Contents
- What is High Protein Diet
- Animal Protein
- Vegetable Protein
- What are Amino Acids ?
- Finding balance, choosing the right kind and amount of protein.
- Possible risk factors associated with a high-protein diet
- Protein and Chronic Diseases
- The Role of Protein in the Body
- High Protein Diet and Weight Loss
- Red Meat Protein and Weight Control
- Health Benefits of Dietary Protein
- Protein in diet (Food Sources)
- What foods are in the Protein Foods Group ?
- How Much Protein Should You Eat ?
- Why is it important to make lean or low-fat choices from the Protein Foods Group ?
- Eating Red Meat and Cardiovascular Disease
- Eating Red Meat and Diabetes Risk
- Eating Red Meat and Cancer
- High Protein Diet and Increased Mortality
- High Protein Diet and Osteoporosis
- Protein and Chronic Diseases
- Protein Health Benefits
- Good Sources of Protein
What is High Protein Diet
Increased protein intakes and supplementation have generally been focused on athletic populations. However, over the past few years high protein diets have become a method used by the general population to enhance weight loss. The low-carbohydrate, high protein, high fat diet promoted by Atkins may be the most popular diet used today for weight loss in the United States 1. The basis behind this diet is that protein is associated with feelings of satiety and voluntary reductions in caloric consumption 2, 3. A recent study has shown that the Atkins diet can produce greater weight reduction at 3 and 6 months than a low-fat, high carbohydrate diet based upon U.S. dietary guidelines 4. However, potential health concerns have arisen concerning the safety of high protein diets. In 2001, the American Heart Association published a statement on dietary protein and weight reduction and suggested that individuals following such a diet may be at potential risk for metabolic, cardiac, renal, bone and liver diseases 5.
The Institute of Medicine recommends that adults get a minimum of 0.8 grams of protein for every kilogram of body weight per day (or 8 grams of protein for every 20 pounds of body weight) 6, 7. In the United States, the recommended daily allowance of protein is 46 grams per day for women over 19 years of age, and 56 grams per day for men over 19 years of age 8. The Institute of Medicine also sets a wide range for acceptable protein intake, anywhere from 10 to 35 percent of calories each day.
A high protein diet is considered high in protein if it exceeds 0.8 g/kg of body weight or the habitual 15-16% of total energy 9.
High-protein (and low carbohydrate) diets (based on a 2000 kcal diet and a 75 kg person) have recently received much attention in form of:
- High Protein Normal Carb 10 ~ 1.3 g/kg/day Protein (20% of total calories), 30% Fat, 50% Carbohydrate,
- USDA Recommended ~ 0.8 g/kg/day Protein (10-35% of total calories), 20-35% Fat, 45-65% Carbohydrate,
- the Atkins diet which is a non-energy-restricting, low carbohydrate (as low as 30 g/day), high-protein/high-fat diet 11 ~ 2.3 g/kg/day Protein (35% of total calories), 59% Fat, 6% Carbohydrate,
- the South Beach diet (low carbohydrate/high protein diet) 12 ~ 2.6 g/kg/day Protein (39% of total calories), 33% Fat, 28% Carbohydrate,
- the Stillman diet (very low carbohydrate/very high protein/low fat) 12 ~ 4.3 g/kg/day Protein (64% of total calories), 33% Fat, 3% Carbohydrate,
- the Zone diet (low carbohydrate/high protein) 12 ~ 2.3 g/kg/day Protein (34% of total calories), 29% Fat, 36% Carbohydrate.
Animal Protein
Proteins from animal sources (i.e. eggs, milk, meat, fish and poultry) provide the highest quality rating of food sources 13. This is primarily due to the ‘completeness’ of proteins from these sources. Animal protein includes all of the building blocks that your body needs. Protein from animal sources during late pregnancy is believed to have an important role in infants born with normal body weights. A low intake of protein from dairy and meat sources during late pregnancy was associated with low birth weights.
In addition to the benefits from total protein consumption, elderly subjects have also benefited from consuming animal sources of protein. Diets consisting of meat resulted in greater gains in lean body mass compared to subjects on a lacto-ovo-vegetarian diet 14. High animal protein diets have also been shown to cause a significantly greater net protein synthesis than a high vegetable protein diet 15. This was suggested to be a function of reduced protein breakdown occurring during the high animal protein diet.
There have been a number of health concerns raised concerning the risks associated with protein emanating primarily from animal sources. Primarily, these health risks have focused on cardiovascular disease (due to the high saturated fat and cholesterol consumption), bone health (from bone resorption due to sulfur-containing amino acids associated with animal protein) and other physiological system disease that will be addressed in the section on the high protein diets.
1. Whey: Whey is a general term that typically denotes the translucent liquid part of milk that remains following the process (coagulation and curd removal) of cheese manufacturing. From this liquid, whey proteins are separated and purified using various techniques yielding different concentrations of whey proteins. There are three main forms of whey protein that result from various processing techniques used to separate whey protein. They are whey powder, whey concentrate, and whey isolate 13.
Whey is one of the two major protein groups of bovine milk, accounting for 20% of the milk while casein accounts for the remainder. All of the constituents of whey protein provide high levels of the essential and branched chain amino acids. The bioactivities of these proteins possess many beneficial properties as well. Additionally, whey is also rich in vitamins and minerals. Whey protein is most recognized for its applicability in sports nutrition. Additionally, whey products are also evident in baked goods, salad dressings, emulsifiers, infant formulas, and medical nutritional formulas.
Whey is a complete protein whose biologically active components provide additional benefits to enhance human function. Whey protein contains an ample supply of the amino acid cysteine. Cysteine appears to enhance glutathione levels, which has been shown to have strong antioxidant properties that can assist the body in combating various diseases 16. In addition, whey protein contains a number of other proteins that positively effect immune function such as antimicrobial activity 17. Whey protein also contains a high concentration of branched chain amino acids (BCAA) that are important for their role in the maintenance of tissue and prevention of catabolic actions during exercise 18.
- Whey Protein Powder
Whey protein powder has many applications throughout the food industry. As an additive it is seen in food products for beef, dairy, bakery, confectionery, and snack products. Whey powder itself has several different varieties including sweet whey, acid whey (seen in salad dressings), demineralized (seen primarily as a food additive including infant formulas), and reduced forms. The demineralized and reduced forms are used in products other than sports supplements.
- Whey Protein Concentrate
The processing of whey concentrate removes the water, lactose, ash, and some minerals. In addition, compared to whey isolates whey concentrate typically contains more biologically active components and proteins that make them a very attractive supplement for the athlete.
- Whey Protein Isolate (WPI)
Isolates are the purest protein source available. Whey protein isolates contain protein concentrations of 90% or higher. During the processing of whey protein isolate there is a significant removal of fat and lactose. As a result, individuals who are lactose-intolerant can often safely take these products 19. Although the concentration of protein in this form of whey protein is the highest, it often contain proteins that have become denatured due to the manufacturing process. The denaturation of proteins involves breaking down their structure and losing peptide bonds and reducing the effectiveness of the protein.
2. Casein: Casein is the major component of protein found in cow (bovine) milk accounting for nearly 70-80% of its total protein and is responsible for the white color of milk 13. It is the most commonly used milk protein in the industry today. Milk proteins are of significant physiological importance to the body for functions relating to the uptake of nutrients and vitamins and they are a source of biologically active peptides. Similar to whey, casein is a complete protein and also contains the minerals calcium and phosphorous. Casein has a PDCAAS (protein digestibility corrected amino acid score) rating of 1.23 (generally reported as a truncated value of 1.0) 20.
Casein exists in milk in the form of a micelle, which is a large colloidal particle. An attractive property of the casein micelle is its ability to form a gel or clot in the stomach. The ability to form this clot makes it very efficient in nutrient supply. The clot is able to provide a sustained slow release of amino acids into the blood stream, sometimes lasting for several hours 21. This provides better nitrogen retention and utilization by the body.
3. Bovine Colostrum: Bovine colostrum is the “pre” milk liquid secreted by female mammals the first few days following birth. This nutrient-dense fluid is important for the newborn for its ability to provide immunities and assist in the growth of developing tissues in the initial stages of life. Evidence exists that bovine colostrum contains growth factors that stimulate cellular growth and DNA synthesis 22 and as might be expected with such properties, it makes for interesting choice as a potential sports supplement.
Although bovine colostrum is not typically thought of as a food supplement, the use by strength/power athletes of this protein supplement as an ergogenic aid has become common. Oral supplementation of bovine colostrum has been demonstrated to significantly elevate insulin-like-growth factor 1 (IGF-1) 23 and enhance lean tissue accruement 24, 25. However, the results on athletic performance improvement are less conclusive. Mero and colleagues (1997) reported no changes in vertical jump performance following 2-weeks of supplementation, and Brinkworth and colleagues 25 saw no significant differences in strength following 8-weeks of training and supplementation in both trained and untrained subjects. In contrast, following 8-weeks of supplementation significant improvements in sprint performance were seen in elite hockey players 26. Further research concerning bovine colostrum supplementation is still warranted.
Vegetable Protein
Vegetable proteins, when combined to provide for all of the essential amino acids, provide an excellent source for protein considering that they will likely result in a reduction in the intake of saturated fat and cholesterol. Popular sources include legumes, nuts and soy. Aside from these products, vegetable protein can also be found in a fibrous form called textured vegetable protein. Textured vegetable protein is produced from soy flour in which proteins are isolated. Textured vegetable protein is mainly a meat alternative and functions as a meat analog in vegetarian hot dogs, hamburgers, chicken patties, etc. It is also a low-calorie and low-fat source of vegetable protein. Vegetable sources of protein also provide numerous other nutrients such as phytochemicals and fiber that are also highly regarded in the diet diet.
1. Soy:
Soy is the most widely used vegetable protein source. The soybean, from the legume family, was first chronicled in China in the year 2838 B.C. and was considered to be as valuable as wheat, barley, and rice as a nutritional staple. It is found in modern American diets as a food or food additive 27. Soybeans, the high-protein seeds of the soy plant, contain isoflavones—compounds similar to the female hormone estrogen (phytoestrogens). Isoflavones are often referred to as phytoestrogens or plant-based estrogens because they have been shown, in cell line and animal studies, to have the ability to bind with the estrogen receptor 28. Research alos suggests that daily intake of soy protein may slightly lower levels of LDL (“bad”) cholesterol. Soy products are used for menopausal symptoms, bone health, improving memory, high blood pressure, and high cholesterol levels 27. In addition to its food uses, soy is available in dietary supplements, in forms such as tablets, capsules, and powders. Soy supplements may contain soy protein, isoflavones (compounds that have effects in the body similar to those of the female hormone estrogen), or other soy components 27.
Soy protein is a high quality protein that has been extensively studied. Soy provides a complete source of dietary protein, meaning that, unlike most plant proteins, it contains all the essential amino acids 29. The quality of soy protein has been assessed through several metabolic studies of nitrogen balance 30, 31, 32, which have demonstrated that soy protein supports nitrogen balance on par with beef and milk proteins. One recent study reported that amino acids from soy protein appear in the serum sooner, but that this may lead to a more rapid breakdown of the amino acids in the liver 33. Americans as a whole still consume very little soy protein. Based on 2003 data from the UN Food and Agriculture Organization, per-capita soy protein consumption is less than 1 gram (g) per day in most European and North American countries, although certain subpopulations such as vegetarians, Asian immigrants, and infants fed soy-based formula consume more. The Japanese, on the other hand, consume an average 8.7 g of soy protein per day; Koreans, 6.2–9.6 g; Indonesians, 7.4 g; and the Chinese, 3.4 g 29.
Traditional soy foods include tofu, which is produced by puréeing cooked soybeans and precipitating the solids, and miso and tempeh, which are made by fermenting soybeans with grains. “Second generation” soy products involve chemical extractions and other processing, and include soy protein isolate and soy flour. These products become primary ingredients in items such as meatless burgers, dietary protein supplements, and infant formula, and are also used as nonnutritive additives to improve the characteristics of processed foods 29.
Soy Protein Types
The soybean can be separated into three distinct categories; flour, concentrates, and isolates. Soy flour can be further divided into natural or full-fat (contains natural oils), defatted (oils removed), and lecithinated (lecithin added) forms. Of the three different categories of soy protein products, soy flour is the least refined form. It is commonly found in baked goods. Another product of soy flour is called textured soy flour. This is primarily used for processing as a meat extender. See Table 1 for protein composition of soy flour, concentrates, and isolates.
Soy concentrate was developed in the late 1960s and early 1970s and is made from defatted soybeans. While retaining most of the bean’s protein content, concentrates do not contain as much soluble carbohydrates as flour, making it more palatable. Soy concentrate has a high digestibility and is found in nutrition bars, cereals, and yogurts.
Isolates are the most refined soy protein product containing the greatest concentration of protein, but unlike flour and concentrates, contain no dietary fiber. Isolates originated around the 1950s in The United States. They are very digestible and easily introduced into foods such as sports drinks and health beverages as well as infant formulas.
Table 1: Protein composition of soy protein forms 13.
| Soy Protein Form | Protein Composition |
|---|---|
| Soy Flour | 50% |
| Soy Concentrate | 70% |
| Soy Isolate | 90% |
What we know about Soy 34, 27
- Consuming soy protein in place of other proteins may lower levels of LDL (“bad”) cholesterol to a small extent 35, 36.
- Soy isoflavone supplements may help to reduce the frequency and severity of menopausal hot flashes, but the effect may be small 37, 38.
- It’s uncertain whether soy supplements can relieve cognitive problems associated with menopause 39.
- Current evidence suggests that soy isoflavone mixtures do not slow bone loss in Western women during or after menopause 40.
- Diets containing soy protein may slightly reduce blood pressure 41.
- There’s not enough scientific evidence to determine whether soy supplements are effective for any other health uses.
- Current National Center for Complementary and Integrative Health-funded studies on soy and its components are investigating a variety of topics, including stroke outcomes, anti-inflammatory effects, and effects on diabetes.
