
Contents
What is Down syndrome
Down syndrome occurs when a baby is born with an extra (third) copy of chromosome 21. Down syndrome is a genetic condition and is not an illness or a disease. Down syndrome occurs as a result of an extra copy of chromosome 21. One in every 700-900 babies born worldwide will have Down syndrome. Almost 10,000 children are born with Down syndrome in the United States each year (one in 691 live births; prevalence of 10.3 per 10,000) 1. Birth rates are highest among mothers of advanced maternal age (one in 400 at 35 years of age, one in 105 at 40 years of age, one in 12 at 45 years of age); however, 80% of all children with Down syndrome are born to mothers younger than 35 years 2.
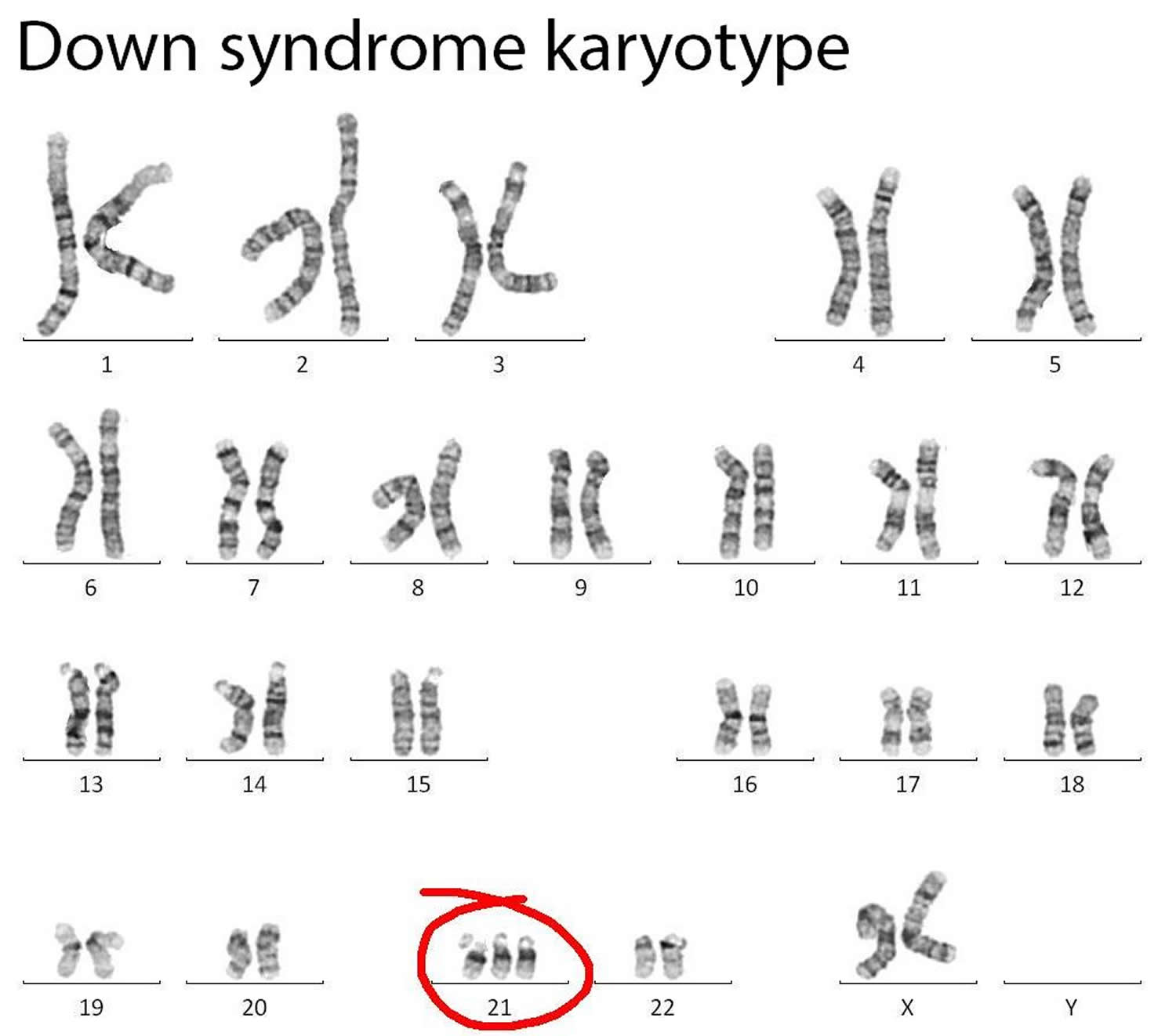
Your bodies are made up of millions of cells. In each cell there are 46 chromosomes (22 pairs of autosomes and 1 sex chromosome). The DNA in your chromosomes determines how you develop. Down syndrome is caused when there is an extra chromosome. People with Down syndrome have 47 chromosomes in their cells instead of 46. They have an extra chromosome 21, which is why Down syndrome is also sometimes known as Trisomy 21. This results in a range of physical characteristics, health and development indications and some level of intellectual disability.
A test for Down syndrome can be carried out before a baby is born. Down syndrome is usually recognized at birth and is confirmed by a blood test. It was named after Dr John Langdon Down who first described it.
Although scientists know how Down syndrome occurs, they do not yet know why it happens. Down syndrome occurs at conception, across all ethnic and social groups and to parents of all ages. It is nobody’s fault. There is no cure for Down syndrome and it does not go away.
Down syndrome is the most common chromosome disorder that scientists know of. One of every 700-900 babies born worldwide will have Down syndrome, although this number is lower in United States. Down syndrome is not a new condition. People with Down syndrome have been recorded throughout history.
People with Down syndrome have:
- some characteristic physical features
- some health and development challenges
- some level of intellectual disability.
Because no two people with Down syndrome are alike, each of these things will vary from one person to another.
Like everyone, people with Down syndrome vary in appearance, ability and personality. But there are some health problems many people with Down syndrome can share.
