Contents
Cranial nerves
The cranial nerves contain the sensory and motor nerve fibers that innervate the head. The cell bodies of the sensory neurons lie either in receptor organs (e.g., the nose for smell, or the eye for vision) or within cranial sensory ganglia, which lie along some cranial nerves (V, VII–X) just external to the brain. The cranial sensory ganglia are directly comparable to the dorsal root ganglia on the spinal nerves. The cell bodies of most cranial motor neurons occur in cranial nerve nuclei in the ventral gray matter of the brain stem—just as cell bodies of spinal motor neurons occur in the ventral gray matter of the spinal cord.
The twelve cranial nerves and the origins of their names are briefly described below.
- I. Olfactory. This is the sensory nerve of smell.
- II. Optic. Because it develops as an outgrowth of the brain, this sensory nerve of vision is not a true nerve at all. It is more correctly called a brain tract.
- III. Oculomotor. The name oculomotor means “eye mover.” This nerve innervates four of the extrinsic eye muscles—muscles that move the eyeball in the orbit.
- IV. Trochlear. The name trochlear means “pulley.” This nerve innervates an extrinsic eye muscle that hooks through a pulley-shaped ligament in the orbit.
- V. Trigeminal. The name trigeminal means “threefold,” which refers to this nerve’s three major branches. The trigeminal nerve provides general sensory innervation to the face and motor innervation to the chewing muscles.
- VI. Abducens. This nerve was so named because it innervates the muscle that abducts the eyeball (turns the eye laterally).
- VII. Facial. This nerve innervates the muscles of facial expression as well as other structures.
- VIII. Vestibulocochlear. This sensory nerve of hearing and equilibrium was once called the auditory nerve.
- IX. Glossopharyngeal. The name glossopharyngeal means “tongue and pharynx,” structures that this nerve helps to innervate.
- X. Vagus. The name vagus means “wanderer.” This nerve “wanders” beyond the head into the thorax and abdomen.
- XI. Accessory. This nerve was once called the spinal accessory nerve. It originates from the cervical region of the spinal cord, enters the skull through the foramen magnum, and exits the skull with the vagus nerve. The accessory nerve carries motor innervation to the trapezius and sternocleidomastoid muscles.
- XII. Hypoglossal. The name hypoglossal means “below the tongue.” This nerve runs inferior to the tongue and innervates the tongue muscles.
Based on the types of fibers they contain, the 12 cranial nerves can be classified into three functional groups:
1. Primarily or exclusively sensory nerves (I, II, VIII) that contain special sensory fibers for smell (I), vision (II), and hearing and equilibrium (VIII).
2. Primarily motor nerves (III, IV, VI, XI, XII) that contain somatic motor fibers to skeletal muscles of the eye, neck, and tongue.
3. Mixed (motor and sensory) nerves (V, VII, IX, X). These mixed nerves supply sensory innervation to the face (through general somatic sensory fibers) and to the mouth and viscera (general visceral sensory), including the taste buds for the sense of taste (special visceral sensory). These nerves also innervate pharyngeal arch muscles (somatic motor), such as the chewing muscles (V) and the muscles of facial expression (VII).
Additionally, four of the cranial nerves (III, VII, IX, X) contain visceral motor fibers that regulate visceral muscle and glands throughout much of the body. These motor fibers belong to the parasympathetic division of the autonomic nervous system. The autonomic nervous system innervates body structures through chains of two motor neurons. The cell bodies of the second neurons occupy autonomic motor ganglia in the peripheral nervous system. The location of these peripheral autonomic ganglia are described in the pathway of these four nerves.
Cranial nerves are traditionally classified as sensory (I, II, VIII), motor (III, IV, VI, XI, XII), or mixed (V, VII, IX, X). In reality, only cranial nerves I and II (for smell and vision) are purely sensory, whereas all of the rest contain both afferent and efferent fibers and are therefore mixed nerves. Those traditionally classified as motor not only stimulate muscle contractions but also contain sensory fibers of proprioception, which provide the brain with feedback for controlling muscle action and make one aware of such things as the position of the tongue and orientation of the head. Cranial nerve VIII, concerned with hearing and equilibrium, is traditionally classified as sensory, but it also has motor fibers that return signals to the inner ear and tune it to sharpen the sense of hearing. The nerves traditionally classified as mixed have sensory functions quite unrelated to their motor functions. For example, the facial nerve (VII) has a sensory role in taste and a motor role in controlling facial expressions.
Figure 1. 12 Cranial nerves

Cranial nerves mnemonic
The following mnemonic phrase can help you remember the first letters of the names of the 12 cranial nerves in their proper order:
“Oh, Oh, Oh, To Touch And Feel Very Good Velvet, AH!”
Cranial nerves function
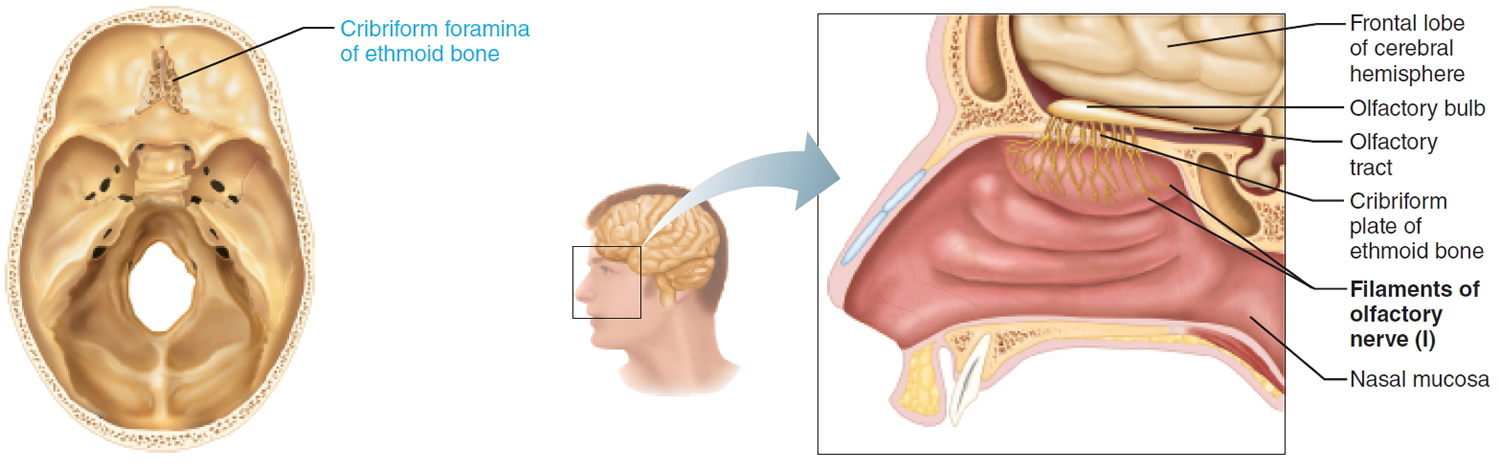
I. Olfactory Nerve
This is the nerve for the sense of smell. It consists of several separate fascicles that pass independently through the cribriform plate in the roof of the nasal cavity. It is not visible on brains removed from the skull because these fascicles are severed by removal of the brain.
