Contents
- What is a colostomy
- Why is colostomy performed?
- Types of Colostomies
- Large intestine
- How a colostomy surgery is carried out
- Recovering from a colostomy surgery
- Living with a colostomy
- What is a colostomy bag
- How to change a colostomy bag
- Colostomy care
- Colostomy irrigation for descending and sigmoid colostomies only
- Colostomy diet
- Colostomy possible complications
- Colostomy reversal
- Ileostomy vs Colostomy
What is a colostomy
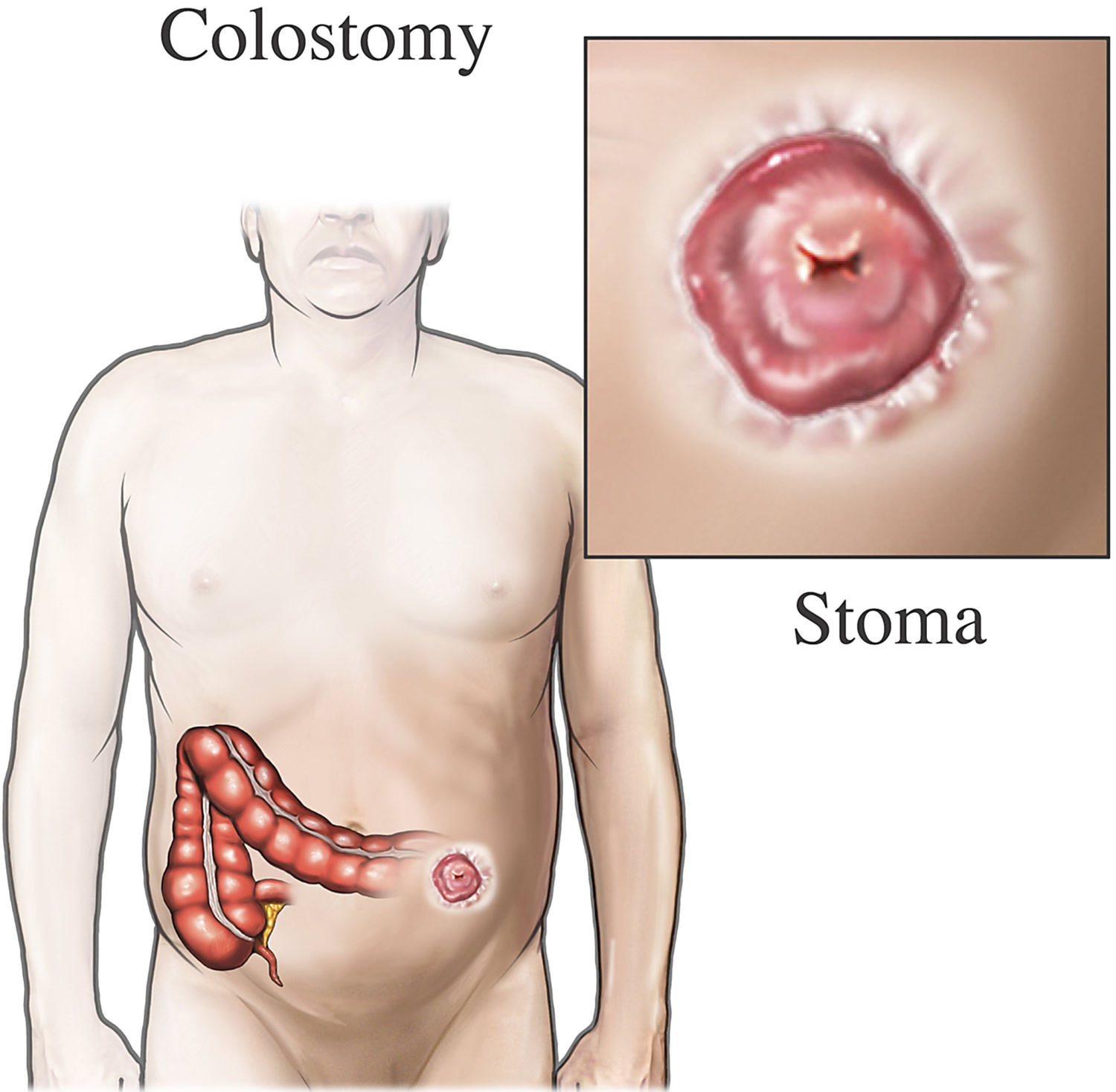
Colostomy is a surgical procedure that brings one end of the large intestine (the colon) out through an opening on the surface of the body (stoma) made in the abdominal wall (see Figures 1 and 2). A stoma (colostomy hole) is an artificial opening on the outside of the tummy or abdomen, where waste (stools or feces) from the colon is then collected using a small bag called a colostomy bag (stoma pouch) that is attached to the abdomen wall (see Figures 2 and 3). A colostomy can be permanent or temporary.
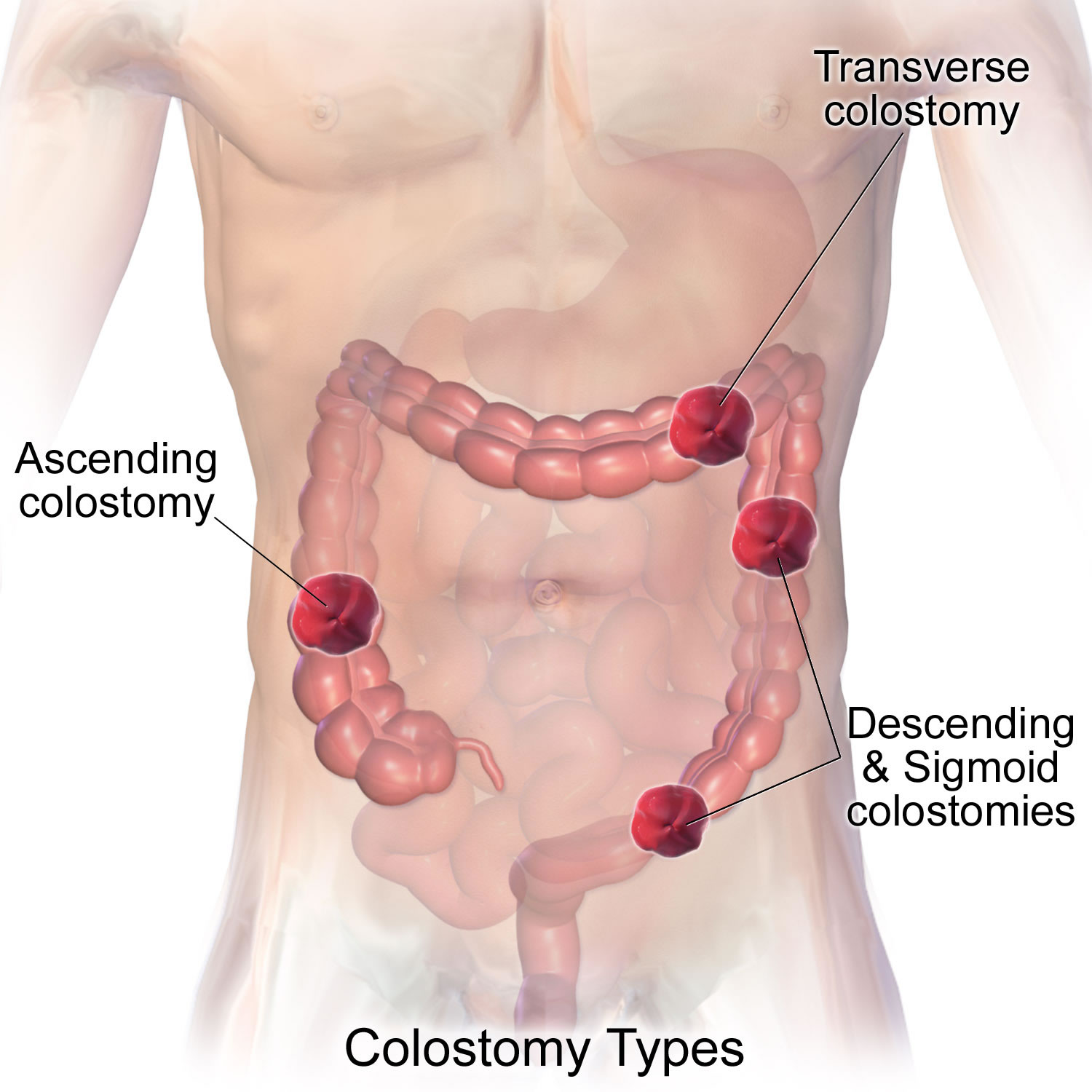
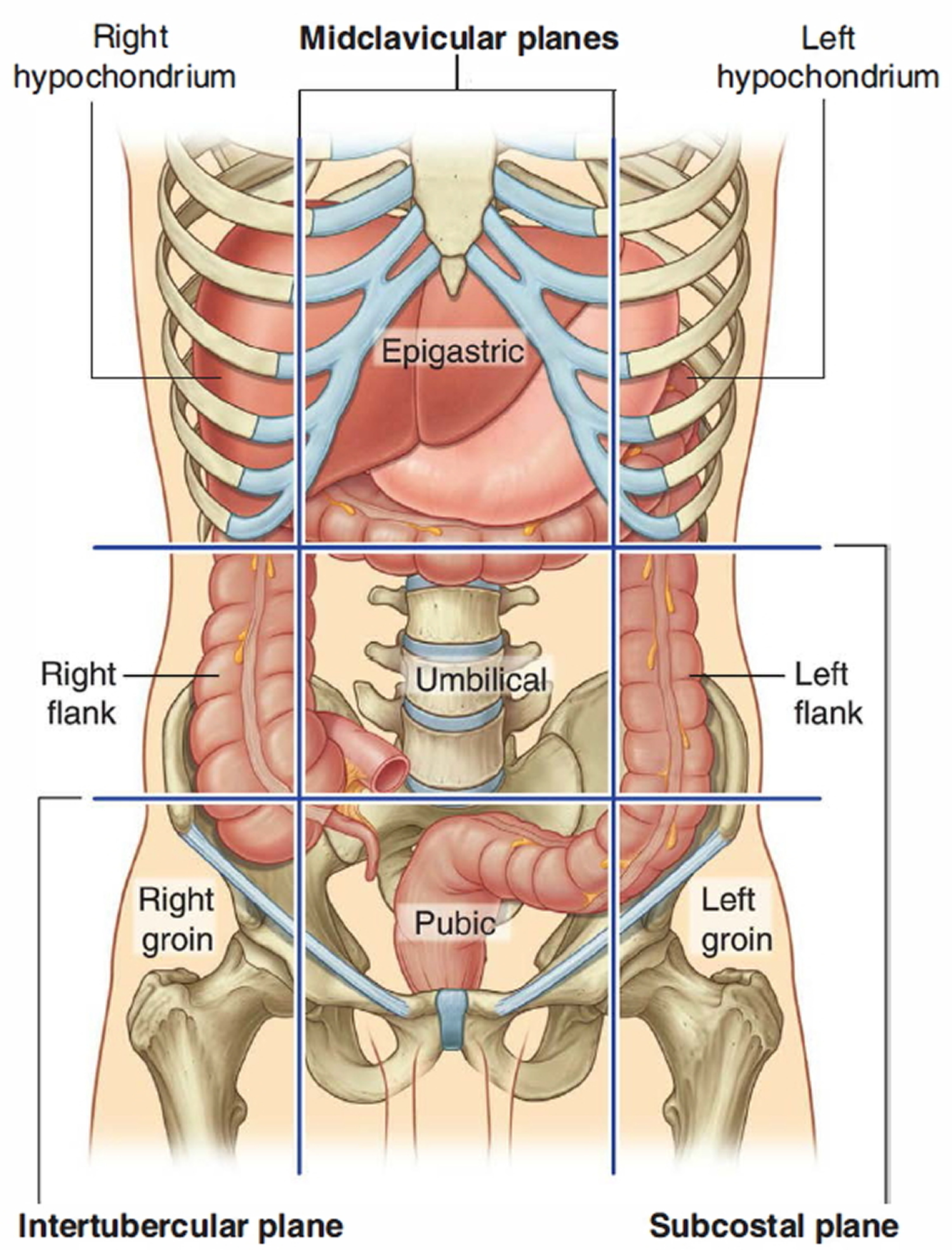
Where the stoma will be on the abdomen depends on which part of the colon is used to make it. Some colostomies are large, some small; some are on the left side of the abdomen, some are on the right, others may be in the middle (see Figure 4 below).
A colostomy is often used after a section of the colon has been removed and the bowel can’t be joined back together.
This may be temporary and followed by another operation to reverse the colostomy at a later date, or it may be permanent.
The colostomy stoma
The position of the colostomy stoma (colostomy hole) will depend on the section of your colon that’s diverted, but it’s usually on the left-hand side of your tummy, below your waist.
If the operation is planned in advance, you’ll meet a specialist stoma nurse to discuss the positioning of the stoma.
The stoma will be red and moist and may bleed slightly, particularly in the beginning – this is normal. It shouldn’t be painful as it doesn’t have a nerve supply.
Stomas can vary in shape and size – some are fairly flat, while others protrude slightly.
Why is colostomy performed?
The colon is the first 1 to 1.5 metres of your large intestine. It absorbs water and nutrients from your stools (feces) and passes the remaining waste to the rectum.
If your colon, rectum or anus do not work properly, surgery can create another way to get rid of waste from your body. A colostomy allows feces and gas to leave your body via the stoma.
Colostomy surgery is done for many different diseases and problems. Some colostomies are done because of cancer; others are not. For instance, a child may need one because of a birth defect. Sometimes a colostomy is only needed for a short time (temporary), but for some people it’s life-long (permanent).
For the thousands of people who have serious digestive diseases, a colostomy can be the start of a new and healthier life. If you’ve had a chronic (long-term) problem or a life-threatening disease like colorectal cancer, you can look forward to feeling better after you recover from colostomy surgery. You can also look forward to returning to most, if not all of the activities you enjoyed in the past.