Figure 1. Normal karyotype
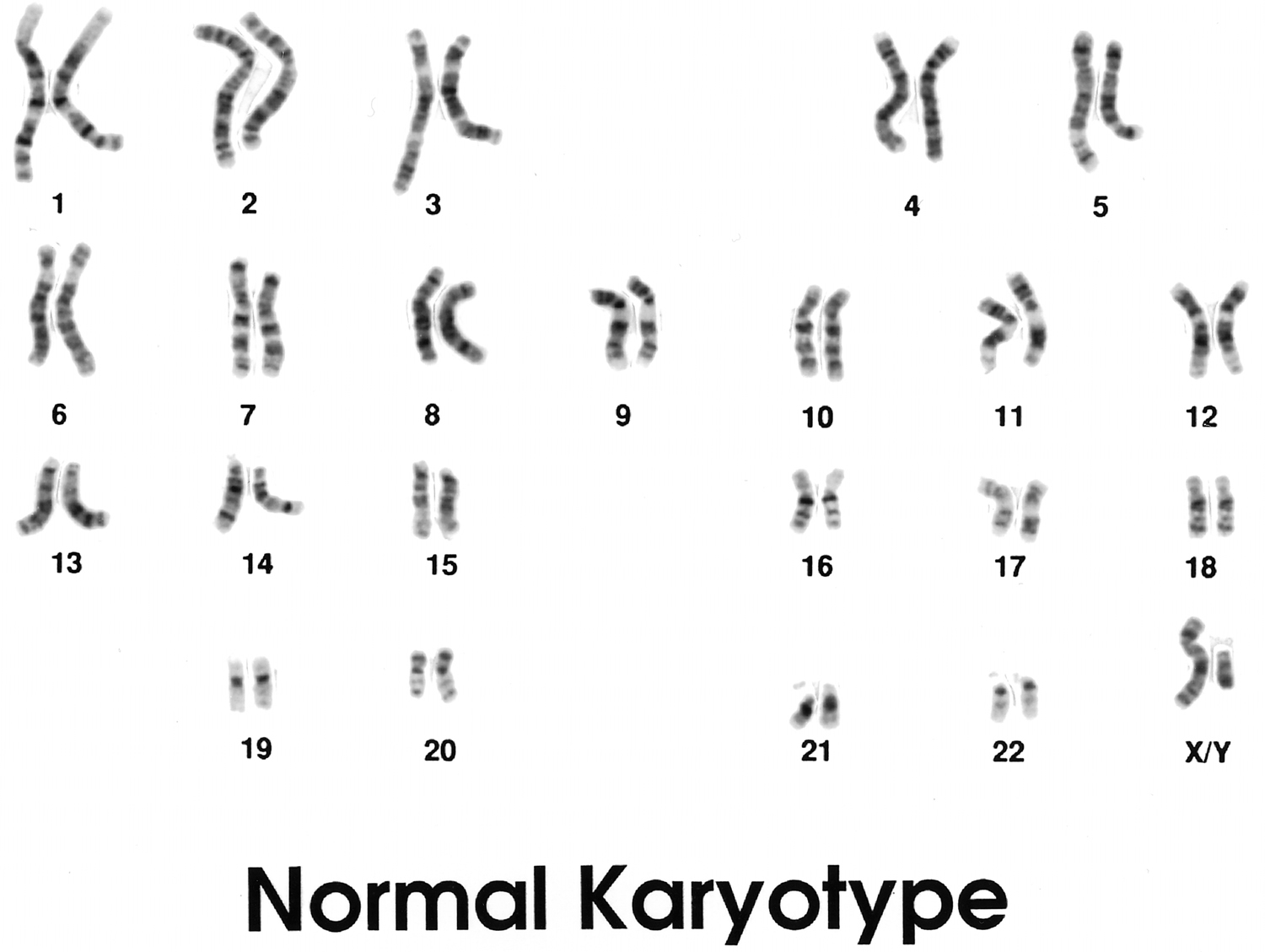
Figure 2. Down syndrome karyotype (note extra copy of chromosome 21)
 Types of Down syndrome
Types of Down syndrome
There are three forms of Down syndrome:
- Trisomy 21: Ninety-five percent of people with Down syndrome have trisomy 21. In this type of Down syndrome, every cell in the body has an extra chromosome 21.
- Mosaic Down syndrome: One to two percent of people with Down syndrome have mosaic Down syndrome. In this type of Down syndrome, only some cells have the extra chromosome 21. The rest of the cells have the usual genetic composition. This sometimes leads to a milder level of intellectual disability and less obvious physical features of Down syndrome.
- Translocation Down syndrome: Three to four percent of people with Down syndrome have translocation Down syndrome. In this type of Down syndrome, extra chromosome 21 material is attached – or translocated – to a different chromosome. This variation does not significantly change the effect of the Down syndrome. Translocation Down syndrome is sometimes hereditary.
The type of Down syndrome is identified by a blood test, usually taken shortly after birth.
Although the chance of having a baby with Down syndrome increases with maternal age, children with Down syndrome are born to mothers of all ages. Most babies with Down syndrome are born to mothers under 35 years of age, because this is the group to which the greatest number of babies are born overall.
Screening and diagnostic tests for Down syndrome are available before a baby is born. Screening tests for Down syndrome are available during the first and second trimesters of pregnancy. These tests will only tell if your baby is at risk of Down syndrome. Further testing can then be done to provide a diagnosis.
Things to consider
In most cases, for every 100 couples who have another baby, 1 will have another baby with Down syndrome. If you’re planning on having more children, talk with your doctor. He or she can help you decide whether to seek genetic counseling before you become pregnant again.
When you first learn that your baby has Down syndrome, you may feel disappointment, grief, anger, frustration, fear, and anxiety about the future. These feelings are all normal. Talking to other parents of children who have Down syndrome can be helpful. They know how you are feeling. You also can talk to your family doctor or visit a support group where you can share your feelings and get additional information.
Down syndrome baby
Babies with Down syndrome are babies. They need the same things, especially love and stimulation, that all babies need. Down syndrome newborns grow and develop in much the same way as other babies. However, they usually reach milestones in development – such as sitting, crawling, walking and talking – at a slower rate.
It is a good idea to make sure that your baby has regular health and development checks. This will allow the health care professionals that you work with to identify and address any issues as soon as possible. Although the most important influence on early development is daily interaction and activities within the family 3, babies with Down syndrome benefit also from structured learning opportunities. Families are encouraged to access the early learning and intervention services that are available from infancy. This will support the development of some of the most important early childhood skills. Early learning and intervention specialists work with families to encourage learning and development in the daily life of the child. Areas of intervention include physiotherapy, occupational therapy (OT), speech and language therapy and early childhood intervention.
Babies who are born with Down syndrome are more likely to have:
- Feeding issues. Learning to suck a bottle or breastfeed may take your baby longer to learn. Breastfeeding is good for all babies, including babies who have Down syndrome. Your doctor, a nurse, a feeding therapist, or another mom who has a baby with Down syndrome can provides tips and special training
- Heart defects. Some heart problems will require surgery within the first year. Other problems will correct themselves over time. If your baby has a heart problem, your doctor will refer you to a cardiologist. He or she will monitor your baby’s heart health until the problem is corrected.
- Hearing issues. Some babies will have partial hearing loss. Babies who have Down syndrome have smaller Eustachian tubes (part of your inner ear). This causes fluid buildup. That can be relieved with tubes. Your doctor will surgically insert the tubes to relieve the fluid. Some babies have permanent nerve damage. This can cause permanent hearing loss. Hearing aids often help your child hear. Without treatment, the hearing loss can affect your baby’s speech development.
- Vision problems. This might include cataracts or other eye issues requiring glasses.
