Contents
What is cystocele
A cystocele, also called a prolapsed bladder or dropped bladder or anterior prolapse, is the bulging or dropping of the bladder into the vagina (see Figure 5 below). The bladder, located in the pelvis between the pelvic bones, is a hollow, muscular, balloon-shaped organ that expands as it fills with urine. During urination, also called voiding, the bladder empties through the urethra, located at the bottom of the bladder. The urethra is the tube that carries urine outside of the body. The vagina is the tube in a woman’s body that runs beside the urethra and connects the womb, or uterus, to the outside of the body.
A woman’s chances of developing a cystocele increase with age, possibly because of weakening muscles and supportive tissues from aging.
Straining the muscles that support your pelvic organs may lead to cystocele. Such straining occurs during vaginal childbirth or with chronic constipation, violent coughing or heavy lifting. A cystocele also tends to cause problems after menopause, when estrogen levels decrease. Whether menopause increases a woman’s chances of developing a cystocele is unclear.
In mild cystocele, you may not notice any signs or symptoms. When signs and symptoms occur, they may include:
- A feeling of fullness or pressure in your pelvis and vagina
- Increased discomfort when you strain, cough, bear down or lift
- A feeling that you haven’t completely emptied your bladder after urinating
- Repeated bladder infections
- Pain or urinary leakage during sexual intercourse
- In severe cases, a bulge of tissue that protrudes through your vaginal opening and may feel like sitting on an egg
Signs and symptoms often are especially noticeable after standing for long periods of time and may go away when you lie down.
A severely prolapsed bladder can be uncomfortable. It can make emptying your bladder difficult and may lead to bladder infections. Make an appointment with your doctor if you have any signs or symptoms that bother you.
For a mild or moderate cystocele, nonsurgical treatment is often effective. In more severe cases, surgery may be necessary to keep the vagina and other pelvic organs in their proper positions.
Cystocele grading
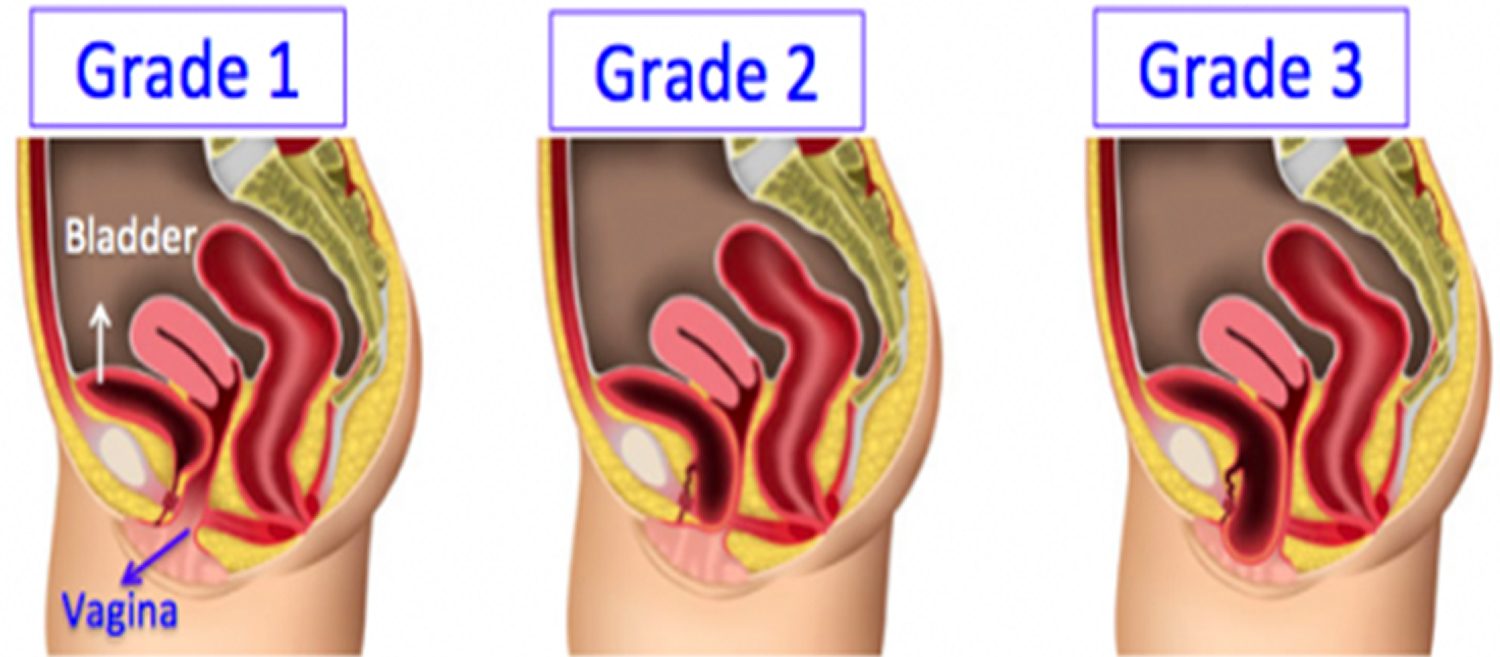
A health care provider uses a grading system to determine the severity of a woman’s cystocele. A cystocele receives one of three grades depending on how far a woman’s bladder has dropped into her vagina:
- Grade 1 — mild, when the bladder drops only a short way into the vagina
- Grade 2 — moderate, when the bladder drops far enough to reach the opening of the vagina
- Grade 3 — most advanced, when the bladder bulges out through the opening of the vagina
What is the pelvic floor and why does it become weak in women?
The pelvic floor is a complex layer of muscles and ligaments which stretches like a hammock from the pubic bone at the front of your pelvis to the coccyx at the bottom your spine.
