
Contents
- What does it mean to eat clean?
- Mediterranean Diet
- DASH Diet
- How to lose belly fat
- How many calories do I need per day?
- How many calories should I eat to lose weight?
- What happens when your calories are too low?
- Setting Realistic Goals
- What is the best way to lose weight?
- Healthy Weight-Loss
- Healthy Eating Choices
- Weight loss exercise
What does it mean to eat clean?
“How to eat clean?” Many clinicians find themselves at a loss to answer this common question from patients. The difficulty of offering a simple answer is understandable. The overwhelming volume of data generated by food and nutrition researchers coupled with sometimes contradictory findings, the seeming flip-flops in recommendations, and the flood of misinformation in diet books and the media can make it seem as though explaining the essentials of healthy eating is akin to describing the intricacies of particle physics. That is unfortunate, because there are now enough solid evidence from reliable sources to weave simple but compelling recommendations about clean eating.
The fundamentals of eating clean encourage you to consume more whole foods — such as fruits, vegetables, lean proteins, whole grains and healthy fats — and limit highly processed snack foods, sweets and other packaged foods.
Eating clean is about eating healthy and nutritious foods, food groups and dietary patterns that aim to:
- promote health and wellbeing;
- reduce your risk of diet-related conditions, such as high cholesterol, high blood pressure and obesity; and
- reduce your risk of chronic diseases such as type 2 diabetes, cardiovascular disease and some types of cancers.
Clean eating isn’t black and white. There’s room for flexibility and modifications, and it doesn’t require avoiding any certain food groups — unless medically necessary.
Clean eating also doesn’t mean that all foods must be consumed in the raw state. Cooking, pasteurizing and preserving are okay.
Replacing meals with store-bought protein shakes or sugary smoothies and juices is not an example of clean eating.
Although research on nutrients such as fats, carbohydrates, and specific vitamins and minerals has been revealing, it has also generated some dead ends, along with myths and confusion about what constitutes clean eating. A key reason is because people eat food, not nutrients. Furthermore, humans tend to follow relatively repeatable dietary patterns. Although it is harder to study dietary patterns than it is to study nutrients, new research has shown how some dietary patterns are good for long-term health.
One dietary pattern that may harm long-term health is the typical Western diet—rich in red meat, highly processed grains, and sugar, and lacking in fruits, vegetables, whole grains, and fiber. A host of studies have emphasized that this type of dietary pattern promotes atherosclerosis and a variety of cardiovascular conditions, including heart attack and stroke, peripheral vascular disease, and heart failure 1, 2.
A clean eating plan gives your body the nutrients it needs every day while staying within your daily calorie goal for weight loss. A clean eating plan also will lower your risk for heart disease and other health conditions 3.
All food and beverage choices matter. Choose a healthy eating pattern at an appropriate calorie level to help achieve and maintain a healthy body weight, support nutrient adequacy, and reduce the risk of chronic disease. Over time, if you eat and drink more calories than your body uses or “burns off,” your body may store the extra energy, leading to weight gain.
According to the Dietary Guidelines for Americans 4, a clean eating is eating a diet that is healthy. A clean eating plan involves:
- Emphasizes vegetables, fruits, whole grains, and fat-free or low-fat milk products.
- Includes lean meats, poultry, fish, beans, eggs, and nuts.
- Is low in saturated fats, trans fats, cholesterol, salt, and added sugars.
- Grains, at least half of which are whole grains.
- Controls portion sizes.
- Balances the calories you take in from food and beverages with the calories burned through physical activity to maintain a healthy weight.
- Consume less than 10 percent of calories per day from added sugars.
- Consume less than 5-7 percent of calories per day from saturated fats.
- Consume less than 2,300 milligrams (mg) per day of sodium (salt).
- If alcohol is consumed, it should be consumed in moderation—up to one drink per day for women and up to two drinks per day for men—and only by adults of legal drinking age. It is not recommended that individuals begin drinking or drink more for any reason.
Here are some tips to help you meet the eat clean guidelines:
- Eating fruits and vegetables of different colors gives your body a wide range of valuable nutrients.
- A variety of vegetables from all of the subgroups—dark green, red and orange, legumes (beans and peas), starchy, and other.
- Fruits, especially whole fruits.
- Include foods that contain fiber such as fruits, vegetables, beans, and whole-grains.
- Eat lean cuts of meat and poultry. Trim away excess fat and remove skin from poultry before cooking.
- Limit calories from added sugars and saturated fats and reduce sodium intake. Consume an eating pattern low in added sugars, saturated fats, and sodium. Cut back on foods and beverages higher in these components to amounts that fit within healthy eating patterns.
- Limiting highly processed, packaged foods with a long list of ingredients, most of which are not natural. Ingredients listed on the food label should mostly be foods that you recognize, such as whole-grain steel cut oats, dried apple, flaxseed and cinnamon. Limit ingredients that you can’t identify or can’t easily pronounce, such as carnauba wax, soy lecithin and artificial flavor.
- Cutting back on foods with added salt, sugar or fat.
- Avoiding foods that are drastically altered compared with their natural form, such as apple juice versus a whole apple, chicken nuggets versus a fresh chicken breast, or vegetable chips versus fresh vegetables. Sometimes processing can be a good thing for foods, such as pasteurization that makes eggs and dairy products safe for consumption. Also, frozen fruits and vegetables are okay because they are minimally processed and can sometimes contain more nutrients than fresh varieties since they are frozen at their peak.
- Pay attention to portion sizes, especially at restaurants.
- Smaller portions equal fewer calories.
- Season your food with lemon juice, herbs, and spices, rather than using butter and salt.
- Choose foods that are baked, broiled, braised, grilled, steamed, sautéed, or boiled, rather than fried.
- Preparing and eating more foods at home. Start with simple meals to help you get into the habit, such as Greek yogurt and fresh berries for breakfast, or a whole-grain roasted turkey and avocado wrap with red pepper slices at lunch.
- When eating out, select a dish from the menu, rather than getting your money’s worth at the all-you-can-eat buffet.
In the United States and other developed countries, the average adult can expect to live 80 years or more 5. With such longevity, it isn’t enough merely to consume the calories needed to sustain the body, build it, and repair it. The foods that supply these calories can influence the risk of developing chronic conditions, which range from heart disease and cancer to osteoporosis and age-related vision loss.
Although much remains to be learned about the role of specific nutrients in decreasing the risk of chronic disease, a large body of evidence supports the utility of healthy dietary patterns that emphasize whole-grain foods, legumes, vegetables, and fruits, and that limit refined starches, red meat, full-fat dairy products, and foods and beverages high in added sugars. Such diets have been associated with decreased risk of a variety of chronic diseases 6.
Diet, of course, is just one approach to preventing illness. Limiting caloric intake to maintain a healthy weight, exercising regularly, and not smoking are three other essential strategies. Compelling data from the Nurses’ Health Study show that women who followed a healthy lifestyle pattern that includes these four strategies were 80% less likely to develop cardiovascular disease over a 14-year period compared to all other women in the study 7. A companion study, the Health Professionals Follow-up Study, showed that similar healthy choices were beneficial in men, even among those who were taking medications to lower blood pressure or cholesterol 8.
Strong evidence shows that clean eating patterns are associated with a reduced risk of cardiovascular disease (coronary heart disease). Moderate evidence indicates that healthy eating patterns also are associated with a reduced risk of type 2 diabetes, certain types of cancers (such as colorectal and postmenopausal breast cancers), overweight, and obesity. Emerging evidence also suggests that relationships may exist between eating patterns and some neurocognitive disorders and congenital anomalies. Within this body of evidence, higher intakes of vegetables and fruits consistently have been identified as characteristics of healthy eating patterns; whole grains have been identified as well. Additionally, some evidence indicates that whole grain intake may reduce risk for coronary heart disease and is associated with lower body weight. Other characteristics of healthy eating patterns have been identified include fat-free or low-fat dairy, seafood, legumes, and nuts. Lower intakes of meats, including processed meats; processed poultry; sugar-sweetened foods, particularly beverages; and refined grains have often been identified as characteristics of healthy eating patterns.
Table 1. Elements of clean healthy eating
| Choose healthy fats over unhealthy fats. | Avoid trans fats, which are generally found in commercially baked products and deep-fried restaurant food. Limit intake of saturated fats, mostly from red meat, butter, milk, and other dairy products (under 8% of calories [17 grams*]) Emphasize polyunsaturated fats from olives and olive oil; canola, peanut, and other nut oils; almonds, cashews, peanuts, and other nuts and nut butters; avocados; sesame, pumpkin, and other seeds (10–15% of calories [22–27 grams*]) Emphasize polyunsaturated fats from vegetables oils such as corn, soybean, and safflower oils; walnuts; fatty fish such as salmon, herring, and anchovies (8–10% of calories [17–22 grams*]) |
| Choose slowly digested carbohydrates over highly refined ones. | Limit intake of sources of rapidly digested carbohydrates such as white flour, white rice, pastries, sugary drinks, and French fries. In their place, emphasize whole grains (such as brown rice, barley, bulgur, quinoa, and wheat berries), whole fruits and vegetables, beans, and nuts. Aim for at least 6 servings of whole grains a day. Choosing a whole-grain breakfast cereal and whole grain bread are excellent starts. |
| Pick the best protein packages by emphasizing plant sources of protein rather than animal sources. | Adopting a “flexitarian” approach to protein has long-term health payoffs. Aim for at least half of protein from plants—beans, nuts, seeds, whole grains, fruits, and vegetables. Choose fish, eggs, poultry for most of the rest, with small amounts of red meat and dairy making up the balance. Aim for two servings of fish per week.** |
| Accentuate fruits and vegetables. | Consider 5 servings of fruit and vegetables a daily minimum; 9 a day is even better. Eat for variety and color. Each day try to get at least one serving of a dark green leafy vegetable, a yellow or orange fruit or vegetable, a red fruit or vegetable, and a citrus fruit. Fresh is usually best, especially if it is local; frozen fruits and vegetables are nearly as good. |
| Opt for low-calorie hydration. | Water is the best choice for hydration. Coffee and tea in moderation (with only a small amount of milk or sugar) are generally safe and healthful beverages. If milk is part of the diet, skim or low-fat milk is best. Avoid sugar-laden drinks such as sodas, fruits drinks, and sports drinks. Limit fresh juice to one small glass a day. Alcohol in moderation (no more than one drink a day for women) if at all. |
| Meet the daily recommendations for vitamins and minerals. | Taking an RDA-level multivitamin-multimineral supplement each day that contains folic acid and 1,000 IU of vitamin D provides an inexpensive nutritional safety net. Many premenopausal women need extra iron, and some women need additional calcium. |
| Daily exercise | Calories expended are as important for good health as the quality and quantity of calories consumed. Current recommendations call for 30 minutes of physical activity such as brisk walking on most, if not all, days of the week. |
Footnotes: *for a diet of 2,000 calories a day; ** low-mercury choices are best, especially for women who are pregnant or breastfeeding
[Source 9 ]Table 2. Elements of 2 healthy dietary patterns
| Mediterranean- type diet |
|
| DASH diet* |
|
Footnote: *In the DASH diet, servings listed are based on a diet of 2,000 calories per day.
[Source 9 ]Mediterranean Diet
The Mediterranean Diet is a way of eating rather than a formal diet plan. The Mediterranean Diet features foods eaten in more than 20 countries bordering the Mediterranean Sea including Greece, Spain, southern Italy, Portugal, Morocco, Cyprus, Croatia and France and each has their own unique culture and cuisine. In reality there is no “one” Mediterranean Diet 10, which in 2010 was recognized by UNESCO as an intangible cultural heritage of humanity. The “Mediterranean diet” encompasses all of them—it’s not one size fits all 11. Despite regional variations, common components and cultural aspects can be identified, namely olive oil as the main source of lipids, the consumption of large amounts of seasonal vegetables, fruits and aromatic herbs (some of them gathered from the wild), as well as small intakes of meat and fish, often replaced or complemented with pulses, as sources of protein.
A Mediterranean-style diet typically includes:
- plenty of fruits, vegetables, bread and other grains, potatoes, beans, nuts and seeds are eaten daily and make up the majority of food consumed;
- olive oil as a primary fat source, may account for up to 40% of daily calories; and
- small portions of cheese or yogurt are usually eaten each day, along with a serving of fish, poultry, or eggs.
Fish and poultry are more common than red meat in the Mediterranean diet. The Mediterranean diet also centers on minimally processed, plant-based foods. Wine may be consumed in low to moderate amounts, usually with meals. Fruit is a common dessert instead of sweets.
Main meals consumed daily should be a combination of three elements: cereals, vegetables and fruits, and a small quantity of legumes, beans or other (though not in every meal). Cereals in the form of bread, pasta, rice, couscous or bulgur (cracked wheat) should be consumed as one–two servings per meal, preferably using whole or partly refined grains. Vegetable consumption should amount to two or more servings per day, in raw form for at least one of the two main meals (lunch and dinner). Fruit should be considered as the primary form of dessert, with one–two servings per meal. Consuming a variety of colors of both vegetables and fruit is strongly recommended to help ensure intake of a broad range of micronutrients and phytochemicals. The less these foods are cooked, the higher the retention of vitamins and the lower use of fuel, thus minimizing environmental impact.
The Mediterranean Diet is characterized by 12:
- An abundance of plant food (fruit, vegetables, breads, cereals, potatoes, beans, nuts, and seeds);
- Minimally processed, seasonally fresh, locally grown foods;
- Desserts comprised typically of fresh fruit daily and occasional sweets containing refined sugars or honey;
- Olive oil (high in polyunsaturated fat) as the principal source of fat;
- Daily dairy products (mainly cheese and yogurt) in low to moderate amounts;
- Fish and poultry in low to moderate amounts;
- Up to four eggs weekly;
- Red meat rarely; and
- Wine in low to moderate amounts with meals.
Here are some things you can do to switch from a traditional Western-style diet to a more Mediterranean way of eating.
- Dip bread in a mix of olive oil and fresh herbs instead of using butter.
- Add avocado slices to your sandwich instead of bacon.
- Have fish for lunch or dinner instead of red meat. Brush it with olive oil, and broil or grill it.
- Sprinkle your salad with seeds or nuts instead of cheese.
- Cook with olive or canola oil instead of butter or oils that are high in saturated fat.
- Choose whole-grain bread, pasta, rice, and flour instead of foods made with white flour.
- Add ground flaxseed to cereal, low-fat yogurt, and soups.
- Cut back on meat in meals. Instead of having pasta with meat sauce, try pasta tossed with olive oil and topped with pine nuts and a sprinkle of Parmesan cheese.
- Dip raw vegetables in a vinaigrette dressing or hummus instead of dips made from mayonnaise or sour cream.
- Have a piece of fruit for dessert instead of a piece of cake.
- Use herbs and spices instead of salt to add flavor to foods.
A Mediterranean-style diet can help you achieve the American Heart Association’s recommendations for a healthy dietary pattern that:
- emphasizes vegetables, fruits, whole grains, beans and legumes;
- includes low-fat or fat-free dairy products, fish, poultry, non-tropical vegetable oils and nuts; and
- limits added sugars, sugary beverages, sodium, highly processed foods, refined carbohydrates, saturated fats, and fatty or processed meats.
This style of eating can play a big role in preventing heart disease and stroke and reducing risk factors such as obesity, diabetes, high cholesterol and high blood pressure. There is some evidence that a Mediterranean diet rich in virgin olive oil may help the body remove excess cholesterol from arteries and keep blood vessels open.
The traditional Mediterranean dietary pattern is of particular interest to healthcare providers and dietary scientists, because of observations from the 1960s that populations in countries of the Mediterranean region, such as Greece and Italy, had lower mortality from cardiovascular disease compared with northern European populations or the US, probably as a result of different eating habits.
However, adherence to the Mediterranean diet dietary pattern has been rapidly decreasing in the region since 2000, particularly in Greece, Portugal and Spain – due to the wide dissemination of the fast-food culture. These observations point to a nutrition transition period that encompasses considerable changes in diet and physical activity patterns, which may be leading to an increase in the incidence of chronic and degenerative diseases in the Mediterranean region.
Traditionally characterized by vegetables, legumes, beans, fruits, nuts, seeds, olives, lots of extra virgin olive oil, high-fiber breads and whole grains and fish, this way of eating not only involves a low consumption of processed food, processed carbohydrates, sweets, chocolate and red meat. The recommended foods are rich with monounsaturated fats, fiber, and omega-3 fatty acids.
The Mediterranean Diet is associated with a lower incidence of mortality from all-causes 13 and is also related to lower incidence of cardiovascular diseases 14, type 2 diabetes 15, certain types of cancer 16, and neurodegenerative diseases 17. The Mediterranean diet is now recognized as one of the most healthy food patterns in the world.
Year after year, the Mediterranean diet comes out on top in the U.S. News and World Report annual ranking of best diets. The Mediterranean diet is also touted as one of the healthiest by many health organizations and dietitians 18.
The atmosphere, the state of being and mindset are equally important: people enjoying long, relaxed meals, the warm climate and a sea breeze full of negative ions. This lifestyle also encourages daily exercise — being active. So try to get at least 2½ hours of moderate aerobic activity a week. It’s fine to do blocks of 10 minutes or more throughout your day and week.
Choose exercises that make your heart beat faster and make you breathe harder. For example, go for a swim or a brisk walk or bike ride. You can also get some aerobic activity in your daily routine. Vacuuming, housework, gardening, and yard work can all be aerobic.
The Mediterranean diet is like other heart-healthy diets in that it recommends eating plenty of fruits, vegetables, and high-fiber grains. But in the Mediterranean diet, an average of 35% to 40% of calories can come from fat. Most other heart-healthy guidelines recommend getting less than 35% of your calories from fat. The fats allowed in the Mediterranean diet are mainly from unsaturated oils such as fish oils, olive oil, and certain nut or seed oils (such as canola, soybean, or flaxseed oil) and from nuts (walnuts, hazelnuts, and almonds). These types of oils may have a protective effect on the heart.
Mediterranean Diet Food List
There’s no one “Mediterranean” diet food list because there are more than 20 countries bordering the Mediterranean Sea. Diets vary between these countries and also between regions within a country. Many differences in culture, ethnic background, religion, economy and agricultural production result in different diets. But the common Mediterranean dietary meal plan (source 19) has these characteristics:
- High consumption of fruits, vegetables, bread and other cereals, potatoes, beans, nuts and seeds
- Olive oil is an important monounsaturated fat source
- Dairy products, fish and poultry are consumed in low to moderate amounts, and little red meat is eaten
- Eggs are consumed zero to four times a week
- Wine is consumed in low to moderate amounts
Mediterranean Diet Meal Plan
- Eating a variety of fruits and vegetables each day, such as grapes, blueberries, tomatoes, broccoli, peppers, figs, olives, spinach, eggplant, beans, lentils, and chickpeas.
- Eating a variety of whole-grain foods each day, such as oats, brown rice, and whole wheat bread, pasta, and couscous.
- Choosing healthy (unsaturated) fats, such as nuts, olive oil, and certain nut or seed oils like canola, soybean, and flaxseed. About 35% to 40% of daily calories can come from fat, mainly from unsaturated fats. More than half the fat calories in a Mediterranean diet come from monounsaturated fats (mainly from olive oil). Monounsaturated fat doesn’t raise blood cholesterol levels the way saturated fat does. (source 19).
- Limiting unhealthy (saturated) fats, such as butter, palm oil, and coconut oil. And limit fats found in animal products, such as meat and dairy products made with whole milk.
- Eating mostly vegetarian meals that include whole grains, beans, lentils, and vegetables.
- Eating fish at least 2 times a week, such as tuna, salmon, mackerel, lake trout, herring, or sardines.
- Eating moderate amounts of low-fat dairy products each day or weekly, such as milk, cheese, or yogurt.
- Eating moderate amounts of poultry and eggs every 2 days or weekly.
- Limiting red meat to only a few times a month in very small amounts. For example, a serving of meat is 3 ounces. This is about the size of a deck of cards.
- Limiting sweets and desserts to only a few times a week. This includes sugar-sweetened drinks like soda.
DASH Diet
DASH stands for Dietary Approaches to Stop Hypertension is similar to a Mediterranean-type diet 20. It is an eating plan that is based on research studies sponsored by the National Heart, Lung, and Blood Institute 21. The DASH diet eating plan includes vegetables, whole grains, poultry, fish, and nuts, and has low amounts of fats, red meats, sweets, and sugared beverages. It is also high in potassium, calcium and magnesium, as well as protein and fiber. This dietary approach has been shown to lower blood pressure, but little has been published regarding weight loss 20. In fact, a systematic review and meta-analysis on observational prospective studies on the effects of Dietary Approaches to Stop Hypertension (DASH)-style diet, showed that the DASH diet can significantly protect against cardiovascular diseases, coronary heart disease, stroke, and heart failure risk by 20%, 21%, 19% and 29%, respectively 22, 23.
The DASH diet is a lifelong approach to healthy eating that’s designed to help treat or prevent high blood pressure (hypertension). The DASH diet encourages you to reduce the sodium in your diet and eat a variety of foods rich in nutrients that help lower blood pressure, such as potassium, calcium and magnesium and eating foods that are low in saturated fat, total fat, and cholesterol, and high in fruits, vegetables, and low fat dairy foods 24.
The DASH Diet
- Emphasizes vegetables, fruits, and fat-free or low-fat dairy products.
- Includes whole grains, fish, poultry, beans, seeds, nuts, and vegetable oils.
- Limits sodium, sweets, sugary beverages, and red meats. The American Heart Association recommends 1,500 mg a day of sodium as an upper limit for all adults.
One teaspoon of table salt has 2,325 mg of sodium. When you read food labels, you may be surprised at just how much sodium some processed foods contain. Even low-fat soups, canned vegetables, ready-to-eat cereals and sliced turkey from the local deli — foods you may have considered healthy — often have lots of sodium
Along with DASH, other lifestyle changes can help lower your blood pressure. They include staying at a healthy weight, exercising, and not smoking.
Blood pressure is usually measured in millimeters of mercury (mmHg) and is recorded as two numbers—systolic pressure (as the heart beats) “over” diastolic pressure (as the heart relaxes between beats)—for example, 120/80 mmHg. Both numbers in a blood pressure test are important, but for people who are age 50
or older, systolic pressure gives the most accurate diagnosis of high blood pressure. Systolic pressure is the top number in a blood pressure reading. It is high if it is 140 mmHg or above 25.
High blood pressure is blood pressure higher than 140/90 mmHg and prehypertension is blood pressure between 120/80 and 139/89 mmHg. Prehypertension means that you don’t have high blood pressure now, but are likely to develop it in the future unless you adopt the healthy lifestyle. High blood pressure is dangerous because it makes your heart work too hard, hardens the walls of your arteries, and can cause the brain to hemorrhage or the kidneys to function poorly or not at all. If not controlled, high blood pressure can lead to heart and kidney disease, stroke and blindness.
Being overweight or obese increases your risk of developing high blood pressure. In fact, your blood pressure rises as your body weight increases. Losing even 10 pounds can lower your blood pressure and losing weight has the biggest effect on those who are overweight and already have hypertension. Overweight and obesity are also risk factors for heart disease. And being overweight or obese increases your chances of developing high blood cholesterol and diabetes—two
more risk factors for heart disease.
The original DASH trial 26 consisted of 459 subjects with systolic blood pressures <160 mm Hg and diastolic blood pressures between 80 and 95 mm Hg. For three weeks, all participants were fed a control diet low in fruits, vegetables, and dairy products, and with a fat content typical of an American diet (37% of daily caloric intake). During the following eight weeks, the participants were randomized to one of three diets: the control diet, a diet rich in fruits and vegetables, or the DASH Diet.
The DASH Diet was not low in sodium (salt), but still reduced blood pressure. A meta-analysis of 56 randomized, controlled trials that included over 3,500 participants did not support universal sodium restriction, but instead only recommended dietary sodium restriction in the elderly 27.
The DASH Diet reduced systolic blood pressure by 5.5 mm Hg and diastolic blood pressure by 3.3 mm Hg, as compared with controls. Subgroup analysis showed that African Americans and those with hypertension had the greatest reduction in blood pressure 26 . The DASH diet results might be applied to a larger group due to the heterogeneous population: half of the participants were women, 60% were African American, and 37% had household incomes of <$30,000 per year. One limitation of applying the DASH Diet to the general population is that the study was carried out in a very controlled setting, where all the meals were prepared for the subjects, and thus no comments may be made regarding attrition rates for the diet.
By following the DASH diet, you may be able to reduce your blood pressure by a few points in just two weeks. Over time, your systolic blood pressure could drop by eight to 14 points, which can make a significant difference in your health risks.
Table 3. Daily Nutrient Goals Used in the DASH Studies (for a 2,100 Calorie Eating Plan)
| Total fat: 27% of calories | Sodium: 2,300 mg* |
| Saturated fat: 6% of calories | Potassium: 4,700 mg |
| Protein: 18% of calories | Calcium: 1,250 mg |
| Carbohydrate: 55% of calories | Magnesium: 500 mg |
| Cholesterol: 150 mg | Fiber: 30 g |
Footnote: 1,500 mg sodium* was a lower goal tested and found to be even better for lowering blood pressure. It was particularly effective for middle-aged and older individuals, African Americans, and those who already had high blood pressure.
Abbreviations: g = grams; mg = milligrams
[Source 28 ]Table 4. Tips for Lowering Salt (Sodium) When Shopping, Cooking, and Eating Out
| Shopping | Cooking | Eating Out |
|---|---|---|
|
|
|
Footnote: *Examples of convenience foods are frozen dinners, prepackaged foods, and soups; examples of condiments are mustard, ketchup, soy sauce, barbecue sauce, and salad dressings.
Most Americans should consume no more than 2.4 grams (2,400 milligrams) of salt (sodium) a day. That equals 6 grams (about 1 teaspoon) of table salt a day. The 6 grams includes all salt and sodium consumed, including that used in cooking and at the table. African Americans and the elderly, are especially sensitive to salt and sodium and should be particularly careful about how much they consume.
Most of the salt (sodium) Americans eat comes from processed and prepared foods, such as breads, cold cuts, pizza, poultry, soups, sandwiches and burgers, cheese, pasta and meat dishes, and salty snacks. Therefore, healthier choices when shopping and eating out are particularly important.
Another DASH diet called DASH-Sodium — calls for cutting back sodium (salt) to 1,500 milligrams a day (about 2/3 teaspoon). Studies of people on the DASH-Sodium plan lowered their blood pressure as well.