Sensory function: Special visceral sensory, sense of smell.
Effect of Damage: Impaired sense of smell. Fracture of the ethmoid bone or lesions of olfactory fibers may result in partial or total loss of smell, a condition known as anosmia
Origin Olfactory receptor cells (bipolar neurons) in the olfactory epithelium of the nasal cavity.
Pathway: Pass through the cribriform foramina of the ethmoid bone to synapse in the olfactory bulb. Fibers of olfactory bulb neurons extend posteriorly beneath the frontal lobe as the olfactory tract. Terminate in the primary olfactory cortex of the cerebrum.
Figure 1. Olfactory nerve (Cranial nerve 1)
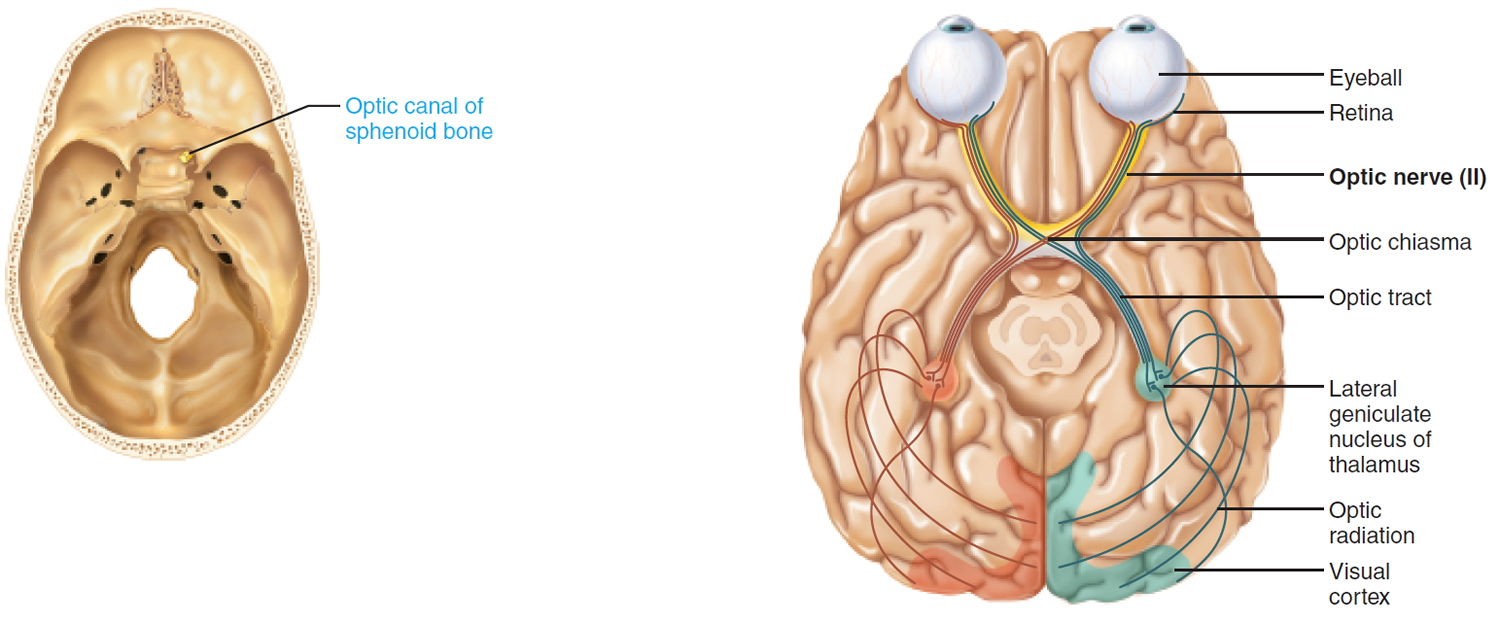
II. Optic Nerve
This is the nerve for vision.
Sensory function: Special somatic sensory, vision.
Effect of Damage: Damage to an optic nerve results in blindness in the eye served by the nerve; damage to the visual pathway distal to the optic chiasma results in partial visual losses; visual defects are called anopsias.
Origin: Retina of the eye.
Pathway: Pass through the optic canal of the sphenoid bone. Optic nerves converge to form the optic chiasma, where fibers partially cross over, then continue as the optic tracts to synapse in the thalamus. Thalamic fibers project to and terminate in the primary visual cortex in the occipital lobe.
Figure 2. Optic nerve (Cranial nerve 2)
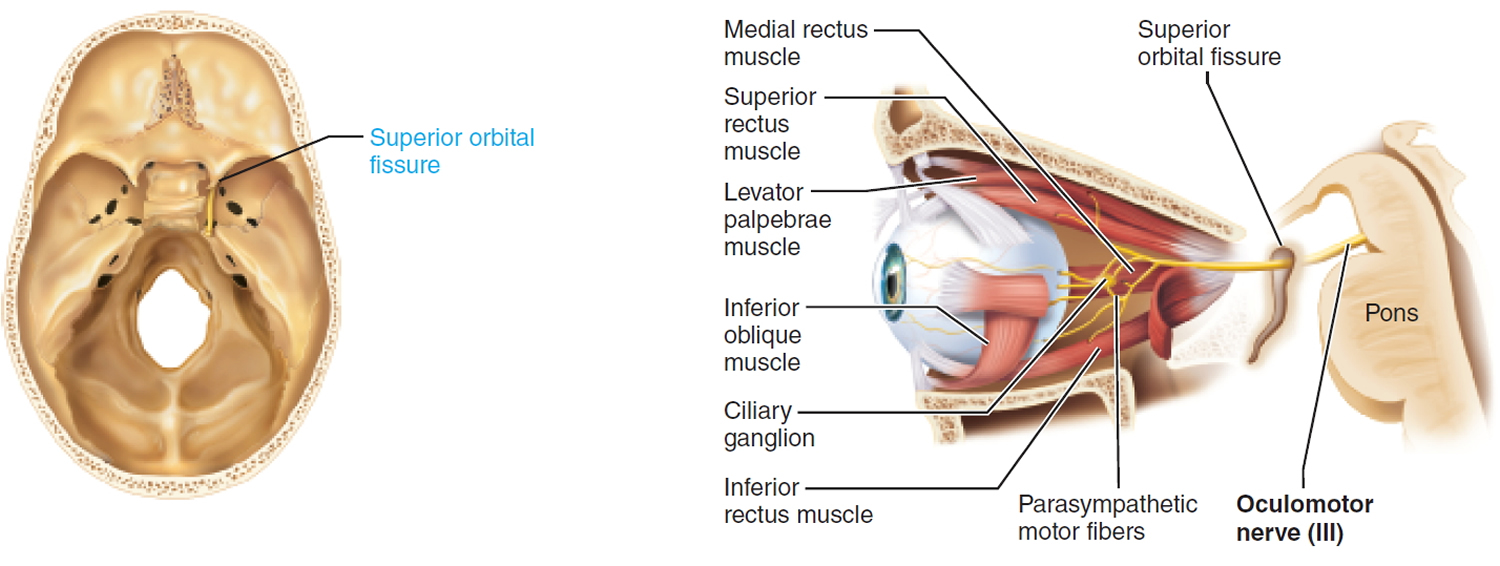
III. Oculomotor Nerve
This is the nerve for vision.
