Contents
What is a desmoid tumor
Desmoid tumor also known as desmoid fibromatosis or aggressive fibromatosis is an abnormal growth that arises from connective tissue that contains fibroblast or myofibroblast cells, which is the tissue that provides strength and flexibility to structures such as bones, ligaments, fascia and muscles 1, 2, 3, 4, 5, 6, 7, 8. The term “desmoid” is from the Greek word “desmos,” which means band or tendon, to illustrate the band- or tendon-like consistency of the tumor 5. According to World Health Organization (WHO), desmoid tumor is a “clonal fibroblastic proliferation that arises in the deep soft tissues and is characterized by infiltrative growth and a tendency toward local recurrence but an inability to metastasize”, even though it may be multifocal in the same limb or body part 9. Typically, a single tumor develops, although some people have multiple tumors. Desmoid tumors can occur anywhere in your body. Desmoid tumors that form in your abdominal wall are called abdominal desmoid tumors; those that arise from the tissue that connects the abdominal organs are called intra-abdominal desmoid tumors; and desmoid tumors found in other regions of your body are called extra-abdominal desmoid tumors. Extra-abdominal desmoid tumors occur most often in the shoulders, upper arms, and upper legs.
Desmoid tumors are fibrous, much like scar tissue 10, 11, 12. Desmoid tumors are generally not considered cancerous (malignant) because they do not spread to other parts of the body (metastasize); however, they can aggressively invade the surrounding tissue, extend along fascial planes, attach to and erode bones, and compress and engulf vessels, nerves, and other hollow organs and can be very difficult to remove surgically 13, 3, 1. Desmoid fibromatosis often recur, even after complete removal 14.
The most common symptom of aggressive fibromatosis or desmoid fibromatosis is pain. Other signs and symptoms of desmoid tumors, which are often caused by growth of the tumor into surrounding tissue, vary based on the size and location of the tumor. Intra-abdominal desmoid tumors can block the bowel, causing constipation. Extra-abdominal desmoid tumors can restrict the movement of affected joints and cause limping or difficulty moving the arms or legs.
Desmoid tumors are rare, affecting an estimated 1 to 2 per 500,000 people worldwide. In the United States, 900 to 1,500 new cases are diagnosed per year 15. In Finland, the estimated incidence of aggressive fibromatosis is less than 4 cases per 1,000,000 population per year 16. Sporadic desmoid tumors are more common than those associated with familial adenomatous polyposis.
Desmoid tumors occur frequently in people with an inherited form of colon cancer called familial adenomatous polyposis (FAP). These individuals typically develop intra-abdominal desmoid tumors in addition to abnormal growths called polyps and cancerous tumors in the colon. Desmoid tumors that are not part of an inherited condition are described as sporadic.
Generally, desmoid tumors can be classified into 2 categories based on their genetics:
- Sporadic desmoid tumors are associated with mutations in the catenin beta 1 (CTNNB1) gene which codes for beta-catenin. Sporadic desmoid tumors are more common than those associated with familial adenomatous polyposis (FAP).
- Associated with adenomatous polyposis coli (APC) gene mutations — tumors occurring as part of syndromic conditions such as in patients with a family history of desmoid tumors, known familial adenomatous polyposis (FAP) or Gardner syndrome.
Other proposed risk factors for desmoid tumor development include trauma, recent surgery, and high estrogen states.
Because of its rarity, desmoid tumor may be misdiagnosed in as many as 30%–40% of cases, resulting in inappropriate or delayed care 17, 18. In one study, the time from patient‐reported symptom onset to desmoid tumor diagnosis exceeded one year for 54% of patients 19.
Standard treatment for aggressive fibromatosis or desmoid fibromatosis ranges from active surveillance for asymptomatic lesions to surgery, radiotherapy, and systemic therapies such as nonsteroidal anti-inflammatory drugs (NSAIDs), anti-estrogens, and tyrosine kinase inhibitors (TKI) 2. Since desmoid tumors do not spread (metastasize), many approaches are nonoperative in nature 20. Many cases of desmoid tumors may remain stable or even regress spontaneously, active observation and regular follow-up are often the initial management approach 21, 22. However, the most successful primary treatment modality for desmoid tumor in patients with active symptoms (ie, volumetric progression and compression symptoms) is surgery with negative surgical margins 22. Positive margins after surgery reflect a high risk for recurrence 23. Surgery plus the administration of nonsteroidal anti-inflammatory medication (NSAIDs), hormonal therapy, targeted biologics, and cytotoxic chemotherapy is sometimes used for patients with rapidly growing tumors or where surgery would be inappropriate 24. Radiotherapy (radiation therapy) is a second-line option where surgery is contraindicated or an adjuvant (add-on) therapy in post-surgical patients with positive margins on initial resection.
Most (~85 percent) desmoid tumors are sporadic and are not inherited. Sporadic tumors result from gene mutations that occur during a person’s lifetime, called somatic mutations. A somatic mutation in one copy of the gene is sufficient to cause the disorder. Somatic mutations in either the CTNNB1 or the APC gene can cause sporadic desmoid tumors.