To further investigate the effects of sodium restriction, the DASH-Sodium Trial 29 looked at the effect on blood pressure of a reduced dietary sodium intake as participants followed either the DASH eating plan or an eating plan typical of what many Americans consume. This second study involved 412 participants. Participants were randomly assigned to one of the two eating plans and then followed for a month at each of the three sodium levels. The three sodium levels were a higher intake of about 3,300 milligrams per day (the level consumed by many Americans), an intermediate intake of about 2,300 milligrams per day, and a lower intake of about 1,200 milligrams per day. Results showed that reducing dietary sodium lowered blood pressure for both eating plans. At each sodium level, blood pressure was lower on the DASH eating plan than on the other eating plan. Additionally, there was no significant difference between high (3,300 milligrams per day) and intermediate sodium (2,300 milligrams per day) intake on diastolic blood pressure for those on the DASH Diet. The greatest blood pressure reductions were for the DASH eating plan at the sodium intake of 1,200 milligrams per day. Those with high blood pressure saw the greatest reductions, but those with prehypertension also had large decreases 29. The DASH Diet can reduce systolic blood pressure by 5.5 mm Hg and diastolic blood pressure by 3.3 mm Hg. However, the effect of sodium reduction on hypertension remains controversial. Lowering sodium to the levels of 1.2 g/day, as achieved in the lowest sodium intake group of the DASH-Sodium Trial, would be nearly impossible without changes in the food industry, as 75% of sodium intake comes from additions made in processing 30.
Detailed analysis showed that the DASH diet and reduced sodium intake reduced blood pressure for all the population subgroups studied. The following list shows the average blood pressure reduction for key subgroups:
- For those with hypertension: 12/6 mm Hg (systolic/diastolic); for those without hypertension, 7/4 mm Hg.
- For those over age 45, 12/6 mm Hg; for those 45 or younger, 6/3 mm Hg.
- For women, 11/5 mm Hg; for men, 7/4 mm Hg.
- For African Americans, 10/5 mm Hg; for non-African Americans, 8/4 mm Hg.
Other results include:
- Compared with the typical American diet, the DASH diet alone (at the higher sodium level) reduced blood pressure by about 6/3 mm Hg for African Americans, and 6/2 mm Hg for other races.
- For those with hypertension, reductions from the DASH diet alone were 7/3 mm Hg; and for those without hypertension, the reductions were 5/3 mm Hg. The effects of sodium reduction appeared in all subgroups and were greater for those who ate the typical American diet, compared with those on the DASH diet.
- The effects from sodium reduction were particularly great for those with hypertension, African Americans, women, and those over age 45. Sodium reduction in those eating the control diet resulted in lower systolic and diastolic pressures by 8.3 mm Hg and 4.4 mm Hg, respectively, in hypertensives, and 5.4 and 2.8 mm Hg, respectively, in non-hypertensives.
“The blood pressure reductions achieved from this combination came in only 4 weeks and persisted through the duration of the study”, said Dr. Denise Simons-Morton, Leader of the NHLBI Prevention Scientific Research Group and a DASH coauthor 31.
Both versions of the DASH diet include lots of whole grains, fruits, vegetables and low-fat dairy products. The DASH diet also includes some fish, poultry and legumes, and encourages a small amount of nuts and seeds a few times a week.
The DASH diet generally includes about 2,000 calories a day. If you’re trying to lose weight, you may need to eat fewer calories. You may also need to adjust your serving goals based on your individual circumstances — something your health care team can help you decide.
Studies showed that DASH lowers high blood pressure and improves levels of cholesterol. This reduces your risk of getting heart disease.
Because the DASH diet is a healthy way of eating, it offers health benefits besides just lowering blood pressure. The DASH diet is also in line with dietary recommendations to prevent osteoporosis, cancer, heart disease, stroke and diabetes.
While the DASH diet is not a weight-loss program, you may indeed lose unwanted pounds because it can help guide you toward healthier food choices. A recent study showed that people can lose weight while following the DASH eating plan and lowering their sodium intake. In a randomized trial of 810 participants called the PREMIER Study 32, 33, who were placed into three groups to lower blood pressure, lose weight, and improve health. The groups included:
- Advice-only group received a 30-minute individual session with a nutritionist, which did not include counseling on how to make behavior changes.
- Established treatment plan, including counseling for 6 months to keep track of their diet, including calorie and sodium consumption, and their physical activity.
- Established treatment plan, plus counseling and use of the DASH diet.
After 6 months, blood pressure levels declined in all three groups. The two groups that received counseling and followed a treatment plan had more weight loss than the advice-only group. However, participants in the established treatment plan who followed the DASH diet had the greatest improvement in their blood pressure 32, 33.
By paying close attention to food labels when you shop, you can consume less sodium. Sodium is found naturally in many foods. But processed foods account for most of the salt and sodium that Americans consume. Processed foods that are high in salt include regular canned vegetables and soups, frozen dinners, lunch meats, instant and ready-to-eat cereals, and salty chips and other snacks.
Dash Diet Guidelines
DASH Diet is a flexible and balanced eating plan that helps you create a heart-healthy eating style for life.
The DASH diet eating plan requires no special foods and has no hard-to-follow recipes. It simply calls for a certain number of daily servings from various food groups to provide your daily and weekly nutritional goals. This plan recommends:
- Eating vegetables, fruits, and whole grains
- Including fat-free or low-fat dairy products, fish, poultry, beans, nuts, and vegetable oils
- Increase potassium intake
- Limiting foods that are high in saturated fat, such as fatty meats, full-fat dairy products, and tropical oils such as coconut, palm kernel and palm oils
- Limiting sugar-sweetened beverages and sweets.
The number of servings depends on the number of calories you’re allowed each day. Your calorie level depends on your age, sex, the amount of lean body mass (muscular, athletic, average or overweight), height and, especially, how active you are. Think of this as an energy balance system—if you want to maintain your current weight, you should take in only as many calories as you burn by being physically active. If you need to lose weight, eat fewer calories than you burn or increase your activity level to burn more calories than you eat.
What Foods To Eat
- Fruits
- Vegetables
- Whole-grains
- Low-fat dairy products
- Skinless poultry and fish
- Nuts and legumes
- Non-tropical vegetable oils
What Foods to Reduce or Avoid
- Saturated and trans fats
- Sodium (salt)
- Red meat (if you do eat red meat, compare labels and select the leanest cuts available)
- Sweets and sugar-sweetened beverages
- Alcohol and caffeine
- Processed foods, which are often high in fat, salt, and sugar
Drinking too much alcohol can increase blood pressure. It also can harm the liver, brain, and heart. Alcoholic drinks also contain calories, which matters if you are trying to lose weight. The Dietary Guidelines for Americans recommends that men limit alcohol to no more than two drinks a day and women to one or less.
The DASH diet doesn’t address caffeine consumption. The influence of caffeine on blood pressure remains unclear. But caffeine can cause your blood pressure to rise at least temporarily. If you already have high blood pressure or if you think caffeine is affecting your blood pressure, talk to your doctor about your caffeine consumption.
Dash Diet Eating Plan
To benefit from the DASH diet eating plan, it is important to consume the appropriate amount of calories to maintain a healthy weight. The DASH diet eating plan can be used to help you lose weight. To lose weight, follow the DASH eating plan and try to reduce your total daily calories gradually. Find out your daily calorie needs or goals with the Body Weight Planner and calorie chart. Talk with your doctor before beginning any diet or eating plan.
General tips for reducing daily calories include:
- Eat smaller portions more frequently throughout the day.
- Reduce the amount of meat that you eat while increasing the amount of fruits, vegetables, whole grains, or dry beans.
- Substitute low-calorie foods, such as when snacking (choose fruits or vegetables instead of sweets and desserts) or drinking (choose water instead of soda or juice), when possible.
Tips for Following DASH Diet
It’s easy to follow the DASH diet. But it might mean making some changes to how you currently eat. To get started:
- DO NOT try to make changes all at once. It’s fine to change your eating habits gradually.
- To add vegetables to your diet, try having a salad at lunch. Or, add cucumber, lettuce, shredded carrots, or tomatoes to your sandwiches.
- There should always been something green on your plate. It’s fine to use frozen vegetables instead of fresh. Just make sure the package does not contain added salt or fat.
- Add sliced fruit to your cereal or oatmeal for breakfast.
- For dessert, choose fresh fruit or low-fat frozen yogurt instead of high-calorie sweets, such as cakes or pies.
- Choose healthy snacks, such as unsalted rice cakes or popcorn, raw vegetables, or yogurt. Dried fruits, seeds, and nuts also make great snack choices. Just keep these portions small.
- Choose whole grain foods for most grain servings to get added nutrients, such as minerals and fiber. For example, choose whole wheat bread or whole grain cereals.
- Think of meat as part of your meal, instead of the main course. Limit your servings of lean meat to 6 ounces (170 grams) a day. You can have two 3-ounce (85 grams) servings during the day. If you now eat large portions of meats, cut them back gradually by a half or a third at each meal.
- Try these snacks ideas: unsalted rice cakes; nuts mixed with raisins; graham crackers; fat-free and low-fat yogurt and frozen yogurt; popcorn with no salt or butter added; raw vegetables.
- Try cooking without meat at least twice each week. Instead, eat beans, nuts, tofu, or eggs for your protein.
- If you are allergic to nuts, use seeds or legumes (cooked dried beans or peas).
Health Benefits of DASH Diet
- Following the DASH diet will provide all the nutrients you need.
- It is safe for both adults and children.
- The diet is flexible enough to follow if you are vegetarian, vegan, or gluten-free.
- It is low in fat and high in fiber, an eating style that is recommended for everyone.
The DASH diet sets the standard for a healthy diet. It has been widely studied and has many health benefits. Following this diet plan may help:
- Lower high blood pressure 34
- Reduce the risk for heart disease, heart failure, and stroke 22, 23
- Help prevent or control type 2 diabetes 35
- Improve cholesterol levels
- Reduce the chance of kidney stones.
Can the DASH diet promote Weight Loss?
The DASH eating plan was not designed to promote weight loss. But it is rich in low-calorie foods such as fruits and vegetables. Therefore, the DASH diet eating plan can be used to help you lose weight. To lose weight, follow the DASH diet eating plan and try to reduce your total daily calories gradually. To lose weight you’ll need to start with finding a way to eat fewer calories than you need. A calorie is a unit of energy, which is in the foods and drinks you consume. Scientifically, the calorie (a unit of energy) was originally defined as the amount of heat required at a pressure of 1 standard atmosphere to raise the temperature of 1 gram of water 1° Celsius. When you hear something contains 100 calories, it’s a way of describing how much energy your body could get from eating or drinking it. However, since calories are too small of a measurement to use when discussing nutrition and exercise, kilocalorie (kcal) measurements are used instead and the term is interchangeable with calories. Kilocalorie (kcal) is a unit of measurement for energy that is equivalent to 1,000 calories. Also,1 kcal or 1 kilocalorie is equivalent to 1 large Calorie (with an uppercase C) or 1,000 calories.
Some countries use kilojoules (kJ) to measure how much energy people get from consuming a food or drink.
- 1 calorie = 4.184 joule
- 1 kilocalorie (kcal) = 4.184 kilojoules (kJ)
- 1 Calorie (1,000 calories) = 4.184 kilojoules (kJ)
Here’s how many calories are in your foods and drinks 36:
- 1 gram of carbohydrate = 4 calories
- 1 gram of protein = 4 calories
- 1 gram of fat = 9 calories
- 1 gram of water = 0 calorie
Most foods and drinks contain calories. You can find out how many calories are in a food by looking at the nutrition facts label. The label also will describe the components of the food such as how many grams of carbohydrate, protein, and fat it contains.
That means if you know how many grams of each one are in a food, you can calculate the total calories. You would multiply the number of grams by the number of calories in a gram of that food component. For example, if a serving of potato chips (about 20 chips) has 10 grams of fat, 90 calories are from fat. That’s 10 grams x 9 calories per gram. Some foods, such as lettuce, contain few calories (1 cup of shredded lettuce has less than 10 calories). Other foods, like peanuts, contain a lot of calories (½ cup of peanuts has 427 calories).
There are many unhealthy misconceptions about weight loss. There are no magical foods or ways to combine foods that melt away excess body fat. To reduce your weight, you’ll have to reduce your calorie intake.
Calories aren’t bad for you. Your body needs calories for energy. Your body uses energy (calorie) for everything you do from breathing and sleeping to exercising. Some people mistakenly believe they have to burn off all the calories they eat or they will gain weight. This isn’t true. Your body needs some calories just to operate — to keep your heart beating and your lungs breathing. When you eat, you’re replacing the energy (calorie) you’ve used, which helps you to maintain a healthy weight. But eating more calories than your body needs and not burning enough of them off through activity can lead to weight gain and other health problems such as type 2 diabetes, heart disease, high blood pressure, certain cancers (e.g., uterine, gallbladder, kidney, liver, and colon cancers) and death 37, 38, 39, 40.
Being overweight or obese is the result of an energy imbalance between your daily energy intake and your energy expenditure resulting in excessive weight gain 41. The amount of energy or calories you get from food and drinks (energy IN) is balanced with the energy your body uses for things like breathing, digesting, and being physically active (energy OUT):
- The same amount of energy IN and energy OUT over time = weight stays the same (Energy Balance)
- More energy IN than OUT over time = Weight Gain
- More energy OUT than IN over time = Weight Loss
In order to lose weight, energy expenditures must exceed energy intake. To lose weight, most people need to reduce the number of calories they get from food and beverages (energy IN) and increase their physical activity (energy OUT). To achieve this imbalance, you can decrease energy intake, increase energy expenditures or combine a decrease in intake with an increase in expenditures. Being physically active and eating fewer calories will help you lose weight and keep the weight off over time. As a result, most weight loss recommendations advise combining a low caloric diet with an exercise program in order to achieve a significant energy deficit 42. A long-standing consistent observation is that regular exercise by itself is prescribed in small to moderate amounts resulting in modest weight loss or in some cases weight gain 43.
Weight loss of about 1 to 1 ½ pounds per week is considered reasonable and more likely to be maintained. For a weight loss of 1 to 1 ½ pounds per week, daily intake should be reduced by 500 to 750 calories. In general 44:
- Eating plans that contain 1,200–1,500 calories each day will help most women lose weight safely.
- Eating plans that contain 1,500–1,800 calories each day are suitable for men and for women who weigh more or who exercise regularly.
Very low calorie diets of fewer than 800 calories per day should not be used unless you are being monitored by your doctor. Because dieting can be harmful because your body responds to these periods of semi-starvation by lowering its metabolic rate. When you lose weight too quickly, you lose fat and muscle. Muscle burns kilojoules, but fat doesn’t. So, when you stop dieting and return to your usual habits, your body will burn even fewer calories than before because the relative amount of muscle in your body has decreased and your metabolic rate is slower. This kind of eating pattern can also affect your general health – just one cycle of weight loss and weight gain can contribute to an increased risk of coronary heart disease (regardless of your body fat levels). That’s why it’s more important to be able to maintain weight loss.
Energy balance is also important for maintaining a healthy weight. To maintain a healthy weight, your energy IN and OUT don’t have to balance exactly every day. It’s the balance over time that helps you maintain a healthy weight.
You can reach and maintain a healthy weight if you:
- Follow a healthy diet, and if you are overweight or obese, reduce your daily intake by 500 calories for weight loss
- Are physically active
- Limit the time you spend being physically inactive
While people vary quite a bit in the amount of physical activity (exercise) they need for weight control, many can maintain their weight by doing 150 to 300 minutes (2 ½ to 5 hours) a week of moderate-intensity activity such as brisk walking. People who want to lose a large amount of weight (more than 5 percent of their body weight) and people who want to keep off the weight that they’ve lost may need to be physically active for more than 300 minutes of moderate-intensity activity each week.
You now know the basics about calories – the key to weight loss for most people is simply finding the right combination of exercise, healthy foods and cutting back on portions will help you lose those extra pounds. No fad diet required. In other words, eat healthily, watch your portions and get moving more. By losing just a few pounds with healthy eating and exercise, you’ll start to feel better. You’ll have more energy. To prevent the weight creeping back on, you need to keep going with the healthy habits you’ve formed.
Adults BMI calculator
Children and teens BMI calculator
Figure 1. Body Mass Index calculator
Table 5. Body Mass Index range
| BMI Range (kg/m²) | Weight class |
| Less than 16.5 kg/m² | Severely Underweight |
| 16.5 – 18.5 kg/m² | Underweight |
| 18.5 – 25 kg/m² | Normal |
| 25 – 30 kg/m² | Overweight |
| 30 – 34.9 kg/m² | Obese, Class 1 |
| 35 – 39.9 kg/m² | Obese, Class 2 |
| More than 40 kg/m² | Obese, Class 3 (Morbidly Obese) |
Figure 2. Body Mass Index chart
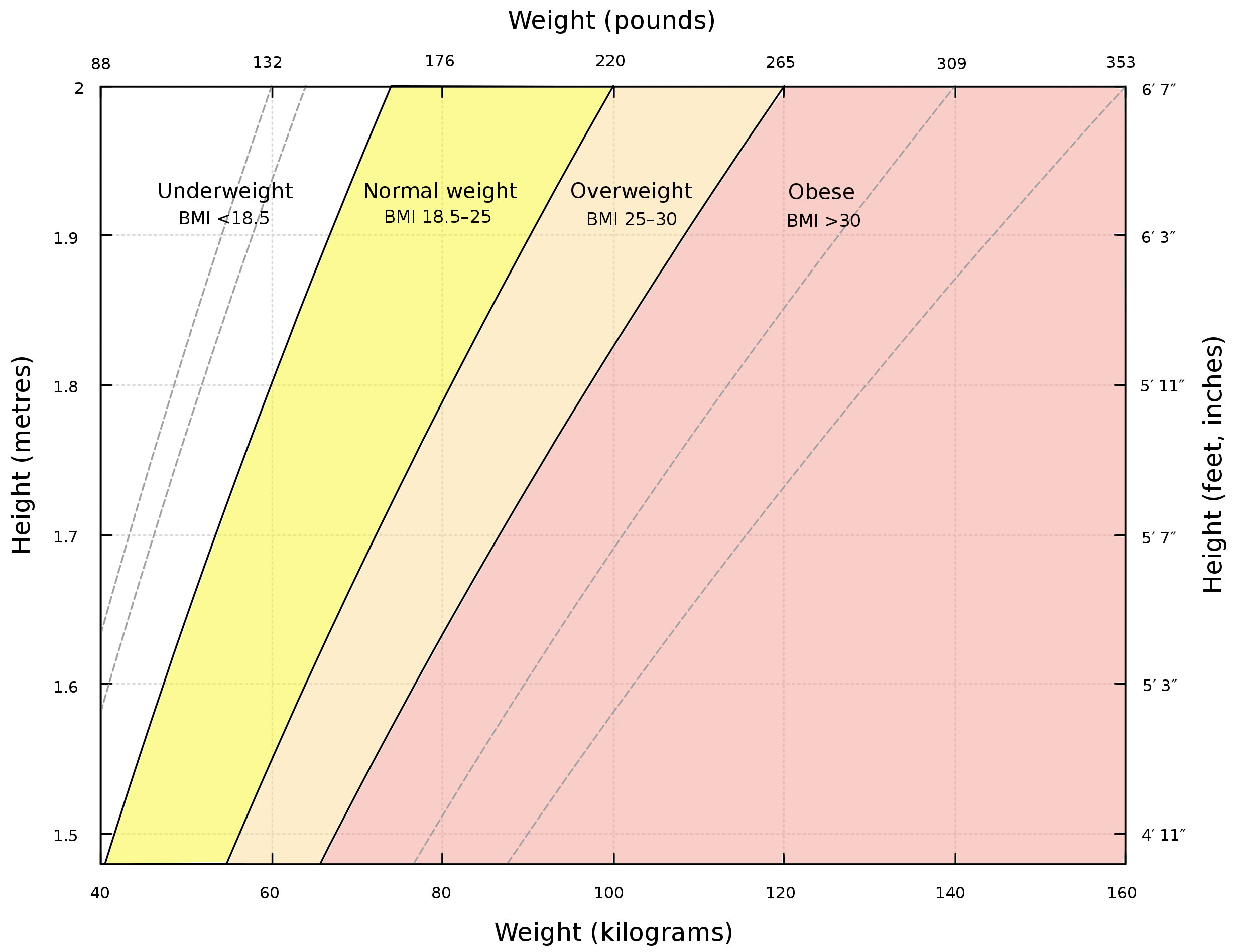
Footnote: A graph of body mass index (BMI) as a function of body mass and body height. The dashed lines represent subdivisions within a major class. The Body mass index scale show all people with high level of muscles also overweight or obese. This is because the BMI scale is designed in accordance to the body fat levels not body muscles mass levels. Therefore, BMI measure is not an accurate measure for muscular individual.
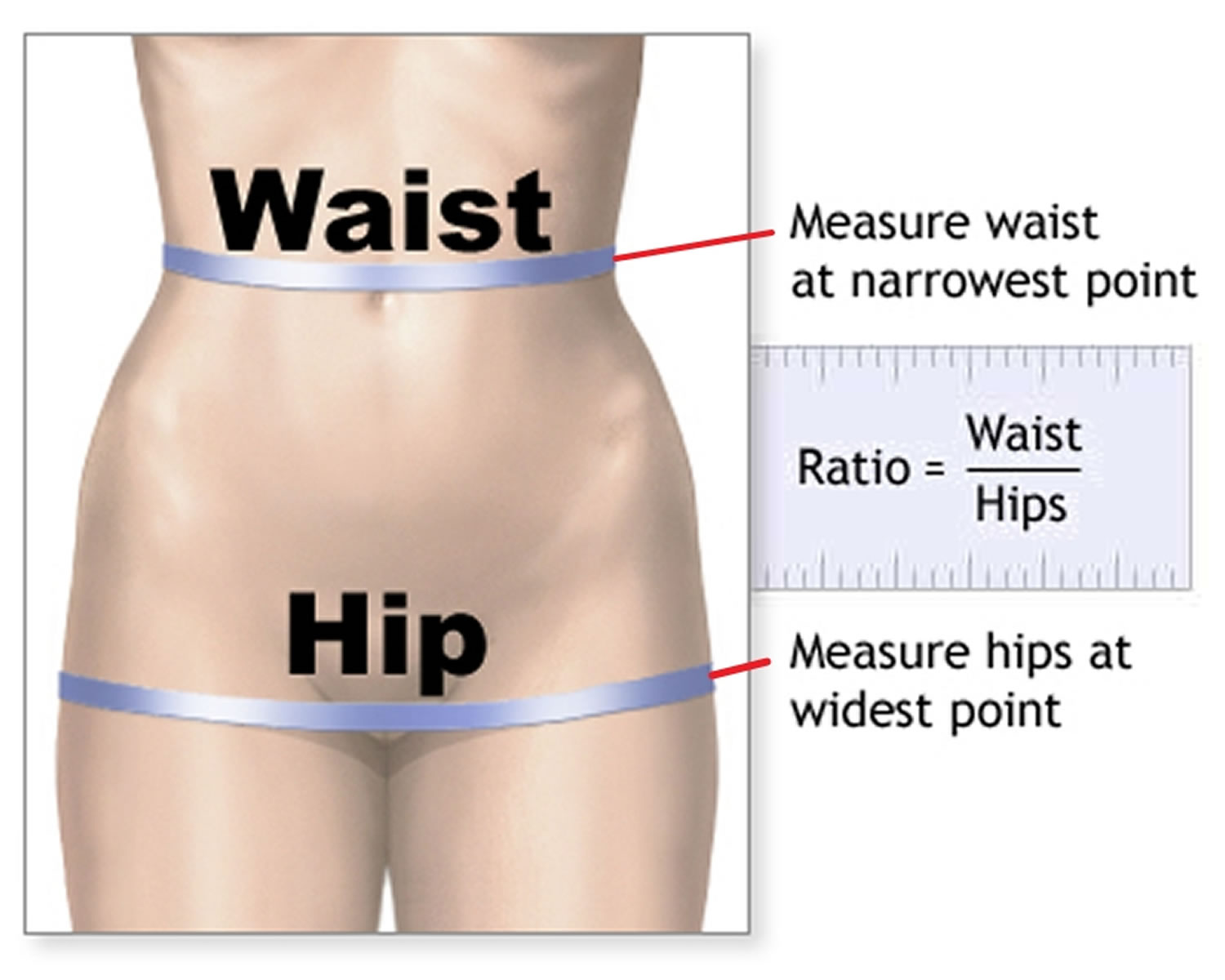
Figure 3. Waist to hip ratio
How to lose belly fat
An active lifestyle and exercise routine, along with eating healthy foods, is the best way to lose weight and lose belly fat. Losing belly fat is not easy like taking a pill for a headache. Getting rid of your belly fat require you to change your beliefs, habits and lifestyle with a lot of sweat and self discipline. It’s a lifelong habit and lifestyle you need to maintain for the rest of your life! Managing your weight is a life-long commitment – not just following a diet for a few weeks to drop pounds. That’s because losing weight isn’t necessarily the problem, it’s keeping it off longer term that is difficult. Popular media is full of fad diets and magic weight loss potions endorsed by celebrities and supported by personal success stories. While many of these diets may help you to lose weight while you’re following them, as soon as you resume your usual lifestyle, the weight starts to creep back on. Remember, if the strategies you’re putting into place to lose weight are not strategies that you’ll be able to follow for the rest of your life, chances are you’ll regain any weight you lose.
There is no single diet that works for everyone. To lose weight you’ll need to start with finding a way to eat fewer calories than you need. This phase is referred to as the “energy deficit” or “hypo-caloric phase” of weight loss. The essential components of weight loss, regardless of type of diet, are decreased energy intake, increased energy output through physical activity, behavioral modification and alterations in the environment that foster all of these 3 components 39.
Most American adults are overweight or obese. What is your current weight? Are you overweight or morbidly obese? Because there’s a huge difference between someone who’s 500 pounds then someone who’s 200 pounds who’s trying to lose belly fat. For someone who’s extremely obese to lose 300 pounds is a lot harder that for someone who’s overweight trying to lose 50 pounds. For example, a 5’4’’ woman weighing 250 pounds with a body mass index (BMI) of 43 kg/m² losing 5% of her body weight, or 12.5 pounds, will have an ending BMI of 41 kg/m². This amount of weight loss could take up to 25 weeks, if she loses one-half a pound per week. Weight loss of one-half a pound to two pounds per week is reasonable and offers the best chance for long-term success, but for extremely heavy people, this may take many months or years. If further weight reduction is necessary after 10% of initial body weight is lost, it can be attempted with an increased calorie deficit after prior weight loss has been maintained for several months. In contrast, obese people often expect to lose 25% to 35% of their initial weight over the first year of obesity treatment. Dieters often maintain these expectations even when they are repeatedly informed that their goals are likely unrealistic even with weight-loss drug treatment 45. It is important to note that one-half to one pound per week of fat loss is a realistic, achievable goal that will improve your health. Additionally, it is difficult to continue to lose weight at such a rapid pace. Because in the beginning (the first several days) of weight-loss from low-calorie diet is due to water loss. This is especially true for those on severely low-caloric diets (with deficits of 1,000 calories per day), those on ketogenic diets, and those on very low carbohydrate diets 46, 47. Ketogenic diets or keto diets consist of 60-80% of calorie intake from fats and limiting carbohydrate consumption to less than 10% of daily intake. While keto diets have been shown to aid in weight loss/fat loss, studies have shown the primary mechanism behind weight loss is due to hunger suppression. A high-fat diet can suppress appetite since it is highly satiating, leading to decreased caloric consumption. Additionally, many studies have shown that calorically matched diets with identical protein levels aid in fat loss just as successfully as a keto diet.