Somatic motor function: Innervate four extrinsic eye muscles that direct the eyeball: superior rectus, medial rectus, inferior rectus, inferior oblique muscles. Innervate levator palpebrae superioris muscle that elevates the upper eyelid. Afferent proprioceptor fibers return from the extrinsic eye muscles.
Visceral motor function (parasympathetic): Constrictor muscles of the iris constrict the pupil. Ciliary muscle controls lens shape.
Effect of Damage: Because the actions of the two extrinsic eye muscles not served by cranial nerve III are unopposed, the eye cannot be moved up or inward, and at rest the eye turns laterally (external strabismus). The upper eyelid droops (ptosis), and the person has double vision.
Origin: Oculomotor nuclei in the ventral midbrain.
Pathway: Pass through the superior orbital fissure to enter the orbit. Parasympathetic fibers from the brain stem synapse with post ganglionic neurons in the ciliary ganglion that innervate the iris and ciliary muscle.
Figure 3. Oculomotor nerve (Cranial nerve 3)
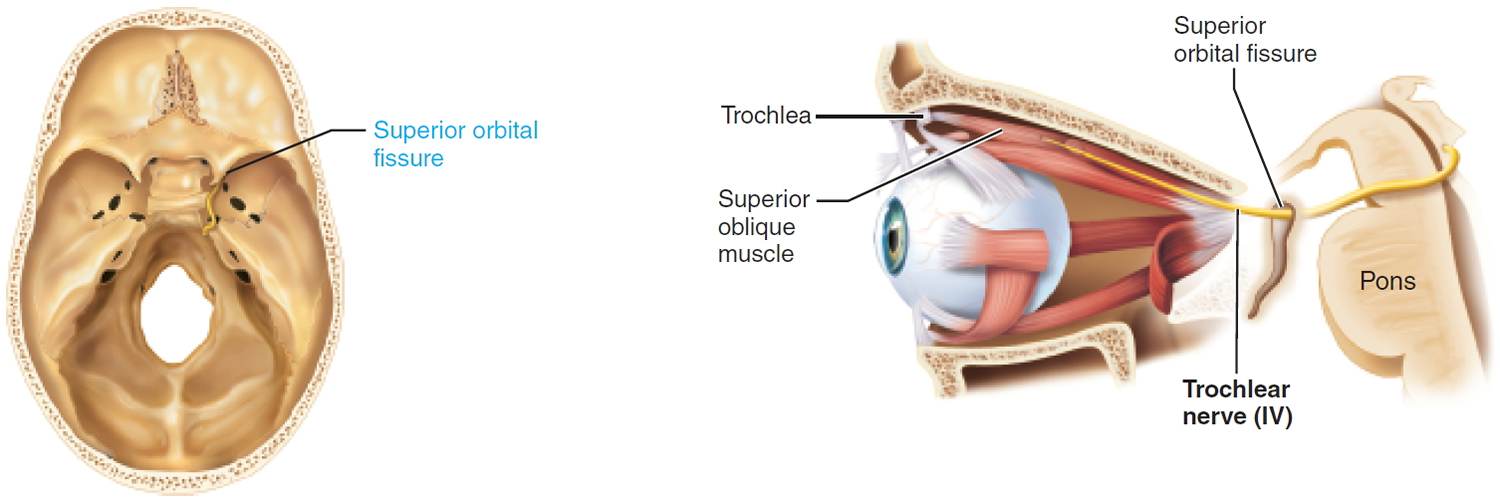
IV. Trochlear Nerve
This is the nerve for vision.
Somatic motor function: Innervate the superior oblique muscle. This muscle passes through a ligamentous pulley at the roof of the orbit, the trochlea, from which its name is derived. Afferent proprioceptor fibers return from the superior oblique.
Effect of Damage: Damage to a trochlear nerve results in double vision and reduced ability to rotate the eye inferolaterally.
Origin: Trochlear nuclei in the dorsal midbrain.
Pathway: Pass ventrally around the midbrain; pass through the superior orbital fissure to enter the orbit.
Figure 4. Trochlear nerve (Cranial nerve 4)
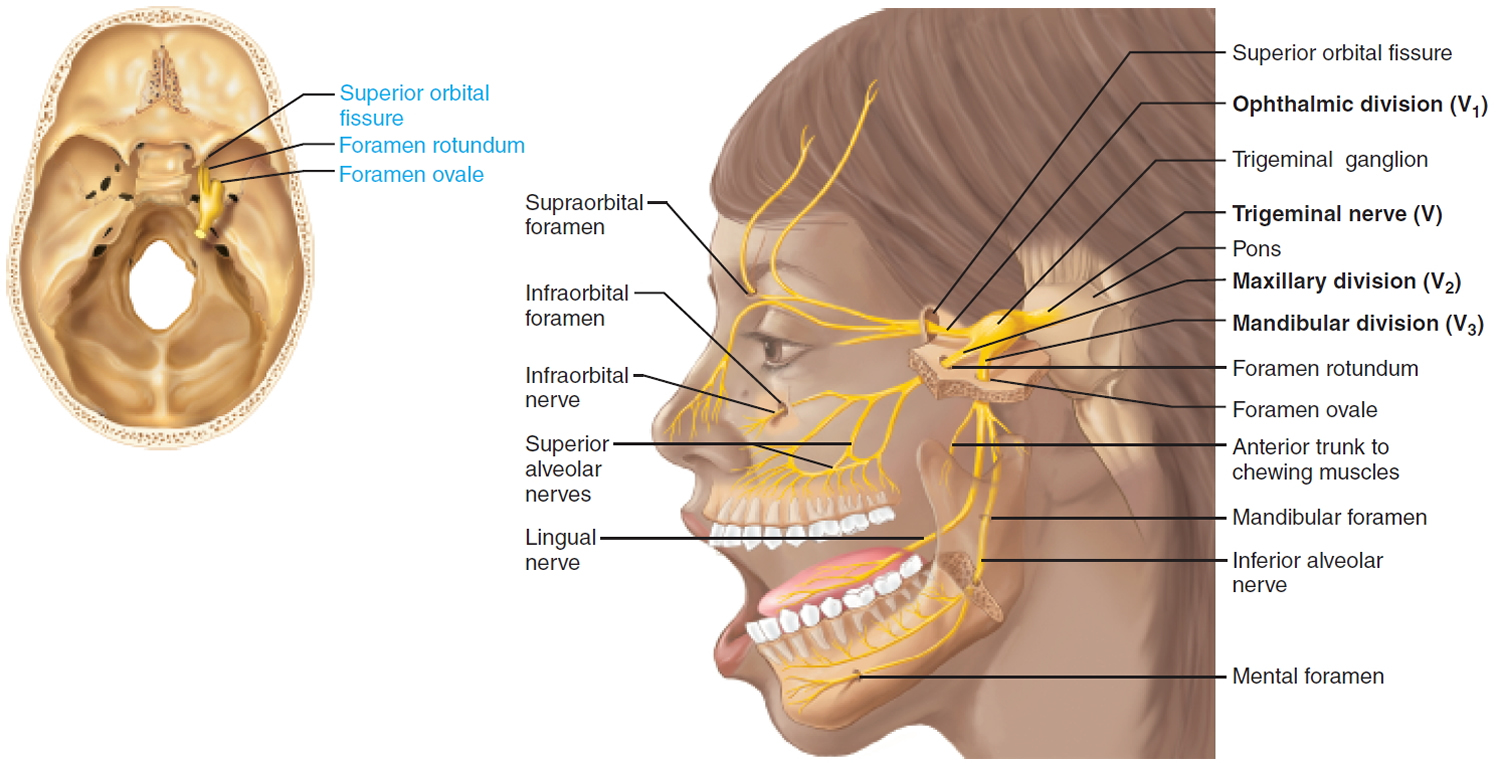
V. Trigeminal Nerve
The large trigeminal nerve forms three divisions (trigeminal = threefold): ophthalmic (V1), maxillary (V2), and mandibular (V3) divisions.