Familial desmoid tumor cases (about 5-10 %) are associated with an inherited form of colon cancer called familial adenomatous polyposis (FAP). An inherited mutation in one copy of the APC gene causes familial adenomatous polyposis (FAP) and predisposes affected individuals to develop desmoid tumors. The desmoid tumors occur when a somatic mutation occurs in the second copy of the APC gene. Patients with mutations in the APC gene are predisposed to forming hundreds of polyps in the intestines and go on to develop colon cancers. Patients with familial adenomatous polyposis (FAP) are often recommended to undergo surgical removal of their intestines. These patients are at a very high risk of developing intra-abdominal desmoid tumors which can arise deep in the abdomen or in the abdominal wall in addition to abnormal growths (called polyps) and cancerous tumors in the colon. In older scientific literature, the combination of FAP and desmoid tumors is termed Gardner’s Syndrome or the condition is sometimes called hereditary desmoid disease.
In some rare cases, desmoid tumors can occur in women who are pregnant. This happens during pregnancy or after a surgical delivery. Many believe that this is caused by a combination of elevated hormones and surgery, however, there is no strong scientific evidence to support this claim. The relationship between pregnancy and desmoid tumors is very rare and consists of mostly anecdotes in the scientific literature.
Other names for desmoid tumor
- aggressive fibromatosis
- deep fibromatosis
- desmoid fibromatosis
- familial infiltrative fibromatosis
- hereditary desmoid disease
- musculoaponeurotic fibromatosis
Figure 1. Abdominal desmoid tumor
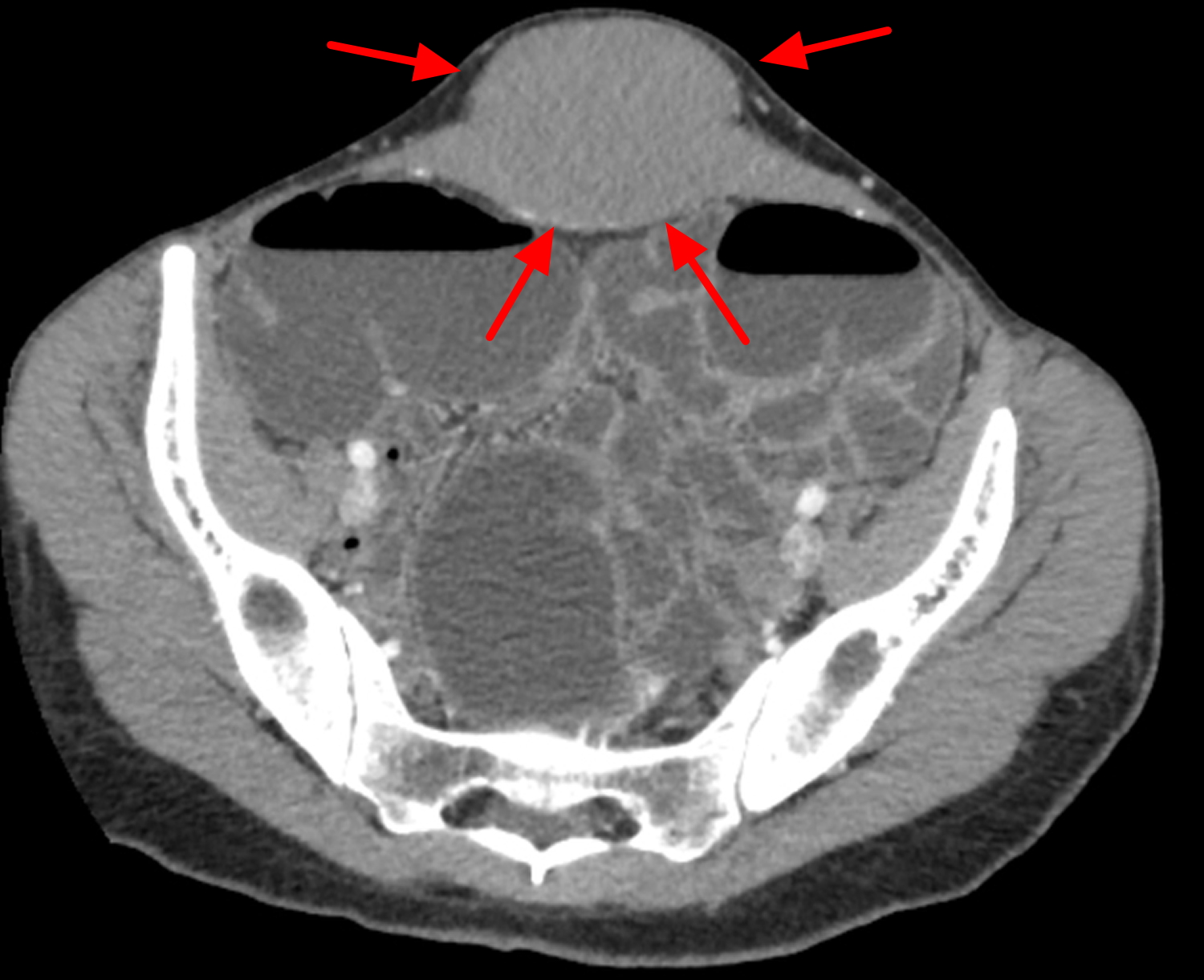
Figure 2. Intra-abdominal desmoid tumor
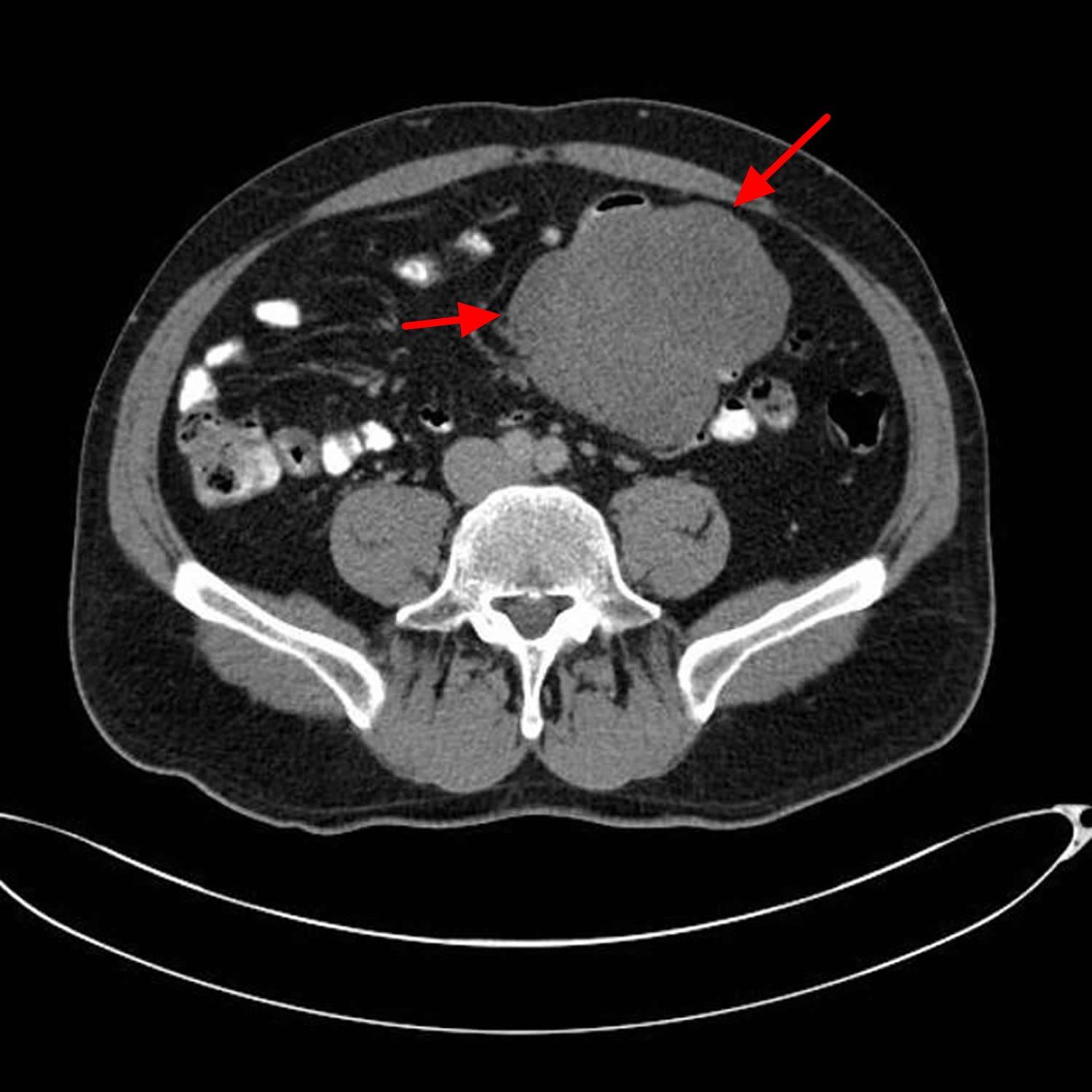
Figure 3. Desmoid tumor (aggressive fibromatosis) MRI
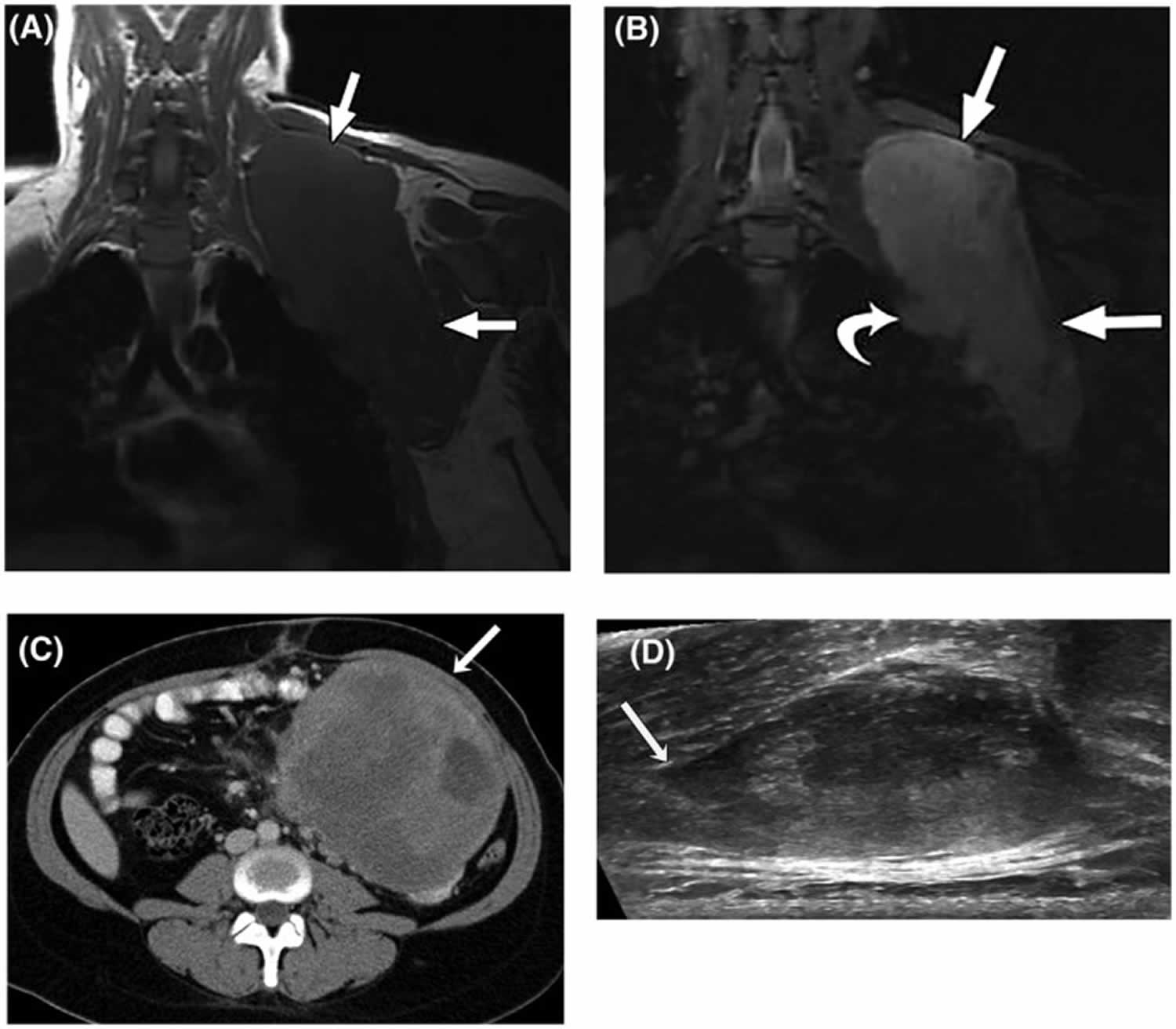
Footnotes: (A) T1‐weighted and (B) T2‐weighted fat‐suppressed magnetic resonance images (MRI) in the coronal plain of a 28‐year‐old woman with a large desmoid tumor (aggressive fibromatosis) in the shoulder region (straight arrows). The curved arrow indicates a nodular protrusion that raises concern for pleural invasion. (C) Axial, contrast‐enhanced computed tomography image from a 27‐year‐old woman with a nonresectable, solitary intra‐abdominal aggressive fibromatosis not associated with familial adenomatous polyposis. An arrow indicates a large, well defined mass adherent to the small bowel and mesenteric vessels. (D) Transverse ultrasound of a sporadic right paraspinal musculature extra‐abdominal desmoid tumor in a 26‐year‐old woman. Linear fascial extension (tail sign) is indicated by the arrow.
[Source 21 ]Figure 4. Aggressive fibromatosis arm MRI
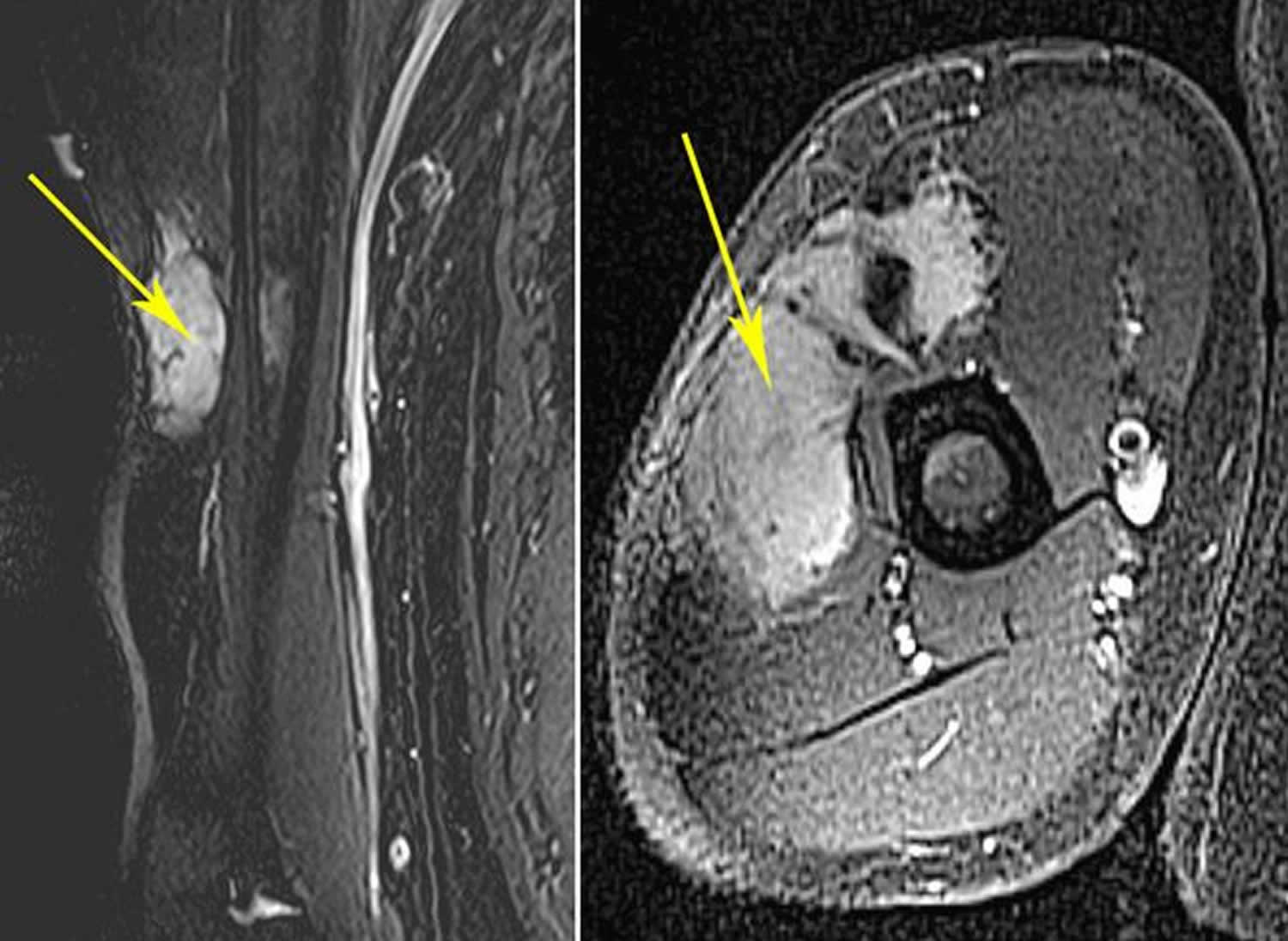
Footnotes: (Left) This MRI shows an extra-abdominal desmoid tumor in the arm. (Right) This MRI shows the same tumor in a cross-section view.
[Source 25 ]Who gets desmoid tumors?
Desmoid tumors or aggressive fibromatosis are rare, affecting an estimated 1 to 2 per 500,000 people worldwide 26. In the United States, 900 to 1,500 new cases are diagnosed per year 26. Typically, desmoid tumors affect young adults between the ages of 35 to 40 years and are more common in women.
Desmoid tumors may develop in 5 to 10% of patients with an inherited form of colon cancer called familial adenomatous polyposis (FAP) and in patients with conditions related to adenomatous polyposis coli (APC) gene mutations.
Can my desmoid tumor be inherited or passed down to my children?
Yes. Generally, desmoid tumors can be classified into 2 categories based on their genetics:
- Sporadic desmoid tumors are associated with mutations in the catenin beta 1 (CTNNB1) gene which codes for beta-catenin. Sporadic desmoid tumors are more common than those associated with familial adenomatous polyposis (FAP).
- Associated with adenomatous polyposis coli (APC) gene mutations — tumors occurring as part of syndromic conditions such as in patients with a family history of desmoid tumors, known familial adenomatous polyposis (FAP) or Gardner syndrome.
Desmoid tumors may develop in 5 to 10% of patients with an inherited form of colon cancer called familial adenomatous polyposis (FAP) and in patients with conditions related to adenomatous polyposis coli (APC) gene mutations.
How do I know if my desmoid tumor is going to be cured?
Complete surgical excision of desmoid tumor or aggressive fibromatosis is the most effective method of cure. This sometimes necessitates removal of most of an anterior compartment of a leg. Extensive cases may require excision plus adjuvant (add-on) treatment including chemotherapy and repeat surgery 27. Positive margins (incomplete resections) after surgery reflect a high risk for recurrence 28. Surgery plus the administration of nonsteroidal anti-inflammatory medication (NSAIDs), hormonal therapy, and cytotoxic chemotherapy is sometimes used, the latter being the most effective pharmacological approach 29. In selected patients, radical resection with intraoperative margin evaluation by frozen sections followed by immediate mesh reconstruction may be a safe and effective procedure providing definitive cure yet minimizing functional limitations 30.
I have desmoid tumor can I get pregnant?
Desmoid tumors can be more complex in pregnancy – a combination of hormonal signalling, trauma, and mechanical constraints may worsen symptoms during this time. Pregnant patients need to be managed in experienced centers with multi-disciplinary team.
Desmoid tumor survival rate
Local recurrence occurs in around 70 percent of cases. Prognosis depends on the type of tumor. Life expectancy is normal for abdominal and extra-abdominal tumors. However, it is lower in cases of intra-abdominal desmoid tumors due to complications such as intestinal obstruction, hydronephrosis or sepsis. Repeated surgical resections are associated with a greater risk of morbidity.