Doctors and dietitians assess weight by measuring your Body Mass Index (BMI), a ratio of weight to height. The BMI is defined as the body mass in kilogram (Kg) that is divided by the square of the body height in meter (m2), and is expressed in units of kg/m², resulting from mass in kilograms and height in meters (see Figure 1). You can also use an online BMI calculator (https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm). A BMI between 25 and 29.9 kg/m² is considered overweight, and obesity is a BMI of 30 kg/m² or higher. Waist to hip ratio should also be measured, in men more than 1:1 and women more than 0:8 is considered significant (see Figure 3). Being overweight or obese puts you at risk for a myriad of health problems, such as ischemic heart disease, high blood pressure, cardiovascular disease, fatty liver disease, breathing problems (obstructive sleep apnea, ventilatory failure and asthma), type 2 diabetes, gastro-esophageal reflux disease (GERD), gallstones, some cancers, Alzheimer’s disease, renal failure and other health problems 48. Ninety per cent of people with type 2 diabetes have a body mass index (BMI) greater than 23 kg/m² and conversely it is estimated that the attributable risk of obesity for diabetes is between 30% and 70% 49.
Many factors can contribute to your weight. These factors include your environment (cultural and societal), family history and genetics, metabolism (the way your body changes food and oxygen into energy), and behavior or habits. Other causes of obesity include reduced physical activity, insomnia, food habits, endocrine disorders, medications, food advertisements, and energy metabolism 50. Most common syndromes associated with obesity include Prader Willi syndrome and MC4R syndromes, others like fragile X, Bardet-Beidl syndrome, Wilson Turner congenital leptin deficiency, and Alstrom syndrome are also associated with obesity 50.
Furthermore, your current health will also affect your ability to do physical activity and do weights to build lean muscle mass. For example, do you have any medical conditions that could hinder you lifting weights and doing aerobic cardio workouts? Because if you have existing medical conditions you may not be able to do the hard workouts in the gym in order to build the muscle mass you wanted.
Another thing to consider is your ‘WHY’. Why are you wanting to build muscle and have six pack abs? Is it for you and you have decided to change your life to live a healthier life? Or are you trying to impress other people? Do you want to ‘look healthy’ or do want to be healthy? Because if you’re doing it for yourself, your chances of reaching your goal is easier than if you’re trying to impress others with your beauty (aesthetic) and your appearance (cosmetic). Your primary reason (your WHY) is to lose enough weight to improve or maintain your health. The aesthetic and cosmetic effects of weight loss are “extra benefits” or ‘icing on the cake’.
Lastly, how serious and motivated are you in wanting your dream outcome like building muscle and losing your belly fat to have six pack abs? Most people are not serious and not motivated to do the work like dieting, eating healthy, exercising and lifting heavy weights. Most people just want a quick solutions like popping weight loss pills, taking supplements and following fad diets (popular celebrity endorsed short term diets that sound too good to be true that can cause nutrient deficiencies, fatigue, weight regain and disordered eating) hoping these quick fix ineffective, unhealthy and dangerous products will give them their dream results. Furthermore, most people want six pack abs to impress others and have the false impression that having big muscles and six pack abs will solve their self esteem and confidence issues. In reality, to become successful and achieve your dream outcome, you’ll need to first change your mindset, your beliefs and become self-aware that anything in life requires sacrifice, time, hard work, effort, being resilient, self-confidence, high self-esteem, healthy diet and dedication.
To achieve your dream outcome like building muscle and losing your belly fat to have six pack abs you’ll have to embrace challenges, views failures as opportunities for growth, and believe in your ability to achieve your dream. It involves setting clear goals (e..g, how much weight you have to lose, how many calories you have to remove from your diet), maintaining a positive outlook, and persisting through obstacles with resilience and determination.
How many calories do I need per day?
The total number of calories you need each day varies depends on a number of factors, namely your age, sex, height, weight, level of physical activity, and pregnancy or lactation status. According to the Dietary Guidelines for Americans, American female adult estimated calorie needs range from 1,600 to 2,400 calories per day and for males 2,000 to 3,000 calories per day 51. The average, healthy, adult, American male consumes approximately 2,800 calories per day, and the average female about 1,800 calories 39. But most people need different amounts of calories based on how their bodies work, how active they are and any weight management goals. And if you want to lose weight you’ll have to reduce your calorie intake.
Here is a general estimate of calories you need each day:
- Sedentary lifestyle (little to no exercise)
- Women: 1,800 to 2,400 calories
- Men: 2,200 to 3,000 calories
- Moderately active lifestyle (engages in moderate exercise/physical activity like walking or light yard work:
- Women: 2,000 to 2,600 calories
- Men: 2,400 to 2,800 calories
- Very active lifestyle (engages in hard exercise/physical activity, or has a physically demanding job):
- Women: 2,200 to 2,800 calories
- Men: 2,800 to 3,200 calories
These are just general guidelines. It’s essential to consult with a nutritionist or a doctor who can give personalized advice based on your specific situation. Remember, it’s not just the quantity but also the quality of calories that matters for overall health.
Obesity results from the accumulation of excessive body fat, which is stored as adipose tissue. An energy deficit of approximately 3,500 calories is required to lose one pound of fat. However, there are several factors that can influence this particular number. These include compensatory changes in your resting metabolism (basal metabolic rate [BMR]), the energy cost of work, and discretionary physical activity, which can sometimes alter this figure by 100 to 200 calories. Your basal metabolic rate (BMR) also known as resting metabolic rate (RMR) is the number of calories your body burns while performing basic life-sustaining functions, such as breathing and keeping your heart beating. Your basal metabolic rate (BMR) is typically between 1,000 and 2,000 calories per day.
How to calculate calories you need for weight loss
You can calculate your basal metabolic rate (BMR) or resting metabolic rate (RMR) using the Mifflin-St Jeor equation 52, which is considered more accurate than the Harris-Benedict equation, especially for lean people. According to the Academy of Nutrition and Dietetics Evidence Analysis Library (EAL), the Mifflin-St. Jeor equation accurately predicted resting metabolic rate (RMR) using actual body weight within +/- 10% of measured RMR in 70% of obese individuals 53. Of the remaining 30%, 9% were overestimations and 21% were underestimations. The individual error range was a maximum overestimate of 15% to a maximum underestimate of 20%” 54. While the Harris-Benedict and WHO equations are often used in clinical practice with reasonable accuracy, results have been mixed regarding their applications to individuals who are overweight or obese 39.
The Mifflin-St Jeor formula for calculating your basal metabolic rate (BMR) or resting metabolic rate (RMR):
- Males Basal metabolic rate [BMR] (kcal/day) = (10 X weight in kilograms) + (6.25 X height in centimeters) – (5 X age in years) + 5 (kcal/day)
- Females Basal metabolic rate [BMR] (kcal/day) = (10 X weight in kilograms) + (6.25 X height in centimeters) – (5 X age in years) – 161 (kcal/day)
You can also use the free online Basal Metabolic Rate (BMR) calculator here: https://www.nasm.org/resources/calorie-calculator
Or the Body Weight Planner (https://www.niddk.nih.gov/health-information/weight-management/body-weight-planner).
The Body Weight Planner allows you to make personalized calorie and physical activity plans to reach a goal weight within a specific time period and to maintain it afterwards.
The Basal Metabolic Rate (BMR) calculator factor in your activity levels, overall goals, and calorie usage to help you craft a weight-loss plan.
Once you have found your basal metabolic rate (BMR), multiply your BMR by your Physical Activity Levels to provide a baseline daily caloric level for weight maintenance:
- Sedentary (light physical activity associated with typical day-to-day life) = 1
- Low Active (walking about 1.5 to 3 miles per day at 3 to 4 miles per hour, in addition to the light physical activity associated with typical day-to-day life), For males = 1.11 and females = 1.20
- Active (walking more than 3 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate intensity physical activity). For males = 1.25 and females = 1.27
- Very Active (walking more than 7.5 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate to vigorous intensity physical activity). For males = 1.48 and females = 1.45
Your Total Daily Energy Expenditure (TDEE) gives you the estimated number of calories you need to maintain your current weight based on your activity level.
To find your Total Daily Energy Expenditure (TDEE) multiply your Basal Metabolic Rate (BMR) by your Physical Activity Levels
For example:
- Sedentary (little to no exercise): BMR x 1
- Lightly active (walking about 1.5 to 3 miles per day at 3 to 4 miles per hour, in addition to the light physical activity associated with typical day-to-day life): BMR x For males = 1.11 and females = 1.20
- Moderately active (moderate exercise/sports 3-5 days/week): BMR x 1.55
- Very active (walking more than 7.5 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate to vigorous intensity physical activity): BMR x For males = 1.48 and females = 1.45
- Super active (very hard exercise & physical job or 2x training): BMR x 1.9
You can increase your basal metabolic rate (BMR) by:
- Exercising more, especially interval training
- Weight training to build muscle mass
- Eating fat-burning foods
- Getting enough sleep
After calculating your basal metabolic rate (BMR) or resting metabolic rate (RMR), your RMR should be multiplied by an appropriate physical activity factor to provide your baseline daily caloric level for weight maintenance. Once your baseline caloric level is known, your recommended calorie intake should be reduced to facilitate your weight loss.
If you want to lose weight, subtract 500 to 1000 calories from your Total Daily Energy Expenditure (TDEE) to get a daily intake goal. For weight gain, add extra calories. Reducing your calorie intake by 500 calories is a common strategy to yield a weight loss of approximately one pound per week, although reductions of up to 750 calories per day are sometimes used 55.
Another approach is to reduce your current caloric intake by 30% 55. Diets that reduce caloric intake relative to energy expenditure result in weight loss, regardless of macronutrient composition 55.
Here’s how to estimate how long it will take to reach your goal:
Jessie’s current weight is 150 lbs. She wants to lose 20 lbs.
- 150lbs – 20lbs = 130lbs.
- 20lbs loss at 2lbs/week = 10 weeks.
- It will take Jessie about 10 week to lose the weight.
Remember, these are general guidelines only. It’s crucial to monitor your progress and adjust as necessary. Consulting with a nutritionist or health professional is always recommended for personalized advice.
How many calories should I eat to lose weight?
For a healthy and sustainable weight loss journey, it’s typically recommended you not to shed more than 2 pounds of fat weekly. This translates to a daily calorie deficit of 1,000 calories. It’s essential to note that when weight loss surpasses 2lbs within a week, it’s often water weight being lost, not just fat.
For those leading a more sedentary lifestyle, aiming to lose 1lb per week is a good starting point. This means creating a daily calorie deficit of 500 calories.
On the other hand, those who are more active naturally have higher daily calorie needs. So, when they’re trying to lose weight, they can afford to eat a bit more since their maintenance calories are already elevated.
For such individuals, aiming for a daily calorie deficit of 500-1,000 calories is realistic, potentially leading to a weight loss rate of up to 2lbs weekly.
What happens when your calories are too low?
Consuming calories below your body’s needs for an extended period can lead to various physiological and psychological consequences. Here’s what can happen when your caloric intake is too low:
- Slower metabolism: Your body might slow down its metabolic rate as a defense mechanism to conserve energy. This can make weight loss harder over time and weight regain more likely once normal eating resumes.
- Nutrient deficiencies: Low calorie intake can lead to inadequate intake of essential vitamins and minerals. Over time, this can result in conditions like anemia, osteoporosis, and impaired immune function.
- Loss of muscle mass: Your body might start breaking down muscle tissue for energy, especially if protein intake is inadequate. This can further slow down metabolism and lead to weakness.
- Hormonal changes: Reduced calorie intake can affect hormone levels, leading to disruptions in menstrual cycles for women, reduced bone density, and other hormonal imbalances.
- Reduced energy and fatigue: You might feel constantly tired or find it difficult to concentrate.
- Mood changes: Low caloric intake can influence mood. This can result in irritability, depression, or anxiety.
- Impaired Immune Function: Your body might become more susceptible to infections due to a weakened immune system.
- Hair and skin problems: You might experience hair loss, dry skin, or brittle nails due to inadequate nutrient intake.
- Digestive problems: Constipation or other digestive issues can occur as a result of reduced fiber and fluid intake.
- Fertility issues: Low calorie and nutrient intake can lead to fertility problems in both men and women.
- Cardiovascular problems: Chronic low calorie intake can affect heart health, leading to low blood pressure, irregular heart rhythms, or other cardiovascular issues.
- Increased risk of gallstones: Rapid weight loss from very low-calorie diets can lead to the development of gallstones.
Setting Realistic Goals
Realistic goals are achievable and manageable within your current circumstances. To set realistic goals, you can use the SMART method, which stands for Specific, Measurable, Attainable, Relevant, and Time-bound:
- Specific: Define exactly what you want to accomplish
- Measurable: Make your goal quantifiable so you can track your progress
- Attainable: Ensure your goal is something you can do with your current resources
- Relevant: Consider how your goal will improve your life or career
- Time-bound: Set a deadline for when you want to achieve your goal
Here are some other tips for setting realistic goals:
- Write it down: Make your goal feel more tangible by writing it down
- Plan your steps: Think of one or two things you are ready, willing and able to change about the way you eat and exercise. Then set a goal for each. Consider three things:
- What is the behavior that you will change? Be specific.
- How often will you do this?
- Don’t try to change too much at once. Be realistic.
- Share your goal: Tell someone you trust about your goal to help you stay accountable and motivated
- Focus on one or two goals at a time: Working on too many goals at once can make it difficult to complete any of them
- Set a range: Set a range of what’s good, great, and excellent to help you stretch your goals
Here are some examples of goals that include the SMART method:
- Eating goal: Four days each week (How Often) I will eat an apple instead of ice cream as my evening snack (Realistic and Specific).
- Physical activity goal: Five days each week (How Often) I will take a 30 minute walk during my lunch hour since I don’t really need the whole hour to eat (Realistic and Specific).
Notice that the eating goal is not “I will eat more fruit” or “I will eat healthier.” The activity goal is not “I’ll walk more.” Goals like that are not specific enough.
There is no single target weight that will meet every one’s goals 39. Optimal weight reduction targets vary depending on your sex, height, weight, health, level of physical activity and medical conditions. Progress toward healthier weight goals should involve a gradual approach that minimizes health risks and is timed to your level of readiness. With time, greater weight loss may be possible if realistic goals are adopted, met, and sustained.
Most people may have unrealistic ideas of how much better they will look with even modest weight loss (i.e. a half-pound per week) 56. You need to have a realistic weight loss target set for yourself, which you have developed during consultation with your healthcare professionals (e.g., your doctor and dietitian). Most people’s weight loss targets are often unrealistically high and their time frames unrealistically short (e.g., targets of 25% or more of body weight in a few weeks rather than many months) 39. Numerous studies have shown that obese individuals hope to lose 25 to 35% of their initial weight within a year or less after beginning obesity treatment 39. Realistically, people only lose 5 to 15% of their initial weight over a year after beginning any kind of obesity treatment 39. Unfortunately, many dieters still maintain unrealistic standards even when they are repeatedly informed that their goals may be unrealistic 45, 57, 58.
A healthy weight-loss target is usually to achieve a weight loss of one-half to two pounds of body weight each week over six months (24 weeks), leading to a decrease of 5 to 10% in body weight from baseline 39. For example a 250 pound, 5’6’’ woman with a BMI of 40 that lost 12.5 pounds over six months, would have a 5% weight loss, and an ending BMI of 38.5. A 10% weight loss would result in a BMI of 36.3. The goal is to maintain this weight loss over time, and that is never easy. A weight loss of 5 to 10% is achievable and moderate enough to decrease some obesity-related risk factors, such as type 2 diabetes, high blood pressure, heart and blood vessel disease, and sleep apnea 59.
Once you set your goals, start setting up a plan to help you achieve them. After that it is vital to begin a weight maintenance program that includes the same three components used for initial weight loss such as dieting, physical activity, and behavior change to help prevent weight regain and maintain your new, healthier lifestyle 53.
Behaviors that will help you lose weight and keep it off
Set the Right Goals
Setting the right goals is an important first step. Most people trying to lose weight focus on just that one goal: weight loss. However, the most productive areas to focus on are the dietary and physical activity changes that will lead to long-term weight change. Successful weight managers are those who select two or three goals at a time that are manageable.
Useful goals should be:
- Specific;
- Attainable (doable); and
- Forgiving (less than perfect).
For example, “exercise more” is a great goal, but it’s not specific. “Walk 5 miles every day” is specific and measurable, but is it doable if you’re just starting out? “Walk 30 minutes every day” is more attainable, but what happens if you’re held up at work one day and there’s a thunderstorm during your walking time another day? “Walk 30 minutes, 5 days each week” is specific, doable, and forgiving. In short, a great goal!
Be prepared for setbacks
Setbacks are normal. After a setback, like overeating at a family or workplace gathering, try to regroup and focus on getting back to your healthy eating plan as soon as you can. Try to eat only when you’re sitting at your dining room or kitchen table. At work, avoid areas where treats may be available. Track your progress using online food or physical activity trackers, such as the Body Weight Planner (https://www.niddk.nih.gov/bwp), that can help you keep track of the foods you eat, your physical activity, and your weight. The Body Weight Planner allows users to make personalized calorie and physical activity plans to reach a goal weight within a specific time period and to maintain it afterwards. These tools may help you stick with it and stay motivated.
Overcome roadblocks
Remind yourself why you want to be healthier. Perhaps you want the energy to play with your nieces and nephews or to be able to carry your own grocery bags. Recall your reasons for making changes when slip-ups occur. Decide to take the first step to get back on track.
Problem-solve to “outsmart” roadblocks. For example, plan to walk indoors, such as at a mall, on days when bad weather keeps you from walking outside.
Ask a friend or family member for help when you need it, and always try to plan ahead. For example, if you know that you will not have time to be physically active after work, go walking with a coworker at lunch or start your day with an exercise video.
Nothing Succeeds Like Success
Shaping is a behavioral technique in which you select a series of short-term goals that get closer and closer to the ultimate goal (e.g., an initial reduction of fat intake from 40 percent of calories to 35 percent of calories, and later to 30 percent). It is based on the concept that “nothing succeeds like success.”
Shaping uses two important behavioral principles:
- Consecutive goals that move you ahead in small steps are the best way to reach a distant point; and
- Consecutive rewards keep the overall effort invigorated.
Reward Success (But Not With Food)
An effective reward is something that is desirable, timely, and dependent on meeting your goal. The rewards you choose may be material (e.g., a movie or music CD, or a payment toward buying a more costly item) or an act of self-kindness (e.g., an afternoon off from work or just an hour of quiet time away from family). Frequent small rewards, earned for meeting smaller goals, are more effective than bigger rewards that require a long, difficult effort.
Balance Your Food Checkbook
“Self-monitoring” refers to observing and recording some aspect of your behavior, such as calorie intake, servings of fruits and vegetables, amount of physical activity, etc., or an outcome of these behaviors, such as weight. Self-monitoring of a behavior can be used at times when you’re not sure how you’re doing, and at times when you want the behavior to improve. Self-monitoring of a behavior usually moves you closer to the desired direction and can produce “real-time” records for review by you and your health care provider. For example, keeping a record of your physical activity can let you and your provider know quickly how you’re doing. When the record shows that your activity is increasing, you’ll be encouraged to keep it up. Some patients find that specific self-monitoring forms make it easier, while others prefer to use their own recording system.
While you may or may not wish to weigh yourself frequently while losing weight, regular monitoring of your weight will be essential to help you maintain your lower weight. When keeping a record of your weight, a graph may be more informative than a list of your weights. When weighing yourself and keeping a weight graph or table, however, remember that one day’s diet and exercise patterns won’t have a measurable effect on your weight the next day. Today’s weight is not a true measure of how well you followed your program yesterday, because your body’s water weight will change from day to day, and water changes are often the result of things that have nothing to do with your weight-management efforts.
Avoid a Chain Reaction
Stimulus (cue) control involves learning what social or environmental cues seem to encourage undesired eating, and then changing those cues. For example, you may learn from reflection or from self-monitoring records that you’re more likely to overeat while watching television, or whenever treats are on display by the office coffee pot, or when around a certain friend. You might then try to change the situation, such as by separating the association of eating from the cue (don’t eat while watching television), avoiding or eliminating the cue (leave the coffee room immediately after pouring coffee), or changing the circumstances surrounding the cue (plan to meet your friend in a nonfood setting). In general, visible and reachable food items are often cues for unplanned eating.
Get the Fullness Message
Changing the way you go about eating can make it easier to eat less without feeling deprived. It takes 15 or more minutes for your brain to get the message that you’ve been fed. Eating slowly will help you feel satisfied. Eating lots of vegetables and fruits can make you feel fuller. Another trick is to use smaller plates so that moderate portions do not appear too small. Changing your eating schedule, or setting one, can be helpful, especially if you tend to skip, or delay, meals and overeat later.
Seek support
Ask for help or encouragement from your family, friends, or health care professionals. You can get support in person, through email or texting, or by talking on the phone. You can also join a support group. Specially trained health professionals can help you change your lifestyle.
Eating behavior
Emotional eating can quickly sabotage weight loss efforts. For example, you have probably heard that some people eat to cope with stress. Others eat to preoccupy themselves when they feel bored. If you can pinpoint the emotions that cause you to reach for food, you can stay on track.
If you have recently eaten and find yourself craving food again, do a quick emotional check. Do you want food because you are hungry or to fill an emotional need?
Here are some tips to keep your eating in check:
- Remember which emotions and situations trigger you to eat.
- Write a list of other things to do to fulfill that emotional need, for example, call a friend, take a walk, drink some water or another zero-calorie beverage, send an email to a pal or do a few yoga stretches.
- Track the food you eat, how hungry you are when you eat and how you feel at the time. You may get a better idea of which emotions trigger eating when you are not physically hungry.
If you are having a hard time, reach out for help. Involve family members and friends to help support your weight loss efforts. Support groups, therapy and members of your health care team can also help.
What is the best way to lose weight?
There is no one best way to lose weight, which is why doctors and dietitians work to understand your personal circumstances when making recommendations. There is no quick fix. Improving your diet and increasing activity can be key to losing weight, although are not the only factors that need to be considered. When aiming to lose weight it is important to have realistic goals that are achievable. Success boosts confidence in your ability to lose weight. A weight loss of between 0.5 to 2 pounds (0.5-1kg) a week is a safe and realistic target. Experts recommend losing 5 to 10 percent of your body weight within the first 6 months of treatment 60. If you weigh 200 pounds, this means losing as little as 10 pounds. Moreover, it’s not just about your weight on the scales, losing inches from your waist helps to lower your risk of conditions like type 2 diabetes and high blood pressure. To reach and stay at a healthy weight over the long term, you must focus on your overall health and lifestyle habits, not just on what you eat. Successful weight-loss programs should promote healthy behaviors that help you lose weight safely, that you can stick with every day, and that help you keep the weight off. People who successfully lose weight and keep it off develop techniques to make their new lifestyle and activity habits an enjoyable way of life and also make them life long.
You weight loss programs and weight loss maintenance programs should focus on changing your behavior to reduce energy intake by cutting unhealthy foods, decreasing sugar‐sweetened beverage consumption and fat intake, portion control, increasing fruit and vegetable intake, and adhering to a diet 61. Additionally, energy expenditure should be promoted through increasing physical activity.
American College of Sports Medicine recommendations for physical activity for Weight Loss and Prevention of Weight Regain for Adults 62:
- Maintain and improving health: 150 minutes/week
- Prevention of weight gain: 150 – 250 minutes/week
- Promote clinically significant weight loss: 225 – 420 minutes/week
- Prevention of weight gain after weight loss: 200 – 300 minutes/week
Strong evidence exists that exercise (physical activity) can reduce weight gain in those at risk for obesity, and many exercise training programs are capable of producing at least modest weight loss (~2 kg) 62. A question often encountered in the clinical setting from patients is how much exercise is needed to lose weight and what type of exercise training should be performed. Overall, the changes in weight in response to exercise training without caloric restriction are highly heterogeneous and individual differences can span weight gain to clinically significant weight loss 63. Patients should should consult their clinicians or dietitians on what are reasonable expectations based on their specific weight loss program. However, research data suggest that physical activity has an important role in the amount of weight regain following successful weight loss 64. Therefore, patients attempting to reduce recidivism after weight loss should engage in physical activity levels above 200 minutes/week 62.
Furthermore, high levels of physical activity and cardiorespiratory fitness (fitness) are inversely associated with cardiovascular disease, type 2 diabetes and all-cause mortality 65. Several epidemiological studies even suggest that high levels of physical activity or cardiorespiratory fitness reduces the health risk of obesity 66, 67. Moreover, cardiorespiratory fitness levels have been shown to alter the relationship of the obesity paradox, where high cardiorespiratory fitness level is associated with greater survival in all body mass index (BMI) categories 68. In summary, patients are encourage to adhere to exercise programs or engage in regular physical activity regardless of the weight loss achieved.
Another question that is often encountered in the clinical setting is if there is a difference between weight loss achieved through dietary means or through exercise training in terms of cardiovascular and type 2 diabetes mellitus risk factors. In an elegantly designed study, Ross et al. 69 randomized obese men (n= 52) to diet-induced weight loss, exercise induced weight loss, exercise without weight loss, or a control group for 3 months. The diet-induced and exercise-induced weight loss groups lost approximately 7 kg of weight (8% weight reduction), and had significant reductions in total fat mass, visceral fat and increased glucose disposal 69. However, the exercise-induced weight loss group had a greater reduction in total fat mass compared to the diet induced weight loss group 69. Importantly, the exercise-induced weight loss improved cardiorespiratory fitness (fitness) whereas the dietary group did not. In the group who performed exercise training without weight loss, the participants still experienced reductions in visceral fat and increased cardiorespiratory fitness.
The observations by Ross et al. 69 reaffirm that an exercise training program still confers health benefits to obese patients even in the absence of weight loss. Although dieting without exercise training has potential cardiovascular benefits, exercise training should be encouraged by to help patients improve cardiorespiratory fitness levels, which is an independent risk factor for cardiovascular diseases, type 2 diabetes mellitus and mortality 10, and may further augment the negative energy balance created by caloric restriction. Lastly, Ross’ observations suggest that there is a rationale for exercise training to be a part of weight loss programs as the authors observed greater changes in visceral fat, oral glucose tolerance, and glucose disposal in the exercise training group with clinically significant weight loss compared to the group with exercise without weight loss group 69.
