
What is cod liver oil
Cod liver oil can be obtained from eating fresh cod liver or by taking cod liver oil supplements. Cod liver oil is commonly extracted from Atlantic cod, Gadus morhua. Cod liver oil contains saturated, monounsaturated and various polyunsaturated fatty acids (PUFAs), including both eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) Omega-3 fatty acids 1. Antibacterial, antiviral and antifungal effects have also been associated with polyunsaturated fatty acids (PUFAs) 2. It has been reported that the unsaturated fatty acids’ (FAs) potency increases with the degree of unsaturation, while esterified fatty acids are less effective than free fatty acids 3. Similarly, for cod liver oil, it has been shown that the extract of free fatty acids from cod liver oil is more potent than cod liver oil containing the same fatty acids in the form of triglycerides 4. Besides the strong antibacterial properties, free fatty acids also possess antiviral properties and the fatty acids extract from cod liver oil has been shown to cause a significant reduction of herpes simplex virus type 1 HSV-1 activity. 1% fatty acids extract caused a 50,000 fold or greater (≥4.7 log10) reduction of viral infectivity in 10 min 5. In addition, PUFAs have been used as penetration enhancers in transdermal and buccal drug formulations 6. To date, the mechanisms by which fatty acids act as antibacterial agents have not been resolved, and this continues to be a subject of some research effort. Although the exact mode of the bactericidal action of fatty acids still remains unclear, the cellular membrane is thought to be the primary target 7. Some people put cod liver oil on their skin to speed healing of wounds, burns, and rashes.
Special interest in cod liver oil supplement use is due to several reasons. Firstly, for its nutrients, cod liver oil contains Omega-3 polyunsaturated fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), which in observational studies have been negatively associated with several cancer sites 8; on the other hand, meta-analyses of trial and/or cohort data have shown no effect of these omega-3 fatty acids in supplement form on cardiovascular disease 9. Cod liver oil is also used as a source of vitamin A and vitamin D and vitamin E of which vitamin D prevents osteomalacia, rickets and has been associated with osteoporosis 10; while chronic intake above 1500 µg/day of vitamin A might increase the risk of fractures 11. Cod liver oil has also been used to treat high cholesterol and high triglyceride levels, kidney disease in people with diabetes, high blood pressure, heart disease, osteoarthritis, rheumatoid arthritis, depression, an autoimmune disease called systemic lupus erythematosus (SLE), glaucoma, and middle ear infections (otitis media). It is also used to prevent respiratory infections, and an age-related eye condition called macular degeneration.
Table 1. Typical fatty acid composition of fatty acid extract from cod liver oil
| Fatty Acid | Amount (%) | |
|---|---|---|
| Name | Shorthand | |
| Saturated fatty acids | ||
| Myristic acid | 14:0 | 3.6 |
| Palmitic acid | 16:0 | 10.4 |
| Stearic acid | 18:0 | 2.6 |
| Monounsaturated fatty acids | ||
| Palmitoleic acid | 16:1 n-7 | 6.5 |
| cis-Vaccenic acid | 18:1 n-7 | 4.4 |
| Oleic acid | 18:1 n-9 | 16.2 |
| Gondoic acid | 20:1 n-9 | 9.4 |
| Gadoleic acid | 20:1 n-11 | 1.6 |
| Erucic acid | 22:1 n-9 | 0.6 |
| Cetoleic acid | 22:1 n-11 | 7.8 |
| Polyunsaturated fatty acids | ||
| Linoleic acid (LA) | 18:2 n-6 | 1.5 |
| Moroctic acid | 18:4 n-3 | 2.4 |
| Eicosapentaenoic acid (EPA) | 20:5 n-3 | 9.3 |
| Docosahexaenoic acid (DHA) | 22:6 n-3 | 11.9 |
Cod liver oil vs Fish oil
Cod liver oil is a type of fish oil is. Fish oil a type of polyunsaturated fatty acids that is derived from fish and contain a rich source of Omega-3 essential fatty acids that are important for a number of functions in your body. Fish oil is commonly found in fatty fish such as salmon, tuna, and trout—and shellfish—such as crab, mussels, and oysters. Omega-3 fatty acids are called essential fatty acids because your body cannot make them and you need it them in your diet.
Although there are other sources you can get the Omega-3 essential fatty acids from, for example Alpha-linolenic acid (ALA) from plant oils such as flaxseed, soybean, and canola oils; only fish oil is rich in Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) Omega-3 essential fatty acids.
Omega-3 Eicosapentaenoic acid (EPA) and Omega-3 Docosahexaenoic acid (DHA) are found in seafood, including fatty fish (e.g., salmon, tuna, and trout) and shellfish (e.g., crab, mussels, and oysters).
Note the differences between the Omega-3 fatty acids found in flaxseed, soybean, vegetable oils (alpha-linolenic acid (ALA)) from those in fish and seafoods (Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA)).
Our bodies can convert plant omega-3 fatty acids, Alpha-linolenic acid (ALA), to fish omega-3 fatty acids, Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA), but only a small fraction about 5% of Alpha-linolenic acid (ALA) to eicosapentaenoic acid (EPA), the level of eicosapentaenoic acid (EPA) in blood does not rise when we eat α-linolenic acid 13.
What are Omega-3 Fatty Acids
Omega-3 fatty acids are polyunsaturated fatty acids found in certain foods. The term “omega-3” refers to their chemical structure. Omega-3 fatty acids cannot be made in the body and must be obtained from food; thus, they are essential fatty acids. There are many forms of omega-3 fatty acids, each with a different length and chemical structure.
Where are omega-3 fatty acids found ?
- The shortest omega-3 fatty acid, α-linolenic acid or Alpha-linolenic acid (ALA), is found in plants and plant oils, including leafy vegetables, walnuts, mustard seed oil, soy bean oil, canola oil and flaxseed oil (which is made up of 50% Alpha-linolenic acid (ALA)).
- The longer omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), are found in algae, which are eaten by fish and baleen whales. We obtain these fatty acids by eating fish (e.g., salmon). Eicosapentaenoic acid and docosahexaenoic acid are often referred to as being from marine or fish sources 13.
Plant omega-3 fatty acids, a different type of omega-3, called Alpha-linolenic acid (ALA), are not the same as fish omega-3 fatty acids. Although their chemical structures are similar, they have important differences, which affect their metabolism in the body.
Plant omega-3 Alpha-linolenic acid (ALA), can be found in some vegetable oils—such as canola and soy oils. Omega-3s are also available as dietary supplements. There is moderate evidence emerging about the health benefits of eating seafood like fish and shellfish. However, the health benefits of taking omega-3 as dietary supplements are unclear.
The main sources of Omega-3 Alpha-linolenic acid (ALA) in the U.S. diet are vegetable oils, particularly canola and soybean oils; flaxseed oil is richer in alpha-linolenic acid (ALA) than soybean and canola oils but is not commonly consumed. The typical North American diet provides approximately 1.4 g of ALA per day, and 0.1 g to 0.2 g of EPA and DHA 14. Alpha-linolenic acid (ALA) can be converted, usually in small amounts, into (Eicosapentaenoic acid) EPA and (Docosahexaenoic acid) DHA in the body.
For those who do not consume fish, the omega-3 fatty acid known as alpha-linolenic acid (ALA) can be a dietary source of some metabolically derived Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA). The desaturation plus elongation reactions in the liver and elsewhere in the body that provide for the conversion of dietary ALA to EPA and DHA are depicted in Figure 4. The conversion of ALA to EPA and DHA occurs to a low extent (about 10%–15% efficiency) in the adult human body 15. Nonetheless, there is evidence that the benefits of the Mediterranean-type diet after myocardial infarction may be partly caused by the higher intake of ALA (commonly found in nonhydrogenated canola oil, ground flaxseed and other selected ALA-enriched foods) 16. A prospective cohort study (Nurses Health Study) revealed an inverse relation between ALA intakes and the risk of fatal ischemic heart disease among women 17. However, the Zutphen Elderly Study did not observe a beneficial effect of dietary ALA on the 10-year risk of coronary artery disease 18. The metabolic conversion of ALA to the longer chain omega-3 fatty acids (EPA and DHA) is thought to mediate any possible cardioprotective effects of dietary ALA. In contrast to the well-recognized serum triglyceride-lowering effect of EPA and DHA, most human intervention studies with ALA (e.g., using flaxseed oil) have not exhibited any lipid-lowering effects. Whereas ALA (from flaxseed oil) at a relatively high dose has been found to improve arterial compliance 19, considerably lower supplementation levels of EPA and DHA improved arterial and endothelial functioning in subjects with hypercholesterolemia 20 and subjects with type 2 diabetes mellitus 21.
When the Food and Nutrition Board of the Institute of Medicine last reviewed omega-3s, insufficient data were available to establish an Estimated Average Requirement (EAR), so the Food and Nutrition Board of the Institute of Medicine established Adequate Intakes (AIs) for all ages based on omega-3 intakes in healthy populations 22. Adequate Intake (AI) is established when evidence is insufficient to develop an Recommended Dietary Allowance (RDA) which is the average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals; intake at this level is assumed to ensure nutritional adequacy.
Table 2 lists the current Adequate Intake (AIs) for omega-3s in grams per day. Human milk contains omega-3s as Alpha-linolenic acid (ALA), Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA), so the Institute of Medicine established an AI for infants from birth to 12 months that is equivalent to the mean intake of omega-3s in healthy, breastfed infants.
For infants, the AIs apply to total omega-3s. For ages 1 and older, the AIs apply only to alpha-linolenic acid (ALA) because ALA is the only omega-3 that is essential. The Institute of Medicine did not establish specific intake recommendations for EPA, DHA or other long chain omega-3s.
Table 2: Adequate Intakes (AIs) for Omega-3s
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months* | 0.5 g | 0.5 g | ||
| 7–12 months* | 0.5 g | 0.5 g | ||
| 1–3 years** | 0.7 g | 0.7 g | ||
| 4–8 years** | 0.9 g | 0.9 g | ||
| 9–13 years** | 1.2 g | 1.0 g | ||
| 14–18 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
| 19-50 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
| 51+ years** | 1.6 g | 1.1 g |
*As total omega-3s
**As ALA
The fish-based and fish-oil–based omega-3 polyunsaturated fatty acids (also referred to as n-3 PUFA) consist of EPA (20 carbon atoms, 5 double bonds) and DHA (22 carbon atoms, 6 double bonds). The general structures for EPA and DHA are shown in Figure 1. Commonly available dietary sources of Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) are listed in Table 2. Whereas plant foods and vegetable oils lack EPA and DHA, some do contain varying amounts of the n-3 PUFA alpha-linolenic acid (ALA), which has 18 carbon atoms and 3 double bonds (Fig. 3). Many vegetable oils are greatly enriched in omega-6 fatty acids (mainly as linoleic acid in corn, safflower, sunflower and soybean oils), but canola oil (nonhydrogenated), ground flaxseed and walnuts are rich sources of ALA.
The typical North American diet provides about 1–3 g of omega-3 PUFA alpha-linolenic acid (ALA) per day but only 0.10–0.15 g of EPA (Eicosapentaenoic acid) plus DHA (Docosahexaenoic acid) per day 23, 24. The very high intake of n-6 PUFA, mostly as linoleic acid (LA) (Fig. 3) in our diet (12–15 g/day) from common vegetable oils (corn, safflower, soybean) and other sources, yields an overall n-6:n-3 dietary ratio (total omega-6 fatty acids in the diet: total omega-3 fatty acids in the diet) of about 8:1. Health Canada has recommended that this ratio be as low as 4:19 to reduce the competitive influence of high LA intakes on ALA metabolism to its longer chain products (such as EPA and DHA). Although high intakes of LA can provide some modest blood cholesterol lowering, experimental studies in animals have raised concerns regarding the enhancing effect of these high intakes on certain cancers 25. This association has not been established in human studies 26.
Figure 1. Omega-3 fatty acids and Omega-6 fatty acids structure
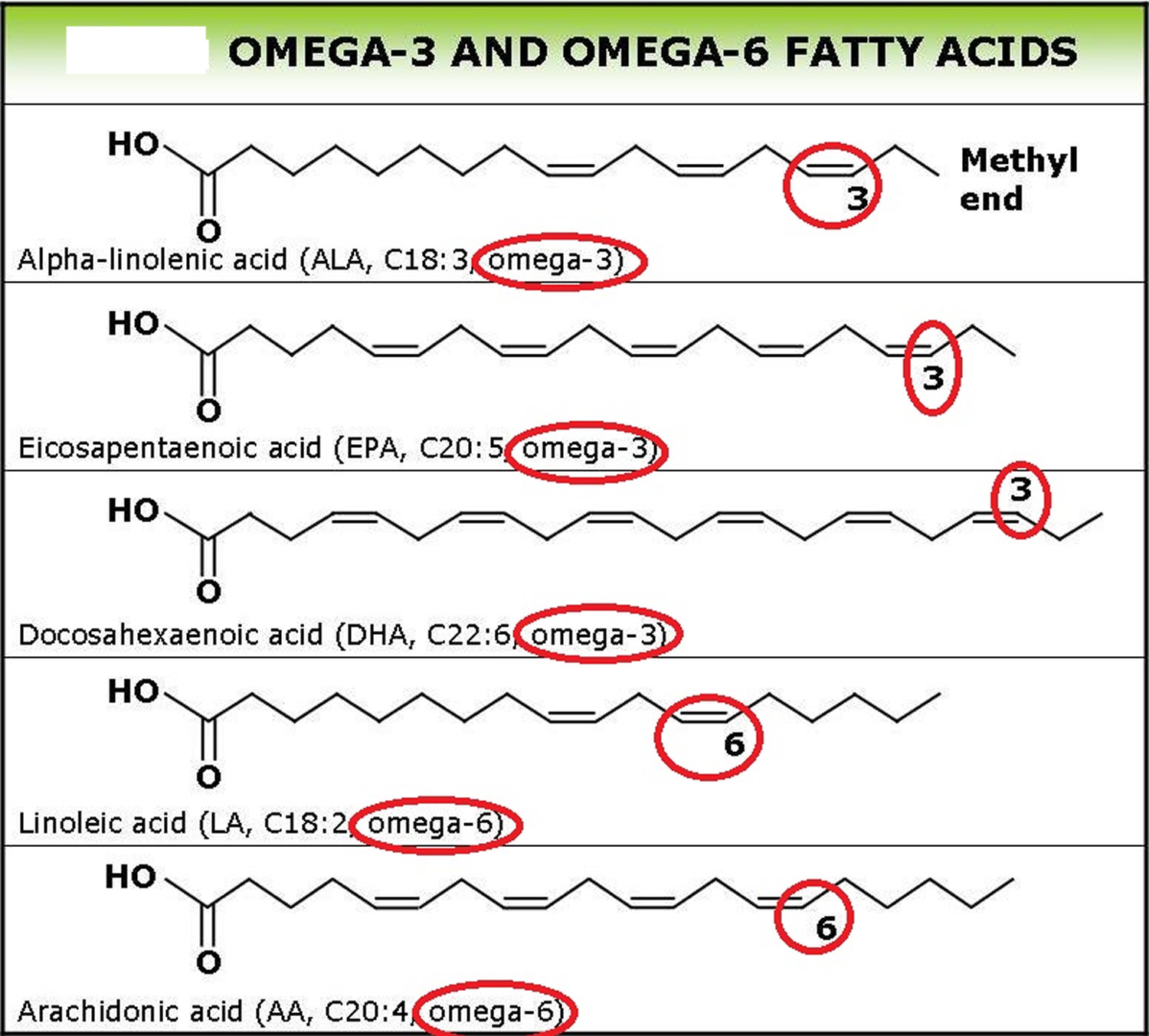
Figure 2. Conversion of dietary ALA to EPA and DHA via Desaturation, elongation and retroconversion of polyunsaturated fatty acids.
