Contents
What is D-Mannose
D-mannose is a simple sugar hexose, a fermentable monosaccharide extracted from the ash Fraxinus ornus and related plants, closely related to glucose (a C-2 epimer of glucose) 1). D-mannose exists naturally in many plants and fruits, and is found in human blood at concentrations less than one-fiftieth of that of glucose 2). D‐mannose powder has been available for some time for the treatment of UTIs in horses, cats and dogs 3). D-mannose is widely accessible for UTI (urinary tract infection) prevention for women 4), 5). D-mannose is rapidly absorbed and in about 30 minutes reaches the peripheral organs, then is excreted by the urinary tract 6). D-mannose can’t be transformed into glycogen, therefore, is not stored in the body 7). A long-term use of D-mannose, in concentrations up to 20%, has not shown any side effect on human metabolism 8). Currently, there are no reports of adverse effects of mannose in humans 9).
D-Mannose is an important metabolic intermediate required for biosynthesis of most of the structural and secretory glycoproteins in the body 10). Mannose-specific transport systems have been identified that may function specifically to retain and utilize mannose 11). Mannose can induce insulin release 12), and increased concentrations of mannose have been found in patients with diabetes mellitus 13), which could cause diabetic complications 14). Serum from patients with invasive candidiasis or aspergillosis have mannose concentrations 10 to 20 times higher than that found in normal serum 15). Carbohydrate-deficient glycoprotein syndrome type I has been shown to be associated with a deficiency of mannose utilization 16).
Table 1. Mannose: The Good, The Bad and The Ugly
| Outcome | Disorder | System | Mannose Effect |
|---|---|---|---|
| GOOD | MPI-CDG | Humans | Reverses most patient symptoms except for liver fibrosis. |
| Zebrafish | Early intervention rescue mpi– morphants. | ||
| Urinary Tract Infection | Humans | Mannose competes E.coli binding of FimH adhesins to epithelium. | |
| PMM2-CDG | Mice | Prenatal mannose rescues embryonic lethality. | |
| BAD/UGLY | MPI-CDG | Mice | Prenatal mannose causes embryonic lethality and eye defects in the survivors. |
| Diabetes | Humans | Diabetic complication: mannose glycates proteins 5 times better than glucose. | |
| Humans, Dogs | High mannose concentration correlates with diabetes. |
Footnote: MPI = Phosphomannose isomerase; CDG = Congenital Disorders of Glycosylation. Mannose supplements treat phosphomannose isomerase (MPI) deficient CDG patients.
MPI-CDG is a form of congenital disorders of N-linked glycosylation, characterized by cyclic vomiting, profound hypoglycemia, failure to thrive, liver fibrosis, gastrointestinal complications (protein-losing enteropathy with hypoalbuminaemia, life-threatening intestinal bleeding of diffuse origin), and thrombotic events (protein C and S deficiency, low anti-thrombine III levels), whereas neurological development and cognitive capacity is usually normal. The clinical course is variable even within families. The disease is caused by loss of function of the gene MPI (15q24.1).
PMM2-CDG is the most frequent form of congenital disorder of N-glycosylation and is characterized by cerebellar dysfunction, abnormal fat distribution, inverted nipples, strabismus and hypotonia. 3 forms of PMM2-CDG can be distinguished: the infantile multisystem type, late-infantile and childhood ataxia-intellectual disability type (3-10 yrs old), and the adult stable disability type. Infants usually develop ataxia, psychomotor delay and extraneurological manifestations including failure to thrive, enteropathy, hepatic dysfunction, coagulation abnormalities and cardiac and renal involvement. The phenotype is however highly variable and ranges from infants who die in the first year of life to mildly involved adults.