A colostomy may be carried out if you have:
- an infection in your abdomen, such as perforated diverticulitis or an abscess
- an injury to the colon or rectum
- a blockage of the large bowel (intestinal obstruction)
- rectal or colon cancer
- wounds or fistulas in the perineum (the area between the anus and vulva in women) or the anus and scrotum in men
- Crohn’s disease
- diverticulitis
- anal cancer
- vaginal cancer or cervical cancer
- bowel incontinence
- Hirschsprung’s disease
Figure 1. Colostomy – Note: Colon cancer surgery with colostomy. Part of the colon containing the cancer and nearby healthy tissue is removed, a stoma is created, and a colostomy bag is attached to the stoma. 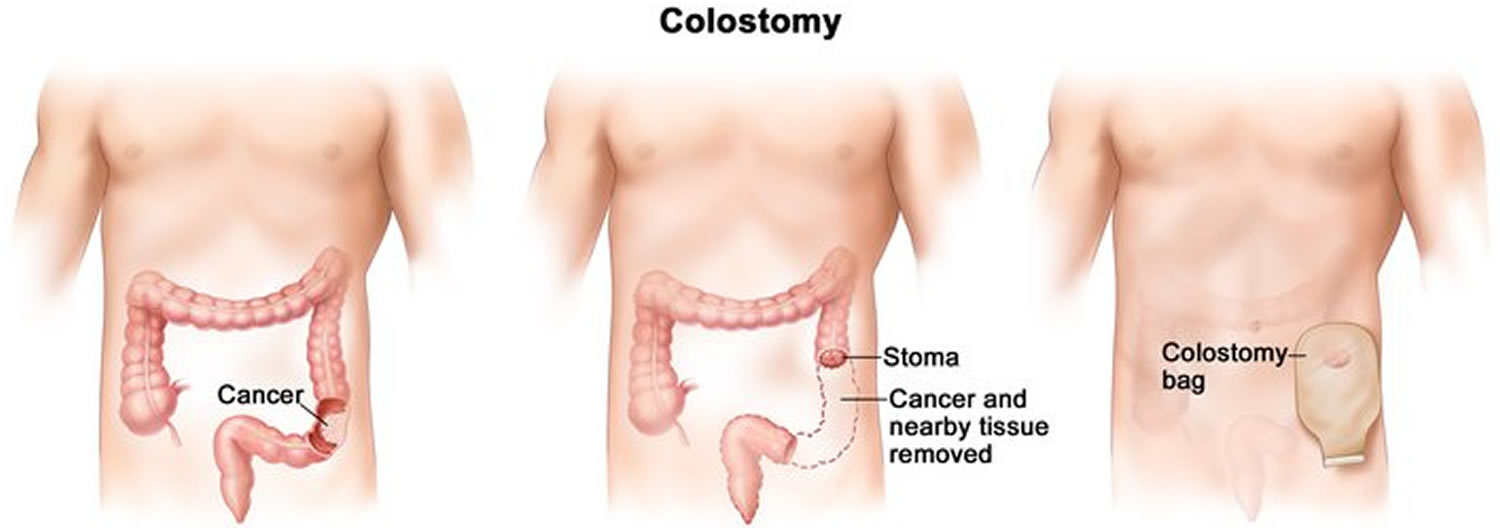
Figure 2. Colostomy stoma (end colostomy)
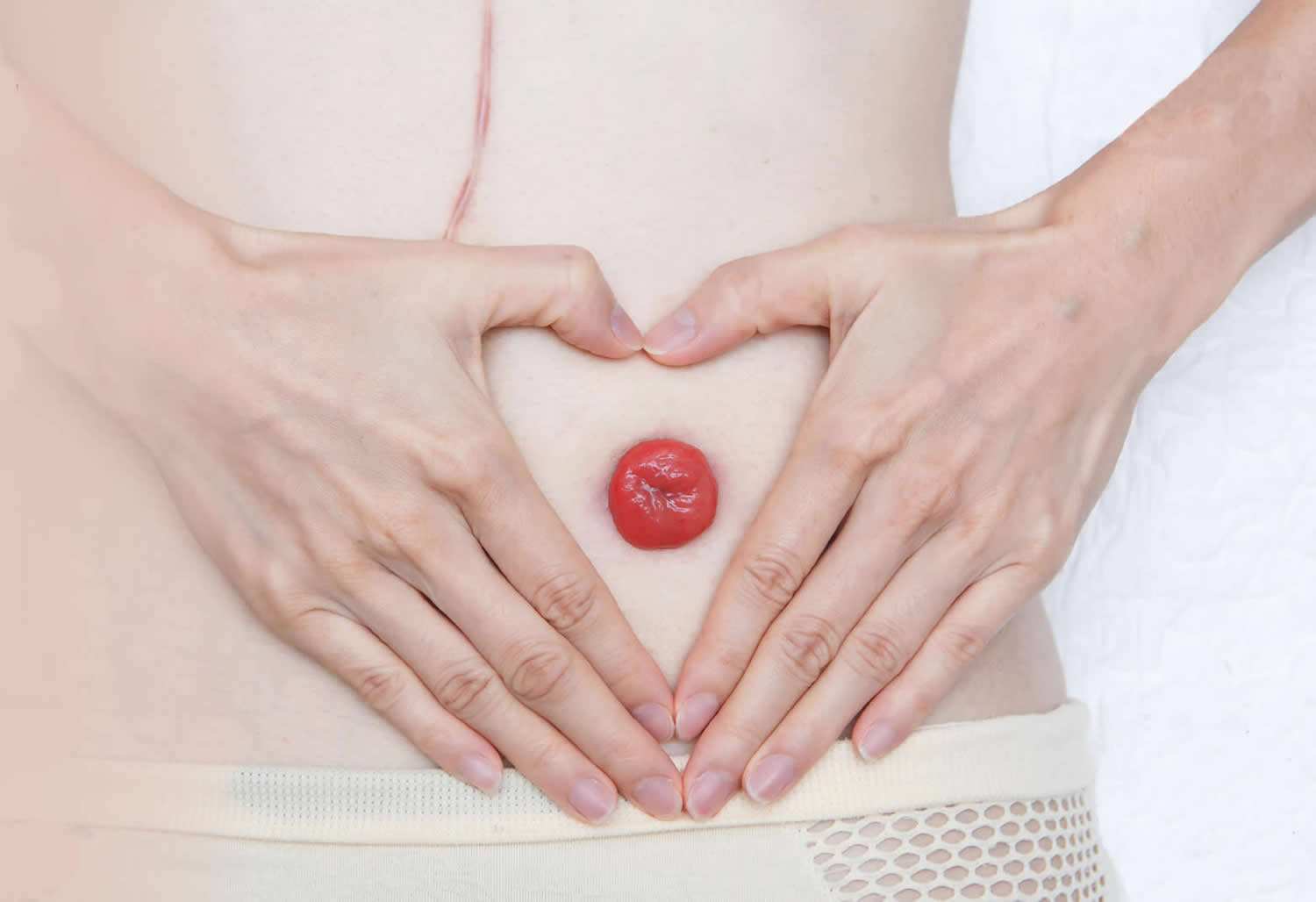
Figure 3. Colostomy bag
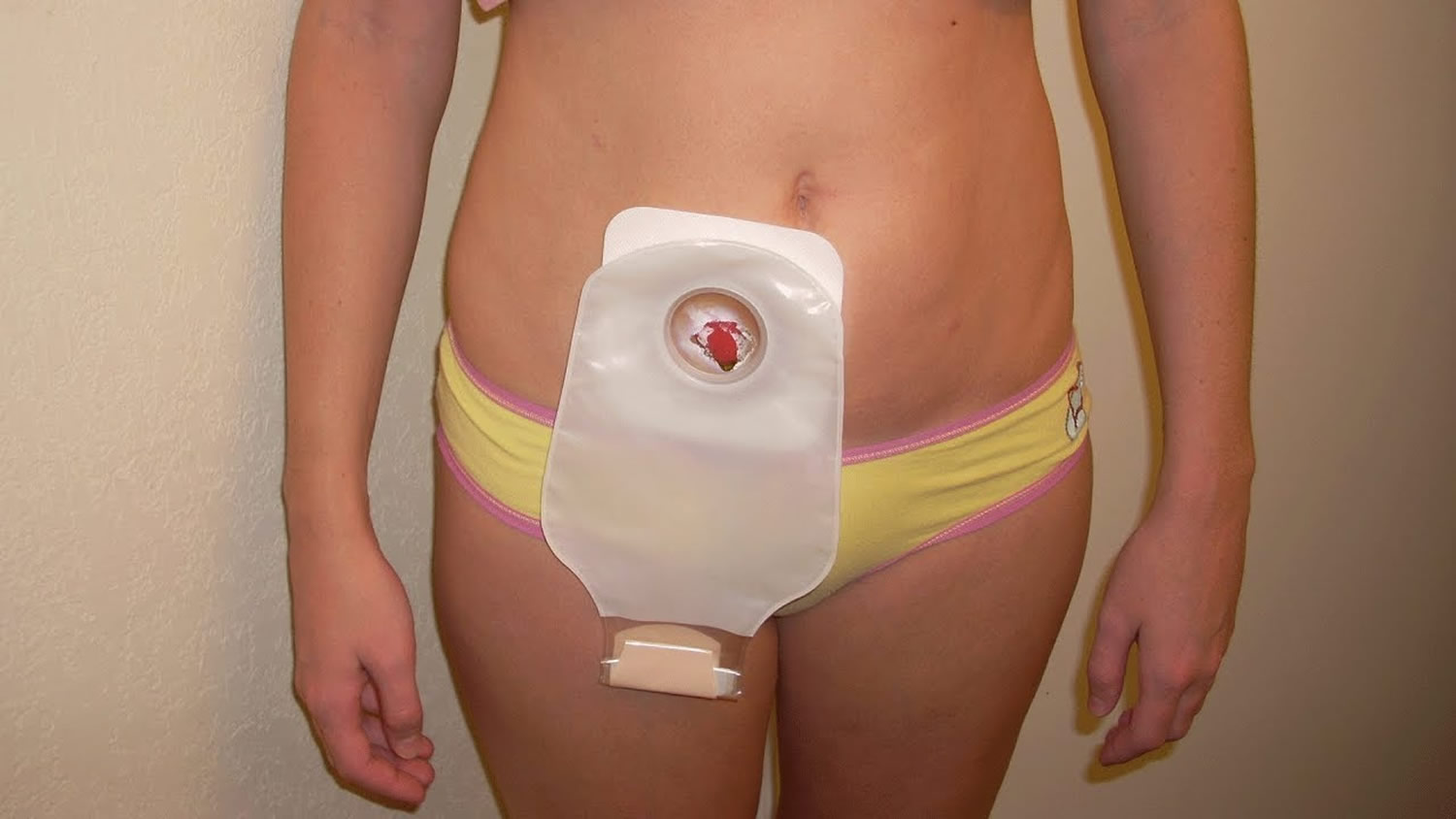
Figure 4. Colostomy stoma opening locations
Types of Colostomies
A colostomy can be short-term (temporary) or life-long (permanent) and can be made in any part of the colon. The different types of colostomies are based on where they are located on the colon.
Temporary colostomies
Certain lower bowel problems are treated by giving part of the bowel a rest. It’s kept empty by keeping stool from getting to that part of the bowel. To do this, a short-term (temporary) colostomy is created so that the bowel can heal. This healing process may take a few weeks, months, or even years. In time, the colostomy will be reversed (removed) and the bowel will work like it did before – the stool will exit from the anus again.
Permanent colostomies
When part of the colon or the rectum becomes diseased, a long-term (permanent) colostomy must be made. The diseased part of the bowel is removed or permanently rested. In this case, the colostomy is not expected to be closed in the future.
Transverse colostomies
There are 2 types of transverse colostomies: the loop transverse colostomy and the double-barrel transverse colostomy. The transverse colostomy is in the upper abdomen, either in the middle or toward the right side of the body. This type of colostomy allows the stool to leave the body before it reaches the descending colon. Some of the colon problems that can lead to a transverse colostomy include:
- Diverticulitis. This is inflammation of diverticula (little sacs along the colon). It can cause abscesses, scarring with stricture (abnormal narrowing), or rupture of the colon and infection in severe cases.
- Inflammatory bowel disease
- Cancer
- Obstruction (blockage)
- Injury
- Birth defects
If there are problems in the lower bowel, the affected part of the bowel might need time to rest and heal. A transverse colostomy may be used to keep stool out of the area of the colon that’s inflamed, infected, diseased, or newly operated on – this allows healing to take place. This type of colostomy is usually temporary. Depending on the healing process, the colostomy may be needed for a few weeks, months, or even years. If you heal over time, the colostomy is likely to be surgically reversed (closed) and you will go back to having normal bowel function.
A permanent transverse colostomy is made when the lower portion of the colon must be removed or permanently rested, or if other health problems make the patient unable to have more surgery. The colostomy is then the permanent exit for stool and will not be closed in the future.
Loop transverse colostomy: The loop colostomy may look like one very large stoma, but it has 2 openings. One opening puts out stool, the other only puts out mucus. The colon normally makes small amounts of mucus to protect itself from the bowel contents. This mucus passes with the bowel movements and is usually not noticed. Despite the colostomy, the resting part of the colon keeps making mucus that will come out either through the stoma or through the rectum and anus. This is normal and expected.
Figure 5. Colostomy types
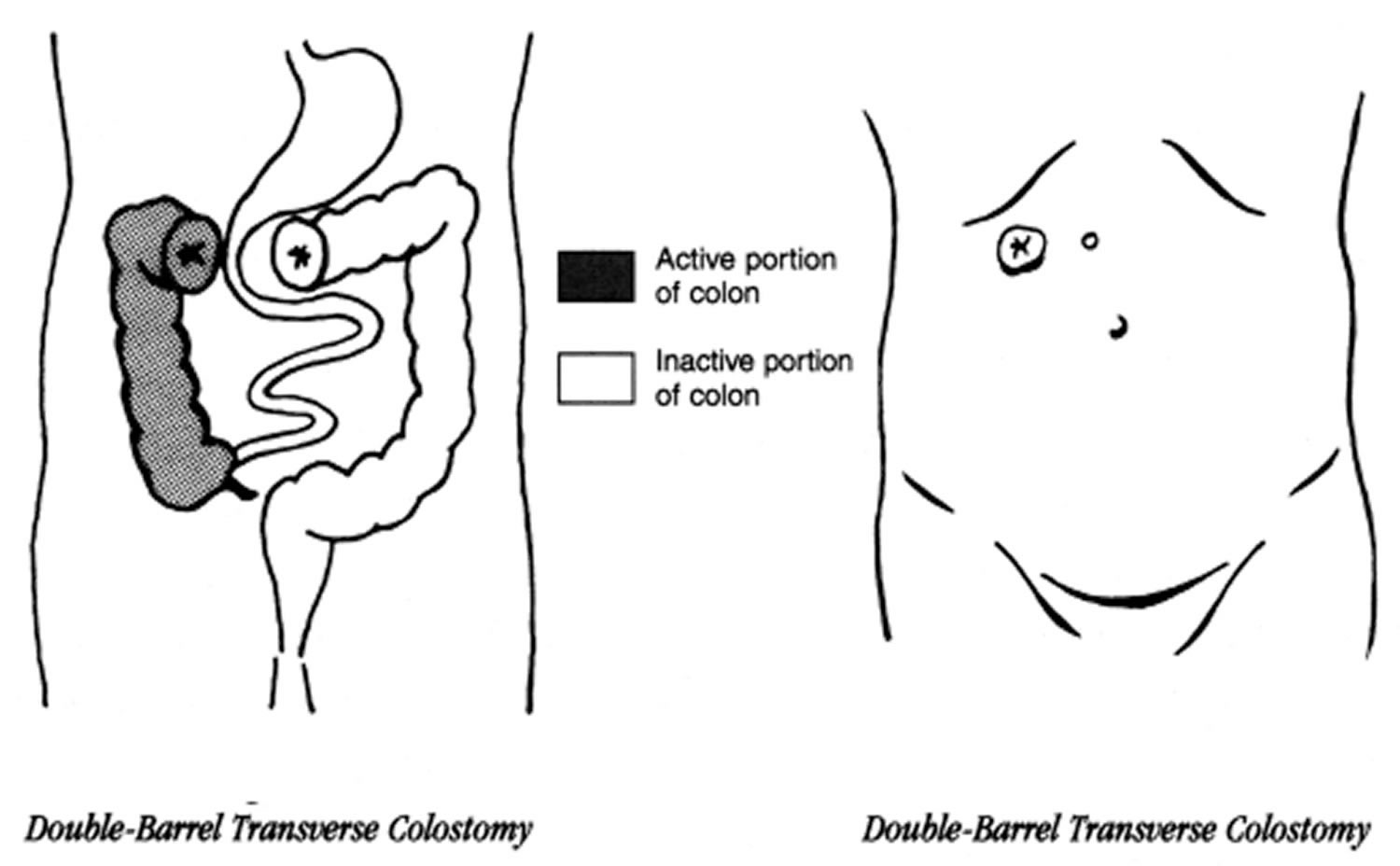
Double-barrel transverse colostomy (Figure 6): When creating a double-barrel colostomy, the surgeon divides the bowel completely. Each opening is brought to the surface as a separate stoma. The 2 stomas may or may not be separated by skin. Here, too, one opening puts out stool and the other puts out only mucus (this smaller stoma is called a mucus fistula). Sometimes the end of the inactive part of the bowel is sewn closed and left inside the belly. Then there’s only one stoma. The mucus from the resting portion of the bowel comes out through the anus.
Figure 6. Double-barrel transverse colostomy
Large intestine
The large intestine extends from the distal end of the ileum to the anus, a distance of approximately 1.5 m in adults (5 ft) long and 6.5 cm (2.5 in.) in diameter. The large intestine is named for its relatively large diameter, not its length. The large intestine absorbs fluids and salts from the gut contents, thus forming feces. The large intestine consists of the cecum, appendix, colon, rectum, and anal canal.
Beginning in the right groin as the cecum, with its associated appendix, the large intestine continues upward as the ascending colon through the right flank and into the right hypochondrium. The ascending colon begins at the ileocecal valve and passes up the right side of the abdominal cavity. It makes a 90° turn at the right colic (hepatic) flexure, near the right lobe of the liver, and crosses the abdomen as the transverse colon to the left hypochondrium. At this position, just below the spleen, the large intestine bends downward, forming the left colic flexure (splenic flexure) and continues as the descending colon through the left flank and into the left groin. Ascending, transverse, and descending colons thus form a squarish, three-sided frame around the small intestine.
The cecum is a blind pouch in the lower right abdominal quadrant inferior to the ileocecal valve. Attached to its lower end is the appendix, a blind tube 2 to 7 cm long. The appendix is densely populated with lymphocytes and is a significant source of immune cells.
The pelvic cavity is narrower than the abdominal cavity, so at the hip bone, the colon turns medially and travels along the iliac fossa before turning downward at the pelvic inlet into the pelvic cavity. The resulting S-shaped portion of the tract is called the sigmoid colon. Visual examination of this region is performed with an instrument called a sigmoidoscope. In the pelvic cavity, the large intestine continues as the rectum, about 15 cm long. Despite its name, the rectum is not quite straight but has three lateral curves as well as an anteroposterior curve. It has three infoldings called transverse rectal folds (rectal valves), which enable it to retain feces while passing gas.
