Contents
What are polyps in the colon
Colon polyps are small benign growths of tissue inside the colon or large intestine or rectum. Benign colon polyps means they are not a cancer and do not spread. You may have one or many polyps. They become more common with age. Some polyps are mushroom-shaped protrusions on the end of a stalk. Others appear as bumps that lie flat against the intestinal wall.
Colon polyps are very common, affecting around 1 in 4 people at some point in their lives. Certain people are more likely than others. Colon polyps are slightly more common in men than women.
You may have a greater chance of getting polyps if you:
- Are over age 50
- Have had polyps before
- Have a family member with polyps
- Have a family history of colon cancer
Most colon polyps do not cause symptoms. If you have symptoms, they may include blood on your underwear or on toilet paper after a bowel movement, blood in your stool, or constipation or diarrhea lasting more than a week.
Some people develop just one polyp, while others may have a few.
There are several types of polyps. Most colon polyps are noncancerous (benign), but one type, the adenomatous polyp, is associated with changes (called mutations) in the DNA of the lining of the colon. These mutations can progress into colon cancer. The larger the polyp, the greater the chance that it contains cancerous cells, which is why it is important to have them removed.
See your doctor if you experience:
- Cramping or abdominal (belly) pain
- Dark stools, or blood in the stool
- A change in bowel habits, such as diarrhea, constipation, or narrowing of the stool, that lasts for more than a few days
- A feeling that you need to have a bowel movement that is not relieved by doing so
- Rectal bleeding
- Weakness and fatigue
- Unintended weight loss
Many of these symptoms can be caused by conditions other than colon cancer, such as infection, hemorrhoids, or irritable bowel syndrome. Still, if you have any of these problems, it’s important to see your doctor right away so the cause can be found and treated, if needed.
You should be screened regularly for polyps if:
- You’re age 50 or older.
- You have risk factors, such as a family history of colon cancer. Some high-risk individuals should begin regular screening much earlier than age 50.
Colon cancer risk
Colon polyps don’t usually turn into cancer. But if some types of polyps (called adenomas) are not removed, there’s a chance they may eventually become cancerous. Doctors believe that most colon cancers develop from adenoma polyps.
However, very few colon polyps will turn into cancer, and it takes many years for this to happen.
Because of the risk of colon polyps developing into cancer, your doctor will always recommend getting colon polyps treated.
Polyps bigger than 1 centimeter (cm) have a higher cancer risk than polyps smaller than 1 centimeter.
Risk factors include:
- Age
- Family history of colon cancer or polyps
- A type of polyp called villous adenoma
A small number of people with polyps may also be linked to some inherited disorders, including:
- Familial adenomatous polyposis (FAP)
- Gardner syndrome (a type of FAP)
- Juvenile polyposis (disease that causes many benign growths in the intestine, usually before 20 years old)
- Lynch syndrome (HNPCC, a disease that raises the chance of many types of cancer, including in the intestine)
- Peutz-Jeghers syndrome (disease that causes intestinal polyps, usually in the small intestine and usually benign)
Types of colon polyps
There are two main categories of polyps, non-neoplastic and precancerous colon polyps.
Non-neoplastic polyps include hyperplastic polyps, inflammatory polyps and hamartomatous polyps. Non-neoplastic polyps typically do not become cancerous.
Precancerous colon polyps also called neoplastic polyps include adenomas and serrated types. Most colon polyps are adenomas. Serrated polyps may become cancerous, depending on their size and location in the colon. In general, the larger a polyp, the greater the risk of cancer, especially with neoplastic polyps.
Inflammatory polyps may be seen with ulcerative colitis or Crohn’s disease of the colon. Although the polyps themselves are not a significant threat, having ulcerative colitis or Crohn’s disease of the colon increases your overall risk of colon cancer.
Precancerous colon polyps
Adenomatous polyps are a common type. They are gland-like growths that develop on the mucous membrane that lines your colon, although it is different in several important ways when it is looked at under the microscope. Adenomatous polyps are also called adenomas and are most often one of the following:
- Tubular polyp, which protrudes out in the lumen (open space) of the colon
- Villous adenoma, which is sometimes flat and spreading, and is more likely to become a cancer
Adenomas can have several different growth patterns that can be seen under the microscope by the pathologist. There are 2 major growth patterns: tubular and villous. Many adenomas have a mixture of both growth patterns, and are called tubulovillous adenomas. Most adenomas that are small (less than ½ inch) have a tubular growth pattern. Larger adenomas may have a villous growth pattern. Larger adenomas more often have cancers developing in them. Adenomas with a villous growth pattern are also more likely to have cancers develop in them.
