Contents
- Transitional cell carcinoma
- Transitional cell carcinoma causes
- Transitional cell carcinoma prevention
- Transitional cell carcinoma symptoms
- Transitional cell carcinoma diagnosis
- Cellular classification of transitional cell cancer of the renal pelvis and ureter
- Transitional cell carcinoma staging of the renal pelvis and ureter
- Transitional cell carcinoma treatment
- Stage 4 transitional cell carcinoma life expectancy
- Transitional cell carcinoma survival rate
- Transitional cell carcinoma prognosis
Transitional cell carcinoma
Transitional cell carcinoma (TCC) also called urothelial carcinoma, is cancer that forms in urothelial cells that line the inside of the bladder, the lower part of the kidneys (the renal pelvises), the ureters, and the proximal urethra. Primary transitional cell carcinoma or urethral carcinoma is considered a rare cancer, accounting for < 1% of all genitourinary cancers 1. According to the Surveillance, Epidemiology and End Results (SEER) database 2004–2016 2, the incidence of primary transitional cell carcinoma (urethral carcinoma) peaked in the > 75 years age group (7.6/million). The age-standardized rate was 4.3/million in men and 1.5/million in women and was almost negligible in those aged < 55 years (0.2/million) 2. However, transitional cell carcinoma or urothelial carcinoma is the most common type of bladder cancer accounting for around 95% of bladder cancers and is the 4th most common cancer among men and the tenth most common in women, in the United States 3. In addition, higher incidence of bladder cancer has been found in different studies with male to female incidence ratios varies between 2:1 to 3:1 4, 5, 6. Transitional cell carcinoma is relatively common in the elderly, as the median age of diagnosis is 72 years old for men and 75 years old for women 7. In addition, transitional cell carcinoma showed to express significant disparities among races 8. Although the incidence of transitional cell carcinomas is 2 times higher in whites in comparison to African Americans 8, 9, African Americans have a worse prognosis and higher tumor stages at presentation 8. In fact, the mortality (death) rates are significantly higher in African Americans, older patients, and females 10, 11, 12.
Transitional cell carcinoma of the renal pelvis, accounts for only 7% of all kidney tumors, and transitional cell cancer of the ureter, accounts for only 1 of every 25 upper urinary tract tumors, are curable in more than 90% of patients if they are superficial and confined to the renal pelvis or ureter 13. Patients with deeply invasive transitional cell carcinomas that are confined to the renal pelvis or ureter have a 10% to 15% likelihood of cure. Patients with transitional cell carcinoma with penetration through the urothelial wall or with distant metastases usually cannot be cured with currently available forms of treatment 13.
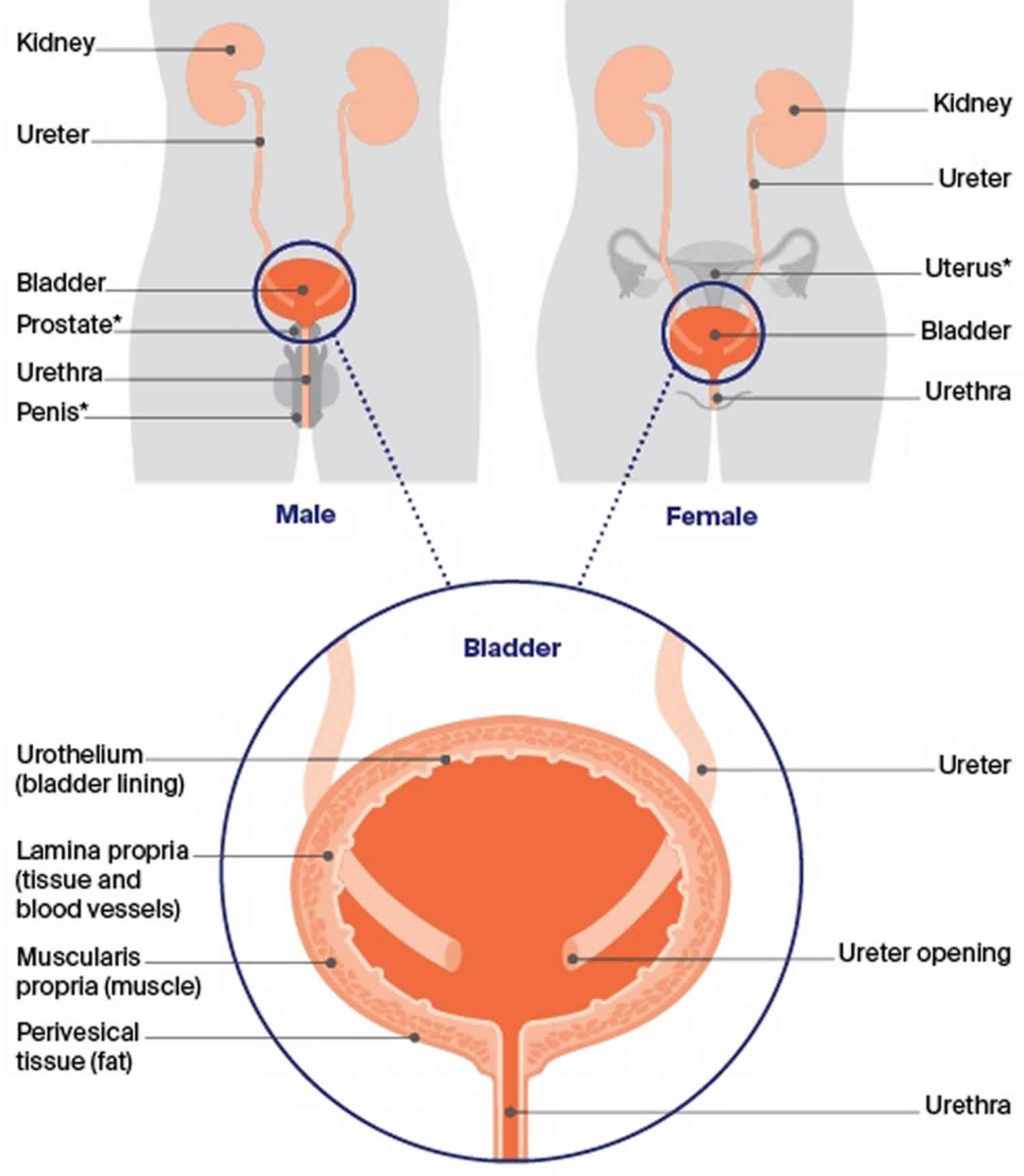
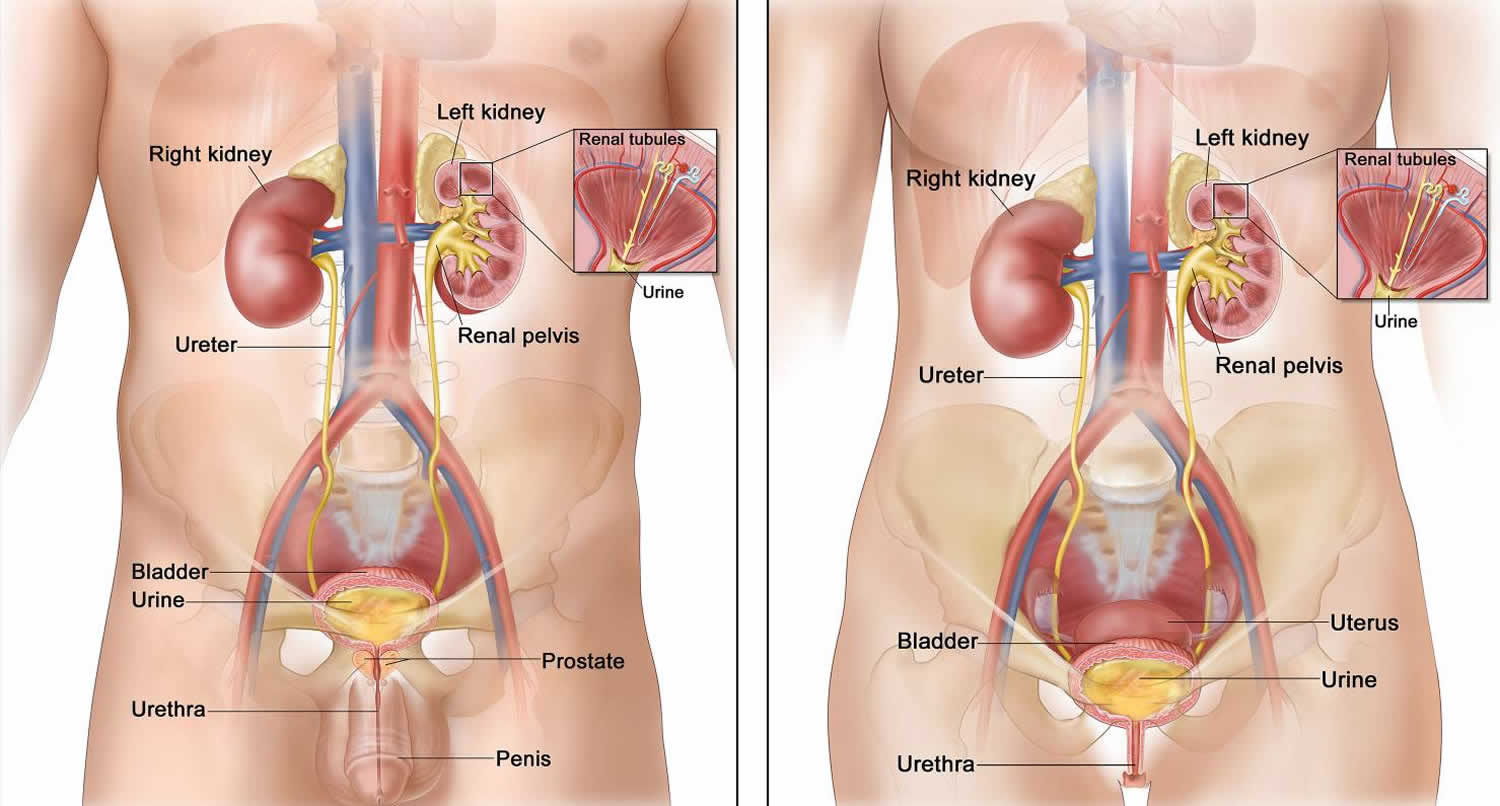
The renal pelvis is the top part of the ureter. The ureter is a long tube that connects the kidney to the bladder. There are two kidneys, one on each side of the backbone, above the waist. The kidneys of an adult are about 5 inches long and 3 inches wide and are shaped like a kidney bean. Tiny tubules in the kidneys filter and clean the blood. They take out waste products and make urine. The urine collects in the middle of each kidney in the renal pelvis. Urine passes from the renal pelvis through the ureter into the bladder. The bladder holds the urine until it passes through the urethra and leaves the body.