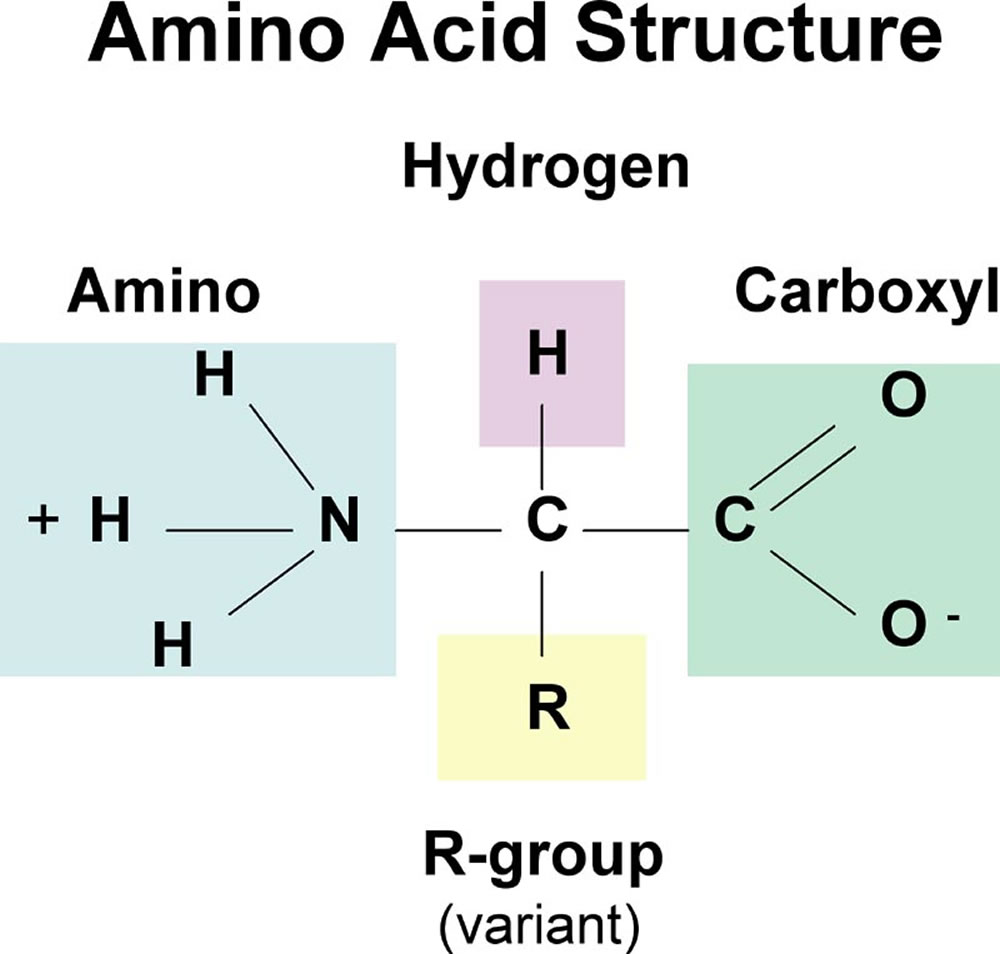
What are Amino Acids ?
Amino acids are organic compounds that combine to form proteins 42. Amino acids and proteins are the building blocks of life that help maintain and repair muscles, organs, and other parts of the body.
Animal protein includes all of the building blocks that your body needs. Plant proteins need to be combined to get all of the building blocks that your body needs.
In the human body, certain amino acids can be converted to other amino acids, proteins, glucose, fatty acids or ketones. For example, in the human body, glucogenic amino acids can be converted to glucose in the process called gluconeogenesis; they include all amino acids except lysine and leucine 43, 44.
Ketogenic amino acids, are amino acids that can be converted into ketone bodies through ketogenesis. In humans, the ketogenic amino acids are leucine and lysine, while threonine, isoleucine, phenylalanine, tyrosine and tryptophan can be either ketogenic or glucogenic 45. Ketones can be used by the brain as a source of energy during fasting or in a low-carbohydrate diet.
When proteins are digested or broken down, amino acids are left.
The human body uses amino acids to make proteins to help the body:
- Break down food
- Grow
- Repair body tissue
- Perform many other body functions
- Amino acids can also be used as a source of energy by the body, like proteins, they can provide about 4 Calories per gram.
Other functions of amino acids:
- Chemical messengers (neurotransmitters) in the nervous system: aspartate, GABA, glutamate, glycine, serine
- Precursors of other neurotransmitters or amino acid-based hormones:
- Tyrosine is a precursor of dopamine, epinephrine, norepinephrine and thyroxine.
- Tryptophan is a precursor of melatonin and serotonin and nicotinic acid (vitamin B3).
- Histidine is a precursor of histamine.
- Glycine is a precursor of heme, a part of hemoglobin.
- Aspartate, glutamate and glycine are precursors of nucleic acids, which are parts of DNA.
Amino acids are classified into three groups:
- Essential amino acids.
- Nonessential amino acids.
- Conditional amino acids.
You do not need to eat essential and nonessential amino acids at every meal, but getting a balance of them over the whole day is important. A diet based on a single plant item will not be adequate, but we no longer worry about pairing proteins (such as beans with rice) at a single meal. Instead we look at the adequacy of the diet overall throughout the day.
Essential Amino Acids
The 9 amino acids are essential (vital), which means they are necessary for the human life and health but cannot be produced in your body so you need to get them from foods 46.
- Histidine (His)
- Isoleucine (Ile)
- Leucine (Leu)
- Lysine (Lys)
- Methionine (Met)
- Phenylalanine (Phe)
- Threonine (Thr)
- Tryptophan (Trp)
- Valine (Val).
Conditionally Essential Amino Acids
These amino acids can be synthesized in your body, but in certain circumstances, like young age, illness or hard exercise, you need to get them in additional amounts from foods to meet the body requirements for them. Ornithine is also considered conditionally essential amino acid, but it does not form proteins 42.
- Arginine (Arg)
- Cysteine (Cys)
- Glutamine (Gln)
- Glycine (Gly)
- Proline (Pro)
- Serine (Ser)
- Tyrosine (Tyr)
Nonessential Amino Acids
These amino acids can be synthesized in your body from other amino acids, glucose and fatty acids, so you do not need to get them from foods.
- Alanine (Ala)
- Asparagine (Asn)
- Aspartic acid (Asp)
- Glutamic acid (Glu)
- Selenocysteine (Sec).
Finding balance, choosing the right kind and amount of protein.
Foods that Contain All 9 Essential Amino Acids
Food protein containing all 9 amino acids in adequate amounts is called complete or high-quality protein.
- ANIMAL FOODS with complete protein include liver (chicken, pork, beef), goose, duck, turkey, chicken, lamb, pork, most fish, rabbit, eggs, milk, cheese (cottage, gjetost, cream, swiss, ricotta, limburger, gruyere, gouda, fontina, edam) and certain beef cuts. Animal foods with incomplete protein include certain yogurts and beef cuts.
- PLANT FOODS with complete protein include spinach, beans (black, cranberry, french, pink, white, winged, yellow), soy, split peas, chickpeas, chestnuts, pistachios, pumpkin seeds, avocado, potatoes, quinoa, a seaweed spirulina, tofu and hummus. Common plant foods with incomplete protein: rice (white and brown), white bread (including whole-wheat), pasta, beans (adzuki, baked, kidney, lima, pinto, snap), peas, lentils, nuts (walnuts, peanuts, hazelnuts, almonds, coconut), sunflower seeds, kamut.
- Foods made of mycoprotein also contain complete protein.
When choosing protein, opt for low-fat options, such as lean meats, skim milk or other foods with high levels of protein. Legumes, for example, can pack about 16 grams of protein per cup and are a low-fat and inexpensive alternative to meat.
Choose main dishes that combine meat and vegetables together, such as low-fat soups, or a stir-fry that emphasizes veggies.
- Some high-protein foods are healthier than others because of what comes along with the protein: healthy fats or harmful ones, beneficial fiber or hidden salt. It’s this protein package that’s likely to make a difference for health. For example, a 6-ounce broiled porterhouse steak is a great source of protein—about 40 grams worth. But it also delivers about 12 grams of saturated fat 47. For someone who eats a 2,000 calorie per day diet, that’s more than 60 percent of the recommended daily intake for saturated fat.
- Watch portion size. Aim for 2- to 3-ounce servings.
- If you’re having an appetizer, try a plate of raw veggies instead of a cheese plate. Cheese adds protein, but also fat.
- A 6-ounce ham steak has only about 2.5 grams of saturated fat, but it’s loaded with sodium—2,000 milligrams worth, or about 500 milligrams more than the daily sodium max.
6-ounces of wild salmon has about 34 grams of protein and is naturally low in sodium, and contains only 1.7 grams of saturated fat 47. Salmon and other fatty fish are also excellent sources of omega-3 fats, a type of fat that’s especially good for the heart. Alternatively, a cup of cooked lentils provides about 18 grams of protein and 15 grams of fiber, and it has virtually no saturated fat or sodium 47.
Sustained satiety is a key component to induce a negative energy balance and to promote weight loss. An ideal weight loss strategy would promote satiety and maintain basal metabolic rates despite a negative energy balance and reduction in fat-free mass. Satiety is multifactorial and influenced by many components including but not limited to the endocrine system, the cognitive and neural system as well as the gastrointestinal system. The hierarchy for macronutrient-induced satiating efficiency is similar to that observed for diet-induced thermogenesis : protein is the most satiating macronutrient followed by carbohydrates and fat, which is least satiating 48. This satiating effect is most significant after high-protein diets 49. Satiety was significantly greater after a 60% protein meal than after a 19% protein meal 50. These findings were confirmed by Crovetti et al. who reported significantly greater satiety after consumption of an isocaloric meal containing 68% protein compared with a 10% protein meal 51. Increased satiety helps to decrease energy intake, which is a requisite for successful weight loss. In general, increased satiety has been observed after meals with a protein content in the range of 25% to 81% 52.
The thermic effect of food (energy expenditure), also called diet-induced thermogenesis, is a metabolic response to food. Food intake results in a transient increase in energy expenditure attributable to the various steps of nutrient processing (i.e. digestion, absorption, transport, metabolism and storage of nutrients). The diet-induced thermogenesis is mostly indicated as percentage increase in energy expenditure over the basic metabolic rate (BMR). The diet-induced thermogenesis values are highest for protein (~15-30%), followed by carbohydrates (~5-10%) and fat (~0-3%) 53, 54. Based on a recent meta-analysis, the thermic effect of food increases ≈ 29 kJ/4184 kJ of ingested food for each increase of 10 percentage points in the percentage of energy from protein 55. In other words, if a subject therefore consumes an 8368 kJ/d diet with 30% energy from protein, then the thermic effect of food will be 58 kJ/d higher than if protein contributes only 20% of the dietary energy. Mikkelsen et al. 56 found that subjects consuming a diet containing 29% of protein had a 891 kJ/d higher resting metabolic rate than subjects consuming the same eucaloric diet with 11% energy from protein. For weight loss, however, diet-induced thermogenesis-related satiety is even more important. A high protein diet is associated with increased 24-h diet-induced energy expenditure 57. The increase in diet-induced thermogenesis may increase satiety.
Long-term effects of high-protein diets depend on the population studied as well as the exact composition of the diet but have generally been shown to include weight reduction and weight loss maintenance as well as beneficial effects on metabolic risk factors such total cholesterol and triacylglycerol. Claessens et al. 58 compared a low-fat, high-carbohydrate diet against a low-fat, high-protein diet. The authors conclude that after 12 weeks of diet intervention, the low-fat, high-protein diet was more effective for weight control.
Clifton et al. analyzed data from 215 obese subjects which were either assigned to a 12 week high-protein or standard-protein diet. The authors conclude that subjects in the high-protein group had beneficial effects on total cholesterol and triacylglycerol and achieved greater weight loss and better lipid results. In another study, Clifton et al. determined the efficacy of a high-protein and high-carbohydrate intake on the maintenance of weight loss after 64 weeks of follow-up. The authors found no significant difference between groups regarding weight loss. Protein intake in grams derived from the dietary records, however, was directly related to weight loss. Westerterp-Plantenga et al. studied that effect of a 20% higher protein intake (18% of energy vs 15% of energy) for subsequent 3 months of weight maintenance after weight loss. They found that higher protein intake resulted in a 50% lower body weight regain over this time, possibly related to increased satiety and decreased energy efficiency. It has to be mentioned, however, that a hypochaloric diet with a high protein content of 20-30% is only relatively high in protein compared to a eucaloric diet with a normal protein level of 10-15% while the absolute amount of protein often does not differ between the two diets.
Other possible mechanisms to explain the improvement in satiety with high-protein diets are:
- The secretion of gut neuropeptides that induce satiation, glucagon-like peptide-1 (GLP-1), cholecystokinin (CCK), and peptide YY (PYY) seem to be increased in response to a high-protein diet.
- High-protein diets may directly promote a satiety response due to a complex homeostatic mechanisms between the peripheral organs and the central nervous system.
- High-protein and low-carbohydrate diets promote hepatic gluconeogenesis to maintain plasma glucose levels. Alteration of gluconeogenesis has been found to contribute to satiety.
- High-protein diets can help preserve lean body mass during weight loss. Mettler et al. examined the effect of increased dietary protein intake (~2.3 g/kg BW/d) on lean body mass maintenance during hypoenergetic weight loss in athletes 59.
- For obese subjects, lowering carbohydrate in favor of protein might be advantageous as dietary carbohydrates might impair fat oxidation 60 whereas low-carbohydrate, high-protein diets reduce adipose tissue development in rats 61. Higher daily protein intake at the expense of fat intake could substantially reduce total energy intake, which could possibly translate to a healthier weight status 62.
Possible risk factors associated with a high-protein diet
- Metabolomics studies revealed that high intake of branched-chain amino acids (BCAAs, Valine, Leucine, Isoleucine) and aromatic amino acids (Phenylalanine, Tyrosine) may be associated with the development of metabolic diseases, that is branched-chain amino acids (BCAA) and related metabolites are more strongly associated with insulin resistance and the incident of diabetes. Importantly, this only occurs in combination with a high-fat diet 63.
- Metabolic ketosis: One of the major concerns for individuals on high protein, low carbohydrate diets is the potential for the development of metabolic ketosis. As carbohydrate stores are reduced the body relies more upon fat as its primary energy source. The greater amount of free fatty acids that are utilized by the liver for energy will result in a greater production and release of ketone bodies in the circulation. This will increase the risk for metabolic acidosis and can potentially lead to a coma and death. A recent multi-site clinical study 4 examined the effects of low-carbohydrate, high protein diets and reported significant elevation in ketone bodies during the first three months of the study. However, as the study duration continued the percentage of subjects with positive urinary ketone concentrations became reduced, and by six months urinary ketones were not present in any of the subjects 4.