Desmoid tumor life expectancy
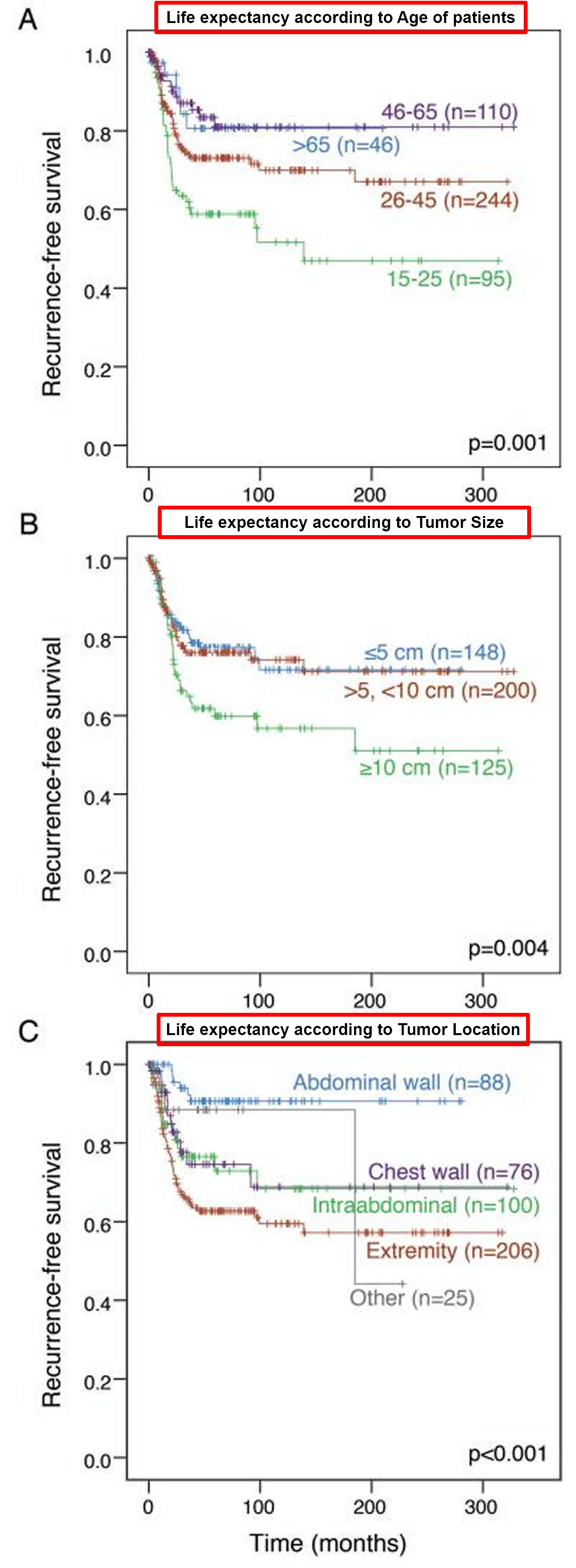
Desmoid tumors were treated surgically in 495 patients (between July 1, 1982, and November 1, 2011 with a median follow-up 60 months) at the Memorial Sloan Kettering Cancer Center. Of 439 patients undergoing complete gross resection, 100 (23%) had recurrence. Of 439 patients undergoing complete gross resection, 100 had recurrence. Among these, 92 (92%) had their recurrence within 5 years. Five-year local recurrence–free survival was 69% (Figure 5) 31.
Size of the patient’s primary desmoid tumor was associated with outcome. Desmoid tumors over 10 cm in largest diameter were associated with 5-year local recurrence–free survival rates of 57% compared to 72% for tumors ≤5 cm and 74% for tumors >5 cm and ≤10 cm (Figure 5B). There was a striking association between site and local recurrence–free survival. Intra-abdominal, chest wall, and extremity tumors had relatively poor outcomes (5-year local recurrence–free survival 76%, 72%, and 60% respectively). Desmoid tumors in the neck, which were considered collectively with extremity lesions in the main analyses, behaved nearly identically to extremity tumors (5-year local recurrence–free survival 43% for neck versus 47% for lower extremity). Abdominal wall tumors had the best outcome (5-year local recurrence–free survival 90% [Figure 5C] vs. 34% in patients ≤25 y.o. with large, extremity tumors [n=11]). Only 8 of 79 patients with abdominal wall tumors had recurrence. All were 40 or younger, and 3 of the 8 had tumors over 10 cm. Only one abdominal wall desmoid tumor that recurred, a rectus sheath lesion, was <5 cm.
A multivariate analysis demonstrated that age, tumor size, and tumor site are independent predictors of recurrence. Margin status (R1 vs. R0) was not associated with altered outcome in the cohort as a whole or in subgroups defined by age or tumor site. However, among patients with small desmoid tumors (<5 cm), R0 resection was associated with longer local recurrence–free survival compared to R1 resection (76 vs. 60%). Margin was not associated with recurrence in larger lesions.
- For access to the Local Recurrence-Free Survival After Surgery tool based on data from patients treated at Memorial Sloan Kettering Cancer Center please go here: The Memorial Sloan Kettering Cancer Centerat https://www.mskcc.org/nomograms/sarcoma/desmoid
Figure 5. Desmoid tumor life expectancy – Recurrence-free survival in 439 patients undergoing complete gross resection of a desmoid tumor stratified by (A) patient age, (B) tumor size, and (C) tumor location.
Desmoid tumor causes
Desmoid tumors result from the proliferation of well-differentiated myofibroblasts or fibroblasts. The exact cause of desmoid tumor or desmoid fibromatosis is still unknown, but they seem to have a multi-factorial origin with hormonal, trauma and genetic factors with mutations in the Wnt/APC/beta-catenin pathway being involved 32, 33, 34, 35.
Mutations in the catenin beta 1 (CTNNB1) gene or the adenomatous polyposis coli (APC) gene cause desmoid tumors 36. CTNNB1 (catenin beta 1) gene mutations particularly at codons 41A, 45F, and 45 (with p.Thr41Ala and p.Ser45Phe being the most common mutations) account for around 90 to 95 percent of sporadic desmoid tumors 2, 15, 37. Mutation 45F is associated with a high risk of recurrence 9, 38, 39. The 5-year recurrence-free survival rate has been reported to be 23% for patients with a 45F mutation, 57% for patients with a 41A mutation, and 65% for those with no mutations 1.
Conversely, hereditary cases, often associated with familial adenomatous polyposis (FAP) or Gardner syndrome as well as 10 to 15 percent of sporadic desmoid tumors, are linked to germline APC (adenomatous polyposis coli) gene mutations 37. Both the CTNNB1 and the APC genes are involved in an important cell signaling pathway that controls the growth and division (proliferation) of cells and the process by which cells mature to carry out specific functions (differentiation).
The CTNNB1 gene provides instructions for making a protein called beta-catenin 40. Beta-catenin protein is present in many types of cells and tissues, where it is primarily found at junctions that connect neighboring cells (adherens junctions) 40. Beta-catenin plays an important role in sticking cells together (cell adhesion) and in communication between cells 40.
The beta-catenin protein is also involved in cell signaling as an essential part of the Wnt signaling pathway 40. Certain proteins in Wnt signaling attach (bind) to beta-catenin, which triggers a multistep process that allows the protein to move into the cell nucleus. Once in the nucleus, beta-catenin interacts with other proteins to control the activity (expression) of particular genes. The Wnt signaling pathway promotes the growth and division (proliferation) of cells and helps determine the specialized functions a cell will have (differentiation). Wnt signaling is known to be involved in many aspects of development before birth. In adult tissues, Wnt signaling plays a role in the maintenance and renewal of stem cells, which are cells that help repair tissue damage and can give rise to other types of cells.
The adenomatous polyposis coli (APC) gene provides instructions for making the APC protein, which plays a critical role in several cellular processes 41. The APC protein acts as a tumor suppressor, which means that it keeps cells from growing and dividing too fast or in an uncontrolled way 41. The APC protein helps control how often a cell divides, how it attaches to other cells within a tissue, and whether a cell moves within or away from a tissue. The APC protein also helps ensure that the number of chromosomes in a cell is correct following cell division. The APC protein accomplishes these tasks mainly through association with other proteins, especially those that are involved in cell attachment and signaling 41.
One protein with which APC associates is beta-catenin 41. Beta-catenin helps control the activity (expression) of particular genes and promotes the growth and division (proliferation) of cells and the process by which cells mature to carry out specific functions (differentiation). Beta-catenin also helps cells attach to one another and is important for tissue formation. Association of APC protein with beta-catenin signals for beta-catenin to be broken down when it is no longer needed 41. When beta-catenin is no longer needed, the APC protein attaches (binds) to it, which signals for it to be broken down. Mutations in the APC gene that cause desmoid tumors lead to a short APC protein that is unable to interact with beta-catenin. As a result, beta-catenin is not broken down and, instead, accumulates in cells. Excess beta-catenin, whether caused by CTNNB1 or APC gene mutations, promotes uncontrolled growth and division of cells, allowing the formation of desmoid tumors.
Most desmoid tumors are sporadic and are not inherited 26. Sporadic tumors result from gene mutations that occur during a person’s lifetime, called somatic mutations. A somatic mutation in one copy of the gene is sufficient to cause the disorder. Somatic mutations (changes in DNA that occur sporadically or randomly) in either the CTNNB1 or the APC gene can cause sporadic desmoid tumors 26.
A history of trauma often surgical to the site of the desmoid tumor is elicited in 1 in 4 cases 42. Desmoid tumors most commonly arise from the rectus abdominis muscle in postpartum women and in scars due to abdominal surgery 43. Implant-associated breast desmoid tumors may also occur 44. An endocrine cause is suggested. Desmoid tumors most commonly appear in young women during or after pregnancy. The tumors regress during menopause 45 and after tamoxifen (a selective estrogen-receptor modulator [SERM]) treatment to reduce the risk of developing breast cancer 46. Desmoid tumors may regress after exposure to oral contraceptives 47.
An inherited mutation in one copy of the APC gene causes familial adenomatous polyposis (FAP) and predisposes affected individuals to develop desmoid tumors. The desmoid tumors occur when a somatic mutation occurs in the second copy of the APC gene. In these cases, the condition is sometimes called hereditary desmoid disease 26.
Desmoid tumor symptoms
Desmoid tumors can develop at virtually any site in your body. Desmoid tumors most commonly present in the abdominal wall; however, they can also occur in your head, neck, arms and legs, and pelvis. Retroperitoneal desmoid fibromatosis are more common in familial polyposis coli and Gardner syndrome after abdominal surgery than in other conditions 48. Desmoid tumors can have a wide range of clinical symptoms or no symptoms at all. Many desmoid tumors are accidentally picked up on a scan or a routine physical exam done for other medical reasons. Many people have no symptoms at the time of diagnosis or even after many years. Some people feel a range of symptoms that range from slight to severe pain, decrease in their movement or range of motion, swelling of the area affected by the desmoid tumor, loss of sleep, anxiety and many other symptoms.
Desmoids deep inside the abdomen or pelvis can also be entirely without symptoms or they can cause bloating, severe pain, rupture of intestines, compression of the kidneys or ureters or rectal bleeding. They can compress critical blood vessels such as the mesenteric vessels and the vena cava. It is important to know that the desmoid tumors that present superficially on the abdominal wall behave much differently than the ones that are deep inside the abdomen or pelvis.
If the desmoid fibromatosis tumor is large enough, it can mimic cancer of the affected organ (eg, breast cancer). In these cases, the only way to establish a definitive diagnosis is to perform a biopsy.
Intra-abdominal and extra-abdominal desmoid fibromatosis
Intra-abdominal aggressive fibromatosis may be seen. Extra-abdominal aggressive fibromatosis may also be seen (rarely) in the urological system, including in the bladder and scrotum 49, 50. Intra-abdominal desmoid tumors remain asymptomatic until their growth and infiltration cause visceral compression. Symptoms of intestinal, vascular, ureteric, or neural involvement may be the initial manifestations. An ethmoidal desmoid tumor has been described in a child 51.
Breast desmoid fibromatosis
Aggressive fibromatosis account for 0.2% of primary breast tumors, developing from muscular fasciae and aponeuroses 52. Desmoid fibromatosis may mimic breast cancer, either in the breasts or, less commonly, in the armpits 53, 54. When a desmoid tumor involves the breast, it may mimic breast cancer on physical examination, mammography, and breast ultrasonography 53.