The final 3 cm of the large intestine is the anal canal, which passes through the levator ani muscle of the pelvic floor and terminates at the anus. Here, the mucosa forms longitudinal ridges called anal columns with depressions between them called anal sinuses. As feces pass through the canal, they press the sinuses and cause them to exude extra mucus and lubricate the canal during defecation. Prominent hemorrhoidal veins form superficial plexuses in the anal columns and around the orifice. Unlike veins in the limbs, they lack valves and are particularly subject to distension and venous pooling. Hemorrhoids are permanently distended veins that protrude into the anal canal or form bulges external to the anus. They can result from the impaired venous return that occurs in obesity and pregnancy.
The muscularis externa of the colon is unusual. Although it completely encircles the colon just as it does the small intestine, its longitudinal fibers are especially concentrated in three thickened, ribbonlike strips. Each strip is called a taenia coli. The muscle tone of the taeniae coli contracts the colon lengthwise and causes its wall to bulge, forming pouches called haustra (singular, haustrum). Haustra are conspicuous in colonic X-rays of living patients, because they disappear when muscle tone is lost at death. In the rectum and anal canal, the longitudinal muscle forms a continuous sheet and haustra are absent. The anus is regulated by two sphincters: an internal anal sphincter composed of smooth muscle of the muscularis externa and an external anal sphincter composed of skeletal muscle of the pelvic diaphragm.
The ascending and descending colon are retroperitoneal and have a serosa only on the anterior surface, whereas the transverse and sigmoid colon are entirely enclosed in serosa and anchored to the posterior abdominal wall by the mesocolon. The serosa of the transverse through sigmoid colon often has omental appendages, also called epiploic appendages, are fat-filled pouches of visceral peritoneum that hang from the intestine. Their significance is unknown.
Figure 7. Large intestine and small intestine
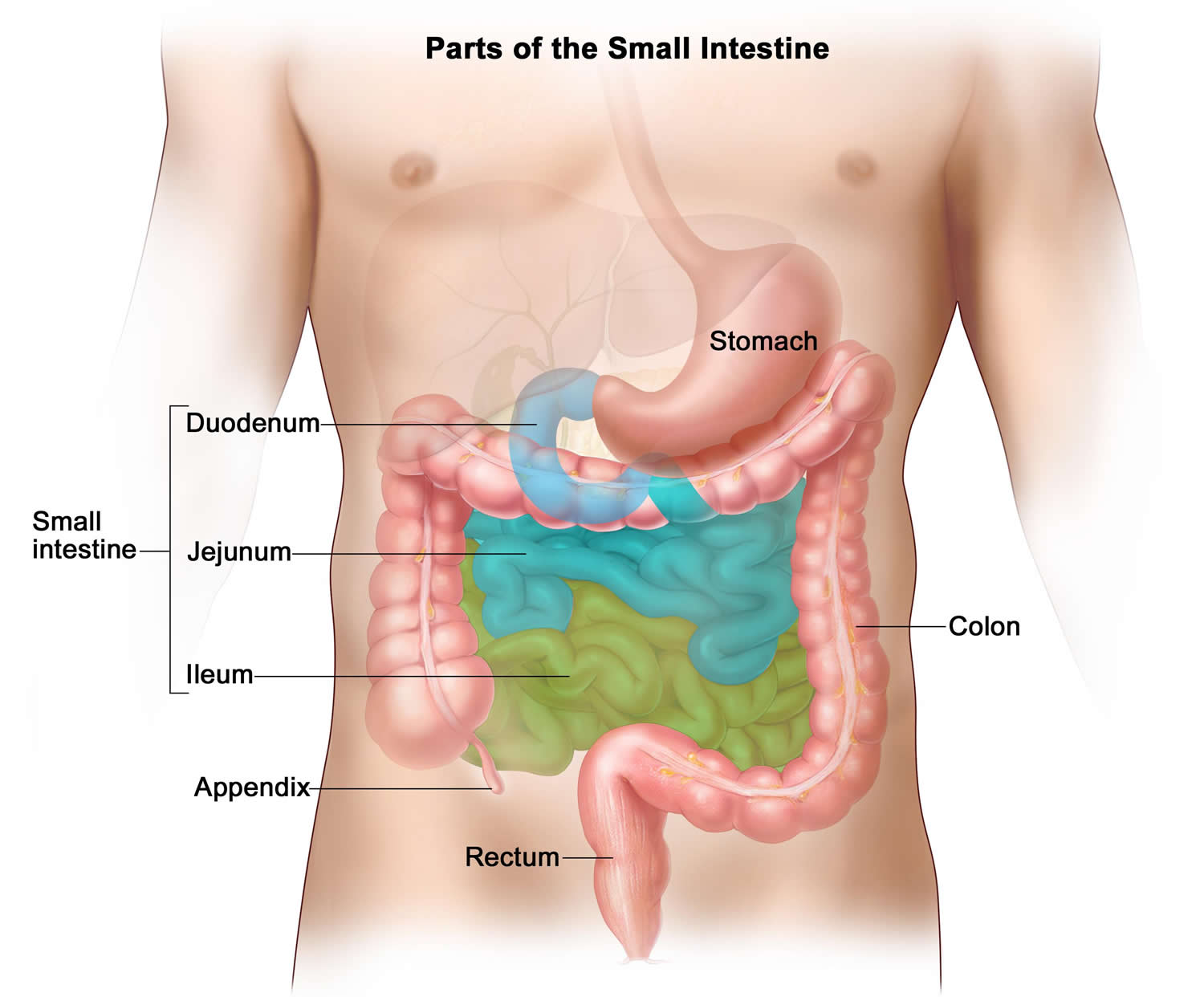
Figure 8. Large intestine
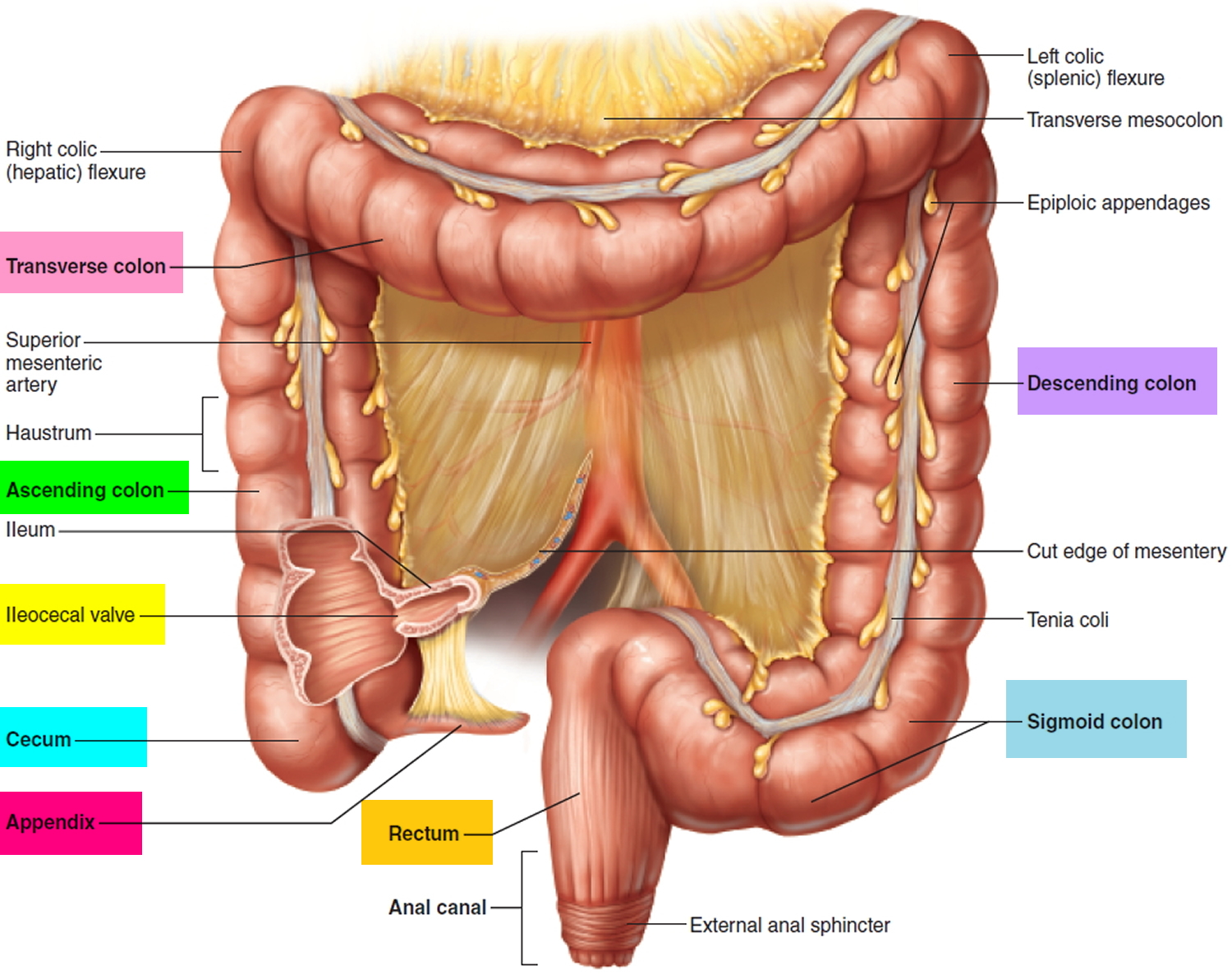
Figure 9. Large intestine location
Function of large intestine
Functions of the Large Intestine:
- Haustral churning, peristalsis, and mass peristalsis drive contents of colon into rectum.
- Bacteria in large intestine convert proteins to amino acids, break down amino acids, and produce some B vitamins and vitamin K.
- Absorption of some water, ions, and vitamins.
- Formation of feces.
- Defecation (emptying rectum).
The wall of the large intestine contains the typical four layers found in the rest of the gastrointestinal tract: mucosa, submucosa, muscularis, and serosa. The mucosa consists of simple columnar epithelium, lamina propria (areolar connective tissue), and muscularis mucosae (smooth muscle). The epithelium contains mostly absorptive and goblet cells. The absorptive cells function primarily in water absorption; the goblet cells secrete mucus that lubricates the passage of the colonic contents. Both absorptive and goblet cells are located in long, straight, tubular intestinal glands (crypts of Lieberkühn) that extend the full thickness of the mucosa. Solitary lymphatic nodules are also found in the lamina propria of the mucosa and may extend through the muscularis mucosae into the submucosa.
Compared to the small intestine, the mucosa of the large intestine does not have as many structural adaptations that increase surface area. There are no circular folds or villi; however, microvilli are present on the absorptive cells. Consequently, much more absorption occurs in the small intestine than in the large intestine.
The mucosa of the large intestine has a simple columnar epithelium in all regions except the lower half of the anal canal, where it has a nonkeratinized stratified squamous epithelium. The latter provides more resistance to the abrasion caused by the passage of feces. There are no circular folds or villi in the large intestine, but there are intestinal crypts. They are deeper than in the small intestine and have a greater density of goblet cells; mucus is their only significant secretion. The lamina propria and submucosa have an abundance of lymphatic tissue, providing protection from the bacteria that densely populate the large intestine.
How a colostomy surgery is carried out
A colostomy is carried out under general anesthetic, using either:
- open surgery (laparotomy) – where a long cut (incision) is made in the tummy to access the colon, or
- laparoscopic surgery (keyhole surgery) – where the surgeon makes several smaller incisions and uses a tiny camera and surgical instruments to access the colon
Generally, keyhole surgery is the preferred option because recovery is quicker and the risk of complications is lower.
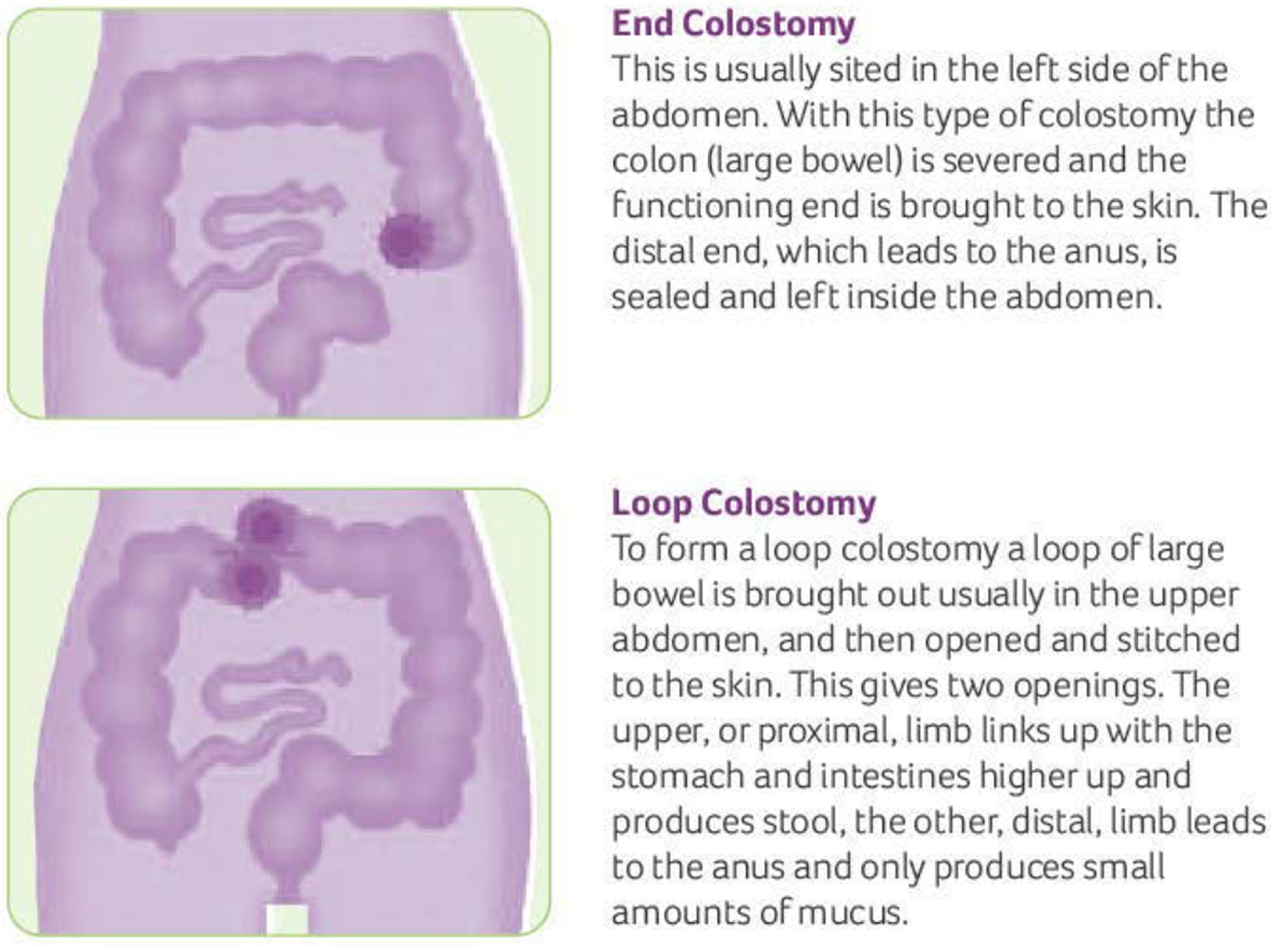
There are two main types of colostomy: a loop colostomy and an end colostomy. The specific technique used will depend on your circumstances.
A loop colostomy is often used if the colostomy is temporary as it’s easier to reverse.
Loop colostomy
In a loop colostomy, a loop of colon is pulled out through a cut in your tummy. The loop is opened up and stitched to your skin to form an opening called a stoma.
