
Contents
- What is chemotherapy
- When chemotherapy is used
- Chemotherapy types
- How does chemotherapy work
- Chemotherapy drugs
- Getting Chemotherapy
- Issues during chemotherapy treatment
- Chemotherapy success rate
- Chemotherapy for breast cancer
- FOLFOX chemotherapy
- Chemotherapy side effects
What is chemotherapy
Chemotherapy also called chemo is a cancer treatment where powerful chemicals, medicines or drugs is used to kill fast-growing cancer cells in your body. Chemotherapy is most often used to treat cancer, since cancer cells grow and multiply much more quickly than most cells in the body. Surgery and radiation therapy remove, kill, or damage cancer cells in a certain area, but chemotherapy can work throughout the whole body. This means chemotherapy can kill cancer cells that have spread (metastasized) to parts of the body far away from the original (primary) tumor.
Chemotherapy may be used to:
- Keep the cancer from spreading
- Make the cancer grow slower
- Kill cancer cells that may have spread to other parts of the body (metastasized)
- Make side effects from cancer better, like pain or blockages
- Cure cancer
There are many different types of chemotherapy medication, but they all work in a similar way. Chemotherapy stop cancer cells reproducing by targeting cells at different phases of the process of forming new cells, called the cell cycle, which prevents them from growing and spreading in the body. Chemotherapy drugs can be used alone or in combination to treat a wide variety of cancers.
Though chemotherapy is an effective way to treat many types of cancer, chemotherapy treatment also carries a risk of side effects. Some chemotherapy side effects are mild and treatable, while others can cause serious complications.
Sometimes chemotherapy is the only treatment you need. More often, chemotherapy is used with surgery or radiation therapy or both. Here’s why:
- Chemotherapy may be used to shrink a tumor before surgery or radiation therapy. Chemotherapy used in this way is called neoadjuvant chemotherapy.
- Chemotherapy may be used after surgery or radiation therapy to help kill any remaining cancer cells. Chemotherapy used in this way is called adjuvant chemotherapy.
- Chemotherapy may be used with other treatments if your cancer comes back.
When chemotherapy is used
Chemotherapy may be used if cancer has spread or there’s a risk it will.
Chemotherapy can be used to:
- try to cure the cancer completely (curative chemotherapy)
- make other treatments more effective – for example, it can be combined with radiotherapy (chemoradiation) or used before surgery (neo-adjuvant chemotherapy)
- reduce the risk of the cancer coming back after radiotherapy or surgery (adjuvant chemotherapy)
- relieve symptoms if a cure isn’t possible (palliative chemotherapy)
The effectiveness of chemotherapy varies significantly. Ask your doctors about the chances of treatment being successful for you.
Goals of chemotherapy
If your doctor has recommended chemotherapy to treat your cancer, it’s important to understand the goals of chemotherapy treatment when making treatment decisions. There are three main goals for chemotherapy (chemo) in cancer treatment:
- Cure
- Control
- Palliation
Cure
If possible, chemotherapy is used to cure cancer, meaning that the cancer is destroyed – it goes away and doesn’t come back.
Most doctors don’t use the word “cure” except as a possibility or intention. So, when giving treatment that has a chance of curing a person’s cancer, the doctor may describe it as treatment with curative intent.
There are no guarantees, and though cure may be the goal, it doesn’t always work out that way. It often takes many years to know if a person’s cancer is really cured.
Control
If cure is not possible, the goal may be to control the disease. Chemo is used to shrink tumors and/or stop the cancer from growing and spreading. This can help the person with cancer feel better and live longer.
In many cases, the cancer doesn’t completely go away, but is controlled and managed as a chronic disease, much like heart disease or diabetes. In other cases, the cancer may even seem to have gone away for a while, but it’s expected to come back. Then chemo can be given again.
Palliation
Chemo can also be used to ease symptoms caused by the cancer. This is called palliative chemotherapy or palliation.
When the cancer is at an advanced stage, meaning it’s not under control and has spread from where it started to other parts of the body, the goal may be to improve the quality of life or help the person feel better. For instance, chemo may be used to help shrink a tumor that’s causing pain or pressure.
It’s important to know that any treatment that’s used to reduce symptoms or improve comfort is called palliative care. For example, anti-nausea treatments or pain medicines are palliative, and can be used at all stages of treatment. It can be confusing when chemo is used as a palliative treatment, because it’s most often used to try to cure or control the cancer. But when it’s used with the goal of comfort, chemo becomes palliative care.
Chemotherapy types
Chemotherapy can be given in several ways. Your doctors will recommend the best type for you.
The most common types are:
- chemotherapy given into a vein (intravenous chemotherapy) – this is usually done in hospital and involves medicine being given through a tube in a vein in your hand, arm or chest
- chemotherapy tablets (oral chemotherapy) – this usually involves taking a course of medication at home, with regular check-ups in hospital
You may be treated with one type of chemotherapy medicine or a combination of different types.
You’ll usually have several treatment sessions, which will typically be spread over the course of a few months.
How does chemotherapy work
Chemotherapy works with the cell cycle
Chemotherapy drugs target cells at different phases of the process of forming new cells, called the cell cycle. Understanding how these drugs work helps doctors predict which drugs are likely to work well together. Doctors can also plan how often doses of each drug should be given based on the timing of the cell phases.
Cancer cells tend to form new cells more quickly than normal cells and this makes them a better target for chemotherapy drugs. However, chemo drugs can’t tell the difference between healthy cells and cancer cells. This means normal cells are damaged along with the cancer cells, and this causes side effects. Each time chemo is given, it means trying to find a balance between killing the cancer cells (in order to cure or control the disease) and sparing the normal cells (to lessen side effects).
The Cell Cycle
The cell cycle is an ordered set of events through which a cell divides to become two identical daughter cells. Non-dividing cells not considered to be in the cell cycle. The cell cycle encompasses four phases pictured in Figure 1 below, they are G1-S-G2-M. The G1 stage stands for “GAP 1” (gap phase 1). The S stage stands for “Synthesis” (DNA synthesis). S stage is the stage when DNA replication occurs. The G2 stage stands for “GAP 2” (gap phase 2). The M stage stands for “mitosis”, and is when nuclear (chromosomes separate) and cytoplasmic (cytokinesis) division occur and produces two identical daughter cells during prophase, prometaphase, metaphase, anaphase, and telophase.
The major event in the cell cycle is the replication of DNA, which occurs in the S phase, and separation of the duplicated chromosomes and the constituents of the cell which occurs in the M phase. Regulation and the initiation and completion of S and M phases ensures the genetic information and other cellular components are duplicated and divided equally between the daughter cells with each cycle.
Interphase is often included in discussions of mitosis, but interphase is technically not part of mitosis, but rather encompasses stages G1, S, and G2 of the cell cycle. During the interphase the cell is engaged in metabolic activity in preparation for mitosis. In interphase of a newly formed cell, a series of changes takes place in the cell and the nucleus, before it is capable of division. This phase is also known as intermitosis. Earlier this stage was known as resting stage because no remarkable activity related to cell division takes place here. Interphase proceeds in a series of three stages, G1, S and G2. Division of cell operates in a cycle, hence the interphase of the cycle is preceded by the previous cycle of M phase and cytokinesis. Interphase is also called the preparatory phase. In the interphase stage the division of nucleus and cytosol does not occur. The cell prepares for division. This is a stage between the end of mitosis and start of the next phase. Many events occur in interphase and most significant event that occurs is the replication of genetic material. Chromosomes are not clearly discerned in the nucleus, although a dark spot called the nucleolus may be visible. The cell may contain a pair of centrioles (or microtubule organizing centers in plants) both of which are organizational sites for microtubules.
G1 Phase
This is the first phase in the interphase. From the end of the previous M phase till the beginning of the DNA synthesis in the next cycle is called the G1 phase, here G indicates gap. This phase is also called growth phase. In this phase the biosynthetic activities of the cell, which shows a considerable slow down during the M phase of resumes it activities at a high rate. In G1 phase there is a marked production of proteins by the use of 20 amino acids. Also enzymes that are required in S phase needed during DNA replication. The duration of the G1 phase is highly variable, also among different cells of the same species. The G1 phase is under the control of the p53 gene.
S phase
The start of the S phase is when the DNA replication commences. When the phase completes all the chromosomes have been replicated. Each chromosome has two sister chromatids. During this phase, the amount of DNA in the cell is doubled but the ploidy of the cell remains unchanged. In this phase the synthesis is completed as soon as possible as the exposed base pairs are sensitive to external factors like drugs or mutagens.
G2 phase
It is again the gap phase which happens during the gap between the DNA synthesis and mitosis. During this phase the cell will continue to grow. The G2 checkpoint mechanism controls to ensure that the cell is ready to enter the M (mitosis) phase and divides.
Mitosis or M phase
The M phase consists of karyokinesis – nuclear division. Mitosis is dvided into several distinct phases, known as:
- Prophase: Chromatin in the nucleus begins to condense and becomes visible in the light microscope as chromosomes. The nucleolus disappears. Centrioles begin moving to opposite ends of the cell and fibers extend from the centromeres. Some fibers cross the cell to form the mitotic spindle.
- Prometaphase: The nuclear membrane dissolves, marking the beginning of prometaphase. Proteins attach to the centromeres creating the kinetochores. Microtubules attach at the kinetochores and the chromosomes begin moving.
- Metaphase: Spindle fibers align the chromosomes along the middle of the cell nucleus. This line is referred to as the metaphase plate. This organization helps to ensure that in the next phase, when the chromosomes are separated, each new nucleus will receive one copy of each chromosome.
- Anaphase: The paired chromosomes separate at the kinetochores and move to opposite sides of the cell. Motion results from a combination of kinetochore movement along the spindle microtubules and through the physical interaction of polar microtubules.
- Telophase: Chromatids arrive at opposite poles of cell, and new membranes form around the daughter nuclei. The chromosomes disperse and are no longer visible under the light microscope. The spindle fibers disperse, and cytokinesis or the partitioning of the cell may also begin during this stage.
- Cytokinesis: In animal cells, cytokinesis results when a fiber ring composed of a protein called actin around the center of the cell contracts pinching the cell into two daughter cells, each with one nucleus. In plant cells, the rigid wall requires that a cell plate be synthesized between the two daughter cells.
The cell cycle is controlled by the complex interplay of cyclin-dependent kinases (CDK -1, -2, -4, -6, -8, -12) and cyclins (cyclin -A, -B, -D, -E). Heterodimers of cyclins and cyclin-dependent kinases (CDKs) function at different points in the cycle. There are several checks and balances, called checkpoints, in the cell cycle to ensure integrity of daughter cells. Cell cycle checkpoints are the regulatory pathways that control the order and the timing of the transitions of the cell cycle. The checkpoints also ensures that critical events such as replication of DNA and segregation of chromosomes are completed before the cell progresses further through the cycle. The cell-cycle checkpoints respond to the cellular damage by slowing the cycle to provide time for repair and it also induces transcription of genes that facilitate the repair. The loss of the checkpoints results in instability of chromosomes and it can result in the transformation of normal cells into cancer cells.
