Contents
What is thymoma
Thymoma is a rare tumor that form in cells on the thymus. Thymomas grow slowly and rarely spread beyond the thymus. There’s also a much rarer form of thymus gland cancer called thymic carcinoma. Thymic carcinoma grows faster, often spreads to other parts of the body, and is harder to treat with a higher risk of relapse and death 1. Thymomas and thymic carcinomas are epithelial tumors of the thymus. The term, thymoma, is customarily used to describe neoplasms that show no overt atypia of the epithelial component. A thymic epithelial tumor that exhibits clear-cut cytologic atypia and histologic features no longer specific to the thymus is known as a thymic carcinoma (also known as type C thymoma) 2.
Thymomas and thymic carcinomas are tumors that start from thymic epithelial cells. Not all doctors agree about the best way to describe and classify these tumors. In the past, thymomas were sometimes divided into benign (non-cancer) thymomas and malignant (cancer) thymomas, based on whether they had grown beyond the thymus into other tissues or organs. Now, most doctors think all thymomas may become cancer over time, and the best way to predict how likely they are to come back after treatment is to describe whether they have grown into tissues beyond the thymus (and if so, how far). This is done by the surgeon who notes whether or not the tumor is attached to nearby organs and by the pathologist who looks at samples from the margins (edges) of the tumor under the microscope. Based on these findings, doctors put thymomas into 2 main types, A and B. Type A thymomas usually grow slowly, but type B thymomas can grow quicker. They can spread to the lungs or the covering of the lungs (pleura). But it’s unusual for them to spread anywhere else in your body.
The 2021 World Health Organization (WHO) Classification system for tumors of the thymus is described below 3:
- Type A
- Composed of bland spindle cells and few scattered lymphocytes
- 60% of these are in stage 1.
- They tend to have good patient outcomes.
- There is an atypical variant that is hypercellular, possesses increased mitotic activity, and/or is necrotic. The presence of necrosis tends to predict an advanced stage.
- Type AB
- This is a mixture of type A and types B1 or B2.
- It is composed of intermixed or distinct components.
- 67% of these are in stage 1.
- Type B1
- Composed of predominantly lymphocytes with scattered epithelial cells, not in clusters
- Also paler medullary islands with rare Hassall corpuscle-like structures
- 50% of these are in stage 1
- Type B2
- Composed of mostly epithelial cells forming clusters and medullary islands may be present
- Atypia may be more present and may show anaplastic features
- 32% of these are in stage 1
- Type B3
- Composed predominantly of large, polygonal cells with increased atypia and few scattered lymphocytes
- Its prognosis is worse than other thymomas but is better than thymic carcinomas.
- Only 19% of these are in stage 1.
Invasive thymomas and thymic carcinomas are relatively rare tumors, which together represent about 0.2% to 1.5% of all malignancies 4. The overall incidence of thymoma is 0.15 cases per 100,000, based on data from the National Cancer Institute Surveillance, Epidemiology and End Results (SEER) Program 5. Thymic carcinomas are rarer and have been reported to account for only 0.06% of all thymic neoplasms 6.
90 out of 100 (90%) thymomas are in the front of your chest but rarely they might develop in your neck.
