Contents
- What is the Diabetic Diet
- Portion Size Versus Serving Size
- How much carbohydrate do you need each day ?
- How can you find out how much carbohydrate is in the foods you eat ?
- What is carbohydrate counting ?
- Which foods contain carbohydrates ?
- What foods and drinks should you limit if you have diabetes ?
- What are added sugars ?
- Healthy diabetic eating includes:
- The American Diabetes Association’s Create Your Plate online interactive meal planning tool
- What Can you Drink ?
- Make your calories count with these nutritious foods:
- What is the difference between Glycemic Index (GI) and Glycemic Load (GL) ?
- Benefits of Low Glycaemic Index or Low Glycaemic Load Diets for Diabetes Mellitus
- Vegetarian Diets Linked to Lower Mortality
- The 1200 Calories Diabetic Diet (Low Calorie Diet)
- Vegetarian Diets and Diabetes
- What is a vegetarian ?
- Why you may try a vegetarian diet ?
- Low Calorie Diet on Weight Loss and the Metabolic Profile of Obese Patients with Type 2 Diabetes Mellitus
- Very Low Calorie Diet in Obese Type 2 Diabetes
- Low Carbohydrate Low Calorie Diet in type 2 Diabetes
What is the Diabetic Diet
The diabetes diet is simply a healthy-eating plan that will help you control your blood sugar. Diabetic diet usually contains low-glycaemic index food, with similar amount of protein, complex carbohydrates, fibres, and unsaturated fatty acids as in food for general public 1. If you have diabetes, your body cannot make or properly use insulin. This leads to high blood glucose, or blood sugar, levels. What you eat is closely connected to the amount of sugar in your blood. The right food choices will help you control your blood sugar level and controlling your blood sugar can prevent the complications of diabetes 2.
- Avoid foods labelled ‘diabetic’ or ‘suitable for diabetics’. These foods contain similar amounts of calories and fat, and they can affect your blood glucose levels. They are usually more expensive and can have a laxative effect. Stick to your usual foods. If you want to have an occasional treat, go for your normal treats and keep an eye on your portions.
There isn’t one specific “diabetes diet.” Healthy eating helps keep your blood sugar in your target range. It is a critical part of managing your diabetes, because controlling your blood sugar can prevent the complications of diabetes.
- The Centers for Disease Control and Prevention has a free recipes ebook for people and their families with diabetes, you download a free copy here 3.
A registered dietitian can also help you make an eating plan just for you. It should take into account your weight, medicines, lifestyle, and other health problems you have.
- To find out about your body mass index (BMI), you can use a FREE online BMI calculators from the Centers for Disease Control and Prevention (CDC) – for Adults 4 and for Children 5
- To find out What and How Much To Eat, you can use a FREE, award-winning, state-of-the-art, online diet and activity tracking tool called SuperTracker 6 from the United States Department of Agriculture Center for Nutrition Policy and Promotion 6. This free application empowers you to build a healthier diet, manage weight, and reduce your risk of chronic diet-related diseases. You can use SuperTracker 6 to determine what and how much to eat; track foods, physical activities, and weight; and personalize with goal setting, virtual coaching, and journaling.
SuperTracker website 6
- To find out about how many calories you should eat to lose weight according to your weight, age, sex, height and physical activity, you can use a FREE online app Body Weight Planner 7
- To find out about the 5 Food Groups you should have on your plate for a meal, you can use a FREE online app ChooseMyPlate 8
There is no one diet for all people with diabetes. There is, however, a “recipe” for eating healthfully that is similar to recommendations for heart health, cancer prevention and weight management.
Healthy Diabetic Eating and Healthy Lifestyle 9 includes:
- Start by knowing how many calories you should be eating and drinking to maintain your weight.
- Limiting foods that are high in sugar.
- Eating smaller portions, spread out over the day.
- Being careful about when and how many carbohydrates you eat.
- Eating a variety of fiber rich whole-grain foods, fruits and vegetables every day.
- Choose poultry and fish without skin and prepare them in healthy ways without added saturated and trans fat. If you choose to eat meat, look for the leanest cuts available and prepare them in healthy and delicious ways.
- Eat a variety of fish at least twice a week, especially fish containing omega-3 fatty acids (for example, salmon, trout and herring).
- Eating less saturated fat and avoid trans fat and replace them with the better fats, monounsaturated and polyunsaturated.
- Limiting your use of alcohol. That means no more than one drink per day if you’re a woman and no more than two drinks per day if you’re a man.
- Lowering salt consumption to less than 1,500 mg day. To lower blood pressure, reducing daily intake to 1,500 mg is desirable because it can lower blood pressure even further. If you can’t meet these goals right now, even reducing sodium intake by 1,000 mg per day can benefit blood pressure.
- Lose excess weight and maintain a healthy weight
- Be physically active. Aim for at least 150 minutes of moderate physical activity or 75 minutes of vigorous physical activity – or an equal combination of both – each week.
- Limit time with the TV, computer, and video.
- Also, don’t smoke tobacco — and avoid secondhand smoke.
In 8 randomised clinical trials 10 with 2241 participants randomised to exercise and diet intervention and 2509 participants to standard recommendation. Furthermore, 178 participants were randomised to an exercise only intervention and 167 participants to a diet only intervention. The duration of the interventions in the trials ranged from one year to six years. Interventions varied between studies but mainly consisted of caloric restriction if the person was overweight, low fat content (especially saturated fat), high carbohydrate content and the increase of fibre intake. Physical activity varied but on average at least 150 minutes each week of brisk walking or other activities such as cycling or jogging were recommended. Interventions were mainly delivered by frequent individual counselling by a physiotherapist, an exercise physiologist and a dietitian. Interventions aimed at increasing exercise combined with diet are able to decrease the incidence of type 2 diabetes mellitus in high risk groups (people with impaired glucose tolerance or the metabolic syndrome) by 37% with exercise and diet. This had favourable effects on body weight, waist circumference and blood pressure 10.
A more recent study to find out the health benefits of soluble dietary fiber on type 2 diabetes 11. A total of 117 patients with type 2 diabetes between the ages of 40 and 70 were assessed. Patients were randomly assigned to one of two groups, and administered extra soluble dietary fiber (10 or 20 g/day), or to a control group (0 g/day) for one month. The 20 g/day soluble dietary fiber group exhibited significantly improved fasting blood glucose and low-density (LDL) lipoprotein “bad cholesterol” levels, as well as a significantly improved insulin resistance index. In addition, 10 and 20 g/day soluble dietary fiber significantly improved the waist and hip circumferences and levels of triglycerides and apolipoprotein A. The results of the present study suggested that increased and regular consumption of soluble dietary fiber led to significant improvements in blood glucose levels, insulin resistance and metabolic profiles 11.
Soluble dietary fiber has been associated with lower postprandial glucose levels and increased insulin sensitivity in diabetic and healthy subjects; these effects were generally attributed to the viscous and/or gelling properties of soluble fiber 12. Soluble dietary fiber exerts physiological effects on the stomach and small intestine that modulate postprandial glycemic responses, including delaying gastric emptying 13, which accounts for ~35% of the variance in peak glucose concentrations following the ingestion of oral glucose 14, modulating gastrointestinal myoelectrical activity and delaying small bowel transit 15, 16, reducing glucose diffusion through the unstirred water layer 17, and reducing the accessibility of α-amylase to its substrates due to the increased viscosity of gut contents 18. Notably, the increased viscosity and gel-forming properties of soluble fiber are predominantly responsible for its glycemic effect, since the hypoglycemic effect can be reversed by the hydrolysis of guar gum or following ultra-high heating and homogenization 13. In addition, the intestinal absorption of carbohydrates was prolonged by soluble dietary fiber, which was partially due to altered incretin levels, including increased glucagon-like peptide 1 levels 18. In experimental clamp studies, soluble dietary fiber also influenced peripheral glucose uptake mechanisms 19, 20, including increasing skeletal muscle expression of the insulin-responsive glucose transporter type 4 (GLUT-4), which enhances skeletal muscle uptake, augments insulin sensitivity and normalizes blood glucose 20. In humans, various fatty acids stimulate the expression of peroxisome proliferator-activated receptor-γ, which increases adipocyte GLUT-4 levels 21.
Increasing dietary fiber intake, which is one of the goals of nutritional counseling, deserves greater attention due to its ability to reduce total cholesterol levels and hyperglycemia in patients with impaired glucose tolerance and type 2 diabetes 22. In addition, increased fiber intake was shown to improve insulin sensitivity and reduce systemic inflammation 23, 24. Previous studies have demonstrated that high-fiber diets (30 g/day) altered biochemical parameters, reduced the severity of type 2 diabetes mellitus and decreased the occurrence of risk factors associated with cardiovascular disease 23, 25. According to Weickert et al 23, nutritional educational studies involving dietary restrictions are typically met with poor treatment compliance. Participants in a previous study were encouraged to progressively alter their eating behaviors, including increasing the frequency of meals and increasing the intake of complex carbohydrates, dietary fiber, fruits, and vegetables, as well as polyunsaturated and monounsaturated fatty acids, including fish and olive oils, respectively 23.
Portion Size Versus Serving Size
Sometimes the portion size and serving size are the same, but sometimes they are not. Over the past few years portions have grown significantly in restaurants, as has the frequency of Americans eating out. Learn how much to put on your plate to help control how much you eat 26.
Here are a couple of important definitions from the National Institutes of Health:
- Portion is how much food you choose to eat at one time, whether in a restaurant, from a package or in your own kitchen. A portion is 100 percent under our control. Many foods that come as a single portion actually contain multiple servings.
- Serving Size is the amount of food listed on a product’s Nutrition Facts label. So all of the nutritional values you see on the label are for the serving size the manufacturer suggests on the package.
Once you understand the difference, it’s easier to determine how much to serve and easier to teach kids the difference between the two. Learn some suggested servings from each food groups you and your kids can eat at mealtime or between meals.
Do you know how much you’re really eating ? Sometimes it’s hard to tell if the portions you are eating are the right serving size for your nutritional needs. Portion sizes have increased drastically over the years, contributing to the rising obesity rate.
Consider these statistics from the American Heart Association and the Robert Woods Johnson Foundation study “A Nation at Risk: Obesity in the United States”:
- Adults today consume an average of 300 more calories per day than they did in 1985.
- Portion sizes have grown dramatically over the last 40 years.
- Americans eat out much more than they used to.
How much carbohydrate do you need each day ?
The daily amount of carbohydrate, protein, and fat for people with diabetes has not been defined—what is best for one person may not be best for another. Everyone needs to get enough carbohydrate to meet the body’s needs for energy, vitamins and minerals, and fiber 27.
- Experts suggest that carbohydrate intake for most people should be between 45 and 65 percent of total calories. People on low-calorie diets and people who are physically inactive may want to aim for the lower end of that range.
One gram of carbohydrate provides about 4 calories, so you’ll have to divide the number of calories you want to get from carbohydrates by 4 to get the number of grams. For example, if you want to eat 1,800 total calories per day and get 45 percent of your calories from carbohydrates, you would aim for about 200 grams of carbohydrate daily. You would calculate that amount as follows:
- 0.45 x 1,800 calories = 810 calories
- 810 ÷ 4 = 202.5 grams of carbohydrate
You’ll need to spread out your carbohydrate intake throughout the day. A dietitian or diabetes educator can help you learn what foods to eat, how much to eat, and when to eat based on your weight, activity level, medicines, and blood glucose targets.
