Contents
- What is end-stage renal disease?
- What is glomerular filtration rate (GFR)?
- What is conservative management in kidney failure?
- What are the pros and cons of conservative management?
- Does dialysis cure kidney failure?
- Can hemodialysis do everything my kidneys once did?
- When do I have to start dialysis?
- What are the pros and cons of having hemodialysis at home?
- What are the pros and cons of having hemodialysis at dialysis center?
- How do I find a dialysis center?
- What are the types of peritoneal dialysis?
- What are the pros and cons of peritoneal dialysis?
- How is kidney transplant done?
- What are the side effects of anti-rejection medicines?
- Paying for medicines
- How do I pay for my kidney transplant?
- How can I get Medicare for kidney failure?
- What health plans does Medicare offer?
- What types of private health insurance can help with kidney failure treatment costs?
- Kidneys
- Stages of kidney disease
- End-stage renal disease causes
- End-stage renal disease prevention
- End-stage renal disease signs and symptoms
- End-stage renal disease complications
- End-stage renal disease diagnosis
- End-stage renal disease treatment
What is end-stage renal disease?
End-stage renal disease (ESRD) also called end-stage kidney disease (ESKD), Stage 5 chronic kidney disease or end-stage renal failure is when you have permanent kidney failure (GFR less than 15 ml/min/1.73m²) that requires a regular course of dialysis (hemodialysis or peritoneal dialysis) or a kidney transplant. End-stage renal disease (ESRD) is the most severe form of chronic kidney disease (CKD) with patients usually requiring kidney replacement therapy in the form of hemodialysis or peritoneal dialysis or kidney transplantation to survive.
Early in chronic kidney disease (CKD), you might have no signs or symptoms. As your chronic kidney disease (CKD) progresses to end-stage renal disease (ESRD), signs and symptoms might include:
- Nausea
- Vomiting
- Loss of appetite
- Fatigue and weakness
- Changes in how much you urinate
- Chest pain, if fluid builds up around the lining of the heart
- Shortness of breath, if fluid builds up in the lungs
- Swelling of feet and ankles
- High blood pressure (hypertension) that’s difficult to control
- Headaches
- Difficulty sleeping
- Decreased mental sharpness
- Muscle twitches and cramps
- Itchy skin
- Weight loss
- Bone pain
- Metallic taste
The signs and symptoms of kidney disease are often nonspecific, meaning they can also be caused by other illnesses. It’s important that you see your doctor if you have signs or symptoms of kidney disease. Because your kidneys can make up for lost function, signs and symptoms might not appear until irreversible damage to your kidneys has occurred.
End-stage renal disease (ESRD) causes may include:
- Diabetes
- High blood pressure
- Polycystic kidney disease
- Tobacco use
- Family history of kidney disease or failure
- Older age
- Frequent use of medications that could be damaging to your kidney.
If you have a medical condition that increases your risk of kidney disease, your doctor is likely to monitor your kidney function with urine and blood tests and your blood pressure during regular office visits. Ask your doctor whether these tests are necessary for you.
End-stage renal disease (ESRD) is kidney failure that is treated by dialysis or kidney transplant.
To replace your lost kidney function, you may have one of four treatment options:
- Hemodialysis. Hemodialysis is a treatment to filter wastes and water from your blood, as your kidneys did when they were healthy. During hemodialysis, your blood goes through a filter, called a dialyzer, outside your body 1. A dialyzer is sometimes called an “artificial kidney”. Hemodialysis helps control blood pressure and balance important minerals, such as potassium, sodium, and calcium, in your blood. At the start of a hemodialysis treatment, a dialysis nurse or technician places two needles into your arm. You may prefer to put in your own needles after you’re trained by your health care team. A numbing cream or spray can be used if placing the needles bothers you. Each needle is attached to a soft tube connected to the dialysis machine. The dialysis machine pumps blood through the filter and returns the blood to your body. During the process, the dialysis machine checks your blood pressure and controls how quickly blood flows through the filter and fluid is removed from your body. You can receive treatment at a dialysis center or at home. Each location has its pros and cons.
- Peritoneal dialysis. Peritoneal dialysis is a treatment for kidney failure that uses the lining of your abdomen, or belly, to filter your blood inside your body 2. Doctors call this lining the peritoneum. A few weeks before you start peritoneal dialysis, a surgeon places a soft tube called a catheter in your belly. When you start treatment, dialysis solution (water with salt and other additives) flows from a bag through the catheter into your belly. When the bag is empty, you disconnect it and place a cap on your catheter so you can move around and do your normal activities. While the dialysis solution is inside your belly, it absorbs wastes and extra fluid from your body 2. You shouldn’t feel any pain. Most people look and feel normal despite a belly full of solution. After a few hours, the solution and the wastes are drained out of your belly into the empty bag. You can throw away the used solution in a toilet or tub. Then, you start over with a fresh bag of dialysis solution. When the solution is fresh, it absorbs wastes quickly. As time passes, filtering slows. For this reason, you need to repeat the process of emptying the used solution and refilling your belly with fresh solution four to six times every day. This process is called an exchange. You can do your exchanges during the day, or at night using a machine that pumps the fluid in and out. For the best results, it is important that you perform all of your exchanges as prescribed. Dialysis can help you feel better and live longer, but it is not a cure for kidney failure.
- Kidney transplant. Kidney transplant is surgery to place a healthy kidney from a person who has just died, or from a living person, into your body to filter your blood.
- Conservative management. Some people with kidney failure choose not to have dialysis or a transplant but continue to receive care from their health care team, take medicines, and monitor their diet and lifestyle choices to preserve your kidney function and quality of life as long as possible.
As part of your treatment for kidney disease, your doctor might recommend that you follow a special diet to help support your kidneys and limit the work they must do. Ask for a referral to a registered dietitian with expertise in kidney disease to learn ways to make your diet easier on your kidneys. You can find a registered dietitian online through the Academy of Nutrition and Dietetics or through your kidney care team. Work closely with your dietitian to develop a meal plan that includes foods and drinks you enjoy eating while maintaining your health.
Depending on your situation, kidney function and overall health, your dietitian might recommend that you:
- Avoid products with added salt. Lower the amount of sodium you eat each day by avoiding products with added salt, including many convenience foods, such as frozen dinners, canned soups and fast foods. Other foods with added salt include salty snack foods, canned vegetables, and processed meats and cheeses.
- Choose lower potassium foods. Your dietitian might recommend that you choose lower potassium foods at each meal. High-potassium foods include bananas, oranges, potatoes, spinach and tomatoes. Examples of low-potassium foods include apples, cabbage, carrots, green beans, grapes and strawberries. Be aware that many salt substitutes contain potassium, so you generally should avoid them if you have kidney failure.
- Limit your protein. Your dietitian will estimate the grams of protein you need each day and make recommendations based on that amount. High-protein foods include lean meats, eggs, milk, cheese and beans. Low-protein foods include vegetables, fruits, breads and cereals.
Doing well with kidney failure is a challenge, and it works best if you:
- stick to your treatment schedule.
- review your medicines with your health care provider at every visit. You are the only one who knows how your body is responding to each of your medicines. It’s really important that your doctor knows which medicines you are taking.
- follow a special eating plan.
- are active most days of the week.
Figure 1. Hemodialysis
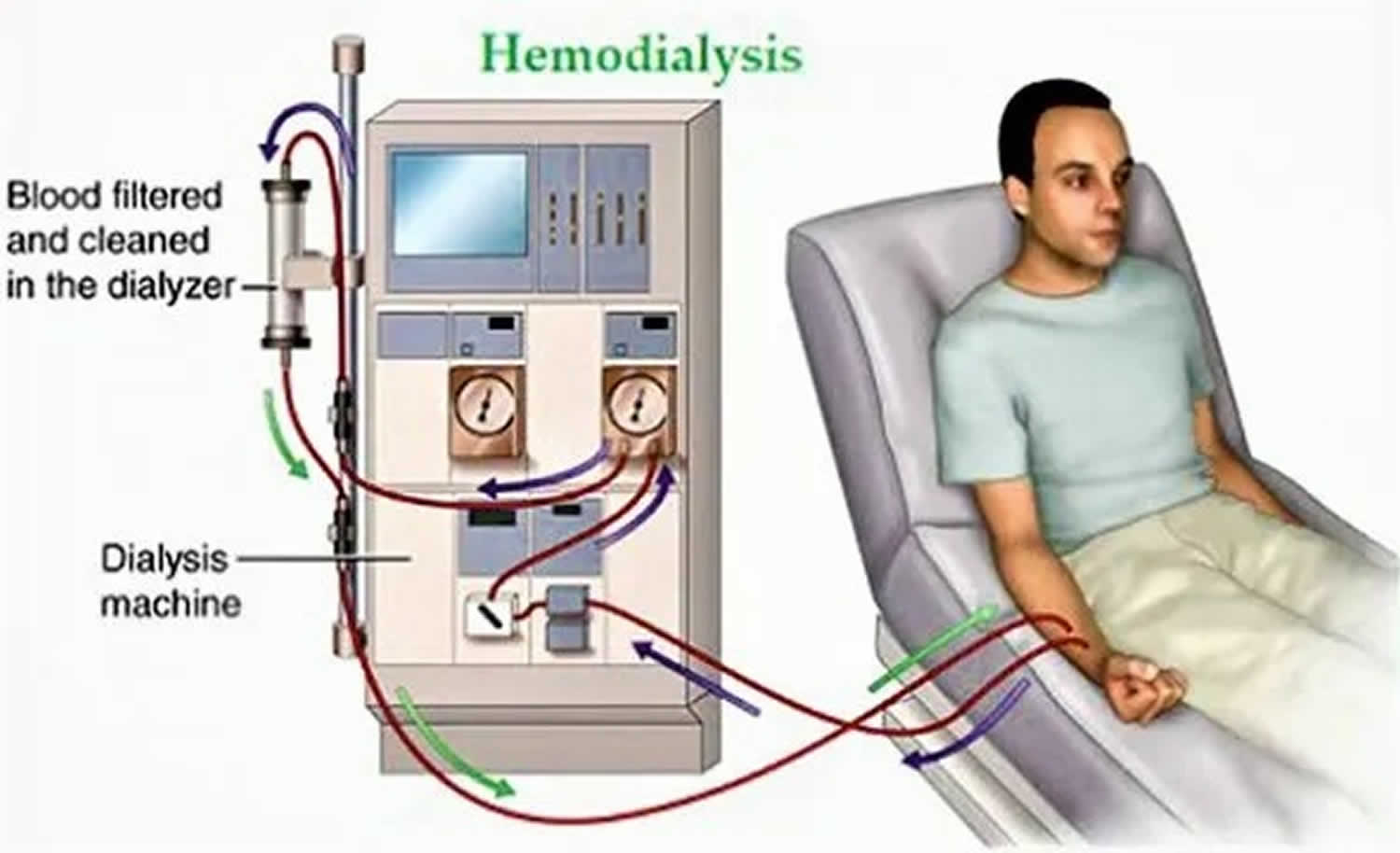
Figure 2. Peritoneal dialysis
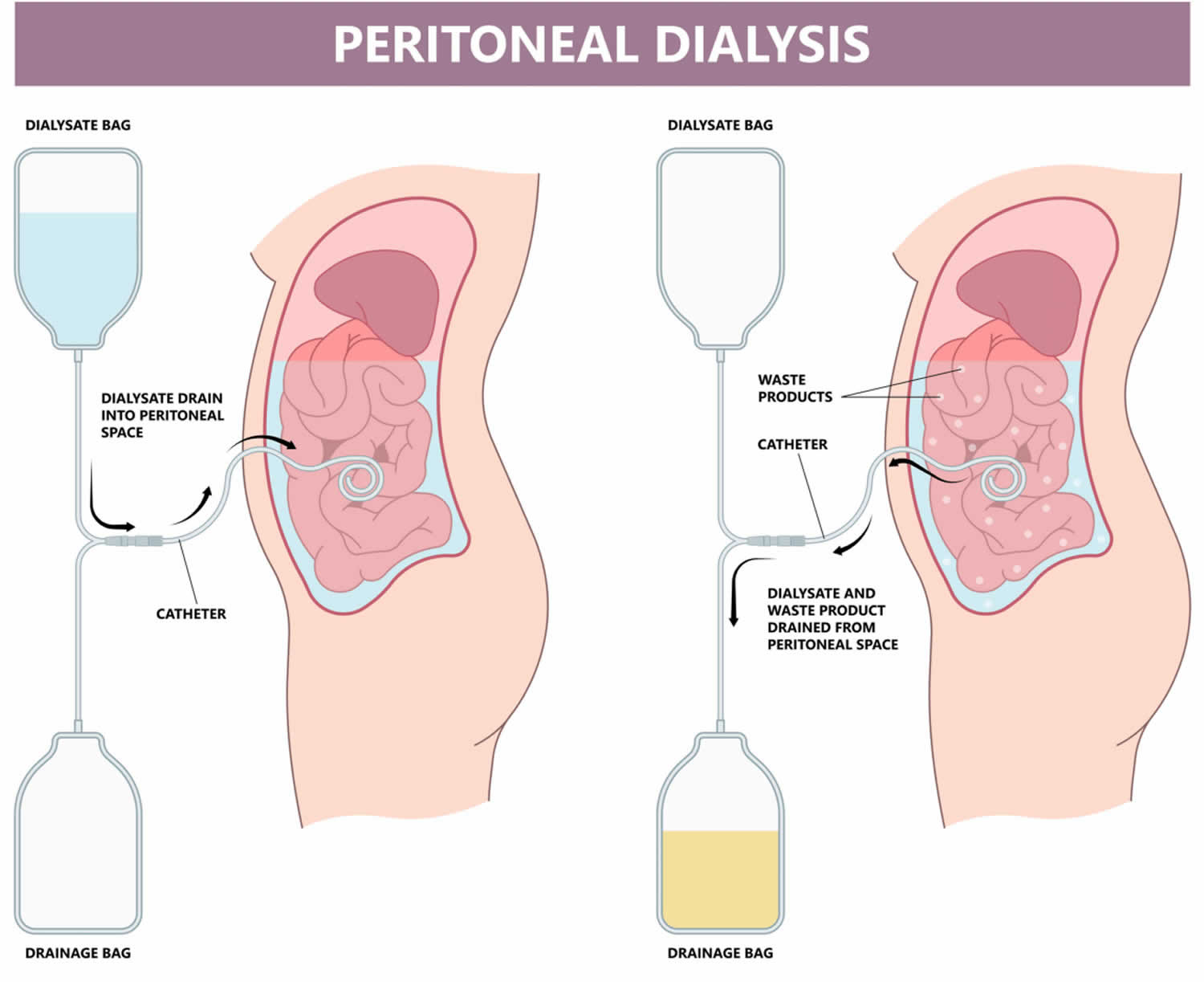
Table 1. Hemodialysis at a dialysis center or at home advantages and disadvantages
| Dialysis Center and Home Hemodialysis Comparison Chart | ||
|---|---|---|
| Dialysis center | Home | |
| Schedule | Three treatments a week for about 4 hours. Monday, Wednesday, Friday; or Tuesday, Thursday, Saturday. | Flexible. Three to seven short or long treatments per week at times that work best for you. |
| Availability | Available in most communities; may require travel in some rural areas. | Becoming more widely available as smaller equipment is developed. |
| Machine/supplies | The clinic has the machine and supplies. | The machine and 2- to 4-weeks’ worth of supplies are in the home. You may need minor changes in your home to connect the machine to electricity and water. |
| Training | The clinic teaches about treatments, diet, liquids, medicines, lab tests, etc. | You and a partner must attend 3 to 8 weeks of home hemodialysis training. |
| Diet and liquids | Strict limits on liquids, phosphorus, sodium, and potassium intake. | Fewer limits on liquids or diet, based on the amount of hemodialysis and lab tests. |
| Level of freedom | Less freedom on treatment days. May feel washed out and tired for hours after each treatment. | More freedom because you set the treatment schedule to meet the total amount prescribed. Work and travel are much easier. |
| Amount of work | Center staff members do hemodialysis tasks. They can teach you to do some tasks. | You and your partner must set up, run, and clean the machine; check vital signs; track the treatments and send in forms; and order supplies. |
| Payment | Medicare and most other health plans cover three hemodialysis treatments a week. | Medicare covers three hemodialysis treatments a week and may cover more for medical reasons; other health plans may cover all hemodialysis treatments. |