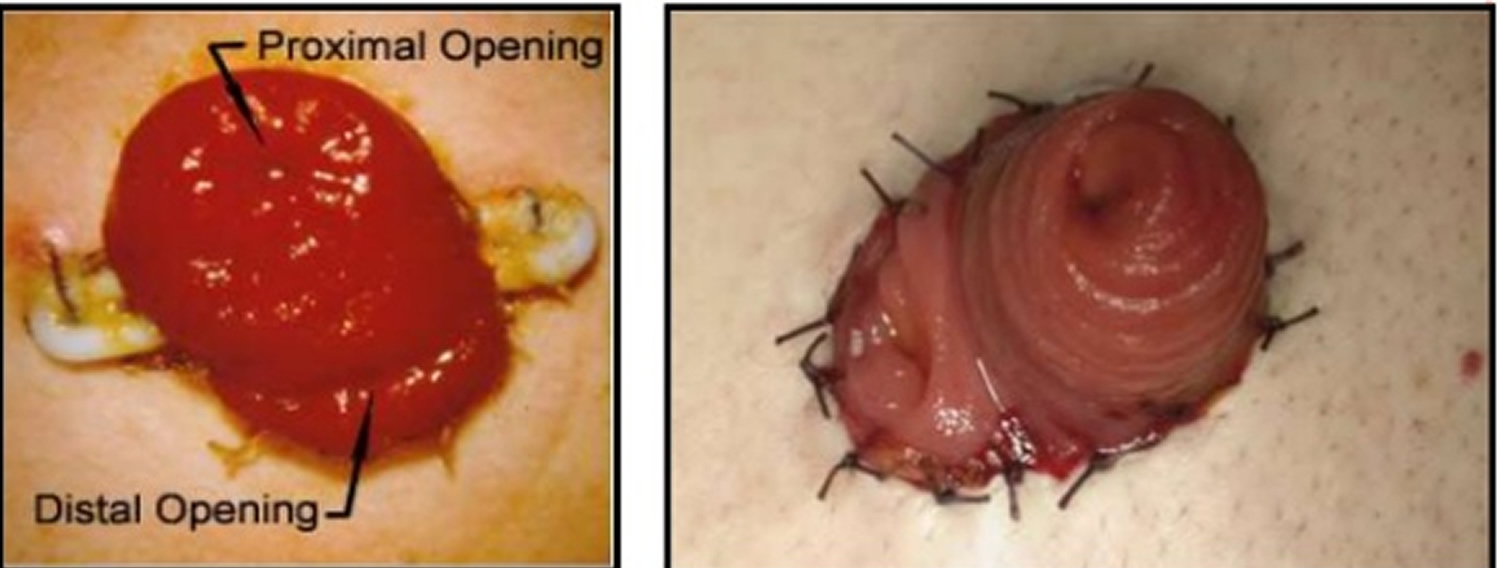
The stoma has two openings that are close together. One is connected to the functioning part of your bowel, where waste leaves your body after the operation.
The other opening is connected to the “inactive” part of your bowel, leading to your rectum.
In some cases, a support device (a rod or bridge) may be used to hold the loop of colon in place while it heals. It’s usually removed after a few days.
Figure 10. Loop colostomy
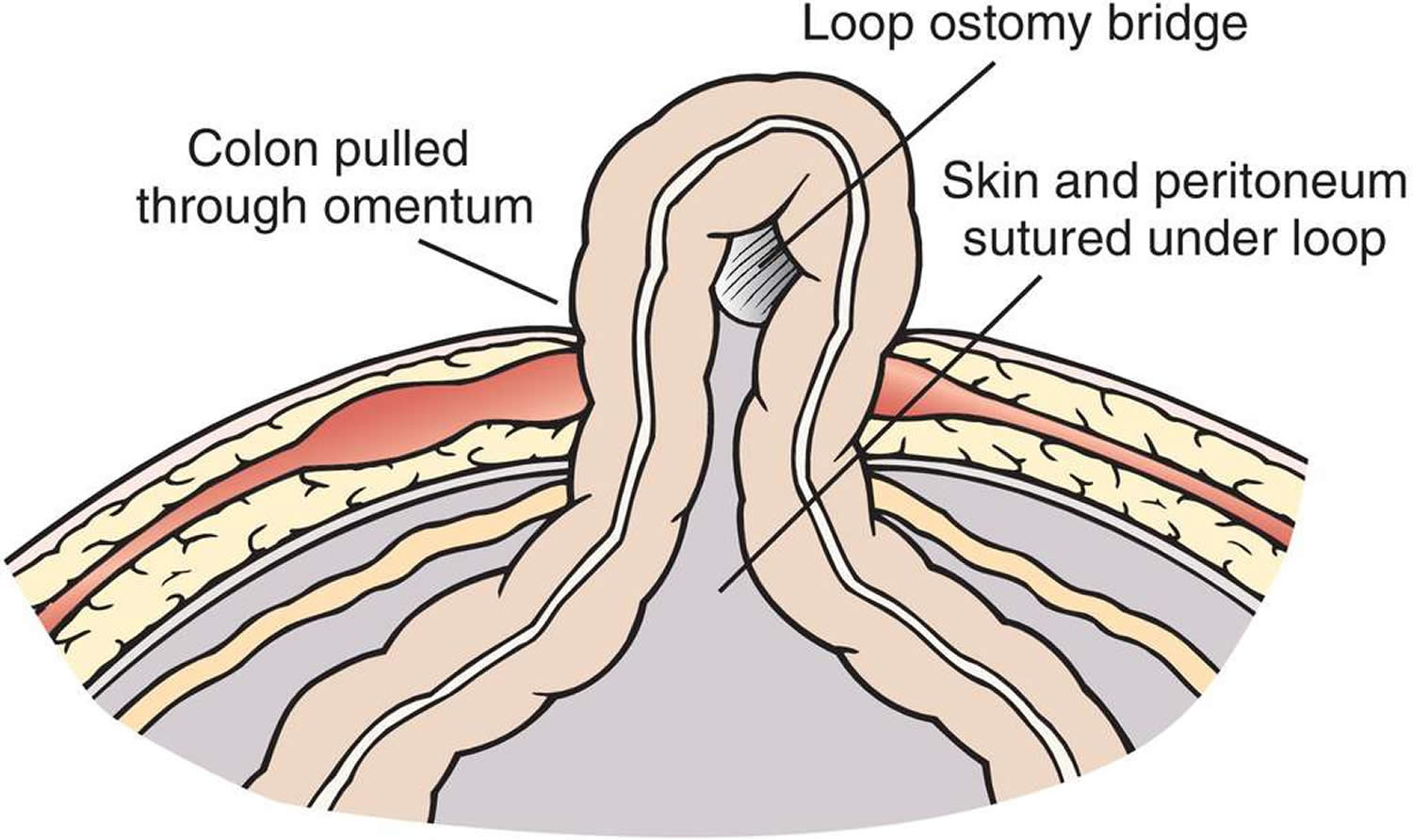
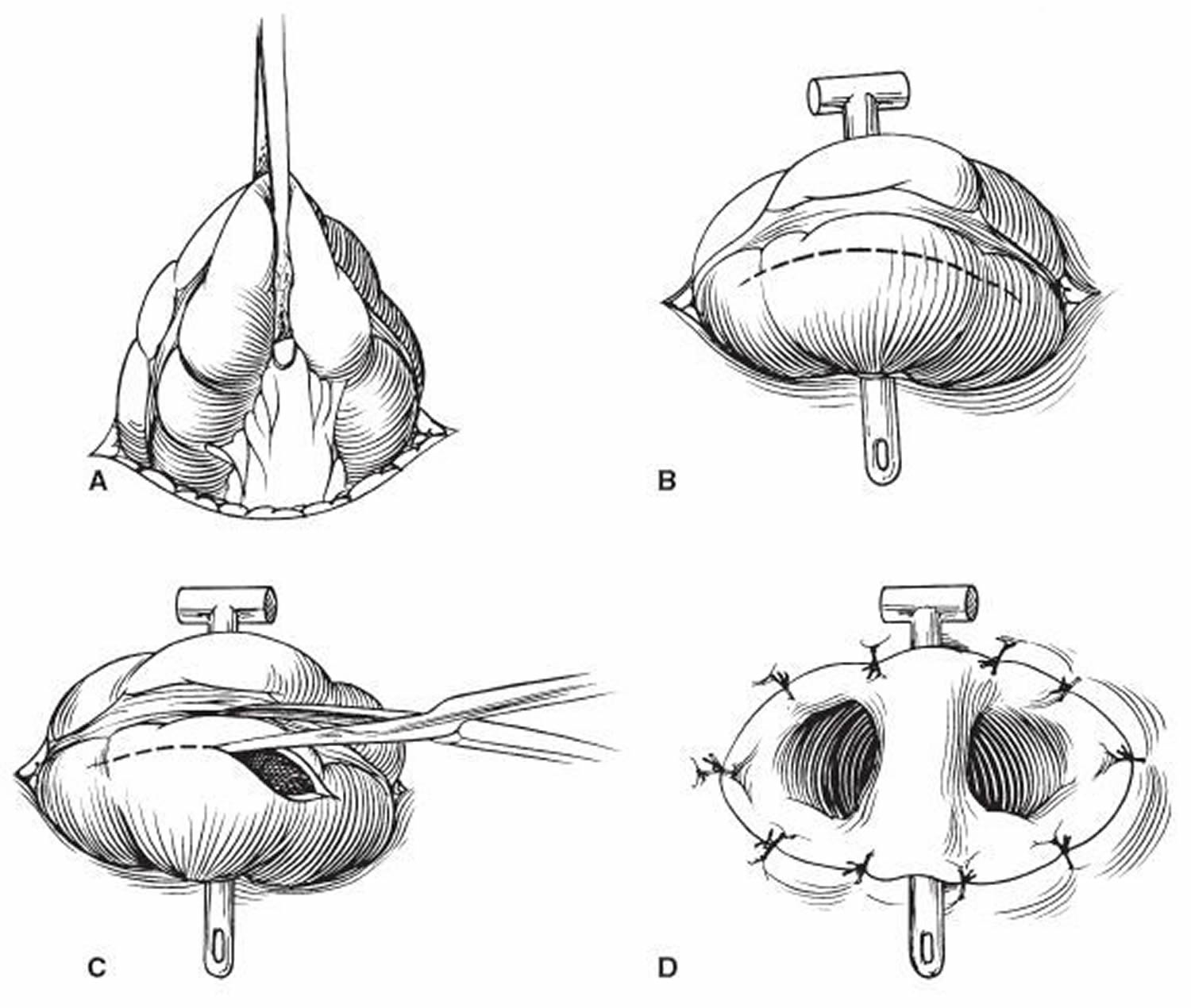
Figure 11. Loop colostomy stoma
End colostomy
With an end colostomy, one end of the colon is pulled out through a cut in your tummy and stitched to the skin to create a stoma.
An end colostomy is often permanent, but temporary end colostomies are sometimes used in emergencies to treat bowel obstructions, colon injuries or bowel cancer.
Figure 12. End colostomy
Recovering from a colostomy surgery
After having a colostomy, you’ll need to recover in hospital for a few days.
You may have:
- a drip in your vein to provide fluids
- a catheter to drain urine from your bladder
- an oxygen mask to help you breathe
A clear colostomy bag will be placed over the stoma so it can be easily monitored and drained. The first bag is often quite large – it’ll usually be replaced with a smaller bag before you go home.
Stoma nurse
While you recover in hospital, a stoma nurse will show you how to care for your stoma, including how to empty and change the bag.
The nurse will teach you how to keep your stoma and surrounding skin clean and free from irritation, and give you advice about preventing infection.
They’ll also explain the different types of equipment available and how to get new supplies.
When you leave hospital, a local stoma nurse will visit you at home, or you may be asked to go to a stoma care clinic.
Going home after a colostomy surgery
Most people are well enough to leave hospital 3 to 10 days after having a colostomy.
Once home, avoid strenuous activities that could place a strain on your abdomen, such as lifting heavy objects.
Your stoma nurse will give you advice about how soon you can go back to normal activities.
In the first few weeks after your operation, you may have more wind than usual (flatulence), and a discharge from your stoma.
This should start to improve as your bowel recovers from the effects of the operation.
Living with a colostomy
Adjusting to life with a colostomy can be challenging, but most people get used to it in time.
You may be concerned that your day-to-day activities will be restricted and other people will notice you’re wearing a colostomy bag.
Modern colostomy equipment is discreet and secure, and you should be able to do most of the activities you enjoyed before without experiencing the symptoms that made the colostomy necessary in the first place.
Your specialist stoma nurse will be able to give you further support and advice to help you adapt to life with a colostomy.
Bathing and showering
The bag can be left in place or taken off while in the bath or shower. Water cannot get into the bag or the stoma. If bathing or showering without a bag, choose a time when the stoma is less active i.e. before rather than after a meal.
Smell and wind
Many people worry that their colostomy will give off a smell that others will notice.
All modern appliances have air filters with charcoal in them, which neutralizes the smell.
Most people will be aware of the smell of their colostomy because it’s their own body. But someone standing next to you won’t be able to smell the stoma.
You’ll have more wind than usual immediately after having a colostomy, but this will slowly reduce as your bowel recovers.
Your stoma nurse can advise you about products you can use to help reduce any smell and give you dietary advice to reduce wind.
Medication
Many medicines are designed to dissolve slowly in your digestive system. Having a colostomy shouldn’t alter the effectiveness of your usual medication.
If you notice any tablets in your appliance, tell your pharmacist or doctor, who will recommend an alternative medication.
Exercise
In the weeks after surgery, some gentle exercise is usually recommended to help recovery.
How well you recover will determine how much exercise you can do. If you feel any pain, stop immediately.
Once you’ve recovered from the operation, you should gradually be able to return to your previous exercise routine.
Most types of exercise are possible with a stoma, including swimming, as all colostomy bags are waterproof.
Electrolyte imbalance
Electrolytes are salts and minerals in the blood, like potassium, magnesium, and sodium. Keeping them balanced is important. When the colon (large intestine) is removed, you’re at a greater risk for electrolyte imbalance. Diarrhea, vomiting, and a lot of sweating can increase this risk.
Dehydration is also a serious concern. Symptoms include increased thirst, dry mouth, decreased urine output, feeling light-headed, and feeling tired. If you get dehydrated, you’ll need to drink more fluids. To avoid dehydration, you should try to drink 8 to 10 eight-ounce glasses of fluid a day. If you have diarrhea, you may need more. Drinks such as Pedialyte contain potassium and sodium. But any liquid containing water (soda, milk, juice, tea, etc.) helps to meet your daily need for fluid.
Loss of appetite, drowsiness, and leg cramps may be signs of sodium loss. Fatigue, muscle weakness, and shortness of breath may be signs of potassium loss. Dehydration, low sodium, and low potassium can all be dangerous and should be treated right away. Keep in mind that some of these symptoms can be caused by other problems which may be emergencies. Call your doctor or your local emergency services number right away if you are dizzy, weak, or having other serious symptoms.
What is a colostomy bag
Colostomy bag (also called stoma bags) is where you feces are collected as they leave your body via the stoma. Your stoma care nurse will help you to decide which colostomy bag is best for you after your operation. Once you get home, you’ll soon start to discover that there are lots of different types of stoma bags. These are designed to meet the different needs of people with stoma have. You should consult your stoma care nurse before changing to a new product. There are also a wide range of accessories available. These include deodorisers, wipes, skin protective wipes, lotions and creams.