How can you find out how much carbohydrate is in the foods you eat ?
You will need to learn to estimate the amount of carbohydrate in foods you typically eat. For example, the following amounts of carbohydrate-rich foods each contain about 15 grams of carbohydrate 27:
- one slice of bread
- one 6-inch tortilla
- 1/3 cup of pasta
- 1/3 cup of rice
- 1/2 cup of canned or fresh fruit or fruit juice or one small piece of fresh fruit, such as a small apple or orange
- 1/2 cup of pinto beans
- 1/2 cup of starchy vegetables such as mashed potatoes, cooked corn, peas, or lima beans
- 3/4 cup of dry cereal or 1/2 cup cooked cereal
- 1 tablespoon of jelly
Some foods are so low in carbohydrates that you may not have to count them unless you eat large amounts. For example, most nonstarchy vegetables are low in carbohydrates. A 1/2-cup serving of cooked nonstarchy vegetables or a cup of raw vegetables has only about 5 grams of carbohydrate.
As you become familiar with which foods contain carbohydrates and how many grams of carbohydrate are in food you eat, carbohydrate counting will be easier.
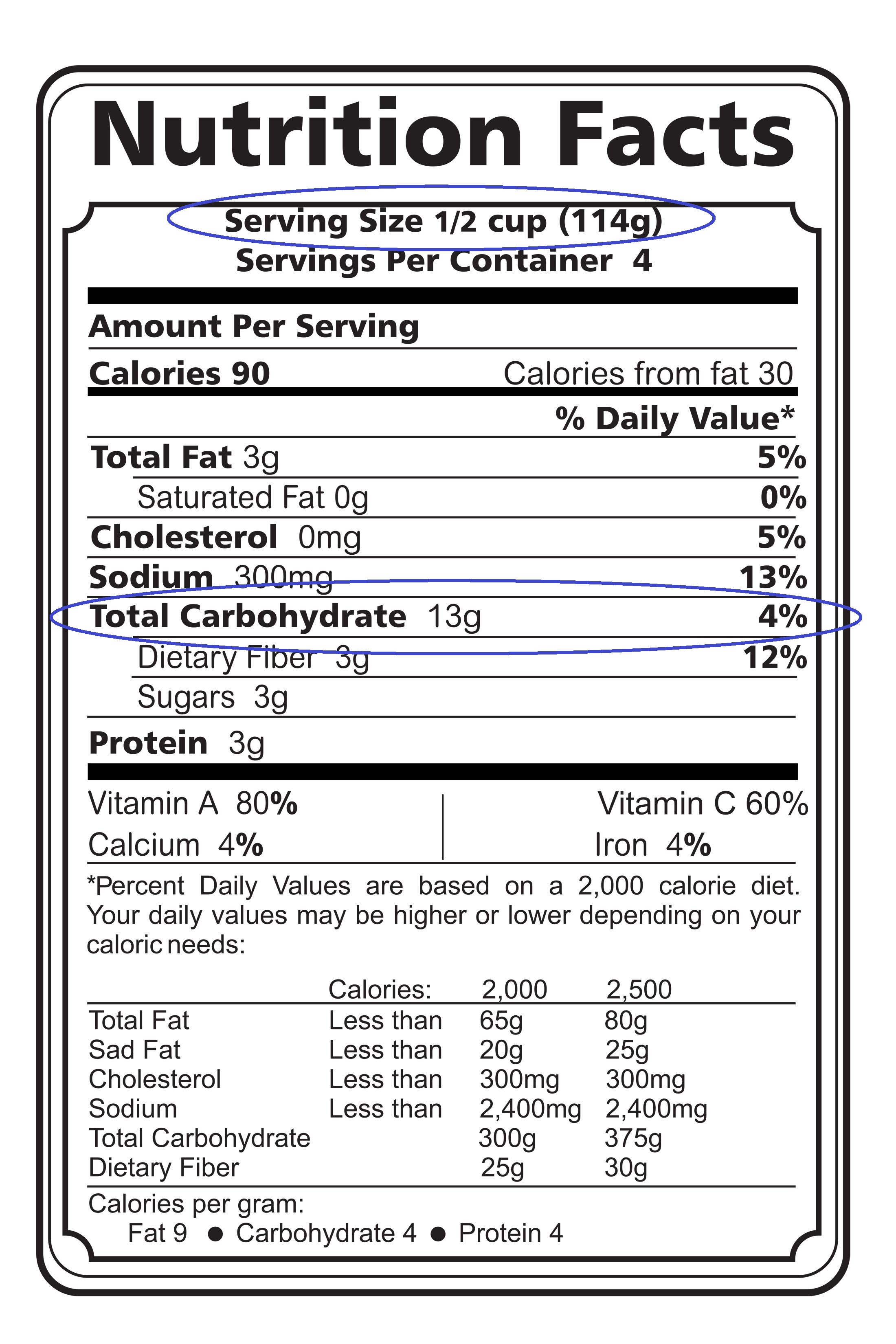
Nutrition Labels
Nutrition labels tell you the total grams of carbohydrate per serving, along with other nutrition information.
Nutrition labels tell you:
- the food’s serving size––such as one slice or 1/2 cup
- the total grams of carbohydrate per serving
- other nutrition information, including calories and the amount of protein and fat per serving
If you have two servings instead of one, such as one cup of pinto beans instead of 1/2 cup, you multiply the number of grams of carbohydrate in one serving—for example, 15—by two to get the total number of grams of carbohydrate—30.
- 15 x 2 = 30
You can find out how many grams of carbohydrate are in the foods you eat by checking the nutrition labels on food packages. Following is an example of a nutrition label:
What is carbohydrate counting ?
Carbohydrate counting, also called carb counting, is a meal planning tool for people with type 1 or type 2 diabetes. Carbohydrate counting involves keeping track of the amount of carbohydrate in the foods you eat each day 27.
The Internet has carbohydrate counting tools that let you enter a type of food and find out what nutrients the food contains, including carbohydrates. Try visiting these sites:
- A calorie and carbohydrate counting tool from the American Diabetes Association 28
- An online database from the U.S. Department of Agriculture Nutrient Data Lab 29
Carbohydrates are one of the main nutrients found in food and drinks. Protein and fat are the other main nutrients. Carbohydrates include sugars, starches, and fiber. Carbohydrate counting can help you control your blood glucose, also called blood sugar, levels because carbohydrates affect your blood glucose more than other nutrients.
The right amount of carbohydrates varies by how you manage your diabetes, including how physically active you are and what medicines you take, if any. Your health care team can help you create a personal eating plan based on carbohydrate counting.
- Healthy carbohydrates, such as whole grains, fruits, and vegetables, are an important part of a healthy eating plan because they can provide both energy and nutrients, such as vitamins and minerals, and fiber. Fiber can help you prevent constipation, lower your cholesterol levels, and control your weight.
- Unhealthy carbohydrates are often food and drinks with added sugars. Although unhealthy carbohydrates can also provide energy, they have little to no nutrients.
The amount of carbohydrate in foods is measured in grams. To count grams of carbohydrate in foods you eat, you’ll need to
- know which foods contain carbohydrates
- learn to estimate the number of grams of carbohydrate in the foods you eat
- add up the number of grams of carbohydrate from each food you eat to get your total for the day
How can carbohydrate counting help you ?
Carbohydrate counting can help keep your blood glucose levels close to normal. Keeping your blood glucose levels as close to normal as possible may help you
- stay healthy longer
- prevent or delay diabetes problems such as kidney disease, blindness, nerve damage, and blood vessel disease that can lead to heart attacks, strokes, and amputations—surgery to remove a body part
- feel better and more energetic
Which foods contain carbohydrates ?
Foods that contain carbohydrates include :
- grains, such as bread, noodles, pasta, crackers, cereals, and rice
- fruits, such as apples, bananas, berries, mangoes, melons, and oranges
- dairy products, such as milk and yogurt
- legumes, including dried beans, lentils, and peas
- snack foods and sweets, such as cakes, cookies, candy, and other desserts
- juices, soft drinks, fruit drinks, sports drinks, and energy drinks that contain sugars
- vegetables, especially “starchy” vegetables such as potatoes, corn, and peas
Potatoes, peas, and corn are called starchy vegetables because they are high in starch. These vegetables have more carbohydrates per serving than nonstarchy vegetables.
Examples of nonstarchy vegetables are asparagus, broccoli, carrots, celery, green beans, lettuce and other salad greens, peppers, spinach, tomatoes, and zucchini.
Foods that do not contain carbohydrates include meat, fish, and poultry; most types of cheese; nuts; and oils and other fats.
What foods and drinks should you limit if you have diabetes ?
Foods and drinks to limit 30 include:
- Fried foods and other foods high in saturated fat and trans fat
- Foods high in salt, also called sodium
- Reduce intake of chips, cookies, cakes, full-fat ice cream, etc.
- Cut back on high calorie snack foods and desserts.
- Sweets, such as baked goods, candy, and ice cream
- Beverages with added sugars, such as juice, regular soda, and regular sports or energy drinks
- Eating too much of even healthful foods can lead to weight gain.
- If you choose to drink alcohol, do so in moderation. (Two or less drinks per day for men and one or less drinks per day for women.)
- Watch your portion sizes.
Drink water instead of sweetened beverages. Consider using a sugar substitute in your coffee or tea.
If you drink alcohol, drink moderately—no more than one drink a day if you’re a woman or two drinks a day if you’re a man. If you use insulin or diabetes medicines that increase the amount of insulin your body makes, alcohol can make your blood glucose level drop too low. This is especially true if you haven’t eaten in a while. It’s best to eat some food when you drink alcohol.
What are added sugars ?
Added sugars are various forms of sugar added to foods or drinks during processing or preparation. Naturally occurring sugars such as those in milk and fruits are not added sugars but are carbohydrates. The most common sources of added sugars for Americans are:
- sugar-sweetened soft drinks, fruit drinks, sports drinks, and energy drinks
- grain-based desserts, such as cakes, cookies, and doughnuts
- milk-based desserts and products, such as ice cream, sweetened yogurt, and sweetened milk
- candy
Reading the list of ingredients for foods and drinks can help you find added sugars, such as
- sugar, raw sugar, brown sugar, and invert sugar—a mixture of fructose and glucose
- corn syrup and malt syrup
- high-fructose corn syrup, often used in soft drinks and juices
- honey, molasses, and agave nectar
- dextrose, fructose, glucose, lactose, and sucrose
For a healthier eating plan, limit foods and drinks with added sugars.
Healthy diabetic eating includes:
- Limiting foods that are high in sugar
- Eating smaller portions, spread out over the day
- Choose healthful foods to support a healthy weight and heart
- Being careful about when and how many carbohydrates you eat
- Eating a variety of whole-grain foods, fruits and vegetables every day
- Limiting your use of alcohol
- Using less salt
To successfully manage diabetes, you need to understand how foods and nutrition affect your body. Food portions and food choices are important. Carbohydrates, fat and protein need to be balanced to ensure blood sugar levels stay as stable as possible. (This is particularly important for people with Type 1 diabetes.)
The key to eating with diabetes is to eat a variety of healthy foods from all food groups, in the amounts your meal plan outlines. For that reason the American Diabetes Association has created:
- The Diabetic Diet Meal Plans 31 and
- A online tool called Create Your Plate 32. With Create Your Plate method, you fill your plate with more non-starchy veggies and smaller portions of starchy foods and protein—no special tools or counting required. You can practice with this interactive tool 32.