The growth pattern is only important because it helps determine when you will need your next colonoscopy to make sure you don’t develop colon cancer in the future.
When adenomas become cancerous, they are known as adenocarcinomas. Adenocarcinomas are cancers that originate in glandular tissue cells. Adenocarcinoma is the most common type of colorectal cancer.
Sessile serrated adenoma (adenomatous polyp) or traditional serrated adenoma (adenomatous polyp)
Colon polyps that tend to grow as slightly flattened, broad-based polyps are referred to as sessile.
Serrated colon polyps (serrated adenomas) have a saw-tooth appearance under the microscope. There are 2 types, which look a little different under the microscope:
- Sessile serrated adenomas (also called sessile serrated polyps)
- Traditional serrated adenomas
These types of polyps are not cancer, but they are pre-cancerous (meaning that they can turn into cancers). Someone who has had one of these types of polyps has an increased risk of later developing cancer of the colon. Hence, both of these types of colon polyp need to be removed from your colon. However, most patients with these colon polyps, never develop colon cancer.
If your adenoma was biopsied but not completely removed, you will need to talk to your doctor about what other treatment you’ll need. Most of the time, adenomas are removed during a colonoscopy. Sometimes, though, the adenoma may be too large to remove during colonoscopy. In such cases you may need surgery to have the adenoma removed.
If you’ve had an adenoma, you will need to have another colonoscopy to make sure that you don’t develop any more adenomas. When your next colonoscopy should be scheduled depends on a number of things, like how many adenomas were found, if any were villous, and if any had high-grade dysplasia. The timing of your next colonoscopy should be discussed with your treating doctor, as he or she knows the details of your specific case.
Non-neoplastic colon polyps
Non-neoplastic polyps include hyperplastic colon polyps, inflammatory polyps and hamartomatous polyps. Non-neoplastic polyps typically do not become cancerous and are not a cause for concern.
Figure 1. Colon polyps

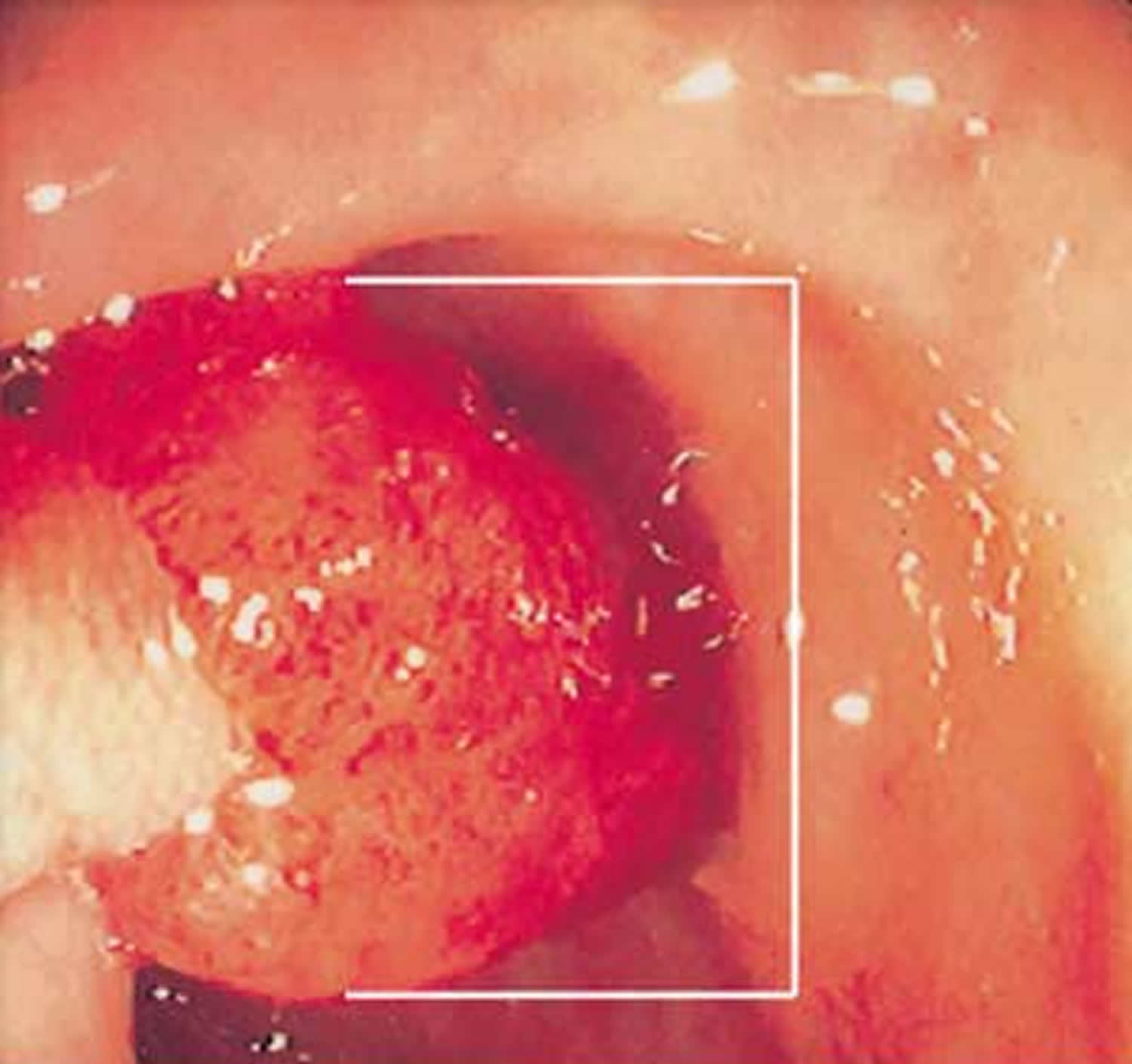
Figure 2. Large colon polyp – large polyps are 10 millimeters (mm) or larger in diameter
Colon polyps outlook (prognosis)
Outlook is excellent if the colon polyps are removed. Polyps that are not removed can develop into cancer over time..
Colorectal Cancer Early Detection
Because colon cancer often doesn’t cause symptoms until it is advanced, the American Cancer Society recommends regular colon cancer screening for most people starting at age 50. People with a family history of the disease or who have certain other risk factors should talk with their doctor about beginning screening at a younger age. Several different tests can be used to screen for colon cancer. Talk with your doctor to find out which tests might be right for you.