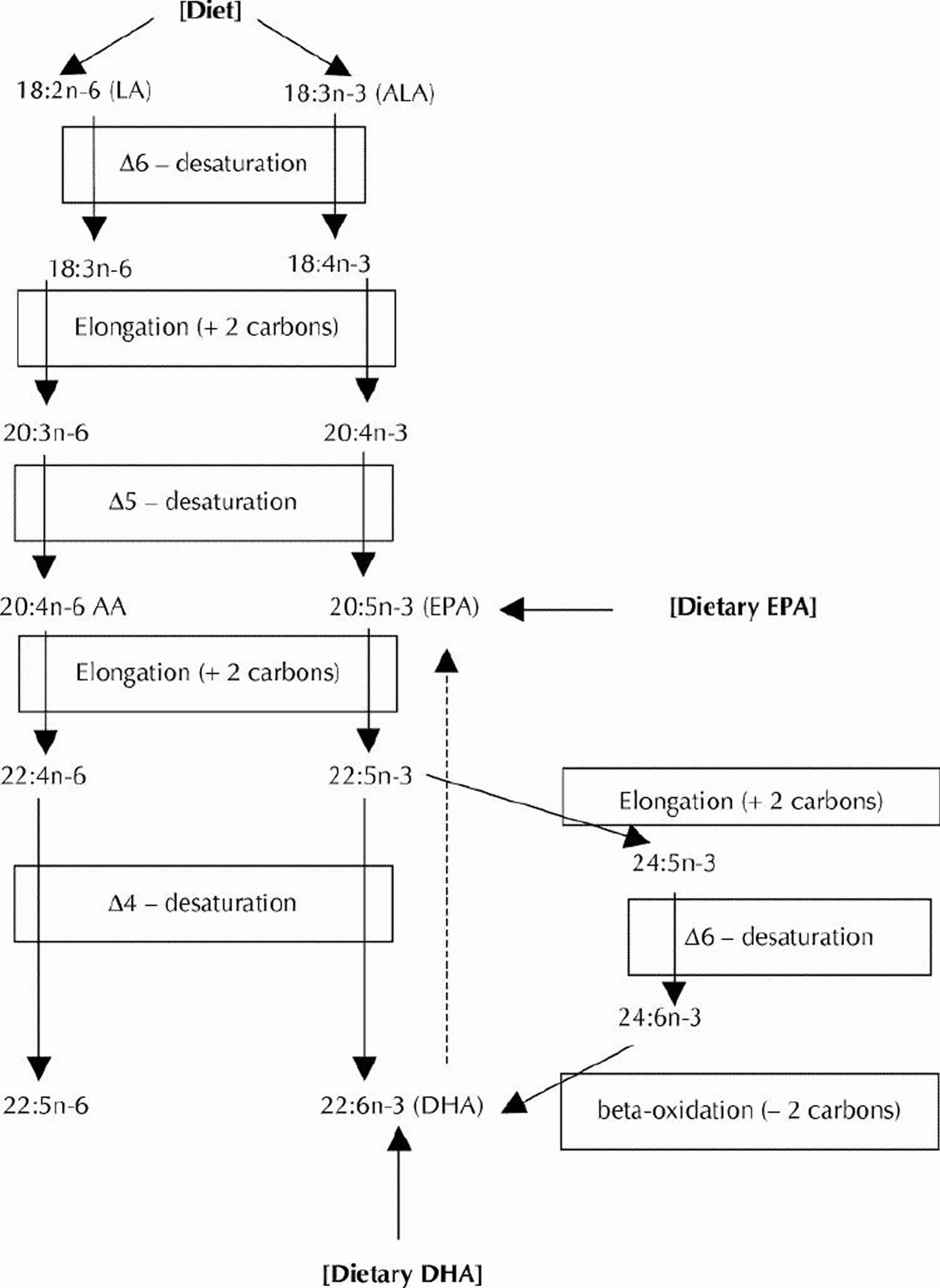
Table 3. Omega-3 Fatty Acid Foods EPA (Eicosapentaenoic acid) and DHA (Docosahexaenoic acid) – Fish and Seafood Sources
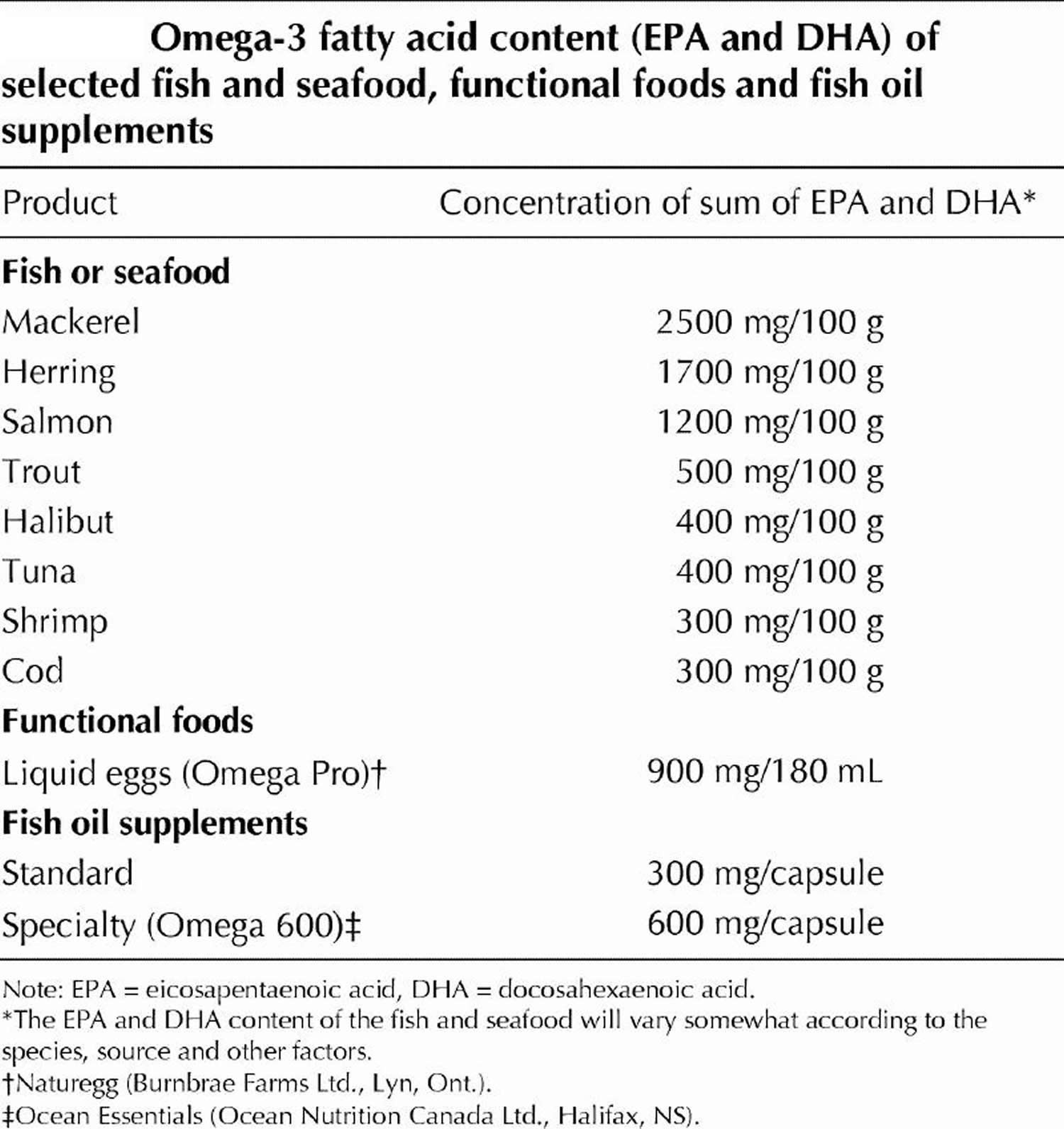
Table 3. EPA (Eicosapentaenoic acid) and DHA (Docosahexaenoic acid) Content of Fish Species
| Fish Species and Description | DHA per 100 g | EPA per 100 g | DHA+EPA per 100 g | DHA+EPA per 85 g (3 oz.) |
|---|---|---|---|---|
| Crustaceans, crab, Alaska king, cooked, moist heat | 0.118 | 0.295 | 0.413 | 0.351 |
| Crustaceans, crab, blue, cooked, moist heat | 0.231 | 0.243 | 0.474 | 0.403 |
| Crustaceans, crab, Dungeness, cooked, moist heat | 0.113 | 0.281 | 0.394 | 0.335 |
| Crustaceans, crab, queen, cooked, moist heat | 0.145 | 0.332 | 0.477 | 0.405 |
| Crustaceans, crayfish, mixed species, farmed, cooked, moist heat | 0.038 | 0.124 | 0.162 | 0.138 |
| Crustaceans, crayfish, mixed species, wild, cooked, moist heat | 0.047 | 0.119 | 0.166 | 0.141 |
| Crustaceans, lobster, northern, cooked, moist heat | 0.031 | 0.053 | 0.084 | 0.071 |
| Crustaceans, shrimp, mixed species, cooked, moist heat | 0.144 | 0.171 | 0.315 | 0.268 |
| Crustaceans, spiny lobster, mixed species, cooked, moist heat | 0.139 | 0.341 | 0.480 | 0.408 |
| Fish, anchovy, European, raw | 0.911 | 0.538 | 1.449 | 1.232 |
| Fish, anchovy, European, canned in oil, drained solids | 1.292 | 0.763 | 2.055 | 1.747 |
| Fish, bass, freshwater, mixed species, cooked, dry heat | 0.458 | 0.305 | 0.763 | 0.649 |
| Fish, bass, striped, cooked, dry heat | 0.750 | 0.217 | 0.967 | 0.822 |
| Fish, bluefish, cooked, dry heat | 0.665 | 0.323 | 0.988 | 0.840 |
| Fish, turbot, cooked, dry heat | 0.123 | 0.09 | 0.213 | 0.181 |
| Fish, carp, cooked, dry heat | 0.146 | 0.305 | 0.451 | 0.383 |
| Fish, catfish, channel, farmed, cooked, dry heat | 0.128 | 0.049 | 0.177 | 0.150 |
| Fish, catfish, channel, wild, cooked, dry heat | 0.137 | 0.100 | 0.237 | 0.201 |
| Fish, caviar, black and red, granular | 3.800 | 2.741 | 6.541 | 5.560 |
| Fish, cod, Atlantic, cooked, dry heat | 0.154 | 0.004 | 0.158 | 0.134 |
| Fish, cod, Pacific, cooked, dry heat | 0.173 | 0.103 | 0.276 | 0.235 |
| Fish, croaker, Atlantic, raw | 0.097 | 0.123 | 0.22 | 0.187 |
| Fish, dolphin fish, cooked, dry heat | 0.113 | 0.026 | 0.139 | 0.118 |
| Fish, drum, freshwater, cooked, dry heat | 0.368 | 0.295 | 0.663 | 0.564 |
| Fish, eel, mixed species, cooked, dry heat | 0.081 | 0.108 | 0.189 | 0.161 |
| Fish, fish portions and sticks, frozen, preheated | 0.128 | 0.086 | 0.214 | 0.182 |
| Fish, flatfish (flounder and sole species), cooked, dry heat | 0.258 | 0.243 | 0.501 | 0.426 |
| Fish, grouper, mixed species, cooked, dry heat | 0.213 | 0.035 | 0.248 | 0.211 |
| Fish, haddock, cooked, dry heat | 0.162 | 0.076 | 0.238 | 0.202 |
| Fish, halibut, Atlantic and Pacific, cooked, dry heat | 0.374 | 0.091 | 0.465 | 0.395 |
| Fish, halibut, Greenland, cooked, dry heat | 0.504 | 0.674 | 1.178 | 1.001 |
| Fish, herring, Atlantic, cooked, dry heat | 1.105 | 0.909 | 2.014 | 1.712 |
| Fish, herring, Atlantic, kippered | 1.179 | 0.97 | 2.149 | 1.827 |
| Fish, herring, Pacific, cooked, dry heat | 0.883 | 1.242 | 2.125 | 1.806 |
| Fish, lingcod, cooked, dry heat | 0.130 | 0.133 | 0.263 | 0.224 |
| Fish, mackerel, Atlantic, cooked, dry heat | 0.699 | 0.504 | 1.203 | 1.023 |
| Fish, mackerel, king, cooked, dry heat | 0.227 | 0.174 | 0.401 | 0.341 |
| Fish, mackerel, Pacific and jack, mixed species, cooked, dry heat | 1.195 | 0.653 | 1.848 | 1.571 |
| Fish, mackerel, Spanish, cooked, dry heat | 0.952 | 0.294 | 1.246 | 1.059 |
| Fish, mullet, striped, cooked, dry heat | 0.148 | 0.18 | 0.328 | 0.279 |
| Fish, ocean perch, Atlantic, cooked, dry heat | 0.271 | 0.103 | 0.374 | 0.318 |
| Fish, perch, mixed species, cooked, dry heat | 0.223 | 0.101 | 0.324 | 0.275 |
| Fish, pike, northern, cooked, dry heat | 0.095 | 0.042 | 0.137 | 0.116 |
| Fish, pike, walleye, cooked, dry heat | 0.288 | 0.11 | 0.398 | 0.338 |
| Fish, pollock, Atlantic, cooked, dry heat | 0.451 | 0.091 | 0.542 | 0.461 |
| Fish, pompano, Florida, cooked, dry heat | ?? | ?? | ?? | 0.620 est |
| Fish, rockfish, Pacific, mixed species, cooked, dry heat | 0.262 | 0.181 | 0.443 | 0.377 |
| Fish, roe, mixed species, cooked, dry heat | 1.747 | 1.26 | 3.007 | 2.556 |
| Fish, roe, mixed species, raw | 1.363 | 0.983 | 2.346 | 1.994 |
| Fish, roughy, orange, raw | 0 | 0.001 | 0.001 | 0.001 |
| Fish, sablefish, cooked, dry heat | 0.920 | 0.867 | 1.787 | 1.519 |
| Fish, sablefish, smoked | 0.945 | 0.891 | 1.836 | 1.561 |
| Fish, salmon, Atlantic, farmed, cooked, dry heat | 1.457 | 0.69 | 2.147 | 1.825 |
| Fish, salmon, Atlantic, wild, cooked, dry heat | 1.429 | 0.411 | 1.84 | 1.564 |
| Fish, salmon, Chinook, cooked, dry heat | 0.727 | 1.01 | 1.737 | 1.476 |
| Fish, salmon, chum, cooked, dry heat | 0.505 | 0.299 | 0.804 | 0.683 |
| Fish, salmon, chum, drained solids with bone | 0.702 | 0.473 | 1.175 | 0.999 |
| Fish, salmon, coho, farmed, cooked, dry heat | 0.871 | 0.408 | 1.279 | 1.087 |
| Fish, salmon, coho, wild, cooked, dry heat | 0.658 | 0.401 | 1.059 | 0.900 |
| Fish, salmon, pink, cooked, dry heat | 0.751 | 0.537 | 1.288 | 1.095 |
| Fish, salmon, sockeye, cooked, dry heat | 0.700 | 0.53 | 1.23 | 1.046 |
| Fish, sardine, Atlantic, canned in oil, drained solids with bone | 0.509 | 0.473 | 0.982 | 0.835 |
| Fish, scup, raw (Porgy—assigned to low omega-3 group) | no data | no data | no data | no data |
| Fish, sea bass, mixed species, cooked, dry heat | 0.556 | 0.206 | 0.762 | 0.648 |
| Fish, sea trout, mixed species, cooked, dry heat | 0.265 | 0.211 | 0.476 | 0.405 |
| Fish, shad, American, raw | 1.321 | 1.086 | 2.407 | 2.046 |
| Fish, shark, mixed species, raw | 0.527 | 0.316 | 0.843 | 0.717 |
| Fish, sheepshead, cooked, dry heat | 0.107 | 0.083 | 0.19 | 0.162 |
| Fish, smelt, rainbow, cooked, dry heat | 0.536 | 0.353 | 0.889 | 0.756 |
| Fish, snapper, mixed species, cooked, dry heat | 0.273 | 0.048 | 0.321 | 0.273 |
| Fish, spot, cooked, dry heat | 0.526 | 0.282 | 0.808 | 0.687 |
| Fish, sturgeon, mixed species, cooked, dry heat | 0.119 | 0.249 | 0.368 | 0.313 |
| Fish, sucker, white, cooked, dry heat | 0.371 | 0.244 | 0.615 | 0.523 |
| Fish, sunfish, pumpkin seed, cooked, dry heat | 0.092 | 0.047 | 0.139 | 0.118 |
| Fish, swordfish, cooked, dry heat | 0.681 | 0.138 | 0.819 | 0.696 |
| Fish, tilefish, cooked, dry heat | 0.733 | 0.172 | 0.905 | 0.769 |
| Fish, trout, mixed species, cooked, dry heat | 0.677 | 0.259 | 0.936 | 0.796 |
| Fish, trout, rainbow, farmed, cooked, dry heat | 0.820 | 0.334 | 1.154 | 0.981 |
| Fish, trout, rainbow, wild, cooked, dry heat | 0.520 | 0.468 | 0.988 | 0.840 |
| Fish, tuna, fresh, bluefin, cooked, dry heat | 1.141 | 0.363 | 1.504 | 1.278 |
| Fish, tuna, light, canned in oil, drained solids | 0.101 | 0.027 | 0.128 | 0.109 |
| Fish, tuna, light, canned in water, drained solids | 0.223 | 0.047 | 0.27 | 0.230 |
| Fish, tuna, skipjack, fresh, cooked, dry heat | 0.237 | 0.091 | 0.328 | 0.279 |
| Fish, tuna, white, canned in water, drained solids | 0.629 | 0.233 | 0.862 | 0.733 |
| Fish, tuna, yellowfin, fresh, cooked, dry heat | 0.232 | 0.047 | 0.279 | 0.237 |
| Fish, whitefish, mixed species, cooked, dry heat | 1.206 | 0.406 | 1.612 | 1.370 |
| Fish, whiting, mixed species, cooked, dry heat | 0.235 | 0.283 | 0.518 | 0.440 |
| Fish, wolffish, Atlantic, cooked, dry heat | 0.405 | 0.393 | 0.798 | 0.678 |
| Frog legs, raw | 0.034 | 0.020 | ||
| Mollusks, abalone, mixed species, raw | 0 | 0.049 | 0.049 | 0.042 |
| Mollusks, clam, mixed species, cooked, moist heat | 0.146 | 0.138 | 0.284 | 0.241 |
| Mollusks, conch, baked or broiled | 0.072 | 0.048 | 0.12 | 0.102 |
| Mollusks, cuttlefish, mixed species, cooked, moist heat | 0.132 | 0.078 | 0.21 | 0.179 |
| Mollusks, mussel, blue, cooked, moist heat | 0.506 | 0.276 | 0.782 | 0.665 |
| Mollusks, octopus, common, cooked, moist heat | 0.162 | 0.152 | 0.314 | 0.267 |
| Mollusks, oyster, eastern, farmed, cooked, dry heat | 0.211 | 0.229 | 0.44 | 0.374 |
| Mollusks, oyster, eastern, wild, cooked, dry heat | 0.291 | 0.26 | 0.551 | 0.468 |
| Mollusks, oyster, Pacific, cooked, moist heat | 0.500 | 0.876 | 1.376 | 1.170 |
| Mollusks, scallop, mixed species, cooked, breaded and fried | 0.103 | 0.086 | 0.18 | 0.161 |
| Mollusks, whelk, unspecified, cooked, moist heat | 0.012 | 0.008 | 0.02 | 0.017 |
Both omega-3 fatty acids from fish and plants appear to reduce the risk of some types of heart disease. However, the results of all studies have not been consistent. Some suggest that fish oil may reduce mortality among patients with coronary heart disease, possibly by stabilizing the heart’s rhythm and by reducing blood clotting. We don’t know as much about the effects of plant omega-3 fatty acids, but they appear to have similar actions in reducing coronary heart disease events.
Animal and human studies 29, 30, 31, 32 in addition to epidemiological surveys 33, 34 have also shown that Omega-3 PUFAs effectively enhance and improve learning capability as well as memory and cognitive function. Moreover, intake of EPA and DHA is reported to reduce the risk of developing Alzheimer’s disease 35.