Checkpoints include the G1/S checkpoint and the G2/M checkpoint. Of particular relevance, p21 and p27 function as regulators of the G1 and S checkpoints. These checkpoints become important in the setting of DNA damage. DNA damage activates these checkpoints to ensure genomic integrity by repairing damaged DNA or forcing the cell to enter a programmed cell death pathway if DNA cannot be repaired. Checkpoints and DNA damage responses are altered in numerous cancers. Proteins like the cyclin dependent kinase (Cdk), kinases and cyclins control the switches for the cell cycle causing the cell to move from G1 to S or G2 to M.Regulatory molecules are of two classes cyclins and cyclin-dependent kinases (Cdk). The genes encoding cyclins and CDKs are conserved among all eukaryotes. Proteins like the p27 and p53 prevent the cells from passing check points. They are also known as protein suppressors. P27 protein binds to cyclin and CDK blocking the entry into the S phase. P53 protein blocks the cell cycle at the M checkpoint if the DNA is damaged. P53 mutation is the most frequent mutation found in cancer cells. P53 functions by blocking the cycle giving the cell time to repair its DNA. If there is severe damage in the DNA the protein causes the cell to apoptosis.
Regulation of the cell cycle
Regulation of the cell cycle is a crucial process to the survival of the cell. Cell regulation includes the detection and repair of genetic damage and also prevention of uncontrolled cell division. The molecular events that control the cell cycle occurs in a sequential fashion and is impossible to reverse the cycle.
How cell division (and thus tissue growth) is controlled is very complex. The following terms are some of the features that are important in regulation, and places where errors can lead to cancer. Cancer is a disease where regulation of the cell cycle goes awry and normal cell growth and behavior is lost.
Cdk (cyclin dependent kinase, adds phosphate to a protein), along with cyclins, are major control switches for the cell cycle, causing the cell to move from G1 to S or G2 to M.
MPF (Maturation Promoting Factor) includes the CdK and cyclins that triggers progression through the cell cycle.
p53 is a protein that functions to block the cell cycle if the DNA is damaged. If the damage is severe this protein can cause apoptosis (cell death).
- p53 levels are increased in damaged cells. This allows time to repair DNA by blocking the cell cycle.
- A p53 mutation is the most frequent mutation leading to cancer. An extreme case of this is Li Fraumeni syndrome, where a genetic a defect in p53 leads to a high frequency of cancer in affected individuals.
p27 is a protein that binds to cyclin and cdk blocking entry into S phase. Recent research suggests that breast cancer prognosis is determined by p27 levels. Reduced levels of p27 predict a poor outcome for breast cancer patients.
Figure 1. Cell Cycle
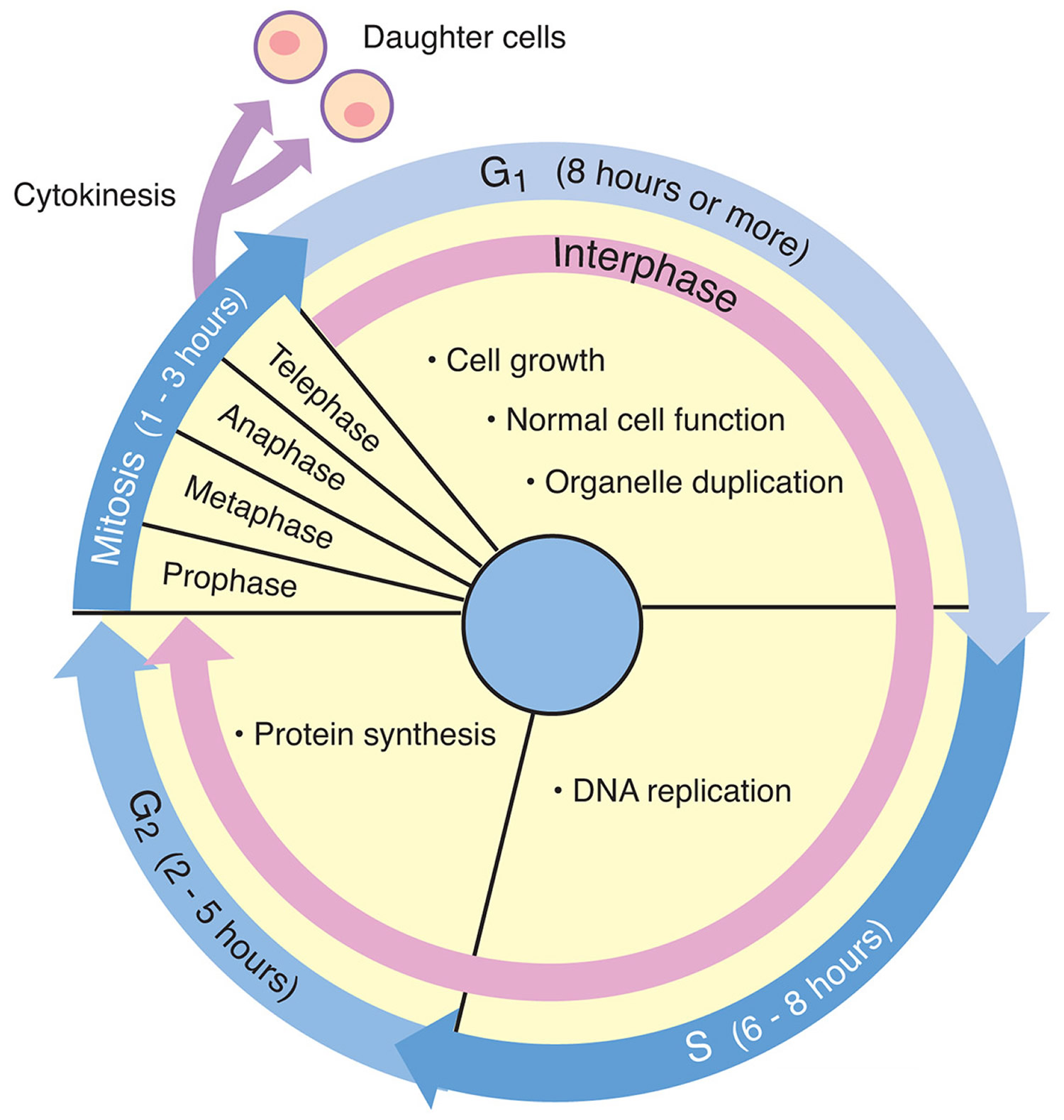 Figure 2. Human cell
Figure 2. Human cell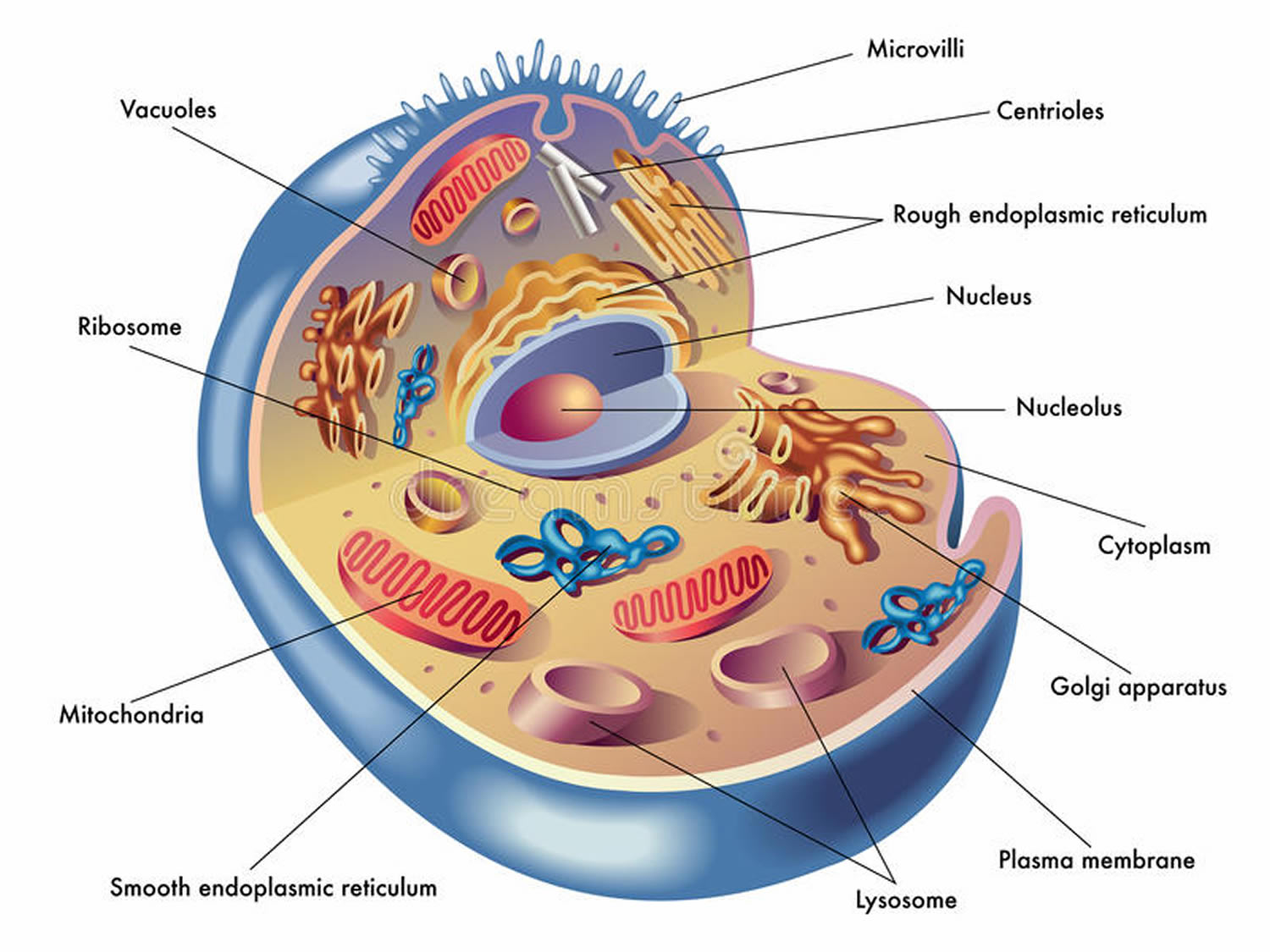
How chemotherapy kills cancer cells
Chemotherapy circulates throughout your body in the bloodstream. So it can treat cancer cells almost anywhere in the body. This is known as systemic treatment.
Chemotherapy kills cells that are in the process of splitting into 2 new cells.
Body tissues are made of billions of individual cells. Once we are fully grown, most of the body’s cells don’t divide and multiply much. They only divide if they need to repair damage.
When cells divide, they split into 2 identical new cells. So where there was 1 cell, there are now 2. Then these divide to make 4, then 8 and so on.
In cancer, the cells keep on dividing until there is a mass of cells. This mass of cells becomes a lump, called a tumor.
Because cancer cells divide much more often than most normal cells, chemotherapy is much more likely to kill them.
Some drugs kill dividing cells by damaging the part of the cell’s control center that makes it divide. Other drugs interrupt the chemical processes involved in cell division.