Desmoid tumor complications
The complications of aggressive fibromatosis or desmoid tumor depends on their location, extent, and infiltrative capacity.
- Intra-abdominal desmoid tumors — may cause intestinal or ureteral obstruction or involve the mesenteric vessels.
- Pelvis desmoid tumors — may infiltrate the urinary bladder or cause hydrosalpinx.
- Extra-abdominal desmoid tumors — may invade the pleura if occurring in the chest or may compress nearby vessels and nerves.
Pain management is crucial due to the potential for the tumor to invade the surrounding tissue and can be very difficult to remove surgically.
Desmoid tumors can be more complex in pregnancy – a combination of hormonal signalling, trauma, and mechanical constraints may worsen symptoms during this time. Pregnant patients need to be managed in experienced centers with multi-disciplinary team.
Desmoid tumor diagnosis
Initial diagnosis is based on imaging techniques (computed tomography [CT scan] and magnetic resonance imaging [MRI scan]) revealing the presence of an infiltrative growing mass. Diagnosis is confirmed by tumor biopsy showing abundant collagen surrounding elongated spindle-shaped cells containing small and regular nuclei and pale cytoplasm. Immunohistological examination shows expression of muscle cell markers (e.g. actin, desmin, vimentine) and absence of CD34. Moreover, diagnosis can be confirmed by screening for mutations of CTNNB1.
In rare circumstance, a biopsy may not be safe or feasible. When a biopsy is recommended, there are a variety of options which include: a core needle biopsy which takes a small piece, usually 1 mm wide by 10 mm long; and, surgical biopsies which may take a portion of the tumor (“incisional biopsy”) or may remove the entire visible tumor (“excisional biopsy”). While an excisional biopsy may remove all visible tumor, when pursuing this option it is necessary to discuss with your surgeon the possibility of leaving some tumor behind – either gross or microscopic – and most importantly, what are the short-term and long-term side effects of the excisional biopsy. The pathologist takes very fine sections of the biopsy material and examines them under the microscope looking for special features that define desmoid tumors.
Histologically, desmoid tumor is usually poorly circumscribed and composed of abundant collagen surrounding poorly circumscribed bundles of spindle cells. The dense bundles of eosinophilic spindle cells contain regular nuclei and pale cytoplasm with neither mitoses nor giant cells. Macrophages, giant cells, and lymphocytes are present peripherally. In most patients, staining for nuclear beta-catenin, vimentin, cyclooxygenase‐2 (COX‐2), c-KIT, PDGFRb, androgen receptors and beta estrogen receptors using immunohistochemistry will be positive and help establish a definitive diagnosis. They are negative for desmin, S-100, h-caldesmon, CD34 and CKIT 55, 56.
Given the high rate of misdiagnosis that occurs, guidelines recommend a second opinion by an expert pathologist for confirmation.
Desmoid tumor differential diagnosis
Differential diagnoses for extra-abdominal desmoid tumors:
- Fibroblastic sarcoma
- Gardner fibroma.
Differential diagnoses for intra-abdominal desmoid tumors:
- Gastrointestinal stromal tumor
- Solitary fibrous tumor
- Inflammatory myofibroblastic tumor
- Sclerosing mesenteritis
- Retroperitoneal fibrosis
- Secondary to certain drugs or an underlying cancer.
Desmoid tumor treatment
For aggressive fibromatosis or desmoid fibromatosis that are asymptomatic or nonprogressive, some prefer a wait-and-see approach 57. However, aggressive, wide surgical resection is the treatment of choice for desmoid fibromatosis or aggressive fibromatosis 58. Complete surgical excision of desmoid fibromatosis or aggressive fibromatosis is the most effective method of cure. This sometimes necessitates removal of most of an anterior compartment of a leg. Extensive cases may require excision plus adjuvant (add-on) treatment including chemotherapy and repeat surgery 27. Positive margins (incomplete resections) after surgery reflect a high risk for recurrence 28. Surgery plus the administration of nonsteroidal anti-inflammatory medication (NSAIDs), hormonal therapy, and cytotoxic chemotherapy is sometimes used, the latter being the most effective pharmacological approach 29. In selected patients, radical resection with intraoperative margin evaluation by frozen sections followed by immediate mesh reconstruction may be a safe and effective procedure providing definitive cure yet minimizing functional limitations 30.
Lesions involving the extremities and deep soft tissues of the trunk have a higher risk of recurrence, as do Gardner syndrome–associated lesions in other locations 59.
In those patients who refuse surgery or are not surgical candidates, the options below may be considered.
Radiation therapy may be used as a treatment for recurrent disease or as primary therapy to avoid mutilating surgical resection. It may be used postoperatively, preoperatively, or as the sole treatment 60.
Systemic therapy is appropriate if a primary complete resection is not feasible or if there is relapse or progression after resection 61. There are a number of novel drug therapy candidates for desmoid tumors 62. Pazopanib, a potent tyrosine kinase inhibitor, represents a promising new therapy for desmoid tumors in adolescent and young adult patients 63.
In November 2023, the US Food and Drug Administration (FDA) approved the first drug for desmoid tumor, nirogacestat (Ogsiveo) 64 . Nirogacestat, a gamma secretase inhibitor, cleaves multiple transmembrane proteins, including Notch, that are believed to play a role in activating pathways that contribute to growth of desmoid tumors 64. Nirogacestat (Ogsiveo) is indicated for adults with progressing tumors who require systemic treatment 64. The approval was supported by results from the phase 3 DeFi clinical trial 65. In the DeFi clinical trial 65, 70 patients were assigned to receive nirogacestat and 72 to receive placebo. Nirogacestat showed a significant progression-free survival (PFS) benefit over placebo; the likelihood of being event-free at 2 years was 76% with nirogacestat and 44% with placebo 65. Between-group differences in progression-free survival (PFS) were consistent across prespecified subgroups. The percentage of patients who had an objective response was significantly higher with nirogacestat than with placebo (41% vs 8%), with a median time to response of 5.6 months and 11.1 months, respectively; the percentage of patients with a complete response was 7% and 0%, respectively 65.
There are a number of new drug therapy candidates for aggressive fibromatosis 66. Pazopanib, a potent tyrosine kinase inhibitor, represents a promising new therapy for aggressive fibromatosis in adolescent and young adult patients 67. Another drug option is sorafenib 68.
Drug therapy with antiestrogens and prostaglandin inhibitors may also be used. Drug therapy result in objective response rates of approximately 40-50% of aggressive fibromatosis; the duration of response is variable 69.
In cases of recurrent extra-abdominal desmoid tumors in which surgery is contraindicated or in cases of recurrence, a chemotherapeutic regimen of doxorubicin, dacarbazine, and carboplatin may be effective. Intra-abdominal desmoid tumors as a part of Gardner syndrome may respond to systemic doxorubicin, and ifosfamide can be useful for patients with complications from the tumor 70. Polychemotherapy has been used 71 and can be combined with targeted therapy with imatinib 72.
Expanded knowledge of familial adenomatosis polyposis–desmoid tumor molecular underpinnings may aid in the development of novel therapeutic strategies 73.
Magnetic resonance‒guided high-intensity focused ultrasound may prove a safe and effective option for selected desmoid tumors 74.
Split-course radiotherapy in patients with desmoid tumors was well tolerated with good outcomes 75.
Active surveillance
Desmoid tumors display a wide range of behaviors and often unpredictable clinical course. This can range from shrinking spontaneously without any intervention, to remaining stable or growing rapidly. In some circumstances especially when patients are asymptomatic, it is reasonable to just watch the tumor carefully with images and/or physical examination. How often you need scans and/or physical exams during a “wait and watch” period will vary for each situation and your treating physician will discuss this with you.
In recent years, as a result of the unsatisfactory results obtained with surgery, the initial approach for desmoid tumors has turned toward a conservative, non-operative strategy, which is now the strategy of choice. It is recommended that all cases have a period of active surveillance. It allows for better predictions concerning the natural history and biology of desmoid tumors and allows the clinician to plan the next step in the therapeutic sequence, since a high percentage of cases reach a stabilization period and some patients even present regression of the tumor 76. Active surveillance was first proposed for patients that had recurrences not amenable for limb salvage; being a benign tumor, the main goal of observation was to avoid mutilating procedures. Under the surveillance period, it was noted that more than half of the tumors stabilized. Afterwards, the same strategy was offered to patients with resectable tumors and the same results were obtained, setting the foundations for what is now the initial treatment of choice; active surveillance 77.
The rationale for active surveillance is based on the fact that most patients will be able to avoid an unnecessary surgical procedure. Approximately 50% of the cases enter a stabilization period in an average of 14 to 19 months. When progressive disease presents, it is usually in the first months of observation and is rarely seen after three years of follow-up. Following this approach, only 14–16% of cases will require a surgical intervention and a quarter of the patients will show tumor regression. It has been demonstrated that the surveillance period can be safely carried out without detrimental outcomes in those patients who progress 78, 79. Recently, Duhil de Bénazé et al 80, reported encouraging outcomes in young patients with an initial wait and see approach. It was proved to be a safe and feasible option, not associated with impair in long term functionality when compared with other treatment strategies 81, 80. Another case-series, carried out by Grignol et al 81, included 142 patients (74 with primary tumors and 68 with recurrent tumors), in which a total of 83 patients were managed with active surveillance and reached a 5-year progression-free survival of 49.9%.
A study of patients with desmoid tumors managed at a referral center in the United Kingdom demonstrated a shift in the trend of treatment over time. The authors reported an increase from 10% in 1998 to 40% in 2016 of patients managed with active surveillance initially 82. In the whole series, they had a 36% of stable disease with 27% of either partial or complete response and 36% of progressive disease. They recorded older age (> 50 years old) as a risk factor for progression when compared with younger patients, as well as upper extremity and chest wall location 82.
The period of active surveillance should include close monitoring of patients with MRI or computed tomography every month for the first two months, then every three months for the first year followed by every six months until the fifth year, and yearly after. The intensity of the surveillance regimen, especially during the first years serves for early identification of rapidly progressive cases. Patients who have tumors in life-threatening locations as well as those with severe pain may avoid the surveillance period.
Surgery
According to the latest European consensus on desmoid tumors, surgery should be considered in cases of progression to medical or radiation therapies, always considering location and age. When surgery is carried out, it should always be done trying to preserve function and after considering all the alternatives for it. Cases of mesenteric or retroperitoneal tumors not associated with familial polyposis can be treated initially with surgery due to the morbidity and symptoms they cause.
Until a few years ago, aggressive, wide surgical resection is the treatment of choice for desmoid tumor or aggressive fibromatosis 57, 83. Complete surgical excision of desmoid tumor is the most effective method of cure. This sometimes necessitates removal of most of an anterior compartment of a leg. However, the 5-year recurrence rate was high, ranging from 25% to 60%, and extensive or disabling procedures were common 10. However, it can be difficult during surgery to determine the outer extent of the tumor. This is because desmoid tumors are not well encapsulated and they often intertwine with other tissues. Historically, most people with desmoid tumors underwent some form of surgery. Over the last few decades, it is increasingly being recognized that desmoid tumors have a high risk of returning even with surgery. While statistics may vary, about 25 to 40 percent of patients who undergo surgery can have a local recurrence (return at or near the original site). The goal of surgery is to remove the entire tumor and minimize the risk of recurrence. Scientific research has shown that some types of desmoid have much higher risk of recurrence after surgery than others. This can be calculated using an online calculator (MSKCC nomogram here: https://www.mskcc.org/nomograms/sarcoma/desmoid). All nomograms are estimations and not always accurate. When making a decision to undergo surgery, you have to have an open conversation with your surgeon about the risk of recurrence, time to recurrence and the short-term and long-term side-effects of the surgery. Increasingly, surgery is falling out of favor for desmoid tumors given their high risk of recurrence and other side effects. In some circumstances, surgery may be the best option and can result in great outcomes including a cure. In conclusion, the decision to undergo surgery is a complex one and should be weighted carefully. As desmoid tumors often recur, a surveillance strategy every 3-6 months is essential.
Desmoid tumors frequently invade a limb’s vital nerves and blood vessels. Because of this, full removal of the tumor may impair function in the surrounding area. Limited surgery, combined with additional treatments, such as radiation or chemotherapy, may be successful in these cases.
For unresectable desmoid tumors or those not amenable to surgical resection with R0 (microscopic tumor clearance) intent or accompanied by an unacceptable function loss, non-surgical treatments comprise radiotherapy, anti-estrogen therapy, non-steroidal anti-inflammatory agents, chemotherapy (e.g. methotrexate, vinblastine/vinorelbine, pegylated liposomal doxorubicin) and/or tyrosine kinase inhibitors (e.g. imatinib, sorafenib).