Data supporting the use of EPA+DHA for potential cardiovascular benefit were derived from trials involving increased fish consumption or fish oil supplementation. These findings shaped the recommendations for the American Heart Association’s (AHA) Scientific Statement on Fish Consumption, Fish Oil, Omega-3 Fatty Acids, and Cardiovascular Disease 36. Key messages from this document are summarized in Table 4. Essentially, patients must consume a lower 1 g dose of EPA+DHA for cardioprotection or a higher 2 to 4 g dose for triglyceride reduction. Although the lower dose can often be achieved with dietary fish, the high dose generally requires supplementation.
Table 4. American Heart Association guidelines for omega-3 fatty acid consumption
| Goal | Recommendation |
| Cardioprotection | |
| Patients without a history of CVD | Consume oily fish 2 or more times weekly. |
| Patients with a history of CHD | Consume 1 g daily of EPH +DHA, preferably from oily fish. Fish oil supplements may be used with physician consultation. |
| Triglyceride lowering | Consume 2-4 g daily of EPA +DHA as capsules with physician consultation. |
Abbreviations: CHD = coronary heart disease; CVD = cardiovascular disease; EPA+DHA = eicosapentaenoic acid+docosahexaenoic acid.
The data from the secondary- and primary-prevention studies support the idea that consumption of very-long-chain Omega-3 fatty acids from fish and fish-oil supplements (EPA and DHA) reduces all-cause mortality, cardiac and sudden death and stroke 37. This conclusion agrees with 2 recent meta-analyses by He at al. 38, 39, and with the results of a 1999 ecologic study by Zhang et al 40. The latter showed a significant association between fish consumption and total mortality across 36 countries on the basis of data from the Food and Agriculture Organization and the World Health Organization 40. However, this conclusion is not applicable to the population of patients with an coronary heart disease, in whom 3 recent randomized clinical trials found inconsistent antiarrhythmic effects and no significant overall effect on mortality 37.
The evidence appears strong for a beneficial effect of very-long-chain Omega-3 fatty acids intakes on cardiovascular disease risk in secondary, but not in primary, prevention because data from randomized clinical trials are available for the former, but less evidence exists to support a beneficial effect on heart attack. There is no high-quality evidence to support a beneficial effect of alpha-linolenic acid (ALA) 37.
Are fish oils essential for human health ?
Many people believe this to be true, but officials are still divided. Vegetarians, who do not have an obvious source of fish oil in their diet, seem to have a low incidence of coronary heart disease. For certain functions, α-linolenic acid (ALA) from vegetable sources may be able to substitute for longer fatty acids, either directly or after partial conversion to eicosapentaenoic acid.
What are the benefits of taking fish-oil supplements ?
It is usually stated that omega-3 fatty acids from fish may reduce cardiac deaths, inflammatory disease, including rheumatoid arthritis and ulcerative colitis, and promote brain development and mental function.
Some doctors recommend fish-oil supplements to prevent or treat cardiovascular disease. Although fish oil does not reduce LDL “bad” cholesterol, it may be recommended to lower serum triglycerides. In addition, infant formula is supplemented with docosahexaenoic acid in Europe to enhance development of the central nervous system because the rapidly growing brain requires large amounts of this fatty acid 13. Docosahexaenoic acid used in infant formula comes from algae.
Evidence for a benefit for fish oils in preventing coronary artery restenosis after angioplasty and rhythm abnormalities is less clear.
Cardiovascular disease (CVD) and CVD risk factors
Many studies have assessed the effects of omega-3s—primarily EPA and DHA—on cardiovascular disease and cardiovascular disease risk factors, such as high blood pressure and elevated plasma lipids. This interest was spurred by epidemiological research dating back to the 1970s that found low rates of myocardial infarction (heart attack) and other coronary events among Greenland Inuit and other fish-eating populations, such as the Japanese 41. Results from observational studies have been consistent with these findings, with several systematic reviews and meta-analyses showing that higher consumption of fish and higher dietary or plasma levels of omega-3s are associated with a lower risk of heart failure 42, coronary disease, and fatal coronary heart disease 43.
Recommendations from the Dietary Guidelines for Americans: The 2015–2020 Dietary Guidelines for Americans states that strong evidence from mostly prospective cohort studies but also randomized controlled trials has shown that eating patterns that include seafood are associated with reduced risk of cardiovascular disease 44. In addition, consuming about 8 ounces per week of a variety of seafood that provides about 250 mg per day EPA and DHA is associated with fewer cardiac deaths in both healthy individuals and those with preexisting cardiovascular disease.
Conclusions about omega-3s and cardiovascular disease: Overall, research indicates that consuming fish and other types of seafood as part of a balanced diet promotes heart health. Fish oil and other LC omega-3 supplements improve blood lipids and appear to reduce the risk of cardiac death. However, their effects on other cardiovascular endpoints are unclear and might vary based on dietary omega-3 intakes and the use of cardioprotective medications.
The FDA has approved a qualified health claim for conventional foods and dietary supplements that contain EPA and DHA 45. It states, “Supportive but not conclusive research shows that consumption of EPA and DHA omega-3 fatty acids may reduce the risk of coronary heart disease.” The FDA also specifies that the labels of dietary supplements should not recommend a daily intake of EPA and DHA higher than 2 g 45. For patients who need to lower their triglycerides, the American Heart Association recommends 2–4 g/day of EPA plus DHA under the care of a physician. Several prescription omega-3 preparations are also available to treat hypertriglyceridemia.
Scientists hope to gain additional insight on the effects of omega-3s for the prevention of CVD from the VITamin D and OmegA-3 TriaL (VITAL) trial. This clinical trial will examine the effects of EPA (465 mg/day) and DHA (375 mg/day) supplementation with or without 2,000 IU/day vitamin D for 5 years in 25,875 older adults on the primary prevention of cancer and CVD 46. Results from this clinical trial and others will shed more light on possible associations between omega-3s and cardiovascular events as well as blood pressure and atrial fibrillation.
Infant health and neurodevelopment
Numerous studies have examined the effects of maternal seafood and omega-3 intakes on infant birth weight, length of gestation, visual and cognitive development, and other infant health outcomes. High concentrations of DHA are present in the cellular membranes of the brain and retina 22, and DHA is important for fetal growth and development. The accumulation of DHA in the retina is complete by birth, whereas accumulation in the brain continues throughout the first 2 years after birth.
In 2016, Agency for Healthcare Research and Quality (AHRQ) published a review on the effects of omega-3 fatty acids on child and maternal health 47. This comprehensive report evaluated the findings from 95 randomized controlled trials and 48 prospective longitudinal studies and nested case-control studies. Most studies examined the effects of fish oil supplements or other DHA and EPA combinations in pregnant or breastfeeding women or of infant formula fortified with DHA plus arachidonic acid, an omega-6. The authors concluded that, except for small beneficial effects on infant birth weight and length of gestation, omega-3 supplementation or fortification has no consistent effects on infant health outcomes.
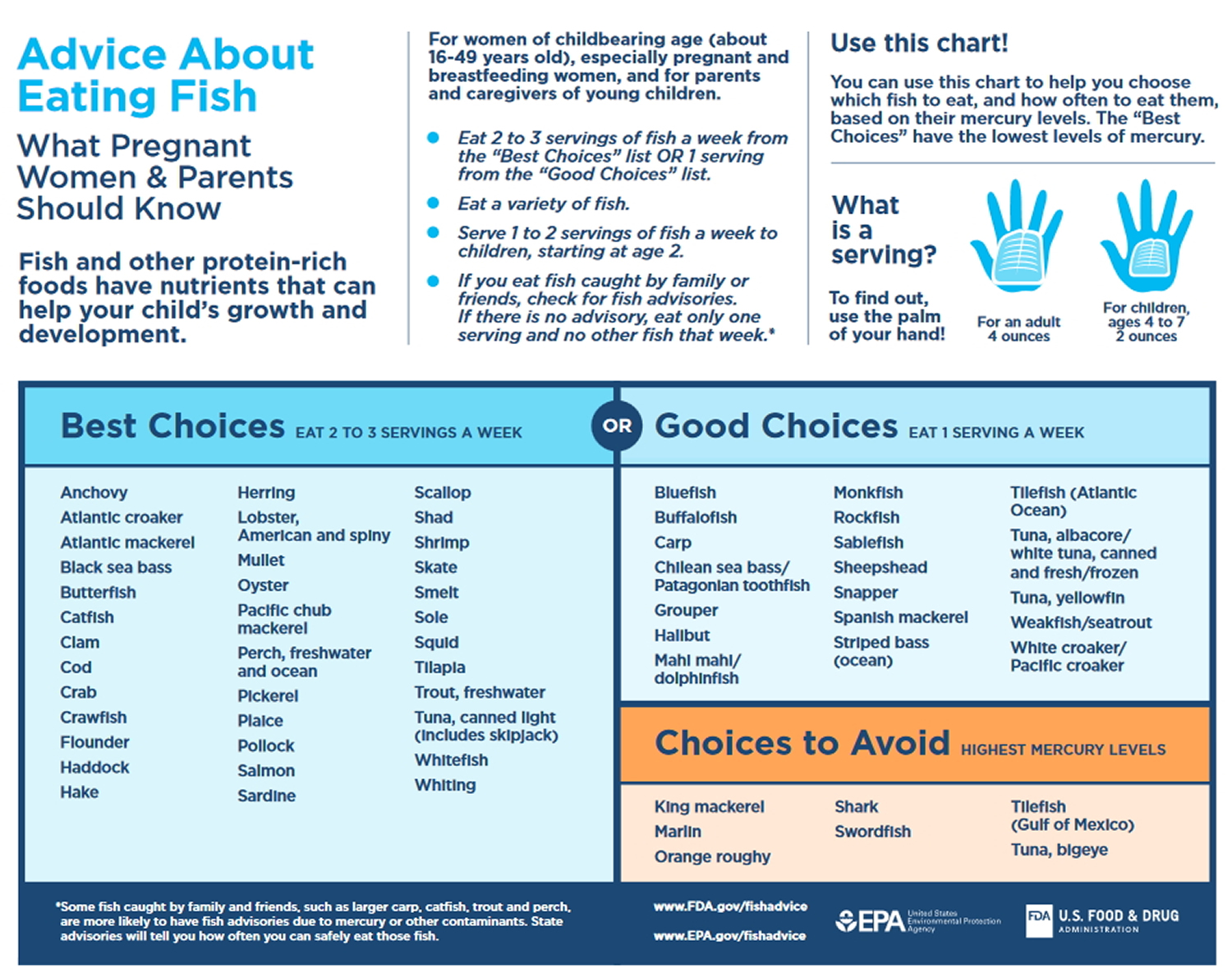
Recommendations from the Dietary Guidelines for Americans: The 2015–2020 Dietary Guidelines for Americans states that women who are pregnant or breastfeeding should consume 8–12 ounces of seafood per week, choosing from varieties that are higher in EPA and DHA and lower in methyl mercury, such as salmon, herring, sardines, and trout. These women should not consume certain types of fish, such as king mackerel, shark, swordfish, and tilefish that are high in methyl mercury, and they should limit the amount of white (albacore) tuna they consume to 6 ounces a week. The American Academy of Pediatrics has similar advice for breastfeeding women, recommending intakes of 200–300 mg DHA per day by consuming one to two servings of fish per week to guarantee a sufficient amount of DHA in breast milk 48.
