no sign that the cancer has spread outside of the cervix or uterus.
- Regional: The cancer has spread beyond the cervix and uterus to nearby lymph nodes.
- Distant: The cancer has spread to nearby organs (like the bladder or rectum) or distant parts of the body such as the lungs or bones.
African American women tend to have the highest mortality and lowest survival rate 14. The survival rate may be less than 50 percent. Contributing factors to differences in outcomes may include differences in the delivery of evidence-based care, later stage of diagnosis, lymph node spreading, age, and size and invasion of the tumor at the time of diagnosis 14.
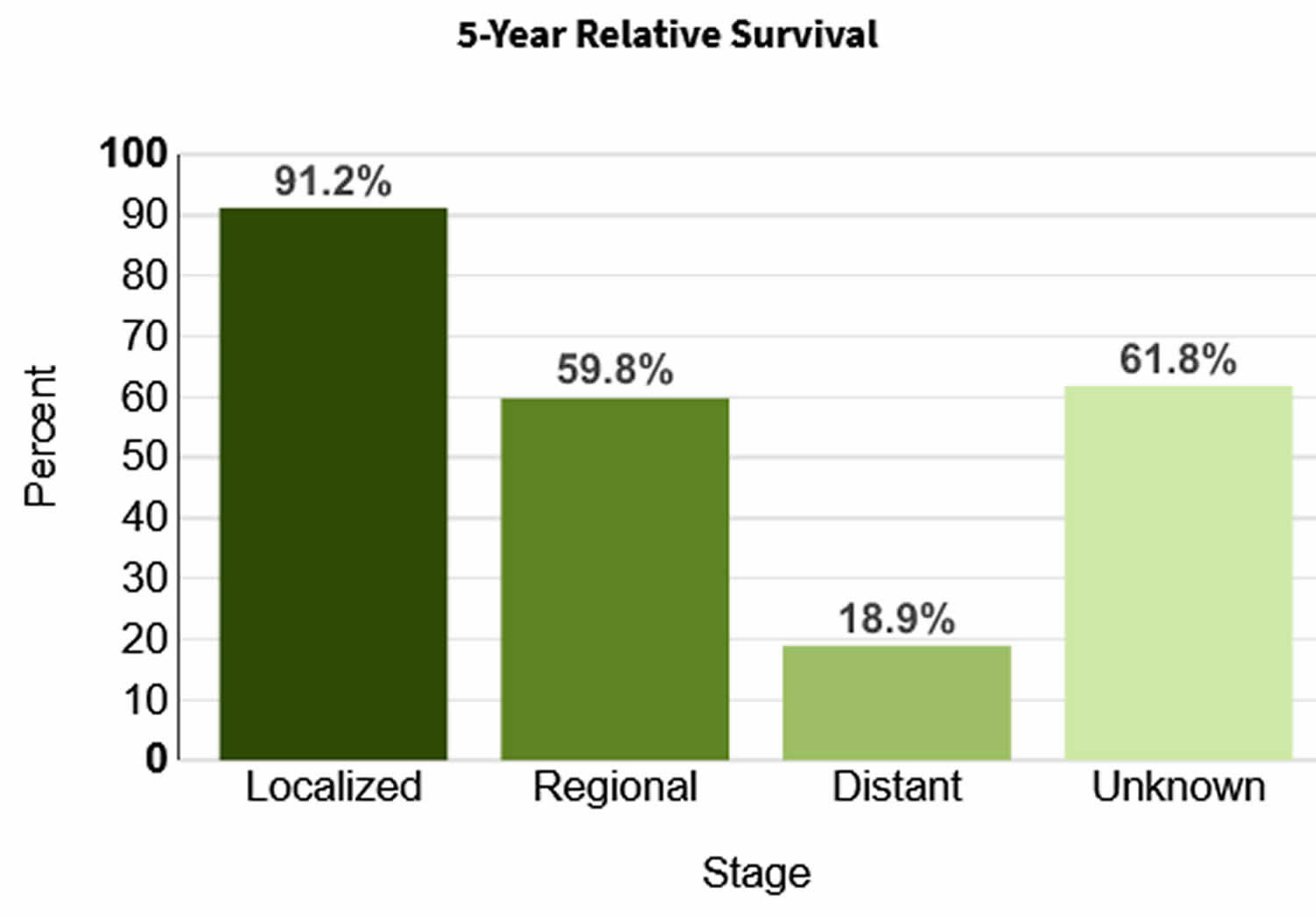
Table 2. 5-year relative survival rates for cervical cancer
| SEER Stage | 5-year Relative Survival Rate |
|---|---|
| Localized | 92% |
| Regional | 59% |
| Distant | 17% |
| All SEER stages combined | 67% |
Footnotes:
- Based on women diagnosed with cervical cancer between 2012 and 2018.