- Diets high in protein pose a potential acid load to the kidneys, mainly as sulfates and phosphates 64. The authors conclude that renal hemodynamics and renal excretion is altered in response to a short-term, high-protein diet. Although depended on the source of protein, interventional studies in humans have shown that high-protein diets have the potential to increase the risk of calcium stone-formation in the urinary tract 64, 65. In a study on bodybuilders consuming a high protein (2.8 g/kg) diet no negative changes were seen in any kidney function tests 66. However, in individuals with existing kidney disease it is recommended that they limit their protein intake to approximately half of the normal RDA level for daily protein intake (0.8 g/kg per day). Lowering protein intake is thought to reduce the progression of renal disease by decreasing hyperfiltration 67. In order to maintain an acid–base balance in the body, people on a high-protein diet should consider ingestion of alkali buffers such as fruits and vegetables high in potassium (alkaline-forming foods). Glutamine or sodium bicarbonate supplements can also help to restore acid–base balance in the body. In general, people experimenting with high-protein diets are advised to monitor their renal function.
Protein and Chronic Diseases
Proteins in food and the environment are responsible for food allergies, which are overreactions of the immune system. Beyond that, relatively little evidence has been gathered regarding the effect of the amount of dietary protein on the development of chronic diseases in healthy people.
However, there’s growing evidence that high-protein food choices do play a role in health—and that eating healthy protein sources like fish, chicken, beans, or nuts in place of red meat (including processed red meat) can lower the risk of several diseases and premature death 8, 68, 69, 70, 71, 72, 73.
- Cardiovascular disease
Research conducted at Harvard School of Public Health has found that eating even small amounts of red meat, especially processed red meat, on a regular basis is linked to an increased risk of heart disease and stroke, and the risk of dying from cardiovascular disease or any other cause 68, 70, 74. Conversely, replacing red and processed red meat with healthy protein sources such as poultry, fish, or beans seems to reduce these risks.
One investigation followed 120,000 men and women in the Nurses’ Health Study and Health Professionals Follow-Up Study for more than two decades 70. For every additional 3-ounce serving of unprocessed red meat the study participants consumed each day, their risk of dying from cardiovascular disease increased by 13 percent.
Processed red meat was even more strongly linked to dying from cardiovascular disease—and in smaller amounts: Every additional 1.5 ounce serving of processed red meat consumed each day—equivalent to one hot dog or two strips of bacon—was linked to a 20 percent increase in the risk of cardiovascular disease death.
Cutting back on red meat could save lives: the researchers estimated that if all the men and women in the study had reduced their total red and processed red meat intake to less than half a serving a day, one in ten cardiovascular disease deaths would have been prevented.
In terms of the amount of protein consumed, there’s evidence that eating a high-protein diet may be beneficial for the heart, as long as the protein comes from a healthy source.
A 20-year prospective study of over 80,000 women found that those who ate low-carbohydrate diets that were high in vegetable sources of fat and protein had a 30 percent lower risk of heart disease compared with women who ate high-carbohydrate, low-fat diets. Diets were given low-carbohydrate scores based on their intake of fat, protein, and carbohydrates 75. However, eating a low-carbohydrate diet high in animal fat or protein did not offer such protection.
Further evidence of the heart benefits of eating healthy protein in place of carbohydrate comes from a randomized trial known as the Optimal Macronutrient Intake Trial for Heart Health (OmniHeart). A healthy diet that replaced some carbohydrate with healthy protein (or healthy fat) did a better job of lowering blood pressure and harmful low-density lipoprotein (LDL) cholesterol than a similarly healthy, higher carbohydrate diet 76.
Similarly, the “EcoAtkins” weight loss trial compared a low-fat, high -carbohydrate, vegetarian diet to a low-carbohydrate vegan diet that was high in vegetable protein and fat. Though weight loss was similar on the two diets, study participants on the high protein diet saw improvements in blood lipids and blood pressure 77.
A more recent study generated headlines because it had the opposite result. In that study, Swedish women who ate low-carbohydrate, high-protein diets had higher rates of cardiovascular disease and death than those who ate lower-protein, higher-carbohydrate diets 78. But the study, which assessed the women’s diets only once and then followed them for 15 years, did not look at what types of carbohydrates or what sources of protein these women ate. That was important because most of the women’s protein came from animal sources.
- Diabetes
Again, protein quality matters more than protein quantity when it comes to diabetes risk 79.
A recent study found that people who ate diets high in red meat, especially processed red meat, had a higher risk of type 2 diabetes than those who rarely ate red or processed meat 71. For each additional serving a day of red meat or processed red meat that study participants ate, their risk of diabetes rose 12 and 32 percent, respectively.
Substituting one serving of nuts, low-fat dairy products, or whole grains for a serving of red meat each day lowered the risk of developing type 2 diabetes by an estimated 16 to 35 percent.
Another study also shows that red meat consumption may increase risk of type 2 diabetes. Researchers found that people who started eating more red meat than usual were found to have a 50% increased risk of developing type 2 diabetes during the next four years, and researchers also found that those who reduced red meat consumption lowered their type 2 diabetes risk by 14% over a 10-year follow-up period.
More evidence that protein quality matters comes from a 20-year study that looked at the relationship between low-carbohydrate diets and type 2 diabetes in women. Low-carbohydrate diets that were high in vegetable sources of fat and protein modestly reduced the risk of type 2 diabetes 80. But low-carbohydrate diets that were high in animal sources of protein or fat did not show this benefit.
For type 1 diabetes (formerly called juvenile or insulin-dependent diabetes), proteins found in cow’s milk have been implicated in the development of the disease in babies with a predisposition to the disease, but research remains inconclusive 81, 82.
- Protein Intake and Liver Disease Risk
The American Heart Association has suggested that high protein diets may have detrimental effects on liver function 5. This is primarily the result of a concern that the liver will be stressed through metabolizing the greater protein intakes. However, there is no scientific evidence to support this contention. Jorda and colleagues 83 did show that high protein intakes in rats produce morphological changes in liver mitochondria. However, they also suggested that these changes were not pathological, but represented a positive hepatocyte adaptation to a metabolic stress.
Protein is important for the liver not only in promoting tissue repair, but to provide lipotropic agents such as methionine and choline for the conversion of fats to lipoprotein for removal form the liver 84. The importance of high protein diets has also been acknowledged for individuals with liver disease and who are alcoholics. High protein diets may offset the elevated protein catabolism seen with liver disease 84, while a high protein diet has been shown to improve hepatic function in individuals suffering from alcoholic liver disease 85.
- Cancer
When it comes to cancer, protein quality again seems to matter more than quantity. Research on the association between protein and cancer is ongoing, but some data shows that eating a lot of red meat and processed meat is linked to an increased risk of colon cancer 8.
In the Nurse’s Health Study and the Health Professionals Follow-Up Study, every additional serving per day of red meat or processed red meat was associated with a 10 and 16 percent higher risk of cancer death, respectively 70.
A 2014 study showed that higher consumption of red meat during adolescence was associated with premenopausal breast cancer, suggesting that choosing other protein sources in adolescence may decrease premenopausal breast cancer risk 86.
People should aim to reduce overall consumption of red meat and processed meat, but when you do opt to have it, go easy on the grill. High-temperature grilling creates potentially cancer-causing compounds in meat, including polycyclic aromatic hydrocarbons and heterocyclic amines. You don’t have to stop grilling, but try these tips for healthy grilling from the American Institute of Cancer Research: Marinate meat before grilling it, partially pre-cook meat in the oven or microwave to reduce time on the grill, and grill over a low flame.
In October 2015, the World Health Organization (WHO)’s International Agency for Research on Cancer announced that consumption of processed meat is “carcinogenic to humans,” and that consumption of red meat is “probably carcinogenic to humans.” 87
The IARC Working Group, comprised of 22 scientists from ten countries, evaluated over 800 studies. Conclusions were primarily based on the evidence for colorectal cancer. Data also showed positive associations between processed meat consumption and stomach cancer, and between red meat consumption and pancreatic and prostate cancer 87.
- Osteoporosis
Digesting protein releases acids into the bloodstream, which the body usually neutralizes with calcium and other buffering agents. Eating lots of protein, then, requires a lot of calcium – and some of this may be pulled from bone.
Following a high-protein diet for a long period of time could weaken bone. In the Nurses’ Health Study, for example, women who ate more than 95 grams of protein a day were 20 percent more likely to have broken a wrist over a 12-year period when compared with those who ate an average amount of protein (less than 68 grams a day) 88. This area of research is still controversial, however, and the findings have not been consistent. Some studies suggest that increasing protein increases risk of fractures; others have linked high-protein diets with increased bone-mineral density, and thus stronger bones 89, 90, 91. Given the effect of protein on bone health is still unclear, but it does appear to be prudent to monitor the amount of animal protein in the diet for susceptible individuals. This may be more pronounced in individuals that may have a genetic predisposition for this. However, if animal protein consumption is modified by other nutrients (e.g. calcium) the effects on bone health may be lessened 13.
- Protein and Weight Control
The same high-protein foods that are good choices for disease prevention may also help with weight control. Researchers at Harvard School of Public Health followed the diet and lifestyle habits of 120,000 men and women for up to 20 years, looking at how small changes contributed to weight gain over time 92.
Those who ate more red and processed meat over the course of the study gained more weight, about one extra pound every four years, while those who ate more nuts over the course of the study gained less weight, about a half pound less every four years.
One study showed that eating approximately one daily serving of beans, chickpeas, lentils or peas can increase fullness, which may lead to better weight management and weight loss 93.
There’s no need to go overboard on protein. Though some studies show benefits of high-protein, low-carbohydrate diets in the short term, avoiding fruits and whole grains means missing out on healthful fiber, vitamins, minerals, and other phytonutrients.
Summary
The mechanisms by which increased long-term dietary protein intake regulate body weight are not well understood but are most likely multifactorial 94. Depending on the diet, lower triacylglycerol levels and hence fat mass loss with a higher-protein diet as well as increased satiety possibly mediated by increased leptin sensitivity have been discussed 95, 96, 97. Fluid loss related to reduced carbohydrate intake and overall caloric restriction have also been discussed to mediate weight loss 5.
There are some risk factors to high protein diets such as increased acid load to the kidneys or high fat content of animal proteins. Awareness of these risk factors enables individuals choosing to consume a high-protein diet to get the most benefit from it.
The Role of Protein in the Body
Protein is in every cell in the body and it’s the building blocks of life. At least 10,000 different proteins make you what you are and keep you that way. They make up about 15% of the average person’s body weight. Your body need protein from the foods you eat to build and maintain bones, muscles and skin. You get proteins in your diet from meat, dairy products, nuts, and certain grains and beans. Proteins from meat and other animal products are complete proteins. This means they supply all of the amino acids the body can’t make on its own. Most plant proteins are incomplete. The basic structure of protein is a chain of amino acids. You should eat different types of plant proteins every day to get all of the amino acids your body needs 98.
It is important to get enough dietary protein to help your body repair cells and make new ones. Protein is also important for growth and development in children, teens, and pregnant women 99. You need to eat protein every day, because your body doesn’t store it the way it stores fats or carbohydrates. How much you need depends on your age, sex, health, and level of physical activity. Most Americans eat enough protein in their diet, most Americans already eat about 12-18% of their calories as protein 100.
Some people, such as vegetarians, do have to pay attention to the protein in their diets. While animal proteins have all the essential amino acids, plant-based proteins can have low amounts of some. That’s why vegetarians have to eat protein from several different sources to get all the different amino acids they need. Vegetarian food combinations that give you complete protein, for example, include rice and beans or peanut butter and bread. Eggs are also a good source of complete protein. People who don’t eat eggs or dairy products need to be particularly careful to get all the essential amino acids they need 100.
Another group that may not get enough protein is older adults. A recent NIH study of men and women in their 70s found that those who ate the least protein lost significantly more muscle than those who ate the most protein. Maintaining muscle is particularly important as you age. Older adults who lose muscle in their legs and hips are more likely to fall and have injuries like broken hips. Those who don’t maintain strong muscles as they age might also have trouble doing basic things like getting up from a chair, walking up stairs or taking a stroll through the park 100.
Increased protein intakes and supplementation have generally been focused on athletic populations. In special cases, these products can prove useful. For elderly people who can’t eat enough protein or patients with diseases that leave them malnourished, a protein supplement can be one way to help get enough protein. However, over the past few years high protein diets have become a method used by the general population to enhance weight reduction. The low-carbohydrate, high protein, high fat diet promoted by Atkins may be the most popular diet used today for weight loss in the United States. Numerous studies have shown that a high-protein diet has major benefits for weight loss and metabolic health. There’s growing evidence 101, 102, 103, 104, 105, 106, 107 that high-protein food choices do play a role in health and that eating healthy protein sources like fish, chicken, beans, or nuts in place of red meat (including processed red meat) can lower the risk of several diseases and premature death.
In terms of the amount of protein consumed, there’s evidence that eating a high-protein diet may be beneficial for the heart, as long as the protein comes from a healthy source.
- A 20-year prospective study of over 80,000 women found that those who ate low-carbohydrate diets that were high in vegetable sources of fat and protein had a 30 percent lower risk of heart disease compared with women who ate high-carbohydrate, low-fat diets. Diets were given low-carbohydrate scores based on their intake of fat, protein, and carbohydrates 108. However, eating a low-carbohydrate diet high in animal fat or protein did not offer such protection.
- Further evidence of the heart benefits of eating healthy protein in place of carbohydrate comes from a randomized trial known as the Optimal Macronutrient Intake Trial for Heart Health (OmniHeart). A healthy diet that replaced some carbohydrate with healthy protein (or healthy fat) did a better job of lowering blood pressure and harmful low-density lipoprotein (LDL) cholesterol than a similarly healthy, higher carbohydrate diet 109.
- Similarly, the “EcoAtkins” weight loss trial compared a low-fat, high -carbohydrate, vegetarian diet to a low-carbohydrate vegan diet that was high in vegetable protein and fat. Though weight loss was similar on the two diets, study participants on the high protein diet saw improvements in blood lipids and blood pressure 110.