The renal pelvis and ureters are lined with transitional cells. These cells can change shape and stretch without breaking apart. Transitional cell cancer starts in these cells. Transitional cell cancer can form in the renal pelvis, the ureter, or both.
Several environmental factors have been associated with transitional cell carcinoma. Cigarette smoking is the most well-established risk factor, being responsible for about 55% of all transitional cell carcinoma cases in the US 14. Aromatic amines are the primary carcinogens of bladder cancer in smoking population 15. Occupational exposures to various carcinogens such as polycyclic aromatic hydrocarbons and chlorinated hydrocarbons are correlated with 20% of transitional cell carcinoma cases, especially in the industrial areas processing paint and dye 16, 17, 18, 19. High levels of arsenic in the drinking water have also been associated with an increased risk of transitional cell carcinoma progression 20.
Furthermore, obesity has been shown to be a major risk factor contributing to transitional cell carcinoma; as shown by a meta-analysis on 15 cohort studies that include more than 38,000 transitional cell carcinoma patients, which investigated the possible correlation between cancer and obesity 21. Sun et al. 21 showed a 4.2% increase in the incidence of bladder cancer for each 5 kg/m³ increase in weight among patients. In fact, Bhaskaran et al. 22 have already shown that obesity is related to 20% of the new cases of transitional cell carcinoma in Britain. These findings are consistent with another study that emphasized the possible role of obesity in increasing the risk of bladder cancer by 28% 23. Nevertheless, studies showed that socioeconomic differences in income and health care services might also be associated with an increased incidence and mortality rates of transitional cell carcinoma 24, 7.
Several genetic factors contribute to transitional cell carcinoma’s development; glutathione S-transferases, which encode important enzymes in the process of carcinogens detoxification, showed to play a major role in bladder cancer occurrence 25. In a meta-analysis that included 63 studies, they studied the possible association between GSTM1 or GSTT1 polymorphism and bladder cancer susceptibility 26. They reported a strong correlation between single gene deletion ‘GSTM1 or GSTT1’ or double deletions of GSTM1/GSTT1 with a higher risk of bladder cancer, especially among Caucasians and Asians 26. Moreover, evidence showed that higher risk of bladder cancer was found in patients with lower acetylation activity due to N-acetyltransferase 2 (NAT2) gene mutation 27. On the other hand, multiple somatic mutations were detected in bladder cancer patients; as Gui et al. 28 confirmed the presence of several mutated genes in transitional cell carcinoma patients that vary according to the grade of disease. In another study that performed a full genomic analysis on 99 patients with transitional cell carcinoma, researchers identified several altered genes and mutations that contribute to transitional cell carcinoma 29. These findings highlight the potential role of genetic variations in the classification, diagnosis and the new approach treatment of bladder cancer.
The main symptom of bladder cancer is blood in your urine. This is the same for both men and women. Bladder cancer can also cause problems with passing urine. If you notice that you have discolored urine and are concerned it may contain blood, make an appointment with your doctor to get it checked. Also make an appointment with your doctor if you have other signs or symptoms that worry you.
For treatment purposes, bladder cancers are often grouped based on if they have invaded into the main muscle layer of the bladder wall (see the image above). A bladder cancer that has not grown into the muscle layer can be described as superficial or non-muscle invasive bladder cancer (NMIBC). These terms include both non-invasive (stage 0) tumors as well as some early (stage I) invasive tumors.
Bladder cancers are also divided into 2 subtypes, papillary and flat, based on how they grow (see Figure 1).
- Papillary carcinomas grow in slender, finger-like projections from the inner surface of the bladder toward the hollow center. Papillary tumors often grow toward the center of the bladder without growing into the deeper bladder layers. These tumors are called non-invasive papillary cancers. Very low-grade (slow growing), non-invasive papillary cancer is sometimes called papillary urothelial neoplasm of low-malignant potential and it tends to have a very good outcome.
- Flat carcinomas do not grow toward the hollow part of the bladder at all. If a flat tumor is only in the inner layer of bladder cells, it’s known as a non-invasive flat carcinoma or a flat carcinoma in situ (CIS).
If either a papillary or flat tumor grows into deeper layers of the bladder, it’s called an invasive urothelial cell carcinoma or invasive transitional cell carcinoma.
Transitional cell carcinoma treatment involves total excision of the ureter with a bladder cuff, renal pelvis, and kidney is recommended in an attempt to provide the greatest likelihood of cure 30.
Figure 1. Transitional cell carcinoma bladder
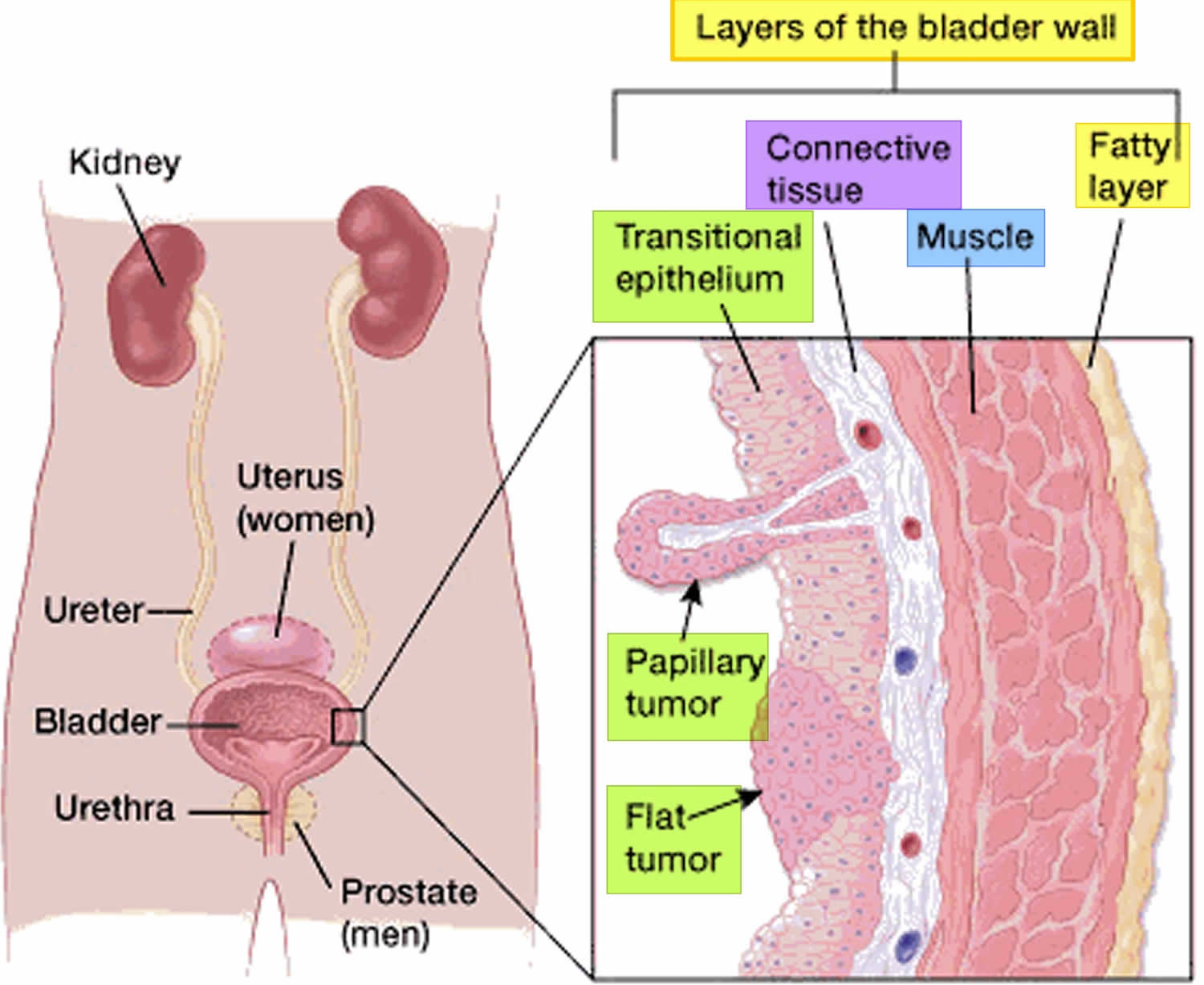
Figure 2. Anatomy of the male urinary system (left panel) and female urinary system (right panel) showing the kidneys, ureters, bladder, and urethra. Urine is made in the renal tubules and collects in the renal pelvis of each kidney. The urine flows from the kidneys through the ureters to the bladder. The urine is stored in the bladder until it leaves the body through the urethra.
Transitional cell carcinoma causes
Researchers do not know exactly what causes most transitional cell carcinomas. But they have found some risk factors and are starting to understand how they cause cells in the bladder, kidneys and ureters to become cancer.
Under conditions of chronic inflammation, such as infection of the bladder with the Schistosoma haematobium parasite, squamous metaplasia may occur in the bladder; the incidence of squamous cell carcinomas of the bladder is higher under conditions of chronic inflammation than is otherwise seen. In addition to transitional cell carcinomas and squamous cell carcinomas, adenocarcinomas, small cell carcinomas, and sarcomas can form in the bladder. In the United States, transitional cell carcinomas represent most (> 90%) bladder cancers. However, a significant number of transitional cell carcinomas have areas of squamous or other differentiation.