Table 1. How to choose the right colostomy bag
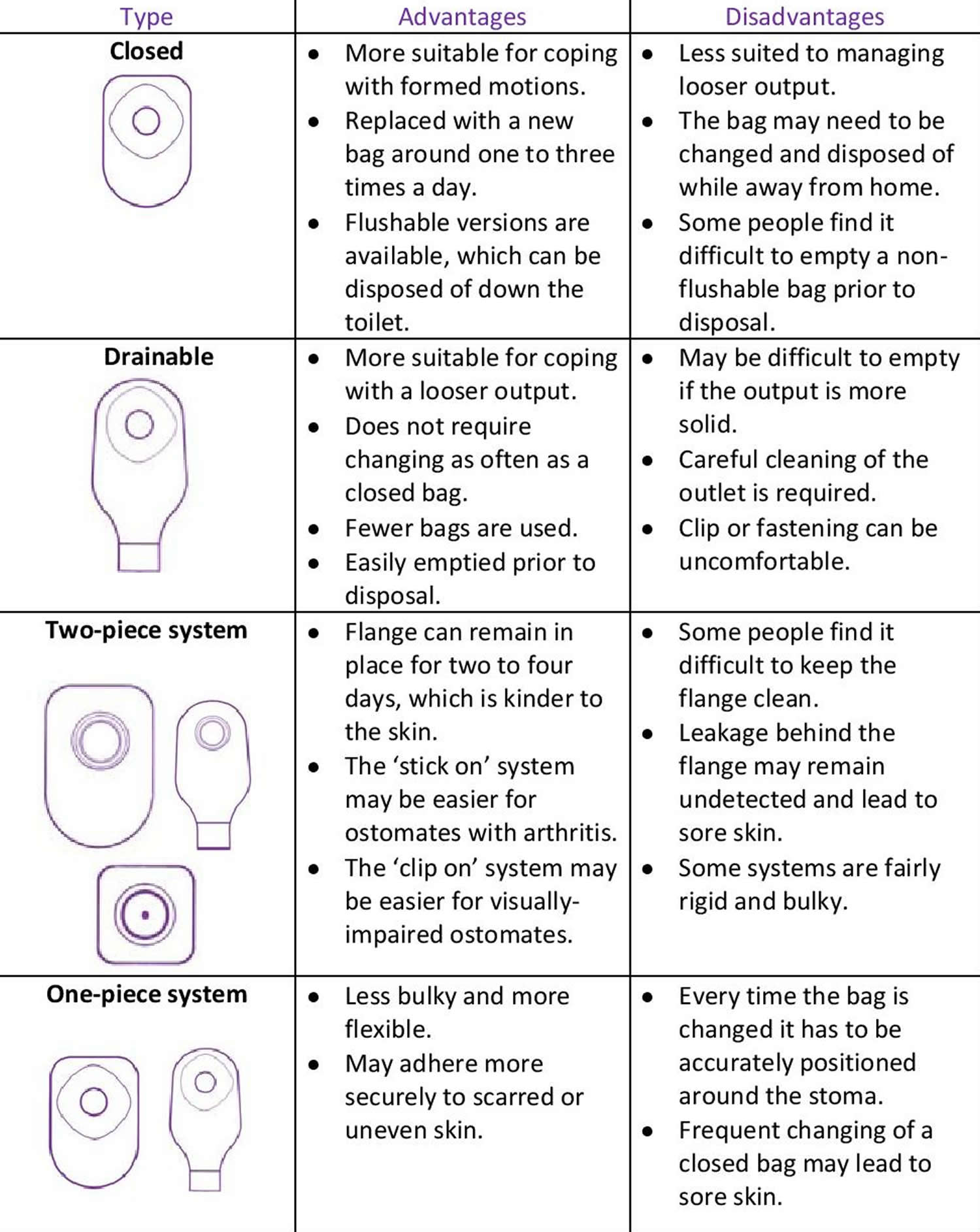
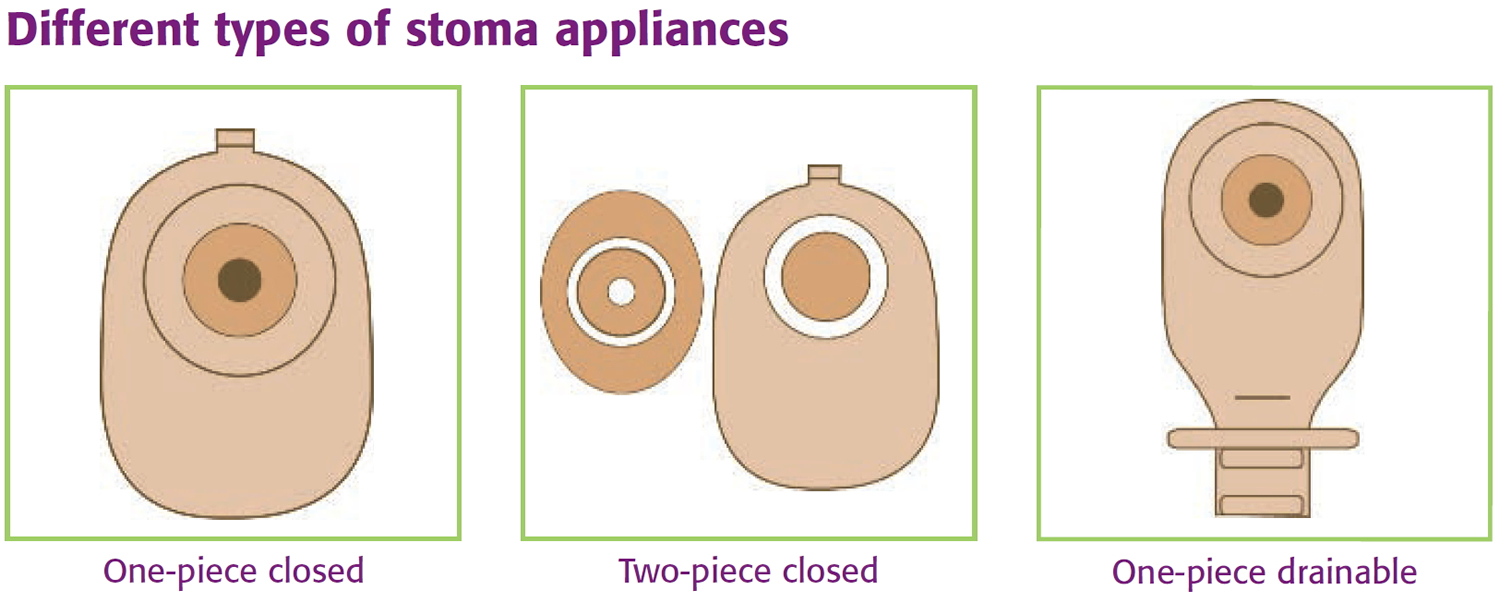
Figure 13. Different types of colostomy bags
Living with a colostomy bag
A colostomy bag is often used to collect your poo (stools). It needs to be removed and replaced when full, usually one to three times a day.
There are also drainable bags that only need to be replaced every one or two days. These may be suitable for people who have particularly loose stools.
A specialist stoma nurse, who usually sees you before and after the colostomy operation, will help you choose the most suitable colostomy equipment.
There’s a wide range of colostomy appliances available, including:
- One-piece colostomy bag – the bag and flange (part that sticks to your skin) are joined together; the appliance is removed when full and then disposed of
- Two-piece colostomy bag – the bag and flange are separate, but can be connected; the flange can be left on your skin for several days, and the bag removed and disposed of several times a day
- Closed colostomy bags which are mainly used for coping with formed motions. They are usually changed several times a day. Closed bags with a special liner which contains the motions and can be flushed down the toilet are available.
- Drainable colostomy bags which are mainly used for coping with liquid motions. They may be worn for longer than closed bags as they can be emptied through an outlet at the bottom and then resealed with an integral Velcro seal or a clip.
Colostomy appliances are made from non-allergic (hypoallergenic) materials to reduce skin irritation. They also contain special filters to prevent any unpleasant odors.
If you have regular and predictable bowel patterns, you may not always need to wear a colostomy bag. But as occasional leakages can happen, it’s recommended that you wear a small stoma cap.
Additional products that can make living with a colostomy more convenient include:
- support belts and girdles
- deodorisers that can be inserted into your appliance
- protective skin wipes
- sprays to remove adhesive
- protective stoma rings
- specially designed underwear and swimwear
Your stoma care nurse will be able to give you more information and advice about equipment.
How to change a colostomy bag
Before you leave hospital your stoma care nurse will show you how to change your bag. S/he will also teach you how to use a stoma guide to check that the hole in the adhesive flange or base-plate is the correct size. If necessary, you will also be shown how to cut the right size and shape using a template.
A colostomy bag is best changed when about three-quarters full. This makes the process easier and the colostomate (a person with colostomy) more comfortable. It is usually carried out in the bathroom, but if the colostomate is seated, this can mean folds or creases form around the stoma making it difficult to achieve a good seal between the skin and the flange/base-plate. It may be best to remove the used colostomy bag and attach the new one when the colostomate is standing. However, if this is not possible then an alternative might be for the colostomate to lay flat on a bed.
1. Before you begin
Check you have everything you need: water, soft wipes, a new colostomy bag, any accessories you use and a plastic disposal bag.
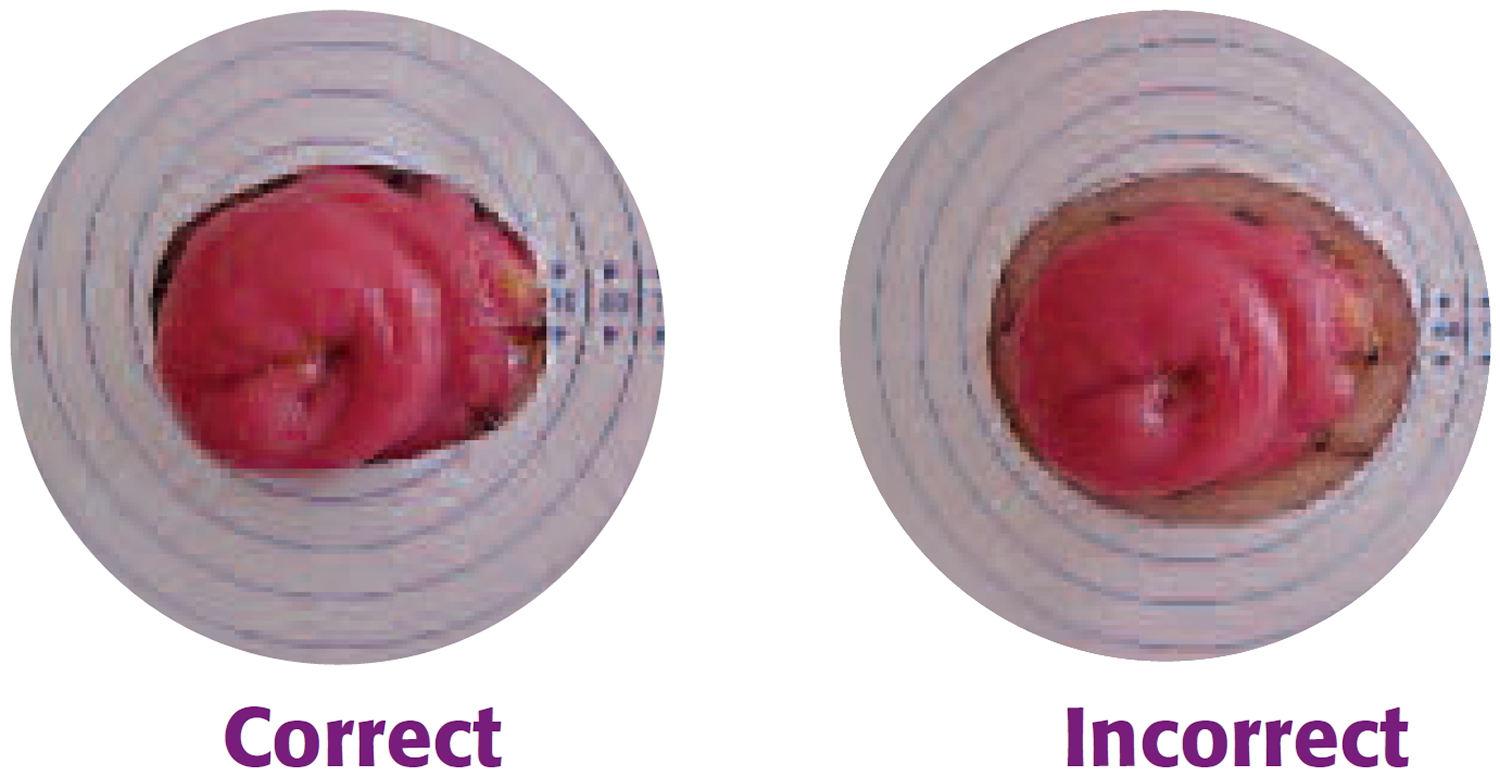
Check whether the hole in the adhesive flange/base-plate has been pre-cut to the size and shape of the stoma. If not, use a template to mark the outline of the stoma and using curved scissors, trim to the correct shape. If the hole is too large skin will show and be irritated by the contents of the bag, which can make it sore. If the hole is too small, it may rub against the stoma and cause it to swell.
Tips:
If you wear a one–piece pouch use the backing paper/film that protects the adhesive on the flange to check that the hole is the correct size. Hold the backing film around your stoma; it can be difficult to see if you are looking down so it may be helpful to stand in front of a mirror or ask someone else to check for you.
There should be a 1–2mm gap all around to prevent the edges of the hole rubbing on the stoma, whilst still ensuring that the contents of the pouch do not come into contact with the skin.
Figure 14. Measuring and cutting a hole in the base-plate of the colostomy bag
2. Removing the old colostomy bag
Remove the old bag, working slowly and gently from the top to the bottom of the flange. medical adhesive remover (available on prescription) can be used to avoid damaging the skin. It is wiped or sprayed beneath the flange as it is peeled away from the skin.
Check the skin around the stoma for any early signs of irritation. Gently clean the stoma and surrounding skin with warm water. Do not use soaps, disinfectants, harsh solvents or baby wipes as these often contain perfume or moisturizers and may affect how the flange/base-plate sticks, or may irritate the skin.
Remember the stoma bleeds easily if it is rubbed too hard, but bleeding should stop quickly. If blood comes from inside the stoma, contact your stoma care nurse.
3. Fitting the new colostomy bag
Gently pat the skin until it is completely dry. If you are prone to sore skin, barrier wipes, sprays and lotions are available.
When your skin is completely dry, fit the new colostomy bag (or base plate), making sure it is secure all the way round. When fitting a one-piece colostomy bag, it helps to bend the top half of the flange away from your body, so that you can see to fit the bottom half around the stoma. Then, with the flat of your hand, press the remainder of the flange in position. The warmth of your hand will ensure that it adheres snugly. Press the flange/base-plate in place for at least half a minute to make sure the seal is secure.
If using a two-piece colostomy bag, then attach the bag to the base-plate.
4. Disposal of used colostomy appliances
Seal the used appliance inside a disposal bag (provided free by suppliers). In a nursing home this can be disposed of with other clinical waste.
The used colostomy appliance may be wrapped up well and put in the dustbin. Some people prefer to empty the contents of the stoma bag into the toilet before discarding it in this way.
Colostomy bags with liners that contain the stools and can be flushed down the toilet are now available.
Colostomy care
- Sore Skin
If the skin around the stoma becomes red and inflamed this can be due to damage when removing the flange/base plate. Using an adhesive remover may help to prevent this. With a two-piece or drainable colostomy bag the flange/base-plate remains in place for several days which reduces skin damage. Sore skin can also result from contact between the contents of the colostomy bag and the skin. Stomas can change in size and shape so check the size of the stoma every few months to make sure the hole in the flange/base-plate fits snugly around the stoma, so that the skin is not exposed. If the problem continues, consult a stoma care nurse who can advise on special products which can heal the skin and do not interfere with the adhesion of the appliance.
- Bleeding
The stoma bleeds easily if it is rubbed a bit too hard. If the bleeding does not stop, or the blood is coming from inside the stoma, consult a stoma care nurse. The stoma may bleed more easily if anticoagulant drugs e.g. Warfarin, or aspirin, are being taken.
- Ballooning
This occurs when gas, expelled through the stoma, collects inside the bag causing it to inflate. Most bags have a filter which allows this gas to escape. Occasionally the filter will become blocked and the bag will need to be changed. If this is happening on a regular basis it may be worth trying a different bag which may have a more effective filter. To ensure the filter doesn’t get wet and become ineffective, when in the bath or shower, cover it with the sticky patch supplied in the box of stoma appliances.
- Pancaking
This occurs when, instead of dropping to the bottom of the bag, the bowel motion collects around the stoma and may seep between the flange and the skin. One of the reasons this happens is because there isn’t enough air in the bag and the two sides stick together. It may help to cover the filter with a sticky patch to prevent gas escaping from the bag or place a small piece of crumpled tissue inside the bag to keep the sides apart. Lubricating the inside of the bag with baby oil or a special gel may help the motion to drop to the bottom of the bag.
- Constipation
Eating more fiber and fruit should help to make motions softer. Constipation can also be the result of not drinking enough fluid or the side effect of medication e.g. certain painkillers or antidepressants (check with your doctor or pharmacist). Unless prescribed by the doctor or stoma care nurse do not use suppositories or enemas as the stoma will reject them. If the stoma has not worked for several days or there is pain or vomiting seek medical advice.
- Loose motions
If a large section of the colon has been removed it is likely that motions will always be fairly liquid and it may be easier to use a drainable bag. If motions are normally formed an episode of diarrhea could be due to a “stomach bug”, stress or emotional upset or certain medication e.g. antibiotics. If diarrhea persists it is important to seek medical advice.
- Odor
There will only be an odor when emptying or changing the bag. This can be reduced by spraying a deodorant or striking a match. Odor while the bag is in place could indicate a leakage or a faulty filter. Drops, gels, capsules and sachets are available to neutralize any odor inside the bag.