A more recent study generated headlines because it had the opposite result. In that study, Swedish women who ate low-carbohydrate, high-protein diets had higher rates of cardiovascular disease and death than those who ate lower-protein, higher-carbohydrate diets 111. But the study, which assessed the women’s diets only once and then followed them for 15 years, did not look at what types of carbohydrates or what sources of protein these women ate. That was important because most of the women’s protein came from animal sources.
For most Americans, however, there’s little benefit to eating more protein than they already do. In long-term studies of high-protein diets, researchers have found that most differences in weight loss can be explained by the amount of calories people eat rather than their protein intake. High-protein diets may make some people feel fuller, but that effect has been hard for researchers to tease out, because many high-protein diets are also high in fat.
Around the world however, millions of people don’t get enough protein. Protein malnutrition leads to the condition known as kwashiorkor. Kwashiorkor is a form of malnutrition that occurs when there is not enough protein in the diet. This disease is more common in very poor countries. It often occurs during a drought or other natural disaster, or during political unrest. These conditions are responsible for a lack of food, which leads to malnutrition. Lack of protein can cause growth failure, loss of muscle mass, decreased immunity, weakening of the heart and respiratory system, and death.
The basis behind this high protein low carbohydrate diet is that protein is associated with feelings of satiety and voluntary reductions in caloric consumption. A recent study has shown that the Atkins diet can produce greater weight reduction at 3 and 6 months than a low-fat, high carbohydrate diet based upon U.S. dietary guidelines. However, potential health concerns have arisen concerning the safety of high protein diets. One of the major concerns for individuals on high protein, low carbohydrate diets is the potential for the development of metabolic ketosis. And there is evidence to suggest that people with certain diseases and conditions should limit their intake. For people with kidney disease, for instance, a reduced-protein diet may help delay the progression towards kidney failure 100.
High Protein Diet and Weight Loss
For years, proponents of some fad diets have claimed that higher amounts of protein facilitate weight loss. Only in recent years have studies begun to examine the effects of high protein diets on energy expenditure, subsequent energy intake and weight loss as compared to lower protein diets.
In this review 112, the authors conducted a systematic review of randomized investigations on the effects of high protein diets on dietary thermogenesis, satiety, body weight and fat loss across 48 studies with duration ranging from 2 minutes (involving satiety), 2 hours (measuring the thermic effect of food), 7 days (subsequent energy intake) and 12 months (for weight loss). The authors concluded that there is convincing evidence that a higher protein diets might increase weight loss in the short term, but further longer term research is required before definitive conclusions can be drawn. Furthermore, a higher protein intake increases thermogenesis and satiety compared to diets of lower protein content. The weight of evidence also suggests that high protein meals lead to a reduced subsequent energy intake. Some evidence suggests that diets higher in protein result in an increased weight loss and fat loss as compared to diets lower in protein, but findings have not been consistent. In dietary practice, it may be beneficial to partially replace refined carbohydrate with protein sources that are low in saturated fat. Although recent evidence supports potential benefit, rigorous longer-term studies are needed to investigate the effects of high protein diets on weight loss and weight maintenance.
People on high-protein diets are advised to choose their source of protein very carefully (i.e. emphasize the use of high-quality protein sources from plant origin). Many protein-rich foods of animal origin (e.g. red meats, eggs and dairy products) also contain high levels of saturated fats and cholesterol. This may put consumers of high-protein diets at higher risk for heart disease, hyperlipidemia and hypercholesterolemia 113. Healthier proteins from vegetables (soy protein, beans, tofu, seitan or nuts) or fish could be a valuable alternative. Finally, all excess protein will eventually be converted to glucose (via gluconeogenesis) or ketone bodies 114, 115. This may also explain the increased gluconeogenesis in response to a high-protein diet, due to high-protein and low-carbohydrate diets promoting hepatic gluconeogenesis to maintain plasma glucose levels.. In a state of low energy demand, these metabolites will be stored as glycogen and fat, which is undesirable if weight loss is the goal. Along these lines, weight loss can only be achieved by establishing a negative calorie balance, though this may be more tenable on a high-protein diet.
Red Meat Protein and Weight Control
The same high-protein foods that are good choices for disease prevention may also help with weight control. Researchers at Harvard School of Public Health followed the diet and lifestyle habits of 120,000 men and women for up to 20 years, looking at how small changes contributed to weight gain over time 116.
- Those who ate more red and processed meat over the course of the study gained more weight, about one extra pound every four years, while those who ate more nuts over the course of the study gained less weight, about a half pound less every four years.
- One study showed that eating approximately one daily serving of beans, chickpeas, lentils or peas can increase fullness, which may lead to better weight management and weight loss 117.
Therefore there’s no need to go overboard on protein. Though some studies show benefits of high-protein, low-carbohydrate diets in the short term, avoiding fruits and whole grains means missing out on healthful fiber, vitamins, minerals, and other phytonutrients.
Health Benefits of Dietary Protein
- Meat, poultry, fish, dry beans and peas, eggs, nuts, and seeds supply many nutrients. These include protein, B vitamins (niacin, thiamin, riboflavin, and B6), vitamin E, iron, zinc, and magnesium.
- Proteins function as building blocks for bones, muscles, cartilage, skin, and blood. They are also building blocks for enzymes, hormones, and vitamins.
- Proteins are one of three nutrients that provide calories (the others are fat and carbohydrates).
- B vitamins found in this food group serve a variety of functions in the body. They help the body release energy, play a vital role in the function of the nervous system, aid in the formation of red blood cells, and help build tissues.
- Iron is used to carry oxygen in the blood. Many teenage girls and women in their child-bearing years have iron-deficiency anemia. They should eat foods high in heme-iron (meats) or eat other non-heme iron containing foods along with a food rich in vitamin C, which can improve absorption of non-heme iron.
- Magnesium is used in building bones and in releasing energy from muscles.
- Zinc is necessary for biochemical reactions and helps the immune system function properly.
- EPA and DHA are omega-3 fatty acids found in varying amounts in seafood. Eating 8 ounces per week of seafood may help reduce the risk for heart disease.
Protein in diet (Food Sources)
Protein foods are broken down into parts called amino acids during digestion. The human body needs a number of amino acids in large enough amounts to maintain good health.
Amino acids are found in animal sources such as meats, milk, fish, and eggs. Animal sources of protein tend to deliver all the amino acids you need. However, animal protein can be high in fat. For example, a 6-ounce broiled porterhouse steak is a great source of protein—about 40 grams worth. But it also delivers about 12 grams of saturated fat 118. For someone who eats a 2,000 calorie per day diet, that’s more than 60 percent of the recommended daily intake for saturated fat. Protein are also found in plant sources such as soy, beans, legumes, nut butters, and some grains (such as wheat germ and quinoa). You do not need to eat animal products to get all the protein you need in your diet. But other non-animal protein sources, such as fruits, vegetables, grains, nuts and seeds, lack one or more essential amino acids 119.
Amino acids are classified into three groups:
- Essential : Essential amino acids cannot be made by the body, and must be supplied by food. They do not need to be eaten at one meal. The balance over the whole day is more important.
- Nonessential : Nonessential amino acids are made by the body from essential amino acids or in the normal breakdown of proteins.
- Conditional : Conditional amino acids are needed in times of illness and stress.
 What foods are in the Protein Foods Group ?
What foods are in the Protein Foods Group ?
All foods made from meat, poultry, seafood, beans and peas, eggs, processed soy products, nuts, and seeds are considered part of the Protein Foods Group 120. Select a variety of protein foods to improve nutrient intake and health benefits, including at least 8 ounces of cooked seafood per week. Young children need less, depending on their age and calorie needs. The advice to consume seafood does not apply to vegetarians. Vegetarian options in the Protein Foods Group include beans and peas, processed soy products, and nuts and seeds. Meat and poultry choices should be lean or low-fat.
The amount of food from the Protein Foods Group you need to eat depends on age, sex, and level of physical activity. Most Americans eat enough food from this group, but need to make leaner and more varied selections of these foods.
How Much Protein Should You Eat ?
The amount of food from the Protein Foods Group you need to eat depends on age, sex, and level of physical activity. Most Americans eat enough food from this group. The Institute of Medicine recommends that adults get a minimum of 0.8 grams of protein for every kilogram of body weight per day (or 8 grams of protein for every 20 pounds of body weight) 6, 7. In the United States, the recommended daily allowance of protein is 46 grams per day for women over 19 years of age, and 56 grams per day for men over 19 years of age 8. The Institute of Medicine also sets a wide range for acceptable protein intake—anywhere from 10 to 35 percent of calories each day. Beyond that, there’s relatively little solid information on the ideal amount of protein in the diet or the healthiest target for calories contributed by protein.
The U.S. Department of Agriculture’s newest food guide, called ChooseMyPlate 121, can help you make healthy eating choices.
The amount of protein you need in your diet will depend on your overall calorie needs. The daily recommended intake of protein for healthy adults is 10% to 35% of your total calorie needs. For example, a person on a 2000 calorie diet could eat 100 grams of protein, which would supply 20% of their total daily calories 122.
| Daily Protein recommendation 123 | ||
|---|---|---|
| Children | 2-3 years old 4-8 years old | 2 ounce equivalents 4 ounce equivalents |
| Girls | 9-13 years old 14-18 years old | 5 ounce equivalents 5 ounce equivalents |
| Boys | 9-13 years old 14-18 years old | 5 ounce equivalents 6 ½ ounce equivalents |
| Women | 19-30 years old 31-50 years old 51+ years old | 5 ½ ounce equivalents 5 ounce equivalents 5 ounce equivalents |
| Men | 19-30 years old 31-50 years old 51+ years old | 6 ½ ounce equivalents 6 ounce equivalents 5 ½ ounce equivalents |
This table below lists specific amounts that count as 1 ounce-equivalent in the Protein Foods Group towards your daily recommended intake.
| Amount that counts as 1 ounce-equivalent in the Protein Foods Group | Common portions and ounce-equivalents | |
|---|---|---|
| Meats | 1 ounce cooked lean beef 1 ounce cooked lean pork or ham | 1 small steak (eye of round, filet) = 3 ½ to 4 ounce-equivalents 1 small lean hamburger = 2 to 3 ounce-equivalents |
| Poultry | 1 ounce cooked chicken or turkey, without skin 1 sandwich slice of turkey (4 ½” x 2 ½” x 1/8″) | 1 small chicken breast half = 3 ounce-equivalents ½ Cornish game hen = 4 ounce-equivalents |
| Seafood | 1 ounce cooked fish or shell fish | 1 can of tuna, drained = 3 to 4 ounce-equivalents 1 salmon steak = 4 to 6 ounce-equivalents 1 small trout = 3 ounce-equivalents |
| Eggs | 1 egg | 3 egg whites = 2 ounce-equivalents 3 egg yolks = 1 ounce-equivalent |
| Nuts and seeds | ½ ounce of nuts (12 almonds, 24 pistachios, 7 walnut halves) ½ ounce of seeds (pumpkin, sunflower, or squash seeds, hulled, roasted) 1 Tablespoon of peanut butter or almond butter | 1 ounce of nuts of seeds = 2 ounce-equivalents |
| Beans and peas | ¼ cup of cooked beans (such as black, kidney, pinto, or white beans) ¼ cup of cooked peas (such as chickpeas, cowpeas, lentils, or split peas) ¼ cup (about 2 ounces) of tofu | 1 cup split pea soup = 2 ounce-equivalents 1 cup lentil soup = 2 ounce-equivalents 1 cup bean soup = 2 ounce-equivalents1 soy or bean burger patty = 2 ounce-equivalents |
(Source 123)
Protein Selection Tips
- Choose lean or low-fat meat and poultry. If higher fat choices are made, such as regular ground beef (75-80% lean) or chicken with skin, the fat counts against your limit for calories from saturated fats.
- If solid fat is added in cooking, such as frying chicken in shortening or frying eggs in butter or stick margarine, this also counts against your limit for calories from saturated fats.
- Select some seafood that is rich in omega-3 fatty acids, such as salmon, trout, sardines, anchovies, herring, Pacific oysters, and Atlantic and Pacific mackerel.
- Processed meats such as ham, sausage, frankfurters, and luncheon or deli meats have added sodium. Check the Nutrition Facts label to help limit sodium intake. Fresh chicken, turkey, and pork that have been enhanced with a salt-containing solution also have added sodium. Check the product label for statements such as “self-basting” or “contains up to __% of __”, which mean that a sodium-containing solution has been added to the product. A 6-ounce ham steak has only about 2.5 grams of saturated fat, but it’s loaded with sodium 2,000 milligrams worth, or about 500 milligrams more than the daily sodium max.
- Choose unsalted nuts and seeds to keep sodium intake low.
- Eating peanuts and certain tree nuts (i.e., walnuts, almonds, and pistachios) may reduce the risk of heart disease when consumed as part of a diet that is nutritionally adequate and within calorie needs. Because nuts and seeds are high in calories, eat them in small portions and use them to replace other protein foods, like some meat or poultry, rather than adding them to what you already eat. In addition, choose unsalted nuts and seeds to help reduce sodium intakes.
Why is it important to eat 8 ounces of seafood per week ?
- Seafood contains a range of nutrients, notably the omega-3 fatty acids, EPA and DHA. Eating about 8 ounces per week of a variety of seafood contributes to the prevention of heart disease. Smaller amounts of seafood are recommended for young children.
- 6-ounces of wild salmon has about 34 grams of protein and is naturally low in sodium, and contains only 1.7 grams of saturated fat. Salmon and other fatty fish are also excellent sources of omega-3 fats, a type of fat that’s especially good for the heart. Alternatively, a cup of cooked lentils provides about 18 grams of protein and 15 grams of fiber, and it has virtually no saturated fat or sodium 118.
- Seafood varieties that are commonly consumed in the United States that are higher in EPA and DHA and lower in mercury include salmon, anchovies, herring, sardines, Pacific oysters, trout, and Atlantic and Pacific mackerel (not king mackerel, which is high in mercury). The health benefits from consuming seafood outweigh the health risk associated with mercury, a heavy metal found in seafood in varying levels.
Why is it important to make lean or low-fat choices from the Protein Foods Group ?
Foods in the meat, poultry, fish, eggs, nuts, and seed group provide nutrients that are vital for health and maintenance of your body. However, choosing foods from this group that are high in saturated fat and cholesterol may have health implications 124.