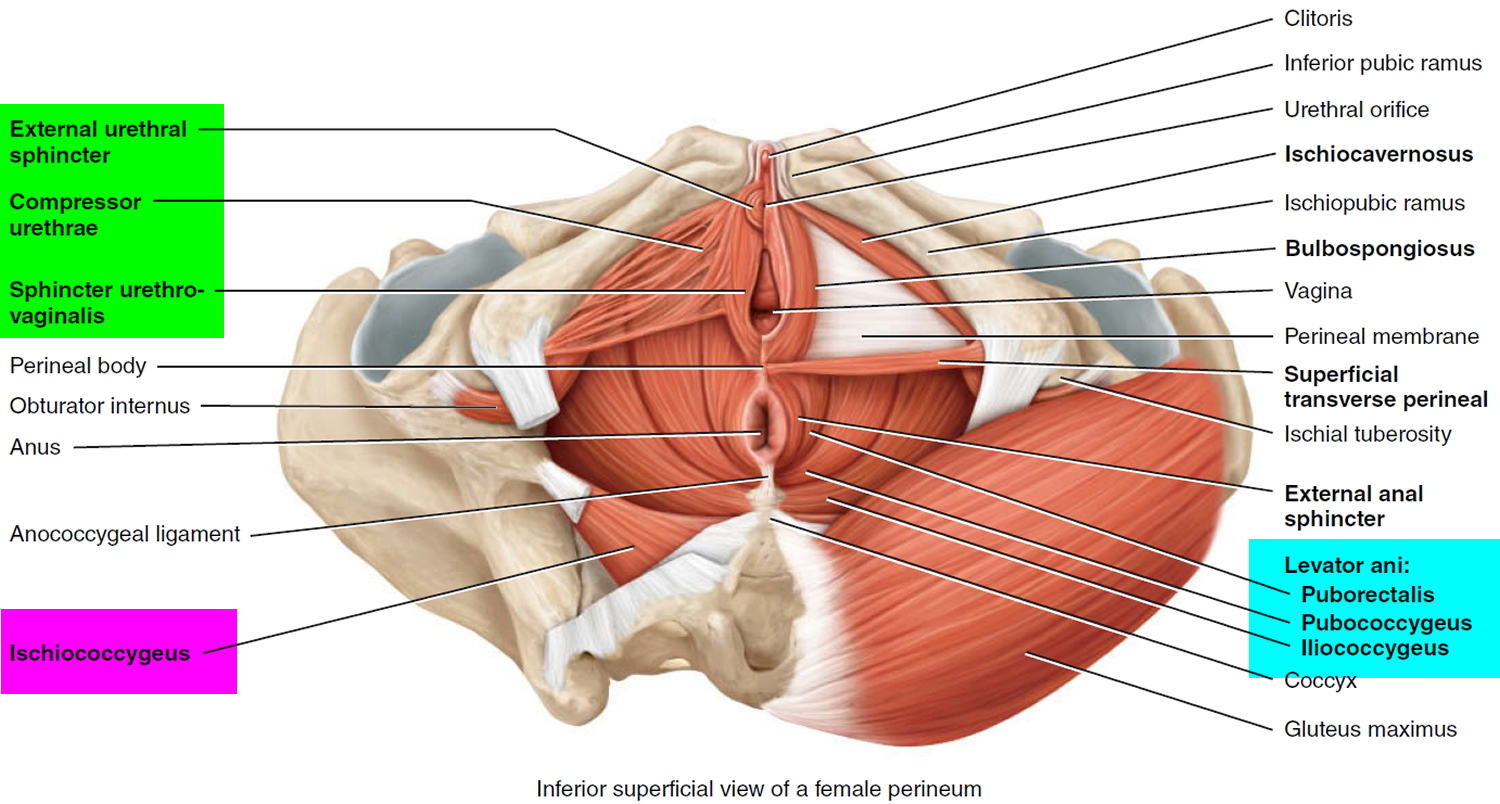
The muscles of the pelvic floor are the levator ani and ischiococcygeus. Along with the fascia covering their internal and external surfaces, these muscles are referred to as the pelvic diaphragm, which stretches from the pubis anteriorly to the coccyx posteriorly, and from one lateral wall of the pelvis to the other. This arrangement gives the pelvic diaphragm the appearance of a funnel suspended from its attachments. The pelvic diaphragm separates the pelvic cavity above from the perineum below. The anal canal and urethra pierce the pelvic diaphragm in both sexes, and the vagina also goes through it in females. The three components of the levator ani muscle are the pubococcygeus, puborectalis, and iliococcygeus. Figure 1 shows these muscles in the female. The levator ani is the largest and most important muscle of the pelvic floor. It supports the pelvic viscera and resists the inferior thrust that accompanies increases in intraabdominal pressure during functions such as forced exhalation, coughing, vomiting, urination, and defecation. The muscle also functions as a sphincter at the anorectal junction, urethra, and vagina. In addition to assisting the levator ani, the ischiococcygeus pulls the coccyx anteriorly after it has been pushed posteriorly during defecation or childbirth.
Figure 1. Pelvic floor female
The pelvic floor has several functions:
- it supports your pelvic and abdominal organs, especially when you are standing or straining
- it helps the water pipe stay closed when you cough, sneeze or strain
- it is used to control leakage of wind or motions from your lower bowel
- it helps to heighten sexual awareness by tightening during intercourse
The pelvic floor can be weakened by childbirth, prolonged straining to empty your bowels, lack of exercise and the menopause. It may also simply become weak as a result of ageing. A weak pelvic floor gives you less control so that you may leak when you exercise, lift, cough or sneeze.