Several environmental factors have been associated with transitional cell carcinoma. Cigarette smoking is the most well-established risk factor, being responsible for about 55% of all transitional cell carcinoma cases in the US 14. Aromatic amines are the primary carcinogens of bladder cancer in smoking population 15. Occupational exposures to various carcinogens such as polycyclic aromatic hydrocarbons and chlorinated hydrocarbons are correlated with 20% of transitional cell carcinoma cases, especially in the industrial areas processing paint and dye 16, 17, 18, 19. High levels of arsenic in the drinking water have also been associated with an increased risk of transitional cell carcinoma progression 20.
Furthermore, obesity has been shown to be a major risk factor contributing to transitional cell carcinoma; as shown by a meta-analysis on 15 cohort studies that include more than 38,000 transitional cell carcinoma patients, which investigated the possible correlation between cancer and obesity 21. Sun et al. 21 showed a 4.2% increase in the incidence of bladder cancer for each 5 kg/m³ increase in weight among patients. In fact, Bhaskaran et al. 22 have already shown that obesity is related to 20% of the new cases of transitional cell carcinoma in Britain. These findings are consistent with another study that emphasized the possible role of obesity in increasing the risk of bladder cancer by 28% 23. Nevertheless, studies showed that socioeconomic differences in income and health care services might also be associated with an increased incidence and mortality rates of transitional cell carcinoma 24, 7.
Several genetic factors contribute to transitional cell carcinoma’s development; glutathione S-transferases, which encode important enzymes in the process of carcinogens detoxification, showed to play a major role in bladder cancer occurrence 25. In a meta-analysis that included 63 studies, they studied the possible association between GSTM1 or GSTT1 polymorphism and bladder cancer susceptibility 26. They reported a strong correlation between single gene deletion ‘GSTM1 or GSTT1’ or double deletions of GSTM1/GSTT1 with a higher risk of bladder cancer, especially among Caucasians and Asians 26. Moreover, evidence showed that higher risk of bladder cancer was found in patients with lower acetylation activity due to N-acetyltransferase 2 (NAT2) gene mutation 27. On the other hand, multiple somatic mutations were detected in bladder cancer patients; as Gui et al. 28 confirmed the presence of several mutated genes in transitional cell carcinoma patients that vary according to the grade of disease. In another study that performed a full genomic analysis on 99 patients with transitional cell carcinoma, researchers identified several altered genes and mutations that contribute to transitional cell carcinoma 29. These findings highlight the potential role of genetic variations in the classification, diagnosis and the new approach treatment of bladder cancer.
Risk factors for developing transitional cell carcinoma
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk. Risk factors for transitional cell carcinoma (urethral carcinoma) of the renal pelvis and ureter include the following:
- Having a personal history of bladder cancer. If you’ve had bladder cancer, you’re more likely to get it again.
- Family history of cancer. If one of your blood relatives, a parent, sibling or child, has a history of bladder cancer, you may have an increased risk of bladder cancer, although it’s rare for bladder cancer to run in families. A family history of Lynch syndrome also known as hereditary nonpolyposis colorectal cancer (HNPCC), can increase your risk of cancer in the urinary system, as well as in the colon, uterus, ovaries and other organs.
- Smoking cigarettes. Smoking cigarettes, cigars or pipes may increase your risk of bladder cancer by causing harmful chemicals to accumulate in the urine. When you smoke, your body processes the chemicals in the smoke and excretes some of them in your urine. These harmful chemicals may damage the lining of your bladder, which can increase your risk of cancer.
- Taking a lot of certain pain medicines, such as phenacetin.
- Being exposed to certain dyes and chemicals used in making leather goods, textiles, plastics, and rubber. Your kidneys play a key role in filtering harmful chemicals from your bloodstream and moving them into your bladder. Because of this, it’s thought that being around certain chemicals may increase the risk of bladder cancer. Chemicals linked to bladder cancer risk include arsenic and chemicals used in the manufacture of dyes, rubber, leather, textiles and paint products.
- Increasing age. Bladder cancer risk increases as you age. Though it can occur at any age, most people diagnosed with bladder cancer are older than 55.
- Being male. Men are more likely to develop bladder cancer than women are.
- Previous cancer treatment. Treatment with the anti-cancer drug cyclophosphamide increases the risk of bladder cancer. People who received radiation treatments aimed at the pelvis for a previous cancer have a higher risk of developing bladder cancer.
- Urethral strictures 31, 32
- Chronic bladder inflammation. Chronic or repeated urinary infections or inflammations (cystitis), such as might happen with long-term use of a urinary catheter, may increase the risk of a squamous cell bladder cancer 33, 34, 35. In some areas of the world, squamous cell carcinoma is linked to chronic bladder inflammation caused by the parasitic infection known as schistosomiasis.
In female transitional cell carcinoma (urethral carcinoma), urethral diverticula 36, 37, 38 and recurrent urinary tract infections 39 have been associated with primary transitional cell carcinoma (urethral carcinoma).
Transitional cell carcinoma prevention
Although there’s no guaranteed way to prevent bladder cancer, you can take steps to help reduce your risk. For instance:
- Don’t smoke. If you don’t smoke, don’t start. If you smoke, talk to your doctor about a plan to help you stop. Support groups, medications and other methods may help you quit.
- Take caution around chemicals. If you work with chemicals, follow all safety instructions to avoid exposure.
- Eat a variety of fruits and vegetables. Choose a diet rich in a variety of colorful fruits and vegetables. The antioxidants in fruits and vegetables may help reduce your risk of cancer.
Transitional cell carcinoma symptoms
Signs and symptoms of transitional cell cancer of the renal pelvis and ureter include blood in the urine and back pain.
These and other signs and symptoms may be caused by transitional cell cancer of the renal pelvis and ureter or by other conditions. There may be no signs or symptoms in the early stages. Signs and symptoms may appear as the tumor grows. Check with your doctor if you have any of the following:
- Blood in the urine.
- A pain in the back that doesn’t go away.
- Extreme tiredness.
- Weight loss with no known reason.
- Painful or frequent urination.
Other symptoms of bladder cancer can include:
- passing urine very often (frequency)
- passing urine very suddenly (urgency)
- pain or a burning sensation when passing urine
Transitional cell carcinoma diagnosis
Tests that examine the abdomen and kidneys are used to detect (find) and diagnose transitional cell cancer of the renal pelvis and ureter.
The following tests and procedures may be used to diagnose transitional cell carcinoma:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Urinalysis: A test to check the color of urine and its contents, such as sugar, protein, blood, and bacteria.
- Ureteroscopy: A procedure to look inside the ureter and renal pelvis to check for abnormal areas. A ureteroscope is a thin, tube-like instrument with a light and a lens for viewing. The ureteroscope is inserted through the urethra into the bladder, ureter, and renal pelvis. A tool may be inserted through the ureteroscope to take tissue samples to be checked under a microscope for signs of disease. Ureteroscopy can be done in a doctor’s office or in the hospital.
- Urine cytology: A laboratory test in which a sample of urine is checked under a microscope for abnormal cells. Cancer in the kidney, bladder, or ureter may shed cancer cells into the urine.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. This may be done during a ureteroscopy or surgery. This procedure is sometimes called transurethral resection of bladder tumor (TURBT). TURBT can also be used to treat bladder cancer.
- CT scan (CAT scan) urogram: A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Retrograde pyelogram: Retrograde pyelogram is an X-ray exam used to get a detailed look at the upper urinary tract. During this test, your doctor threads a thin tube (catheter) through your urethra and into your bladder to inject contrast dye into your ureters. The dye then flows into your kidneys while X-ray images are captured.
- Ultrasound: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. An ultrasound of the abdomen may be done to help diagnose cancer of the renal pelvis and ureter.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the pelvis. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Cellular classification of transitional cell cancer of the renal pelvis and ureter
Most bladder cancers start in the innermost lining of the bladder, which is called the urothelium or transitional epithelium. As the cancer grows into or through the deeper layers in the bladder wall, it has a higher stage, becomes more advanced, and can be harder to treat.
Over time, the cancer might grow outside the bladder and into nearby structures. It might spread to nearby lymph nodes, or to other parts of the body. When bladder cancer spreads, it tends to go to the lymph nodes, the bones, the lungs, or the liver.
Grade of transitional cell cancer of the upper tract has generally been found to correlate with stage. Superficial tumors are generally grade 1 or 2, whereas the majority of infiltrative tumors are grades 3 and 4. Prognosis is worse for patients with high-grade (grades 3 and 4) tumors than for those with low-grade (grades 1 and 2) tumors.
Transitional cell carcinoma of the bladder grade
Transitional cell carcinoma of the bladder are further classified based on how the cancer cells appear when viewed through a microscope. This is known as the grade, and your doctor may describe bladder cancer as either low grade or high grade:
- Low-grade bladder cancer. This type of cancer has cells that are closer in appearance and organization to normal cells (well differentiated). A low-grade tumor usually grows more slowly and is less likely to invade the muscular wall of the bladder than is a high-grade tumor. Low-grade bladder cancer often recurs in the bladder after treatment but rarely invades the muscular wall of the bladder or spreads to other parts of the body. Patients rarely die from low-grade bladder cancer.
- High-grade bladder cancer. This type of cancer has cells that are abnormal-looking and that lack any resemblance to normal-appearing tissues (poorly differentiated). A high-grade tumor tends to grow more aggressively than a low-grade tumor and may be more likely to spread to the muscular wall of the bladder and other tissues and organs. High-grade bladder cancer commonly recurs in the bladder and has a strong tendency to invade the muscular wall of the bladder and spread to other parts of the body. High-grade bladder cancer is treated more aggressively than low-grade bladder cancer and is much more likely to result in death. Almost all deaths from bladder cancer result from high-grade disease.
Bladder cancer is also divided into muscle-invasive and nonmuscle-invasive disease, based on invasion of the muscularis propria (also referred to as the detrusor muscle), which is the thick muscle deep in the bladder wall.
- Non-invasive cancers are still only in the inner layer of cells (the transitional epithelium). They have not grown into the deeper layers. A cancer that is only in this inner layer might also be called carcinoma in situ (CIS) or stage 0 cancer. Nonmuscle-invasive cancer can often be treated by removing the tumor(s) via a transurethral approach. Sometimes chemotherapy or other treatments are introduced into the bladder with a catheter to help fight the cancer.
