Contents
What is cervical dystonia
Cervical dystonia, also known as spasmodic torticollis, is a painful neurological condition characterized by excessive pulling of the muscles of the neck and shoulder resulting in abnormal movements of the head (dystonia). Over 60% of people with cervical dystonia will need analgesics to manage the pain associated with the condition. Dystonia is the term used to describe uncontrollable and sometimes painful muscle spasms caused by incorrect signals from the brain leading to twisting movements or abnormal postures. Cervical dystonia is the most common form of dystonia and it is characterized by involuntary muscle contractions in the neck that cause abnormal movements and postures of the neck and head. Cervical dystonia is a type of focal dystonia (where only one body part is affected) that affects the neck muscles. The spasms and contractions may either be sustained or continuous or may come and go resembling tremor. Involuntary contractions and spasms in the neck muscles can range from mild to severe and cause your head and neck to twist or be pulled forwards, backwards or from side to side. In cervical dystonia, most commonly, the head turns to one side or the other 1. The turning or tilting movements may be accompanied by shaking movement (tremor) and/or soreness of the muscles of the neck and shoulders.
The most common type of twisting associated with cervical dystonia is when your chin is pulled toward your shoulder. Some people experience a combination of abnormal head postures. A jerking motion of the head also may occur.
Many people who have cervical dystonia also experience neck pain that can radiate into the shoulders. The disorder also can cause headaches. In some people, the pain from cervical dystonia can be exhausting and disabling.
In society, there is a lot of prejudice and stigmatization associated with the condition, and as a result a large proportion of people with cervical dystonia are depressed and socially withdrawn. Reports indicate that 25 to 40% of people with cervical dystonia are unemployed due to their disability, which also contributes to their depression.
The severity of cervical dystonia can vary, but the disorder can cause significant neck pain, stiffness and discomfort as well as difficulty due to the abnormal postures. It can affect quality of life and activities of daily living including employment. The symptoms of cervical dystonia can sometimes be relieved by touching your chin, neck or the back of your head. The reasons for this are unclear.
Cervical dystonia typically begins in middle age, and rarely begins in adolescence and young adulthood. The cause of cervical dystonia is unknown, although a genetic susceptibility is thought to underlie some cases. If cervical dystonia begins in infancy or early childhood, secondary causes should be investigated.
Cervical dystonia affects women approximately twice as often as men. It is the most common form of focal dystonia in an office setting. Cervical dystonia may affect individuals of any age, but typically develops in people between 40 and 60 years of age. Cervical dystonia affects people of all ethnic backgrounds. The exact incidence or prevalence of cervical dystonia in the general population is unknown but is estimated to be about 60,000 people in the United States.
It is very rare for children to develop cervical dystonia. If a child experiences twisting of the neck it is likely to be a similar but separate condition known as congenital torticollis. Congenital torticollis is present in some babies at birth. A muscle in the neck is shortened which causes their head to be tilted to the side. This condition can commonly be improved with physical therapy.
Some 5 to 21% of people with cervical dystonia experienced trauma or injury to the neck or head before they experienced cervical dystonia. However, this does not mean that these people contracted the condition as a result of the trauma. It is still largely unknown whether traumatic events cause the dystonia or act as a trigger for a dormant pre-existing condition. cervical dystonia that occurs after brain or neck injury is clinically different from other forms of the condition. In particular, post-injury cervical dystonia does not improve after sleep, and the head and neck tend to have a more limited range of motion.
Cervical dystonia often begins slowly and usually reaches a plateau over a few months or years 2. The cause of cervical dystonia is often unknown. In some cases there is a family history. Several genes have been associated with cervical dystonia, including GNAL, THAP1, CIZ1, and ANO3 3. Other cases may be linked to an underlying disease (e.g. Parkinson disease), neck trauma, or certain medications. Treatment may include local injections of botulinum toxin, pain medications, benzodiazepines (anti-anxiety medications), anticholinergics, physical therapy, or surgery.