Figure 2. Urinary tract anatomy
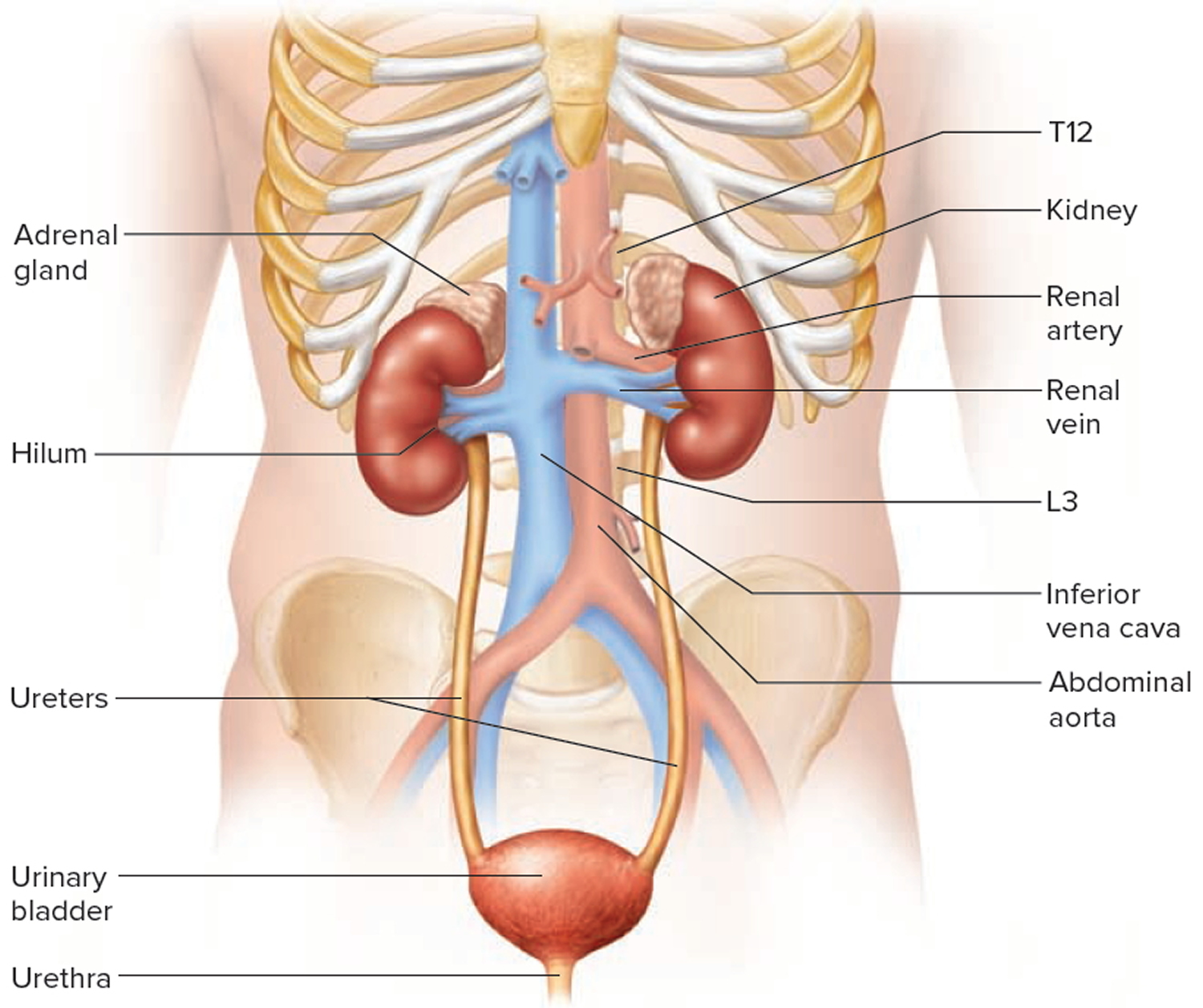
Figure 3. Urinary bladder anatomy
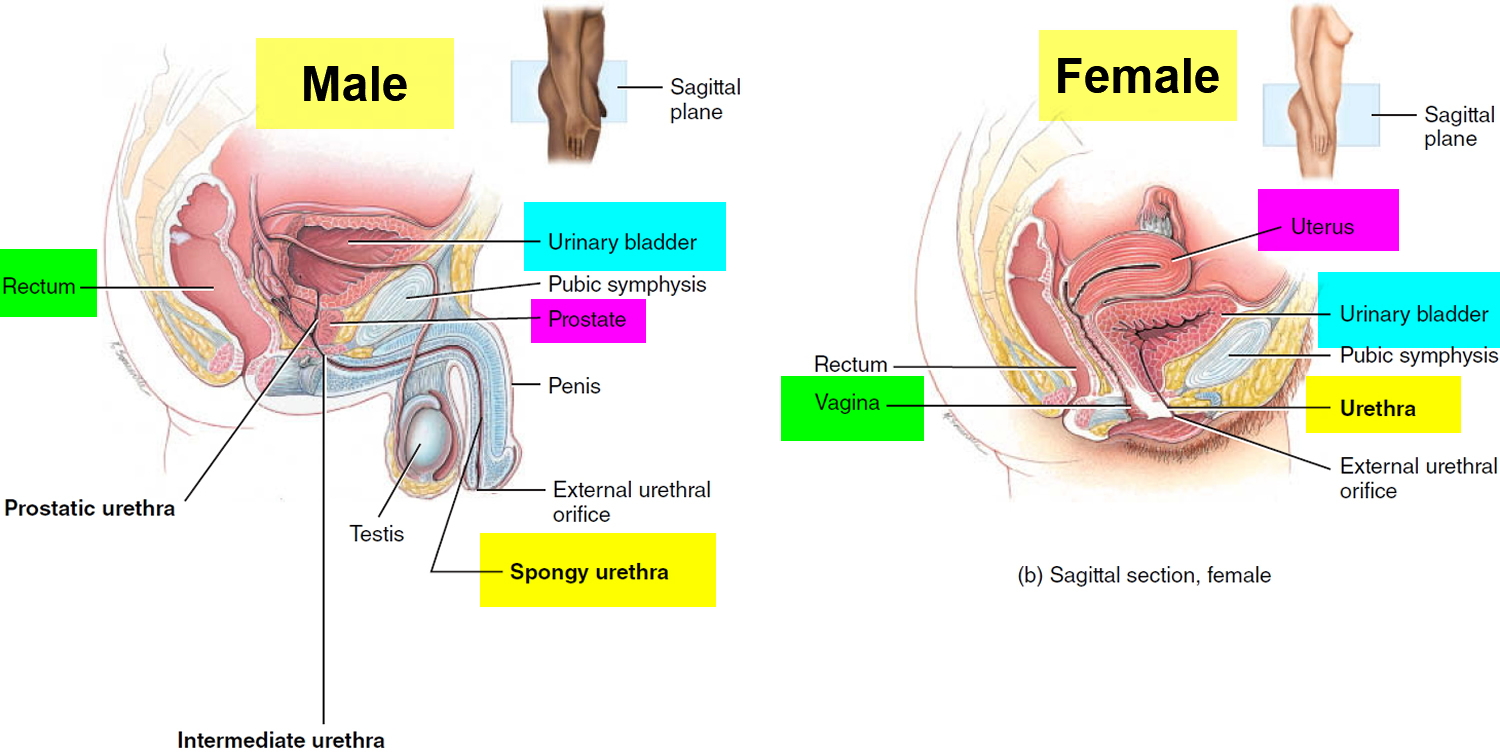
Figure 4. Urinary bladder anatomy
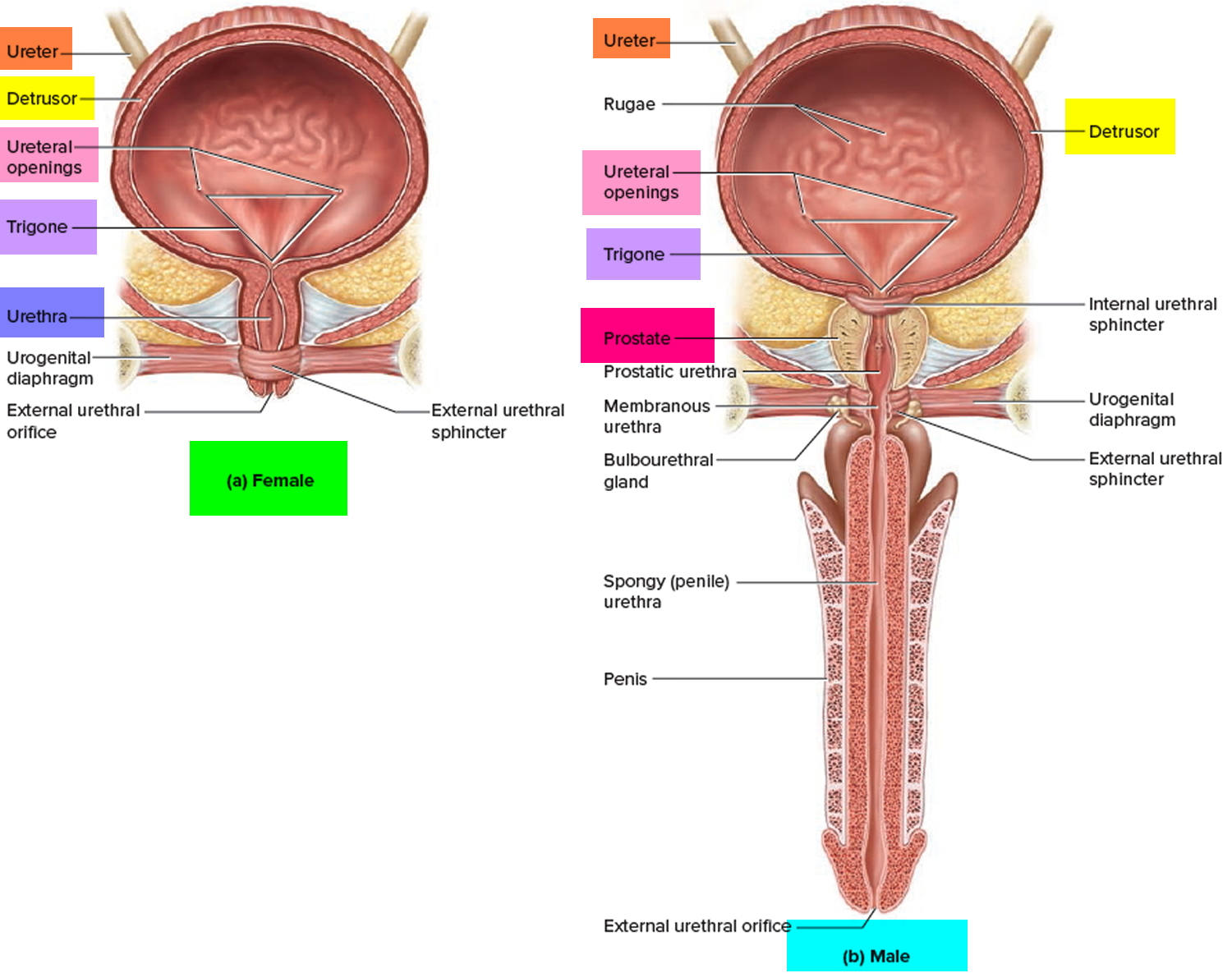 Figure 5. Cystocele
Figure 5. Cystocele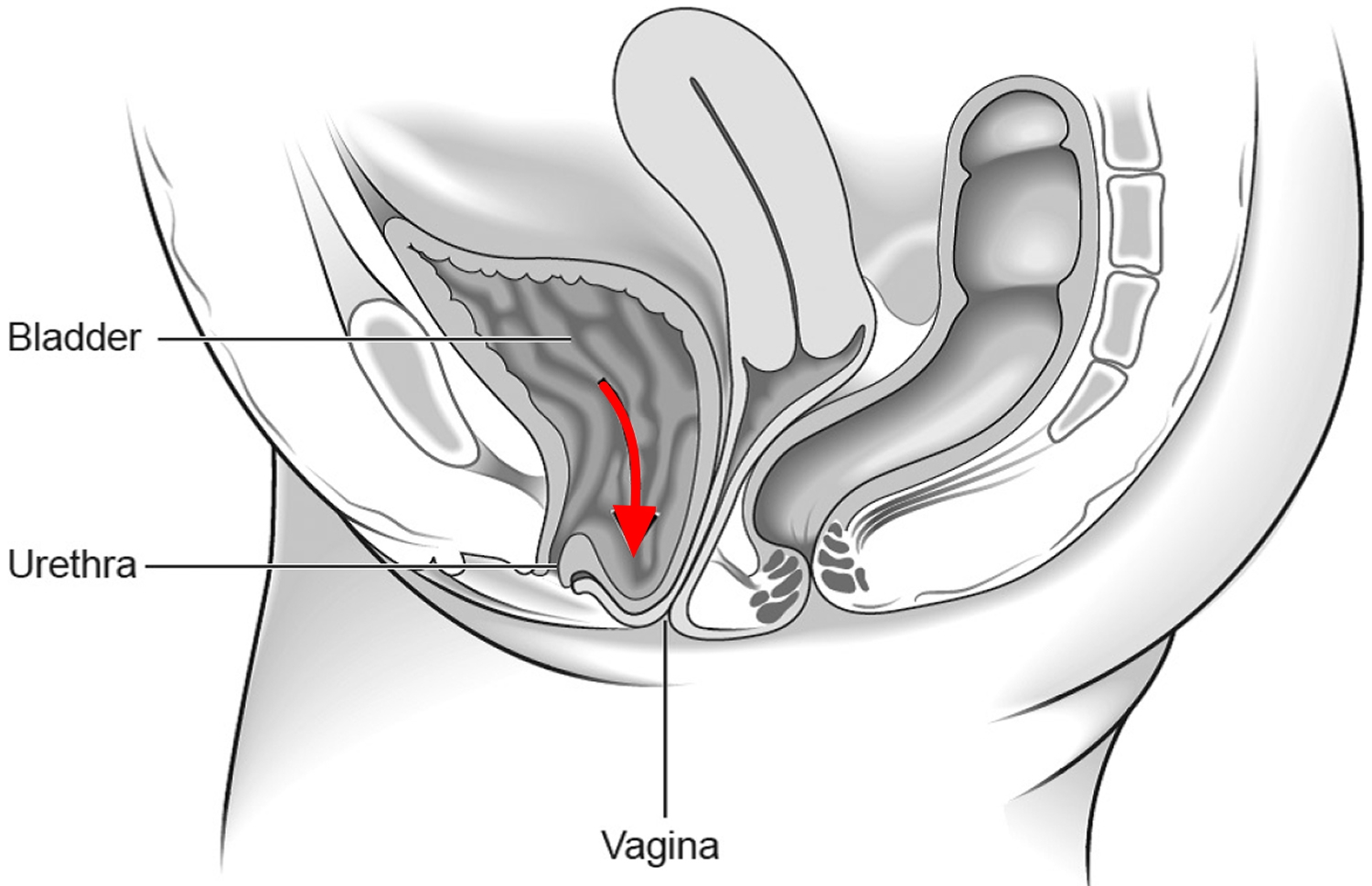
Cystocele and rectocele
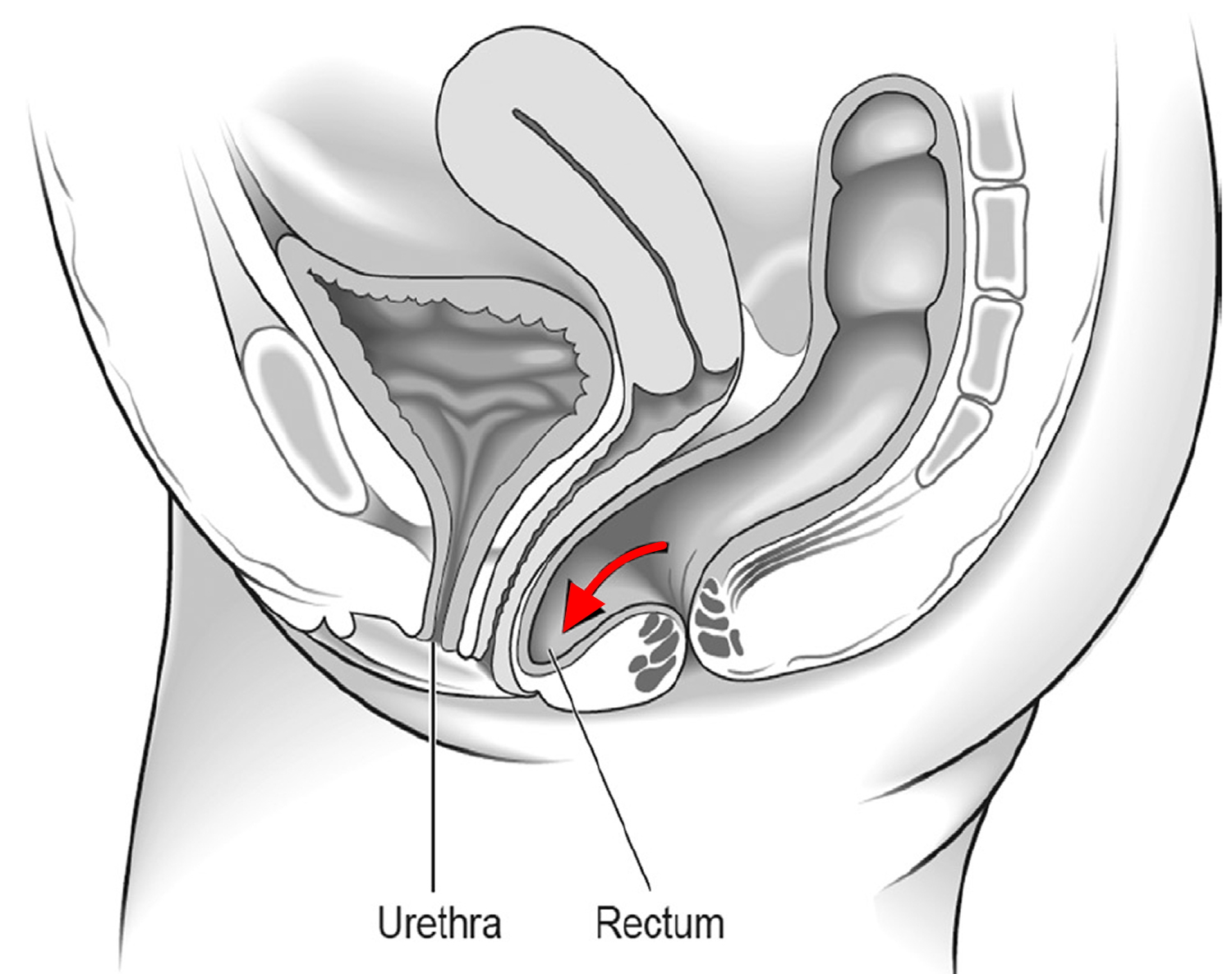
A rectocele is a herniation (bulge) of the front wall of the rectum into the back wall of the vagina (see Figure 6). The tissue between the rectum and the vagina is known as the rectovaginal septum and this structure can become thin and weak over time, resulting in a rectocele. When rectoceles are small, most women have no symptoms. A rectocele may be an isolated finding or occur as part of a generalized weakening of the pelvic floor muscles. Other pelvic organs such as the bladder (cystocele) and the small intestine (enterocele), can bulge into the vagina, leading to similar symptoms as rectocele.
The finding of a small rectocele on examination is very common and is of no concern if the patient does not have significant symptoms. When a rectocele becomes large, stool can become trapped within it, making it difficult to have a bowel movement or creating a sensation of incomplete evacuation. Symptoms are usually due to stool trapping, difficulty passing stool, and protrusion of the back of the vagina through the vaginal opening. During bowel movements, women with large, symptomatic rectoceles may describe the need to put their fingers into their vagina and push back toward the rectum to allow the stool to pass (“splinting”). Rectoceles are more common in women who have delivered children vaginally.
Rectocele causes
The exact cause of a rectocele is unknown, but symptomatic rectoceles usually occur in conjunction with weakening of the pelvic floor.
