Contents
- Myelodysplastic syndromes
- Myelodysplastic syndrome types
- Myelodysplastic syndrome causes
- Myelodysplastic syndrome risk factors
- Myelodysplastic syndrome prevention
- Myelodysplastic syndrome symptoms
- Myelodysplastic syndrome complications
- Myelodysplastic syndrome diagnosis
- Myelodysplastic syndrome treatment
- Myelodysplastic syndrome prognosis
- Myelodysplastic syndrome life expectancy
Myelodysplastic syndromes
Myelodysplastic syndromes also called MDS or myelodysplasia are a group of blood cancers in which immature blood cells (blood stem cells) in the bone marrow do not become mature red blood cells, white blood cells, or platelets or become healthy blood cells 1, 2, 3. These immature blood cells, called blasts, do not work the way they should and either die in the bone marrow or soon after they go into the blood 4, 5. In myelodysplastic syndromes (MDS), some of the blood cells (white blood cells, red blood cells, and platelets) in your bone marrow are abnormal (dysplastic) and have problems making new blood cells. Many of the blood cells formed by these bone marrow cells are defective. Defective cells often die earlier than normal cells, and the body also destroys some abnormal blood cells, leaving the person without enough normal blood cells. Different cell types can be affected, although the most common finding in MDS is a shortage of red blood cells (anemia), infection or easy bleeding.
Myelodysplastic syndromes (MDS) occurs as a result of a mutation (change) in one or more of the genes that control blood cell development. This change or changes results in the abnormal growth of blood stem cells.
There are several different types of MDS, based on how many types of blood cells are affected and other factors. Myelodysplastic syndromes (MDS) types include:
- Myelodysplastic syndromes with multilineage dysplasia: In this subtype, two or three blood cell types (red blood cells, platelets, or white blood cells) are abnormal. Less than 5% of the cells in the bone marrow are blasts and less than 1% of the cells in the blood are blasts. If red blood cells are affected, they may have extra iron. Myelodysplastic syndromes with multilineage dysplasia may progress to acute myeloid leukemia (AML).
- Myelodysplastic syndromes with single-lineage dysplasia: One blood cell type — white blood cells, red blood cells or platelets — is low in number and appears abnormal under the microscope. There are changes in 10% or more of two other types of blood cells. Less than 5% of the cells in the bone marrow are blasts and less than 1% of the cells in the blood are blasts.
- Myelodysplastic syndromes with ring sideroblasts: This subtype involves a low number of one or more blood cell types. There are too few red blood cells in the blood and the patient has anemia. A characteristic feature is that existing red blood cells in the bone marrow contain rings of excess iron. The number of white blood cells and platelets is normal.
- Myelodysplastic syndrome associated with an isolated del(5q) chromosome abnormality: People with this subtype have low numbers of red blood cells and the patient has anemia and the red blood cells have a specific mutation in their DNA (change in the chromosome 5). Less than 5% of the cells in the bone marrow and blood are blasts. .
- Myelodysplastic syndromes with excess blasts: In this subtype, any of the three types of blood cells — red blood cells, white blood cells or platelets — might be low and appear abnormal under a microscope. Very immature blood cells (blasts) are found in the blood and bone marrow. Five percent to 19% of the cells in the bone marrow are blasts. There also may be changes to the white blood cells and platelets. Myelodysplastic syndromes with excess blasts may progress to acute myeloid leukemia (AML).
- Myelodysplastic syndromes unclassifiable. In this subtype, there are reduced numbers of one or more types of mature blood cells and the cells might look abnormal under the microscope. Sometimes the blood cells appear normal, but analysis might find that the cells have DNA changes that are associated with myelodysplastic syndromes.
In about 1 in 3 patients, MDS can progress to a rapidly growing cancer of bone marrow cells called acute myeloid leukemia (AML). In the past, MDS was sometimes referred to as pre-leukemia or smoldering leukemia. Because most patients do not get leukemia, MDS used to be classified as a disease of low malignant potential. Now that doctors have learned more about MDS, it is considered to be a form of blood cancer.
Overall, MDS is relatively uncommon. The number of people diagnosed with myelodysplastic syndromes (MDS) in the United States each year is not known for sure 6. Some estimates have put this number at about 10,000, for an annual age-adjusted incidence rate of approximately 4.4 to 4.6 cases per 100,000 people 7, 6.
Myelodysplastic syndromes (MDS) is uncommon before age 50, and the risk increases as a person gets older (usually older than 60 years) 6. Myelodysplastic syndromes (MDS) is most commonly diagnosed in people in their 70s, although patients as young as 2 years have been reported 8, 9. The number of new cases diagnosed each year is likely increasing as the average age of the US population increases.
People with myelodysplastic syndromes (MDS) might not experience signs and symptoms at first. In time due shortages of one or more types of blood cells (cytopenias), myelodysplastic syndromes might cause:
- Fatigue
- Shortness of breath
- Unusual paleness (pallor), which occurs due to a low red blood cell count (anemia)
- Easy or unusual bruising or bleeding, which occurs due to a low blood platelet count (thrombocytopenia)
- Pinpoint-sized red spots just beneath the skin that are caused by bleeding (petechiae)
- Frequent infections, which occur due to a low white blood cell count (leukopenia)
Sometimes myelodysplastic syndromes (MDS) is found on blood tests, even before symptoms appear.
Other symptoms can include:
- Weight loss
- Fever
- Bone pain
- Loss of appetite
- Frequent or severe nosebleeds or bleeding from the gums.
These symptoms are more likely to be caused by something other than MDS. Still, if you have any of these symptoms, especially if they don’t go away or get worse over time, see your doctor so that the cause can be found and treated, if needed.
Management of myelodysplastic syndromes is most often intended to slow the disease, ease symptoms and prevent complications. Common measures include blood transfusions and medications to boost blood cell production. In certain situations, a bone marrow transplant, also known as a stem cell transplant, may be recommended to replace your bone marrow with healthy bone marrow from a donor.
Figure 1. Myelodysplastic syndromes
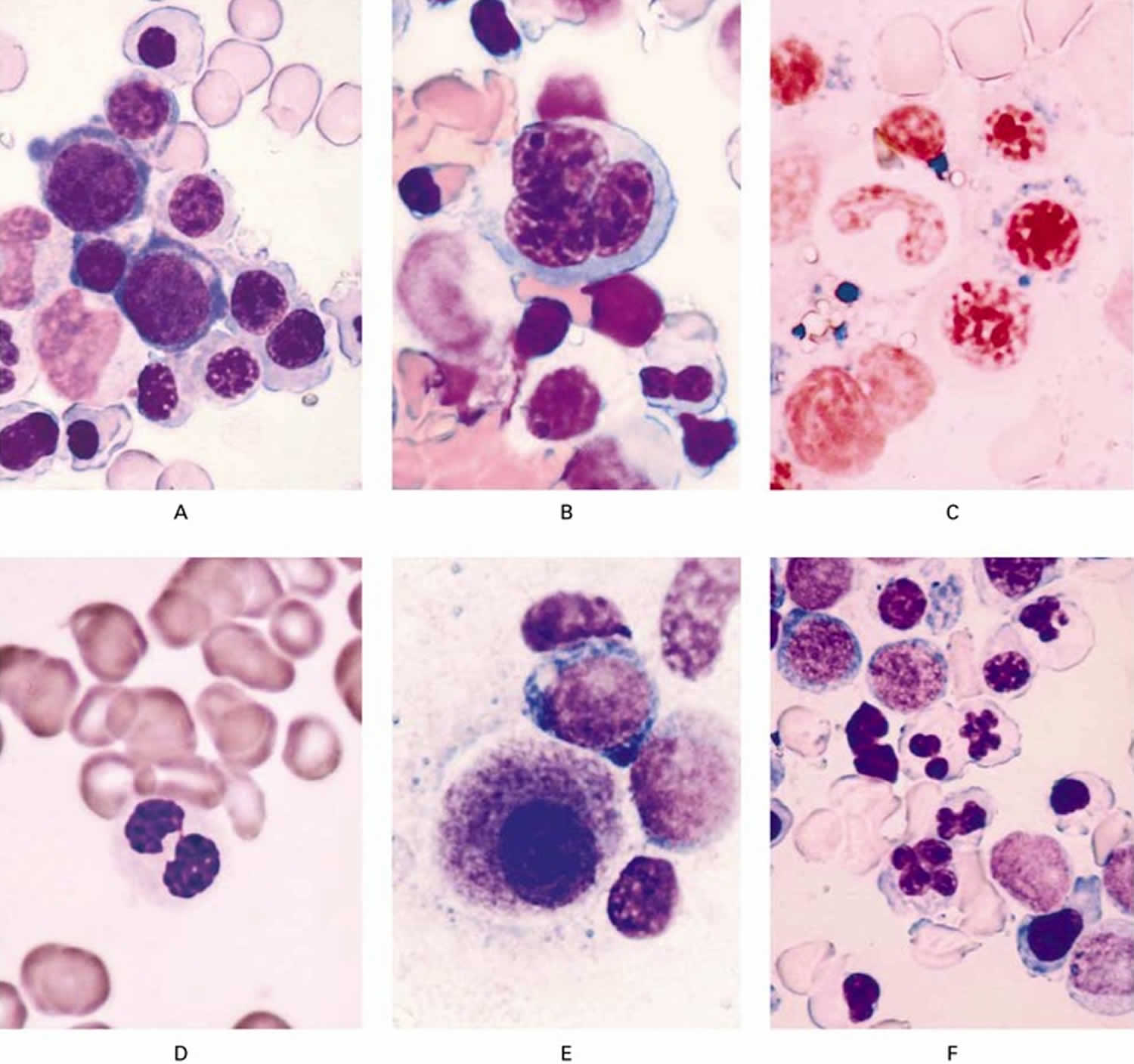
Footnotes: (A) Shows megaloblastic erythropoiesis with cytoplasmic blebbing in a bone marrow specimen (Wright–Giemsa stain, ×100). (B) A multinucleated erythroid precursor in a bone marrow specimen (Wright–Giemsa stain, ×100). (C) A ringed sideroblast in a bone marrow specimen (Prussian blue stain, ×100). (D) a pseudo-Pelger–Huët neutrophil in a specimen of peripheral blood (Wright–Giemsa stain, ×100). (E) A bone marrow micromegakaryocyte (Wright–Giemsa stain, ×100). (F) Misshapen nuclei in bone marrow erythroid precursors (Wright–Giemsa stain, ×100).