Extensive cases may require excision plus adjuvant (add-on) treatment including chemotherapy and repeat surgery 84. In selected patients, radical resection with intraoperative margin evaluation by frozen sections followed by immediate mesh reconstruction may be a safe and effective procedure providing definitive cure yet minimizing functional limitations 85. However, there has been a recent tendency to more conservative management 32. Active surveillance MRI has become a popular option 86.
Amputations should seldom be used for aggressive fibromatosis and only in cases of unresectable and severe, untreatable symptomatic recurrent disease or when some treatment-related side effects (surgery +/− radiation therapy) cause significant loss of function or disabling chronic symptoms 87, 88, 89.
Evidence suggests that pregnancy does not adversely affect surgical outcomes 90.
Lesions involving the extremities and deep soft tissues of the trunk have a higher risk of recurrence, as do Gardner syndrome–associated lesions in other locations 91.
Systemic therapy
Current indications for systemic treatment include rapidly progressive desmoid fibromatosis or patient rejection to active surveillance. Systemic treatment options for desmoid fibromatosiss include non-steroid anti-inflammatory drugs (NSAIDs), anti-hormonal therapies, tyrosine kinase inhibitors (TKI), and conventional “low dose” chemotherapeutic regimens, including liposomal doxorubicin.
Anti-inflammatories have shown the ability to block the beta-catenin pathway mediated by cyclooxygenase‐2 (COX‐2) or prostaglandins, and thus induce an objective response and improve pain control. The proposed mechanism of this response is due to cyclooxygenase‐2 (COX‐2) overexpression in the tumor microenvironment, causing increased expression of platelet-derived growth factor (PDGF) that contributes to tumor growth, stimulates angiogenesis and promotes pathways of resistance to apoptosis. Among the most widely used non-steroid anti-inflammatory drugs (NSAIDs) are sulindac, indomethacin, meloxicam and celecoxib 92.
Anti-hormonal agents have been used with favorable results even though experts do not know precisely its mechanism of action. The pathway of transforming growth factor beta may be implicated. Tamoxifen and toremifene are the most widely used agents. In one study, progression-free survival was 90% at 12 and 24 months. According to RECIST, partial response, stable disease, and disease progression were observed in 25%, 65% and 10% of patients, respectively. They can be used alone or in combination with anti-inflammatory (anti-COX2) drugs. They are generally the first line of treatment due to their good tolerance and low toxicity profile. Unfortunately, response is usually poor, mostly achieving stabilization of the disease and improvement in pain, which can be observed promptly after treatment has started 93.
In November 2023, the US Food and Drug Administration (FDA) approved the first drug for desmoid tumor, nirogacestat (Ogsiveo) 64 . Nirogacestat, a gamma secretase inhibitor, cleaves multiple transmembrane proteins, including Notch, that are believed to play a role in activating pathways that contribute to growth of desmoid tumors 64. Nirogacestat (Ogsiveo) is indicated for adults with progressing tumors who require systemic treatment 64. The approval was supported by results from the phase 3 DeFi clinical trial 65. In the DeFi clinical trial 65, 70 patients were assigned to receive nirogacestat and 72 to receive placebo. Nirogacestat showed a significant progression-free survival (PFS) benefit over placebo; the likelihood of being event-free at 2 years was 76% with nirogacestat and 44% with placebo 65. Between-group differences in progression-free survival (PFS) were consistent across prespecified subgroups. The percentage of patients who had an objective response was significantly higher with nirogacestat than with placebo (41% vs 8%), with a median time to response of 5.6 months and 11.1 months, respectively; the percentage of patients with a complete response was 7% and 0%, respectively 65.
Controversy exists for the use of systemic chemotherapy in a disease that does not carry a metastatic potential; however, it should be considered as the first line treatment in patients with rapidly progressive or unresectable symptomatic desmoid fibromatosis. Drugs used include doxorubicin (alone or in combination with dacarbazine), vinorelbine, vinblastine, and methotrexate. The anthracycline-based regimen is similar to the one used in sarcomas and is associated with high response rates. It is administered for 6–8 cycles, and regardless of the combination used, objective response or stabilization of the disease is achieved in 80% of the cases, with a lasting response in 45% of patients 94.
Tyrosine kinase inhibitors (TKI) have shown objective responses, despite the fact that their mechanism of action is not fully understood in this circumstance. Still, by blocking the receptor phosphorylation, activation, and proliferation of the kinase, they inhibit growth and block cell proliferation. Agents used include imatinib, nilotinib, sorafenib, sunitinib, and pazopanib. Pazopanib, a potent tyrosine kinase inhibitor, represents a promising new therapy for aggressive fibromatosis in adolescent and young adult patients 67. Imatinib, a selective tyrosine kinase inhibitor (TKI), inhibits several receptors including ABL, PDGFR, and CKIT and has demonstrated a 3-year progression-free survival of 58% with 6% regression after 19–26 months of treatment with a clinical benefit in 84% of the patients 95, 96, 97.
In the DESMOPAZ randomized open phase 2 trial, where patients with progressive desmoid fibromatosis were included, and randomly assigned to pazopanib or vinblastine and methotrexate. The primary objective was the proportion of patients who did not progress in the first six months with 83.7% for pazopanib and 45% for methotrexate-vinblastine. Adverse events were well tolerated 98.
Gounder et al 99 conducted a phase 3, double-blind study in 87 patients with desmoid fibromatosis and progressive symptomatic or recurrent disease. One arm received sorafenib 400 mg orally daily and was compared with placebo. Crossover to the sorafenib group was allowed for patients in the placebo group with progressive disease. The primary objective was progression-free survival. Objective response rates and adverse events were also evaluated. The 2-year progression-free survival rate was 81% in the sorafenib group and 36% in the placebo group. Before crossover, the objective response rate was 33% in the sorafenib group and 20% in the placebo group. Among the patients receiving sorafenib, the most frequently reported adverse events were grade 1 or 2 events, namely rash (73%), fatigue (67%), hypertension (55%), and diarrhea (51%). The high response rate in the placebo group is to be noted and can suggest a proportion of patients with spontaneous regression 99.
Finally, several new pieces of evidence support the concept that deregulation of the mammalian target of the rapamycin (mTOR) cell proliferation/survival pathway may play an important role in tumor biology when the APC/beta-catenin pathway is disrupted. Sirolimus, a drug that inhibits the mammalian target of rapamycin (mTOR), is currently being evaluated as an anti-cancer agent in desmoid tumor 100.
Radiation Therapy
The role of radiotherapy is controversial. Indications for its use in desmoid fibromatosis are debated due to its toxicity, especially in the young population. In the Italian-French consensus it is recommended in progressive disease or in the absence of other therapeutic alternatives 95. In a retrospective review of 22 articles the local control rate was 75% when radiotherapy + surgery was used, 78% for radiotherapy and 61% for surgery, including patients with positive and negative margins; therefore they suggest its use in anatomical sites where surgery can generate considerable morbidity, such as head and neck 101.
The recommended dose is 50–56 Gy in 2 Gy fractions. Other studies have published doses greater than 56 Gy, but they have failed to demonstrate improvement in local control and are associated with greater toxicity including edema, pathological fractures, fibrosis, soft tissue necrosis or vascular complications as well as radio-induced neoplasms 102. In 2017 a meta-analysis was published and concluded that adjuvant radiotherapy should be considered especially in those patients with R1 or R2 resections, since they are at greatest risk of recurrence 103.
Adjuvant radiation therapy
The role of radiation therapy in desmoid tumors has been debated. In a study 31, there was no improvement in outcomes in patients who had received radiation therapy during the course of their treatment (5-year local recurrence–free survival 68% vs 72% without radiation; Figure 6A). Additionally, adjuvant radiation therapy was not significantly associated with improved local recurrence–free survival in any subset of tumors (stratified by size, site, and patient age at diagnosis) except extremity tumors. Adjuvant radiation was most commonly used for extremity tumors (in 23% of these patients), and radiation for extremity tumors was associated with a 15% absolute reduction in local recurrence; local recurrence–free survival among patients with extremity tumors was 71% with radiation vs. 56% without.
Figure 6. Desmoid tumor life expectancy in patients receiving adjuvant radiation
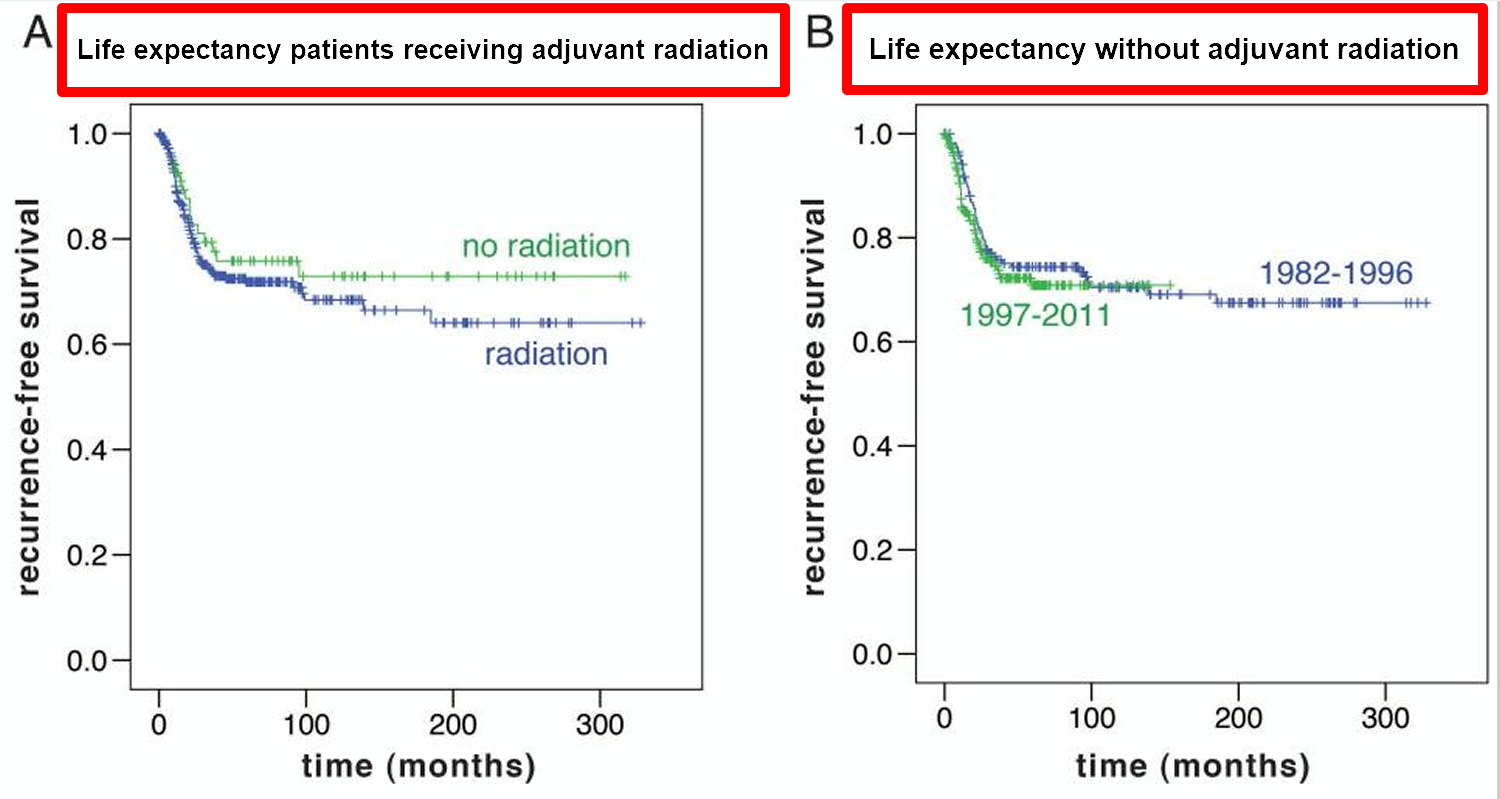
Footnotes: (A) Recurrence-free survival in patients receiving adjuvant radiation versus those not treated with radiation. (B) Recurrence-free survival in patients treated before 1997, when 30% of patients received adjuvant radiation, versus during 1997 and later, when only 7% of patients received adjuvant radiation.
[Source 31]Long-Term Monitoring
It is recommended to monitor patients in an outpatient setting, to perform a physical examination and imaging every 3–4 months, for the first 2 years. Subsequently, the intervals may be longer, and the clinician may choose to alternate MR imaging and ultrasound. When active surveillance is chosen, it should be performed with magnetic resonance imaging (MRI) and with CT for intra-abdominal tumors every month the first 2 months, then every 3 months for a year followed by every 6 months for 5 years and annually thereafter.