- Diets that are high in saturated fats raise “bad” cholesterol levels in the blood. The “bad” cholesterol is called LDL (low-density lipoprotein) cholesterol. High LDL cholesterol, in turn, increases the risk for coronary heart disease. Some food choices in this group are high in saturated fat. These include fatty cuts of beef, pork, and lamb; regular (75% to 85% lean) ground beef; regular sausages, hot dogs, and bacon; some luncheon meats such as regular bologna and salami; and some poultry such as duck. To help keep blood cholesterol levels healthy, limit the amount of these foods you eat.
- Diets that are high in cholesterol can raise LDL cholesterol levels in the blood. Cholesterol is only found in foods from animal sources. Some foods from this group are high in cholesterol. These include egg yolks (egg whites are cholesterol-free) and organ meats such as liver and giblets. To help keep blood cholesterol levels healthy, limit the amount of these foods you eat.
- A high intake of fats makes it difficult to avoid consuming more calories than are needed.
Eating Red Meat and Cardiovascular Disease
Research conducted at Harvard School of Public Health has found that eating even small amounts of red meat, especially processed red meat, on a regular basis is linked to an increased risk of heart disease and stroke, and the risk of dying from cardiovascular disease or any other cause 102, 104, 106. Conversely, replacing red and processed red meat with healthy protein sources such as poultry, fish, or beans seems to reduce these risks.
- One investigation followed 120,000 men and women in the Nurses’ Health Study and Health Professionals Follow-Up Study for more than two decades 104. For every additional 3-ounce serving of unprocessed red meat the study participants consumed each day, their risk of dying from cardiovascular disease increased by 13 percent.
- Processed red meat was even more strongly linked to dying from cardiovascular disease—and in smaller amounts: Every additional 1.5 ounce serving of processed red meat consumed each day—equivalent to one hot dog or two strips of bacon—was linked to a 20 percent increase in the risk of cardiovascular disease death.
- Cutting back on red meat could save lives: the researchers estimated that if all the men and women in the study had reduced their total red and processed red meat intake to less than half a serving a day, one in ten cardiovascular disease deaths would have been prevented.
Eating Red Meat and Diabetes Risk
Again, protein quality matters more than protein quantity when it comes to diabetes risk 125.
- A recent study found that people who ate diets high in red meat, especially processed red meat, had a higher risk of type 2 diabetes than those who rarely ate red or processed meat 105. For each additional serving a day of red meat or processed red meat that study participants ate, their risk of diabetes rose 12 and 32 percent, respectively.
- Substituting one serving of nuts, low-fat dairy products, or whole grains for a serving of red meat each day lowered the risk of developing type 2 diabetes by an estimated 16 to 35 percent.
- Another study also shows that red meat consumption may increase risk of type 2 diabetes. Researchers found that people who started eating more red meat than usual were found to have a 50% increased risk of developing type 2 diabetes during the next four years, and researchers also found that those who reduced red meat consumption lowered their type 2 diabetes risk by 14% over a 10-year follow-up period.
- More evidence that protein quality matters comes from a 20-year study that looked at the relationship between low-carbohydrate diets and type 2 diabetes in women. Low-carbohydrate diets that were high in vegetable sources of fat and protein modestly reduced the risk of type 2 diabetes 126. But low-carbohydrate diets that were high in animal sources of protein or fat did not show this benefit.
For type 1 diabetes (formerly called juvenile or insulin-dependent diabetes), proteins found in cow’s milk have been implicated in the development of the disease in babies with a predisposition to the disease, but research remains inconclusive 127, 128.

Eating Red Meat and Cancer
When it comes to cancer, protein quality again seems to matter more than quantity. Research on the association between protein and cancer is ongoing, but some data shows that eating a lot of red meat and processed meat is linked to an increased risk of colon cancer 101.
- In the Nurse’s Health Study and the Health Professionals Follow-Up Study, every additional serving per day of red meat or processed red meat was associated with a 10 and 16 percent higher risk of cancer death, respectively 104.
- A 2014 study showed that higher consumption of red meat during adolescence was associated with premenopausal breast cancer, suggesting that choosing other protein sources in adolescence may decrease premenopausal breast cancer risk 129.
- People should aim to reduce overall consumption of red meat and processed meat, but when you do opt to have it, go easy on the grill. High-temperature grilling creates potentially cancer-causing compounds in meat. Heterocyclic amines (HCAs) and polycyclic aromatic hydrocarbons (PAHs) are chemicals formed when muscle meat, including beef, pork, fish, or poultry, is cooked using high-temperature methods, such as pan frying or grilling directly over an open flame 130. In laboratory experiments, HCAs and PAHs have been found to be mutagenic—that is, they cause changes in DNA that may increase the risk of cancer.
- HCAs are formed when amino acids (the building blocks of proteins), sugars, and creatine (a substance found in muscle) react at high temperatures. PAHs are formed when fat and juices from meat grilled directly over an open fire drip onto the fire, causing flames. These flames contain PAHs that then adhere to the surface of the meat. PAHs can also be formed during other food preparation processes, such as smoking of meats 130.
- HCAs are not found in significant amounts in foods other than meat cooked at high temperatures. PAHs can be found in other charred foods, as well as in cigarette smoke and car exhaust fumes.
- Even though no specific guidelines for HCA/PAH consumption exist, concerned individuals can reduce their exposure by using several cooking methods:+ Avoiding direct exposure of meat to an open flame or a hot metal surface and avoiding prolonged cooking times (especially at high temperatures) can help reduce HCA and PAH formation 131.
+ Using a microwave oven to cook meat prior to exposure to high temperatures can also substantially reduce HCA formation by reducing the time that meat must be in contact with high heat to finish cooking 131.
+ Continuously turning meat over on a high heat source can substantially reduce HCA formation compared with just leaving the meat on the heat source without flipping it often 131.
+ Removing charred portions of meat and refraining from using gravy made from meat drippings can also reduce HCA and PAH exposure 131.
In October 2015, the World Health Organization (WHO)’s International Agency for Research on Cancer (IARC) announced that consumption of processed meat is “carcinogenic to humans,” and that consumption of red meat is “probably carcinogenic to humans.” 132
- The IARC Working Group, comprised of 22 scientists from ten countries, evaluated over 800 studies.
- Conclusions were primarily based on the evidence for colorectal cancer. Data also showed positive associations between processed meat consumption and stomach cancer, and between red meat consumption and pancreatic and prostate cancer 132.
High Protein Diet and Increased Mortality
A high-protein diet during middle age was associated with higher mortality in a new study 133. In adults over 65, however, a high-protein diet was linked to lower mortality 133. A team led by Dr. Valter Longo at the University of Southern California set out to explore the link between dietary protein and mortality. The researchers analyzed information on more than 6,800 U.S. adults, ages 50 and over, from the Third National Health and Nutrition Examination Survey (NHANES III), a periodic health and nutritional survey of the U.S. population. Participants were categorized into 3 groups based on the percent of self-reported calorie intake that came from protein: high (20% or more), moderate (10-19%), or low (less than 10%). They were further split into 2 age categories: 50 to 65, and 66 and older.
Adults in the 50 to 65 group who reported a high protein intake had a 75% increase in overall mortality and were 4 times more likely to die from cancer during the following 18 years than those in the low protein group. The moderate-protein diet was associated with a 3-fold increase in cancer mortality compared to the low-protein diet.
These associations—which were adjusted for numerous factors including smoking, waist circumference, and chronic conditions—weren’t altered when the percentage of calories from fat or carbohydrate were considered. However, the associations were only found when the proteins were derived from animal, rather than plant, sources.
Conversely, in participants ages 65 and older, those who consumed high amounts of protein had a 28% lower risk of dying from any cause and a 60% lower risk of dying from cancer. These associations weren’t influenced by whether the protein was derived from animal or plant sources.
A high-protein diet was also associated with a 5-fold increase in diabetes mortality across all ages. One limitation of the study, the researchers note, is that the participants’ protein intake was based on a single 24-hour dietary recall. The study also didn’t examine the effects of specific types of plant- or animal-derived proteins, such as beef or fish.
Mouse studies confirmed the effects of high protein intake. Mice fed a higher protein diet had increased progression of breast and melanoma tumors than those fed a lower protein diet. The low-protein diet, however, had detrimental effects in very old mice. The link between diet and longevity appeared to be moderated by a pathway involving insulin-like growth factor 1 (IGF-1) 133.
Highlights from this study:
- High protein intake is linked to increased cancer, diabetes, and overall mortality.
- High IGF-1 levels increased the relationship between mortality and high protein.
- Higher protein consumption may be protective for older adults.
- Plant-derived proteins are associated with lower mortality than animal-derived proteins.
High Protein Diet and Osteoporosis
Digesting protein releases acids into the bloodstream, which the body usually neutralizes with calcium and other buffering agents. Eating lots of protein, then, requires a lot of calcium – and some of this may be pulled from bone. This area of research is still controversial, however, and the findings have not been consistent. Some studies suggest that increasing protein increases risk of fractures; others have linked high-protein diets with increased bone-mineral density, and thus stronger bones 134, 135, 136.
- Following a high-protein diet for a long period of time could weaken bone. In the Nurses’ Health Study, for example, women who ate more than 95 grams of protein a day were 20 percent more likely to have broken a wrist over a 12-year period when compared with those who ate an average amount of protein (less than 68 grams a day) 137.
Protein and Chronic Diseases
Proteins in food and the environment are responsible for food allergies, which are overreactions of the immune system. Beyond that, relatively little evidence has been gathered regarding the effect of the amount of dietary protein on the development of chronic diseases in healthy people.
However, there’s growing evidence that high-protein food choices do play a role in health and that eating healthy protein sources like fish, chicken, beans, or nuts in place of red meat (including processed red meat) can lower the risk of several diseases and premature death 101, 102, 103, 104, 105, 106, 107.
Protein Health Benefits
Protein provides the building blocks that help maintain and repair muscles, organs, and other parts of the body. Protein foods are important sources of nutrients in addition to protein, including B vitamins (e.g., niacin, vitamin B12, vitamin B6, and riboflavin), selenium, choline, phosphorus, zinc, copper, vitamin D, and vitamin E).
One ounce (30 grams) of most protein-rich foods contains 7 grams of protein. An ounce (30 grams) equals:
- 1 oz (30 g) of meat fish or poultry
- 1 large egg
- ¼ cup (60 milliliters) tofu
- ½ cup (65 grams) cooked beans or lentils
- 1 Tbsp (14 grams) peanut butter
Low fat dairy is also a good source of protein.
Whole grains contain more protein than refined or “white” products
Children and teens may need different amounts, depending on their age. Some healthy sources of meat protein include:
- Turkey or chicken with the skin removed, or bison (also called buffalo meat)
- Lean cuts of beef or pork, such as round, top sirloin, or tenderloin (trim away any visible fat)
- Fish or shellfish
Other good sources of protein include:
- Pinto beans, black beans, kidney beans, lentils, split peas, or garbanzo beans
- Nuts and seeds, including almonds, hazelnuts, mixed nuts, peanuts, peanut butter, sunflower seeds, or walnuts (just watch how much you eat, because nuts are high in fat)
- Tofu, tempeh, and other soy protein products
- Low-fat dairy products
Nutrients provided by various types of protein foods differ. For example, meats provide the most zinc, while poultry provides the most niacin. Meats, poultry, and seafood provide heme iron, which is more bioavailable than the non-heme iron found in plant sources. Heme iron is especially important for young children and women who are capable of becoming pregnant or who are pregnant. Seafood provides the most vitamin B12 and vitamin D, in addition to almost all of the polyunsaturated omega-3 fatty acids, eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). Eggs provide the most choline, and nuts and seeds provide the most vitamin E. Soy products are a source of copper, manganese, and iron, as are legumes 138.
Even though a higher protein intake can have health benefits for many people, it is not necessary for everyone.
Most people already eat protein at around 15% of calories, which is more than enough to prevent deficiency.
However, in certain cases, people can benefit from eating much more than that, or up to 25-30% of calories.
If you need to lose weight, improve your metabolic health or gain muscle mass and strength, then ensuring that you eat enough protein is important.
However, there are vastly different opinions on how much protein we actually need. Most official nutrition organizations recommend a fairly modest protein intake.
The DRI (Dietary Reference Intake) is 0.8 grams of protein per kilogram of body weight, or 0.36 grams per pound. The Recommended Dietary Allowance or Dietary Reference Intake is the amount of a nutrient you need to meet your basic nutritional requirements. In a sense, it’s the minimum amount you need to keep from getting sick — not the specific amount you are supposed to eat every day.
This amounts to:
- 56-91 grams per day for the average sedentary man.
- 46-75 grams per day for the average sedentary woman.
For a relatively active adult, eating enough protein to meet the recommended dietary allowance would supply as little as 10% of his or her total daily calories. In comparison, the average American consumes around 16% of his or her daily calories in the form of protein, from both plant and animal sources.
Although this meager amount may be enough to prevent downright deficiency, studies show that it is far from sufficient to ensure optimal health and body composition. But it turns out that the “right” amount of protein for any one individual depends on many factors – including activity levels, age, muscle mass, physique goals and current state of health.
Proteins are made out of smaller molecules called amino acids, which are linked together like beads on a string. The linked amino acids form long protein chains, which are then folded into complex shapes. Some of these amino acids can be produced by the body, while we must get others from the diet. The ones we can not produce and must get from our foods are called the “essential” amino acids.
Role of Protein
Proteins are nitrogen-containing substances that are formed by amino acids. They serve as the major structural component of muscle and other tissues in the body. In addition, they are used to produce hormones, enzymes and hemoglobin. Proteins can also be used as energy; however, they are not the primary choice as an energy source. For proteins to be used by the body they need to be metabolized into their simplest form, amino acids. There have been 20 amino acids identified that are needed for human growth and metabolism. Twelve of these amino acids (eleven in children) are termed nonessential, meaning that they can be synthesized by our body and do not need to be consumed in the diet. The remaining amino acids cannot be synthesized in the body and are described as essential meaning that they need to be consumed in our diets. The absence of any of these amino acids will compromise the ability of tissue to grow, be repaired or be maintained.
In athletes supplementing their diets with additional protein, casein has been shown to provide the greatest benefit for increases in protein synthesis for a prolonged duration. However, whey protein has a greater initial benefit for protein synthesis. These differences are related to their rates of absorption. It is likely a combination of the two could be beneficial, or smaller but more frequent ingestion of whey protein could prove to be of more value. Considering the paucity of research examining various sources of protein in sport supplementation studies, further research appears warranted on examining the benefits of these various protein sources.
