Contents
What is dermatomyositis
Dermatomyositis is a rare type of inflammatory myopathy characterized by inflammatory and degenerative changes of the muscles and skin. Dermatomyositis is diagnosed in 2-10 people per million each year. Myopathy is a group of muscle diseases that involves inflammation of the muscles or associated tissues, such as the blood vessels that supply the muscles. Dermatomyositis associated symptoms and physical findings may vary widely from case to case as patients may present differently.
Dermatomyositis can affect adults and children, but commonly onset is following middle-age. In adults, dermatomyositis usually occurs from the late 40s to early 60s. In children (juvenile dermatomyositis), it most often appears between 5 and 15 years of age. Juvenile dermatomyositis has a better prognosis than adult patients. Dermatomyositis is more common in Caucasians and females are affected about twice as often as males.
Muscle abnormalities may begin with aches and weakness of the muscles of the trunk, upper arms, hips, and thighs (proximal muscles). Muscles may be stiff, sore, tender and, eventually, show signs of degeneration (atrophy). Affected individuals may experience difficulty in performing certain functions, such as raising their arms and/or climbing stairs or develop speech and swallowing difficulties. Skin abnormalities associated with dermatomyositis often include a distinctive reddish-purple rash (heliotrope rash) on the upper eyelid or across the cheeks and bridge of the nose in a “butterfly” distribution and on the forehead and scalp. Other characteristic rashes include scaling and redness of the knuckles, elbows, knees, and/or other extensor regions (Gottron papules and sign); an abnormal accumulation of fluid (edema) in body tissues surrounding the eyes; and/or other features. The symptoms of childhood (juvenile) dermatomyositis are similar to those associated with the adult form of the disorder. However, onset is usually more sudden. In addition, abnormal accumulations of calcium deposits (calcifications) in muscle and skin tissues as well as involvement of the digestive (gastrointestinal [GI]) tract are more common in juvenile dermatomyositis. Introduction
The inflammatory myopathies are a group of diseases that involve chronic muscle inflammation and weakness. The cause of dermatomyositis is unknown, but the disease has much in common with autoimmune disorders, in which your immune system mistakenly attacks your body tissues for unknown reasons, leading to inflammation or swelling. Small blood vessels in muscular tissue are particularly affected in dermatomyositis. Inflammatory cells surround the blood vessels and eventually lead to destruction of muscle fibers.
Table 1. Definitions of terms used to describe dermatomyositis
| Term | Definition |
|---|---|
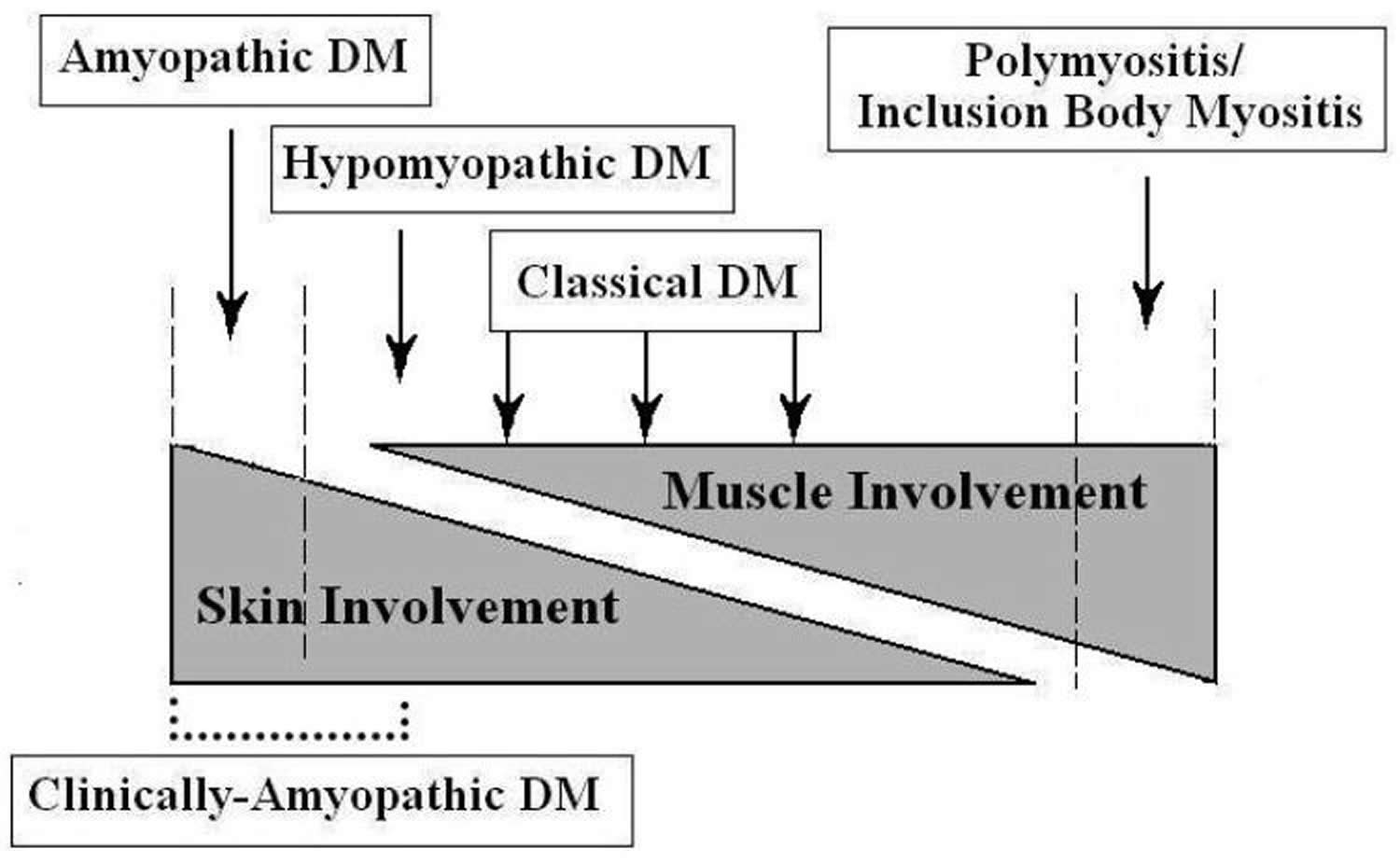
