Contents
What is cholecystectomy
Cholecystectomy is a surgery to remove the gallbladder due to gallstones causing pain or infection and is one of the most common operations performed on adults in the United States. Gallstones that cause biliary colic (acute pain in the abdomen caused by spasm or blockage of the cystic or bile duct) are the most common reason for a cholecystectomy. Gallstones are one of the major causes of morbidity in western society. It is estimated that the incidence of symptomatic cholecystolithiasis is up to 2.17 per thousand inhabitants 1 with an annual performance rate of cholecystectomies of more than 500,000 in the USA 2.
The gallbladder is not an essential organ, which means a person can live normally without a gallbladder. Once the gallbladder is removed, bile flows out of the liver through the hepatic and common bile ducts and directly into the duodenum, instead of being stored in the gallbladder.
Surgeons perform two types of cholecystectomy:
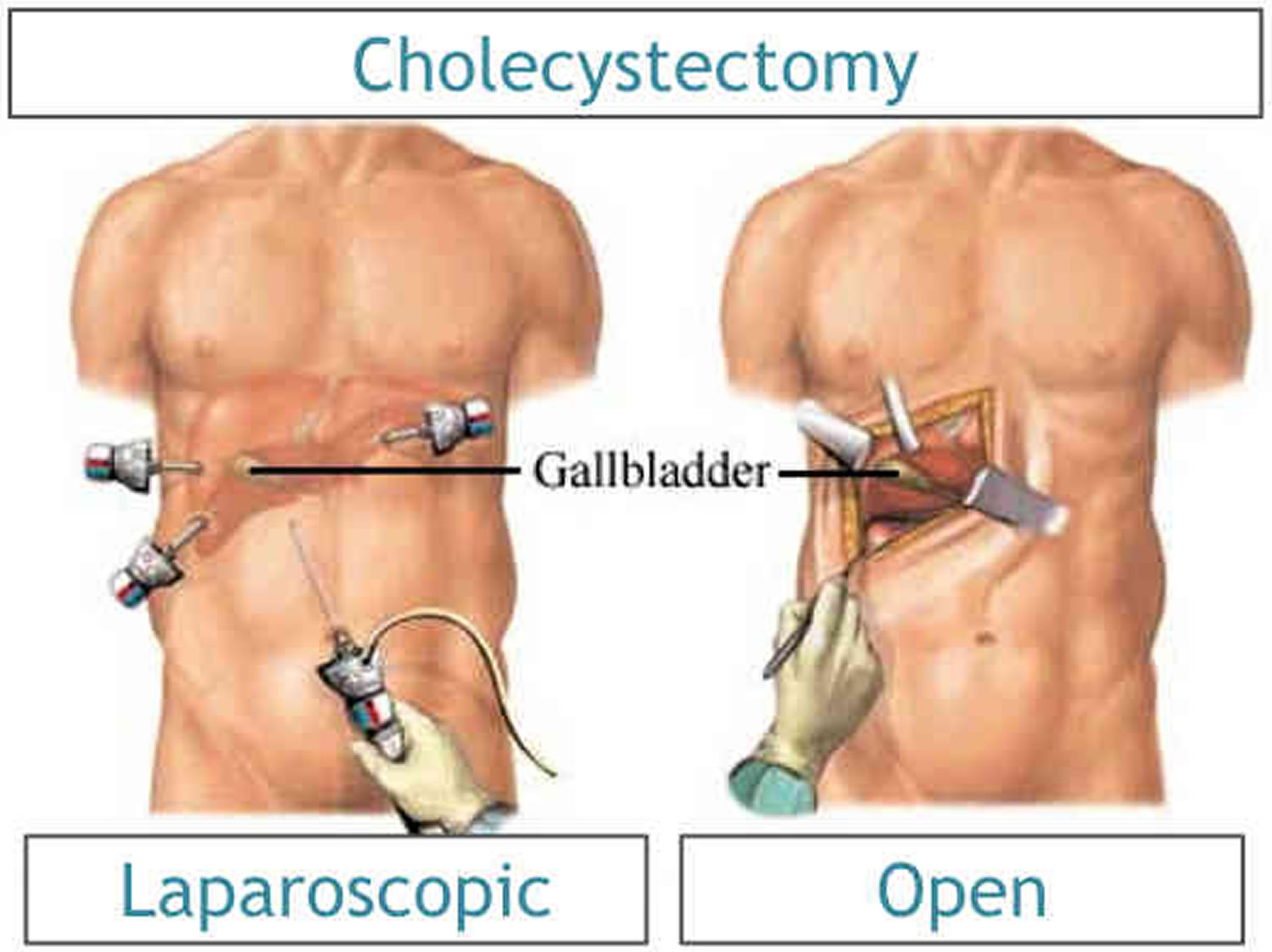
- Laparoscopic cholecystectomy. The gallbladder is removed with laparoscopic instruments (a long, thin telescope with a light and camera at the end) placed into the abdomen through several small incisions. Almost all surgeons perform cholecystectomies with laparoscopy. The laparoscopic cholecystectomy procedure takes about 1 to 2 hours. Surgeons perform many laparoscopic cholecystectomies on an outpatient basis, meaning you may be able to go home the same day. You will probably be able to return to normal physical activity in about a week.
- Open cholecystectomy. The surgeon makes an incision approximately 6 inches long in the upper right side of the abdomen under the rib cage and cuts through the fat and muscle to the gallbladder. A surgeon performs an open cholecystectomy when your gallbladder is severely inflamed, infected, or scarred from other operations. Your doctor may perform an open cholecystectomy if problems occur during a laparoscopic cholecystectomy. The gallbladder is removed, and any ducts are clamped off. The site is stapled or sutured closed. A small drain may be placed going from the inside to the outside of the abdomen. The drain is usually removed in the hospital. The procedure takes about 1 to 2 hours. After the surgery, you may need to stay in the hospital for up to a week. You will probably be able to return to normal physical activity after about a month.
Both techniques are performed under general anaesthetic, which means you’ll be asleep during the operation and won’t feel any pain while it’s carried out.
Until the end of the 1980s, open cholecystectomy was the gold standard for treatment of stones in the gallbladder 3. Laparoscopic cholecystectomy was introduced in 1985 4 and rapidly became the method of choice for surgical removal of the gallbladder 2.
Laparoscopic (keyhole) cholecystectomy surgery is used most often because you can leave hospital sooner, recover faster and are left with smaller scars than with an open procedure.
