Contents
What is chagas disease
Chagas disease is caused by the parasite Trypanosoma cruzi, which is transmitted to animals and people by insect vectors triatomine bugs (also known as reduviid or kissing bugs or cone-nose bug or vinchuca – see Figures 1 to 6) – a blood-sucking insect that feeds on humans and animals 1 and is found only in the Americas (mainly, in rural areas of Latin America where poverty is widespread). Chagas disease (Trypanosoma cruzi infection) is also referred to as American trypanosomiasis. Chagas disease is named after the Brazilian physician Carlos Chagas, who discovered the disease in 1909 2.
Chagas disease infection can also occur from:
- mother-to-baby (congenital),
- contaminated blood products (transfusions),
- an organ transplanted from an infected donor,
- laboratory accident, or
- contaminated food or drink (rare)
Chagas disease is endemic throughout much of Mexico, Central America, and South America where an estimated 8 million people are infected 3. The triatomine bug thrives under poor housing conditions (for example, mud walls, thatched roofs), so in endemic countries, people living in rural areas are at greatest risk for acquiring infection. Public health efforts aimed at preventing transmission have decreased the number of newly infected people and completely halted vectorborne transmission in some areas. Infection acquired from blood products, organ transplantation, or congenital transmission continues to pose a threat.
By applying published seroprevalence figures to immigrant populations, the Centers for Disease Control and Prevention (CDC) estimates that more than 300,000 persons with Trypanosoma cruzi infection live in the United States. Most people with Chagas disease in the United States acquired their infections in endemic countries. Although there are triatomine bugs in the U.S., only rare vectorborne cases of Chagas disease have been documented.
The transmission of Chagas disease via blood transfusion is a recognized risk, however screening tests were approved by the Food and Drug Administration and they are currently in use by blood banks. During the acute phase of illness, blood film examination generally reveals the presence of trypomastigotes. During the chronic phase of infection, parasitemia is low; immunodiagnosis is a useful technique for determining whether the patient is infected.
Table 1. Countries where Chagas’ disease is endemic and estimates of the seroprevalence and number of infected inhabitants
| Region | Country where Chagas’ disease is endemica | Estimated seroprevalence (%)b | Estimated no. of infected individualsb |
|---|---|---|---|
| North America | United States | NDA | 300,167c |
| Mexico | 1.03 | 1,100,000 | |
| Central America | Belize | 0.74 | 2,000 |
| Costa Rica | 0.53 | 23,000 | |
| El Salvador | 3.37 | 232,000 | |
| Honduras | 3.05 | 220,000 | |
| Guatemala | 1.98 | 250,000 | |
| Nicaragua | 1.14 | 58,600 | |
| Panama | 0.01 | 21,000 | |
| South America | Argentina | 4.13 | 1,600,000 |