Cervical dystonia may be classified as “primary” or “secondary.” Primary dystonia refers to dystonia with no clear identifiable cause and is referred to as idiopathic. In primary dystonia, there is no known structural abnormality in the central nervous system, and no underlying disease present. Primary cervical dystonia is associated with a hereditary component in approximately 12% of cases, and it may possibly be linked to previous neck injury.
Secondary dystonia occurs as a consequence or symptom of an underlying abnormality or disease (e.g. Parkinson disease) and has a clear cause which can be inherited or acquired. Cervical dystonia may be linked to the use of certain medications (e.g. neuroleptics), excessive toxin ingestion (e.g. in carbon monoxide poisoning), or structural lesions due to trauma (primarily of the basal ganglia).
Other names for Cervical Dystonia
- focal dystoniaidiopathic cervical dystonia
- isolated (formally primary) cervical dystonia
- spasmodic torticollis
- spasmodic wryneck
- torticollis
Cervical dystonia classification
Cervical dystonia can be classified as focal or generalized.
- Focal cervical dystonia is the most common and affects a small muscle group in the neck.
- Generalized cervical dystonia typically starts at an earlier age and is widespread throughout the cervical spine.
Cervical dystonia can also be classified either as a primary or a secondary symptom.
Primary cervical dystonia
Cervical dystonia is said to be primary when it is not a symptom associated with any other neurological (brain) condition but is a disorder on its own. The cause of primary cervical dystonia is still largely unknown. Commonly people with cervical dystonia will have a family history of movement disorders which suggests a genetic factor however no specific information on genes has been identified yet.
Secondary cervical dystonia
Cervical dystonia is said to be secondary when it is caused by other neurological conditions. There can be many different causes of secondary cervical dystonia symptoms but whether they are truly causes of cervical dystonia or simply triggers that activate the disorder remains to be determined. cervical dystonia can evolve after the following physiological events or diseases:
- Neck or head injury – after the injury cervical dystonia can occur immediately or up to 12 months after the event;
- Cervical dystonia can be a secondary symptom associated with Parkinsons disease and associated Parkinsonian disorders;
- Cervical dystonia can be a secondary symptom of Wilsons disease;
- Abnormal birth;
- Abnormal development history;
- Abnormalities present at birth such as abnormal head and neck shape are associated with the very rare cases of childhood cervical dystonia;
- Exposure to toxins; or
- Use of older neuroleptics, anti-nausea medication or anti-vertigo medication.
Cervical dystonia causes
In most cases of cervical dystonia, the cause is unknown. Cervical dystonia is classified as an isolated dystonia or primary dystonia if there are no other associated abnormal findings, such as spasticity, Parkinsonism or ataxia. Most isolated cervical dystonia had no identifiable underlying causes. However, in some cases, cervical dystonia can arise from another underlying cause and be considered secondary cervical dystonia (occurring as consequence of another disorder or condition). In most cases, primary cervical dystonia (isolated cervical dystonia) is idiopathic although a genetic susceptibility may be present as evidenced by a positive family history in approximately 10-25% of cases. There are several gene mutations associated with cervical dystonia (GNAL, THAP1, CIZ1, ANO3) and several possible environmental factors. The genes responsible for these types of dystonia are passed down through families in a pattern that’s known as autosomal dominant. This means if you have one of these abnormal genes, there’s a one in two chance your children will inherit that gene and develop dystonia. However, at this time there is no gene test that is recommended for clinical purposes in people with cervical dystonia. Some cases of cervical dystonia may have an identifiable cause (secondary cervical dystonia). In these cases, cervical dystonia may develop due to the use of certain drugs such as anti-psychotics or certain nausea medications with dopamine receptor blocking activity.
In most secondary cervical dystonia, such as those due to toxins or degenerative brain diseases, there are additional signs and symptoms other than cervical dystonia. Whether trauma to the neck could cause cervical dystonia remains controversial. Cervical dystonia is a neurological disorder. However there are some non-neurological conditions that may mimic cervical dystonia. In children with slippage of the vertebrae in the neck (atlanto-axial subluxation), there may be a twisting of the head that is very painful and requires specialized orthopedic treatments. Some infants are born with a shortening of one of the muscles in the neck (congenital infantile torticollis) that causes a head turn. Is some children with esophageal reflux, there can also be posturing of the head. There are additional conditions, including functional movement disorders that may appear similar to cervical dystonia but are non-neurologic in origin.