What is glomerular filtration rate (GFR)?
Each kidney has about one million tiny “tiny network of blood vessels that are the cleaning units of your kidney” called renal corpuscles or glomeruli. The glomerular filtration rate (GFR) shows how much blood is filtered per minute. In healthy people, this is between 85 and 135 milliliters per minute – based on a body surface area of 1.73 m² that is used for calculating the GFR.
However, it would be very difficult to measure the GFR directly. That’s why it’s usually estimated glomerular filtration rate (eGFR)– for instance, using the level of creatinine in the blood. Creatinine is a breakdown product of the muscles. The most commonly used formula for estimating the GFR uses serum creatinine, the person’s age, sex and race.
- eGFR (mL/min/1.73 m2) = 175 x (serum creatinine)–1.154 x (Age)–0.203 x (0.742 if female) x (1.212 if African American)
- End Stage Kidney failure (stage 5) is an eGFR < 15 ml/minute.
- eGFR is not reliable for patients with rapidly changing creatinine levels, extremes in muscle mass and body size, or altered diet patterns.
- For a free Glomerular Filtration Rate (GFR) Calculators please go here: https://www.niddk.nih.gov/health-information/professionals/clinical-tools-patient-management/kidney-disease/laboratory-evaluation/glomerular-filtration-rate-calculators/recommended
What is conservative management in kidney failure?
Conservative management for kidney failure means that your health care team continues your care without dialysis or a kidney transplant 3. The focus of care is on your quality of life and symptom control. The decision to start dialysis is yours. For most people, dialysis may extend and improve quality of life. For others who have serious conditions in addition to kidney failure, dialysis may seem like a burden that only prolongs suffering 3.
You have the right to decide how your kidney failure will be treated 3. You may want to speak with your family, doctor, counselor, or renal social worker who helps people with kidney disease to help you make this decision.
If you decide not to begin dialysis treatments, you may live for a few weeks or for several months, depending on your health and your remaining kidney function. Many of the complications of kidney failure can be treated with medicines, but only dialysis or kidney transplant can filter wastes from your blood 3. As your kidney function declines, you may want to consider adding hospice, or end-of-life care. You can have hospice care in a facility or at home. The hospice program is designed to meet end-of-life physical and emotional needs. Hospice care focuses on relieving pain and other symptoms.
Whether or not you choose to use hospice, your doctor can give you medicines to make you more comfortable. Your doctor can also give you medicines to treat the problems of kidney failure, such as anemia or weak bones. You may restart dialysis treatment if you change your mind.
What are the pros and cons of conservative management?
The pros and cons of conservative management depend on your current health status. Weigh the pros and cons with the help of your doctor.
Does dialysis cure kidney failure?
No. Even when very well done, dialysis only replaces part of your kidney function. Hemodialysis and peritoneal dialysis allow people with kidney failure to feel better and continue doing the things they enjoy, but neither replaces all of the jobs that healthy kidneys do. Over the years, kidney disease can cause other problems, such as heart disease, bone disease, arthritis, nerve damage, infertility, and malnutrition. These problems won’t go away with dialysis; however, doctors now have new and better ways to prevent or treat them. You should discuss these problems and their treatments with your doctor.
Can hemodialysis do everything my kidneys once did?
No. Hemodialysis can replace part, but not all, of your kidney function. Dialysis will help improve your energy level, and changes you make to your diet can help you feel better. Limiting how much water and other liquid you drink and take in through foods can help keep too much fluid from building up in your body between treatments. Medicines also help you maintain your health while on dialysis.
When do I have to start dialysis?
For most people, the need for dialysis comes on slowly. Symptoms, such as losing your desire to eat and losing muscle, may begin so slowly that you don’t notice them. Many people start dialysis when their kidney function (glomerular filtration rate [GFR]) is between 5 and 10. When kidney function is this low, you may have symptoms from kidney failure and starting dialysis may help relieve them. Starting dialysis can help you regain your appetite and maintain your strength, which is harder to rebuild than it is to retain. Your kidney doctor can help you decide the best time to begin treatment.
What are the pros and cons of having hemodialysis at home?
Home hemodialysis lets you have longer or more frequent dialysis, which comes closer to replacing the work healthy kidneys do, usually three to seven times per week, and with treatment sessions that last between 2 and 10 hours 1. Machines for home use are small enough to sit on an end table 1. If you choose to have your hemodialysis at home, you’ll still see your doctor once per month.
Flexible schedule
You can choose a schedule that fits the way you live. You can use 1:
- Standard home hemodialysis: 3 times a week or every other day for 3 to 5 hours.
- Short daily hemodialysis: 5 to 7 days per week for 2 to 4 hours at a time.
- Nightly home hemodialysis: 3 to 6 times per week while you sleep.
Your doctor will decide how many treatments you need each week for daily or nightly home hemodialysis.
More dialysis filters your blood more thoroughly
Compared with a standard hemodialysis schedule, daily or nightly home hemodialysis will let you 1:
- Eat and drink more normally
- Take fewer blood pressure medicines
Healthy kidneys work 24 hours a day, 7 days a week. Getting more hemodialysis feels more like having healthy kidneys and lowers your chances for problems that are common with a standard hemodialysis schedule, such as 1:
- Painful muscle cramps from removing too much fluid too quickly.
- High blood pressure, which can cause a headache or, in rare cases, a stroke.
- Low blood pressure, which can make you faint, feel sick to your stomach, or be more likely to fall.
- High phosphate levels, which can weaken bones and make your skin itch.
Better quality of life
Standard hemodialysis can make you feel tired or washed out for several hours after each treatment. People who have switched from standard hemodialysis to longer or more frequent hemodialysis report they feel better, with more energy, less nausea, and better sleep. They also may report a better quality of life 4.
Training for home hemodialysis
Most dialysis centers require that you have a trained partner in your home during hemodialysis treatments, so you must ask a family member or friend to go through the training with you 1. The clinic’s home-training nurse will teach you important safety skills.
During training, you and your care partner will learn to 1:
- Set up the machine
- Take steps to prevent infection
- Place needles into the vascular access
- Respond to any alarms from the machine
- Check your weight, temperature, blood pressure, and pulse
- Record treatment details for the clinic
- Clean the machine
- Throw out used supplies safely
- Track used supplies and order new ones
Training may take 4½ to 6 hours, 5 days a week, for 3 to 8 weeks. If you already know how to place the needles into your access, training may take less time.
The home-training nurse will make sure that you and your partner feel confident and may visit your home to help with your first at-home treatment. In addition to providing training and a hemodialysis machine that stays in your home, the dialysis center also provides 24-hour support if you have a question or problem. Some programs also monitor treatments over the internet.
Disadvantages of home hemodialysis
- Not all dialysis centers offer home hemodialysis training and support.
- You and a family member or friend will have to set aside several weeks for training.
- Helping with treatments may be stressful for your treatment partner.
- You need space at home to store the hemodialysis machine and supplies.
You’ll need to learn to put dialysis needles into your vascular access. - Medicare and private insurance companies may limit the number of home hemodialysis treatments they will pay for. Few people can afford the costs for additional treatments.
What are the pros and cons of having hemodialysis at dialysis center?
Most people go to a dialysis center for treatment. At the dialysis center, doctors and nurses set up and help you connect to the dialysis machine. A team of health care workers will be available to help you. You will continue to see your doctor. Other team members may include nurses, health care technicians, a dietitian, and a social worker.
Set schedule
You’ll have a fixed time slot for your treatments, usually three times per week: Monday, Wednesday, and Friday; or Tuesday, Thursday, and Saturday. Each dialysis session lasts about 4 hours. When choosing a dialysis schedule, think about your work and child care or other caregiving duties.
Nighttime option
Some dialysis centers offer nighttime treatments. These treatments occur at the dialysis center 3 nights a week while you sleep, which takes longer. Getting longer overnight dialysis treatments means 1:
- Your days are free.
- You have fewer diet changes.
- Your liquid allowance (how much liquid you can drink) is closer to normal.
- You may have a better quality of life than with a standard hemodialysis schedule. Longer treatment sessions may reduce your symptoms.
Disadvantages of dialysis center
- The center arranges treatments, so your schedule is less flexible.
- You must travel to the center for treatment.
- A longer time between treatments means you will have the strictest limits on diet and liquids—because wastes and extra fluid can build up in your body. Having too much fluid in your blood can raise blood pressure and stress your heart. Removing too much fluid too fast during standard hemodialysis also can stress the heart.
- You may have more “ups and downs” in how you feel from day to day because of the longer time between treatments.
- Feeling better after a treatment may take a few hours.
How do I find a dialysis center?