Most currently available infant formulas in the United States contain DHA and arachidonic acid. However, the authors of a paper published by the American Academy of Family Physicians and of two Cochrane reviews (one on full-term infants and one on preterm infants) have concluded that the evidence is insufficient to recommend the use of infant formulas that are supplemented with these fatty acids 50, 51, 52.
Cancer prevention
Researchers have hypothesized that higher intakes of omega-3s from either foods or supplements might reduce the risk of cancer due to their anti-inflammatory effects and potential to inhibit cell growth factors 53. For example, some studies have shown associations between higher intakes and/or blood levels of omega-3s and a decreased risk of certain cancers, including breast and colorectal cancers 54. Other studies have found no associations between omega-3s and cancer risk, and some have even found associations in the opposite direction, suggesting that omega-3s might increase the risk of certain cancers such as prostate cancer 55, 56. To date, no large-scale clinical trials have examined the effects of omega-3s on the primary prevention of cancer in the general population, although a large clinical trial that addresses this question, the VITAL trial, is currently underway 46. The VITAL trial will examine the effects of EPA (465 mg/day) and DHA (375 mg/day) supplementation (with and without 2,000 IU/day vitamin D) for 5 years in 25,875 older adults on the primary prevention of cancer and cardiovascular disease 46. Results from this clinical trial will shed more light on possible associations between these omega-3s and cancer.
Results from observational studies however, have been inconsistent and vary by cancer site and other factors, including gender and genetic risk. Overall, data from observational studies show no consistent relationship between omega-3s and overall cancer risk. Although there are some suggestions of reduced risk for breast and possibly colorectal cancers with higher long chain omega-3 intakes, randomized clinical trials are needed to confirm these findings.
Breast cancer
Evidence from several observational studies suggests that higher intakes of long chain omega-3s are associated with a lower risk of breast cancer, but clinical trials are needed to confirm this finding. In the prospective Singapore Chinese Health Study of 35,298 women aged 45–74 years, those in the top three quartiles of dietary long chain omega-3 intake had a 26% lower risk of breast cancer after an average of 5.3 years of follow-up than those in the lowest quartile 57. Similarly, among 35,016 female participants aged 50–76 years in the Vitamins And Lifestyle cohort, those who reported current use of fish-oil supplements had a 32% lower risk of breast cancer after a mean of 6 years than those who did not take fish oil 58.
According to a systematic review of three case-control studies and five prospective studies published in 2007–2011, evidence is increasing that higher intakes of dietary and supplemental LC omega-3s are associated with a lower risk of breast cancer 59. Similarly, the authors of a meta-analysis of data from 21 prospective cohort studies concluded that women with the highest dietary intakes and/or tissue levels of long chain omega-3s had a 14% lower risk of breast cancer than those with the lowest intakes and tissue levels 54. These authors also found a dose-response relationship between higher intakes of combined long chain omega-3s and reduced breast cancer risk. Intakes of ALA and of fish, however, had no association with differences in breast cancer risk. This finding, which could be due to varying levels of omega-3s in different fish species, warrants further investigation.
Colorectal cancer
Limited evidence from observational studies suggests that greater consumption of fish and long chain omega-3s is associated with a reduced risk of colorectal cancer 59.
The authors of a meta-analysis of 19 prospective cohort studies found no significant association between fish intake and risk of colorectal cancer overall. However, a stratified analysis showed that for participants with the highest fish consumption (those who ate fish at least seven times more often per month than those with the lowest fish consumption), the risk of colorectal cancer was 22% lower than that for the lowest fish consumers 60. Results from a more recent systematic review and meta-analysis of 22 prospective cohort studies and 19 case-control studies indicate that fish consumption is inversely associated with colorectal cancer risk. In this analysis, 21 of the studies distinguished between colon cancer and rectal cancer. The risk of rectal cancer was 21% lower for participants with the highest fish intakes (as much as one serving/day) compared to those with the lowest fish intakes (as little as none), but fish consumption had no significant association with risk of colon cancer alone 61.
Results from the Vitamins And Lifestyle cohort study suggest that associations between fish or LC omega-3 intakes and colorectal cancer risk might vary by such factors as gender and genetic risk. In this study, researchers evaluated associations between colorectal cancer risk and EPA/DHA intakes from fatty fish (salmon and fresh tuna) and fish oil supplements in 68,109 Washington residents aged 50–76 62. The amount of fatty fish consumed ranged from none to 0.8 servings per week or more. Overall, EPA and DHA intakes (from either diet or supplements) and fatty fish consumption were not associated with colorectal cancer risk, but associations varied by genetic characteristics (certain inherited genetic mutations are associated with an increased risk of colorectal cancer). For individuals in the lowest two tertiles of genetic risk, higher fatty fish consumption and higher total EPA and DHA intakes were inversely associated with colorectal cancer risk. For individuals in the highest tertile of genetic risk, higher total EPA and DHA intakes were positively associated with colorectal cancer risk. Risk also varied by gender. Among men, use of fish oil supplements reduced colorectal cancer risk by an average of 34% or more depending on the frequency and duration of use, but this effect did not occur among women. Additional research is needed to clarify possible associations between fish and omega-3 intakes and colorectal cancer risk.
Prostate cancer
Several prospective and case-control studies have investigated associations between either blood levels or intakes of omega-3s and risk of low-grade or high-grade prostate cancer. Results from these studies have been inconsistent.
A few case-control and case-cohort studies have found positive associations between blood levels of LC omega-3s and prostate cancer risk (particularly high-grade disease that is more advanced and more likely to spread than low-grade cancer), suggesting that omega-3s might increase prostate cancer risk. In a nested case-control analysis of men aged 55–84 years participating in the Prostate Cancer Prevention Trial, serum phospholipid levels of DHA were positively associated with risk of high-grade, but not low-grade, prostate cancer 63. Serum EPA levels, however, were not associated with risk of either grade of the disease.
Similarly, results from a case-cohort study within the Selenium and Vitamin E Cancer Prevention (SELECT) trial showed that men in the highest quartile of plasma phospholipid LC omega-3s had a 44% higher risk of low-grade prostate cancer and a 71% higher risk of high-grade prostate cancer than those in the lowest quartile 56. An analysis of data from the European Prospective Investigation into Cancer and Nutrition cohort also found a higher prostate cancer risk in men with higher plasma levels of LC omega-3s 64. Among whites participating in the Multiethnic Cohort Study, higher levels of omega-3s in erythrocyte membranes and higher ratios of omega-3s to omega-6s were both associated with an increased risk of prostate cancer. However, the results showed no associations, even with advanced or high-grade disease, for other ethnic groups or for the population as a whole 65.
Although the findings from the Prostate Cancer Prevention Trial and the SELECT trial suggest that higher LC omega-3 intakes might increase prostate cancer risk, some scientists have questioned the significance of these findings 66. They have noted, for example, that in the SELECT trial 56, the difference in the omega-3 levels in the men with and without prostate cancer was very small and of questionable physiological significance. Other scientists have pointed out that localized (even high-grade) prostate cancers usually progress slowly and are common on autopsy in men who have died from other causes, suggesting that prostate cancer mortality is a more critical endpoint than prostate cancer incidence 67. Finally, desaturation enzymes that convert ALA into EPA and DHA can be upregulated in some cancer cells, suggesting the possibility that it was the disease that raised the omega-3 levels, not the omega-3 levels that raised the disease risk 68.
Results from other observational studies using dietary intake data suggest that higher intakes of fish and/or omega-3s reduce prostate cancer risk. Both fish and omega-3 consumption were associated with a lower risk of fatal prostate cancer in a cohort of 293,464 men participating in the NIH-AARP study 69. In the Health Professionals Follow-up Study, a prospective cohort of over 47,000 men aged 40–75 years, those who consumed fish more than three times per week had a lower risk of metastatic prostate cancer than those who consumed fish less than twice per month 70. However, men who used fish oil supplements did not have a decreased risk of prostate cancer.
A number of systematic reviews and meta-analyses of prospective studies of the effects of fish intakes, omega-3 intakes, and omega-3 blood levels on prostate cancer risk have had inconsistent findings as well. For example, circulating levels of EPA, but not DHA, were positively associated with prostate cancer risk in a meta-analysis of 5,098 men with prostate cancer and 6,649 men without prostate cancer from seven studies 71. Another meta-analysis of 12 studies that included 4,516 men with prostate cancer and 5,728 men without prostate cancer found that high serum levels of these LC omega-3s were positively associated with high-grade disease 72. In other analyses, dietary intakes of LC omega-3s had no effect on prostate cancer risk 73, whereas fish consumption decreased prostate cancer mortality but had no effect on prostate cancer incidence 74. A 2015 meta-analysis found no significant associations between dietary intakes or blood levels of long chain omega-3s and total prostate cancer risk 75. The authors noted that most dietary-intake studies included in their meta-analysis found inverse associations, whereas biomarker studies of blood levels of these fatty acids found positive associations.
Overall, the evidence to date shows no consistent relationships between prostate cancer risk or mortality and omega-3 intakes or blood levels.
Other cancers
Evidence is limited for a role of omega-3s in the prevention of cancers at other sites. For example, evidence is insufficient to determine whether omega-3s affect the risk of skin cancers, including basal-cell carcinoma, squamous-cell carcinoma, and melanoma 76. Findings from the Australian Ovarian Cancer Study suggest that there is no association between total or individual omega-3 intakes from foods and ovarian cancer risk 77.
Associations between omega-3 intakes and endometrial cancer have been mixed. Some evidence indicates that dietary intakes of EPA and DHA may provide protection from the development of endometrial cancer 78. Other evidence indicates that they decrease risk in normal-weight women but have no effect or even increase risk in overweight or obese women 79.
A systematic review and meta-analysis of 9 prospective cohort and 10 case-control studies did not find an association between fish or long chain -omega-3 intakes and risk of pancreatic cancer 80. Similarly, systematic reviews and meta-analyses have not found significant associations between fish consumption and risk of gastric or esophageal cancers 81.
Summary
Overall, data from observational studies show no consistent relationship between omega-3s and overall cancer risk. Although there are some suggestions of reduced risk for breast and possibly colorectal cancers with higher long chain omega-3 intakes, randomized clinical trials are needed to confirm these findings.
The VITAL trial will examine the effects of EPA (465 mg/day) and DHA (375 mg/day) supplementation (with and without 2,000 IU/day vitamin D) for 5 years in 25,875 older adults on the primary prevention of cancer and cardiovascular disease 46. Results from this clinical trial will shed more light on possible associations between these omega-3s and cancer.
Alzheimer’s disease, dementia, and cognitive function
Some, but not all, observational studies suggest that diets high in long chain omega-3s are associated with a reduced risk of cognitive decline, Alzheimer’s disease, and dementia 82, 83. Because DHA is an essential component of cellular membrane phospholipids in the brain, researchers hypothesize that long chain omega-3s might protect cognitive function by helping to maintain neuronal function and cell- membrane integrity within the brain 83. This hypothesis is supported by findings from case-control studies indicating that patients with Alzheimer’s disease have lower serum levels of DHA than cognitively healthy people 84, 85. Lower serum DHA levels are also associated with more cerebral amyloidosis (build-up of protein deposits called amyloids) in healthy older adults, whereas higher DHA is correlated with preservation of brain volume 86.
Several systematic reviews and meta-analyses, including a Cochrane review, have assessed the effects of omega-3 supplementation on cognitive function and dementia in healthy older adults and those with Alzheimer’s disease or cognitive impairment 83, 87, 88, 89. Overall, the findings indicate that LC omega-3 supplementation does not affect cognitive function in healthy older adults or in people with Alzheimer’s disease compared to placebo. For people with mild cognitive impairment, omega-3s may improve certain aspects of cognitive function, including attention, processing speed, and immediate recall 89. However, these findings need to be confirmed in additional clinical trials.
Age-Related Macular Degeneration (AMD)
Age-Related Macular Degeneration (AMD) is a major cause of vision loss among older adults. In most cases, severe vision loss is associated with advanced AMD, which consists of either central geographic atrophy (dry AMD, the most common form) or neovascular AMD (wet AMD). Based on DHA’s presence as a structural lipid in retinal cellular membranes and the beneficial effects of EPA-derived eicosanoids on retinal inflammation, neovascularization, and cell survival, researchers have suggested that these long chain omega-3s have cytoprotective effects in the retina that may help prevent the development or progression of AMD 90.
Results from observational studies suggest that people who consume higher amounts of fatty fish and/or dietary long chain omega-3s have a lower risk of developing AMD. In the cross-sectional EUREYE study of 2,275 participants aged 65 years or older, those who ate fatty fish at least once per week had a 53% lower risk of neovascular AMD than those who consumed fatty fish less often 91. Results were similar in a study in 681 elderly male twins 92 and an analysis of 38,022 healthy female health professionals 93. In the latter study, women in the highest tertiles of dietary DHA plus EPA intake (median of 330 mg/day) had a 38% lower risk of developing AMD during an average of 10 years of follow-up than those in those in the lowest tertile (median intake of 80 mg/day). Higher serum and erythrocyte membrane levels of EPA (but not DHA) have also been associated with a lower risk of neovascular AMD 94.