[Source 5Normal bone marrow
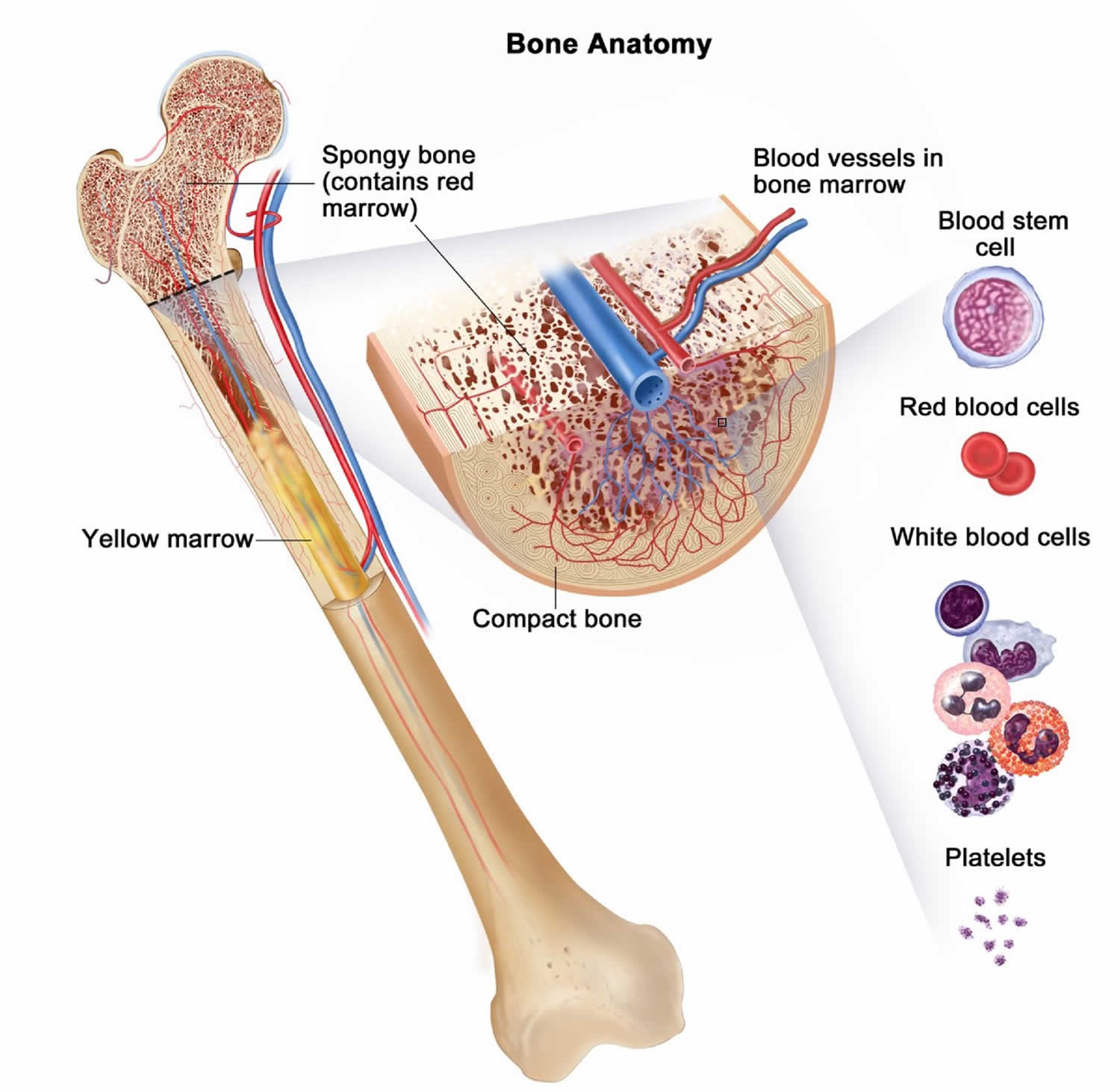
Bone marrow is found in the middle of certain bones. Bone marrow is made up of blood-forming cells, fat cells, and supporting tissues (Figure 3). A small fraction of the blood-forming cells are blood stem cells. Stem cells are needed to make new blood cells (Figure 2).
There are 3 main types of blood cells: red blood cells, white blood cells, and platelets.
- Red blood cells (erythrocytes) pick up oxygen in your lungs and carry it to the rest of the body. Red blood cells (erythrocytes) also bring carbon dioxide back to the lungs. Having too few red blood cells is called anemia. It can make a person feel tired and weak and look pale. Severe anemia can cause shortness of breath.
- White blood cells (leukocytes) are important in defending the body against infection. There are different types of white blood cells:
- Granulocytes are white blood cells that have granules that can be seen under the microscope. In the bone marrow, granulocytes develop from young cells called myeloblasts. The most common type of granulocyte is the neutrophil. When the number of neutrophils in the blood is low, the condition is called neutropenia. This can lead to severe infections.
- Monocytes are also important in protecting the body against germs. The cells in the bone marrow that turn into monocytes are called monoblasts.
- Lymphocytes make proteins called antibodies that help the body fight germs. They can also directly kill invading germs. Lymphocytes are not usually abnormal in MDS.
- Platelets (thrombocytes) are thought of as a type of blood cell, but they are actually small pieces of a cell. They start as a large cell in the bone marrow called the megakaryocyte. Pieces of this cell break off and enter the bloodstream as platelets. You need platelets for your blood to clot. They plug up damaged areas of blood vessels caused by cuts or bruises. A shortage of platelets, called thrombocytopenia, can result in abnormal bleeding or bruising.