| Bolivia | 6.75 | 620,000 | |
| Brazil | 1.02 | 1,900,000 | |
| Chile | 0.99 | 160,200 | |
| Colombia | 0.96 | 436,000 | |
| Ecuador | 1.74 | 230,000 | |
| Guyana | 1.29 | 18,000 | |
| Suriname | NDA | NDA | |
| French Guiana | NDA | NDA | |
| Paraguay | 2.54 | 150,000 | |
| Peru | 0.69 | 192,000 | |
| Uruguay | 0.66 | 21,700 | |
| Venezuela | 1.16 | 310,000 |
Figure 1. Kissing bug (Triatoma indictiva – female) – which if infected can transmit Trypanosoma cruzi

Figure 2. Kissing bug (Triatoma sanguisuga) – which if infected can transmit Trypanosoma cruzi

Figure 3. Kissing bug (Triatoma rubida – female) – which if infected can transmit Trypanosoma cruzi

Figure 4. Kissing bug (Triatoma gerstaeckeri – female) – which if infected can transmit Trypanosoma cruzi

Figure 5. Kissing bug (Triatoma protracta) – which if infected can transmit Trypanosoma cruzi

Figure 6. Various Triatomine Bugs in all Life Stages
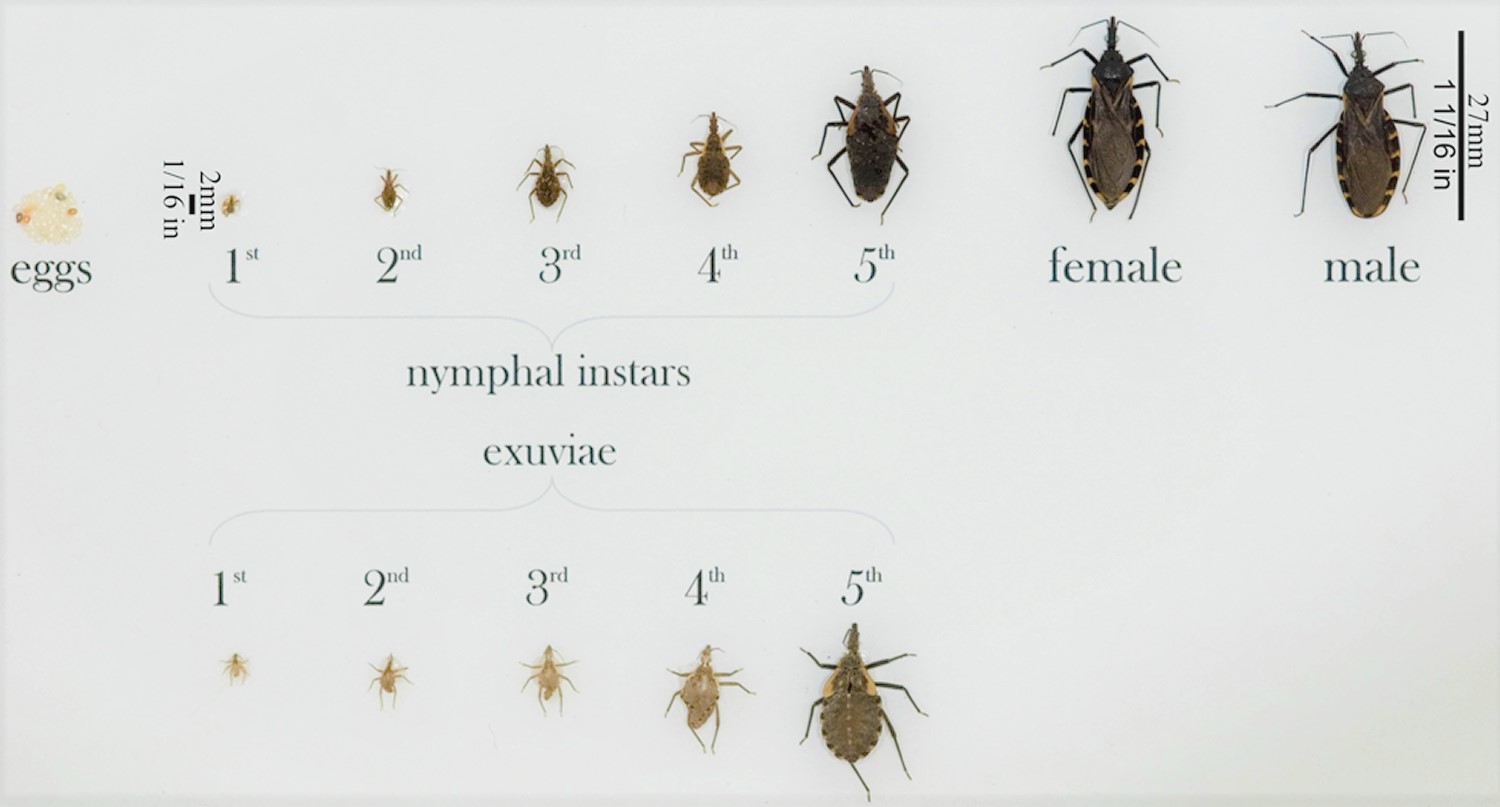
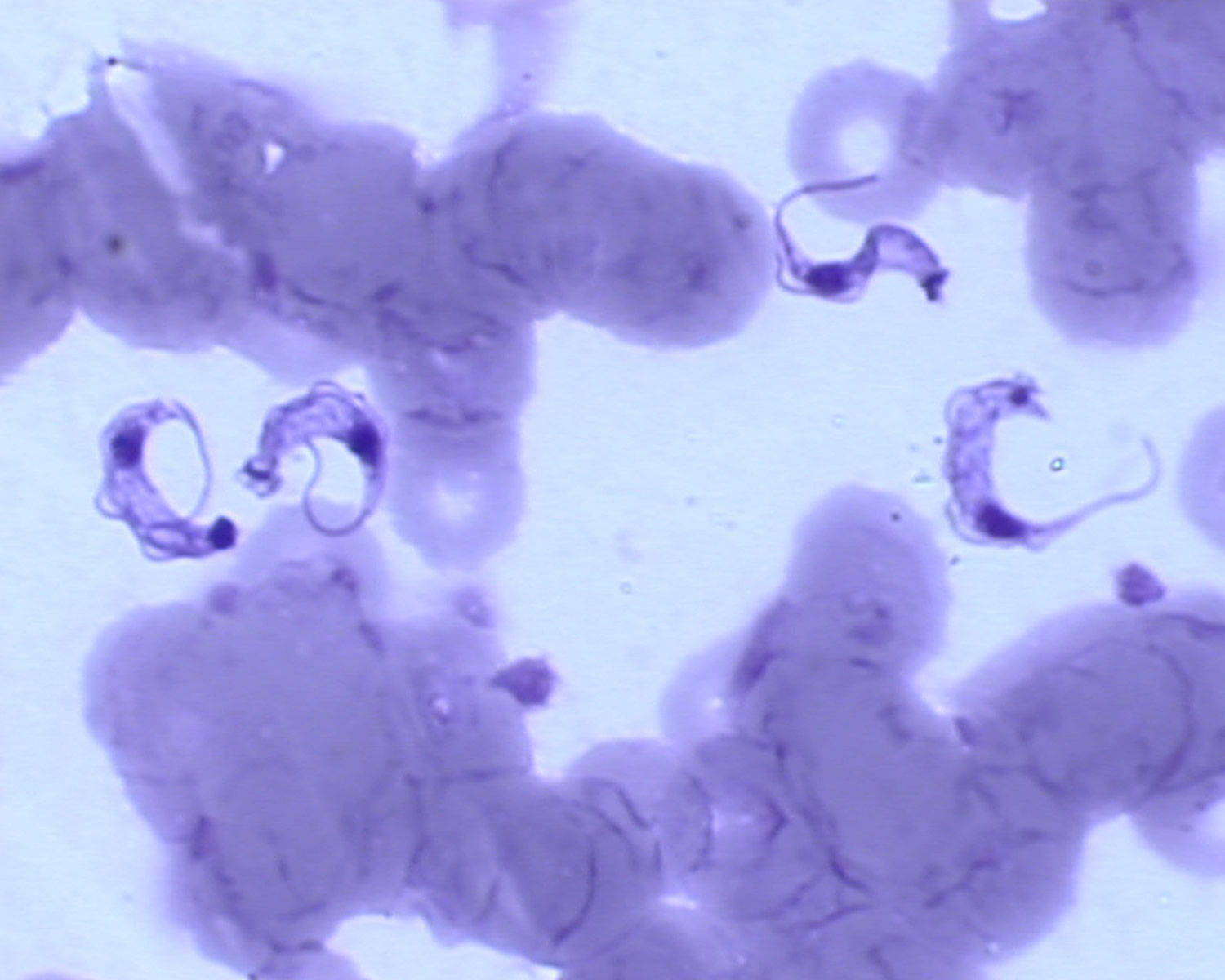
Figure 7. Trypanosoma cruzi trypomastigotes in a thin blood smear

Trypanosoma cruzi Life Cycle
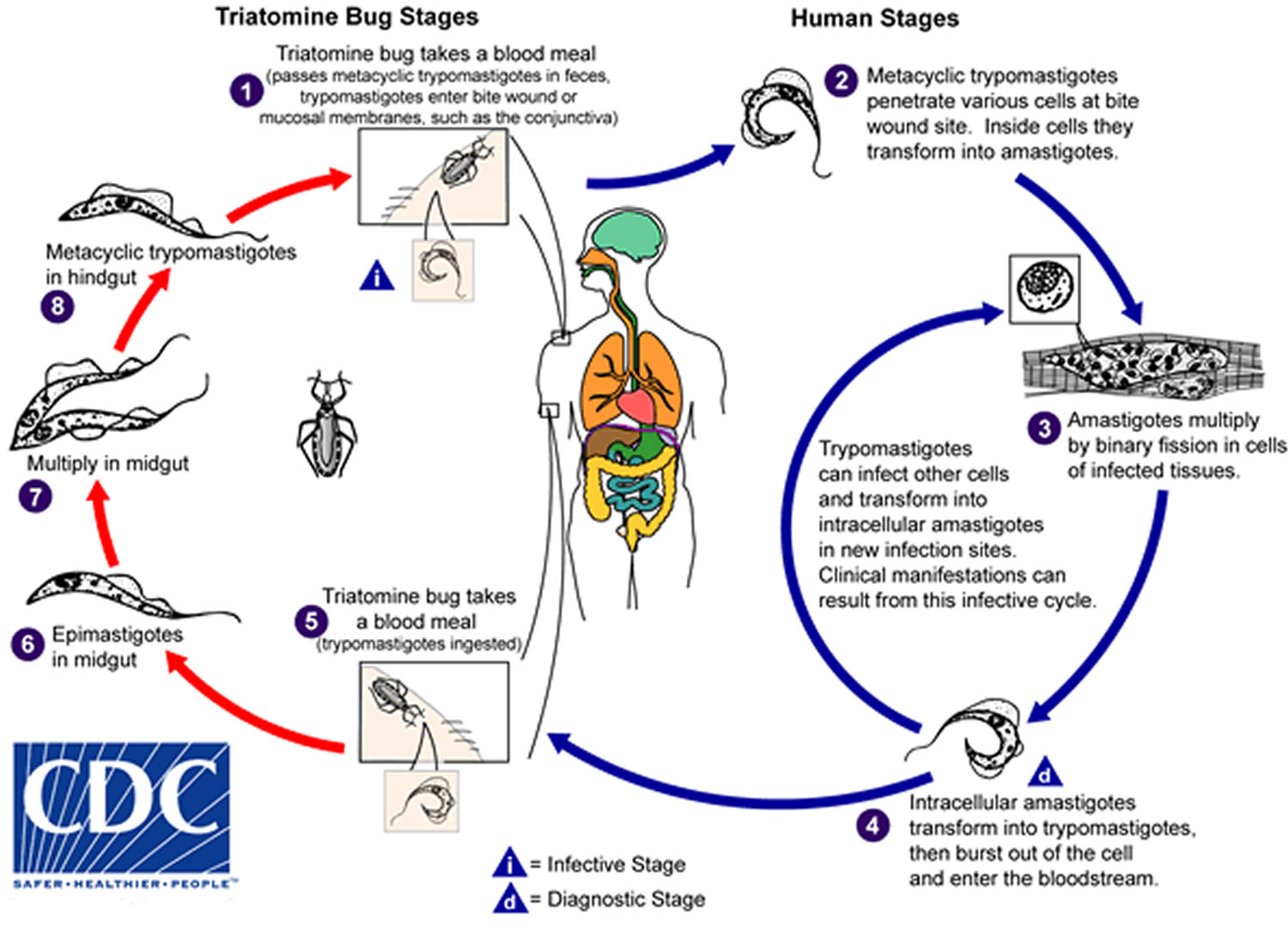
An infected triatomine insect vector (or “kissing” bug) takes a blood meal and releases trypomastigotes in its feces near the site of the bite wound. Trypomastigotes enter the host through the wound or through intact mucosal membranes, such as the conjunctiva (number 1). Common triatomine vector species for trypanosomiasis belong to the genera Triatoma, Rhodnius, and Panstrongylus. Inside the host, the trypomastigotes invade cells near the site of inoculation, where they differentiate into intracellular amastigotes (number 2). The amastigotes multiply by binary fission (number 3) and differentiate into trypomastigotes, and then are released into the circulation as bloodstream trypomastigotes (number 4). Trypomastigotes infect cells from a variety of tissues and transform into intracellular amastigotes in new infection sites. Clinical manifestations can result from this infective cycle. The bloodstream trypomastigotes do not replicate (different from the African trypanosomes). Replication resumes only when the parasites enter another cell or are ingested by another vector. The “kissing” bug becomes infected by feeding on human or animal blood that contains circulating parasites (number 5). The ingested trypomastigotes transform into epimastigotes in the vector’s midgut (number 6). The parasites multiply and differentiate in the midgut (number 7) and differentiate into infective metacyclic trypomastigotes in the hindgut (number 8).
Trypanosoma cruzi can also be transmitted through blood transfusions, organ transplantation, transplacentally, and in laboratory accidents.
Figure 8. Chagas disease lifecycle
Chagas disease causes
The cause of Chagas disease is the parasite Trypanosoma cruzi, which is transmitted from an insect known as the triatomine bug. These insects can become infected by Trypanosoma cruzi when they ingest blood from an animal already infected with the parasite.