The American Diabetes Association’s Create Your Plate online interactive meal planning tool
The American Diabetes Association’s Create Your Plate online interactive meal planning tool divides your daily food requirements according to the percentage daily requirement for each major food groups: 25 percent Protein, 25 percent Grains and Starchy Foods and 50 percent Non-starchy Vegetables 32. Creating your plate lets you still choose the foods you want, but changes the portion sizes so you are getting larger portions of non-starchy vegetables and a smaller portion of starchy foods. The healthy meal combinations are endless.
Using the 7 simple steps to Create Your Plate 32 you can simply and effectively manage your diabetes and lose weight at the same time. When you are ready, you can try new foods within each food category.
Try these seven steps to get started:
- Using your dinner plate, put a line down the middle of the plate. Then on one side, cut it again so you will have three sections on your plate.
- Fill the largest section with non-starchy vegetables.
- Now in one of the small sections, put grains and starchy foods.
- And then in the other small section, put your protein.
- Add a serving of fruit, a serving of dairy or both as your meal plan allows.
- Choose healthy fats in small amounts. For cooking, use oils. For salads, some healthy additions are nuts, seeds, avocado and vinaigrettes.
- To complete your meal, add a low-calorie drink like water, unsweetened tea or coffee.
The food groups are :
Vegetables
- Non-starchy Vegetables 33
The following is a list of common non-starchy vegetables:
- Amaranth or Chinese spinach
- Artichoke
- Artichoke hearts
- Asparagus
- Baby corn
- Bamboo shoots
- Beans (green, wax, Italian)
- Bean sprouts
- Beets
- Brussels sprouts
- Broccoli
- Cabbage (green, bok choy, Chinese)
- Carrots
- Cauliflower
- Celery
- Chayote
- Coleslaw (packaged, no dressing)
- Cucumber
- Daikon
- Eggplant
- Greens (collard, kale, mustard, turnip)
- Hearts of palm
- Jicama
- Kohlrabi
- Leeks
- Mushrooms
- Okra
- Onions
- Pea pods
- Peppers
- Radishes
- Rutabaga
- Salad greens (chicory, endive, escarole, lettuce, romaine, spinach, arugula, radicchio, watercress)
- Sprouts
- Squash (cushaw, summer, crookneck, spaghetti, zucchini)
- Sugar snap peas
- Swiss chard
- Tomato
- Turnips
- Water chestnuts
- Yard-long beans
Generally, non-starchy vegetables have about 5 grams of carbohydrate in ½ cup cooked or 1 cup raw. Most of the carbohydrate is fiber so unless you eat more than 1 cup of cooked or 2 cups of raw at a time, you may not need to count the carbohydrates from the non-starchy vegetables.
The best choices are fresh, frozen and canned vegetables and vegetable juices without added sodium, fat or sugar.
If using canned or frozen vegetables, look for ones that say low sodium or no salt added on the label.
As a general rule, frozen or canned vegetables in sauces are higher in both fat and sodium.
If using canned vegetables with sodium, drain the vegetables and rinse with water. Then cook the rinsed vegetables in fresh water. This will cut back on how much sodium is left on the vegetables.
For good health, try to eat at least 3-5 servings of vegetables a day. This is a minimum and more is better! A serving of vegetables is:
- ½ cup of cooked vegetables or vegetable juice
- 1 cup of raw vegetables
- Starchy Starchy Vegetables and Grains 34
Grains
- At least half of your grains for the day should be whole grains. A whole grain is the entire grain—which includes the bran, germ and endosperm (starchy part).
The most popular grain in the US is wheat so that will be our example. To make 100% whole wheat flour, the entire wheat grain is ground up. “Refined” flours like white and enriched wheat flour include only part of the grain – the starchy part, and are not whole grain. They are missing many of the nutrients found in whole wheat flour.
Examples of whole grain wheat products include 100% whole wheat bread, pasta, tortillas, and crackers. But don’t stop there! There are many whole grains to choose from.
Finding whole grain foods can be a challenge. Some foods only contain a small amount of whole grain but will say it contains whole grain on the front of the package. For all cereals and grains, read the ingredient list and look for the following sources of whole grains as the first ingredient:
Best Choices
- Bulgur (cracked wheat)
- Whole wheat flour/
- Whole oats/oatmeal
- Whole grain corn/corn meal
- Popcorn
- Brown rice
- Whole rye
- Whole grain barley
- Whole farro
- Wild rice
- Buckwheat
- Buckwheat flour
- Triticale
- Millet
- Quinoa
- Sorghum
If you suffer from Celiac disease or gluten intolerance :
- Celiac disease is a digestive disorder. When someone with celiac disease eats food containing gluten, their body reacts by damaging the small intestine. Uncomfortable symptoms such as abdominal pain often occur. The damage to the small intestine also interferes with the body’s ability to make use of the nutrients in food. About 1% of the total population has celiac disease. It is more common in people with type 1 diabetes. An estimated 10% of people with type 1 also have celiac. The only way to manage celiac disease is to completely avoid all foods that have gluten. Following a gluten-free diet will prevent permanent damage to your body and will help you feel better.
- Gluten Intolerance : There are also many people who are said to have a gluten intolerance. When these people eat foods that contain gluten, they also experience uncomfortable symptoms. However, they test negative for celiac disease and actual damage to their small intestine does not occur. More research about gluten intolerance is needed, but avoiding foods with gluten should help to relieve these symptoms.
Gluten is a protein found in wheat, rye, barley and all foods that are made with these grains.
Starchy Vegetables
Starchy vegetables are great sources of vitamins, minerals and fiber . The best choices do not have added fats, sugar or sodium.
Try a variety such as:
- Parsnip
- Plantain
- Potato
- Pumpkin
- Acorn squash
- Butternut squash
- Green Peas
- Corn
Best Choices of Dried Beans, Legumes, Peas and Lentils
Try to include dried beans into several meals per week. They are a great source of protein and are loaded with fiber, vitamins and minerals.
- Dried beans such as black, lima, and pinto
- Lentils
- Dried peas such as black-eyed and split
- Fat-free refried beans
- Vegetarian baked beans
Fruits 35
Wondering if you can eat fruit ? Yes !
Fruits are loaded with vitamins, minerals and fiber just like vegetables.
Fruit contains carbohydrate so you need to count it as part of your meal plan. Having a piece of fresh fruit or fruit salad for dessert is a great way to satisfy your sweet tooth and get the extra nutrition you’re looking for.
The best choices of fruit are any that are fresh, frozen or canned without added sugars.
- Choose canned fruits in juice or light syrup
- Dried fruit and 100% fruit juice are also nutritious choices, but the portion sizes are small so they may not be as filling as other choices. Only 2 tablespoons of dried fruit like raisins or dried cherries contains 15 grams of carbohydrate so be cautious with your portion sizes!
- Includes oranges, melon, berries, apples, bananas, and grapes
For Carbohydrate Counters
- A small piece of whole fruit or about ½ cup of frozen or canned fruit has about 15 grams of carbohydrate. Servings for most fresh berries and melons are from ¾ – 1 cup.
- Fruit juice can range from 1/3 -1/2 cup for 15 grams of carbohydrate.
Fruit can be eaten in exchange for other sources of carbohydrate in your meal plan such as starches, grains, or dairy.
Protein 36
The biggest difference among foods in this group is how much fat they contain, and for the vegetarian proteins, whether they have carbohydrate.
Meats do not contain carbohydrate so they do not raise blood glucose levels. A balanced meal plan usually has about 2-5 ounces of meat.
Most plant-based protein foods, like beans and soy products, and any breaded meats contain carbohydrate. It’s best to read food labels carefully for these foods.
In general there is about 15 grams of carbohydrate in ½ cup beans, and between 5 to 15 grams in soy-based products like veggie burgers and “chicken” nuggets.
The best choices are:
- Plant-based proteins
- Fish and seafood
- Chicken and other poultry
- Cheese and eggs
Fish and Seafood
Try to include fish at least 2 times per week.
- Fish high in omega-3 fatty acids like Albacore tuna, herring, mackerel, rainbow trout, sardines, and salmon
- Other fish including catfish, cod, flounder, haddock, halibut, orange roughy, and tilapia
- Shellfish including clams, crab, imitation shellfish, lobster, scallops, shrimp, oysters.
Poultry
Choose poultry without the skin for less saturated fat and cholesterol.
- Chicken, turkey, cornish hen
Game
- Buffalo, ostrich, rabbit, venison
- Dove, duck, goose, or pheasant (no skin)
Beef, Pork, Veal, Lamb
If you decide to have these, choose the leanest options, which are:
- Select or Choice grades of beef trimmed of fat including: chuck, rib, rump roast, round, sirloin, cubed, flank, porterhouse, T-bone steak, tenderloin
- Beef jerky
- Lamb: chop, leg, or roast
- Organ meats: heart, kidney, liver
- Veal: loin chop or roast
- Pork: Canadian bacon, center loin chop, ham, tenderloin
Cheese and Eggs
- Reduced-fat cheese
- Cottage cheese
- Egg whites and egg substitutes
Dairy 37
Including sources of dairy in your diet is an easy way to get calcium and high-quality protein.
The best choices of dairy products are:
- Fat-free or low-fat (1% milk)
- Plain non-fat yogurt (regular or Greek yogurt)
- non-fat light yogurt (regular or Greek yogurt)
- unflavored fortified soy milk
If you are lactose intolerant or don’t like milk, you may want to try fortified soy milk, rice milk, or almond milk as a source of calcium and vitamin D.
Tips for Carb Counters
- 1 cup of milk or yogurt is equal to 1 small piece of fruit or 1 slice of bread
- Each 1 cup serving of milk or 6 ounce serving of yogurt has about 12 grams of carbohydrate and 8 grams of protein. Greek yogurt is higher in protein than regular yogurt, with about 12 grams per 6 ounce serving.
- If you are trying to switch to lower fat dairy products, take the time to get used to the taste and texture difference. For example, first change from whole milk to 2%. Then to 1% or non-fat milk.
- Switching from whole to 1% milk will save you 70 calories and 4 grams of saturated fat in every serving!
Eat more fiber by eating more whole-grain foods 38. Whole grains can be found in:
- Breakfast cereals made with 100% whole grains.
- Oatmeal.
- Whole grain rice.
- Whole-wheat bread, bagels, pita bread, and tortillas.
What Can you Drink ?
Food often takes center stage when it comes to diabetes. But don’t forget that the beverages you drink can also have an effect on your weight and blood glucose!
The American Diabetes Association recommends choosing zero-calorie or very low-calorie drinks 39. This includes:
- Water
- Unsweetened teas
- Coffee no added sugar
- Diet soda
- Other low-calorie drinks and drink mixes
You can also try flavoring your water with a squeeze of lemon or lime juice for a light, refreshing drink with some flavor. All of these drinks provide minimal calories and carbohydrate. If you choose to drink juice, be sure the label says it is 100% juice with no sugar added. Juice provides a lot of carbohydrates in a small portion, so be sure to count it in your meal plan. Usually about 4 ounces or less of juice contains 15 grams of carbohydrate and 50 or more calories.
What to Avoid
Avoid sugary drinks like regular soda, fruit punch, fruit drinks, energy drinks, sweet tea, and other sugary drinks. These will raise blood glucose and can provide several hundred calories in just one serving! See for yourself:
- One 12-ounce can of regular soda has about 150 calories and 40 grams of carbohydrate. This is the same amount of carbohydrate in 10 teaspoons of sugar!