Healthy Weight-Loss
Healthy weight loss is key for long-term weight maintenance. A variety of weight loss methods are available, from minimally structured self-guided methods to medically supervised very low calorie diet (VLCD; e.g., 400–800 kcal/day) regimens 70. Intensive, very low-calorie diets (VLCDs; e.g., ≤800 calories per day and especially <500 calories) produce significantly greater initial weight loss; however, these results are often not maintained over time 70. In a study done in 2008, participants were enrolled in a program designed to help maintain weight loss 70. Participants all initially lost weight using one of three methods, very low calorie diet (VLCD; e.g., 400–800 kcal/day), commercial programs or a self-guided approach 70. At the start of the study, those who had used a very low calorie diet (VLCD; e.g., 400–800 kcal/day) lost up to 24% of highest body weight in the last two year compared to those in the commercial programs and self-guided approaches who lost 17% 70. Results showed that those who used a very low calorie diet (VLCD; e.g., 400–800 kcal/day) regained significantly more weight than the other two groups by six months in the weight maintenance program 70. However, those who had lost weight using a self-guided method were able to maintain their initial weight loss with great success 70. It should be emphasized that the primary reason for losing weight is for better health outcomes; therefore, weight loss should occur by using healthy methods that can be maintained throughout your life 39. Concentrating on improving health outcomes and other risk factors rather than simply on weight loss is vital 39.
In most people, a 10% weight loss target can be achieved with a calorie deficit of 500 to 1,000 calories per day, leading to weight losses of one pound to two pounds per week (i.e. total calories deficit of 3,500 to 7,000 per week) 39. Cutting down on alcohol, dietary fats and sugary carbohydrates is a practical way to produce this calorie deficit 71. A comprehensive analysis of data that focuses on dieting and weight loss found that increased lean tissue (muscle tissue) is lost if the energy deficit of the diet is too large in combination with rapid weight loss 72. In contrast, inclusion of exercise (both cardio workout and weightlifting) and adequate dietary protein (60 grams per day, ranging from 0.8 g to 1.5 g per kg of body weight) helps to minimize muscle tissue loss 72. These dietary strategies should be incorporated into dietary treatment plans to minimize muscle mass reduction and maximize fat loss 39.
For women, a weight reduction plan of eating approximately 1,000 to 1,200 calories per day is suitable. According to the National Institutes of Health and the National Heart, Lung, and Blood Institute, a 1,200 – 1,600 calorie allowance for men or women who weigh 165 pounds, or more, and who exercise regularly is recommended 39. These calorie amounts along with increased physical activity and behavioral modification will likely produce a caloric deficit to achieve the targeted weight loss plan of one to two pounds per week 73. With a caloric deficit of 500 to 1000 calories per day, if followed with perfect adherence, after six months, weight loss of 26 to 52 pounds would be expected. However, in reality, losses are usually between 20 to 25 pounds, since adherence is never perfect 74.
It is recommended that you dieting should last for 6 months or less, because according to research after about six months, most people have great difficulty sticking to any diet, especially if it is very strict 39. Furthermore, your weight will plateau as your energy intake fluctuates and as your resting metabolic rate and energy output decrease. After six months of weight loss, you should focus on maintenance of the weight loss through a combination of diet therapy, physical activity, and behavior modification. If successful, after several months you can start a new weight loss cycle again 39. If further weight reduction is necessary after 10% of initial body weight is lost, it can be attempted with an increased calorie deficit after prior weight loss has been maintained for several months.
When you do not engage in a weight management program that includes all three components (i.e., diet therapy, physical activity, and behavior modification) you’re risking regaining all or extra weight increase 53, 74. Most people regain one-third of their lost weight in one year, and nearly half return to their original weight within five years 57. The more frequently you have has contact with your healthcare provider (doctor and dietitian), the weight loss and maintenance outcomes tend to be more successful 53.
Now you know the basics about calories and healthy weight loss, the key to weight loss for most people is simply finding the right combination of exercise, healthy foods and cutting back on portions will help you lose those extra pounds. No fad diet required. In other words, eat healthily, watch your portions and get moving more. By losing just a few pounds with healthy eating and exercise, you’ll start to feel better. You’ll have more energy. To prevent the weight creeping back on, you need to keep going with the healthy habits you’ve formed.
Low-Calorie Diets (LCDs)
Low-Calorie Diets (LCDs) are eating plans or meal plans that reduce your caloric intake to about 1,200 to 1,500 calories in women, and 1,500 to 1,800 calories in men 39. Low-Calorie Diets (LCDs) will result in weight loss if they are adhered to perfectly, regardless of their macronutrient composition 55, 75. This is because these low caloric levels will result in a caloric deficit for most overweight and obese adults. The National Institutes of Health have recommended low calorie diets (LCDs) of 1,000 to 1200 calories for women, and 1,200 to 1,600 calories per day for men, although adherence may be difficult with lower caloric intake 74. Either way, the rationale is that on such eating plans, a deficit of approximately 500 to 1,000 calories per day will be created, which should result in a slow progressive weight loss of one to two pounds per week 39. The MyPlate.gov website (https://www.myplate.gov/) that can be accessed by consumers provides a simple visual reminder to choose a variety of foods throughout the day and throughout the week. It represents what and how much to eat from each of the food groups over the course of the day, whether you eat on a plate, from a bowl, or another way.
It is important to recognize that when using fixed calorie diet plans, that even with perfect adherence, individuals will vary greatly in their weight loss. This is because their resting energy needs and physical activity, and thus energy outputs, often differ markedly, and may fluctuate even within an individual.
1200 Calories eating plan
Over the next 12 weeks you’re going to make healthier choices to help you lose weight and keep it off. From today, you’ll stick to a daily calorie intake of 1200 Calories.
Table 6. 1200 Calories Traditional American Cuisine
| Breakfast | Energy (Kcal) | Fat (gram) | % Fat | Exchange for: |
| Whole-wheat bread, 1 med. slice | 70 | 1.2 | 15 | (1 Bread/Starch) |
| Jelly, regular, 2 tsp | 30 | 0 | 0 | (½ Fruit) |
| Cereal, shredded wheat, ½ Cup | 104 | 1 | 4 | (1 Bread/Starch) |
| Milk, 1%, 1 Cup | 102 | 3 | 23 | (1 Milk) |
| Orange juice, ¾ Cup | 78 | 0 | 0 | (1½ Fruit) |
| Coffee, regular, 1 Cup | 5 | 0 | 0 | (Free) |
| Breakfast Total | 389 | 5.2 | 10 | |
| Lunch | Energy (Kcal) | Fat (gram) | % Fat | Exchange for: |
| Roast beef sandwich | ||||
| Whole-wheat bread, 2 medium slices | 139 | 2.4 | 15 | (2 Bread/Starch) |
| Lean roast beef, unseasoned, 2oz | 60 | 1.5 | 23 | (2 Lean Protein) |
| Lettuce, 1 leaf | 1 | 0 | 0 | |
| Tomato, 3 med. slices | 10 | 0 | 0 | (1 Vegetable) |
| Mayonnaise, low-calorie, 1 tsp | 15 | 1.7 | 96 | (1⁄3 Fat) |
| Apple, 1 medium | 80 | 0 | 0 | (1 Fruit) |
| Water | 0 | 0 | 0 | (Free) |
| Lunch Total | 305 | 5.6 | 16 | |
| Dinner | Energy (Kcal) | Fat (gram) | % Fat | Exchange for: |
| Salmon, 2 oz edible | 103 | 5 | 40 | (2 Lean Protein) |
| Vegetable oil, 1½ tsp | 60 | 7 | 100 | (1½ Fat) |
| Baked potato, ¾ medium | 100 | 0 | 0 | (1 Bread/Starch) |
| Margarine, 1 tsp | 34 | 4 | 100 | (1 Fat) |
| Green beans ½ Cup, seasoned with margarine | 52 | 2 | 4 | (1 Vegetable) (½ Fat) |
| Carrots, seasoned | 35 | 2 | 0 | (1 Vegetable) |
| White dinner roll, 1 small | 70 | 2 | 26 | (1 Bread/Starch) |
| Iced tea, unsweetened | 0 | 0 | 0 | (Free) |
| Water | 0 | 0 | 0 | (Free) |
| Dinner Total | 454 | 20 | 39 | |
| Snack | Energy (Kcal) | Fat (gram) | % Fat | Exchange for: |
| Popcorn, 2½ Cups | 69 | 0 | 0 | (1 Bread/Starch) |
| Margarine, ¾ tsp | 30 | 3 | 100 | (¾ Fat) |
| Grand Total | 1247 | 34 | 24 |
Footnotes: Total Calories = 1,247; Total Carb = 58% kcals; Total Fat = 26% kcals; Saturated Fat = 7% kcals; Cholesterol = 96 mg; Protein = 19% kcals; Sodium (salt) = 1,043 mg (No salt added in recipe preparation or as seasoning). Consume at least 32 oz (950 ml) water. Recommended Dietary Allowance (RDA) is average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%-98%) healthy people. 100% RDA met for all nutrients except: vitamin E 80%, vitamin B2 96%, vitamin B6 94%, Calcium 68%, Iron 63% and Zinc 73%.
[Source 76 ]1600 Calories eating plan
Table 7. 1600 Calories Traditional American Cuisine
| Breakfast | Energy (Kcal) | Fat (gram) | % Fat | Exchange for: |
| Whole-wheat bread, 1 medium slice | 70 | 1.2 | 15 | (1 Bread/Starch) |
| Jelly, regular, 2 tsp | 30 | 0 | 0 | (½ Fruit) |
| Cereal, shredded wheat, ½ Cup | 104 | 1 | 4 | (1 Bread/Starch) |
| Milk, 1%, 1 Cup | 102 | 3 | 23 | (1 Milk) |
| Orange juice, ¾ Cup | 78 | 0 | 0 | (1½ Fruit) |
| Coffee, regular, 1 Cup | 5 | 0 | 0 | (Free) |
| Milk, 1%, 1 oz | 13 | 0.03 | 23 | (1⁄8 Milk) |
| Breakfast Total | 402 | 5.23 | 12 | |
| Lunch | Energy (Kcal) | Fat (gram) | % Fat | Exchange for: |
| Roast beef sandwich | ||||
| Whole-wheat bread, 2 medium slices | 139 | 2.4 | 15 | (2 Bread/Starch) |
| Lean roast beef, unseasoned, 2 oz | 60 | 1.5 | 23 | (2 Lean Protein) |
| American cheese, low-fat and low-sodium, 1 slice (¾ oz) | 46 | 1.8 | 36 | (1 Lean Protein) |
| Lettuce, 1 leaf | 1 | 0 | 0 | |
| Tomato, 3 medium slices | 10 | 0 | 0 | (1 Vegetable) |
| Mayonnaise, low-calorie, 2 tsp | 30 | 3.3 | 99 | (2⁄3 Fat) |
| Apple, 1 medium | 80 | 0 | 0 | (1 Fruit) |
| Water | 0 | 0 | 0 | (Free) |
| Lunch Total | 366 | 9 | 22 | |
| Dinner | Energy (Kcal) | Fat (gram) | % Fat | Exchange for: |
| Salmon, 3 oz edible | 155 | 7 | 40 | (3 Lean Protein) |
| Vegetable oil, 1½ tsp | 60 | 7 | 100 | (1½ Fat) |
| Baked potato, ¾ medium | 100 | 0 | 0 | (1 Bread/Starch) |
| Margarine, 1 tsp | 34 | 4 | 100 | (1 Fat) |
| Green beans ½ Cup, seasoned with margarine | 52 | 2 | 4 | (1 Vegetable) (½ Fat) |
| Carrots ½ Cup, seasoned with margarine | 52 | 2 | 4 | (1 Vegetable) (½ Fat) |
| White dinner roll, 1 medium | 80 | 3 | 33 | (1 Bread/Starch) |
| Ice milk, ½ Cup | 92 | 3 | 28 | (½ Fat) |
| Iced tea, unsweetened, 1 Cup | 0 | 0 | 0 | (Free) |
| Water | 0 | 0 | 0 | (Free) |
| Dinner Total | 625 | 28 | 40 | |
| Snack | Energy (Kcal) | Fat (gram) | %Fat | Exchange for: |
| Popcorn, 2½ Cups | 69 | 0 | 0 | (1 Bread/Starch) |
| Margarine, 1½ tsp | 51 | 6 | 100 | (1½ Fat) |
| Grand Total | 1490 | 48 | 29 |
Footnotes: Total Calories = 1,490; Total Carb = 52% kcals; Total Fat = 29% kcals; Saturated Fat = 8% kcals; Cholesterol = 142 mg; Protein = 19% kcals; Sodium (salt) = 1,341 mg (No salt added in recipe preparation or as seasoning). Consume at least 32 oz (950 ml) water. Recommended Dietary Allowance (RDA) is average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%-98%) healthy people. 100% RDA met for all nutrients except: vitamin E 99%, Iron 73% and Zinc 91%.
[Source 77 ]Very-Low-Calorie Diets (VLCDs)
Very-Low-Calorie Diets (VLCDs) are eating plans or meal plans that reduce your caloric intake to about 800 calories or less per day with a total of 50 to 80 grams of protein and 100% of the Reference Daily Intake (RDI) for vitamins and minerals per day, and are designed to produce very rapid weight loss while still preserving lean muscle mass 53. Very-Low-Calorie Diets (VLCDs) are reserved for special uses and for people at high obesity-related health risks where it is imperative to lose weight because of their potential for greater adverse metabolic effects and the consequent need for more extensive medical monitoring. Possible side effects of very-low-calorie diets (VLCDs) are fatigue, constipation, nausea, or diarrhea to more serious risks such as ketoacidosis and gallstones 39. Very-Low-Calorie Diets (VLCDs) contraindications include recent heart attack (myocardial infarction), heart conduction disorders, history of cardiovascular disease, kidney or liver disease, cancer, type 1 diabetes, and pregnancy 39. Behavioral contraindications to their use include bulimia nervosa, major depression, bipolar disorder, substance abuse, and acute psychiatric illness 39.
Very-Low-Calorie Diets (VLCDs) are often prescribed by your doctor as a form of intensive diet therapy, which require close medical supervision by a physician specializing in obesity care and should not be used long-term 39. Very-Low-Calorie Diets (VLCDs) are intended to induce quick and significant weight loss of about 3 to 5 pounds per week or 14 to 21 kilograms over 11 to 14 weeks 39. Very-Low-Calorie Diets (VLCDs) are sometimes used to provide a jump-start to further obesity treatment. This is typically done through meal-replacement liquid diets 78. Any diet, regardless of its caloric level, that provides less than half of an individual’s energy needs can be considered a Very-Low-Calorie Diet (VLCD) for that individual. However, virtually all adults have energy needs that exceed 1,000 calories per day, and therefore any diet below 500 calories, and for most individuals, diets below 800 calories, are Very-Low-Calorie Diets (VLCDs) 39. Depending on your caloric requirements, other dieting regimens that are higher in calories may also be VLCD for some people with very high energy needs using this same rule of thumb; for example, a 1,200 calorie diet prescribed to a man whose usual intake is 3,000 calories would also qualify as a VLCD 39.
According to the National Task Force on the Prevention and Treatment of Obesity, Very-Low-Calorie Diets (VLCDs) in patients with BMI >30 are usually effective in promoting significant short-term weight loss, in addition to improving coexisting obesity-related conditions (e.g., obstructive sleep apnea, poorly-controlled type 2 diabetes, hypertriglyceridemia) 79. However, Very-Low-Calorie Diets (VLCDs) require close metabolic monitoring with at least every 2 weeks doctor visits, and should only be prescribed and adjusted under the supervision of a physician specializing in obesity care 39.
The main advantages of the VLCD for patients include a rapid improvement in blood pressure, blood glucose, serum lipids and often-psychological status. For those who require surgery, the rapid loss of weight may reduce some of the surgical risks associated with obesity 39.
There are 2 major types of very-low-calorie diets (VLCDs) currently in use; commercial and “home-made” preparations. The commercial very-low-calorie diets (VLCDs) preparations include powdered products that are rich in egg- or milk-based proteins, are mixed with water, and consumed four to five times per day 39. The commercial products must provide at least 70 grams of protein by law, and often contain much higher amounts of high quality protein (70 to 100 grams), 50 to 100 grams carbohydrate, and up to 15 grams fat per day, plus vitamins and minerals in amounts to meet the Recommended Dietary Allowances (RDA) 39. These products are formulated under U.S. Food and Drug Administration (FDA) regulatory specifications. They are convenient and have a predictable and adequate composition when used as directed. Their major disadvantage compared to home preparations is their higher cost. The formulas or prepackaged meals are relatively choice-free and help dieters avoid contact with conventional foods, which in some cases may facilitate dietary adherence and remove temptation.
Several commercial weight loss programs are available that provide an entire program of commercially prepared very-low-calorie diets (VLCDs) plus the other essential aspects of a sound weight control program, including dietetic advice, exercise, behavioral modification, and supervision during the VLCD and post VLCD phases. The choices include the programs of HMRTM (Health Management Resources), OptifastTM (Novartis Nutrition), and MedifastTM. These programs employ health professionals who are trained in weight management, and a structured program that encourages adherence. The major disadvantage is that they are expensive ($3,000 to $34,000 for 26 to 28 weeks), and costs may not be covered by health insurance 80. Also, there is the uncertainty that the weight that is lost will remain so over the long run. Therefore a serious psychological as well as economic investment of effort in long-term weight management is also mandatory.
“Home made” VLCD regimens are sometimes referred to as “protein-sparing fasts” or “protein sparing modified fasts” (PSMF) 39. This is a misnomer since they do not “spare” protein except in contrast to a total fast. “Home made” very-low-calorie diets (VLCDs) are usually based on lean meat, fish or poultry and a few other foods plus supplements of two to three grams of potassium chloride and a multivitamin or multimineral supplement in amounts approximating the Recommended Dietary Allowances (RDA) 39. Without such supplementation, they may be nutritionally inadequate 39. When dieters are provided with appropriate dietetic counseling and health supervision by a physician who is experienced in the use of very-low-calorie diets (VLCDs) and other aspects of a complete weight reduction program, these formulations are also safe and generate rapid weight loss 39. The extremely low caloric versions of VLCDs (e.g., less than or equal to 800 calories per day), which are low in carbohydrate and sodium, promote a mild ketosis that gradually leads to diuresis and rapid weight loss in the first several days on the diet.
There seems to be little difference in outcomes between commercial and properly formulated homemade very-low-calorie diets (VLCDs). The National Institute of Health expert panel review of existing studies found that preservation of weight loss over the long-term (e.g., >1 year) was not different on Very-Low-Calorie Diets (VLCDs) from that of Low-Calorie Diets (LCDs) since most patients gained back 30 to 50% of the lost weight 39. Studies of VLCDs vary in their long-term results, but weight regain is common (3.1 to 3.7 kg during 21-38 weeks afterwards) 55. Combining a VLCD with behavior therapy, physical activity, and active physician follow-up may help to prevent this weight regain, and lend to greater weight loss 81. As such, the long-term advantages of VLCDs in weight control are unclear. Although weight gain is common after cessation of VLCDs, individual clinicians may decide that the expense and quick initial weight loss are worth it for their patient 53.
Patients on VLCDs should drink at least two liters of water per day to make up for decreased food intake and to prevent dehydration 39. Avoidance of caffeinated beverages is sometimes recommended, as they can further the risk of dehydration, although moderate use is not prohibited 39. Electrolyte imbalances may occur, and so may nutrient deficiencies if measures are not taken to prevent them on “home-made” VLCD, by use of appropriate supplements. Minor side effects that occur, even with appropriate physician monitoring of heart and general health status, include fatigue, dizziness due to orthostatic hypotension, muscle cramps, gastrointestinal distress (constipation and/or diarrhea), and cold intolerance 39. The risk of cholelithiasis (gallstones) is increased, and seems to be particularly high when weight loss is very rapid (e.g., >1.5 kilograms/week) 39. The risk of cholelithiasis (gallstones) can be decreased by administering ursodeoxycholic acid, including a moderate amount of fat in the diet, and limiting the amount of weight loss to 1.5 kilograms per week 80.
Alternate-day fasting
On typical alternate-day fasting diets, dieters consume 25% of their energy needs on the fast day, and food intake as necessary or desired (ad libitum) the next day 39. Many of the alternate-day fasting studies do not include control groups that undertake other dietary approaches to weight loss, plus the sample sizes have been small (15 to 64 subjects) and the durations short (8 to 12 weeks) 82, 83, 84, 85, 86. However, results to date show similar weight loss and improvements in metabolic factors as compared to studies using other dietary approaches to weight loss, as well as good adherence. For example, Varady et al 82 found that alternate-day fasting was a viable diet option, helping obese patients not only to lose weight, but to also decrease their risk of coronary artery disease (coronary heart disease). Emerging evidence suggests that the relative contribution of fat and carbohydrate in alternate-day fasting diets does not have an impact on weight and blood lipid profiles 87. An alternative fasting regimen that has become popular among some dieters is two days of fasting followed by five days of usual eating. Further research is needed with larger samples, dietary control groups, and longer durations before alternate-day fasting’s widespread use for weight loss purposes 39.
An alternative intermittent fasting regimen that has become popular among some dieters is two non-consecutive days of fasting and five unrestrictive days of usual eating each week 39. This “5:2 Diet”, developed by Dr. Michael Mosley in the United Kingdom, has spread widely throughout Europe, and now the United States. For the two fast days, men are to eat no more than 600 kcals, and women 500 kcals. Usually this consists of a very light breakfast and dinner with little or no lunch 39. Anecdotally, weight loss has been similar to other dietary approaches to weight loss (2 pounds/week) for short terms (6 weeks) 39. However, research is lacking on the “5:2 Diet”, so its long-term safety and efficacy has not been tested, and its appropriateness in varying populations is currently unknown 39.
Intermittent fasting
Intermittent fasting also known as “periodic fasting”, “time‐restricted feeding”, “alternate-day fasting” or “reduced meal frequency”, is when people restrict the time (e.g., 16–48 hours) during the day when they can eat 88, is another way of reducing food intake that is gaining attention as a strategy for weight loss and health benefits. Alternate-day fasting is one type of intermittent fasting that consists of a “fast day” (eating no calories to one-fourth of caloric needs) alternating with a “fed day,” or a day of unrestricted eating. Intermittent fasting focuses on the timing of when you can consume meals either within a day or a week. For example, someone may eat only during a 12-hour time period, such as 7 a.m. to 7 p.m. Skipping meals commonly consists of a daily fast for 16 hours, a 24-hour fast on alternate days, or a fast 2 days per week on non-consecutive days 89. Intermittent fasting is not a diet plan. While it may have some of the same health benefits as a diet, it’s really an eating pattern. It means you fast (don’t eat) during a certain period of time each day (usually an extended period of time). You then eat during another period of time each day (usually a smaller period of time). While you’re fasting, you can drink beverages that don’t contain calories, including water, black coffee, and unsweetened tea. There is still much for scientists and doctors to learn about intermittent fasting. Researchers have conducted only a few studies of intermittent fasting as a strategy for weight loss. They have no long-term data on the safety, how it affects the body and its systems and effectiveness of intermittent fasting for long-term weight maintenance.
Some popular approaches to intermittent fasting include:
- Alternate-day fasting. Eat a normal diet one day and either completely fast or have one small meal (less than 500 calories) the next day.
- 5:2 fasting. Eat a normal diet five days a week and fast two days a week.
- Daily time-restricted fasting. Eat normally but only within an eight-hour window each day. For example, skip breakfast but eat lunch around noon and dinner by 8 p.m.
How fasting and eating is divided each day is called an eating schedule. One of the most common, easy-to-follow schedules is 16:8. This means you fast for a 16-hour period of time and eat your daily meals during an 8-hour period of time. For example, you may want to fast from 7 p.m. until 11 a.m. the next day. You would then eat a healthy lunch and dinner between 11 a.m. and 7 p.m. You wouldn’t eat anything after 7 p.m. until 11 a.m. the next day. This is just an example of times. You can select any 16-hour and 8-hour block of time that works best for your schedule. But it’s important to keep your eating window at the same every day.
Other intermittent fasting schedules include 18:6 (when you fast for 18 hours and eat for 6 hours) or alternating days. With alternating days, you fast for 24 hours, then eat a healthy diet for the next 24 hours, then fast again for the following 24 hours. This schedule continues using the every-other-day format. Another schedule option is 5:2. This is when you fast for two days a week, and eat a normal, healthy diet the other five days. This is a little different, though, as this schedule allows you eat one small meal of 500 to 600 calories on your fasting days.
The time you’re allowed to eat is called your eating window. During your eating window, focus on eating a healthy diet and maintaining portion control. Don’t eat too many calories and avoid junk food and fast food. While you don’t need to eat anything in particular, you do need to make sure you’re getting the nutrition you need. Some people choose to use the Mediterranean diet as a guideline for what to eat. This plan focuses on fruits, vegetables, beans, whole grains, and fish. You can also choose lean proteins and healthy fats.
During fasting, caloric consumption often ranges from zero to 25% of caloric needs 88. Alternative day fasting may consist of 24-hour fasts followed by a 24-hour eating period that can be done several times a week such as a 5:2 strategy when there are 2 fast days mixed into 5 nonrestrictive days 90. For time restricted fast programs, variations include 16-hour fasts with 8 hour feeding times, 20-hour fasts with 4-hour feed times or other similar versions 90. While both caloric restriction and intermittent fasting may result in overall decreased caloric intake, this is not integral to intermittent fasting. Intermittent fasting has been linked to better glucose control in both humans and animals 91. However, long-term adherence to caloric restriction is low while adherence to intermittent fasting may be more promising.
While researchers are still studying intermittent fasting, some research has shown it offers some health benefits. For starters, it’s common to lose weight when following intermittent fasting. That’s because your body is using fat—not glucose—as its energy source. Additionally, if you make wise food choices when you do eat, you’re likely eating fewer calories than before you started intermittent fasting. If you add exercise to the mix, it’s a great combination for not only weight loss, but also improved health benefits. Intermittent fasting may help people who have cardiovascular disease, neurological disorders, and some cancers. Intermittent fasting may also help lower your bad cholesterol and improve symptoms of arthritis.
The majority of studies of intermittent fasting in humans have considered whether intermittent fasting can be a potential strategy to reduce weight and correct adverse metabolic parameters amongst obese and overweight subjects 92. This is important since the problems of long term adherence to continuous calorie restriction for weight management are well known 93. Losing weight and being physically active help lower your risk of obesity-related diseases, such as diabetes, sleep apnea and some types of cancer. For these diseases, intermittent fasting seems to be about as beneficial as any other type of diet that reduces overall calories. Johnson et al. 94 undertook the first trial of intermittent fasting for weight loss amongst 10 obese subjects with asthma which tested alternate days of an 85% energy restricted low carbohydrate diet regimen. This study reported beneficial reductions in serum cholesterol and triglycerides, markers of oxidative stress (8-isoprostane, nitrotyrosine, protein carbonyls, and 4-hydroxynonenal adducts) and inflammation (serum tumor necrosis factor-α) 94. Circulating ketone levels were also elevated on the fasting days 94. In more recent 27 clinical trials, intermittent fasting resulted in weight loss, ranging from 0.8% to 13.0% of baseline body weight 88. Weight loss occurred regardless of changes in overall caloric intake. In the studies of 2 to 12 weeks’ duration, body mass index (BMI) decreased, on average, by 4.3% to a median of 33.2 kg/m². Therefore intermittent fasting shows promise as a primary care intervention for obesity, but little is known about long-term sustainability and health effects. Longer-duration studies are needed to understand how intermittent fasting might contribute to effective weight-loss strategies. Symptoms such as hunger remained stable or decreased, and no adverse events were reported. While intermittent fasting is a moderately successful strategy for weight loss, it shows promise for improving glycemic control, although it does pose a potential risk of hypoglycemia. However, to lose weight and keep it off, the best strategy is to adopt healthy eating and exercise habits that you enjoy so you can stick with them over time.