Secondary dystonia
Secondary dystonia, also known as acquired dystonia, can have a wide range of causes, including:
- Parkinson’s disease – a neurological condition caused by the lack of a neurotransmitter called dopamine
- Huntington’s disease – a genetic condition that can lead to psychiatric problems and difficulties with behaviour, feeding, communication and abnormal movements
- Wilson’s disease – a genetic condition that leads to a build-up of copper in the body’s tissues
- Multiple sclerosis (MS) – a condition caused by damage to the nervous system
- Cerebral palsy – a condition caused by brain damage that occurs before or soon after birth
- Certain medications – such as antipsychotics (used to treat certain mental health conditions) or anticonvulsants (used to treat epilepsy) which can cause dystonia in a small number of people
- Infections – such as HIV or encephalitis
- Injury – to the skull or spine
- Brain tumours
- Stroke– a serious medical condition, where the blood supply to part of the brain is cut off
- Poisoning – such as carbon monoxide poisoning
Risk factors for cervical dystonia
Risk factors for cervical dystonia include:
- Age. While the disorder can occur in people of any age, it most commonly begins after age 30.
- Your sex. Women are more likely to develop cervical dystonia than are men.
- Family history. If a close family member has cervical dystonia or some other type of dystonia, you are at higher risk of developing the disorder.
Cervical dystonia complications
In some cases, the involuntary muscle contractions associated with cervical dystonia can spread to nearby areas of your body. The most common locations include the face, jaw, arms and trunk.
People who have cervical dystonia also may develop bone spurs that may reduce the amount of space in the spinal canal. This can cause tingling, numbness and weakness in your arms, hands, legs or feet.
Cervical dystonia prognosis (outlook)
Like all neurological illnesses, the expression and presentation of cervical dystonia between different people is highly varied.
Around 10% of people will experience pain in the craniocervical region before the onset of dystonia symptoms. Once symptoms of cervical dystonia begin, they will usually worsen for an average of 5 years before plateauing. 10-20% of people experience a reduction of symptoms, but they are highly likely to reoccur, sometimes even years later. In some people, the dystonia may spread beyond the craniocervical region.
Up to 75% of people with cervical dystonia will at some stage experience widespread pain over the neck and shoulders. The pain is described as diffuse and exhausting, and branches out from the direction that the head is twisted. The degree of pain is related to the degree of muscle contraction and the spasms experienced.
It has been shown that stress can worsen the symptoms of cervical dystonia. Therefore, people who feel self-conscious and stressed about their condition are likely to experience a more severe form of the illness. Physical activity and physical exertion are also shown to worsen symptoms.
A large proportion of people with cervical dystonia report depression due to their disability and the disturbed body images associated with the condition. People with cervical dystonia largely feel their social relationships are negatively affected, which in turn reduces their motivation to socialize.