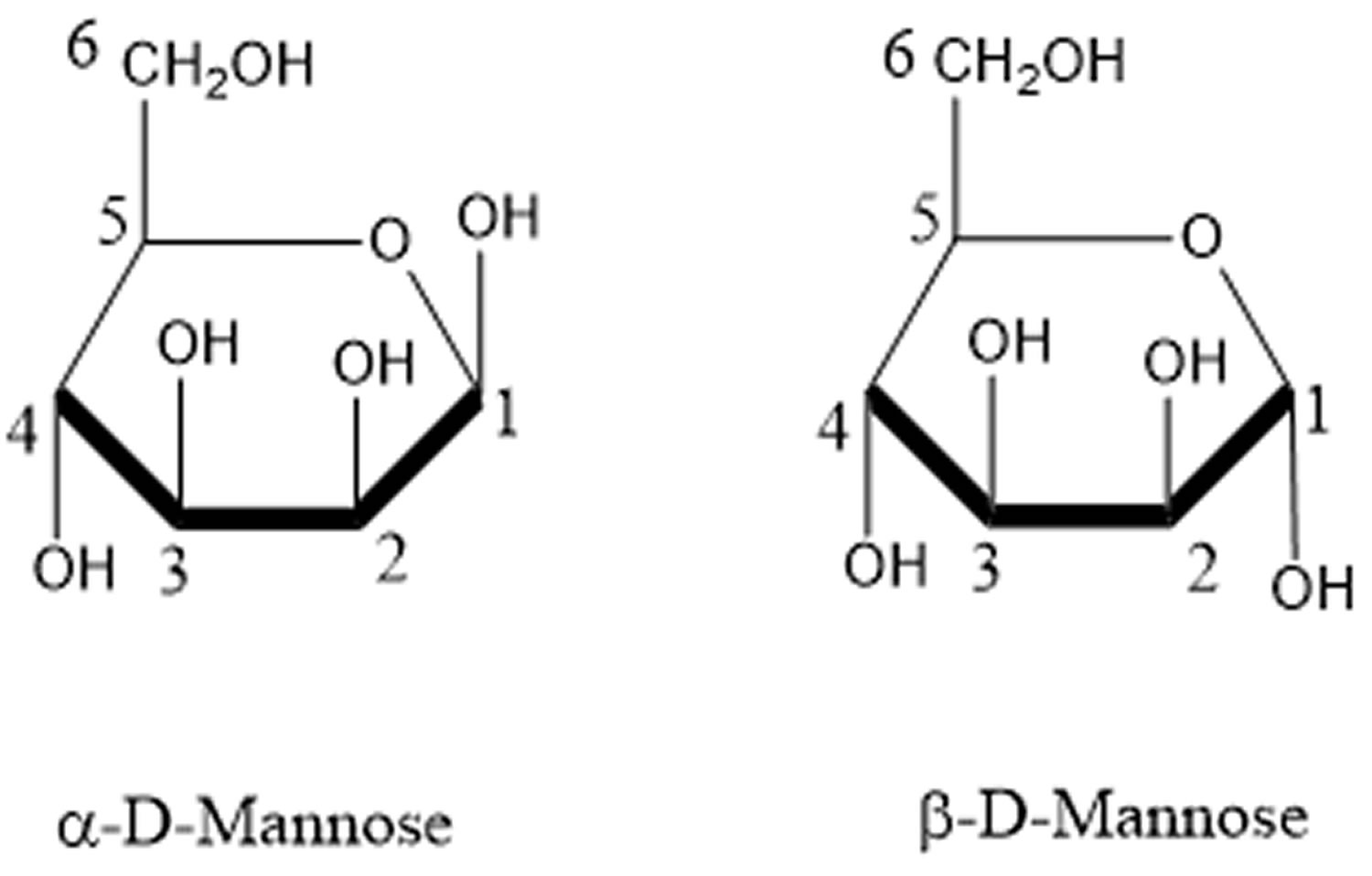
[Source 17) ]Figure 1. D-mannose
Mannose Chemistry
D-Mannose is the 2-epimer of glucose and exists primarily as sweet-tasting alpha- (67%) or as a bitter-tasting beta- (33%) anomer of the pyranose 18); furanose forms comprise <2%. Mannose is ~5x as active as glucose in non-enzyamtic glycation 19), which may explain why evolution did not favor it as a biological energy source. In the laboratory, mannose can be generated by oxidation of mannitol or by base-catalyzed epimerization of glucose through fructose 20). L-Mannose is not normally used in biological systems; however, its structural similarity to naturally occurring L-rhamnose enables some plant enzymes to use L-mannose as an unnatural substrate in vitro 21).