To get the benefits of intermittent fasting, you need to fast for at least 12 hours. That’s how long it takes your body to switch from using glucose for energy to using fat for energy. Additionally, it will take your body a while to get used to this new eating schedule. So don’t expect results right away. You may need to wait between 2 and 4 weeks to see or feel any results.
It may take 2 to 4 weeks for your body to get used to eating on an intermittent fasting schedule. During those first few weeks, you may have headaches and feel hungry, grouchy, or tired. Know you may feel this way before you start and make a plan to push through these feelings. After a few weeks, your body will get used to this eating pattern and those symptoms should go away. In the end, many people say that feel better following an intermittent fasting lifestyle.
High Protein Weight Loss Diets
High protein weight-loss diets are those that provide more than 1.6 grams per kilogram of desirable weight per day 39. Self-prescribed high protein weight-loss diets vary in their composition from about 28 to 65% of energy, providing 71 to 163 grams of protein per day. High protein weight-loss diets are currently popular as a new strategy for losing weight, and are usually quite low in their carbohydrate content. Some are clearly ketogenic, and severely limit carbohydrates to below 50 grams per day. Examples include the Doctor’s Quick Weight Loss Diet, The Dukan Diet, Dr. Atkins Diet Revolution, The 17 Day Diet and various iterations of the Paleo Diet 39. Diets that are extremely high in protein should not be undertaken for long periods of time, since their long-term safety has not been sufficiently studied.
Other diets are extremely high in protein, very low in carbohydrate and ketogenic, but also very high in fat, is Protein Power 95. Two other high protein diets with enough carbohydrate so that they are not likely to be ketogenic are The Zone and Sugar Busters 39.
Many high protein diets include elaborate instructions that prescribe strict, structured eating schedules, and involve limited food variety and dietary flexibility. The high protein diets that are ketogenic also induce quick initial weight loss because of their low caloric level, and their diuretic effect owing to glycogen depletion, and sodium and water loss 39. They may also be associated with decreased appetite due to the high protein intake, since protein may show to be particularly satiating 96, 97. Ketosis has long been said to reduce appetite, although little data supports this. Nonetheless, for some patients these constraints may help them to achieve and maintain low calorie intakes over the short run.
However, popular high protein weight-loss diets are not risk-free. Many of these high protein weight-loss diets advocate very high intakes of protein from meat and other foods that are also often high in saturated fat, cholesterol and sodium while they are low in dietary fiber, antioxidants, potassium, calcium, magnesium, and some vitamins 39. The purine content of meat, poultry, seafood, eggs, seeds, and nuts is high, and can increases uric acid levels and risk of gout in susceptible individuals 39. The high protein load may also increase urinary calcium loss if it is not buffered 98. In patients with diabetic kidney disease (diabetic nephropathy), very high protein diets may speed progression, although the data are not definitive 99. Because many high protein diets are often by default low in carbohydrate, they also can cause an increase in ketosis. Finally, high protein weight-loss diets do not necessarily promote greater long-term weight loss as compared to other healthier eating options 100, 101, 102.
Weight-loss programs to avoid
A fad weight loss diet is any diet that promises fast weight loss without a scientific basis. These diets often eliminate entire food groups and as a result do not provide a wide range of important nutrients. Fad diets may provide short-term results but they are difficult to sustain and can cause serious health problems. The best approach to weight loss is to follow a long-term, healthy and balanced eating plan and to exercise regularly.
Avoid weight-loss programs that make any of the following promises:
- Lose weight without diet or exercise!
- Lose weight while eating as much as you want of all your favorite foods!
- Lose 30 pounds in 30 days!
- Lose weight in specific problem areas of your body!
Other warning signs to look out for include:
- very small print, asterisks, and footnotes, which may make it easy to miss important information
- before-and-after photos that seem too good to be true
- personal endorsements that may be made up
You can report false claims or scams by weight-loss programs to the Federal Trade Commission (https://www.ftc.gov).
Fad diets often lead to fast weight loss at first. But most of this weight loss is water and lean muscle, rather than fat. When you eat very little, your body begins to break down muscle to meet energy (kilojoule) needs. Unfortunately, this occurs much more easily than the breakdown of fat stores.
Breaking down muscle leads to:
- Water loss, making it seem like you’re losing weight quickly
- A reduced metabolic rate, so when the diet is stopped, it is much easier for your body to gain fat than it was prior to going on the diet.
As a result, over time, people can diet themselves fatter.
Fad diets often encourage a short-term change in eating behavior, rather than encouraging long-term, sustainable changes. It is essential that any diet meets nutritional needs, is practical and suitable for individual lifestyles.
Regular physical activity is important for those wanting to lose weight to help maintain muscle mass.
Healthy Eating Choices
Carbohydrates
Carbohydrates are your body’s fuel. Carbohydrates also play roles in gut health and immune function 103. For healthy children and adults, carbohydrates should make up approximately 45 to 65% of energy intake based on the minimum required glucose for brain function 103. However, some carbohydrates are more nutritious than others.
Foods that contain the most carbohydrates include:
- Fruit.
- Vegetables, especially potatoes and corn.
- Legumes, including dried beans, peas and lentils.
- Grains.
- Bread.
- Breakfast cereal.
- Rice, pasta and noodles.
- Low-fat milk and yoghurt.
These foods are rich in vitamins, minerals and antioxidants and are generally low in fat. This makes them well suited to a healthy eating plan. Some are excellent sources of dietary fibre, including wholegrain varieties, legumes, fruit and vegetables.
Foods with lots of added sugar like soft drinks, alcohol and sweets are another source of carbohydrates, but these contribute extra kilojoules with few vitamins and minerals.
Optimal carbohydrate intake should consist of high fiber, nutrient-dense whole grains, fruits, vegetables and legumes, without the added sugar 36.
The Dietary Guidelines for Americans recommends that carbohydrates should make up 45 to 65% of one’s daily calories 104. To calculate how many grams of carbohydrates you need, multiply your daily calorie requirements by 0.45 and 0.65 to obtain calories from carbohydrates.
- (A) 0.45 x 2000 = 900 calories
- (B) 0.65 x 2000 = 1300 calories
Divide answers in step 1 by 4 since there are 4 calories per 1 gram of carbohydrate
- (A) 900/4 = 225g of carbohydrate
- (B) 1300/4 = 325g of carbohydrate
Carbohydrates are eaten in the form of simple carbohydrates, like monosaccharides and disaccharides, or complex carbohydrates, like oligosaccharides and polysaccharides 103. Monosaccharides are the basic building blocks of all carbohydrates and include glucose, fructose, and galactose. Glucose is the simplest type of carbohydrates and is the major source of energy for your body’s cells 103. Glycogen is the storage form of glucose in animals and is present in the liver and muscle, but there is little to none in the diet.
Disaccharides contain two sugar units and include lactose, sucrose, and maltose. Lactose is a carbohydrate found in milk, and sucrose is basic table sugar.
Oligosaccharides consist of 3 to 10 sugar units and include raffinose and stachyose, which are in legumes.
Polysaccharides include greater than ten sugar units and consist of starches, glycogen, and fibers, like pectin and cellulose. Starches like amylose are in grains, starchy vegetables, and legumes and consist of glucose monomers.
Fibers are plant polysaccharides like pectin and cellulose found in whole grains, fruits, vegetables, and legumes but are not digestible by humans. However, fibers play a major role in gut health and function and can be digested by microbiota (microorganisms) in the large intestine 105. The recommended fiber intake is greater than 38 g for men and 25 g for women, which is the intake that research has observed to lower the risk of coronary artery disease (a heart disease that affects the main blood vessels that supply blood to the heart).
Does eating more carbohydrates cause body fat?
If carbohydrates control body fat, then you would expect that low-carb diets are less “fattening” than higher carbohydrate diets. This means that low carb diets should add less body fat to people than higher carbohydrate diets do. This is true in the most basic sense in that when you overconsume calories (Calorie IN more than Calorie OUT). You do store at least some of the excess calories as body fat. But studies don’t support that view that low-carb diets are less “fattening” than higher carbohydrate diets. It turns out that excess carbohydrates are relatively difficult to store as body fat, at least compared to fats.
In one study where people were overfed carbohydrates and fats, fats were stored ~20% more efficiently than carbs 106. In another study where people were overfed carbohydrates, there was a very minimal conversion of carbohydrates to stored body fat, indicating that it is very inefficient to turn carbohydrates into body fat 107.
Furthermore, low-carb diets are not necessary for weight loss, nor are they alone sufficient for weight loss. Carbs don’t necessarily control body fat after all. Over the last several decades there have been dozens of scientific studies comparing low-carb diets to other diets to examine their efficacy 108. There are plenty of studies whose results do not support the idea that carbohydrates per se control body fat. For example, in one study of 4,451 people, there was a lower risk of being obese or overweight if you consumed a moderate to high carbohydrate diet when compared to a lower carbohydrate diet 109. That study found consuming a low-carbohydrate (approximately <47% energy) diet is associated with greater likelihood of being overweight or obese among healthy, free-living adults 109.
Another study found that there was no real association between BMI and daily carbohydrate intake, suggesting that if carbohydrates did control body fat, it would be a relatively minor effect 110.
Ultimately, science tells us that carbohydrates are not more fattening than fats; in fact, it would make more sense to eat a few too many carbohydrates than a few too many fats. Indeed, this is what you see when you follow people who over-consume carbohydrates versus fats – they tend to gain a little less body fat 111.
Are low-carb diets are better for weight loss than other diets?
The majority of the clinical trials that have examined whether low-carb diets are better than other diets for fat loss show that low-carb diets result in the same amount of weight loss as other diets 112.
When you tightly control people’s diets and measure virtually every part of their metabolism, it is apparent that low-carb diets are not better for weight loss 113. They might be slightly worse for body fat loss than low-fat diets. This holds true even if you go to very low levels of carbohydrate intake 114.
Furthermore, when people adopt a low-carb diet in the real world and over more extended periods, they still see very similar results for weight-loss.
The primary findings from these studies have been:
- Low-carb diets are not necessary for weight loss. Virtually all types of diets can and do result in weight loss when there is a negative energy balance (i.e. an energy deficit).
- From a body fat mass perspective, low-carb diets may result in inferior fat mass reductions in shorter term diets.
- Adherence to low-carb diets is no better or worse compared to most other forms of dieting.
- Low-carb diets often result in more immediate water weight loss and glycogen depletion than moderate-carb diets.
In conclusion, although the idea that carbohydrates control body fat has been popular in the media, there is little scientific evidence to support it. Unless you have extreme levels of carbohydrate intake (Calorie IN more than Calorie OUT), there is no real link between carbohydrates and body fat. From scientific studies, it turns out that carbohydrates are less fattening than dietary fat. When followed in the real-world, low-carb diets can be useful for weight loss, but they are not any more effective than other low calorie diets.
Very low-carb diets can often result in a state called ketosis. This occurs when dietary carbohydrates are low enough, or fat is high enough, such that the body begins producing ketones at a level that allows them to accumulate.
It is often touted that being in a state of ketosis increases fat loss, but there is no good evidence to suggest that is true. In fact, one recent study showed that fat loss is similar, if not inferior, in a state of ketosis 115. If you choose to adopt a low-carb diet, ketosis may be a result of that process, but should not be the primary focus.
Furthermore, there is some evidence that if someone is an athlete engaging in higher intensity, higher volume exercise, ketogenic diets should be avoided as they can impair performance 116, 117.
Very low carbohydrate diets can come with unwanted and potentially dangerous side effects when followed for extended periods. For example, cardiac dysfunction, impairment of physical activity, hair loss, nausea, digestive issues, and lipid abnormalities are all common side effects.
How many carbs should you eat a day to lose weight?
For otherwise healthy individuals with no underlying medical conditions, there does not appear to be a truly minimal amount of carbohydrates that need to be consumed daily.
Your daily recommendations for carb intake are based on two primary criteria:
- Your total daily calorie requirements (your basal metabolic rate [BMR] or resting metabolic rate [RMR])
- Your intensity or volume of physical activity.
Higher total daily calorie needs come with higher recommendations for total daily carb intake, while lower total daily calorie needs come with lower recommendations. Furthermore, as your body relies heavily on carbohydrate intake for moderate to higher intensity physical activity, carb recommendations will increase as your total volume and intensity of activity increase.
Your total daily calorie intake can be estimated using the Mifflin-St Jeor formula above. However, there are also online tools that can be used that can help you determine how many calories you should consume daily. Such as the free online Basal Metabolic Rate (BMR) calculator here: https://www.nasm.org/resources/calorie-calculator
Or the Body Weight Planner (https://www.niddk.nih.gov/health-information/weight-management/body-weight-planner).
The Body Weight Planner allows you to make personalized calorie and physical activity plans to reach a goal weight within a specific time period and to maintain it afterwards.
After that, the number of carbs grams per unit of body weight can be estimated based on current guidelines from the American College of Sports Medicine and the Academy of Nutrition and Dietetics. These recommendations are generalized as follows 118:
- Light Activity: 3-5 g carb/kg/day
- Moderate Activity (1 hour of moderate exercise): 5-7 g carb/kg/day
- High Activity (1-3 hours of intense, endurance exercise): 6-10 g carb/kg/day
- Very High (4-5 hours of intense, endurance exercise): 8-12 g carb/kg/day
It is often recommended that more moderate carbohydrate intakes (1 to 3 g/kg/day) are consumed even in the context of weight loss.
Your muscles need carbs to fuel and recover from your workouts. At least 40% of your total daily calories should come from good carbs. Eat carbs 60 to 90 minutes prior to your workout, and then eat a combo of carbs and protein (2:1 ratio) within an hour after you finish.
Although many nutrition labels count all carbohydrates toward calorie intake, the truth is not all carbohydrates provide a meaningful number of calories as the human body does not digest and extract energy from all forms of carbohydrates.
In most situations, dietary fiber is considered a non-digestible carb and does not contribute to the total carbohydrate intake. As such, in many cases, fiber is subtracted from total carb intake. The grams of fiber is often subtracted from the total carbs grams to yield a total of usable carbs grams. For example, a food label may list 34 g total carbohydrate consisting of 4 g fiber and 6 g added sugar. By subtracting dietary fiber (4 grams of fiber) from total carbohydrates (34 grams) = 30 grams of usable carbs.
Protein
Protein is an essential nutrient that you need throughout life. Proteins are the building blocks of life. Protein is in every cell in your body. The basic structure of protein is a chain of amino acids 119. A protein is a chain of amino acids bound to one another via peptide bonds (chemical bond linking amino acids together to form a protein). When someone eats protein, it is broken down into its amino acids.
Your body needs protein to make, maintain, repair and renew bones, muscles, cartilage, hormones, enzymes, neurotransmitters, vitamins, blood and skin cells 103, 120, 121. Proteins provide energy (calories) if necessary, the others are fat and carbohydrates. Proteins do everything from fighting infections to helping cells divide. Protein is also important for growth and development in children, teens, and pregnant women.
Excess or deficiency of protein can lead to disease, resulting in nervous system defects, metabolic problems, organ failure, and even death 119. Clinical symptoms of inadequate intake of essential amino acids may include depression, anxiety, insomnia, fatigue, weakness, and growth stunting in the young. These symptoms are mostly caused by a lack of protein synthesis in the body because of the lack of essential amino acids 121. Kwashiorkor and marasmus are examples of more severe clinical disorders caused by malnutrition and inadequate intake of essential amino acids as a macronutrient 121.
High protein diets can promote weight loss via increased insulin sensitivity, fatty acid oxidation, appetite suppression, and feeling full. However, caution is necessary for people with diabetes who have gout because protein can elevate niacin levels, which may exacerbate gout-related symptoms.
The protein in your food is broken down into parts called amino acids during digestion. Your body needs a number of amino acids in large enough amounts to maintain good health. While there are hundreds of amino acids, humans use only 20 amino acids 119, 121.
Amino acids are classified into three groups 119:
- Essential amino acids. Essential amino acids cannot be made by your body, and must be supplied by food. Essential amino acids do not need to be eaten at every meal. The balance over the whole day is more important. There are 9 essential amino acids:
- Histidine
- Isoleucine
- Leucine
- Lysine
- Methionine
- Phenylalanine
- Threonine
- Tryptophan
- Valine
- Nonessential amino acids. Nonessential amino acids are made by your body from essential amino acids or in the normal breakdown of proteins. There are 5 amino acids that are termed non-essential amino acids:
- Alanine
- Asparagine
- Aspartic acid
- Glutamic acid
- Serine
- Conditionally Essential amino acids. Conditionally Essential amino acids are needed in times of illness, stress, starvation or inborn errors of metabolism. A healthy body can make conditionally essential amino acids under normal physiologic conditions. There are 6 amino acids that are called conditionally essential amino acids:
- Arginine
- Cysteine
- Glutamine
- Glycine
- Proline
- Tyrosine
You get protein (amino acids) in your diet from animal and plant-based foods such as meat, fish, eggs, dairy products, nuts, and certain grains, beans, peas, and lentils 122. Proteins from meat and other animal products are complete proteins. This means they supply all of the amino acids your body can’t make on its own. Most plant proteins are incomplete. So you should eat different types of plant proteins every day to get all nine essential amino acids your body needs. For example, pairing protein sources like rice and beans, hummus, pita bread, or oatmeal topped with almond butter. Regarding volume, it may be necessary to eat more plant-based foods to get a similar amount of protein and amino acid profile provided by animal-based proteins 123.
- Animal protein – protein-containing foods from animals are meat, chicken, fish, eggs and dairy products. Meat and poultry foods should be lean or low-fat, like 93% lean ground beef, pork loin, and skinless chicken breasts. Choose seafood options that are higher in healthy fatty acids called omega-3s fatty acid and lower in methylmercury, such as salmon, anchovies, and trout. And stay away from processed meats or artificial (fake) meat.
- Vegetable protein – protein-containing foods from plants include tofu, nuts, seeds, lentils, dried beans and peas, and soy milk.
Good protein choices include:- Soy protein
- Beans
- Nuts
- Fish
- Lean chicken with no skin
- Lean beef
- Pork
- Salmon
- Anchovies
- Trout
- Low-fat dairy products
It is important to get enough dietary protein. You need to eat protein every day, because your body doesn’t store it the way it stores fats or carbohydrates. Furthermore, protein foods provide nutrients important for maintaining your health and body. How much protein you need depends on your age, sex, height, weight, health, and level of physical activity. The amount can also depend on whether or not you are pregnant or breastfeeding.
The recommended protein intake is 0.8 to 1 gram per kilogram of body weight per day 124. For strength training athletes adequate protein intake should range between 1.2 and 1.7 grams of protein per kilogram of body weight per day or 0.5 to 0.8 grams per pound of body weight 125, 126, 127, 128.
For healthy children ages 1 to 3 approximately 5 to 20% and children ages 4 to 18 approximately 10 to 30% of daily energy intake should come from protein. The daily recommended intake of protein for healthy adults is 10% to 35% of your daily energy intake based on the adequate amount needed for nitrogen equilibrium 36. One gram of protein supplies 4 calories. Therefore, if you consume 2,000 calories per day, this would work out to be between 200 to 700 calories of protein per day, you could eat 100 grams of protein, or 400 calories from protein, which would supply 20% of your total daily calories.
The recommended daily intakes (RDIs) can also be calculated by your body weight. The Academy of Nutrition and Dietetics recommends that the average individual should consume 0.8 grams of protein per kilogram or 0.35 grams per pound of body weight per day for general health. So a person that weighs 75 kg (165 pounds) should consume an average of 60 grams of protein per day. Since there are approximately four calories per gram of protein, 60 grams of protein would result in the intake of 240 calories.
How much protein do I need?
How much protein you need depends on your age, sex, height, weight, health, and level of physical activity. The amount can also depend on whether or not you are pregnant or breastfeeding. The recommended protein intake is 0.8 to 1 gram per kilogram of body weight per day 124. For strength training athletes adequate protein intake should range between 1.2 and 1.7 grams of protein per kilogram of body weight per day or 0.5 to 0.8 grams per pound of body weight 125, 126, 127, 128.
How to calculate your daily protein needs:
Convert body weight in pounds to kilograms (round to the nearest 10th). Multiply weight in kilograms by the range that best fits your activity levels.
Let’s look at an example:
- Convert pounds into kilograms 150lbs / 2.2 = 68.2kg
The recommended protein intake is 0.8 to 1 gram per kilogram of body weight per day
- 68.2kg (0.8g grams of protein per kilogram) = 54.6g
- 68.2kg (1g grams of protein per kilogram) = 68.2g
For strength training athletes adequate protein intake should range between 1.2 and 1.7 grams of protein per kilogram of body weight per day.
- 68.2kg (1.2g grams of protein per kilogram) = 81.8g
- 68.2kg (1.7g grams of protein per kilogram) = 115.9g
Here are some practical protein equivalents in common foods. One ounce (30 grams) of most protein-rich foods contains 7 grams of protein. An ounce (30 grams) equals:
- 1 oz (30 g) of meat fish or poultry
- 1 large egg has six grams of protein
- ¼ cup (60 milliliters) tofu
- ½ cup (65 grams) cooked beans or lentils
- 1 cup of dry beans has about 16 grams of protein
- 1 cup of milk has eight grams of protein
- 1 cup of soy milk has about seven grams of protein
Low fat dairy is also a good source of protein. An eight ounce container of yogurt has about 11 grams of protein
Most Americans eat enough protein in their diet but need to select leaner varieties of meat and poultry. Americans may also need to increase the variety of protein foods selected and choose meats less often. However, if you are vegetarian or vegan, the advice to eat meat, poultry, and seafood does not apply to you. Vegetarian protein options include beans, peas, lentils, nuts, seeds, and soy products.
What counts as an ounce-equivalent in the protein foods group?
The following examples count as 1 ounce-equivalent from the protein foods group 120:
- 1 ounce of meat, poultry, or fish
- ¼ cup cooked beans
- 1 egg
- 1 tablespoon of peanut butter
- ½ ounce of nuts or seeds
- ¼ cup (about 2 ounces) of tofu
- 1 ounce tempeh, cooked
The table below lists amounts that count as 1 ounce-equivalent in the protein foods group towards your daily recommended amount.
Table 8. Daily protein foods general recommendations by age
| Daily Protein Recommendation* in Ounce-Equivalents | ||
|---|---|---|
| Toddlers | 12 to 23 months | 2 ounce-equivalent |
| Children | 2-3 yrs 4-8 yrs | 2 to 4 ounce-equivalent 3 to 5½ ounce-equivalent |
| Girls | 9-13 yrs 14-18 yrs | 4 to 6 ounce-equivalent 5 to 6½ ounce-equivalent |
| Boys | 9-13 yrs 14-18 yrs | 5 to 6½ ounce-equivalent 5½ to 7 ounce-equivalent |
| Women | 19-30 yrs 31-59 yrs 60+ yrs | 5 to 6½ ounce-equivalent 5 to 6 ounce-equivalent 5 to 6 ounce-equivalent |
| Men | 19-30 yrs 31-59 yrs 60+ yrs | 6½ to 7 ounce-equivalent 6 to 7 ounce-equivalent 5½ to 6½ ounce-equivalent |
How much protein do you need for optimal muscle maintenance?
How much protein you need depends on your age, sex, height, weight, health, and level of physical activity. The amount can also depend on whether or not you are pregnant or breastfeeding. The recommended protein intake is 0.8 to 1 gram per kilogram of body weight per day 124. For strength training athletes adequate protein intake should range between 1.2 and 1.7 grams of protein per kilogram of body weight per day or 0.5 to 0.8 grams per pound of body weight 125, 126, 127, 128.
How to calculate your daily protein needs:
Convert body weight in pounds to kilograms (round to the nearest 10th). Multiply weight in kilograms by the range that best fits your activity levels.
Let’s look at an example:
- Convert pounds into kilograms 150lbs / 2.2 = 68.2kg
The recommended protein intake is 0.8 to 1 gram per kilogram of body weight per day
- 68.2kg (0.8g grams of protein per kilogram) = 54.6g
- 68.2kg (1g grams of protein per kilogram) = 68.2g
For strength training athletes adequate protein intake should range between 1.2 and 1.7 grams of protein per kilogram of body weight per day.
- 68.2kg (1.2g grams of protein per kilogram) = 81.8g
- 68.2kg (1.7g grams of protein per kilogram) = 115.9g
Muscle mass is built when the net protein balance is positive: that is muscle protein synthesis exceeds muscle protein breakdown. Research shows muscle protein turnover is the greatest after working out. Additionally, it has been shown that muscle mass increases over time when resistance exercise (i.e. weight lifting, body weight exercises, etc) is combined with nutrient intake.
However, as you age, you need to increase your protein intake 125. Around 50 years of age, you need to increase the protein in your diets to 1 gram per kilogram of your body weight to maintain muscle mass 125. People that exercise regularly also need to eat more protein than the recommended daily intake 125.
Several studies performed by the group of Philip and others showed that protein supplementation did not further increase muscle strength among individuals who consumed adequate amounts of dietary protein 128, 129, 126, 130. However, with the aim of maximizing performance, individuals seeking to gain muscle mass are likely to consume more protein with the misconceived belief that large quantities of protein consumption might generate more muscle protein 131.
To increase muscle mass in combination with physical activity, it is recommended that a person that lifts weights regularly or is training for a running or cycling event eat a range of 1.2 to 1.7 grams of protein per kilogram of body weight per day, or 0.5 to 0.8 grams per pound of body weight 125. Consequently, the same 75
kilogram individual should increase their protein intake to 75 grams (300 calories) to 128 grams (512 calories) in order to gain muscle mass. This level of intake can generally be met through diet alone and without additional protein and amino acid supplementation 125.
When should I consume protein?
The process of protein turnover is increased with resistance training and can remain elevated for up to 48 hours in people beginning a new resistance training program 125. Therefore it is important to provide enough energy including protein so there is a sufficient pool of amino acids available to repair and build new muscle. You do not want to exercise on an empty stomach. In fact, exercising in an unfed state leads to an increase in protein loss making it more difficult for your body to both repair and build muscle 125. Your body can only use approximately 20–40 g of protein per meal. For best results, eat around this much protein every 3 to 4 hours.