Triatomine bugs live primarily in mud, thatch or adobe huts in Mexico, South America and Central America. They hide in crevices in the walls or roof during the day, then come out at night — often feeding on sleeping humans.
Infected bugs defecate after feeding, leaving behind Trypanosoma cruzi parasites on the skin. The parasites can then enter your body through your eyes, mouth, a cut or scratch, or the wound from the bug’s bite.
Scratching or rubbing the bite site helps the parasites enter your body. Once in your body, the parasites multiply and spread.
You may also become infected by:
- Eating uncooked food contaminated with feces from T. cruzi-infected bugs
- Being born to a woman infected with T. cruzi
- Having a blood transfusion containing infected blood
- Getting an organ transplant containing viable T. cruzi
- Working in a laboratory where there’s an accidental exposure to the parasite
- Spending time in a forest that contains infected wild animals, such as raccoons and opossums
Risk factors for Chagas disease
The following factors may increase your risk of getting Chagas disease:
- Living in impoverished rural areas of Central America, South America and Mexico
- Living in a residence that contains triatomine bugs
- Receiving a blood transfusion or organ transplant from a person who carries the infection
It’s rare for travelers to the at-risk areas in South America, Central America and Mexico to contract Chagas disease because travelers tend to stay in well-constructed buildings, such as hotels. Triatomine bugs are usually found in structures built with mud or adobe or thatch.
Where are triatomine bugs typically found?
Triatomine bugs (also called reduviid bugs, “kissing” bugs, cone-nosed bugs, and blood suckers) can live indoors, in cracks and holes of substandard housing, or in a variety of outdoor settings including:
- Beneath porches
- Between rocky structures
- Under cement
- In rock, wood, brush piles, or beneath bark
- In rodent nests or animal burrows
- In outdoor dog houses or kennels
- In chicken coops or houses
They are typically found in the southern United States, Mexico, Central America, and South America (as far south as southern Argentina). The map below details triatomine occurrence by U.S. state.
Eleven different species of triatomine bugs have been found in the southern United States:
- Paratriatoma hirsuta
- Triatoma gerstaeckeri
- Triatoma incrassata
- Triatoma indictiva
- Triatoma lecticularia
- Triatoma neotomae
- Triatoma protracta
- Triatoma recurva
- Triatoma rubida
- Triatoma rubrofasciata
- Triatoma sanguisuga
Triatomines are primarily nocturnal and feed on the blood of mammals (including humans), birds, and reptiles. Triatomine bugs live in a wide range of environmental settings, generally within close proximity to a blood host. In areas of Latin America where human Chagas disease is an important public health problem, the bugs nest in cracks and holes of substandard housing.
Because most indoor structures in the United States are built with plastered walls and sealed entryways to prevent insect invasion, triatomine bugs rarely infest indoor areas of houses. Discovery of immature stages of the bug (wingless, smaller nymphs) inside may be an indication of infestation. When the bugs are found inside, they are likely to be in one of the following settings:
- Near pet resting areas
- In areas of rodent infestation
- In and around beds and bedrooms, especially under or near mattresses or night stands.
Can I get Chagas disease from a triatomine bug?
Yes. However, the transmission of Chagas disease from a bug to a human is not easy. The parasite that causes the disease is in the bug feces. The bug generally defecates on or near a person while it is feeding on his or her blood, generally when the person is sleeping. Transmission occurs when fecal material gets rubbed into the bite wound or into a mucous membrane (for example, the eye or mouth), and the parasite enters the body.
It is important to note that not all triatomine bugs are infected with the parasite that causes Chagas disease. The likelihood of getting Chagas disease from a triatomine bug in the United States is low, even if the bug is infected.
How can I tell if the bug I’ve found is a triatomine and not another kind of bug?
There are many beetles and non-triatomine reduviid bugs that resemble the triatomine bug. Two examples of non-triatomine reduviid bugs that do not feed on human blood are the wheel bug and the western corsair. Some plant-feeding bugs, such as the leaf-footed bug, also resemble the triatomine. If you are unsure if the bug you’ve found is a triatomine, you may wish to consult with an expert, such as an entomologist for clarification.
How can I keep triatomine bugs away from my home?
Synthetic pyrethroid sprays have been used successfully in Latin America to eliminate house infestations. Although similar chemicals are available in the United States, none have been specifically approved for use against triatomine bugs. A licensed pest control operator should be consulted if considering the use of insecticides. Please note that roach hotels or other “bait” formulations do not work against triatomine bugs. Long lasting insecticide treated bednets and curtains have been shown to kill these bugs.