Figure 2. Hematopoiesis (the process of all three types of blood cells formation)
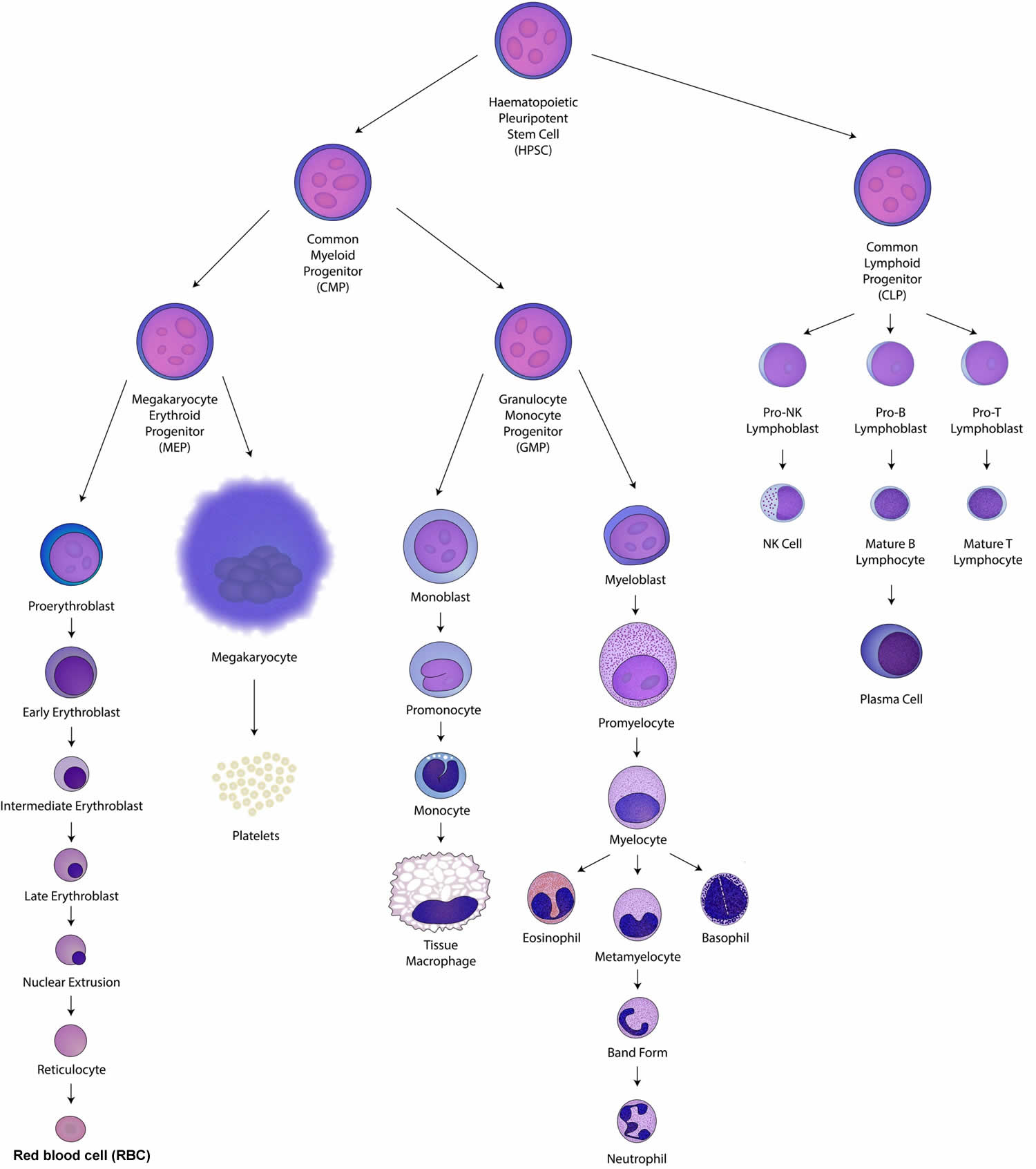
Footnotes: Hematopoietic stem cells (HSCs) also called hematopoietic plueripotent stem cell (HPSC) are the stem cells that give rise to both the common myeloid progenitor (CMP) and lymphoid progenitor (CLP) cells of blood cells through the process of hematopoiesis. Common myeloid progenitors (CMPs) can general all mature myeloid cells while granulocyte-monocyte progenitors (GMPs) or megakaryocyte-erythroid progenitors (MEPs) produce only myeloid or monocytic and megakaryocytic or erythroid lineage cells respectively. B and T lymphocytes and NK cells differentiate from the common lymphoid progenitor (CLP).
[Source 10 ]Figure 3. Bone marrow anatomy
 Myelodysplastic syndrome types
Myelodysplastic syndrome types
Myelodysplastic syndromes (MDS) are classified using the World Health Organization (WHO) classification system, which was most recently updated in 2016 11. It divides MDS into types based mainly on how the cells in the bone marrow look under the microscope, as well as some other factors:
- How many early forms of cell types in the bone marrow (red blood cells, white blood cells, or platelets) show dysplasia (look abnormal under the microscope).
- How many types of low blood cell counts (cytopenias) a person has.
- What portion of early red blood cells are ring sideroblasts (cells that contain rings of iron deposits around the nucleus).
- The portion of blasts (very early forms of blood cells) in the bone marrow or blood.
- Certain chromosome changes in the bone marrow cells.
Based on these factors, the World Health Organization (WHO) system recognizes 6 main types of MDS 11, 12:
- MDS with multilineage dysplasia (MDS-MLD)
- MDS with single lineage dysplasia (MDS-SLD)
- MDS with ring sideroblasts (MDS-RS)
- MDS with excess blasts (MDS-EB)
- MDS with isolated del(5q)
- MDS unclassifiable (MDS-U)
Because small differences in the way the cells look can change the diagnosis, doctors may sometimes disagree on a patient’s exact type of MDS.
Along with the World Health Organization (WHO) classification, myelodysplastic syndromes (MDS) can also be classified based on the underlying cause. This is known as a clinical classification.
- If no cause can be identified, it’s called primary MDS. This type is more common myelodysplastic syndromes (MDS).
- When the cause of the disease is known, it’s called secondary MDS. Secondary MDS is often related to prior cancer treatment, or it develops in someone who already had a different bone marrow disease.
Identifying MDS as primary or secondary is important because the secondary type is much less likely to respond to treatment.
Table 1. Myelodysplastic syndromes (MDS) comparison of the French-American-British (FAB) and World Health Organization (WHO) classification Classifications
| FAB (1982) | WHO (2008) |
|---|---|
| Myelodysplastic Syndromes | |
| Refractory anemia. | Refractory anemia. |
| Refractory cytopenia with multilineage dysplasia. Refractory cytopenia with unilineage dysplasia. | |
| Refractory anemia with ring sideroblasts. | Refractory anemia with ring sideroblasts. |
| Refractory anemia with excess blasts. | Refractory anemia with excess blasts -1 and -2. |
| Myelodysplastic syndrome, unclassifiable. | |
| Myelodysplastic syndrome associated with del(5q). | |
| Reclassified from MDS to: | |
| Refractory anemia with excess blasts in transformation. | Acute myeloid leukemia identified as AML with multilineage dysplasia following a myelodysplastic syndrome. |
| Chronic myelomonocytic leukemia. | Myelodysplastic and myeloproliferative diseases. |
Abbreviations: AML = acute myeloid leukemia; FAB = French-American-British classification scheme; MDS = myelodysplastic syndromes; WHO = World Health Organization.
[Source 3 ]MDS with multilineage dysplasia (MDS-MLD)
In MDS with multilineage dysplasia (MDS-MLD):
- Dysplasia is seen in at least 10% of the early cells of 2 or 3 cell types (red blood cells, white blood cells, and/or megakaryocytes [the cells that make platelets]) in the bone marrow.
- The person has low numbers of at least 1 type of blood cell.
- There is a normal number (less than 5%) of very early cells called blasts in the bone marrow, and blasts are rare (or absent) in the blood.
MDS with multilineage dysplasia (MDS-MLD) is the most common type of MDS. In the past, it was referred to as refractory cytopenia with multilineage dysplasia (RCMD).
MDS with single lineage dysplasia (MDS-SLD)
In MDS with single lineage dysplasia (MDS-SLD):
- Dysplasia is seen in at least 10% of the early cells of 1 cell type (either red blood cells, white blood cells, or megakaryocytes [the cells that make platelets]) in the bone marrow.
- The person has low numbers of 1 or 2 types of blood cells, but normal numbers of the other type(s).
- There is a normal number (less than 5%) of very early cells called blasts in the bone marrow, and blasts are rare (or absent) in the blood.
MDS with single lineage dysplasia (MDS-SLD) is not common. It seldom, if ever, progresses to acute myeloid leukemia (AML) 12. Patients with this type of MDS can often live a long time, even without treatment 12.
MDS with single lineage dysplasia (MDS-SLD) was referred to as refractory cytopenia with unilineage dysplasia (RCUD) in the previous classification system. It includes refractory anemia (RA), refractory neutropenia (RN), and refractory thrombocytopenia (RT), depending on which cell type is affected 12.
MDS with ring sideroblasts (MDS-RS)
In MDS with ring sideroblasts (MDS-RS), many of the early red blood cells are ring sideroblasts. For this diagnosis, at least 15% of the early red blood cells must be ring sideroblasts (or at least 5% if the cells also have a mutation in the SF3B1 gene).
MDS with ring sideroblasts (MDS-RS) is further divided into 2 types, based on how many of the cell types in the bone marrow are affected by dysplasia:
- MDS with ring sideroblasts with single lineage dysplasia (MDS-RS-SLD): dysplasia in only one cell type
- MDS with ring sideroblasts with multilineage dysplasia (MDS-RS-MLD): dysplasia in more than one cell type
MDS with ring sideroblasts (MDS-RS) is not common. It rarely turns into acute myeloid leukemia (AML) and the outcome for people with this type is generally better than for some other types of MDS 12.
MDS with ring sideroblasts (MDS-RS) was previously referred to as refractory anemia with ring sideroblasts (RARS) 12.
MDS with excess blasts (MDS-EB)
In MDS with excess blasts (MDS-EB), there are more blasts than normal in the bone marrow and/or blood. The person also has low numbers of at least one type of blood cell. There may or may not be severe dysplasia in the bone marrow.