Protein is not just about quantity. It’s also about quality.
Generally speaking, animal protein provides all the essential amino acids in the right ratio for us to make full use of them (only makes sense, since animal tissues are similar to our own tissues).
If you’re eating animal products (like meat, fish, eggs, or dairy) every day, then you’re probably already doing pretty well, protein-wise.
If you don’t eat animal foods, then it is a bit more challenging to get all the protein and essential amino acids that your body needs.
Bottom Line: Protein is a structural molecule assembled out of amino acids, many of which the body can’t produce on its own. Animal foods are usually high in protein, with all the essential amino acids that we need.

Good Sources of Protein
The best sources of protein are meats, fish, eggs and dairy products. They have all the essential amino acids that your body needs.
There are also some plants that are fairly high in protein, like quinoa, legumes and nuts.
1. Protein Can Reduce Appetite and Hunger Levels
Studies show that protein is by far the most filling. It helps you feel more full, with less food. A high-protein diet reduces hunger, helping you eat fewer calories. This is caused by improved function of weight regulating hormones.
Part of the reason is that protein reduces your level of the hunger hormone ghrelin. It also boosts the satiety hormone peptide YY, which makes you feel full.
This effect can be powerful. In one study, increasing protein from 15 to 30% of calories made overweight women eat 441 fewer calories each day, without intentionally restricting anything.
If you need to lose weight or belly fat, then consider replacing some of the carbs and fats you are eating with protein. It can be as simple as making your potato or rice serving smaller, while adding a few extra bites of meat or fish.
2. Protein Can Increase Muscle Mass and Strength
Protein forms the building blocks of muscles. Therefore, it seems logical that eating more protein would help you build more of them.
Perhaps not surprisingly, numerous studies show that eating plenty of protein can help increase muscle mass and strength.
If you’re physically active, lifting weights, or trying to gain muscle and strength, then you need to make sure that you’re getting enough protein.
Keeping protein high can also help prevent muscle loss when your body is in a “catabolic” (breaking down) state, such as during weight loss.
Bottom Line: Muscle is made primarily of protein. A high protein intake can help you gain muscle mass and strength, and can reduce muscle loss when losing weight.
3. Protein is Good For Your Bones (Not The Other Way Around)
There is an ongoing myth that protein (mostly animal protein) is bad for your bones. This is based on the idea that protein increases “acid load” in the body, leading to calcium being leached from the bones in order to neutralize the acid.
However, most long-term studies show that protein, including animal protein, has major benefits for bone health.
People who eat more protein tend to maintain their bone mass better as they get older, and tend to have a much lower risk of osteoporosis and fractures. This is especially important for women, who are at high risk of osteoporosis after menopause. Eating plenty of protein and staying active is a good way to help prevent that from happening.
Bottom Line: People who eat more protein tend to have better bone health as they get older. They have a much lower risk of osteoporosis and fractures.
4. Protein Can Reduce Cravings and Desire for Late-Night Snacking
A food craving is different from normal hunger. It is not just about your body needing energy or nutrients, it is about your brain needing a “reward”.
Just like a drug addict, alcoholic and smoker, the craving for junk food feels exactly the same as a craving for drugs, alcohol and nicotine.
Unfortunately, cravings can be incredibly hard to control. The best way to overcome them may be to prevent them from showing up in the first place. One of the best ways to do that is to increase your protein intake.
One study in overweight men showed that increasing protein to 25% of calories reduced cravings by 60%, and reduced the desire to snack at night by half.
Bottom Line: Eating more protein has been shown to reduce cravings and desire for late-night snacking. Just eating a high-protein breakfast may have a powerful effect.
5. Protein Can Boost Metabolism and Increase Fat Burning
Eating food can boost your metabolism for a short while. That’s because the body uses energy (calories) to digest and make use of the nutrients in foods. This is referred to as the thermic effect of food.
However, not all foods are the same in this regard. In fact, protein has a much higher thermic effect (20-35%) than fat or carbs (5-15%).
A high protein intake has been shown to significantly boost metabolism and increase the amount of calories you burn. This can amount to 80 to 100 more calories burned each day.
One study on protein during overfeeding found that a high protein group burned 260 more calories per day than a low-protein group. This is equivalent to an hour of moderate-intensity exercise per day !
Bottom Line: A higher protein intake has been shown to boost your metabolism significantly, helping you burn more calories throughout the day.
6. Protein Can Lower Your Blood Pressure
High blood pressure (hypertension) is a major cause of heart attacks, strokes and chronic kidney disease.
Interestingly, a higher protein intake has been shown to lower blood pressure in several studies. In a review of 40 controlled trials, increased protein lowered systolic blood pressure by 1.76 mmHg on average, and diastolic blood pressure by 1.15 mmHg.
One study found that, in addition to lowering blood pressure, a high-protein diet also reduced LDL cholesterol and triglycerides.
Bottom Line: Several studies have shown that a higher protein intake can lower blood pressure. Some studies also show improvements in other risk factors for heart disease.
7. Protein Can Help You Lose Weight and Keep it Off in The Long-Term
When it comes to losing weight, protein is the king of nutrients. As mentioned above, a high protein diet boosts metabolism and leads to automatic reduction in calorie intake and cravings. For this reason, it is not surprising to see that people who increase their protein intake tend to lose weight automatically.
In one study in overweight women, eating protein at 30% of calories caused them to lose 11 pounds (5 kg) in 12 weeks, without intentionally restricting anything.
Protein also has benefits for fat loss when intentionally restricting calories. In a 12-month study of 130 overweight people on a calorie-restricted diet, the high-protein group lost 53% more body fat than a normal-protein group eating the same number of calories.
Of course, losing weight is just the beginning. Maintaining the lost weight is actually a much bigger challenge for most people.
Just a modest increase in protein intake has been shown to help with weight maintenance. In one study, increasing protein from 15% to 18% of calories reduced weight regain by 50%.
If you want to lose weight, keep it off and prevent obesity in the future, then consider making a permanent increase your protein intake.
Bottom Line: Eating a lot of protein has numerous benefits for weight loss. It can help you lose more fat, and help you keep it off in the long-term.
8. Protein Does Not Harm Healthy Kidneys
Many people wrongly believe that a high protein intake harms your kidneys.
It is true that in people with pre-existing kidney disease, restricting protein intake can be beneficial. This should not be taken lightly, as kidney problems can be very serious.
However, while high protein intake may be harmful in people with kidney problems, it does NOT mean that it has any relevance to people with healthy kidneys.
In fact, numerous studies have looked at this and found that high-protein diets have no harmful effects in people who are free of kidney disease.
Bottom Line: It is true that protein can cause harm in people with kidney problems, but this has no relevance to people with healthy kidneys.
9. Protein Can Help Your Body Repair Itself After Injury
Protein can help your body repair after it has been injured. This makes perfect sense, given that it forms the main building blocks of the body’s tissues and organs.
Numerous studies have shown that eating more protein after injury can help speed up recovery.
Bottom Line: Eating more protein can help you recover faster after you have been injured.
10. Protein Can Help You Keep Fit as You Get Older
One of the consequences of aging, is that your muscles shrink. This is referred to as age-related sarcopenia, and is one of the main causes of frailty, bone fractures and reduced quality of life in old age.
Eating more protein is one of the best ways to prevent age-related sarcopenia. Staying physically active is also crucial, and lifting weights or doing some sort of resistance exercise can work wonders.
Substituting Healthy Proteins
Cutting back on red meat offers a life-extending dividend. In the Harvard School of Public Health study, adopting a diet with less than half a serving of red meat a day could have prevented about 1 in 10 deaths.
Swapping out red meat for more healthful protein sources is another life-extending option. Six good choices include:
- Fish
- Chicken and turkey
- Nuts
- Beans
- Low-fat dairy products
- Whole grains
Replacing one serving a day of red meat with one of these options reduced mortality in the study by 7% to 19%.
Of course, these numbers apply to a large group of people. How switching will affect you is hard to predict. It’s a good bet that reducing meat consumption—particularly processed meat (e.g. salamis, pepperonis, kabanas, sausages, bacon, ham)—is likely to score you an advantage.
Bottom Line: Eating plenty of protein can help reduce the muscle wasting associated with aging.
- High-protein, low-fat diets are effective for weight loss and favorably alter biomarkers in healthy adults. Johnston CS, Tjonn SL, Swan PD. J Nutr. 2004 Mar; 134(3):586-91. https://www.ncbi.nlm.nih.gov/pubmed/14988451/[↩]
- Short-term satiety in preschool children: a comparison between high protein meal and a high complex carbohydrate meal. Araya H, Hills J, Alviña M, Vera G. Int J Food Sci Nutr. 2000 Mar; 51(2):119-24. https://www.ncbi.nlm.nih.gov/pubmed/10953755/[↩]
- High-protein weight-loss diets: are they safe and do they work? A review of the experimental and epidemiologic data. Eisenstein J, Roberts SB, Dallal G, Saltzman E. Nutr Rev. 2002 Jul; 60(7 Pt 1):189-200. https://www.ncbi.nlm.nih.gov/pubmed/12144197/[↩]
- A randomized trial of a low-carbohydrate diet for obesity. Foster GD, Wyatt HR, Hill JO, McGuckin BG, Brill C, Mohammed BS, Szapary PO, Rader DJ, Edman JS, Klein S. N Engl J Med. 2003 May 22; 348(21):2082-90. https://www.ncbi.nlm.nih.gov/pubmed/12761365/[↩][↩][↩]
- Dietary protein and weight reduction: a statement for healthcare professionals from the Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association. St Jeor ST, Howard BV, Prewitt TE, Bovee V, Bazzarre T, Eckel RH, Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association. Circulation. 2001 Oct 9; 104(15):1869-74. https://www.ncbi.nlm.nih.gov/pubmed/11591629/[↩][↩][↩]
- Harvard School of Public Health. Nutrition Source: Protein. https://www.hsph.harvard.edu/nutritionsource/what-should-you-eat/protein/[↩][↩]
- Institute of Medicine, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients). 2005, National Academies Press: Washington, DC. http://national-academies.org/[↩][↩]
- Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. 2007, World Cancer Research Fund, American Institute for Cancer Research.: Washington, DC. http://www.aicr.org/assets/docs/pdf/reports/Second_Expert_Report.pdf[↩][↩][↩][↩]
- US Department of Agriculture, Agricultural Research Service, Beltsirlle Human Nutrition Centre, Food Surveys Research Group (Beltsirlle, MD) https://www.ars.usda.gov/[↩]
- Soenen S, Bonomi AG, Lemmens SG, Scholte J, Thijssen MA, van Berkum F, Westerterp-Plantenga MS. Relatively high-protein or ‘low-carb’ energy-restricted diets for body weight loss and body weight maintenance? Physiol Behav. 2012;107:374–380. doi: 10.1016/j.physbeh.2012.08.004. https://www.ncbi.nlm.nih.gov/pubmed/22935440[↩]
- Atkins RC. Dr. Atkins’ new diet revolution. 1st Quill edn. New York: Quill; 2002.[↩]
- St Jeor ST, Howard BV, Prewitt TE, Bovee V, Bazzarre T, Eckel RH, Nutrition Committee of the Council on Nutrition PA, Metabolism of the American Heart A Dietary protein and weight reduction: a statement for healthcare professionals from the Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association. Circulation. 2001;104:1869–1874. doi: 10.1161/hc4001.096152. https://www.ncbi.nlm.nih.gov/pubmed/11591629[↩][↩][↩]