Other precautions to prevent house infestation include:
- Sealing cracks and gaps around windows, walls, roofs, and doors
- Removing wood, brush, and rock piles near your house
- Using screens on doors and windows and repairing any holes or tears
- If possible, making sure yard lights are not close to your house (lights can attract the bugs)
- Sealing holes and cracks leading to the attic, crawl spaces below the house, and to the outside
- Having pets sleep indoors, especially at night
- Keeping your house and any outdoor pet resting areas clean, in addition to periodically checking both areas for the presence of bugs
Could I be allergic to the bite of a triatomine bug?
Yes. The saliva of certain types of triatomines can cause an allergic reaction in some people. An allergic reaction may be characterized by severe redness, itching, swelling, welts, hives, or, rarely, anaphylactic shock (severe allergic reaction). Persons at risk of anaphylactic shock should consult a physician to obtain medication to use in case of a bite. It is important to note that not all triatomines are infected with the parasite even though they may cause an allergic reaction.
The appearance of an allergic reaction after a triatomine bite does not mean that you have been infected with the parasite Trypanosoma cruzi, the cause of Chagas disease. The mild swelling that may develop at the site of parasite inoculation (where the parasite entered the body through the skin or mucous membranes) is called a chagoma. When the parasite enters the body through the conjunctiva of the eye, the swelling around the eye is called Romaña’s sign. Chagomas, including Romaña’s sign, usually last longer than an allergic reaction and are less likely to be severely itchy.
What do I do if I think I may have acquired Chagas disease?
If you suspect you have Chagas disease, consult your health care provider. Or, to find a physician familiar with diagnosis and treatment of Chagas disease and other parasitic infections, ask your general practitioner or primary care physician for a referral. You may wish to consider visiting a physician who specializes in infectious diseases.
Chagas disease prevention
Vaccines against T. cruzi are still being researched and are not yet available
Triatomine insects infest poor-quality dwellings and are most active at night. Travelers who sleep indoors, in well-constructed facilities (e.g. air-conditioned or screened hotel rooms) are at low risk of exposure and infection.
Other preventive measures include spraying infested dwellings with residual insecticides, using bed nets treated with insecticides, wearing protective clothing, and using insect repellant.
If you live in a high-risk area for Chagas disease, these steps can help you prevent infection:
- Avoid sleeping in a mud, thatch or adobe house. These types of residences are more likely to harbor triatomine bugs.
- Use insecticide-soaked netting over your bed when sleeping in thatch, mud or adobe houses.
- Use insecticides to remove insects from your residence.
- Use insect repellent on exposed skin.
In endemic areas of Mexico, Central America, and South America improved housing and spraying insecticide inside housing to eliminate triatomine bugs has significantly decreased the spread of Chagas disease. Further, screening of blood donations for Chagas is another important public health tool in helping to prevent transfusion-acquired disease. Early detection and treatment of new cases, including mother-to-baby (congenital) cases, will also help reduce the burden of disease.
Travelers should be aware of bloodborne and foodborne routes of transmission.
In the United States and in other regions where Chagas disease is now found but is not endemic, control strategies are focused on preventing transmission from blood transfusion, organ transplantation, and mother-to-baby.
Chagas disease symptoms
Chagas disease has an acute and a chronic phase. If untreated, infection is lifelong.
Acute Chagas disease occurs immediately after infection, may last up to a few weeks or months, and parasites may be found in the circulating blood. Infection may be mild or asymptomatic, but can present with manifestations that include fever, anorexia, lymphadenopathy, mild hepatosplenomegaly, and myocarditis. There may be fever or swelling around the site of inoculation (where the parasite entered into the skin or mucous membrane). Romaña’s sign (unilateral palpebral and periocular swelling) may appear as a result of conjunctival contamination with the vector’s feces. A nodular lesion or furuncle, usually called chagoma, can appear at the site of inoculation. Rarely, acute infection may result in severe inflammation of the heart muscle or the brain and lining around the brain.
Most acute cases resolve over a period of a few weeks or months into an asymptomatic chronic form of the disease.
Figure 9. Romaña’s sign – the swelling of the child’s eyelid, is a marker of acute Chagas disease. The swelling is due to bug feces being accidentally rubbed into the eye, or because the bite wound was on the same side of the child’s face as the swelling.