MDS with excess blasts (MDS-EB) is further divided into 2 types, based on how many of the cells in the bone marrow or blood are blasts:
- MDS-EB1: blasts make up 5% to 9% of the cells in the bone marrow, or 2% to 4% of the cells in the blood
- MDS-EB2: blasts make up 10% to 19% of the cells in the bone marrow, or 5% to 19% of the cells in the blood
MDS with excess blasts (MDS-EB) accounts for about 1 in 4 cases of MDS. It is one of the types most likely to turn into acute myeloid leukemia (AML), with the risk being higher for MDS-EB2 than for MDS-EB1 12.
MDS with excess blasts (MDS-EB) was previously referred to as refractory anemia with excess blasts (RAEB) 12.
MDS with isolated del(5q)
In MDS with isolated del(5q), the chromosomes of the bone marrow cells are missing part of chromosome number 5. There may also be one other chromosome abnormality, as long as it isn’t a loss of part or all of chromosome 7. The person also has low numbers of 1 or 2 types of blood cells (usually red blood cells), and there is dysplasia in at least 1 cell type in the bone marrow.
MDS with isolated del(5q) is not common. It occurs most often in older women 12. For reasons that aren’t clear, patients with MDS with isolated del(5q) tend to have a good prognosis (outlook). They often live a long time and rarely go on to develop acute myeloid leukemia (AML).
MDS, unclassifiable (MDS-U)
MDS, unclassifiable (MDS-U) is uncommon. For MDS, unclassifiable (MDS-U), the findings in the blood and bone marrow don’t fit any other type of MDS. For example, the numbers of any one of the cell types may be low in the blood, but less than 10% of that type of cell looks abnormal in the bone marrow. Or the cells in the bone marrow have at least one certain chromosome abnormality that is only seen in MDS or leukemia.
MDS, unclassifiable (MDS-U) is rare, so it has not been studied well enough to predict prognosis (outlook) 12.
Myelodysplastic syndrome causes
Most myelodysplastic syndromes have no known cause. Others are caused by exposure to cancer treatments, such as chemotherapy and radiation, or to toxic chemicals, such as benzene.
Scientists have made great progress in understanding how certain changes in the DNA in bone marrow cells may cause myelodysplastic syndromes to develop. DNA is the chemical that makes up our genes, which control how your cells function. Usually mutations in several different genes inside bone marrow cells are needed before a person develops MDS. Some of the mutations most often seen in MDS cells include those in the DNMT3A, TET2, ASXL1, TP53, RUNX1, SRSF2, and SF3B1 genes 13. Some of these gene changes can be inherited from a parent, but more often they happen during a person’s lifetime.
Inherited gene changes
Researchers have found the gene changes that cause some rare inherited syndromes (like familial platelet disorder with a propensity to myeloid malignancy) linked to an increased risk of developing MDS. This syndrome is caused by inherited changes in the RUNX1 gene. Normally, this gene helps control the development of blood cells. Changes in this gene can lead to blood cells not maturing like they normally would, which can increase the risk of developing MDS.
Gene changes acquired during a person’s lifetime
Often, it’s not known why people without inherited syndromes develop MDS. Some outside exposures can lead to MDS by damaging the DNA inside bone marrow cells. For example, tobacco smoke contains chemicals that can damage genes. Exposure to radiation or certain chemicals such as benzene or some chemotherapy drugs can also cause mutations that lead to MDS. But sometimes the gene changes that lead to MDS seem to occur for no apparent reason. Many of these gene changes are probably just random events that sometimes happen inside a cell, without having an outside cause.
Gene changes inside cells can build up over a person’s lifetime, which might help explain why MDS largely affects older people.
Myelodysplastic syndrome risk factors
Anything that increases a person’s chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop myelodysplastic syndromes, and they will develop in people who don’t have any known risk factors. Talk with your doctor if you think you may be at risk. Risk factors for myelodysplastic syndromes include the following 14, 15:
Past treatment with chemotherapy or radiation therapy for cancer
Chemotherapy or radiation therapy, both of which are commonly used to treat cancer, can increase your risk of myelodysplastic syndromes. When MDS is caused by cancer treatment it is called secondary MDS or treatment-related MDS.
- The risk of secondary MDS varies based on the type and doses of drugs. It might also be affected by the type of cancer the chemo is treating. Combining these drugs with radiation therapy increases the risk further. People who have had stem cell transplants (bone marrow transplants) can also develop MDS because of the very high doses of chemo they received. Still, only a small percentage of people who are treated with these medicines will eventually develop MDS.
- Some of the drugs that can lead to MDS include:
- Mechlorethamine (nitrogen mustard)
- Procarbazine
- Chlorambucil
- Cyclophosphamide
- Ifosfamide
- Etoposide
- Teniposide
- Doxorubicin
Older age
Older age is one of the most important risk factors for MDS. MDS is uncommon in people younger than 50, and most cases are found in people in their 70s or 80s.
Exposure to certain chemicals
- Being exposed to certain chemicals, including tobacco smoke, pesticides, fertilizers, and solvents such as benzene.
- Being exposed to heavy metals, such as mercury or lead.
Environmental exposures
Some environmental exposures have been linked to MDS:
- High-dose radiation exposure such as surviving an atomic bomb blast or nuclear reactor accident increases the risk of developing MDS.
- Long-term workplace exposure to benzene and certain chemicals used in the petroleum and rubber industries can also increase the risk of developing MDS.
Sex
Myelodysplastic syndromes (MDS) is more common in men than in women. The reason for this is not clear, although it might have to do with men having been more likely to smoke or to be exposed to certain chemicals in the workplace in the past.
Genetic syndromes
People with certain inherited syndromes are more likely to develop MDS. These syndromes are caused by abnormal (mutated) genes that have been passed on from one or both parents. Examples include:
- Fanconi anemia
- Shwachman-Diamond syndrome
- Diamond Blackfan anemia
- Familial platelet disorder with a propensity to myeloid malignancy
- Severe congenital neutropenia
- Dyskeratosis congenita
Familial myelodysplasia
In some families, myelodysplastic syndromes (MDS) occurs more often than would be expected. Sometimes this is due to a known gene mutation that runs in the family, but in other cases the cause isn’t clear.
Smoking
Smoking increases the risk of myelodysplastic syndromes (MDS). Many people know that smoking can cause cancer of the lungs, but it can also cause cancer in other parts of the body that don’t come into direct contact with smoke. Cancer-causing substances in tobacco smoke are absorbed into the blood as it passes through the lungs. Once in the bloodstream, these substances spread to many parts of the body.
Myelodysplastic syndrome prevention
There is no sure way to prevent myelodysplastic syndromes (MDS). But there are things you can do that might lower your risk.
- Not smoking. Since smoking is linked to an increased risk of MDS, not smoking can lower the risk. Of course, people who don’t smoke are also less likely than people who smoke to develop many other types of cancers, as well as heart disease, stroke, and other diseases.
- Avoiding exposure to radiation or certain chemicals. Avoiding known cancer-causing industrial chemicals, such as benzene, might lower your risk of developing MDS.
Treating cancer with radiation and certain chemotherapy drugs can increase the risk of MDS. Doctors are studying ways to limit the risk of MDS in patients who get these treatments. For some cancers, doctors may try to avoid using the chemotherapy drugs that are more likely to lead to MDS. Some people, however, may need these specific drugs. Often, the obvious benefits of treating life-threatening cancers with chemo and radiation therapy must be balanced against the small chance of developing MDS several years later.
Myelodysplastic syndrome symptoms
People with myelodysplastic syndromes (MDS) might not experience signs and symptoms at first. In time due shortages of one or more types of blood cells (cytopenias), myelodysplastic syndromes might cause:
- Fatigue
- Shortness of breath
- Unusual paleness (pallor), which occurs due to a low red blood cell count (anemia)
- Easy or unusual bruising or bleeding, which occurs due to a low blood platelet count (thrombocytopenia)
- Pinpoint-sized red spots just beneath the skin that are caused by bleeding (petechiae)
- Frequent infections, which occur due to a low white blood cell count (leukopenia)
Sometimes myelodysplastic syndromes (MDS) is found on blood tests, even before symptoms appear.
Other symptoms can include:
- Weight loss
- Fever
- Bone pain
- Loss of appetite
- Frequent or severe nosebleeds or bleeding from the gums.
These symptoms are more likely to be caused by something other than MDS. Still, if you have any of these symptoms, especially if they don’t go away or get worse over time, see your doctor so that the cause can be found and treated, if needed.
Myelodysplastic syndrome complications
Complications of myelodysplastic syndromes include:
- Anemia. Reduced numbers of red blood cells can cause anemia, which can make you feel tired.
- Recurrent infections. Having too few white blood cells increases your risk of serious infections.
- Bleeding that won’t stop. Lacking platelets in your blood to stop bleeding can lead to excessive bleeding.
- Increased risk of cancer. Some people with myelodysplastic syndromes might eventually develop a cancer of the bone marrow and blood cells (leukemia).
Myelodysplastic syndrome diagnosis
A physical exam, medical history and tests might be used if your doctor suspects that you have a myelodysplastic syndrome.