Less likely health issues include:
- intestinal blockage at birth requiring surgery
- hip dislocation
- thyroid disease
- anemia (red blood cells can’t carry enough oxygen to the body) and iron deficiency (anemia where the red blood cells don’t have enough iron)
- leukemia in infancy or early childhood.
Developmental milestones
Your baby will reach all the same infant and toddler milestones. However, it will take him or her a little longer. Early intervention physical and occupational therapy, as well as academic support can help children who have Down syndrome develop.
This includes:
- motor (crawling, walking, feeding, dressing, handwriting)
- language (talking and vocabulary development)
- social (turn-taking, sharing, eye contact, manners)
- academic skills (early reading, counting).
The earlier you baby starts receiving therapy, the better he or she will develop and succeed in life.
Many towns and cities have support groups, organizations, and community resources to help parents who have children with Down syndrome. These resources also are helpful for grandparents, siblings, and other family members. Your doctor can tell you where to find these resources in your community.
Growth and development
Once your baby is home, regular check-ups with the family doctor are important. Your baby might be slow to crawl, slow to walk and slow to talk. You can help your child develop through:
Physiotherapy assists with the development of:
- muscle tone
- motor control
- the balance your body needs for gross motor skills such as crawling and walking.
Occupational therapy assists with the development of:
- the way your hands work
- the way your eyes see and your brain perceives the world around you
- the way different parts of your bodies work together, such as hand-eye coordination
- the fine motor skills you need for moving your fingers and hands
- dressing and other self-care tasks.
Speech and language therapy assists with the development of:
- the muscles you use for speaking
- speech articulation skills
- language and communication skills
- feeding.
Early intervention teachers assist with the development of:
- the learning, social and play skills needed for early childhood activities.
Most children with Down syndrome will experience some delay in all areas of their development. However, the degree of delay will vary in each individual and will not be the same across all areas.
Speech and language development are commonly the areas of greatest delay. Some people have great difficulty speaking clearly and fluently. The diffculties that some people with Down syndrome can experience are related to a combination of physical factors, including muscular development and the activity of the brain that is required to produce clear speech.
Research shows that children with Down syndrome benefit a great deal from learning a system of keyword signs from very early in life. Key word signing helps to alleviate some of the frustration associated with taking longer to learn to speak (which in turn can lead to difficult behavior). It also supports other areas of learning and helps to overcome many of the issues related to delayed language development. One widely used keyword vocabulary sign system is called Makaton.
Some children also benefit from augmentative systems, such as picture symbols, to enhance early communication. Many children with Down syndrome can learn to sight read simple words from an early age and this has been shown to assist the development of speech and language skills.
Both learning keyword signing and early reading can be pursued through early intervention services, or parents can access programs to teach their child at home. All children with Down syndrome will benefit from regular and ongoing speech therapy. Because it takes longer for people with Down syndrome to learn things, skills that seem to happen effortlessly or automatically in other children may need to be care fully taught. New learning often requires mores structure and greater repetition.
New skills may need to be broken into smaller steps and repeated several times. A child with Down syndrome should be encouraged to learn all the things that other young children learn. And, as with all children, early learning forms the foundation for the skills and knowledge you need later in life.
Socially appropriate behavior should be encouraged and expected right from the beginning. Children with Down syndrome benefit from boundary setting in the same way as other children. Parenting a child with Down syndrome will, in many ways, not be very different from parenting any other child. Good parenting practices apply to all children. And as with all children, consistency of approach is important. Most babies and young children can and do attend childcare centers, playgroups and pre-school settings alongside children of the same age. They will learn a great deal from joining in with other young children.
Down Syndrome Kids
Kids with Down syndrome tend to share certain physical features such as a flat facial profile, an upward slant to the eyes, small ears, and a protruding tongue. Although children with Down’s syndrome share some common physical characteristics, they don’t all look the same. A child with Down’s will look more like their family members than other children who have the syndrome.
Low muscle tone (called hypotonia) is also characteristic of children with Down syndrome, and babies in particular may seem especially “floppy.” Though this can and often does improve over time, most children with Down syndrome typically reach developmental milestones — like sitting up, crawling, and walking — later than other kids.
- Around 1 in every 10 kids with Down’s also have other conditions, such as autism spectrum disorder (ASD) or attention deficit hyperactivity disorder (ADHD).
At birth, kids with Down syndrome are usually of average size, but they tend to grow at a slower rate and remain smaller than their peers. For infants, low muscle tone may contribute to sucking and feeding problems, as well as constipation and other digestive issues. Toddlers and older kids may have delays in speech and self-care skills like feeding, dressing, and toilet teaching.
Down syndrome affects kids’ ability to learn in different ways, but most have mild to moderate intellectual impairment. Kids with Down syndrome can and do learn, and are capable of developing skills throughout their lives. They simply reach goals at a different pace — which is why it’s important not to compare a child with Down syndrome against typically developing siblings or even other children with the condition.
Kids with Down’s syndrome will also have different personalities and abilities. Everyone born with Down’s syndrome will have some degree of learning disability, but this will be different for each person.
Kids with Down syndrome have a wide range of abilities, and there’s no way to tell at birth what they will be capable of as they grow up.
Medical Problems Associated With Down syndrome
While some kids with Down syndrome have no significant health problems, others may experience a host of medical issues that require extra care. For example, almost half of all children born with Down syndrome will have a congenital heart defect.
Kids with Down syndrome are also at an increased risk of developing pulmonary hypertension, a serious condition that can lead to irreversible damage to the lungs. All infants with Down syndrome should be evaluated by a pediatric cardiologist.
Approximately half of all kids with Down syndrome also have problems with hearing and vision. Hearing loss can be related to fluid buildup in the inner ear or to structural problems of the ear itself. Vision problems commonly include strabismus (cross-eyed), near- or farsightedness, and an increased risk of cataracts.
Regular evaluations by an otolaryngologist (ear, nose, and throat doctor), audiologist, and an ophthalmologist are necessary to detect and correct any problems before they affect language and learning skills.
Other medical conditions that may happen more frequently in kids with Down syndrome include thyroid problems, stomach and intestinal problems, seizure disorders, breathing problems, including sleep apnea and asthma, obesity, an increased chance of infections, and a higher risk of childhood leukemia. People with Down syndrome sometimes have an unstable upper spine and should be evaluated by a doctor before participating in physical activities. Fortunately, many of these conditions are treatable.
Down Syndrome in Adults
Adults who have Down syndrome need regular health care. Perhaps you have an adult child, brother or sister who has Down syndrome. Your relative needs the same preventive care as an adult who doesn’t have Down syndrome. Also help your relative get checked for special medical problems that are more common in people who have Down syndrome. For example, a doctor should check your relative for thyroid disease, arthritis and problems with vision, hearing and the cervical spine.
With a little planning, your can lead a more independent life. Common things to plan for include the following:
- Housing options such as group homes, supervised independent living or family-owned independent housing. It’s good to make plans for your relative to live independent of you.