The effects on dividing cells
Chemotherapy damages cells as they divide.
In the center of each living cell is a dark blob, called the nucleus. The nucleus is the control center of the cell. It contains chromosomes, which are made up of genes.
These genes have to be copied exactly each time a cell divides into 2 to make new cells.
Figure 3. Human cells division
Chemotherapy damages the genes inside the nucleus of cells.
Some drugs damage cells at the point of splitting. Some damage the cells while they’re making copies of all their genes before they split. Chemotherapy is much less likely to damage cells that are at rest, such as most normal cells.
You might have a combination of different chemotherapy drugs. This will include drugs that damage cells at different stages in the process of cell division. This means there’s more chance of killing more cells.
Why chemotherapy causes side effects
The fact that chemotherapy drugs kill dividing cells helps to explain why chemotherapy causes side effects. It affects healthy body tissues where the cells are constantly growing and dividing, such as:
- your hair, which is always growing
- your bone marrow, which is constantly producing blood cells
- your skin and the lining of your digestive system, which are constantly renewing themselves
Because these tissues have dividing cells, chemotherapy can damage them. But normal cells can replace or repair the healthy cells that are damaged by chemotherapy.
So the damage to healthy cells doesn’t usually last. Most side effects disappear once your treatment is over. Some side effects such as sickness or diarrhea might only happen during the days you are actually having the drugs.
Chemotherapy drugs
There are more than 100 chemotherapy or chemotherapy drugs that are used to treat cancer – either alone or in combination with other drugs or treatments. These drugs are very different in their chemical composition, how they are taken, their usefulness in treating specific forms of cancer, and their side effects.
You and your cancer doctor, called an oncologist, will decide what chemotherapy drug or combination of drugs you will get. Your doctor will choose the chemotherapy doses, how the drugs will be given, and how often and how long you’ll get chemotherapy treatment. All of these decisions will depend on the type of cancer, where it is, how big it is, and how it affects your normal body functions and overall health.
Cancer can be treated with a single chemotherapy drug, but often several drugs are used in a certain order or in certain combinations (called combination chemotherapy). Different drugs that work in different ways can work together to kill more cancer cells. This can also help lower the chance that the cancer may become resistant to any one chemotherapy drug.
Types of chemotherapy drugs
chemotherapy drugs can be grouped by how they work, their chemical structure, and their relationships to other drugs. Some drugs work in more than one way, and may belong to more than one group. (Note: not all chemotherapy drugs are listed here.)
Knowing how the drug works is important in predicting side effects from it. This helps doctors decide which drugs are likely to work well together. If more than one drug will be used, this information also helps them plan exactly when each of the drugs should be given (in which order and how often).
Alkylating agents
Alkylating agents keep the cell from reproducing by damaging its DNA. These drugs work in all phases of the cell cycle and are used to treat many different cancers, including cancers of the lung, breast, and ovary as well as leukemia, lymphoma, Hodgkin disease, multiple myeloma, and sarcoma, .
Because these drugs damage DNA, they can affect the cells of the bone marrow which make new blood cells. In rare cases, this can lead to leukemia. The risk of leukemia from alkylating agents is “dose-dependent,” meaning that the risk is small with lower doses, but goes up as the total amount of the drug used gets higher. The risk of leukemia after getting alkylating agents is highest about 5 to 10 years after treatment.
Examples of alkylating agents include:
- Altretamine
- Busulfan
- Carboplatin
- Carmustine
- Chlorambucil
- Cisplatin
- Cyclophosphamide
- Dacarbazine
- Lomustine
- Melphalan
- Oxaliplatin
- Temozolomide
- Thiotepa
Antimetabolites
Antimetabolites interfere with DNA and RNA growth by substituting for the normal building blocks of RNA and DNA. These agents damage cells during the phase when the cell’s chromosomes are being copied. They are commonly used to treat leukemias, cancers of the breast, ovary, and the intestinal tract, as well as other types of cancer.
Examples of antimetabolites include:
- 5-fluorouracil (5-FU)
- 6-mercaptopurine (6-MP)
- Capecitabine (Xeloda®)
- Cytarabine (Ara-C®)
- Floxuridine
- Fludarabine
- Gemcitabine (Gemzar®)
- Hydroxyurea
- Methotrexate
- Pemetrexed (Alimta®)
Anti-tumor antibiotics
These drugs are not like the antibiotics used to treat infections. They work by changing the DNA inside cancer cells to keep them from growing and multiplying.
Anthracyclines: Anthracyclines are anti-tumor antibiotics that interfere with enzymes involved in copying DNA during the cell cycle. (Enzymes are proteins that start, help, or speed up the rate of chemical reactions in cells.) They are widely used for a variety of cancers.
Examples of anthracyclines include:
- Daunorubicin
- Doxorubicin (Adriamycin®)
- Epirubicin
- Idarubicin
A major concern when giving these drugs is that they can permanently damage the heart if given in high doses. For this reason, lifetime dose limits are often placed on these drugs.
Anti-tumor antibiotics that are not anthracyclines include:
- Actinomycin-D
- Bleomycin
- Mitomycin-C
- Mitoxantrone (also acts as a topoisomerase II inhibitor)
Topoisomerase inhibitors
These drugs interfere with enzymes called topoisomerases, which help separate the strands of DNA so they can be copied. (Enzymes are proteins that cause chemical reactions in living cells.) Topoisomerase inhibitors are used to treat certain leukemias, as well as lung, ovarian, gastrointestinal, and other cancers.
Topoisomerase inhibitors are grouped according to which type of enzyme they affect:
Topoisomerase I inhibitors include:
- Topotecan
- Irinotecan (CPT-11).
Topoisomerase II inhibitors include:
- Etoposide (VP-16)
- Teniposide.
- Mitoxantrone (also acts as an anti-tumor antibiotic)
Topoisomerase II inhibitors can increase the risk of a second cancer – acute myelogenous leukemia (AML) – as early as 2 to 3 years after the drug is given.
Mitotic inhibitors
Mitotic inhibitors are compounds derived from natural products, such as plants. They work by stopping cells from dividing to form new cells but can damage cells in all phases by keeping enzymes from making proteins needed for cell reproduction.
Examples of mitotic inhibitors include:
- Docetaxel
- Estramustine
- Ixabepilone
- Paclitaxel
- Vinblastine
- Vincristine
- Vinorelbine
They are used to treat many different types of cancer including breast, lung, myelomas, lymphomas, and leukemias. These drugs may cause nerve damage, which can limit the amount that can be given.
Corticosteroids
Corticosteroids, often simply called steroids, are natural hormones and hormone-like drugs that are useful in the treatment of many types of cancer, as well as other illnesses. When these drugs are used as part of cancer treatment, they are considered chemotherapy drugs.
Examples of corticosteroids include:
- Prednisone
- Methylprednisolone (Solumedrol®)
- Dexamethasone (Decadron®)
Steroids are also commonly used to help prevent nausea and vomiting caused by chemo. They are used before chemo to help prevent severe allergic reactions, too.
Other chemotherapy drugs
Some chemotherapy drugs act in slightly different ways and do not fit well into any of the other categories.
Examples include drugs like L-asparaginase, which is an enzyme, and the proteosome inhibitor bortezomib (Velcade®).
Other types of drugs used to treat cancer
Other drugs and biological treatments are used to treat cancer, but aren’t considered chemotherapy. They often have less side effects than chemotherapy.. Many are used along with chemo.
Targeted therapies
Targeted therapies attack cancer cells more specifically than traditional chemotherapy drugs. These drugs can be used as part of the main treatment, or they may be used after treatment to keep the cancer under control or keep it from coming back.
Differentiating agents
These drugs act on the cancer cells to make them mature into normal cells. Examples include the retinoids, tretinoin (ATRA or Atralin®) and bexarotene (Targretin®), as well as arsenic trioxide (Arsenox®).
Hormone therapy
Drugs in this category are sex hormones, or hormone-like drugs, that are used to slow the growth of breast, prostate, and endometrial (uterine) cancers, which normally grow in response to natural sex hormones in the body. They work by making the cancer cells unable to use the hormone they need to grow, or by preventing the body from making the hormone.
Immunotherapy
Some treatments are given to people with cancer to help their immune systems recognize and attack cancer cells.
Determining which chemotherapy drugs to use
In some cases, the best choice of doses and schedules for each chemotherapy drug is clear, and most doctors would recommend the same treatment. In other cases, less may be known about the single best way to treat people with certain types and stages of cancer. In these cases, different doctors might choose different chemotherapy drug combinations with different schedules.
Factors to consider when choosing which chemotherapy drugs to use include:
- The type of cancer
- The stage of the cancer (how far it has spread)
- The patient’s age
- The patient’s overall health
- Other serious health problems (such as heart, liver, or kidney diseases)
- Types of cancer treatments given in the past
Doctors take these factors into account, along with information published in medical journals and textbooks describing the outcomes of similar patients treated with chemotherapy.
Determining chemotherapy doses
Most chemotherapy (chemo) drugs are strong medicines that have a fairly narrow range for dose safety and effectiveness. Taking too little of a drug will not treat the cancer well and taking too much may cause life-threatening side effects. For this reason, doctors must calculate chemotherapy doses very precisely.
Depending on the chemotherapy drug(s) to be given, there are different ways to determine chemotherapy doses. Most chemotherapy drugs are measured in milligrams (mg).
The overall dose may be based on a person’s body weight in kilograms (1 kilogram = 2.2 pounds). For instance, if the standard dose of a chemotherapy drug is 10 milligrams per kilogram (10 mg/kg), a person weighing 110 pounds (50 kilograms) would get 500 mg (10 mg/kg x 50 kg).
Some chemotherapy doses are determined based on body surface area (BSA), which are calculated using height and weight. Body surface area is expressed in meters squared (m²).
Because children’s bodies process chemotherapy drugs differently, dosages for children and adults differ, even after body surface area is taken into account. Children may have different levels of sensitivity to the chemotherapy drugs, too. For the same reasons, dosages of some chemotherapy drugs may also be adjusted for people who:
- Are elderly
- Have poor nutritional status
- Are obese
- Have already taken or are currently taking other medicines
- Have already had or are currently getting radiation therapy
- Have low blood cell counts
- Have liver or kidney diseases
Determining a chemotherapy schedule (cycle)
Chemotherapy is commonly given at regular intervals called cycles. A cycle may be a dose of one or more drugs followed by several days or weeks without treatment. This gives normal cells time to recover from chemotherapy drug side effects. Sometimes, chemotherapy doses may be given a certain number of days in a row, or every other day for several days, followed by a period of rest. Some chemotherapy drugs work best when given continuously over a set number of days.
Each chemotherapy drug is given on a schedule that makes the most of its anti-cancer actions and minimizes side effects. If more than one chemotherapy drug is used, the treatment plan will say how often and exactly when each chemotherapy drug should be given. The number of chemotherapy cycles given may be decided before treatment starts, based on the type and stage of cancer. In some cases, the number is flexible, and will take into account how the treatment affects the cancer and the person’s overall health.