Tests might include:
- Blood tests. Your doctor might order blood tests to determine the number of red cells, white cells and platelets and look for unusual changes in the size, shape and appearance of various blood cells.
- Removing bone marrow for testing. During a bone marrow biopsy and aspiration, a thin needle is used to withdraw (aspirate) a small amount of liquid bone marrow, usually from a spot on the back of your hipbone. Then a small piece of bone with its marrow is removed (biopsy).
Blood and bone marrow samples are sent for laboratory analysis. Specialized tests can determine the specific characteristics of your cells that will be helpful for determining the type of myelodysplastic syndrome you have, your prognosis and your treatment options.
Blood cell counts and blood cell examination
The complete blood count (CBC) is a test that measures the levels of red blood cells, white blood cells, and platelets in your blood. The CBC is often done with a differential count (or “diff”), which is a count of the different types of white blood cells in the blood sample. In a blood smear, some of the blood is put on a slide to see how the cells look under the microscope.
Patients with MDS often have too few red blood cells (anemia). They may have shortages of white blood cells and blood platelets as well. Patients with some types of MDS might also have myeloblasts (“blasts”) in the blood. These are very early forms of blood cells that are normally only found in bone marrow. Blasts in the blood are not normal and are often a sign of a bone marrow problem. Blood cells from MDS patients may also have certain abnormalities in size, shape, or other features that can be seen under the microscope.
Blood abnormalities may suggest MDS, but the doctor cannot make an exact diagnosis without examining a sample of bone marrow cells.
Other blood tests
The doctor may also order tests to check for other possible causes of low blood counts. For example, low levels of iron, vitamin B12, or folate can cause anemia. If one of these is found to be abnormal, a diagnosis of MDS is much less likely.
Bone marrow tests
Bone marrow samples are obtained from a bone marrow aspiration and biopsy, tests that are usually done at the same time. The samples are usually taken from the back of the pelvic (hip) bone. These tests are used first for diagnosis and classification, and they may be repeated later to tell if the MDS is responding to treatment or is transforming into an acute leukemia.
In bone marrow aspiration, the skin over the hip and the surface of the bone is numbed with local anesthetic, which may cause a brief stinging or burning sensation. A thin, hollow needle is then inserted into the bone, and a syringe is used to suck out a small amount of liquid bone marrow. Even with the anesthetic, most patients still have some brief pain when the marrow is removed.
A bone marrow biopsy is usually done just after the aspiration. A small piece of bone and marrow is removed with a slightly larger needle that is put into the bone. The biopsy may also cause some brief pain. Once the biopsy is done, pressure will be applied to the site to help prevent bleeding.
Lab tests of bone marrow or blood samples
A pathologist (a doctor specializing in the diagnosis of diseases using laboratory tests) examines the bone marrow and blood samples under a microscope. Other doctors, such as a hematologist (a doctor specializing in medical treatment of diseases of the blood and blood-forming tissues), might review these as well.
The doctors will look at the size, shape, and other features of the cells. The percentage of cells in the bone marrow or blood that are blasts (very early forms of blood cells) is particularly important. In MDS, the blasts do not mature properly, so there may be too many blasts and not enough mature cells.
For a diagnosis of MDS, a patient must have less than 20% blasts in the bone marrow and blood. A patient who has more than 20% blasts is considered to have acute myeloid leukemia (AML).
Other types of lab tests can also be done on the bone marrow or blood samples to help diagnose MDS:
Flow cytometry and immunocytochemistry
For both flow cytometry and immunocytochemistry, samples of cells are treated with antibodies, which are proteins that stick only to certain other proteins on cells. For immunocytochemistry, the cells are then looked at under a microscope to see if the antibodies stuck to them (meaning they have these proteins), while for flow cytometry a special machine is used.
These tests can be helpful in distinguishing different types of MDS or leukemia from one another and from other diseases.
Chromosome tests
These tests look at the chromosomes (long strands of DNA) inside the cells. Each cell should have 46 chromosomes (23 pairs). Abnormal chromosomes are common in MDS (see below).
Cytogenetics
In this test, the cells are looked at under a microscope to see if the chromosomes have any abnormalities. A drawback of this test is that it usually takes about 2 to 3 weeks because the cells must grow in lab dishes for a couple of weeks before their chromosomes can be viewed.
The results of cytogenetic testing are written in a shorthand form that describes which chromosome changes are present. For example:
- A minus sign (-) or the abbreviation “del” is used to mean a deletion. For example, if a copy of chromosome 7 is missing, it can be written as -7 or del(7). Often, only a part of the chromosome is lost. There are 2 parts to a chromosome, called p and q. The loss of the q part of chromosome 5 is written 5q- or del(5q).
- A plus sign (+) is used when there is an addition (an extra copy of all or part of a chromosome). +8, for example, means that chromosome 8 has been duplicated, and there are too many copies of it within the cell.
- The letter t is used to indicate a translocation, in which parts of two chromosomes have traded places with each other. For example, if chromosomes 8 and 21 have swapped pieces, it would be written as t(8;21)
Certain chromosome changes in MDS cells can help predict the likely course of MDS. For example, a deletion of a part of chromosome 5, or del(5q), usually predicts a better outcome (as long as there is no more than one other chromosome change, and it isn’t a loss of part of chromosome 7). Changes in 3 or more chromosomes or the deletion of chromosome 7 tend to have a poorer outlook.
Fluorescent in situ hybridization (FISH)
Fluorescent in situ hybridization (FISH) test looks more closely at cell DNA using fluorescent dyes that only attach to specific gene or chromosome changes. An advantage of FISH is that it doesn’t require actively dividing cells, so it can usually provide results within a couple of days. FISH is very good for finding translocations – it can even find some that may be too small to be seen with usual cytogenetic testing.
Polymerase chain reaction (PCR)
Polymerase chain reaction (PCR) is a very sensitive DNA test that can also find some chromosome changes too small to be seen under a microscope, even if there are very few abnormal cells in a sample.
Other molecular and genetic tests
Other types of lab tests can also be done on the samples to look for specific gene or other changes in the MDS cells. This is sometimes referred to as biomarker testing.
For example, the MDS cells are tested for changes (mutations) in genes such as IDH1. People whose MDS cells have changes in this gene are more likely to be helped by treatment with certain targeted therapy drugs.
Myelodysplastic syndrome treatment
Myelodysplastic syndrome treatment is most often intended to slow the disease, ease symptoms and prevent complications. There’s no cure for myelodysplastic syndromes, but some medications can help slow the progression of the disease.
The treatment approach for myelodysplastic syndromes (MDS) depends on a number of factors, such as:
- The type of MDS you have
- The prognostic score (risk group) of your MDS
- Your age, overall health, and preferences
If you have no symptoms, treatment might not be needed right away. Instead, your doctor might recommend regular exams and lab tests to monitor your condition and to see if the disease progresses.
If treatment is needed, a bone marrow transplant also known as a stem cell transplant (SCT) is usually considered the only way to potentially cure MDS, so it may be the treatment of choice for younger, relatively healthy patients if a matched donor is available. Unfortunately, many people with MDS are older or in poor health and might not be good candidates for a stem cell transplant.
When stem cell transplant is not an option, MDS is very unlikely to be cured, but it can often still be treated. The main goal of treatment is to relieve symptoms and avoid complications and side effects.
If low blood counts are causing problems, supportive care treatments such as transfusions or blood cell growth factors may be helpful. Careful general medical care and measures to prevent and treat infections are also very important. Supportive care is important regardless of whether a person is getting other treatments for MDS.
If other treatment is needed, a chemotherapy drug such as azacitidine (Vidaza) or decitabine (Dacogen) is often the first choice, especially for patients with lower-risk forms of MDS. These drugs can often improve blood counts, and many patients need fewer transfusions and have a better quality of life, with less fatigue. These drugs can also help some people live longer. Another option for some people might be medicines to suppress the immune system, such as ATG and cyclosporine.
If a person has the del(5q) type of MDS (where the cells are missing part of chromosome 5), lenalidomide (Revlimid) is often used as the first treatment. If this drug doesn’t help, treatment with azacitidine or decitabine is often the next option.
For some patients with more advanced MDS, such as those whose prognostic scores are high risk or higher, or those whose MDS looks like it is becoming acute myeloid leukemia (AML), standard chemotherapy drugs might be an option. Unfortunately, this treatment can often be too toxic for patients who are elderly or who have many other medical problems. For young and healthy patients, though, the treatment is similar to treatment for AML.
If one type of treatment doesn’t work or if it stops working, another one might be tried. Many new medicines to treat MDS are also being studied in clinical trials. Because the best options to treat MDS aren’t clear, and because MDS often becomes hard to treat over time, taking part in a clinical trial might be a good option at some point. Ask your doctor about clinical trials for which you might be eligible.