Gallstones are hardened digestive fluid that can form in your gallbladder. The medical term for gallstone formation is cholelithiasis. Gallstones can leave the gallbladder and block the flow of bile to the ducts and cause pain and swelling of the gallbladder. A gallstone in the common bile duct is called choledocholithiasis. Cholecystitis is inflammation of the gallbladder, which can happen suddenly (acute) or over a longer period of time (chronic). Gallstone Pancreatitis is caused by stones moving into and blocking the common bile duct, the pancreatic duct, or both. A cholecystectomy may be recommended 5.
The most common symptoms of cholecystitis are 5:
- Sharp pain in the right abdomen
- Low grade fever
- Nausea and bloating
- Jaundice (yellowing of the skin) may occur if gallstones are in the common bile duct
Benefits of gallbladder removal are pain relieve, treat infection and, in most cases, stop gallstones from coming back.
Possible risks of cholecystectomy include — Bile leak, bile duct injury, bleeding, infection of the abdominal cavity (peritonitis), fever, liver injury, infection, numbness, raised scars, hernia at the incision, anesthesia complications, puncture of the intestine, and death 5.
Risks of not having cholecystectomy operation — The possibility of continued pain, worsening symptoms, infection or bursting of the gallbladder, serious illness, and possibly death 6.
The day of your gallbladder removal surgery — You will not eat for 4 hours but may drink clear liquids up to 2 hours before the operation. Most often, you will take your normal medication with a sip of water. You will need someone to drive you home.
Gallbladder removal recovery — If you do not have complications, you usually will go home the same day after a laparoscopic procedure or in 1 to 2 days after an open procedure.
Figure 1. Cholecystectomy
Why does your gallbladder need to be removed?
Surgery to remove the gallbladder is usually carried out if you have painful gallstones. These are small stones that can form in the gallbladder as a result of an imbalance in the substances that make up bile.
A cholecystectomy is most commonly performed to treat gallstones and the complications they cause. Your doctor may recommend a cholecystectomy if you have:
- Gallstones in the gallbladder (cholelithiasis)
- Gallstones in the bile duct (choledocholithiasis)
- Gallbladder inflammation (cholecystitis)
- Pancreas inflammation (pancreatitis) due to gallstones
Gallstones often cause no symptoms and you may not realize you have them, but occasionally they can block the flow of bile and irritate the gallbladder (acute cholecystitis) or pancreas (acute pancreatitis).
This can cause symptoms such as:
- sudden and intense tummy pain
- feeling and being sick
- yellowing of the skin and the whites of the eyes (jaundice)
Very occasionally it may be possible to take tablets to dissolve gallstones, but surgery to remove the gallbladder is the most effective treatment in the vast majority of cases.
You’ll need to have a pre-operative assessment in hospital during the weeks leading up to your gallbladder removal surgery (cholecystectomy).
Gallbladder removal surgery preparation
How you prepare
You’ll need to have a pre-operative assessment in hospital during the weeks leading up to your gallbladder removal surgery (cholecystectomy).
During this appointment:
- you may have some blood tests and a general health check to make sure that you’re fit for surgery and determine whether a keyhole or open procedure (see below) is most suitable for you
- you can discuss any concerns or ask any questions about your operation
- you’ll be advised about things you can do to reduce your risk of problems after surgery, such as stopping smoking
- you’ll be told about when you need to stop eating and drinking before your operation – this will usually be from the night before.
To prepare for a cholecystectomy, your surgeon may ask you to:
- Eat nothing the night before your surgery. You may drink a sip of water with your medications, but avoid eating and drinking at least four hours before your surgery.
- Stop taking certain medications and supplements. Tell your doctor about all the medications and supplements you take. Continue taking most medications as prescribed. Your doctor may ask you to stop taking certain medications and supplements because they may increase your risk of bleeding.
Prepare for your recovery
Plan ahead for your recovery after surgery. For instance:
- Plan for a hospital stay. Most people go home the same day of their cholecystectomy, but complications can occur that require one or more nights in the hospital. If the surgeon needs to make a long incision in your abdomen to remove your gallbladder, you may need to stay in the hospital longer. It’s not always possible to know ahead of time what procedure will be used. Plan ahead in case you need to stay in the hospital by bringing personal items, such as your toothbrush, comfortable clothing, and books or magazines to pass the time.
- Find someone to drive you home and stay with you. Ask a friend or family member to drive you home and stay close the first night after surgery.
Gallbladder removal side effects
You can live perfectly normally without a gallbladder, so there aren’t usually any long-term effects from gallbladder removal surgery.
However, it’s common to experience some temporary side effects while you recover, including:
- swollen, bruised and painful wounds – this should start to improve within a few days; regular painkillers such as paracetamol may help reduce the discomfort
- feeling sick – you may feel sick as a result of the anaesthetic or painkillers you’ve been given, but this should pass quickly
- pain in your tummy and shoulders – this is a result of the gas used to inflate your tummy and should pass after a couple of days; painkillers can be taken to relieve the discomfort
- bloating, flatulence and diarrhea – this can last a few weeks; eating high-fibre food such as fruit, vegetables, brown rice and wholemeal bread can help to firm up your stools, and your doctor may also be able to prescribe medication to help
- fatigue, mood swings and irritability – these feelings should improve as you recover
These side effects are completely normal and not usually a cause for concern. You only need to contact your GP, the hospital or NHS 111 for advice if they’re particularly severe or persistent.
A cholecystectomy carries a small risk of complications including:
- Bile leak
- Bleeding
- Blood clots
- Heart problems
- Infection
- Injury to nearby structures, such as the bile duct, liver and small intestine
- Pancreatitis
- Pneumonia
Your risk of complications depends on your overall health and the reason for your cholecystectomy.
Gallbladder removal complications
Removal of the gallbladder (cholecystectomy) is considered a relatively safe procedure, but like all operations there is a small risk of complications.
Infection
Some people develop a wound or internal infection after a gallbladder removal.
Signs of a possible infection include increasing pain, swelling or redness, and pus leaking from a wound. See your doctor if you develop these symptoms, as you may need a short course of antibiotics.
Bleeding
Bleeding can occur after your operation, although this is rare. If it does occur, it may require a further operation to stop it.
Bile leakage
When the gallbladder is removed, special clips are used to seal the tube that connects the gallbladder to the main bile duct. However, bile fluid can occasionally leak out into the tummy (abdomen) after the gallbladder is removed.
Symptoms of a bile leak include tummy pain, feeling sick, a fever and a swollen tummy.
Sometimes this fluid can be drained off. Occasionally, an operation is required to drain the bile and wash out the inside of your tummy.
Bile leakage occurs in around 1% of cases.
