
Contents
What are dental sealants
Dental sealants are thin, protective coatings (made from plastic or other dental materials) that adhere to the chewing surface of your back teeth (molars) to prevent dental cavities or tooth decay. Dental sealants protect the chewing surfaces from cavities by covering them with a protective shield that blocks out germs and food. Once applied, sealants protect against 80% of cavities for 2 years and continue to protect against 50% of cavities for up to 4 years. However, dental sealants are no substitute for brushing and flossing, but dental sealants can keep cavities from forming and may even stop early stages of tooth decay from becoming a full-blown cavity.
In fact, dental sealants have been shown to reduce the risk of decay by nearly 80% in molars. This is especially important when it comes to your child’s dental health. In October 2016, the Centers for Disease Control and Prevention (CDC) 1 released a report on the importance of dental sealants for school-aged children, of which only 43% of children ages 6-11 have. According to the CDC, “school-age children without sealants have almost three times more cavities than children with sealants.”
Dental sealants can be clear, white, or slightly tinted. Usually, you cannot see a sealant when a child talks or smiles.
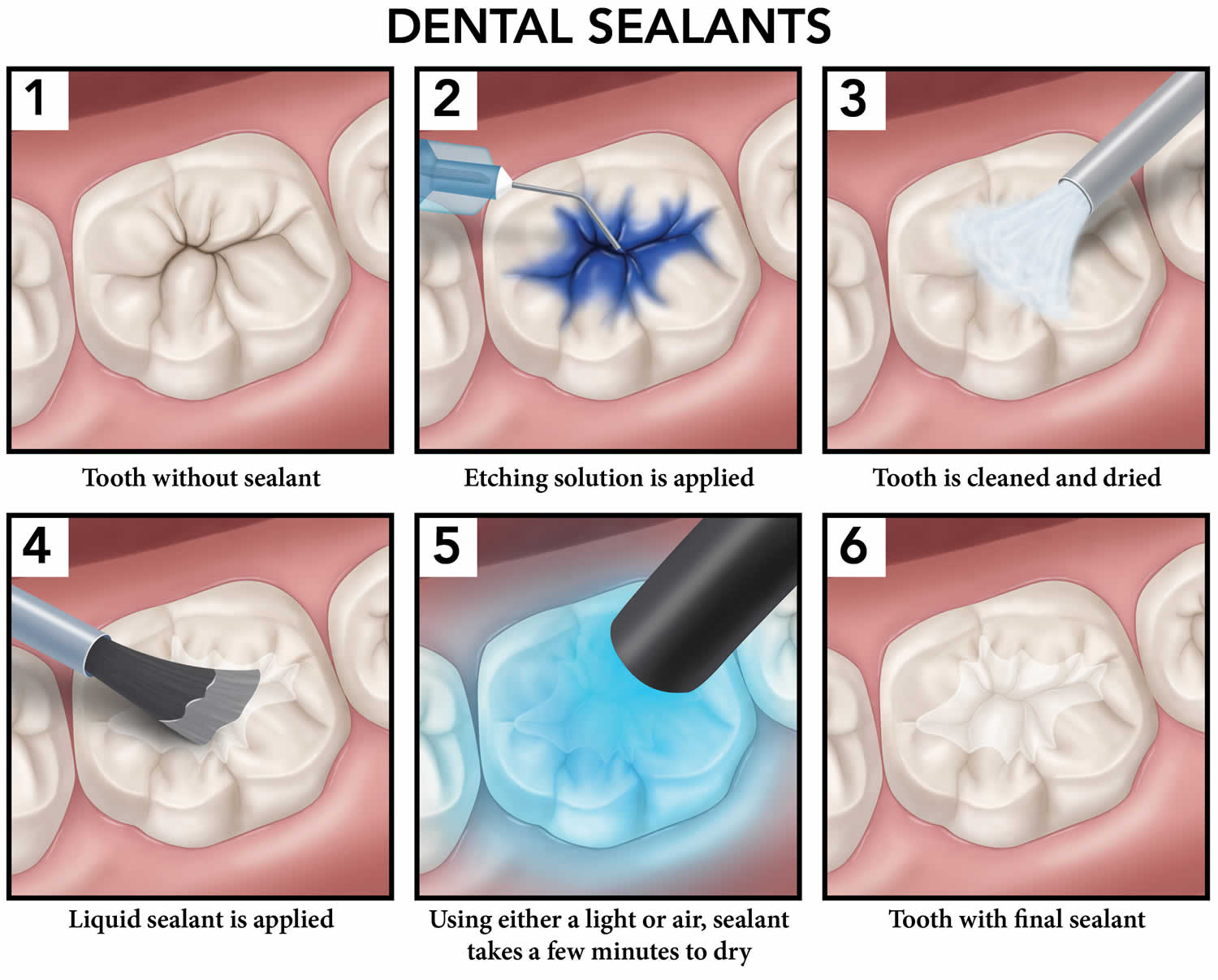
Figure 1. Dental sealants procedure
Are dental sealants safe?