Occurrence, origins and dietary sources of mannose
Mannose occurs in microbes, plants and animals. Free mannose is found in small amounts in many fruits such as oranges, apples and peaches 22) and in mammalian plasma at 50–100 μM 23). More often, mannose occurs in homo-or hetero-polymers such as yeast mannans (α-mannose) where it can account for nearly 16% of dry weight 24) or in galactomannans 25). Ivory nuts, composed of β-mannans (sometimes called vegetable ivory) are quite hard and used for carving and manufacturing buttons. In fact, ivory nut shavings were the original industrial source of mannose 26). Coffee beans, fenugreek and guar gums are rich sources of galactomannans 27), but these plant polysaccharides are not degraded in the mammalian gastrointestinal tract and, therefore, provide very little bio-available mannose for glycan synthesis. These polysaccharides are partially digested by anaerobic bacteria in the colon 28). Small amounts of bio-available mannose occur in glycoproteins.
Mannose metabolism in cells
Mannose is transported into mammalian cells via facilitated diffusion hexose transporters of the SLC2A group (GLUT) present primarily on the plasma membrane. Various cell lines transport 6.5 – 23.0 nmols/hr/mg protein 29), but no mannose-specific or -preferential transporters have been reported among the 14 distinct GLUT transporters found in humans 30). Most studies of GLUT substrate specificity assess only transport of glucose and fructose, but very rarely mannose transport. Several reports describe SGLT-like mannose transporters in the intestine and kidney, where they could deliver free mannose from the diet or recover it from the urine 31). To date, there is no evidence for the physiological importance of these transporters. Within the cell, mannose is phosphorylated by hexokinase (HK) to produce mannose-6-phosphate (Man-6-P), which serves as a common substrate for three competing enzymes. It is either catabolized by phosphomannose isomerase (MPI) or directed into N-glycosylation via phosphomannomutase (PMM2). Another minor pathway utilizes mannose for synthesis of 2-keto-3-deoxy-D-glycero-D-galacto-nononic acid (KDN), a sialic-acid related molecule found in fish and mammals 32) (Figure 2). The fate of Man-6-P largely depends on the ratio of MPI to PMM2 within a cell 33) – higher ratio leads to greater catabolism, while lower ratio favors the glycosylation pathway. PMM2-derived mannose-1-phosphate (Man-1-P) is then incorporated into several glycosylation intermediates including GDP-mannose (GDP-Man), GDP-fucose, and dolichol phosphate mannose (Dol-P-Man). These intermediates then contribute to N-glycosylation, O-glycosylation, C-mannosylation, and GPI anchor synthesis (Figure 2).
Mannose metabolism in humans
Human plasma contains ~50μM mannose which is primarily derived from N-glycan processing 34). Mannose is absorbed through the intestine and metabolized. A bolus of <0.2g/Kg body weight increases mannose concentration by 3-fold with a clearance T 1/2 of ~ 4hr, without affecting glucose concentration. Higher doses cause mild gastro-intestinal discomfort, but no other side effects 35). Pregnant women with diabetes mellitus show elevated mannose levels in fasted blood and amniotic fluid which correlated with high glucose concentration 36) and several show that mannose levels are closely linked to glucose metabolism 37). How this impacts glycosylation is not known.
Multiple genetic disorders disrupt intermediary mannose metabolism. Genetic defects in MPI and PMM2 cause MPI-CDG and PMM2-CDG, two congenital disorders of glycosylation (CDG). These patients have substantially reduced enzyme activities and suffer from multi-organ insufficiencies. PMM2-CDG is the most prevalent type of CDG, typically showing hypotonia, psychomotor retardation, cerebellar hypoplasia and cerebral atrophy 38). MPI-CDG patients have hypoglycemia, coagulopathy, hepato-intestinal symptoms, and in some cases liver fibrosis 39), but they are neurologically normal 40).