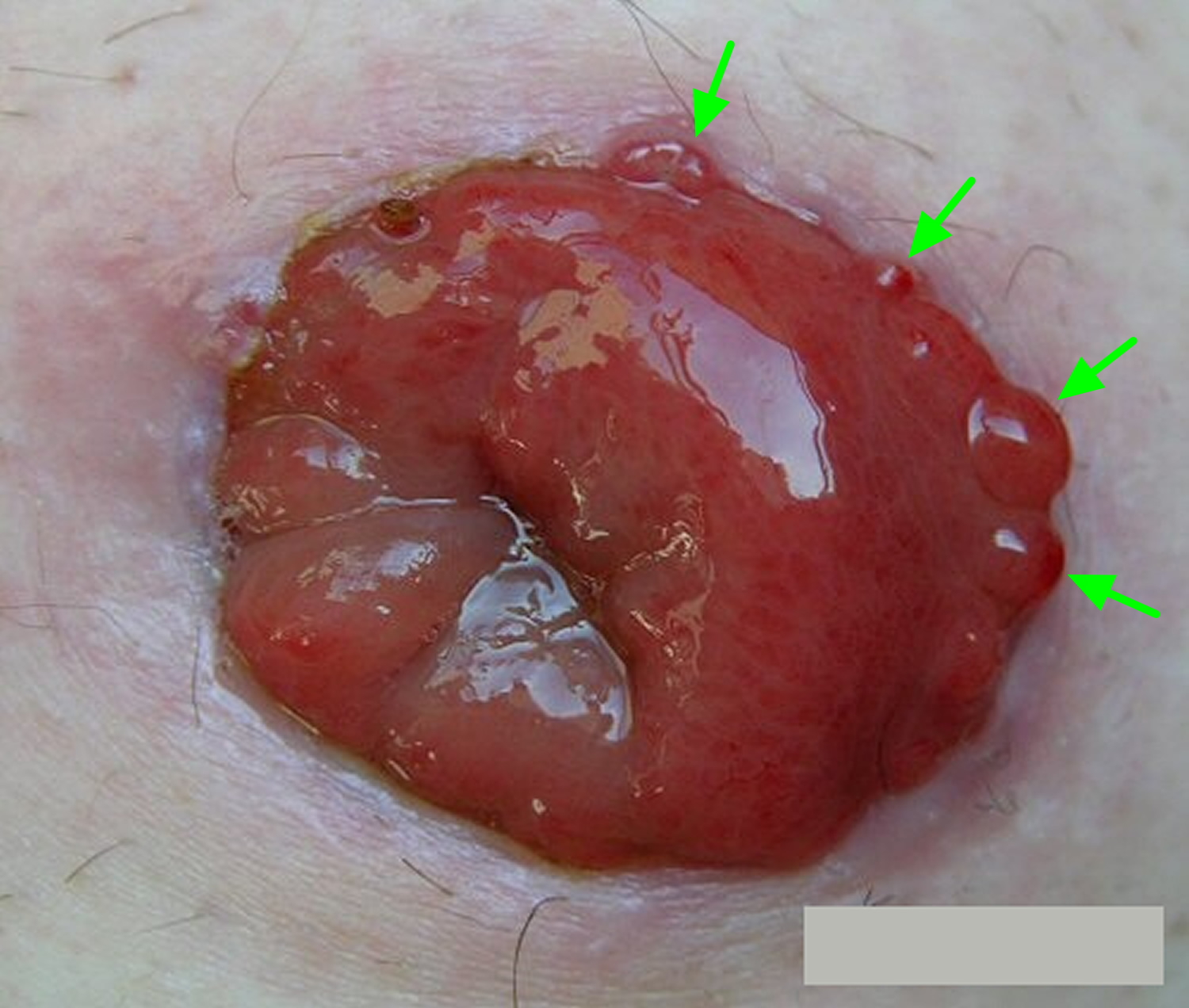
- Granulomas
Granulomas are very common and are small areas of over granulation tissue that appear as fleshy protuberances like tiny beads of varying sizes. Granulomas occur on the surface of the stoma or more commonly at the muco–cutaneous junction (the join between the bowel and the skin).
Granulomas develop as a result of over-healing of damaged skin or the stoma surface, possibly due to friction from the bag. Granulomas can be due to inflammation, infection or fecal irritation from the stomal output. Irritation from the ostomy appliance can also be a common cause. Some, but not all, stoma granulomas can cause bleeding and discomfort when touched when the skin around the stoma is being cleaned. This bleeding can cause problems with adherence of the colostomy bag. . Also, if they are large they may prevent pouch adhesion which may result in leakage problems.
What can you do to prevent stoma granulomas?
Ensure that the hole in the flange/baseplate of your pouch is the right size, so that the edge does not rub against the stoma. Good colostomy bag changing techniques are an important part of reducing the risk of granuloma formation:
- Remove the used colostomy appliance slowly and gently. Start at the top and support the skin as you go. Use adhesive remover spray/wipes to reduce damage to the skin.
- Wipe away any feces with toilet paper then wash the stoma and surrounding skin with warm water and dry the area thoroughly using dry wipes or kitchen
roll. - When fitting a new appliance, bend the top half away from the body so that you can see to fit the bottom half accurately around the stoma, then press the remainder of the flange into position.
Some people, however, appear to be more susceptible to the formation of granulomas than others.
Figure 15. Stoma granulomas
Available treatment
Your stoma care nurse will take you through the treatment available, the main option being 75% silver nitrate applied to the granulomas approximately two to three times a week. This needs to be done by a healthcare professional, either the stoma consultants, stoma care nurse or your doctor. A stoma Orabase paste can be applied to prevent friction on the stoma surface and a lubricating gel placed in the pouch can help prevent the pouch rubbing on the stoma surface. Other treatment options include the application of Haelan Tape or application of liquid nitrogen.
If you think you may have stoma granulomas, then please contact your stoma care nurse for a review. Some specially trained stoma care nurses and consultants may also use curette and cautery (a special instrument is used to cut out the granuloma and the wound is cauterised or burnt closed).
Will granulomas eventually go away without treatment?
Usually some form of treatment is required, even if it is only the application of Orabase Paste when the granuloma is very small. The earlier the treatment is started the better.
Are granulomas likely to re–occur?
Yes, some people do find that granulomas can re–occur and they should seek a stoma care nurse review as soon as they feel they have re–appeared.
Prolapsed stoma
A prolapse of the stoma occurs when the bowel protrudes through the stomal opening in the skin to a greater extent than was anticipated. The amount of protruding bowel can vary from 2-3cm to more than 10cm. Although when this first happens it can be very distressing and frightening it is usually not serious. However, a review by a stoma care nurse is essential.
A prolapse can occur in any stoma type but is more common in loop stomas. There are many causes, the most common are:
- An over sized hole made in the abdominal wall at surgery
- Increased abdominal pressure due to tumor, pregnancy, coughing and sneezing
- Excessive exertion e.g., heavy lifting
- Poorly developed abdominal muscular support (infants)
- Obesity
How do I manage a prolapsed stoma?
There are two ways of managing a prolapse:
- Conservative management
Your stoma care nurse will advise on how you should look after the stoma and give you help in reducing the swelling. He/she will also advise you on which specialist pouches are available and also on the use of abdominal support garments.
- Surgical management
If a prolapse is too large to manage conservatively, or if it has become discolored, surgical intervention may be required. This will involve removal of the prolapsed section of the bowel and resiting of the stoma.
If you have a prolapse stoma please contact your local stoma care nurse for advice and support.
Colostomy irrigation for descending and sigmoid colostomies only
Irrigation is an alternative to wearing a colostomy bag. It involves washing out your colon with water either every day or every other day.
To do this, you gently insert a small device into your stoma and attach it to a bag full of water.
You slowly move water into your colon so it washes it out. The equipment is then disposed of once the process is complete. A cap is used to cover your stoma in between irrigations.
Advantages of irrigation include:
- you choose when you want to perform irrigation
- you don’t have to wear a colostomy appliance (but may have to wear a small cap)
- you should be able to enjoy a more varied diet
- you should have less gas (flatulence)
Disadvantages of irrigation include:
- it’s a time-consuming process that takes 45 to 60 minutes to complete, usually on a daily basis
- for the best results, irrigation should be carried out at the same time every day, which may be difficult when you’re away from home on holiday or with work. If it is difficult to irrigate then normal bowel function will resume. It is suggested that the irrigator always takes pouches (both closed and drainable) with them as a precaution when away from home; even irrigators cannot guarantee they will not get diarrhea.
Irrigation isn’t always possible. For example, it’s not suitable for people with Crohn’s disease or diverticulitis, or if you’re having radiotherapy or chemotherapy.
Irrigation probably isn’t advisable for young children as it’s quite time-consuming.
Who can have colostomy irrigation
- Those with an end colostomy situated in the lower part of the large bowel (for descending and sigmoid colostomies only), motion should normally be semi–formed or formed.
- Reasonable eyesight and dexterity are required to be able to manage the procedure successfully.
- Colostomates will need to make an informed choice about undertaking this procedure and be motivated and keen to succeed.
- The surgeon’s consent, or that of a stoma nurse, must be obtained prior to commencing irrigation, since with some medical conditions irrigation is inadvisable. It is advised that the patient’s doctor is informed.
Who cannot have colostomy irrigation
- People with complications such as a prolapse, stenosis or large hernia.
- Those with further bowel disease e.g. Crohn’s disease or diverticulitis.
- Irrigation may not be successful for those suffering from persistent diarrhea.
- Young children who have difficulty sitting still for the required time. As with all teaching of young children, if the child is old enough to take an interest in the working of the stoma, it may be possible to overcome this difficulty by making a game of it: “Let’s see how long you can go without needing a bag”.
- People with renal or cardiac problems. Irrigation could cause fluid overload, or slow the heart rate excessively by stimulating the vagus nerve.
When can colostomy irrigation start?
Irrigation can be taught post–operatively when the bowel has started to function. However, many people have more than enough to cope with, in coming to terms with major surgery, and most stoma care nurses prefer to wait two or three months so that the patient has had a period of recovery and adjustment. A useful guide is when normal appetite has returned.
Irrigation needs to be performed when the toilet or bathroom is free, which in some cases may be for up to an hour. It is important to relax, having to rush can lead to anxiety and is likely to cause the procedure to fail. Irrigation should as far as possible always be performed at the same time of day but it is better to be flexible and not worry if this is impossible. It is a procedure that improves with practice and knowledge of your bowels.
What equipment and supplies you need in order to do colostomy irrigation?
Irrigation equipment is available on prescription from various manufacturers.
The equipment always has the same basic components:
- Water reservoir
- Tubing with flow control
- A cone: a nozzle with a smooth rounded tip to make it easy to insert into the stoma, and which is flared out to enable it to make a seal round the stoma
- Lubricating jelly to aid the insertion of the cone
- Irrigation belt and flange (not normally required for colostomates using two–piece appliances)
- Disposable irrigation sleeve
- Disposal bag
- Tissues or toilet paper
- New appliance to be worn, and any accessories used
Figure 16. Colostomy irrigation equipment
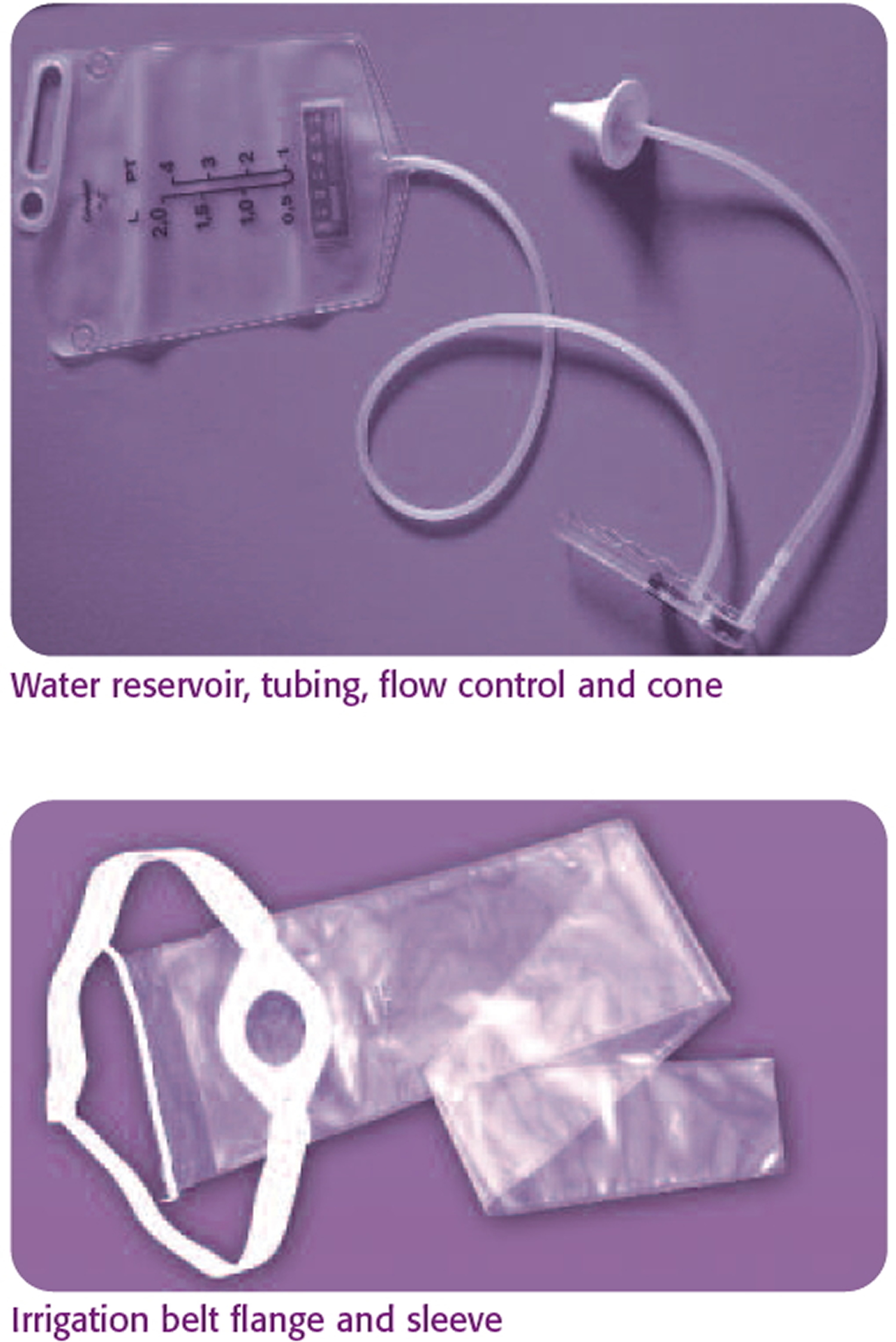
Figure 17. Stoma plug and cap

The water container should be clear, enabling the water level to be seen, and should preferably have a liquid crystal temperature indicator. The flow control should be easy to operate with one hand. The irrigation flange should give a secure seal around the stoma and the disposable sleeve should be long enough to hang into the toilet. It can be trimmed if needed. Once used, the flange and cone should be washed with antibacterial soapy water, dried and stored until their next use. There is normally no need to wash the reservoir.
How to perform colostomy irrigation
- Connect the reservoir, tubing and cone together. Fill the reservoir with tepid 98.6 to 100.4 °F (37–38° C) tap water and hang it on a hook, such that the bottom of the reservoir is at shoulder level or slightly above when the colostomate is in the position adopted for irrigation.
- Open the flow control to allow water through the tubing to expel air, and then close the control when the desired amount of water remains in the reservoir.
- Fit the irrigation sleeve over the stoma and sit on the toilet, or on a stool adjacent to it, so that the sleeve hangs into the bowl.
- Lubricate the cone and insert it gently into the stoma following the direction of the bowel. The stoma care nurse will help with this at first.
- Open the flow control on the reservoir and allow the water to run slowly into the bowel. This should take 8–15 minutes. Most people use 800ml to 1.2 liters but the optimum amount may vary from 700ml to about 1.6 liters. Patients get to know by experience what quantity works best for them. Should cramping or pain be experienced during this time close the flow control, massage the abdomen and wait a few minutes before restarting. For the first irrigations patients may wish to restrict the rate of flow, but with experience they usually find that they can let the colon determine the rate.
- When the water has run in, remove the cone from the stoma and close the top of the sleeve.
- After a few minutes water and stools will begin to flow into the irrigation sleeve. After the main flush, it is possible to flush out and bring the end of the sleeve to fix firmly in with the top of the sleeve, enabling you to get on with other things until you are sure that evacuation is complete. It can take up to 30 minutes to complete the evacuation. An opportunity to catch up with some reading.
- Wait about five minutes after everything appears to have been expelled, then remove the sleeve, wash and dry around the stoma and apply the usual stoma
cap or appliance. - Dispose of the sleeve in the usual way, or wash thoroughly and reuse. Wash cone and base plate with antibacterial cleansing soap, allow to dry and store until next time.
If it doesn’t work one day, try again the next day. Create a calm relaxed and undisturbed atmosphere and have another go. It is advisable to stop irrigating if there is illness or diarrhea, it can be resumed when you’re well.
Colostomy diet
In the first few weeks after having a colostomy, you’ll probably be advised to have a low-fiber diet.
This is because a high-fiber diet can increase the size of your stools, which can temporarily block your bowel. After around eight weeks, you’ll usually be able to go back to a normal diet.
As you recover, you can start to eat a healthy, balanced diet that includes plenty of fresh fruit and vegetables.
You should be able to return to the diet you previously enjoyed. If you previously had a restricted diet, you should be able to reintroduce the restricted foods.
It is not necessary for people with a colostomy to follow a special diet unless they have been advised to do so by their doctor for another specific medical reason. Some people may find that certain foods cause problems i.e. too much fiber may cause loose motions or beans may cause excessive wind. However, this varies from person to person and many colostomy patients find they can eat anything. If a food is suspected of causing problems it is advisable to try it again at intervals, separated by at least a week, before eliminating it altogether.
Colostomy possible complications
There are a number of possible problems you may experience after having a colostomy.
Rectal discharge
If you’ve had a colostomy but your rectum and anus are intact, you may have some mucus discharge from your bottom. Mucus is produced by the lining of the bowel to help the passage of stools.