Bisphenol A (BPA) is a synthetic chemical resin used worldwide to produce plastic products such as polycarbonate plastics (clear plastics) and epoxy resins. Polycarbonate plastics have many applications including use in some food and drink packaging, e.g., water and infant bottles, compact discs, impact-resistant safety equipment, and medical devices. Epoxy resins are used as lacquers to coat metal products such as food cans, bottle tops, and water supply pipes. Some dental sealants and composites may also contribute to BPA exposure.
Bisphenol A (BPA) is also a component of the bisphenol A diglycidylether methacrylate (Bis-GMA), which is a monomer found in resin-based dental sealants 2. Although BPA is not present in a pure form in these materials, its derivatives, the Bis-GMA and the Bis-DMA are. Consequentially, trace molecules can be found due to degradation, incomplete polymerisation or impurity deriving from the manufacturing process. Moreover, BPA can also be released by resin-based materials because of the enzymatic salivary hydrolysis of BPA derivatives, such as the bis-GMA or the bis-DMA 3.
Human health effects from BPA at low environmental exposures are unknown 4. BPA has been shown to affect the reproductive systems of laboratory animals. More research is needed to understand the human health effects of exposure to BPA 4.
One reason people may be concerned about BPA is because human exposure to BPA is widespread. The 2003-2004 National Health and Nutrition Examination Survey (NHANES III) conducted by the Centers for Disease Control and Prevention (CDC) found detectable levels of BPA in 93% of 2517 urine samples from people six years and older. The CDC NHANES data are considered representative of exposures in the United States. Another reason for concern, especially for parents, may be because some animal studies report effects in fetuses and newborns exposed to BPA.
In the fall of 2014, U.S. Food and Drug Administration (FDA) experts from across the agency, specializing in toxicology, analytical chemistry, endocrinology, epidemiology, and other fields, completed a four-year review of more than 300 scientific studies 5. The FDA review has not found any information in the evaluated studies to prompt a revision of FDA’s safety assessment of BPA in food packaging at this time.
- “FDA continues to review the available information and studies on BPA. FDA will update its assessment of BPA and will take additional action if warranted. Based on FDA’s ongoing safety review of scientific evidence, the available information continues to support the safety of BPA for the currently approved uses in food containers and packaging.” 6
The FDA’s National Center for Toxicological Research is continuing with an additional study:
- Rodent chronic toxicity study, which is currently underway. Using the data and design from the rodent subchronic study, the National Toxicology Program/Food and Drug Administration (NTP/FDA) is conducting a long-term toxicity study of BPA in rodents to assess a variety of endpoints, including novel endpoints where questions have been raised. As an addition to this core study, FDA is providing extra animals and tissues to a consortium of grantees 7 selected and funded by the National Institute of Environmental Health Sciences to address other critical questions.
A 2019 systematic review of exposure to bisphenol A (BPA) from dental treatment 8 found that urinary BPA concentrations increase 24 hours after dental treatment. One study showed that urinary BPA concentrations return to baseline by 14 days. Additional research is needed to determine the magnitude of change from pre- to post-dental treatment and the trajectory of urinary BPA concentrations post-treatment 8.
There is a number of reports on BPA exposure and adverse perinatal development 2. Molar Incisor Hypomineralisation is a recently reported condition which affects the first molars and the permanent incisors. Randomly scattered white opacities are present on the enamel and a variable prevalence of 2.4% to 40% is reported in children aged 6 to 8 years 2. Although there are different possible causes for this condition, an association with postnatal BPA exposure has been made and is possibly related to the fact that ameloblasts are susceptible to BPA exposure 2.
How long do dental sealants last?
Dental sealants have been shown to still work 9 years after placement. However, sometimes they do fall off, so they should be checked at regular dental appointments. If a tooth loses a sealant, the protective shield is gone and the tooth can get a cavity. Missing sealants are easy to replace.
