Contents
What is a D&C
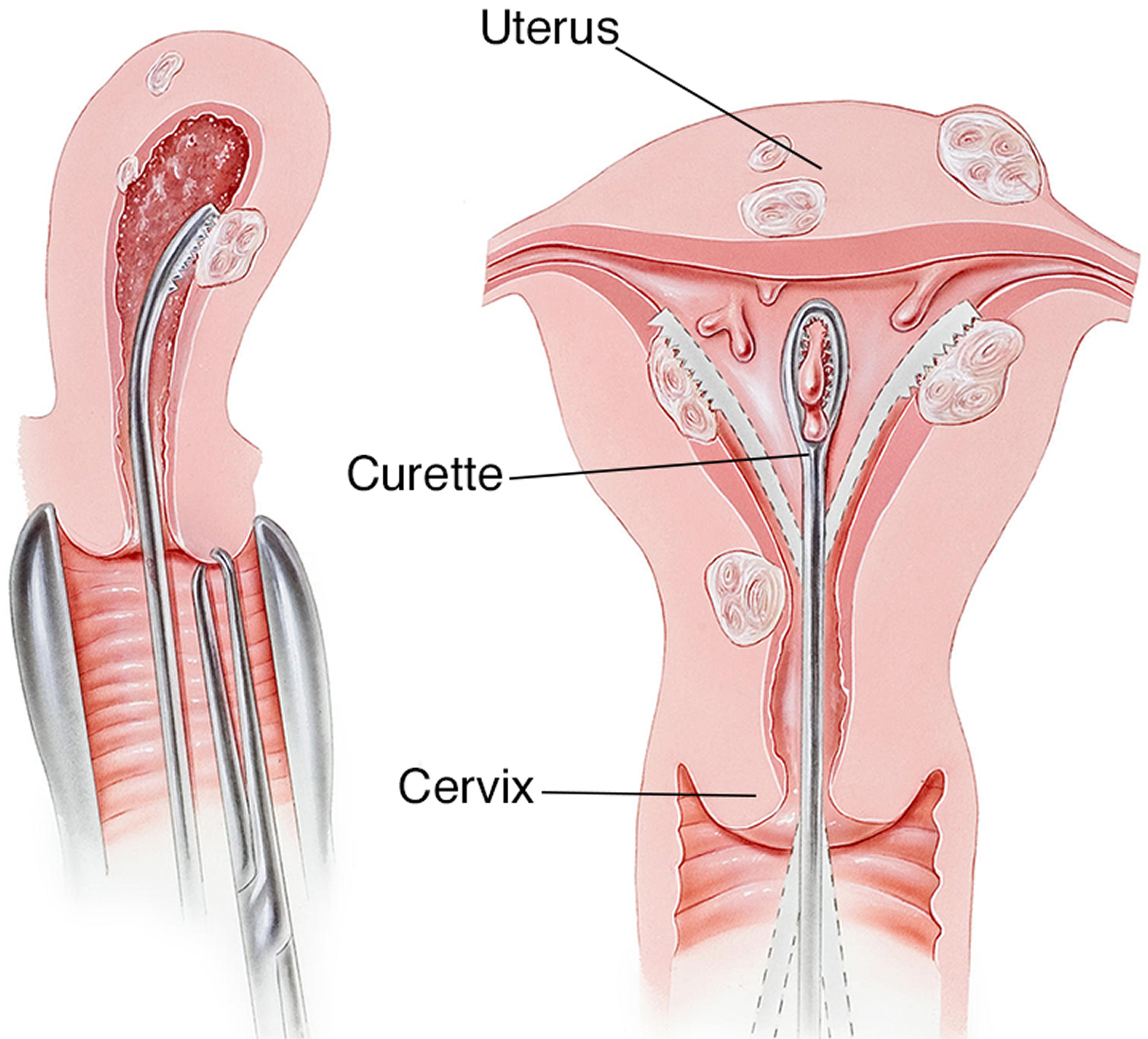
D&C also called dilation and curettage, is a surgical procedure in which the cervix (lower, narrow part of the uterus) is opened (dilated) and a thin instrument is inserted into the uterus so that the uterine lining (endometrium) can be scraped with a curette (spoon-shaped instrument) to remove abnormal tissues. This instrument (curette) is used to remove tissue from the inside of the uterus (curettage). Curettes used in a D&C can be sharp or use suction.
D&C refers to opening of the cervix (dilatation) followed by removal of tissue from inside the uterus (curettage). The D&C procedure is used to diagnose and treat many conditions that affect the uterus, such as abnormal bleeding, bleeding after menopause or if you have abnormal endometrial cells. A small sample of the tissue is sent to a laboratory for testing, allowing a pathologist to identify conditions such as polyps or uterine cancer.
Other related procedures used for diagnosing and treating the endometrium include endometrial ablation, hysteroscopy, in which a slender device is used to view the inside of the uterus and hysterectomy.
A D&C can also be used to remove all the contents from inside your womb, for example after a miscarriage or abortion (to prevent heavy bleeding), to remove remnants of the placenta after childbirth, or to remove polyps. A sample of tissue from inside the uterus can be viewed under a microscope to tell whether any cells are abnormal.