When colon cancer is found early, before it has spread, the 5-year relative survival rate is 90%. This means 9 out of 10 people with early-stage cancer survive at least 5 years. But if the cancer has had a chance to spread outside the colon, survival rates are lower.
People at average risk
The American Cancer Society believes that preventing colorectal cancer (and not just finding it early) should be a major reason for getting tested. Having colon polyps found and removed keeps some people from getting colorectal cancer. You are encouraged to have tests that have the best chance of finding both colon polyps and colon cancer if these tests are available to you and you are willing to have them. But the most important thing is to get tested, no matter which test you choose.
Starting at age 50, men and women at average risk for developing colorectal cancer should use one of the screening tests below:
Tests that find colon polyps and colon cancer
- Colonoscopy every 10 years
- CT colonography (virtual colonoscopy) every 5 years*
- Flexible sigmoidoscopy every 5 years*
- Double-contrast barium enema every 5 years*
Tests that mainly find colon cancer
- Fecal immunochemical test (FIT) every year*,**
- Guaiac-based fecal occult blood test (gFOBT) every year*,**
- Stool DNA test every 3 years*
*Colonoscopy should be done if test results are positive.
** Highly sensitive versions of these tests should be used with the take-home multiple sample method. A gFOBT or FIT done during a digital rectal exam in the doctor’s office is not enough for screening.
People at increased or high risk
If you are at an increased or high risk of colorectal cancer, you might need to start colorectal cancer screening before age 50 and/or be screened more often. The following conditions make your risk higher than average:
- A personal history of colorectal cancer or adenomatous polyps
- A personal history of inflammatory bowel disease (ulcerative colitis or Crohn’s disease)
- A strong family history of colorectal cancer or polyps
- A known family history of a hereditary colorectal cancer syndrome such as familial adenomatous polyposis (FAP) or Lynch syndrome (hereditary non-polyposis colon cancer or HNPCC)
The table below suggests screening guidelines for people with increased or high risk of colorectal cancer based on specific risk factors. Some people may have more than one risk factor. Refer to the table below and discuss these recommendations with your health care provider. Your provider can suggest the best screening option for you, as well as any changes in the schedule based on your individual risk.