Changing chemotherapy doses and schedules
In most cases, the most effective chemotherapy doses and schedules of chemotherapy drugs to treat specific cancers have been found by testing them in clinical trials. It’s important, when possible, to get the full course of chemotherapy, the full dose, and keep the cycles on schedule. This gives a person the best chance of getting the maximum benefit from chemotherapy treatment.
There may be times, though, when serious side effects require adjusting the chemotherapy plan (dose and/or schedule) to allow you time to recover. Sometimes, you might be given supportive medicines to help your body recover more quickly. Again, the key is to give enough chemotherapy to kill the cancer cells without causing other serious problems.
Getting Chemotherapy
Chemotherapy can be carried out in many different ways, depending on your circumstances.
Learn the basics about getting chemotherapy and important safety precautions you need to consider to protect your health and those you live with.
Before treatment starts
If you’re diagnosed with cancer, you’ll be cared for by a team of specialists. Your team will recommend chemotherapy if they think it’s the best option for you, but the final decision is yours.
Making this decision can be difficult. You may find it useful to write a list of questions to ask your care team.
For example, you may want to find out:
- what the aim of treatment is – for example, is it being used to cure your cancer, relieve your symptoms or make other treatments more effective
- about possible side effects and what can be done to prevent or relieve them
- how effective chemotherapy is likely to be
- whether any other treatments could be tried instead
If you agree with your team’s recommendation, they’ll start to plan your treatment once you’ve given your consent to treatment.
Tests and checks
Before chemotherapy begins, you’ll have tests to check your general health and make sure the treatment is suitable for you.
The tests you’ll have may include:
- blood tests – to check things such as how well your liver and kidneys are working, and how many blood cells you have
- X-rays and scans – to check the size of your cancer
- measurements of your height and weight – to help your team work out the correct dose
During treatment you’ll also have tests to monitor your progress.
Your treatment plan
Chemotherapy involves several treatment sessions, typically spread over the course of a few months.
Before treatment starts, your care team will draw up a plan that outlines:
- the type of chemotherapy you’ll have
- how many treatment sessions you’ll need
- how often you’ll need treatment – after each treatment you’ll have a break before the next session to allow your body to recover
Your treatment plan will depend on things such as the type of cancer you have and what the aim of treatment is.
Where will I get chemotherapy?
The place you get your treatment depends on which chemotherapy (chemo) drugs you’re getting, the drug doses, your hospital’s policies, your insurance coverage, what you prefer, and what your doctor recommends.
You may get chemotherapy:
- At home
- In your doctor’s office
- In a clinic
- In a hospital’s outpatient infusion center
- In a hospital
Some of these settings may have private treatment rooms, while others treat many patients together in one large room. Ask your doctor or nurse about this ahead of time so you know what to expect your first day.
How often will I need chemotherapy and how long will it last?
How often you get chemotherapy and how long your treatment lasts depend on the kind of cancer you have, the goals of the treatment, the drugs being used, and how your body responds to them.
You may get treatments daily, weekly, or monthly, but they’re usually given in on-and-off cycles. This means, for example, that you may get chemotherapy the first 2 weeks and then have a week off, making it a cycle that will start over every 3 weeks. The time off lets your body build healthy new cells and regain its strength.
Your cancer care team can tell you how many cycles are planned and how long they expect your treatment to last.
Many people wonder how long the actual chemotherapy drugs stay in their body and how they’re removed. Your kidneys and liver break down most chemotherapy drugs which then leave your body through urine or stool. How long it takes your body to get rid of the chemotherapy drugs depends on many things, including the type of chemotherapy you get, other medicines you take, your age, and how well your kidneys and liver work. Your cancer care team will tell you if you need to take any special precautions because of the chemotherapy drugs you are getting.
If your cancer comes back, you might have chemotherapy again. This time, you could be given different chemotherapy drugs to relieve symptoms or to slow the cancer’s growth or spread. Side effects might be different, depending on the chemotherapy drugs, the doses, and how they’re given.
What should I eat before my first chemotherapy treatment?
Your chemotherapy can take anywhere from a few minutes to many hours. Make sure you eat something before treatment. Most people find that a light meal or snack an hour or so before chemotherapy works best. If you’ll be there several hours, plan ahead and bring a small meal or snacks in an insulated bag or cooler. Find out if there’s a refrigerator or microwave you can use.
Can I be around my family and friends while I’m getting chemotherapy?
Most chemotherapy drugs make you less able to fight infection, but there are ways you can avoid them.
- Stay away from anyone who is sick.
- Wash your hands often, especially before touching your face, nose, mouth, or eyes. Ask your family and friends to do the same when they are with you.
- Very few treatments require you to avoid close contact with loved ones for a short amount of time. If this is something you’ll have to do, your doctor will tell you about it when going over treatment options.
- Make sure your vaccinations are up to date. The flu shot is especially important because people with cancer are at high risk of serious flu complications. Your health care provider will recommend which vaccines you need.
- Infections can be picked up from food and drinks. So, food safety is very important when your immune system is weak. Talk to your cancer care team about whether you need to follow a special diet during your cancer treatment.
- Some pets can also transmit infections. So be sure to keep them healthy and take precautions when you’re around them.
How can I protect myself and those I live with while I’m getting chemotherapy?
There are many things you can do during and after chemotherapy to keep yourself and your loved ones from being affected by the chemotherapy drugs while your body is getting rid of them. It takes about 48 hours for your body to break down and/or get rid of most chemotherapy drugs.
Most of the waste comes out in your body fluids – urine, stool, tears, and vomit. The drugs are also in your blood. When chemotherapy drugs get outside your body, they can harm or irritate skin – yours or even other people’s. Keep in mind that this means toilets can be a hazard for children and pets, and it’s important to be careful. Talk to your cancer care team about these and any other precautions you should follow.
During – and for 48 hours after – chemotherapy:
- Flush the toilet twice after you use it. Put the lid down before flushing to avoid splashing. If possible, you may want to use a separate toilet during this time. If this is not possible, wear gloves to clean the toilet seat after each use.
- Both men and women should sit on the toilet to use it. This cuts down on splashing.
- Always wash your hands with warm water and soap after using the toilet. Dry your hands with paper towels and throw them away.
- If you vomit into the toilet, clean off all splashes and flush twice. If you vomit into a bucket or basin, carefully empty it into the toilet without splashing the contents and flush twice. Wash out the bucket with hot, soapy water and rinse it; empty the wash and rinse water into the toilet, then flush. Dry the bucket with paper towels and throw them away.
- Caregivers should wear 2 pairs of throw-away gloves if they need to touch any of your body fluids. (These can be bought in most drug stores.) They should always wash their hands with warm water and soap afterward – even if they had gloves on.
- If a caregiver does come in contact with any of your body fluids, they should wash the area very well with warm water and soap. It’s not likely to cause any harm, but try to avoid this. At your next visit, let your doctor know this happened. Being exposed often may lead to problems, and extra care should be taken to avoid this.
- Any clothes or sheets that have body fluids on them should be washed in your washing machine – not by hand. Wash them in warm water with regular laundry detergent. Do not wash them with other clothes. If they can’t be washed right away, seal them in a plastic bag.
- If using throw-away adult diapers, underwear, or sanitary pads, seal them in 2 plastic bags and throw them away with your regular trash.
Will I be able to work while I’m getting chemotherapy?
Whether you can work during cancer treatment depends on:
- The type of treatment you are getting
- The stage of your cancer
- Your overall health
- The kind of work you do
What you can do and whether you will need to limit how much you do will depend on how you feel during treatment. Some people with cancer can still go to work and do their usual everyday tasks while they get treatment. Others find that they need more rest or just feel too sick to do much. Your doctor may also want you to limit some of your activities.
Still, many people are able to keep working while they’re getting cancer treatment. Some people work their usual full-time schedules. Some work the same schedules with special conditions, like being closer to the office bathroom so it’s easier to deal with side effects. Others need a less demanding schedule, like taking extra days off or even working part time for a while.
The willingness and ability of your workplace to accommodate any special needs you might have will affect your success at working during treatment. Talk with your employer about what you might need at this time. Under federal and state laws, some employers may be required to let you work a flexible schedule to meet your treatment needs.
Tips for working while you are getting treatment
It’s important to figure out how you will continue to work while you are being treated for cancer. These tips might help you better manage your time and work:
- Plan chemotherapy treatments late in the day or right before the weekend to allow time to recover.
- Explore options like working from home some days. This might help you feel less tired and allow you to take care of yourself more easily if you have problems.
- Getting help at home can mean more energy for work. Certain daily chores may be divided among friends and family members.
- Unless there is a reason not to, let co-workers know about your situation. They can be great sources of support. They may even be able to help you come up with ways to better manage your work during this time.
- Keep your supervisor up to date on how well your schedule or other changes are working for you.
- Make a log of your usual work schedule and duties. Refer to it when you set up flex-time, shifted duties, or time off.
- Make a detailed list of job duties so you can direct others in handling things when you’re out of the office.
Legal protections
You have the same rights as anyone else in the workplace and should be given equal opportunities, regardless of whether you tell people at work about your cancer. Hiring, promotion, and how you are treated in the workplace should depend entirely on your abilities and qualifications. As long as you are able to fulfill your job duties, you can’t legally be fired for being sick. You also shouldn’t have to accept a position you never would have considered before your illness. Many people with job problems related to cancer are protected by federal laws like the Rehabilitation Act and the Americans with Disabilities Act (https://www.ada.gov/).
Some people also benefit from the Family and Medical Leave Act (FMLA). This law lets many people with serious illnesses take unpaid leave to get medical care or manage their symptoms. The leave can take many forms, such as a part-time schedule for a limited time, or taking off 1 or 2 days a week for a while. Not all employers are required to follow FMLA. Talk to someone in your human resources department or another workplace expert to find out what your options are.
What if you can’t keep working during treatment?
Sometimes, even with good planning and extra time off, you find it’s just too much to keep working during cancer treatment. If cancer treatment starts causing too many problems for you at work, talk to your supervisor. Explain that you want to keep working, but you need to take some time away from work.
Talk to someone from your human resources department to find out if you have short-term or long-term disability insurance at your job. If you do, get applications for both – just in case. In general, short-term disability pays you some portion of your income for the first few months you are unable to work. If you must be out longer, some employers also carry long-term disability insurance, which usually starts after 6 months of disability. You must meet the insurance company’s definition of disability to get this income.
Talk with your doctor about how your treatment and symptoms are affecting your work to decide whether or when you should think about taking time off. Your doctor will need to help you by filling out part of the disability application.
Keep in mind that it can hurt you to put off going on short-term disability. Some people have had to go to great lengths to prove that they can’t do their job after they’ve spent weeks forcing themselves to go to work when they could barely get out of bed. Don’t wait until your work performance suffers before you decide to take time away from work. If you are fired for doing a poor job, you can lose your health insurance as well as your income. And if you’re fired, you cannot collect disability benefits. If you need time off from work to focus on getting well, take it.
How will I be given chemotherapy?