Injury to the bile duct
In around 1 in 500 cases, the bile duct is damaged during a gallbladder removal.
If this happens during surgery, it may be possible to repair it straight away. In some cases, further surgery is needed after your original operation.
Injury to the intestine, bowel and blood vessels
The surgical instruments used to remove the gallbladder can also injure surrounding structures, such as the intestine, bowel and blood vessels.
This type of injury is rare, occurring in around 1 in 1,000 cases, and can usually be repaired at the time of the operation. Sometimes injuries are noticed afterwards and a further operation is needed.
Deep vein thrombosis
Some people are at a higher risk of blood clots developing after surgery. This is known as deep vein thrombosis (DVT) and usually occurs in a leg vein.
This can be serious because the clot can travel around the body and could block the flow of blood into the lungs (pulmonary embolism).
You may be given special compression stockings to wear after the operation to prevent this happening.
Risks from general anaesthetic
There are several serious complications associated with having a general anaesthetic, but these are very rare.
Complications include allergic reaction and death. Being fit and healthy before your operation reduces the risk of any complications occurring.
Post-cholecystectomy syndrome
Some people experience symptoms similar to those caused by gallstones after surgery, including :
- tummy pain
- indigestion
- diarrhea
- yellowing of the eyes and skin (jaundice)
- a high temperature (fever) of 38 °C (100.4 °F) or above
This is known as post-cholecystectomy syndrome and it’s thought to be caused by bile leaking into areas such as the stomach or by gallstones being left in the bile ducts.
In most cases symptoms are mild and short-lived, but they can persist for many months. If you do have persistent symptoms, you should contact your doctor for advice.
You may benefit from a procedure to remove any remaining gallstones, or medication to relieve your symptoms.
Table 1. Open Cholecystectomy and Laparoscopic Cholecystectomy Risks and Complications
| Risks | Percent for Average Patient | Comment |
|---|---|---|
| Pneumonia: Infection in the lungs | Open 1.7% Laparoscopic 0.2% | You can decrease your risk by rinsing with mouthwash the morning of your operation (to decrease mouth bacteria), quitting smoking before your operation, and getting up often to walk post-operatively. |
| Heart complication: Heart attack or sudden stopping of the heart | Open 0.7% Laparoscopic 0.1% | Problems with your heart or lungs can be affected by general anesthesia. Your anesthesia provider will take your history and suggest the best option for you. |
| Wound infection | Open 7.6% Laparoscopic 1% | Antibiotics are not routinely given except for high-risk patients. You should wash your abdomen with an antimicrobial soap such as dial the night before the operation. |
| Urinary tract infection: Infection of the bladder or kidneys | Open 1.5% Laparoscopic 0.5% | A Foley catheter is placed during surgery to drain the urine. Let your surgical team know if you have trouble urinating after the tube is removed—this is more common in older men or if an epidural is used for pain. |
| Blood clot: A blood clot in the legs can travel to the lung | Open 1% Laparoscopic 0.2% | Longer surgery and bed rest increase the risk. Walking 5 times/day and wearing support stockings reduce the risk. |
| Renal (kidney) failure: Kidneys no longer function in making urine and/or cleaning the blood of toxins | Open 0.9% Laparoscopic 0.1% | Pre-existing renal problems, Type 1 diabetes, being over 65 years old, and other medications may increase the risk. |
| Return to surgery | Open 3.3 % Laparoscopic 0.8% | Bile leakage or a retained stone may cause a return to surgery. Your surgical team is prepared to reduce all risks of return to surgery. |
| Death | Open 0.8% Laparoscopic 0.1% | Your surgical team will review for possible complications and be prepared to decrease all risks. |
| Discharge to nursing or rehabilitation facility | Open 5.4% Laparoscopic 0.6% | Pre-existing health conditions can increase this risk. |
| Bile Duct Injury/Leakage | 0.50% | Injury can happen between 1 week to 6 months after the operation from fever, pain, jaundice, or bile leakage from the incision. Further testing and surgery may be needed. |
| Retained common bile duct stone | 4% to 40% | A gallstone may pass after surgery and block the bile from draining. The stone should be removed because of an increased risk of biliary obstruction or inflammation of the pancreas or bile duct. |
| Pregnancy Complications, premature labor and fetal loss | Fetal loss 4% (uncomplicated removal) up to 60% if pancreatitis | Most pregnant women with gallstones will have no symptoms during pregnancy. If you have biliary disease or pancreatitis, gallbladder removal will be offered to reduce maternal complications. |
The Gallbladder
The gallbladder is a pear-shaped sac in a depression on the liver’s under surface. The gallbladder is lined with epithelial cells and has a strong layer of smooth muscle in its wall. The gallbladder stores bile between meals, reabsorbs water to concentrate bile, and contracts to release bile into the small intestine. It connects to the cystic duct, which in turn joins the common hepatic duct (Figure 3).