Thymomas and thymic carcinomas are most common in people between the ages of 40 through 60 years 7. But children and elderly people can also get these tumors.
Thymoma’s can vary in how they behave. Some grow very slowly. Others grow faster and can spread to the lungs or the covering of the lungs (the pleura). It’s very unusual for them to spread anywhere else in your body.
Like many other cancers, scientists don’t know exactly what causes thymomas.
Some people with thymomas also have a condition affecting their immune system. Around 30 out of 100 people diagnosed with thymoma’s (30%) have another condition called myasthenia gravis. Myasthenia gravis is an autoimmune disease. Thymoma has been linked to other autoimmune diseases, such as:
- systemic lupus erythematosus (SLE)
- rheumatoid arthritis
Thymoma has also been linked to blood conditions such as pernicious anemia, hypogammaglobulinemia, and red cell aplasia.
The thymus gland
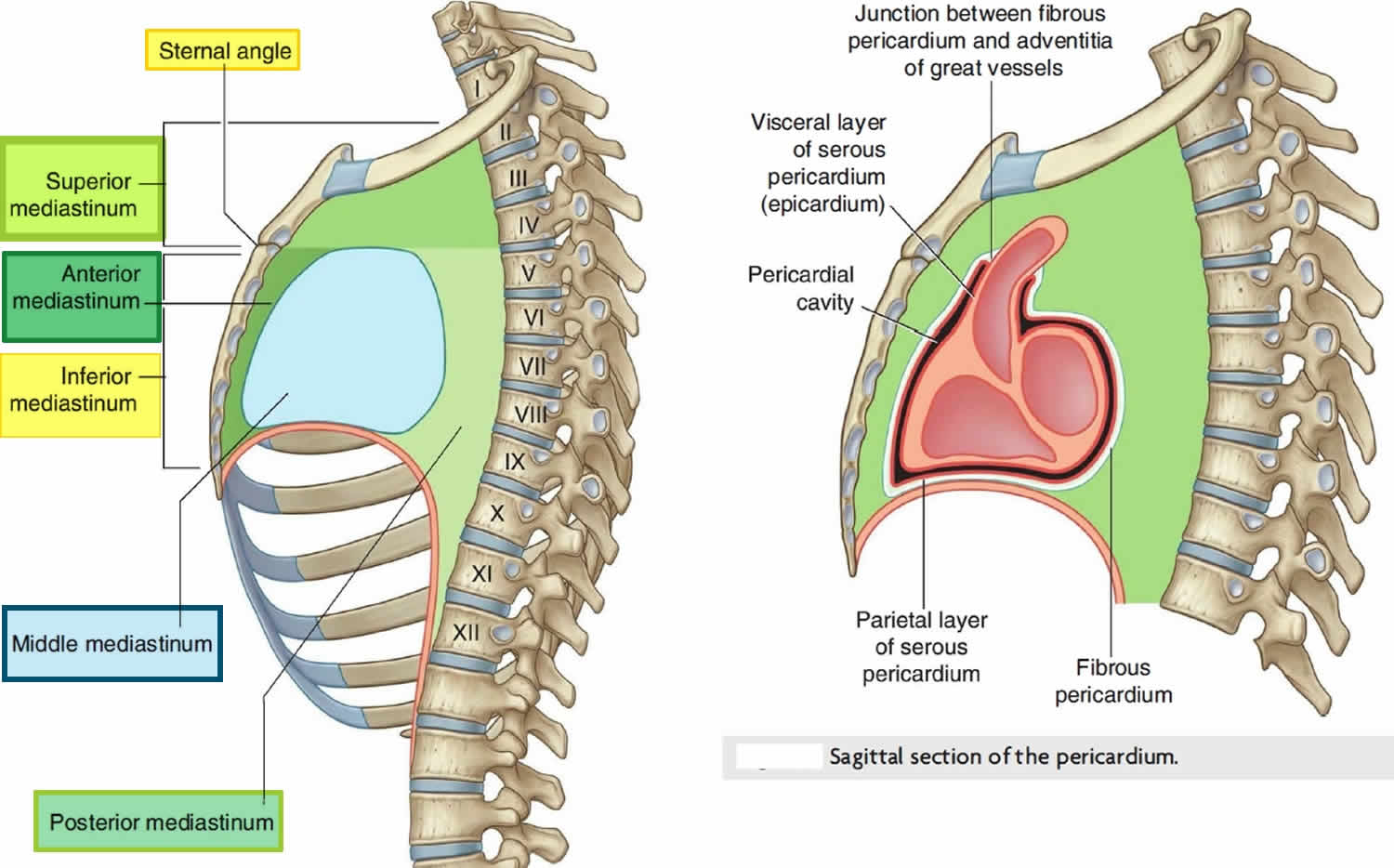
The thymus gland is a small organ located just behind the breast bone (sternum) in the front part of the chest in between your lungs. The thymus is in a part of the chest called the mediastinum, the space in the chest between the lungs that also contains the heart, part of the aorta, the esophagus (the tube that connects the mouth to the stomach), part of the trachea (windpipe), and many lymph nodes. The thymus gland sits just in front of and above the heart. Ninety percent of thymomas and thymic carcinomas occur in the anterior mediastinum 8. They are the most common malignancies of the anterior mediastinum 9.
The thymus gland is involved in the development of white blood cells called T lymphocytes (also known as T cells). These white blood cells are part of your immune system and fight infection.
The thymus gland is divided into 2 halves, called lobes. It has an irregular shape. There are a lot of small bumps called lobules on its surface. The thymus has 3 main layers:
- The medulla is the inside part of the thymus.
- The cortex is the layer that surrounds the medulla.
- The capsule is the thin covering over the outside of the thymus.
The thymus reaches its maximum weight of about 1 ounce during puberty. Then it decreases in size during adulthood as it’s replaced by fat tissue.
The thymus is an important part of the body’s immune system. During fetal development and childhood, the thymus is involved in the production and maturation of T lymphocytes, a type of white blood cell. T lymphocytes develop in the thymus and then travel to lymph nodes (bean-sized collections of immune system cells) throughout the body. There they help the immune system protect the body from viruses, fungus, and other types of infections.
The thymus is made of different types of cells. Each kind can develop into different types of cancer:
- Epithelial cells give the thymus its structure and shape. Thymomas and thymic carcinomas, which are the main focus of the rest of this post, develop from these cells.
- Lymphocytes make up most of the rest of the thymus. Whether in the thymus or in other parts of the body, these immune system cells can develop into cancers called Hodgkin disease and non-Hodgkin lymphoma.
- Kulchitsky cells, or neuroendocrine cells, are much less common cells that normally release certain hormones. These cells can give rise to cancers called carcinoid tumors. This document does not discuss carcinoid tumors of the thymus. Much of the information in Lung Carcinoid Tumor and Gastrointestinal Carcinoid Tumors also applies to carcinoids of the thymus.