Supportive therapy
Supportive therapies are treatments that help treat or prevent the symptoms or complications of myelodysplastic syndromes (MDS), as opposed to treating the MDS directly. Supportive therapy might be used alone or along with other treatments for MDS. The main purpose of this type of treatment is to improve the comfort and quality of life for someone diagnosed with cancer no matter what stage the cancer or the goal of treatment might be. You might also hear supportive care referred to as palliative care, symptom management, or comfort care.
For example, for many patients with MDS, one of the main goals of treatment is to prevent the problems caused by low blood cell counts.
Treating low red blood cell counts (anemia)
Low red blood cell counts (anemia) can cause severe fatigue and other symptoms. Patients with MDS and anemia that’s causing symptoms might benefit from getting injections of a manmade version of the growth factor erythropoietin, which can sometimes help the bone marrow make new red blood cells.
If this isn’t helpful, red blood cell transfusions might be needed. Blood transfusions with healthy blood cells from donors can be used to replace red blood cells and platelets in people with myelodysplastic syndromes. Blood transfusions can help control symptoms. Some people are concerned about a slight risk of infections (such as hepatitis or HIV) spread by blood transfusion, but this possibility is very unlikely, and the benefits of the transfused cells greatly outweigh this risk.
For people with some types of MDS who haven’t been helped by erythropoietin growth factors and who need regular blood transfusions, treatment with a drug called a red blood cell maturation agent, such as luspatercept, might be an option. This type of drug can sometimes help lower the number of transfusions a person needs.
Treating iron build up from blood transfusions
Blood transfusions can cause excess iron to build up in the body. The iron can build up over time in the liver, heart, and other organs, affecting how they function. This is usually seen only in people who receive many transfusions over a period of years. Patients at risk for iron overload are often advised to avoid taking iron supplements or multivitamins that contain iron.
Drugs called chelating agents, which bind with the iron so that the body can get rid of it, can be used in patients who develop iron overload from red blood cell transfusions (unless they have poor kidney function).
- Deferoxamine (Desferal) is usually given as an infusion under the skin, using a small, portable pump. This can be inconvenient because the infusion must be done slowly (over at least 8 hours) each day or on most days of the week.
- Deferasirox (Exjade, Jadenu) is a newer drug that is taken by mouth (as a tablet, dissolved in juice or water, or sprinkled on food) once a day.
Treating low platelet counts
MDS patients with low platelet counts might have problems with bleeding or bruising easily. The options for treating a shortage of platelets might include platelet transfusions or treatment with certain growth factor drugs. If bleeding is not helped by these treatments, another option might be treatment with a drug called an antifibrinolytic agent, such as aminocaproic acid (Amicar).
Treating low white blood cell counts
Patients with low white blood cell counts are more likely to get infections, and the infections are more likely to be serious. It’s important to avoid cuts and scrapes, and take care of them right away if they do happen. Patients should tell their doctors right away about any possible signs of infection, such as fever, signs of pneumonia (cough, shortness of breath), or urinary tract infection (burning when urinating).
Doctors typically treat known or suspected bacterial infections with antibiotics. For serious infections, a white blood cell growth factor may also be used. This drug can raise the white blood cell count to help fight the infection.
Medications
Treatment for myelodysplastic syndromes might include medications that:
- Increase the number of blood cells your body makes. Called growth factors, these medications are artificial versions of substances found naturally in your bone marrow. Growth factors that stimulate your bone marrow to make more red blood cells can help reduce your need for frequent blood transfusions. Growth factors that promote white blood cell production may reduce your risk of infection.
- Stimulate blood cells to mature. Medications that help stimulate the blood cells to mature can reduce the need for frequent blood transfusions in people who aren’t helped by growth factors. Some of these drugs may also reduce the risk that the disease may progress to leukemia.
- Suppress your immune system. Medications that suppress or control your immune system are used in certain myelodysplastic syndromes to reduce your need for red blood cell transfusions.
- Help people with a certain genetic abnormality. If your myelodysplastic syndrome is associated with a gene mutation called isolated del(5q), your doctor might recommend lenalidomide (Revlimid).
- Treat infections. If your condition causes you to have infections, you’ll receive treatments to control them.
Hematopoietic growth factors
Shortages of blood cells (red blood cells, white blood cells, or platelets) cause most of the symptoms in people with myelodysplastic syndromes (MDS). Hematopoietic growth factors can often help bring the blood counts closer to normal.
Hematopoietic growth factors are hormone-like substances that help bone marrow make new blood cells. These substances occur naturally in the body, but scientists have found ways to make large amounts of them in the lab. Patients can get these factors in larger doses than would be made by their own body.
Other medicines that raise blood cell counts in different ways might also be helpful for some people.
Patients usually receive growth factors and similar drugs through subcutaneous (under the skin) injections. Your health care team can give the injections, or you or your family members might be able to learn to give them at home.
Red blood cell growth factors
- Epoetin (Epogen or Procrit) is a manmade version of the growth factor erythropoietin (EPO), which promotes red blood cell production. It can help some patients avoid red blood cell transfusions. Giving some patients both epoetin and granulocyte colony stimulating factor (G-CSF) can improve their response to the epoetin.
- Darbepoetin alfa (Aranesp) is a long-acting form of epoetin. It works in the same way but was designed to be given less often.
- Luspatercept (Reblozyl) isn’t a manmade version of a natural growth factor, but it is another medicine that can help the body make more healthy red blood cells. Known as a red blood cell maturation agent, this drug affects TGF-β proteins in the bone marrow. TGF-β proteins normally help control how quickly new cells in the bone marrow mature into functioning red blood cells, so that there aren’t too many or too few of them in the body. By acting on specific TGF-β proteins, luspatercept helps the bone marrow make more healthy, full grown red blood cells.
White blood cell growth factors
- Granulocyte colony stimulating factor (G-CSF, filgrastim, or Neupogen) and granulocyte macrophage-colony stimulating factor (GM-CSF, sargramostim, or Leukine) can improve white blood cell production. These are not used routinely to prevent infections, but they can help some MDS patients whose main problem is a shortage of white blood cells and who have frequent infections.
- Pegfilgrastim (Neulasta) is a long-acting form of G-CSF. It works in the same way but can be given less often.
Platelet growth factors
- Drugs called thrombopoietin-receptor agonists, such as romiplostim (Nplate) and eltrombopag (Promacta) might help some people with MDS who have very low platelet levels, although this is still being studied.
- A drug called oprelvekin (interleukin-11, IL-11, or Neumega) can be used to raise platelet counts after chemotherapy and in some other diseases. But for most MDS patients, this drug has not been found to be very helpful.
Studies are under way to find the best way to predict which patients will be helped by growth factors and similar drugs, as well as the best way to combine growth factors with each other and with other treatments, such as chemotherapy.
Chemotherapy
Chemotherapy (chemo) is the use of drugs for treating a disease such as cancer. Some chemo drugs can be swallowed as pills, while others are injected by needle into a vein or muscle. These drugs are considered systemic treatment because they enter the bloodstream and reach most areas of the body. This type of treatment is useful for diseases such as MDS that are not only in one part of the body. The purpose of the chemo is to kill the abnormal stem cells in the bone marrow and allow normal ones to grow back.
Hypomethylating agents
These types of chemo drugs affect the way certain genes inside a cell are controlled. These drugs activate some genes that help cells mature. They also kill cells that are dividing rapidly. Examples of this type of drug include:
- Azacitidine (Vidaza)
- Decitabine (Dacogen)
In some MDS patients, using one of these drugs can improve blood counts (sometimes enough so that blood transfusions aren’t needed), improve quality of life, lower the chance of getting leukemia, and even help a person live longer.
Azacitidine can be injected under the skin or into a vein (IV), often for 7 days in a row, once a month.
Decitabine is often injected into a vein (IV) over 3 hours every 8 hours for 3 days. This is repeated every 6 weeks. Decitabine can also be given by IV over an hour, each day for 5 days in a row, and repeated every 4 weeks.
A newer form of this drug, known as Inqovi, combines decitabine with cedazuridine, which helps stop the decitabine from being broken down in the digestive system. This allows the drug to be taken by mouth as a tablet, typically once a day for 5 days in a row, which is repeated every 4 weeks.
Hypomethylating agents can have some of the same side effects as standard chemo drugs, but these side effects are usually milder.
A major side effect of hypomethylating agents is usually an early drop in blood cell counts, which tends to get better as the drug begins to work. Other side effects can include:
- Fever
- Nausea/vomiting
- Diarrhea or constipation
- Fatigue and weakness
Standard chemotherapy drugs
Standard chemo drugs are less useful for MDS than the hypomethylating agents, so they are not used often. But higher-risk MDS is more likely to progress to acute myeloid leukemia (AML), so some patients with these types of MDS may receive the same chemo treatment as AML patients.
The chemo drug most often used for MDS is cytarabine (ara-C). It can be given by itself at a low-dose, which can often help control the disease, but doesn’t often put it into remission.