Your doctor, nurse, or social worker can help you find a dialysis center that’s convenient for you. Under Medicare rules, you have the right to choose the dialysis center where you’ll receive treatment. You may want to use Dialysis Facility Compare, which rates all dialysis centers according to quality. Your doctor will give your medical information to the dialysis center you choose.
Most large cities have more than one dialysis center to choose from. You can visit the centers to see which one best fits your needs. For example, you can ask about a center’s rules for laptop and cellphone use, as well as for having visitors. You may want the center to be close to your home to save travel time. If you live in a rural area, the closest dialysis center may be far from your home. If you’d have a hard time getting to the dialysis center, you may want to consider home dialysis treatments such as home hemodialysis or peritoneal dialysis.
What are the types of peritoneal dialysis?
You can choose the type of peritoneal dialysis that best fits your life:
- Continuous ambulatory peritoneal dialysis (CAPD). With continuous ambulatory peritoneal dialysis (CAPD) an exchange takes about 30 to 40 minutes, and most people need to do four exchanges per day. You sleep with solution in your belly at night.
- Automated peritoneal dialysis. Automated peritoneal dialysis uses a machine called a cycler to do three to five exchanges per night while you sleep. You may have to do one exchange during the day without the machine.
The main differences between the two types of peritoneal dialysis are:
- the schedule of exchanges
- one uses a machine and the other is done by hand
If one type of peritoneal dialysis doesn’t suit you, talk with your doctor about trying the other type.
You may need a combination of continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis if you weigh more than 175 pounds or if your peritoneum filters wastes slowly 5. For example, some people use a cycler (automated peritoneal dialysis machine) at night and perform one exchange during the day. Others do four exchanges during the day and use a minicycler to perform one or more exchanges during the night. You’ll work with your doctor to find the best schedule for you.
What are the pros and cons of peritoneal dialysis?
With either continuous ambulatory peritoneal dialysis (CAPD) or automated peritoneal dialysis, you gain a sense of control over your treatments and don’t need the help of a partner. After you’re trained, you can do continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis by yourself. With peritoneal dialysis, you’ll have boxes of dialysis solution taking up space in your home.
Continuous ambulatory peritoneal dialysis (CAPD) pros
- You don’t need a machine to do continuous ambulatory peritoneal dialysis (CAPD).
- You can do continuous ambulatory peritoneal dialysis (CAPD) at the times you choose, as long as you complete the required number of exchanges each day.
- You can do continuous ambulatory peritoneal dialysis (CAPD) in many locations.
- You can travel as long as you bring dialysis supplies with you or have them delivered to where you’re going.
Continuous ambulatory peritoneal dialysis (CAPD) cons
- Continuous ambulatory peritoneal dialysis (CAPD) can disrupt your daily routine.
- Continuous ambulatory peritoneal dialysis (CAPD) is a continuous treatment, and you need to do all exchanges 7 days a week.
Automated peritoneal dialysis pros
- You can do exchanges at night while you sleep.
- You may not have to perform exchanges during the day.
- You can travel as long as you bring dialysis supplies with you or have them delivered to where you’re going.
Automated peritoneal dialysis cons
- You need a machine. If you travel, you may have to carry your cycler with you.
- Your connection to the cycler limits your movement at night.
How is kidney transplant done?
Kidney transplant is surgery to place a healthy donor kidney into your body. A working, transplanted kidney does a better job filtering wastes and keeping you healthy than dialysis, but it still isn’t a cure. When you have a kidney transplant, surgeons usually leave your old kidneys in place and connect the donated kidney to an artery and a vein in your groin. The surgeon also transplants the ureter from the donor to let urine flow from your new kidney into your bladder. The transplanted kidney takes over the job of filtering your blood.
Your body normally attacks anything it sees as foreign, so to keep your body from attacking the donor kidney, you will need to take immunosuppressants also called anti-rejection medicines. Like all strong medicines, anti-rejection medicines have side effects.
A transplant center can place you on the waiting list for a donor kidney if you have permanent kidney damage and your kidney function is 20 or less. While you’re waiting for a kidney transplant, you may need to start dialysis.
What are the side effects of anti-rejection medicines?
Some anti-rejection medicines (immunosuppressants) may change your appearance. Your face may get fuller, you may gain weight, or you may develop acne or facial hair. Not all people have these side effects.
Anti-rejection medicines (immunosuppressants) weaken your immune system, which can lead to infections. In some people over long periods of time, a weakened immune system can increase their risk of developing cancer. Some anti-rejection medicines cause cataracts, diabetes, extra stomach acid, high blood pressure, and bone disease.
When used over time, anti-rejection medicines (immunosuppressants) may also cause liver or kidney damage in some people. Your transplant team will order regular tests to monitor the levels of anti-rejection medicines in your blood and to measure your liver and kidney function.
Paying for medicines
Drug discount programs may help you find the medicines you need for free or at a lower cost. Try these resources:
- BenefitsCheckUp. Seniors with limited incomes can search for help with medicines, health care, rent, and other needs through this service of the National Council on Aging.
- Blink Health. Blink Health has negotiated prices for 15,000 medicines that may cost less than you’d pay with your insurance online or at your local pharmacy.
- GoodRx. GoodRx compares prices and provides coupons for FDA-approved drugs at over 70,000 pharmacies. Your medicines may cost less with the coupon than with your insurance.
- Medicine Assistance Tool. Some drug manufacturers have programs that provide free or low-cost drugs to people who meet their guidelines.
- NeedyMeds. This organization lists programs that help pay for medicines and supplies. You can search by medicine or manufacturer name.
- RxAssist. An online resource that lists drug company assistance programs, state programs, discount drug cards, copay help, and more.
- Rx Outreach. A nonprofit, mail-order pharmacy that provides affordable medicine to people in need through its website or by phone at 1-888-RXO-1234 (1-888-796-1234).
- State Pharmaceutical Assistance Program. Some states have programs that limit drug costs for people with limited income or who are elderly.
How do I pay for my kidney transplant?
Medicare, the Federal Government health insurance program, will pay for your kidney transplant and care for 3 years after the transplant. Medicare will also pay for your donor’s surgery and his or her care.
How can I get Medicare for kidney failure?
Visit Medicare.gov (https://www.medicare.gov/basics/end-stage-renal-disease) and search on “I have end-stage renal disease” to find information about whether you qualify for Medicare and how to sign up.
What health plans does Medicare offer?
Medicare has two main ways to get coverage: Original Medicare, which includes Part A and Part B, or a Medicare Advantage Plan, also called Part C. You can also choose to have prescription drug coverage through Medicare Part D.
Most people with kidney failure are not allowed to join a Medicare Advantage plan. However, beginning in 2021, the 21st Century Cures Act will allow people with ESRD to choose a Medicare Advantage plan instead of Original Medicare. Medicare Advantage plans may limit where you get care, but they cap out-of-pocket costs. With Original Medicare, there is no cap on out-of-pocket costs, but you can get care anywhere that Medicare is accepted.
You can find out more about the Medicare health plans by visiting Medicare.gov and searching on “ESRD,” then clicking on “Signing up for Medicare if you have ESRD.”
Other Medicare health plans are available that have special rules or are for specific groups of people. Medicare offers more information about these alternate plans online.
What types of private health insurance can help with kidney failure treatment costs?
Some people with kidney failure use private health insurance to help pay for their health care
- Group health insurance. People buy this kind of health insurance through their employer, union, or a family member’s employer or union. Group health plans pay for the first 30 months from the time you become eligible for Medicare for kidney failure. After that, a group plan can work with Medicare to help pay for costs that aren’t paid for by Medicare, such as copays, coinsurance, and deductibles. If you have or are eligible for group health insurance, you can contact the benefits administrator at the company or union that provides your insurance to find out what the plan covers and how it works with Medicare.
- Individual health insurance. People buy this coverage for themselves and their families.
- The Health Insurance Marketplace offers health insurance plans to people who are legally present in the United States and who don’t have any other health insurance options. You can find, compare, and buy individual insurance plans in most states—or connect to your state’s insurance marketplace at HealthCare.gov. You cannot enroll in a Health Insurance Marketplace plan if you already have Medicare. Some people choose to keep their Marketplace plan instead of enrolling in Medicare. You may pay more for Medicare later if you don’t enroll in Medicare when you first become eligible.
- Insurance companies, agents, brokers, and online insurance stores are other ways to find and buy individual health insurance plans. Learn how to find a trustworthy insurance company at USA.gov.
- Medigap also called Medicare Supplemental Insurance. People buy this extra health insurance from a private company. Medigap plans help cover some costs that are not covered by Original Medicare, such as copays, coinsurance, and deductibles. If you’re 65, federal law protects your right to buy a Medigap plan. If you’re under 65 and are on dialysis, you may or may not be able to buy a Medigap policy from a licensed insurance company in your home state. Learn more online about Medigap rules, benefits, deadlines, and premiums here (https://www.medicare.gov/health-drug-plans/medigap).