Rectoceles are usually caused by thinning of the rectovaginal septum (the tissue between the rectum and vagina) and weakening of the pelvic floor muscles. There are many things that can lead to weakening of the pelvic floor, including:
- Vaginal deliveries
- Trauma from vaginal delivery (e.g. the use of forceps or vacuum during delivery, tearing or episiotomy, which is a surgical cut in the muscular area between the vagina and the anus made just before delivery)
- History of constipation
- Chronic straining with bowel movements
- Gynecological (e.g. hysterectomy) or rectal surgeries
In addition, a history of chronic constipation and excessive straining with bowel movements are thought to play a contributory role in developing a rectocele. Multiple gynecological or rectal surgeries can also lead to weakening of the pelvic floor and rectocele formation.
Rectocele symptoms
The majority of patients with a rectocele have no symptoms. In fact, approximately 40% of all women will have a rectocele found on routine physical examination. When symptoms are present, they may be categorized as either rectal or vaginal.
- Rectal symptoms may include:
- Difficulty having a complete bowel movement
- Stool getting stuck in the bulge of the rectum
- The need to press against the vagina and/or space between the rectum and the vagina (perineal body) in order to have a bowel movement
- Straining with bowel movements
- The urge to have multiple bowel movements throughout the day
- Constipation
- Rectal pain
- Vaginal symptoms can include the sensation of a bulge or fullness in the vagina, tissue protruding out of the vagina, discomfort with sexual intercourse, and vaginal bleeding.