Through a vein
Most chemotherapy drugs are put right into your bloodstream directly into a vein (intravenous chemotherapy) through a tiny, soft, plastic tube called a catheter. A needle is used to put the catheter into a vein in your forearm or hand; then the needle is taken out, leaving the catheter behind. This is called intravenous or IV treatment.
Intravenous chemotherapy can be done using:
- a cannula – a small tube that’s placed into a vein in the back of your hand or lower arm for a short time
- a peripherally inserted central catheter (PICC) line – a small tube inserted into a vein in your arm that usually stays in place for several weeks or months
- a central line – similar to a PICC, but inserted into your chest and connected to one of the veins near your heart
- an implanted port (chemotherapy port) – a small device inserted under the skin that’s kept in place until your treatment course finishes; medicine is given using a needle inserted into the device through the skin
The time it takes to have a dose of intravenous chemotherapy can range from several hours to several days.
Intravenous chemotherapy drugs are given in these ways:
- The chemotherapy drugs can be given quickly through the catheter right from a syringe over a few minutes. This is called an IV push.
- An IV infusion can last from a few minutes to a few hours. A mixed drug solution flows from a plastic bag through tubing that’s attached to the catheter. The flow is often controlled by a machine called an IV pump.
- Continuous infusions are sometimes needed and can last from 1 to 7 days. These are always controlled by electronic IV pumps.
The needles and catheters can scar and damage veins with ongoing chemo. Another option is a central venous catheter (CVC). A central venous catheter is a bigger catheter that’s put into a large vein in the chest or arm. It stays in as long as you’re getting treatment so you won’t need to be stuck with a needle each time. Different kinds of central venous catheters are available.
Many people talk about central venous catheter options with their doctor even before starting treatment. Some find out during treatment that they need a central venous catheter because their hand and arm veins aren’t going to last to complete the planned chemo. Your doctor can help you decide if you need a central venous catheter and the right type of central venous catheter for you.
By mouth
You swallow the chemo as a pill, capsule, or liquid – just like other medicines. Oral chemotherapy can often be taken at home. If you take chemotherapy drugs by mouth, it’s very important to take the exact dosage, at the right time, for as long as you’re supposed to do so. Chemotherapy drug you swallow is as strong as other forms of chemo and works just as well. But oral chemotherapy drugs cost a lot. Many times you have to pay more of your own money for them than you pay for chemo that’s given with a needle in the hospital or clinic. If you have health insurance, this might mean a higher co-pay. Make sure you know how much you’ll have to pay for each treatment.
How do I take my oral chemo?
You should have clear instructions on how much and when to take your chemo. Sometimes chemo is given in rounds or cycles. This cuts down on the harm to healthy cells and allows the chemo to kill more cancer cells. Your doctor will talk to you about when you will need to take your chemo. Be sure to take it just the way your doctor or nurse has told you.
Make sure you know how to deal with your chemo drugs. Sometimes you need to wear gloves when touching the drugs. Some drugs have to be kept in the bottle or box they came in. Also be sure you know how to get rid of doses when you don’t need them anymore. Some might have to be taken back to the drug store to be thrown away safely.
Be sure to tell your doctor or nurse about any problems you have taking your chemo. For instance, if you’re throwing up or feel sick to your stomach, you may feel too sick to take your chemo. Or, you may not be able to keep your chemo down and may throw it up. Your doctor needs to know about any problems so they can change your treatment plan, if needed.
Oral chemo doses are set up so that the same level of drug stays in your body to kill the cancer cells. Not taking your chemo the right way can affect how well it works, and may even allow the cancer to grow.
Sometimes dose changes are needed, but don’t make any changes unless your doctor tells you to do so. Even after you start feeling better, you may still have cancer cells in your body that the chemo must fight.
Will I still need to see my doctor?
Even though you take oral chemotherapy at home, you will still need to see your cancer care team. They will watch for changes in the cancer and see how you are doing with your chemo plan. Blood tests and scans will be done to see how your body and the cancer are doing with the chemo.
If you miss a dose or are late taking one, tell your doctor or nurse about it. They need to know about this when deciding if treatment is working. It may also help the doctor decide whether to change how much of the medicine you take or when you take it.
What can I expect from oral chemotherapy?
The side effects of any form of chemo vary from drug to drug and from person to person. Your cancer care team may not be able to tell you what side effects you’ll have, but they can tell you what to watch for.
Some oral chemotherapy drugs can cause things like:
- Stomach upset (nausea)
- Throwing up (vomiting)
- Loose or watery poop (diarrhea)
- Hair loss
- Mouth sores
- Skin changes
- Low blood counts
Oral chemotherapy goes through your whole body to kill cancer cells wherever they might be. But it also harms healthy, normal cells. This causes side effects.
Make sure you know what side effects to look for before you start chemo. Also ask if there are any side effects that you should call the cancer care team about right away.
Telling your team about side effects as soon as they happen can help make sure that they don’t get too bad. Your doctor may have to change how much you take or give you other drugs to help you feel better. If you aren’t sure about a side effect and can’t reach your doctor, don’t take your chemo until you talk to someone on your cancer care team.
Taking chemotherapy at home gives you more freedom without having a lot of treatment visits. You may not be seeing your doctor and nurses very often, but be sure to call them with any questions or concerns you have.
Before starting oral chemo, talk to your doctor or nurse about any concerns or questions you have. Get answers to all of your questions about oral chemo before you start taking it.
The success of oral chemotherapy depends a lot on you – it’s important to take the right dose of the chemotherapy drug, at the right time, just as you’ve been told. Your cancer care team is there to help you do this.
Intrathecal or IT
IT chemotherapy is put into the spinal canal and goes into the fluid that surrounds the brain and spinal cord to reach cancer cells there. This fluid is called the cerebrospinal fluid or CSF. This is important because most chemotherapy drugs delivered by IV or by mouth are unable to reach the brain due to the blood-brain barrier.
chemotherapy can be delivered to the CSF through a needle placed in the spinal area, or a long-term catheter and port that can be put under the skin on your head during surgery. This port is called an Ommaya reservoir. The Ommaya is a small drum-like device with a small tube attached to it. The tube goes into the CSF in a cavity of your brain. The Ommaya stays in place under your scalp until treatment is done.
Intra-arterial
In this use, the chemotherapy drug is put right into the main artery that supplies blood to the tumor to treat a single area (such as the liver, an arm, or leg). This method helps limit the effect the drug has on other parts of the body and is called regional chemotherapy.
Intracavitary
chemotherapy drugs may be given through a catheter into an enclosed area of the body such as the abdomen (this is called intraperitoneal chemotherapy) or chest (called intrapleural chemotherapy).
Intramuscular or IM
The drug is put in through a needle into a muscle (as an injection or shot).
Intralesional
A needle is used to put the drug right into a tumor. It’s only possible when the tumor can be safely reached with a needle.
Intravesical
The chemotherapy is put right into the bladder through a soft catheter. It stays in for a few hours and is then drained out, and the catheter is removed.
Topical
The drug is put right on an area of cancer on the skin as a cream, gel, or ointment.
Issues during chemotherapy treatment
During chemotherapy treatment, there are a number of important things to bear in mind.
Pregnancy and contraception
Chemotherapy can sometimes affect your sex life. It can affect men and women differently. It’s important to avoid pregnancy while you’re having chemotherapy.
Women should avoid becoming pregnant while having chemotherapy, as many chemotherapy medicines can cause birth defects.
Use a barrier method of contraception, such as a condom, and contact your care team immediately if you think you may have become pregnant.
Men having chemotherapy should use condoms throughout their course of treatment, even if their partner is taking contraception.
Contraception
It’s important to use reliable contraception during treatment. Avoid getting pregnant while you or your partner are having chemotherapy. This is because the drugs may harm the baby.
If you have or have had breast cancer, your doctor might advise you not to take the contraceptive pill. This is because the hormones in it might affect the cancer.
It is not known for sure whether or not chemotherapy drugs can be passed on through semen or secretions from the vagina. Because of this some doctors advise people to use a barrier method (such as condoms, female condoms or dental dams) if you have sex during treatment. This applies to vaginal, anal or oral sex.
Generally, doctors advise a barrier method only for the time you are actually having the treatment and for about a week after your treatment.
Advice like this can be worrying, but this does not mean that you have to avoid being intimate with your partner. You can still have close contact with your partner and continue to enjoy sex.
Sex and chemotherapy
Some people carry on with their sex lives as normal during chemotherapy. Others find their treatment changes how they feel emotionally or physically.
Effects of chemotherapy on your sex life
Some changes are simple and won’t last long. They won’t affect your sex life permanently.
Sometimes you may feel:
- too tired
- not strong enough to be very active
- sick or sore
- not in the mood
- anxious or low
Your anxiety might not seem related to sex. For example, you may be worried about the cancer and how your treatment is going. Or you may be worried about money, or about how you family are coping with your illness.
These things can cause stress, which can affect your interest in sex. It’s important to talk to your partner about how you feel.
Remember – the changes to your sex life don’t usually last long. There’s usually no medical reason to stop having sex during chemo. The drugs won’t have any long term physical effects on your performance or enjoyment of sex. Cancer can’t be passed on to your partner during sex.
Sex and chemotherapy for women
Some women find that chemotherapy does not affect their sex lives. Others find that their sex life changes, but goes back to normal after the treatment.
You might feel tired or sick as a result of chemotherapy. This might make you feel less interested in sex for a while.
The emotional effects of having cancer can also affect your sex life. It’s important to talk to your partner about how you feel. Your cancer specialist nurse can give you support with this if you need it. You may want to talk to them with your partner.
Sex and chemotherapy for men
Some men lead normal sex lives during treatment. Others find that their sex lives change, but go back to normal afterwards. Chemotherapy doesn’t usually have a permanent effect on your sex life.
You might feel tired or sick as a result of chemotherapy. These changes may make you feel less interested in sex for a while.
More rarely, chemotherapy can make a man’s testosterone levels drop. Testosterone is the male sex hormone. Chemotherapy can also affect the nerves that control erections.
So some men find that while they’re having treatment, they lose interest in sex. Or they have trouble getting and keeping an erection.
These changes are usually temporary and don’t last more than a couple of weeks after the treatment has finished.
The emotional effects of having cancer can also affect your sex life. Some men feel differently about themselves. You may worry about your ability to have sex, or about your ability to father children (fertility). These worries can also lower your desire and your ability to have an erection.
High dose treatment
Higher doses of chemotherapy are more likely to affect your sex life. You may have high dose chemotherapy with a stem cell or bone marrow transplant.
Many people having this treatment have radiotherapy as well. This combination is more likely to make you lose your sex drive or have erection problems.
This may happen during treatment and for a while afterwards. Research shows that high dose treatment reduces some men’s testosterone levels for a while.
Chemotherapy success rate
The chance of the chemotherapy curing your cancer depends on the type of cancer you have.
- With some types of cancer, most people are cured by chemotherapy
- With other types of cancer, fewer people are completely cured
Examples of cancers where chemotherapy works very well are testicular cancer and Hodgkin lymphoma.
With some cancers, chemotherapy can’t cure the cancer on its own. But it can help in combination with other types of treatment.
For example, many people with breast or bowel cancer have chemotherapy after surgery to help lower the risk of the cancer coming back.