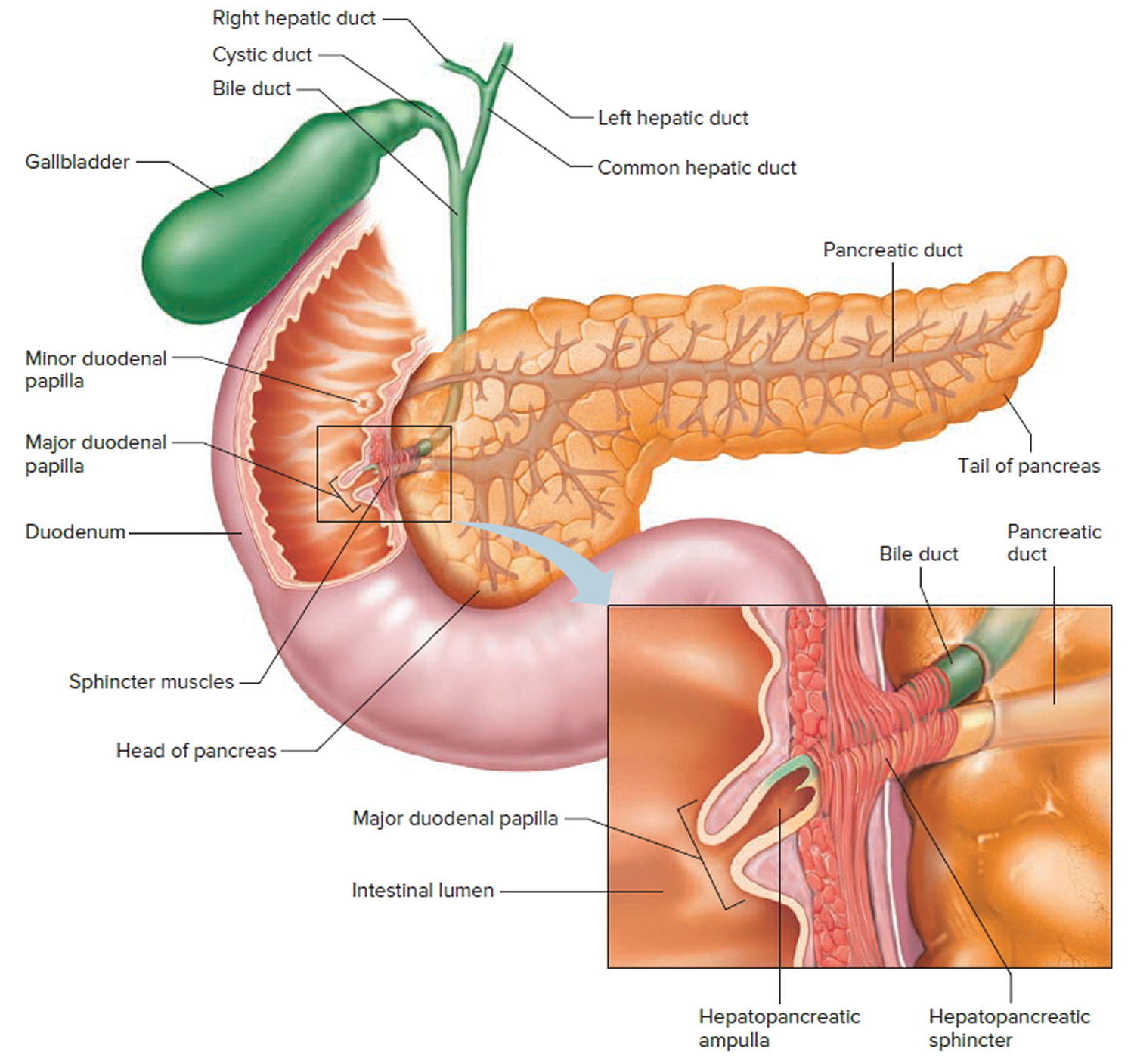
The common hepatic duct and cystic duct join to form the bile duct (common bile duct). It leads to the duodenum where the hepatopancreatic sphincter guards its exit (Figure 4). Because this sphincter normally remains contracted, bile collects in the bile duct. It backs up into the cystic duct and flows into the gallbladder, where it is stored.
Cholesterol in bile may precipitate under certain conditions and form crystals called gallstones. Gallstones in the bile duct may block bile flow into the small intestine and cause considerable pain. A surgical procedure called a cholecystectomy can remove the gallbladder when gallstones are obstructive. The surgery can often be done with a laparoscope (small, lit probe) on an outpatient basis.
Figure 2. Gallbladder location
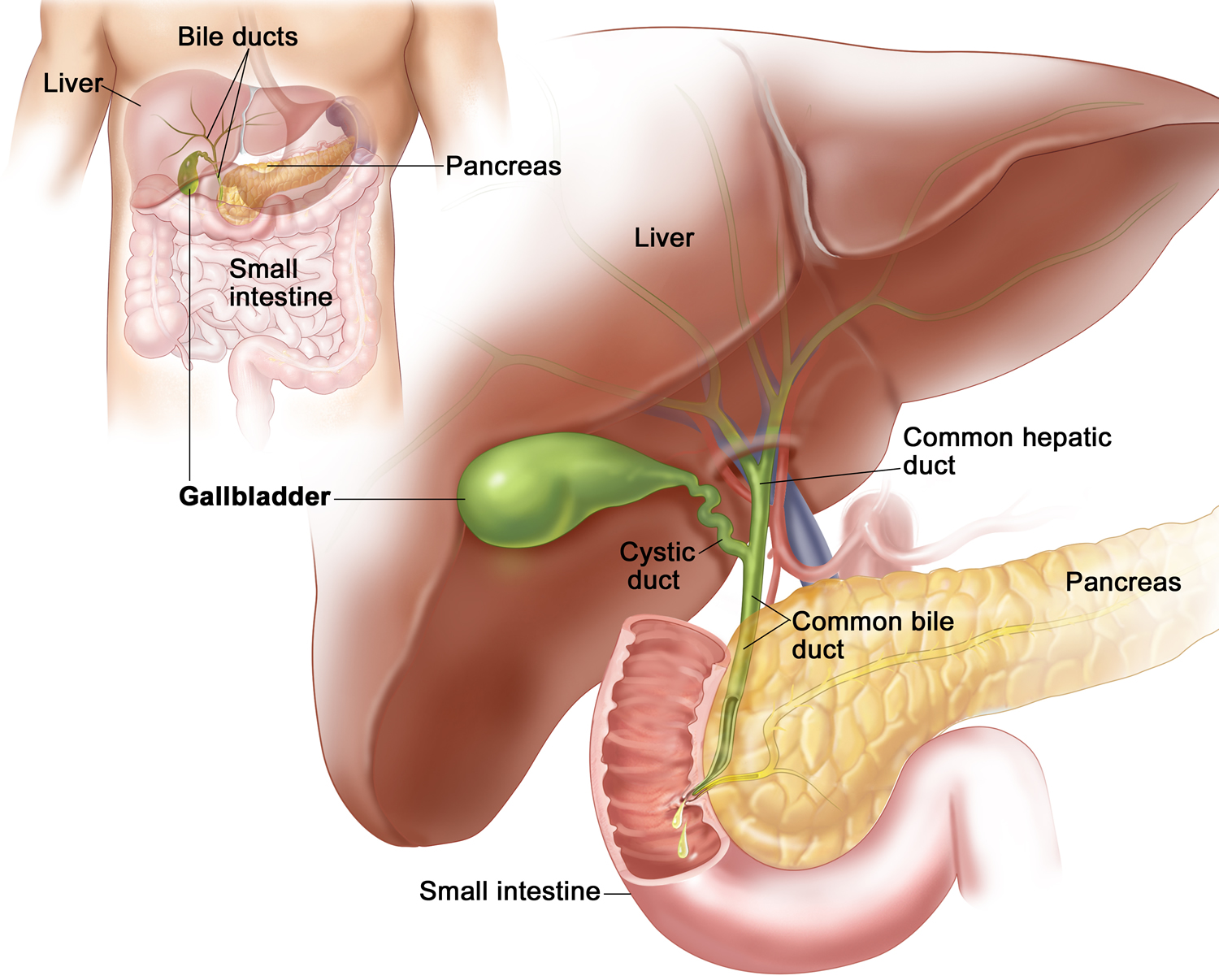
Figure 3. Gallbladder anatomy