In the AREDS study, a dietary supplement formulation containing 15 mg beta-carotene, 400 IU vitamin E, 500 mg vitamin C, 80 mg zinc, and 2 mg copper reduced the risk of advanced AMD in people with intermediate AMD or advanced AMD in one eye 95. Data from a nested cohort study within the AREDS population indicated that participants who reported the highest omega-3 intakes were about 30% less likely to develop central geographic atrophy and neovascular AMD than other participants 96.
These findings, combined with other epidemiological evidence, formed the basis for the AREDS2 clinical trial that examined whether adding 350 mg DHA and 650 mg EPA to the AREDS formulation further reduced the risk of progression to advanced AMD 97. The results showed that EPA and DHA did not provide any additional benefits after a median follow-up of 5 years. These findings are in line with those from a Cochrane review 98 that included the results from AREDS2 and the Nutritional AMD Treatment 2 study 99, a 3-year randomized clinical trial of LC omega-3 supplements (840 mg/day DHA and 270 mg/day EPA) in patients with early age-related maculopathy and neovascular AMD. The Cochrane review authors concluded that long chain omega-3 supplementation for up to 5 years in people with AMD does not reduce the risk of progression to advanced AMD or of moderate to severe vision loss.
Dry eye disease
About 14% of adults in the United States have dry eye disease, a chronic condition in which decreased tear volume and quality leads to ocular surface inflammation and damage, causing discomfort and visual impairment 100. Older women, in particular, have a higher risk of dry eye disease than other groups, possibly because of hormonal changes that affect the tear-producing glands 100. Researchers hypothesize that omega 3s—particularly EPA and DHA—might reduce the risk of dry eye disease and relieve its symptoms because of their anti-inflammatory activity, and many patients take them as adjunctive treatments to artificial tears and other medications.
Some, but not all, observational studies show inverse associations between self-reported dietary consumption of omega-3s and risk of dry eye disease. For example, in a cross-sectional study of 32,470 women aged 45–84 participating in the Women’s Health Study, those in the highest quintile of total dietary omega-3 intake (mean of 1,990 mg/day) had a 17% lower risk of dry eye disease than those in the lowest quintile (mean intake of 920 mg/day) 101. The study found a similar association for DHA—women in the highest versus the lowest quintiles of DHA intake had a 12% lower risk of dry eye disease; however, the results showed no significant associations for EPA. But in another cross-sectional study of 322 postmenopausal women, total dietary omega-3 intakes were not correlated with the prevalence of dry eye disease 102.
Results from clinical trials using omega-3 supplementation, primarily EPA and DHA, have had mixed results in reducing the symptoms and signs of dry eye disease. Furthermore, there is no consensus on the optimal dose, composition, or length of omega-3 treatment for this condition 103.
The studies that have found beneficial effects from omega-3 supplementation for symptoms and signs of dry eye disease include one showing that daily supplementation with 1,000 mg omega-3s (650 mg EPA plus 350 mg DHA) for 3 months in 518 men and women (mean age about 40 years) living in northern India reduced symptoms and some signs of dry eye disease compared with placebo 104. In another clinical trial of 105 men and women, daily treatment with supplements containing 2,240 mg omega-3s (1,680 mg EPA and 560 mg DHA as re-esterified triglycerides) for 12 weeks also reduced symptoms of dry eye disease compared with placebo 105. In addition, the supplements increased tear break-up time and decreased tear osmolarity (which would be likely to reduce ocular surface damage).
However, another large, randomized, double-blind clinical trial conducted in the United States found that EPA and DHA from fish oil supplements are no better than placebo at relieving symptoms or signs of dry eye disease 100. This 12-month trial included 535 participants (about 81% female) aged 18 years or older (mean age about 58 years) with at least a 6-month history of moderate to severe dry eye disease. Among them, 349 participants received daily supplements of 3,000 mg omega-3s (2,000 mg EPA plus 1,000 mg DHA), and 186 received a placebo containing 5,000 mg olive oil. Participants could continue taking medications for dry eyes, including artificial tears and prescription anti-inflammatory eye drops, as well as omega-3 supplements as long as the total dose of EPA plus DHA was less than 1,200 mg per day. At the end of the study, symptoms were less severe than at baseline in both groups, but the results showed no significant differences between groups. Groups also showed no significant differences compared with baseline in signs of dry eye disease, including conjunctive and cornea integrity as well as tear volume and quality.
Overall, the evidence to date shows no consistent relationship between omega-3s and dry eye disease. More research is warranted to fully understand whether increased intakes of dietary or supplemental omega-3s help reduce the risk of dry eye disease and whether they are beneficial as an adjunct treatment.
Rheumatoid arthritis
Rheumatoid arthritis (RA) is an autoimmune disease characterized by chronic inflammation of the joints. Its symptoms include pain, swelling, stiffness, and functional impairments. RA is typically treated with nonsteroidal antiinflammatory drugs (NSAIDs), corticosteroids, and disease-modifying antirheumatic drugs. Due to their antiinflammatory effects, some scientists hypothesize that long chain omega-3s reduce some of the symptoms of rheumatoid arthritis and patients’ reliance on NSAIDs and corticosteroids.
A 2012 systematic review concluded that the types of omega-3s found in seafood and fish oil may be modestly helpful in relieving symptoms of rheumatoid arthritis. In the studies included in the review, many of the participants reported that when they were taking fish oil they had briefer morning stiffness, less joint swelling and pain, and less need for anti-inflammatory drugs to control their symptoms.
Reviews and meta-analyses of studies that assessed whether fish oil and long chain omega-3s are beneficial for rheumatoid arthritis have had inconsistent findings. Some suggest that they do not significantly affect the clinical symptoms of RA but do reduce the amounts of NSAIDs and corticosteroids that patients need. Others indicate that LC omega-3s reduce joint swelling and pain, morning stiffness, and number of painful joints in addition to reducing NSAID use. Some researchers suggest that differences in findings could be due in part to whether patient-determined use of NSAIDs is considered a measure of pain.
Findings to date suggest that long chain omega-3s may be helpful as an adjunctive treatment to pharmacotherapy for ameliorating the symptoms of rheumatoid arthritis 106, 107. However, more research is needed to confirm this finding.
Depression
A 2016 meta-analysis of 26 studies found a 17% lower risk of depression with higher fish intake 108. However, a 2015 Cochrane review of 26 studies found insufficient evidence to determine whether omega-3s (1,000 to 6,600 mg/day EPA, DHA, and/or other omega-3s) are beneficial for major depressive disorder in adults 109. The authors did find a small-to-modest beneficial effect on depressive symptoms, but they concluded that this effect was not clinically significant.
Bipolar disorder
This systematic review (source 110) investigated the efficacy of omega-3 fatty acids for bipolar disorder. Five randomised controlled trials met inclusion criteria for the review. Only one trial provided data that could be analysed, investigating ethyl-EPA as an adjunctive treatment in a mixed outpatient population. Some positive benefits were found for depressive symptoms but not for mania, and no adverse events were reported. There is currently insufficient evidence on which to base any clear recommendations concerning omega-3 fatty acids for bipolar disorder. However, given the general health benefits and safety of omega-3, the preliminary evidence from this review provides a strong case for well-powered, high-quality trials in specific index populations.
Results from one study showed positive effects of omega-3 as an adjunctive treatment for depressive but not manic symptoms in bipolar disorder. These findings must be regarded with caution owing to the limited data available. There is an acute need for well-designed and executed randomised controlled trials in this field.
Inflammatory bowel disease
The authors of a systematic review of 19 randomized controlled trials concluded that the available evidence does not support the use of omega-3 supplements to treat active or inactive inflammatory bowel disease 111. Similarly, the authors of a Cochrane review concluded that, based on the evidence from two large, high-quality studies, omega-3 supplements are probably not effective for maintaining remission in people who have Crohn’s disease 112.
Autism Spectrum Disorders
It has been suggested that difficulties associated with autism spectrum disorders may be explained in part by lack of omega-3 fatty acids, and that supplementation of these essential fatty acids may lead to improvement of symptoms. To date there is no high quality evidence that omega-3 fatty acids supplementation is effective for improving core and associated symptoms of autism spectrum disorder. Given the paucity of rigorous studies in this area, there is a need for large well-conducted randomised controlled trials that examine both high and low functioning individuals with autism spectrum disorder and that have longer follow-up periods 113.
ADHD
A systematic review and meta-analysis of 10 studies in children with ADHD or related neurodevelopmental disorders, such as developmental coordination disorder, found no improvements with omega-3 supplementation on measures of emotional lability, oppositional behavior, conduct problems, or aggression 114. However, in subgroup analyses of only the higher-quality studies and those with strict inclusion criteria, omega-3 supplementation (60 to 1,296 mg/day EPA and/or DHA) did significantly improve parent-rated emotional lability and oppositional behavior.
Childhood allergies
A systematic review and meta-analysis of 10 prospective cohort studies and 5 randomized clinical trials on omega-3 intakes during pregnancy and outcomes of childhood allergic disease (eczema, rhino-conjunctivitis, and asthma) found inconsistent results 115. Although the authors could not draw firm conclusions due to the heterogeneity of the studies and their results, they concluded that the overall findings were “suggestive” of a protective association between higher maternal intakes of LC omega-3s or fish and incidence of allergic disease symptoms in the offspring. The authors of a Cochrane review that included eight LC omega-3 supplementation trials concluded that there is limited evidence to support the use of LC omega-3 supplements by women during pregnancy and/or lactation for reducing the risk of allergic disease in their children 116.
Cystic fibrosis
A Cochrane review of four studies of cystic fibrosis found that omega-3 supplements (300 to 5,400 mg/day EPA and/or DHA) might improve lung function and increase blood levels of essential fatty acids in people with cystic fibrosis 117. However, the authors concluded that there is not enough evidence to recommend routine use of omega-3 supplements by people with cystic fibrosis.
What is cod liver oil good for
Since the 19th century, cod liver oil, for its source of vitamin D, has been used as one of the remedies to cure rickets 118. Rickets, a disease of vitamin D deficiency, although rare, is still diagnosed in the United States. Cod liver oil has been the most commonly used supplement in the US for decades. Vitamin D status is determined by diet and degree of exposure to sunlight. Individuals with dark skin pigmentation who reside in northern latitudes or those with poor sun exposure are most at risk for seasonal hypovitaminosis D 119. Breast milk is a poor source of vitamin D 120. Low vitamin D status is commonly observed at northern latitudes such as in Scandinavia during wintertime, with a drop in serum concentrations of 25-hydroxyvitamin D (s-25(OH)D) and a corresponding increase in serum parathyroid hormone levels (PTH) and bone turnover 121. In addition to latitude and season, individual sun exposure and vitamin D supplementation are strong predictors of vitamin D status 122. Maintaining serum concentrations of 25-hydroxyvitamin D (s-25(OH)D) and suppressing parathyroid hormone levels (PTH) through winter is expected to be beneficial in order to prevent bone resorption. Possible direct means of increasing wintertime vitamin D status at northern latitudes may be increased fortification of foods 123, or increased supplementation. Current recommended dietary intake of vitamin D for adults in European countries and the US varies between 0–15 μg/day (20 μg/day for elderly in the US) 124, 125. Daily supplementation with 10 μg (400 IU) vitamin D is recommended to elderly individuals with low sun exposure in the Nordic countries 126. Norwegian Health Authorities have recommended 5 ml of cod liver oil daily (400 IU of vitamin D) for more than 60 years to prevent diseases like rickets, formerly more prevalent in areas with little access to vitamin D-rich fatty fish 127. A survey from 1997 estimated that about 35% of the Norwegian population and 50% of those aged 60–79 were still using the supplement on a daily basis 128.
There seems to be large variation in s-25(OH)D in response to oral supplementation. According to a summary of various studies published up to 1999 129, a daily dose of 10 μg (400 IU) vitamin D led to an average increase in serum concentrations of 25-hydroxyvitamin D (s-25(OH)D) of 31 nmol/l, although with large variation between studies, suggesting that additional factors may influence the degree of increase. A systematic review concluded that the degree of PTH suppression achieved by vitamin D supplementation depends not only on baseline PTH and increase in serum concentrations of 25-hydroxyvitamin D (s-25(OH)D), but also on the subjects’ age and mobility 130. Healthy young students in Coleraine, Northern Ireland (55°N) who received a daily oral supplement of 15 μg (600 IU) vitamin D3 for 8 weeks in late winter, increased their mean serum concentrations of 25-hydroxyvitamin D (s-25(OH)D) from 47.9 to 86.5 nmol/l, but the supplementation did not influence PTH levels or bone turnover significantly 131. In a recent 2-center double-blind placebo-controlled study from the same group, 215 persons aged 20–40 received 0, 5, 10, or 15 μg vitamin D3 daily during 22 weeks in late winter, but supplementation did not affect PTH levels or bone turnover 132. Elderly osteoporotic women in sunshine abundant São Paulo, Brazil (23°S) who received 10 μg (400 IU) vitamin D3 daily for three months increased their mean s-25(OH)D from 46.7 to 59.5 nmol/l, whereas PTH levels or bone turnover were not significantly affected 133.
Serum concentrations of 25-hydroxyvitamin D (s-25(OH)D) above 50 nmol/l has been associated with optimal musculoskeletal function in elderly 134, and this level is commonly used as cut-off for vitamin D sufficiency in European populations 135. However, some advocate a target serum concentrations of 25-hydroxyvitamin D (25(OH)D) in the adult European and US population of at least 75 nmol/l for optimal fall and fracture prevention, and this requires daily supplementation of at least 18–25 μg (700–1000 IU) 136.
In the first randomized trial from Norway compared the effect of two different modes of administration of vitamin D3 – fish oil capsule containing Omega-3 fatty acids vs. multivitamin tablet on markers of the vitamin D endocrine system and bone turnover. In that Norwegian study 137 healthy adults aged 19–48 years living in Oslo, Norway (59°N) were randomized to receive a daily dose of 10 μg vitamin D3 given as either fish oil capsules or multivitamin tablets during four weeks in late winter. Serum samples from baseline and after 28 days were analyzed for 25-hydroxyvitamin D (s-25(OH)D), 1,25-dihydroxyvitamin D (s-1,25(OH)2D), intact parathyroid hormone (s-iPTH), and osteoclast-specific tartrate-resistant acid phosphatase 5b (s-TRACP). Fifty-five eligible participants completed the intervention (74% of those randomized). The researchers found no effect of type of vitamin D supplement (solid multivitamin tablet or fish oil capsule containing Omega-3 fatty acids) on either increase in vitamin D status 138 or in the change in parathyroid hormone (PTH), the active vitamin D hormone, or osteoclast activity. Four weeks of daily supplementation with 10 μg vitamin D3 decreased mean intact parathyroid hormone and increased osteoclast-specific tartrate-resistant acid phosphatase 5b concentration, and this did not differ by mode of administration. The results suggest an increased bone resorption following vitamin D supplementation in young individuals, despite a decrease in parathyroid hormone levels 137.