Figure 1. Thymus gland
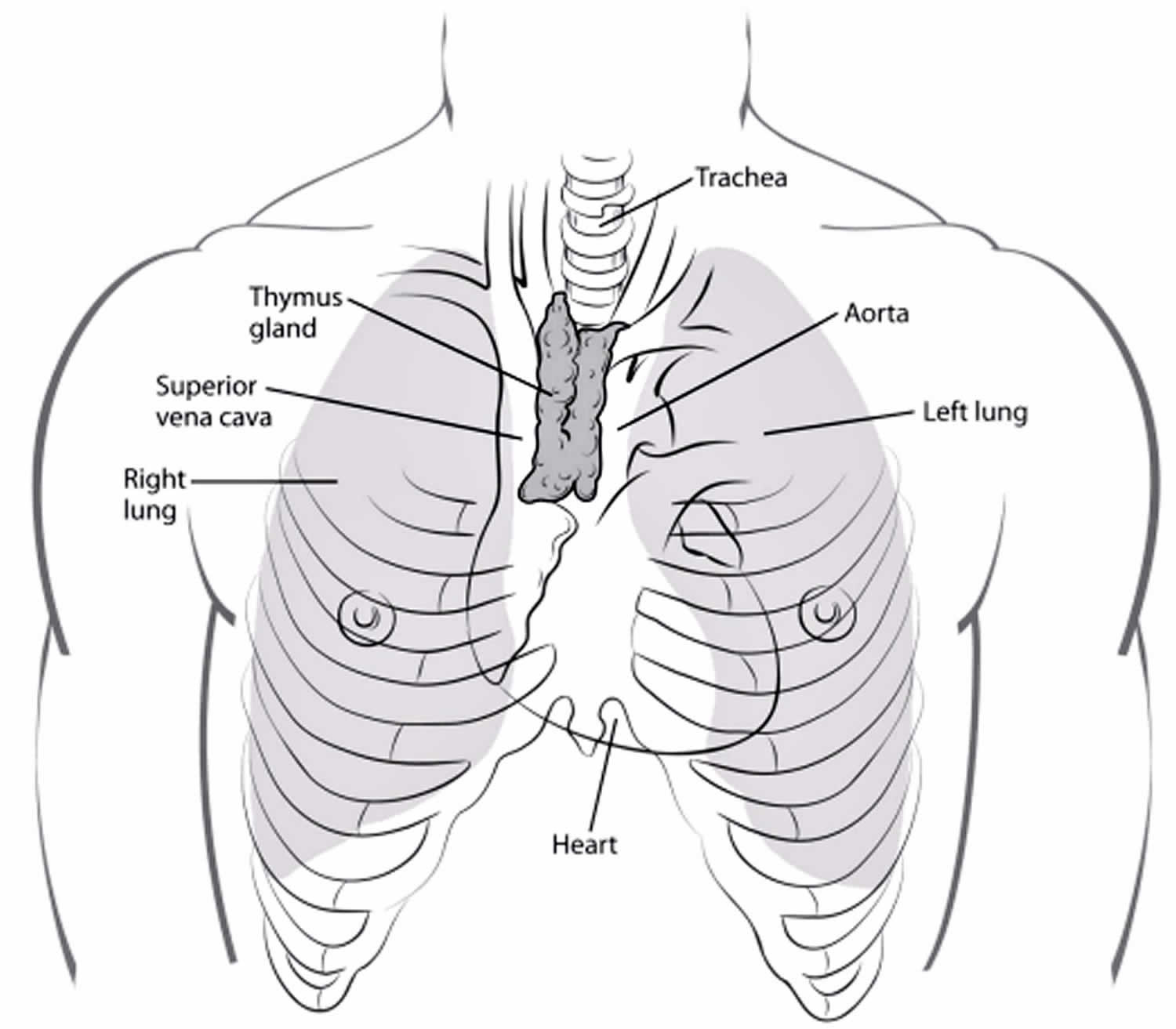
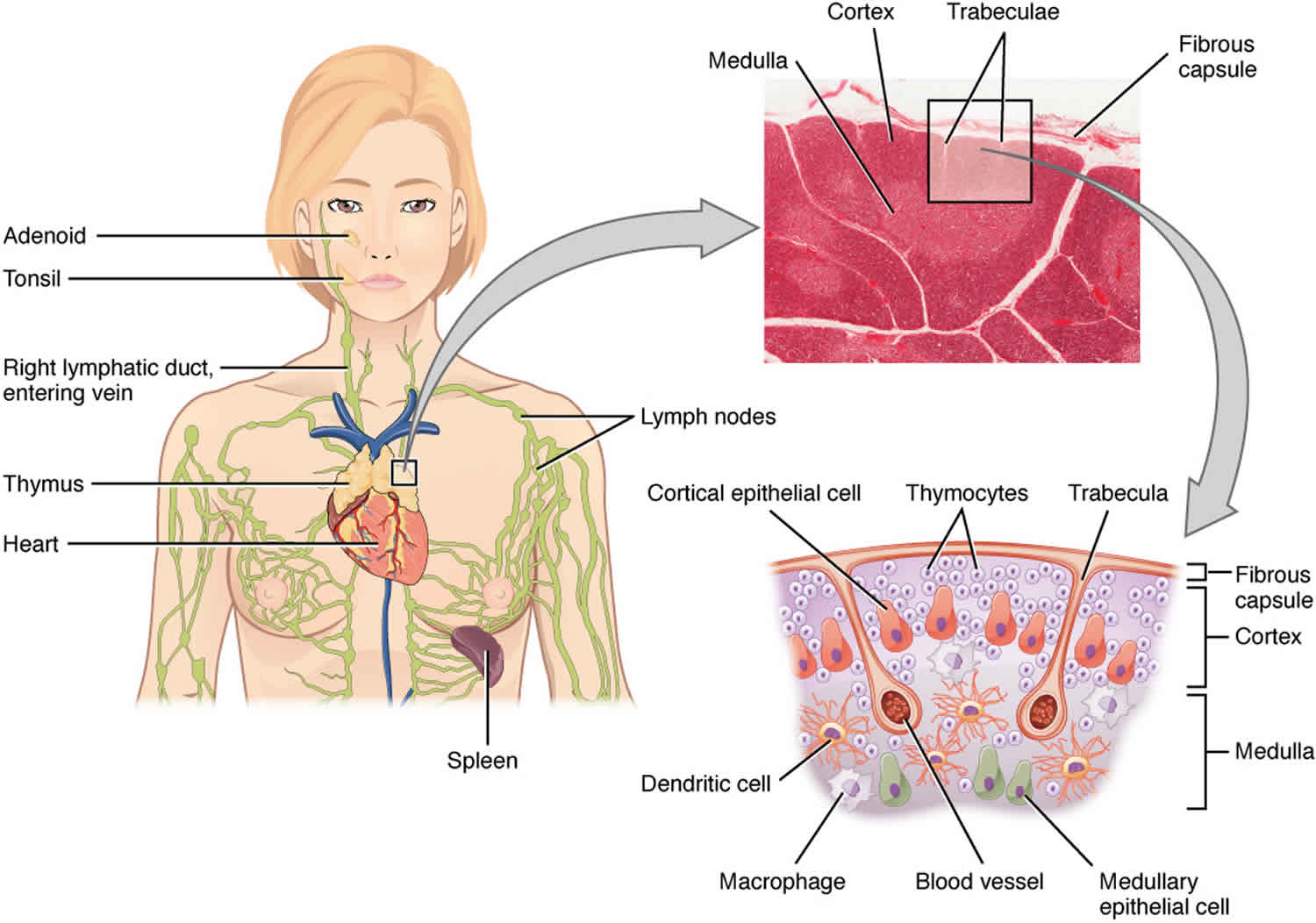
Figure 2. Mediastinum
Thymoma symptoms
Many thymic tumors are found on an x-ray or scan done for some other reason, before the patient has symptoms. The rest are brought to the attention of a doctor after a person starts to have symptoms. These may be related to the tumor itself, or they may be part of a paraneoplastic syndrome.