Desmoid tumor prognosis
The clinical outcome of aggressive fibromatosis or desmoid tumors may be unpredictable 21, 104, 105, 13, 106. Some tumors resolve spontaneously and others frequently recur despite surgical intervention.
The clinical outcome of aggressive fibromatosis or desmoid tumors can be divided into 4 main groups based on tumor progression:
- Remains stable after diagnosis (most common). Frequently, an initial growth phase is followed by stabilization 107, 108, 109.
- Spontaneously resolves. Spontaneous regressions occur in 20%–30% of patients who are followed for 2–3 years 110, 111. The prognostic value of miRNA expression profiling has been suggested as a way to delineate surgical candidates from those who might be monitored without treatment 112.
- Undergoes cycles of progression and resolution.
- Progresses rapidly causing local infiltration with potential obstruction of vital structures and organs.
Intra-abdominal desmoid tumors carry the highest risk of complications, and patients with syndromic conditions such as familial adenomatous polyposis (FAP) are more likely to have more invasive, symptomatic tumors. Treatment focuses on preventing symptomatic disease rather than total cure; in 70% of patients, the tumor recurs following definitive management, such as surgery or radiotherapy.
Local desmoid tumor recurrence rates are reported to be as high as 70% 113. A positive surgical margin is a significant risk factor for recurrence 114, 115.
Factors significantly associated with shorter progression‐free survival (PFS) include age (younger than 37 years), tumor size (>7 cm), and tumor location (extra‐abdominal) 116, 117, 118, 119.
Intra-abdominal desmoid tumors may kill patients with familial adenomatous polyposis (FAP) 120. Five-year survival rates of such patients with stage 1, 2, 3, and 4 intra-abdominal desmoid tumors were found to be 95%, 100%, 89%, and 76%, respectively 113. The 5-year survival rate of stage 4 patients with severe pain or narcotic dependency, tumor size larger than 10 cm, and need for total parenteral nutrition was only 53% 113.
A study of 179 patients with primary, sporadic desmoid tumors who had complete surgical resection found that those with the S45F mutation had a greater tendency for local recurrence than those without it 121.
- Master SR, Mangla A, Shah C. Desmoid Tumor. [Updated 2024 Mar 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459231[↩][↩][↩]
- Fritchie KJ, Crago AM. Soft Tissue and Bone Tumours, 5th edition. Lyon, France: International Agency for Research on Cancer; 2020. Desmoid Fibromatosis.[↩][↩][↩]
- Ito M, Yokoyama K, Ariizumi Y, Kano Y, Yamamoto K, Asakage T, Tateishi U. Desmoid Fibromatosis Involving the Retropharyngeal and Danger Spaces: A Case Report. Cureus. 2024 Dec 18;16(12):e75969. doi: 10.7759/cureus.75969[↩][↩]
- Murli D, Smriti V, Yadav S, Trivedi B, Qureshi SS. Desmoid Fibromatosis of the Oesophagus Creating an Oesophageal Diverticulum in a 2-year-old Girl. Afr J Paediatr Surg. 2024 Jul 1;21(3):210-212. doi: 10.4103/ajps.ajps_120_22[↩]
- Zhao J, Cheng F, Yao Z, Zheng B, Niu Z, He W. Surgical Management of a Giant Desmoid Fibromatosis of Abdominal Wall With Vessels Invasion in a Young Man: A Case Report and Review of the Literature. Front Surg. 2022 Apr 11;9:851164. doi: 10.3389/fsurg.2022.851164[↩][↩]
- Jang J, Cavallo K, Lee J. Complex Surgical Management of Extensive Chest-Wall Desmoid Fibromatosis. Cureus. 2024 Oct 16;16(10):e71670. doi: 10.7759/cureus.71670[↩]
- Subhawong TK, Feister K, Sweet K, Alperin N, Kwon D, Rosenberg A, Trent J, Wilky BA. MRI Volumetrics and Image Texture Analysis in Assessing Systemic Treatment Response in Extra-Abdominal Desmoid Fibromatosis. Radiol Imaging Cancer. 2021 Jul;3(4):e210016. doi: 10.1148/rycan.2021210016[↩]
- Kangas-Dick A, Ali M, Poss M, Khoury T, Takabe K. Diagnosis and Management of Desmoid Fibromatosis of the Breast. World J Oncol. 2024 Jun;15(3):394-404. doi: 10.14740/wjon1844[↩]
- Ganeshan D, Amini B, Nikolaidis P, Assing M, Vikram R. Current Update on Desmoid Fibromatosis. J Comput Assist Tomogr. 2019 Jan-Feb;43(1):29-38. doi: 10.1097/RCT.0000000000000790[↩][↩]
- Garcia-Ortega DY, Martín-Tellez KS, Cuellar-Hubbe M, Martínez-Said H, Álvarez-Cano A, Brener-Chaoul M, Alegría-Baños JA, Martínez-Tlahuel JL. Desmoid-Type Fibromatosis. Cancers (Basel). 2020 Jul 9;12(7):1851. doi: 10.3390/cancers12071851[↩][↩]
- Braschi-Amirfarzan M, Keraliya AR, Krajewski KM, Tirumani SH, Shinagare AB, Hornick JL, Baldini EH, George S, Ramaiya NH, Jagannathan JP. Role of Imaging in Management of Desmoid-type Fibromatosis: A Primer for Radiologists. Radiographics. 2016 May-Jun;36(3):767-82. doi: 10.1148/rg.2016150153[↩]
- Leithner A, Gapp M, Radl R, Pascher A, Krippl P, Leithner K, Windhager R, Beham A. Immunohistochemical analysis of desmoid tumours. J Clin Pathol. 2005 Nov;58(11):1152-6. doi: 10.1136/jcp.2005.026278[↩]
- Kasper B, Ströbel P, Hohenberger P. Desmoid tumors: clinical features and treatment options for advanced disease. Oncologist. 2011;16(5):682-93. doi: 10.1634/theoncologist.2010-0281[↩][↩]
- Zhao CX, Dombrowski ND, Perez-Atayde AR, Robson CD, Afshar S, Janeway KA, Rahbar R. Desmoid tumors of the head and neck in the pediatric population: Has anything changed? Int J Pediatr Otorhinolaryngol. 2021 Jan;140:110511. doi: 10.1016/j.ijporl.2020.110511[↩]
- Extra-abdominal desmoid tumor fibromatosis: a multicenter EMSOS study. Cuomo P, Scoccianti G, Schiavo A, et al. BMC Cancer. 2021;21:437. doi: 10.1186/s12885-021-08189-6[↩][↩]
- The desmoid tumor. I. Incidence, sex-, age- and anatomical distribution in the Finnish population. Reitamo JJ, Häyry P, Nykyri E, Saxén E. Am J Clin Pathol. 1982;77:665–673. doi: 10.1093/ajcp/77.6.665[↩]
- Lucas A, Braggio D, Hernandez L, Mercier K. A retrospective collection of diagnostic data from the Desmoid Tumor Research Foundation natural history study [abstract]. J Clin Oncol. 2021;39(15 suppl):e23549.[↩]
- Kasper B, Baumgarten C, Garcia J, Bonvalot S, et al; Desmoid Working Group. An update on the management of sporadic desmoid-type fibromatosis: a European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann Oncol. 2017 Oct 1;28(10):2399-2408. doi: 10.1093/annonc/mdx323[↩]
- Mercier KA, Hernandez L, Boulanger V, Seebald A, Rossov S, Milligan K. Quality of life and tumor location in patients with desmoid tumors: data from the Desmoid Tumor Research Foundation natural history study [abstract]. J Clin Oncol. 2019;37(15 suppl):e18291.[↩]
- Fiore M, Crago A, Gladdy R, Kasper B. The Landmark Series: Desmoid. Ann Surg Oncol. 2021 Mar;28(3):1682-1689. doi: 10.1245/s10434-020-09395-5[↩]
- Riedel RF, Agulnik M. Evolving strategies for management of desmoid tumor. Cancer. 2022 Aug 15;128(16):3027-3040. doi: 10.1002/cncr.34332[↩][↩][↩]
- Desmoid Tumor. https://emedicine.medscape.com/article/1060887-overview[↩][↩]
- Buitendijk S, van de Ven CP, Dumans TG, den Hollander JC, Nowak PJ, Tissing WJ, Pieters R, van den Heuvel-Eibrink MM. Pediatric aggressive fibromatosis: a retrospective analysis of 13 patients and review of literature. Cancer. 2005 Sep 1;104(5):1090-9. doi: 10.1002/cncr.21275[↩]
- Inoue Y, Ishida H, Ueno H, Kobayashi H, Yamaguchi T, Konishi T, Tomita N, Matsubara N, Ishida F, Hinoi T, Kanemitsu Y, Watanabe T, Sugihara K. The treatment of desmoid tumors associated with familial adenomatous polyposis: the results of a Japanese multicenter observational study. Surg Today. 2017 Oct;47(10):1259-1267. doi: 10.1007/s00595-017-1500-3[↩]
- Extra-Abdominal Desmoid Tumors. https://orthoinfo.aaos.org/en/diseases–conditions/extra-abdominal-desmoid-tumors[↩]
- Desmoid tumor. https://medlineplus.gov/genetics/condition/desmoid-tumor[↩][↩][↩][↩][↩]
- Ramirez RN, Otsuka NY, Apel DM, Bowen RE. Desmoid tumor in the pediatric population: a report of two cases. J Pediatr Orthop B. 2009 May. 18(3):141-4[↩][↩]
- Buitendijk S, van de Ven CP, Dumans TG, et al. Pediatric aggressive fibromatosis: a retrospective analysis of 13 patients and review of literature. Cancer. 2005 Sep 1. 104(5):1090-9.[↩][↩]
- Inoue Y, Ishida H, Ueno H, Kobayashi H, Yamaguchi T, Konishi T, et al. The treatment of desmoid tumors associated with familial adenomatous polyposis: the results of a Japanese multicenter observational study. Surg Today. 2017 Mar 1.[↩][↩]
- Bertani E, Chiappa A, Testori A, et al. Desmoid tumors of the anterior abdominal wall: results from a monocentric surgical experience and review of the literature. Ann Surg Oncol. 2009 Jun. 16(6):1642-9[↩][↩]
- Crago AM, Denton B, Salas S, et al. A prognostic nomogram for prediction of recurrence in desmoid fibromatosis. Annals of surgery. 2013;258(2):347-353. doi:10.1097/SLA.0b013e31828c8a30. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4096320/[↩][↩][↩][↩]
- Desmoid Tumor Working Group. The management of desmoid tumours: A joint global consensus-based guideline approach for adult and paediatric patients. Eur J Cancer. 2020 Mar;127:96-107. doi: 10.1016/j.ejca.2019.11.013[↩][↩]
- Crago AM, Chmielecki J, Rosenberg M, O’Connor R, Byrne C, Wilder FG, Thorn K, Agius P, Kuk D, Socci ND, Qin LX, Meyerson M, Hameed M, Singer S. Near universal detection of alterations in CTNNB1 and Wnt pathway regulators in desmoid-type fibromatosis by whole-exome sequencing and genomic analysis. Genes Chromosomes Cancer. 2015 Oct;54(10):606-15. doi: 10.1002/gcc.22272[↩]
- Martinez Trufero J., Pajares Bernad I., Torres Ramon I., Hernando C.J., Pazo Cid R. Desmoid Type Fibromatosis: Who, When, and How to Treat. Curr. Treat. Options Oncol. 2017;18:29. doi: 10.1007/s11864-017-0474-0[↩]
- Fiore M., MacNeill A., Gronchi A., Colombo C. Desmoid-Type Fibromatosis: Evolving Treatment Standards. Surg. Oncol. Clin. N. Am. 2016;25:803–826. doi: 10.1016/j.soc.2016.05.010[↩]
- Dômont J, Salas S, Lacroix L, et al. High frequency of beta-catenin heterozygous mutations in extra-abdominal fibromatosis: a potential molecular tool for disease management. Br J Cancer. 2010;102:1032–6. doi: 10.1038/sj.bjc.6605557[↩]