The AGES-Reykjavik Study (age 66–96 years; N=4798) found no significant association between retrospective intake of cod liver oil in adolescence or midlife and hip bone mineral density among participants 139. Current intake was also not associated with hip bone mineral density in men. Women with daily intake of cod liver oil had slightly higher Z-scores average 0.1 higher of both femoral neck and trochanteric region compared to those with the lowest frequency of consumption (intake of <once/week). Current cod liver oil intake of both sexes was positively associated with serum 25(OH)D concentration, individuals with intake of <once/week, 1–6 times/week and daily intake having concentrations of approximately 40nmol/L, 50nmol/L, and 60nmol/L respectively. Although significant, this difference is slight and clinical relevance is questionable 139. In conclusion, the research found no evidence that cod liver oil intake at any age might be harmful to hip bone mineral density in old age. For current intake a slight positive association was seen for hip bone mineral density among women. Possibly, the relatively high median serum 25(OH)D concentration in the study population, even among those not taking cod liver oil or other vitamin D containing supplements, may mask any putative, more profound relationship between current intake and hip bone mineral density. Current daily intake of cod liver oil was associated with an increase of approximately 20nmol/L in 25(OH)D concentration, compared to no intake or less than once a week.
The significance of cod liver oil intake at various ages for bone health in old age warrants further study, especially intake during childhood and adolescence, as cod liver oil is supplied in several schools and child care centers in Iceland for public health purposes.
There is ongoing research concerning the role of omega-3 fatty acids in bone health, as bone loss due to increased osteoclast activity may be mediated by inflammatory cytokines, and some studies suggest a protective effect of omega-3 fatty acids on bone resorption 140. In bone marrow from ovarioectomized mice, addition of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) led to significantly reduced osteoclast-specific tartrate-resistant acid phosphatase 5b activity and osteoclastogenesis 141. A protective effect of omega-3 fatty acids (0.5 g/day) in fish oil on bone resorption was not supported in the data in young adults, as subjects’ serum osteoclast-specific tartrate-resistant acid phosphatase 5b increased regardless of being randomized to ingest fish oil capsules containing omega-3 fatty acids, or solid tablets. The increase in serum osteoclast-specific tartrate-resistant acid phosphatase 5b was even slightly higher in the group ingesting fish oil capsules (not shown/not significant) 137.
The appropriate dose of cod liver oil depends on several factors such as the user’s age, health, and several other conditions. At this time there is not enough scientific information to determine an appropriate range of doses for cod liver oil. Keep in mind that natural products are not always necessarily safe and dosages can be important. Be sure to follow relevant directions on product labels and consult your pharmacist or physician or other healthcare professional before using.
How effective is cod liver oil?
The effectiveness ratings for cod liver oil are as follows:
Insufficient evidence to rate effectiveness for:
- Age-related macular degeneration. People who eat a lot of fish and take cod liver oil don’t have a lower risk of developing this condition compared to people who just eat a lot of fish.
- Irregular heartbeat. Taking cod liver oil by mouth might reduce a specific type of irregular heartbeat in some people. But it’s not known if this reduces the risk of heart-related death. Taking cod liver oil by mouth does not seem to reduce irregular heartbeat in men with irregular heartbeat after a heart attack.
- Depression. Taking cod liver oil has been linked with a 29% lower chance of older adults having depression symptoms.
- High cholesterol levels in the blood. Taking cod liver oil by mouth doesn’t lower cholesterol levels in people with high cholesterol. But it might increase “good” high-density lipoprotein cholesterol levels in people with type 1 diabetes and high cholesterol. Also it might lower blood fats called “triglycerides” in men who have had a heart attack. But cod liver oil doesn’t improve these outcomes in people with an inherited form of high cholesterol.
- High blood pressure. Taking cod liver oil by mouth seems to slightly lower blood pressure in healthy people and those with slightly high blood pressure. But it’s not clear if this reduction is clinically meaningful for people with very high cholesterol.
- Inflammatory bowel disease. Some people with inflammatory bowel disease have joint pain. Taking cod liver oil might reduce joint pain in some people with this condition.
- Osteoarthritis. Taking cod liver oil along with an NSAID doesn’t reduce swelling in people with osteoarthritis better than taking an NSAID alone.
- Ear infections in young children. Taking cod liver oil and a multivitamin might reduce the need to use medicine to treat ear infections in young children by about 12%.
- Airway infections. Giving young children cod liver oil and a multivitamin seems to reduce the number of doctor’s office visits for airway infections.
- Rheumatoid arthritis. Taking cod liver oil might decrease pain, morning stiffness, and swelling in some patients with rheumatoid arthritis. Also, taking cod liver oil and fish oil seems to reduce the need to use medicine to treat joint swelling in people with this condition.
- Vitamin D deficiency. Taking cod liver oil seems to increase blood levels of vitamin D in some people. But it’s not clear if cod liver oil increases vitamin D to normal levels in people with low levels of vitamin D.
- Wound healing.
- Other conditions.
More evidence is needed to rate cod liver oil for these uses.
Cod liver oil side effects
Cod liver oil is likely safe for most adults and children when taken by mouth. It can cause side effects including belching, bad breath, heartburn, loose stools, and nausea. Taking cod liver oil with meals can often decrease these side effects.
High doses of cod liver oil are POSSIBLY UNSAFE. They might keep blood from clotting and can increase the chance of bleeding. Vitamin A and vitamin D levels might also become too high with high doses of cod liver oil.
The safety of cod liver oil when used on the skin is unknown.
Special precautions and warnings
Pregnancy and breast-feeding: Cod liver oil is possibly safe when used in amounts that provide no more than the recommended daily intakes of vitamin A and vitamin D. Cod liver oil is POSSIBLY UNSAFE when taken in larger amounts. Women who are pregnant or breast-feeding should not take cod liver oil that provides more than about 3000 mcg of vitamin A and 100 mcg of vitamin D.
Diabetes: There has been some concern that cod liver oil or other fish oils might increase blood sugar in people with diabetes. But there is no strong research that supports this concern.
High blood pressure: Cod liver oil can lower blood pressure and might cause blood pressure to go too low if used along with medications for high blood pressure. Be careful when using cod liver oil if you are taking high blood pressure drugs.
Interactions with medications
Moderate
Be cautious with this combination.
- Medications for high blood pressure (Antihypertensive drugs)
Cod liver oil seems to decrease blood pressure. Taking cod liver oil along with medications for high blood pressure might cause your blood pressure to go too low.
Some medications for high blood pressure include captopril (Capoten), enalapril (Vasotec), losartan (Cozaar), valsartan (Diovan), diltiazem (Cardizem), amlodipine (Norvasc), hydrochlorothiazide (HydroDIURIL), furosemide (Lasix), and many others.
- Medications that slow blood clotting (Anticoagulant / Antiplatelet drugs)
Cod liver oil might slow blood clotting. Taking cod liver oil along with medications that also slow clotting might increase the chances of bruising and bleeding.
Some medications that slow blood clotting include aspirin, clopidogrel (Plavix), diclofenac (Voltaren, Cataflam, others), dipyridamole (Persantine), ibuprofen (Advil, Motrin, others), naproxen (Anaprox, Naprosyn, others), dalteparin (Fragmin), enoxaparin (Lovenox), heparin, ticlopidine (Ticlid), warfarin (Coumadin), and others.
- Interactions with herbs and supplements
Herbs and supplements that lower blood pressure (hypotensive herbs and supplements)
Cod liver oil might lower blood pressure. It has the potential to add to blood pressure lowering effects of other herbs and supplements that also lower blood pressure. Other herbs and supplements that can lower blood pressure include andrographis, casein peptides, cat’s claw, coenzyme Q10, L-arginine, lycium, stinging nettle, theanine, and others.
Herbs and supplements that might slow blood clotting
Cod liver oil might slow blood clotting. Using cod liver oil with herbs and supplements that also slow blood clotting might increase the chance of bruising and bleeding in some people. These herbs include angelica, borage seed oil, clove, danshen, garlic, ginger, ginkgo, red clover, turmeric, willow, and others.
- Shahidi F. Nutraceutical and Specialty Lipids and Their Co-Products. CRC Press; Boca Raton, FL, USA: 2006. pp. 231–232.[↩]
- Thibane V.S., Kock J.L., Ells R., Wyk P.W., Pohl C.H. Effect of marine polyunsaturated fatty acids on biofilm formation of Candida albicans and Candida dubliniensis. Mar. Drugs. 2010;8:2597–2604. doi: 10.3390/md8102597 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2992994/[↩]
- Kabara J.J., Swieczkowski D.M., Conley A.J., Truant T.J.P. Fatty Acids and Derivatives as Antimicrobial Agents. Antimicrob. Agents Chemother. 1972;2:23–28. doi: 10.1128/AAC.2.1.23[↩]
- Loftsson T., Ilievska B., Asgrimsdottir G.M., Ormarsson O.T., Stefansson E. Fatty acids from marine lipids: Biological activity, formulation and stability. J. Drug Deliv. Sci. Technol. 2016 doi: 10.1016/j.jddst.2016.03.007[↩]
- Loftsson T., Thormar H., Hjalmarsdottir M. Antibacterial activities of fatty acids extracts from cod liver oil. 1997. unpublsihed work.[↩]
- Loftsson T., Gudmundsdóttir T.K., Fridriksdóttir H., Sigurdardóttir A.M., Thorkelsson J., Gudmundsson G., Hjaltason B. Fatty acids from cod-liver oil as skin penetration enhancers. Pharmazie. 1995;50:188–190.[↩]
- Desbois A.P., Smith V.J. Antibacterial free fatty acids: Activities, mechanisms of action and biotechnological potential. Appl. Microbiol. Biotechnol. 2009;85:1629–1642. doi: 10.1007/s00253-009-2355-3[↩]
- Brasky T.M., Lampe J.W., Potter J.D., Patterson R.E., White E. Specialty supplements and breast cancer risk in the VITamins And Lifestyle (VITAL) Cohort. Cancer Epidemiol. Biomark. Prev. 2010;19:1696–1708. doi: 10.1158/1055-9965.EPI-10-0318 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2906099/[↩]
- Chowdhury R., Stevens S., Gorman D., Pan A., Warnakula S., Chowdhury S., Ward H., Johnson L., Crowe F., Hu F.B., et al. Association between fish consumption, long chain omega 3 fatty acids, and risk of cerebrovascular disease: Systematic review and meta-analysis. BMJ. 2012;345:e6698. doi: 10.1136/bmj.e6698 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3484317/[↩]
- Scientific Advisory Committee on Nutrition (SACN) Update on Vitamin D. The Stationary Office (TSO); London, UK: 2007.[↩]
- Mulholland C.A., Benford D.J. What is known about the safety of multivitamin-multimineral supplements for the generally healthy population? Theoretical basis for harm. Am. J. Clin. Nutr. 2007;85:318S–322S[↩]
- Fatty acids from cod-liver oil as skin penetration enhancers. Loftsson T, Gudmundsdóttir TK, Fridriksdóttir H, Sigurdardóttir AM, Thorkelsson J, Gudmundsson G, Hjaltason B. Pharmazie. 1995 Mar; 50(3):188-90. https://www.ncbi.nlm.nih.gov/pubmed/7732049[↩]
- Jenkins DJA, Josse AR. Fish oil and omega-3 fatty acids. CMAJ : Canadian Medical Association Journal. 2008;178(2):150. doi:10.1503/cmaj.071754. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2174990/[↩][↩][↩]
- Dietary intakes of omega-6 and omega-3 polyunsaturated fatty acids and the risk of breast cancer. Thiébaut AC, Chajès V, Gerber M, Boutron-Ruault MC, Joulin V, Lenoir G, Berrino F, Riboli E, Bénichou J, Clavel-Chapelon F. Int J Cancer. 2009 Feb 15; 124(4):924-31. https://www.ncbi.nlm.nih.gov/pubmed/19035453/[↩]
- Dietary linoleic acid influences desaturation and acylation of deuterium-labeled linoleic and linolenic acids in young adult males. Emken EA, Adlof RO, Gulley RM. Biochim Biophys Acta. 1994 Aug 4; 1213(3):277-88. https://www.ncbi.nlm.nih.gov/pubmed/7914092/[↩]
- Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Circulation. 1999 Feb 16; 99(6):779-85. https://www.ncbi.nlm.nih.gov/pubmed/9989963/[↩]
- Dietary intake of alpha-linolenic acid and risk of fatal ischemic heart disease among women. Hu FB, Stampfer MJ, Manson JE, Rimm EB, Wolk A, Colditz GA, Hennekens CH, Willett WC. Am J Clin Nutr. 1999 May; 69(5):890-7. http://ajcn.nutrition.org/content/69/5/890.long[↩]
- alpha-Linolenic acid intake is not beneficially associated with 10-y risk of coronary artery disease incidence: the Zutphen Elderly Study. Oomen CM, Ocké MC, Feskens EJ, Kok FJ, Kromhout D. Am J Clin Nutr. 2001 Oct; 74(4):457-63. http://ajcn.nutrition.org/content/74/4/457.long[↩]