Following the acute phase, most infected people enter into a prolonged asymptomatic form of disease (called “chronic indeterminate”) during which few or no parasites are found in the blood. During this time, most people are unaware of their infection. Many people may remain asymptomatic for life and never develop Chagas-related symptoms. However, an estimated 20 – 30% of infected people will develop debilitating and sometimes life-threatening medical problems over the course of their lives.
The symptomatic chronic form may not occur for years or even decades after initial infection. Its manifestations include cardiomyopathy (the most serious manifestation); pathologies of the digestive tract such as megaesophagus and megacolon; and weight loss. Chronic Chagas disease and its complications can be fatal.
Chagas disease complications
If Chagas disease progresses to the chronic phase, serious heart or digestive complications may occur. These may include:
- Heart failure. Heart failure occurs when your heart becomes so weak or stiff that it can’t pump enough blood to meet your body’s needs.
- Heart rhythm abnormalities that can cause sudden death.
- Enlargement of the esophagus (megaesophagus). This rare condition is caused by the abnormal widening (dilation) of your esophagus, which can result in difficulty with swallowing and digestion.
- Enlargement of the colon (megacolon). Megacolon occurs when your colon becomes abnormally dilated, causing abdominal pain, distention and severe constipation.
In people who have suppressed immune systems (for example, due to AIDS or chemotherapy), Chagas disease can reactivate with parasites found in the circulating blood. This occurrence can potentially cause severe disease.
Chagas disease diagnosis
Your doctor will conduct a physical exam, asking about your symptoms and any factors that put you at risk of Chagas disease.
If you have the signs and symptoms of Chagas disease, blood tests can confirm the presence of the T. cruzi parasite or the proteins that your immune system creates (antibodies) to fight the parasite in your blood.
The diagnosis of Chagas disease can be made by observation of the parasite (trypomastigotes) in a blood smear by microscopic examination (see Figure 7 above) or cerebral spinal fluid (CSF). A thick and thin blood smear are made and stained for visualization of parasites. However, a blood smear works well only in the acute phase of infection when parasites are seen circulating in blood.
If you’re diagnosed with Chagas disease, you’ll likely undergo additional tests to determine whether the disease has entered the chronic phase and caused heart or digestive complications. These tests may include:
- Electrocardiogram, a procedure that records the electrical activity of your heart
- Chest X-ray, which lets your doctor see if your heart is enlarged
- Echocardiogram, a test that uses sound waves to capture moving images of your heart, allowing your doctor to see any changes to the heart or its function
- Abdominal X-ray, a procedure that uses radiation to capture images of your stomach, intestines and colon
- Upper endoscopy, a procedure in which you swallow a thin, lighted tube (endoscope) that transmits images of your esophagus onto a screen
During the chronic stage, trypomastigotes are usually not found circulating in blood and serologic testing is recommended. Amastigotes may be found in biopsy specimens stained with hematoxylin-and-eosin (H&E) or Giemsa.
Diagnosis of chronic Chagas disease is made after consideration of the patient’s clinical findings, as well as by the likelihood of being infected, such as having lived in an endemic country. Diagnosis is generally made by testing with at least two different serologic tests.
The indirect fluorescent antibody (IFA) test and a commercial enzyme immuno assay (EIA) are available at CDC. When using this test cross-reactivity can occur with sera from patients with leishmaniasis, a protozoan disease that occurs in some of the same geographical areas as T. cruzi. CDC also utilizes an FDA-cleared enzyme immunoassay (EIA). This assay uses recombinant antigens for antibody detection and provides additional information to inform the diagnosis. Various serologic methods are commercially available in other countries for laboratory diagnosis of Chagas disease. The sensitivity and specificity of these tests are highly variable. CDC recommends confirmatory testing if positive or negative results obtained elsewhere are suspicious.
Molecular Testing
Molecular diagnosis of Chagas disease is performed for cases of transfusion or transplant transmission are suspected and for congenital Chagas. Laboratory exposures can also be monitored using PCR. At CDC molecular detection of T. cruzi DNA is performed using a combination of three real-time PCR assays. Acceptable specimen types are EDTA blood (minimum of 2.2 ml), heart biopsy tissue (in saline or paraffin-embedded) and, in cases of suspected cerebral involvement, CSF. Using PCR to detect Trypanosoma cruzi DNA in EDTA blood is appropriate only when the parasitemia is expected to be high, such as in the acute phase of the infection or in re-activation of chronic Chagas disease due to immunosuppression. PCR can also be useful for early detection of T. cruzi in transplant-transmitted recipients of organs from donors with chronic Chagas disease. The diagnosis of chronic Chagas disease in patients without immunosuppression should be performed with serology.