Research suggests there are several benefits to pre-exercise protein supplementation 125. Pre-exercise protein supplementation helps to improve body composition by increasing resting energy expenditure up to 48 hours after exercise 125. This is important because it suggests that pre-exercise protein ingestion will not only help increase lean muscle mass and strength, but will also simultaneously reduce fat mass 125. However, the most scientifically supported and most significant benefits of consuming protein prior to exercise may be improved recovery and hypertrophy. This is thought to occur because of improved amino acid delivery 125.
Make sure you have a healthy diet that meets the current protein intake recommendations and then use supplements to add anything else you might need. A good diet will not make a mediocre athlete into a champion, but poor food choices can turn a champion into a mediocre athlete. The International Olympic Committee (IOC) position stand is that “the use of supplements does not compensate for poor food choices and an inadequate diet”. Reinforcing this importance of food, researchers have found that athletes eating a diet rich in nitrates from vegetables (not supplements) for just 10 days were able to enhance their exercise performance, compared to when they were eating their usual diet 132.
Protein supplement
Protein supplementation has been shown to improve muscle building with regular exercise training. Protein supplementation should contain a high amount of the amino acid leucine, which is responsible for muscle protein synthesis. Whey protein is a great option for leucine. Eating less protein may not be enough to rebuild muscles, and eating more doesn’t usually give you more benefits.
Whey protein is beneficial in supporting muscle adaptations due to its rapid absorption rate in addition to casein that has a slower and more sustained rate of amino acid absorption over a few hours 125. Branched chain amino acids are similarly beneficial and have been shown to aid in recovery from exercise with respect to not only protein synthesis but also aiding in replacing our muscle glycogen and delaying fatigue associated with exercise.
Protein supplementation after exercise may have a more profound impact on skeletal muscle hypertrophy. Several studies have demonstrated that protein ingestion following an acute bout of resistance training stimulates muscle protein synthesis for up to three hours 125. In contrast, failing to eat after exercise
may limit protein synthesis and therefore limit potential progress in lean muscle tissue development. Research actually suggests there may be an “anabolic window” such that protein intake within an hour of exercise has the greatest influence on resistance training adaptations 125.
Generally, naturally occurring animal proteins contain 2:1:1 ratio of leucine, isoleucine and valine. These proteins have been identified as providing optimal support of muscle adaptations with exercise training. In order to meet the recommended RDA a consumption of approximately 45 mg/kg/day of leucine and 22.5 mg/kg/day of isoleucine and valine is suggested 125.
What is the best protein powder supplement?
Creatine monohydrate is generally safe and can help you build more muscle mass 133, 134, 135, 136, 137, 138. Always check with your doctor before starting any supplement.
Creatine (N-[aminoiminomethyl]-N-methyl glycine) is an amino acid–like compound that is produced in your liver, kidney, pancreas, and possibly the brain from the biosynthesis of the essential amino acids methionine, glycine, and arginine, or obtained from dietary sources 139. The primary dietary sources are high-protein foods including meat, fish, and poultry. Once synthesized or ingested, creatine is transferred from the plasma through the intestinal wall into other tissues by specific creatine transporters located in skeletal muscles, the kidney, heart, liver, and brain.
Creatine as a dietary supplement is a tasteless, crystalline powder that readily dissolves in liquids and is marketed as creatine monohydrate or as a combination with phosphorous 140. The majority of creatine (95%) is stored in skeletal muscle (fast twitch, type 2): two-thirds in a phosphorylated form and one-third as free creatine 141. Creatine serves as an energy substrate for the contraction of skeletal muscle. The intention of creatine supplementation is to increase resting phosphocreatine levels in muscles, as well as free creatine, with the goal of postponing fatigue, even briefly, for sports-enhancing results 133.
Creatine is one of the most widely used dietary supplements. Athletes, body builders, and military personnel use creatine to enhance muscle mass and increase strength. Creatine is also used as an ergogenic aid to improve performance of high-intensity exercise of short duration 142, 143, 144. Creatine’s popularity as a dietary supplement was further increased by a 2006 study demonstrating its positive effect on cognitive and psychomotor performance 145.
Experiments among athletes and military personnel indicate that creatine taken at levels commonly available in supplements produces minimal, if any, side effects 144, 146. Using evidence from well-designed, randomized controlled human clinical trials of creatine, Shao and Hathcock 146 concluded that chronic intake of 5 g/ day of creatine was safe and posed no significant health risks.
Muscle creatine concentrations are increased by 20% with creatine monohydrate supplementation 141. Creatine monohydrate supplements increase lean body mass, as well as strength, power and effectiveness in short-duration, high-intensity exercises 147. The increase in body mass may be a result of the increase in intracellular water related to the osmotic properties of creatine 148. Studies on creatine monohydrate supplementation have shown short-duration improvements in sports performance and strength: specifically, in maximum-intensity exercises, muscle power, number of repetitions, muscle endurance, speed and total strength 149.
The use of creatine monohydrate can yield increases in power during short sprints of maximum intensity, which can be even more evident when repeated sprints are accompanied by short recovery periods 138. Furthermore, with creatine monohydrate supplementation, effects are also observed in muscle glycogen stores 148. This is important because the availability of muscle glycogen is the main determinant of sports performance in resistance exercises, and its depletion can lead to muscle fatigue 150. In addition, creatine monohydrate is one of the few sports foods supplements or ergogenic aids (substance used for the purpose of enhancing performance) with health claims authorised by the EFSA and the European Commission (EC), due to its evident effects on the health and sports performance of athletes 151, 152.
The approved health claims are ‘Creatine increases physical performance in repeated bursts of high-intensity exercise in the short term’ and ‘Daily creatine consumption can enhance the effect of resistance training on muscle strength in adults over the age of 55’. These health claims refer to the 3-g dose of creatine monohydrate 152. Resistance training should be performed at least three times per week for several weeks, at an intensity of at least 65–75% of one repetition maximum (1RM). The target population is adults over the age of 55, who are engaged in regular resistance training 152. Creatine in combination with resistance training and improvement in muscle strength 152.
Fat
You need to eat some fat even when you are trying to lose weight. The human body needs small amounts (3 to 6 grams) of essential fatty acids (Omega-6 and Omega-3 fatty acids). Fat is important for many body processes. Fat helps your body absorb nutrients and move nutrients around your body. Some fat is necessary as a carrier for the fat-soluble vitamins A, D, E, and K. Fat is the main source of energy storage in your body, fat contributes to cellular structure and function, fat keeps you warm, and protects your organs 153, 154, 155. Fat also helps with hormone production. Therefore your diet should not be devoid of fat. However, because fat is calorically dense (1 gram of fat has 9 calories of energy), it is often decreased on weight-loss diets to reduce energy intake.
Fat needs will vary by individual and will depend largely on your body composition goals and body types. For example, dietary fat recommendations are slightly higher in competitive athletes than non-athletes to promote health, maintain healthy hormone function, and maintain energy balance. Typical recommendations for athletes are 30 to 50% of total energy intake.
There are 4 main types of fats:
- Unsaturated fats are those that are liquid at room temperature. Examples include olive, peanut, and canola oils. We want to include as many unsaturated fats in our diet because they can decrease bad cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 and omega-6 fatty acids. Unsaturated fats are typically classified by how many hydrogen bonds they have in their structure: either 1 (mono) or two or more (poly).
- Monounsaturated fats. Monounsaturated fat is a type of unsaturated fat. Monounsaturated fats are liquid at room temperature but start to harden when chilled. Monounsaturated fats is one of the healthy fats, along with polyunsaturated fat. Monounsaturated fats are good for your health in several ways:
- Monounsaturated fats can help lower your LDL (bad) cholesterol level. Cholesterol is a soft, waxy substance that can cause clogged, or blocked, arteries (blood vessels). Keeping your LDL level low reduces your risk for heart disease and stroke.
- Eating plant foods high in monounsaturated fats, particularly extra virgin olive oil and tree nuts, may benefit heart health and blood sugar regulation. Monounsaturated fats from plants may lower bad cholesterol and raise good cholesterol. They also may improve the control of blood sugar levels. Replacing saturated fats with monounsaturated fats in your diet may lower the level of bad cholesterol and triglycerides in your blood. Triglycerides are fat cells that circulate in the bloodstream and are stored in the body’s fat cells. A high level of triglycerides in the blood increases the risk of diseases of the heart and blood vessels.
- Monounsaturated fats help develop and maintain your cells.
- Monounsaturated fats are found in plant foods, such as nuts, avocados, and vegetable oils. Monounsaturated fats are found in red meats and dairy products. About half the fats in these foods are saturated and half monounsaturated. Many plants and plant oils are high in monounsaturated fats but low in saturated fats. These include:
- Oils from olives, peanuts, canola seeds, safflower seeds, and sunflower seeds.
- Avocadoes.
- Pumpkin seeds.
- Sesame seeds.
- Almonds.
- Cashews.
- Peanuts and peanut butter.
- Pecans.
- Polyunsaturated fats. Polyunsaturated fat is a type of unsaturated fat. Polyunsaturated fats are liquid at room temperature but start to harden when chilled. Polyunsaturated fats include omega-3 and omega-6 fats. These are essential fatty acids that your body needs for brain function and cell growth. Your body does not make essential fatty acids, so you must get them from food. Polyunsaturated fats can help lower your LDL (bad) cholesterol. Cholesterol is a soft, waxy substance that can cause clogged or blocked arteries (blood vessels). Having low LDL cholesterol reduces your risk for heart disease. Polyunsaturated fats is one of the healthy fats, along with monunsaturated fat. Polyunsaturated fat is found in plant and animal foods, such as salmon, vegetable oils, and some nuts and seeds.
- Omega-3 fatty acids are good for your heart in several ways. They help:
- Reduce triglycerides, a type of fat in your blood
- Reduce the risk of developing an irregular heartbeat (arrhythmia)
- Slow the buildup of plaque, a substance comprising fat, cholesterol, and calcium, which can harden and clog your arteries
- Slightly lower your blood pressure
- Sources of omega-3 fatty acids include:
- Fish such as salmon, anchovies, mackerel, herring, sardines and tuna.
- Oils from canola seeds, soybeans, walnuts and flaxseed.
- Soybeans.
- Chia seeds.
- Flaxseed.
- Walnuts.
- Omega-6 fatty acids may help:
- Control your blood sugar
- Reduce your risk for diabetes
- Lower your blood pressure
- Sources of omega-6 fatty acids include:
- Corn oil.
- Cottonseed oil.
- Peanut oil.
- Soybean oil.
- Sunflower oil.
- Omega-3 fatty acids are good for your heart in several ways. They help:
- Saturated fats. Saturated fats are those that are solid at room temperature. Examples include margarine, butter, whole fat dairy products, the fat marbling in meats, and coconut oil. Saturated fats don’t need to be avoided entirely, but diets high in saturated fats can increase bad cholesterol and triglycerides, increasing the risk for heart disease. The Dietary Guidelines for Americans suggest that less than 10% of calories a day should be from saturated fats. The American Heart Association recommends that saturated fats only make up 5 to 6% of your daily calories. For a 2,000 calorie diet, that is a total of 100 calories, or 11 grams a day. Foods high in saturated fats include:
- Foods baked or fried using saturated fats.
- Meats, including beef, lamb, pork as well as poultry, especially with skin.
- Lard.
- Dairy products like butter and cream.
- Whole or 2% milk.
- Whole-milk cheese or yogurt.
- Oils from coconuts, palm fruits, or palm kernels.
- Trans fats. Trans fatty acids are unhealthy fats that form when vegetable oil goes through a process called hydrogenation. This leads the fat to harden and become solid at room temperature. Hydrogenated fats, partially hydrogenated oils (PHOs) or “trans fats,” are often used to keep some foods fresh for a long time. Trans fats are unsaturated fats that are artificially turned into saturated fats and increase heart disease and stroke risk by raising bad LDL cholesterol and decreasing good HDL cholesterol levels. High LDL (bad) cholesterol along with low HDL (good) cholesterol levels can cause cholesterol to build up in your arteries (blood vessels). This increases your risk for heart disease and stroke. Trans fats have also been known to increase the risk of developing type 2 diabetes. Trans fats are most commonly found in fried foods, frozen baked products such as pizza, non-dairy coffee creamers, vegetable shortenings, some margarines, crackers, cookies, snack foods, and other foods made with or fried in partially hydrogenated oils (PHOs). Because of the health risks from trans fats, the United States Food and Drug Administration (FDA) has banned food manufacturers from adding partially hydrogenated oils (PHOs) to foods. Although the food industry has greatly reduced the use of trans fat in recent years, trans fat may still be found in many fried, packaged, or processed foods. There are very small amounts of naturally occurring trans fat in meats and dairy from grazing animals, such as cows, sheep and goats. You should avoid foods made with hydrogenated and partially hydrogenated oils (such as hard butter and margarine). They may contain high levels of trans fatty acids. It is important to read nutrition labels on foods. This will help you know what kinds of fats, and how much, your food contains.
How much fat do I need?
To prevent any fatty acid deficiencies it is recommended that you consume at minimum 1g of fat per kg of body weight per day. According to the Dietary Guidelines for Americans 104, fats should make up 20 to 35% of your total daily calorie intake. For those attempting to lose body fat, 0.5 to 1 fat per kg of body weight per day should be consumed per day to avoid essential fatty acid deficiency. For healthy children ages 1 to 3, ages 4 to 18, and adults, approximately 30 to 40%, 25 to 15%, and 20 to 35% of daily energy intake should come from fat, respectively 103. Approximately 5 to 10% of your daily fat energy intake should consist of Omega−6 fatty acids (linoleic acid) and 0.6 to 1.2% of Omega−3 fatty acids (alpha-linolenic acid, eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) 36. Both omega−6 fatty acids (linoleic acid) and omega−3 fatty acids (alpha-linolenic acid, eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) are considered essential fatty acids, meaning that they must be obtained from your diet 156. Apha-linolenic acid can be converted into eicosapentaenoic acid (EPA) and then to docosahexaenoic acid (DHA), but the conversion (which occurs primarily in your liver) is very limited, with reported rates of less than 15% 157, 158. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are essential fatty acids, meaning the body can’t produce them and they must come from your diet 159. Therefore, consuming eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) directly from foods and/or dietary supplements is the only practical way to increase levels of these fatty acids in your body.
Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are omega-3 fatty acids found in varying amounts in seafood such as cold-water fish like salmon, tuna, herring, and mackerel, as well as in fish oil supplements and seaweed. Eating 8 ounces per week of seafood may help reduce the risk for heart disease.
Some researchers propose that the relative intakes of omega-6s and omega-3s, the omega-6/omega-3 ratio, may have important implications for the cause of many chronic diseases, such as heart and blood vessels disease (cardiovascular disease) and cancer 160, but the optimal ratio, if any, has not been defined 161. Others have concluded that the omega-6/omega-3 ratios are too nonspecific and are insensitive to individual fatty acid levels 162, 163, 164.. Most agree that raising EPA and DHA blood levels is far more important than lowering linoleic acid or arachidonic acid levels 158.
For someone who weighs 150lbs (68kg), this would equate to 34-68g fat per day. Using both of these references you can calculate your daily fat needs:
To calculate your daily fat needs:
- Convert body weight in pounds to kilograms (round to the nearest 10th). Multiply weight in kilograms by 1.
Let’s look at an example:
- Convert pounds into kilograms 150lbs / 2.2 = 68.2kg
The recommended fat intake is 1 gram per kilogram of body weight per day
- 68.2kg (1g grams of fat per kilogram) = 68.2g of fat per day
Weight loss diets that are moderate to low in fat (20 to 30% of calories) are called “balanced deficit” diets because they maintain a reasonable balance among macronutrients similar to that recommended in MyPlate, DASH, and the Dietary Guidelines for Americans 104, 81. They tend to achieve most of the caloric deficit by reducing fat from the typical level in North American Diets of about 34% or more of calories to 20 to 30% fat, 15% protein, and 55 to 65% of calories from carbohydrates. Some examples of low fat diets are the Weight Watchers Diet (25% fat, 20% protein, and 55% carbohydrate, with 26 grams of dietary fiber), Jenny Craig, the National Cholesterol Education Program Step 1 diet (25% fat), diets based on the MyPlate, the DASH diet, the Shape up and Drop 10 diet of Shape Up! America and the Nutrisystem diet 39. Popular diet books using this approach include The Biggest Loser Diet, The Mayo Clinic Diet and The Engine 2 Die 39. These dietary patterns have been extensively reviewed and appear to be effective for weight reduction on low calorie diets for most individuals 39.
Very low-fat diets such as the Pritikin Diet 165, the Ornish Diet 166 and The Spark Solution Diet 167 have been advocated not only for weight reduction, but also for improving cardiovascular risk profiles. The Ornish Diet 166, which is very low in fat (13% of calories) and saturated fat, very high in carbohydrate (81% of calories) and very high in fiber (38 grams), is part of a program that includes nonsmoking, exercise and behavior modification. The Ornish Diet 166 was shown to reduce some cardiovascular risk factors in a limited long term study. For those who can adhere to the Ornish regime it may be helpful. However, it may not be appropriate for all populations, such as diabetics.
What are Healthy fats?
Healthy fats include:
- Monounsaturated fats
- Polyunsaturated fats (omega-3 and omega-6).
The healthier fats are unsaturated fats. They can be found in sunflower oil, safflower oil, peanut and olive oils, poly- and mono-unsaturated margarine spreads, nuts, seeds and avocado. These are much better for you than the saturated fat found in butter, cream, fatty meats, sausages, biscuits, cakes and fried foods.
Foods that contain healthy monounsaturated fats include:
- Avocados and their oils/spreads
- Unsalted nuts such as almonds, cashews and peanuts and their butters/spreads
- Olives and their oils/spreads
- Cooking oils made from plants or seeds, including: olive, canola, peanut, sunflower, soybean, sesame and safflower.
Foods that contain healthy polyunsaturated fats (omega-3 and omega-6) include:
- Oily fish like salmon, mackerel and sardines
- Tahini (sesame seed spread)
- Linseed (flaxseed) and chia seeds
- Soybean, sunflower, safflower, canola oil and margarine spreads made from these oils
- Pine nuts, walnuts and brazil nuts.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
What are Unhealthy fats?
Unhealthy fats include:
- Saturated fat
- Trans fat
Foods rich in unhealthy fats include:
- Animal fats including butter, ghee and lard along with the visible fat/skin on meat
- Hydrogenated plant oils like copha, vegetable shortening and some margarines
- Coconut oil
- Processed foods such as baked goods (cakes, biscuits and pastries), processed meat ( bacon, sausages, salami) and fried and takeaway foods.
Replace foods rich in saturated and trans fats with foods rich in healthy unsaturated fats as part of a healthy diet.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
Vitamins and minerals
An optimal diet generally provides all the vitamins, minerals, and other micronutrients needed for good health. However, many women in the U.S., and a very large percentage of poor women, do not follow optimal diets 168. Thus, for most women a daily multivitamin-multimineral supplement provides good insurance against nutritional deficiencies. Such supplements usually include extra iron, which is needed by the 9% to 11% of premenopausal women with iron deficiency 169.
The most firmly established benefit of vitamin supplements is that additional folic acid can reduce the risk of neural tube defects by approximately 70% 170. Current guidelines call for all women of childbearing age to take a daily supplement containing 400 to 800 micrograms (μg) of folic acid, or 4 milligrams (mg) for women with a child with a neural tube defect.
Calcium is important for the maintenance of bone strength. Precisely how much calcium is needed is a controversial question. World Health Organization guidelines recommend an intake of 400 mg/day. In the United Kingdom, 700 mg/day is considered adequate for women aged 19 years and older. In the United States, dietary guidelines recommend that adult women receive 1,500 mg of calcium daily 171, in large part by consuming 3 servings of low-fat or fat-free dairy products a day 172. A lower-calorie, no-fat option is to get calcium from supplements.
For maintaining bone strength, other factors—including physical activity and vitamin D—are as important, or more important, than calcium. There is mounting evidence that current recommendations for vitamin D (200–600 IU/day, depending on age) are too low, and that 1,000 IU/day provides better protection against fractures and possibly heart disease and some cancers 173 (see Vitamin D). Excess intake of preformed vitamin A (retinol) has been associated with an increased risk of hip fracture, possibly by competing with vitamin D 174. However, elevated risk is seen at intakes slightly higher than the current Dietary Reference Intake of 700 μg per day. Given this concern, a multivitamin that delivers much of its vitamin A as beta-carotene is preferred.
Weight loss exercise
Regular physical activity is one of the most important things you can do to improve your health. Being active may help you live longer and protect you from developing serious health problems, such as type 2 diabetes, heart disease, stroke, and certain types of cancer.
Regular physical activity is linked to many health benefits, such as 175:
- lower blood pressure and blood glucose, or blood sugar
- healthy bones, muscles, and joints
- a strong heart and lungs
- better sleep at night and improved mood.
A 2013 report estimated that 18.2% of deaths annually in the United States (approximately 465,000 deaths) could be attributable to overweight and obesity 176. Another 2013 article asserted that there is no such thing as “healthy obesity” 177.
Moving more and sitting less have tremendous benefits for everyone, regardless of age, sex, race, ethnicity, or current fitness level 178. Individuals with a chronic disease or a disability benefit from regular physical activity, as do women who are pregnant 178. The scientific evidence showed physical activity is linked with even more positive health outcomes than previously thought with benefits even with small amounts physical activity. The Physical Activity Guidelines for Americans, 2nd edition 178, define regular physical activity as at least 150 minutes a week of moderate-intensity aerobic activity, such as brisk walking. Brisk walking is a pace of 3 miles per hour or faster. A moderate-intensity activity makes you breathe harder but does not overwork or overheat you. You should also do muscle-strengthening activities at least 2 days a week.You may reach this goal by starting with 5 minutes of physical activity several times a day, 5 to 6 days a week. You could then gradually work up to 10 minutes per session, 3 times a day. If you do even more activity, you may gain even more health benefits 179.
For most healthy adults, the Department of Health and Human Services recommends these exercise guidelines:
- Aerobic activity. Get at least 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity a week, or a combination of moderate and vigorous activity. The guidelines suggest that you spread out this exercise during the course of a week. Greater amounts of exercise will provide even greater health benefits. But even small amounts of physical activity are helpful. Being active for short periods of time throughout the day can add up to provide health benefits.
- Strength training. Do strength training exercises for all major muscle groups at least two times a week. Aim to do a single set of each exercise, using a weight or resistance level heavy enough to tire your muscles after about 12 to 15 repetitions.
When combined with healthy eating, regular physical activity may also help you control your weight. However, research shows that even if you can’t lose weight or maintain your weight loss, you still can enjoy important health benefits from regular physical activity 180, 175.
Physical activity also can be a lot of fun if you do activities you enjoy and are active with other people. Being active with others may give you a chance to meet new people or spend more time with family and friends. You also may inspire and motivate one another to get and stay active.
How much physical activity should I do to lose weight?
Physical activity is important in weight loss and all weight loss programs should include physical activity. If left on their own, most dieters become more sedentary during weight loss, especially if their diets are very low in calories 39. This is because a markedly negative energy balance reduces your exercise tolerance, your body’s maximal power output and increases your body’s sense of perceived exertion 181. Therefore, conscious efforts to increase physical activity while dieting should be attempted.
According to the 2008 Physical Activity Guidelines for Americans, recommendations for weight loss include engaging in 45 to 75 minutes of moderate-intensity activity per day 182. This can include activities such as walking at least three miles per hour, participating in water aerobics, ballroom dancing, or gardening. Alternatively, individuals could instead participate in 22 minutes of vigorous activity per day, such as swimming, jogging, jumping rope, or hiking. However, physical activity alone, without a reduction of calories, only induces modest reductions in body weight 39. Few studies to date have incorporated enough physical activity to achieve even a 5% weight loss using a physical activity intervention alone 39. When physical activity is paired with calorie restriction, it has a synergistic effect on weight loss 39. Despite physical activity modest effects on weight loss, physical activity is also essential for improving health-related outcomes relevant to many obesity related medical conditions (e.g., heart disease, type 2 diabetes, and possibly some cancers) 183. Physical activity is also vital in preventing weight regain and may enhance quality of life 183. There is a strong association between physical activity at follow-up and maintenance of weight loss. Data from the National Weight Control Registry, a registry of more than 3,000 individuals who have successfully maintained at least a 30-pound weight loss for a minimum of one year, shows that 90% of the individuals report that physical activity is crucial to their long-term weight maintenance. They report expending, on average, 2,700 calories per week in exercise, the energy equivalent of walking four miles seven days a week 71.
Once you lose weight, physical activity and exercise are still important for maintaining weight loss. For weight maintenance, 60 minutes of moderate activity per day or 30 minutes of vigorous activity per day is recommended 39. In addition, weight resistance activities, which involve all the major muscle groups, are recommended for two or more days per week 39. Resistance training increases muscle strength by making your muscles work against a weight or force. Different forms of resistance training include using free weights, weight machines, resistance bands, your own body weight or any other object that causes your muscles to contract.
Recent evidence supports the benefits of resistance training in increasing and/or maintaining lean body mass and bone mineral density 184, 185 and highlights their effects on muscular strength and muscle building 186, 187. Muscle building occurs when the size and/or number of myofibrils (actin and myosin) within a muscle fiber increases. It’s more common in fast-twitch muscles than slow-twitch muscles, and Type 2A fibers grow the most. Muscle building is a slow process. When you lift heavy weights, your muscles tear and your body experiences metabolic stress. In response, your body tells the proteins to increase, and your muscles slowly grow 188.
Exercise and weight maintenance
The American College of Sports Medicine position stand on physical activity intervention strategies to promote weight loss and weight regain emphasize the distinction between the minimum levels of physical activity to maintain health (150 minutes per week) and higher levels of physical activity to prevent weight regain (200 minutes per week) 62. Therefore, obese individuals who have successfully lost weight require a substantial amount of physical activity to maintain this weight loss 62. As indicated in the American College of Sports Medicine position, several major limitations to research of physical activity on weight regain exist including the observational and the retrospective nature of the existing literature from randomized trials 62. However, several studies in this area deserve mentioning. Using data from a physical activity weight loss study, Jakicic et al. 189 observed a dose response between the amount of self-reported physical activity per week and long-term success with weight loss at 18 months of intervention (composed of caloric restriction and exercise training). Adults who exercised greater than 200 minutes per week (−13.1 kg) lost more weight compared to those who exercised between 150-199 min per week (−8.5 kg), and those that exercised less than 150 minutes week (−3.5 kg) 189. A different study by Jakicic et al. 190 observed similar findings in post hoc analyses of a weight loss intervention composed of both caloric restriction and exercise training in women. After 12 months of intervention, women with greater than 200 min/week (13.6%) had maintained significantly greater percentage of weight loss compared to those who had exercised at 150-199 min/week (9.5%), and less than 150 min/week (4.7%). Lastly, Andersen et al. 191 evaluated the effect of low-fat diet (1200 kcals/day) in combination with either structured aerobic exercise training or lifestyle activity (patients were advised to increase their physical activity to recommended levels), and both groups lost approximately 8 kg of weight following 16 weeks of intervention. Weight maintenance was monitored for 1 year after the intervention, and those who were the most active lost additional weight (1.9 kg) whereas the group that was the least active regained a substantial amount of weight (4.9 kg). These data suggest that physical activity has an important role in the amount of weight regain following successful weight loss. Therefore patients attempting to reduce recidivism after weight loss are encouraged to engage in physical activity levels above 200 minutes/week 62.