- One cup of fruit punch and other sugary fruit drinks have about 100 calories (or more) and 30 grams of carbohydrate.
Make your calories count with these nutritious foods:
- Healthy carbohydrates. During digestion, sugars (simple carbohydrates) and starches (complex carbohydrates) break down into blood glucose. Focus on the healthiest carbohydrates, such as fruits, vegetables, whole grains, legumes (beans, peas and lentils) and low-fat dairy products.
- Fiber-rich foods. Dietary fiber includes all parts of plant foods that your body can’t digest or absorb. Fiber moderates how your body digests and helps control blood sugar levels. Foods high in fiber include vegetables, fruits, nuts, legumes (beans, peas and lentils), whole-wheat flour and wheat bran.
- Heart-healthy fish. Eat heart-healthy fish at least twice a week. Fish can be a good alternative to high-fat meats. For example, cod, tuna and halibut have less total fat, saturated fat and cholesterol than do meat and poultry. Fish such as salmon, mackerel, tuna, sardines and bluefish are rich in omega-3 fatty acids, which promote heart health by lowering blood fats called triglycerides. Avoid fried fish and fish with high levels of mercury, such as tilefish, swordfish and king mackerel.
- “Good” fats. Foods containing monounsaturated and polyunsaturated fats can help lower your cholesterol levels. These include avocados, almonds, pecans, walnuts, olives, and canola, olive and peanut oils. But don’t overdo it, as all fats are high in calories.
The glycemic index, or GI, measures how a carbohydrate-containing food raises blood glucose. Foods are ranked based on how they compare to a reference food — either glucose or white bread.
A food with a high GI raises blood glucose more than a food with a medium or low GI.
Meal planning with the GI involves choosing foods that have a low or medium GI. If eating a food with a high GI, you can combine it with low GI foods to help balance the meal.
Examples of carbohydrate-containing foods with a low GI include dried beans and legumes (like kidney beans and lentils), all non-starchy vegetables, some starchy vegetables like sweet potatoes, most fruit, and many whole grain breads and cereals (like barley, whole wheat bread, rye bread, and all-bran cereal).
Meats and fats don’t have a GI because they do not contain carbohydrate.
Low GI Foods (55 or less)
- 100% stone-ground whole wheat or pumpernickel bread
- Oatmeal (rolled or steel-cut), oat bran, muesli
- Pasta, converted rice, barley, bulgar
- Sweet potato, corn, yam, lima/butter beans, peas, legumes and lentils
- Most fruits, non-starchy vegetables and carrots
Medium GI (56-69)
- Whole wheat, rye and pita bread
- Quick oats
- Brown, wild or basmati rice, couscous
High GI (70 or more)
- White bread or bagel
- Corn flakes, puffed rice, bran flakes, instant oatmeal
- Shortgrain white rice, rice pasta, macaroni and cheese from mix
- Russet potato, pumpkin
- Pretzels, rice cakes, popcorn, saltine crackers
- melons and pineapple
What Affects the GI of a Food ?
Fat and fiber tend to lower the GI of a food. As a general rule, the more cooked or processed a food, the higher the GI; however, this is not always true.
Below are a few specific examples of other factors that can affect the GI of a food:
- Ripeness and storage time — the more ripe a fruit or vegetable is, the higher the GI.
- Processing — juice has a higher GI than whole fruit; mashed potato has a higher GI than a whole baked potato, stone ground whole wheat bread has a lower GI than whole wheat bread.
- Cooking methods — how long a food is cooked (al dente pasta has a lower GI than soft-cooked pasta), frying, boiling and baking.
- Fibre: wholegrains and high-fibre foods act as a physical barrier that slows down the absorption of carbohydrate. This is not the same as ‘wholemeal’, where, even though the whole of the grain is included, it has been ground up instead of left whole. For example, some mixed grain breads that include wholegrains have a lower GI than wholemeal or white bread.
- Fat lowers the GI of a food. For example, chocolate has a medium GI because of it’s fat content, and crisps will actually have a lower GI than potatoes cooked without fat.
- Protein lowers the GI of food. Milk and other diary products have a low GI because they are high in protein and contain fat.
- Variety — converted long-grain white rice has a lower GI than brown rice but short-grain white rice has a higher GI than brown rice.
Your food choices matter a lot when you’ve got diabetes. Some are better than others.
Nothing is completely off limits. Even items that you might think of as “the worst” could be occasional treats — in tiny amounts. But they won’t help you nutrition-wise, and it’s easiest to manage your diabetes if you mainly stick to the “best” options.
What is the difference between Glycemic Index (GI) and Glycemic Load (GL) ?
Your blood glucose rises and falls when you eat a meal containing carbs. How high it rises and how long it remains high depends on the quality of the carbohydrates (the GI) and the quantity (the serve size). Glycemic load or GL combines both the quality and quantity of carbohydrate in one ‘number’. It’s the best way to predict blood glucose values of different types and amounts of food.
The formula is:
GL = (GI x available carbohydrate in a 100g serving) divided by 100.
Let’s take a single apple as an example.
It has a GI of 40 and it contains 15 grams of carbohydrate.
GL = 40 x 15/100 = 6 g
What about a small baked potato?
Its GI is 80 and it contains 15 g of carbohydrate.
GL = 80 x 15/100 = 12 g
You can think of GL as the amount of carbohydrate in a food “adjusted” for its glycemic potency.
- Low GL = <10
- Medium GL = 11-19
- High GL = >20
Therefore the Glycemic Load takes into account the amount of carbohydrate consumed and is a more accurate measure of the impact of a food on blood sugars. As a general rule foods that have a low GL usually have a low GI and those with a medium to high GL value almost always have a very high GI value.
Here is an abbreviated chart of the glycemic index and glycemic load, per serving, for more than 100 common foods.
| FOOD | Glycemic index (glucose = 100) | Serving size (grams) | Glycemic load per serving |
| BAKERY PRODUCTS AND BREADS | |||
| Banana cake, made with sugar | 47 | 60 | 14 |
| Banana cake, made without sugar | 55 | 60 | 12 |
| Sponge cake, plain | 46 | 63 | 17 |
| Vanilla cake made from packet mix with vanilla frosting (Betty Crocker) | 42 | 111 | 24 |
| Apple muffin, made with rolled oats and sugar | 44 | 60 | 13 |
| Apple muffin, made with rolled oats and without sugar | 48 | 60 | 9 |
| Waffles, Aunt Jemima® | 76 | 35 | 10 |
| Bagel, white, frozen | 72 | 70 | 25 |
| Baguette, white, plain | 95 | 30 | 14 |
| Coarse barley bread, 80% kernels | 34 | 30 | 7 |
| Hamburger bun | 61 | 30 | 9 |
| Kaiser roll | 73 | 30 | 12 |
| Pumpernickel bread | 56 | 30 | 7 |
| 50% cracked wheat kernel bread | 58 | 30 | 12 |
| White wheat flour bread, average | 75 | 30 | 11 |
| Wonder® bread, average | 73 | 30 | 10 |
| Whole wheat bread, average | 69 | 30 | 9 |
| 100% Whole Grain® bread (Natural Ovens) | 51 | 30 | 7 |
| Pita bread, white | 68 | 30 | 10 |
| Corn tortilla | 52 | 50 | 12 |
| Wheat tortilla | 30 | 50 | 8 |
| BEVERAGES | |||
| Coca Cola® (US formula) | 63 | 250 mL | 16 |
| Fanta®, orange soft drink | 68 | 250 mL | 23 |
| Lucozade®, original (sparkling glucose drink) | 95 | 250 mL | 40 |
| Apple juice, unsweetened | 41 | 250 mL | 12 |
| Cranberry juice cocktail (Ocean Spray®) | 68 | 250 mL | 24 |
| Gatorade, orange flavor (US formula) | 89 | 250 mL | 13 |
| Orange juice, unsweetened, average | 50 | 250 mL | 12 |
| Tomato juice, canned, no sugar added | 38 | 250 mL | 4 |
| BREAKFAST CEREALS AND RELATED PRODUCTS | |||
| All-Bran®, average | 44 | 30 | 9 |
| Coco Pops®, average | 77 | 30 | 20 |
| Cornflakes®, average | 81 | 30 | 20 |
| Cream of Wheat® | 66 | 250 | 17 |
| Cream of Wheat®, Instant | 74 | 250 | 22 |
| Grape-Nuts® | 75 | 30 | 16 |
| Muesli, average | 56 | 30 | 10 |
| Oatmeal, average | 55 | 250 | 13 |
| Instant oatmeal, average | 79 | 250 | 21 |
| Puffed wheat cereal | 80 | 30 | 17 |
| Raisin Bran® | 61 | 30 | 12 |
| Special K® (US formula) | 69 | 30 | 14 |
| GRAINS | |||
| Pearled barley, average | 25 | 150 | 11 |
| Sweet corn on the cob | 48 | 60 | 14 |
| Couscous | 65 | 150 | 9 |
| Quinoa | 53 | 150 | 13 |
| White rice, boiled, type non-specified | 72 | 150 | 29 |
| Quick cooking white basmati | 63 | 150 | 26 |
| Brown rice, steamed | 50 | 150 | 16 |
| Parboiled Converted white rice (Uncle Ben’s®) | 38 | 150 | 14 |
| Whole wheat kernels, average | 45 | 50 | 15 |
| Bulgur, average | 47 | 150 | 12 |
| COOKIES AND CRACKERS | |||
| Graham crackers | 74 | 25 | 13 |
| Vanilla wafers | 77 | 25 | 14 |
| Shortbread | 64 | 25 | 10 |
| Rice cakes, average | 82 | 25 | 17 |
| Rye crisps, average | 64 | 25 | 11 |
| Soda crackers | 74 | 25 | 12 |
| DAIRY PRODUCTS AND ALTERNATIVES | |||
| Ice cream, regular, average | 62 | 50 | 8 |
| Ice cream, premium (Sara Lee®) | 38 | 50 | 3 |
| Milk, full-fat, average | 31 | 250 mL | 4 |
| Milk, skim, average | 31 | 250 mL | 4 |
| Reduced-fat yogurt with fruit, average | 33 | 200 | 11 |
| FRUITS | |||
| Apple, average | 36 | 120 | 5 |
| Banana, raw, average | 48 | 120 | 11 |
| Dates, dried, average | 42 | 60 | 18 |
| Grapefruit | 25 | 120 | 3 |
| Grapes, black | 59 | 120 | 11 |
| Oranges, raw, average | 45 | 120 | 5 |
| Peach, average | 42 | 120 | 5 |
| Peach, canned in light syrup | 52 | 120 | 9 |
| Pear, raw, average | 38 | 120 | 4 |
| Pear, canned in pear juice | 44 | 120 | 5 |
| Prunes, pitted | 29 | 60 | 10 |
| Raisins | 64 | 60 | 28 |
| Watermelon | 72 | 120 | 4 |
| BEANS AND NUTS | |||
| Baked beans | 40 | 150 | 6 |
| Black-eyed peas | 50 | 150 | 15 |
| Black beans | 30 | 150 | 7 |
| Chickpeas | 10 | 150 | 3 |
| Chickpeas, canned in brine | 42 | 150 | 9 |
| Navy beans, average | 39 | 150 | 12 |
| Kidney beans, average | 34 | 150 | 9 |
| Lentils | 28 | 150 | 5 |
| Soy beans, average | 15 | 150 | 1 |
| Cashews, salted | 22 | 50 | 3 |
| Peanuts | 13 | 50 | 1 |
| PASTA and NOODLES | |||
| Fettucini | 32 | 180 | 15 |
| Macaroni, average | 50 | 180 | 24 |
| Macaroni and Cheese (Kraft®) | 64 | 180 | 33 |
| Spaghetti, white, boiled, average | 46 | 180 | 22 |
| Spaghetti, white, boiled 20 min | 58 | 180 | 26 |
| Spaghetti, whole-grain, boiled | 42 | 180 | 17 |
| SNACK FOODS | |||
| Corn chips, plain, salted | 42 | 50 | 11 |
| Fruit Roll-Ups® | 99 | 30 | 24 |
| M & M’s®, peanut | 33 | 30 | 6 |
| Microwave popcorn, plain, average | 65 | 20 | 7 |
| Potato chips, average | 56 | 50 | 12 |
| Pretzels, oven-baked | 83 | 30 | 16 |
| Snickers Bar®, average | 51 | 60 | 18 |
| VEGETABLES | |||
| Green peas | 54 | 80 | 4 |
| Carrots, average | 39 | 80 | 2 |
| Parsnips | 52 | 80 | 4 |
| Baked russet potato | 111 | 150 | 33 |
| Boiled white potato, average | 82 | 150 | 21 |
| Instant mashed potato, average | 87 | 150 | 17 |
| Sweet potato, average | 70 | 150 | 22 |
| Yam, average | 54 | 150 | 20 |
| MISCELLANEOUS | |||
| Hummus (chickpea salad dip) | 6 | 30 | 0 |
| Chicken nuggets, frozen, reheated in microwave oven 5 min | 46 | 100 | 7 |
| Pizza, plain baked dough, served with parmesan cheese and tomato sauce | 80 | 100 | 22 |
| Pizza, Super Supreme (Pizza Hut®) | 36 | 100 | 9 |
| Honey, average | 61 | 25 | 12 |
The complete list of the glycemic index and glycemic load for more than 1,000 foods can be found in the article “International tables of glycemic index and glycemic load values: 2008” by Fiona S. Atkinson, Kaye Foster-Powell, and Jennie C. Brand-Miller in the December 2008 issue of Diabetes Care, Vol. 31, number 12, pages 2281-2283. (Source 40).