How to prepare for the D&C procedure
Your doctor will ask you a series of questions before a D&C. Make sure you tell them if you are pregnant or might be pregnant, or if you have a history of bleeding or allergies. You should follow any instructions on drinking and eating.
Sometimes your doctor may start dilating your cervix a few hours before the procedure, either with a medication called misoprostol (Cytotec) — given orally or vaginally — to soften the cervix or with a small rod called a laminaria, which is inserted into the cervix and left in place for a while.
Contact your doctor if you experience any of the following after a D&C:
- Bleeding that’s heavy enough that you need to change pads every hour
- Fever
- Cramps lasting more than 48 hours
- Pain that gets worse instead of better
- Foul-smelling discharge from the vagina
How long does a D&C take?
The D&C procedure normally takes 5 to 10 minutes, but you will need to wait in recovery for a few hours afterwards.
How long do you bleed after a D&C?
You might have light bleeding for 10 to 14 days, which may become heavier when you do physical activity such as lifting. Use sanitary pads and not tampons. Your next period may also be heavier than usual.
You should see your doctor 1 to 2 weeks after the D&C procedure, but call them earlier if you experience:
- bleeding after menopause (you need to change the pad every hour)
- fever
- cramps for more than 48 hours
- worsening pain
- a foul-smelling discharge from the vagina
Pregnancy after D&C
Up to 20% of pregnancies result in spontaneous abortion 1. Dilation and curettage (D&C) has been the traditional treatment throughout most of the 20th and 21st centuries 2.
Review of the literature regarding the effect of induced abortion on late pregnancy outcomes yields conflicting results 3. Some studies have suggested that dilation and curettage may predispose to negative future pregnancy outcomes, including higher rates of spontaneous abortion, incompetent cervix, preterm labor, preterm rupture of membranes, early neonatal death, and ectopic pregnancy 4. Multiple dilation and curettage procedures have even been associated with first trimester bleeding, abnormal presentations, placenta abruption, fetal distress, low birth weight, short gestation, and major malformations in subsequent pregnancies 5. The World Health Organization (WHO) in 1979 reported that second trimester spontaneous pregnancy loss was more common in women who had a history of induced abortion compared to primigravid women 6. Other studies concluded that second trimester dilation and evacuation (D&E) was not a risk factor for midtrimester pregnancy loss or spontaneous preterm birth 6. Overall, few studies are available pertaining to the effect of dilation and curettage on future pregnancy outcome, and it is questionable whether existing studies accounted for all confounding variables, including differences in medical history and demographics.
Expectant management has been shown to be successful in 82%–96% of women. Medical management is considered safe and effective, with success rates as high as 95% 7.
The current study 3 suggests that dilation and curettage may predispose to postpartum hemorrhage. It is important to consider the effects of surgical management for miscarriage on future pregnancy outcomes.
Other studies have also described an increase in abnormal bleeding during pregnancy following a D&C. In a study performed by Harlap and Davies in 1975, women with a history of induced abortion reported an increased frequency of first trimester bleeding compared to women with no prior abortions 8. Linn et al. observed an increase in first trimester bleeding in women with a history of one induced abortion, and an increase in first and third trimester bleeding and placental abruption in women with a history of two or more induced abortions 5. It is known that endomyometrial injury is frequent following D&C; in a study performed by Beuker et al. 9 in 2005, myometrium was observed microscopically among products of conception in 44% and 35% of termination and miscarriage tissues, respectively. Levin et al. 10 proposed that curettage itself may increase the risk of subsequent pregnancy loss, and that multiple induced abortions may somehow impair implantation or placentation. This study also suggests that uterine curettage may predispose to abnormal bleeding following delivery.
This study 3 does not demonstrate that cervical dilation during D&C predisposes to cervical insufficiency as previously described. Patients with a history of both dilation and curettage had no increase in poor pregnancy outcomes over patients who underwent curettage alone without mechanical dilation 3. The incidence of cervical incompetence was similar to that reported when patients with preexisting disease were excluded 11. Patients with an incompetent cervix may be at higher risk of requiring a D&C in a subsequent pregnancy secondary to retained placenta or incomplete abortion, which could explain the high incidence of cervical incompetence in this cohort. Other studies have suggested that rigid mechanical dilation, especially above 9 mm, may cause significant cervical trauma. Further research on this topic should be performed to determine at what point dilation becomes significant.
It is important to consider the effects of surgical management for missed and incomplete abortion on future pregnancy outcomes when managing patients. Nonsurgical management is an effective and safe alternative that carries a lower incidence of both short- and medium-term complications in randomized controlled trials 12. A more conservative approach may also decrease healthcare costs due to a reduction in the number of surgical procedures 12. Patient satisfaction should also be considered, and women have expressed high acceptance and satisfaction with conservative management 12. At the least, women should be given the opportunity to choose a treatment option after being informed of all the risks and alternatives. If surgical management is chosen, premedication with cytotec, or preoperative placement of laminaria, could reduce mechanical injury to the cervix and should be considered.
Uterus anatomy
The uterus is a hollow, muscular organ shaped somewhat like an inverted pear. The uterus receives the embryo that develops from an oocyte fertilized in the uterine tube, and sustains its development.