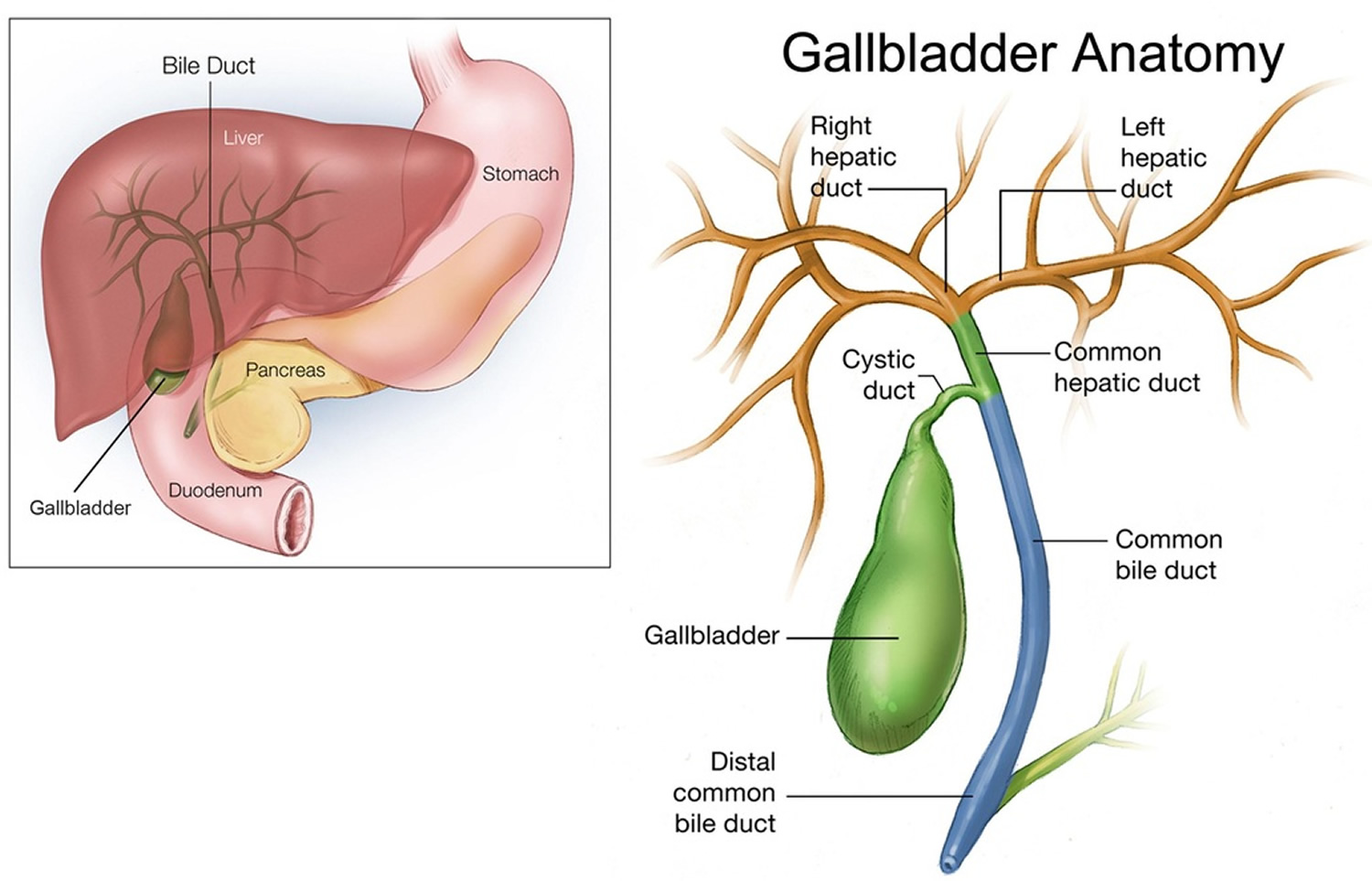
Figure 4. The common bile duct is closely associated with the pancreatic duct and the duodenum
Gallbladder function
Following a meal, the mixing movements of the stomach wall aid in producing a semifluid paste of food particles and gastric juice called chyme.
As chyme enters the duodenum (the proximal portion of the small intestine), accessory organs—the pancreas, liver, and gallbladder—add their secretions.
Bile is a yellowish-green liquid continuously secreted from hepatic (liver) cells. In addition to water, bile contains bile salts, bile pigments (bilirubin and biliverdin), cholesterol, and electrolytes. Of these, bile salts are the most abundant and are the only bile components that have a digestive function.
Bile pigments are breakdown products of hemoglobin from red blood cells and are normally secreted in the bile.