- Invasive cancers have grown into deeper layers of the bladder wall. Muscle-invasive cancer is much more likely to spread to other parts of the body and are harder to treat. Muscle-invasive cancer is generally treated by either removing the bladder or treating the bladder with radiation and chemotherapy. As noted above, high-grade cancers are much more likely to be muscle-invasive than low-grade cancers. Thus, muscle-invasive cancers are generally treated more aggressively than nonmuscle-invasive cancers.
Transitional cell carcinoma staging of the renal pelvis and ureter
After transitional cell cancer of the renal pelvis and ureter has been diagnosed, your doctor may recommend additional tests to determine whether your cancer has spread within the renal pelvis and ureter or to your lymph nodes or to other areas of your body. The process used to find out if cancer has spread within the renal pelvis and ureter or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The doctor will use results of the diagnostic tests to help find out the stage of the disease. The stages of bladder cancer are indicated by Roman numerals ranging from 0 to IV (4). The lowest stages indicate a cancer that’s confined to the inner layers of the bladder and that hasn’t grown to affect the muscular bladder wall. The highest stage — stage IV (4) — indicates cancer that has spread to lymph nodes or organs in distant areas of the body.
The following tests and procedures may also be used in the staging process:
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- Bone scan: A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner.
- CT scan
- Magnetic resonance imaging (MRI)
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body and forms a tumor (metastatic tumor) in another part of the body.
Cancer may spread from where it began to other parts of your body.
When cancer spreads to another part of your body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if transitional cell cancer of the ureter spreads to the lung, the cancer cells in the lung are actually ureter cancer cells. The disease is metastatic cancer of the ureter, not lung cancer.
Though comparable in many respects to staging systems described for bladder cancer, unique structural aspects of the renal pelvis and ureter have led to several differences in the classification schema of tumors that involve the upper tracts. Clinical staging is based on a combination of radiographic procedures (e.g., intravenous pyelogram and computed tomographic scans) and, more recently, ureteroscopy and biopsy.
The advent of rigid and flexible ureteroscopic techniques has permitted endoscopic access to the ureter and renal pelvis. This may permit greater accuracy in preoperative definition of the stage and grade of an upper tract neoplasm. In addition, fulguration and endourological access permit resection or laser coagulation of highly selected low-stage, low-grade lesions of the ureters 40. However, this approach is still under clinical evaluation because there is the possibility of inaccurate assessment of the stage and extent of disease, and the adequacy and risks of such treatment have not yet been defined 41.
Because of the inaccessibility of ureteral and pelvic anatomy, accurate staging requires pathologic analysis of the surgically excised specimen.
American Joint Committee on Cancer (AJCC) TNM (tumor, node, metastasis) staging system
The American Joint Committee on Cancer (AJCC) has designated staging by TNM (tumor, node, metastasis) to define carcinoma of the renal pelvis and ureter 42. The American Joint Committee on Cancer (AJCC) TNM staging system has demonstrated accurate predictions of survival. The American Joint Committee on Cancer (AJCC) TNM (tumor, node, metastasis) staging system may be a better predictor of prognosis than tumor grade, although both are strongly predictive of survival. Median survival for patients with tumors confined to the subepithelial connective tissue was 91.1 months compared with 12.9 months for patients with tumors invading the muscularis and beyond, in one report. Flow cytometry analysis identifies low-stage, low-grade tumors at high risk of recurrence by virtue of their aneuploid histograms 43.
The following stages are used for transitional cell cancer of the renal pelvis and/or ureter:
Stage 0 (Noninvasive Papillary Carcinoma and Carcinoma in Situ)
In stage 0, abnormal cells are found in tissue lining the inside of the renal pelvis or ureter. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is divided into stages 0a and 0is, depending on the type of tumor:
- Stage 0a is also called noninvasive papillary carcinoma, which may look like long, thin growths that grow out from the tissue lining the inside of the renal pelvis or ureter.
- Stage 0is is also called carcinoma in situ, which is a flat tumor on the tissue lining the inside of the renal pelvis or ureter.
Table 1. Definitions of AJCC TNM Stage 0
| Stage | TNM | Definition |
|---|---|---|
| 0a | Ta, N0, M0 | Ta = Papillary noninvasive carcinoma. |
| N0 = No regional lymph node metastasis. | ||
| M0 = No distant metastasis. | ||
| 0is | Tis, N0, M0 | Tis = Carcinoma in situ. |
| N0 = No regional lymph node metastasis. | ||
| M0 = No distant metastasis. |
Abbreviations: T = primary tumor; N = regional lymph node; M = distant metastasis.
[Source 44 ]Stage 1
In stage 1, cancer has formed and has spread from the tissue lining the inside of the renal pelvis or ureter to the connective tissue layer.
Table 2. Definitions of AJCC TNM Stage 1
| Stage | TNM | Definition |
|---|---|---|
| 1 | T1, N0, M0 | T1 = Tumor invades subepithelial connective tissue. |
| N0 = No regional lymph node metastasis. | ||
| M0 = No distant metastasis. |
Abbreviations: T = primary tumor; N = regional lymph node; M = distant metastasis.
[Source 44 ]Stage 2
In stage 2, cancer has spread to the muscle layer of the renal pelvis or ureter.
Table 3. Definitions of AJCC TNM Stage 2
| Stage | TNM | Definition |
|---|---|---|
| 2 | T2, N0, M0 | T2 = Tumor invades the muscularis. |
| N0 = No regional lymph node metastasis. | ||
| M0 = No distant metastasis. |
Abbreviations: T = primary tumor; N = regional lymph node; M = distant metastasis.
[Source 44 ]Stage 3
In stage 3, cancer has spread:
- from the muscle layer of the renal pelvis to fat around the renal pelvis or to tissue in the kidney; or
- from the muscle layer of the ureter to fat around the ureter.
Table 4. Definitions of AJCC TNM Stage 3
| Stage | TNM | Definition |
|---|---|---|
| 3 | T3, N0, M0 | T3 = For renal pelvis only: Tumor invades beyond muscularis into peripelvic fat or into the renal parenchyma. For ureter only: Tumor invades beyond muscularis into periureteric fat. |
| N0 = No regional lymph node metastasis. | ||
| M0 = No distant metastasis. |
Abbreviations: T = primary tumor; N = regional lymph node; M = distant metastasis.
[Source 44 ]Stage 4
In stage 4, cancer has spread to at least one of the following:
- a nearby organ.
- the layer of fat around the kidney.
- lymph nodes.
- other parts of the body, such as the lung, liver, or bone.
Table 5. Definitions of AJCC TNM Stage 4
| Stage | TNM | Definition |
|---|---|---|
| 4 | T4, N0, M0 | T4 = Tumor invades adjacent organs, or through the kidney into the perinephric fat. |
| N0 = No regional lymph node metastasis. | ||
| M0 = No distant metastasis. | ||
| Any T, N1, M0 | TX = Primary tumor cannot be assessed. | |
| T0 = No evidence of primary tumor. | ||
| Ta = Papillary noninvasive carcinoma. | ||
| Tis = Carcinoma in situ. | ||
| T1 = Tumor invades subepithelial connective tissue. | ||
| T2 = Tumor invades the muscularis. | ||
| T3 = For renal pelvis only: Tumor invades beyond muscularis into peripelvic fat or into the renal parenchyma. For ureter only: Tumor invades beyond muscularis into periureteric fat. | ||
| T4 = Tumor invades adjacent organs, or through the kidney into the perinephric fat. | ||
| N1 = Metastasis in a single lymph node, ≤2 cm in greatest dimension. | ||
| M0 = No distant metastasis. | ||
| Any T, N2, M0 | Any T = See descriptions above in this table, stage IV, Any T, N1, M0. | |
| N2 = Metastasis in a single lymph node, >2 cm; or multiple lymph nodes. | ||
| M0 = No distant metastasis. | ||
| Any T, Any N, M1 | Any T = See descriptions above in this table, stage IV, Any T, N1, M0. | |
| NX = Regional lymph nodes cannot be assessed. | ||
| N0 = No regional lymph node metastasis. | ||
| N1 = Metastasis in a single lymph node, ≤2 cm in greatest dimension. | ||
| N2 = Metastasis in a singl lymph node, >2 cm; or multiple lymph nodes. | ||
| M1 = Distant metastasis. |
Abbreviations: T = primary tumor; N = regional lymph node; M = distant metastasis.
[Source 44 ]Localized, regional, or metastatic staging system
Transitional cell cancer of the renal pelvis and ureter is also described as localized, regional, or metastatic.
Each of these classifications has been subclassified into categories of unicentricity or multicentricity. The latter category indicates a more pervasive tumor diathesis and generally a less favorable prognosis.
Although the localized, regional, or metastatic classifications have prognostic significance, they can be determined only at the time of nephroureterectomy, which is the treatment of choice for patients with this disease. Because of the high incidence of tumor recurrence within the intramural ureter among patients who have had incomplete excision of this area, nephroureterectomy includes the entire ureter and a margin of periureteral orifice mucosa (i.e., bladder cuff).
Localized
- The cancer is found only in the kidney.
Patients with localized disease may be classified into three groups:
- Group 1: Low-grade tumor confined to the urothelium without lamina propria invasion (papilloma grade I transitional cell cancer).
- Group 2: Grade 1–3 carcinomas without demonstrable subepithelial invasion or focal microscopic invasion or papillary carcinomas with carcinoma in situ and/or carcinoma in situ elsewhere in the urothelium.
- Group 3: High-grade tumors that have infiltrated the renal pelvic wall or renal parenchyma or both but remain confined to the kidney. Infiltration of muscle in the upper tract may not be associated with as much potential for distant dissemination as appears to be the case for bladder cancer.
Regional
- The cancer has spread to tissues around the kidney and to nearby lymph nodes and blood vessels in the pelvis.
- Group 4: Extension of tumors beyond the renal pelvis or parenchyma and invasion of peripelvic and perirenal fat, lymph nodes, hilar vessels, and adjacent tissues.