This mixed nerve is the general somatic sensory nerve of the face for touch, temperature, and pain. The mandibular division supplies somatic motor innervation to the chewing muscles.
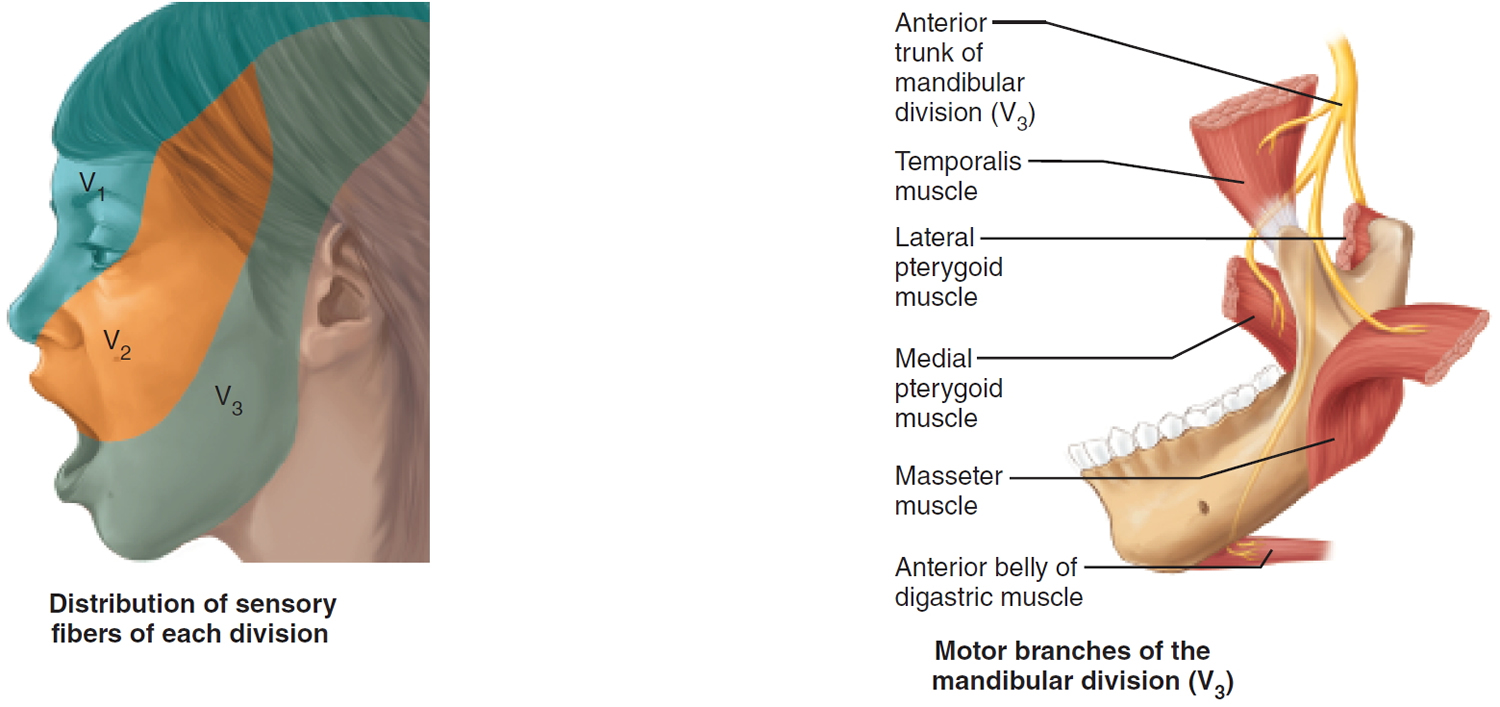
Sensory function:
- V1 General somatic sensation from skin of anterior scalp and forehead, upper eyelid and nose, nasal cavity mucosa, cornea, and lacrimal gland.
- V2 General somatic sensation from skin of cheek, upper lip, and lower eyelid, nasal cavity mucosa, palate, upper teeth.
- V3 General somatic sensation from skin of chin and temporal region of scalp, anterior tongue and lower teeth.
Somatic motor function: V3 Innervate the muscles of mastication: temporalis, masseter, pterygoids, anterior belly of digastric. Afferent proprioceptor fibers return from these muscles.
Clinical significance: Anesthesia for Upper and Lower Jaws. Dentists desensitize upper and lower jaws by injecting local anesthetic (such as Novocain) into alveolar branches of the maxillary and mandibular divisions of the trigeminal nerve, respectively. This blocks pain-transmitting fibers from the teeth, and the surrounding tissues become numb.
Origin: Sensory receptors in skin and mucosa of face. Motor fibers from trigeminal motor nucleus in pons.
Pathway: Cell bodies of sensory neurons of all three divisions located in the large trigeminal ganglion. Fibers extend to trigeminal nuclei in the pons.
Through the Skull: V1 Superior orbital fissure. Cutaneous Branch: Supraorbital foramen.
Through the Skull: V2 Foramen rotundum. Cutaneous Branch: Infraorbital foramen.
Through the Skull: V3 Foramen ovale and Mandibular foramen. Cutaneous Branch: Mental foramen.