Figure 2. Mannose metabolic pathway
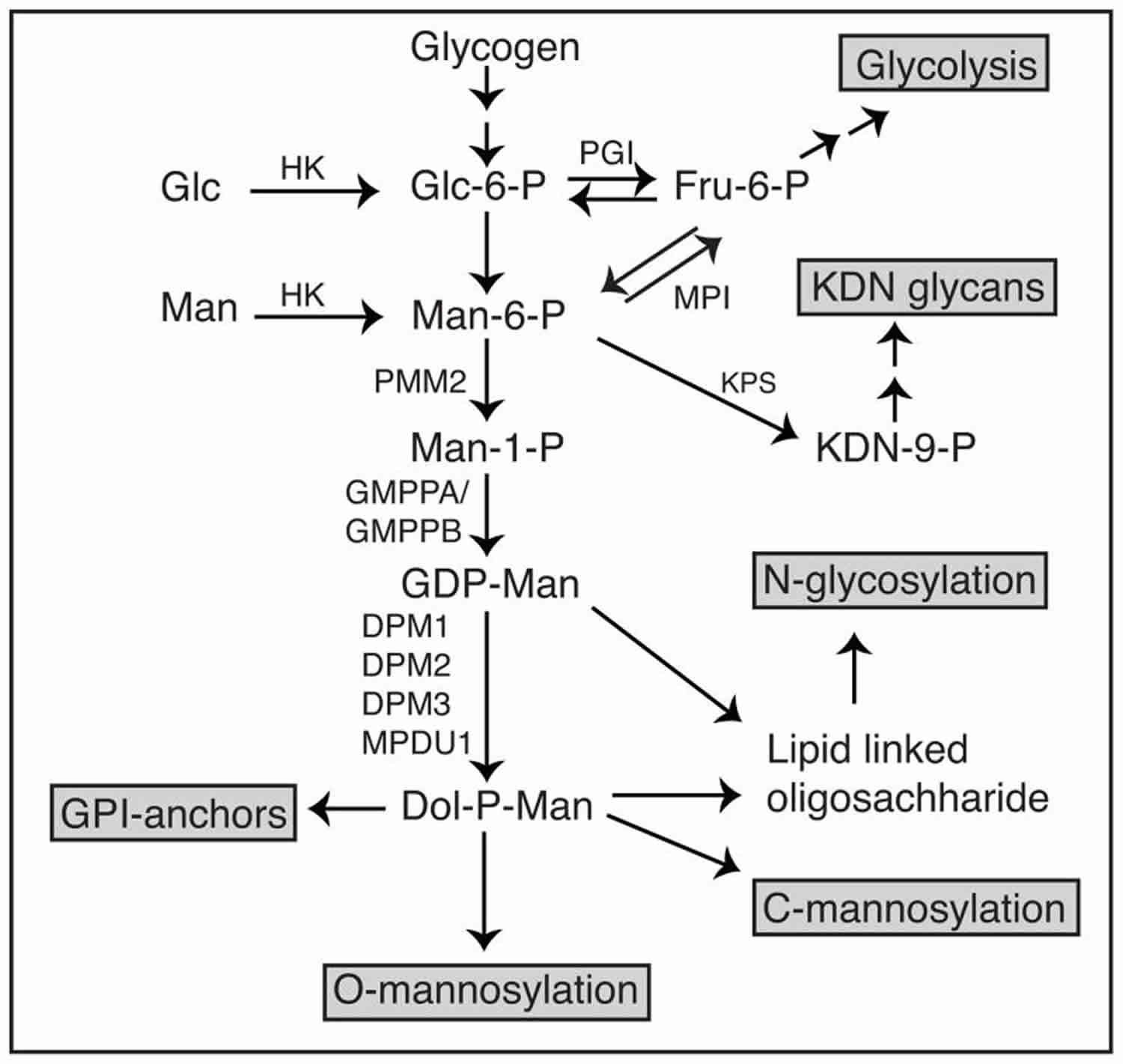 Abbreviations: Man = Mannose; Glc = Glucose; HK = Hexokinase; MPI = phosphomannose isomerase; PMM2 = phosphomannomutase; GMPP(A/B) = GDP-mannose pyro-phosphorylase (A/B); PGI = phosphoglucose isomerase; KPS = KDN-9-phosphate synthase; Man-6-P = mannose-6-phosphate; Fru-6-P = fructose-6-phosphate,Glc-6-P = glucose-6-phosphate; GDP-Man = GDP-mannose; Dol-P-Man = dolichol phosphate mannose; DPM = Dol-P-Man synthase.