Metastatic
- The cancer has spread to other parts of the body.
Recurrent Transitional Cell Cancer of the Renal Pelvis and Ureter
Recurrent transitional cell cancer of the renal pelvis and ureter is cancer that has recurred (come back) after it has been treated. The cancer may come back in the renal pelvis, ureter, or other parts of the body.
Transitional cell carcinoma treatment
There are different types of treatment for patients with transitional cell cancer of the renal pelvis and ureter. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Management algorithms have been developed to standardize the management of transitional cell carcinoma 45. Adult patients with blood in urine (hematuria) should first undergo cytology and/or cystoscopy. If urine cytology or bladder biopsy is positive, the patient should undergo transurethral resection of bladder tumors (TURBT) or imaging of the upper urinary tract. Non-muscle invasive transitional cell carcinoma should be managed based on the risk stratification, while the management of muscle-invasive transitional cell carcinoma should be based on the extent and stage of the disease.
Management of non-muscle invasive transitional cell carcinoma has its basis on the risk stratification done following transurethral resection of bladder tumors (TURBT) and relies on tumor stage, number, size, pathological grade, associated carcinoma in situ (CIS), lymphovascular invasion, or presence of aberrant histology. Based on the risk assessment, patients are categorized as low, intermediate, or high risk 46:
- Low-risk tumors include primary, solitary, Ta, LG/G1, < 3 cm, no carcinoma in situ (CIS). Management of low-risk patients is through a single postoperative instillation of intravesical chemotherapy followed by surveillance > 5 years; adjuvant intravesical treatment is not indicated.
- Intermediate-risk tumors: all tumors not defined in the two adjacent categories (between the category of low and high risk). Intermediate risk patients are managed by a single installation of intravesical chemotherapy, followed by induction and 1 year of maintenance intravesical therapy with Bacillus Calmette–Guérin (BCG) or chemotherapy (mitomycin or doxorubicin), followed by life-long surveillance.
- High-risk tumors: any of the following: T1 tumor, HG/G3 tumor, carcinoma in situ (CIS), multiple and recurrent and large (>3 cm) Ta G1G2 tumors (all conditions must be present). High-risk patients are re-staged through TURB in 4-6 weeks. Based on the results, the patient is either managed by intravesical Bacillus Calmette–Guérin (BCG) or radical cystectomy. Radical cystectomy entails the resection of the bladder, adjacent organs, and regional lymph nodes. In men, resection of the prostate and seminal vesicles are usually done. In women, resection of the uterus, cervix, ovaries, and anterior vagina is the norm. Urinary diversion through an orthotopic neobladder is the preferred urinary diversion procedure because it enables the patient to void and thereby improves the patient’s quality of life 47.
Management of patients with non-muscle invasive transitional cell carcinoma is with endoscopic resection and risk-based intravesical therapy, like bacillus Calmette-Guérin (BCG). Bacillus Calmette–Guérin (BCG) is a vaccine originally for tuberculosis, but has been shown to decrease recurrence and decrease progression (up to 37% compared to no BCG therapy) of transitional cell carcinoma when compared to chemotherapy. Patients should then undergo active surveillance, urine cytology screening, and/or adjunctive molecular screening. Cystectomy should be an option for tumors refractory to conservative management. Management of muscle-invasive transitional cell carcinoma is with cystectomy with or without chemotherapy. Neo-adjuvant / adjuvant therapy can be incorporated based on disease staging and the presence or absence of metastasis 46, 47.
Management of muscle-invasive bladder cancer has its basis in the stage and whether the patient is a surgical candidate and whether the patient willing to accept the consequences of radical cystectomy. Stage 2 and 3 can be managed either with combined cisplatin/radical cystectomy or combined modality (TURBT and chemoradiation). Stage 4 metastatic disease treatment is with platinum-based chemotherapy combination. Two combinations have been found to be equally efficient; the first includes a combination of methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) and is generally regarded as the standard first-line regimen. The second combines gemcitabine and cisplatin (GC). Checkpoint inhibitors targeting the programmed cell death-1 protein (PD-1) or its ligand (PD-L1) is the preferred option for refractory patients to platinum-based chemotherapy regimens.
Figure 3. Management of primary transitional cell carcinoma (urethral carcinoma)
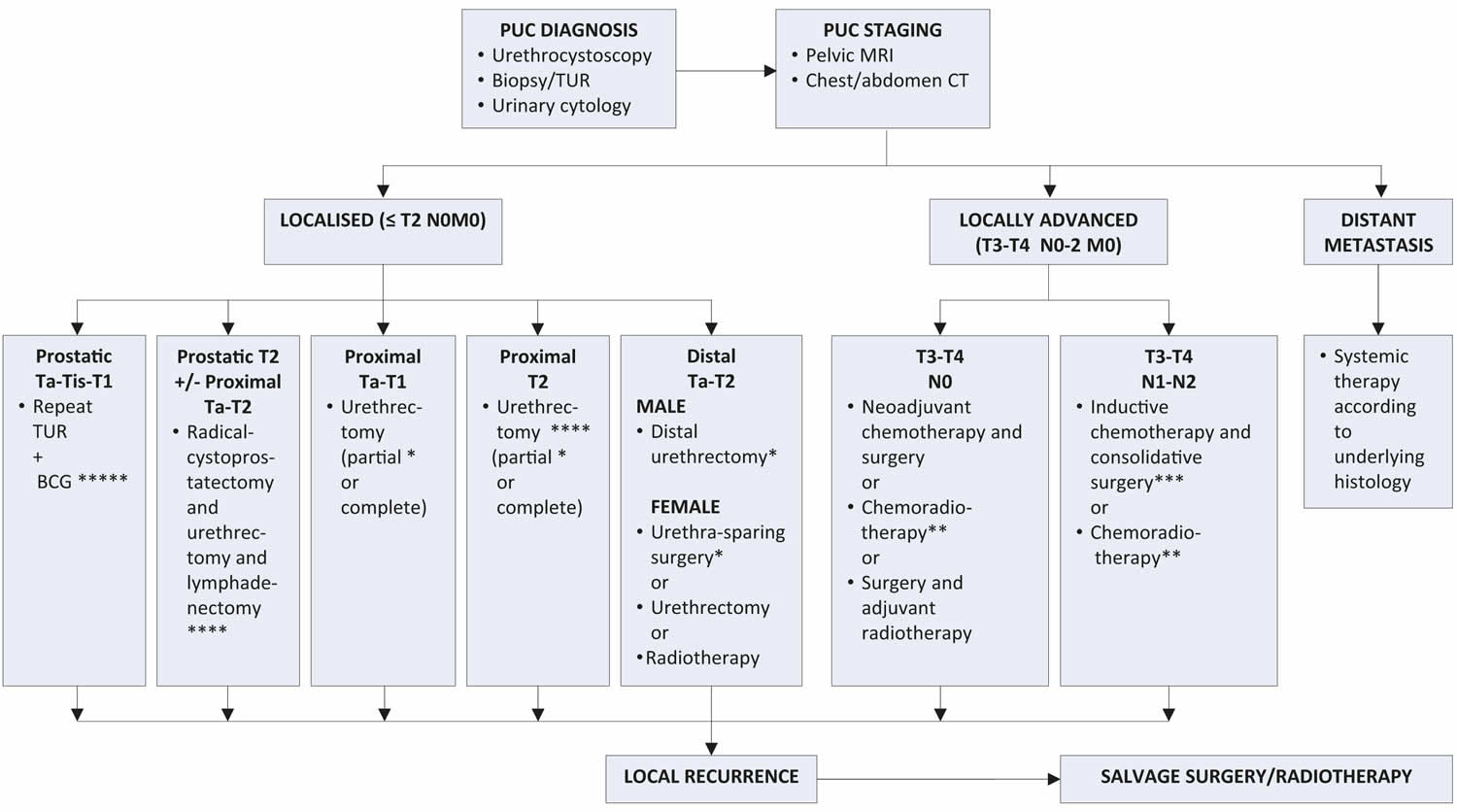
Footnotes:
* Ensure complete circumferential assessment if penile-preserving/urethra-sparing surgery or partial urethrectomy is intended.
** Squamous cell carcinoma.
*** Regional lymphadenectomy should be considered in clinically enlarged lymph nodes.
**** Consider neoadjuvant chemotherapy.
***** In extensive or BCG-unresponsive disease: consider (primary) cystoprostatectomy +/- urethrectomy + lymphadenectomy.
Abbreviations: BCG = bacillus Calmette-Guérin; CT = computed tomography; MRI = magnetic resonance imaging; PUC = primary urethral carcinoma; TUR = transurethral resection.
[Source 48 ]Treatment Options for Transitional Cell Cancer of the Renal Pelvis and Ureter
Localized Transitional Cell Cancer of the Renal Pelvis and Ureter
Treatment of localized transitional cell cancer of the renal pelvis and ureter may include the following:
- Surgery (nephroureterectomy with cuff of bladder or segmental resection of ureter only if the tumor is superficial and located in the distal third of the ureter).
- A clinical trial of fulguration.
- A clinical trial of laser surgery.
- A clinical trial of segmental resection of the renal pelvis.
- A clinical trial of regional chemotherapy.
- A clinical trial of regional biologic therapy.
Regional Transitional Cell Cancer of the Renal Pelvis and Ureter
- Treatment of regional transitional cell cancer of the renal pelvis and ureter is usually done in a clinical trial.
Metastatic Transitional Cell Cancer of the Renal Pelvis and Ureter
- Treatment of metastatic transitional cell cancer of the renal pelvis and ureter is usually done in a clinical trial, which may include chemotherapy.
Recurrent Transitional Cell Cancer of the Renal Pelvis and Ureter
- Treatment of recurrent transitional cell cancer of the renal pelvis and ureter is usually done in a clinical trial, which may include chemotherapy.
Surgery
One of the following surgical procedures may be used to treat transitional cell cancer of the renal pelvis and ureter:
- Nephroureterectomy: Surgery to remove the entire kidney, the ureter, and the bladder cuff (tissue that connects the ureter to the bladder).