- Work options such as sheltered workshops, supported employment and regular employment, with or without a job coach. Employment and social activities add increased meaning to life and may encourage responsible independence in your relative.
- Recreation options such as adult day care, the Special Olympics and other activities that involve exercise, hobbies and interests.
- Special estate planning, education beyond high school and self-help training.
Down syndrome life expectancy
Most of the young people growing up with Down syndrome today will lead quite ordinary lives in the community. Some people with Down syndrome may not need much help to lead an ordinary life, while others may require a lot of support.
As recently as the 1950s, life expectancy for people with Down syndrome was as low as 15 years of age. In recent times, progress in medical and social sciences has very much improved the health and the quality of life enjoyed by people with Down syndrome. In U.S. today, most people with Down syndrome will enjoy a long and healthy life. Today, someone with Down syndrome can expect to live more than 60 years, depending on the severity of health problems.
There are some common health issues and some more serious medical conditions that are more likely to occur in people with Down syndrome than in other people. People with Down syndrome often have lowered general immunity compared to the general population. This means that they may be more susceptible to infections and common illnesses, especially in early childhood. However, a diagnosis of Down syndrome does not mean that someone cannot have a healthy life. Some people with Down syndrome are very fit and healthy, while others experience a range of health issues.
Regular health checks may be required for specific issues. Living a healthy lifestyle is important, including keeping fit and getting regular exercise.
Even with a healthy diet, there can be a tendency for both children and adults with Down syndrome to become overweight. An active lifestyle with plenty of physical activity helps to counterbalance this tendency and encourages general health and fitness.
A small percentage of people with Down syndrome will require a high level of living support. This may be because of complex health issues or a greater degree of intellectual disability.
The most important influence on early development is daily interaction and activities within the family.
Down syndrome medical and health matters
If you have Down syndrome, you may have a higher chance of some health problems than other people. You may also have lower immunity. This means you may get sick more often especially in early childhood.
People with Down syndrome have a higher risk of problems seeing or hearing. You will also tend to have gut or heart defects.
Everyone with Down syndrome has some degree of learning difficulty. You may need speech and language therapy to help you speak clearly.
A healthy diet and physical activity are important for everyone including people with Down syndrome. You have a higher risk than other people of:
- being overweight
- having low thyroid levels
- osteoporosis.
Regular checks may be required for health problems including your teeth development.
There are many people with Down syndrome who are happy, healthy and leading independent lives but you may need more support to help you achieve the kind of life that most people take for granted.
Having an intellectual disability
Down syndrome is the most common cause of intellectual disability that doctors know of. Everyone who has Down syndrome will have some level of intellectual disability. There will be some delay in development and some level of learning difficulty. Because everyone is unique, the level of delay will be different for each person.
While some people with Down syndrome may need relatively little support to lead an ordinary life, others may require a significant level of support to attain basic living skills.
When a baby is born, there is no way to tell what level of intellectual disability the child may have. Nor can scientists predict the way in which this may affect a person’s life. Down syndrome affects, but does not determine development. What happens after birth will be more important in shaping the outlook for a person with Down syndrome, than the occurrence of the extra chromosome at conception. Just like everyone else, the development of individuals with Down syndrome is significantly influenced by family, environment, cultural and social factors.
For many people with Down syndrome, speaking clearly can be difficult. Although a lot of people with Down syndrome speak fluently and clearly, many will need speech and language therapy to achieve this. Very often, people with Down syndrome can understand a lot more than they can express with words. This often means that their abilities are underestimated, which can make them feel frustrated.
Some people with Down syndrome will find it very difficult to develop language skills and speak clearly. This may be made worse by hearing loss.
Living an ordinary life
People with Down syndrome are not fundamentally different from anyone else. They have the same needs and aspirations in life that we all do, including:
- a good place to live
- meaningful employment
- the opportunity to enjoy the company of friends and family
- intimacy
- having a role in our community.
However, achieving these goals is harder for people with Down syndrome than it is for everyone else. Many people with Down syndrome are likely to need some level of support to help them achieve the kind of life that most people take for granted.
Having Down syndrome will not be the most important influence on how that person develops and lives their life.
In the past, many people with Down syndrome have not had the opportunity to develop to their full potential. Often, they have been separated from the rest of the community, living in segregated settings such as care institutions. Low expectations were placed on them and there were limited opportunities for learning and personal growth.
Today scientists recognize that growing up in families and communities, with the same rights and responsibilities as everyone else, is vital to the development of people with Down syndrome.
To be a part of a community you have to be in it. This means that people who have only experienced life in a segregated setting may find it difficult to be included in the general community. Life for people who grow up being included in families and communities will be very different than it has been for those who have always lived in care facilities.
Encouraging children with Down syndrome to go to a school with their peers from their community has many benefits. It opens the way for a smooth transition to adulthood and encourages meaningful inclusion in the community.
People with Down syndrome need opportunities to reach their full potential, like we all do. When given these opportunities, they become valued and productive members of their families and the community.
To be a part of a community you have to be in it.
One of the greatest challenges that people with Down syndrome face is the attitudes of other people who do not understand what it means to have Down syndrome. Despite much change, many people still don’t see the individual person. Instead they just see ‘Down syndrome’ and expect everyone with Down syndrome to be more or less the same.
People with Down syndrome are very different from each other, just as we are all different. Every person with Down syndrome is unique, with their own talents, abilities, thoughts and interests. And, like everyone else, people with Down syndrome have strengths and weaknesses. While one person may read very well but find basic mathematics difficult, another might be a first-class cook and live independently in the community, but will have to work hard to speak clearly. Family passions, culture, interests and skills are also likely to be shared by people with Down syndrome, as they may be by other members of the family.
People with Down syndrome do not all look alike. In fact, people with Down syndrome look more like other people in their own family than they look like others with Down syndrome. Although there are some physical features associated with Down syndrome, there is large variation in how many of these features an individual may have. For some people, one feature may be very prominent while in another it may not exist at all. Importantly, the physical characteristics of Down syndrome that a person may have do not tell us anything about that person’s intellectual ability.
Another common misconception is that all people with Down syndrome are happy and affectionate. People with Down syndrome experience all the same emotions as everyone else. They get happy, sad, embarrassed, frustrated, thoughtful and fall in and out of love, just as we all do. They may, however, find it difficult to express their feelings in words. This can lead to frustration and the expression of feelings through behaviors.
What causes Down syndrome
Doctors know how Down syndrome occurs but not why. The body cells of most people have 46 chromosomes.
People with Down syndrome have an extra chromosome 21 in their body cells. Having this extra chromosone happens by chance – not because of anything parents have done.
Human cells normally contain 23 pairs of chromosomes. One chromosome in each pair comes from your father, the other from your mother.