Cervical dystonia symptoms
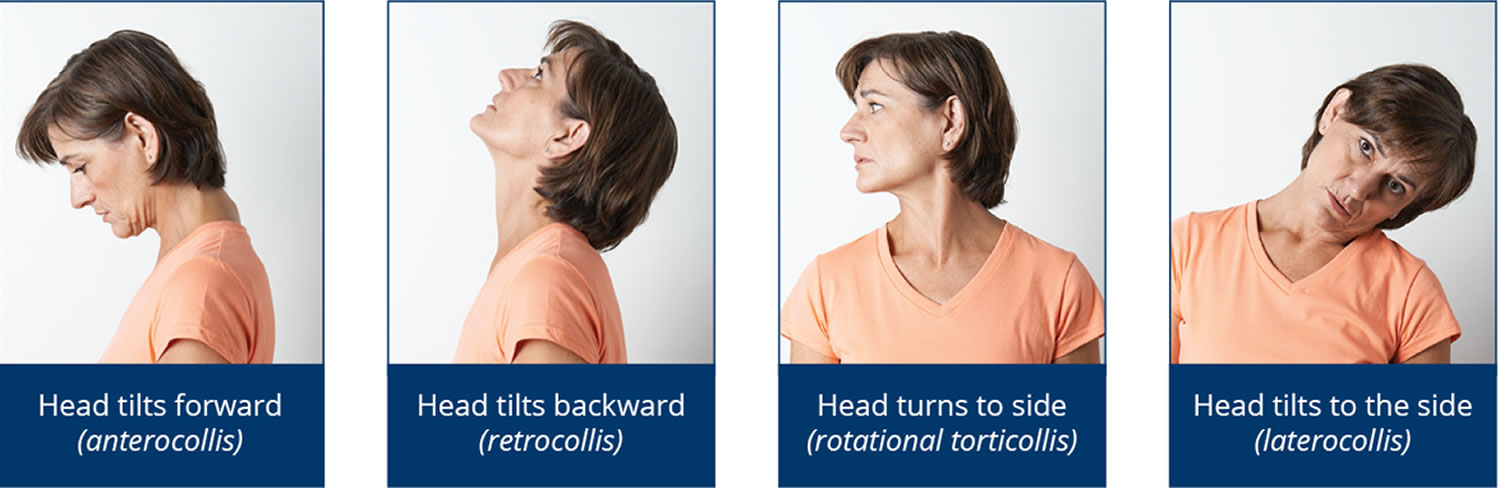
The symptoms of cervical dystonia may begin slowly and can involve any of the muscles of the neck. The head posture in cervical dystonia can vary. The most common abnormal posture associated with cervical dystonia is the twisting of the chin toward a shoulder so that the head rotates sideways (torticollis). Other abnormal postures associated with cervical dystonia including anterocollis, in which the head tips forward; retrocollis, in which the head is tilted backward; or laterocollis, in which the head tilts toward one side. There can also be shifting of the head on the shoulders in a forward (anterior sagittal shift) or backward (posterior sagittal shift) direction. Often cervical dystonia is complex and combines several angles of head movement. In some people with isolated cervical dystonia, there may also be a postural tremor of the hands. Symptoms of cervical dystonia vary over the course of the disorder. Studies of the natural history of cervical dystonia are needed to better understand the natural history of this disorder.
Symptoms may temporarily worsen with stress or excitement. The dystonia can be activated by certain postures or positions. This varies in individual patients. Symptoms may improve with the performance of sensory tricks, such as touching the cheek or the back of the head. A small percentage of individuals experience a spontaneous recovery (remission) after symptom onset. This remission is often temporary, lasting days to years, with recurrence of symptoms. It is likely that less than 1 percent of affected individuals have permanent remissions.
There can be secondary problems arising from cervical dystonia that include cervical spine arthritis, compression of nerve roots, and sometimes narrowing of the spinal cord in the neck (cervical stenosis). Pain related directly to cervical dystonia typically is on the same side as the head turn and is felt as muscular pain in the area of the overactive muscles. Pain can potentially become severe and disabling.
People with dystonia may show a wide and diverse array of features that can include the following in varying degrees:
- Unusual posture, postural responses and postural control;
- Abnormal vestibular functioning;
- Altered perception of body orientation in space;
- Head jerking;
- “Sensory tricks” for relieving muscle tension (e.g. gently touching the face, neck or head at a specific place);
- Neck spasms and neck pain;
- Head rotation (twisting neck), including rotational torticollis and head tilt.
Almost all people with cervical dystonia consider it to be a disability, predominantly due to the pain experienced as a result of muscle overactivity. Individuals with cervical dystonia report that it has a significant negative impact on their quality of life.
Cervical dystonia diagnosis
Diagnosing cervical dystonia isn’t straightforward. It involves using a stepwise approach that starts by identifying the precise nature and specific features of your movement disorders.
A diagnosis of cervical dystonia is based upon clinical examination, a detailed patient history, and knowledge of the disorder.