With some cancers, if a cure is unlikely, your doctor may still suggest chemotherapy to:
- shrink the cancer
- relieve your symptoms
- give you a longer life by controlling the cancer or putting it into remission
What remission means
Remission is a word doctors often use when talking about cancer. It means that after treatment there is no sign of the cancer.
You might hear your doctor talk about complete remission and partial remission.
Complete remission
This means that the cancer can’t be detected on scans, x-rays, or blood tests, etc. Doctors sometimes call this a complete response.
Partial remission
This means the treatment has killed some of the cells, but not all. The cancer has shrunk, but can still be seen on scans and doesn’t appear to be growing.
The treatment might have stopped the cancer from growing. Or the treatment could have made the cancer smaller so that other treatments are more likely to help, such as surgery or radiotherapy. This is sometimes called a partial response.
Another term doctors use is stable disease. This can mean that the cancer has stayed the same size or it might even have grown by a small amount.
Chemotherapy for breast cancer
Most women with breast cancer will have some type of surgery to remove the tumor. Depending on the type of breast cancer and how advanced it is, you might need other types of treatment as well, either before or after surgery, or sometimes both.
Not all women with breast cancer will need chemotherapy, but there are several situations in which chemotherapy may be recommended:
- After surgery (adjuvant chemotherapy): Adjuvant chemotherapy is used to try to kill any cancer cells that might have been left behind or have spread but can’t be seen, even on imaging tests. If these cells were allowed to grow, they could form new tumors in other places in the body. Adjuvant chemotherapy can lower the risk of breast cancer coming back.
- Before surgery (neoadjuvant chemotherapy): Neoadjuvant chemotherapy can be used to try to shrink the tumor so it can be removed with less extensive surgery. Because of this, neoadjuvant chemotherapy is often used to treat cancers that are too big to be removed by surgery at the time of diagnosis (called locally advanced cancers). Also, by giving chemotherapy before the tumor is removed, doctors can better see how the cancer responds to it. If the first set of chemotherapy drugs doesn’t shrink the tumor, your doctor will know that other drugs are needed.It should also kill any cancer cells that have spread but can’t be seen. Just like adjuvant chemotherapy, neoadjuvant chemotherapy can lower the risk of breast cancer coming back.
- For advanced breast cancer: chemotherapy can be used as the main treatment for women whose cancer has spread outside the breast and underarm area, either when it is diagnosed or after initial treatments. The length of treatment depends on how well the chemotherapy is working and how well you tolerate it.
Sometimes it is not clear if chemotherapy will be helpful. There are tests available, such as Oncotype DX and Mammoprint, that can help determine which women will most likely benefit from chemotherapy after breast surgery.
Breast Cancer Gene Expression Tests
Tests that look at the patterns of certain genes (sometimes called gene expression profiling) can help predict if some early-stage (stage 1 or 2) breast cancers are likely to come back after initial treatment. Doctors can use this information to know which women will most likely benefit from chemotherapy after breast surgery.
What are breast cancer gene expression tests?
Looking at the patterns of a number of different genes at the same time can help predict if certain stage 1 or 2 breast cancers are likely to come back after initial treatment. Tests like these are part of what’s being called “personalized medicine” – learning more about your cancer to specially tailor your treatment.
The Oncotype DX® and the MammaPrint® are examples of tests that look at different sets of breast cancer genes. And there are more tests in development.
How are the breast cancer gene expression tests done?
Oncotype DX®: The Oncotype DX test is used for small hormone receptor-positive tumors that have not spread to more than 3 lymph nodes, but it may be used for more advanced tumors, too. It can also be used for DCIS (ductal carcinoma in situ or stage 0 breast cancer).
This test looks at a set of 21 genes in cancer cells from tumor biopsy samples to get a “recurrence score,” which is a number between 0 and 100. The score reflects the risk of the breast cancer coming back (recurring) in the next 10 years and how likely you will benefit from getting chemo after surgery.
- A lower score (usually 0-10) means a low risk of recurrence. Most women with low-recurrence scores probably do not benefit from chemotherapy.
- An intermediate score (usually 11-25) means an intermediate risk of recurrence. Most women with intermediate-recurrence scores probably will not benefit from chemo, although women younger than 50 with a higher intermediate score (16-25) might. Women in this group should discuss the possible risks and benefits of chemo with their doctor.
- A high score (usually 26-100) means a higher risk of recurrence. Women with high-recurrence scores are more likely to benefit from chemo to help lower the chance of the cancer coming back.
MammaPrint®: This test can be used to help determine how likely breast cancers are to recur in a distant part of the body after treatment. It can be used in any type of breast cancer that’s small (stage 1 or 2) and has spread to no more than 3 lymph nodes. Hormone and HER2 status are assessed as part of this test.
The test looks at 70 different genes to determine if the cancer is at low risk or high risk of coming back (recurring) in the next 10 years. The test results come back as either “low risk” or “high risk.”
What do the breast cancer gene expression test results mean?
Gene expression testing (gene profiling) can help predict which women will most likely benefit from chemotherapy after breast surgery. This is called adjuvant chemotherapy. Hormone therapy is a standard treatment for hormone receptor-positive breast cancers, but it’s not always clear when to use chemotherapy. These tests can help guide that decision.
Still, these breast cancer gene expression tests cannot tell any one woman for certain if her cancer will come back with or without chemotherapy. Many doctors use these tests (along with other information) to help make decisions about offering chemotherapy. Keep in mind that these tests aren’t needed in all cases. For instance, if you have a fast-growing or a stage 4 breast cancer, you don’t need these tests because you should get chemotherapy as part of standard treatment.
These breast cancer gene expression tests continue to be studied in large clinical trials to better understand how and when to best use them. In the meantime, women might want to ask their doctors if these tests might be useful for them.
Which chemotherapy drugs are used for breast cancer?
In most cases especially as adjuvant or neoadjuvant treatment, chemotherapy is most effective when combinations of drugs are used. Today, doctors use many different combinations, and it’s not clear that any single combination is clearly the best.
The most common drugs used for adjuvant and neoadjuvant chemotherapy include:
- Anthracyclines, such as doxorubicin (Adriamycin) and epirubicin (Ellence)
- Taxanes, such as paclitaxel (Taxol) and docetaxel (Taxotere)
- 5-fluorouracil (5-FU)
- Cyclophosphamide (Cytoxan)
- Carboplatin (Paraplatin)
Most often, combinations of 2 or 3 of these chemotherapy drugs are used.
Chemotherapy for advanced breast cancer
Chemotherapy drugs useful in treating women with breast cancer that has spread include:
- Taxanes, such as paclitaxel (Taxol), docetaxel (Taxotere), and albumin-bound paclitaxel (Abraxane)
- Anthracyclines (Doxorubicin, pegylated liposomal doxorubicin, and Epirubicin)
- Platinum agents (cisplatin, carboplatin)
- Vinorelbine (Navelbine)
- Capecitabine (Xeloda)
- Gemcitabine (Gemzar)
- Ixabepilone (Ixempra) Albumin-bound paclitaxel (nab-paclitaxel or Abraxane)
- Eribulin (Halaven)
Although drug combinations are often used to treat early breast cancer, advanced breast cancer more often is treated with single chemo drugs. Still, some combinations, such as paclitaxel plus carboplatin, are commonly used to treat advanced breast cancer.
For cancers that are HER2-positive, one or more drugs that target HER2 may be used with chemotherapy.
How is breast cancer chemotherapy given?
Chemotherapy drugs for breast cancer are typically given into a vein (IV), either as an injection over a few minutes or as an infusion over a longer period of time. This can be done in a doctor’s office, chemotherapy clinic, or in a hospital setting.
Often, a slightly larger and sturdier IV is required in the vein system to administer chemotherapy. They are known as central venous catheters (CVCs), central venous access devices (CVADs), or central lines. They are used to put medicines, blood products, nutrients, or fluids right into your blood. They can also be used to take out blood for testing.
Many different kinds of central venous catheters are available. The 2 most common types are the port and the PICC line. For breast cancer patients, the central line is typically placed on the opposite side of the breast that had surgery.
Doctors give chemotherapy in cycles, with each period of treatment followed by a rest period to give you time to recover from the effects of the drugs. Cycles are most often 2 or 3 weeks long. The schedule varies depending on the drugs used. For example, with some drugs, the chemotherapy is given only on the first day of the cycle. With others, it is given for a few days in a row, or once a week. Then, at the end of the cycle, the chemotherapy schedule repeats to start the next cycle.
Adjuvant and neoadjuvant chemotherapy is often given for a total of 3 to 6 months, depending on the drugs used. The length of treatment for advanced breast cancer is based on how well it is working and what side effects you have.
Dose-dense chemotherapy
Doctors have found that giving the cycles of certain chemotherapy drugs closer together can lower the chance that the cancer will come back and improve survival for some women. For example, a drug that would normally be given every 3 weeks might be given every 2 weeks. This can be done for both neoadjuvant and adjuvant treatment. It can lead to more problems with low blood cell counts, so it’s not an option for all women.
Possible side effects of chemotherapy for breast cancer
Chemotherapy drugs can cause side effects. These depend on the type and dose of drugs given, and the length of treatment. Some of the most common possible side effects include:
- Hair loss
- Nail changes
- Mouth sores
- Loss of appetite or weight changes
- Nausea and vomiting
- Diarrhea
Chemotherapy can also affect the blood-forming cells of the bone marrow, which can lead to:
- Increased chance of infections (from low white blood cell counts)
- Easy bruising or bleeding (from low blood platelet counts)
- Fatigue (from low red blood cell counts and other reasons)
These side effects usually go away after treatment is finished. There are often ways to lessen these side effects. For example, drugs can be given to help prevent or reduce nausea and vomiting.
Other side effects are also possible. Some of these are more common with certain chemotherapy drugs. Ask your cancer care team about the possible side effects of the specific drugs you are getting.
Menstrual changes and fertility issues
For younger women, changes in menstrual periods are a common side effect of chemotherapy. Premature menopause (not having any more menstrual periods) and infertility (not being able to become pregnant) may occur and may be permanent. Some chemotherapy drugs are more likely to cause this than others. The older a woman is when she gets chemotherapy, the more likely it is that she will go through menopause or become infertile as a result. When this happens, there is an increased risk of bone loss and osteoporosis. There are medicines that can treat or help prevent problems with bone loss.
Even if your periods have stopped while you are on chemotherapy, you may still be able to get pregnant. Getting pregnant while on chemotherapy could lead to birth defects and interfere with treatment. If you are pre-menopausal before treatment and are sexually active, it’s important to discuss using birth control with your doctor. It is not a good idea for women with hormone receptor-positive breast cancer to take hormonal birth control (like birth control pills), so it’s important to talk with both your oncologist and your gynecologist (or family doctor) about what options would be best in your case. Women who have finished treatment (like chemotherapy) can safely go on to have children, but it’s not safe to get pregnant while on treatment.
If you think you might want to have children after being treated for breast cancer, talk with your doctor before you start treatment.