Another option is to give the same, intense type of chemo that is used for younger patients with AML. This means giving cytarabine at a higher dose, along with other chemo drugs. This is more often used in younger, healthier patients with higher-risk forms of MDS (like MDS with excess blasts). Some of the chemo drugs that can be combined with cytarabine are:
- Idarubicin
- Daunorubicin
Other chemo drugs might be used as well.
Patients who get the higher-dose treatment are more likely to have their MDS go into remission, but they can also have more severe, even life-threatening side effects, so this treatment is typically given in the hospital. Still, this treatment may be an option for some patients with advanced MDS.
Chemo drugs can cause many side effects. These depend on the type and dose of the drugs given and how long they are taken. Common side effects include:
- Hair loss
- Mouth sores
- Loss of appetite
- Nausea and vomiting
- Low blood counts
MDS patients already have low blood counts, which often become even worse for a time before they get better.
- Low white blood cell counts lead to an increased risk of serious infections.
- Low platelet counts can lead to problems with easy bruising and serious bleeding, including bleeding into the brain or the intestine.
- Low red blood cell counts (anemia) can lead to fatigue and shortness of breath. In people with heart problems, severe anemia can lead to a heart attack.
If a patient’s blood cell counts become too low, they may need supportive therapy (including transfusions or growth factors) to help prevent or treat serious side effects.
Most side effects from chemo will go away after treatment is finished. Your health care team can often suggest ways to lessen side effects. For example, drugs can be given to help prevent or reduce nausea and vomiting.
Chemo drugs can also affect other organs. For example:
- Idarubicin and daunorubicin can damage the heart, so they are often not given to patients who already have heart problems.
- Cytarabine can affect the brain and cause balance problems, sleepiness, and confusion. This is more common with higher doses.
If serious side effects occur, the chemo treatments may have to be reduced or stopped, at least temporarily. It’s important to carefully monitor and adjust drug doses, because some of these side effects can be permanent.
Immunomodulating drugs
Lenalidomide (Revlimid) belongs to a class of drugs known as immunomodulating drugs (IMiDs). It seems to work well in low-grade MDS, often eliminating the need for blood transfusions, at least for a time. The drug seems to work best in people whose MDS cells are missing a part of chromosome 5 (MDS-del(5q)). But it can also help some MDS patients that do not have this abnormal chromosome.
Lenalidomide (Revlimid) side effects can include:
- Lowered blood counts (most often the white cell count and platelet count)
- Diarrhea or constipation
- Fatigue and weakness
Lenalidomide (Revlimid) can also increase the risk of serious blood clots that start in the veins in the legs called a deep vein thrombosis or DVT. Sometimes, part of a DVT (deep vein thrombosis) can break off and travel to the lungs called a pulmonary embolus (PE), where it can cause breathing problems or even death.
Lenalidomide (Revlimid) might also cause serious birth defects if given to pregnant women. Because of this, it’s only available through a special program by the drug company.
Immune system suppression
Drugs that suppress the immune system can help some patients with lower-risk MDS. These drugs are most helpful for people with low numbers of cells in the bone marrow called hypocellular bone marrow.
Anti-thymocyte globulin (ATG) is an antibody against a type of white blood cell called the T-lymphocyte, which helps control immune reactions. For some patients with MDS, T-lymphocytes interfere with normal blood cell production, so ATG can be helpful. ATG is given as an infusion through a vein. It must be given in the hospital because it can sometimes cause severe allergic reactions leading to low blood pressure and problems breathing.
Cyclosporine is another drug that can suppress the immune system. It can be used along with ATG to help some patients with MDS. Side effects of cyclosporine can include loss of appetite and kidney damage.
Targeted therapy
In some people with MDS, the cancer cells have a change (mutation) in the IDH1 gene, which normally helps cells make the IDH1 protein. Mutations in this gene can lead to an abnormal IDH1 protein, which can stop MDS cells from maturing the way they normally would.
Ivosidenib (Tibsovo) is an IDH1 inhibitor. It blocks the abnormal IDH1 protein, which seems to help the cancer cells mature into more normal cells. This drug can be used in people with advanced, previously treated MDS, if the cancer cells are found to have an IDH1 mutation. Your doctor can test your cancer cells to see if they have an IDH1 mutation.
This drug is taken by mouth, once a day.
Common side effects of ivosidenib can include fatigue, nausea, vomiting, abdominal (belly) pain or swelling, diarrhea, loss of appetite, cough, low red blood cell counts (anemia), rash, and changes in lab tests showing the drug is affecting the liver.
Less common but more serious side effects can include changes in heart rhythm, pneumonia, and jaundice (yellowing of the eyes and skin).
Bone marrow transplant
A bone marrow transplant also known as a stem cell transplant (SCT), is the only treatment option that offers the potential of a cure for myelodysplastic syndromes. But this treatment carries a high risk of serious complications and it’s generally reserved for people who are healthy enough to endure it.
During a bone marrow transplant, high doses of chemotherapy drugs and/or total body irradiation are used to clear out the defective blood cells from your bone marrow. Then the abnormal bone marrow stem cells are replaced with healthy, donated cells (allogeneic transplant).
In some situations, less intense chemotherapy drugs can be used to reduce the risks of bone marrow transplant for older adults and those who might not otherwise be considered for this treatment.
There are 2 main types of stem cell transplant:
- For an allogeneic stem cell transplant, after the bone marrow is destroyed, the patient receives blood-forming stem cells from another person — the donor. This is the type of transplant typically used for MDS. The results of this treatment tend to be best when the donor’s cell type (also known as the HLA type) is closely matched to the patient’s cell type and the donor is closely related to the patient, such as a brother or sister. Less often, the donor is matched to the patient, but is not related.
- In an autologous stem cell transplant, the patient gets back their own stem cells (which were removed before treatment). This type of transplant is not typically used for patients with MDS because the patient’s bone marrow contains abnormal stem cells.
Allogeneic stem cell transplants can have serious, even life-threatening, side effects, so they are typically done in younger patients who are in relatively good health. Patients in their 60s or even 70s have been transplanted successfully, but in older patients the stem cell transplant is generally done using less intensive (reduced intensity) chemotherapy and/or radiation. The lower doses may not kill all the bone marrow cells, but they are just enough to allow the donor cells to take hold and grow in the bone marrow. The lower doses also cause fewer side effects, which makes this type of transplant easier for older patients to tolerate. Still, some serious side effects are still possible.
Lifestyle and home remedies
Because people with certain myelodysplastic syndromes have low white blood cell counts, they’re subject to recurrent, and often serious, infections.
To reduce your risk of infections:
- Wash your hands. Wash hands frequently and thoroughly with warm, soapy water, especially before eating or preparing food. Carry an alcohol-based hand sanitizer for times when water isn’t available.
- Take care with food. Thoroughly cook all meat and fish. Avoid fruits and vegetables you can’t peel, especially lettuce, and wash all produce you do use before peeling it. To increase safety, you might want to avoid all raw foods.
- Avoid people who are ill. Try to avoid close contact with anyone who is sick, including family members and co-workers.
Myelodysplastic syndrome prognosis
Myelodysplastic syndrome prognosis is directly related to the number of bone marrow blast cells, to certain cytogenetic abnormalities, and to the amount of peripheral blood cytopenias 3. By convention, MDS are reclassified as acute myeloid leukemia (AML) with myelodysplastic features when blood or bone marrow blasts reach or exceed 20%. Many patients succumb to complications of cytopenias before progression to this stage.
Myelodysplastic syndromes (MDS) are a group of blood cancers of the bone marrow. Myelodysplastic syndrome prognosis (outlook) isn’t based on the size of a tumor or whether the cancer has spread. Because of this, doctors use other factors to predict prognosis (outlook) and decide when to treat. Some of these factors have been combined to develop scoring systems.
Revised International Prognostic Scoring System (IPSS-R)
The revised International Prognostic Scoring Sytem (IPSS-R) is an important standard for ssessing prognosis of primary untreated adult patients with myelodysplastic syndromes (MDS). The revised International Prognostic Scoring System (IPSS-R) is based on 5 factors 16:
- The percentage of blasts (very early forms of blood cells) in the bone marrow
- The type and number of chromosome abnormalities in the cells
- The level of red blood cells (measured as hemoglobin) in the patient’s blood
- The level of platelets in the patient’s blood
- The level of neutrophils (a type of white blood cell) in the patient’s blood
Each factor is given a score, with the lowest scores having the best prognosis (outlook). Then the scores for the factors are added up to put people with MDS into 5 risk groups:
- Very low risk
- Low risk
- Intermediate risk
- High risk
- Very high risk
These risk groups can be used to help predict a person’s outlook. This can be helpful when trying to determine the best treatment options.
This system has some important limitations. For example, it was developed before many of the current treatments for MDS were available, so it only took into account people who were not treated for their MDS. It also did not include people who have MDS as a result of getting chemotherapy (secondary MDS). But this system can still be helpful and is still widely used.