Table 1. American Cancer Society Guidelines on Screening and Surveillance for the Early Detection of Colorectal Adenomas and Cancer in People at Increased Risk or High Risk
| INCREASED RISK – People who have a history of polyps on prior colonoscopy | |||
| Risk category | When to test | Recommended test(s) | Comment |
| People with small rectal hyperplastic polyps | Same age as those at average risk | Colonoscopy, or other screening options at same intervals as for those at average risk | Those with hyperplastic polyposis syndrome are at increased risk for adenomatous polyps and cancer and should have more intensive follow-up. |
| People with 1 or 2 small (no more than 1 cm) tubular adenomas with low-grade dysplasia | 5 to 10 years after the polyps are removed | Colonoscopy | Time between tests should be based on other factors such as prior colonoscopy findings, family history, and patient and doctor preferences. |
| People with 3 to 10 adenomas, or a large (at least 1 cm) adenoma, or any adenomas with high-grade dysplasia or villous features | 3 years after the polyps are removed | Colonoscopy | Adenomas must have been completely removed. If colonoscopy is normal or shows only 1 or 2 small tubular adenomas with low-grade dysplasia, future colonoscopies can be done every 5 years. |
| People with more than 10 adenomas on a single exam | Within 3 years after the polyps are removed | Colonoscopy | Doctor should consider possible genetic syndrome (such as FAP or Lynch syndrome). |
| People with sessile adenomas that are removed in pieces | 2 to 6 months after adenoma removal | Colonoscopy | If entire adenoma has been removed, further testing should be based on doctor’s judgment. |
| INCREASED RISK – People who have had colorectal cancer | |||
| Risk category | When to test | Recommended test(s) | Comment |
| People diagnosed with colon or rectal cancer | At time of colorectal surgery, or can be 3 to 6 months later if person doesn’t have cancer spread that can’t be removed | Colonoscopy to look at the entire colon and remove all polyps | If the tumor presses on the colon/rectum and prevents colonoscopy, CT colonoscopy (with IV contrast) or DCBE may be done to look at the rest of the colon. |
| People who have had colon or rectal cancer removed by surgery | Within 1 year after cancer resection (or 1 year after colonoscopy to make sure the rest of the colon/rectum was clear) | Colonoscopy | If normal, repeat in 3 years. If normal then, repeat test every 5 years. Time between tests may be shorter if polyps are found or there’s reason to suspect Lynch syndrome. After low anterior resection for rectal cancer, exams of the rectum may be done every 3 to 6 months for the first 2 to 3 years to look for signs of recurrence. |
| INCREASED RISK – People with a family history | |||
| Risk category | Age to start testing | Recommended test(s) | Comment |
| Colorectal cancer or adenomatous polyps in any first-degree relative before age 60, or in 2 or more first-degree relatives at any age (if not a hereditary syndrome). | Age 40, or 10 years before the youngest case in the immediate family, whichever is earlier | Colonoscopy | Every 5 years. |
| Colorectal cancer or adenomatous polyps in any first-degree relative aged 60 or older, or in at least 2 second-degree relatives at any age | Age 40 | Same test options as for those at average risk. | Same test intervals as for those at average risk. |
| HIGH RISK | |||
| Risk category | Age to start testing | Recommended test(s) | Comment |
| Familial adenomatous polyposis (FAP) diagnosed by genetic testing, or suspected FAP without genetic testing | Age 10 to 12 | Yearly flexible sigmoidoscopy to look for signs of FAP; counseling to consider genetic testing if it hasn’t been done | If genetic test is positive, removal of colon (colectomy) should be considered. |
| Lynch syndrome (hereditary non-polyposis colon cancer or HNPCC), or at increased risk of Lynch syndrome based on family history without genetic testing | Age 20 to 25 years, or 10 years before the youngest case in the immediate family | Colonoscopy every 1 to 2 years; counseling to consider genetic testing if it hasn’t been done | Genetic testing should be offered to first-degree relatives of people found to have Lynch syndrome mutations by genetic tests. It should also be offered if 1 of the first 3 of the modified Bethesda criteria is met.* |
| Inflammatory bowel disease: -Chronic ulcerative colitis -Crohn’s disease | Cancer risk begins to be significant 8 years after the onset of pancolitis (involvement of entire large intestine), or 12-15 years after the onset of left-sided colitis | Colonoscopy every 1 to 2 years with biopsies for dysplasia | These people are best referred to a center with experience in the surveillance and management of inflammatory bowel disease. |
Colon polyps causes
Doctors don’t know the exact cause of colon polyps. Mutations in certain genes can cause cells to continue dividing even when new cells aren’t needed. These extra cells then form into a bump, which is the polyp. In the colon and rectum, this unregulated growth can cause polyps to form. Polyps can develop anywhere in your large intestine.