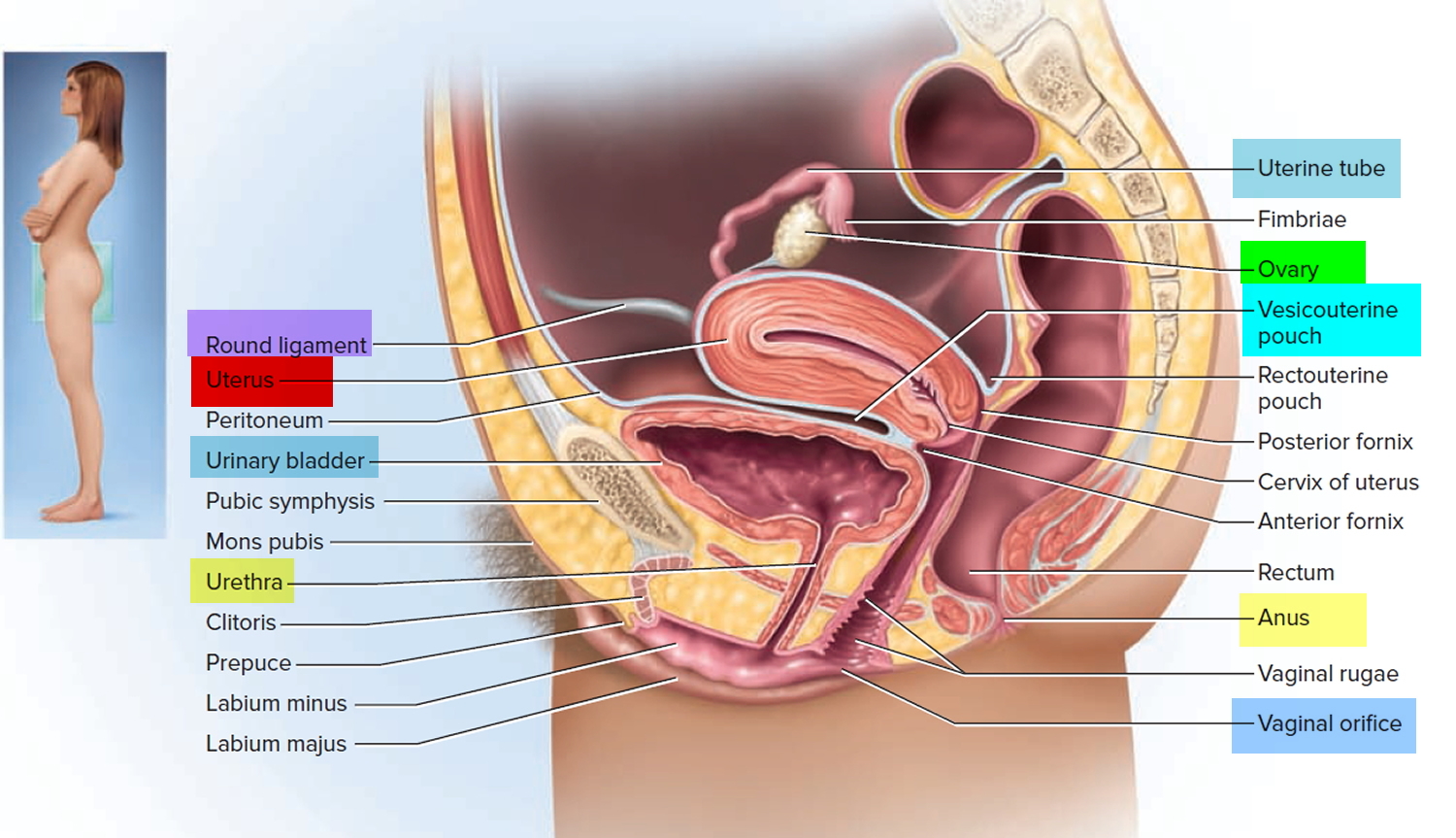
In its nonpregnant, adult state, the uterus is about 7 centimeters long, 5 centimeters wide (at its broadest point), and 2.5 centimeters in diameter. The size of the uterus changes greatly during pregnancy and it is somewhat larger in women who have been pregnant. The uterus is located medially in the anterior part of the pelvic cavity, superior to the vagina, and usually bends forward over the urinary bladder (see Figure 3).
The upper two-thirds or body (corpus), of the uterus has a domeshaped top called the fundus (see Figure 1). The uterine tubes (also called Fallopian tubes) connect at the upper lateral edges of the uterus. The lower third of the uterus is called the cervix. This tubular part extends downward into the upper part of the vagina. The cervix surrounds the opening called the cervical orifice, through which the uterus opens to the vagina.
The uterine wall is thick and has three layers (Figure 1). The endometrium, the inner mucosal layer, is covered with columnar epithelium and contains abundant tubular glands (Figure 3). The myometrium, a thick, middle, muscular layer, consists largely of bundles of smooth muscle cells. During the monthly female menstrual cycles and during pregnancy, the endometrium and myometrium change extensively. The perimetrium consists of an outer serosal layer, which covers the body of the uterus and part of the cervix.