- Women now being diagnosed with cervical cancer may have a better outlook than these numbers show. Treatments improve over time, and these numbers are based on women who were diagnosed and treated at least five years earlier.
- These numbers apply only to the stage of the cancer when it is first diagnosed. They do not apply later on if the cancer grows, spreads, or comes back after treatment.
- These numbers don’t take everything into account. Survival rates are grouped based on how far the cancer has spread, but your age, overall health, how well the cancer responds to treatment, and other factors will also affect your outlook.
HPV and Cancer
What is HPV?
HPV is short for human papilloma virus. HPVs are a large group of related viruses. Each virus in the group is given a number, which is called an HPV type.
Most HPV types cause warts on the skin, such as on the arms, chest, hands, or feet. Other types are found mainly on the body’s mucous membranes. Mucous membranes are the moist surface layers that line organs and parts of the body that open to the outside, such as the vagina, anus, mouth, and throat. The HPV types found on mucous membranes are sometimes called genital HPV. They generally do not live on the skin.
Genital HPV is not the same as HIV or herpes. HPV is divided into 2 main groups:
Low-risk HPV types
Some types of HPV can cause warts (papillomas) on or around the genitals and anus of both men and women. Women may also have warts on the cervix and in the vagina. Because these HPV types rarely cause cancer, they are called “low-risk” viruses.
High-risk HPV types
Other types of HPV are called “high-risk” because they can cause cancer in both men and women. Doctors worry more about the cell changes and pre-cancers linked to these types, because they’re more likely to grow into cancers over time. Common high-risk HPV types include HPV 16 and 18.
Infection with HPV is very common. In most people, the body is able to clear the infection on its own. But sometimes, the infection doesn’t go away. Chronic, or long-lasting infection, especially when it’s caused by certain high-risk HPV types, can cause cancer over time.
How do people get HPV ?
HPV can be passed from one person to another by skin-to-skin contact, such as occurs with sexual activity. The main way HPV is spread is through sexual activity, including vaginal, anal, and oral sex. HPV can be spread even when an infected person has no visible signs or symptoms.
The virus can also be spread by genital contact without sex, although this is not common.
HPV infection is very common. Most men and women who have ever had sex get at least one type of genital HPV at some time in their lives. Anyone who has had sex can get HPV, even if it was only with only one person, but infections are more likely in people who have had many sex partners. Even if a person delays sexual activity until marriage, or only has one partner, they are still at risk of HPV infection if their partner has been exposed.
You cannot get HPV from:
- Toilet seats
- Hugging or holding hands
- Swimming pools or hot tubs
- Sharing food or utensils
- Being unclean
You can have HPV:
- Even if it has been years since you were sexually active
- Even if you do not have any signs or symptoms
Cancers linked to HPV infection
Cervical cancer
Cervical cancer is the most common cancer linked to HPV in women. Nearly all cervical cancers are caused by HPV.
Cervical cancer can be found early and even prevented with routine screening tests. The Pap test looks for changes in cervical cells caused by HPV infection. The HPV test looks for the infection itself.
- Cervical cancer is preventable with vaccines and regular screening tests. More than half of the women in the United States who get cervical cancer have never had or rarely had a Pap test.
Vulvar cancer
HPV can also cause cancer of the vulva, which is the outer part of the female genital organs. This cancer is much less common than cervical cancer.
There’s no standard screening test for this cancer other than routine physical exams.
Vaginal cancer
Most vaginal cancers contain HPV.
Many vaginal pre-cancers also contain HPV, and these changes may be present for years before turning into cancer. These pre-cancers can sometimes be found with the same Pap test that’s used to test for cervical cancer and pre-cancer. If a pre-cancer is found, it can be treated, stopping cancer before it really starts.
Penile cancer
In men, HPV can cause cancer of the penis. It’s more common in men with HIV and those who have sex with other men.
There’s no standard screening test to find early signs of penile cancer. Because almost all penile cancers start under the foreskin of the penis, they may be noticed early in the course of the disease.
Anal cancer
HPV can cause cancer of the anus in both men and women. It’s more common in people with HIV and in men who have sex with other men.