Although these signs and symptoms might be caused by thymus tumors, they can also be caused by other conditions. Still, if you have any of these problems, it’s important to see your doctor right away so the cause can be found and treated, if needed.
At the time of diagnosis, most patients with thymoma or thymic carcinoma are asymptomatic 10.
The thymus is in the middle of the chest, near the airways and certain blood vessels.
Tumors in the thymus can press on nearby structures, causing symptoms such as:
- chest pain
- a cough that won’t go (which may bring up bloody sputum)
- shortness of breath
- difficulty swallowing
- hoarseness of the voice
- loss of appetite
- weight loss
The thymus is close to the superior vena cava. The superior vena cava carries blood from your head and upper body to your heart. The cancer can press on it and cause superior vena cava syndrome. Symptoms can include:
- Swelling in the face, neck, and upper chest, sometimes with a bluish color
- Swelling of the visible veins in this part of the body
- Headaches
- Feeling dizzy or light-headed
Sometimes thymus gland tumors don’t cause any symptoms. They can be found by accident, when you’re having a chest x-ray, CT of the chest or a CT angiogram for something else.
Paraneoplastic syndromes
Paraneoplastic autoimmune syndromes are associated with thymoma and are rarely associated with thymic carcinomas 11. These are conditions that are related to the cancer but that are not caused directly by the tumor mass. For example, people with thymomas may develop autoimmune diseases, where the immune system starts to attack the body itself. Part of the normal function of the thymus is to help keep the immune system in check, which may help explain why this happens.
Myasthenia gravis
About 30% to 65% of people with thymomas also have myasthenia gravis 12. This is by far the most common autoimmune disease associated with thymomas. In this disease, the immune system forms antibodies that block the chemical signals that signal the muscles to move. This causes severe muscle weakness. People with myasthenia gravis tire easily. They may notice problems climbing stairs or walking long distances.
Although patients have decreased muscle strength throughout the body, symptoms caused by weakness of the muscles of the eyes, neck, and chest may be the most troublesome. Weakness of the eye muscles can cause blurred or double vision and drooping eyelids, while weak neck muscles can lead to problems with swallowing. Weakness of the chest muscles and diaphragm can cause problems breathing and shortness of breath.
Many people with thymomas have myasthenia gravis, but most people with myasthenia gravis don’t have thymomas. Many people with myasthenia gravis have other, noncancerous abnormalities of the thymus gland. Myasthenia gravis can be treated by removing the thymus (whether or not a thymoma is present) or with medicines that either strengthen the chemical signals to muscles or weaken the immune attack on the muscles.
Red cell aplasia
Red cell aplasia, in which the body’s ability to make new red blood cells is severely reduced, occurs in about 5% of thymoma patients 13. Red blood cells carry oxygen from the lungs to other tissues of the body. Reduced red blood cell production causes anemia (low red blood cell counts). Symptoms of anemia can include weakness, dizziness, shortness of breath, and tiring easily. The usual treatment is to remove the thymus gland.
Hypogammaglobulinemia
Hypogammaglobulinemia is a disorder in which the body makes low amounts of infection-fighting antibodies (also known as gamma globulins). This leaves the person susceptible to infections. About 5% to 10% of thymoma patients develop hypogammaglobulinemia. About 10% of patients with hypogammaglobulinemia have a thymoma. Removing the thymus does not help correct this disease.
Other autoimmune diseases
Many other autoimmune diseases have also been linked to thymoma. However, they are much less common than myasthenia gravis, pure red cell aplasia, or hypogammaglobulinemia. Some examples include 14:
- Acute pericarditis.
- Addison disease.
- Agranulocytosis.
- Alopecia areata.
- Cushing syndrome.
- Hemolytic anemia.
- Limbic encephalopathy.
- Myocarditis.
- Nephrotic syndrome.
- Parahypopituitarism.
- Pernicious anemia.
- Aplastic anemia.
- Polymyositis.
- Rheumatoid arthritis.
- Sarcoidosis.
- Scleroderma.
- Sensorimotor radiculopathy.
- Sjogren (Sjögren) syndrome.
- Stiff-person syndrome.
- Systemic lupus erythematosus.
- Thyroiditis.
- Ulcerative colitis.
Most people who have these autoimmune diseases do not have a thymoma.
Thymoma causes
At the present time scientists don’t know exactly what causes thymomas 15. There is a strong association of thymomas with myasthenia gravis and other paraneoplastic syndromes such as total red cell aplasia, polymyositis, systemic lupus erythematosus, Cushing syndrome, and syndrome of inappropriate antidiuretic hormone secretion 16, 17, 18, 19. Thirty to forty percent of patients with a thymoma experience symptoms suggestive of myasthenia gravis 15. Myasthenia gravis is a rare condition that affects the immune system and causes muscle weakness. An additional 5% of patients have paraneoplastic syndromes.