Figure 5. Trigeminal nerve (Cranial nerve 5)
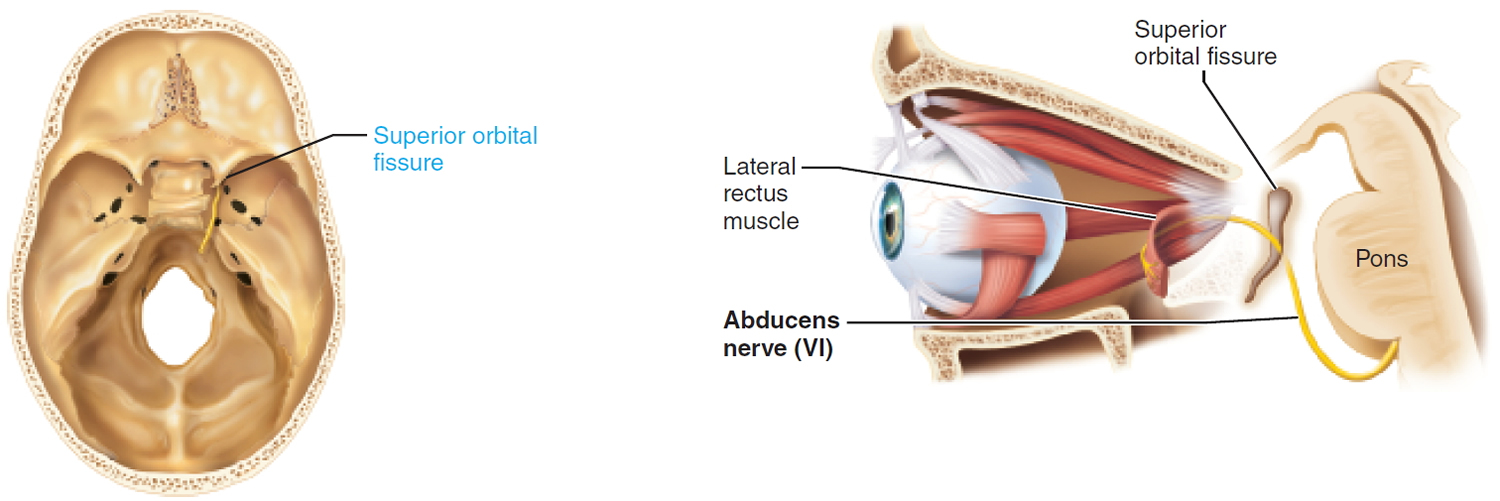
VI. Abducens Nerve
Somatic motor function: Innervate the lateral rectus muscle. This muscle abducts the eye. Afferent proprioceptor fibers return from the lateral rectus.
Effect of Damage: In abducens nerve paralysis, the eye cannot be moved laterally; at rest, affected eyeball turns medially (internal strabismus).
Origin: Abducens nuclei in the inferior pons.
Pathway: Pass through the superior orbital fissure to enter the orbit.
Figure 6. Abducens nerve (Cranial nerve 6)
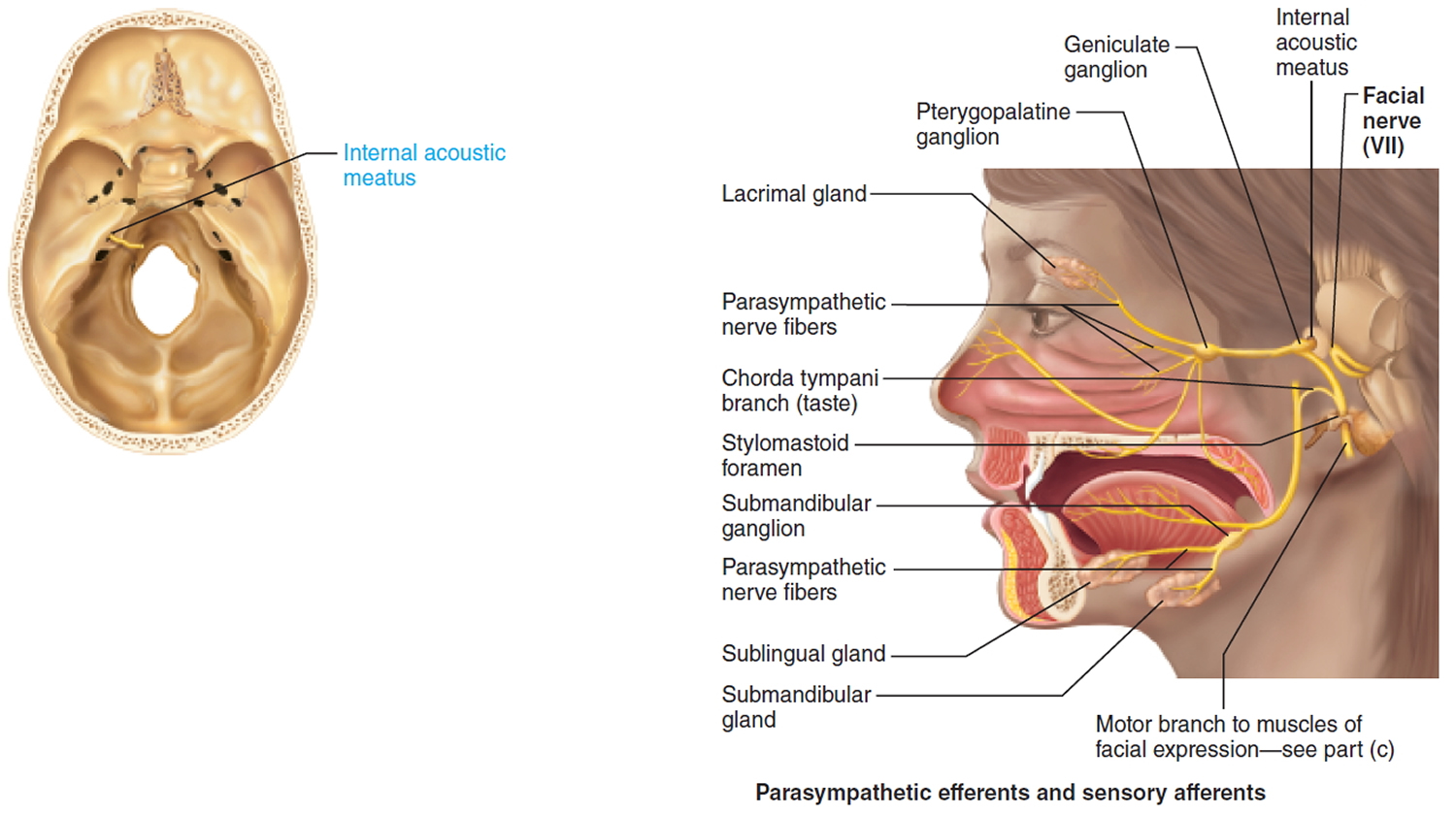
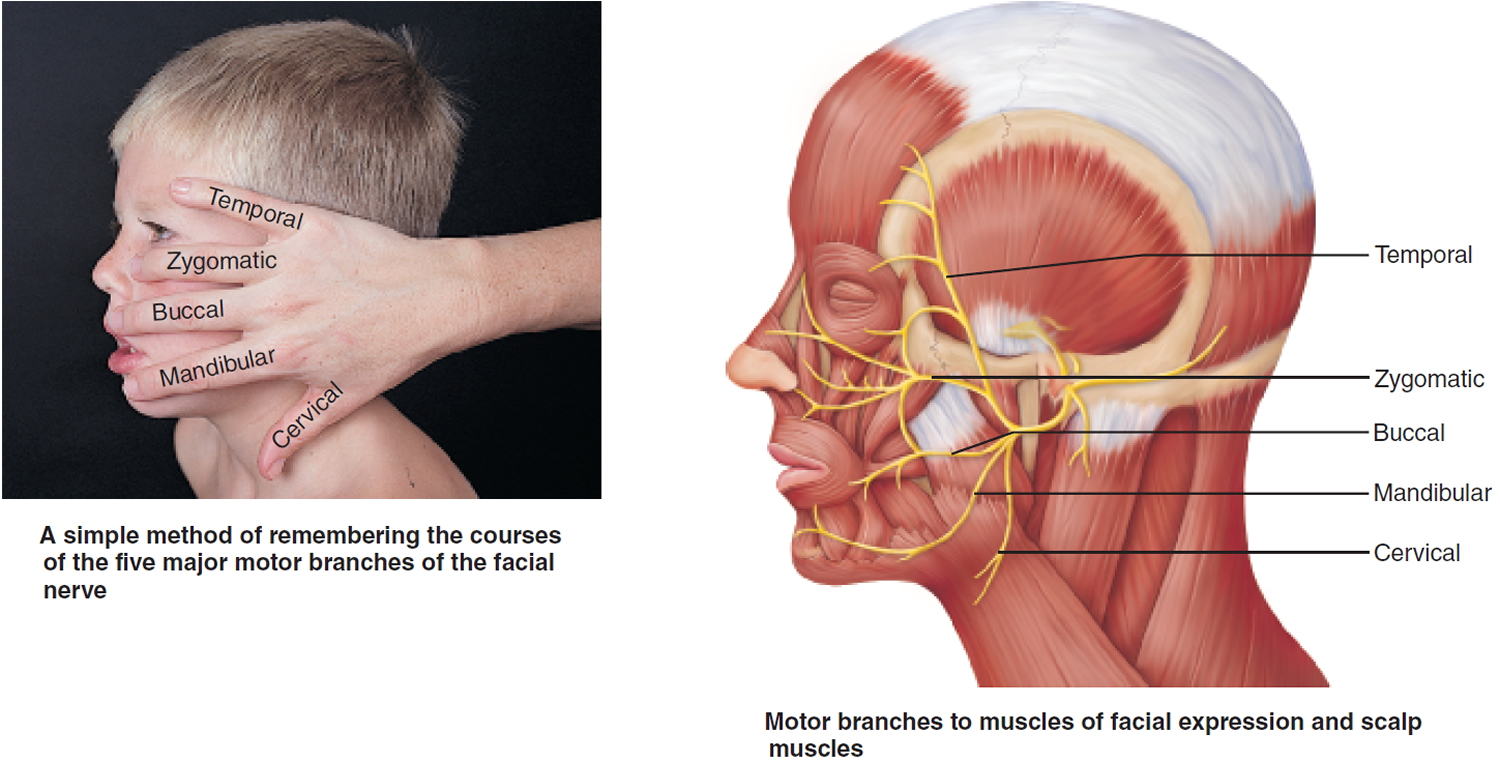
VII. Facial Nerve
A mixed nerve: Chief somatic motor nerve to the facial muscles; parasympathetic innervation to glands; special sensory taste from the tongue.
Sensory function: Special visceral sensory from taste buds on anterior two-thirds of tongue. General somatic sensory from small patch of skin on the ear.
Somatic motor function: Five major branches on face: temporal, zygomatic, buccal, mandibular, and cervical, to innervate the facial muscles. Also innervates the posterior belly of digastric. Afferent proprioceptor fibers return from these muscles.
Visceral motor function (parasympathetic): Innervate the lacrimal (tear) glands, nasal and palatine glands, and the submandibular and sublingual salivary glands.