| Amyopathic dermatomyositis | A subset of dermatomyositis patients characterised by biopsy-confirmed hallmark cutaneous manifestations of classical dermatomyositis occurring for 6 months or longer with no clinical evidence of proximal muscle weakness and no serum muscle enzyme abnormalities. If more extensive muscle testing is carried out, the results should be within normal limits (if such results are positive or abnormal, the patient can be classified as having “hypomyopathic dermatomyositis”). |
| Classic dermatomyositis | Patients having the hallmark cutaneous manifestations of dermatomyositis, proximal muscle weakness, and laboratory evidence of muscle inflammation that is characteristic of dermatomyositis. |
| Hypomyopathic dermatomyositis | A designation for patients with cutaneous dermatomyositis and no clinical evidence of muscle disease (i.e. weakness) for 6 months or longer, who during evaluation are found to have subclinical evidence of myositis upon laboratory (e.g. muscle enzymes), electrophysiological, and/or radiological evaluation. |
| Clinically amyopathic dermatomyositis | A term that includes both amyopathic dermatomyositis and/or hypomyopathic dermatomyositis patients (i.e. clinically amyopathic dermatomyositis = amyopathic dermatomyositis + hypomyopathic dermatomyositis). The clinically amyopathic dermatomyositis designation has been coined to emphasize the fact that the predominant clinical problem is skin disease. |
Figure 1. Idiopathic Inflammatory Dermatomyopathy Spectrum
The most common signs and symptoms of dermatomyositis include:
- Skin changes. A violet-colored or dusky red rash develops, most commonly on your face and eyelids and on knuckles, elbows, knees, chest and back. The rash, which can be itchy and painful, is often the first sign of dermatomyositis.
- Muscle weakness. Progressive muscle weakness involves the muscles closest to the trunk, such as those in your hips, thighs, shoulders, upper arms and neck. The weakness affects both the left and right sides of your body, and tends to gradually worsen.
There’s no cure for dermatomyositis, but periods of symptom improvement (remission) can occur. Treatment can clear the skin rash and help you regain muscle strength and function.
Most patients will require treatment throughout their lifetime, but dermatomyositis completely resolves in about one-in-five patients. Patients who have disease affecting their heart or lungs, or who also have an underlying cancer do less well and may ultimately die from their disease.
Dermatomyositis Associated conditions
Dermatomyositis may cause other conditions or put you at higher risk of developing them, including:
- Raynaud’s phenomenon. This condition causes your fingers, toes, cheeks, nose and ears to turn pale when exposed to cold temperatures.
- Other connective tissue diseases. Other conditions, such as lupus, rheumatoid arthritis, scleroderma and Sjogren’s syndrome, can occur with dermatomyositis (overlap syndromes).
- Cardiovascular disease. Dermatomyositis can cause heart muscle inflammation (myocarditis). In a small number of people who have dermatomyositis, congestive heart failure and heart arrhythmias develop.
- Lung disease. Interstitial lung disease can occur with dermatomyositis. Interstitial lung disease refers to a group of disorders that cause scarring (fibrosis) of lung tissue, making the lungs stiff and inelastic. Signs and symptoms include a dry cough and shortness of breath.