Screening tests for anal cancer are not routinely recommended for all people. Still, some experts recommend anal cytology testing (also called an anal Pap test because it’s much like the Pap test used for cervical cancer) for people at higher risk of anal cancer. This includes men who have sex with men, women who have had cervical cancer or vulvar cancer, anyone who is HIV-positive, and anyone who has had an organ transplant.
Mouth and throat cancer
HPV is found in some mouth and throat cancers in men and women. Most cancers found in the back of the throat, including the base of the tongue and tonsils, are HPV-related. These are the most common HPV-related cancers in men.
There’s no standard screening test to find these cancers early. Still, many can be found early during routine exams by a dentist, doctor, dental hygienist, or by self-exam.
Can HPV infection be prevented ?
There’s no sure way to prevent infection with all the different types of HPV. But there are things you can do to lower your chances of being infected. There are also vaccines that can be used to protect young people from the HPV types most closely linked to cancer and genital warts.
HPV is passed from one person to another during contact with an infected part of the body. Although HPV can be spread during sexual contact – including vaginal, anal, and oral sex – sex isn’t the only way for the infection to spread. All that’s needed is skin-to-skin contact with an area of the body infected with HPV. There may be other ways to become infected with HPV that aren’t yet clear.
HPV can be present for years without causing any symptoms. It doesn’t always cause warts or any other symptoms. Someone can have the virus and pass it on without knowing it.
Condom use
Condoms (“rubbers”) provide some protection against HPV, but they do not completely prevent infection.
Condoms must be used correctly every time sex occurs. Even then, condoms can’t protect completely because they don’t cover every possible HPV-infected area of the body, such as the skin on the genital or anal area. Still, condoms do provide some protection against HPV, and they also help protect against some other sexually transmitted infections.
A new condom should be used with each sex act. The condom should be put on BEFORE any genital, oral, or anal contact and kept on until sex is finished.
Limiting sex partners
If you are sexually active, limiting the number of sex partners and avoiding sex with people who have had many other sex partners can help lower your risk of exposure to genital HPV. But again, HPV is very common, so having sex with even one other person can put you at risk.
HPV vaccines
HPV vaccines can prevent infection with certain types of HPV, including types that are linked to HPV-related cancers, as well as types linked to anal and genital warts.
- HPV vaccines are approved for use in males and females. They can only be used to prevent HPV infection – they don’t help treat an existing infection. To work best, the vaccines should be given at or before age 11 or 12.
Testing for HPV
The HPV tests on the market are only approved to find cervical HPV infection in women. They can be used to help test women at certain ages and after certain Pap test findings to help look for cervical cancer.
- There’s no approved HPV test to find HPV on the penis or vulva, or in the anus, mouth, or throat.
- There’s no test for men or women to check one’s overall “HPV status.”
- For cervical cancer screening, the American Cancer Society recommends that women ages 30 to 65 get both an HPV test and Pap test every 5 years. (Another option for these women is just a Pap test every 3 years. While this can find the cell changes caused by HPV, it does not find HPV infection.)
There’s no treatment for the virus itself, but there are treatments for the cell changes that HPV can cause.
Cancer is easiest to treat when it’s found early – while it’s small and before it has spread. Some cancer screening tests can find early cell changes caused by HPV, and these changes can be treated before they even become cancer.
Visible genital warts can be removed with prescribed medicines. They can also be treated by a health care provider.
Things to remember about HPV
- HPV is a very common virus. Most men and women who have ever had sexual contact will get HPV at some time in their lives.
- There is no treatment for HPV, but in most cases it goes away without treatment.
- Having HPV does not mean you will get cancer. Most of the time HPV goes away by itself.
- Certain people are at higher risk for HPV-related health problems. This includes gay and bisexual men and people with weak immune systems (including those who have HIV/AIDS).
- Most HPV infections that lead to cancer can be prevented with vaccines.
- Most cervical cancers can be prevented by regular screening.
HPV Vaccine Facts and Fears
Vaccines to prevent human papillomavirus (HPV) infections are safe and effective. They can protect girls and boys from getting several different types of cancer when they get older. The American Cancer Society recommends the vaccine as one way to keep more people from getting cancer. HPV vaccines protect against high-risk types of the virus that cause most cervical cancers. The virus is also linked to cancers of the vulva, vagina, penis, anus, and throat. HPV vaccination is cancer prevention.
However, myths and rumors shared on social media, blogs, and alternative health websites make claims that may scare people away from this life-saving vaccine. The medical experts at the American Cancer Society have put together a list of facts about the HPV vaccine 16.