- Segmental resection of the ureter: A surgical procedure to remove the part of the ureter that contains cancer and some of the healthy tissue around it. The ends of the ureter are then reattached. This treatment is used when the cancer is superficial and in the lower third of the ureter only, near the bladder.
New types of treatment are being tested in clinical trials
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied.
The development of new instrumentation for endourological treatment of upper tract transitional cell cancer has provided new options for regional management of these cancers. Introduction of electrofulguration and resection instruments or laser probes either transureterally or percutaneously may permit destruction of a primary cancer. Introduction of cytotoxic agents has also been employed. Although a biopsy can be taken for staging purposes, the accuracy of this remains to be determined. The efficacy of treatment by these maneuvers has not been established.
Fulguration
Fulguration is a surgical procedure that destroys tissue using an electric current. A tool with a small wire loop on the end is used to remove the cancer or to burn away the tumor with electricity.
Segmental resection of the renal pelvis
This is a surgical procedure to remove localized cancer from the renal pelvis without removing the entire kidney. Segmental resection may be done to save kidney function when the other kidney is damaged or has already been removed.
Laser surgery
A laser beam (narrow beam of intense light) is used as a knife to remove the cancer. A laser beam can also be used to kill the cancer cells. This procedure may also be called laser fulguration.
Transurethral and percutaneous access to the upper tract have permitted the use of laser therapy in the control of superficial upper tract transitional cell cancers. This approach is dependent on accurate staging and adequate visualization of the lesions that need to be coagulated. Results of this approach are at present too preliminary to assess. Therapeutic efficacy, however, will depend on staging accuracy at initial treatment and the ease of monitoring such patients for disease recurrence and possible progression.
Regional chemotherapy and regional biologic therapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. Biologic therapy is a treatment that uses the patient’s immune system to fight cancer; substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer. Regional treatment means the anticancer drugs or biologic substances are placed directly into an organ or a body cavity such as the abdomen, so the drugs will affect cancer cells in that area. Clinical trials are studying chemotherapy or biologic therapy using drugs placed directly into the renal pelvis or the ureter.
The dramatic successes that have been reported with intravesical cytotoxic (thiotepa, mitomycin, doxorubicin) or immunologic/inflammatory (Bacillus Calmette Guerin [BCG], interferon) therapy for superficial transitional cell cancers in the bladder have led to the occasional use of these agents in the treatment of upper tract cancers. Long-term follow-up of the results of such treatments has generally not been reported, and the efficacy of this approach cannot be assessed, largely because experience has been limited to those patients whose compromised clinical status (solitary kidney, renal failure, medical risks for surgery) may have influenced clinical outcome. The use of this approach will be limited by the following:
- The extent of disease in the renal pelvis.
- The access that these agents may have to the area of disease.
- The sensitivity of the cancer being treated.
- The adequacy and accuracy of initial tumor staging and continued monitoring.
Follow-up tests
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Stage 4 transitional cell carcinoma life expectancy
The prognosis for any patient with metastatic or recurrent transitional cell cancer is poor. The proper management of recurrence depends on the sites of recurrence, extent of prior therapy, and individual patient considerations. Chemotherapy regimens that have been shown effective for metastatic bladder cancer have generally been applied to transitional cell cancers arising from other sites. Patients with distant metastases have a poor prognosis and can be appropriately offered treatment on a clinical trial.
In patients with metastatic or recurrent transitional cell carcinoma of the bladder, combination chemotherapy has produced high response rates and occasional complete responses 49. Results from a randomized trial that compared methotrexate, vinblastine, doxorubicin, and cisplatin (M-VAC) to single-agent cisplatin in advanced bladder cancer show a significant advantage with M-VAC in both response rate and median survival. The overall response rate with M-VAC in this cooperative group trial was 39% 50.
Other chemotherapy agents that have shown activity in metastatic transitional cell cancer include the following 51:
- Paclitaxel.
- Ifosfamide.
- Gallium nitrate.
- Gemcitabine.
- Pemetrexed.
Ifosfamide, gallium nitrate, and pemetrexed have shown limited activity in patients previously treated with cisplatin.
Transitional cell carcinoma survival rate
The American Joint Committee on Cancer (AJCC) TNM (tumor, node, metastasis) staging system may be a better predictor of prognosis than tumor grade, although both are strongly predictive of survival. Median survival for patients with tumors confined to the subepithelial connective tissue was 91.1 months compared with 12.9 months for patients with tumors invading the muscularis and beyond, in one report. Flow cytometry analysis identifies low-stage, low-grade tumors at high risk of recurrence by virtue of their aneuploid histograms 43.
According to the Rare Cancers in Europe (RARECARE) project, the one- and 5-year relative overall survival rates in patients with transitional cell carcinoma (urethral carcinoma) in Europe are 71% and 54%, respectively 52. Based on longer follow-up, an analysis of the Surveillance, Epidemiology, and End Results (SEER) database, comparing prognostic factors in rare pathological types of primary transitional cell carcinoma (urethral carcinoma) (n = 257) and common pathological groups (n = 2,651), reported 10-year overall survival rates of 42.4% and 31.9%, respectively 53. Cancer-specific survival rates at five and ten years were 68% and 60%, respectively 54. Age (> 60 years), race (others vs. whites), T-stage (T3/T4 vs. Ta–T2) and M-stage (M1 vs. M0) were independent prognostic risk factors for overall survival and cancer-specific survival in rare pathological variants 53.
The Surveillance, Epidemiology, and End Results (SEER) database maintained by the National Cancer Institute (NCI) tracks 5-year relative survival rates for bladder cancer in the United States, based on how far the cancer has spread. The SEER database, however, does not group cancers by American Joint Committee on Cancer (AJCC) TNM stages (stage 1, stage 2, stage 3, etc.). Instead, Surveillance, Epidemiology, and End Results (SEER) groups cancers into localized, regional, and distant stages:
- Localized: There is no sign that the cancer has spread outside of the bladder.
- Regional: The cancer has spread from the bladder to nearby structures or lymph nodes.
- Distant: The cancer has spread to distant parts of the body such as the lungs, liver or bones.
Table 6. 5-year relative survival rates for bladder cancer (based on people diagnosed with bladder cancer between between 2012 and 2018)
| SEER stage | 5-year relative survival rate |
| Localized | 69.6% |
| In situ alone | 96% |
| Regional | 39% |
| Distant | 7.7% |
| All SEER stages combined | 77.1% |
Footnote:
- People now being diagnosed with bladder cancer may have a better outlook than these numbers show. Treatments improve over time, and these numbers are based on people who were diagnosed and treated at least five years earlier.
- These numbers apply only to the stage of the cancer when it is first diagnosed. They do not apply later on if the cancer grows, spreads, or comes back after treatment.
- These numbers don’t take everything into account. Survival rates are grouped based on how far the cancer has spread, but your age, overall health, how well the cancer responds to treatment, and other factors will also affect your outlook.
*SEER = Surveillance, Epidemiology, and End Results
[Source 55 ]Predictors of survival in primary transitional cell carcinoma or urethral carcinoma
Prognostic factors of worse survival in patients with primary urethral carcinoma are 56:
- Advanced age (> 65 years) and black race 57, 58, 59
- Higher stage, grade, nodal involvement 60, 61 and metastasis 62
- Increased tumour size and proximal tumour location 62
- Underlying (non-urothelial or unconventional) histology 63, 61, 59, 62
- Presence of concomitant bladder cancer 64
- Extent of surgical treatment and treatment modality 58, 62, 61
- Treatment in academic centers 65
- Location of recurrence (urethral vs. non-urethral) 66.
Some limitations have to be considered when interpreting these results as the number of patients included in most studies were low 67.
Transitional cell carcinoma prognosis
The prognosis of transitional cell carcinoma depends on multiple factors. TNM stage is the most important prognostic factor of urinary bladder carcinoma. The major prognostic factor at the time of diagnosis of upper tract transitional cell cancer is the depth of infiltration into or through the uroepithelial wall. Most superficial tumors are likely to be well differentiated, while infiltrative tumors are likely to be poorly differentiated. The incidence of synchronous or metachronous contralateral upper tract cancers ranges from 2% to 4%; the incidence of subsequent bladder cancer after previous upper tract transitional cell cancer ranges from 30% to 50% 68. When involvement of the upper tract is diffuse (involving both the renal pelvis and ureter), the likelihood of subsequent development of bladder cancer increases to 75%. DNA ploidy has not added significant prognostic information beyond that provided by stage and grade 69.
The 5-year overall survival for pT1 (papillary tumor invasion into subepithelial connective tissue) is 75%, for pT2 (papillary tumor invasion into detrusor muscle or muscularis propria) is 50%, and for pT3 (papillary tumor extends beyond detrusor muscle into the perivesical fat) is 20%. The invasion of muscularis propria (bladder detrusor muscle) determines whether the patient staging is pT1 vs. pT2. Some histologic variants of transitional cell carcinoma have a relatively poorer prognosis when compared to typical transitional cell carcinoma. These variants include urothelial carcinoma with rhabdoid features, urothelial micro-papillary carcinoma, plasmacytoid carcinoma, sarcomatoid carcinoma, small cell carcinoma, and undifferentiated carcinoma. Other poor prognostic factors of transitional cell carcinoma include lymphovascular invasion, the presence of urothelial carcinoma in situ, recurrence, large tumor size, and multicentricity 46.
Recurrent transitional cell cancer of the renal pelvis and ureter prognosis
The prognosis for any patient with metastatic or recurrent transitional cell cancer is poor. The proper management of recurrence depends on the sites of recurrence, extent of prior therapy, and individual patient considerations. Chemotherapy regimens that have been shown effective for metastatic bladder cancer have generally been applied to transitional cell cancers arising from other sites. Patients with distant metastases have a poor prognosis and can be appropriately offered treatment on a clinical trial.