Figure 1. Uterus anatomy
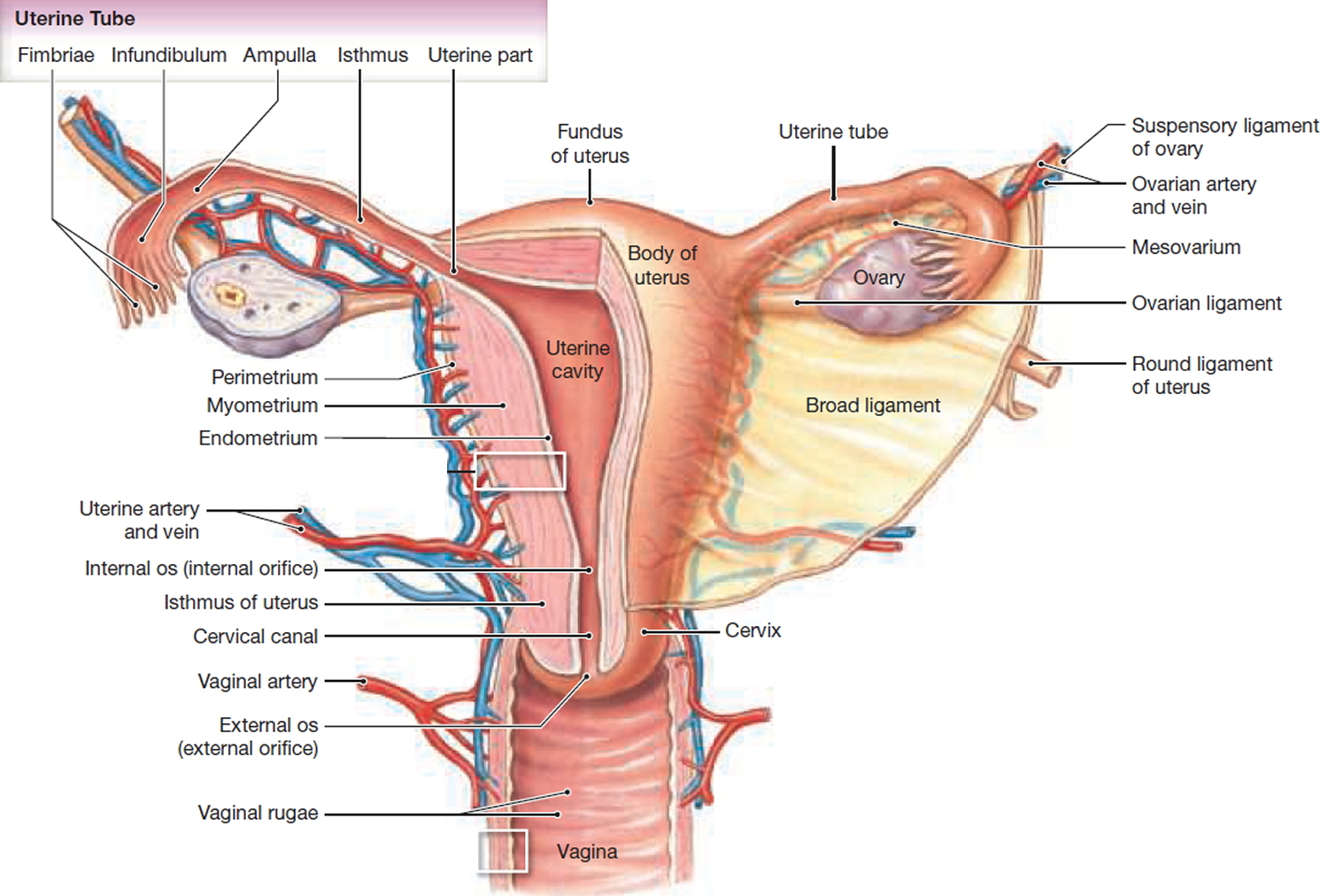
Figure 2. Uterus location
The menstrual cycle
With each menstrual cycle, the endometrium (Figure 3 below) prepares itself to nourish a fetus, as increased levels of estrogen and progesterone help to thicken its walls. If implantation of the fertilized egg does not occur, the lining of the endometrium, coupled with blood and mucus from the vagina and cervix (the lower, narrow part of the uterus located between the bladder and the rectum), make up the menstrual flow (also called menses) that leaves the body through the vagina. After menopause, menstruation stops and a woman should not have any bleeding.