The specialist will try to identify which type of dystonia classification your movement disorders fall into, taking into consideration a number of factors, including:
- how old you were when your symptoms started
- the order in which your symptoms developed
- the speed at which the condition is progressing
- the results of initial tests and investigations
It’s important to confirm whether you have primary or secondary dystonia to help determine the type of treatment you need.
In primary dystonia, muscle spasms are the only symptom and there’s no other associated condition. Secondary dystonia is caused by an underlying health condition, injury or some other type of damage.
No specific laboratory or imaging test confirms a diagnosis of cervical dystonia. There are no abnormalities in laboratory or imaging tests. Magnetic resonance imaging (MRI) of the brain is normal, and MRI of the neck does not help with the diagnosis unless compression of the spinal cord is suspected. Electromyography is not indicated unless there are additional signs of nerve irritation.
If you have the typical signs of late-onset focal dystonia, you may not need to have specific investigations. However, you may need to have a series of tests and examinations to confirm whether you have primary or secondary dystonia.
These tests are described below:
- Your recent medical and family history will be discussed – for example, whether you’ve recently had a head injury, or whether you have a relative with dystonia.
- Urine and blood tests – to check how well your organs, such as your liver, are functioning and whether you have an infection or high levels of toxins in your body.
- Genetic testing – a DNA sample can be taken from your blood and checked for the abnormal genes associated with some types of dystonia; genetic testing can also confirm whether your dystonia is caused by a genetic condition, such as Huntington’s disease.
- A magnetic resonance imaging (MRI) scan – can check whether there’s any damage to your brain, or whether you have a condition that’s affecting your brain, such as a tumor.
If you have early-onset dystonia, you may also be given a course of medication called levodopa. If your symptoms improve significantly after taking levodopa, a diagnosis of dopa-responsive dystonia can be made.
Cervical dystonia treatment
There is no cure for cervical dystonia. There are a number of treatment techniques that can control the involuntary movements and spasms of cervical dystonia, including medication, physiotherapy, and in some cases, surgery.
The aim is to provide relief from the abnormal movements and postures of dystonia, plus any associated pain and discomfort.
In some cases, other conditions that arise as a result of dystonia, such as stress, anxiety or depression, may also need to be treated.
Treatment for dystonia should be based on the individual and their specific needs. As different people respond differently to different treatments, it may be necessary to try several options to find out which one works best.
There are essentially four main types of treatment for dystonia. They are:
- Botulinum toxin
- Medications
- Physiotherapy
- Surgery, including deep brain stimulation (DBS)
These treatments may be used alone or in combination. In addition, physical therapy may provide a helpful complement to medical treatment. In some cases, if there is a trick such as touching the chin, a soft cervical collar may be beneficial.
- Wherever possible, physiotherapy, medication or botulinum medication will be used to treat dystonia rather than surgery, particularly in the case of children and young people.
Not every treatment option for cervical dystonia is successful for all affected individuals. Therefore, no single strategy is appropriate for every case. Most therapies are symptomatic and are intended to relieve spasms, pain and disturbed postures or functions. Identifying the treatment regimen that is most effective in individual cases may require patience and perseverance on the part of the patient and physician.
Cervical dystonia botox
Botulinum toxin injections are the treatment of choice for cervical dystonia. Botulinum toxin is a neurotoxin that is injected into the dystonic neck muscles in small doses. Botulinum toxin works by preventing the nerve from releasing a messenger, called acetylcholine, that tells the muscle to contract. This causes weakness of the muscle. The effect of botulinum toxin on the muscle begins approximately 2-3 days following injection, peaks at around 4 weeks, and provides relief for approximately 2-6 months. Botulinum toxin treatment is not a cure, but rather a symptom treatment. When the effect of botulinum toxin wears off, the symptoms of cervical dystonia recur and another injection is needed to sustain benefit. The site of the injection may feel painful for a few days, but this should soon pass.
Other side effects of botulinum toxin will depend on which part of your body is injected. For example, injections:
- in the neck area may cause swallowing difficulties (dysphagia)
- It is important to seek medical attention immediately if any difficulties in speech, breathing or swallowing occur.
These types of side effects should pass after about a week.