What kinds of physical activities can I do?
You don’t need to be an athlete or have special skills or equipment to make physical activity part of your life. Many types of activities you do every day, such as walking your dog or going up and down steps at home or at work, may help improve your health. Try different activities you enjoy. If you like an activity, you’re more likely to stick with it. Anything that gets you moving around, even for a few minutes at a time, is a healthy start to getting fit.
The four main types of physical activity are aerobic, muscle-strengthening, bone-strengthening, and stretching. Aerobic activity is the type that benefits your heart and lungs the most. Table 4 summarizes the expected weight change from different exercise training programs in obese patients and describe the overall likelihood for clinically significant weight loss.
A well-known physiologic effect of exercise or physical activity is that it expends energy. A metabolic equivalent of task or MET, is a unit useful for describing the energy expenditure of a specific physical activity. A MET is the ratio of the rate of energy expended during an activity to the rate of energy expended at rest. For example, 1 MET is the rate of energy expenditure while at rest. A 4 MET activity expends 4 times the energy used by the body at rest. If a person does a 4 MET activity for 30 minutes, they have done 4 x 30 = 120 MET-minutes (or 2.0 MET-hours) of physical activity. A person could also achieve 120 MET-minutes by doing an 8 MET activity for 15 minutes.
Table 4. Expected weight loss from different modalities of exercise training
| Exercise modality | Weight Loss | Clinically significant weight loss |
| Pedometer-based step goal | Range: 0 to 1 kg of weight loss | Unlikely |
| Aerobic Exercise Training only | Range: 0 to 2kg of weight loss | Possible, but only with extremely high exercise volumes |
| Resistance Training only | None | Unlikely |
| Aerobic and Resistance training only | Range: 0 to 2kg of weight loss | Possible, but only with extremely high volumes of aerobic exercise training |
| Caloric restriction combined with aerobic exercise training | Range: −9 kg to −13 kg | Possible |
Walking
Walking is free and easy to do—and you can do it almost anywhere. Walking will help you:
- burn calories
- improve your fitness
- lift your mood
- strengthen your bones and muscles
You can download fitness apps that let you enter information to track your progress using a computer or smart phone or other mobile device.
Devices you can wear, such as pedometers and fitness trackers, may help you count steps, calories, and minutes of physical activity. Trackers can help you set goals and monitor progress. You wear most of these devices on your wrist like a watch, or clipped to your clothing.
Keeping an activity journal is another good way to help you stay motivated and on track to reach your fitness goals.
If you are concerned about safety, try walking in a shopping mall or park where it is well lit and other people are around. Many malls and parks have benches where you can take a quick break. Walking with a friend or family member is safer than walking alone and may provide the social support you need to meet your activity goals.
If you don’t have time for a long walk, take several short walks instead. For example, instead of a 30-minute walk, add three 10-minute walks to your day. Shorter spurts of activity are easier to fit into a busy schedule.
Aerobic exercise
Aerobic exercise is also called endurance activity, moves your large muscles, such as those in your arms and legs. Running, swimming, walking, bicycling, dancing, and doing jumping jacks are examples of aerobic activity. Aerobic exercise makes your heart beat faster than usual. You also breathe harder during this type of activity. Over time, regular aerobic activity makes your heart and lungs stronger and able to work better.
Below are examples of aerobic activities. Depending on your level of fitness, they can be light, moderate, or vigorous in intensity:
- Pushing a grocery cart around a store
- Gardening, such as digging or hoeing that causes your heart rate to go up
- Walking, hiking, jogging, running
- Water aerobics or swimming laps
- Bicycling, skateboarding, rollerblading, and jumping rope
- Ballroom dancing and aerobic dancing
- Tennis, soccer, hockey, and basketball
You can do aerobic activity with light, moderate, or vigorous intensity. Moderate- and vigorous-intensity aerobic exercises are better for your heart than light-intensity activities. However, even light-intensity activities are better than no activity at all.
The level of intensity depends on how hard you have to work to do the activity. To do the same activity, people who are less fit usually have to work harder than people who are more fit. So, for example, what is light-intensity activity for one person may be moderate-intensity for another.
Absolute rates of energy expenditure during physical activity are commonly described as light, moderate, or vigorous intensity. Energy expenditure is expressed by multiples of the metabolic equivalent of task (MET), where 1 MET is the rate of energy expenditure while sitting at rest.
- Light-intensity activity
- Light-intensity activities are common daily activities that don’t require much effort.
- Light-intensity activity is non-sedentary waking behavior that requires less than 3.0 METs; examples include walking at a slow or leisurely pace (2 miles per hour [mph] or less), cooking activities, or light household chores.
- Moderate-Intensity activity
- Moderate-intensity activities make your heart, lungs, and muscles work harder than light-intensity activities do.
- On a scale of 0 to 10, moderate-intensity activity is a 5 or 6 and produces noticeable increases in breathing and heart rate. A person doing moderate-intensity activity can talk but not sing.
- Moderate-intensity activity requires 3.0 to less than 6.0 METs; examples include walking briskly (2.5 to 4 mph), playing doubles tennis, or raking the yard.
- Vigorous-Intensity activity
- Vigorous-intensity activities make your heart, lungs, and muscles work hard. On a scale of 0 to 10, vigorous-intensity activity is a 7 or 8. A person doing vigorous-intensity activity can’t say more than a few words without stopping for a breath. Vigorous-intensity activity examples include jogging, running, carrying heavy groceries or other loads upstairs, shoveling snow, or participating in a strenuous fitness class. Many adults do no vigorous-intensity physical activity.
- Vigorous-intensity activity requires 6.0 or more METs.
Bicycling
Riding a bicycle spreads your weight among your arms, back, and hips. For outdoor biking, you may want to try a mountain bike. Mountain bikes have wider tires and are sturdier than road bikes with thinner tires. You can buy a larger gel padded seat to make biking more comfortable.
For indoor biking, you may want to try a recumbent bike. On this type of bike, you sit lower to the ground with your legs reaching forward to the pedals. Your body is in more of a reclining position, which may feel better than sitting straight up. The seat on a recumbent bike is also wider than the seat on a regular bike.
Water workouts
Swimming and water workouts put less stress on your joints than walking, biking, or dancing. If your feet, back, or joints hurt when you stand, water activities may be best for you. If you feel self-conscious about wearing a bathing suit, you can wear shorts and a T-shirt while you swim.
You don’t need to know how to swim to work out in water. You can do shallow- or deep-water exercises at either end of the pool without swimming. For instance, you can do laps while holding onto a kickboard and kicking your feet. You also can walk or jog across the width of the pool while moving your arms.
For shallow-water workouts, the water level should be between your waist and chest. During deep-water workouts, most of your body is underwater. For safety and comfort, wear a foam belt or life jacket.
Exercising in water
lets you be more flexible. You can move your body in water in ways you may not be able to on land.
reduces your risk of hurting yourself. Water provides a natural cushion, which keeps you from pounding or jarring your joints.
helps prevent sore muscles.
keeps you cool, even when you are working hard.
Dancing
Dancing can be a lot of fun while it tones your muscles, strengthens your heart and lungs, and boosts your mood. You can dance at a health club, dance studio, or even at home. Just turn on some lively music and start moving. You also can dance to a video on your TV or phone.
If you have trouble standing on your feet for a long time, try dancing while sitting down. Chair dancing lets you move your arms and legs to music while taking the weight off your feet.
- Iqbal R, Anand S, Ounpuu S, Islam S, Zhang X, Rangarajan S, et al. Dietary patterns and the risk of acute myocardial infarction in 52 countries: results of the INTERHEART study. Circulation. 2008;118(19):1929–37. http://circ.ahajournals.org/content/118/19/1929.long[↩]
- Mente A, de Koning L, Shannon HS, Anand SS. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med. 2009;169(7):659–69. https://www.ncbi.nlm.nih.gov/pubmed/19364995[↩]
- National Institutes of Health. Healthy Eating Plan. https://www.nhlbi.nih.gov/health/educational/lose_wt/eat/calories.htm[↩]
- U.S. Department of Health and Human Services. The Dietary Guidelines for Americans. https://health.gov/dietaryguidelines/[↩]
- National Vital Statistics Reports Volume June 30, 2016; 65,Number 4. Deaths: Final Data for 2014. https://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_04.pdf[↩]
- Eyre H, Kahn R, Robertson RM. Preventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Diabetes Care. 2004;27(7):1812–24. https://www.ncbi.nlm.nih.gov/pubmed/15220271[↩]
- Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med. 2000;343(1):16–22. http://www.nejm.org/doi/full/10.1056/NEJM200007063430103 [↩]
- Chiuve SE, McCullough ML, Sacks FM, Rimm EB. Healthy lifestyle factors in the primary prevention of coronary heart disease among men: benefits among users and nonusers of lipid-lowering and antihypertensive medications. Circulation. 2006;114(2):160–7. http://circ.ahajournals.org/content/114/2/160.long[↩]
- Skerrett PJ, Willett WC. Essentials of Healthy Eating: A Guide. Journal of midwifery & women’s health. 2010;55(6):492-501. doi:10.1016/j.jmwh.2010.06.019. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3471136/[↩][↩]
- Altomare, R., Cacciabaudo, F., Damiano, G., Palumbo, V. D., Gioviale, M. C., Bellavia, M., Tomasello, G., & Lo Monte, A. I. (2013). The mediterranean diet: a history of health. Iranian journal of public health, 42(5), 449–457. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3684452[↩]
- Castro-Quezada, I., Román-Viñas, B., & Serra-Majem, L. (2014). The Mediterranean diet and nutritional adequacy: a review. Nutrients, 6(1), 231–248. https://doi.org/10.3390/nu6010231[↩]
- F.B. Hu. The Mediterranean Diet and mortality—olive oil and beyond. N Engl J Med, 348 (2003), pp. 2595-2596[↩]
- Sofi F., Macchi C., Abbate R., Gensini G.F., Casini A. Mediterranean diet and health. Biofactors. 2013;39:335–342. doi: 10.1002/biof.1096[↩]
- Estruch R., Ros E., Salas-Salvadó J., Covas M.I., Corella D., Arós F., Gómez-Gracia E., Ruiz-Gutiérrez V., Fiol M., Lapetra J., et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013;368:1279–1290. doi: 10.1056/NEJMoa1200303[↩]
- Mitrou P.N., Kipnis V., Thiébaut A.C., Reedy J., Subar A.F., Wirfält E., Flood A., Mouw T., Hollenbeck A.R., Leitzmann M.F., et al. Mediterranean dietary pattern and prediction of all-cause mortality in a US population: Results from the NIH-AARP Diet and Health Study. Arch. Intern. Med. 2007;167:2461–2468. doi: 10.1001/archinte.167.22.2461[↩]
- Couto E., Boffetta P., Lagiou P., Ferrari P., Buckland G., Overvad K., Dahm C.C., Tjønneland A., Olsen A., Clavel-Chapelon F., et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer. 2011;104:1493–1499. doi: 10.1038/bjc.2011.106[↩]
- Sofi F., Abbate R., Gensini G.F., Casini A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010;92:1189–1196. doi: 10.3945/ajcn.2010.29673[↩]
- Widmer, R. J., Flammer, A. J., Lerman, L. O., & Lerman, A. (2015). The Mediterranean diet, its components, and cardiovascular disease. The American journal of medicine, 128(3), 229–238. https://doi.org/10.1016/j.amjmed.2014.10.014[↩]
- American Heart Association – Mediterranean Diet – http://www.heart.org/HEARTORG/HealthyLiving/HealthyEating/Nutrition/Mediterranean-Diet_UCM_306004_Article.jsp[↩][↩]
- Journal of the American College of Cardiology Volume 45, Issue 9, 3 May 2005, Pages 1379-1387. Diets and Cardiovascular Disease: An Evidence-Based Assessment. http://www.sciencedirect.com/science/article/pii/S0735109705003670[↩][↩]
- National Institutes of Health. National Heart, Blood and Lung Institute. Description of the DASH Eating Plan. https://www.nhlbi.nih.gov/health/health-topics/topics/dash[↩]
- Salehi-Abargouei A, Maghsoudi Z, Shirani F, Azadbakht L. Nutrition. 2013 Apr;29(4):611-8. doi: 10.1016/j.nut.2012.12.018. Effects of Dietary Approaches to Stop Hypertension (DASH)-style diet on fatal or nonfatal cardiovascular diseases–incidence: a systematic review and meta-analysis on observational prospective studies. http://www.nutritionjrnl.com/article/S0899-9007(13)00007-5/fulltext[↩][↩]
- Fung TT, Chiuve SE, McCullough ML, Rexrode KM, Logroscino G, Hu FB. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch Intern Med. 2008 Apr 14;168(7):713-20. PMID: 18413553. http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/414155[↩][↩]
- National Institutes of Health. National Heart, Blood and Lung Institute. Your Guide To Lowering Your Blood Pressure With DASH. https://www.nhlbi.nih.gov/files/docs/public/heart/dash_brief.pdf[↩]
- National Institutes of Health. National Heart, Blood and Lung Institute. Your Guide to Lowering Blood Pressure. https://www.nhlbi.nih.gov/files/docs/public/heart/hbp_low.pdf[↩]
- L.J. Appel, T.J. Moore, E. Obarzenek, et al.A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med, 336 (1997), pp. 1117-1124[↩][↩]
- J.P. Midgley, A.G. Matthew, C.M. Greenwood, A.G. Logan. Effect of reduced dietary sodium on blood pressure: a meta-analysis of randomized controlled trials. JAMA, 275 (1996), pp. 1590-1597[↩]
- National Institutes of Health. National Heart, Blood and Lung Institute. Your Guide to Lowering Blood Pressure with DASH. https://www.nhlbi.nih.gov/files/docs/public/heart/new_dash.pdf[↩]
- F.M. Sacks, L.P. Svetkey, W.M. Vollmer, et al.Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) DietN Engl J Med, 344 (2001), pp. 3-10[↩][↩]
- P.K. Whelton, J. He, L.J. Appel, et al.Primary prevention of hypertension: clinical and public health advisory from the National High Blood Pressure ProgramJAMA, 288 (2002), pp. 1882-1888[↩]
- National Institutes of Health. National Heart, Blood and Lung Institute. NHLBI Study Finds DASH Diet And Reduced Sodium Lowers Blood Pressure For All. https://www.nhlbi.nih.gov/news/press-releases/2001/nhlbi-study-finds-dash-diet-and-reduced-sodium-lowers-blood-pressure-for-all[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. PREMIER Study. https://www.nhlbi.nih.gov/research/resources/obesity/completed/premier.htm[↩][↩]
- Appel LJ, Champagne CM, Harsha DW, et al. Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA 2003;289:2083-93. [↩][↩]
- Blumenthal JA, Babyak MA, Hinderliter A, Watkins LL, Craighead L, Lin PH, Caccia C, Johnson J, Waugh R, Sherwood A. Effects of the DASH diet alone and in combination with exercise and weight loss on blood pressure and cardiovascular biomarkers in men and women with high blood pressure: the ENCORE study. Arch Intern Med. 2010 Jan 25;170(2):126-35. PMID: 20101007. https://www.ncbi.nlm.nih.gov/pubmed/20101007[↩]
- de Koning L, Chiuve SE, Fung TT, Willett WC, Rimm EB, Hu FB. Diet-quality scores and the risk of type 2 diabetes in men. Diabetes Care. 2011 May;34(5):1150-6. PMID: 21464460. https://www.ncbi.nlm.nih.gov/pubmed/21464460[↩]
- Trumbo P, Schlicker S, Yates AA, Poos M; Food and Nutrition Board of the Institute of Medicine, The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J Am Diet Assoc. 2002 Nov;102(11):1621-30. doi: 10.1016/s0002-8223(02)90346-9. Erratum in: J Am Diet Assoc. 2003 May;103(5):563.[↩][↩][↩][↩]
- Adams KF, Schatzkin A, Harris TB, et al. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006;355:763–78. doi: 10.1056/NEJMoa055643[↩]
- Field AE, Barnoya J, Colditz G. Epidemiology and health and economic consequences of obesity. In: Wadden TA, Stunkard AJ, editors. Handbook of Obesity Treatment. New York: The Guilford Press; 2002. pp. 3–18.[↩]
- Dwyer JT, Melanson KJ, Sriprachy-anunt U, et al. Dietary Treatment of Obesity. [Updated 2015 Feb 28]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278991[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol. 2014 Jul 1;63(25 Pt B):2985-3023. doi: 10.1016/j.jacc.2013.11.004. Erratum in: J Am Coll Cardiol. 2014 Jul 1;63(25 Pt B):3029-3030.[↩]
- Thomas, D. M., Bouchard, C., Church, T., Slentz, C., Kraus, W. E., Redman, L. M., Martin, C. K., Silva, A. M., Vossen, M., Westerterp, K., & Heymsfield, S. B. (2012). Why do individuals not lose more weight from an exercise intervention at a defined dose? An energy balance analysis. Obesity reviews : an official journal of the International Association for the Study of Obesity, 13(10), 835–847. https://doi.org/10.1111/j.1467-789X.2012.01012.x[↩]
- Aim for Healthy Weight. https://www.nhlbi.nih.gov/health/educational/lose_wt/index.htm[↩]
- Slentz CA, Duscha BD, Johnson JL, Ketchum K, Aiken LB, Samsa GP, Houmard JA, Bales CW, Kraus WE. Effects of the amount of exercise on body weight, body composition, and measures of central obesity: STRRIDE–a randomized controlled study. Arch Intern Med. 2004 Jan 12;164(1):31-9. doi: 10.1001/archinte.164.1.31[↩]
- Velthuis-te Wierik EJ, Westerterp KR, Van den Berg H. Effect of a moderately energy-restricted diet on energy metabolism and body composition in non-obese men. Int J Obes Relat Metab Disord. 1995;19:318–24.[↩]
- Fabricatore AN, Wadden TA, Womble LG, Sarwer DB, Berkowitz RI, Foster GD, Brock JR. The role of patients’ expectations and goals in the behavioral and pharmacological treatment of obesity. Int J Obes (Lond). 2007 Nov;31(11):1739-45. doi: 10.1038/sj.ijo.0803649[↩][↩]
- Van Itallie T. Dietary approaches to the treatment of obesity. In: Stunkard A, editor. Obesity. Philadelphia: WB Sanders, 1980: 249-261.[↩]
- Adam-Perrot A, Clifton P, Brouns F. Low-carbohydrate diets: nutritional and physiological aspects. Obes Rev. 2006 Feb;7(1):49-58. doi: 10.1111/j.1467-789X.2006.00222.x[↩]
- Global BMI Mortality Collaboration, Di Angelantonio E, Bhupathiraju ShN, Wormser D, Gao P, Kaptoge S, Berrington de Gonzalez A, Cairns BJ, Huxley R, Jackson ChL, Joshy G, Lewington S, Manson JE, Murphy N, Patel AV, Samet JM, Woodward M, Zheng W, Zhou M, Bansal N, Barricarte A, Carter B, Cerhan JR, Smith GD, Fang X, Franco OH, Green J, Halsey J, Hildebrand JS, Jung KJ, Korda RJ, McLerran DF, Moore SC, O’Keeffe LM, Paige E, Ramond A, Reeves GK, Rolland B, Sacerdote C, Sattar N, Sofianopoulou E, Stevens J, Thun M, Ueshima H, Yang L, Yun YD, Willeit P, Banks E, Beral V, Chen Zh, Gapstur SM, Gunter MJ, Hartge P, Jee SH, Lam TH, Peto R, Potter JD, Willett WC, Thompson SG, Danesh J, Hu FB. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016 Aug 20;388(10046):776-86. doi: 10.1016/S0140-6736(16)30175-1[↩]
- Action on obesity: Comprehensive care for all. Royal College of Physicians 10 Sep 2015. https://www.rcplondon.ac.uk/file/1283/download[↩]
- Panuganti KK, Nguyen M, Kshirsagar RK, et al. Obesity (Nursing) [Updated 2020 Dec 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK568702[↩][↩]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025. 9th Edition. December 2020. https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf[↩]
- Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr. 1990 Feb;51(2):241-7. doi: 10.1093/ajcn/51.2.241[↩]
- American Dietetic Association (ADA). Adult Weight Management Guideline: Major Recommendations. ADA Evidence Analysis Library 2014. https://www.andeal.org/vault/pq132.pdf[↩][↩][↩][↩][↩][↩]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults–The Evidence Report. National Institutes of Health, 6: 51S-179S. https://doi.org/10.1002/j.1550-8528.1998.tb00690.x[↩]
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel, 2013. Expert Panel Report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity (Silver Spring). 2014 Jul;22 Suppl 2:S41-410. doi: 10.1002/oby.20660[↩][↩][↩][↩][↩]
- Koplan JP, Dietz WH. Caloric imbalance and public health policy. JAMA. 1999 Oct 27;282(16):1579-81. doi: 10.1001/jama.282.16.1579[↩]
- Van Dorsten B, Lindley EM. Cognitive and behavioral approaches in the treatment of obesity. Endocrinol Metab Clin North Am. 2008 Dec;37(4):905-22. doi: 10.1016/j.ecl.2008.08.003[↩][↩]
- Foster GD, Wadden TA, Vogt RA, Brewer G. What is a reasonable weight loss? Patients’ expectations and evaluations of obesity treatment outcomes. J Consult Clin Psychol. 1997 Feb;65(1):79-85. doi: 10.1037//0022-006x.65.1.79[↩]
- Estruch R, Martínez-González MA, Corella D, Salas-Salvadó J, Ruiz-Gutiérrez V, Covas MI, Fiol M, Gómez-Gracia E, López-Sabater MC, Vinyoles E, Arós F, Conde M, Lahoz C, Lapetra J, Sáez G, Ros E; PREDIMED Study Investigators. Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized trial. Ann Intern Med. 2006 Jul 4;145(1):1-11. doi: 10.7326/0003-4819-145-1-200607040-00004. Erratum in: Ann Intern Med. 2018 Aug 21;169(4):270-271. doi: 10.7326/L18-0374[↩]
- Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation. 2014;129:S102–S138.[↩]
- Varkevisser, R., van Stralen, M. M., Kroeze, W., Ket, J., & Steenhuis, I. (2019). Determinants of weight loss maintenance: a systematic review. Obesity reviews : an official journal of the International Association for the Study of Obesity, 20(2), 171–211. https://doi.org/10.1111/obr.12772[↩]
- Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK; American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2009 Feb;41(2):459-71. doi: 10.1249/MSS.0b013e3181949333. Erratum in: Med Sci Sports Exerc. 2009 Jul;41(7):1532.[↩][↩][↩][↩][↩][↩][↩]
- Church TS, Martin CK, Thompson AM, Earnest CP, Mikus CR, Blair SN. Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women. PLoS One. 2009;4(2):e4515. doi: 10.1371/journal.pone.0004515[↩]
- Swift, D. L., Johannsen, N. M., Lavie, C. J., Earnest, C. P., & Church, T. S. (2014). The role of exercise and physical activity in weight loss and maintenance. Progress in cardiovascular diseases, 56(4), 441–447. https://doi.org/10.1016/j.pcad.2013.09.012[↩][↩]
- Swift DL, Lavie CJ, Johannsen NM, Arena R, Earnest CP, O’Keefe JH, Milani RV, Blair SN, Church TS. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circ J. 2013;77(2):281-92. doi: 10.1253/circj.cj-13-0007[↩]
- Lee CD, Blair SN, Jackson AS. Cardiorespiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men. Am J Clin Nutr. 1999 Mar;69(3):373-80. doi: 10.1093/ajcn/69.3.373[↩]
- Wei M, Kampert JB, Barlow CE, Nichaman MZ, Gibbons LW, Paffenbarger RS Jr, Blair SN. Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. JAMA. 1999 Oct 27;282(16):1547-53. doi: 10.1001/jama.282.16.1547[↩]
- McAuley, P. A., Kokkinos, P. F., Oliveira, R. B., Emerson, B. T., & Myers, J. N. (2010). Obesity paradox and cardiorespiratory fitness in 12,417 male veterans aged 40 to 70 years. Mayo Clinic proceedings, 85(2), 115–121. https://doi.org/10.4065/mcp.2009.0562[↩]
- Ross R, Dagnone D, Jones PJ, Smith H, Paddags A, Hudson R, Janssen I. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men. A randomized, controlled trial. Ann Intern Med. 2000 Jul 18;133(2):92-103. doi: 10.7326/0003-4819-133-2-200007180-00008[↩][↩][↩][↩][↩]
- Marinilli Pinto A, Gorin AA, Raynor HA, Tate DF, Fava JL, Wing RR. Successful weight-loss maintenance in relation to method of weight loss. Obesity (Silver Spring). 2008 Nov;16(11):2456-61. doi: 10.1038/oby.2008.364[↩][↩][↩][↩][↩][↩][↩]