- Cancer. Studies have shown an increased risk of developing certain forms of cancer in adults patients with dermatomyositis. Dermatomyositis in adults has been linked to an increased likelihood of developing cancer, particularly of the cervix, lungs, lymphoma, pancreas, breasts, ovaries and gastrointestinal tract. Risk of cancer increases with age, although it appears to level off three years or so after a diagnosis of dermatomyositis. Dermatomyositis can also develop after you receive a diagnosis of cancer.
Figure 2. Dermatomyositis rash



Figure 3. Dermatomyositis rash (Gottron papules and signs)

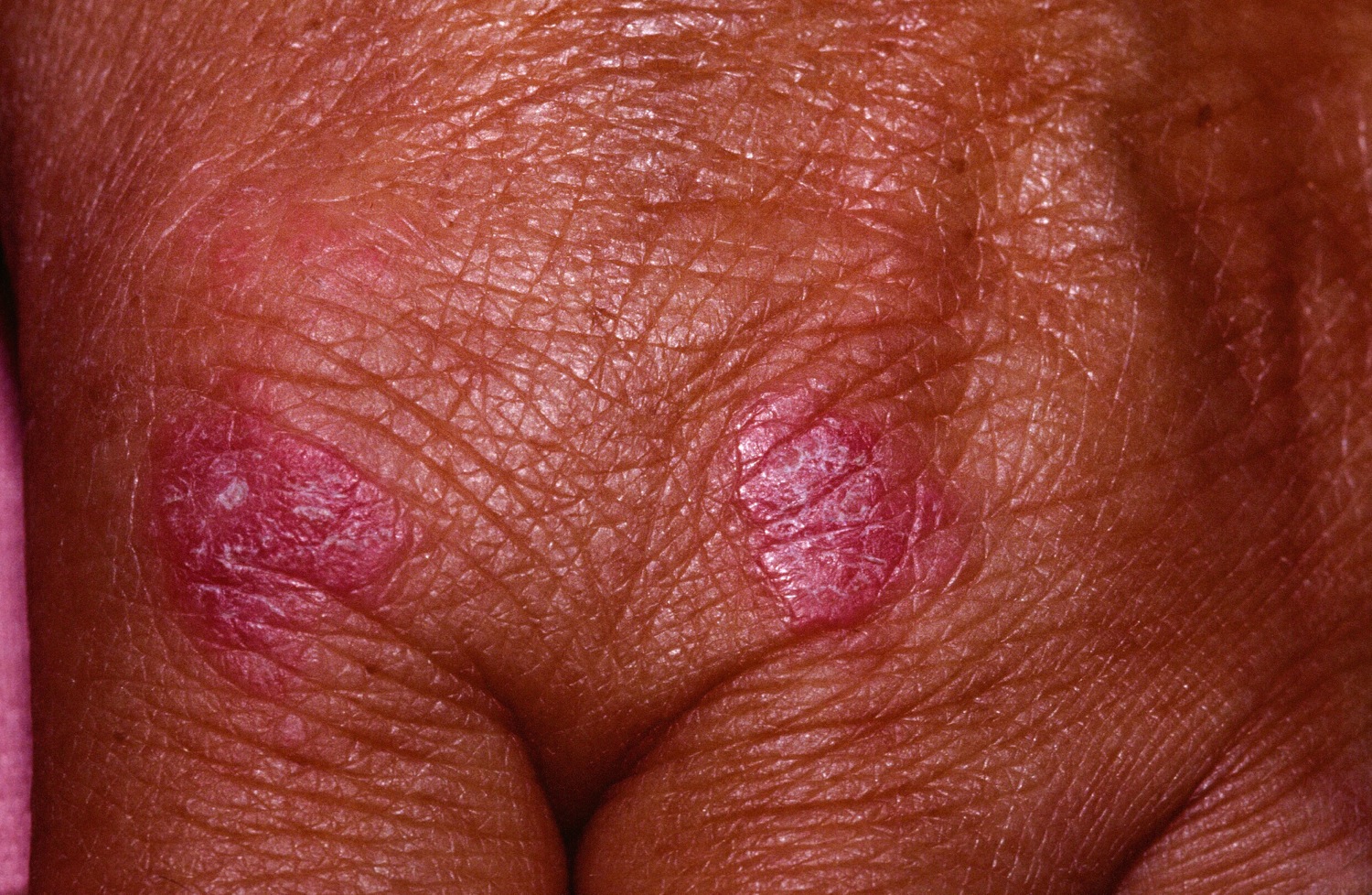
Figure 4. Dermatomyositis rash (note the erythema along the glabellar area/ lower forehead and mild periorbital erythema. The latter finding is called a heliotrope)

Amyopathic dermatomyositis
Amyopathic dermatomyositis also called dermatomyositis sine myositis, is a subset of dermatomyositis patients characterized by biopsy-confirmed hallmark cutaneous manifestations of classic dermatomyositis occurring for 6 months or longer with no clinical evidence of proximal muscle weakness and no serum muscle enzyme abnormalities 2. If more extensive muscle testing is carried out, the results should be within normal limits (if such results are positive or abnormal, the patient can be classified as having “hypomyopathic dermatomyositis” 3. Preliminary population-based data suggest that amyopathic dermatomyositis might account for 20% of all dermatomyositis patients 4, this percentage may be higher in Asian populations 5. Several studies also have indicated an increased risk of lung disease 6, but the extent of this risk is unclear.
Clinically, amyopathic dermatomyositis is frequently associated with interstitial lung disease, which usually has a rapidly progressive, fatal clinical course. Although clinically, amyopathic dermatomyositis-related interstitial lung disease is well described, data on the histopathology of clinically, amyopathic dermatomyositis-interstitial lung disease are limited. Organizing pneumonia and pulmonary vasculitis have rarely been reported. The prevalence of interstitial lung disease in patients with amyopathic dermatomyositis is higher in Korea and Japan than in Western countries 7. The reported prevalence of interstitial lung disease in Korean patients with amyopathic dermatomyositis is 83.3%, while Yamanishi reported that 71% of 21 Japanese patients with amyopathic dermatomyositis had interstitial lung disease 8. In Asian populations, amyopathic dermatomyositis-interstitial lung disease is reportedly rapidly progressive and frequently unresponsive to glucocorticoid treatment, leading to poor survival 9.
Figure 5. Amyopathic dermatomyositis
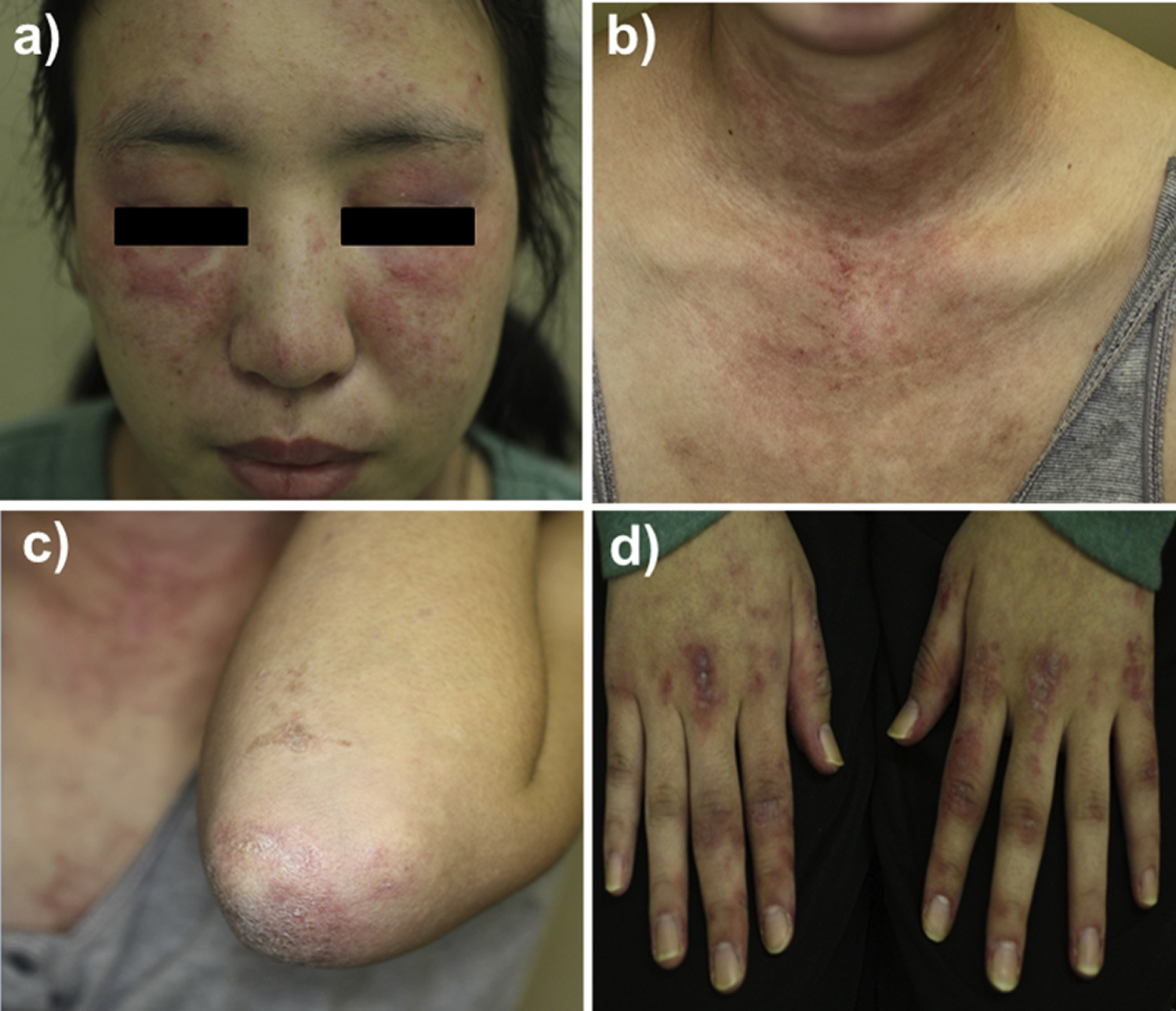
Note: Physical findings suggestive of clinically amyopathic dermatomyositis. a) facial erythema and heliotrope rash; b) erythema over the V area of the neck; c) scaly erythema with ulceration over the elbow; d) Gottron’s sign.