WHO Prognostic Scoring System (WPSS)
The World Health Organization (WHO) scoring system (WPSS) is based on 3 factors 17, 18, 19, 20:
- The type of MDS based on the WHO classification (For example, certain types of MDS-SLD and MDS-del(5q) tend to have the best outlook, whereas MDS-EB tends to have the worst.)
- Chromosome abnormalities (grouped as good, intermediate, or poor)
- Whether or not the patient needs regular blood transfusions
Each factor is given a score, with the lowest scores having the best outlook. Then the scores are added up to put people with MDS into 5 risk groups:
- Very low risk
- Low risk
- Intermediate risk
- High risk
- Very high risk
These risk groups can be used to help predict a person’s outlook, as well as how likely the MDS is to transform into acute myeloid leukemia (AML). This can be helpful when trying to determine the best treatment options. But as with the IPSS-R, this system has some important limitations. For example, it does not include people who have MDS as a result of getting chemotherapy (known as secondary MDS).
Both the International Prognostic Scoring System (IPSS-R) and the WHO Prognostic Scoring System (WPSS) can be complex, and different doctors might use different systems. If you have MDS, talk to your doctor about which system they use, which risk group you are in, and what it might mean for your treatment and outlook.
Other prognostic factors
Along with the factors used in these scoring systems, doctors have found other factors that can also help predict a person’s prognosis (outlook). These include:
- A person’s age
- A person’s performance status (how well they’re able to do normal daily activities)
- The severity of low blood cell counts
- The results of certain blood tests, such as the serum ferritin level
- Certain gene or chromosome changes that are not accounted for in the scoring systems
Myelodysplastic syndrome life expectancy
Survival statistics are a way for doctors and patients to get a general idea of the outlook (prognosis) for people with a certain type of cancer. Survival statistics can’t tell you how long you will live, but they may help give you a better understanding about how likely it is that your treatment will be successful. Some people will want to know the survival statistics for their cancer, and some people won’t. If you don’t want to know, you don’t have to.
There are some limitations to remember:
- The numbers below are based on patients diagnosed with a myelodysplastic syndrome (MDS) some time ago. Improvements in treatment since these numbers were gathered may result in a better outlook for people now being diagnosed with MDS.
- These numbers are based on prognostic scores that take into account certain factors, such as the type of MDS, the results of certain blood tests, and whether the abnormal cells have certain chromosome changes. But other factors might also affect a person’s outlook, such as the patient’s age and health, and how well the disease responds to treatment.
- These survival statistics are only estimates – they can’t predict what will happen to any individual person. Many other factors can also affect a person’s outlook. We understand that these statistics can be confusing and may lead you to have more questions. Talk to your doctor to better understand your specific situation.
Your doctor can tell you how the numbers below apply to you.
The following survival statistics are based on the revised International Prognostic Scoring System (IPSS-R) risk groups. It’s important to note that this system is based largely on people who were diagnosed many years ago and who did not get treatments such as chemotherapy for their MDS.
Table 2. Myelodysplastic syndrome Revised International Prognostic Scoring System (IPSS-R) risk group life expectancy
| IPSS-R risk group | Median survival |
|---|---|
| Very low | 8.8 years |
| Low | 5.3 years |
| Intermediate | 3 years |
| High | 1.6 years |
| Very high | 0.8 years |
Table 3. Myelodysplastic syndrome WHO Prognostic Scoring System (WPSS) risk group life expectancy
| WPSS Risk Group | Median Survival | Risk of AML (within 5 years) |
|---|---|---|
| Very low | 11.8 years | 3% |
| Low | 5.5 years | 14% |
| Intermediate | 4 years | 33% |
| High | 2.2 years | 54% |
| Very high | 9 months | 84% |
Footnote: The WHO Prognostic Scoring System (WPSS) risk groups can also be used to predict outcome – both median survival and the chance that the MDS will transform into acute myeloid leukemia (AML) within 5 years. These statistics were published in 2007 based on patients diagnosed between 1982 and 2004.
[Source 21 ]- Myelodysplastic syndromes (MDS). https://www.leukaemia.org.au/blood-cancer/myelodysplastic-syndromes[↩]
- What Are Myelodysplastic Syndromes? https://www.cancer.org/cancer/types/myelodysplastic-syndrome/about/what-is-mds.html[↩]
- PDQ Adult Treatment Editorial Board. Myelodysplastic Syndromes Treatment (PDQ®): Health Professional Version. 2022 Sep 30. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK66015[↩][↩][↩]
- PDQ Adult Treatment Editorial Board. Myelodysplastic Syndromes Treatment (PDQ®): Patient Version. 2023 Mar 31. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65798[↩]
- Heaney ML, Golde DW. Myelodysplasia. N Engl J Med. 1999 May 27;340(21):1649-60. doi: 10.1056/NEJM199905273402107[↩][↩]
- Key Statistics for Myelodysplastic Syndromes. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/about/key-statistics.html[↩][↩][↩]
- Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer. 2007 Apr 15;109(8):1536-42. doi: 10.1002/cncr.22570[↩]
- Tuncer MA, Pagliuca A, Hicsonmez G, Yetgin S, Ozsoylu S, Mufti GJ. Primary myelodysplastic syndrome in children: the clinical experience in 33 cases. Br J Haematol. 1992 Oct;82(2):347-53. doi: 10.1111/j.1365-2141.1992.tb06428.x[↩]
- Sekeres MA, Schoonen WM, Kantarjian H, List A, Fryzek J, Paquette R, Maciejewski JP. Characteristics of US patients with myelodysplastic syndromes: results of six cross-sectional physician surveys. J Natl Cancer Inst. 2008 Nov 5;100(21):1542-51. doi: 10.1093/jnci/djn349[↩]
- Haematopoiesis. https://www.learnhaem.com/courses/anaemia/lessons/normal-haematopoiesis/topic/haematopoiesis[↩]
- Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. Blood. 2016 Jul 21;128(3):462-463. https://doi.org/10.1182/blood-2016-06-721662[↩][↩]
- Types of Myelodysplastic Syndromes. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/about/mds-types.html[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- What Causes Myelodysplastic Syndromes? https://www.cancer.org/cancer/types/myelodysplastic-syndrome/causes-risks-prevention/what-causes.html[↩]
- Du Y, Fryzek J, Sekeres MA, Taioli E. Smoking and alcohol intake as risk factors for myelodysplastic syndromes (MDS). Leuk Res. 2010 Jan;34(1):1-5. doi: 10.1016/j.leukres.2009.08.006[↩]
- Strom SS, Gu Y, Gruschkus SK, Pierce SA, Estey EH. Risk factors of myelodysplastic syndromes: a case-control study. Leukemia. 2005 Nov;19(11):1912-8. doi: 10.1038/sj.leu.2403945[↩]
- Greenberg PL, Tuechler H, Schanz J, et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood. 2012 Sep 20;120(12):2454-65. doi: 10.1182/blood-2012-03-420489[↩]
- Della Porta MG, Tuechler H, Malcovati L, et al. Validation of WHO classification-based Prognostic Scoring System (WPSS) for myelodysplastic syndromes and comparison with the revised International Prognostic Scoring System (IPSS-R). A study of the International Working Group for Prognosis in Myelodysplasia (IWG-PM). Leukemia. 2015 Jul;29(7):1502-13. doi: 10.1038/leu.2015.55[↩]
- Garcia-Manero G, Shan J, Faderl S, Cortes J, Ravandi F, Borthakur G, Wierda WG, Pierce S, Estey E, Liu J, Huang X, Kantarjian H. A prognostic score for patients with lower risk myelodysplastic syndrome. Leukemia. 2008 Mar;22(3):538-43. doi: 10.1038/sj.leu.2405070[↩]
- Kantarjian H, O’Brien S, Ravandi F, Cortes J, Shan J, Bennett JM, List A, Fenaux P, Sanz G, Issa JP, Freireich EJ, Garcia-Manero G. Proposal for a new risk model in myelodysplastic syndrome that accounts for events not considered in the original International Prognostic Scoring System. Cancer. 2008 Sep 15;113(6):1351-61. doi: 10.1002/cncr.23697[↩]
- Malcovati L, Della Porta MG, Strupp C, Ambaglio I, Kuendgen A, Nachtkamp K, Travaglino E, Invernizzi R, Pascutto C, Lazzarino M, Germing U, Cazzola M. Impact of the degree of anemia on the outcome of patients with myelodysplastic syndrome and its integration into the WHO classification-based Prognostic Scoring System (WPSS). Haematologica. 2011 Oct;96(10):1433-40. doi: 10.3324/haematol.2011.044602[↩]
- Survival Statistics for Myelodysplastic Syndromes. https://www.cancer.org/cancer/types/myelodysplastic-syndrome/detection-diagnosis-staging/survival.html[↩][↩]

{kind=link}