The lining of the bowel continues producing mucus, even though it no longer serves any purpose. The longer the remaining section of your bowel, the more likely you are to have rectal discharge.
The mucus can vary, from a clear “egg white” to a sticky, glue-like consistency. It can either leak out of your bottom or build up into a ball, which can become uncomfortable.
Some people have rectal discharge every few weeks, while others have several episodes a day.
- Contact your doctor if there’s blood or pus in the discharge – it may be a sign of infection or tissue damage.
Managing the discharge
You may find it helps if you sit on the toilet every day and push down as if passing a stool. This should remove any mucus and stop it building into a ball.
But some people find this difficult because surgery can reduce the sensation in the rectum. Contact your doctor if this is the case, as you may need further treatment.
Glycerine suppositories that you insert into your bottom can often help. When the capsules dissolve, they make the mucus more watery, so it’s easier to get rid of.
The mucus can sometimes irritate the skin around your bottom. Using a barrier skin cream should help. You may need to try a few before you find one that works for you. Ask your pharmacist for advice.
Some people find that eating certain foods increases mucus production. While there’s no scientific evidence to support this, you may want to try keeping a food diary for a few weeks to see whether certain foods could be linked to an increase in mucus production.
Parastomal hernia
A parastomal hernia is where the intestines push through the muscles around the stoma, resulting in a noticeable bulge under the skin.
To reduce your risk of getting a parastomal hernia:
- wear a support garment (belt or underwear)
- avoid heavy lifting and straining
- maintain a healthy weight – being overweight can place additional strain on your abdominal muscles
A parastomal hernia isn’t usually painful, but it may be more difficult to hold the colostomy appliance in place and change it.
Most hernias can be managed with the help and support of your stoma nurse. In some cases, surgery may be needed to repair the hernia. But the hernia can come back, even after surgery.
Stoma blockage
Some people develop a blockage in their stoma as the result of a build-up of food.
Signs of a blockage include:
- not passing many stools, or passing watery stools
- bloating and swelling in your tummy
- tummy cramps
- a swollen stoma
- nausea or vomiting, or both
If you think your stoma is blocked, you should:
- avoid eating solid food for the time being
- drink plenty of fluids
- massage your tummy and the area around your stoma
- lie on your back, pull your knees up to your chest, and roll from side to side for a few minutes
- take a warm bath for 15 to 20 minutes to help relax your tummy muscles
When to get medical help
After trying these steps, if there’s no improvement within two hours, you should contact your doctor or stoma nurse immediately as there’s a risk your colon could burst.
Or go to your nearest local accident and emergency (A&E) department at a hospital.
Preventing a stoma blockage
To reduce your risk of developing a stoma blockage:
- chew your food slowly and thoroughly
- drink plenty of fluids
- avoid eating large amounts of food at one time
Also, avoid eating foods known to cause blockages, such as corn, celery, popcorn, nuts, coleslaw, coconut macaroons, grapefruit, dried fruit, potato skins, apple skins, orange pith, and Chinese vegetables like bamboo shoots and water chestnuts.
Other possible complications
Other problems you can have after a colostomy include:
- skin problems – where the skin around the stoma becomes irritated and sore; your stoma care team will explain how to manage this
- stomal fistula – where a small channel or hole develops in the skin alongside the stoma; depending on the position of the fistula, appropriate bags and good skin management may be all that’s needed to treat this problem
- stoma retraction – where the stoma sinks below the level of the skin after the initial swelling goes down, which can lead to leakages because the colostomy bag doesn’t form a good seal; different types of pouches and appliances can help, although further surgery may sometimes be needed
- stoma prolapse – where the stoma comes out too far above the level of the skin; using a different type of colostomy bag can sometimes help if the prolapse is small, although further surgery may be required
- stomal stricture – where the stoma becomes scarred and narrowed; further surgery may be needed to correct it if there’s a risk of blockage
- stomal leakage – where digestive waste leaks from the colon on to the surrounding skin or within the abdomen; trying different bags and appliances (e.g. barrier rings, paste to fill in creases or crevices in the skin, or flange extenders) may help an external leak, but further surgery may be needed if the leak is internal
- stomal ischemia – where the blood supply to the stoma is reduced after surgery; further surgery may be needed
- rectal discomfort – after an operation to form a colostomy some people still experience the sensation of rectal fullness and feel as if they need to pass a motion in the normal way. Sitting on the toilet and relaxing the muscles in this area may provide some relief.
Other Medical Conditions
If a person with colostomy develops dementia this can be a challenge. However, if a person who already has dementia requires surgery to form a stoma, this can be even more problematic as they may be unable to learn or remember the techniques to cope with a stoma. They may also try to remove the bags. There are many different types of bag available and some are more difficult to remove. Consult your stoma care nurse for details. Wearing clothes which restrict access to the bag or a support garment may help.
Colostomy reversal
If you have a temporary colostomy, you’ll need another operation to reverse it at a later date.
A colostomy reversal will only be carried out when you’re in good health and have fully recovered from the effects of the initial operation. This will usually be at least 12 weeks after the initial colostomy surgery.
The reversal may need to be delayed for longer if you need further treatment, such as chemotherapy, or you haven’t recovered from the original operation.
But there’s no time limit for having a reversal, and some people live with their colostomy for several years before it’s reversed.
How a colostomy reversal is carried out
Closure of a loop colostomy or ileostomy is a reasonably simple procedure and in 95% of cases does not require any further incisions in the abdomen. A small rim of skin is cut around the stoma (about 2mm) and the incision is deepened until the abdominal cavity is reached. Once this has happened the bowel and abdominal cavity are checked to ensure that there is nothing still attached to the bowel. The bowel is then closed – either stitched by hand or stapled together.
Reversal of an end colostomy or ileostomy is more difficult because one end of the bowel that is to be rejoined is in the abdomen. This usually means that the surgeon has to open the abdomen via making a larger incision through the old scar so the surgeon can locate and reattach the two sections of colon. As a result of the increased surgery (compared to the closure of a loop stoma), there will be a longer stay in hospital and a greater recovery time before normal activities can be resumed and there’s a greater risk of complications.
However, it is possible to reverse an end colostomy using keyhole surgery (laparoscopy), but this is dependent on a surgeon’s training. Even when this attempted, there is no guarantee that it won’t be necessary to convert to the open operation, as the aforementioned adhesions can cause severe problems laparoscopically. If this type of surgery is carried out successfully then it is likely that there will be less post–operative pain and a shorter stay in hospital.
How long in hospital?
Length of hospital stay depends on the type of operation performed. For the closure of a loop colostomy it will be around 3 to 5 days. For the closure of an end colostomy you can expect a stay of between 5 and 10 days. Most people are well enough to leave hospital 3 to 10 days after having colostomy reversal surgery. The surgeons caring for you will want to be sure that you cope with your bowel movements once again, as it is fairly common to pass looser and more frequent stools than you may have been used to in the past. They will also want to ensure that the area where the join (anastomosis) was formed has not narrowed (strictured) as a result of scarring, as this can lead to a partial or full blockage of the bowel. If this happens, then it may be necessary to have the area stretched. This is normally carried out using a colonoscope (See colonoscopy).
Recovering from a colostomy reversal
It’s likely to take some time before your bowel movements return to normal. Some people have constipation or diarrhea, but this usually gets better with time.
You may have a sore bottom after the reversal, but this should improve as you get used to passing stools through your anus again.
After every bowel movement, it may help if you:
- wash the skin around your anus with warm water
- pat it dry with a soft cloth
- apply a barrier cream
Avoid using baby wipes, talcum powder or scented toilet tissues as they can cause further irritation. If these measures prove inadequate then you should contact your stoma care nurse for specialist advice.
Other possible problems include needing to go to the toilet more often or more urgently than usual, excessive wind (flatulence), and some bowel incontinence or leakage.
Although a colostomy reversal is usually a smaller procedure than the initial colostomy operation, it still takes several weeks to recover and return to normal activities.
When you get home, your return to normal activities will be determined by your physical condition before the operation and, again, on the type of operation you had. It can be at least ten weeks before you are able to lift heavy weights or fully use your abdominal muscles. Driving will be allowed only when you can perform an emergency stop without any pain, or fear of pain.
Initially, your diet might require adjustment. The period after a reversal can be similar to the time the stoma was originally formed, with loose bowels and sudden urges to go. Some people develop inflammation of the lower part of the colon. This sometimes occurs when part of the colon hasn’t been used for time. This can lead to loose stools, with some bleeding and mucus, but this usually settles down without the need for treatment.
What to eat after a colostomy reversal
Your digestive system may be sensitive after a colostomy reversal. It may help to avoid eating large meals and eating late at night, and to eat little and often.
Certain foods are also more likely to irritate the gut.
It may help to limit or avoid:
- citrus fruits – such as grapefruits and oranges
- spicy food – such as curries
- large fatty meals
- vegetables that increase flatulence – such as cabbage, Brussel sprouts and onions
- large amounts of alcohol or fizzy drinks
Anti–diarrhea medication, softeners, or bulking agents may be required to improve consistency.
Bowel function following stoma reversal
It takes time for bowel function to settle into some sort of pattern. How long varies from person to person, as does the perception of what is satisfactory function.
During the first few weeks following a reversal, bowel function can be erratic.
The following are quite common at first:
- Loose motions (which can swing to constipation).
- Going to the toilet to pass feces more frequently.
- Having some degree of urgency when going to the toilet.
- Difficult determining wind from a motion.
- Sore skin around the back passage (anus).
It is often difficult to predict exactly how problematic bowel function will be. It is not usually due to the type of stoma that you had, but more likely to be:
- The amount of colon and/or rectum removed.
- Treatments and the health of the remaining colon and/or rectum.
- Other previous pelvic surgery and/or any previous or co–existing pelvic disease.
- The distance of the join in the colon/rectum from the back passage.
- Capability of anal sphincters.
- Personal perceptions about whether function is satisfactory.
The reasons why the above occur are many. Having an understanding of these will be useful when discussing the possibility of a reversal with your surgeon and making a decision about whether to proceed.
Feces enters the colon as a liquid and one of the main functions of the colon is to re–absorb water back into the body. When a significant section of the colon is removed, the consistency of waste matter will become more liquid. This may in turn result in the need for more frequent toilet visits and, with this, concerns regarding control. Exercises which build up and strengthen the anal sphincter muscles can help in preventing the leakage of gas and stools from the back passage.
Treatments such as chemotherapy and radiotherapy to the pelvis can delay the return of acceptable bowel function. In some cases the damage may make function more unpredictable and for some it may be painful.
Previous pelvic disease or abdominal surgery may make stoma reversal difficult and may also affect long–term function.
The use of stapling guns for rejoining bowel has allowed surgeons to make a lower join (anastomosis) in the rectum, thus reducing the necessity to remove the back passage and form a permanent colostomy. However, this can have an impact on subsequent bowel function and control. The rectum acts as a reservoir or ‘holding area’ for feces. When a significant portion is removed and the scar line is close to the sphincter muscles, what is commonly known as anterior resection syndrome can result. It is characterized by the following symptoms:
- Increased frequency.
- Urgency and a feeling of the need to defecate.
- Fragmentation of the motion (a feeling of not having completed passing feces).
- Inability to distinguish ‘wind’ from motion resulting in soiling or possible incontinence.
The above settles down for most people, but can take a significant time to do so. Childbirth, age and trauma are just some of the processes that can have a detrimental effect on sphincter control in general. If the initial stoma surgery causes a looser output or reduces ‘holding’ capacity, then control of bowel function following a reversal can be more difficult. Pelvic floor and sphincter exercises to aid bowel control can help.
Colostomy reversal possible complications
All surgery carries risks, but fortunately life–threatening complications with stoma reversals are rare. As with any surgery there will be general complications that can arise from undergoing a surgical procedure. Your surgeon will discuss these with you before your operation. There are also some that are specific to stoma reversals:
- Ileus (temporary paralysis of the bowel)
Sometimes the bowel is slow to start working after surgery, particularly if it has been handled by the surgeon. Disturbances in your body’s salt balance and some pain medications can also increase the risk of this occurring. If this happens the bowel will need to be rested, which involves stopping food and taking minimal amounts of water. Fluid given via a vein (a drip) is used to replace fluids and you may need a tube down your nose to your stomach (nasogastric tube) which decompresses the bowel and helps it to start up again.
- Bowel obstruction
If there is a physical blockage or problems with adhesions causing a blockage another operation may be required. Fortunately this type of physical blockage is rare immediately after an operation.
- Anastomotic leak (breakdown of the join in your bowel)
If this is suspected you will be started on antibiotics and it is likely that another operation will be required. However, this complication can take a controlled form, whereby an abscess forms. If this is the case there may not be a need for surgical intervention, as it may be possible to control it with antibiotics and drainage under X–ray guidance.
- Urinary and sexual function
This may be affected temporarily but the risk of this being permanent is higher in surgery to reconnect an end colostomy, as the nerves controlling these functions lie in this region.
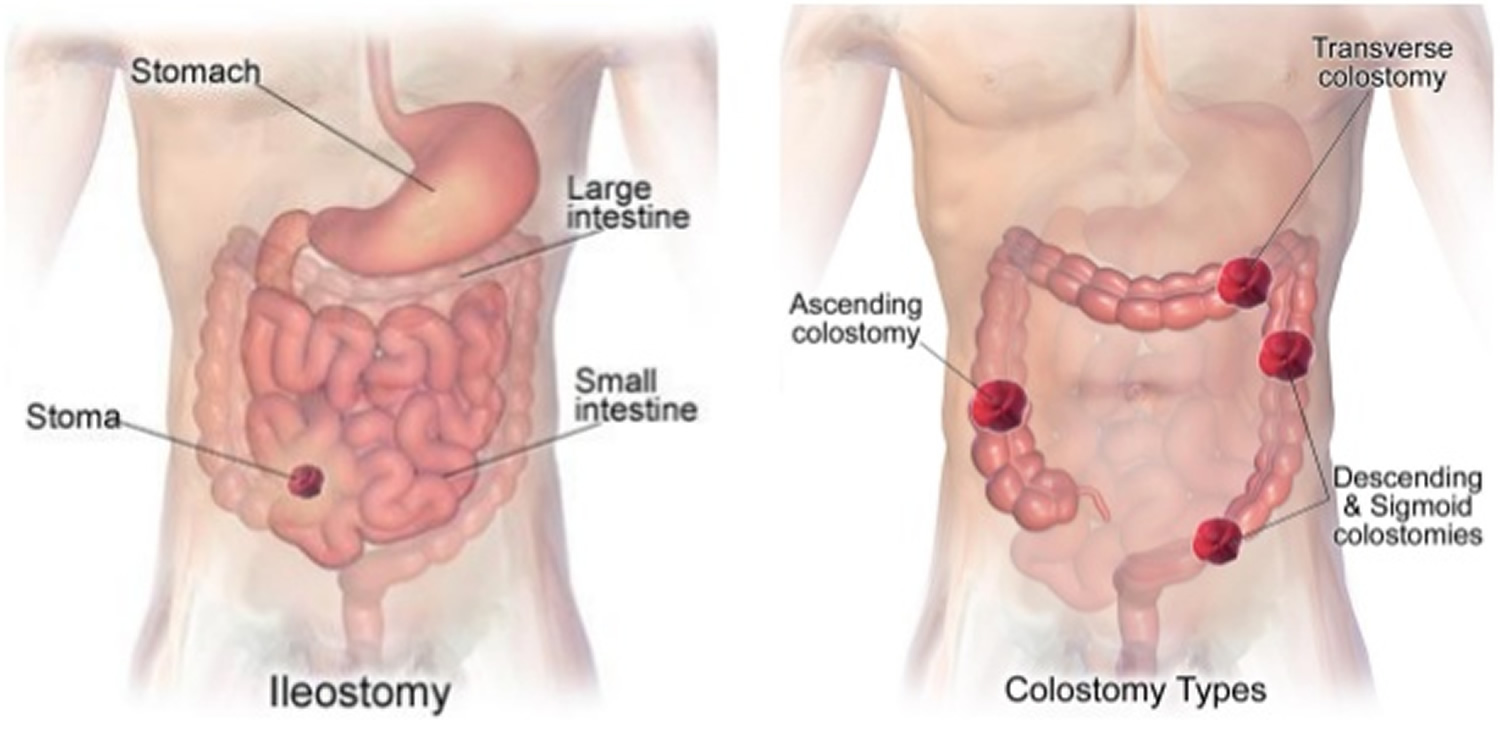
Ileostomy vs Colostomy
An ileostomy is a surgically made opening on the skin of the belly where the small bowel (small intestine) is diverted through an opening in the tummy (abdomen). An ileostomy replaces the rectum as the place where waste of the digestive system (stool) leaves the body. Stool that comes from your ileostomy is thin or thick liquid. It is not solid like the stool that came from your rectum. An ileostomy may be needed if the colon is damaged, inflamed or doesn’t work properly.