[Source 10]Juvenile dermatomyositis
Juvenile dermatomyositis is an inflammatory disease that causes muscle weakness and a skin rash on the eyelids and knuckles. Approximately three in 1,000,000 children are affected by juvenile dermatomyositis. Juvenile dermatomyositis affects an estimated 3,000-5,000 children in the United States. All age and ethnic groups are affected. Most cases occur in children ages 5-10. Roughly 1 in 5 children also has joint symptoms, but they are likely to be mild. Remission is possible, but a minority of children with Juvenile dermatomyositis may have a more chronic disease course.
Juvenile dermatomyositis causes
The cause of juvenile dermatomyositis is unknown. It is believed that abnormalities in the body’s immune system lead to inflammation and damage to muscle cells or the blood vessels in the muscle and skin.
Juvenile dermatomyositis symptoms
The first sign of Juvenile dermatomyositis is usually a red or purplish skin rash on the eyelids or cheeks. A patchy rash may also appear around the nails, elbows, knees, chest and back. Muscle weakness may begin at the same time as the skin rash, or it may begin days, weeks or months after. The weakness is usually in the neck, shoulders, back and stomach. Running, climbing stairs, sitting from a lying position or standing from a seated position may become difficult.
Other signs may include falling, weak voice (dysphonia) or problems swallowing (dysphagia). About half of children with Juvenile dermatomyositis have pain in their muscles. Some children may develop calcinosis (hardened lumps of calcium under the skin) or contractures, in which muscles shorten and cause joints to stay bent.
Juvenile dermatomyositis diagnosis
To make a diagnosis of Juvenile dermatomyositis, the doctor will examine the child and ask questions about his or her medical history and symptoms. The telltale dermatomyositis rash is an important part of the diagnosis. Specific diagnostic tests that may be done include:
- Magnetic resonance imaging. MRI can reveal subtle muscle inflammation and swelling early in the disease.
- Electromyography. This test measures the electrical activity in the muscles by inserting a thin needle into the affected area.
- Muscle biopsy. A small piece of muscle tissue is removed and examined under a microscope. In Juvenile dermatomyositis, inflammatory cells surround and damage the small blood vessels in the muscle. This can be seen with a biopsy.
- Blood tests. Laboratory tests can measure the levels of certain enzymes (proteins) produced by inflamed muscles. A blood test also can detect autoantibodies associated with Juvenile dermatomyositis, which can help determine the best treatment.
- Nailfold capillaroscopy. This noninvasive test involves placing a bit of oil onto the skin at the bottom of a fingernail. The nail is then examined using a magnifying scope. It can reveal swelling and changes in the capillaries (blood vessels).
Juvenile dermatomyositis treatment
The goal of Juvenile dermatomyositis treatment is to reduce inflammation, improve function and prevent disability. This is accomplished through a combination of medications, physical and speech therapy and self-care methods.
Medications that may be prescribed include:
- Corticosteroids. Corticosteroids are powerful anti-inflammatory drugs. They often are used first in treating inflammatory myopathies such as Juvenile dermatomyositis, because they work quickly. Due to side effects, they are not used for a long time.
- Methotrexate. Methotrexate works more slowly to reduce inflammation in Juvenile dermatomyositis, but it has fewer side effects than corticosteroids.
- Intravenous immunoglobulin (IVIg). Immunoglobulin contains healthy antibodies from blood donors. They can block harmful antibodies that attack muscle and skin.
- Other drugs. Other medications that may be used in the treatment of Juvenile dermatomyositis include cyclosporine, azathioprine, tacrolimus, hydroxychloroquine or anti-TNF therapy.
Additional treatments include:
- Physical therapy. Exercises can maintain and improve strength and flexibility. Physical therapy is directed at preventing muscle wasting, stiffness and contractures.
- Speech therapy. If the throat muscles become weak, speech therapy can help improve speech and swallowing.
- Skin protection. Sun protection may help control skin disease and potential muscle disease. Sunscreen, wide-brimmed hats, protective clothing and avoiding sun exposure during peak hours are important.
Self care
Since juvenile dermatomyositis can be a chronic (long-term) disease, it is important to take a proactive part in treatment. Maintaining good general health is essential. Physical activity and performing prescribed physical therapy exercises will help the person regain and maintain muscle strength. If swallowing is affected, preparing foods that are safe to eat and performing speech therapy exercises will aid in nutrition and overall well-being.
Dermatomyositis causes
Dermatomyositis is considered one of the connective tissue diseases, like systemic sclerosis and lupus erythematosus. Why dermatomyositis occurs remains unknown but research is taking place to identify factors that may play a part in its development, some of which are listed below.