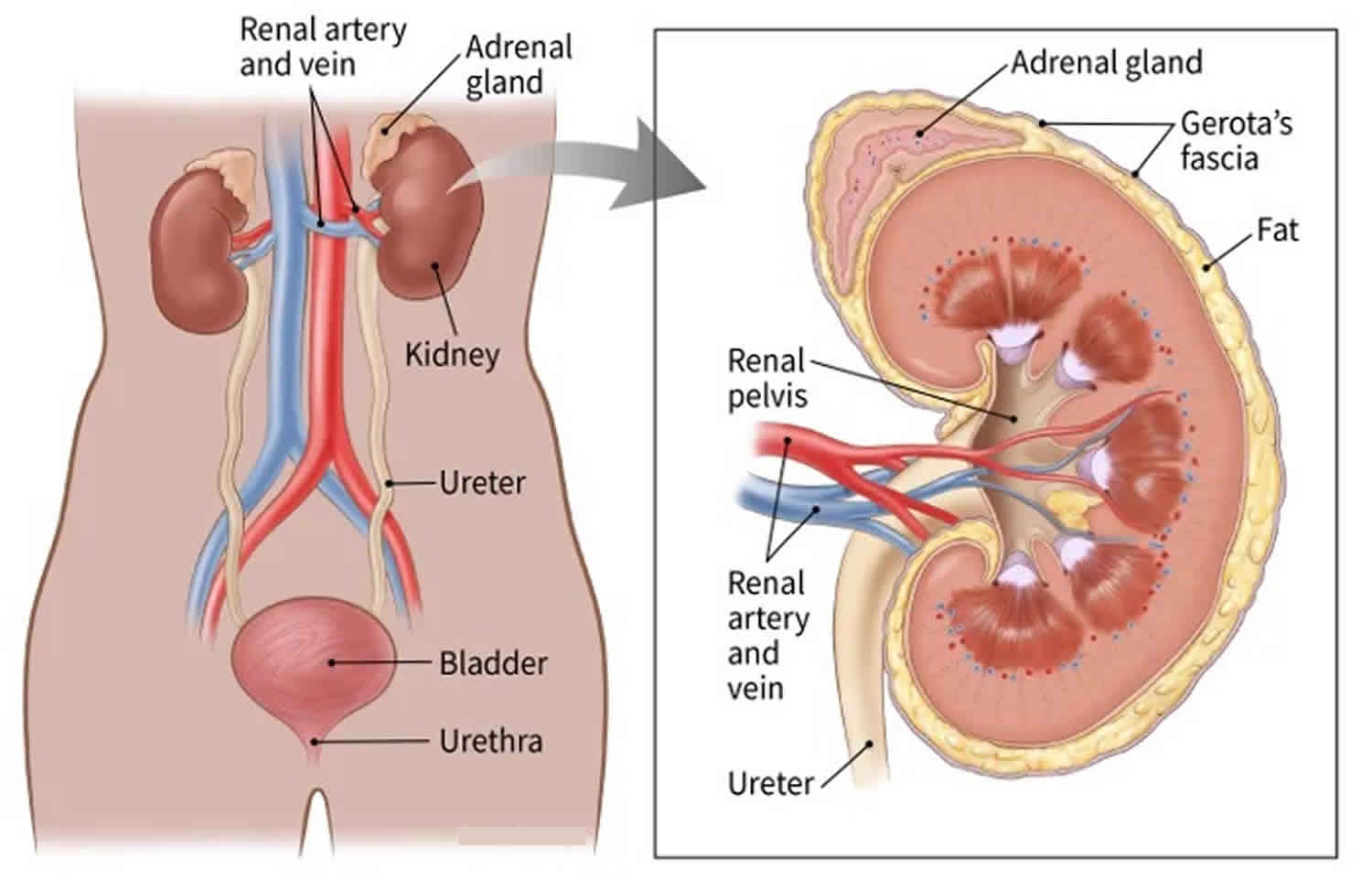
Kidneys
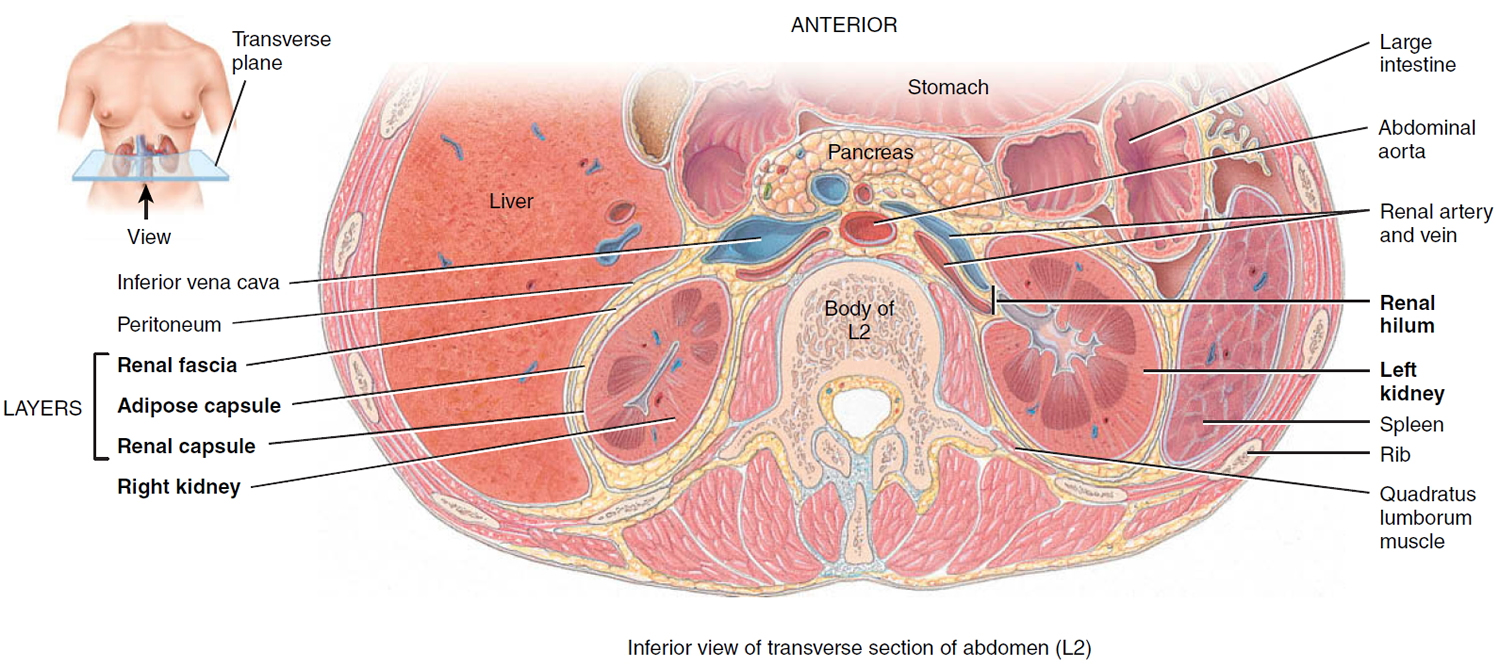
The kidneys are a pair of reddish, kidney bean–shaped organs, each about the size of a fist that are located just above your waist between the peritoneum and the posterior wall of the abdomen. Because their position is posterior to the peritoneum of the abdominal cavity, the organs are said to be retroperitoneal. The kidneys are located between the levels of the last thoracic vertebrae T12 and third lumbar (L3) vertebrae, a position where they are partially protected by ribs 11 and 12. If these lower ribs are fractured, they can puncture the kidneys and cause significant, even life-threatening damage. The right kidney is slightly lower than the left (see Figure 1) because the liver occupies considerable space on the right side superior to the kidney.
A typical adult kidney is 10–12 cm (4–5 in.) long, 5–7 cm (2–3 in.) wide, and 3 cm (1 in.) thick—about the size of a bar of bath soap—and weighs about 135–150 g (4.5–5 oz). The concave medial border of each kidney faces the vertebral column (see Figure 2). Near the center of the concave border is an indentation called the renal hilum, through which the ureter emerges from the kidney along with blood vessels, lymphatic vessels, and nerves.
Three layers of tissue surround each kidney. The deep layer, the renal capsule, is a smooth, transparent sheet of dense irregular connective tissue that is continuous with the outer coat of the ureter. It serves as a barrier against trauma and helps maintain the shape of the kidney. The middle layer, the adipose capsule, is a mass of fatty tissue surrounding the renal capsule. It also protects the kidney from trauma and holds it firmly in place within the abdominal cavity. The superficial layer, the renal fascia, is another thin layer of dense irregular connective tissue that anchors the kidney to the surrounding structures and to the abdominal wall. On the anterior surface of the kidneys, the renal fascia is deep to the peritoneum.
Figure 3. Kidney location
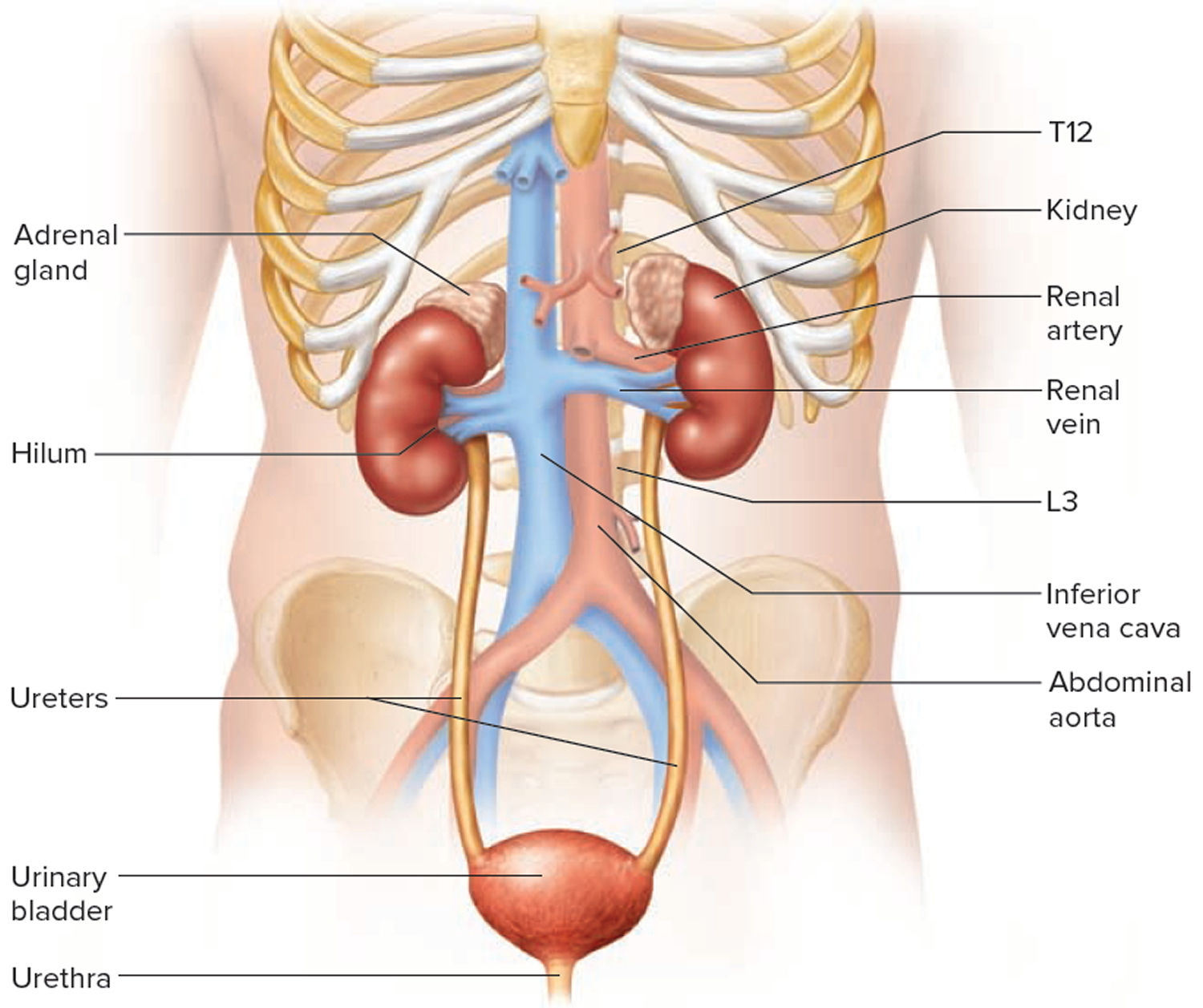
Figure 4. Kidney location (transverse section)
Kidney anatomy
A frontal section through the kidney reveals two distinct regions: a superficial, light red region called the renal cortex and a deep, darker reddish-brown inner region called the renal medulla (medulla = inner portion). The renal medulla consists of several cone-shaped renal pyramids. The base (wider end) of each pyramid faces the renal cortex, and its apex (narrower end), called a renal papilla, points toward the renal hilum. The renal cortex is the smooth-textured area extending from the renal capsule to the bases of the renal pyramids and into the spaces between them. It is divided into an outer cortical zone and an inner juxtamedullary zone. Those portions of the renal cortex that extend between renal pyramids are called renal columns.
Together, the renal cortex and renal pyramids of the renal medulla constitute the parenchyma or functional portion of the kidney. Within the parenchyma are the functional units of the kidney—about 1 million microscopic structures called nephrons. Filtrate (filtered fluid) formed by the nephrons drains into large papillary ducts, which extend through the renal papillae of the pyramids. The papillary ducts drain into cuplike structures called minor and major calyces. Each kidney has 8 to 18 minor calyces and 2 or 3 major calyces. A minor calyx receives filtrate from the papillary ducts of one renal papilla and delivers it to a major calyx. Once the filtrate enters the calyces it becomes urine because no further reabsorption can occur. The reason for this is that the simple epithelium of the nephron and ducts becomes transitional epithelium in the calyces. From the major calyces, urine drains into a single large cavity called the renal pelvis and then out through the ureter to the urinary bladder.
The hilum expands into a cavity within the kidney called the renal sinus, which contains part of the renal pelvis, the calyces, and branches of the renal blood vessels and nerves. Adipose tissue helps stabilize the position of these structures in the renal sinus.