- Immunohistochemistry for beta-catenin in the differential diagnosis of spindle cell lesions: analysis of a series and review of the literature. Carlson JW, Fletcher CD. Histopathology. 2007;51:509–514. doi: 10.1111/j.1365-2559.2007.02794.x[↩][↩]
- Timbergen MJM, van de Poll-Franse LV, Grünhagen DJ, van der Graaf WT, Sleijfer S, Verhoef C, Husson O. Identification and assessment of health-related quality of life issues in patients with sporadic desmoid-type fibromatosis: a literature review and focus group study. Qual Life Res. 2018 Dec;27(12):3097-3111. doi: 10.1007/s11136-018-1931-3[↩]
- Couto Netto SD, Teixeira F, Menegozzo CAM, Leão-Filho HM, Albertini A, Ferreira FO, Akaishi EH, Utiyama EM. Sporadic Abdominal Wall Desmoid type Fibromatosis: treatment paradigm after thirty two years. BMC Surg. 2018 Jun 7;18(1):37. doi: 10.1186/s12893-018-0367-6[↩]
- CTNNB1 gene. https://medlineplus.gov/genetics/gene/ctnnb1[↩][↩][↩][↩]
- APC gene. https://medlineplus.gov/genetics/gene/apc[↩][↩][↩][↩][↩]
- Lopez R, Kemalyan N, Moseley HS, Dennis D, Vetto RM. Problems in diagnosis and management of desmoid tumors. Am J Surg. 1990 May;159(5):450-3. doi: 10.1016/s0002-9610(05)81243-7[↩]
- Desmoid Tumor. https://emedicine.medscape.com/article/1060887-overview#a5[↩]
- Jeong WS, Oh TS, Sim HB, Eom JS. Desmoid tumor following augmentation mammoplasty with silicone implants. Arch Plast Surg. 2013 Jul;40(4):470-2. doi: 10.5999/aps.2013.40.4.470[↩]
- Lotfi AM, Dozois RR, Gordon H, Hruska LS, Weiland LH, Carryer PW, Hurt RD. Mesenteric fibromatosis complicating familial adenomatous polyposis: predisposing factors and results of treatment. Int J Colorectal Dis. 1989;4(1):30-6. doi: 10.1007/BF01648547[↩]
- Wilcken N, Tattersall MH. Endocrine therapy for desmoid tumors. Cancer. 1991 Sep 15;68(6):1384-8. doi: 10.1002/1097-0142(19910915)68:6<1384::aid-cncr2820680634>3.0.co;2-f[↩]
- Waddell WR. Treatment of intra-abdominal and abdominal wall desmoid tumors with drugs that affect the metabolism of cyclic 3′,5′-adenosine monophosphate. Ann Surg. 1975 Mar;181(3):299-302. doi: 10.1097/00000658-197503000-00009[↩]
- Raynham WH, Louw JH. Desmoid tumours in familial polyposis of the colon. S Afr J Surg. 1971 Jul-Sep;9(3):133-40.[↩]
- Shi B, Zhu Y, Xu Z, Liu Y, Zheng B, Qi T. Aggressive fibromatosis in the urological system. Report of two adult patients and review of the literature. Urol Int. 2007;78(1):93-6. doi: 10.1159/000096945[↩]
- Kohno J, Sumiyoshi T, Tsutsumi N, Maeno A, Okubo K, Mitsumori K, Nishimura K, Shintaku M. [Scrotal desmoid tumor in a patient with familial adenomatous polyposis]. Hinyokika Kiyo. 2015 Jan;61(1):27-31. Japanese.[↩]
- Neri HA, Villagra EJ, Alvarez AC, Valencia P, Jiménez E, de la Torre C, Rodríguez MA, Espinosa R. Ethmoidal desmoid tumor in a pediatric patient. Otolaryngol Head Neck Surg. 2007 Jan;136(1):137-8. doi: 10.1016/j.otohns.2005.10.056[↩]
- Muller M, Dessogne P, Baron M, Picquenot JM, Riopel C, Diologent B, Dupre PF, Collet M. Fibromatose mammaire chez une fillette de neuf ans [Desmoid tumor of the breast in a 9 years old little girl]. Ann Pathol. 2011 Feb;31(1):41-5. French. doi: 10.1016/j.annpat.2010.09.011[↩]
- Pajares B, Galera I, Ribelles N, Polo M. Insidious mastalgia hiding a desmoid tumour of the breast. Clin Transl Oncol. 2010 Jan;12(1):63-5. doi: 10.1007/s12094-010-0468-x[↩][↩]
- Mekhail FG, Montgomery JR, Spicer PJ. Imaging findings of a biopsy-proven desmoid tumor of the axilla in a young female. Radiol Case Rep. 2022 Feb 3;17(4):1050-1053. doi: 10.1016/j.radcr.2022.01.054[↩]
- Kotiligam D., Lazar A.J.F., Pollock R., Lev D. Desmoid tumor: A disease opportune for molecular insights. Histol. Histopathol. 2008;23:117–126. doi: 10.14670/HH-23.117[↩]
- Owens C.L., Sharma R., Ali S.Z. Deep fibromatosis (desmoid tumor): Cytopathologic characteristics, clinicoradiologic features, and immunohistochemical findings on fine-needle aspiration. Cancer. 2007;111:166–172. doi: 10.1002/cncr.22689[↩]
- Oudot C, Defachelles AS, Minard-Colin V, Olschwang S, Fourcade L, Helfre S, Orbach D. Les tumeurs desmoïdes en pédiatrie : état des connaissances actuelles [Desmoid tumors in children: current strategy]. Bull Cancer. 2013 May;100(5):518-28. French. doi: 10.1684/bdc.2013.1747[↩][↩]
- Soto-Miranda MA, Sandoval JA, Rao B, Neel M, Krasin M, Spunt S, et al. Surgical Treatment of Pediatric Desmoid Tumors. A 12-Year, Single-Center Experience. Ann Surg Oncol. 2013 Jul 10.[↩]
- Cates JM, Stricker TP, Sturgeon D, Coffin CM. Desmoid-type fibromatosis-associated Gardner fibromas: prevalence and impact on local recurrence. Cancer Lett. 2014 Oct 28. 353(2):176-81.[↩]
- El-Haddad M, El-Sebaie M, Ahmad R, et al. Treatment of aggressive fibromatosis: the experience of a single institution. Clin Oncol (R Coll Radiol). 2009 Dec. 21(10):775-80.[↩]
- Sparber-Sauer M, Seitz G, von Kalle T, Vokuhl C, Leuschner I, Scheer M, et al. Systemic therapy of aggressive fibromatosis in children and adolescents: Report of the Cooperative Weichteilsarkom Studiengruppe (CWS). Pediatr Blood Cancer. 2018 Jan 5.[↩]
- Mercier KA, Al-Jazrawe M, Poon R, Acuff Z, Alman B. A Metabolomics Pilot Study on Desmoid Tumors and Novel Drug Candidates. Sci Rep. 2018 Jan 12. 8 (1):584.[↩]
- Agresta L, Kim H, Turpin BK, Nagarajan R, Plemmons A, Szabo S, et al. Pazopanib therapy for desmoid tumors in adolescent and young adult patients. Pediatr Blood Cancer. 2018 Jan 31.[↩]
- Desmoid Tumor Treatment & Management. https://emedicine.medscape.com/article/1060887-treatment[↩][↩][↩][↩][↩][↩]
- Gounder M, Ratan R, Alcindor T, et al. Nirogacestat, a γ-Secretase Inhibitor for Desmoid Tumors. N Engl J Med. 2023 Mar 9;388(10):898-912. doi: 10.1056/NEJMoa2210140[↩][↩][↩][↩][↩][↩][↩][↩]
- Mercier KA, Al-Jazrawe M, Poon R, Acuff Z, Alman B. A Metabolomics Pilot Study on Desmoid Tumors and Novel Drug Candidates. Sci Rep. 2018 Jan 12;8(1):584. doi: 10.1038/s41598-017-18921-7[↩]
- Agresta L, Kim H, Turpin BK, Nagarajan R, Plemmons A, Szabo S, Dasgupta R, Sorger JI, Pressey JG. Pazopanib therapy for desmoid tumors in adolescent and young adult patients. Pediatr Blood Cancer. 2018 Jun;65(6):e26968. doi: 10.1002/pbc.26968[↩][↩]
- Johns MS, Merritt WT 3rd, Rhodes L, Ford CN, Thompson M, Lee WM, Sheldon Y, Petrelli NJ, Tiesi GJ. A cost analysis of sorafenib for desmoid tumors. J Oncol Pharm Pract. 2023 Apr;29(3):663-668. doi: 10.1177/10781552221077927[↩]
- Mendenhall WM, Zlotecki RA, Morris CG, Hochwald SN, Scarborough MT. Aggressive fibromatosis. Am J Clin Oncol. 2005 Apr;28(2):211-5. doi: 10.1097/01.coc.0000144817.78549.53[↩]
- Bhama PK, Chugh R, Baker LH, Doherty GM. Gardner’s syndrome in a 40-year-old woman: successful treatment of locally aggressive desmoid tumors with cytotoxic chemotherapy. World J Surg Oncol. 2006 Dec 17. 4:96.[↩]
- Constantinidou A, Jones RL, Scurr M, Al-Muderis O, Judson I. Advanced aggressive fibromatosis: Effective palliation with chemotherapy. Acta Oncol. 2010 Aug 30.[↩]
- Knechtel G, Stoeger H, Szkandera J, Dorr K, Beham A, Samonigg H. Desmoid tumor treated with polychemotherapy followed by imatinib: a case report and review of the literature. Case Rep Oncol. 2010 Aug 6. 3(2):287-93.[↩]
- Colombo C, Foo WC, Whiting D, Young ED, Lusby K, Pollock RE, et al. FAP-related desmoid tumors: a series of 44 patients evaluated in a cancer referral center. Histol Histopathol. 2012 May. 27(5):641-9.[↩]
- Avedian RS, Bitton R, Gold G, Butts-Pauly K, Ghanouni P. Is MR-guided High-intensity Focused Ultrasound a Feasible Treatment Modality for Desmoid Tumors?. Clin Orthop Relat Res. 2016 Mar. 474 (3):697-704.[↩]
- Luo J, Jin K, Qian S, Ma X, Pan Z, Yao W, et al. Single institution experience of split course radiotherapy in patients with desmoid tumors. Onco Targets Ther. 2019. 12:1741-1748.[↩]
- Improta L., Tzanis D., Bouhadiba T., Abdelhafidh K., Bonvalot S. Desmoid tumours in the surveillance era: What are the remaining indications for surgery? Eur. J. Surg. Oncol. 2020;46:1310–1314. doi: 10.1016/j.ejso.2020.04.025[↩]
- Al-Jazrawe M., Au M., Alman B. Optimal therapy for desmoid tumors: Current options and challenges for the future. Expert Rev. Anticancer Ther. 2015;15:1443–1458. doi: 10.1586/14737140.2015.1096203[↩]
- Bonvalot S., Eldweny H., Haddad V., Rimareix F., Missenard G., Oberlin O., Vanel D., Terrier P., Blay J.Y., Le Cesne A., et al. Extra-abdominal primary fibromatosis: Aggressive management could be avoided in a subgroup of patients. Eur. J. Surg. Oncol. 2008;34:462–468. doi: 10.1016/j.ejso.2007.06.006[↩]
- Salas S., Dufresne A., Bui B., Blay J.Y., Terrier P., Ranchere-Vince D., Bonvalot S., Stoeckle E., Guillou L., Le Cesne A., et al. Prognostic factors influencing progression-free survival determined from a series of sporadic desmoid tumors: A wait-and-see policy according to tumor presentation. J. Clin. Oncol. 2011;29:3553–3558. doi: 10.1200/JCO.2010.33.5489[↩]
- de Bénazé G.D., Vigan M., Corradini N., Minard-Colin V., Marie-Cardine A., Verite C., Defachelles A.S., Thebaud E., Castex M.P., Sirvent N., et al. Functional analysis of young patients with desmoid-type fibromatosis: Initial Surveillance Does not Jeopardize Long Term Quality of life. Eur. J. Surg. Oncol. 2020;46:1294–1300. doi: 10.1016/j.ejso.2020.02.028[↩][↩]
- Grignol V.P., Pollock R., Howard J.H.H. Management of Desmoids. Surg. Clin. N. Am. 2016;96:1015–1030. doi: 10.1016/j.suc.2016.05.008[↩][↩]
- van Houdt W.J., Husson O., Patel A., Jones R.L., Smith M.J., Miah A.B., Messiou C., Moskovic E., Al-Muderis O., Benson C., et al. Outcome of primary desoid tumors at all anatomic locations initially managed with active surveillance. Ann. Surg. Oncol. 2019;26:4699–4706. doi: 10.1245/s10434-019-07826-6[↩][↩]
- Soto-Miranda MA, Sandoval JA, Rao B, Neel M, Krasin M, Spunt S, Jenkins JJ, Davidoff AM, Ver Halen JP. Surgical treatment of pediatric desmoid tumors. A 12-year, single-center experience. Ann Surg Oncol. 2013 Oct;20(11):3384-90. doi: 10.1245/s10434-013-3090-7[↩]