Figure 3. Endometrium of the uterus and its blood supply
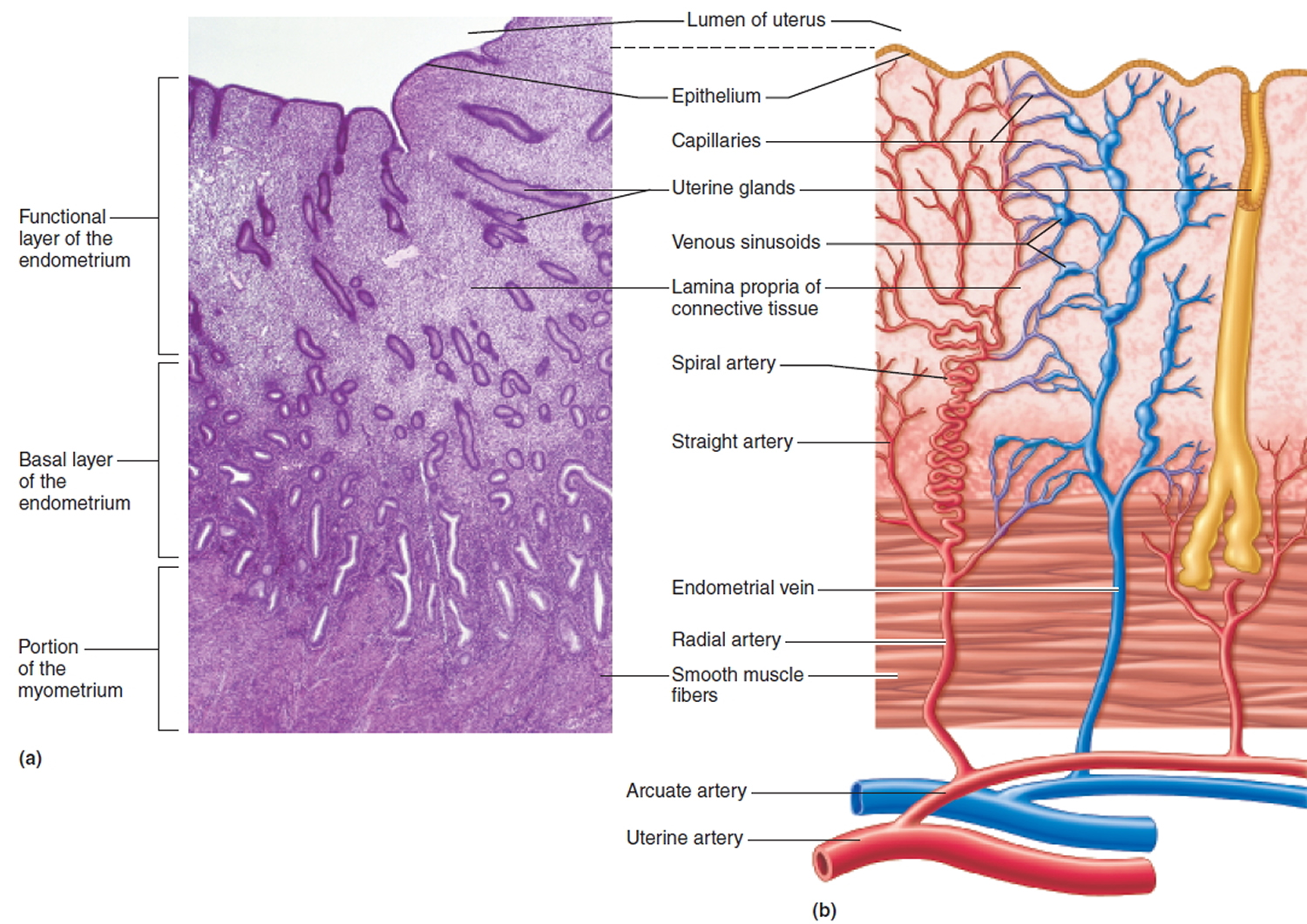 Figure 4. Dilation and curettage
Figure 4. Dilation and curettage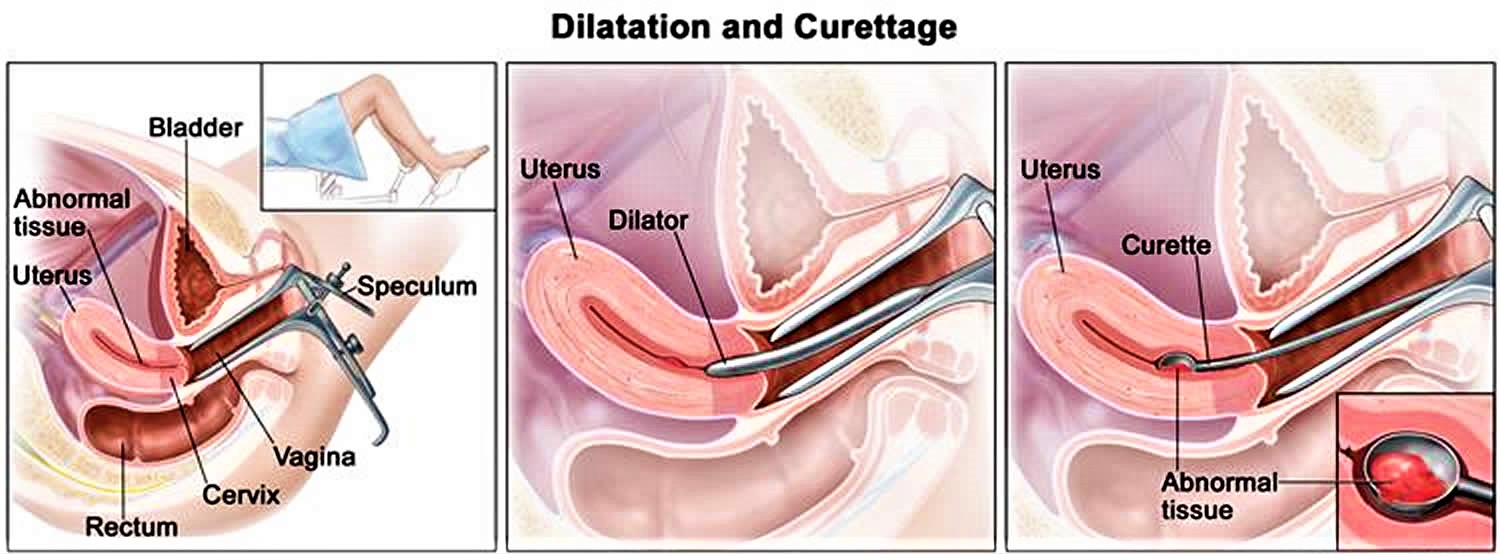
Reasons for D&C procedure
A D&C may be used as a diagnostic or therapeutic procedure for abnormal bleeding. A D&C may be performed to determine the cause of abnormal or excessive uterine bleeding, to detect cancer, or as part of infertility (inability to become pregnant) investigation.