Down syndrome results when abnormal cell division involving chromosome 21 occurs. These cell division abnormalities result in an extra partial or full chromosome 21. This extra genetic material is responsible for the characteristic features and developmental problems of Down syndrome. Any one of three genetic variations can cause Down syndrome:
- Trisomy 21. About 95 percent of the time, Down syndrome is caused by trisomy 21 — the person has three copies of chromosome 21, instead of the usual two copies, in all cells. This is caused by abnormal cell division during the development of the sperm cell or the egg cell.
- Mosaic Down syndrome. In this rare form of Down syndrome, a person has only some cells with an extra copy of chromosome 21. This mosaic of normal and abnormal cells is caused by abnormal cell division after fertilization.
- Translocation Down syndrome. Down syndrome can also occur when a portion of chromosome 21 becomes attached (translocated) onto another chromosome, before or at conception. These children have the usual two copies of chromosome 21, but they also have additional genetic material from chromosome 21 attached to another chromosome.
There are no known behavioral or environmental factors that cause Down syndrome.
Risk factors for Down syndrome
Some parents have a greater risk of having a baby with Down syndrome. Risk factors include:
- Advancing maternal age. A woman’s chances of giving birth to a child with Down syndrome increase with age because older eggs have a greater risk of improper chromosome division. A woman’s risk of conceiving a child with Down syndrome increases after 35 years of age. However, most children with Down syndrome are born to women under age 35 because younger women have far more babies. At age 35, your risk of having a baby with Down syndrome is about 1 in 350. At age 40, the risk is 1 in 100. By age 45, your risk is 1 in 30.
- Being carriers of the genetic translocation for Down syndrome. Both men and women can pass the genetic translocation for Down syndrome on to their children.
- Having had one child with Down syndrome. Parents who have one child with Down syndrome and parents who have a translocation themselves are at an increased risk of having another child with Down syndrome. If you have a baby with Down syndrome, you have a 1 in 100 chance of having another one. A genetic counselor can help parents assess the risk of having a second child with Down syndrome.
Is Down syndrome inherited?
Most cases of Down syndrome are not inherited, but occur as random events during the formation of reproductive cells (eggs and sperm). An error in cell division called nondisjunction results in reproductive cells with an abnormal number of chromosomes. For example, an egg or sperm cell may gain an extra copy of chromosome 21. If one of these atypical reproductive cells contributes to the genetic makeup of a child, the child will have an extra chromosome 21 in each of the body’s cells.
Mosaic Down syndrome is also not inherited. It occurs as a random error during cell division early in fetal development. As a result, some of the body’s cells have the usual two copies of chromosome 21, and other cells have three copies of the chromosome.
Translocation Down syndrome can be passed from parent to child. However, only about 3 to 4 percent of children with Down syndrome have translocation and only some of them inherited it from one of their parents.
When balanced translocations are inherited, the mother or father has some rearranged genetic material from chromosome 21 on another chromosome, but no extra genetic material. This means he or she has no signs or symptoms of Down syndrome, but can pass an unbalanced translocation on to children, causing Down syndrome in the children.
Down syndrome prevention
There’s no way to prevent Down syndrome. If you’re at high risk of having a child with Down syndrome or you already have one child with Down syndrome, you may want to consult a genetic counselor before becoming pregnant.
A genetic counselor can help you understand your chances of having a child with Down syndrome. He or she can also explain the prenatal tests that are available and help explain the pros and cons of testing.
Screening for Down syndrome
Screening tests for Down syndrome are available during the first and second trimesters of pregnancy. These tests will only tell if your baby is at risk of Down syndrome. Further testing can then be done to provide a diagnosis.
There are 3 types of screening tests that are available that tell you if your baby might be at risk of having Down syndrome. Further diagnostic tests can then be done to confirm the results.
Each test has advantages, disadvantages and limitations. The decision to have testing during pregnancy to determine the risk of Down syndrome is a personal one and it is best made when you have all the available information. You don’t have to have prenatal testing if you don’t wish to.
Combined first trimester screening
This involves a blood test and an ultrasound scan.
Women may be offered 2 ultrasounds at the beginning of their pregnancy:
- a dating scan between weeks 6 and 14 of pregnancy
- if you choose to be screened for Down syndrome, a nuchal translucency scan between 11 weeks and 13 weeks and 6 days of pregnancy, combined with a blood test (called combined first trimester screening).
At the nuchal translucency scan, the sonographer measures the thickness of the nuchal translucency (a pocket of fluid) at the back of your baby’s neck.
You have the blood test between 9 and 14 weeks. The blood test measures the levels of two different hormones that occur naturally in your blood during pregnancy. When there’s a genetic condition the levels of these hormones are usually abnormal.
- Blood test. This blood test measures the levels of pregnancy-associated plasma protein-A (PAPP-A) and the pregnancy hormone known as human chorionic gonadotropin (HCG). Abnormal levels of PAPP-A and HCG may indicate a problem with the baby.
- The triple screen or quadruple screen (also called the multiple marker test). These tests measure the quantities of normal substances in the mother’s blood. As the names imply, triple screen tests for three markers; the quadruple screen includes one additional marker and is more accurate. These tests are typically offered between 15 and 18 weeks of pregnancy.
The information from the blood test is combined with your age and the nuchal translucency measurement and used to work out your individual chance of having a baby with Down syndrome.
If it has not been possible for you to have the combined screening test in early pregnancy, you may be offered a different blood test between 14 and 20 weeks.
This test is called 2nd trimester maternal serum screening (2TMSS) test or Non-invasive prenatal testing (NIPT).
A new blood test called cell-free DNA screen has become available that screens for Down Syndrome and two other related genetic disorders. It tests fetus DNA fragments in the mother’s blood to predict the baby’s risk for birth defects. And while very accurate the cell-free DNA screen is still a screening test, so if it comes back as being abnormal (positive), then a diagnostic test will still be required (see below).
It can be done from around 10 weeks, and while it may replace combined first trimester screening, it shouldn’t replace the 12-week ultrasound as this also screens for structural problems such as spina bifida.
Second trimester screening
If it has not been possible for you to have the combined screening test or the Non-invasive prenatal testing in early pregnancy, you may be offered a different blood test between 14 and 20 weeks.
This test is called 2nd trimester maternal serum screening (2TMSS) test) and measures proteins associated with pregnancy. This information is combined with your age and used to work out your individual chance of having a baby with Down syndrome.
None of the screenings can diagnose Down syndrome. They only indicate that your risk of having a baby with Down syndrome is higher. Some women test positive in the screen but have perfectly healthy babies.
The only way to diagnose Down syndrome before birth is through diagnostic testing. This involves checking the tissue and fluid in the womb for the extra chromosome. This can be done through:
- Chorionic villus sampling (CVS). This takes a sample of the placenta during weeks 10 and 14 of pregnancy.
- Amniocentisis. This takes a sample of the amniotic fluid during weeks 14 to 18 of pregnancy.
- Percutaneous umbilical blood sampling (PUBS). This is also called cordocentesis. It takes a sample of the fetal blood in the umbilical cord during weeks 18 to 22 of pregnancy. It is the most accurate test.