Thymoma is also linked to other diseases, such as 20:
- Red cell aplasia
- Hypogammaglobulinemia
- Pernicious anemia
- Systemic lupus erythematosus (SLE)
- Rheumatoid arthritis
Thymoma diagnosis
If you have signs or symptoms that suggest you might have a thymus tumor, your doctor will want to take a complete medical history to check for symptoms. You will also be asked about your general health.
A physical exam provides information about possible signs of thymic cancer and other health problems. Patients with thymic cancer will sometimes have a fullness that the doctor can feel in the lower neck area.
Thymomas are often suspected if you have signs and symptoms associated with myasthenia gravis, hypogammaglobulinemia, or red cell aplasia.
In about 50% of the patients, thymomas and thymic carcinomas are detected by chance with plain-film chest radiography 7.
Imaging tests
Imaging tests use x-rays, magnetic fields, or radioactive substances to create pictures of the inside of your body. Imaging tests may be done for a number of reasons, including:
- To help find a suspicious area that might be cancer
- To learn how far cancer may have spread
- To help see if treatment is working
- To look for signs that cancer has come back
Chest x-ray
A chest x-ray may be the first imaging test a doctor orders if he or she suspects a problem in the middle of the chest. It may be able to show if there is a tumor in the chest. In some cases, a chest x-ray may find tumors when the person is having the x-ray done for another reason. But some thymomas are small or in places that may not show up on a chest x-ray. If your doctor is still suspicious or if a change is seen on the chest x-ray, a CT scan may be ordered.
Computed tomography (CT) scan
A CT scan uses x-rays to make detailed, cross-sectional images of your body. Unlike a regular x-ray, a CT scan creates detailed images of the soft tissues in the body. A chest CT with contrast is often used.
CT scans can also be used to guide a biopsy needle precisely into a suspected tumor or metastasis. This is called a CT-guided needle biopsy.
Magnetic resonance imaging (MRI) scan
Like CT scans, MRI scans provide detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays.
MRI of the chest may be done to look more closely at thymus tumors. They are most often used for people who cannot have a CT scan for medical reasons (like problems with the IV contrast). MRI images are also particularly useful in looking for cancer that may have spread to the brain or spinal cord.
Positron emission tomography (PET) scan
For a PET scan, you are injected with a slightly radioactive form of sugar, which collects mainly in cancer cells. A special camera is then used to create a picture of areas of radioactivity in the body. The picture is not detailed like a CT or MRI scan, but a PET scan can look for possible areas of cancer spread in all areas of the body at once.
A PET scan can help give the doctor a better idea of whether a change seen on another imaging test is a tumor or not. If you have already been diagnosed with cancer, your doctor may use this test to see if the cancer has spread to lymph nodes or other parts of the body. A PET scan can also be useful if your doctor thinks the cancer may have spread but doesn’t know where.
Certain machines are able to perform both a PET and CT scan at the same time (PET/CT scan). This lets the doctor compare areas of higher radioactivity on the PET scan with the more detailed pictures of that area on the CT. Combined PET/CT is used more often than PET (alone) in looking at thymomas.
Blood tests
Blood tests can’t be used to diagnose thymomas, but they may be helpful in some situations. For example, blood tests may be done to look for certain antibodies if myasthenia gravis or another autoimmune disorder is suspected. Other blood tests might be done to make sure a mass in the middle of the chest isn’t a germ cell tumor or part of the thyroid gland.
If a thymoma is diagnosed, blood cell counts and blood chemistry tests are done to get an idea of a person’s overall health, especially if surgery is planned. Also, tests for myasthenia gravis will be done before any surgery. This is because myasthenia gravis is very common in people with a thymoma, and, if not treated, it can cause problems with the drugs used during surgery. People getting chemotherapy need regular blood tests to make sure the drugs aren’t having unwanted effects on the bone marrow, kidneys, or other organs.
Biopsy procedures
Although signs, symptoms, and imaging tests can suggest that a thymic tumor is likely, doctors can’t be certain of the diagnosis without looking at the tumor under a microscope.
For most cancers, taking out a small piece of the tumor (known as a biopsy) is needed to confirm whether a tumor is present and, if so, to determine its type. For thymomas, this is rarely done because doctors can usually tell that the tumor is very likely a thymoma based on how it looks on imaging tests. Because of this, doctors often remove the entire tumor rather than do a biopsy. This provides tissue for a diagnosis and treats the tumor at the same time. The specimen is sent to the lab after surgery to confirm the diagnosis.
If the tumor can’t be removed completely during surgery, a biopsy might be done to confirm the diagnosis. This helps the doctor decide if more treatment is needed after surgery.
If the doctor suspects a different type of tumor, a biopsy (usually a needle biopsy) might be done before surgery.
Thymoma stages
After someone is diagnosed with thymoma or thymus cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes the extent of the cancer in the body. It helps determine how serious the cancer is and how best to treat it. Doctors also use a cancer’s stage when talking about survival statistics.
Thymoma ranges from stages I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means cancer has spread more. And within a stage, an earlier letter means a lower stage. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
The staging system used for thymus cancer is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
- The extent (size) of the tumor (T): Has the cancer grown into nearby structures and if so, how far as it grown?
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby superficial or deep lymph nodes?
- The spread (metastasis) to distant sites (M): Has the cancer spread to the outer linings of the lungs or heart or to distant organs?
The system described below is the most recent American Joint Committee on Cancer (AJCC) system effective January 2018. This staging system is used to stage thymomas, thymic carcinomas and neuroendocrine tumors of the thymus.
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The staging system in the table below uses the pathologic stage (also called the surgical stage). It is determined by examining tissue removed during an operation. Sometimes, if surgery is not possible right away or at all, the cancer will be given a clinical stage instead. This is based on the results of a physical exam, biopsy, and imaging tests (CT or MRI scan, x-rays, PET scan, etc) done before surgery.
Cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Thymoma stages American Joint Committee on Cancer (AJCC) system
| AJCC Stage | Stage grouping | Stage description* |
|---|---|---|
| 1
| T1a N0 M0 | The cancer has not spread into the outer layer of the thymus OR it has grown into the nearby fatty tissues but not into the mediastinal pleura (the thin layer covering the space between the 2 lungs) (T1a). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| OR | ||
| T1b N0 M0 | The cancer has grown into the nearby fatty tissue and the mediastinal pleura (the thin layer covering the space between the 2 lungs) (T1b). It has not spread to nearby lymph nodes (N0) or distant sites (M0). | |
| 2 | T2 N0 M0 | The cancer has grown into the nearby fatty tissue and into the pericardium (the tissue sac containing the heart) (T2). It has not spread to nearby lymph nodes (N0) or distant sites (M0). |
| 3A | T3 N0 M0 | The cancer is growing into nearby tissues or organs, including the lungs, the vessels carrying blood into or out of the lungs, the main blood vessels taking blood away from the heart (the superior vena cava), or the phrenic nerve (the nerve that controls the diaphragm and breathing) (T3). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| 3B
| T4 N0 M0 | The cancer is growing into nearby tissues or organs, including the trachea (windpipe), esophagus (feeding tube), or the main blood vessels pumping blood away from the heart (T4). It has not spread to nearby lymph nodes (N0) or distant sites (M0). |
| 4A | Any T N1 M0
| The cancer might or might not have grown into nearby tissues or organs (Any T) AND has spread to nearby lymph nodes in the front chest cavity (N1). It has not spread to distant sites (M0). |
| OR | ||
| Any T N0 or N1 M1a | The cancer might or might not have grown into nearby tissues or organs (Any T) and might or might not have spread to nearby lymph nodes (N0 or N1). The cancer has spread to the pleura (lining of the lung) or the pericardium (lining of the heart) (M1a). | |
| 4B | Any T N2 M0 or M1a | The cancer might or might not have grown into nearby tissues or organs (Any T) AND has spread to the lymph nodes deep in the chest cavity or the neck (N2) and might or might not have spread to the pleura (lining of the lung) or the pericardium (lining of the heart) (M0 or M1b). |
| OR | ||
| Any T Any N M1b | The cancer might or might not have grown into nearby tissues or organs (Any T), might or might not have spread to nearby lymph nodes in the chest cavity or neck (Any N), but has spread to the inside of the lungs or other distant organs (M1b). | |
Footnote:
* The following additional categories are not listed in the table above:
- TX: Main tumor cannot be assessed due to lack of information.
- T0: No evidence of a primary tumor.
- NX: Regional lymph nodes cannot be assessed due to lack of information.
Masaoka-Koga system
Sometimes the Masaoka-Koga Clinical Stage is also used 22.
- Stage 1: Completely encapsulated tumor
- Stage 2. Microscopic invasion of the capsule
- Stage 3. Macroscopic invasion into surrounding structures
- Stage 4A. Pleural or pericardial metastases/nodules
- Stage 4B. Lymphogenous or hematogenous (distant) metastases
Thymoma treatment
The most common treatments for thymoma are:
- surgery
- radiotherapy
- chemotherapy
You might have one or more of these treatments. Most people with operable thymoma are cured with either surgery alone or surgery followed by radiotherapy.
Surgery
The main treatment for thymus gland cancer is an operation to remove it.
Many thymomas are covered in a fibrous sheet called a capsule. These thymomas are often quite easy to remove and are usually cured with surgery alone.
The most common surgery for thymus gland tumors is the complete removal of the thymus gland (thymectomy) and the cancer. The surgeon often makes a cut down the middle of the chest, to remove the thymus and cancer. This is called a sternotomy.
Sometimes you might have keyhole surgery instead. Keyhole surgery involves your surgeon making small incisions (cuts) rather than large ones, they then carry the surgery out through these excisions.
Radiotherapy
Radiotherapy means the use of radiation, usually x-rays, to treat cancer cells.
You might have radiotherapy after surgery (post operative radiotherapy) if:
- your surgeon thinks they haven’t been able to remove all the cancer
- there is a high risk that your thymoma will come back
The surgeon removes as much of the cancer as possible. They then use radiotherapy to try and kill off any cancer cells left behind.
You might have radiotherapy as your main treatment if you can’t have surgery.
Chemotherapy
Chemotherapy uses anti cancer (cytotoxic) drugs to destroy cancer cells.
You might have chemotherapy:
- to try and shrink the cancer so that surgery is possible (neoadjuvant chemotherapy)
- if your cancer comes back
The chemotherapy drugs you might have include cisplatin, carboplatin, doxorubicin etoposide, paclitaxel, and cyclophosphamide.
If you have thymic carcinoma, you might have post operative chemotherapy (chemotherapy after surgery). Your doctor decides whether you need this, based on whether your surgeon can remove all the tumour.
Unfortunately, if your thymus gland tumour does come back, it can be difficult to get rid of it altogether. But treatment can often keep it under control for some time.
Your doctor will be able to tell you more, by keeping a close eye on how your cancer responds to treatment.
Follow-up
Because of the increased risk of second malignancies and the fact that thymoma can recur after a long interval, it has been recommended that surveillance should be lifelong 23. After treatment, annual imaging is recommended even though no clinical trials have shown benefit to such imaging. It is recommended that a CT chest is ordered every six months for two years and annually for five years in cases of thymic carcinoma and ten years in cases of thymomas 15. Thymic tumors tend to recur as pleural nodules, most commonly with a mean length of 8 to 68 months after treatment.
The measurement of interferon-alpha and interleukin-2 antibodies is helpful to identify patients with a thymoma recurrence 24.