Effect of Damage: Bell’s palsy, characterized by paralysis of facial muscles on affected side and partial loss of taste sensation, may develop rapidly (often overnight). It is caused by herpes simplex (viral) infection, which produces inflammation and swelling of the facial nerve. The lower eyelid droops, the corner of the mouth sags (making it difficult to eat or speak normally), and the eye constantly drips tears and cannot be completely closed. The condition may disappear spontaneously without treatment.
Origin: Fibers emerge from the pons, just lateral to abducens.
Pathway: Fibers enter the temporal bone via the internal acoustic meatus. Chorda tympani branches off to innervate the two salivary glands and tongue. Branch to facial muscles emerges from the temporal bone through the stylomastoid foramen and courses to lateral aspect of face. Cell bodies of sensory neurons are in geniculate ganglion. Cell bodies of postganglionic parasympathetic neurons are in pterygopalatine and submandibular ganglia on the trigeminal nerve
Figure 7. Facial nerve (Cranial nerve 7)
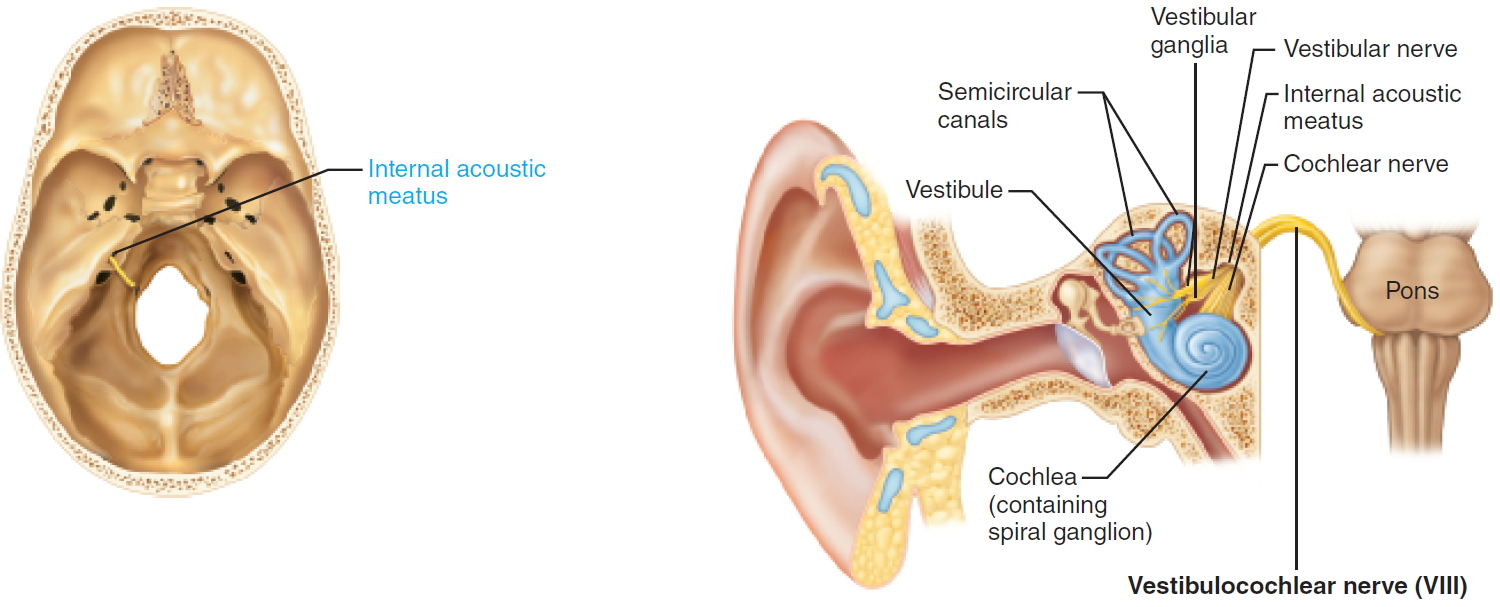
VIII. Vestibulocochlear Nerve
Sensory function: Vestibular branch: Special somatic sensory, equilibrium. Cochlear branch: Special somatic sensory, hearing. Small motor component adjusts the sensitivity of the sensory receptors.
Effect of Damage: Lesions of cochlear nerve or cochlear receptors result in central or nerve deafness, whereas damage to vestibular division produces dizziness, rapid involuntary eye movements, loss of balance, nausea, and vomiting.