Benefits of Low Glycaemic Index or Low Glycaemic Load Diets for Diabetes Mellitus
To assess the effects of low glycaemic index or low glycaemic load, diets on glycaemic control in people with diabetes, eleven relevant randomised controlled trials, lasting 1 to 12 months, involving 402 participants were analysed 41.
There was a significant decrease in the glycated haemoglobin A1c (HbA1c) -0.5%. Episodes of hypoglycaemia were significantly fewer with low glycaemic index or low glycaemic load compared to high GI diet in one trial (difference of -0.8 episodes per patient per month), and proportion of participants reporting more than 15 hyperglycaemic episodes per month was lower for low-GI diet compared to measured carbohydrate exchange diet in another study (35% versus 66%). No study reported on mortality, morbidity or costs. The review authors concluded a low-GI diet can improve glycaemic control in diabetes without compromising hypoglycaemic events 41. This result is consistent with another smaller trial involving eight type 2 diabetes mellitus patients who were given carbohydrate foods with either a high or low glycemic index over a 2 weeks period 42.
I) Starches
Your body needs carbs. But you want to choose wisely. Use this list as a guide.
Best Choices
- Whole grains, such as brown rice, oatmeal, quinoa, millet, or amaranth
- Baked sweet potato
- Items made with whole grains and no (or very little) added sugar
Worst Choices
- Processed grains, such as white rice or white flour
- Cereals with little whole grains and lots of sugar
- White bread
- French fries
- Fried white-flour tortillas
II) Vegetables
Load up! You’ll get fiber and very little fat or salt (unless you add them). Remember, potatoes and corn count as carbs.
Best Choices
- Fresh veggies, eaten raw or lightly steamed, roasted, or grilled
- Plain frozen vegetables, lightly steamed
- Greens such as kale, spinach, and arugula. Iceberg lettuce is not as great, because it’s low in nutrients.
- Low sodium or unsalted canned vegetables
- Go for a variety of colors: dark greens, red or orange (think of carrots or red peppers), whites (onions) and even purple (eggplants). The 2015 U.S. guidelines recommend 2.5 cups of veggies per day.
Worst Choices
- Canned vegetables with lots of added sodium
- Veggies cooked with lots of added butter, cheese, or sauce
- Pickles, if you need to limit sodium — otherwise, pickles are okay.
- Sauerkraut, for the same reason as pickles — so, limit them if you have high blood pressure
Vegetarian Diets Linked to Lower Mortality
Adults who eat a more plant-based diet may be boosting their chance of living longer, according to a large analysis.
Researchers studied more than 73,000 Seventh-day Adventist men and women ages 25 and older 43. The participants were categorized into dietary groups at the time of recruitment based on their reported food intake during the previous year. Nearly half of the participants were nonvegetarian, eating red meat, poultry, fish, milk and eggs more than once a week. Of the remaining, 8% were vegan (eating red meat, fish, poultry, dairy or eggs less than once a month); 29% were lacto-ovo vegetarians (eating eggs and/or dairy products, but red meat, fish or poultry less than once per month); 10% were pesco-vegetarians (eating fish, milk and eggs but rarely red meat or poultry); and 5% were semi-vegetarian (eating red meat, poultry and fish less than once per week).
Over about 6 years, there were 2,570 deaths among the participants. The researchers found that vegetarians (those with vegan, and lacto-ovo-, pesco-, and semi-vegetarian diets) were 12% less likely to die from all causes combined compared to nonvegetarians. The death rates for subgroups of vegans, lacto-ovo–vegetarians, and pesco-vegetarians were all significantly lower than those of nonvegetarians.
Those on a vegetarian diet tended to have a lower rate of death due to cardiovascular disease, diabetes, and renal disorders such as kidney failure. No association was detected in this study between diet and deaths due to cancer. The researchers also found that the beneficial associations between a vegetarian diet and mortality tended to be stronger in men than in women.
The researchers note several limitations to the study. Participants only reported their diet at the beginning of the study, and their eating patterns might have changed over time. In addition, they were only followed for an average of 6 years; it may take longer for dietary patterns to influence mortality 43.
III) Fruits
They give you carbohydrates, vitamins, minerals, and fiber. Most are naturally low in fat and sodium. But they tend to have more carbs than vegetables do.
Best Choices
- Fresh fruit
- Plain frozen fruit or fruit canned without added sugar
- Sugar-free or low-sugar jam or preserves
- No-sugar-added apple sauce
Worst Choices
- Canned fruit with heavy sugar syrup
- Chewy fruit rolls
- Regular jam, jelly, and preserves (unless you have a very small portion)
- Sweetened apple sauce
- Fruit punch, fruit drinks, fruit juice drinks
IV) Protein
You have lots of choices, including beef, chicken, fish, pork, turkey, seafood, beans, cheese, eggs, nuts, and tofu.
Best Choices
The American Diabetes Association lists these as the top options:
- Plant-based proteins, such as beans, nuts, seeds, or tofu
- Fish and seafood
- Chicken and other poultry (Choose the breast meat if possible.)
- Eggs and low-fat dairy
If you eat meat, keep it low in fat. Trim the skin off poultry.
Try to include some plant-based protein from beans, nuts, or tofu, even if you’re not a vegetarian or vegan. You’ll get nutrients and fiber that aren’t in animal products.
Worst Choices
- Fried meats
- Higher-fat cuts of meat, such as ribs
- Pork bacon
- Regular cheeses
- Poultry with skin
- Deep-fried fish
- Deep-fried tofu
- Beans prepared with lard
V) Dairy
Keep it low in fat. If you want to splurge, keep your portion small.
Best Choices
- 1% or skim milk
- Low-fat yogurt
- Low-fat cottage cheese
- Low-fat or nonfat sour cream
Worst Choices
- Regular yogurt
- Regular cottage cheese
- Regular sour cream
- Regular ice cream
- Regular half-and-half
VI) Fats, Oils, and Sweets
They’re tough to resist. But it’s easy to get too much and gain weight, which makes it harder to manage your diabetes.
Best Choices
- Natural sources of vegetable fats, such as nuts, seeds, or avocados (high in calories, so keep portions small)
- Foods that give you omega-3 fatty acids, such as salmon, tuna, or mackerel
- Plant-based oils, such as canola, grapeseed, or olive oils
Worst Choices
- Anything with artificial trans fat in it. It’s bad for your heart. Check the ingredient list for anything that’s “partially hydrogenated,” even if the label says it has 0 grams of trans fat.
VII) Drinks
When you down a favorite drink, you may get more calories, sugar, salt, or fat than you bargained for. Read the labels so you know what’s in a serving.
Best Choices
- Water, unflavored or flavored sparkling water
- Unsweetened tea (add a slice of lemon)
- Coffee, black or with added low-fat milk and sugar substitute
Worst Choices
- Light beer, small amounts of wine, or non-fruity mixed drinks
- Regular sodas
- Regular beer, fruity mixed drinks, dessert wines
- Sweetened tea
- Coffee with sugar and cream
- Flavored coffees and chocolate drinks
- Energy drinks
The 1200 Calories Diabetic Diet (Low Calorie Diet)
The 1200 calorie diet is a low-calorie diet (LCD) 44. The 1200 calorie diet is not used for diabetics or as a substitute to healthy diabetic diet outline above, instead the 1200 calories diet (low-calorie diet) is used mainly to treat obesity and for weight loss.
A typical LCD may provide:
- 1,000–1,200 calories/day for a woman
- 1,200–1,600 calories/day for a man
The number of calories may be adjusted based on your age, weight, and how active you are. A 1200 calorie diet is a low-calorie diet usually consists of regular foods, but could also include meal replacements. As a result, you may find this type of diet much easier to follow than a very low calorie diet. In the long term, 1200 calorie diet is a low-calorie diets have been found to lead to the same amount of weight loss as very low calorie diets (VLCDs) 44.