Causes of abnormal bleeding include the presence of abnormal tissues, such as fibroid tumors (benign tumors that develop in the uterus, also called myomas) polyps, or cancer of the endometrium or uterus. Tissues obtained from the D&C can be examined under a microscope. Abnormal uterine bleeding may also be due a hormone imbalance or disorder (particularly estrogen and progesterone) especially in women approaching menopause or after menopause.
A suction D&C uses suction to remove uterine contents. A suction D&C may be used following a miscarriage to remove the fetus and other tissues if they have not all been naturally passed. Infection or heavy bleeding can occur if these tissues are not completely removed.
Occasionally following childbirth, small pieces of the placenta (afterbirth) remain adhered to the endometrium and are not passed. This can cause bleeding or infection. A D&C may be used to remove these fragments so that the endometrium can heal properly.
There may be other reasons for your doctor to recommend a D&C.
D&C to diagnose a condition
Your doctor might recommend a type of D&C called endometrial sampling to diagnose a condition if:
- You have abnormal uterine bleeding
- You experience bleeding after menopause
- Your doctor discovers abnormal endometrial cells during a routine test for cervical cancer
To perform the test, your doctor collects a tissue sample from the lining of your uterus (endometrium) and sends the sample to a lab for testing. The test can check for:
- Endometrial hyperplasia — a precancerous condition in which the uterine lining becomes too thick
- Uterine polyps
- Uterine cancer
D&C to treat a condition
When performing a therapeutic D&C, your doctor removes the contents from inside your uterus, not just a small tissue sample. Your doctor may do this to:
- Clear out tissues that remain in the uterus after a miscarriage or abortion to prevent infection or heavy bleeding
- Remove a molar pregnancy, in which a tumor forms instead of a normal pregnancy
- Treat excessive bleeding after delivery by clearing out any placenta that remains in the uterus
- Remove cervical or uterine polyps, which are usually noncancerous (benign)
Your doctor may perform the D&C along with another procedure called a hysteroscopy. During a hysteroscopy, your doctor inserts a slim instrument with a light and camera on the end into your vagina, through your cervix and up into your uterus.
Your doctor then views the lining of your uterus on a screen, noting any areas that look abnormal, making sure there aren’t any polyps and taking tissue samples as needed. During a hysteroscopy, your doctor can also remove uterine polyps and fibroid tumors.
D&C complications
As with any surgical procedure, complications may occur. Dilation and curettage is usually very safe, and complications are rare. However, there are risks. Some possible complications of a D&C may include, but are not limited to, the following:
- Heavy bleeding
- Infection. Infection after a D&C is possible, but rare.
- Perforation of the uterine wall or bowel. Perforation of the uterus occurs when a surgical instrument pokes a hole in the uterus. This happens more often in women who were recently pregnant and in women who have gone through menopause. Most perforations heal on their own. However, if a blood vessel or other organ is damaged, a second procedure may be necessary to repair it.
- Damage to the cervix. If the cervix is torn during the D&C, your doctor can apply pressure or medicine to stop the bleeding, or can close the wound with stitches (sutures).
- A reaction to the anaesthetic
- Adhesions (scar tissue) may develop inside the uterus, leading to infertility or changes to your menstruation – known as Asherman syndrome, this is very rare and can often be treated with surgery
Patients who are allergic to or sensitive to medications, iodine, or latex should notify their doctor.
If you are pregnant or suspect that you may be pregnant, you should notify your health care provider.
There may be other risks depending on your specific medical condition. Be sure to discuss any concerns with your doctor prior to the procedure.
A vaginal, cervical, or pelvic infection may interfere with a D&C.
Before the D&C procedure
- Your doctor will explain the D&C procedure to you and offer you the opportunity to ask any questions that you might have about the procedure.
- You will be asked to sign a consent form that gives your permission to do the procedure. Read the form carefully and ask questions if something is not clear.
In addition to a complete medical history, your doctor may perform a complete physical examination to ensure you are in good health before undergoing the procedure. You may undergo blood tests or other diagnostic tests.
If your D&C procedure requires general, spinal, or epidural anesthesia, you will be asked to fast for eight hours before the procedure, generally after midnight. If your procedure is to be done under local anesthesia, your doctor will give you instructions about fasting.
- If you are pregnant or suspect that you are pregnant, you should notify your health care provider. He or she may recommend a pregnancy test prior to the procedure.
- Notify your doctor if you are sensitive to or are allergic to any medications, iodine, latex, tape, and anesthetic agents (local and general).