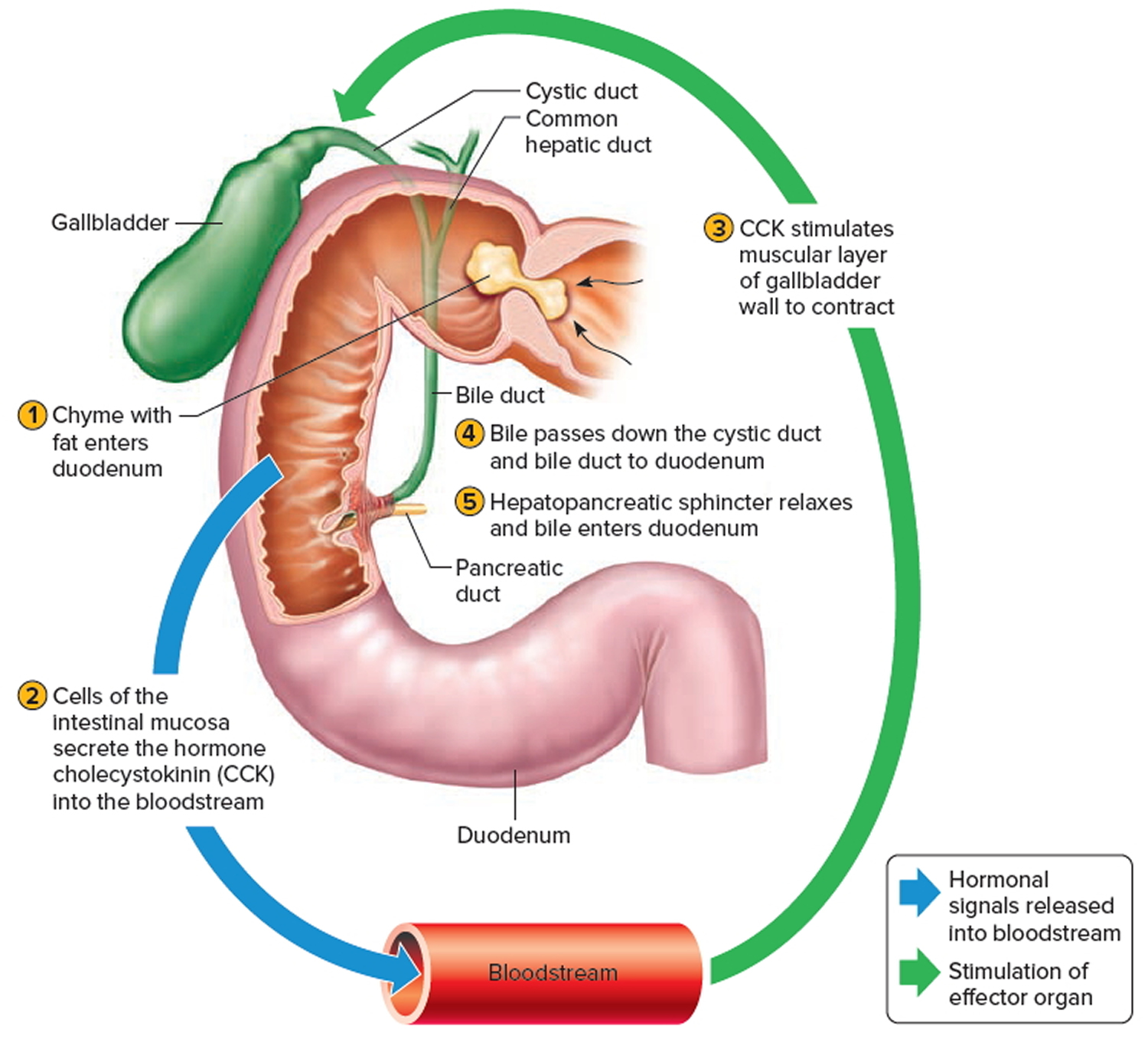
Normally bile does not enter the duodenum until cholecystokinin stimulates the gallbladder to contract. Proteins and fats in chyme in the duodenum stimulate
the intestinal wall to release cholecystokinin. Cholecystokinin travels via the bloodstream to the pancreas also, where it stimulate the pancreas to release its pancreatic juice that has a high concentration of digestive enzymes.
The hepatopancreatic sphincter usually remains contracted until a peristaltic wave in the duodenal wall approaches it. Then the sphincter relaxes, and bile is squirted into the duodenum (see Figure 5).
Note: Cholecystokinin produced by the intestinal wall cells, in response to proteins and fats in the small intestine, decreases secretory activity of gastric glands and inhibits gastric motility; stimulates pancreas to secrete fluid with a high digestive enzyme concentration and stimulates gallbladder to contract and release bile.
Figure 5. Fatty chyme entering the duodenum stimulates the gallbladder to release bile
Gallbladder removal recovery time
How long it takes to recover from gallbladder removal surgery (cholecystectomy) depends on whether you had a laparoscopic (keyhole) or open procedure.
Most people who have keyhole surgery are able to leave hospital on the same day as the operation. It will usually take around two weeks to return to your normal activities.
After open surgery, you’ll usually have to stay in hospital for three to five days and your recovery time will be longer. It can take around six to eight weeks to return to your normal activities.
In either case, you’ll need to arrange for someone to take you home from hospital. Someone should also stay with you for at least 24 hours if you go home the same day as your operation, as you may still be feeling the effects of the anaesthetic.
Diet after gallbladder removal
Most people don’t need to follow a special diet after having surgery to remove their gallbladder, as the gallbladder isn’t essential for digestion.
You can usually start eating normally a few hours after your operation, although you’ll probably prefer to eat small meals to start with.
Most people won’t experience digestive problems after a cholecystectomy. Your gallbladder isn’t essential to healthy digestion. Some people may experience occasional loose stool after the procedure, which generally resolves over time. Discuss with your doctor any changes in your bowel habits or new symptoms following your procedure.
You may have been advised to follow a low-fat diet for several weeks before surgery, but this doesn’t need to be continued afterwards. Instead, you should aim to have a generally healthy, balanced diet (including some fats).
If you experience side effects from surgery – including indigestion, bloating, flatulence or diarrhea – it may help to make some small adjustments to your diet, such as:
- avoid drinks containing caffeine – such as coffee and tea
- avoid foods that make the problems worse – such as spicy or fatty foods
- gradually increase your intake of fiber – good sources of fiber include fresh fruit and vegetables, wholegrain rice, wholewheat pasta and bread, seeds, nuts and oats
Your doctor can also recommend medication if you have diarrhea.
Side effects of gallbladder surgery usually only last a few weeks, although diarrhea can be a more persistent problem for a small number of people.
If you’ve had other organs removed as well as your gallbladder, such as your pancreas, you may have problems digesting food. You’ll be advised about any changes you need to make to your diet after surgery in these cases.
Life after gallbladder removal
Your surgeon can give you specific advice about when you can return to your normal activities. Generally speaking, after keyhole surgery you can:
- eat a normal diet straight away – you can return to a normal diet even if you were advised to avoid certain foods before your operation, although you should try to have a generally healthy and balanced diet (read more about diet after gallbladder surgery)
- do gentle exercises, such as walking – but be careful not to push yourself too hard too soon and ask your surgeon or doctor for advice about returning to more strenuous exercise
- drive again after a week or so – but first make sure you can wear a seat belt and practice an emergency stop without feeling any discomfort
- have sex as soon as you feel up to it – but try not to place weight on your wounds until they’ve healed
- return to work after 10-14 days, depending on what your job involves
It can take a bit longer to return to these activities after open gallbladder removal surgery. For example, you may not be able to drive or return to work for around four to eight weeks.
Laparoscopic cholecystectomy
Laparoscopic gallbladder removal is surgery to remove the gallbladder using a medical device called a laparoscope (a long, thin telescope with a light and camera at the end). This technique is the most common for simple cholecystectomy. When you’re having a laparoscopic cholecystectomy, your doctor made 1 to 3 small incisions in your belly and used a special instrument called a laparoscope to take out your gallbladder. During keyhole gallbladder removal surgery a small incision (about 2-3cm) is made by your belly button and two or three smaller incisions (about 1cm or less) or made on the right side of your tummy. Ports (hollow tubes) are inserted into the openings. Surgical tools and a lighted camera are placed into the ports. The abdomen is inflated with carbon dioxide gas to make it easier to see the internal organs. The gallbladder is removed, the gas is released from your tummy and the port openings are closed with sutures, surgical clips, or glue. Your surgeon may start with a laparoscopic technique and need to change (convert) to an open laparotomy technique. The procedure takes about 1 to 2 hours. You can usually go home later the same day.