- Traditional American Cuisine (non-diabetic) : 1,200 Calories
| Breakfast | Energy (Kcal) | Fat (GM) | %Fat | Exchange for: |
|---|---|---|---|---|
| Whole-wheat bread, 1 med. slice | 70 | 1.2 | 15 | (1 Bread/Starch) |
| Jelly, regular, 2 tsp | 30 | 0 | 0 | (½ Fruit) |
| Cereal, shredded wheat, ½ C | 104 | 1 | 4 | (1 Bread/Starch) |
| Milk, 1%, 1 C | 102 | 3 | 23 | (1 Milk) |
| Orange juice, ¾ C | 78 | 0 | 0 | (1½ Fruit) |
| Coffee, regular, 1 C | 5 | 0 | 0 | (Free) |
| Breakfast Total | 389 | 5.2 | 10 |
| Lunch | Energy (Kcal) | Fat (GM) | %Fat | Exchange for: |
|---|---|---|---|---|
| Roast beef sandwich | ||||
| Whole-wheat bread, 2 med. slices | 139 | 2.4 | 15 | (2 Bread/Starch) |
| Lean roast beef, unseasoned, 2oz | 60 | 1.5 | 23 | (2 Lean Protein) |
| Lettuce, 1 leaf | 1 | 0 | 0 | |
| Tomato, 3 med. slices | 10 | 0 | 0 | (1 Vegetable) |
| Mayonnaise, low-calorie, 1 tsp | 15 | 1.7 | 96 | (1⁄3 Fat) |
| Apple, 1 med. | 80 | 0 | 0 | (1 Fruit) |
| Water, 1 C | 0 | 0 | 0 | (Free) |
| Lunch Total | 305 | 5.6 | 16 |
| Dinner | Energy (Kcal) | Fat (GM) | %Fat | Exchange for: |
|---|---|---|---|---|
| Salmon, 2 oz edible | 103 | 5 | 40 | (2 Lean Protein) |
| Vegetable oil, 1½ tsp | 60 | 7 | 100 | (1½ Fat) |
| Baked potato, ¾ med. | 100 | 0 | 0 | (1 Bread/Starch) |
| Margarine, 1 tsp | 34 | 4 | 100 | (1 Fat) |
| Green beans, seasoned with margarine, ½ C | 52 | 2 | 4 | (1 Vegetable) (½ Fat) |
| Carrots, seasoned | 35 | 2 | 0 | (1 Vegetable) |
| White dinner roll, 1 small | 70 | 2 | 26 | (1 Bread/Starch) |
| Iced tea, unsweetened, 1 C | 0 | 0 | 0 | (Free) |
| Water, 2 C | 0 | 0 | 0 | (Free) |
| Dinner Total | 454 | 20 | 39 |
| Snack | Energy (Kcal) | Fat (GM) | %Fat | Exchange for: |
|---|---|---|---|---|
| Popcorn, 2½ C | 69 | 0 | 0 | (1 Bread/Starch) |
| Margarine, ¾ tsp | 30 | 3 | 100 | (¾ Fat) |
| Grand Total | 1,247 | 34 | 24 |
| Calories: | 1,247 | SFA, % kcals: | 7 | |
| Total Carb, % kcals: | 58 | Cholesterol, mg: | 96 | |
| Total Fat, % kcals: | 26 | Protein, % kcals: | 19 | |
| Sodium,* mg: | 1,043 |
(Source 45).
In a multi-center, randomized controlled trial, designed to determine whether intentional weight loss reduces cardiovascular morbidity and mortality in overweight individuals with type 2 diabetes 46. The study involving a total of 5,145 participants, with a mean age of 60 years and body mass index of 36.0 kg/m2 (obese), who have been randomly assigned to a lifestyle intervention or to enhanced usual care condition (i.e., Diabetes Support and Education).
In that Look AHEAD study 46, the participants were instructed to do unsupervised at home moderately-intense physical activity to ≥ 175 minutes a week (engage in brisk walking or similar aerobic activity). And are encouraged to replace two meals and one snack a day with liquid shakes and meal bars.
As part of the dietary intervention 46, participants are instructed to eat a self-selected diet of conventional foods but restrict their intake of fat as a mean to reduce total calories. They are prescribed < 30% of calories from fat, with < 10% from saturated fat. This is similar to the diet prescribed in the the Diabetes Prevention Program 47.
- The energy goal for persons < 114 kg (250 lb) is 1200−1500 kcal/d and
- 1500−1800 kcal/d for individuals ≥ 114 kg.
- Participants count calories and fat grams with the aid of a booklet provided.
Portion control: During weeks 3−19, a portion-controlled meal plan is prescribed to facilitate participants’ adherence to their calorie goals. All individuals are encouraged to replace two meals (typically breakfast and lunch) with a liquid shake and one snack with a bar 48. They are to consume an evening meal of conventional foods (which includes the option of frozen food entrees) and to add fruits and vegetables to their diet until they reach their daily calorie goal. Participants potentially can choose from four meal replacements, including SlimFast (SlimFast Foods), Glucerna (Ross Laboratories), OPTIFAST (Novartis Nutrition) and HMR (HMR, Inc.). All products are provided free of charge. Persons who decline meal replacements are provided detailed menu plans that specify conventional foods to be consumed. A variety of meals are offered but all are intended to control portion sizes and calories. From weeks 20−22, participants decrease their use of meal replacements while increasing the consumption of conventional foods.
Rationale for portion control: Meal replacements were included, within a diet of 1200−1500 kcal/d, because they significantly increase weight loss compared with prescribing isocaloric diets comprised of conventional foods 48. A meta-analysis of six randomised control trials showed that liquid meal replacements induced a loss approximately 3 kg greater than that produced by a conventional diet 49. Obese individuals typically underestimate their calorie intake by 40%−50% when consuming a diet of conventional foods 50 because of difficulty in estimating portion sizes, macronutrient composition, and calorie content, as well as in remembering all foods consumed. Meal replacements appear to decrease these difficulties and simplify food choices. Portion-controlled servings of conventional foods similarly facilitate weight loss, as shown by Jeffery and Wing 51, and other investigators 52, 53. Ultimately, simply providing patients detailed menu plans, with accompanying shopping lists, provides sufficient structure to significantly increase weight loss 54.
Look AHEAD investigators initially were concerned that the high sugar content of some meal replacement products might adversely affect glycemic control. This concern, however, was alleviated by findings in patients with type 2 diabetes that a meal-replacement plan (that included SlimFast) was associated with significantly greater weight losses and reductions in fasting blood sugar than was a conventional reducing diet with the same calorie goal 55. Additional studies found that when participants achieved significant negative energy balance, as expected in Look AHEAD, short-term gylcemic control improved, independent of weight loss 56, 57.
Conclusion of the Look AHEAD Study: The Look AHEAD’s Intensive Lifestyle Intervention produced clinically meaningful weight loss (≥5%) at year 8 in 50% of patients with type 2 diabetes and can be used to manage other obesity-related co-morbid conditions.
The Diabetes Prevention Program trial 47 was a major multicenter clinical research study aimed at discovering whether modest weight loss through dietary changes and increased physical activity or treatment with the oral diabetes drug metformin (Glucophage) could prevent or delay the onset of type 2 diabetes in study participants. At the beginning of the Diabetes Prevention Program trial, participants were all overweight and had blood glucose, also called blood sugar, levels higher than normal but not high enough for a diagnosis of diabetes—a condition called prediabetes.
In the DPP, participants from 27 clinical centers around the United States were randomly divided into different treatment groups. The first group, called the lifestyle intervention group, received intensive training in diet, physical activity, and behavior modification. By eating less fat and fewer calories and exercising for a total of 150 minutes a week, they aimed to lose 7 percent of their body weight and maintain that loss.
The second group took 850 mg of metformin twice a day. The third group received placebo pills instead of metformin. The metformin and placebo groups also received information about diet and exercise but no intensive motivational counseling. A fourth group was treated with the drug troglitazone (Rezulin), but this part of the study was discontinued after researchers discovered that troglitazone can cause serious liver damage. The participants in this group were followed but not included as one of the intervention groups.
All 3,234 study participants (1,079 randomized to lifestyle intervention) were overweight and had prediabetes, averaged 51 years of age at baseline, with 20% aged ≥60 years; 68% were women, 55% were Caucasian. Which are well-known risk factors for the development of type 2 diabetes. In addition, 45 percent of the participants were from minority groups-African American, Alaska Native, American Indian, Asian American, Hispanic/Latino, or Pacific Islander-at increased risk of developing diabetes.
The calorie goals were calculated by estimating the daily calories needed to maintain the participant’s starting weight and subtracting 500–1,000 calories/day (depending on initial body weight) to achieve a 1–2 pound per week weight loss. The fat goals, given in grams of fat per day, were based on 25% of calories from fat. The fat and calorie goals were used as a means to achieve the weight loss goal rather than as a goal in and of itself. Therefore, if a participant reported consuming more than the calorie or fat goal but was losing weight as planned, the coach did not emphasize greater calorie or fat reduction. Participants were encouraged to gradually achieve the fat and calorie levels through better choices of meals and snack items, healthier food preparation techniques, and careful selection of restaurants, including fast food, and the items offered. Four standard calorie levels were used:
- 1,200 kcal/day (33 g fat) for participants with an initial body weight of 120–170 lbs,
- 1,500 kcal/day (42 g fat) for participants with a body weight of 175–215 lbs,
- 1,800 kcal/day (50 g fat) for participants with a body weight of 220–245 lbs and
- 2,000 kcal/ day (55 g fat) for participants weighing >250 lbs.
In the Diabetes Prevention Program trial 47 the goal for physical activity was selected to approximate at least 700 kcal/week expenditure from physical activities. For ease of translation to participants, this goal was described as at least 150 min of moderate physical activities similar in intensity to brisk walking. This goal was adopted for the Diabetes Prevention Program trial because it was determined to be achievable and likely to be beneficial in preventing diabetes based on previous studies.
Conclusion of the DPP trial: The DPP’s results indicate that millions of high-risk people can delay or avoid developing type 2 diabetes by losing weight through regular physical activity and a diet low in fat and calories. Weight loss and physical activity lower the risk of diabetes by improving the body’s ability to use insulin and process glucose. The DPP also suggests that taking metformin can help delay the onset of diabetes, although less dramatically 58.
Vegetarian Diets and Diabetes
More and more people are choosing to follow a vegetarian diet for many different reasons. It’s estimated that two per cent of the population now don’t eat meat or fish 59.
Reasons for switching to a vegetarian diet include:
- the health benefits
- ethical and moral reasons
- religious or cultural reasons
- concern for animal welfare
- concern about the environment and sustainability
- taste – some people just don’t like the taste of meat or fish.
A vegetarian diet, based on unprocessed foods, can provide many health benefits for us all, whether or not you have diabetes.
If you have diabetes, it’s important to be more aware of how what you eat affects your body and, in turn, you’ll hopefully become more health conscious.
So what is a vegetarian diet ? Are there any ways it could help manage diabetes ? Does it provide any health benefits for people with diabetes ?
For advice and help with what to eat and including vegetarian recipes go to the Vegetarian Society 60.
What is a vegetarian ?
According to the Vegetarian Society 61, a vegetarian is:
- “Someone who lives on a diet of grains, pulses, legumes, nuts, seeds, vegetables, fruits, fungi, algae, yeast and/or some other non-animal-based foods (e.g. salt) with, or without, dairy products, honey and/or eggs. A vegetarian does not eat foods that consist of, or have been produced with the aid of products consisting of or created from, any part of the body of a living or dead animal. This includes meat, poultry, fish, shellfish*, insects, by-products of slaughter** or any food made with processing aids created from these.”
- * Shellfish are typically ‘a sea animal covered with a shell’. We take shellfish to mean; Crustaceans (hard external shell) e.g. lobsters, crayfish, crabs, prawns, shrimps; Molluscs (most are protected by a shell) e.g. mussels, oysters, winkles, limpets, clams, etc. Also includes cephalopods such as cuttlefish, squid, octopus.
- ** By-products of slaughter includes gelatine, isinglass and animal rennet.
- Eggs: Many lacto-ovo vegetarians will only eat free-range eggs. This is because of welfare objections to the intensive farming of hens. Through its Vegetarian Society Approved trademark scheme, the Vegetarian Society will only license its trademark to products containing free-range eggs where eggs are used.
There are different types of vegetarians:
- Lacto-ovo-vegetarians eat both dairy products and eggs (usually free range). This is the most common type of vegetarian diet 62.
- Lacto-vegetarians eat dairy products, but avoid eggs.
- Ovo-vegetarian. Eats eggs but not dairy products.
- Vegans do not any products derived from animals – no meat, fish, dairy or eggs.
For advice and help with what to eat and including vegetarian recipes go to the Vegetarian Society 60.
It is important to keep an eye on portions sizes of high-fat foods such as cheese and nuts or you might find yourself putting on weight. With the increased risk of cardiovascular disease in people with diabetes, keeping your weight under control and reducing blood pressure and blood cholesterol are all essential and plant-based foods can help with these.