Figure 5. Kidney anatomy
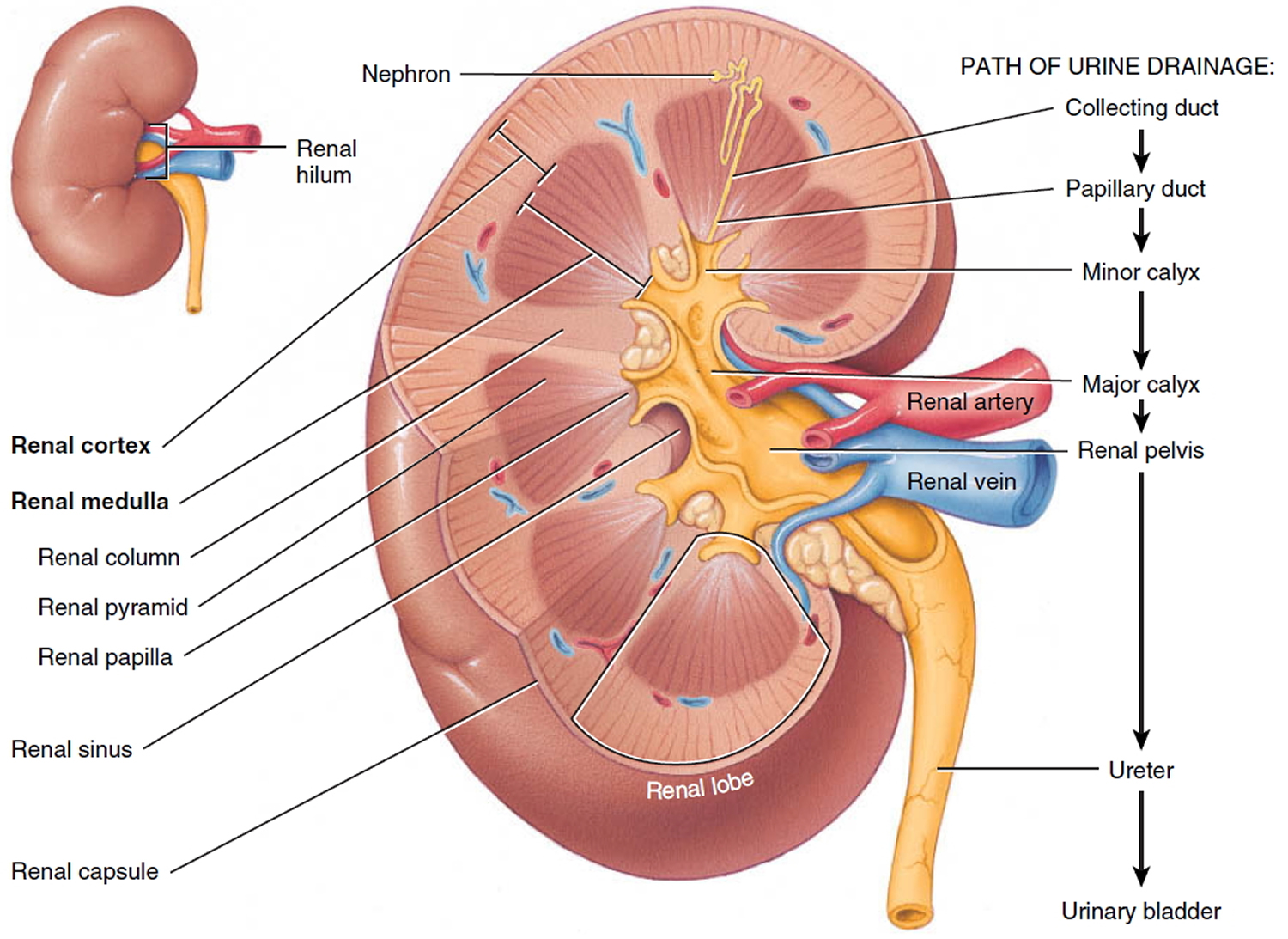
Figure 6. Kidney structure
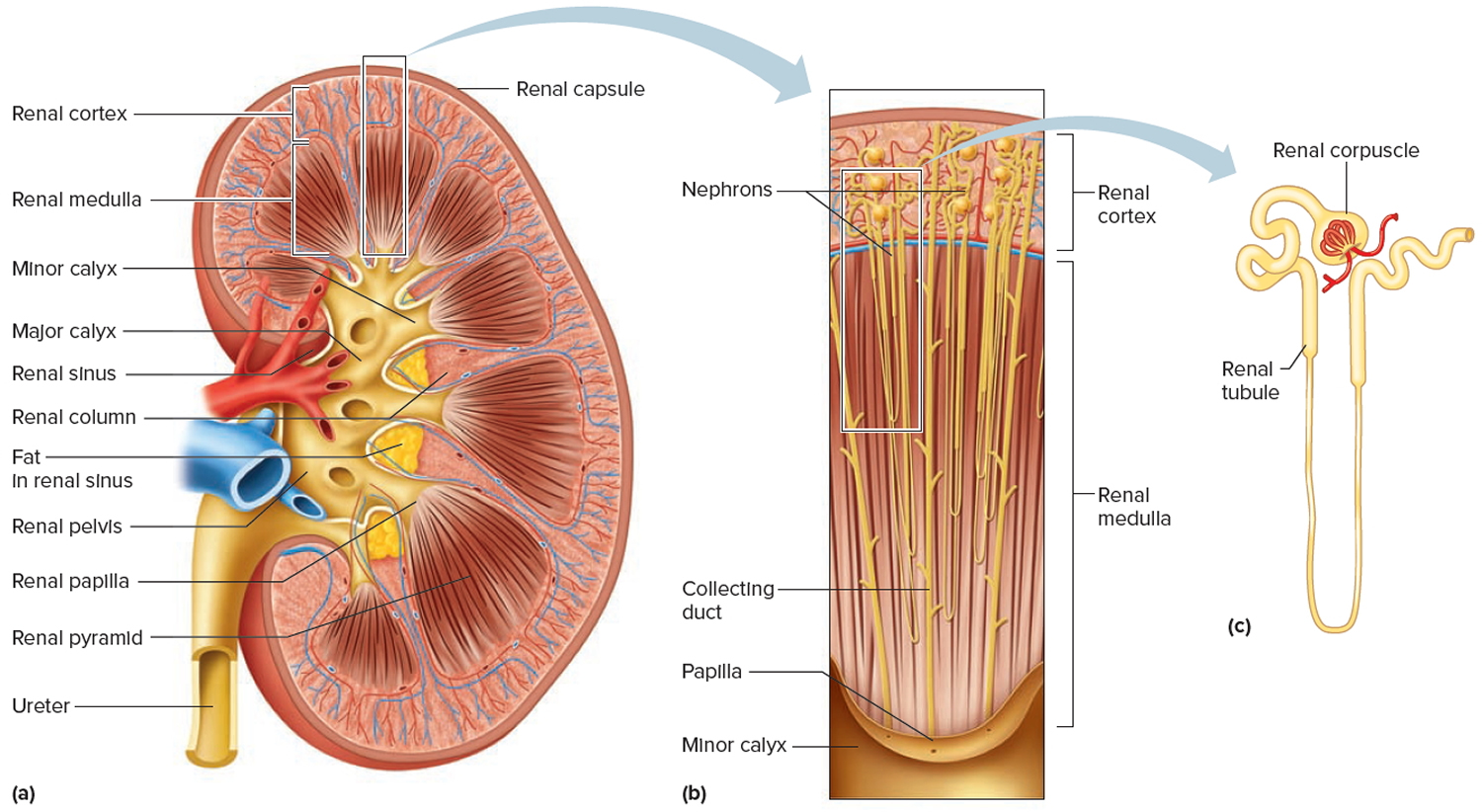
Figure 7. Microcirculation of the kidney
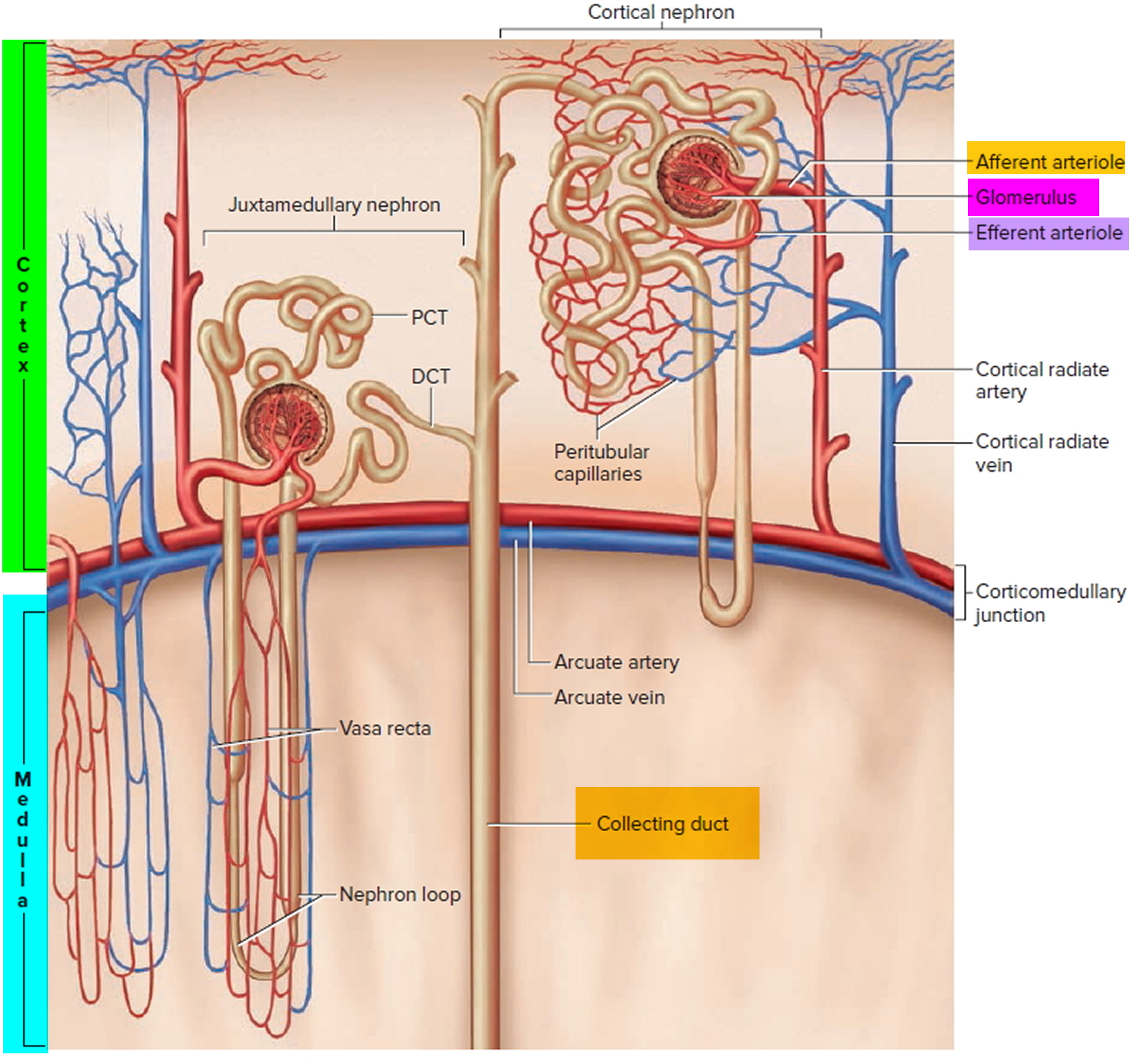
Note: DCT = distal convoluted tubule; PCT = proximal convoluted tubule
Kidney function
The primary function of the kidneys is to help maintain homeostasis by regulating the composition (including pH) and the volume of the extracellular fluid. The kidneys accomplish this by removing metabolic wastes from the blood and combining the wastes with excess water and electrolytes to form urine, which they then excrete.
Kidneys maintain homeostasis
- Regulatory function
- Control composition and volume of blood
- Maintain stable concentrations of inorganic anions such as sodium (Na), potassium (K), and calcium (Ca)
- Maintain acid-base balance
- Excretory function
- Produce urine
- Remove metabolic wastes including nitrogenous waste
Kidneys blood filtration and urine production
- Filtration: Glomeruli generate ultrafiltrate of the plasma.
- Reabsorption: Tubules selectively reabsorb substances from the ultrafiltrate.
- Secretion: Tubules secrete substances into the urine.
Examples:
- Potassium is reabsorbed from and secreted into the urine by the tubules.
- Sodium is generally reabsorbed by the tubules.
- Organic acids are secreted into the urine.
- Albumin is generally reabsorbed within the tubules.
Damaged kidneys allow albumin to cross the filtration barrier into the urine
- Increased glomerular permeability allows albumin (and other proteins) to cross the glomerulus into the urine.
- Higher levels of protein within the tubule may exacerbate kidney damage by exceeding tubules’ ability to reabsorb the proteins.
- An elevated urine albumin-to-creatinine ratio (UACR) is used to identify damaged kidneys. Urine albumin-to-creatinine ratio (UACR) results are used for screening, diagnosing, and treating chronic kidney disease. Forty percent of people are identified with chronic kidney disease on the basis of urine albumin alone.
The kidneys have several other important functions:
- Produce Erythropoietin which stimulates marrow production of red blood cells.
- Playing a role in the activation of vitamin D [activate 25(OH)D to 1,25 (OH)2D (active vitamin D)].
- Helping to maintain blood volume and blood pressure by secreting the enzyme Renin.
- Metabolize drugs and endogenous substances (e.g., insulin).
In patients with kidney failure:
- Kidneys cannot maintain homeostasis.
- Kidney failure is associated with fluid, electrolyte, and hormonal imbalances and metabolic abnormalities.
- End stage kidney failure means the patient is on dialysis or has a kidney transplant.
Stages of kidney disease
There are 5 stages of kidney disease. To determine what stage you have, your doctor performs a blood test to check your glomerular filtration rate (GFR) or estimated glomerular filtration rate (eGFR). The GFR measures how much blood the kidneys filter each minute, recorded as milliliters per minute (mL/min). As the GFR declines, so does your kidney function.
When your kidneys no longer work at a level that’s necessary to keep you alive, you have end-stage renal disease. End-stage renal disease usually occurs when kidney function is less than 15% of typical kidney function.