Origin: Sensory receptors in the inner ear for hearing (within the cochlea) and for equilibrium (within the semicircular canals and vestibule).
Pathway: From the inner ear cavity within the temporal bone, fibers pass through the internal acoustic meatus, merge to form the vestibulocochlear nerve and enter the brain stem at the pons. Sensory nerve cell bodies for vestibular branch located in vestibular ganglia; for the cochlear branch, in the spiral ganglia within the cochlea.
Figure 8. Vestibulocochlear nerve (Cranial nerve 8)
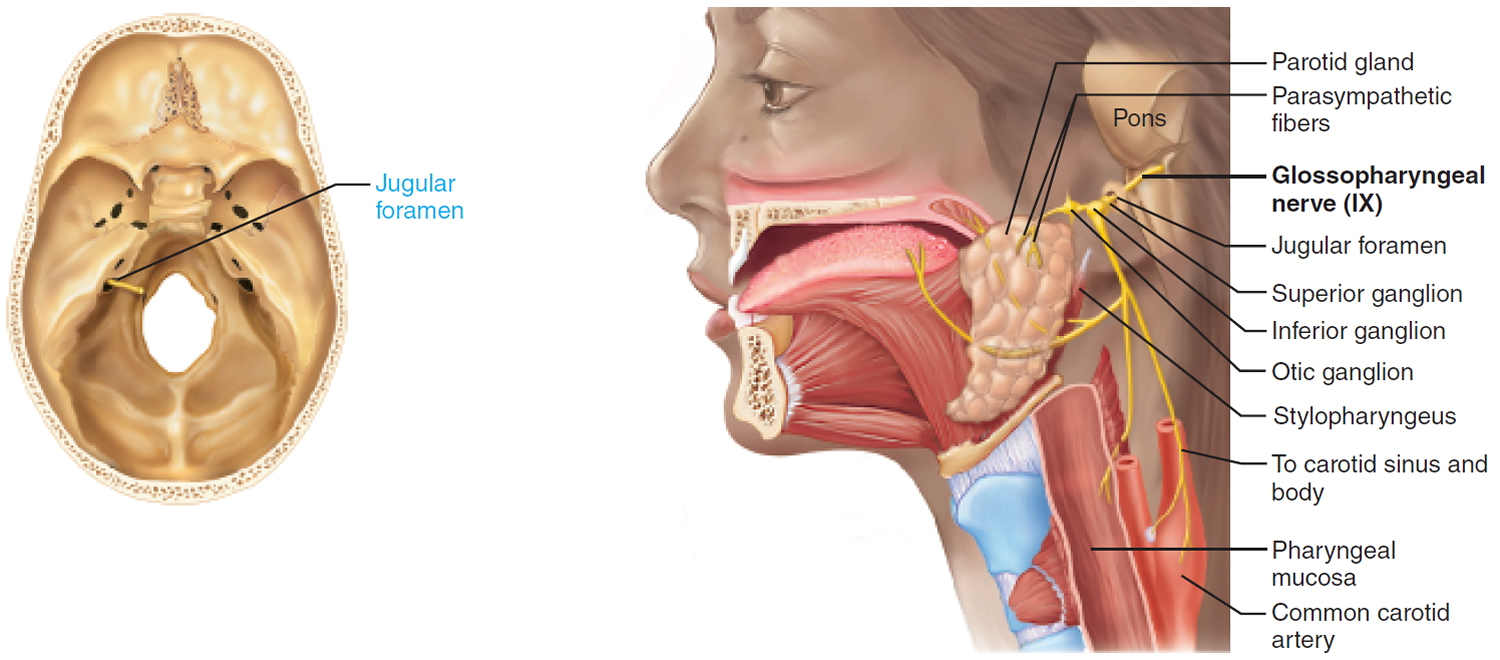
IX. Glossopharyngeal Nerve
Mixed nerve innervating the tongue (general and special sensory), the pharynx, and the parotid salivary gland.
Sensory function: Special visceral sensory from taste buds on posterior third of tongue. General visceral sensory from posterior third of tongue, pharyngeal mucosa, chemoreceptors in the carotid body (which monitor O2 and CO2 in the blood and regulate respiratory rate and depth), and baroreceptors of carotid sinus (regulate blood pressure). General somatic sensory from small area of skin on external ear.
Somatic motor function: Innervate a pharyngeal muscle, stylopharyngeus, which elevates the pharynx during swallowing. Afferent proprioceptor fibers return from this muscle.
Effect of Damage: Injury or inflammation of glossopharyngeal nerves impairs swallowing and taste on the posterior third of the tongue.
Origin: Fibers emerge from the medulla oblongata.
Pathway: Fibers pass through the jugular foramen and travel to the pharynx. Cell bodies of sensory neurons are located in the superior and inferior ganglia. Cell bodies of postganglionic parasympathetic neurons are in otic ganglion on the trigeminal nerve.
Figure 9. Glossopharyngeal nerve (Cranial nerve 9)
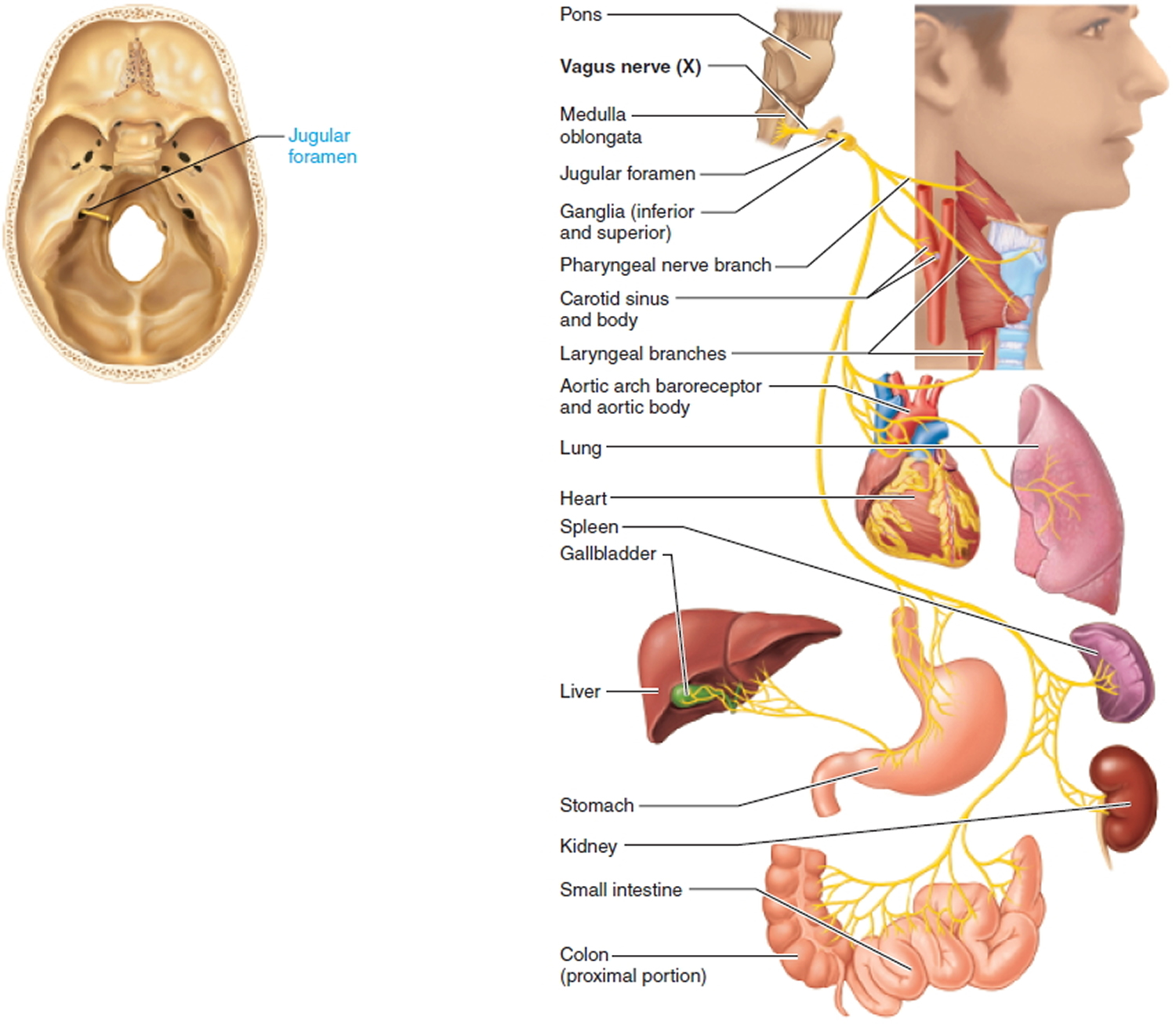
 X. Vagus Nerve
X. Vagus Nerve
Mixed nerves; major function is parasympathetic innervation to the thoracic and abdominal viscera.