Thymoma prognosis
The prognosis (the outlook for chances of survival) after treatment of a thymus cancer depends to a large extent on its stage. But other features are also important such as the type of thymus cancer and whether the surgeon is able to remove the entire tumor.
A German series studied the prognosis of various stages of thymic tumors. Their findings are summarized below 15:
- The prognosis was found to be excellent for Masaoka stage 1 and 2 thymomas.
- The prognosis was worse following resection in Masaoka stage 3 thymomas.
- There was a 27% recurrence rate and an 83% 10-year survival in Masaoka stage 3 thymomas.
- Masaoka stage 4 thymomas have a 10-year survival rate of 47%.
- There was no tumor-related death seen in type A, AB, or B1 disease (Masaoka stage 1 and 2)
- There was a rate of tumor-related death of 9, 19, and 17% in B2, B3, or thymic carcinoma and a rate of death of 50% to 60% in Masaoka stage 3 and 4 thymomas.
Thymoma has been associated with an increased risk of second malignancies (approximately 17% to 28% risk after thymectomy). In a review of the SEER (Surveillance, Epidemiology, and End Results) database of thymoma cases in the United States between 1973 and 1998, 849 cases were identified (overall incidence, 0.15 per 100,000 person-years) 25. In this study, there was an excess risk of B cell non-Hodgkin lymphoma, gastrointestinal cancers, and soft tissue sarcomas 15.
Risk of second malignancy appears to be unrelated to any of the following 25:
- Thymectomy.
- Radiation therapy.
- A clinical history of myasthenia gravis.
Standard primary treatment for patients with these types of tumors is surgical resection with en bloc resection for invasive tumors, if possible 26. Depending on tumor stage, there are multimodality treatment options, which include the use of radiation therapy and chemotherapy with or without surgery 27.
Thymic carcinomas have a greater propensity to capsular invasion and metastases than thymomas. Patients more often present with advanced disease, with a 5-year survival of 30% to 50% 28. Owing to the paucity of cases, optimal management of thymic carcinoma has yet to be defined. As with thymoma, primary treatment is surgical resection; however, multimodality treatment with surgery, radiation, and chemotherapy are often used because of the more-advanced stage and greater risk of relapse.
Thymoma survival rates
Survival rates can give you an idea of what percentage of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding of how likely it is that your treatment will be successful.
Keep in mind that survival rates are estimates and are often based on previous outcomes of large numbers of people who had a specific cancer, but they can’t predict what will happen in any particular person’s case. These statistics can be confusing and may lead you to have more questions. Talk with your doctor about how these numbers may apply to you, as he or she is familiar with your situation.
A relative survival rate compares people with the same type and stage of thymus cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific stage of thymus cancer is 70%, it means that people who have that cancer are, on average, about 70% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
The SEER (Surveillance, Epidemiology, and End Results) database tracks 5-year relative survival rates for thymus cancer in the United States, based on how far the cancer has spread. The SEER database, however, does not group cancers by AJCC TNM stages (stage 1, stage 2, stage 3, etc.). Instead, it groups cancers into localized, regional, and distant stages:
- Localized: There is no sign that the cancer has spread outside of the thymus.
- Regional: The cancer has spread outside of the thymus to nearby structures or lymph nodes.
- Distant: The cancer has spread to distant parts of the body such as the lining of the heart or the inside of the lungs.
Table 2. 5-year relative survival rates for thymus cancer (based on people diagnosed with thymus cancer between 2008 and 2014)
| SEER Stage | 5-Year Relative Survival Rate |
| Localized | 88% |
| Regional | 77% |
| Distant | 45% |
| All SEER stages combined | 70% |
Footnote:
- These numbers apply only to the stage of the cancer when it is first diagnosed. They do not apply later on if the cancer grows, spreads, or comes back after treatment.
- These numbers don’t take everything into account. Survival rates are grouped based on how far the cancer has spread, but your age, overall health, type of thymus cancer, whether the entire cancer can be removed, how well the cancer responds to treatment, and other factors can also affect your outlook.
- People now being diagnosed with thymus cancer may have a better outlook than these numbers show. Treatments improve over time, and these numbers are based on people who were diagnosed and treated at least five years earlier.