- Seagle HM, Strain GW, Makris A, Reeves RS; American Dietetic Association. Position of the American Dietetic Association: weight management. J Am Diet Assoc. 2009 Feb;109(2):330-46. doi: 10.1016/j.jada.2008.11.041[↩][↩]
- Chaston TB, Dixon JB, O’Brien PE. Changes in fat-free mass during significant weight loss: a systematic review. Int J Obes (Lond). 2007 May;31(5):743-50. doi: 10.1038/sj.ijo.0803483[↩][↩]
- U.S.Department of Health and Human Services, National Institues of Health, National Heart LaBI. Aim for a Healthy Weight. NIH publication No. 05-5213. 2005.[↩]
- National Heart LaBI. Guidelines on Overweight and Obesity: Electronic Textbook 2000. https://www.nhlbi.nih.gov/files/docs/guidelines/prctgd_c.pdf[↩][↩][↩]
- Freedman MR, King J, Kennedy E. Popular diets: a scientific review. Obes Res. 2001 Mar;9 Suppl 1:1S-40S. doi: 10.1038/oby.2001.113[↩]
- Traditional American Cuisine: 1,200 Calories. https://www.nhlbi.nih.gov/health/educational/lose_wt/eat/menus_tac_1200.htm[↩]
- Traditional American Cuisine: 1,600 Calories. https://www.nhlbi.nih.gov/health/educational/lose_wt/eat/menus_tac_1600.htm[↩]
- Kushner RF, Kus8.4hner N, Jackson Blatner D. Counseling Overweight Adults: The Lifestyle Patterns Approach and Toolkit. Chicago. American Dietetic Association, 2009.[↩]
- Atkinson RL, Dietz WH, Foreyt JP, et al. Very Low-Calorie Diets. JAMA. 1993;270(8):967–974. doi:10.1001/jama.1993.03510080071034[↩]
- Tsai AG, Wadden TA. Systematic review: an evaluation of major commercial weight loss programs in the United States. Ann Intern Med. 2005 Jan 4;142(1):56-66. doi: 10.7326/0003-4819-142-1-200501040-00012[↩][↩]
- Very Low-Calorie Diets. https://www.govinfo.gov/content/pkg/GOVPUB-HE20-PURL-LPS78142/pdf/GOVPUB-HE20-PURL-LPS78142.pdf[↩][↩]
- Varady KA, Bhutani S, Church EC, Klempel MC. Short-term modified alternate-day fasting: a novel dietary strategy for weight loss and cardioprotection in obese adults. Am J Clin Nutr. 2009 Nov;90(5):1138-43. doi: 10.3945/ajcn.2009.28380[↩][↩]
- Klempel MC, Bhutani S, Fitzgibbon M, Freels S, Varady KA. Dietary and physical activity adaptations to alternate day modified fasting: implications for optimal weight loss. Nutr J. 2010 Sep 3;9:35. doi: 10.1186/1475-2891-9-35[↩]
- Bhutani S, Klempel MC, Kroeger CM, Trepanowski JF, Varady KA. Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity (Silver Spring). 2013 Jul;21(7):1370-9. doi: 10.1002/oby.20353[↩]
- Eshghinia S, Mohammadzadeh F. The effects of modified alternate-day fasting diet on weight loss and CAD risk factors in overweight and obese women. J Diabetes Metab Disord. 2013 Jan 9;12(1):4. doi: 10.1186/2251-6581-12-4[↩]
- Klemsdal TO, Holme I, Nerland H, Pedersen TR, Tonstad S. Effects of a low glycemic load diet versus a low-fat diet in subjects with and without the metabolic syndrome. Nutr Metab Cardiovasc Dis. 2010 Mar;20(3):195-201. doi: 10.1016/j.numecd.2009.03.010[↩]
- Klempel MC, Kroeger CM, Varady KA. Alternate day fasting increases LDL particle size independently of dietary fat content in obese humans. Eur J Clin Nutr. 2013 Jul;67(7):783-5. doi: 10.1038/ejcn.2013.83[↩]
- Welton, S., Minty, R., O’Driscoll, T., Willms, H., Poirier, D., Madden, S., & Kelly, L. (2020). Intermittent fasting and weight loss: Systematic review. Canadian family physician Medecin de famille canadien, 66(2), 117–125. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7021351[↩][↩][↩]
- Fung J. The obesity code. Unlocking the secrets of weight loss. Vancouver, BC: Greystone Books; 2016.[↩]
- Dong, T. A., Sandesara, P. B., Dhindsa, D. S., Mehta, A., Arneson, L. C., Dollar, A. L., Taub, P. R., & Sperling, L. S. (2020). Intermittent Fasting: A Heart Healthy Dietary Pattern?. The American journal of medicine, 133(8), 901–907. https://doi.org/10.1016/j.amjmed.2020.03.030[↩][↩]
- Catenacci VA, Pan Z, Ostendorf D, Brannon S, Gozansky WS, Mattson MP, Martin B, MacLean PS, Melanson EL, Troy Donahoo W. A randomized pilot study comparing zero-calorie alternate-day fasting to daily caloric restriction in adults with obesity. Obesity (Silver Spring). 2016 Sep;24(9):1874-83. doi: 10.1002/oby.21581[↩]
- Mattson, M. P., Longo, V. D., & Harvie, M. (2017). Impact of intermittent fasting on health and disease processes. Ageing research reviews, 39, 46–58. https://doi.org/10.1016/j.arr.2016.10.005[↩]
- Anastasiou CA, Karfopoulou E, Yannakoulia M. Weight regaining: From statistics and behaviors to physiology and metabolism. Metabolism. 2015 Nov;64(11):1395-407. doi: 10.1016/j.metabol.2015.08.006[↩]
- Johnson JB, Summer W, Cutler RG, Martin B, Hyun DH, Dixit VD, Pearson M, Nassar M, Telljohann R, Maudsley S, Carlson O, John S, Laub DR, Mattson MP. Alternate day calorie restriction improves clinical findings and reduces markers of oxidative stress and inflammation in overweight adults with moderate asthma. Free Radic Biol Med. 2007 Mar 1;42(5):665-74. doi: 10.1016/j.freeradbiomed.2006.12.005. Epub 2006 Dec 14. Erratum in: Free Radic Biol Med. 2007 Nov 1;43(9):1348. Tellejohan, Richard [corrected to Telljohann, Richard].[↩][↩][↩]
- Eades M. Protein Powder. New York: Bantam Books, 1996.[↩]
- Stubbs RJ, van Wyk MC, Johnstone AM, Harbron CG. Breakfasts high in protein, fat or carbohydrate: effect on within-day appetite and energy balance. Eur J Clin Nutr. 1996 Jul;50(7):409-17.[↩]
- Crovetti R, Porrini M, Santangelo A, Testolin G. The influence of thermic effect of food on satiety. Eur J Clin Nutr. 1998 Jul;52(7):482-8. doi: 10.1038/sj.ejcn.1600578[↩]
- Eisenstein J, Roberts SB, Dallal G, Saltzman E. High-protein weight-loss diets: are they safe and do they work? A review of the experimental and epidemiologic data. Nutr Rev. 2002 Jul;60(7 Pt 1):189-200. doi: 10.1301/00296640260184264[↩]
- American Diabetes Association. Nutrition recommendations and principles for people with diabetes mellitus. Diabetes Care. 2000 Jan;23 Suppl 1:S43-6.[↩]
- Grundy SM, Hansen B, Smith SC Jr, Cleeman JI, Kahn RA; American Heart Association; National Heart, Lung, and Blood Institute; American Diabetes Association. Clinical management of metabolic syndrome: report of the American Heart Association/National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Circulation. 2004 Feb 3;109(4):551-6. doi: 10.1161/01.CIR.0000112379.88385.67[↩]
- Klein S, Sheard NF, Pi-Sunyer X, Daly A, Wylie-Rosett J, Kulkarni K, Clark NG; American Diabetes Association; North American Association for the Study of Obesity; American Society for Clinical Nutrition. Weight management through lifestyle modification for the prevention and management of type 2 diabetes: rationale and strategies: a statement of the American Diabetes Association, the North American Association for the Study of Obesity, and the American Society for Clinical Nutrition. Diabetes Care. 2004 Aug;27(8):2067-73. doi: 10.2337/diacare.27.8.2067[↩]
- Johnston BC, Kanters S, Bandayrel K, Wu P, Naji F, Siemieniuk RA, Ball GD, Busse JW, Thorlund K, Guyatt G, Jansen JP, Mills EJ. Comparison of weight loss among named diet programs in overweight and obese adults: a meta-analysis. JAMA. 2014 Sep 3;312(9):923-33. doi: 10.1001/jama.2014.10397[↩]
- Morris AL, Mohiuddin SS. Biochemistry, Nutrients. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554545[↩][↩][↩][↩][↩][↩]
- Dietary Guidelines for Americans. https://www.dietaryguidelines.gov/[↩][↩][↩]
- Cummings JH, Stephen AM. Carbohydrate terminology and classification. Eur J Clin Nutr. 2007 Dec;61 Suppl 1:S5-18. doi: 10.1038/sj.ejcn.1602936[↩]
- Horton TJ, Drougas H, Brachey A, Reed GW, Peters JC, Hill JO. Fat and carbohydrate overfeeding in humans: different effects on energy storage. Am J Clin Nutr. 1995 Jul;62(1):19-29. doi: 10.1093/ajcn/62.1.19[↩]
- Minehira K, Vega N, Vidal H, Acheson K, Tappy L. Effect of carbohydrate overfeeding on whole body macronutrient metabolism and expression of lipogenic enzymes in adipose tissue of lean and overweight humans. Int J Obes Relat Metab Disord. 2004 Oct;28(10):1291-8. doi: 10.1038/sj.ijo.0802760[↩]
- Hall KD. A review of the carbohydrate-insulin model of obesity. Eur J Clin Nutr. 2017 Mar;71(3):323-326. doi: 10.1038/ejcn.2016.260. Epub 2017 Jan 11. Erratum in: Eur J Clin Nutr. 2017 May;71(5):679. doi: 10.1038/ejcn.2017.21[↩]
- Merchant AT, Vatanparast H, Barlas S, Dehghan M, Shah SM, De Koning L, Steck SE. Carbohydrate intake and overweight and obesity among healthy adults. J Am Diet Assoc. 2009 Jul;109(7):1165-72. doi: 10.1016/j.jada.2009.04.002[↩][↩]
- Yunsheng Ma, Barbara Olendzki, David Chiriboga, James R. Hebert, Youfu Li, Wenjun Li, MaryJane Campbell, Katherine Gendreau, Ira S. Ockene, Association between Dietary Carbohydrates and Body Weight, American Journal of Epidemiology, Volume 161, Issue 4, 15 February 2005, Pages 359–367, https://doi.org/10.1093/aje/kwi051[↩]
- Do Carbohydrates Control Body Fat? https://blog.nasm.org/do-carbohydrates-control-body-fat[↩]
- Nordmann AJ, Nordmann A, Briel M, Keller U, Yancy WS Jr, Brehm BJ, Bucher HC. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Arch Intern Med. 2006 Feb 13;166(3):285-93. doi: 10.1001/archinte.166.3.285. Erratum in: Arch Intern Med. 2006 Apr 24;166(8):932.[↩]
- Hall KD, Bemis T, Brychta R, et al. Calorie for Calorie, Dietary Fat Restriction Results in More Body Fat Loss than Carbohydrate Restriction in People with Obesity. Cell Metab. 2015 Sep 1;22(3):427-36. doi: 10.1016/j.cmet.2015.07.021[↩]
- Hall KD, Chen KY, Guo J, et al. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am J Clin Nutr. 2016 Aug;104(2):324-33. doi: 10.3945/ajcn.116.133561[↩]
- Hall KD, Chen KY, Guo J, Lam YY, Leibel RL, Mayer LE, Reitman ML, Rosenbaum M, Smith SR, Walsh BT, Ravussin E. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am J Clin Nutr. 2016 Aug;104(2):324-33. doi: 10.3945/ajcn.116.133561[↩]
- Burke, L.M. (2021), Ketogenic low-CHO, high-fat diet: the future of elite endurance sport?. J Physiol, 599: 819-843. https://doi.org/10.1113/JP278928[↩]
- Burke LM, Ross ML, Garvican-Lewis LA, Welvaert M, Heikura IA, Forbes SG, Mirtschin JG, Cato LE, Strobel N, Sharma AP, Hawley JA. Low carbohydrate, high fat diet impairs exercise economy and negates the performance benefit from intensified training in elite race walkers. J Physiol. 2017 May 1;595(9):2785-2807. doi: 10.1113/JP273230[↩]
- How Many Carbs Should You Eat a Day to Lose Weight? https://blog.nasm.org/how-many-carbs-should-you-eat-a-day-to-lose-weight[↩]
- LaPelusa A, Kaushik R. Physiology, Proteins. [Updated 2022 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555990[↩][↩][↩][↩]
- Protein Foods. https://www.myplate.gov/eat-healthy/protein-foods[↩][↩]
- Lopez MJ, Mohiuddin SS. Biochemistry, Essential Amino Acids. [Updated 2024 Apr 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557845[↩][↩][↩][↩]
- Pasiakos SM, Agarwal S, Lieberman HR, Fulgoni VL 3rd. Sources and Amounts of Animal, Dairy, and Plant Protein Intake of US Adults in 2007-2010. Nutrients. 2015 Aug 21;7(8):7058-69. doi: 10.3390/nu7085322[↩]
- O’Neil CE, Keast DR, Fulgoni VL, Nicklas TA. Food sources of energy and nutrients among adults in the US: NHANES 2003–2006. Nutrients. 2012 Dec 19;4(12):2097-120. doi: 10.3390/nu4122097[↩]
- Acheson KJ. Diets for body weight control and health: the potential of changing the macronutrient composition. Eur J Clin Nutr. 2013 May;67(5):462-6. doi: 10.1038/ejcn.2012.194[↩][↩][↩]
- Protein Intake for Optimal Muscle Maintenance. https://www.acsm.org/docs/default-source/files-for-resource-library/protein-intake-for-optimal-muscle-maintenance.pdf[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Hector A. J., Phillips S. M. Protein recommendations for weight loss in elite athletes: a focus on body composition and performance. International Journal of Sport Nutrition and Exercise Metabolism . 2018;28(2):170–177. doi: 10.1123/ijsnem.2017-0273[↩][↩][↩][↩]
- Passariello C. L., Marchionni S., Carcuro M., et al. The Mediterranean athlete’s nutrition: are protein supplements necessary? Nutrients . 2020;12(12):p. 3681. doi: 10.3390/nu12123681[↩][↩][↩]
- Stokes T., Hector A., Morton R., McGlory C., Phillips S. Recent perspectives regarding the role of dietary protein for the promotion of muscle hypertrophy with resistance exercise training. Nutrients . 2018;10(2):p. 180. doi: 10.3390/nu10020180[↩][↩][↩][↩]
- Finger D., Goltz F. R., Umpierre D., Meyer E., Rosa L. H. T., Schneider C. D. Effects of protein supplementation in older adults undergoing resistance training: a systematic review and meta-analysis. Sports Medicine . 2015;45(2):245–255. doi: 10.1007/s40279-014-0269-4[↩]
- Morton R. W., Murphy K. T., McKellar S. R., et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. British Journal of Sports Medicine . 2018;52(6):376–384. doi: 10.1136/bjsports-2017-097608[↩]
- Phillips S. M., Van Loon L. J. C. Dietary protein for athletes: from requirements to optimum adaptation. Journal of Sports Sciences . 2011;29(1):S29–S38. doi: 10.1080/02640414.2011.619204[↩]
- Porcelli S, Pugliese L, Rejc E, Pavei G, Bonato M, Montorsi M, La Torre A, Rasica L, Marzorati M. Effects of a Short-Term High-Nitrate Diet on Exercise Performance. Nutrients. 2016 Aug 31;8(9):534. doi: 10.3390/nu8090534[↩]
- Butts J, Jacobs B, Silvis M. Creatine Use in Sports. Sports Health. 2018 Jan/Feb;10(1):31-34. Doi: 10.1177/1941738117737248[↩][↩]
- Bird SP. Creatine supplementation and exercise performance: a brief review. J Sports Sci Med. 2003 Dec 1;2(4):123-32. https://pmc.ncbi.nlm.nih.gov/articles/PMC3963244[↩]
- Cooke WH, Grandjean PW, Barnes WS. Effect of oral creatine supplementation on power output and fatigue during bicycle ergometry. J Appl Physiol (1985). 1995 Feb;78(2):670-3. doi: 10.1152/jappl.1995.78.2.670[↩]
- Rawson ES, Gunn B, Clarkson PM. The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res. 2001 May;15(2):178-84.[↩]
- Ellery SJ, Walker DW, Dickinson H. Creatine for women: a review of the relationship between creatine and the reproductive cycle and female-specific benefits of creatine therapy. Amino Acids. 2016 Aug;48(8):1807-17. doi: 10.1007/s00726-016-2199-y[↩]
- Molina Juan L, Sospedra I, Perales A, González-Díaz C, Gil-Izquierdo A, Martínez-Sanz JM. Analysis of health claims regarding creatine monohydrate present in commercial communications for a sample of European sports foods supplements. Public Health Nutr. 2021 Jan 20;24(4):1-9. doi: 10.1017/S1368980020005121[↩][↩]
- Institute of Medicine (US) Committee on Nutrition, Trauma, and the Brain; Erdman J, Oria M, Pillsbury L, editors. Nutrition and Traumatic Brain Injury: Improving Acute and Subacute Health Outcomes in Military Personnel. Washington (DC): National Academies Press (US); 2011. 10, Creatine. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209321[↩]
- Stricker PR. Other ergogenic agents. Clin Sports Med. 1998 Apr;17(2):283-97. doi: 10.1016/s0278-5919(05)70081-8[↩]
- Butts J, Jacobs B, Silvis M. Creatine Use in Sports. Sports Health. 2018 Jan/Feb;10(1):31-34. doi: 10.1177/1941738117737248[↩][↩]
- Bemben MG, Lamont HS. Creatine supplementation and exercise performance: recent findings. Sports Med. 2005;35(2):107-25. doi: 10.2165/00007256-200535020-00002[↩]
- Branch JD. Effect of creatine supplementation on body composition and performance: a meta-analysis. Int J Sport Nutr Exerc Metab. 2003 Jun;13(2):198-226. doi: 10.1123/ijsnem.13.2.198[↩]
- Institute of Medicine (US) Committee on Dietary Supplement Use by Military Personnel; Greenwood MRC, Oria M, editors. Use of Dietary Supplements by Military Personnel. Washington (DC): National Academies Press (US); 2008. Available from: https://www.ncbi.nlm.nih.gov/books/NBK3977[↩][↩]
- McMorris T, Harris RC, Howard AN, Langridge G, Hall B, Corbett J, Dicks M, Hodgson C. Creatine supplementation, sleep deprivation, cortisol, melatonin and behavior. Physiol Behav. 2007 Jan 30;90(1):21-8. doi: 10.1016/j.physbeh.2006.08.024[↩]
- Shao A, Hathcock JN. Risk assessment for creatine monohydrate. Regul Toxicol Pharmacol. 2006 Aug;45(3):242-51. doi: 10.1016/j.yrtph.2006.05.005[↩][↩]
- Burke LM. Practical Issues in Evidence-Based Use of Performance Supplements: Supplement Interactions, Repeated Use and Individual Responses. Sports Med. 2017 Mar;47(Suppl 1):79-100. doi: 10.1007/s40279-017-0687-1[↩]
- Rawson ES, Miles MP, Larson-Meyer DE. Dietary Supplements for Health, Adaptation, and Recovery in Athletes. Int J Sport Nutr Exerc Metab. 2018 Mar 1;28(2):188-199. doi: 10.1123/ijsnem.2017-0340[↩][↩]
- Kreider RB, Kalman DS, Antonio J, Ziegenfuss TN, Wildman R, Collins R, Candow DG, Kleiner SM, Almada AL, Lopez HL. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2017 Jun 13;14:18. doi: 10.1186/s12970-017-0173-z[↩]
- Maughan RJ, Greenhaff PL, Hespel P. Dietary supplements for athletes: emerging trends and recurring themes. J Sports Sci. 2011;29 Suppl 1:S57-66. doi: 10.1080/02640414.2011.587446[↩]
- European Comission (2018) EU Register on Nutrition and Health Claims. Brussels: European Commission.[↩]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2016. Scientific opinion on creatine in combination with resistance training and improvement in muscle strength: evaluation of a health claim pursuant to Article 13(5) of Regulation (EC) No 1924/2006. EFSA Journal 2016; 14(2):4400, 17 pp. doi:10.2903/j.efsa.2016.4400[↩][↩][↩][↩]
- Del Razo Olvera FM, Melgarejo Hernández MA, Mehta R, Aguilar Salinas CA. Setting the Lipid Component of the Diet: A Work in Process. Adv Nutr. 2017 Jan 17;8(1):165S-172S. doi: 10.3945/an.116.013672[↩]
- Tvrzicka E, Kremmyda LS, Stankova B, Zak A. Fatty acids as biocompounds: their role in human metabolism, health and disease–a review. Part 1: classification, dietary sources and biological functions. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2011 Jun;155(2):117-30. doi: 10.5507/bp.2011.038[↩]
- Jacobs DR, Tapsell LC. Food synergy: the key to a healthy diet. Proc Nutr Soc. 2013 May;72(2):200-6. doi: 10.1017/S0029665112003011[↩]
- Jones PJH, Papamandjaris AA. Lipids: cellular metabolism. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:132-48.[↩]
- Harris WS. Omega-3 fatty acids. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:577-86.[↩]
- Omega-3 Fatty Acids, https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional[↩][↩]
- Jones PJH, Rideout T. Lipids, sterols, and their metabolites. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014.[↩]
- Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood). 2008 Jun;233(6):674-88. doi: 10.3181/0711-MR-311[↩]
- Wang C, Chung M, Lichtenstein A, Balk E, Kupelnick B, DeVine D, et al. Effects of omega-3 fatty acids on cardiovascular disease. Summary, evidence report/technology assessment no. 94. https://archive.ahrq.gov/downloads/pub/evidence/pdf/o3cardio/o3cardio.pdf[↩]
- Stanley JC, Elsom RL, Calder PC, Griffin BA, Harris WS, Jebb SA, Lovegrove JA, Moore CS, Riemersma RA, Sanders TA. UK Food Standards Agency Workshop Report: the effects of the dietary n-6:n-3 fatty acid ratio on cardiovascular health. Br J Nutr. 2007 Dec;98(6):1305-10. doi: 10.1017/S000711450784284X[↩]
- Harris WS, Davidson MH. RE: Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2014 Apr;106(4):dju019. doi: 10.1093/jnci/dju019[↩]
- Fritsche KL. Too much linoleic acid promotes inflammation-doesn’t it? Prostaglandins Leukot Essent Fatty Acids. 2008 Sep-Nov;79(3-5):173-5. doi: 10.1016/j.plefa.2008.09.019[↩]
- Pritikin M, McGrady PM. The Pritikin Program for Diet and Exercise. New York: Bantum Books, 1980.[↩]
- Ornish D. Can lifestyle changes reverse coronary heart disease? World Rev Nutr Diet. 1993;72:38-48. doi: 10.1159/000422326[↩][↩][↩]
- Hand B and Romine S. The Spark Solution. HarperOne, 2014.[↩]
- Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med. 2000;343(1):16–22. http://www.nejm.org/doi/full/10.1056/NEJM200007063430103[↩]
- Looker AC, Dallman PR, Carroll MD, Gunter EW, Johnson CL. Prevalence of iron deficiency in the United States. JAMA. 1997;277(12):973–6. https://www.ncbi.nlm.nih.gov/pubmed/9091669[↩]
- MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet. 1991;338(8760):131–7. https://www.ncbi.nlm.nih.gov/pubmed/1677062[↩]
- Institute of Medicine. Dietary reference intakes: calcium, phosphorous, magnesium, vitamin D, and fluoride. National Academy Press; 1997. https://www.nap.edu/read/5776/chapter/1[↩]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. Dietary guidelines for Americans 2005. Washington, DC: U.S. Department of Agriculture; 2015-2020. https://health.gov/dietaryguidelines/[↩]
- Stechschulte SA, Kirsner RS, Federman DG. Vitamin D: bone and beyond, rationale and recommendations for supplementation. Am J Med. 2009;122(9):793–802. https://www.ncbi.nlm.nih.gov/pubmed/19699370[↩]
- Feskanich D, Singh V, Willett WC, Colditz GA. Vitamin A intake and hip fractures among postmenopausal women. JAMA. 2002;287(1):47–54. https://www.ncbi.nlm.nih.gov/pubmed/11754708[↩]
- Gaesser GA, Tucker WJ, Jarrett CL, Angadi SS. Fitness versus Fatness: Which Influences Health and Mortality Risk the Most? Curr Sports Med Rep. 2015 Jul-Aug;14(4):327-32. doi: 10.1249/JSR.0000000000000170[↩][↩]
- Masters RK, Reither EN, Powers DA, et al. The impact of obesity on US mortality levels: the importance of age and cohort factors in population estimates. Am. J. Public Health. 2013; 103: 1895–901.[↩]
- Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions?: A systematic review and meta-analysis. Ann Intern Med. 2013 Dec 3;159(11):758-69. doi: 10.7326/0003-4819-159-11-201312030-00008[↩]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd edition. Washington, DC: U.S. Department of Health and Human Services; 2018. https://odphp.health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf[↩][↩][↩]
- The Physical Activity Guidelines for Americans. https://odphp.health.gov/our-work/nutrition-physical-activity/physical-activity-guidelines/current-guidelines[↩]
- Barry VW, Baruth M, Beets MW, Durstine JL, Liu J, Blair SN. Fitness vs. fatness on all-cause mortality: a meta-analysis. Prog Cardiovasc Dis. 2014 Jan-Feb;56(4):382-90. doi: 10.1016/j.pcad.2013.09.002[↩]
- Wildman REC, Miller BS. Sports and Fitness Nutrition. Australia: Thomson/Wadsworth, 2004.[↩]
- 2008 Physical Activity Guidelines for Americans. https://odphp.health.gov/sites/default/files/2019-09/paguide.pdf[↩]
- Melanson KJ. CE Test: Food Intake Regulation in Body Weight Management: A Primer. Nutrition Today 2004; 39(5).[↩][↩]
- Cava E., Yeat N. C., Mittendorfer B. Preserving healthy muscle during weight loss. Advances in Nutrition: An International Review Journal . 2017;8(3):511–519. doi: 10.3945/an.116.014506[↩]
- Westcott W. L. Resistance training is medicine. Current Sports Medicine Reports . 2012;11(4):209–216. doi: 10.1249/JSR.0b013e31825dabb8[↩]
- Gomes G. K., Franco C. M., Nunes P. R. P., Orsatti F. L. High-frequency resistance training is not more effective than low-frequency resistance training in increasing muscle mass and strength in well-trained men. The Journal of Strength & Conditioning Research . 2019;33(1):S130–S139. doi: 10.1519/JSC.0000000000002559[↩]
- Sabag A., Najafi A., Michael S., Esgin T., Halaki M., Hackett D. The compatibility of concurrent high intensity interval training and resistance training for muscular strength and hypertrophy: a systematic review and meta-analysis. Journal of Sports Sciences . 2018;36(21):2472–2483. doi: 10.1080/02640414.2018.1464636[↩]
- Defining Muscular Hypertrophy & Growth Training Best Practices. https://blog.nasm.org/sports-performance/defining-muscular-hypertrophy-and-training-growth-best-practices[↩]
- Jakicic JM, Winters C, Lang W, Wing RR. Effects of intermittent exercise and use of home exercise equipment on adherence, weight loss, and fitness in overweight women: a randomized trial. JAMA. 1999 Oct 27;282(16):1554-60. doi: 10.1001/jama.282.16.1554[↩][↩]
- Jakicic JM, Marcus BH, Gallagher KI, Napolitano M, Lang W. Effect of exercise duration and intensity on weight loss in overweight, sedentary women: a randomized trial. JAMA. 2003 Sep 10;290(10):1323-30. doi: 10.1001/jama.290.10.1323[↩]
- Andersen RE, Wadden TA, Bartlett SJ, Zemel B, Verde TJ, Franckowiak SC. Effects of lifestyle activity vs structured aerobic exercise in obese women: a randomized trial. JAMA. 1999 Jan 27;281(4):335-40. doi: 10.1001/jama.281.4.335[↩]





{kind=link}