Symptomatic rectoceles can lead to excessive straining with bowel movements, the urge to have multiple bowel movements throughout the day, and rectal discomfort. Fecal incontinence or smearing may occur as small pieces of stool can be retained in a rectocele (stool trapping), only to later seep out of the anus. Significant stool trapping can also result in an increase in the sense of needing to have a bowel movement, as the stool stuck in the rectocele returns to the low rectum when the patient stands, thereby giving the patient the urge to defecate again.
Figure 6. Rectocele
How is a rectocele diagnosed?
Often, a rectocele is easily recognized on physical examination at rest or with performance of various maneuvers. This often includes a bimanual or speculum examination. Additionally, a digital rectal exam will be performed which usually demonstrates a weakness in the anterior wall of the rectum (the side closest to the vagina). In instances of very large rectoceles, the back wall of the vagina may bulge out beyond the opening of the vagina. Smaller rectoceles may only be obvious when the woman strains. A special x-ray, called defecography can be useful in the diagnosis of a rectocele. A defecography can visualize and confirm a rectocele. Defecography study is very specific and can pinpoint the size of the rectocele and the degree to which the rectum is emptied. During this exam, the patient will sit and be asked to defecate on a specially-designed commode after contrast material is instilled in the rectum, vagina and bladder. In the presence of a rectocele, the contrast material can be seen bulging from the front of the rectum into the back of the vagina. Sometimes the contrast material stays in the rectocele while the liquid in the rectum is expelled — this is called “stasis”, or stool trapping. If a rectocele is present, this study can document the size and the ability to completely empty the rectum. In general, if the rectocele is larger than 2 centimeters and/or has significant retention of contrast, it is considered abnormal.