There is a slight risk that these tests can cause a miscarriage. So these tests are used only when there is a higher chance of a genetic problem in the baby. This could be if the mother is 35 or older or if you have received an abnormal screening result. After birth, your doctor can test the baby’s blood for the extra chromosome. This is done if the baby has any of the physical signs or birth defects of Down syndrome.
Diagnostic tests
If the screening tests come back indicating that there is a risk that your baby may have Down syndrome, your doctor will explain the results to you and help you to decide whether you want to have further testing. One of your options will be to have a further diagnostic test which provides a definite answer.
The diagnostic test will either be by chorionic villus sampling (CVS) or amniocentesis. Your doctor will explain the result to you and help you to decide whether you want to have further testing.
Amniocentesis or CVS is done when there is an increased risk that the baby may have genetic disorders or birth defects. It is often done if:
- You are 35 years of age or older by the time your baby is due. You have an increased risk of having a baby with a chromosome abnormality. This could include Down syndrome.
- You had a screening test that showed there could be a problem.
- You have had a child with Down syndrome or another disorder. This could include spina bifida.
- You or your partner is a known carrier of a genetic disorder, such as cystic fibrosis.
Before either procedure, you may have counseling with a genetic expert. This allows you to learn about the conditions the test may find. You will have a better idea of what those mean for you and your baby.
How is amniocentesis performed?
In this procedure, a sample of amniotic fluid (fluid around the baby) is removed from your uterus. A doctor inserts a long, thin needle through your abdomen into your uterus. He or she withdraws a small amount of fluid. The fluid is sent to a laboratory for evaluation. In the lab, the fluid can be tested for:
- genetic abnormalities
- infection
- signs of lung development.
Your body will make more fluid to replace the fluid that is taken out. The baby will not be hurt during the procedure. Some women feel mild cramping during or after the procedure. Your doctor may tell you to rest on the day of the test. Usually you can resume normal activity the next day.
How is chorionic villus sampling (CVS) performed?
CVS removes a small sample of placenta tissue from the uterus. The sample is then sent to the lab for testing.
The sample can be taken 2 ways:
- A catheter (thin tube) through the vagina. The catheter is inserted into the vagina. It is passed through the cervix and into the uterus. The doctor uses images from an ultrasound to guide the catheter to the best spot for sampling.
- A needle through the abdomen. The sample can also be obtained by inserting a needle into the abdomen. The needle then withdraws placenta tissue. Again, ultrasound is used to guide the needle.
Local anesthesia is used for this test to reduce pain and discomfort. Most women feel fine after the test. Some may have mild bleeding (spotting) afterward.
When are the tests performed?
Amniocentesis is usually performed during the 15th week of pregnancy or later. Chorionic villus sampling (CVS) is usually performed between the 10th and 12th weeks of pregnancy.
Is one test better than the other?
The main benefit of chorionic villus sampling (CVS) is that it can be done earlier in the pregnancy. It is very accurate in detecting genetic abnormalities. But it does not detect some things that amniocentesis does. These include:
- neural tube defects (involving the spinal column or brain)
- birth defects
- Rh incompatibility (when the mother has Rh-negative blood and the baby has Rh-positive blood).
Amniocentesis might be the best option if:
- You previously had a baby with a neural tube defect.
- You or your partner have a neural tube defect.
- The results of other tests during your pregnancy have been abnormal. This could include a blood screening test done in early pregnancy.
Chorionic villus sampling (CVS) may be better if you and your doctor want to know the test results during your first trimester.
Things to consider
Amniocentesis and chorionic villus sampling (CVS) carry a few small risks. These include:
- miscarriage
- infection or injury to the baby
- leaking of amniotic fluid
- vaginal bleeding.
The risks of chorionic villus sampling (CVS) are slightly higher than for amniocentesis. Your doctor will talk to you about the risks and benefits of amniocentesis and CVS.
Dealing with the results
It’s always difficult when you’re told that something is wrong with your baby, especially if you’re faced with a painful decision about the future of your pregnancy.
Your doctor will make sure you see the appropriate health professionals to help you get all the information and support you need so you can make the right choices for you and your family.
Down syndrome symptoms
Each person with Down syndrome is an individual — intellectual and developmental problems may be mild, moderate or severe. Some people are healthy while others have significant health problems such as serious heart defects.
Children and adults with Down syndrome have distinct facial features. Though not all people with Down syndrome have the same features, some of the more common features include:
- Flattened face
- Small head
- Short neck
- Protruding tongue
- Upward slanting eye lids (palpebral fissures)
- Unusually shaped or small ears
- Poor muscle tone
- Broad, short hands with a single crease in the palm
- Relatively short fingers and small hands and feet
- Excessive flexibility
- Tiny white spots on the colored part (iris) of the eye called Brushfield’s spots
- Short height
Infants with Down syndrome may be average size, but typically they grow slowly and remain shorter than other children the same age. This includes when they learn to roll over, sit, stand, and walk. They do reach these milestones, but it takes them longer. Physical issues in areas such as the heart, brain and GI tract can cause health problems.
In addition to physical signs, people with Down syndrome often have problems with thinking and learning. These problems include:
- short attention span
- poor judgment
- impulsive behavior
- slow learning
- delayed language and speech.
While these kinds of problems are common, they are rarely severe.
Intellectual disabilities
Most children with Down syndrome have mild to moderate cognitive impairment. Language is delayed, and both short and long-term memory is affected.
Medical conditions
Many different medical conditions are seen in people with Down syndrome, including:
- Birth defects involving the heart, such as an atrial septal defect or ventricular septal defect
- Dementia may be seen
- Eye problems, such as cataracts (most children with Down syndrome need glasses)
- Early and massive vomiting, which may be a sign of a gastrointestinal blockage, such as esophageal atresia and duodenal atresia
- Hearing problems, probably caused by repeated ear infections
- Hip problems and risk of dislocation
- Long-term (chronic) constipation problems
- Sleep apnea (because the mouth, throat, and airway are narrowed in children with Down syndrome)
- Teeth that appear later than normal and in a location that may cause problems with chewing
- Underactive thyroid (hypothyroidism)
Down syndrome complications
People with Down syndrome can have a variety of complications, some of which become more prominent as they get older. These complications can include:
- Heart defects. About half the children with Down syndrome are born with some type of congenital heart defect. These heart problems can be life-threatening and may require surgery in early infancy. Severe heart problems may lead to early death.
- Gastrointestinal (GI) defects. GI abnormalities occur in some children with Down syndrome and may include abnormalities of the intestines, esophagus, trachea and anus. The risk of developing digestive problems, such as GI blockage, heartburn (gastroesophageal reflux) or celiac disease, may be increased.
- Immune disorders. Because of abnormalities in their immune systems, people with Down syndrome are at increased risk of developing autoimmune disorders, some forms of cancer, and infectious diseases, such as pneumonia.