- Palmieri G, Montella L, Martignetti A, et al.: Somatostatin analogs and prednisone in advanced refractory thymic tumors. Cancer 94 (5): 1414-20, 2002.[↩]
- Urgesi A, Monetti U, Rossi G, et al.: Aggressive treatment of intrathoracic recurrences of thymoma. Radiother Oncol 24 (4): 221-5, 1992.[↩]
- Marx A, Chan JKC, Chalabreysse L, Dacic S, Detterbeck F, French CA, Hornick JL, Inagaki H, Jain D, Lazar AJ, Marino M, Marom EM, Moreira AL, Nicholson AG, Noguchi M, Nonaka D, Papotti MG, Porubsky S, Sholl LM, Tateyama H, Thomas de Montpréville V, Travis WD, Rajan A, Roden AC, Ströbel P. The 2021 WHO Classification of Tumors of the Thymus and Mediastinum: What Is New in Thymic Epithelial, Germ Cell, and Mesenchymal Tumors? J Thorac Oncol. 2022 Feb;17(2):200-213. https://www.jto.org/article/S1556-0864(21)03258-5/pdf[↩]
- Okumura M, Shiono H, Inoue M, et al.: Outcome of surgical treatment for recurrent thymic epithelial tumors with reference to world health organization histologic classification system. J Surg Oncol 95 (1): 40-4, 2007[↩]
- Ruffini E, Mancuso M, Oliaro A, et al.: Recurrence of thymoma: analysis of clinicopathologic features, treatment, and outcome. J Thorac Cardiovasc Surg 113 (1): 55-63, 1997[↩]
- Bonomi PD, Finkelstein D, Aisner S, et al.: EST 2582 phase II trial of cisplatin in metastatic or recurrent thymoma. Am J Clin Oncol 16 (4): 342-5, 1993.[↩]
- Loehrer PJ Sr, Wang W, Johnson DH, et al.: Octreotide alone or with prednisone in patients with advanced thymoma and thymic carcinoma: an Eastern Cooperative Oncology Group phase II trial. J Clin Oncol 22 (2): 293-9, 2004[↩][↩]
- Harper PG, Highly M, Rankin E, et al.: Ifosfamide monotherapy demonstrates high activity in malignant thymoma. [Abstract] Proceedings of the American Society of Clinical Oncology 10: A-1049, 300, 1991[↩]
- Fornasiero A, Daniele O, Ghiotto C, et al.: Chemotherapy for invasive thymoma. A 13-year experience. Cancer 68 (1): 30-3, 1991[↩]
- Loehrer PJ Sr, Wang W, Johnson DH, et al.: Octreotide alone or with prednisone in patients with advanced thymoma and thymic carcinoma: an Eastern Cooperative Oncology Group phase II trial. J Clin Oncol 22 (2): 293-9, 2004.[↩]
- Cucchiara BL, Forman MS, McGarvey ML, et al.: Fatal subacute cytomegalovirus encephalitis associated with hypogammaglobulinemia and thymoma. Mayo Clin Proc 78 (2): 223-7, 2003.[↩]
- Morgenthaler TI, Brown LR, Colby TV, et al.: Thymoma. Mayo Clin Proc 68 (11): 1110-23, 1993[↩]
- Cameron RB, Loehrer PJ, Thomas CR Jr: Neoplasms of the mediastinum. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2011, pp 871-81[↩]
- Schmidt-Wolf IG, Rockstroh JK, Schüller H, et al.: Malignant thymoma: current status of classification and multimodality treatment. Ann Hematol 82 (2): 69-76, 2003.[↩]
- Robinson SP, Akhondi H. Thymoma. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559291[↩][↩][↩][↩][↩]
- Rubinstein MM, Goss C, Avecilla ST, Dubé GP, Riely GJ, Mones JV. Management of thymoma-associated pure red cell aplasia: A novel use of blood substitute HBOC-201 in a Jehovah’s Witness. Clin Case Rep. 2019 Dec 26;8(2):289-292. doi: 10.1002/ccr3.2626[↩]
- Sideris A, Huang J. Commentary: Toward a better understanding of the natural history of surgically treated thymoma associated with paraneoplastic syndromes. J Thorac Cardiovasc Surg. 2020 Jul;160(1):316-317. doi: 10.1016/j.jtcvs.2019.12.059[↩]
- Rajan A, Zhao C. Deciphering the biology of thymic epithelial tumors. Mediastinum. 2019 Sep;3:36. doi: 10.21037/med.2019.08.03[↩]
- Hashimoto S, Hayasaka K, Suzuki K, Endoh M, Yanagawa N, Shiono S. Thymic Small Cell Carcinoma Associated With Lambert-Eaton Myasthenic Syndrome. Ann Thorac Surg. 2020 May;109(5):e347-e348. doi: 10.1016/j.athoracsur.2019.08.080[↩]
- Thymus gland cancer. https://www.cancerresearchuk.org/about-cancer/thymus-gland-cancer[↩]
- Thymus Cancer Stages. https://www.cancer.org/cancer/thymus-cancer/detection-diagnosis-staging/staging.html[↩]
- Ruffini E, Fang W, Guerrera F, Huang J, Okumura M, Kim DK, Girard N, Billè A, Boubia S, Cangir AK, Detterbeck F, Falkson C, Filosso PL, Giaccone G, Kondo K, Infante M, Lucchi M, Marino M, Marom EM, Nicholson AG, Rimner A, Rami-Porta R, Asamura H; Staging and Prognostic Factors Committee; Staging and Prognostic Factors-Thymic Domain Subcommittee; Staging and Prognostic Factors Subcommittees; Members of the Advisory Boards. The International Association for the Study of Lung Cancer Thymic Tumors Staging Project: The Impact of the Eighth Edition of the Union for International Cancer Control and American Joint Committee on Cancer TNM Stage Classification of Thymic Tumors. J Thorac Oncol. 2020 Mar;15(3):436-447. doi: 10.1016/j.jtho.2019.11.013[↩]
- Evoli A, Minisci C, Di Schino C, et al.: Thymoma in patients with MG: characteristics and long-term outcome. Neurology 59 (12): 1844-50, 2002[↩]
- Buckley C, Newsom-Davis J, Willcox N, et al.: Do titin and cytokine antibodies in MG patients predict thymoma or thymoma recurrence? Neurology 57 (9): 1579-82, 2001[↩]
- Engels EA, Pfeiffer RM: Malignant thymoma in the United States: demographic patterns in incidence and associations with subsequent malignancies. Int J Cancer 105 (4): 546-51, 2003.[↩][↩]
- Ogawa K, Toita T, Uno T, et al.: Treatment and prognosis of thymic carcinoma: a retrospective analysis of 40 cases. Cancer 94 (12): 3115-9, 2002.[↩]
- Schmidt-Wolf IG, Rockstroh JK, Schüller H, et al.: Malignant thymoma: current status of classification and multimodality treatment. Ann Hematol 82 (2): 69-76, 2003[↩]
- Eng TY, Fuller CD, Jagirdar J, et al.: Thymic carcinoma: state of the art review. Int J Radiat Oncol Biol Phys 59 (3): 654-64, 2004.[↩]
- Survival Rates for Thymus Cancer. https://www.cancer.org/cancer/thymus-cancer/detection-diagnosis-staging/survival-rates.html[↩]

{kind=link}