Most often the colon (large intestine) absorbs most of the water that you eat and drink. With an ileostomy in place, the colon is no longer being used. This means that the stool from your ileostomy has far more liquid than a typical bowel movement from the rectum.
The stool now comes out from the ileostomy and empties into a pouch that is attached to the skin around your stoma. The pouch is made to fit your body well. You must wear it all the time.
The waste that collects will be liquid or pasty, depending on what you eat, what medicines you take, and other things. Waste collects constantly, so you will need to empty the pouch 5 to 8 times a day.
When is an ileostomy needed?
Ileostomies are formed to either temporarily or permanently stop digestive waste passing through the full length of the small intestine or colon.
There are a number of reasons why this may be necessary, including:
- to allow the small intestine or colon to heal after it’s been operated on – for example, if a section of bowel has been removed to treat bowel cancer
- to relieve inflammation of the colon in people with Crohn’s disease or ulcerative colitis
- to allow for complex surgery to be carried out on the anus or rectum
Crohn’s disease
Crohn’s disease is a long-term condition where the digestive system becomes inflamed. Common symptoms include:
- diarrhea
- abdominal pain
- extreme tiredness (fatigue)
Crohn’s disease can usually be controlled with medication, but surgery to create an ileostomy may sometimes be recommended to temporarily divert digestive waste away from the inflamed section of the digestive system to give it a chance to heal.
Ulcerative colitis
Ulcerative colitis is a long-term condition where the lining of the large intestine or large bowel (colon or rectum) becomes inflamed. Common symptoms include:
- bloody diarrhea
- abdominal pain
- a frequent need to pass stools
In most cases symptoms can be controlled with medication. However, surgery to remove the colon and form an ileostomy or ileo-anal pouch – an internal pouch to store stools created using the end of the small intestine – may be recommended if the condition is particularly severe or doesn’t respond to medication.
Bowel cancer
Bowel cancer is a type of cancer that develops inside the colon or rectum. Chemotherapy or radiotherapy, or a combination of both, may be used to shrink the cancer first, before the affected section of bowel is removed.
Depending on the size and position of the removed section of bowel, a temporary ileostomy, permanent ileostomy, or an ileo-anal pouch may be formed during the operation.
In some cases, a section of your colon may need to be diverted out of your tummy (abdomen). This is known as a colostomy, rather than an ileostomy.
Less common uses
Some of the less common reasons why surgery to form an ileostomy is needed are described below.
Familial adenomatous polyposis
Familial adenomatous polyposis (FAP) is a rare condition that triggers the growth of non-cancerous lumps of tissue inside the colon.
Although the lumps are non-cancerous to begin with, there’s a very high risk that, over time, at least one will turn cancerous. More than 99% of people with FAP have bowel cancer by the time they’re 50 years old.
Because of the high risk of developing cancerous lumps, it’s usually recommended that a person diagnosed with FAP has their colon removed. It’s usually replaced with an ileo-anal pouch, or occasionally a permanent ileostomy.
Bowel obstruction
A bowel obstruction occurs when part of the digestive system becomes blocked by food, fluids, or waste products. This can happen if part of the person’s digestive system is scarred or inflamed, or if their digestive system is unusually narrow.
If the colon becomes completely blocked, it’s usually necessary to remove the colon and form an ileostomy. This can be temporary or permanent, depending on the underlying cause of the obstruction.
Injury
A significant injury to the colon, such as a puncture or impact injury, can result in the colon becoming permanently damaged.
In these cases, it may be necessary to remove the colon and form an ileostomy. Whether this is a temporary or permanent ileostomy depends on the type and extent of the injury.
Figure 18. Ileostomy vs Colostomy
How ileostomy is performed
There are several different ways an ileostomy can be formed, depending on the reason why the operation is being carried out.
The opening in your tummy (abdomen) where waste material exits the body after the operation (stoma) will normally be located on the righthand side.
However, you’ll usually meet a specialist stoma nurse before the operation to discuss specific possible locations. The stoma nurse may draw a dot on your abdomen to let the surgeon know where the preferred site is.
Ileostomy operations are carried out under general anesthetic, which means you’ll be asleep during the procedure and won’t experience any pain as it’s carried out.
The main types of ileostomy are described below.
Figure 19. Ileostomy types
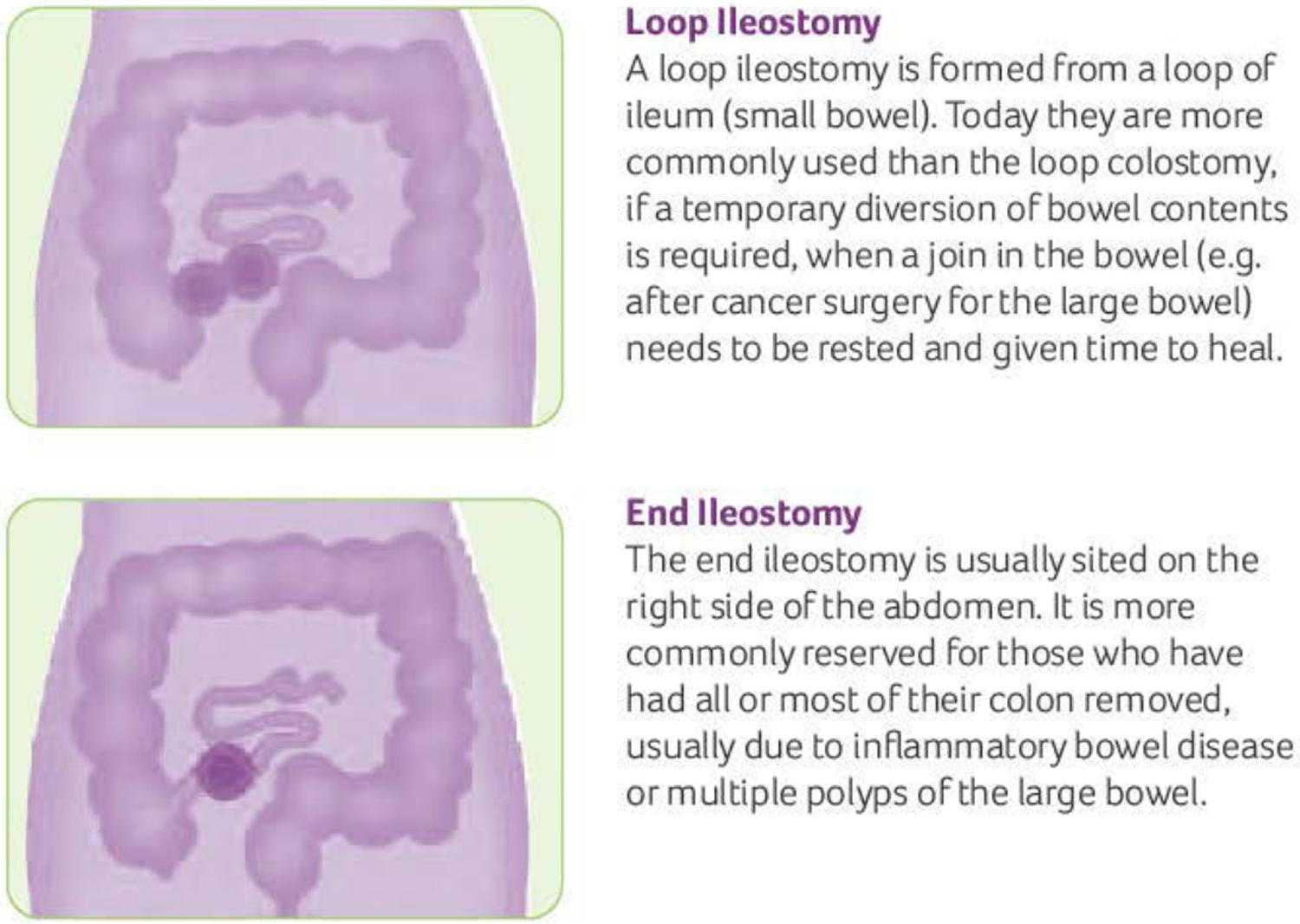
Loop ileostomy
To form a loop ileostomy, a loop of small intestine is pulled out through a cut (incision) in your abdomen.
This section of intestine is then opened up and stitched to the skin to form a stoma. The colon and rectum are left in place.
In these cases, the stoma will have two openings, although they’ll be close together and you may not be able to see both.
One of the openings is connected to the functioning part of your bowel. This is where waste products leave your body after the operation.
The other opening is connected to the “inactive” part of your bowel that leads down to your rectum.
The loop ileostomy is usually temporary and may be reversed during a second operation at a later date.
There’s no time limit for having an ileostomy reversed and some people may live with one for several years before it’s reversed.
Reversing a loop ileostomy is a relatively straightforward procedure that’s carried out under general anesthetic.
A cut (incision) is made around the stoma and the section of small intestine is pulled out of the tummy (abdomen). The area that had been divided to form the stoma is then stitched back together and placed back inside the abdomen.
End ileostomy
An end ileostomy normally involves removing the whole of the colon (large intestine) through an incision in your abdomen.
The end of the small intestine (ileum) is divided and brought out of the abdomen through a smaller incision, and stitched on to the skin to form a stoma.
Over time, the stitches dissolve and the stoma heals on to the skin. After the operation, waste material comes out of the opening in the abdomen into a bag that goes over the stoma.
This type of ileostomy is often, but not always, permanent.
It’s sometimes possible to reverse an end ileostomy if most of the large intestine (colon) has been sealed and left inside the abdomen.
However, the surgeon will need to make a larger incision to locate and reattach the small and large intestines. It therefore takes longer to recover from this type of surgery and there’s a greater risk of complications.
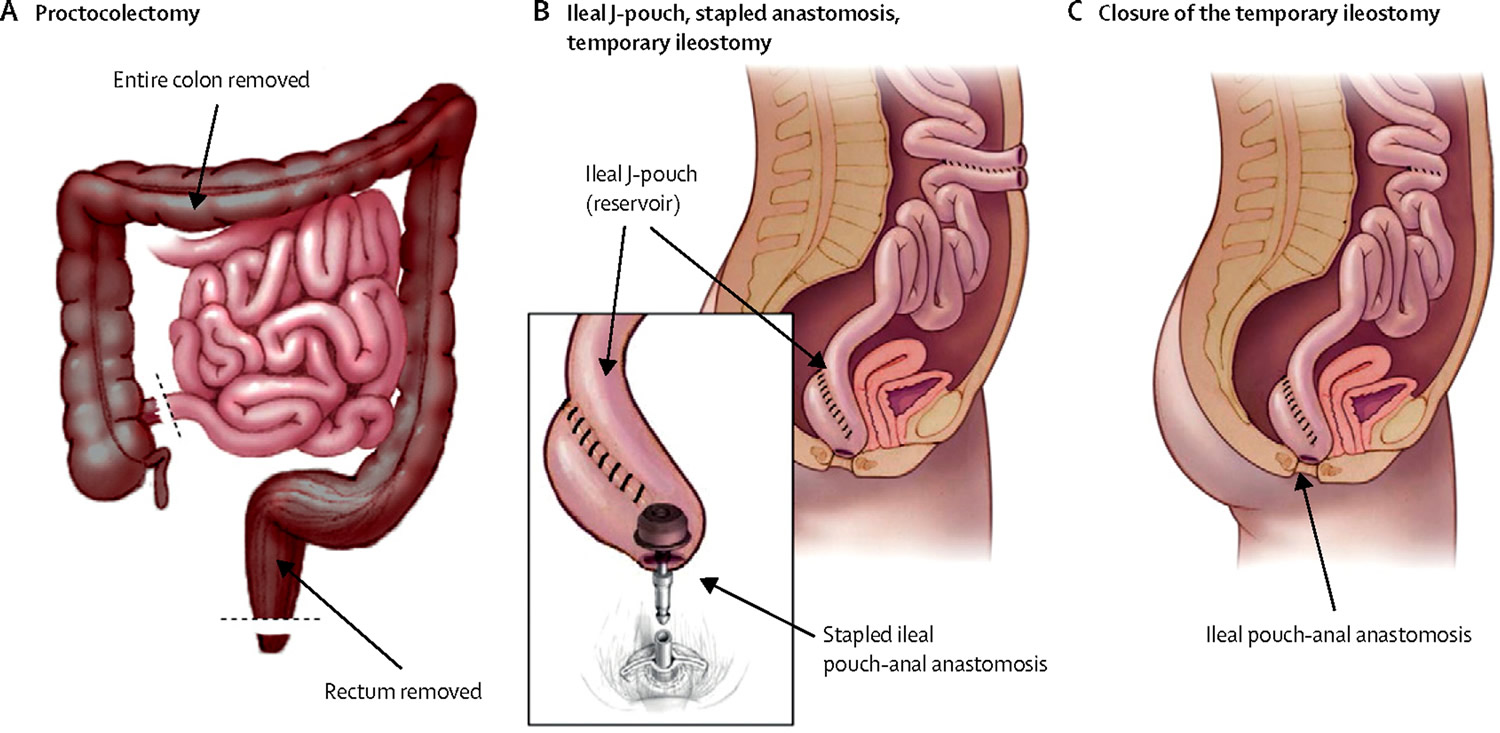
Continent Ileostomy (Ileo-anal) pouch
In some cases, it may be possible to have a permanent internal ileo-anal pouch, also known as a J pouch, formed instead of an ileostomy.
An ileo-anal pouch is created from the ileum (the end of the small intestine) and joined to the anus, so waste material passes out of your body in the normal way. The pouch stores the waste material until you excrete it when you go the toilet.
The area around the pouch usually needs to heal before it’s used, so a temporary loop ileostomy may be created above the pouch. A second, smaller operation is usually carried out a few months later to close the loop ileostomy.
Figure 20. Ileoanal anastomosis (J pouch surgery)
Ileostomy procedure recovery
After an ileostomy procedure, you’ll need to stay in hospital for a few days while you recover.
When you wake up after the operation, you may be attached to a drip placed directly into your vein that provides fluids (an intravenous drip) and have an oxygen mask or nasal tubes (cannula) to help you breathe. These will be removed as you recover.
A special bag is also placed over the opening in your abdomen (stoma). The stoma will initially appear large because the effects of surgery cause it to swell. It usually shrinks during the weeks after the operation, reaching its final size after about eight weeks.
Living with an ileostomy
Whilst the diet, the equipments, exercise, activities and stoma care are similar between ileostomy and colostomy, dehydration could become a problem for people with ileostomy. Since you no longer have a large intestine (colon), you’re at greater risk from dehydration. This is because one of the functions of the colon is to reabsorb water and minerals back into the body.
It’s therefore important to drink plenty of water if you have an ileostomy, particularly in hot weather or during periods where you’re more active than normal. Sachets of fluid replacement solutions to help reduce dehydration are also available from pharmacies.
Short bowel syndrome
This condition happens when surgery is done to remove a large part of the small intestine. Short bowel syndrome needs special attention because there’s not enough intestine left to absorb the nutrients the body needs.
People with short bowel syndrome must be under a doctor’s care. They must be closely watched to make sure they’re taking in enough calories, carbohydrates, proteins, fats, vitamins, and minerals. They can live a normal life, but must be careful to avoid diarrhea, and be within quick reach of medical care. The shorter the small intestine, the more watery the discharge will be. This may reduce the time a pouch can be worn because the skin barrier breaks down more rapidly.
Living with an Continent Ileostomy (ileo-anal) pouch
Living with an ileo-anal pouch is different from living with an ileostomy because the procedure doesn’t involve creating a stoma in the tummy (abdomen). Instead, digestive waste is stored in an internal pouch and excreted through the rectum and anus.
If you’ve had an ileo-anal pouch, you may find you need to empty it up to 20 times a day during the first few days after the operation.
However, the number of times you need to go to the toilet will slowly reduce as the pouch expands and you get used to controlling muscles that surround it.
Most people find their pouch activity settles down after 6 to 12 months, although the number of bowel movements will differ from person to person.
Improving muscle control
Exercising the muscles that control the passing of stools (pelvic floor muscles) can help make going to the toilet easier if you have an ileo-anal pouch. It can also reduce the likelihood of accidental leaks during the first few weeks after the operation.
Pelvic floor exercises, as outlined below, are a good way of improving your muscle control:
- sit or lie comfortably with your knees slightly apart
- without moving your abdominal muscles, squeeze the muscle around the back passage as if you’re trying to stop passing wind
- hold this contraction as long as you can – at least two seconds, increasing up to 10 seconds as you improve
- relax for the same amount of time before repeating
Ideally aim for 10 short, fast and strong contractions.
Anal soreness
Anal soreness or itchiness is common in people with an ileo-anal pouch. Having regular baths should help to relieve this. Using a skin protection cream is also recommended. Your doctor will be able to advise you about the best cream for you.





{kind=link}