As a part of kidney disease staging, your doctor also might test whether you have protein in your urine (proteinuria).
Each chronic kidney disease patient is classified into one of the following 5 stages of chronic kidney disease based on their estimated glomerular filtration rate (eGFR) and the level of proteinuria, because management and prognosis varies according to the progression of damage.
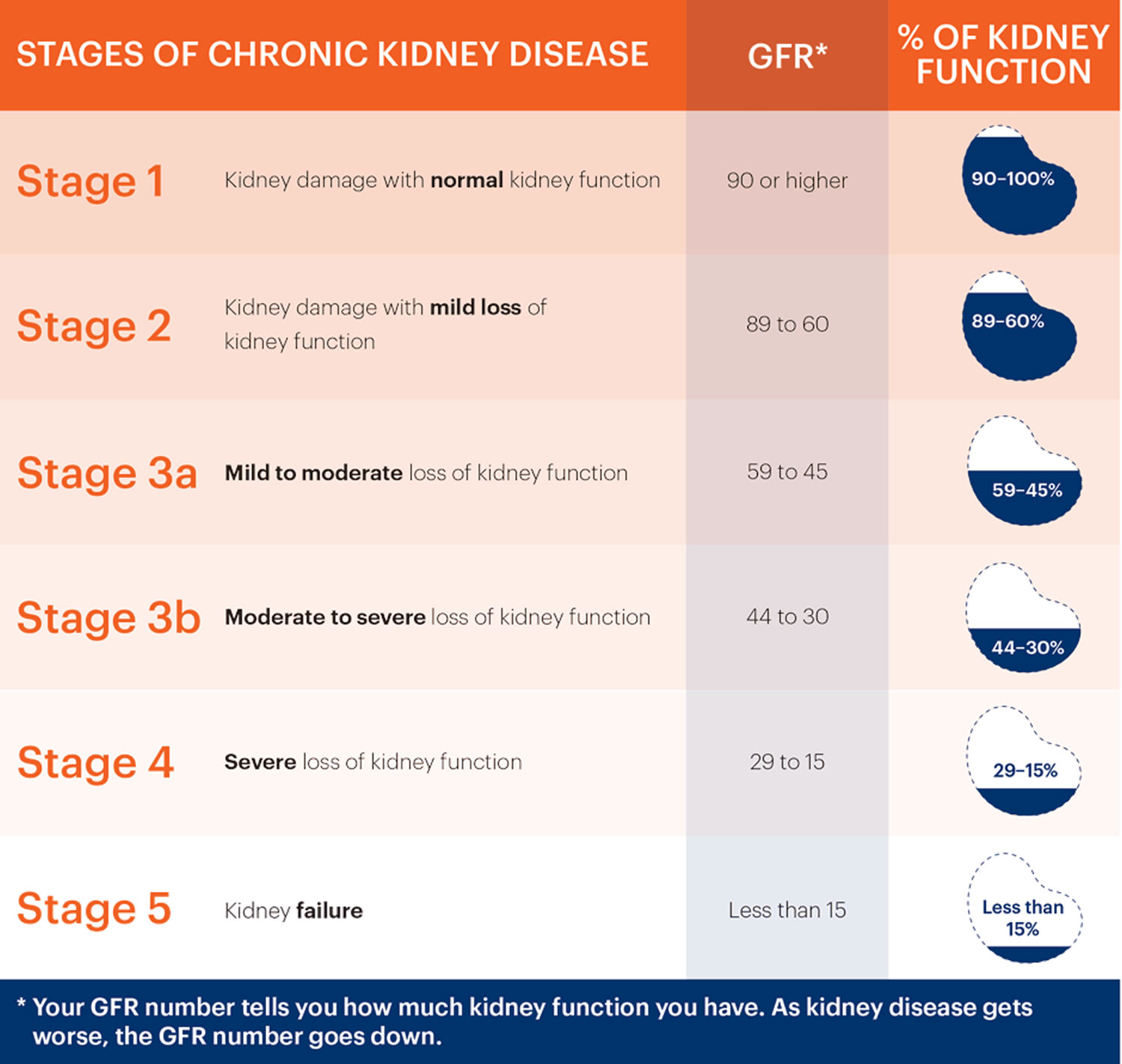
- Stage 1: Kidney damage with normal or increased eGFR (above 90 mL/min/1.73 m²), but other tests have detected signs of kidney damage
- Stage 2: Mild reduction in eGFR (60-89 mL/min/1.73 m²), with other signs of kidney damage
- Stage 3: Moderate reduction in eGFR (30-59 mL/min/1.73 m²)
- Stage 3a (G3a) – an eGFR of 45 to 59ml/min/1.73 m²
- Stage 3b (G3b) – an eGFR of 30 to 44ml/min/1.73 m²
- Stage 4: Severe reduction in eGFR (15-29 mL/min/1.73 m²)
- Stage 5 (End Stage Kidney Disease or ESRD): Kidney failure (eGFR less than 15 mL/min/1.73 m²), meaning the kidneys have lost almost all of their function and require dialysis
Alongside your glomerular filtration rate (GFR), your urine albumin:creatinine ratio (ACR) can help give a more accurate picture of how well your kidneys are working.
Your albumin:creatinine ratio (ACR) result is given as a stage from 1 to 3:
- A1 – an ACR of less than 3mg/mmol
- A2 – an ACR of 3 to 30mg/mmol
- A3 – an ACR of more than 30mg/mmol
For both glomerular filtration rate (GFR) and ACR, a higher stage indicates more severe kidney disease.
Figure 8. Chronic kidney disease stages
Kidney disease stage 1
Stage 1 kidney disease means you have a normal estimated glomerular filtration rate (eGFR) of 90 ml/min per 1.73m² or greater and mild damage to your kidneys. Your kidneys are still working well, so you may not have any symptoms, but you may have signs of kidney damage or physical damage to your kidneys. You may have other signs of kidney damage, such as protein in your urine (proteinuria) or blood in your urine (hematuria). The presence of protein alone means you are in Stage 1 kidney disease.
At stage 1 kidney disease, there is a lot you can do to help keep your kidneys working well for as long as possible. Here are some healthy life changes you can make:
- Eat a kidney-friendly diet. A dietitian is a nutrition expert who can look at results from your lab tests and help you plan healthy meals and snacks you’ll want to eat — your “kidney diet.”
- Be active for at least 30 minutes on most days of the week. This can be anything from walking or riding a bike to swimming or dancing.
- Keep a healthy weight. Talk with your doctor about what a healthy weight is for you.
- Quit smoking or using tobacco.
What are the symptoms of stage 1 kidney disease?
Most people with stage 1 kidney disease do not have any symptoms that affect their health, which is why many people do not know they have it. However, there are some signs of Stage 1 kidney disease people may notice themselves, or that doctors may notice when testing for kidney damage or other health conditions.
Signs and symptoms of stage 1 kidney disease include:
- High blood pressure
- Swelling in your hands or feet
- Urinary tract infections
- Protein in your urine
- Blood in your urine (also called hematuria)
- Kidney damage that shows up in an ultrasound, CT scan, MRI, or kidney biopsy
Stage 1 kidney disease treatment
At stage 1 kidney disease, doctors mostly focus on slowing down kidney damage and keeping your kidneys working well for as long as possible.
Doctors will work with you to:
- Control your blood sugar if you have diabetes.
- Keep your blood pressure in a healthy range (less than 120/80 mmHG, is best).
- Decide if you should start or stop any medicines to help protect your kidneys.
If you do not have a nephrologist (kidney doctor), talk to your regular doctor about finding one. You and your nephrologist can work together to make a treatment plan just for you.
Kidney disease stage 2
Stage 2 kidney disease means your eGFR has gone down to between 60 and 89 ml/min/1.73m², and you have mild damage to your kidneys. Most of the time, your kidneys are still working well, so you may not have any symptoms. You may have other signs of kidney damage, such as protein in your urine or physical damage.
Many people with Stage 2 kidney disease do not have any symptoms. However, if you have a family history of kidney disease, or a health condition that can damage your kidneys, such as diabetes or high blood pressure, your doctor may test the health of your kidneys.
To find out what stage of kidney disease you are in and what caused your kidney disease, your doctor will do tests, such as:
- GFR blood tests (a blood test)
- Blood pressure checks
- Urine tests
- Imaging tests to take detailed pictures of the inside of your body, such as ultrasound, CT scan or MRI
- Kidney biopsy (taking out part of your kidney tissue to look at it under a microscope)
- Genetic testing (if doctors suspect a rare disease or one that runs in your family)
In Stage 2 kidney disease, making healthy choices to slow down the damage to your kidneys is important.
Here are some tips you can use:
- Eat a kidney-friendly diet. A dietitian is a nutrition expert who can look at results from your lab tests and help you plan healthy meals and snacks you’ll want to eat: your “kidney diet.”
- Be active for at least 30 minutes on most days of the week. This can be anything from walking or riding a bike to swimming or dancing.
- Keep a healthy weight. Talk with your doctor about what a healthy weight is for you.
- Quit smoking or using tobacco.
What are the symptoms of stage 2 kidney disease?
Often, symptoms of kidney disease do not start until stage 3 kidney disease, which is why many people with stage 2 kidney disease might not know they have it. However, there are some signs of stage 2 kidney disease people may notice, or that doctors may notice when testing for kidney damage or other health conditions.
Signs and symptoms of stage 2 kidney disease include:
- Protein in your urine
- High blood pressure
- Swelling in your hands or feet
- Urinary tract infections
- Blood in your urine (hematuria)
- Kidney damage that shows up in an ultrasound, CT scan, MRI or kidney biopsy
Stage 2 kidney disease treatment
Your doctor will work with you to slow down kidney damage and to keep your kidneys working well for as long as possible.
Your doctor can help you:
- Control your blood sugar if you have diabetes.
- Keep your blood pressure in a healthy range (less than 120/80 mmHG, is best).
- Decide if you start or stop any medicines to help protect your kidneys.
If you do not have a nephrologist (kidney doctor), talk to your regular doctor about finding one. You and your nephrologist can work together to make a treatment plan just for you.
Kidney disease stage 3
Stage 3 kidney disease means you have an GFR between 30 and 59 ml/min/1.73m² and you have mild to moderate damage to your kidneys. Your kidneys do not work as well as they should to filter waste and extra fluid out of your blood. This waste can build up in your body and begin to cause other health problems, such as high blood pressure and bone disease. You may begin to have symptoms, such as feeling weak and tired or swelling in your hands or feet, but you do not need a dialysis or a kidney transplant..
Stage 3 kidney disease is split into two substages based on your GFR:
- Stage 3a means you have an eGFR between 45 and 59 ml/min/1.73m²
- Stage 3b means you have an eGFR between 30 and 44 ml/min/1.73m²
With treatment and healthy life changes, many people in Stage 3 do not move to Stage 4 or Stage 5.
To find out what stage of kidney disease you are in and find out what caused your kidney disease, your doctor will do tests, such as:
- GFR blood tests
- Urine tests
- Blood pressure checks
- Imaging tests to take detailed pictures of the inside of your body, such as ultrasound, CT scan or MRI
- Kidney biopsy (a procedure where doctors take a small piece of tissue from your kidneys to look at it under a microscope)
- Genetic testing (if doctors suspect a rare disease or one that runs in your family)
What are the symptoms of stage 3 kidney disease?
Some people with stage 3 kidney disease do not have any symptoms. But for many people with stage 3 kidney disease is when their kidney disease begins to affect their health, and they start to notice symptoms.
Symptoms of stage 3 kidney disease may include:
- Feeling weak and tired
- Swelling in your hands or feet
- Skin that feels dry or itchy
- Pain in your lower back
- Muscle cramps
- Trouble sleeping
- Restless leg syndrome (an uncomfortable feeling in your legs that makes it hard to sit still or fall asleep)
- Urinating more or less often than normal
- Urine that is foamy or darker in color than usual
Stage 3 kidney disease treatment
Doctors treat Stage 3 kidney disease with medicines that help with your symptoms and with other health problems kidney disease can cause, such as diabetes and high blood pressure.