- Genetic predisposition
- Underlying cancer (more likely in the elderly)
- Autoimmune defect (immune reaction against self)
- Infectious or toxic agents acting as triggers
- Drug-induced (implicated drugs include hydroxyurea, penicillamine, statins, quinidine, and phenylbutazone)
The specific underlying cause(s) of dermatomyositis remain unknown. However, evidence suggests that genetic, immune, and environmental factors play some role. Underlying genetic and immune mechanisms may be suggested by various findings, including an increased frequency of certain genetically determined HLAs or “human leukocyte antigens” in individuals with the disorder. HLAs are proteins that play an important role in the body’s immune system, influence the outcome of transplantation, and appear to affect an individual’s predisposition to certain diseases. Evidence suggests that certain HLAs have an increased frequency in children and adults with dermatomyositis. However, the specific implications of such findings are not fully understood.
Dermatomyositis is thought to belong to a group of disorders in which the body’s natural immune defenses inappropriately act against the body’s own tissues (autoimmune disorders). In dermatomyositis, an abnormal immune reaction appears to lead to obstructive inflammatory changes of blood vessels within muscle, connective tissues of the skin, and other tissues; patchy degeneration, wasting (atrophy), and regeneration of muscle fibers; thinning of the outermost skin layer (epidermis); and/or other associated findings.
Reports indicate that certain infectious agents (i.e. coxsackie virus, parvovirus, echovirus, HIV, human T-cell lymphotrophic virus Type 1, and Toxoplasma and Borrelia species) have been suggested as potential triggers for dermatomyositis. Some researchers suggest that, in genetically predisposed individuals, the presence of foreign viral proteins (antigens) that are similar to some of the body’s own proteins may trigger the production of antibodies that improperly “cross-react” or act against the body’s own cells (i.e., intramuscular blood vessels), leading to the inflammatory changes and muscle tissue damage seen in dermatomyositis. Environmental factors have also been seen to play a role in cases of juvenile dermatomyositis that develop/exacerbate in the months of April and May. In addition, researchers indicate that the association of dermatomyositis with underlying malignancies in some adults may suggest an abnormal autoimmune response directed against a common antigen in muscle and the cancerous tumor. There have also been some reports in which dermatomyositis has appeared to occur following certain vaccinations or the use of particular medications (i.e., penicillamine, the statins, quinidine, and phenylbutazone). Dermatomyositis may be initiated or exacerbated following silicone breast implants or collagen injections. However, the implications of such findings remain unknown and more data is required to establish the association.
Dermatomyositis complications
Possible complications of dermatomyositis include:
- Difficulty swallowing. If the muscles in your esophagus are affected, you can have problems swallowing (dysphagia), which can cause weight loss and malnutrition.
- Aspiration pneumonia. Difficulty swallowing can also cause you to breathe food or liquids, including saliva, into your lungs (aspiration).
- Breathing problems. If the condition affects your chest muscles, you might have breathing problems, such as shortness of breath.
- Calcium deposits. These can occur in your muscles, skin and connective tissues (calcinosis) as the disease progresses. These deposits are more common in children with dermatomyositis and develop earlier in the course of the disease.
Dermatomyositis prognosis
With early diagnosis and treatment, prognosis is good. Survival rates of 80 and 73% at five and eight years respectively have been reported. Factors which point to a poor outcome include late diagnosis, difficult-to-treat disease, older age, cancer, fever, difficulty swallowing and fibrosis in the lungs.
Dermatomyositis symptoms
In those with dermatomyositis, the onset of symptoms may be gradual (insidious) or sudden (acute). The symptoms often wax and wane for no apparent reason.
In many patients the first sign of dermatomyositis is the presence of a symptomless, itchy or burning rash. The rash often, but not always, develops before the muscle weakness.
- Reddish or bluish-purple patches mostly affect sun exposed areas.
- A violaceous rash may also affect cheeks, nose, shoulders, upper chest and elbows.
- Purple eyelids, which are described as heliotrope, as they resemble the heliotrope flower, Heliotropium peruvianum, which has small purple petals.
- Purple papules or plaques are found on bony prominences, especially the knuckles (Gottron papules).
- Ragged cuticles and prominent blood vessels on nail folds are best seen by capillaroscopy or dermoscopy.
- A scaly scalp and thinned out hair may occur.
- Less commonly, there is poikiloderma, in which the skin is atrophic (pale, thin skin), red (dilated blood vessels) and brown (post-inflammatory pigmentation).
Calcinosis affects some people, especially children and adolescents
- It presents as hard yellow or white lumps under the skin.
- These usually appear on fingers or over joints.
- Sometimes these nodules may poke through the skin and ulcerate.
- The ulcers may become infected.
Some patients have swollen joints and Raynaud phenomenon (this term refers to fingers that go very white and stiff in cold conditions, then purple as they warm again).
Muscle weakness may arise at the same time as the rash, or it may occur weeks, months or years later. Proximal muscles are affected, that is, those closest to the trunk (upper arms, thighs).
The first indication of myositis is when the following everyday movements become difficult.
- Climbing stairs or walking
- Rising from a sitting or crouching position
- Lifting objects
- Raising arms above the shoulders, e.g. combing hair
- Difficulty swallowing (dysphagia)
Occasionally the affected muscles ache and become tender to touch.
The major symptom of dermatomyositis is muscle weakness, most often affecting the trunk and muscles closest to the trunk (i.e., proximal muscles), such as the hips, thighs, shoulders, upper arms, and neck. The affected muscles may be stiff, sore, and/or tender and, eventually, may show signs of degeneration and muscle wasting (atrophy). Muscle weakness and degeneration progress and may lead to an awkward manner of walking (gait) and a gradual inability to perform certain tasks, such as lifting the arms, climbing steps, or dressing. Characteristic signs may include an inability to raise the head from the pillow when lying down or to rise unassisted from the floor. In some people with the disorder, involvement of muscles of the neck, tongue, and/or throat may eventually result in difficulties swallowing (dysphagia) and/or articulating speech (dysphonia). In rare cases, weakening of muscles of the chest wall and diaphragm may cause respiratory difficulties, potentially leading to life-threatening complications without prompt, appropriate treatment. In addition, in some with chronic, long-term disease, certain joints may become fixed in a permanently bent (flexed) position (contractures) and lead to problems in walking.