In order for botulinum toxin injections to be successful, it is critical that the injecting physician be well-versed in cervical dystonia, the functional anatomy of the neck muscles, and the type and doses of botulinum toxin to use.
There are now four brands of Botulinum toxin that have been approved by the Food and Drug Administration (FDA) for the treatment of individuals with cervical dystonia. There are three brands of botulinum toxin serotype A, including onabotulinumtoxinA (BOTOX, Allergan Inc.) abobotulinumtoxinA (Dysport, Tercica Inc) and incobotulinumtoxinA (Xeomin, Merz Pharmaceuticals). There is one formulation of botulinum toxin type B called rimabotulinumtoxinB (Myobloc, Solstice, US World Meds). These brands are not interchangeable, and each should be administered as a unique drug. At this time, there is no clinical data that supports the use of one over the other. The most frequent side effects from the injection are swallowing difficulties, pain and sometimes neck weakness. These side effects are usually mild and transient, lasting a few weeks. The FDA has a “black box” warning concerning the use of any of these toxins that indicates that the toxin can spread from the injection site. However, with the doses used for cervical dystonia the clinical effects of spread of toxin are rare.
Medications
Currently, there are no oral medications that are FDA approved for use in dystonia. Among the oral medications used, dopaminergic agents (levodopa), anticholinergic agents (benztropine, trihexyphenidyl), baclofen and clonazepam are the most frequently used. These drugs are usually most effective in children with generalized dystonia. In adults, the side effects of these agents, including memory problems and sedation, often occur before an effective dose can be reached.
There are a number of different medications that can be used to treat dystonia.
Anticholinergics
Anticholinergics are a type of medication that can be used to effectively treat all types of dystonia.
However, they’re mainly used to treat generalised dystonia, because botulinum toxin now tends to be used to treat focal dystonia and segmental dystonia (see below).
Anticholinergics work by blocking the release of a neurotransmitter called acetylcholine, known to cause muscle spasms in some cases of dystonia. Trihexyphenidyl and procyclidine are two examples of anticholinergics.
Side effects of anticholinergics include:
- dry mouth
- constipation
- difficulties urinating
- blurred vision
- memory problems
- confusion
Baclofen
Baclofen is a medication that’s sometimes used to treat spasticity (excessive muscular tension) caused by stroke or multiple sclerosis. However, it’s also helps in treating people with dystonia.
In particular, daily doses of baclofen are effective in treating people with segmental and generalized dystonia, as well as those with oromandibular dystonia.
Common side effects of Baclofen include:
- kidney problems – seek medical advice if you develop symptoms such as sleepiness or lethargy (lack of energy)
- nausea – this may be reduced by taking Baclofen with food or milk
- drowsinesss
- balance and co-ordination problems
- confusion
Intrathecal baclofen
Intrathecal baclofen (e.g. Lioresal Intrathecal) injected in the high cervical spine has shown success in treating cervical dystonia. After treatment, people have reported increased range of motion in the neck muscles, ease of care and improved quality of life. Common side-effects associated with baclofen include injection site reactions and medication related side-effects such as drowsiness, somnolence, dizziness, headache and nausea.
Muscle relaxants
Muscle relaxants are sometimes used to treat cases of dystonia that fail to respond to other types of medication. They work by increasing the levels of a neurotransmitter called gamma-aminobutyric acid (GABA), which helps to relax affected muscles.
Diazepam, lorazepam and clonazepam are all types of muscle relaxants that may be used to treat dystonia.
Depending on the pattern of your symptoms, muscle relaxants can be given by injection (intravenously) or in tablet form (orally).
Side effects of muscle relaxants include:
- drowsiness
- tiredness
- muscle weakness
- dizziness
- impaired co-ordination
These side effects should be temporary and disappear once your body gets used to the medication. If you have symptoms of dizziness, avoid driving and operating heavy machinery.
Don’t suddenly stop taking muscle relaxants. If you do, you’ll experience withdrawal symptoms such as anxiety, sweating or tremors (shaking).
If your care team decides you should stop taking muscle relaxants, your dose will gradually be reduced.