These medicines include:
- Blood pressure medicines like ACE inhibitors and angiotensin receptor blockers (angiotensin 2 receptor antagonists) (even if you do not have high blood pressure, these medicines can help slow the damage to your kidneys to keep them working well as long as possible)
- Diabetes medicines to keep your blood sugar at a healthy level (even if you do not have diabetes)
- Calcium and vitamin D supplements to keep your bones strong
- Diuretics to help with swelling (these are medicines that help your kidneys get rid of salt and water and make you urinate more)
- Iron supplements to help with anemia (not enough red blood cells in your body)
You may also need to stop taking certain medicines that can worsen the damage to your kidneys, such as pain medicines called NSAIDs (nonsteroidal anti-inflammatory drugs) and some arthritis medicines. Tell your doctor about all the medicines you take even ones they did not prescribe.
How can I slow down the damage to my kidneys?
Healthy life changes can make a big difference in how you feel and can help keep your kidneys working well for as long as possible. Eating kidney-friendly foods in the right amounts is one of the best ways to slow the damage to your kidneys from kidney disease and to feel your best. A dietitian is a nutrition expert who can look at results from your lab tests and help you plan healthy meals and snacks you’ll want to eat: your “kidney diet.”
Here are other healthy changes that will help slow the damage to your kidneys:
- Be active for at least 30 minutes on most days of the week. This can be anything from walking or riding a bike to swimming or dancing.
- If you have diabetes, follow your treatment plan to keep your blood sugar within your target range.
- Quit smoking or using tobacco.
Kidney disease stage 4
Stage 4 kidney disease means you have an GFR between 15 and 29 ml/min/1.73m² and moderate to severe damage to your kidneys. Your kidneys do not work as well as they should to filter waste out of your blood. This waste can build up in your body and cause other health problems, such as high blood pressure, bone disease and heart disease. You will likely have symptoms such as swelling of your hands and feet and pain in your lower back.
Stage 4 kidney disease means that your kidneys are moderately or severely damaged and are not working as well as they should to filter waste from your blood. Waste products may build up in your blood and cause other health problems, such as:
- High blood pressure
- Anemia (not enough red blood cells in your body)
- Bone disease
- Heart disease
- High potassium
- High phosphorus
- Metabolic acidosis (a buildup of acid in your body)
Stage 4 kidney disease is the last stage before kidney failure. It is important to have regular visits with a nephrologist (kidney doctor) to take steps to slow kidney damage and plan ahead for possible treatments for kidney failure.
To find out what stage of kidney disease you are in and what caused your kidney disease, your doctor will do tests, such as:
- GFR blood tests
- Urine tests
- Blood pressure checks
- Imaging tests to take detailed pictures of the inside of your body, such as ultrasound, CT scan or MRI
- Kidney biopsy (a procedure where doctors take a small piece of tissue from your kidneys to look at it under a microscope)
- Genetic testing (if doctors suspect a rare disease or one that runs in your family)
What are the symptoms of stage 4 kidney disease?
Symptoms of Stage 4 kidney disease may include:
- Feeling weak and tired
- Swelling in your arms or legs
- Urinating more or less often than normal
- Pain in your lower back
- Muscle cramps
- Feeling sick to your stomach or throwing up
- Feeling less hungry than normal
Stage 4 kidney disease treatment
You will need to see a nephrologist (kidney doctor). Your nephrologist will treat Stage 4 kidney disease with medicines that help with your symptoms and other health problems that kidney disease can cause, such as diabetes and high blood pressure.
These medicines include:
- Blood pressure medicines like ACE inhibitors and angiotensin receptor blockers (angiotensin 2 receptor antagonists) (even if you do not have high blood pressure, these medicines can help slow the damage to your kidneys to keep them working well as long as possible)
- Diabetes medicines to keep your blood sugar at a healthy level (even if you do not have diabetes)
- Calcium and vitamin D supplements to keep your bones strong
- Diuretics to help with swelling (these are medicines that help your kidneys get rid of salt and water and make you urinate more)
- Erythropoiesis-stimulating agents or iron supplements to help with anemia (not enough red blood cells in your body)
Your doctor may tell you to stop taking medicines that can damage your kidneys, such as pain medicines called NSAIDs (nonsteroidal anti-inflammatory medicines).
Your nephrologist will decide if your kidneys are close to failure and if you need to start treatment. If you need treatment, they will talk with you about your choices, which include:
- Dialysis, which is a treatment to clean your blood when your kidneys are not able to. Learn more about the 2 types of dialysis.
- A kidney transplant, which is surgery to give you a kidney from someone else’s body. Learn more about kidney transplants.
How can I slow down the damage to my kidneys?
There is usually no cure for chronic kidney disease, and you usually cannot reverse the kidney damage you already have by the time you get to stage 4 kidney disease. However, you can take steps to slow down the damage to your kidneys and help you feel your best.
To slow down the damage to your kidneys, your doctor will recommend that you:
- Have visits with a nephrologist about every three months.
- Meet with a dietitian to help you create and follow a kidney-friendly eating plan.
- Keep your blood pressure at a healthy level. Your doctor may prescribe blood pressure medicines like ACE inhibitors and angiotensin receptor blockers (angiotensin 2 receptor antagonists).
- Keep your blood sugar at a healthy level if you have diabetes.
- Be active for at least 30 minutes on most days of the week. This can be anything from walking or riding a bike to swimming or dancing.
- Quit smoking or using tobacco.
How long can I live with Stage 4 kidney disease?
How long you may live (your life expectancy) depends on many things, such as:
- Your age when diagnosed with chronic kidney disease
- How well you follow your treatment plan
- Other health problems you have
Kidney disease stage 5
Stage 5 kidney disease also known as End Stage Kidney Disease or ESRD, which means you have an eGFR less than 15 ml/min/1.73m² and severe damage to your kidneys. Your kidneys are getting very close to failure or have already failed (stopped working). Because your kidneys have stopped working to filter waste out of your blood, waste products build up in your body, which can make you very sick and cause other health problems. When your kidneys fail, treatment options to survive include dialysis or a kidney transplant.
Stage 5 kidney disease means that your kidneys are severely damaged and have stopped doing their job to filter waste from your blood. Waste products may build up in your blood and cause other health problems, such as:
- High blood pressure
- Anemia (not enough red blood cells in your body)
- Bone disease
- Heart disease
- High potassium
- High phosphorus
- Metabolic acidosis (a buildup of acid in your body)
To find out what stage of kidney disease you are in and find out what caused your kidney disease, your doctor may do other tests, including:
- GFR blood tests
- Urine tests
- Blood pressure checks
- Imaging tests to take detailed pictures of the inside of your body, such as ultrasound, CT scan or MRI
- Kidney biopsy (a procedure where doctors take a small piece of tissue from your kidneys to look at it under a microscope)
- Genetic testing (if doctors suspect a rare disease or one that runs in your family)
What are the symptoms of stage 5 kidney disease?
You may have these symptoms in stage 5 kidney disease if your kidneys begin to fail:
- Feeling weak and tired
- Swelling in your arms, hands, legs or feet
- Making little or no urine
- Headaches
- Pain in your lower back
- Muscle cramps
- Feeling sick to your stomach or throwing up
- Feeling less hungry than normal
- Trouble breathing
- Changes in your skin color
Stage 5 kidney disease treatment
You will need to see a nephrologist (kidney doctor). Your nephrologist will discuss your treatment options, which include:
- Dialysis, which is a treatment to clean your blood when your kidneys are not able to. Learn more about the two types of dialysis.
- A kidney transplant, which is surgery to give you a kidney from someone else’s body. Learn more about kidney transplants.
Your doctor will help you decide which treatment is best for you and create a plan to manage your kidney disease. As part of the plan, your doctor may give you medicines to help with your symptoms and other health problems kidney disease can cause, such as diabetes and high blood pressure.
Your medicines may include:
- Blood pressure medicines like ACE inhibitors and angiotensin receptor blockers (angiotensin 2 receptor antagonists) (even if you do not have high blood pressure, these medicines can help slow the damage to your kidneys to keep them working well as long as possible)
- Diabetes medicines to keep your blood sugar at a healthy level (even if you do not have diabetes)
- Calcium and vitamin D supplements to keep your bones strong
- Diuretics to help with swelling (these are medicines that help your kidneys get rid of salt and water and make you urinate more)
- Phosphorus binders, which prevent your body from absorbing phosphorus from foods you eat
- Erythropoiesis-stimulating agents or to help with anemia (i.e., not enough red blood cells in your body)
Your doctor may tell you to stop taking medicines that can damage your kidneys, such as pain medicines called NSAIDs (nonsteroidal anti-inflammatory medicines).
What steps can I take to manage Stage 5 kidney disease?
At Stage 5 kidney disease, there is usually no cure and you cannot reverse the damage to kidney function. There are treatment options for kidney failure that can help you live life.
Your doctor will recommend that you:
- Have visits with a nephrologist to check your blood levels and overall health.
- Meet with a dietitian to help you create and follow a kidney-friendly eating plan. Your eating plan may involve limiting certain things to prevent them from building up in your body, such as fluids, potassium, salt (sodium) or phosphorus.
- Keep your blood pressure at a healthy level. They may prescribe blood pressure medicines like ACE inhibitor and ARBs.
- Keep your blood sugar at a healthy level if you have diabetes.
- Be active for at least 30 minutes on most days of the week. This can be anything from walking or riding a bike to swimming or dancing.
- Quit smoking or using tobacco.
How long can I live with Stage 5 kidney disease?
How long you may live (your life expectancy) depends on many things, such as:
- Your age when diagnosed with chronic kidney disease
- How well you follow your treatment plan
- Your overall health
- Your wishes.
End-stage renal disease causes
End-stage renal disease (ESRD) is usually caused by other disease or condition that impairs kidney function, causing kidney damage to worsen over several months or years such as a disease like diabetes or high blood pressure. Diabetes means that your blood sugar is too high and diabetes is the most common cause of kidney failure. High blood pressure is the second most common cause of kidney failure. End-stage renal disease (ESRD) is often the result of a combination of different problems.
End-stage renal disease (ESRD) can be caused by:
- High blood pressure (hypertension) – over time, this can put strain on the small blood vessels in the kidneys and stop the kidneys working properly
- Diabetes (type 1 diabetes or type 2 diabetes) – too much glucose in your blood can damage the tiny filters in the kidneys
- High cholesterol – this can cause a build-up of fatty deposits in the blood vessels supplying your kidneys, which can make it harder for them to work properly
- Kidney infections also called pyelonephritis
- Glomerulonephritis – an inflammation of the kidney’s filtering units (glomeruli)
- Interstitial nephritis, an inflammation of the kidney’s tubules and surrounding structures
- Polycystic kidney disease (PKD) – an inherited condition where growths called cysts develop in the kidneys
- Other inherited kidney diseases
- Hemolytic uremic syndrome in children
- IgA vasculitis
- Renal artery stenosis
- Lupus nephritis is the medical name for kidney disease caused by lupus
- Kidney cancer
- Vesicoureteral reflux (VUR), a condition that causes urine to back up into your kidneys
- Disorders in which the body’s immune system attacks its own cells and organs, such as anti-GBM disease (Goodpasture’s disease)
- Prolonged obstruction of the urinary tract – for example, from kidney stones that keep coming back, or an enlarged prostate
- Long-term, regular use of certain medicines – such as lithium and non-steroidal anti-inflammatory drugs (NSAIDs) that are toxic to the kidneys
- Plasma cell dyscrasias or neoplasm
- Heavy metal poisoning, such as lead poisoning
- Sickle Cell Nephropathy which accounts for less than 1% of end-stage renal disease (ESRD) patients in the United States 6
- Rare genetic conditions, such as Alport syndrome
You can help prevent end-stage renal disease (ESRD) by making healthy lifestyle changes and ensuring any underlying conditions you have are well controlled.
Risk factors for developing end-stage renal disease
Risk factors are things that give you a higher chance of having a condition, such as kidney disease. Having one of these risk factors does not mean that you will get kidney disease. But if you do, and you find and treat kidney disease early, you may be able to prevent it from getting worse.
Risk factors that can increase your risk of chronic kidney disease include:
- Diabetes. Diabetes is the leading risk factor for kidney disease and the most common cause of kidney failure. High blood sugar from diabetes damages your kidneys and lowers their ability to filter waste and fluid from your blood. Over time, this causes kidney disease. If you have diabetes, healthy eating, being active and taking medicine can help slow or avoid damage to your kidneys.
- High blood pressure. High blood pressure is a leading risk factor for kidney disease and the second most common cause of kidney failure, after diabetes. When you have high blood pressure, the force of your blood flowing through the tiny blood vessels in your kidneys can cause damage. High blood pressure can also be a symptom of kidney disease. Keeping your blood pressure under control can help prevent kidney disease or keep it from getting worse.
- Heart (cardiovascular) disease.