Individuals with dermatomyositis also develop characteristic skin changes that, in some cases, may precede muscle weakness. These characteristic skin changes may be the only sign of dermatomyositis at the start in up to 40% of people. Skin abnormalities often include a distinctive reddish-purple or lilac (i.e., heliotrope) rash that may be present on the upper eyelids (heliotrope eyelids); the forehead; the cheeks and bridge of the nose (“butterfly rash”); and/or other regions. In addition, affected skin on the extensor surfaces of certain joints, such as the knuckles, elbows, knees, or other regions, may tend to become scaly, with central areas of tissue loss (atrophy) that lack or have increased pigmentation (Gottron sign). A “dusky” reddish (erythematous) rash may also develop on the upper arms, upper legs, and upper trunk. The rash tends to be itchy and can lead to trouble sleeping for many people. Although the skin rashes frequently fade completely, they may be followed by brownish discolorations (hyperpigmentation) of the skin, atrophy, scarring, and/or loss of color (depigmentation) of patches of skin (vitiligo). Dermatomyositis may also be associated with distinctive changes of the nails that can include: bluish-red, scaling lesions around the base of the nails; reddish “shininess” of the nail folds; abnormal widening (dilation) of capillaries of the nailbeds; or other findings. Additional skin manifestations may include an abnormal accumulation of fluid in body tissues (edema) surrounding the eyes (periorbital area) and in other facial regions; an increased sensitivity to light (photosensitivity); and/or other findings. In some cases of long-term chronic disease, atrophic changes may result in binding of skin to underlying tissue structures. Some affected individuals, particularly children, may also have abnormal accumulations of calcium deposits (calcinosis) in affected muscles and tissues under the skin (subcutaneous tissues), potentially leading to contractures and localized muscle atrophy. Itching and scaling lesions may develop on the scalp leading to significant hair loss.
Some individuals with dermatomyositis may also develop symptoms such as low-grade fever, a general feeling of ill health (malaise), shortness of breath (dyspnea), pain in multiple joints (polyarthralgia), weight loss, and/or other abnormalities. In some cases, affected individuals, particularly those who have muscle inflammation (myositis) in association with other connective tissue disorders, experience Raynaud phenomenon. This is a condition in which sudden contraction of blood vessels supplying the fingers and toes (digits) causes a temporary interruption of blood flow and associated numbness, tingling, abnormal discoloration of the digits, and pain. Episodes are most commonly triggered by exposure to cold temperatures. (For more information, choose “Raynaud” as your search term in the Rare Disease Database).
Muscle weakness and impairment may progress to affect other areas of the body, including muscles of the GI tract, within the cardiovascular system (i.e., heart, blood vessels, and blood circulation), and/or the lungs. In rare cases the heart muscle may weaken (cardiomyopathy) or irregularity of the heartbeat can occur (arrhythmias). Inflammation of the lung tissue (interstitial pneumonitis or interstitial lung disease) can result in breathing difficulties (dyspnea) and coughing. Some studies have shown plaque accumulation in the arteries (atherosclerosis) in people with dermatomyositis.
Furthermore, in some individuals with dermatomyositis, there may be an association with an underlying cancer (malignancy). Reports indicate that the malignancy may precede, occur in association with, or develop subsequent to the onset of dermatomyositis. Malignancy-associated dermatomyositis appears to occur more frequently in individuals over the age 40-50. Although there is no characteristic cancer site or type, experts indicate that underlying malignancies most commonly arise in the GI tract, lungs, breast, ovary, testis, or certain white blood cells (lymphocytes) or lymphoid tissue (i.e., certain lymphomas and leukemias, multiple myeloma). The relationship between dermatomyositis and malignancies is not fully understood.
The symptoms and physical findings associated with childhood dermatomyositis are similar to those observed in adult dermatomyositis. Onset is usually more sudden (acute) than in the adult form and often involves skin manifestations followed by muscle weakness. Calcification of muscles and tissues is more frequent and widespread in childhood dermatomyositis as compared to adult forms. The deposits have a high calcium content and tend to be firm, white, or flesh-colored nodules over bony areas which can include the elbows, knees, and extremities. These calcifications often develop within three years of diagnosis but may develop up to 20 years later. Affected children also tend to have widespread inflammation of blood vessels (vasculitis), with more frequent involvement of the GI tract. In those with GI vasculitis, associated findings may include abdominal pain; difficult, infrequent, or incomplete passing of stools (constipation); or the passage of tarry, black stools (melena) or vomiting of blood due to the development of sores or eroded areas in the lining of the GI tract (bleeding peptic ulcers). Children may also develop a tiptoe gait secondary to a stiffening of the ankles. Malignancy is rarely associated with the childhood form of dermatomyositis.
In rare cases known as dermatomyositis sine myositis, the skin abnormalities associated with dermatomyositis may occur without the associated muscle abnormalities.
Dermatomyositis diagnosis
If your doctor suspects you have dermatomyositis, he or she might suggest some of the following tests:
- Blood analysis. A blood test will let your doctor know if you have elevated levels of muscle enzymes, such as creatine kinase (CK) and aldolase. Increased creatine kinase and aldolase levels can indicate muscle damage. A blood test can also detect autoantibodies associated with different symptoms of dermatomyositis, which can help in determining the best medication and treatment.
- Chest X-ray. This simple test can check for signs of the type of lung damage that sometimes occurs with dermatomyositis.
- Electromyography. A doctor with specialized training inserts a thin needle electrode through the skin into the muscle to be tested. Electrical activity is measured as you relax or tighten the muscle, and changes in the pattern of electrical activity can confirm a muscle disease. The doctor can determine which muscles are affected.
- MRI. A scanner creates cross-sectional images of your muscles from data generated by a powerful magnetic field and radio waves. Unlike a muscle biopsy, an MRI can assess inflammation over a large area of muscle.