Sensory function: General visceral sensory from the thoracic and abdominal viscera, mucosa of larynx and pharynx, carotid sinus (baroreceptor for blood pressure), and carotid and aortic bodies (chemoreceptors for respiration). Special visceral sensory from taste buds on the epiglottis. General somatic sensory from small area of skin on external ear.
Somatic motor function: IInnervates skeletal muscles of the pharynx and larynx involved in swallowing and vocalization. Afferent proprioceptor fibers return from the muscles of the larynx and pharynx.
Visceral motor function (parasympathetic): Innervates the heart, lungs, and abdominal viscera through the transverse colon. Regulates heart rate, breathing, and digestive system activity.
Effect of Damage: Vagal nerve paralysis can lead to hoarseness or loss of voice, difficulty swallowing and impaired digestive system motility. Total destruction of both vagus nerves is incompatible with life, because these parasympathetic nerves are crucial in maintaining the normal state of visceral organ activity; without their influence, the activity of the sympathetic nerves, which mobilize and accelerate vital body processes (and shut down digestion), would be unopposed.
Origin: Fibers emerge from medulla oblongata.
Pathway: Fibers exit the skull through the jugular foramen and descend through the neck into the thorax and abdomen.
Figure 10. Vagus nerve (Cranial nerve 10)
XI. Accessory Nerve
Somatic motor function: Innervate the trapezius and sternocleidomastoid muscles that move the head and neck. Afferent proprioceptor fibers return from these muscles.
Effect of Damage: Injury to the spinal root of one accessory nerve causes the head to turn toward the side of the injury as result of sternocleidomastoid muscle paralysis; shrugging of that shoulder (role of trapezius muscle) becomes difficult.
Origin: Forms from ventral rootlets arising from C1–C5 of the spinal cord. Long considered to have both a cranial and spinal portion, the cranial rootlets have been shown to be part of the vagus nerves.
Pathway: Upon emerging from the spinal cord, spinal rootlets merge to form the accessory nerves, pass into the skull through the foramen magnum, and then exit the skull through the jugular foramen.
Figure 11. Accessory nerve (Cranial nerve 11)

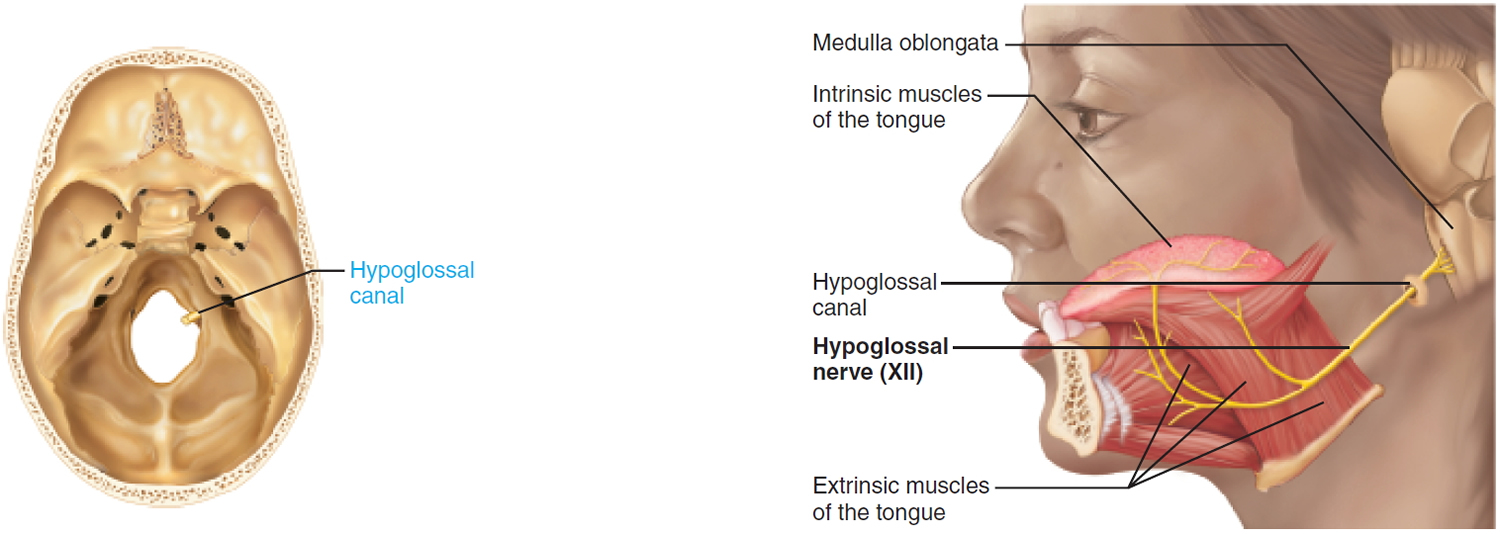
XII. Hypogloassal Nerve
Somatic motor function: Innervate the intrinsic and extrinsic muscles of the tongue. Aid tongue movements during feeding, swallowing, and speech. Afferent proprioceptor fibers return from these muscles.
Effect of Damage: Damage to hypoglossal nerves causes difficulties in speech and swallowing. If both nerves are impaired, the person cannot protrude the tongue; if only one side is affected, the tongue deviates (leans) toward affected side. Eventually the paralyzed side begins to atrophy.
Origin: From a series of roots from the hypoglossal nuclei in the ventral medulla oblongata.
Pathway: Exit the skull through the hypoglossal canal and travel to the tongue.
Figure 12. Hypoglossal nerve (Cranial nerve 12)

{kind=link}