Why you may try a vegetarian diet ?
Plant-based foods, particularly fruit and vegetables, nuts, pulses and seeds have been shown to help in the treatment of many chronic diseases and are often associated with lower rates of Type 2 diabetes, less hypertension, lower cholesterol levels and reduced cancer rates 63.
These foods are also higher in fibre, antioxidants, folate and phytochemicals, which are all good for our general health.
Vegetarian diets have been shown to be beneficial for people with Type 2 diabetes where weight loss is often the most effective way to manage the condition. A wholefood vegetarian diet often contains fewer calories and can help you to maintain a healthy body weight.
In a review of scientific publications from 1946- December 2013, it was found that the consumption of vegetarian diets was associated with a significant reduction in HbA1c and a non-significant reduction in fasting blood glucose concentration 64.
In another randomised study with 74 patients with type 2 diabetes, who were given either calorie restricted (-500 kcal/day) vegetarian diet (37 subjects) or calorie restricted (-500 kcal/day) conventional diabetic diet (37 subjects) over 24 weeks 65. In the second 12 weeks of the study, the calorie restricted diets were combined with aerobic exercise. Participants were examined at baseline, 12 weeks and 24 weeks. Forty-three per cent of participants in the calorie restricted (-500 kcal/day) vegetarian diet group and 5% of participants in the calorie restricted (-500 kcal/day) conventional diabetic diet group reduce their diabetes medication. Body weight decreased more in the calorie restricted vegetarian diet group (-6.2 kg) than in the calorie restricted conventional diabetic diet group (-3.2 kg). An increase in insulin sensitivity was significantly greater in the calorie restricted vegetarian diet group than in the calorie restricted conventional diabetic diet group. A reduction in both visceral and subcutaneous fat was greater in the calorie restricted vegetarian diet group than in the calorie restricted conventional diabetic diet group. Plasma adiponectin increased (a protein hormone produced and secreted exclusively by adipocytes (fat cells) that regulates the metabolism of lipids and glucose. High blood levels of adiponectin are associated with a reduced risk of heart attack. Low levels of adiponectin are found in people who are obese (and who are at increased risk of a heart attack) and leptin decreased (a hormone produced mainly by adipocytes (fat cells) that is involved in the regulation of body fat. Leptin interacts with areas of the brain that control hunger and behavior and signals that the body has had enough to eat. Leptin tells your brain that you have enough energy stored in your fat cells to engage in normal) in the calorie restricted vegetarian diet group, with no change in the calorie restricted conventional diabetic diet group. Differences between groups were greater after the addition of exercise training. Changes in insulin sensitivity and enzymatic oxidative stress markers correlated with changes in visceral fat 65.
Low Calorie Diet on Weight Loss and the Metabolic Profile of Obese Patients with Type 2 Diabetes Mellitus
A small study 66 with 60 patients (23 males and 37 postmenopausal females) who have type 2 diabetes and are obese, to compare the effects of low calorie diet (1800 kcal/day) plus intensive insulin therapy (4 insulin injections/day) versus low calorie diet (1800 kcal/day) plus conventional insulin therapy (2/3 insulin injections/day). At 6 months post-interventions, there were significant reductions were observed in the body weight, body mass index (BMI), HbA1c for all participants and cholesterol. At 1 year, median body weight reduction was 4.5 kg for patients on low calorie diet (1800 kcal/day) plus intensive insulin therapy and 4.8 kg for those on low calorie diet (1800 kcal/day) plus conventional insulin therapy. The conclusion was a 12-month 1800-kcal low calorie dietary intervention achieved significant body weight loss and HbA1c reductions irrespectively of insulin regimen. The low calorie diet (1800 kcal/day) plus conventional insulin therapy was associated with body weight loss greater than 8.0%, whereas low calorie diet (1800 kcal/day) plus intensive insulin therapy was associated with higher rates of normoglycemia 66.
Very Low Calorie Diet in Obese Type 2 Diabetes
A small study was conducted with fifty-one obese subjects (24 with diabetes and 27 obese without diabetes) to compare weight loss and change in body composition in obese subjects with and without type 2 diabetes mellitus during a very-low-calorie diet (VLCD) program 67. After 24 weeks of intervention, there was no difference in weight loss between the 2 groups. Both groups completing the study per protocol had near-identical weight change during the program, with similar weight loss at 24 weeks (diabetes: 8.5 ± 1.3 kg vs control: 9.4 ± 1.2 kg). Change in fat mass index correlated with change in body mass index (BMI) in both groups, but change in fat mass index per unit change in BMI was less in the diabetic group compared with controls, which persisted after adjusting for age, sex, and baseline BMI. Insulin concentrations remained higher and peak β-hydroxybutyrate concentrations were lower in the diabetic compared with the control group. The conclusion was while following a 24-week very-low-calorie diet program, obese subjects with and without diabetes achieved comparable weight loss; but the decrease in body fat per unit weight loss was less in diabetic subjects. Hyperinsulinemia may have inhibited lipolysis in the diabetic group; however, further investigation into other factors is needed 67.
Low Carbohydrate Low Calorie Diet in type 2 Diabetes
In a very small study 68 comparing the effects of low carbohydrate low calorie diet (1800 kcal for men and 1600 kcal for women, distributed as 20 % carbohydrates, 30 % protein and 50 % fat) and high carbohydrate low calorie diet (1600-1800 kcal for men and 1400-1600 kcal for women, consisted of approximately 60 % carbohydrates, 15 % protein and 25 % fat) in two groups of obese patients with type 2 diabetes. The diets were tested with regard to glycaemic control and bodyweight. A group of 16 obese patients with type 2 diabetes was advised on a low-carbohydrate diet, Fifteen obese diabetes patients on a high-carbohydrate diet were control group. Positive effects on the glucose levels were seen very soon. After 6 months a marked reduction in bodyweight of patients in the low-carbohydrate diet group was observed, and this remained one year later. After 6 months the mean changes in the low-carbohydrate group and the control (high carbohydrate low calorie diet) group respectively were fasting blood glucose: -3.4 and -0.6 mmol/l; HBA1c: -1.4 % and -0.6 %; Body Weight: -11.4 kg and -1.8 kg; BMI: -4.1 kg/m2 and -0.7 kg/m2. In conclusion, a low-carbohydrate diet is an effective tool in the treatment of obese patients with type 2 diabetes 68.
- J Health Popul Nutr. 2012 Dec; 30(4): 447–455. Factors Associated with Consumption of Diabetic Diet among Type 2 Diabetic Subjects from Ahmedabad, Western India. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3763616/[↩]
- U.S. National Library of Medicine, Medline Plus. Diabetic Diet. https://medlineplus.gov/diabeticdiet.html[↩]
- https://www.cdc.gov/diabetes/ndep/cdcinfo/ndep_pdf/tasty-recipes-508.pdf[↩]
- BMI Calculator Adults. https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html[↩]
- BMI Calculator Children. https://nccd.cdc.gov/dnpabmi/Calculator.aspx[↩]
- https://supertracker.usda.gov/[↩][↩][↩][↩]
- Body Weight Planner. https://www.supertracker.usda.gov/bwp/index.html[↩]
- ChooseMyPlate. https://www.choosemyplate.gov/[↩]
- American Heart Association. The American Heart Association’s Diet and Lifestyle Recommendations. http://www.heart.org/HEARTORG/HealthyLiving/HealthyEating/Nutrition/The-American-Heart-Associations-Diet-and-Lifestyle-Recommendations_UCM_305855_Article.jsp[↩]
- Cochrane Review 16 July 2008. Exercise or exercise and diet for preventing type 2 diabetes mellitus. http://www.cochrane.org/CD003054/ENDOC_exercise-or-exercise-and-diet-for-preventing-type-2-diabetes-mellitus[↩][↩]
- Chen C, Zeng Y, Xu J, et al. Therapeutic effects of soluble dietary fiber consumption on type 2 diabetes mellitus. Experimental and Therapeutic Medicine. 2016;12(2):1232-1242. doi:10.3892/etm.2016.3377. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4950069/[↩][↩]
- Therapeutic effects of psyllium in type 2 diabetic patients. Sierra M, García JJ, Fernández N, Diez MJ, Calle AP. Eur J Clin Nutr. 2002 Sep; 56(9):830-42. https://www.ncbi.nlm.nih.gov/pubmed/12209371/[↩]
- Dietary fibres, fibre analogues, and glucose tolerance: importance of viscosity. Jenkins DJ, Wolever TM, Leeds AR, Gassull MA, Haisman P, Dilawari J, Goff DV, Metz GL, Alberti KG. Br Med J. 1978 May 27; 1(6124):1392-4. https://www.ncbi.nlm.nih.gov/pubmed/647304/[↩][↩]
- Gastric emptying in early noninsulin-dependent diabetes mellitus. Jones KL, Horowitz M, Carney BI, Wishart JM, Guha S, Green L. J Nucl Med. 1996 Oct; 37(10):1643-8. https://www.ncbi.nlm.nih.gov/pubmed/8862300/[↩]
- Action of guar gums on the viscosity of digestive contents and on the gastrointestinal motor function in pigs. Cherbut C, Albina E, Champ M, Doublier JL, Lecannu G. Digestion. 1990; 46(4):205-13. https://www.ncbi.nlm.nih.gov/pubmed/2178135/[↩]
- Effect of viscous fiber (guar) on postprandial motor activity in human small bowel. Schönfeld J, Evans DF, Wingate DL. Dig Dis Sci. 1997 Aug; 42(8):1613-7. https://www.ncbi.nlm.nih.gov/pubmed/9286225/[↩]
- Effect of gel-forming gums on the intestinal unstirred layer and sugar transport in vitro. Johnson IT, Gee JM. Gut. 1981 May; 22(5):398-403. https://www.ncbi.nlm.nih.gov/pubmed/7250752/[↩]
- Role of viscous guar gums in lowering the glycemic response after a solid meal. Leclère CJ, Champ M, Boillot J, Guille G, Lecannu G, Molis C, Bornet F, Krempf M, Delort-Laval J, Galmiche JP. Am J Clin Nutr. 1994 Apr; 59(4):914-21. https://www.ncbi.nlm.nih.gov/pubmed/7818627/[↩][↩]
- Dietary guar gum improves insulin sensitivity in streptozotocin-induced diabetic rats. Cameron-Smith D, Habito R, Barnett M, Collier GR. J Nutr. 1997 Feb; 127(2):359-64. https://www.ncbi.nlm.nih.gov/pubmed/9039840/[↩]