- Notify your doctor of all medications (prescribed and over-the-counter) and herbal supplements that you are taking.
- Notify your doctor if you have a history of bleeding disorders or if you are taking any anticoagulant (blood-thinning) medications, aspirin, or other medications that affect blood clotting. It may be necessary for you to stop these medications prior to the procedure.
If a sedative is given before the procedure, you will need someone to drive you home afterwards.
- Arrange for someone to help you get home because you may be drowsy after the anesthesia wears off.
- Clear your schedule to allow enough time for the procedure and recovery afterward. You’ll likely spend a few hours in recovery after the procedure.
You may want to bring a sanitary napkin to wear home after the procedure.
Based on your medical condition, your doctor may request other specific preparation.
In some cases, your doctor may start the process of dilating your cervix a few hours or even a day before the procedure. This helps your cervix open gradually and is usually done when your cervix needs to be dilated more than in a standard D&C, such as during pregnancy terminations or with certain types of hysteroscopy.
To promote dilation, your doctor uses a medication called misoprostol (Cytotec) — given orally or vaginally — to soften the cervix or inserts a slender rod made of laminaria into your cervix. The laminaria gradually expands by absorbing the fluid in your cervix, causing your cervix to open.
During the D&C procedure
A D&C may be performed in a doctor’s office, on an outpatient basis, or as part of your stay in a hospital. Procedures may vary depending on your condition and your doctor’s practices.
The type of anesthesia will depend on the specific procedure being performed and your medical history. Some D&C procedures may be performed while you are asleep under general anesthesia, or while you are awake under spinal or epidural anesthesia or with a local anaesthetic, where just the area around your cervix is numb. If spinal or epidural anesthesia is used, you will have no feeling from your waist down. The anesthesiologist will continuously monitor your heart rate, blood pressure, breathing, and blood oxygen level during the surgery.
Once you can’t feel anything, your doctor will insert an instrument called a speculum into your vagina so they can see your cervix. They will slowly dilate the cervix using a series of thicker and thicker rods. They will then remove the rods and insert an instrument called a curette to scrape away the lining of the uterus. This can also be done with suction.
The D&C procedure normally takes 5 to 10 minutes, but you will need to wait in recovery for a few hours afterwards.
Generally, a D&C follows this process:
- You will be asked to remove clothing and be given a gown to wear.
- You will be instructed to empty your bladder.
- You lie on your back on an operating or examination table, with your feet and legs supported as for a pelvic examination.
- An intravenous (IV) line may be started in your arm or hand.
- A urinary catheter may be inserted.
- Your doctor will insert an instrument called a speculum into your vagina to spread the walls of the vagina apart to expose the cervix.
- Your cervix may be cleansed with an antiseptic solution.
- For local anesthesia, the doctor may numb the area using a small needle to inject medication.
- If general or regional anesthesia is used, the anesthesiologist will continuously monitor your heart rate, blood pressure, breathing, and blood oxygen level during surgery.
- A type of forceps, called a tenaculum, may be used to hold the cervix steady for the procedure.
- The inside of the cervical canal may be scraped with a small curette if the cervical tissue needs to be examined.
- A thin, rod-like instrument, called a uterine sound, may be inserted through the cervical opening to determine the length of the uterus. If you have local anesthesia, this may cause some cramping. The sound will then be removed.
- The cervix will be dilated by inserting a series of thin rods. Each rod will be larger in diameter than the previous one. This process will gradually enlarge the opening of the cervix so that the curette (spoon-shaped instrument) can be inserted.
- The curette will be inserted through the cervical opening into the uterus and the sharp spoon-shaped edges will be passed across the lining of the uterus to scrape away the tissues. In some cases, suction may be used to remove tissues. If you have local anesthesia, this may cause cramping.
- The instruments will be removed.
Any tissues collected with the procedure will be sent to the lab for examination. Pregnancy tissues (called products of conception) may be sent to the lab for culture or testing for genetic or chromosomal abnormalities.
What to expect after a D&C
The recovery process will vary depending on the type of procedure performed and type of anesthesia that was administered.
If you received regional or general anesthesia, you will be taken to the recovery room for observation. If you had general anesthesia, you may become nauseated or vomit, or you might have a sore throat if a tube was placed in your windpipe to help you breathe. With general anesthesia or light sedation, you may also feel drowsy for several hours.
Once your blood pressure, pulse, and breathing are stable and you are alert, you will be taken to your hospital room or discharged to your home. If this procedure was performed on an outpatient basis, you should plan to have another person drive you home.
After a D&C using local anesthesia, you may rest for about two hours before going home.
You may want to wear a sanitary pad for bleeding. It is normal to have some spotting or light vaginal bleeding for a few days after the procedure.
You may experience cramping for the first few days after a D&C.
Normal side effects of a D&C may last a few days and include:
- Mild cramping
- Spotting or light bleeding
For discomfort from cramping, your doctor may suggest taking ibuprofen (Advil, Motrin IB, others) or another medication.
You should be able to resume your normal activities within a day or two.
You may be instructed not to douche, use tampons, or have intercourse for two to three days after a D&C, or for a period of time recommended by your doctor.
Wait to put anything in your vagina until your cervix returns to normal to prevent bacteria from entering your uterus, possibly causing an infection.