Abbreviations: Man = Mannose; Glc = Glucose; HK = Hexokinase; MPI = phosphomannose isomerase; PMM2 = phosphomannomutase; GMPP(A/B) = GDP-mannose pyro-phosphorylase (A/B); PGI = phosphoglucose isomerase; KPS = KDN-9-phosphate synthase; Man-6-P = mannose-6-phosphate; Fru-6-P = fructose-6-phosphate,Glc-6-P = glucose-6-phosphate; GDP-Man = GDP-mannose; Dol-P-Man = dolichol phosphate mannose; DPM = Dol-P-Man synthase.
D-Mannose UTI treatment
The European Food Safety Authority Panel concludes that “a cause and effect relationship has not been established between the consumption of the cranberry extract and D-mannose containing food supplement (D-mannose 1200 mg and cranberry extract not less than 400 mg) and the reduction of the risk of urinary tract infection by inhibiting the adhesion of certain bacteria in the urinary tract” 42). A small pilot study done in 2015 43) involving 43 Italian women aged between 18 and 65 years (mean age 46.7) with symptoms of acute cystitis (dysuria, frequency, urgency, supra-pubic pain, nicturia, and hematuria) or asymptomatic with diagnosis of UTI using D-mannose for acute uncomplicated cystitis where D-mannose compound was administered twice daily for 3 days and then once a day for 10 days. After completing the initial 10 days treatment, one month after diagnosis patients were consecutively randomized in two groups: some women received prophylaxis (n = 22) with D-mannose for 6 months (once a day for a week every other month) and others remained untreated (n = 21). Of those treated with D-mannose a week per month every other month, 1 (4.5%) had a recurrence within 6 months. UTIs onset was 43 days in the group undergoing D-mannose prophylaxis compared to 28 days for the placebo group (no D-mannose). D-mannose treatment did not present any side effect also in a long-term schedule. In that pilot study, D-mannose had significant effects on specific symptoms, such as on painful urination, frequent urination, urgency, supra-pubic pain, tenesmus and nightime urination. No statistically significant differences were observed regarding backache and blood in urine (hematuria). Also in other studies 44), 45) no significant differences in the prevalence and severity of blood in urine (hematuria) were recorded. Mean follow up was 11.8 months (range between 8.2 and 14 months). Two of these 43 patients had no resolution of symptoms and they needed the addition of antibiotic therapy to resolve the infection. The conclusion from the pilot study was that D-mannose might be effective for reducing the incidence of UTI in selected patients with uncomplicated acute cystitis in a 6-month period and consequently in increasing women’s quality of life. However, randomized clinical trial will be required to validate and confirm the results of this study, considering particularly the small sample size, but initial findings show that D-mannose may be useful for UTI prevention, but further clinical trials will be necessary 46), 47).
D-Mannose dosage for UTI
From a small pilot study 48), D-mannose 1.5 g mixed with sodium bicarbonate, sorbitol and silicon dioxide was taken twice daily for 3 days and then once a day for 10 days for acute uncomplicated cystitis. And for prophylaxis, D-mannose 1.5 g compound was taken once a day for a week every other month 49).
References [ + ]


{kind=link}