- Skin or muscle biopsy. A small piece of skin or muscle is removed for laboratory analysis. A skin sample can help confirm the diagnosis of dermatomyositis. A muscle biopsy might reveal inflammation in your muscles or other problems, such as damage or infection. If the skin biopsy confirms the diagnosis, a muscle biopsy might not be necessary.
Dermatomyositis treatment
There’s no cure for dermatomyositis, but treatment can improve your skin and your muscle strength and function. Goals of treatment are to improve function and prevent disability. Treatment should be started early, with co-ordination between the physiotherapist, team of medical professionals, such as pediatricians or internists; physicians who specialize in the diagnosis and treatment of connective tissue disorders (rheumatologists); specialists in the functioning of the immune system (immunologists); and/or other health care professionals. The earlier treatment is started in the course of dermatomyositis, the more effective it is.
The aim of physiotherapy is to prevent muscle wasting and loss of movement. Initial therapy consists of passive stretching and splinting, with strength-building exercises once inflammation subsides. Wearing sunscreen and protective clothing is advised. Antihistamines may be useful in controlling symptoms of itching.
Steroid medications, such as prednisolone are the treatment of choice. In difficult-to-treat cases, the addition of an immunosuppressant drug may be necessary.
In general, treatment for the muscle involvement associated with dermatomyositis requires the use of glucocorticoids. Treatment for the skin findings associated with dermatomyositis includes: sun avoidance, sunscreens, topical glucocorticoids, anti-malarial agents, methotrexate, mycophenolate mofetil, and/or intravenous immunoglobulin (IVIg).
Medications
Medications used to treat dermatomyositis include:
- Corticosteroids. Drugs such as prednisone can control dermatomyositis symptoms quickly. But prolonged use can have serious side effects. So your doctor, after prescribing a relatively high dose to control your symptoms, might gradually reduce as your symptoms improve.
- Corticosteroid-sparing agents. When used with a corticosteroid, these drugs can decrease the dose and side effects of the corticosteroid. The two most common medications for dermatomyositis are azathioprine (Azasan, Imuran) and methotrexate (Trexall).
- Rituximab (Rituxan). More commonly used to treat rheumatoid arthritis, rituximab is an option if initial therapies don’t adequately control your symptoms.
- Antimalarial medications. For a persistent rash, your doctor might prescribe an antimalarial medication, such as hydroxychloroquine (Plaquenil).
- Sunscreens. Protecting your skin from sun exposure by applying sunscreen and wearing protective clothing and hats is important for managing the rash of dermatomyositis.
High dose glucocorticoid therapy may produce adverse side effects, particularly after prolonged use, such as a decrease in bone density, causing bones to become brittle and weakened (osteoporosis); increasing, “superimposed” muscle weakness due to effects of the medication (i.e., corticosteroid myopathy); tissue swelling (edema); peptic ulcers; elevated blood pressure; elevated blood sugar levels; weight gain with fat deposits in the abdomen, face, and/or back of the neck or other findings. Physicians may recommend certain measures to help prevent or minimize adverse effects, such as appropriate, alternative day therapy; administration of proper calcium and vitamin D supplementation; or the use of other medications (i.e., H2-receptor blockers or proton pump inhibitors). In some affected individuals, certain adverse effects may necessitate a decrease in dosage or discontinuation of therapy and substitution of another appropriate treatment. However, treatment with glucocorticoids should never be abruptly stopped unless under the direct supervision of a physician.
Therapy with other immunosuppressive drugs, such as azathioprine, methotrexate, mycophenoloate mofetil, cyclophosphamide, tacrolimus, or cyclosporine, may be beneficial for some affected individuals who have an insufficient response to steroid therapy alone, dose-limiting adverse effects, or frequent relapses. For example, preliminary investigations have shown that some affected individuals may benefit from combination therapy with azathioprine and steroids, with the addition of immunosuppressant therapy often allowing the use of lower steroid doses and therefore less adverse effects from the steroid treatment. Rituximab is a monoclonal antibody directed against the CD20 protein on the surface of B cells and has shown some benefit in the treatment of dermatomyositis. In addition, reports indicate that some affected individuals have obtained benefit from methotrexate therapy for five years or more and in both muscle and skin disease. However, therapy with such immunosuppressive agents may have serious adverse effects, such as an increased susceptibility to infections and other effects. In some patients who do not improve while on glucocorticoid therapy, with or without additional immunosuppressive treatment, have been shown to benefit in the short-term from receiving monthly high-dose intravenous immunoglobulin (IVIG) for 6 months. Thus, as with steroid therapy, individuals who undergo treatment with immunosuppressive agents require ongoing monitoring to ensure appropriate response, to help minimize or manage possible side effects, and to make any necessary dosage adjustments or treatment substitutions.
Antimalarial agents, such as hydroxychloroquine, may be useful in treating the skin manifestations of the disease and allow for a lower dose of glucocorticoids; however, these patients may be at an increased risk of eruption associated with treatment. Calcium-channel blockers, mainly diltiazem, have been used in treating calcinosis in patients that develop calcium deposits.
In affected individuals with an associated malignancy, reports suggest that dermatomyositis often improves with removal of the underlying cancer*. Experts indicate that individuals with malignancy-associated dermatomyositis may also sometimes respond to therapy with glucocorticoids such as prednisone. (*Depending upon the specific form, stage, and grade of the malignancy and other factors, recommended cancer treatment may include surgical removal of the malignancy; administration of certain chemotherapy drugs; radiation therapy; and/or other measures. During radiation therapy, radiation via x-rays or other sources of radioactivity is passed through selected regions of the body to destroy cancer cells and shrink tumors.)
In some cases, physical therapy may be recommended to help improve muscle strength and avoid the development of contractures. For individuals with calcifications, physicians may sometimes recommend surgical removal of calcium deposits. Treatment for other findings potentially associated with dermatomyositis (i.e., difficulty swallowing and/or breathing; speech problems; and/or abnormalities of the heart, lungs, and/or GI tract) is symptomatic and supportive. Affected individuals should be closely monitored by physicians so that proper preventive measures may be taken to help avoid serious complications potentially associated with this disorder.