- Soluble dietary fibre improves insulin sensitivity by increasing muscle GLUT-4 content in stroke-prone spontaneously hypertensive rats. Song YJ, Sawamura M, Ikeda K, Igawa S, Yamori Y. Clin Exp Pharmacol Physiol. 2000 Jan-Feb; 27(1-2):41-5. https://www.ncbi.nlm.nih.gov/pubmed/10696527/[↩][↩]
- Troglitazone effects on gene expression in human skeletal muscle of type II diabetes involve up-regulation of peroxisome proliferator-activated receptor-gamma. Park KS, Ciaraldi TP, Lindgren K, Abrams-Carter L, Mudaliar S, Nikoulina SE, Tufari SR, Veerkamp JH, Vidal-Puig A, Henry RR. J Clin Endocrinol Metab. 1998 Aug; 83(8):2830-5. https://www.ncbi.nlm.nih.gov/pubmed/9709955/[↩]
- Consumption of both resistant starch and beta-glucan improves postprandial plasma glucose and insulin in women. Behall KM, Scholfield DJ, Hallfrisch JG, Liljeberg-Elmståhl HG. Diabetes Care. 2006 May; 29(5):976-81. https://www.ncbi.nlm.nih.gov/pubmed/16644623/[↩]
- Cereal fiber improves whole-body insulin sensitivity in overweight and obese women. Weickert MO, Möhlig M, Schöfl C, Arafat AM, Otto B, Viehoff H, Koebnick C, Kohl A, Spranger J, Pfeiffer AF. Diabetes Care. 2006 Apr; 29(4):775-80. https://www.ncbi.nlm.nih.gov/pubmed/16567814/[↩][↩][↩][↩]
- Whole-grain, bran, and cereal fiber intakes and markers of systemic inflammation in diabetic women. Qi L, van Dam RM, Liu S, Franz M, Mantzoros C, Hu FB. Diabetes Care. 2006 Feb; 29(2):207-11. https://www.ncbi.nlm.nih.gov/pubmed/16443861/[↩]
- Evidence-based nutrition principles and recommendations for the treatment and prevention of diabetes and related complications. American Diabetes Association. Diabetes Care. 2002 Jan; 25(1):202-12. https://www.ncbi.nlm.nih.gov/pubmed/11772917/[↩]
- American Heart Association. Portion Size Versus Serving Size. https://healthyforgood.heart.org/Eat-smart/Articles/Portion-Size-Versus-Serving-Size[↩]
- The National Institute of Diabetes and Digestive and Kidney Diseases Health Information Center. Carbohydrate Counting & Diabetes. https://www.niddk.nih.gov/health-information/diabetes/overview/diet-eating-physical-activity/carbohydrate-counting[↩][↩][↩]
- American Diabetes Association. MyFoodAdvisor Recipes. http://www.diabetes.org/mfa-recipes/[↩]
- USDA Food Composition Databases. https://ndb.nal.usda.gov/ndb/[↩]
- The National Institute of Diabetes and Digestive and Kidney Diseases Health Information Center. Diabetes Diet, Eating, & Physical Activity. https://www.niddk.nih.gov/health-information/diabetes/overview/diet-eating-physical-activity[↩]
- American Diabetes Association. All of Our Meal Plans. http://www.diabetes.org/mfa-recipes/meal-plans/meal-plans.html[↩]
- American Diabetes Association. Create Your Plate. http://www.diabetes.org/food-and-fitness/food/planning-meals/create-your-plate/[↩][↩][↩][↩]
- American Diabetes Association. Non-starchy Vegetables. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/making-healthy-food-choices/non-starchy-vegetables.html[↩]
- American Diabetes Association. Grains and Starchy Vegetables. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/making-healthy-food-choices/grains-and-starchy-vegetables.html[↩]
- American Diabetes Association. Fruits. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/making-healthy-food-choices/fruits.html[↩]
- American Diabetes Association. Protein Foods. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/making-healthy-food-choices/meat-and-plant-based-protein.html[↩]
- American Diabetes Association. Dairy. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/making-healthy-food-choices/dairy.html[↩]
- Centers for Disease Control and Prevention. Managing Diabetes: Eat Right ! https://www.cdc.gov/diabetes/managing/eatright.html[↩]
- American Diabetes Association. What Can I Drink ? http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/making-healthy-food-choices/what-can-i-drink.html[↩]
- Diabetes Care 2008 Dec; 31(12): 2281-2283. https://doi.org/10.2337/dc08-1239. International Tables of Glycemic Index and Glycemic Load Values: 2008. http://care.diabetesjournals.org/content/31/12/2281.full[↩]
- Cochrane Review 21 January 2009. Low glycaemic index, or low glycaemic load, diets for diabetes mellitus. http://www.cochrane.org/CD006296/ENDOC_low-glycaemic-index-or-low-glycaemic-load-diets-for-diabetes-mellitus[↩][↩]
- Am J Clin Nutr. 1988 Aug;48(2):248-54. Low-glycemic-index starchy foods in the diabetic diet. https://www.ncbi.nlm.nih.gov/pubmed/3407604[↩]
- JAMA Intern Med. 2013;173(13):1230-1238. doi:10.1001/jamainternmed.2013.6473. Vegetarian Dietary Patterns and Mortality in Adventist Health Study 2. http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/1710093[↩][↩]
- The National Institute of Diabetes and Digestive and Kidney Diseases Health Information Center. Very Low-calorie Diets. https://www.niddk.nih.gov/health-information/weight-management/very-low-calorie-diets[↩][↩]
- National Institutes of Health. Traditional American Cuisine: 1,200 Calories. https://www.nhlbi.nih.gov/health/educational/lose_wt/eat/menus_tac_1200.htm[↩]
- Obesity (Silver Spring). 2006 May; 14(5): 737–752. doi: 10.1038/oby.2006.84. The Look AHEAD Study: A Description of the Lifestyle Intervention and the Evidence Supporting It. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2613279/[↩][↩][↩]
- Diabetes Care. 2002 Dec; 25(12): 2165–2171. The Diabetes Prevention Program (DPP), Description of lifestyle intervention. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1282458/[↩][↩][↩]
- Metabolic and weight-loss effects of a long-term dietary intervention in obese patients. Ditschuneit HH, Flechtner-Mors M, Johnson TD, Adler G. Am J Clin Nutr. 1999 Feb; 69(2):198-204.https://www.ncbi.nlm.nih.gov/pubmed/9989680/[↩][↩]
- Weight management using a meal replacement strategy: meta and pooling analysis from six studies. Heymsfield SB, van Mierlo CA, van der Knaap HC, Heo M, Frier HI. Int J Obes Relat Metab Disord. 2003 May; 27(5):537-49. https://www.ncbi.nlm.nih.gov/pubmed/12704397/[↩]
- Discrepancy between self-reported and actual caloric intake and exercise in obese subjects. Lichtman SW, Pisarska K, Berman ER, Pestone M, Dowling H, Offenbacher E, Weisel H, Heshka S, Matthews DE, Heymsfield SB. N Engl J Med. 1992 Dec 31; 327(27):1893-8. https://www.ncbi.nlm.nih.gov/pubmed/1454084/[↩]
- Strengthening behavioral interventions for weight loss: a randomized trial of food provision and monetary incentives. Jeffery RW, Wing RR, Thorson C, Burton LR, Raether C, Harvey J, Mullen M. J Consult Clin Psychol. 1993 Dec; 61(6):1038-45. https://www.ncbi.nlm.nih.gov/pubmed/8113481/[↩]
- A randomized trial of improved weight loss with a prepared meal plan in overweight and obese patients: impact on cardiovascular risk reduction. Metz JA, Stern JS, Kris-Etherton P, Reusser ME, Morris CD, Hatton DC, Oparil S, Haynes RB, Resnick LM, Pi-Sunyer FX, Clark S, Chester L, McMahon M, Snyder GW, McCarron DA. Arch Intern Med. 2000 Jul 24; 160(14):2150-8. https://www.ncbi.nlm.nih.gov/pubmed/10904458/[↩]
- Nutritionally complete prepared meal plan to reduce cardiovascular risk factors: a randomized clinical trial. Haynes RB, Kris-Etherton P, McCarron DA, Oparil S, Chait A, Resnick LM, Morris CD, Clark S, Hatton DC, Metz JA, McMahon M, Holcomb S, Snyder GW, Pi-Sunyer FX, Stern JS. J Am Diet Assoc. 1999 Sep; 99(9):1077-83. https://www.ncbi.nlm.nih.gov/pubmed/10491676/[↩]
- Food provision vs structured meal plans in the behavioral treatment of obesity. Wing RR, Jeffery RW, Burton LR, Thorson C, Nissinoff KS, Baxter JE. Int J Obes Relat Metab Disord. 1996 Jan; 20(1):56-62. https://www.ncbi.nlm.nih.gov/pubmed/8788323/[↩]
- Liquid meal replacements and glycemic control in obese type 2 diabetes patients. Yip I, Go VL, DeShields S, Saltsman P, Bellman M, Thames G, Murray S, Wang HJ, Elashoff R, Heber D. Obes Res. 2001 Nov; 9 Suppl 4():341S-347S. https://www.ncbi.nlm.nih.gov/pubmed/11707563/[↩]
- Caloric restriction per se is a significant factor in improvements in glycemic control and insulin sensitivity during weight loss in obese NIDDM patients. Wing RR, Blair EH, Bononi P, Marcus MD, Watanabe R, Bergman RN. Diabetes Care. 1994 Jan; 17(1):30-6. https://www.ncbi.nlm.nih.gov/pubmed/8112186/[↩]
- The effect of short periods of caloric restriction on weight loss and glycemic control in type 2 diabetes. Williams KV, Mullen ML, Kelley DE, Wing RR. Diabetes Care. 1998 Jan; 21(1):2-8. https://www.ncbi.nlm.nih.gov/pubmed/9538962/[↩]
- N Engl J Med. 2002 Feb 7;346(6):393-403. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. https://www.ncbi.nlm.nih.gov/pubmed/11832527[↩]
- Dietary intake and nutritional status of young vegans and omnivores in Sweden. Larsson CL, Johansson GK. Am J Clin Nutr. 2002 Jul; 76(1):100-6. https://www.ncbi.nlm.nih.gov/pubmed/12081822/[↩]
- The Vegetarian Society. https://www.vegsoc.org/food[↩][↩]
- The Vegetarian Society. https://www.vegsoc.org/[↩]
- The Vegetarian Society. https://www.vegsoc.org/definition[↩]
- Diabetes UK. Vegetarian diets and diabetes. https://www.diabetes.org.uk/Guide-to-diabetes/Enjoy-food/Eating-with-diabetes/vegetarian-diets/[↩]
- Cardiovasc Diagn Ther. 2014 Oct; 4(5): 373–382. doi: 10.3978/j.issn.2223-3652.2014.10.04. Vegetarian diets and glycemic control in diabetes: a systematic review and meta-analysis. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4221319/[↩]
- Diabet Med. 2011 May;28(5):549-59. doi: 10.1111/j.1464-5491.2010.03209.x. Vegetarian diet improves insulin resistance and oxidative stress markers more than conventional diet in subjects with Type 2 diabetes. https://www.ncbi.nlm.nih.gov/pubmed/21480966[↩][↩]
- Adv Ther. 2016 Mar;33(3):447-59. doi: 10.1007/s12325-016-0300-2. Epub 2016 Feb 17. Obese Patients with Type 2 Diabetes on Conventional Versus Intensive Insulin Therapy: Efficacy of Low-Calorie Dietary Intervention. https://www.ncbi.nlm.nih.gov/pubmed/26886777[↩][↩]
- Metabolism. 2012 Jun;61(6):873-82. doi: 10.1016/j.metabol.2011.10.017. Epub 2011 Dec 5. Less fat reduction per unit weight loss in type 2 diabetic compared with nondiabetic obese individuals completing a very-low-calorie diet program. https://www.ncbi.nlm.nih.gov/pubmed/22146094?dopt=Abstract[↩][↩]
- Ups J Med Sci. 2005;110(1):69-73. Lasting improvement of hyperglycaemia and bodyweight: low-carbohydrate diet in type 2 diabetes–a brief report. https://www.ncbi.nlm.nih.gov/pubmed/15801687?dopt=Abstract[↩][↩]





{kind=link}