Laparoscopic gallbladder removal recovery time
Recovering from laparoscopic cholecystectomy will take about 1 to 3 weeks for most people. You may have some of these symptoms as you recover:
- Pain in your belly. You may also feel pain in one or both shoulders. This pain comes from the gas still left in your belly after the surgery. The pain should ease over several days to a week.
- A sore throat from the breathing tube. Sucking on ice chips or gargling may be soothing.
- Nausea, and maybe throwing up. Your surgeon can provide you with nausea medicine if needed.
- Loose stools after eating. This may last 4 to 8 weeks. However, in some cases it can last longer.
- Bruising around your wounds. This will go away on its own.
- Skin redness around your wounds. This is normal.
Preventing pneumonia and blood clots
Movement and deep breathing after your operation can help prevent postoperative complications such as blood clots, fluid in your lungs, and pneumonia. Every hour, take 5 to 10 deep breaths and hold each breath for 3 to 5 seconds.
When you have an operation, you are at risk of getting blood clots because of not moving during anesthesia. The longer and more complicated your surgery, the greater the risk. This risk is decreased by getting up and walking 5 to 6 times per day, wearing special support stockings or compression boots on your legs, and, for high-risk patients, taking a medication that thins your blood.
Activity
Start walking after surgery. Begin your everyday activities as soon as you feel up to it. Move around the house and shower, and use the stairs during your first week home. If it hurts when you do something, stop doing that activity.
You may be able to drive after 2 or 3 days if you are not taking strong pain drugs (narcotics). You may lift 15 pounds (7 kilograms) or less. DO NOT do any heavy lifting or straining for the first 1 to 2 weeks.
You may be able to go back to a desk job within a week. Talk to your health care provider if your work is physical.
- Slowly increase your activity. Be sure to get up and walk every hour or so to prevent blood clot formation.
- Patients usually take 1 to 3 weeks to return comfortably to normal activity 7.
- You may go home the same day after a laparoscopic repair. If you have other health conditions or complications such as nausea, vomiting, bleeding, or difficulty passing urine, you may stay longer.
- Persons sexually active before the operation reported being able to return to sexual activity in 14 days (average).
Work and return to school
You may usually return to work 1 week after laparoscopic or open repair, as long as you don’t do any heavy lifting. Discuss the timing with your surgeon.
Do not lift items heavier than 10 pounds or participate in strenuous activity for at least 4 to 6 weeks.
Wound Care
If sutures, staples, or glue were used to close your skin, you may take off the wound dressings and take a shower the day after surgery.
If tape strips (Steri-strips) were used to close your skin, cover the wounds with plastic wrap before showering for the first week after surgery. DO NOT try to wash the Steri-strips off. Let them fall off on their own.
DO NOT soak in a bathtub or hot tub, or go swimming, until your doctor tells you it is OK.
In many cases, dissolvable stitches will be used to close your wounds. These should start to disappear by themselves within a week or two.
If non-dissolvable stitches were used, you’ll usually need to have them removed by a nurse at your doctor surgery after 7-10 days. You’ll be given an appointment for this before you leave hospital.
You’ll be told about how to look after your wound and stitches, including how long any dressings need to stay on, when they should be replaced and when you can start having showers or baths.
There will be scars where the cuts were made in your tummy. These will probably be red and obvious at first, but should fade over time.
Gallbladder removal diet
Eat a normal diet. You may want to avoid greasy or spicy foods for a while.
- When you wake up from the anesthesia, you will be able to drink small amounts of liquid. If you do not feel sick, you can begin eating regular foods.
- Continue to drink about 8 to 10 glasses of water per day.
- Eat a high-fiber diet so you don’t strain while having a bowel movement.
High-Fiber Foods
Foods high in fiber include beans, bran cereals and whole-grain breads, peas, dried fruit (figs, apricots, and dates), raspberries, blackberries, strawberries, sweet corn, broccoli, baked potatoes with skin, plums, pears, apples, greens, and nuts.
Bowel Movements
Anesthesia, decreased activity, and pain medication (narcotics) can contribute to constipation. Avoid straining with bowel movements by increasing the fiber in your diet with high-fiber foods or over-the-counter medicines (like Metamucil® and FiberCon®). Be sure you are drinking 8 to 10 glasses of fluid each day. Your surgeon may prescribe a stool softener if necessary.
When to call your doctor
Call your healthcare provider if:
- You have a fever above 101°F (38.3°C).
- Your surgical wound is bleeding, red, or warm to the touch.
- Your surgical wound has thick, yellow or green, or milky drainage or bad-smelling drainage from your wound site
- You have pain that is not helped with your pain medicines.
- It is hard to breathe.
- You have a cough that does not go away.
- You cannot drink or eat.
- Your skin or the white part of your eyes turns yellow.
- Your stools are a gray color.
- Continuous vomiting
- Strong or continuous abdominal pain or swelling of your abdomen
- No bowel movement 2 to 3 days after the operation
Open cholecystectomy
Open gallbladder removal is surgery to remove the gallbladder through a large cut in your abdomen. The surgeon made a 5 to 7 inch (13 to 20 centimeters) incision (cut) in your belly. The surgeon then removed your gallbladder by reaching in through the incision, separating it from its attachments, and gently lifting it out.
An open procedure may be recommended if you can’t have keyhole surgery – for example, because you have a lot of scar tissue from previous surgery on your tummy.
It’s also sometimes necessary to turn a keyhole procedure into an open one during the operation if your surgeon is unable to see your gallbladder clearly or remove it safely.
Your surgeon can explain why they feel an open procedure is best for you and if you’re due to have keyhole surgery, the risk of it becoming an open procedure should be discussed beforehand.
During open gallbladder removal surgery:
- a larger incision (about 10-20 cm) is made in your tummy, underneath your ribs
- surgical instruments are used to remove your gallbladder
- the incision is closed with stitches and is covered with a dressing
You’ll usually need to stay in hospital for a few days afterwards. Recovery typically takes six to eight weeks.
Open gallbladder removal recovery time
Recovering from open gallbladder removal surgery takes 4 to 8 weeks. You may have some of these symptoms as you recover:
- Pain in your belly. You may also have pain in one or both shoulders for several days after surgery. This comes from the gas still in your belly after your surgery.