In patients with metastatic or recurrent transitional cell carcinoma of the bladder, combination chemotherapy has produced high response rates and occasional complete responses 49. Results from a randomized trial that compared methotrexate, vinblastine, doxorubicin, and cisplatin (M-VAC) with single-agent cisplatin in advanced bladder cancer show a significant advantage with methotrexate, vinblastine, doxorubicin, and cisplatin (M-VAC) in both response rate and median survival. The overall response rate with M-VAC in this cooperative group trial was 39% 50.
Other chemotherapy agents that have shown activity in metastatic transitional cell cancer include the following 70:
- Paclitaxel.
- Ifosfamide.
- Gallium nitrate.
- Gemcitabine.
- Pemetrexed.
Ifosfamide, gallium nitrate, and pemetrexed have shown limited activity in patients previously treated with cisplatin.
- Gatta G, van der Zwan JM, Casali PG, Siesling S, Dei Tos AP, Kunkler I, Otter R, Licitra L, Mallone S, Tavilla A, Trama A, Capocaccia R; RARECARE working group. Rare cancers are not so rare: the rare cancer burden in Europe. Eur J Cancer. 2011 Nov;47(17):2493-511. doi: 10.1016/j.ejca.2011.08.008[↩]
- Wenzel M, Nocera L, Collà Ruvolo C, Würnschimmel C, Tian Z, Shariat SF, Saad F, Briganti A, Tilki D, Mandel P, Becker A, Kluth LA, Chun FKH, Karakiewicz PI. Incidence rates and contemporary trends in primary urethral cancer. Cancer Causes Control. 2021 Jun;32(6):627-634. doi: 10.1007/s10552-021-01416-2[↩][↩]
- Al-Husseini MJ, Kunbaz A, Saad AM, Santos JV, Salahia S, Iqbal M, Alahdab F. Trends in the incidence and mortality of transitional cell carcinoma of the bladder for the last four decades in the USA: a SEER-based analysis. BMC Cancer. 2019 Jan 10;19(1):46. doi: 10.1186/s12885-019-5267-3[↩]
- Mallin K, David KA, Carroll PR, Milowsky MI, Nanus DM. Transitional cell carcinoma of the bladder: racial and gender disparities in survival (1993 to 2002), stage and grade (1993 to 2007) J Urol. 2011;185:1631–1636. doi: 10.1016/j.juro.2010.12.049[↩]
- Horstmann M, Witthuhn R, Falk M, Stenzl A. Gender-specific differences in bladder cancer: a retrospective analysis. Gend Med. 2008;5:385–394. doi: 10.1016/j.genm.2008.11.002[↩]
- Patafio FM, Robert Siemens D, Wei X, Booth CM. Is there a gender effect in bladder cancer? A population-based study of practice and outcomes. Can Urol Assoc J. 2015;9:269–274. doi: 10.5489/cuaj.2927[↩]
- Brandt MP, Gust KM, Mani J, Vallo S, Höfner T, Borgmann H, et al. Nationwide analysis on the impact of socioeconomic land use factors and incidence of urothelial carcinoma. Cancer Epidemiol. 2017;2018(52):63–69. doi: 10.1016/j.canep.2017.12.001[↩][↩][↩]
- Lee CT, Dunn RL, Williams C, Underwood W. Racial disparity in bladder cancer: trends in tumor presentation at diagnosis. J Urol. 2006;176:927–933. doi: 10.1016/j.juro.2006.04.074[↩][↩][↩]
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. doi: 10.3322/caac.21166[↩]
- Cárdenas-Turanzas M, Cooksley C, Pettaway CA, Sabichi A, Grossman HB, Elting L. Comparative outcomes of bladder Cancer. Obstet Gynecol. 2006;108:169–175. doi: 10.1097/01.AOG.0000223885.25192.91[↩]
- Prout GR, Wesley MN, McCarron PG, Chen VW, Greenberg RS, Mayberry RM, et al. Survival experience of black patients and white patients with bladder carcinoma. Cancer. 2004;100:621–630. doi: 10.1002/cncr.11942[↩]
- Underwood W, Dunn RL, Williams C, Lee CT. Gender and geographic influence on the racial disparity in bladder cancer mortality in the US. J Am Coll Surg. 2006;202:284–290. doi: 10.1016/j.jamcollsurg.2005.09.009[↩]
- Transitional Cell Cancer of the Renal Pelvis and Ureter Treatment (PDQ®)–Health Professional Version. https://www.cancer.gov/types/kidney/hp/transitional-cell-treatment-pdq[↩][↩]
- Freedman ND. Association between smoking and risk of bladder Cancer among men and women. JAMA. 2011;306:737. doi: 10.1001/jama.2011.1142[↩][↩]
- Ross RK, Jones PA, Yu MC. Bladder cancer epidemiology and pathogenesis. Semin Oncol. 1996 Oct;23(5):536-45.[↩][↩]
- Samanic CM, Kogevinas M, Silverman DT, Tardon A, Serra C, Malats N, et al. Occupation and bladder cancer in a hospital-based case-control study in Spain. Occup Environ Med. 2008;65:347–353. doi: 10.1136/oem.2007.035816[↩][↩]
- Talaska G. Aromatic amines and human urinary bladder cancer: exposure sources and epidemiology. J Environ Sci Heal – Part C Environ Carcinog Ecotoxicol Rev. 2003;21:29–43. doi: 10.1081/GNC-120021372[↩][↩]
- Bonassi S, Mfrlo F, Pearce N, Puntoni R. Bladder cancer and occupational exposure to polycyclic aromatic hydrocarbons. Int J Cancer. 1989;44:648–651. doi: 10.1002/ijc.2910440415[↩][↩]
- King WD, Marrett LD. Case-control study of bladder cancer and chlorination by-products in treated water (Ontario, Canada) Cancer Causes Control. 1996;7:596–604. doi: 10.1007/BF00051702[↩][↩]
- Baris D, Waddell R, Beane Freeman LE, Schwenn M, Colt JS, Ayotte JD, et al. Elevated bladder Cancer in northern New England: the role of drinking water and arsenic. JNCI J Natl Cancer Inst. 2016;108:1–9. doi: 10.1093/jnci/djw099[↩][↩]
- Sun J-W, Zhao L-G, Yang Y, Ma X, Wang Y-Y, Xiang Y-B. Obesity and risk of bladder Cancer: a dose-response meta-analysis of 15 cohort studies. PLoS One. 2015;10:e0119313. doi: 10.1371/journal.pone.0119313[↩][↩][↩][↩]
- Bhaskaran K, Douglas I, Forbes H, dos-Santos-Silva I, Leon DA, Smeeth L. Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5·24 million UK adults. Lancet (London, England) 2014;384:755–765. doi: 10.1016/S0140-6736(14)60892-8[↩][↩]
- Koebnick C, Michaud D, Moore SC, Park Y, Hollenbeck A, Ballard-Barbash R, et al. Body mass index, physical activity, and bladder Cancer in a large prospective study. Cancer Epidemiol Biomark Prev. 2008;17:1214–1221. doi: 10.1158/1055-9965.EPI-08-0026[↩][↩]
- Ward EM, Fedewa SA, Cokkinides V, Virgo K. The Association of Insurance and Stage at diagnosis among patients aged 55 to 74 years in the National Cancer Database. Cancer J. 2010;16:614–621. doi: 10.1097/PPO.0b013e3181ff2aec[↩][↩]
- Hengstler JG, Arand M, Herrero ME, Oesch F. Polymorphisms of N-acetyltransferases, glutathione S-transferases, microsomal epoxide hydrolase and sulfotransferases: influence on cancer susceptibility. Recent Results Cancer Res. 1998;154:47–85. doi: 10.1007/978-3-642-46870-4_4[↩][↩]
- Yu C, Hequn C, Longfei L, Long W, Zhi C, Feng Z, et al. GSTM1 and GSTT1 polymorphisms are associated with increased bladder cancer risk: Evidence from updated meta-analysis. Oncotarget. 2017;8:3246–3258. doi: 10.18632/oncotarget.13702[↩][↩][↩][↩]
- Zhu Z, Zhang J, Jiang W, Zhang X, Li Y, Xu X. Risks on N-acetyltransferase 2 and bladder cancer: a meta-analysis. Onco Targets Ther. 2015;8:3715–3720. doi: 10.2147/OTT.S82927[↩][↩]
- Gui Y, Guo G, Huang Y, Hu X, Tang A, Gao S, et al. Frequent mutations of chromatin remodeling genes in transitional cell carcinoma of the bladder. Nat Genet. 2011;43:875–878. doi: 10.1038/ng.907[↩][↩]
- Guo G, Sun X, Chen C, Wu S, Huang P, Li Z, et al. Whole-genome and whole-exome sequencing of bladder cancer identifies frequent alterations in genes involved in sister chromatid cohesion and segregation. Nat Genet. 2013;45:1459–1463. doi: 10.1038/ng.2798[↩][↩]
- PDQ Adult Treatment Editorial Board. Transitional Cell Cancer of the Renal Pelvis and Ureter Treatment (PDQ®): Health Professional Version. 2019 Mar 24. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK66010[↩]
- Krukowski J, Czajkowski M, Kłącz J, Wawrzaszek O, Gołębiewska M, Matuszewski M. Primary urethral carcinoma – unexpected cause of urethral stricture. Case report and review of the literature. Med Ultrason. 2019 Nov 24;21(4):494-496. doi: 10.11152/mu-2015[↩]
- Guo H, Peng X, Jin C, Wang L, Chen F, Sa Y. Lichen Sclerosus Accompanied by Urethral Squamous Cell Carcinoma: A Retrospective Study From a Urethral Referral Center. Am J Mens Health. 2018 Sep;12(5):1692-1699. doi: 10.1177/1557988318782095[↩]
- Colapinto V, Evans DH. Primary carcinoma of the male urethra developing after urethroplasty for stricture. J Urol. 1977 Oct;118(4):581-4. doi: 10.1016/s0022-5347(17)58111-2[↩]