Risk factors for developing colon polyps
Factors that may contribute to the formation of colon polyps or cancer include:
- Age. Most people with colon polyps are 50 or older.
- Inflammatory intestinal conditions, such as ulcerative colitis and Crohn’s disease.
- Family history. You’re more likely to develop colon polyps or cancer if you have a parent, sibling or child with them. If many family members have them, your risk is even greater. In some people, this connection isn’t hereditary.
- Tobacco and alcohol use.
- Obesity and lack of exercise.
- Race. African-Americans are at higher risk of developing colon cancer.
- Type 2 diabetes that isn’t well-controlled.
Hereditary polyp disorders
Rarely, people inherit genetic mutations that cause colon polyps to form. If you have one of these genetic mutations, you are at much higher risk of developing colorectal cancer. Screening and early detection can help prevent the development or spread of these cancers.
Hereditary disorders that cause colon polyps include:
- Lynch syndrome, also called hereditary nonpolyposis colorectal cancer. People with Lynch syndrome tend to develop relatively few colon polyps, but those polyps can quickly become malignant. Lynch syndrome is the most common form of inherited colon cancer and is also associated with tumors in the breast, stomach, small intestine, urinary tract and ovaries.
- Familial adenomatous polyposis (FAP), a rare disorder that causes hundreds or even thousands of polyps to develop in the lining of your colon beginning during your teenage years. If the polyps aren’t treated, your risk of developing colon cancer is nearly 100 percent, usually before age 40. Genetic testing can help determine your risk of FAP.
- Gardner’s syndrome, a variant of FAP that causes polyps to develop throughout your colon and small intestine. You may also develop noncancerous tumors in other parts of your body, including your skin, bones and abdomen.
- MYH-associated polyposis (MAP), a condition similar to FAP that is caused by mutations in the MYH gene. People with MAP often develop multiple adenomatous polyps and colon cancer at a young age. Genetic testing can help determine your risk of MAP.
- Peutz-Jeghers syndrome, a condition that usually begins with freckles developing all over the body, including the lips, gums and feet. Then noncancerous polyps develop throughout the intestines. These polyps may become malignant, so people with this condition have an increased risk of colon cancer.
- Serrated polyposis syndrome, a condition that leads to multiple serrated adenomatous polyps in the upper part of the colon. These polyps may become malignant.
How to prevent colon polyps
You can greatly reduce your risk of colon polyps and colorectal cancer by having regular screenings. Certain lifestyle changes also can help:
- Adopt healthy habits. Include plenty of fruits, vegetables and whole grains in your diet and reduce your fat intake. Limit alcohol consumption and quit tobacco. Stay physically active and maintain a healthy body weight.
- Talk to your doctor about calcium and vitamin D. Studies have shown that increasing your consumption of calcium may help prevent recurrence of colon adenomas. But it isn’t clear whether calcium has any protective benefits against colon cancer. Other studies have shown that vitamin D may have a protective effect against colorectal cancer.
- Consider your options if you’re at high risk. If you have a family history of colon polyps, consider having genetic counseling. If you’ve been diagnosed with a hereditary disorder that causes colon polyps, you’ll need regular colonoscopies starting in young adulthood.
Your provider can order a colonoscopy or other screening tests (see the American Cancer Society Guidelines on Screening and Surveillance for the Early Detection of Colorectal Adenomas and Cancer above) :
- These tests help prevent colon cancer by finding and removing polyps before they become cancer. This may reduce the chance of developing colon cancer, or at least help catch it in its most treatable stage.
- Most people should begin these tests at age 50. Those with a family history of colon cancer or colon polyps may need to be screened at an earlier age or more often.