Fact 1: The vaccine is safe.
Years of studying people who have had the HPV vaccine show that it is safe. The HPV vaccine may make some people dizzy and nauseated when it is injected, but it hardly ever causes bad side effects. More than 80 million doses of the HPV vaccine have been given in the US with no serious problems. Data from clinical trials and initial post-marketing surveillance conducted in several continents show all three HPV vaccines [Gardasil 4v (Merck&Co, Kenilworth, NJ, US), Gardasil 9v (Merck&Co, Kenilworth, NJ, US), and Cervarix 2v (GlaxoSmithKline Biologicals, Rixensart, Belgium)] to be safe. However, rare cases of anaphylaxis (1.7 cases in 1 million doses), a life threatening allergic reaction, have been reported 17. The autoimmune/inflammatory syndrome induced by adjuvants have been reported in 3.6 cases per 100,000 vaccine doses16,17. An adjuvant is an ingredient used in some vaccines that helps create a stronger immune response in people receiving the vaccine. Adjuvants help the body to produce an immune response strong enough to protect the person from the disease he or she is being vaccinated against. Moreover, it remains controversial if the rare death cases after HPV vaccine could be linked to the adjuvant or the vaccine itself 18, 19. Despite the rare cases of post-vaccination syndromes, HPV vaccines are reported as being very safe and are the most effective preventive option 8.
Fact 2: The HPV vaccine causes no bad side effects.
The Centers for Disease Control and Prevention (CDC) have found no proof that HPV vaccines cause bad side effects. Like other vaccines, there may be common temporary side effects like pain, redness, and/or swelling where the shot was given. In rare cases, a person may have an allergic reaction to certain vaccines if they’re allergic to yeast or latex.
Fact 3: The HPV vaccine does not cause fertility problems.
Research has not shown that HPV vaccines cause fertility problems (problems having kids). The vaccine can help protect women from future fertility problems linked to cervical cancer. The HPV vaccine is a safe way to help protect health and the ability to have healthy babies.
Fact 4: The HPV vaccine does not contain harmful ingredients.
Some parents are worried about vaccine ingredients, one being aluminum. There is aluminum in the HPV vaccine, but it’s a safe amount. Aluminum-containing vaccines have been used for years and in more than 1 billion people. In fact – we come in contact with aluminum every day. It’s in foods we eat, water, and even breast milk. Every day, babies, children, and adults come into contact with more aluminum than what’s in the vaccine.
Fact 5: Getting the HPV vaccine is not opening the door to having sex.
Vaccines are used to help prevent diseases. They’re most useful when given before you come in contact with a virus. Young teens build more antibodies against the HPV vaccine (see Fact 8) and are less likely to already have HPV. So it’s better to get vaccinated as a teen than to wait to get it later.
Getting the HPV vaccine does not lead to changes in sexual behavior. The age when teens start having sex, the risk of sexually transmitted diseases, and number of pregnancies are much the same when comparing teens who have been vaccinated to those who have not.
HPV is so common that almost everyone will come in contact with it at some point in their lives. Even if someone waits until marriage to have sex, they could still get infected with HPV if their partner had previous contact. Vaccinating your child against HPV helps protect them.
Fact 6: The HPV vaccine is for both males and females.
Both males and females can get infected with HPV. About 8 or 9 out of 10 sexually active adults will have at least one type of HPV in their lifetime. Many people know that cervical cancer is caused by HPV. But there are cancers found in men that are linked to HPV infection. These include cancer of the anus, penis, throat, and tongue.
HPV vaccines are strongly recommended for boys and girls to help protect against HPV-linked cancers and genital warts. The HPV vaccine helps reduce the spread of HPV in both males and females.
Fact 7: The HPV vaccine works and can help prevent cervical cancer.
The HPV vaccine protects against almost all cervix HPV infections and pre-cancers.
Studies have shown that HPV vaccines can prevent infections and pre-cancers caused by HPV. Women in the United States, along with women in other countries that give the HPV vaccine, have fewer cervix changes and fewer cases of genital warts.
Fact 8: The HPV vaccine lasts a long time – maybe forever.
If your child gets the HPV vaccine they will make proteins called antibodies that fight the virus. Antibodies give strong and long-lasting protection. While there’s no sign that this protection will go down over time, studies are being done to watch this.
Current studies suggest that the vaccine protection lasts a long time. If studies show that protection drops, a booster shot may be needed, just like some other vaccines.