- Mohanty NK, Jolly BB, Saxena S, Dawson L. Squamous cell carcinoma of perineal urethrostomy. Urol Int. 1995;55(2):118-9. doi: 10.1159/000282765[↩]
- Sawczuk I, Acosta R, Grant D, White RD. Post urethroplasty squamous cell carcinoma. N Y State J Med. 1986 May;86(5):261-3.[↩]
- Ahmed K, Dasgupta R, Vats A, Nagpal K, Ashrafian H, Kaj B, Athanasiou T, Dasgupta P, Khan MS. Urethral diverticular carcinoma: an overview of current trends in diagnosis and management. Int Urol Nephrol. 2010 Jun;42(2):331-41. doi: 10.1007/s11255-009-9618-x[↩]
- Chung DE, Purohit RS, Girshman J, Blaivas JG. Urethral diverticula in women: discrepancies between magnetic resonance imaging and surgical findings. J Urol. 2010 Jun;183(6):2265-9. doi: 10.1016/j.juro.2010.02.016[↩]
- Thomas AA, Rackley RR, Lee U, Goldman HB, Vasavada SP, Hansel DE. Urethral diverticula in 90 female patients: a study with emphasis on neoplastic alterations. J Urol. 2008 Dec;180(6):2463-7. doi: 10.1016/j.juro.2008.08.040[↩]
- Libby B, Chao D, Schneider BF. Non-surgical treatment of primary female urethral cancer. Rare Tumors. 2010 Sep 30;2(3):e55. doi: 10.4081/rt.2010.e55[↩]
- Grossman HB, Schwartz SL, Konnak JW: Ureteroscopic treatment of urothelial carcinoma of the ureter and renal pelvis. J Urol 148 (2 Pt 1): 275-7, 1992[↩]
- Heney NM, Nocks BN, Daly JJ, et al.: Prognostic factors in carcinoma of the ureter. J Urol 125 (5): 632-6, 1981[↩]
- Renal Pelvis and Ureter. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, 749–55[↩]
- Huben RP, Mounzer AM, Murphy GP: Tumor grade and stage as prognostic variables in upper tract urothelial tumors. Cancer 62 (9): 2016-20, 1988[↩][↩]
- AJCC: Renal pelvis and ureter. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 749–55.[↩][↩][↩][↩][↩]
- Kaseb H, Aeddula NR. Bladder Cancer. [Updated 2022 Oct 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536923[↩]
- Babjuk M, Böhle A, Burger M, Capoun O, Cohen D, Compérat EM, Hernández V, Kaasinen E, Palou J, Rouprêt M, van Rhijn BWG, Shariat SF, Soukup V, Sylvester RJ, Zigeuner R. EAU Guidelines on Non-Muscle-invasive Urothelial Carcinoma of the Bladder: Update 2016. Eur Urol. 2017 Mar;71(3):447-461. doi: 10.1016/j.eururo.2016.05.041[↩][↩][↩]
- Chang SS, Bochner BH, Chou R, Dreicer R, Kamat AM, Lerner SP, Lotan Y, Meeks JJ, Michalski JM, Morgan TM, Quale DZ, Rosenberg JE, Zietman AL, Holzbeierlein JM. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J Urol. 2017 Sep;198(3):552-559. doi: 10.1016/j.juro.2017.04.086. Epub 2017 Apr 26. Erratum in: J Urol. 2017 Nov;198(5):1175.[↩][↩]
- Primary Urethral Carcinoma Disease Management. https://uroweb.org/guidelines/primary-urethral-carcinoma/chapter/disease-management[↩]
- Sternberg CN, Yagoda A, Scher HI, et al.: Methotrexate, vinblastine, doxorubicin, and cisplatin for advanced transitional cell carcinoma of the urothelium. Efficacy and patterns of response and relapse. Cancer 64 (12): 2448-58, 1989[↩][↩]
- Loehrer PJ Sr, Einhorn LH, Elson PJ, et al.: A randomized comparison of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: a cooperative group study. J Clin Oncol 10 (7): 1066-73, 1992[↩][↩]
- Sweeney CJ, Roth BJ, Kabbinavar FF, et al.: Phase II study of pemetrexed for second-line treatment of transitional cell cancer of the urothelium. J Clin Oncol 24 (21): 3451-7, 2006.[↩]
- RARECARENet. Surveillance of Rare Cancers in Europe. 2019. https://www.rarecare.eu/default.asp[↩]
- Abudurexiti M, Wang J, Shao N, Wan FN, Zhu Y, Dai B, Ye DW. Prognosis of rare pathological primary urethral carcinoma. Cancer Manag Res. 2018 Dec 7;10:6815-6822. doi: 10.2147/CMAR.S184197[↩][↩]
- Swartz MA, Porter MP, Lin DW, Weiss NS. Incidence of primary urethral carcinoma in the United States. Urology. 2006 Dec;68(6):1164-8. doi: 10.1016/j.urology.2006.08.1057[↩]
- Cancer Stat Facts: Bladder Cancer. https://seer.cancer.gov/statfacts/html/urinb.html[↩]
- Primary Urethral Carcinoma Prognosis. https://uroweb.org/guidelines/primary-urethral-carcinoma/chapter/prognosis[↩]
- Wenzel M, Deuker M, Stolzenbach F, Nocera L, Collà Ruvolo C, Tian Z, Shariat SF, Saad F, Briganti A, Kluth LA, Chun FKH, Karakiewicz PI. The effect of race/ethnicity on histological subtype distribution, stage at presentation and cancer specific survival in urethral cancer. Urol Oncol. 2021 Jun;39(6):369.e9-369.e17. doi: 10.1016/j.urolonc.2020.11.031[↩]
- Champ CE, Hegarty SE, Shen X, Mishra MV, Dicker AP, Trabulsi EJ, Lallas CD, Gomella LG, Hyslop T, Showalter TN. Prognostic factors and outcomes after definitive treatment of female urethral cancer: a population-based analysis. Urology. 2012 Aug;80(2):374-81. doi: 10.1016/j.urology.2012.02.058[↩][↩]
- Wenzel M, Collà Ruvolo C, Würnschimmel C, Nocera L, Hoeh B, Tian Z, Saad F, Briganti A, Tilki D, Banek S, Mandel P, Becker A, Kluth LA, Chun FKH, Karakiewicz PI. Epidemiology of Unconventional Histological Subtypes of Urethral Cancer. Urol Int. 2023;107(1):15-22. doi: 10.1159/000525673[↩][↩]
- Gakis G, Morgan TM, Efstathiou JA, Keegan KA, Mischinger J, Todenhoefer T, Schubert T, Zaid HB, Hrbacek J, Ali-El-Dein B, Clayman RH, Galland S, Olugbade K Jr, Rink M, Fritsche HM, Burger M, Chang SS, Babjuk M, Thalmann GN, Stenzl A, Daneshmand S. Prognostic factors and outcomes in primary urethral cancer: results from the international collaboration on primary urethral carcinoma. World J Urol. 2016 Jan;34(1):97-103. doi: 10.1007/s00345-015-1583-7[↩]
- Panettieri V, Rancati T, Onjukka E, Ebert MA, Joseph DJ, Denham JW, Steigler A, Millar JL. External Validation of a Predictive Model of Urethral Strictures for Prostate Patients Treated With HDR Brachytherapy Boost. Front Oncol. 2020 Jun 11;10:910. doi: 10.3389/fonc.2020.00910[↩][↩][↩]
- Rabbani, F. (2011), Prognostic factors in male urethral cancer. Cancer, 117: 2426-2434. https://doi.org/10.1002/cncr.25787[↩][↩][↩][↩]
- Wenzel M, Deuker M, Nocera L, Collà Ruvolo C, Tian Z, Shariat SF, Saad F, Briganti A, Becker A, Kluth LA, Chun FKH, Karakiewicz PI. Comparison Between Urothelial and Non-Urothelial Urethral Cancer. Front Oncol. 2021 Jan 29;10:629692. doi: 10.3389/fonc.2020.629692[↩]
- Gakis G, Efstathiou JA, Daneshmand S, Keegan KA, Clayman RH, Hrbacek J, Ali-El-Dein B, Zaid HB, Schubert T, Mischinger J, Todenhöfer T, Galland S, Olugbade K Jr, Rink M, Fritsche HM, Burger M, Chang SS, Babjuk M, Thalmann GN, Stenzl A, Morgan TM. Oncological Outcomes of Patients with Concomitant Bladder and Urethral Carcinoma. Urol Int. 2016;97(2):134-41. doi: 10.1159/000448335[↩]
- Stone BV, Hill SC, Moses KA. The effect of centralization of care on overall survival in primary urethral cancer. Urol Oncol. 2021 Feb;39(2):133.e17-133.e26. doi: 10.1016/j.urolonc.2020.09.020[↩]
- Gakis G, Schubert T, Morgan TM, Daneshmand S, Keegan KA, Mischinger J, Clayman RH, Brisuda A, Ali-El-Dein B, Galland S, Gregg J, Balci M, Olugbade K Jr, Rink M, Fritsche HM, Burger M, Babjuk M, Stenzl A, Thalmann GN, Kübler H, Efstathiou JA. The prognostic effect of salvage surgery and radiotherapy in patients with recurrent primary urethral carcinoma. Urol Oncol. 2018 Jan;36(1):10.e7-10.e14. doi: 10.1016/j.urolonc.2017.09.012[↩]
- Derksen JW, Visser O, de la Rivière GB, Meuleman EJ, Heldeweg EA, Lagerveld BW. Primary urethral carcinoma in females: an epidemiologic study on demographical factors, histological types, tumour stage and survival. World J Urol. 2013 Feb;31(1):147-53. doi: 10.1007/s00345-012-0882-5[↩]
- Krogh J, Kvist E, Rye B: Transitional cell carcinoma of the upper urinary tract: prognostic variables and post-operative recurrences. Br J Urol 67 (1): 32-6, 1991.[↩]
- Corrado F, Ferri C, Mannini D, et al.: Transitional cell carcinoma of the upper urinary tract: evaluation of prognostic factors by histopathology and flow cytometric analysis. J Urol 145 (6): 1159-63, 1991.[↩]
- Sweeney CJ, Roth BJ, Kabbinavar FF, et al.: Phase II study of pemetrexed for second-line treatment of transitional cell cancer of the urothelium. J Clin Oncol 24 (21): 3451-7, 2006[↩]

{kind=link}