- Sleep apnea. Because of soft tissue and skeletal changes that lead to the obstruction of their airways, children and adults with Down syndrome are at greater risk of obstructive sleep apnea.
- Obesity. People with Down syndrome have a greater tendency to be obese compared with the general population.
- Spinal problems. Some people with Down syndrome may have a misalignment of the top two vertebrae in the neck (atlantoaxial instability). This condition puts them at risk of serious injury to the spinal cord from overextension of the neck.
- Leukemia. Young children with Down syndrome have an increased risk of leukemia, which can also cause early death.
- Dementia. People with Down syndrome have a greatly increased risk of dementia — signs and symptoms may begin around age 30s. Having Down syndrome also increases the risk of developing Alzheimer’s disease. These symptoms include memory loss and personality changes.
- Other problems. Down syndrome may also be associated with other health conditions, including endocrine problems, dental problems, seizures, ear infections, and hearing and vision problems.
For people with Down syndrome, getting routine medical care and treating issues when needed can help with maintaining a healthy lifestyle.
Down syndrome diagnosis
A doctor can often make a diagnosis of Down syndrome at birth based on how the baby looks. The doctor may hear a heart murmur when listening to the baby’s chest with a stethoscope.
A blood test can be done to check for the extra chromosome and confirm the diagnosis.
Most babies born with Down’s syndrome are diagnosed soon after birth and may have:
- floppiness (hypotonia)
- eyes that slant upwards and outwards
- a small mouth with a tongue that may stick out
- a flat back of the head
- below-average weight and length at birth
- their palm may have only one crease across it
Other tests that may be done include:
- Echocardiogram and ECG to check for heart defects (usually done soon after birth)
- X-rays of the chest and gastrointestinal tract
People with Down syndrome need to be closely screened for certain medical conditions. They should have:
- An eye exam every year during infancy
- Hearing tests every 6 to 12 months, depending on age
- Dental exams every 6 months
- X-rays of the upper or cervical spine between ages 3 and 5 years
- Pap smears and pelvic exams beginning during puberty or by age 21
- Thyroid testing every 12 months
Screening tests during pregnancy
The American College of Obstetricians and Gynecologists recommends offering the option of screening tests and diagnostic tests for Down syndrome to all pregnant women, regardless of age.
- Screening tests can indicate the likelihood or chances that a mother is carrying a baby with Down syndrome. But these tests can’t tell for sure or diagnose whether the baby has Down syndrome.
- Diagnostic tests can identify or diagnose whether your baby has Down syndrome.
Your health care provider can discuss the types of tests, advantages and disadvantages, benefits and risks, and the meaning of your results. If appropriate, your provider may recommend that you talk to a genetics counselor.
Screening for Down syndrome is offered as a routine part of prenatal care. Although screening tests can only identify your risk of carrying a baby with Down syndrome, they can help you make decisions about more-specific diagnostic tests.
Screening tests include the first trimester combined test and the integrated screening test.
The first trimester combined test
The first trimester combined test, which is done in two steps, includes:
- Blood test. This blood test measures the levels of pregnancy-associated plasma protein-A (PAPP-A) and the pregnancy hormone known as human chorionic gonadotropin (HCG). Abnormal levels of PAPP-A and HCG may indicate a problem with the baby.
- Nuchal translucency test. During this test, an ultrasound is used to measure a specific area on the back of your baby’s neck. This is known as a nuchal translucency screening test. When abnormalities are present, more fluid than usual tends to collect in this neck tissue.
Using your age and the results of the blood test and the ultrasound, your doctor or genetic counselor can estimate your risk of having a baby with Down syndrome.
Integrated screening test
The integrated screening test is done in two parts during the first and second trimesters of pregnancy. The results are combined to estimate the risk that your baby has Down syndrome.
- First trimester. Part one includes a blood test to measure PAPP-A and an ultrasound to measure nuchal translucency.
- Second trimester. The quad screen measures your blood level of four pregnancy-associated substances: alpha fetoprotein, estriol, HCG and inhibin A.
Diagnostic tests during pregnancy
If your screening test results are positive or worrisome, or you’re at high risk of having a baby with Down syndrome, you might consider more testing to confirm the diagnosis. Your health care provider can help you weigh the pros and cons of these tests.
Diagnostic tests that can identify Down syndrome include:
- Chorionic villus sampling (CVS). In CVS, cells are taken from the placenta and used to analyze the fetal chromosomes. This test is typically performed in the first trimester, between 10 and 13 weeks of pregnancy. The risk of pregnancy loss (miscarriage) from a CVS is very low.
- Amniocentesis. A sample of the amniotic fluid surrounding the fetus is withdrawn through a needle inserted into the mother’s uterus. This sample is then used to analyze the chromosomes of the fetus. Doctors usually perform this test in the second trimester, after 15 weeks of pregnancy. This test also carries a very low risk of miscarriage.
- Percutaneous umbilical blood sampling (PUBS). This is also called cordocentesis. It takes a sample of the fetal blood in the umbilical cord during weeks 18 to 22 of pregnancy. It is the most accurate test.
There is a slight risk that these tests can cause a miscarriage. So these tests are used only when there is a higher chance of a genetic problem in the baby. This could be if the mother is 35 or older or if you have received an abnormal screening result. After birth, your doctor can test the baby’s blood for the extra chromosome. This is done if the baby has any of the physical signs or birth defects of Down syndrome.
Preimplantation genetic diagnosis is an option for couples undergoing in vitro fertilization who are at increased risk of passing along certain genetic conditions. The embryo is tested for genetic abnormalities before it’s implanted in the womb.
Diagnostic tests for newborns
After birth, the initial diagnosis of Down syndrome is often based on the baby’s appearance. But the features associated with Down syndrome can be found in babies without Down syndrome, so your health care provider will likely order a test called a chromosomal karyotype to confirm diagnosis. Using a sample of blood, this test analyzes your child’s chromosomes. If there’s an extra chromosome 21 in all or some cells, the diagnosis is Down syndrome.
Down syndrome treatment
Early intervention for infants and children with Down syndrome can make a major difference in improving their quality of life. Because each child with Down syndrome is unique, treatment will depend on individual needs. Also, different stages of life may require different services.
Treatment could start when your child is a baby. This could happen if he or she is born with a problem, such as a heart defect. They may be screened for other problems that commonly occur with Down syndrome. These include hypothyroidism, hearing loss, vision problems, blood disorders, and digestive problems.
Multidisciplinary health professional team care
If your child has Down syndrome, you’ll likely rely on a team of specialists that can provide medical care and help him or her develop skills as fully as possible. Depending on your child’s particular needs, your team may include some of these experts:
- Primary care pediatrician to coordinate and provide routine childhood care
- Pediatric cardiologist
- Pediatric gastroenterologist
- Pediatric endocrinologist
- Developmental pediatrician
- Pediatric neurologist
- Pediatric ear, nose and throat (ENT) specialist
- Pediatric eye doctor (ophthalmologist)
- Audiologist
- Speech pathologist
- Physical therapist
- Occupational therapist
You’ll need to make important decisions about your child’s treatment and education. Build a team of health care providers, teachers and therapists you trust. These professionals can help evaluate the resources in your area and explain state and federal programs for children and adults with disabilities.