- Cervical Cancer—Patient Version. https://www.cancer.gov/types/cervical[↩][↩]
- What Is Cervical Cancer ? https://www.cancer.org/cancer/cervical-cancer/prevention-and-early-detection/what-is-cervical-cancer.html[↩]
- Key Statistics for Cervical Cancer. https://www.cancer.org/cancer/cervical-cancer/about/key-statistics.html[↩]
- Cervical Cancer — Cancer Stat Facts. https://seer.cancer.gov/statfacts/html/cervix.html[↩][↩]
- Deng, H., Hillpot, E., Mondal, S. et al. HPV16-Immortalized Cells from Human Transformation Zone and Endocervix are More Dysplastic than Ectocervical Cells in Organotypic Culture. Sci Rep 8, 15402 (2018). https://doi.org/10.1038/s41598-018-33865-2[↩]
- How Many Cancers Are Linked with HPV Each Year? https://www.cdc.gov/cancer/hpv/statistics/cases.htm[↩]
- Basic Information about HPV and Cancer. https://www.cdc.gov/cancer/hpv/basic_info/index.htm[↩][↩]
- Szymonowicz, K. A., & Chen, J. (2020). Biological and clinical aspects of HPV-related cancers. Cancer biology & medicine, 17(4), 864–878. https://doi.org/10.20892/j.issn.2095-3941.2020.0370[↩][↩]
- Luria L, Cardoza-Favarato G. Human Papillomavirus. [Updated 2022 Jan 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448132[↩]
- Human Papillomaviruses. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Volume 90. https://publications.iarc.fr/_publications/media/download/2799/9c5cbdc5c9ae322a22b5026c9e594451149a763f.pdf[↩]
- Human Papillomavirus (HPV) Vaccination: What Everyone Should Know. https://www.cdc.gov/vaccines/vpd/hpv/public/index.html[↩]
- The American Cancer Society Guidelines for the Prevention and Early Detection of Cervical Cancer. https://www.cancer.org/cancer/cervical-cancer/detection-diagnosis-staging/cervical-cancer-screening-guidelines.html[↩]
- Bhatla, N, Aoki, D, Sharma, DN, Sankaranarayanan, R. Cancer of the cervix uteri: 2021 update. Int J Gynecol Obstet. 2021; 155(Suppl. 1): 28– 44. https://doi.org/10.1002/ijgo.13865[↩][↩]
- Rauh-Hain JA, Melamed A, Schaps D, Bregar AJ, Spencer R, Schorge JO, Rice LW, Del Carmen MG. Racial and ethnic disparities over time in the treatment and mortality of women with gynecological malignancies. Gynecol Oncol. 2018 Apr;149(1):4-11. doi: 10.1016/j.ygyno.2017.12.006[↩][↩]
- Survival Rates for Cervical Cancer. https://www.cancer.org/cancer/cervical-cancer/detection-diagnosis-staging/survival.html[↩]
- HPV Vaccine: Facts and Fears. https://www.cancer.org/cancer/cancer-causes/infectious-agents/hpv/hpv-vaccine-facts-and-fears.html[↩]
- McNeil, M. M., Weintraub, E. S., Duffy, J., Sukumaran, L., Jacobsen, S. J., Klein, N. P., Hambidge, S. J., Lee, G. M., Jackson, L. A., Irving, S. A., King, J. P., Kharbanda, E. O., Bednarczyk, R. A., & DeStefano, F. (2016). Risk of anaphylaxis after vaccination in children and adults. The Journal of allergy and clinical immunology, 137(3), 868–878. https://doi.org/10.1016/j.jaci.2015.07.048[↩]
- Cervantes, J. L., & Doan, A. H. (2018). Discrepancies in the evaluation of the safety of the human papillomavirus vaccine. Memorias do Instituto Oswaldo Cruz, 113(8), e180063. https://doi.org/10.1590/0074-02760180063[↩]
- Palmieri, B., Poddighe, D., Vadalà, M., Laurino, C., Carnovale, C., & Clementi, E. (2017). Severe somatoform and dysautonomic syndromes after HPV vaccination: case series and review of literature. Immunologic research, 65(1), 106–116. https://doi.org/10.1007/s12026-016-8820-z[↩]

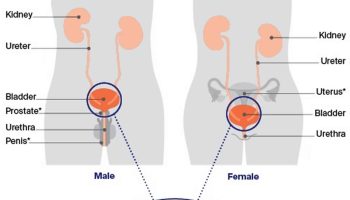
{kind=link}