- Ramirez RN, Otsuka NY, Apel DM, Bowen RE. Desmoid tumor in the pediatric population: a report of two cases. J Pediatr Orthop B. 2009 May;18(3):141-4. doi: 10.1097/BPB.0b013e3283298923[↩]
- Bertani E, Chiappa A, Testori A, Mazzarol G, Biffi R, Martella S, Pace U, Soteldo J, Vigna PD, Lembo R, Andreoni B. Desmoid tumors of the anterior abdominal wall: results from a monocentric surgical experience and review of the literature. Ann Surg Oncol. 2009 Jun;16(6):1642-9. doi: 10.1245/s10434-009-0439-z[↩]
- Ben Haj Amor M, Ploton L, Ceugnart L, Taïeb S. Imagerie par résonance magnétique des tumeurs desmoïdes : critères d’évaluations actuels [Magnetic resonance imaging of desmoid-type fibromatosis: Current evaluation criteria]. Bull Cancer. 2020 Mar;107(3):359-363. French. doi: 10.1016/j.bulcan.2019.11.009[↩]
- Stojadinovic A., Leung D.H., Hoos A., Jaques D.P., Lewis J.J., Brennan M.F. Analysis of the prognostic significance of microscopic margins in 2084 localized primary adult soft tissue sarcomas. Ann. Surg. 2002;235:424–434. doi: 10.1097/00000658-200203000-00015[↩]
- Gronchi A., Casali P.G., Mariani L., Lo Vullo S., Colecchia M., Lozza L., Bertulli R., Fiore M., Olmi P., Santinami M., et al. Quality of surgery and outcome in extra-abdominal aggressive fibromatosis: A series of patients surgically treated at a single institution. J. Clin. Oncol. 2003;21:1390–1397. doi: 10.1200/JCO.2003.05.150[↩]
- Lewis J.J., Boland P.J., Leung D.H., Woodruff J.M., Brennan M.F. The enigma of desmoid tumors. Ann. Surg. 1999;229:866–872. doi: 10.1097/00000658-199906000-00014[↩]
- Cates JM. Pregnancy does not increase the local recurrence rate after surgical resection of desmoid-type fibromatosis. Int J Clin Oncol. 2015 Jun;20(3):617-22. doi: 10.1007/s10147-014-0743-x[↩]
- Cates JM, Stricker TP, Sturgeon D, Coffin CM. Desmoid-type fibromatosis-associated Gardner fibromas: prevalence and impact on local recurrence. Cancer Lett. 2014 Oct 28;353(2):176-81. doi: 10.1016/j.canlet.2014.07.020[↩]
- Crago A.M., Denton B., Salas S., Dufresne A., Mezhir J.J., Hameed M., Gonen M., Singer S., Brennan M.F. A prognostic nomogram for prediction of recurrence in desmoid fibromatosis. Ann. Surg. 2013;258:347–353. doi: 10.1097/SLA.0b013e31828c8a30[↩]
- Yang S., Wang X., Jiang H., Wang Y., Li Z., Lu H. Effective treatment of aggressive fibromatosis with celecoxib guided by genetic testing. Cancer Biol. Ther. 2017;18:757–760. doi: 10.1080/15384047.2017.1373215[↩]
- Janinis J., Patriki M., Vini L., Aravantinos G., Whelan J.S. The pharmacological treatment of aggressive fibromatosis: A systematic review. Ann. Oncol. 2003;14:181–190. doi: 10.1093/annonc/mdg064[↩]
- Garbay D., Le Cesne A., Penel N., Chevreau C., Marec-Berard P., Blay J.Y., Debled M., Isambert N., Thyss A., Bompas E., et al. Chemotherapy in patients with desmoid tumors: A study from the French Sarcoma Group (FSG) Ann. Oncol. 2012;23:182–186. doi: 10.1093/annonc/mdr051[↩][↩]
- Skubitz K.M., Manivel J.C., Clohisy D.R., Frolich J.W. Response of imatinib-resistant extra-abdominal aggressive fibromatosis to sunitinib: Case report and review of the literature on response to tyrosine kinase inhibitors. Cancer Chemother Pharmacol. 2009;64:635–640. doi: 10.1007/s00280-009-1010-0[↩]
- Chugh R., Wathen J.K., Patel S.R., Maki R.G., Meyers P.A., Schuetze S.M., Priebat D.A., Thomas D.G., Jacobson J.A., Samuels B.L., et al. Efficacy of imatinib in aggressive fibromatosis: Results of a phase II multicenter Sarcoma Alliance for Research through Collaboration (SARC) trial. Clin. Cancer Res. 2010;16:4884–4891. doi: 10.1158/1078-0432.CCR-10-1177[↩]
- Toulmonde M., Pulido M., Ray-Coquard I., Andre T., Isambert N., Chevreau C., Penel N., Bompas E., Saada E., Bertucci F., et al. Pazopanib or methotrexate–vinblastine combination chemotherapy in adult patients with progressive desmoid tumours (DESMOPAZ): A non-comparative, randomised, open-label, multicentre, phase 2 study. Lancet. 2019;20:1263–1272. doi: 10.1016/S1470-2045(19)30276-1[↩]
- Gounder M.M., Mahoney M.R., Van Tine B.A., Ravi V., Attia S., Deshpande H.A., Gupta A.A., Milhem M.M., Conry R.M., Movva S., et al. Sorafenib for Advanced and Refractory Desmoid Tumors. J. Med. 2018;379:2417–2428. doi: 10.1056/NEJMoa1805052[↩][↩]
- Skubitz K.M. Biology and Treatment of Aggressive Fibromatosis or Desmoid Tumor. Mayo Clin. Proc. 2017;92:947–964. doi: 10.1016/j.mayocp.2017.02.012[↩]
- A Pilot Study Evaluating the Use of mTor Inhibitor Sirolimus in Children and Young Adults With Desmoid-Type Fibromatosis. https://clinicaltrials.gov/study/NCT01265030[↩]
- Gronchi A., Colombo C., Le Péchoux C., Dei Tos A.P., Le Cesne A., Marrari A., Penel N., Grignani G., Blay J.Y., Casali P.G., et al. Sporadic desmoid-type fibromatosis: A stepwise approach to a non-metastasising neoplasm–A position paper from the Italian and the French Sarcoma Group. Ann. Oncol. 2014;25:578–583. doi: 10.1093/annonc/mdt485[↩]
- Janssen M.L., van Broekhoven D.L., Cates J.M., Salas S., Bonvalot S., Grünhagen D.J., Verhoef C. Meta-analysis of the influence of surgical margin and adjuvant radiotherapy on local recurrence after resection of sporadic desmoid-type fibromatosis. Br. J. Surg. 2017;104:347–357. doi: 10.1002/bjs.10477[↩]
- A prognostic nomogram for prediction of recurrence in desmoid fibromatosis. Crago AM, Denton B, Salas S, et al. Ann Surg. 2013;258:347–353. doi: 10.1097/SLA.0b013e31828c8a30[↩]
- Penel N, Coindre JM, Bonvalot S, Italiano A, Neuville A, Le Cesne A, Terrier P, Ray-Coquard I, Ranchere-Vince D, Robin YM, Isambert N, Ferron G, Duffaud F, Bertucci F, Rios M, Stoeckle E, Le Pechoux C, Guillemet C, Courreges JB, Blay JY. Management of desmoid tumours: A nationwide survey of labelled reference centre networks in France. Eur J Cancer. 2016 May;58:90-6. doi: 10.1016/j.ejca.2016.02.008[↩]
- Prognostic factors influencing progression-free survival determined from a series of sporadic desmoid tumors: a wait-and-see policy according to tumor presentation. Salas S, Dufresne A, Bui B, et al. J Clin Oncol. 2011;29:3553–3558. doi: 10.1200/JCO.2010.33.5489[↩]
- Gronchi A, Raut CP. Optimal approach to sporadic desmoid tumors: from radical surgery to observation. Time for a consensus? Ann Surg Oncol. 2012 Dec;19(13):3995-7. doi: 10.1245/s10434-012-2636-4[↩]
- Kim Y, Rosario MS, Cho HS, Han I. Factors Associated with Disease Stabilization of Desmoid-Type Fibromatosis. Clin Orthop Surg. 2020 Mar;12(1):113-119. doi: 10.4055/cios.2020.12.1.113[↩]
- Stoeckle E, Coindre JM, Longy M, Binh MB, Kantor G, Kind M, de Lara CT, Avril A, Bonichon F, Bui BN. A critical analysis of treatment strategies in desmoid tumours: a review of a series of 106 cases. Eur J Surg Oncol. 2009 Feb;35(2):129-34. doi: 10.1016/j.ejso.2008.06.1495[↩]
- Gounder MM, Mahoney MR, Van Tine BA, et al. Sorafenib for advanced and refractory desmoid tumors. N Engl J Med. 2018;379(25):2417‐2428[↩]
- Bonvalot S, Ternès N, Fiore M, Bitsakou G, Colombo C, Honoré C, Marrari A, Le Cesne A, Perrone F, Dunant A, Gronchi A. Spontaneous regression of primary abdominal wall desmoid tumors: more common than previously thought. Ann Surg Oncol. 2013 Dec;20(13):4096-102. doi: 10.1245/s10434-013-3197-x[↩]
- Dufresne A, Paturel M, Alberti L, Philippon H, Duc A, Decouvelaere AV, Cassier P, Blay JY. Prediction of desmoid tumor progression using miRNA expression profiling. Cancer Sci. 2015 May;106(5):650-5. doi: 10.1111/cas.12640[↩]
- Desmoid Tumor. https://emedicine.medscape.com/article/1060887-overview#a2[↩][↩][↩]
- Huang PW, Tzen CY. Prognostic factors in desmoid-type fibromatosis: a clinicopathological and immunohistochemical analysis of 46 cases. Pathology. 2010 Feb;42(2):147-50. doi: 10.3109/00313020903494078[↩]
- Meazza C, Bisogno G, Gronchi A, Fiore M, Cecchetto G, Alaggio R, Milano GM, Casanova M, Carli M, Ferrari A. Aggressive fibromatosis in children and adolescents: the Italian experience. Cancer. 2010 Jan 1;116(1):233-40. doi: 10.1002/cncr.24679[↩]
- Constantinidou A, Scurr M, Judson I, Litchman C. Clinical presentation of desmoid tumor. In: Litchman C, ed. Desmoid Tumor. Springer Science; 2012:5‐16.[↩]
- Salas S, Dufresne A, Bui B, Blay JY, Terrier P, Ranchere-Vince D, Bonvalot S, Stoeckle E, Guillou L, Le Cesne A, Oberlin O, Brouste V, Coindre JM. Prognostic factors influencing progression-free survival determined from a series of sporadic desmoid tumors: a wait-and-see policy according to tumor presentation. J Clin Oncol. 2011 Sep 10;29(26):3553-8. doi: 10.1200/JCO.2010.33.5489[↩]
- Crago AM, Denton B, Salas S, Dufresne A, Mezhir JJ, Hameed M, Gonen M, Singer S, Brennan MF. A prognostic nomogram for prediction of recurrence in desmoid fibromatosis. Ann Surg. 2013 Aug;258(2):347-53. doi: 10.1097/SLA.0b013e31828c8a30[↩]
- Bishop AJ, Zarzour MA, Ratan R, Torres KE, Feig BW, Wang WL, Lazar AJ, Moon BS, Roland CL, Guadagnolo BA. Long-Term Outcomes for Patients With Desmoid Fibromatosis Treated With Radiation Therapy: A 10-Year Update and Re-evaluation of the Role of Radiation Therapy for Younger Patients. Int J Radiat Oncol Biol Phys. 2019 Apr 1;103(5):1167-1174. doi: 10.1016/j.ijrobp.2018.12.012[↩]
- Quintini C, Ward G, Shatnawei A, Xhaja X, Hashimoto K, Steiger E, Hammel J, Diago Uso T, Burke CA, Church JM. Mortality of intra-abdominal desmoid tumors in patients with familial adenomatous polyposis: a single center review of 154 patients. Ann Surg. 2012 Mar;255(3):511-6. doi: 10.1097/SLA.0b013e31824682d4[↩]
- Colombo C, Miceli R, Lazar AJ, Perrone F, Pollock RE, Le Cesne A, Hartgrink HH, Cleton-Jansen AM, Domont J, Bovée JV, Bonvalot S, Lev D, Gronchi A. CTNNB1 45F mutation is a molecular prognosticator of increased postoperative primary desmoid tumor recurrence: an independent, multicenter validation study. Cancer. 2013 Oct 15;119(20):3696-702. doi: 10.1002/cncr.28271[↩]





{kind=link}