How is a rectocele treated?
A rectocele should only be treated if you are having significant symptoms that interfere with your quality of life. Surgical treatment is reserved for only the most severe cases of symptomatic rectocele. In the absence of severe symptoms, the recommended treatment for a rectocele is non-surgical, and focused on optimizing stool consistency to aid in the passage of stool. This often involves increasing fiber intake (which may also include taking a daily fiber supplement) and increasing fluid intake. Biofeedback, which is a special form of pelvic floor physical therapy aimed at improving your rectal sensation and pelvic floor muscle contraction, may also be helpful. As described below, you may insert one or two fingers into your vagina to splint the vagina during attempts to pass stool.
Nonsurgical treatment
The vast majority of a patient’s symptoms associated with a rectocele can be managed effectively without surgery.
The goal is to have good daily bowel habits and softer stools. Avoiding constipation and straining with bowel movements will reduce the risk of a bulge associated with a rectocele.
Preventive and Medical Tips
- Eating a high-fiber diet and taking over-the-counter fiber supplements (25-35 grams of fiber/day)
- Drinking more water (typically 6-8 glasses daily)
- Avoiding excessive straining with bowel movements
- Applying pressure to the back of the vagina during bowel movements
- Pelvic floor exercises such as Kegel pelvic floor exercise
- Biofeedback, a special form of pelvic floor physical therapy aimed at improving rectal sensation and pelvic floor muscle contraction
- Stool softeners
- Hormone replacement therapy
During bowel movements, it is important to avoid straining, therefore, if you do not have the urge to have a bowel movement, do not force defecation. In addition, it is always important to avoid prolonged sitting periods on the toilet.
Surgical treatment
The surgical management of rectoceles should only be performed if you continue to have symptoms despite the use of conservative measures such as fiber, water, and pelvic floor strengthening. These symptoms should be significant enough that they interfere with your activities of daily living, meaning that you cannot comfortably do the things you usually do on a daily basis. Colorectal surgeons, gynecologists and urogynecologists are trained in the diagnosis and treatment of this condition. These trained physicians can perform surgeries to attempt repair of a rectocele.
There are multiple ways to approach the surgery including: transanally (through the anus), through the perineum (the space between the anus and vagina), and through the vagina. All of these aim to remove the extra tissue that makes up the rectocele and reinforce the rectovaginal septum (the tissue between the rectum and the vagina). This can be done by plication (stitching the tissue together). Occasionally, mesh (a prosthetic material or patch) can be used to reinforce the repair.
The S.T.A.R.R. (stapled transanal rectal resection) procedure uses a special stapling device that removes the redundant tissue and staples it together at the same time. This technique should only be used if a patient has other problems such as obstructive defecation or mucosal prolapse (rectal tissue that protrudes out of the anus). This is a newer procedure that is not performed by all colon and rectal surgeons, and its success and complication rates are still being studied.
A rectocele can also be repaired through the abdomen, either laparoscopically or open. This approach has been proven safe and effective, but there may not be any benefit over other types of rectocele repair. The approach will depend on the size of the rectocele and the symptoms associated with the rectocele.
The overall success of the surgery depends on the symptoms, length of time symptoms have been present, and approach of surgery. Risks of surgical correction include bleeding, infection and pain during intercourse (dyspareunia), fecal incontinence, rectovaginal fistula (a communication between the rectum and vagina), as well as a risk that the rectocele may recur or worsen.
Some studies report significant improvement in about 75-90% of patients. However, the success rates seem to decrease over time and, at two years, only 50-60% of patients can expect to have significant improvement. In addition, patients with fecal incontinence may have better results with a transperineal or vaginal approach, as the transanal approach has been shown to occasionally worsen continence. A surgeon who is familiar with the technique and has experience repairing rectoceles will have the best results.
Cystocele causes
A cystocele occurs when the muscles and supportive tissues between a woman’s bladder and vagina weaken and stretch, letting the bladder sag from its normal position and bulge into the vagina or through the vaginal opening. In a cystocele, the bladder tissue remains covered by the vaginal skin. A cystocele may result from damage to the muscles and tissues that hold the pelvic organs up inside the pelvis. A woman’s pelvic organs include the vagina, cervix, uterus, bladder, urethra, and small intestine. Damage to or weakening of the pelvic muscles and supportive tissues may occur after vaginal childbirth and with conditions that repeatedly strain or increase pressure in the pelvic area, such as:
- repetitive straining for bowel movements
- constipation
- chronic or violent coughing
- heavy lifting
- being overweight or obese
- pregnancy and vaginal childbirth
Risk factors for cystocele
These factors may increase your risk of anterior prolapse:
- Childbirth. Women who have vaginally delivered one or more children have a higher risk of anterior prolapse.
- Aging. Your risk of anterior prolapse increases as you age. This is especially true after menopause, when your body’s production of estrogen — which helps keep the pelvic floor strong — decreases.
- Hysterectomy. Having your uterus removed may contribute to weakness in your pelvic floor support.
- Genetics. Some women are born with weaker connective tissues, making them more susceptible to anterior prolapse.
- Obesity. Women who are overweight or obese are at higher risk of anterior prolapse.
Cystocele prevention
To reduce your risk of developing anterior prolapse, try these self-care measures:
- Perform Kegel pelvic floor exercises on a regular basis. These exercises can strengthen your pelvic floor muscles, and this is especially important after you have a baby.
- Treat and prevent constipation. High-fiber foods can help.
- Avoid heavy lifting, and lift correctly. When lifting, use your legs instead of your waist or back.
- Control coughing. Get treatment for a chronic cough or bronchitis, and don’t smoke.
- Avoid weight gain. Talk to your doctor to determine your ideal weight and get advice on weight-loss strategies, if you need them.
Cystocele symptoms
The symptoms of a cystocele may include
- a vaginal bulge
- the feeling that something is falling out of the vagina
- the sensation of pelvic heaviness or fullness
- difficulty starting a urine stream
- a feeling of incomplete urination
- frequent or urgent urination
Women who have a cystocele may also leak some urine as a result of movements that put pressure on the bladder, called stress urinary incontinence. These movements can include coughing, sneezing, laughing, or physical activity, such as walking. Urinary retention—the inability to empty the bladder completely—may occur with more severe cystoceles if the cystocele creates a kink in the woman’s urethra and blocks urine flow.
Women with mild cystoceles often do not have any symptoms.
Cystocele diagnosis
Diagnosing a cystocele requires medical tests and a physical exam of the vagina. Medical tests take place in a health care provider’s office, an outpatient center, or a hospital. The health care provider will ask about symptoms and medical history.