Taking aspirin, naproxen, ibuprofen, or similar medicines may help reduce the risk for new polyps. Be aware that these medicines can have serious side effects if taken for a long time. Side effects include bleeding in the stomach or colon and heart disease. Talk with your provider before taking these medicines.
Colon polyps signs and symptoms
Colon polyps don’t usually cause any symptoms, so most people with polyps won’t know they have them. They are often picked up during screening for colon cancer.
But some people with colon polyps experience:
- Rectal bleeding. This can be a sign of colon polyps or cancer or other conditions, such as hemorrhoids or minor tears in your anus.
- Change in stool color. Blood can show up as red streaks in your stool or make stool appear black. A change in color may also be caused by foods, medications and supplements.
- Change in bowel habits. Constipation or diarrhea that lasts longer than a week may indicate the presence of a large colon polyp. But a number of other conditions can also cause changes in bowel habits.
- Pain. A large colon polyp can partially obstruct your bowel, leading to crampy abdominal pain.
- Iron deficiency anemia. Bleeding from polyps can occur slowly over time, without visible blood in your stool. Chronic bleeding robs your body of the iron needed to produce the substance that allows red blood cells to carry oxygen to your body (hemoglobin). The result is iron deficiency anemia, which can make you feel tired and short of breath.
Colon polyps diagnosis
Colon polyps are usually found when your colon is being looked at for another reason or during screening for colon cancer.
Screening tests play a key role in detecting polyps before they become cancerous. These tests can also help find colorectal cancer in its early stages, when you have a good chance of recovery.
Screening methods include:
- Colonoscopy, the most sensitive test for colorectal polyps and cancer. If polyps are found, your doctor may remove them immediately or take tissue samples (biopsies) for analysis.
- Virtual colonoscopy (CT colonography), a minimally invasive test that uses a CT scan to view your colon. Virtual colonoscopy requires the same bowel preparation as a colonoscopy. If a polyp is found, you’ll need a colonoscopy to have it removed.
- Flexible sigmoidoscopy, in which a slender, lighted tube is inserted in your rectum to examine it and the last third of your colon (sigmoid) and rectum. If a polyp is found, you’ll need a colonoscopy to have it removed.
- Stool-based tests. This type of test works by checking for the presence of blood in the stool or assessing your stool DNA. If your stool test is positive you will need a colonoscopy.
Monitoring colon polyps
Some people with a certain type of colon polyp may be at risk of it coming back in the future (recurring).
This is uncommon, but means you’ll need examining (by colonoscopy) at regular intervals of around three to five years. This is to catch any further polyps that may develop and potentially turn into colon cancer.
Colon polyps treatment
Colorectal polyps should be removed because some can develop into cancer.
There are several methods for treating colon polyps, but the most common procedure involves physically removing the colon polyp using a wire loop. This happens during a procedure called a colonoscopy.
The colonoscopy involves passing a flexible tube called a colonoscope through your bottom and up into your colon. The colonoscope has a wire attached to it with an electric current through it. This wire is used to either burn off (cauterize) or cut off (snare) the polyp. Both of these methods are painless.
In rare cases, colon polyps may need to be treated by surgically removing part of the colon (a colectomy). This is usually only done when the colon polyp has some cell changes, if it is particularly large, or if there are a lot of colon polyps. This is surgery to remove part of the colon that has the polyps.
After the polyp or polyps have been removed, they are sent to specialists in a laboratory, who will inform your consultant if:
- the polyp has been completely removed
- there is any risk of it regrowing
- there is any cancerous change in the polyp
If there is a cancerous change in the colon polyp, you may need further treatment (depending on the degree and extent of change). Your specialist will be able to advise you on this.
Follow-up care
If you have had an adenomatous polyp or a serrated polyp, you are at increased risk of colon cancer. The level of risk depends on the size, number and characteristics of the adenomatous polyps that were removed.
You’ll need follow-up screenings for polyps. Your doctor is likely to recommend a colonoscopy:
- In five to 10 years if you had only one or two small adenomas
- In three years if you had more than two adenomas, adenomas measuring 0.4 inches (about 1 centimeter) or larger, or certain adenomas
- Within three years if you had more than 10 adenomas
- Within six months if you had a very large adenoma or an adenoma that had to be removed in pieces
It’s important to fully prepare your colon before a colonoscopy. If stool remains in the colon and obstructs your doctor’s view of the colon wall, you will likely need a follow-up colonoscopy sooner than the guidelines specify.





{kind=link}