- J Sports Sci Med. 2004 Sep; 3(3): 118–130. International Society of Sports Nutrition Symposium, June 18-19, 2005, Las Vegas NV, USA – Symposium – Macronutrient Utilization During Exercise: Implications For Performance And Supplementation. Protein – Which is Best ? https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3905294/[↩][↩][↩][↩][↩]
- Effects of an omnivorous diet compared with a lactoovovegetarian diet on resistance-training-induced changes in body composition and skeletal muscle in older men. Campbell WW, Barton ML Jr, Cyr-Campbell D, Davey SL, Beard JL, Parise G, Evans WJ. Am J Clin Nutr. 1999 Dec; 70(6):1032-9. https://www.ncbi.nlm.nih.gov/pubmed/10584048/[↩]
- Effect of protein source and quantity on protein metabolism in elderly women. Pannemans DL, Wagenmakers AJ, Westerterp KR, Schaafsma G, Halliday D. Am J Clin Nutr. 1998 Dec; 68(6):1228-35. https://www.ncbi.nlm.nih.gov/pubmed/9846851/[↩]
- Whey protein concentrate (WPC) and glutathione modulation in cancer treatment. Bounous G. Anticancer Res. 2000 Nov-Dec; 20(6C):4785-92. https://www.ncbi.nlm.nih.gov/pubmed/11205219/[↩]
- Functional properties of whey, whey components, and essential amino acids: mechanisms underlying health benefits for active people (review). Ha E, Zemel MB. J Nutr Biochem. 2003 May; 14(5):251-8. https://www.ncbi.nlm.nih.gov/pubmed/12832028/[↩]
- Branched-chain amino acids augment ammonia metabolism while attenuating protein breakdown during exercise. MacLean DA, Graham TE, Saltin B. Am J Physiol. 1994 Dec; 267(6 Pt 1):E1010-22. https://www.ncbi.nlm.nih.gov/pubmed/7810616/[↩]
- Geiser M. (2003) The wonders of whey protein. NSCA’s Performance Training Journal 2, 13-15[↩]
- Infusion of soy and casein protein meals affects interorgan amino acid metabolism and urea kinetics differently in pigs. Deutz NE, Bruins MJ, Soeters PB. J Nutr. 1998 Dec; 128(12):2435-45. https://www.ncbi.nlm.nih.gov/pubmed/9868192/[↩]
- Slow and fast dietary proteins differently modulate postprandial protein accretion. Boirie Y, Dangin M, Gachon P, Vasson MP, Maubois JL, Beaufrère B. Proc Natl Acad Sci U S A. 1997 Dec 23; 94(26):14930-5. https://www.ncbi.nlm.nih.gov/pubmed/9405716/[↩]
- Purification and characterization of cell growth factor in bovine colostrum. Kishikawa Y, Watanabe T, Watanabe T, Kubo S. J Vet Med Sci. 1996 Jan; 58(1):47-53. https://www.ncbi.nlm.nih.gov/pubmed/8645756/[↩]
- Effects of bovine colostrum supplementation on serum IGF-I, IgG, hormone, and saliva IgA during training. Mero A, Miikkulainen H, Riski J, Pakkanen R, Aalto J, Takala T. J Appl Physiol (1985). 1997 Oct; 83(4):1144-51. https://www.ncbi.nlm.nih.gov/pubmed/9338422/[↩]
- The effects of bovine colostrum supplementation on body composition and exercise performance in active men and women. Antonio J, Sanders MS, Van Gammeren D. Nutrition. 2001 Mar; 17(3):243-7. https://www.ncbi.nlm.nih.gov/pubmed/11312068/[↩]
- Bovine colostrum supplementation does not affect plasma buffer capacity or haemoglobin content in elite female rowers. Brinkworth GD, Buckley JD. Eur J Appl Physiol. 2004 Mar; 91(2-3):353-6. https://www.ncbi.nlm.nih.gov/pubmed/14685867/[↩][↩]
- The effect of bovine colostrum supplementation on exercise performance in elite field hockey players. Hofman Z, Smeets R, Verlaan G, Lugt Rv, Verstappen PA. Int J Sport Nutr Exerc Metab. 2002 Dec; 12(4):461-9. https://www.ncbi.nlm.nih.gov/pubmed/12500989/[↩]
- National Center for Complementary and Integrative Health. Soy. https://nccih.nih.gov/health/soy/ataglance.htm[↩][↩][↩][↩]
- Enderlin CA, Coleman EA, Stewart CB, et al.: Dietary soy intake and breast cancer risk. Oncol Nurs Forum 36 (5): 531-9, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19726393?dopt=Abstract[↩]
- Environ Health Perspect. 2006 Jun; 114(6): A352–A358. The Science of Soy: What Do We Really Know ? https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1480510/[↩][↩][↩]
- Young VR, Puig M, Queiroz E, Scrimshaw NS, Rand WM. Evaluation of the protein quality of an isolated soy protein in young men: relative nitrogen requirements and effects of methionine supplementation. Am J Clin Nutr. 1984;39:16–24. https://www.ncbi.nlm.nih.gov/pubmed/6537870/[↩]
- Baglieri A, Mahe S, Zidi S, Huneau JF, Thuillier F, Marteau P, Tome D. Gastro-jejunal digestion of soya-bean-milk protein in humans. Br J Nutr. 1994;72:519–532. doi: 10.1079/BJN19940056. https://www.ncbi.nlm.nih.gov/pubmed/7986784[↩]
- Mariotti F, Mahe S, Benamouzig R, Luengo C, Dare S, Gaudichon C, Tome D. Nutritional value of [15N]-soy protein isolate assessed from ileal digestibility and postprandial protein utilization in humans. J Nutr. 1999;129:1992–1997. https://www.ncbi.nlm.nih.gov/pubmed/10539774/[↩]
- Bos C, Metges CC, Gaudichon C, Petzke KJ, Pueyo ME, Morens C, Everwand J, Benamouzig R, Tome D. Postprandial kinetics of dietary amino acids are the main determinant of their metabolism after soy or milk protein ingestions in humans. J Nutr. 2003;133:1308–1315. https://www.ncbi.nlm.nih.gov/pubmed/12730415[↩]
- The Agency for Healthcare Research and Quality. Effects of Soy on Health Outcomes. https://archive.ahrq.gov/clinic/epcsums/soysum.htm[↩]
- Anderson JW, Bush HM. Soy protein effects on serum lipoproteins: a quality assessment and meta-analysis of randomized, controlled studies. Journal of the American College of Nutrition. 2011;30(2):79-91. https://www.ncbi.nlm.nih.gov/pubmed/21730216[↩]
- Fed Regist. 1999 Oct 26;64(206):57700-33. Food labeling: health claims; soy protein and coronary heart disease. Food and Drug Administration, HHS. Final rule. https://www.ncbi.nlm.nih.gov/pubmed/11010706?dopt=Abstract[↩]
- Lethaby A, Marjoribanks J, Kronenberg F, et al. Phytoestrogens for menopausal vasomotor symptoms. Cochrane Database of Systematic Reviews. 2013;(12):CD001395. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001395.pub4/full[↩]
- Taku K, Melby MK, Kronenberg F, et al. Extracted or synthesized soybean isoflavones reduce menopausal hot flash frequency and severity: systematic review and meta-analysis of randomized controlled trials. Menopause. 2012;19(7):776-790. https://www.ncbi.nlm.nih.gov/pubmed/22433977[↩]
- Clement YN, Onakpoya I, Hung SK, et al. Effects of herbal and dietary supplements on cognition in menopause: a systematic review. Maturitas. 2011;68(3):256-263. https://www.ncbi.nlm.nih.gov/pubmed/21237589[↩]
- Ricci E, Cipriani S, Chiaffarino F, et al. Soy isoflavones and bone mineral density in perimenopausal and postmenopausal Western women: a systematic review and meta-analysis of randomized controlled trials. Journal of Women’s Health. 2010;19(9):1609-1617. https://www.ncbi.nlm.nih.gov/pubmed/20673147[↩]
- Dong J-Y, Tong X, Wu Z-W, et al. Effect of soya protein on blood pressure: a meta-analysis of randomised controlled trials. British Journal of Nutrition. 2011;106(3):317-326. https://www.ncbi.nlm.nih.gov/pubmed/21342608[↩]
- U.S. National Library of Medicine. Medline Plus. Amino acids. https://medlineplus.gov/ency/article/002222.htm[↩][↩]
- Brosnan J (2003). “Interorgan amino acid transport and its regulation”. J Nutr 133 (6 Suppl 1): 2068S-2072S.[↩]
- Young V, Ajami A (2001). “Glutamine: the emperor or his clothes?”. J Nutr 131 (9 Suppl): 2449S-59S; discussion 2486S-7S.[↩]
- Wikipedia. Ketogenic amino acid. https://en.wikipedia.org/wiki/Ketogenic_amino_acid[↩]
- Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients) ( 2005 ) /10 Protein and Amino Acids. https://www.nap.edu/read/10490/chapter/12#593[↩]
- Agriculture, U.D.o., USDA Nutrient Database for Standard Reference, Release 14. 2005.[↩][↩][↩]
- Proteins and satiety: implications for weight management. Soenen S, Westerterp-Plantenga MS. Curr Opin Clin Nutr Metab Care. 2008 Nov; 11(6):747-51. https://www.ncbi.nlm.nih.gov/pubmed/18827579/[↩]
- Westerterp-Plantenga MSL-MN, Lejeune MPGM. Dietary protein, metabolism, and body-weight regulation: dose–response effects. Int J Obesity (Silver Spring) 2006;30:S16–S23.[↩]
- Stubbs RJ, van Wyk MC, Johnstone AM, Harbron CG. Breakfasts high in protein, fat or carbohydrate: effect on within-day appetite and energy balance. Eur J Clin Nutr. 1996;50:409–417. https://www.ncbi.nlm.nih.gov/pubmed/8862476[↩]
- Crovetti R, Porrini M, Santangelo A, Testolin G. The influence of thermic effect of food on satiety. Eur J Clin Nutr. 1998;52:482–488. doi: 10.1038/sj.ejcn.1600578. https://www.ncbi.nlm.nih.gov/pubmed/9683329[↩]
- Veldhorst M, Smeets A, Soenen S, Hochstenbach-Waelen A, Hursel R, Diepvens K, Lejeune M, Luscombe-Marsh N, Westerterp-Plantenga M. Protein-induced satiety: effects and mechanisms of different proteins. Physiol Behav. 2008;94:300–307. doi: 10.1016/j.physbeh.2008.01.003. https://www.ncbi.nlm.nih.gov/pubmed/18282589[↩]
- Acheson KJ. Influence of autonomic nervous system on nutrient-induced thermogenesis in humans. Nutrition. 1993;9:373–380. https://www.ncbi.nlm.nih.gov/pubmed/8400596[↩]
- Westerterp KR. Diet induced thermogenesis. Nutr Metab (Lond) 2004;1:5. doi: 10.1186/1743-7075-1-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC524030/[↩]
- Eisenstein J, Roberts SB, Dallal G, Saltzman E. High-protein weight-loss diets: are they safe and do they work? A review of the experimental and epidemiologic data. Nutr Rev. 2002;60:189–200. doi: 10.1301/00296640260184264. https://www.ncbi.nlm.nih.gov/pubmed/12144197[↩]
- Mikkelsen PB, Toubro S, Astrup A. Effect of fat-reduced diets on 24-h energy expenditure: comparisons between animal protein, vegetable protein, and carbohydrate. Am J Clin Nutr. 2000;72:1135–1141. https://www.ncbi.nlm.nih.gov/pubmed/11063440[↩]
- Westerterp-Plantenga MS, Rolland V, Wilson SA, Westerterp KR. Satiety related to 24 h diet-induced thermogenesis during high protein/carbohydrate vs high fat diets measured in a respiration chamber. Eur J Clin Nutr. 1999;53:495–502. doi: 10.1038/sj.ejcn.1600782. https://www.ncbi.nlm.nih.gov/pubmed/10403587[↩]
- The effect of a low-fat, high-protein or high-carbohydrate ad libitum diet on weight loss maintenance and metabolic risk factors. Claessens M, van Baak MA, Monsheimer S, Saris WH. Int J Obes (Lond). 2009 Mar; 33(3):296-304. https://www.ncbi.nlm.nih.gov/pubmed/19153580/[↩]
- Increased protein intake reduces lean body mass loss during weight loss in athletes. Mettler S, Mitchell N, Tipton KD. Med Sci Sports Exerc. 2010 Feb; 42(2):326-37. https://www.ncbi.nlm.nih.gov/pubmed/19927027/[↩]
- Reduced oxidation of dietary fat after a short term high-carbohydrate diet. Roberts R, Bickerton AS, Fielding BA, Blaak EE, Wagenmakers AJ, Chong MF, Gilbert M, Karpe F, Frayn KN. Am J Clin Nutr. 2008 Apr; 87(4):824-31. https://www.ncbi.nlm.nih.gov/pubmed/18400703/[↩]
- A high-protein, high-fat, carbohydrate-free diet reduces energy intake, hepatic lipogenesis, and adiposity in rats. Pichon L, Huneau JF, Fromentin G, Tomé D. J Nutr. 2006 May; 136(5):1256-60. https://www.ncbi.nlm.nih.gov/pubmed/16614413/[↩]
- Change in daily energy intake associated with pairwise compositional change in carbohydrate, fat and protein intake among US adults, 1999-2010. An R, Burd NA. Public Health Nutr. 2015 Jun; 18(8):1343-52. https://www.ncbi.nlm.nih.gov/pubmed/25203716/[↩]
- Interplay between lipids and branched-chain amino acids in development of insulin resistance. Newgard CB. Cell Metab. 2012 May 2; 15(5):606-14. https://www.ncbi.nlm.nih.gov/pubmed/22560213/[↩]
- Effect of low-carbohydrate high-protein diets on acid-base balance, stone-forming propensity, and calcium metabolism. Reddy ST, Wang CY, Sakhaee K, Brinkley L, Pak CY. Am J Kidney Dis. 2002 Aug; 40(2):265-74. https://www.ncbi.nlm.nih.gov/pubmed/12148098/[↩][↩]
- The effect of high animal protein intake on the risk of calcium stone-formation in the urinary tract. Robertson WG, Heyburn PJ, Peacock M, Hanes FA, Swaminathan R. Clin Sci (Lond). 1979 Sep; 57(3):285-8. https://www.ncbi.nlm.nih.gov/pubmed/573189/[↩]
- Do regular high protein diets have potential health risks on kidney function in athletes ? Poortmans JR, Dellalieux O. Int J Sport Nutr Exerc Metab. 2000 Mar; 10(1):28-38. https://www.ncbi.nlm.nih.gov/pubmed/10722779/[↩]
- The hyperfiltration theory: a paradigm shift in nephrology. Brenner BM, Lawler EV, Mackenzie HS. Kidney Int. 1996 Jun; 49(6):1774-7. https://www.ncbi.nlm.nih.gov/pubmed/8743495/[↩]
- Bernstein, A.M., et al., Major dietary protein sources and risk of coronary heart disease in women. Circulation, 2010. 122(9): p. 876-83. https://www.ncbi.nlm.nih.gov/pubmed/20713902[↩][↩]
- Aune, D., G. Ursin, and M.B. Veierod, Meat consumption and the risk of type 2 diabetes: a systematic review and meta-analysis of cohort studies. Diabetologia, 2009. 52(11): p. 2277-87. https://www.ncbi.nlm.nih.gov/pubmed/19662376[↩]
- Pan, A., et al., Red meat consumption and mortality: results from 2 prospective cohort studies. Arch Intern Med, 2012. 172(7): p. 555-63. https://www.ncbi.nlm.nih.gov/pubmed/22412075[↩][↩][↩][↩]