You may also have other restrictions on your activity, including no strenuous activity or heavy lifting.
Because a D&C removes the lining of the uterus, the lining must build back up. Your next menstrual period may begin earlier or later than usual.
You may resume your normal diet unless your doctor advises you differently.
Take a pain reliever for cramping or soreness as recommended by your doctor. Aspirin or certain other pain medications may increase the chance of bleeding. Be sure to take only recommended medications.
Your doctor will advise you on when to return for further treatment or care.
Notify your doctor if you have any of the following:
- Heavy bleeding
- Foul-smelling drainage from your vagina
- Fever and/or chills
- Severe abdominal pain
Your doctor may give you additional or alternate instructions after the procedure, depending on your particular situation.
D&C recovery
It will take you a while to recover if you have had a general anaesthetic, and you should have someone with you when you go home. You should also not drive, operate machinery or drink alcohol for at least 24 hours after the procedure. You can get back to normal activities in a day or two.
You might feel some cramping and discomfort after a D&C, which you can control with paracetamol and with a heat pack. You might have light bleeding for 10 to 14 days, which may become heavier when you do physical activity such as lifting. Use sanitary pads and not tampons. Your next period may also be heavier than usual.
You should see your doctor 1 to 2 weeks after the D&C procedure, but call them earlier if you experience:
- bleeding after menopause (you need to change the pad every hour)
- fever
- cramps for more than 48 hours
- worsening pain
- a foul-smelling discharge from the vagina
D&C recovery time
Normal side effects of a D&C may last a few days and include:
- Mild cramping
- Spotting or light bleeding
For discomfort from cramping, your doctor may suggest taking ibuprofen (Advil, Motrin IB, others) or another medication.
How many days rest after D&C?
You should be able to resume your normal activities within a day or two.
You may be instructed not to douche, use tampons, or have intercourse for two to three days after a D&C, or for a period of time recommended by your doctor.
Wait to put anything in your vagina until your cervix returns to normal to prevent bacteria from entering your uterus, possibly causing an infection.
You may also have other restrictions on your activity, including no strenuous activity or heavy lifting.
- Management of spontaneous abortion. Griebel CP, Halvorsen J, Golemon TB, Day AA. Am Fam Physician. 2005 Oct 1; 72(7):1243-50. https://www.aafp.org/afp/2005/1001/p1243.html[↩]
- A comparison of medical management with misoprostol and surgical management for early pregnancy failure. Zhang J, Gilles JM, Barnhart K, Creinin MD, Westhoff C, Frederick MM, National Institute of Child Health Human Development (NICHD) Management of Early Pregnancy Failure Trial. N Engl J Med. 2005 Aug 25; 353(8):761-9. https://www.nejm.org/doi/10.1056/NEJMoa044064[↩]
- Lohmann-Bigelow J, Longo SA, Jiang X, Robichaux AG. Does Dilation and Curettage Affect Future Pregnancy Outcomes? The Ochsner Journal. 2007;7(4):173-176. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096409/[↩][↩][↩][↩]
- Madore C., Hawes W. E., Many F., et al. A study on the effects of induced abortion on subsequent pregnancy outcome. Am J Obstet Gynecol. 1981;139:516–521 https://www.ncbi.nlm.nih.gov/pubmed/7468718[↩]
- Linn S., Schoenbaum S. C., Monson R. R., et al. The relationship between induced abortion and outcome of subsequent pregnancies. Am J Obstet Gynecol. 1983;146:136–140. https://www.ncbi.nlm.nih.gov/pubmed/6682630[↩][↩]
- Kalish R. B., Chasen S. T., Rosenzweig L. B., et al. Impact of midtrimester dilation and evacuation on subsequent pregnancy outcome. Am J Obstet Gynecol. 2002;187:882–885 https://www.ncbi.nlm.nih.gov/pubmed/12388969[↩][↩]
- Nanda K., Peloggia A., Grimes D., et al. The Cochrane Library, Issue 2, 2007. Oxford: Update Software; Expectant care versus surgical treatment for miscarriage[↩]
- Harlap S., Davies A. M. Late sequelae of induced abortion: complications and outcome of pregnancy and labor. Am J Epidemiol. 1975;102:217–224 https://www.ncbi.nlm.nih.gov/pubmed/1163527[↩]
- Beuker J. M., Erwich J. J., Khong T. Y. Is endomyometrial injury during termination of pregnancy or curettage following miscarriage the precursor to placenta accreta? J Clin Pathol. 2005;58:273–275. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1770603/[↩]
- Levin A. A., Schoenbaum S. C., Monson R. R., et al. Association of induced abortion with subsequent pregnancy loss. JAMA. 1980;243:2495–2499 https://www.ncbi.nlm.nih.gov/pubmed/7382035[↩]
- Vyas N. A., Vink J. S., Ghidini A., et al. Risk factors for cervical insufficiency after term delivery. Am J Obstet Gynecol. 2006;195:787–791 https://www.ncbi.nlm.nih.gov/pubmed/16949413[↩]
- Tam W. H., Tsui M. H. Y., Lok I. H., et al. Long-term reproductive outcome subsequent to medical versus surgical treatment for miscarriage. Hum Reprod. 2005;20:3355–3359[↩][↩][↩]





{kind=link}