Physiotherapy
Physiotherapy uses specific exercises to help you maintain a full range of motion, improve your posture and prevent the shortening or weakening of affected muscles.
Some people with dystonia find their symptoms improve by simply touching the affected body part or a nearby area. This is known as a “sensory trick” or “geste antagoniste”.
For example, people with cervical dystonia (where the neck muscles spasm and tighten) often find their symptoms improve by touching the back of their head or the side of their face.
Pain management
Many people with certain types of dystonia experience pain, caused by spasms or repeated twisting of joints. You may be referred to a pain management programme to help with managing chronic pain.
Surgery
Surgery may be recommended if your cervical dystonia symptoms don’t respond to botulinum toxin, medication or physiotherapy.
Surgical treatments for cervical dystonia are of two types:
- Deep brain stimulation (DBS) is effective for cervical dystonia and may be appropriate for patients who lose their response to botulinum toxin, or have a form of cervical dystonia that is difficult to treat with the injections, in particular anterocollis. During surgery, two small holes will be drilled into your skull. The surgeon will pass electrodes through each hole and position them in a part of the basal ganglia called the globus pallidus. The basal ganglia is part of the brain that affects muscle movement. The electrodes are connected to stimulators which send small electrical pulses to the brain. Although the precise mechanism is not clear, the electrical impulses seem to “reset” the brain and improve the dystonic movements. After the deep brain stimulation is placed, the stimulators are programmed for the optimal outcome.The most common complication of deep brain stimulation is that either the pulse generator stops working or the electrodes become displaced, which may require further surgery to correct.Deep brain stimulation is a relatively new technique, so there’s little information regarding its long-term safety or effectiveness. Therefore, before deciding to have deep brain stimulation, you should discuss the risks and benefits of the treatment with your surgical team.If you have deep brain stimulation, you’re likely to need a series of follow-up appointments. This is because in most cases the signals produced by the pulse generator need to be adjusted to ensure your symptoms are being properly controlled.
It may be several weeks or months before you begin to feel the benefit of deep brain stimulation. The benefit should continue to increase for a few years following surgery.
- Selective peripheral denervation in which the nerves to the dystonic muscles are cut. During the procedure, the surgeon will make an incision in your neck, before cutting some of the nerves connected to muscles prone to spams. The surgery will be carried out under general anesthetic, which means you’ll be unconscious throughout the procedure and unable to feel pain or discomfort. After the procedure, you’ll lose some feeling in your neck because the nerves have been disconnected. Although this has been reported to be effective, this approach is limited by the ability to access the nerve involved, the need for considerable expertise of the surgeon, and the potential for side effects. Side effects from the surgery are not uncommon and following surgery, there is a long period of rehabilitation. These days the selective peripheral denervation surgery only tends to be used in a few, select cases.
- Possible complications include:
- infection in the neck
- short-term swelling of the neck
- a feeling of pins and needles in the neck
- occasional short episodes of neck pain
Coping and support
Severe cases of cervical dystonia may make you feel uncomfortable in social situations or even limit your abilities to accomplish everyday tasks such as driving. Many people with cervical dystonia feel isolated and depressed.
Stress exacerbates the symptoms of cervical dystonia so learning to manage your stress levels may be an effective way that you can control your condition. Try to relax and take deep breaths when you feel yourself tensing up. Physical therapists and psychologists can help you to develop further techniques that may help.
Social support is also an important part of cervical dystonia therapy. Support groups can provide you with further information about the condition and it will give you a chance to talk to people that understand what you are going through.
Remember that you’re not alone. A number of organizations and support groups are dedicated to providing information and support for you and your family — whether you have the disorder or you have a friend or family member who does.
Your doctor may be able to suggest support groups available in your area, or there are a number of good sites on the internet with information about local support groups.
- Cervical Dystonia. Dystonia Coalition. https://www.rarediseasesnetwork.org/cms/dystonia/Learn-More/Disorder-Definitions[↩]
- Dystonias Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Dystonias-Information-Page[↩]
- Comella CL. Cervical Dystonia. NORD. https://rarediseases.org/rare-diseases/cervical-dystonia/ [↩]





{kind=link}