If a woman has difficulty emptying her bladder, a health care provider may measure the amount of urine left in the woman’s bladder after she urinates. The remaining urine is called the postvoid residual. A health care provider can measure postvoid residual with a bladder ultrasound. A bladder ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off the bladder to create an image and show the amount of remaining urine. A specially trained technician performs the procedure, and a radiologist—a doctor who specializes in medical imaging—interprets the images. A woman does not need anesthesia.
A health care provider can also use a catheter—a thin, flexible tube—to measure a woman’s postvoid residual. The health care provider inserts the catheter through the woman’s urethra into her bladder to remove and measure the amount of remaining urine after the woman has urinated. A postvoid residual of 100 mL or more is a sign that the woman is not completely emptying her bladder. A woman receives local anesthesia.
A health care provider may use a voiding cystourethrogram—an x-ray exam of the bladder—to diagnose a cystocele as well. A woman gets a voiding cystourethrogram while urinating. The x-ray images show the shape of the woman’s bladder and let the health care provider see any problems that might block normal urine flow. An x-ray technician performs a voiding cystourethrogram, and a radiologist interprets the images. A woman does not need anesthesia; however, some women may receive sedation. A health care provider may order additional tests to rule out problems in other parts of a woman’s urinary tract.
Your doctor might also run a test on a urine sample to look for signs of a bladder infection, if it seems that you’re retaining more urine in your bladder than is normal after urinating.
Cystocele treatment
Cystocele treatment depends on the severity of the cystocele, whether you have any symptoms and whether you have any related conditions, such as a uterus that slips into the vaginal canal (uterine prolapse). If a woman’s cystocele does not bother her, a health care provider may recommend only that she avoid heavy lifting or straining, which could worsen her cystocele. If a woman has symptoms that bother her and wants treatment, the health care provider may recommend pelvic muscle exercises, a vaginal pessary, or surgery.
Pelvic floor, or Kegel, exercises involve strengthening pelvic floor muscles. Strong pelvic floor muscles more effectively hold pelvic organs in place. A woman does not need special equipment for Kegel exercises.
The exercises involve tightening and relaxing the muscles that support pelvic organs. A health care provider can help a woman learn proper technique.
Your doctor may recommend using estrogen — usually a vaginal cream, pill or ring — especially if you’ve already experienced menopause. This is because estrogen, which helps keep pelvic muscles strong, decreases after menopause.
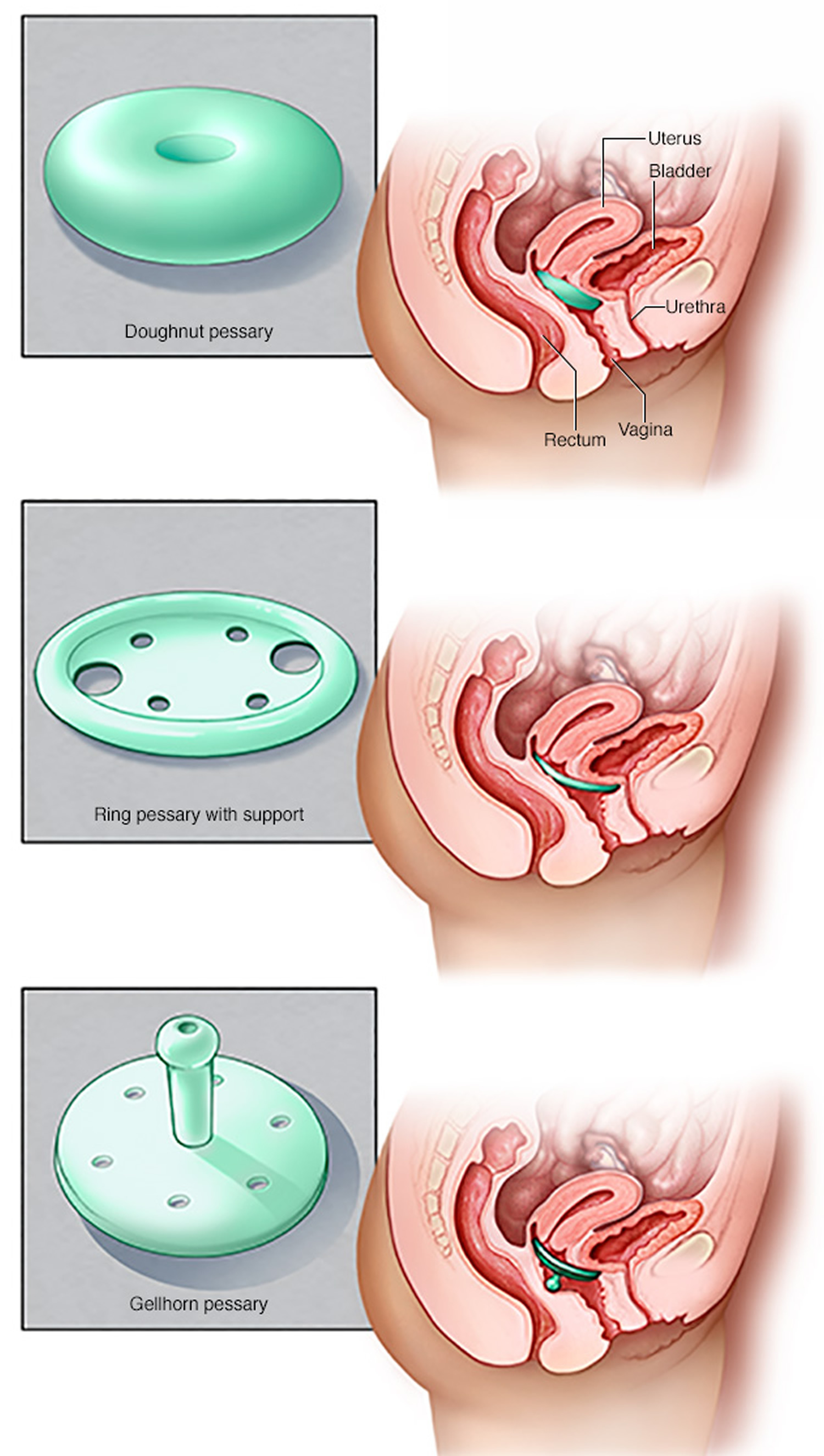
A vaginal pessary is a small, silicone medical device placed in the vagina that supports the vaginal wall and holds the bladder in place. Pessaries come in a number of shapes and sizes. A health care provider has many options to choose from to find the most comfortable pessary and help you decide which type would best suit your needs.
Figure 7. Vaginal pessaries
How to do pelvic floor exercise for your pelvic muscles
To do pelvic floor or Kegel exercises, you just squeeze your pelvic floor muscles. The part of your body including your hip bones is the pelvic area. At the bottom of the pelvis, several layers of muscle stretch between your legs. The muscles attach to the front, back, and sides of the pelvic bone.
Kegel exercises are designed to make your pelvic floor muscles stronger. These are the muscles that hold up your bladder and help keep it from leaking.