- Incision pain for 1 to 2 weeks. This pain should get better each day.
- Sore throat from the breathing tube. Sucking on ice chips or gargling may be soothing.
- Nausea, and maybe throwing up (vomiting). Your surgeon can provide you with nausea medicine, if needed.
- Loose stools after eating. This may last 4 to 8 weeks. Rarely, the diarrhea can continue. Your health care provider can discuss treatment options with you.
- Bruising around your wound. This will go away on its own.
- Skin redness around your wound. This is normal.
- A small amount of watery or dark bloody fluid from the incision. This is normal for several days after surgery.
The surgeon may have left 1 or 2 drainage tubes in your belly:
- One will help remove any fluid or blood that is left in your belly.
- The second tube will drain bile while you recover. This tube will be removed by your surgeon in 2 to 4 weeks. Before the tube is removed, you will have a special x-ray called a cholangiogram.
- You will receive instructions for caring for these drains before leaving the hospital.
Preventing pneumonia and blood clots
Movement and deep breathing after your operation can help prevent postoperative complications such as blood clots, fluid in your lungs, and pneumonia. Every hour, take 5 to 10 deep breaths and hold each breath for 3 to 5 seconds.
When you have an operation, you are at risk of getting blood clots because of not moving during anesthesia. The longer and more complicated your surgery, the greater the risk. This risk is decreased by getting up and walking 5 to 6 times per day, wearing special support stockings or compression boots on your legs, and, for high-risk patients, taking a medication that thins your blood.
Activity
Plan to have someone drive you home from the hospital. DO NOT drive yourself home.
You should be able to do most of your regular activities in 4 to 8 weeks. Before that:
- DO NOT lift anything heavier than 10 to 15 pounds (5 to 7 kilograms) until you see your provider.
- Avoid all strenuous activity. This includes heavy exercising, weightlifting, and other activities that make you breathe hard or strain.
- Taking short walks and using stairs are OK.
- Light housework is OK.
- DO NOT push yourself too hard. Slowly increase how much you exercise.
Managing pain:
- Your provider will prescribe pain medicines to use at home.
- If you are taking pain pills 3 or 4 times a day, try taking them at the same times each day for 3 to 4 days. They may be more effective this way.
- Try getting up and moving around if you are having some pain in your belly. This may ease your pain.
Press a pillow over your incision when you cough or sneeze to ease discomfort and protect your incision.
Make sure your home is safe as you are recovering.
Wound Care
Change the dressing over your surgical wound once a day, or sooner if it becomes dirty. Your provider will tell you when you no longer need to keep your wound covered. Keep the wound area clean by washing it with mild soap and water.
You may remove the wound dressings and take showers if sutures, staples, or glue were used to close your skin.
- Always wash your hands before and after touching near your incision site.
- Do not soak in a bathtub until your stitches, Steri-Strips®, or staples are removed. You may take a shower after the second postoperative day unless you are told not to.
- Follow your surgeon’s instructions on when to change your bandages.
- A small amount of drainage from the incision is normal. If the dressing is soaked with blood, call your surgeon.
- If you have Steri-Strips in place, they will fall off in 7 to 10 days.
- If you have a glue-like covering over the incision, just let the glue to flake off on its own.
- Avoid wearing tight or rough clothing. It may rub your incisions and make it harder for them to heal.
- Your scars will heal in about 4 to 6 weeks and will become softer and continue to fade over the next year.
If tape strips (Steri-strips) were used to close your incision:
- Cover the incision with plastic wrap before showering for the first week.
- DO NOT try to wash off the Steri-strips or glue. Let them fall off on their own.
DO NOT soak in a bathtub, hot tub, or go swimming until your provider tells you it is OK.
Self-care
Eat a normal diet, but you may want to avoid greasy or spicy foods for a while.
If you have hard stools:
- Try to walk and be more active, but do not overdo it.
- If you can, take less of some of the pain medicines your provider gave you. Some can cause constipation.
- Try a stool softener. You can get these at any pharmacy without a prescription.
- Ask your provider whether you can take milk of magnesia or magnesium citrate. DO NOT take any laxatives without first asking your provider.
- Ask your provider about foods that are high in fiber, or try using psyllium (Metamucil).
High-Fiber Foods
Foods high in fiber include beans, bran cereals and whole-grain breads, peas, dried fruit (figs, apricots, and dates), raspberries, blackberries, strawberries, sweet corn, broccoli, baked potatoes with skin, plums, pears, apples, greens, and nuts.
Follow-up:
You will see your provider for a follow-up appointment in the weeks after your gallbladder removal surgery.
When to call the doctor
Call your provider if:
- You have a fever above 101°F (38.3°C).
- Your surgical wound is bleeding, red, or warm to the touch.
- Your surgical wound has thick, yellow or green, or milky drainage or bad-smelling drainage from your wound site
- You have pain that is not helped with your pain medicines.
- It is hard to breathe.
- You have a cough that does not go away.
- You cannot drink or eat.
- Your skin or the white part of your eyes turns yellow.
- Your stools are a gray color.
- Continuous vomiting
- Strong or continuous abdominal pain or swelling of your abdomen
- No bowel movement 2 to 3 days after the operation.
- Steiner CA, Bass EB, Talamini MA, Pitt HA, Steinberg EP. Surgical rates and operative mortality for open and laparoscopic cholecystectomy in Maryland. New England Journal of Medicine 1994;330(6):403-8.[↩]
- NIH Consensus Development Panel on Gallstones and Laparoscopic Cholecystectomy. Journal of the American Medical Association 1993;269(8):1018-24.[↩][↩]
- Keus F, de Jong J, Gooszen HG, Laarhoven CJHM. Small-incision versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No.: CD004788. DOI: 10.1002/14651858.CD004788.pub2. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD004788.pub2/full[↩]
- Mühe E. The first cholecystectomy through the laparoscope [Die erste Cholecystektomie durch das Laparoskop]. Langenbecks Archiv für Chirurgie 1986;369:804.[↩]
- Jackson PG, Evans S. Biliary System. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 19th ed. Philadelphia, PA: Saunders Elsevier; 2012:chap 55.[↩][↩][↩]
- Gurusamy KS, Davidson BR. Surgical treatment of gallstones. Gastroenterol Clin N Am. 2010 Jun;39(2):229-44, viii.[↩]
- Nawaz H, Papachristou GI. Endoscopic treatment of post- cholecystectomy bile leaks: updates and recent advances. Ann Gastroenterol. 2011;24(3):161-163[↩]





{kind=link}