- Arterial compliance in obese subjects is improved with dietary plant n-3 fatty acid from flaxseed oil despite increased LDL oxidizability. Nestel PJ, Pomeroy SE, Sasahara T, Yamashita T, Liang YL, Dart AM, Jennings GL, Abbey M, Cameron JD. Arterioscler Thromb Vasc Biol. 1997 Jun; 17(6):1163-70. http://atvb.ahajournals.org/content/17/6/1163.long[↩]
- Dietary supplementation with marine omega-3 fatty acids improve systemic large artery endothelial function in subjects with hypercholesterolemia. Goodfellow J, Bellamy MF, Ramsey MW, Jones CJ, Lewis MJ. J Am Coll Cardiol. 2000 Feb; 35(2):265-70. https://www.ncbi.nlm.nih.gov/pubmed/10676668/[↩]
- Fish oil improves arterial compliance in non-insulin-dependent diabetes mellitus. McVeigh GE, Brennan GM, Cohn JN, Finkelstein SM, Hayes RJ, Johnston GD. Arterioscler Thromb. 1994 Sep; 14(9):1425-9. http://atvb.ahajournals.org/content/14/9/1425.long[↩]
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005.[↩][↩][↩]
- Omega-3 fatty acid content of the US food supply. Raper NR, Cronin FJ, Exler J. J Am Coll Nutr. 1992 Jun; 11(3):304-8. https://www.ncbi.nlm.nih.gov/pubmed/1619182/[↩]
- Kris-Etherton PM, Taylor DS, Yu-Poth S, Huth P, Moriarty K, Fishell V, et al. Polyunsaturated fatty acids in the food chain in the United States. Am J Clin Nutr 2000;71(Suppl 1):179-88.[↩]
- Breast cancer risk in rats fed a diet high in n-6 polyunsaturated fatty acids during pregnancy. Hilakivi-Clarke L, Onojafe I, Raygada M, Cho E, Clarke R, Lippman ME. J Natl Cancer Inst. 1996 Dec 18; 88(24):1821-7. https://www.ncbi.nlm.nih.gov/pubmed/8961971/[↩]
- Linoleic acid intake and cancer risk: a review and meta-analysis. Zock PL, Katan MB. Am J Clin Nutr. 1998 Jul; 68(1):142-53. https://www.ncbi.nlm.nih.gov/pubmed/9665108/[↩]
- Holub BJ. Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Hoffer LJ, Jones PJ, eds. CMAJ: Canadian Medical Association Journal. 2002;166(5):608-615. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩][↩]
- EPA and DHA Content of Fish Species. https://health.gov/dietaryguidelines/dga2005/report/html/table_g2_adda2.htm[↩]
- Dullemeijer C, Durga J, Brouwer IA, et al. n 3 fatty acid proportions in plasma and cognitive performance in older adults. Am J Clin Nutr. 2007;86:1479–1485. https://www.ncbi.nlm.nih.gov/pubmed/17991662[↩]
- Kannass KN, Colombo J, Carlson SE. Maternal DHA levels and toddler free-play attention. Dev Neuropsychol. 2009;34:159–174. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752039/[↩]
- Muldoon MF, Ryan CM, Sheu L, Yao JK, Conklin SM, Manuck SB. Serum phospholipid docosahexaenonic acid is associated with cognitive functioning during middle adulthood. J Nutr. 2010;140:848–853. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2838625/[↩]
- Bauer I, Crewther DP, Pipingas A, Rowsell R, Cockerell R, Crewther SG. Omega-3 fatty acids modify human cortical visual processing: a double-blind, crossover study. PLoS One. 2011;6:e28214. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3235106/[↩]
- van Gelder BM, Tijhuis M, Kalmijn S, Kromhout D. Fish consumption, n-3 fatty acids, and subsequent 5-y cognitive decline in elderly men: the Zutphen Elderly Study. Am J Clin Nutr. 2007;85:1142–1147. https://www.ncbi.nlm.nih.gov/pubmed/17413117[↩]
- González S, Huerta JM, Fernández S, Patterson AM, Lasheras C. The relationship between dietary lipids and cognitive performance in an elderly population. Int J Food Sci Nutr. 2010;61:217–225. https://www.ncbi.nlm.nih.gov/pubmed/20001761[↩]
- Jicha GA, Markesbery WR. Omega-3 fatty acids: potential role in the management of early Alzheimer’s disease. Clin Interv Aging. 2010;5:45–61. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2854051/[↩]
- Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Kris-Etherton PM, Harris WS, Appel LJ, American Heart Association. Nutrition Committee. Circulation. 2002 Nov 19; 106(21):2747-57. http://circ.ahajournals.org/content/106/21/2747.long[↩][↩]
- Am J Clin Nutr July 2006, vol. 84 no. 1 5-17. n−3 Fatty acids from fish or fish-oil supplements, but not α-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-prevention studies: a systematic review. http://ajcn.nutrition.org/content/84/1/5.long[↩][↩][↩]
- He K, Song Y, Daviglus ML, et al. Accumulated evidence on fish consumption and coronary heart disease mortality: a meta-analysis of cohort studies. Circulation 2004;109:2705–11. http://circ.ahajournals.org/content/109/22/2705[↩]
- He K, Song Y, Daviglus ML, et al. Fish consumption and incidence of stroke. A meta-analysis of cohort studies. Stroke 2004;35:1538–42. http://stroke.ahajournals.org/content/35/7/1538[↩]
- Zhang J, Sasaki S, Amano K, Kesteloot H. Fish consumption and mortality from all causes, ischemic heart disease, and stroke: an ecological study. Prev Med 1999;28:520–9. https://www.ncbi.nlm.nih.gov/pubmed/10329343 [↩][↩]
- Harris WS. Omega-3 fatty acids. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:577-86.[↩]
- Djousse L, Akinkuolie AO, Wu JH, Ding EL, Gaziano JM. Fish consumption, omega-3 fatty acids and risk of heart failure: a meta-analysis. Clin Nutr 2012;31:846-53. https://www.ncbi.nlm.nih.gov/pubmed/22682084?dopt=Abstract[↩]
- Del Gobbo LC, Imamura F, Aslibekyan S, Marklund M, Virtanen JK, Wennberg M, et al. Omega-3 polyunsaturated fatty acid biomarkers and coronary heart disease: pooling project of 19 cohort studies. JAMA Intern Med 2016;176:1155-66. https://www.ncbi.nlm.nih.gov/pubmed/27357102?dopt=Abstract[↩]
- U.S. Department of Health and Human Services, U.S. Department of Agriculture. https://health.gov/dietaryguidelines/2015/guidelines/[↩]
- U.S. Food and Drug Administration. Summary of qualified health claims subject to enforcement discretion 2014. https://www.fda.gov/Food/FoodborneIllnessContaminants/Metals/ucm393070.htm[↩][↩]
- Pradhan AD, Manson JE. Update on the Vitamin D and OmegA-3 trial (VITAL). J Steroid Biochem Mol Biol 2016;155:252-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4600007/[↩][↩][↩][↩]
- Newberry SJ, Chung M, Booth M, Maglione M, Tang AM, C.E. OH, et al. Omega-3 fatty acids and maternal and child health: an updated systematic review. Evidence Report/Technology Assessment No. 224. (Prepared by the RAND Southern California Evidence-based Practice Center under Contract No. 290-2012-00006-I.) AHRQ Publication No. 16-E003-EF. Rockville, MD: Agency for Healthcare Research and Quality; 2016.[↩]
- Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012;129:2011-3552. https://www.ncbi.nlm.nih.gov/pubmed/22371471?dopt=Abstract[↩]
- U.S. Food and Drug Administration. Eating Fish: What Pregnant Women and Parents Should Know. https://www.fda.gov/downloads/Food/FoodborneIllnessContaminants/Metals/UCM536321.pdf[↩]
- O’Connor NR. Infant formula. Am Fam Physician 2009;79:565-70. https://www.ncbi.nlm.nih.gov/pubmed/19378873?dopt=Abstract[↩]
- Simmer K, Patole SK, Rao SC. Long-chain polyunsaturated fatty acid supplementation in infants born at term. Cochrane Database Syst Rev 2011:CD000376. https://www.ncbi.nlm.nih.gov/pubmed/22161363?dopt=Abstract[↩]
- Schulzke SM, Patole SK, Simmer K. Long-chain polyunsaturated fatty acid supplementation in preterm infants. Cochrane Database Syst Rev 2011:CD000375. https://www.ncbi.nlm.nih.gov/pubmed/21328248?dopt=Abstract[↩]
- Weylandt KH, Serini S, Chen YQ, Su HM, Lim K, Cittadini A, et al. Omega-3 polyunsaturated fatty acids: the way forward in times of mixed evidence. Biomed Res Int 2015;2015:143109.[↩]
- Zheng JS, Hu XJ, Zhao YM, Yang J, Li D. Intake of fish and marine n-3 polyunsaturated fatty acids and risk of breast cancer: meta-analysis of data from 21 independent prospective cohort studies. BMJ 2013;346:f3706.[↩][↩]
- MacLean CH, Newberry SJ, Mojica WA, Khanna P, Issa AM, Suttorp MJ, et al. Effects of omega-3 fatty acids on cancer risk: a systematic review. JAMA 2006;295:403-15. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0022772/[↩]
- Brasky TM, Darke AK, Song X, Tangen CM, Goodman PJ, Thompson IM, et al. Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst 2013;105:1132-41. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3735464/[↩][↩][↩]
- Gago-Dominguez M, Yuan JM, Sun CL, Lee HP, Yu MC. Opposing effects of dietary n-3 and n-6 fatty acids on mammary carcinogenesis: The Singapore Chinese Health Study. Br J Cancer 2003;89:1686-92.[↩]
- Brasky TM, Lampe JW, Potter JD, Patterson RE, White E. Specialty supplements and breast cancer risk in the VITamins And Lifestyle (VITAL) Cohort. Cancer Epidemiol Biomarkers Prev 2010;19:1696-708.[↩]
- Gerber M. Omega-3 fatty acids and cancers: a systematic update review of epidemiological studies. Br J Nutr 2012;107 Suppl 2:S228-39.[↩][↩]
- Geelen A, Schouten JM, Kamphuis C, Stam BE, Burema J, Renkema JM, et al. Fish consumption, n-3 fatty acids, and colorectal cancer: a meta-analysis of prospective cohort studies. Am J Epidemiol 2007;166:1116-25.[↩]
- Wu S, Feng B, Li K, Zhu X, Liang S, Liu X, et al. Fish consumption and colorectal cancer risk in humans: a systematic review and meta-analysis. Am J Med 2012;125:551-9 e5[↩]
- Kantor ED, Lampe JW, Peters U, Vaughan TL, White E. Long-chain omega-3 polyunsaturated fatty acid intake and risk of colorectal cancer. Nutr Cancer 2014;66:716-27.[↩]
- Brasky TM, Till C, White E, Neuhouser ML, Song X, Goodman P, et al. Serum phospholipid fatty acids and prostate cancer risk: results from the prostate cancer prevention trial. Am J Epidemiol 2011;173:1429-39[↩]
- Dahm CC, Gorst-Rasmussen A, Crowe FL, Roswall N, Tjonneland A, Drogan D, et al. Fatty acid patterns and risk of prostate cancer in a case-control study nested within the European Prospective Investigation into Cancer and Nutrition. Am J Clin Nutr 2012;96:1354-61.[↩]
- Park SY, Wilkens LR, Henning SM, Le Marchand L, Gao K, Goodman MT, et al. Circulating fatty acids and prostate cancer risk in a nested case-control study: the Multiethnic Cohort. Cancer Causes Control 2009;20:211-23.[↩]
- Alexander W. Prostate cancer risk and omega-3 Fatty Acid intake from fish oil: a closer look at media messages versus research findings. P T 2013;38:561-4.[↩]
- Torfadottir JE, Stampfer MJ, Mucci LA, Giovannucci EL. RE: Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst 2014;106:dju018[↩]
- Harris WS, Davidson MH. RE: Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst 2014;106:dju019[↩]
- Bosire C, Stampfer MJ, Subar AF, Park Y, Kirkpatrick SI, Chiuve SE, et al. Index-based dietary patterns and the risk of prostate cancer in the NIH-AARP diet and health study. Am J Epidemiol 2013;177:504-13.[↩]
- Augustsson K, Michaud DS, Rimm EB, Leitzmann MF, Stampfer MJ, Willett WC, et al. A prospective study of intake of fish and marine fatty acids and prostate cancer. Cancer Epidemiol Biomarkers Prev 2003;12:64-7.[↩]
- Crowe FL, Appleby PN, Travis RC, Barnett M, Brasky TM, Bueno-de-Mesquita HB, et al. Circulating fatty acids and prostate cancer risk: individual participant meta-analysis of prospective studies. J Natl Cancer Inst 2014;106[↩]
- Chua ME, Sio MC, Sorongon MC, Morales ML, Jr. The relevance of serum levels of long chain omega-3 polyunsaturated fatty acids and prostate cancer risk: A meta-analysis. Can Urol Assoc J 2013;7:E333-43.[↩]
- Chua ME, Sio MC, Sorongon MC, Dy JS. Relationship of dietary intake of omega-3 and omega-6 Fatty acids with risk of prostate cancer development: a meta-analysis of prospective studies and review of literature. Prostate Cancer 2012;2012:826254.[↩]
- Szymanski KM, Wheeler DC, Mucci LA. Fish consumption and prostate cancer risk: a review and meta-analysis. Am J Clin Nutr 2010;92:1223-33.[↩]
- Alexander DD, Bassett JK, Weed DL, Barrett EC, Watson H, Harris W. Meta-analysis of long-chain omega-3 polyunsaturated fatty acids (LC omega-3PUFA) and prostate cancer. Nutr Cancer 2015;67:543-54.[↩]
- Noel SE, Stoneham AC, Olsen CM, Rhodes LE, Green AC. Consumption of omega-3 fatty acids and the risk of skin cancers: a systematic review and meta-analysis. Int J Cancer 2014;135:149-56.[↩]
- Ibiebele TI, Nagle CM, Bain CJ, Webb PM. Intake of omega-3 and omega-6 fatty acids and risk of ovarian cancer. Cancer Causes Control 2012;23:1775-83.[↩]
- Arem H, Neuhouser ML, Irwin ML, Cartmel B, Lu L, Risch H, et al. Omega-3 and omega-6 fatty acid intakes and endometrial cancer risk in a population-based case-control study. Eur J Nutr 2013;52:1251-60.[↩]
- Brasky TM, Rodabough RJ, Liu J, Kurta ML, Wise LA, Orchard TS, et al. Long-chain omega-3 fatty acid intake and endometrial cancer risk in the Women’s Health Initiative. Am J Clin Nutr 2015;101:824-34.[↩]
- Qin B, Xun P, He K. Fish or long-chain (n-3) PUFA intake is not associated with pancreatic cancer risk in a meta-analysis and systematic review. J Nutr 2012;142:1067-73.[↩]
- Han YJ, Li J, Huang W, Fang Y, Xiao LN, Liao ZE. Fish consumption and risk of esophageal cancer and its subtypes: a systematic review and meta-analysis of observational studies. Eur J Clin Nutr 2013;67:147-54.[↩]
- Dangour AD, Whitehouse PJ, Rafferty K, Mitchell SA, Smith L, Hawkesworth S, et al. B-vitamins and fatty acids in the prevention and treatment of Alzheimer’s disease and dementia: a systematic review. J Alzheimers Dis 2010;22:205-24. https://www.ncbi.nlm.nih.gov/pubmed/20847412?dopt=Abstract[↩]
- Sydenham E, Dangour AD, Lim WS. Omega 3 fatty acid for the prevention of cognitive decline and dementia. Cochrane Database Syst Rev 2012;6:CD005379. https://www.ncbi.nlm.nih.gov/pubmed/22696350?dopt=Abstract[↩][↩][↩]