Dental sealants controversy
Bisphenol A (BPA) is a synthetic chemical resin used worldwide to produce plastic products. Bisphenol A (BPA) is also a component of the bisphenol A diglycidylether methacrylate (Bis-GMA), which is a monomer found in resin-based dental sealants 2. Although BPA is not present in a pure form in these materials, its derivatives, the Bis-GMA and the Bis-DMA are. Consequentially, trace molecules can be found due to degradation, incomplete polymerisation or impurity deriving from the manufacturing process. Moreover, BPA can also be released by resin-based materials because of the enzymatic salivary hydrolysis of BPA derivatives, such as the bis-GMA or the bis-DMA 3. The controversy about dental sealants possible toxicity begins around the early ’30s. Even if the amount of BPA released by dental sealants is well below the limit proposed by the U.S. Environmental Protection Agency and the European Food Safety Authority 2.
In a 2014 study by McKinney et al. 9, despite the
fact that children who had dental sealants had a BPA concentration 20% to 25% higher than children with no dental sealants, there was no statistically significant
association between the number of resin-based dental sealants and urinary BPA concentrations. The American Dental Association Science Institute tested the BPA release from 12 dental sealants used by dentists in the U.S.: The results indicated that BPA release from dental sealants is very low, about 0.09 nanograms per day 2. This amount is well below the limit proposed for a 6-year-old child (who weighs about 20 kilograms, or 44 pounds) by the US Environmental Protection Agency (1 million nanograms per day) and the European Food Safety Authority (80,000 nanograms per day).
Conclusions
There is strong evidence that resin-based dental sealants improve children’s oral health 2. Also, BPA exposure from dental materials seems transient and can potentially be controlled. Moreover, most studies report that BPA levels detected in vitro and in vivo are lower than the current recommended tolerable daily intake (TDI). The tolerable daily intake (TDI) value has been modified over the years and may be further reduced in the near future. Dentists must be aware of these possibilities and should take appropriate measures.
In conclusion, dental practitioners should be knowledgeable and give parents reliable and timely advices and answers about the topic.
Recommendations for resin-based dental sealants application
To reduce BPA exposure during application of resin-based dental sealants precautionary measures should be taken, and since the higher risk for potential exposure is the immediate post-dental sealants application, these measures are particularly relevant.
One technique entails removal of residual monomer by rubbing the monomer layer with pumice on a cotton roll or having the patient gargling for 30 seconds and spitting immediately after application of the dental sealant or composite. However, proper rinsing and spitting can be challenging for most children, hence rinsing with an air-water syringe may be a suitable substitute. As for all dental procedures, the use of a rubber dam to control the operative field would further limit potential exposure.
- Dental Sealants Prevent Cavities. https://www.cdc.gov/vitalsigns/dental-sealants/index.html[↩]
- Dental Sealants Part 4: Bisphenol A: What dentists should know. Eur J Paediatr Dent. 2018 Dec;19(4):333-334. doi: 10.23804/ejpd.2018.19.04.15 http://ejpd.eu/EJPD_2018_19_4_15.pdf[↩][↩][↩][↩][↩][↩][↩][↩]
- Rathee M, Malik P, Singh J. Bisphenol A in dental sealants and its estrogen like effect. Indian J Endocrinol Metab 2012; 16: 339[↩][↩]
- Bisphenol A (BPA) Factsheet. https://www.cdc.gov/biomonitoring/BisphenolA_FactSheet.html[↩][↩]
- Bisphenol A (BPA): Use in Food Contact Application. https://www.fda.gov/downloads/NewsEvents/PublicHealthFocus/UCM424266.pdf[↩]
- Bisphenol A (BPA): Use in Food Contact Application. https://www.fda.gov/NewsEvents/PublicHealthFocus/ucm064437.htm[↩]
- Schug et al. (2013) A new approach to synergize academic and guideline-compliant research: the CLARITY-BPA research program. Reprod Toxicol. 40:35-40.[↩]
- Marzouk, T., Sathyanarayana, S., Kim, A. S., Seminario, A. L., & McKinney, C. M. (2019). A Systematic Review of Exposure to Bisphenol A from Dental Treatment. JDR Clinical & Translational Research, 4(2), 106–115. https://doi.org/10.1177/2380084418816079[↩][↩]
- McKinney C, Rue T, Sathyanarayana S, Martin M, Seminario AL, et al. Dental sealants and restorations and urinary bisphenol A concentrations in children in the 2003-2004 National Health and Nutrition Examination Survey. J Am Dent Assoc 2014; 145: 745-750.[↩]





{kind=link}