If you are pregnant when you get breast cancer, you still can be treated. Certain chemotherapy drugs can be taken safely during the last 2 trimesters of pregnancy.
Heart damage
Doxorubicin, epirubicin, and some other chemotherapy drugs rarely can cause permanent heart damage (called cardiomyopathy). The risk is highest if the drug is used for a long time or in high doses.
Most doctors will check your heart function with a test like an echocardiogram (an ultrasound of the heart) or a MUGA scan before starting one of these drugs. They also carefully control the doses, watch for symptoms of heart problems, and may repeat the heart test during treatment. If the heart function begins to worsen, treatment with these drugs will be temporarily or permanently stopped. Still, in some people, signs of damage might not appear until months or years after treatment stops. Damage from these drugs happens more often if other drugs that can cause heart damage (such as those that target HER2) are used also, so doctors are more cautious when these drugs are used together.
Nerve damage (neuropathy)
Many drugs used to treat breast cancer, including the taxanes (docetaxel and paclitaxel), platinum agents (carboplatin, cisplatin), vinorelbine, eribulin, and ixabepilone, can damage nerves outside of the brain and spinal cord. This can sometimes lead to symptoms (mainly in the hands and feet) like numbness, pain, burning or tingling sensations, sensitivity to cold or heat, or weakness. In most cases this goes away once treatment is stopped, but it might last a long time in some women or may become permanent . There are medicines that could help.
Treatment is mostly given to relieve the pain that can come with chemotherapy-induced peripheral neuropathy. Some of the drugs used include:
- Steroids for a short time until a long-term treatment plan is in place
- Patches or creams of numbing medicine that can be put right on the painful area (for example, lidocaine patches or capsaicin cream)
- Antidepressant medicines, often in smaller doses than are used to treat depression
- Anti-seizure medicines, which are used to help many types of nerve pain
- Opioids or narcotics, for when pain is severe
Researchers are looking at which drugs work best to relieve this kind of pain. It may take more than one try to find out what works best for you.
Other treatments that can be tried to ease nerve pain and its effects on your life include:
- Electrical nerve stimulation
- Occupational therapy
- Physical therapy
- Relaxation therapy
- Guided imagery
- Distraction
- Acupuncture
- Biofeedback
Physical therapy and occupational therapy may be able to make you stronger. They might also help you find ways to do things that you aren’t able to do because of chemotherapy-induced peripheral neuropathy.
Hand-foot syndrome
Certain chemotherapy drugs, such as capecitabine and liposomal doxorubicin, can irritate the palms of the hands and the soles of the feet. This is called hand-foot syndrome. Early symptoms include numbness, tingling, and redness. If it gets worse, the hands and feet can become swollen and uncomfortable or even painful. The skin may blister, leading to peeling or even open sores. There is no specific treatment, although some creams or steroids given before chemotherapy may help. These symptoms gradually get better when the drug is stopped or the dose is lowered. The best way to prevent severe hand-foot syndrome is to tell your doctor when symptoms first come up, so that the drug dose can be changed or other medicines can be given.
Chemo brain
Many women who are treated for breast cancer report a slight decrease in mental functioning. They may have some problems with concentration and memory, which may last a long time. Although many women have linked this to chemotherapy, it also has been seen in women who did not get chemotherapy as part of their treatment. Still, most women function well after treatment. In studies that have found chemotherapy brain to be a side effect of treatment, the symptoms most often last for a few years.
Increased risk of leukemia
Very rarely, certain chemotherapy drugs can cause diseases of the bone marrow, such as myelodysplastic syndromes or even acute myeloid leukemia, a cancer of white blood cells. When this happens it is usually within 10 years after treatment. For most women, the benefits of chemotherapy in helping prevent breast cancer from coming back or in extending life are far likely to exceed the risk of this rare but serious complication.
Feeling unwell or tired (fatigue)
Many women do not feel as healthy after chemotherapy as they did before. There is often a residual feeling of body pain or achiness and a mild loss of physical functioning. These may be very subtle changes that happen slowly over time.
Fatigue is another common problem for women who have received chemotherapy. This may last up to several years. It can often be helped, so it’s important to let your doctor or nurse know about it. Exercise, naps, and conserving energy may be recommended. If you have sleep problems, they can be treated. Sometimes women become depressed, which may be helped by counseling and/or medicines.
FOLFOX chemotherapy
FOLFOX chemotherapy is a combination of chemotherapy drugs used to treat bowel cancer. FOLFOX chemotherapy is also known as Oxaliplatin de Gramont or OxMdG, which means modified Oxaliplatin de Gramont.
FOLFOX chemotherapy is made up of:
- Folinic acid (also called leucovorin, FA or calcium folinate)
- Fluorouracil (5FU)
- Oxaliplatin
FOLFOX chemotherapy drugs destroy quickly dividing cells, such as cancer cells.
How you have FOLFOX chemotherapy
You have folinic acid, 5FU and oxaliplatin into your bloodstream. If you have a central line, a PICC line or a portacath, you may be able to have the infusions of 5FU at home.
If you are at home, you have the infusions through a small pump. You can keep the pump in a small bag, or a bag on a belt (like a bum bag). You’ll need to go back to the hospital for the second day of your treatment, to have the pump changed. Or sometimes a chemotherapy nurse may be able to change the infusion at your home.
When you have FOLFOX chemotherapy treatment
You have FOLFOX chemotherapy as cycles of treatment each lasting 2 weeks. Depending on your needs, you may have up to 12 cycles.
Day 1
- oxaliplatin through a drip into the bloodstream over 2 hours
- an injection of folinic acid into the bloodstream at the same time
- an injection of 5FU into a cannula or central line into the bloodstream
- an infusion of 5FU through a drip or pump into the bloodstream for 22 hours (or 46 hours if you have modified Oxaliplatin de Gramont)
Day 2
- folinic acid as an injection or through a drip into the bloodstream for 2 hours
- an injection into the bloodstream of 5FU
- a 5FU infusion through a drip or pump into the bloodstream for 22 hours
Day 3 to 14
- you have no treatment for 12 days
Then you start the cycle again.
Tests during FOLFOX chemotherapy treatment
You have blood tests before starting treatment and during your treatment. They check your levels of blood cells and other substances in the blood. They also check how well your liver and kidneys are working.
FOLFOX chemotherapy Important information
Other medicines
Cancer drugs can interact with some other medicines and herbal products. Tell your doctor or pharmacist about any medicines you are taking. This includes vitamins, herbal supplements and over the counter remedies.
Pregnancy and contraception
This treatment might harm a baby developing in the womb. It is important not to become pregnant or father a child while you are having treatment and for a few months afterwards. Talk to your doctor or nurse about effective contraception before starting treatment.
Breastfeeding
Don’t breastfeed during this treatment because the drug may come through in your breast milk.
Treatment for other conditions
Always tell other doctors, nurses, pharmacists or dentists that you’re having this treatment if you need treatment for anything else, including teeth problems.
DPD deficiency
Around 5 out of 100 people (5%) have low levels of an enzyme called DPD (dihydropyrimidine dehydrogenase) in their bodies. A lack of DPD (dihydropyrimidine dehydrogenase) can mean you’re more likely to have severe side effects from fluorouracil. It doesn’t cause symptoms so you won’t know if you have a dihydropyrimidine dehydrogenase deficiency. Contact your doctor if your side effects are severe.
Immunizations
Don’t have immunizations with live vaccines while you’re having treatment and for at least 6 months afterwards.
In the US, live vaccines include rubella, mumps, measles, BCG, yellow fever and shingles vaccine (Zostavax).
You can:
- have other vaccines, but they might not give you as much protection as usual
- have the flu vaccine
- be in contact with other people who’ve had live vaccines as injections
Avoid contact with people who’ve had live vaccines taken by mouth (oral vaccines). This includes the rotavirus vaccine given to babies. The virus is in the baby’s urine for up to 2 weeks and can make you ill. So, avoid changing their nappies for 2 weeks after their vaccination if possible. Or wear disposable gloves and wash your hands well afterwards.
You also need to avoid anyone who has had oral polio or typhoid vaccination recently.
FOLFOX chemotherapy side effects
Tell your doctor or nurse if you have any side effects so they can help you manage them. Your nurse will give you a contact number to ring if you have any questions or problems. If in doubt, call them.
Common side effects
Each of these effects happens in more than 1 in 10 people (10%). You might have one or more of them.
Increased risk of getting an infection
Signs of an infection include headaches, aching muscles, a cough, a sore throat, pain passing urine, or feeling cold and shivery.
Contact your treatment centre straight away if you have any of these signs or if your temperature goes above 100.5°F (38 °C). Severe infections can be life threatening.
Chemotherapy reduces the number of white blood cells in the blood. This increases your risk of infections. White blood cells help fight infections.
When the level is very low it is called neutropenia.
You have antibiotics if you develop an infection. You might have them as tablets or as injections into the bloodstream (intravenously). To have them into your bloodstream you need to go into hospital.
Breathlessness and looking pale
Chemotherapy makes the level of red blood cells fall (anemia). Red blood cells contain hemoglobin, which carries oxygen around the body. When the level of red blood cells is low you have less oxygen going to your cells. This can make you breathless and look pale. Tell your doctor or nurse if you feel breathless.
You have regular blood tests to check your red blood cell levels. You might need a blood transfusion if the level is very low. After a transfusion, you will be less breathless and less pale.
You can also feel tired and depressed when your blood count is low and feel better once it is back to normal. The levels can rise and fall during your treatment. So it can feel like you are on an emotional and physical roller coaster.
Bruising, bleeding gums or nosebleeds
You might notice you:
- bruise more easily
- have nosebleeds
- have bleeding gums when you brush your teeth
This is due to a drop in the number of platelets that help clot your blood.
If your platelets get very low you may have lots of tiny red spots or bruises on your arms or legs called petechiae.
Tell your doctor or nurse straight away if you have petechiae.
You’ll have a platelet transfusion if your platelet count is very low. It is a drip of a clear fluid containing platelets. It takes about 15 to 30 minutes. The new platelets start to work right away.
Tiredness and weakness (fatigue) during and after treatment
You might feel very tired during your treatment. It might take 6 months to a year for your energy levels to get back to normal after the treatment ends. A low red blood cell count will also make you feel tired.
You can do things to help yourself, including some gentle exercise. It’s important not to push yourself too hard. Try to eat a well balanced diet.
Talk to your doctor or nurse if you are finding the tiredness difficult to manage.
Feeling or being sick
Feeling or being sick happens to about 7 out of every 10 people (70%) but is usually well controlled with anti sickness drugs. If the sickness is not controlled, let your nurse know as there are other anti sickness medicines that may work better for you.
Pain in the vein
This drug may cause pain along the vein where you have the injection. Tell your nurse if this happens. They may need to give the drug more slowly.
Diarrhea
Tell your doctor or nurse if you have diarrhea. They can prescribe medicine to help you.
Drink at least 2.5 liters of fluid a day. This helps to keep you hydrated.
Ask your nurse about soothing creams to apply around your back passage (rectum). The skin in that area can get very sore and even break if you have severe diarrhea. Contact your doctor or nurse immediately if you have diarrhea 4 or more times a day, or any diarrhea at night.