Early intervention
Early intervention involves specialized programs and resources. These are provided to babies and toddlers with Down syndrome and their families. It usually lasts until the child turns 3 years old. Research has shown that early intervention improves outcomes for these children later in life.
Therapies
There are a variety of therapies that can help a child with Down syndrome. These include:
- Physical therapy – exercises and activities that increase strength, improve posture and balance, and build motor skills. Many children with Down syndrome have low muscle tone. Physical therapy can be particularly helpful for them.
- Speech therapy – helps them communicate better and improve their language skills. Children with Down syndrome often speak later than other children. This therapy can help them develop those skills.
- Occupational therapy – adjusts everyday activities to the child’s abilities. This therapy teaches skills your child will use every day. These include eating, getting dressed, and caring for themselves.
- Behavioral therapy – helps your child cope with his or her condition. Complicated feelings and behaviors often go along with it. Children with Down syndrome get frustrated and can develop compulsive behaviors. They are more likely to have ADHD or other mental health issues. Therapy with a mental health professional can help.
Special education and training is offered in most communities for children with delays in mental development. Speech therapy may help improve language skills. Physical therapy may teach movement skills. Occupational therapy may help with feeding and performing tasks. Mental health care can help both parents and the child manage mood or behavior problems. Special educators are also often needed.
Assistive devices
An assistive device is any tool, technology, or piece of equipment that helps your child function more easily. This could include something as simple as a modified pencil that makes writing easier. Or it might be a special touchscreen computer that allows your child to communicate.
Living with Down syndrome
There are other health problems that often go along with having Down syndrome. Every person with Down syndrome is different. Your child may or may not have or develop any of these other conditions.
- Poor muscle tone. This makes it harder for them to learn to roll over, sit up and walk. Physical therapy can help with these problems.
- Heart defects. About half of babies who have Down syndrome also have a heart problem. An ultrasound exam of your baby’s heart will show any defects. Surgery may be necessary to fix the heart problems associated with Down syndrome.
- Digestive problems. Some babies who have Down syndrome have problems swallowing. Others may have blockages in their intestines. Surgery may be necessary to fix these problems. Once they are fixed, they usually cause no further harm. Children are more likely to have Celiac disease. This causes intestinal problems when they eat gluten, a protein in wheat.
- Hearing problems. Up to 75% of children with Down syndrome have problems with their hearing. They need regular hearing screenings and might need to have the problems corrected.
- Vision problems. Some babies have eye problems, such as cataracts (cloudy lenses) or crossed eyes. Corrective lenses or surgery may be necessary to fix these problems.
- Infections. Down syndrome causes problems with the immune system that makes it harder to fight infection. Your child may have colds, ear infections, and sinus infections more often than other children. It’s important for children with Down syndrome to receive all of their recommended vaccines.
- Blood disorders. Those with Down syndrome are more likely to have blood problems. These could include anemia (low iron) and polycythemia (high levels of red blood cells). Children with Down syndrome are more likely to develop leukemia (cancer of the white blood cells).
- Premature aging. Adults with Down syndrome can develop health problems normally caused by aging. These include dementia, memory loss, high cholesterol, diabetes, cataracts, and early menopause.
- Learning disabilities. At birth, it isn’t possible to tell how smart a baby who has Down syndrome will be. Intelligence ranges from low normal to very slow to learn.
- Obesity can become a problem for older children and adults. Getting plenty of activity and avoiding high-calorie foods are important. Before beginning sports activities, the child’s neck and hips should be examined.
Behavioral training can help people with Down syndrome and their families deal with the frustration, anger, and compulsive behavior that often occur. Parents and caregivers should learn to help a person with Down syndrome deal with frustration. At the same time, it is important to encourage independence.
Teen girls and women with Down syndrome are usually able to get pregnant. There is an increased risk for sexual abuse and other types of abuse in both males and females. It is important for those with Down syndrome to:
- Be taught about pregnancy and taking the proper precautions
- Learn to advocate for themselves in difficult situations
- Be in a safe environment
Keep your child physically healthy. Provide therapy or treatment for his or her impairments. This will help them be better able to learn. With therapy, many children with Down syndrome grow up to have jobs and live independently.
Coping and support
When you learn your child has Down syndrome, you may experience a range of emotions, including anger, fear, worry and sorrow. You may not know what to expect, and you may worry about your ability to care for a child with a disability. The best antidote for fear and worry is information and support.
Support Groups
The following resources can provide more information on Down syndrome:
- National Down Syndrome Society — www.ndss.org
- National Down Syndrome Congress — www.ndsccenter.org
Consider these steps to prepare yourself and to care for your child:
- Ask your health care provider about early intervention programs in your area. Available in most states, these special programs offer infants and young children with Down syndrome stimulation at an early age (typically until age 3) to help develop motor, language, social and self-help skills.
- Learn about educational options for school. Depending on your child’s needs, that may mean attending regular classes (mainstreaming), special education classes or both. With your health care team’s recommendations, work with the school to understand and choose appropriate options.
- Seek out other families who are dealing with the same issues. Most communities have support groups for parents of children with Down syndrome. You can also find internet support groups. Family and friends can also be a source of understanding and support.
- Participate in social and leisure activities. Take time for family outings and look in your community for social activities such as park district programs, sports teams or ballet classes. Although some adaptations may be required, children and adults with Down syndrome can enjoy social and leisure activities.
- Encourage independence. Your child’s abilities may be different from other children’s abilities, but with your support and some practice your child may be able to perform tasks such as packing lunch, managing hygiene and dressing, and doing light cooking and laundry.
- Prepare for the transition to adulthood. Opportunities for living, working, and social and leisure activities can be explored before your child leaves school. Community living or group homes, and community employment, day programs or workshops after high school require some advance planning. Ask about opportunities and support in your area.
Expect a bright future. Most people with Down syndrome live with their families or independently, go to mainstream schools, read and write, participate in the community, and have jobs. People with Down syndrome can live fulfilling lives.
- Carroll KN, Arbogast PG, Dudley JA, Cooper WO. Increase in incidence of medically treated thyroid disease in children with Down Syndrome after rerelease of American Academy of Pediatrics Health Supervision guidelines. Pediatrics. 2008;122(2):e493–e498.[↩]
- National Down Syndrome Society. Down syndrome facts. https://www.ndss.org/about-down-syndrome/down-syndrome-facts/[↩]
- Mahoney, G et al (2006) ‘Responsive teaching: early intervention for children with Down syndrome and other disabilities.’ Down Syndrome Research and Practice 11(1) 18-28.[↩]





{kind=link}