Chagas disease treatment
Treatment for Chagas disease is recommended for people diagnosed early in the course of infection (acute phase), congenital infection, and for those with suppressed immune systems. Many patients with chronic infection may also benefit from treatment.
There are two approaches to therapy of Chagas disease: antiparasitic treatment and symptomatic treatment.
Antiparasitic treatment
Antiparasitic treatment is indicated for all cases of acute or reactivated Chagas disease due to impaired immunity and for chronic Trypanosoma cruzi infection in children up to age 18. Congenital infections are considered acute disease. Children with indeterminate-phase Chagas disease may also benefit from antiparasitic treatment. Treatment is strongly recommended for adults up to 50 years old with chronic infection who do not already have advanced Chagas cardiomyopathy. For adults older than 50 years with chronic T. cruzi infection, the decision to treat with antiparasitic drugs should be individualized, weighing the potential benefits and risks for the patient. Physicians should consider factors such as the patient’s age, clinical status, preference, and overall health. It is thought that adults with long-standing indeterminate-phase disease are unlikely to benefit from antiparasitic treatment, although more scientific studies are needed.
The two drugs used to treat infection with Trypanosoma cruzi are nifurtimox and benznidazole. Benznidazole is approved by FDA for use in children 2–12 years of age but is not yet available in U.S. pharmacies. Nifurtimox is not currently FDA approved. Both drugs are currently available under investigational protocols from Centers for Disease Control and Prevention (CDC).
Once Chagas disease reaches the chronic phase, medications won’t cure the disease. But, the drugs may be offered to people younger than age 50 because they may help slow the progression of the disease and its most serious complications.
Antiparasitic medications have significant side effects and offer no benefits in patients with established cardiac or gastrointestinal complications of chronic Chagas disease. Side effects are fairly common with both drugs and tend to be more frequent and more severe with increasing age.
Common side effects of benznidazole treatment include:
- allergic dermatitis
- peripheral neuropathy
- anorexia and weight loss
- insomnia
The most common side effects of nifurtimox are:
- anorexia and weight loss
- polyneuropathy
- nausea
- vomiting
- headache
- dizziness or vertigo
Contraindications for treatment include severe hepatic and/or renal disease. As safety for infants exposed through breastfeeding has not been documented, withholding treatment while breastfeeding is also recommended. The following table outlines recommended dosage regimens by age group:
Table 2. Antiparasitic treatment
| Drug | Age group | Dosage and duration |
|---|---|---|
| Benznidazole | < 12 years | 5-7.5 mg/kg per day orally in 2 divided doses for 60 days |
| 12 years or older | 5-7 mg/kg per day orally in 2 divided doses for 60 days | |
| Nifurtimox | ≤ 10 years | 15-20 mg/kg per day orally in 3 or 4 divided doses for 90 days |
| 11-16 years | 12.5-15 mg/kg per day orally in 3 or 4 divided doses for 90 days | |
| 17 years or older | 8-10 mg/kg per day orally in 3 or 4 divided doses for 90 days |
Symptom-specific supportive measures are used to treat chronic disease, such as:
- Pacemakers or antiarrhythmic drugs for patients with heart rhythm abnormalities
- Special diets, laxatives, and surgical procedures for patients with gastrointestinal complications
- Triatomine Testing. http://www.dshs.texas.gov/idcu/health/zoonosis/Triatominae/[↩]
- Chagas C. 1909. Nova tripanosomiaze humana. Estudos sobre morfolojia e o ciclo evolutivo do Schizotrypanum cruzi n.g., n. sp., ajente etiolojico de nova entidade morbida do homen. Mem. Inst. Oswaldo Cruz 1:159–218[↩]
- Parasites – American Trypanosomiasis (also known as Chagas Disease). https://www.cdc.gov/parasites/chagas/epi.html[↩]
- Bern C, Kjos S, Yabsley MJ, Montgomery SP. Trypanosoma cruzi and Chagas’ Disease in the United States. Clinical Microbiology Reviews. 2011;24(4):655-681. doi:10.1128/CMR.00005-11. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3194829/[↩]





{kind=link}