Building up your pelvic muscles with Kegel exercises can help with your bladder control.
Let your doctor, nurse, or therapist help you. Many people have trouble finding the right muscles. Your doctor, nurse, or therapist can check to make sure you are doing the exercises correctly. You can also exercise by using special weights or biofeedback. Ask your health care team about these exercise aids.
Don’t squeeze other muscles at the same time. Be careful not to tighten your stomach, legs, or other muscles. Squeezing the wrong muscles can put more pressure on your bladder control muscles. Just squeeze the pelvic muscle. Don’t hold your breath.
Step 1
Sit comfortably with your knees slightly apart. Imagine that you are trying to stop yourself passing wind from your bowel. To do this, you must squeeze the muscle around the back passage. Try lifting and squeezing the muscle as if you have wind. If you sense a “pulling” feeling, you are squeezing the right muscles for pelvic exercises. You should be able to feel the muscle move and your buttocks or legs should not move at all. You should notice that the skin around your back passage tightens up and creates the sensation of lifting you from your chair.
Step 2
Imagine that you are sitting on the toilet to pass urine and try to stop yourself from producing a stream of urine. You should be using the same group of muscles that you used before but you will find this a little more difficult. Do not try to stop the urinary stream when you are actually passing water because it can cause problems with bladder emptying.
Or you can lie down and put your finger inside your vagina. Squeeze as if you were trying to stop urine from coming out. If you feel tightness on your finger, you are squeezing the right pelvic muscles.
Step 3
Try to tighten the muscles around your back passage and vagina, by lifting up inside as if you are trying to stop passing wind and urine at the same time. Do not tense your abdomen, squeeze your legs together, tighten your buttocks or hold your breath. If you can master this, most of the muscle contraction should be coming from the pelvic floor.
How do you practice the exercises?
You need to develop two types of muscle activity, slow and fast.
- to practice slow contractions
- do the exercises above and try to hold the pelvic floor tight for up to ten seconds. Rest for four seconds and then repeat the contraction as many times as you can, up to a maximum of ten
- to practice quick contractions
- draw the pelvic floor rapidly upwards and hold this for one second. Repeat up to a maximum of ten times. This will protect you against sudden leakage during coughing, laughing or exercise
- Aim to do one set of slow contractions followed by one set of fast contractions up to six times a day. Do not over-do it or the muscles will get tired. The exercises can be performed standing, sitting or lying down but you may find it easier at first to do them sitting down.
Other things that help
- Get into the habit of doing your exercises regularly and linking them to everyday activities e.g. do them after emptying your bladder, while answering the telephone, standing in a queue or whenever you turn on a tap. Do your pelvic exercises at least three times a day. Every day, use three positions: lying down, sitting, and standing. You can exercise while lying on the floor, sitting at a desk, or standing in the kitchen. Using all three positions makes the muscles strongest.
- At first, find a quiet spot to practice—your bathroom or bedroom—so you can concentrate. Lie on the floor. Pull in the pelvic muscles and hold for a count of 3. Then relax for a count of 3. Work up to 10 to 15 repeats each time you exercise.
- If you are not sure you are doing the exercises correctly, insert a thumb or two fingers into the vagina and try the exercises; you should feel a gentle squeeze as the muscles contract
- Use the pelvic floor exercises to prevent leakage before you do anything which might make you leak; this way, your control will gradually improve
- Drink normally – six to eight cups (two liters) per day – avoiding caffeine and alcohol if you can
- Avoid going to the toilet “just in case”; go only when you feel that your bladder is full
- Watch your weight; extra weight puts more strain on your pelvic floor muscles and your bladder
- Avoid constipation. Straining can put excessive pressure on your bladder and bowels
- Pelvic floor exercises take three to six months to produce maximum benefit, but you should continue them for life to prevent problems recurring or worsening; you should seek help from a health professional there is little or no change in your symptoms after exercising for three months
- Other methods which help some women include weighted vaginal cones, biofeedback and electrical stimulation; consult your doctor, urologist or specialist nurse for more details
Be patient. Don’t give up. It’s just 5 minutes, three times a day. You may not feel your bladder control improve until after 3 to 6 weeks. Still, most women do notice an improvement after a few weeks.
Use the Exercise Log below to keep track of your sessions.
Week: ______________
My Pelvic Muscle Exercise Log
Sunday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Monday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Tuesday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Wednesday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Thursday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Friday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Saturday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Figure 7. Pelvic floor muscle exercise log – use this sheet as a master for making copies that you can use to record your exercises week after week.
 Cystocele surgery
Cystocele surgery
A health care provider may recommend surgery to repair the vaginal wall support and reposition the woman’s bladder to its normal position. The most common cystocele repair is an anterior vaginal repair—or anterior colporrhaphy. The surgeon makes an incision in the wall of the woman’s vagina and repairs the defect by folding over and sewing together extra supportive tissue between the vagina and bladder. The repair tightens the layers of tissue that separate the organs, creating more support for the bladder. A surgeon who specializes in the urinary tract or female reproductive system performs an anterior vaginal repair in a hospital. The woman receives either regional or general anesthesia. The woman may stay overnight in the hospital, and full recovery may take up to 4 to 6 weeks.
If you have a prolapsed uterus. For cystocele associated with a prolapsed uterus, your doctor may recommend removing the uterus (hysterectomy) in addition to repairing the damaged pelvic floor muscles, ligaments and other tissues.
If you’re thinking about becoming pregnant, your doctor may recommend that you delay surgery until after you’re done having children. Using a pessary may help relieve your symptoms in the meantime. The benefits of surgery can last for many years, but there’s some risk of recurrence — which may mean another surgery at some point.
Dealing with incontinence
If your anterior prolapse is accompanied by stress incontinence — involuntary loss of urine during strenuous activity — your doctor may recommend one of a number of procedures to support the urethra (urethral suspension) and ease your incontinence symptoms.
Home remedies
Kegel exercises strengthen your pelvic floor muscles, which support the uterus, bladder and bowel. A strengthened pelvic floor provides better support for your pelvic organs and relief from symptoms associated with anterior prolapse.
To perform Kegel exercises, follow these steps:
- Tighten (contract) your pelvic floor muscles — the muscles you use to stop urinating.
- Hold the contraction for five seconds, then relax for five seconds. (If this is too difficult, start by holding for two seconds and relaxing for three seconds.)
- Work up to holding the contraction for 10 seconds at a time.
- Do three sets of 10 repetitions of the exercises each day.
Ask your health care provider for feedback on whether you’re using the right muscles. Kegel exercises may be most successful when they’re taught by a physical therapist and reinforced with biofeedback. Biofeedback involves using monitoring devices that help ensure you’re tightening the proper muscles with optimal intensity and length of time.
Once you’ve learned the proper method, you can do Kegel exercises discreetly just about anytime, whether you’re sitting at your desk or relaxing on the couch.





{kind=link}