Diet and physical activity also play an important role in dermatomyositis. For example, patients with severe muscle inflammation should incorporate more protein in their diet to compensate for the loss. Patients with dysphagia may require a special diet to avoid certain foods that may exacerbate their symptoms. Additional non-pharmacological recommendations include: avoidance and/or protection from the sun; elevation of the head of the bed; not eating before bedtime; and general bed rest.
Therapy
Depending on the severity of your symptoms, your doctor might suggest:
- Physical therapy. A physical therapist can show you exercises to help maintain and improve your strength and flexibility and advise you about an appropriate level of activity.
- Speech therapy. If your swallowing muscles are affected, speech therapy can help you learn how to compensate for those changes.
- Dietetic assessment. Later in the course of dermatomyositis, chewing and swallowing can become more difficult. A registered dietitian can teach you how to prepare easy-to-eat foods.
Surgical and other procedures
- Intravenous immunoglobulin (IVIg). IVIg is a purified blood product that contains healthy antibodies from thousands of blood donors. These antibodies can block the damaging antibodies that attack muscle and skin in dermatomyositis. Given as an infusion through a vein, IVIg treatments are expensive and might need to be repeated regularly for the effects to continue.
- Surgery. Surgery might be an option to remove painful calcium deposits and prevent recurrent skin infections.
Home remedies
With dermatomyositis, areas affected by your rash are more sensitive to the sun. Wear protective clothing or high-protection sunscreen when you go outside.
Coping and support
Living with a chronic autoimmune disease can make you wonder whether you’re up to the challenge. To help you cope, try supplementing your medical care with the following:
- Know your illness. Read all you can about dermatomyositis and other muscle and autoimmune disorders. Talk to people who have a similar condition. Don’t be afraid to ask your doctor questions concerning your illness, diagnosis or treatment plan.
- Be a part of your medical team. Consider yourself, your doctor and other medical experts involved in your care as a united front in the fight against your disease. Following the treatment plan you agreed to is vital. Keep your doctor updated on any new signs or symptoms you develop.
- Get active. A regular exercise routine can help you maintain and build your muscle strength. Be sure to get a detailed plan and recommendations from your doctor or physical therapist before starting an exercise program.
- Rest when you’re tired. Don’t wait until you’re exhausted. This will only set you back further as your body tries to recuperate. Learning to pace yourself can help you maintain a consistent level of energy, accomplish just as much and feel better emotionally.
- Avoid eating food before bedtime and raising the bed head for those with difficulty swallowing
- Acknowledge your emotions. Denial, anger and frustration are normal when dealing with an illness. Things don’t seem normal or fair and likely seem out of your control. Feelings of fear and isolation are common, so stay close to your family and friends. Try to maintain your daily routine as best you can and don’t neglect doing things you enjoy. Many people find support groups helpful.
- Avoid excessive sun exposure and use sun protection measures, including sunscreens, to minimize the harmful effects of the sun on already damaged and photosensitive skin
- A systematic review of adult-onset clinically amyopathic dermatomyositis (dermatomyositis siné myositis): a missing link within the spectrum of the idiopathic inflammatory myopathies. Gerami P, Schope JM, McDonald L, Walling HW, Sontheimer RD. J Am Acad Dermatol. 2006 Apr; 54(4):597-613. https://www.ncbi.nlm.nih.gov/pubmed/16546580/[↩][↩]
- Gerami P, Schope JM, Mcdonald L, Walling HW, Sontheimer RD. A systematic review of adult-onset clinically amyopathic dermatomyositis (dermatomyositis sine myositis): a missing link within the spectrum of the idiopathic inflammatory myopathies. J Am Acad Dermatol. 2006;54:597–613 https://www.ncbi.nlm.nih.gov/pubmed/16546580[↩]
- Ghazi E, Sontheimer RD, Werth VP. The importance of including amyopathic dermatomyositis in the idiopathic inflammatory myositis spectrum. Clinical and experimental rheumatology. 2013;31(1):128-134. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3883437/[↩]
- Incidence of dermatomyositis and clinically amyopathic dermatomyositis: a population-based study in Olmsted County, Minnesota. Bendewald MJ, Wetter DA, Li X, Davis MD. Arch Dermatol. 2010 Jan; 146(1):26-30. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2886726/[↩]
- Dermatomyositis: an overview of recent progress with emphasis on dermatologic aspects. Sontheimer RD. Dermatol Clin. 2002 Jul; 20(3):387-408. https://www.ncbi.nlm.nih.gov/pubmed/12170874/[↩]
- [A case of amyopathic dermatomyositis with rapidly progressive interstitial pneumonia]. Nanke Y, Tateisi M, Yamagata H, Hara M, Kamatani N. Ryumachi. 2000 Aug; 40(4):705-10. https://www.ncbi.nlm.nih.gov/pubmed/11021175/[↩]
- Interstitial lung disease in clinically amyopathic dermatomyositis (CADM) patients: a retrospective study of 41 Chinese Han patients. Sun Y, Liu Y, Yan B, Shi G. Rheumatol Int. 2013 May; 33(5):1295-302. https://www.ncbi.nlm.nih.gov/pubmed/23143553/[↩]
- Interstitial lung disease in patients with polymyositis, dermatomyositis and amyopathic dermatomyositis. Kang EH, Lee EB, Shin KC, Im CH, Chung DH, Han SK, Song YW. Rheumatology (Oxford). 2005 Oct; 44(10):1282-6. https://www.ncbi.nlm.nih.gov/pubmed/15972351/[↩]
- Interstitial lung diseases associated with amyopathic dermatomyositis. Suda T, Fujisawa T, Enomoto N, Nakamura Y, Inui N, Naito T, Hashimoto D, Sato J, Toyoshima M, Hashizume H, Chida K. Eur Respir J. 2006 Nov; 28(5):1005-12. https://www.ncbi.nlm.nih.gov/pubmed/16837503/[↩]
- Suzuki A, Kondoh Y, Taniguchi H, et al. Lung histopathological pattern in a survivor with rapidly progressive interstitial lung disease and anti-melanoma differentiation-associated gene 5 antibody-positive clinically amyopathic dermatomyositis. Respiratory Medicine Case Reports. 2016;19:5-8. doi:10.1016/j.rmcr.2016.05.008. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4910142/[↩]





{kind=link}