- Pan, A., et al., Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am J Clin Nutr, 2011. 94(4): p. 1088-96. https://www.ncbi.nlm.nih.gov/pubmed/21831992[↩][↩]
- Bernstein, A.M., et al., Dietary protein sources and the risk of stroke in men and women. Stroke, 2012. 43(3): p. 637-44. www.ncbi.nlm.nih.gov/pubmed/22207512[↩]
- Song, M., Fung, T.T., Hu, F.B., et al. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality. JAMA Intern Med. Published online August 01, 2016. https://www.hsph.harvard.edu/news/hsph-in-the-news/healthy-eating-red-meat-stroke-hu/[↩]
- Bernstein, A.M., et al., Dietary protein sources and the risk of stroke in men and women. Stroke, 2012. 43(3): p. 637-44. https://www.ncbi.nlm.nih.gov/pubmed/22207512[↩]
- Halton, T.L., et al., Low-carbohydrate-diet score and the risk of coronary heart disease in women. N Engl J Med, 2006. 355(19): p. 1991-2002. https://www.ncbi.nlm.nih.gov/pubmed/17093250[↩]
- Appel, L.J., et al., Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: results of the OmniHeart randomized trial. JAMA, 2005. 294(19): p. 2455-64. https://www.ncbi.nlm.nih.gov/pubmed/16287956[↩]
- Jenkins, D.J., et al., The effect of a plant-based low-carbohydrate (“Eco-Atkins”) diet on body weight and blood lipid concentrations in hyperlipidemic subjects. Arch Intern Med, 2009. 169(11): p. 1046-54. https://www.ncbi.nlm.nih.gov/pubmed/19506174[↩]
- Lagiou, P., et al., Low carbohydrate-high protein diet and incidence of cardiovascular diseases in Swedish women: prospective cohort study. BMJ, 2012. 344: p. e4026. https://www.ncbi.nlm.nih.gov/pubmed/22735105[↩]
- Ley, S. H., Sun, Q., Willett, W. C., Eliassen, A. H., Wu, K., Pan, A., … & Hu, F. B. (2014). Associations between red meat intake and biomarkers of inflammation and glucose metabolism in women. Am J Clin Nutr, February 2014. http://ajcn.nutrition.org/content/early/2013/11/27/ajcn.113.075663.short[↩]
- Halton, T.L., et al., Low-carbohydrate-diet score and risk of type 2 diabetes in women. Am J Clin Nutr, 2008. 87(2): p. 339-46. www.ncbi.nlm.nih.gov/pubmed/18258623[↩]
- Akerblom, H.K., et al., Environmental factors in the etiology of type 1 diabetes. Am J Med Genet, 2002. 115(1): p. 18-29. https://www.ncbi.nlm.nih.gov/pubmed/12116173[↩]
- Vaarala, O., et al., Removal of Bovine Insulin From Cow’s Milk Formula and Early Initiation of Beta-Cell Autoimmunity in the FINDIA Pilot Study. Arch Pediatr Adolesc Med, 2012. https://www.ncbi.nlm.nih.gov/pubmed/22393174[↩]
- Long-term high-protein diet induces biochemical and ultrastructural changes in rat liver mitochondria. Jordá A, Zaragozá R, Portolés M, Báguena-Cervellera R, Renau-Piqueras J. Arch Biochem Biophys. 1988 Sep; 265(2):241-8. https://www.ncbi.nlm.nih.gov/pubmed/3421703/[↩]
- Navder K.P., Lieber C.S. (2003b) Nutrition and alcoholism. : Nutritional Aspects and Clinical Management of Chronic Disorders and Diseases. : Bronner F., editor. Boca Raton, FL: CRC Press; 307-320[↩][↩]
- A study of oral nutritional support with oxandrolone in malnourished patients with alcoholic hepatitis: results of a Department of Veterans Affairs cooperative study. Mendenhall CL, Moritz TE, Roselle GA, Morgan TR, Nemchausky BA, Tamburro CH, Schiff ER, McClain CJ, Marsano LS, Allen JI. Hepatology. 1993 Apr; 17(4):564-76. https://www.ncbi.nlm.nih.gov/pubmed/8477961/[↩]
- Farvid MS, Cho E, Chen WY, Eliassen AH, Willett WC. Adolescent meat intake and breast cancer risk. Int J Cancer, 2014. https://www.ncbi.nlm.nih.gov/pubmed/?term=farvid+cho+adolescent+meat+intake+and+breast+cancer+risk[↩]
- Bouvard V, Loomis D, Guyton KZ, Grosse Y, Ghissassi FE, Benbrahim-Tallaa L, Guha N1, Mattock H, Straif K; International Agency for Research on Cancer Monograph Working Group (2015). Carcinogenicity of consumption of red and processed meat. Lancet Oncol doi: 10.1016/S1470-2045(15)00444-1. https://www.ncbi.nlm.nih.gov/pubmed/?term=26514947[↩][↩]
- Feskanich, D., et al., Protein consumption and bone fractures in women. Am J Epidemiol, 1996. 143(5): p. 472-9. https://www.ncbi.nlm.nih.gov/pubmed/8610662[↩]
- Darling, A.L., et al., Dietary protein and bone health: a systematic review and meta-analysis. Am J Clin Nutr, 2009. 90(6): p. 1674-92. https://www.ncbi.nlm.nih.gov/pubmed/19889822[↩]
- Kerstetter, J.E., A.M. Kenny, and K.L. Insogna, Dietary protein and skeletal health: a review of recent human research. Curr Opin Lipidol, 2011. 22(1): p. 16-20. https://www.ncbi.nlm.nih.gov/pubmed/21102327[↩]
- Bonjour, J.P., Protein intake and bone health. Int J Vitam Nutr Res, 2011. 81(2-3): p. 134-42. https://www.ncbi.nlm.nih.gov/pubmed/22139564[↩]
- Mozaffarian, D., et al., Changes in diet and lifestyle and long-term weight gain in women and men. N Engl J Med, 2011. 364(25): p. 2392-404. http://www.nejm.org/doi/full/10.1056/NEJMoa1014296[↩]
- Li SS, Kendall CW, de Souza RJ, Jayalath VH, Cozma AI, Ha V, Mirrahimi A, Chiavaroli L, Augustin LS, Blanco Mejia S, Leiter LA, Beyene J, Jenkins DJ, Sievenpiper JL. Dietary pulses, satiety and food intake: a systematic review and meta-analysis of acute feeding trials. Obesity, 2014. Aug;22(8):1773-80. https://www.ncbi.nlm.nih.gov/pubmed/24820437[↩]
- Nutr Metab (Lond). 2014; 11: 53. Published online 2014 Nov 19. doi: 10.1186/1743-7075-11-53. A high-protein diet for reducing body fat: mechanisms and possible caveats. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4258944/#CR8[↩]
- Long-term effects of a high-protein weight-loss diet. Clifton PM, Keogh JB, Noakes M. Am J Clin Nutr. 2008 Jan; 87(1):23-9. https://www.ncbi.nlm.nih.gov/pubmed/18175733/[↩]
- Protein diets, body weight loss and weight maintenance. Martens EA, Westerterp-Plantenga MS. Curr Opin Clin Nutr Metab Care. 2014 Jan; 17(1):75-9. https://www.ncbi.nlm.nih.gov/pubmed/24310056/[↩]
- A high-protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations. Weigle DS, Breen PA, Matthys CC, Callahan HS, Meeuws KE, Burden VR, Purnell JQ. Am J Clin Nutr. 2005 Jul; 82(1):41-8. https://www.ncbi.nlm.nih.gov/pubmed/16002798/[↩]
- U.S. National Library of Medicine, MedlinePlus. Dietary Proteins. https://medlineplus.gov/dietaryproteins.html[↩]
- U.S. National Library of Medicine, MedlinePlus. Protein in diet. https://medlineplus.gov/ency/article/002467.htm[↩]
- National Institutes of Health News in Health. How Much Protein Do You Need ? https://newsinhealth.nih.gov/2008/March/docs/01features_01.htm[↩][↩][↩][↩]
- Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. 2007, World Cancer Research Fund, American Institute for Cancer Research.: Washington, DC.[↩][↩][↩]
- Bernstein, A.M., et al., Major dietary protein sources and risk of coronary heart disease in women. Circulation, 2010. 122(9): p. 876-83.[↩][↩][↩]
- Aune, D., G. Ursin, and M.B. Veierod, Meat consumption and the risk of type 2 diabetes: a systematic review and meta-analysis of cohort studies. Diabetologia, 2009. 52(11): p. 2277-87.[↩][↩]
- Pan, A., et al., Red meat consumption and mortality: results from 2 prospective cohort studies. Arch Intern Med, 2012. 172(7): p. 555-63.[↩][↩][↩][↩][↩]
- Pan, A., et al., Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am J Clin Nutr, 2011. 94(4): p. 1088-96.[↩][↩][↩]
- Bernstein, A.M., et al., Dietary protein sources and the risk of stroke in men and women. Stroke, 2012. 43(3): p. 637-44.[↩][↩][↩]
- Song, M., Fung, T.T., Hu, F.B., et al. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality. JAMA Intern Med. Published online August 01, 2016.[↩][↩]
- Halton, T.L., et al., Low-carbohydrate-diet score and the risk of coronary heart disease in women. N Engl J Med, 2006. 355(19): p. 1991-2002.[↩]
- Appel, L.J., et al., Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: results of the OmniHeart randomized trial. JAMA, 2005. 294(19): p. 2455-64.[↩]
- Jenkins, D.J., et al., The effect of a plant-based low-carbohydrate (“Eco-Atkins”) diet on body weight and blood lipid concentrations in hyperlipidemic subjects. Arch Intern Med, 2009. 169(11): p. 1046-54.[↩]
- Lagiou, P., et al., Low carbohydrate-high protein diet and incidence of cardiovascular diseases in Swedish women: prospective cohort study. BMJ, 2012. 344: p. e4026.[↩]
- J Am Coll Nutr. 2004 Oct;23(5):373-85. The effects of high protein diets on thermogenesis, satiety and weight loss: a critical review. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0021577/[↩]
- Dietary fat intake and the risk of coronary heart disease in women. Hu FB, Stampfer MJ, Manson JE, Rimm E, Colditz GA, Rosner BA, Hennekens CH, Willett WC. N Engl J Med. 1997 Nov 20; 337(21):1491-9. https://www.ncbi.nlm.nih.gov/pubmed/9366580/[↩]
- Utilization and preferred metabolic pathway of ketone bodies for lipid synthesis by isolated rat hepatoma cells. Hildebrandt LA, Spennetta T, Elson C, Shrago E. Am J Physiol. 1995 Jul; 269(1 Pt 1):C22-7. https://www.ncbi.nlm.nih.gov/pubmed/7631749/[↩]
- Amino acid ingestion and glucose metabolism–a review. Gannon MC, Nuttall FQ. IUBMB Life. 2010 Sep; 62(9):660-8. https://www.ncbi.nlm.nih.gov/pubmed/20882645/[↩]
- Mozaffarian, D., et al., Changes in diet and lifestyle and long-term weight gain in women and men. N Engl J Med, 2011. 364(25): p. 2392-404.[↩]
- Li SS, Kendall CW, de Souza RJ, Jayalath VH, Cozma AI, Ha V, Mirrahimi A, Chiavaroli L, Augustin LS, Blanco Mejia S, Leiter LA, Beyene J, Jenkins DJ, Sievenpiper JL. Dietary pulses, satiety and food intake: a systematic review and meta-analysis of acute feeding trials. Obesity, 2014. Aug;22(8):1773-80.[↩]
- Agriculture, U.D.O., USDA Nutrient Database for Standard Reference, Release 14. 2005.[↩][↩]
- Harvard School of Public Health. The Nutrition Source : Protein. https://www.hsph.harvard.edu/nutritionsource/what-should-you-eat/protein[↩]
- USDA ChooseMyPlate. All about the Protein Foods Group. https://www.choosemyplate.gov/protein-foods[↩]
- https://www.choosemyplate.gov/[↩]
- US Department of Health and Human Services and US Department of Agriculture. 2015-2020 Dietary Guidelines for Americans. 8th Edition. December 2015. https://health.gov/dietaryguidelines/2015/guidelines/[↩]
- U.S. Department of Agriculture ChooseMyPlate. All about the Protein Foods Group. https://www.choosemyplate.gov/protein-foods[↩][↩]
- U.S. Department of Agriculture ChooseMyPlate. Nutrients and health benefits. https://www.choosemyplate.gov/protein-foods-nutrients-health[↩]
- Ley, S. H., Sun, Q., Willett, W. C., Eliassen, A. H., Wu, K., Pan, A., … & Hu, F. B. (2014). Associations between red meat intake and biomarkers of inflammation and glucose metabolism in women. Am J Clin Nutr, February 2014.[↩]
- Halton, T.L., et al., Low-carbohydrate-diet score and risk of type 2 diabetes in women. Am J Clin Nutr, 2008. 87(2): p. 339-46.[↩]
- Akerblom, H.K., et al., Environmental factors in the etiology of type 1 diabetes. Am J Med Genet, 2002. 115(1): p. 18-29.[↩]
- Vaarala, O., et al., Removal of Bovine Insulin From Cow’s Milk Formula and Early Initiation of Beta-Cell Autoimmunity in the FINDIA Pilot Study. Arch Pediatr Adolesc Med, 2012.[↩]
- Farvid MS, Cho E, Chen WY, Eliassen AH, Willett WC. Adolescent meat intake and breast cancer risk. Int J Cancer, 2014.[↩]
- Cross AJ, Sinha R. Meat-related mutagens/carcinogens in the etiology of colorectal cancer. Environmental and Molecular Mutagenesis 2004; 44(1):44–55. https://www.ncbi.nlm.nih.gov/pubmed/15199546[↩][↩]
- Knize MG, Felton JS. Formation and human risk of carcinogenic heterocyclic amines formed from natural precursors in meat. Nutrition Reviews 2005; 63(5):158–165. https://www.ncbi.nlm.nih.gov/pubmed/15971410[↩][↩][↩][↩]
- Bouvard V, Loomis D, Guyton KZ, Grosse Y, Ghissassi FE, Benbrahim-Tallaa L, Guha N1, Mattock H, Straif K; International Agency for Research on Cancer Monograph Working Group (2015). Carcinogenicity of consumption of red and processed meat. Lancet Oncol doi: 10.1016/S1470-2045(15)00444-1.[↩][↩]
- Levine, Morgan E. et al. Low Protein Intake Is Associated with a Major Reduction in IGF-1, Cancer, and Overall Mortality in the 65 and Younger but Not Older Population. Cell Metabolism , Volume 19 , Issue 3 , 407 – 417. http://www.cell.com/cell-metabolism/fulltext/S1550-4131(14)00062-X[↩][↩][↩]
- Darling, A.L., et al., Dietary protein and bone health: a systematic review and meta-analysis. Am J Clin Nutr, 2009. 90(6): p. 1674-92.[↩]
- Kerstetter, J.E., A.M. Kenny, and K.L. Insogna, Dietary protein and skeletal health: a review of recent human research. Curr Opin Lipidol, 2011. 22(1): p. 16-20.[↩]
- Bonjour, J.P., Protein intake and bone health. Int J Vitam Nutr Res, 2011. 81(2-3): p. 134-42.[↩]
- Feskanich, D., et al., Protein consumption and bone fractures in women. Am J Epidemiol, 1996. 143(5): p. 472-9.[↩]
- National Academy of Sciences, Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. National Academy Press. Washington, DC, 2005.[↩]





{kind=link}