Mouth sores and ulcers
Your mouth might become sore about 5 to 10 days after you start treatment. It usually clears up gradually 3 to 4 weeks after your treatment ends.
Your doctor or nurse can give you mouthwashes to help prevent infection. You have to use these regularly to get the most protection.
Tell your doctor or nurse straight away if your mouth is really sore. They can help to reduce the discomfort. Some people need strong painkillers to help control mouth pain so they can eat and drink.
Tips for managing mouth sores and ulcers:
- Clean your mouth and teeth gently every morning and evening and after each meal.
- Use mouthwashes as advised by your doctor or nurse. Let them know if the mouthwash stings. They can tell you to stop using it or dilute it with water.
- Use dental floss daily but be gentle so that you don’t harm your gums, and don’t floss if you have very low platelets.
- Avoid neat spirits, tobacco, hot spices, garlic, onion, vinegar and salty food.
- Moisten meals with gravies and sauces to make swallowing easier.
- Avoid acidic fruits such as oranges, grapefruit or lemons.
Menstrual periods stopping
Women might stop having periods (amenorrhea) but this may be temporary.
Loss of fertility
Talk to your doctor before starting treatment if you think you may want to have a baby in the future.
- Men
You may be able to store sperm before starting treatment.
It can take a few months or sometimes years for fertility to return to normal. You can have sperm counts to check your fertility when your treatment is over. Ask your doctor about it.
- Women
Chemotherapy can cause an early menopause. This stops you from being able to become pregnant in the future. Talk to your doctor about this before your treatment. It’s sometimes possible to store eggs or embryos before treatment.
A mild or severe allergic reaction to oxaliplatin
An allergic reaction can happen during or shortly after your treatment.
A mild allergic reaction causes a rash, itching or a red face.
Some people can have a more severe reaction. You might have steroids and other medicine before your treatment to try to stop this happening. Let your nurse or doctor know straight away if you have:
- a sudden skin rash
- itching
- breathlessness
- swelling of the lips, face or throat
Your chemotherapy nurse will keep a close eye on you and give treatment straight away if this happens.
Occasional side effects
Each of these effects happens in more than 1 in 100 people (1%). You might have one or more of them.
Soreness, redness and peeling on palms and soles of feet
The skin on your hands and feet can become sore, red, and peel. You might also have tingling, numbness, pain and dryness. This is called hand-foot syndrome or palmar plantar syndrome.
Runny nose
You might have a runny nose while having treatment.
Skin sensitivity to sunlight
Don’t use sunbeds or sit in the sun. Cover up or use sunscreen if you go out in the sun.
Remember to put sun cream on your head or wear a hat if you have lost hair there.
A brown marking on the skin following the vein
A brown marking on the skin following the line of the vein where fluorouracil has been injected can appear. This usually fades over time. Speak to your doctor or nurse if you are worried about this.
Hair thinning
Your hair may thin. It usually begins falling out gradually within 2 to 3 weeks after treatment starts.
Your hair grows back once your treatment has finished. This can take several months and your hair is likely to be softer.
Brittle, chipped and ridged nails
Your nails can have a blue tinge or become darker. Or they might flake, be painful and thicken where the nail starts growing (the nail bed).
Watery or sore eyes
Watery eyes is also called excessive tearing or epiphora. It may be due to a blockage in the drainage system of the eye, caused by swelling of the nearby tissues. Or your eyes may make too many tears.
Tell your doctor or nurse if this is a problem. They can prescribe medicines to help reduce swelling.
Some irritants can make the watering worse. These can include dust, pollen or animal hairs. Try to avoid them or wear protective goggles.
Your eyes may be sore because the drugs cause a reaction on the inside of your eyelids. Or you may not be making enough tears. Your eyes can feel sore and gritty and might be red.
Tell your doctor or nurse if you have dry eyes. They can prescribe eye drops, ointments or artificial tears for you.
Warm compresses can help your eye to drain if you have an infection.
Rare side effects
Each of these effects happens in fewer than 1 in 100 people (1%). You might have one or more of them.
Difficulty swallowing or breathing
This can be triggered by cold air in the first 5 days after having oxaliplatin. This usually clears up on its own.
Tell your doctor or nurse if you have this and avoid cold drinks or ice cubes for the first few days after treatment.
Ringing in your ears (tinnitus)
You might notice a ringing sound in your ears (tinnitus). This often gets better on its own once the treatment ends.
Chemotherapy side effects
Cancer cells tend to grow fast, and chemotherapy drugs kill fast-growing cells. But because these chemotherapy drugs travel throughout the body, they can affect normal, healthy cells that are fast-growing, too. Damage to healthy cells causes side effects. Side effects are not always as bad as you might expect, but many people worry about this part of cancer treatment.
As well as killing cancer cells, chemotherapy can damage some healthy cells in the body, such as blood cells, skin cells and cells in the stomach.
The normal cells most likely to be damaged by chemotherapy are :
- Blood-forming cells in the bone marrow
- Hair follicles
- Cells in the mouth, digestive tract, and reproductive system
This can cause a range of unpleasant side effects, such as:
- feeling tired most of the time
- feeling sick and vomiting
- hair loss
- an increased risk of picking up infections
- a sore mouth
- dry, sore or itchy skin
- diarrhea or constipation
Many of these side effects can be treated or prevented and most, if not all, will pass after treatment stops.
Some chemotherapy drugs can damage cells in the heart, kidneys, bladder, lungs, and nervous system. Sometimes, you can take medicines with the chemotherapy to help protect your body’s normal cells. There are also treatments to help relieve side effects.
Doctors try to give chemotherapy at levels high enough to treat cancer, while keeping side effects at a minimum. They also try to avoid using multiple chemotherapy drugs that have similar side effects.
What are common chemotherapy side effects?
Most people worry about whether they’ll have side effects from chemotherapy, and, if so, what they’ll be like. Here are some of the more common side effects caused by chemotherapy:
- Fatigue
- Hair loss
- Easy bruising and bleeding
- Infection
- Anemia (low red blood cell counts)
- Nausea and vomiting
- Appetite changes
- Constipation
- Diarrhea
- Mouth, tongue, and throat problems such as sores and pain with swallowing
- Nerve and muscle problems such as numbness, tingling, and pain
- Skin and nail changes such as dry skin and color change
- Urine and bladder changes and kidney problems
- Weight changes
- Chemo brain, which can affect concentration and focus
- Mood changes
- Changes in libido and sexual function
- Fertility problems
Chemotherapy drug interactions and side effects
When looking at how best to combine chemotherapy drugs, doctors must look at interactions between chemotherapy drugs and other medicines the person is taking, including over-the-counter medicines, vitamins, and supplements. These interactions may make side effects worse and affect how well chemotherapy drugs work.
It’s important that you tell your doctor about all medicines, including over-the counter medicines, vitamins, herbal or dietary supplements you are taking– even if you only take them “as needed.”
For instance, platelets help blood clot and prevent bleeding. Many chemotherapy drugs lower the number of platelets for a time. Taking aspirin or other related drugs can also weaken blood platelets. This isn’t a problem for healthy people with normal platelet counts. But if a person has low platelet counts from chemotherapy, this combination might put them at risk of a serious bleeding problem.
Your doctor can talk with you about the safety of using other medicines, vitamins, and supplements while you are being treated for cancer.
How vitamins affect chemotherapy drugs
Many people want to take an active role in improving their overall health. They want to help their body’s natural defenses fight the cancer and speed up their recovery from chemotherapy.
Because most people think of vitamins as a safe way to improve health, it’s not surprising that many people with cancer take high doses of one or more vitamins. But some vitamins might make chemotherapy less effective.
Certain vitamins, such as A, E, and C act as antioxidants. This means that they can prevent formation of ions (free radicals) that damage DNA. This damage is thought to have an important role in causing cancer.
Some chemotherapy drugs (as well as radiation treatments) work by producing these same types of free radical ions. These ions damage the DNA of cancer cells so the cells are unable to grow and reproduce. Some scientists believe that taking high doses of antioxidants during treatment may make chemotherapy or radiation less effective.
Few studies have been done to fully test this theory. But until more is known about the effects of vitamins on chemotherapy, keep these points in mind:
- If your doctor has not told you to take vitamins, it’s best not to take any.
- A simple multivitamin is probably OK for people who want to take a vitamin supplement, but always check with your doctor first.
- It’s safest to avoid taking high doses of antioxidant vitamins or supplements during cancer treatment. Ask your doctors if and when it might be OK to start such vitamins after treatment.
- If you’re concerned about nutrition, you can usually get plenty of vitamins by eating a well-balanced diet.
What do I need to know about side effects?
- Every person doesn’t get every side effect, and some people get few, if any.
- The severity of side effects (how bad they are) varies greatly from person to person. Be sure to talk to your cancer care team about which side effects are most common with your chemo, how long they might last, how bad they might be, and when you should call the doctor’s office about them.
- Your doctor may give you medicines to help prevent certain side effects before they happen.
- Some chemo drugs cause long-term side effects, like heart or nerve damage or fertility problems. Still, many people have no long-term problems from chemo. Ask your doctor if the chemo drugs you’re getting have long-term effects.
While side effects can be unpleasant, they must be weighed against the need to kill the cancer cells.
Be sure to talk to your cancer care team about which side effects are most common with your chemo, how long they might last, how bad they might be, and when you should call the doctor’s office about them.
How long do side effects last?
Many side effects go away fairly quickly after treatment ends, but some may take months or even years to completely go away. The time it takes to get over some side effects and get your energy back varies from person to person. It depends on many factors, including your overall health and the drugs you were given.
Many side effects go away fairly quickly, but some might take months or even years to go away completely. Sometimes the side effects can last a lifetime, such as when chemo causes long-term damage to the heart, lungs, kidneys, or reproductive organs. Certain types of chemo sometimes cause delayed effects, such as a second cancer that may show up many years later.
People often become discouraged about how long their treatment lasts or the side effects they have. If you feel this way, talk to your cancer care team. You may be able to change your medicine or treatment schedule. They also may be able to suggest ways to reduce any pain and discomfort you have.
When to call your cancer care team about side effects from chemotherapy
While you’re getting chemotherapy, you’ll probably notice every physical change and imbalance. Do not take any physical symptoms you have lightly.
Some side effects are short-lived and minor, but others may be a sign of serious problems. You should not be the judge. Make sure you know how to reach someone on your team any time, including after hours, weekends, and holidays.
Contact your cancer care team right away if you have any of the following symptoms during chemo treatment:
- A fever of 100.5 °F (38 °C) or greater (taken by mouth)
- Bleeding or unexplained bruising
- A rash or allergic reaction, such as swelling of the mouth or throat, severe itching, trouble swallowing
- Intense chills
- Pain or soreness at the chemo injection site or catheter site
- Unusual pain, including intense headaches
- Shortness of breath or trouble breathing (If you’re having trouble breathing call your local emergency services number first.)
- Long-lasting diarrhea or vomiting
- Bloody stool or blood in your urine
Ask your cancer care team if there are any other problems they should know about right away.





{kind=link}