- Chew EY, Clemons TE, Agron E, Launer LJ, Grodstein F, Bernstein PS, et al. Effect of omega-3 fatty acids, lutein/zeaxanthin, or other nutrient supplementation on cognitive function: the AREDS2 randomized clinical trial. JAMA 2015;314:791-801. https://www.ncbi.nlm.nih.gov/pubmed/26305649?dopt=Abstract[↩]
- Tully AM, Roche HM, Doyle R, Fallon C, Bruce I, Lawlor B, et al. Low serum cholesteryl ester-docosahexaenoic acid levels in Alzheimer’s disease: a case-control study. Br J Nutr 2003;89:483-9. https://www.ncbi.nlm.nih.gov/pubmed/12654166?dopt=Abstract[↩]
- Yassine HN, Feng Q, Azizkhanian I, Rawat V, Castor K, Fonteh AN, et al. Association of serum docosahexaenoic acid with cerebral amyloidosis. JAMA Neurol 2016. https://www.ncbi.nlm.nih.gov/pubmed/27532692?dopt=Abstract[↩]
- Jiao J, Li Q, Chu J, Zeng W, Yang M, Zhu S. Effect of n-3 PUFA supplementation on cognitive function throughout the life span from infancy to old age: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr 2014;100:1422-36. https://www.ncbi.nlm.nih.gov/pubmed/25411277?dopt=Abstract[↩]
- Yurko-Mauro K, Alexander DD, Van Elswyk ME. Docosahexaenoic acid and adult memory: a systematic review and meta-analysis. PLoS One 2015;10:e0120391. https://www.ncbi.nlm.nih.gov/pubmed/25786262?dopt=Abstract[↩]
- Mazereeuw G, Lanctot KL, Chau SA, Swardfager W, Herrmann N. Effects of omega-3 fatty acids on cognitive performance: a meta-analysis. Neurobiol Aging 2012;33:1482 e17-29. https://www.ncbi.nlm.nih.gov/pubmed/22305186?dopt=Abstract[↩][↩]
- SanGiovanni JP, Chew EY. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog Retin Eye Res 2005;24:87-138. https://www.ncbi.nlm.nih.gov/pubmed/15555528?dopt=Abstract[↩]
- Augood C, Chakravarthy U, Young I, Vioque J, de Jong PT, Bentham G, et al. Oily fish consumption, dietary docosahexaenoic acid and eicosapentaenoic acid intakes, and associations with neovascular age-related macular degeneration. Am J Clin Nutr 2008;88:398-406. https://www.ncbi.nlm.nih.gov/pubmed/18689376?dopt=Abstract[↩]
- Seddon JM, George S, Rosner B. Cigarette smoking, fish consumption, omega-3 fatty acid intake, and associations with age-related macular degeneration: the US Twin Study of Age-Related Macular Degeneration. Arch Ophthalmol 2006;124:995-1001. https://www.ncbi.nlm.nih.gov/pubmed/16832023?dopt=Abstract[↩]
- Christen WG, Schaumberg DA, Glynn RJ, Buring JE. Dietary omega-3 fatty acid and fish intake and incident age-related macular degeneration in women. Arch Ophthalmol 2011;129:921-9. https://www.ncbi.nlm.nih.gov/pubmed/21402976?dopt=Abstract[↩]
- Merle BM, Benlian P, Puche N, Bassols A, Delcourt C, Souied EH, et al. Circulating omega-3 Fatty acids and neovascular age-related macular degeneration. Invest Ophthalmol Vis Sci 2014;55:2010-9. https://www.ncbi.nlm.nih.gov/pubmed/24557349?dopt=Abstract[↩]
- A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 2001;119:1417-36. https://www.ncbi.nlm.nih.gov/pubmed/11594942?dopt=Abstract[↩]
- Sangiovanni JP, Agron E, Meleth AD, Reed GF, Sperduto RD, Clemons TE, et al. ω-3 Long-chain polyunsaturated fatty acid intake and 12-y incidence of neovascular age-related macular degeneration and central geographic atrophy: AREDS report 30, a prospective cohort study from the Age-Related Eye Disease Study. Am J Clin Nutr 2009;90:1601-7. https://www.ncbi.nlm.nih.gov/pubmed/19812176?dopt=Abstract[↩]
- Age-Related Eye Disease Study 2 Research G. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013;309:2005-15. https://www.ncbi.nlm.nih.gov/pubmed/23644932?dopt=Abstract[↩]
- Lawrenson JG, Evans JR. Omega 3 fatty acids for preventing or slowing the progression of age-related macular degeneration. Cochrane Database Syst Rev 2015;4:CD010015. www.ncbi.nlm.nih.gov/pubmed/25856365?dopt=Abstract[↩]
- Souied EH, Delcourt C, Querques G, Bassols A, Merle B, Zourdani A, et al. Oral docosahexaenoic acid in the prevention of exudative age-related macular degeneration: the Nutritional AMD Treatment 2 study. Ophthalmology 2013;120:1619-31. https://www.ncbi.nlm.nih.gov/pubmed/23395546?dopt=Abstract[↩]
- The Dry Eye Assessment and Management Study Research Group. Omega-3 fatty acid supplementation for treatment of dry eye disease. N Engl J Med 2018;378:1681-90. https://www.ncbi.nlm.nih.gov/pubmed/29652551[↩][↩][↩]
- Miljanović B, Trivedi KA, Dana MR, Gilbard JP, Buring JE, Schaumberg DA. Relation between dietary n-3 and n-6 fatty acids and clinically diagnosed dry eye syndrome in women. Am J Clin Nutr 2005;82:887-93. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1360504/[↩]
- Ziemanski JF, Wolters LR, Jones-Jordan L, Nichols JJ, Nichols KK. Relation between dietary essential fatty acid intake and dry eye disease and meibomian gland dysfunction in postmenopausal women. Am J Ophthalmol 2018;189:29-40. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5967412/[↩]
- Hom MM, Asbell P, Barry B. Omegas and dry eye: more knowledge, more questions. Optom Vis Sci 2015;92:948-56.[↩]
- Bhargava R, Kumar P, Kumar M, Mehra N, Mishra A. A randomized controlled trial of omega-3 fatty acids in dry eye syndrome. Int J Ophthalmol 2013;18;6:811-6.[↩]
- Epitropoulos AT, Donnenfeld ED, Shah ZA, Holland EJ, Gross M, Faulkner WJ, Matossian C, Lane SS, Toyos M, Bucci FA Jr, Perry HD. Effect of oral re-esterified omega-3 nutritional supplementation on dry eyes. Cornea 2016;35:1185-91.[↩]
- James M, Proudman S, Cleland L. Fish oil and rheumatoid arthritis: past, present and future. Proc Nutr Soc 2010;69:316-23. https://www.ncbi.nlm.nih.gov/pubmed/20509981?dopt=Abstract[↩]
- Goldberg RJ, Katz J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain 2007;129:210-23. https://www.ncbi.nlm.nih.gov/pubmed/17335973?dopt=Abstract[↩]
- Li F, Liu X, Zhang D. Fish consumption and risk of depression: a meta-analysis. J Epidemiol Community Health 2016;70:299-304. https://www.ncbi.nlm.nih.gov/pubmed/26359502?dopt=Abstract[↩]
- Appleton KM, Sallis HM, Perry R, Ness AR, Churchill R. Omega-3 fatty acids for depression in adults. Cochrane Database Syst Rev 2015;11:CD004692. https://www.ncbi.nlm.nih.gov/pubmed/26537796?dopt=Abstract[↩]
- Cochcrane Review 16 April 2008 – Omega-3 fatty acids for bipolar disorder – http://www.cochrane.org/CD005169/DEPRESSN_omega-3-fatty-acids-for-bipolar-disorder[↩]
- Cabre E, Manosa M, Gassull MA. Omega-3 fatty acids and inflammatory bowel diseases – a systematic review. Br J Nutr 2012;107 Suppl 2:S240-52. https://www.ncbi.nlm.nih.gov/pubmed/22591898?dopt=Abstract[↩]
- Lev-Tzion R, Griffiths AM, Leder O, Turner D. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev 2014;2:CD006320. https://www.ncbi.nlm.nih.gov/pubmed/24585498?dopt=Abstract[↩]
- Cochcrane Review 9 November 2011 – Omega-3 fatty acids for autism spectrum disorders – http://www.cochrane.org/CD007992/BEHAV_omega-3-fatty-acids-for-autism-spectrum-disorders-asd[↩]
- Cooper RE, Tye C, Kuntsi J, Vassos E, Asherson P. The effect of omega-3 polyunsaturated fatty acid supplementation on emotional dysregulation, oppositional behaviour and conduct problems in ADHD: A systematic review and meta-analysis. J Affect Disord 2016;190:474-82. https://www.ncbi.nlm.nih.gov/pubmed/26551407?dopt=Abstract[↩]
- Best KP, Gold M, Kennedy D, Martin J, Makrides M. Omega-3 long-chain PUFA intake during pregnancy and allergic disease outcomes in the offspring: a systematic review and meta-analysis of observational studies and randomized controlled trials. Am J Clin Nutr 2016;103:128-43. https://www.ncbi.nlm.nih.gov/pubmed/26675770?dopt=Abstract[↩]
- Gunaratne AW, Makrides M, Collins CT. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst Rev 2015;7:CD010085. https://www.ncbi.nlm.nih.gov/pubmed/26197477?dopt=Abstract[↩]
- Oliver C, Watson H. Omega-3 fatty acids for cystic fibrosis. Cochrane Database Syst Rev 2016;1:CD002201. https://www.ncbi.nlm.nih.gov/pubmed/26730723?dopt=Abstract[↩]
- Vitamin D, cod-liver oil, sunlight, and rickets: a historical perspective. Rajakumar K. Pediatrics. 2003 Aug; 112(2):e132-5. http://pediatrics.aappublications.org/content/112/2/e132.long[↩]
- Institute of Medicine. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington, DC: National Academy Press; 1997: 251–287[↩]
- Holick MF. Vitamin D: the underappreciated D-lightful hormone that is important for skeletal and cellular health. Curr Opin Endocrinol Diabetes.2002;9 :87– 98[↩]
- Vitamin D deficiency: a worldwide problem with health consequences. Holick MF, Chen TC. Am J Clin Nutr. 2008 Apr; 87(4):1080S-6S. https://www.ncbi.nlm.nih.gov/pubmed/18400738/[↩]
- Brot C, Vestergaard P, Kolthoff N, Gram J, Hermann AP, Sørensen OH. Vitamin D status and its adequacy in healthy Danish perimenopausal women: relationships to dietary intake, sun exposure and serum parathyroid hormone. Br J Nutr. 2001;86(Suppl 1):S97–S103 https://www.ncbi.nlm.nih.gov/pubmed/11520426[↩]
- Pedersen JI. Vitamin D requirement and setting recommendation levels – current Nordic view. Nutr Rev. 2008;66:S165–S169[↩]
- Doets EL, de Wit LS, Dhonukshe-Rutten RA, Cavelaars AE, Raats MM, Timotijevic L, Brzozowska A, Wijnhoven TM, Pavlovic M, Totland TH, Andersen LF, Ruprich J, Pijls LT, Ashwell M, Lambert JP, Veer P, de Groot LC. Current micronutrient recommendations in Europe: towards understanding their differences and similarities. Eur J Nutr. 2008;47(Suppl 1):17–40 https://www.ncbi.nlm.nih.gov/pubmed/18427858[↩]
- Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Food and Nutrition Board: Dietary Reference Intakes for Calcium and Vitamin D. National Academies Press, Washington D.C; 2011 https://www.ncbi.nlm.nih.gov/books/NBK56070/[↩]
- Nordic Council of Ministers. Nordic Nutrition Recommendations., Copenhagen; 2004.[↩]
- Birgisdottir BE, Brantsaeter AL, Kvalem HE, et al. Fish liver and seagull eggs, vitamin D-rich foods with a shadow: Results from the Norwegian Fish and Game Study. Mol Nutr Food Res 2012; 56: 388–398 https://www.ncbi.nlm.nih.gov/pubmed/22319024[↩]
- Alexander J, Frøyland L, Hemre G-I, et al. A comprehensive assessment of fish and other seafood in the Norwegian diet. The Norwegian Scientific Committee for Food Safety (VKM), https://www.vkm.no/english/[↩]
- Vieth R. Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. Am J Clin Nutr. 1999;69:842–856 https://www.ncbi.nlm.nih.gov/pubmed/10232622[↩]
- Björkman M, Sorva A, Tilvis R. Responses of parathyroid hormone to vitamin D supplementation: a systematic review of clinical trials. Arch Gerontol Geriatr. 2009;48:160–166. doi: 10.1016/j.archger.2007.12.005 https://www.ncbi.nlm.nih.gov/pubmed/18243368[↩]
- Barnes MS, Robson PJ, Bonham MP, Strain JJ, Wallace JM. Effect of vitamin D supplementation on vitamin D status and bone turnover markers in young adults. Eur J Clin Nutr. 2006;60:727–733. doi: 10.1038/sj.ejcn.1602374[↩]
- Seamans KM, Hill TR, Wallace JM, Horigan G, Lucey AJ, Barnes MS, Taylor N, Bonham MP, Muldowney S, Duffy EM, Strain JJ, Kiely M, Cashman KD. Cholecalciferol supplementation throughout winter does not affect markers of bone turnover in healthy young and elderly adults. J Nutr. 2010;140:454–460. doi: 10.3945/jn.109.113480[↩]
- Pignotti GA, Genaro PS, Pinheiro MM, Szejnfeld VL, Martini LA. Is a lower dose of vitamin D supplementation enough to increase 25(OH)D status in a sunny country? Eur J Nutr. 2010;49:277–283. doi: 10.1007/s00394-009-0084-0[↩]
- Wicherts IS, van Schoor NM, Boeke AJ, Visser M, Deeg DJ, Smit J, Knol DL, Lips P. Vitamin D status predicts physical performance and its decline in older persons. J Clin Endocrinol Metab. 2007;92:2058–2065. doi: 10.1210/jc.2006-1525[↩]
- Meyer HE, Brunvand L, Brustad M, Holvik K, Johansson L, Paulsen JE. Tiltak for å sikre en god vitamin D-status i befolkningen (Measures to ensure a good vitamin D status in the population) Norwegian National Nutrition Council, Oslo; 2006.[↩]
- Bischoff-Ferrari H. Vitamin D: What is an adequate vitamin D level and how much supplementation is necessary? Best Pract Res Clin Rheumatol. 2009;23:789–795. doi: 10.1016/j.berh.2009.09.005[↩]
- Holvik K, Madar AA, Meyer HE, Lofthus CM, Stene LC. Changes in the vitamin D endocrine system and bone turnover after oral vitamin D3 supplementation in healthy adults: results of a randomised trial. BMC Endocrine Disorders. 2012;12:7. doi:10.1186/1472-6823-12-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3406987/[↩][↩][↩]
- A randomised comparison of increase in serum 25-hydroxyvitamin D concentration after 4 weeks of daily oral intake of 10 microgram cholecalciferol from multivitamin tablets or fish oil capsules in healthy young adults. Holvik K, Madar AA, Meyer HE, Lofthus CM, Stene LC. Br J Nutr. 2007 Sep; 98(3):620-5. https://www.cambridge.org/core/journals/british-journal-of-nutrition/article/randomised-comparison-of-increase-in-serum-25hydroxyvitamin-d-concentration-after-4-weeks-of-daily-oral-intake-of-10-g-cholecalciferol-from-multivitamin-tablets-or-fish-oil-capsules-in-healthy-young-adults/36965B7E3DC80ADB1D505F46E4AC188A/core-reader[↩]
- Eysteinsdottir T, Halldorsson TI, Thorsdottir I, et al. Cod liver oil consumption at different periods of life and bone mineral density in old age. The British journal of nutrition. 2015;114(2):248-256. doi:10.1017/S0007114515001397 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5490077[↩][↩]
- Poulsen RC, Moughan PJ, Kruger MC. Long-chain polyunsaturated fatty acids and the regulation of bone metabolism. Exp Biol Med. 2007;232:1275–1288. doi: 10.3181/0704-MR-100[↩]
- Sun D, Krishnan A, Zaman K, Lawrence R, Bhattacharya A, Fernandes G. Dietary n-3 fatty acids decrease osteoclastogenesis and loss of bone mass in ovariectomized mice. J Bone Miner Res. 2003;18:1206–1216. doi: 10.1359/jbmr.2003.18.7.1206[↩]



{kind=link}