- Smoking
- Obesity
- Being Black, Native American or Asian American.
- Family history of kidney disease.
- Abnormal kidney structure.
- Older age.
- Frequent use of medications that can damage the kidneys.
End-stage renal disease prevention
To reduce your risk of developing kidney disease:
- Follow instructions on over-the-counter medications. When using nonprescription pain relievers, such as aspirin, ibuprofen (Advil, Motrin IB, others) and acetaminophen (Tylenol, others), follow the instructions on the package. Taking too many pain relievers for a long time could lead to kidney damage.
- Maintain a healthy weight. If you’re at a healthy weight, maintain it by being physically active most days of the week. If you need to lose weight, talk with your doctor about strategies for healthy weight loss.
- Don’t smoke. Cigarette smoking can damage your kidneys and make existing kidney damage worse. If you’re a smoker, talk to your doctor about strategies for quitting. Support groups, counseling and medications can all help you to stop.
- Manage your medical conditions with your doctor’s help. If you have diseases or conditions that increase your risk of kidney disease, work with your doctor to control them. Ask your doctor about tests to look for signs of kidney damage.
End-stage renal disease signs and symptoms
Signs and symptoms of chronic kidney disease develop over time if kidney damage progresses slowly. In the early stages of chronic kidney disease, you might have few signs or symptoms. You might not realize that you have kidney disease until the condition is advanced. This is because your kidneys have a greater capacity to do their job than is needed to keep you healthy. For example, you can donate one kidney and remain healthy. You can also have kidney damage without any symptoms because, despite the damage, your kidneys are still doing enough work to keep you feeling well. For many people, the only way to know if you have kidney disease is to get your kidneys checked with blood and urine tests.
Loss of kidney function can cause a buildup of fluid or body waste or electrolyte problems. Depending on how severe it is, loss of kidney function can cause:
- Nausea
- Vomiting
- Loss of appetite
- Fatigue and weakness
- Sleep problems
- Urinating more or less
- Decreased mental sharpness
- Muscle cramps
- Swelling of feet and ankles
- Dry, itchy skin
- High blood pressure (hypertension) that’s difficult to control
- Shortness of breath, if fluid builds up in the lungs
- Chest pain, if fluid builds up around the lining of the heart
Signs and symptoms of kidney disease are often nonspecific. This means they can also be caused by other illnesses. Because your kidneys are able to make up for lost function, you might not develop signs and symptoms until irreversible damage has occurred.
Make an appointment with your doctor if you have signs or symptoms of kidney disease. Early detection might help prevent kidney disease from progressing to kidney failure.
Early stages of chronic kidney disease
Kidney disease does not tend to cause symptoms when it’s at an early stage. This is because the body is usually able to cope with a significant reduction in kidney function. Kidney disease is often only diagnosed at this stage if a routine test for another condition, such as a blood or urine test, detects a possible problem. If it’s found at an early stage, medicine and regular tests to monitor it may help stop it becoming more advanced.
Later stages of chronic kidney disease
A number of symptoms can develop if kidney disease is not found early or it gets worse despite treatment.
Later stages of chronic kidney disease symptoms can include:
- weight loss and poor appetite
- swollen ankles, feet or hands – as a result of water retention (edema)
- shortness of breath
- tiredness
- blood in your pee (urine)
- an increased need to pee – particularly at night
- difficulty sleeping (insomnia)
- itchy skin
- muscle cramps
- feeling sick
- headaches
- erectile dysfunction in men
People with late stage chronic kidney disease can also develop anemia, bone disease, and malnutrition. This stage of chronic kidney disease is known as kidney failure, end-stage renal disease or established renal failure. It may eventually require treatment with dialysis or a kidney transplant.
End-stage renal disease complications
End-stage renal disease can affect almost every part of your body. Potential complications include:
- Fluid retention, which could lead to swelling in your arms and legs, high blood pressure, or fluid in your lungs (pulmonary edema)
- A sudden rise in potassium levels in your blood (hyperkalemia), which could impair your heart’s function and can be life-threatening
- Anemia
- Heart disease. If you have kidney disease, it increases your chances of having a stroke or heart attack.
- High blood pressure can be both a cause and a result of kidney disease. High blood pressure damages your kidneys, and damaged kidneys don’t work as well to help control your blood pressure.
- Weak bones and an increased risk of bone fractures
- Decreased sex drive, erectile dysfunction or reduced fertility
- Damage to your central nervous system, which can cause difficulty concentrating, personality changes or seizures
- Decreased immune response, which makes you more vulnerable to infection
- Pericarditis, an inflammation of the saclike membrane that envelops your heart (pericardium)
- Pregnancy complications that carry risks for the mother and the developing fetus
- Irreversible damage to your kidneys (end-stage kidney disease), eventually requiring either dialysis or a kidney transplant for survival
End-stage renal disease diagnosis
To diagnose end-stage renal disease, your doctor may ask you about your family’s and your medical history. Among other things, your doctor might ask questions about whether you’ve been diagnosed with high blood pressure, if you’ve taken a medication that might affect kidney function, if you’ve noticed changes in your urinary habits and whether you have family members who have kidney disease. Next, your doctor performs a physical exam, checking for signs of problems with your heart or blood vessels, and conducts a neurological exam, along with other tests such as:
- Blood tests, to measure the amount of waste products, such as creatinine and urea, in your blood
- Urine tests, to check the level of the protein albumin in your urine
- Imaging tests, such as ultrasound, MRI or CT scan, to assess your kidneys and look for unusual areas
- Removing a sample of kidney tissue (biopsy), to examine under a microscope to learn what type of kidney disease you have and how much damage there is
Certain tests might be repeated over time to help your doctor follow the progress of your kidney disease.
Blood test
The main test for kidney disease is a blood test. The test measures the levels of a waste product called creatinine and urea in your blood. Your doctor uses your blood test results, plus your age, size, gender and ethnic group to calculate how many milliliters (mL) of waste your kidneys should be able to filter in a minute. This calculation is known as your estimated glomerular filtration rate (eGFR). Healthy kidneys should be able to filter more than 90mL/min. You may have CKD if your rate is lower than this.
Your test results can be used to determine how damaged your kidneys are, known as the stage of CKD.
This can help your doctor decide the best treatment for you and how often you should have tests to monitor your condition.
The Glomerular filtration rate (GFR) provides an estimate of how much blood is filtered by the kidneys each minute.
- The formula used to estimate GFR uses serum creatinine, age, gender, and race. In normal kidneys GFR > 60 ml/minute. A GFR of less than 60 ml/minute/1.73m² may mean you have kidney disease
- eGFR (mL/min/1.73 m2) = 175 x (serum creatinine)–1.154 x (Age)–0.203 x (0.742 if female) x (1.212 if African American)
- End Stage Kidney failure (stage 5) is an eGFR < 15 ml/minute. Most people below this level need dialysis or a kidney transplant. Talk with your health care provider about your treatment options.
- eGFR is not reliable for patients with rapidly changing creatinine levels, extremes in muscle mass and body size, or altered diet patterns.
- For a free Glomerular Filtration Rate (GFR) Calculators please go here: https://www.niddk.nih.gov/health-information/professionals/clinical-tools-patient-management/kidney-disease/laboratory-evaluation/glomerular-filtration-rate-calculators/recommended
Table 2. Reference Table for Population Mean eGFR from NHANES III
| Age (years) | Mean eGFR (mL/min/1.73 m²) |
|---|---|
| 20–29 | 116 |
| 30–39 | 107 |
| 40–49 | 99 |
| 50–59 | 93 |
| 60–69 | 85 |
| 70 | 75 |
Each chronic kidney disease patient is classified into one of the following 5 stages of CKD based on their estimated glomerular filtration rate (eGFR) and the level of proteinuria, because management and prognosis varies according to the progression of damage.
- CKD Stage 1: Kidney damage with normal or increased eGFR (above 90 mL/min/1.73 m²), but other tests have detected signs of kidney damage
- CKD Stage 2: Mild reduction in eGFR (60-89 mL/min/1.73 m²), with other signs of kidney damage
- CKD Stage 3: Moderate reduction in eGFR (30-59 mL/min/1.73 m²)
- Stage 3a (G3a) – an eGFR of 45 to 59ml/min/1.73 m²
- Stage 3b (G3b) – an eGFR of 30 to 44ml/min/1.73 m²
- CKD Stage 4: Severe reduction in eGFR (15-29 mL/min/1.73 m²)
- CKD Stage 5 (End Stage Kidney Disease or ESRD): Kidney failure (eGFR less than 15 mL/min/1.73 m²), meaning the kidneys have lost almost all of their function and require dialysis
Alongside your eGFR, your urine albumin:creatinine ratio (ACR) can help give a more accurate picture of how well your kidneys are working.
Urine test
A urine test is also done to:
- check the levels of substances called albumin and creatinine in your urine – known as the albumin:creatinine ratio (ACR) or urine albumin-to-creatinine ratio (UACR)
- Doctors use your urine albumin-to-creatinine ratio (UACR) to estimate how much albumin would pass into your urine over 24 hours. A urine albumin result of
- 30 mg/g or less is normal
- more than 30 mg/g may be a sign of kidney disease
- Albumin is a protein found in your blood. A healthy kidney doesn’t let albumin pass into the urine. A damaged kidney lets some albumin pass into the urine. The less albumin in your urine, the better. Having albumin in the urine is called albuminuria. The amount of protein in urine is taken as a sign of how bad the damage is.
- If you have kidney disease, measuring the albumin in your urine helps your doctor know which treatment is best for you. A urine albumin level that stays the same or goes down may mean that treatments are working.
- Doctors use your urine albumin-to-creatinine ratio (UACR) to estimate how much albumin would pass into your urine over 24 hours. A urine albumin result of
- check for blood in your urine. Healthy kidneys usually almost completely prevent certain substances in the blood from entering the urine. Kidney damage may become noticeable when blood is found in urine. Blood and protein are only found in significant amounts in urine if the kidneys are damaged.
If you have albumin in your urine, your doctor may want you to repeat the urine test one or two more times to confirm the results.
Alongside your eGFR, your urine albumin:creatinine ratio (ACR) can help give a more accurate picture of how well your kidneys are working.
You can tell that your treatments are working if your:
- GFR stays the same
- urine albumin stays the same or goes down
Your albumin:creatinine ratio (ACR) result is given as a stage from 1 to 3:
- A1 – an ACR of less than 3 mg/mmol
- A2 – an ACR of 3 to 30 mg/mmol
- A3 – an ACR of more than 30 mg/mmol
For both eGFR and ACR, a higher stage indicates more severe kidney disease.
Other tests
Sometimes other tests are also used to assess the level of damage to your kidneys.
These may include:
- an ultrasound scan, MRI scan or CT scan – to see what the kidneys look like and check whether there are any blockages
- a kidney biopsy – a small sample of kidney tissue is removed using a needle and the cells are examined under a microscope for signs of damage. Kidney biopsy is often done with local anesthesia using a long, thin needle that’s inserted through your skin and into your kidney. The biopsy sample is sent to a lab for testing to help determine what’s causing your kidney problem.
End-stage renal disease treatment
End-stage renal disease (ESRD) is kidney failure that is treated by dialysis or kidney transplant.
To replace your lost kidney function, you may have one of four treatment options:
- Hemodialysis. Hemodialysis is a treatment to filter wastes and water from your blood, as your kidneys did when they were healthy. During hemodialysis, your blood goes through a filter, called a dialyzer, outside your body 1. A dialyzer is sometimes called an “artificial kidney”. Hemodialysis helps control blood pressure and balance important minerals, such as potassium, sodium, and calcium, in your blood. At the start of a hemodialysis treatment, a dialysis nurse or technician places two needles into your arm. You may prefer to put in your own needles after you’re trained by your health care team. A numbing cream or spray can be used if placing the needles bothers you. Each needle is attached to a soft tube connected to the dialysis machine. The dialysis machine pumps blood through the filter and returns the blood to your body. During the process, the dialysis machine checks your blood pressure and controls how quickly blood flows through the filter and fluid is removed from your body. You can receive treatment at a dialysis center or at home. Each location has its pros and cons.
- Peritoneal dialysis. Peritoneal dialysis is a treatment for kidney failure that uses the lining of your abdomen, or belly, to filter your blood inside your body 2. Doctors call this lining the peritoneum. A few weeks before you start peritoneal dialysis, a surgeon places a soft tube called a catheter in your belly. When you start treatment, dialysis solution (water with salt and other additives) flows from a bag through the catheter into your belly. When the bag is empty, you disconnect it and place a cap on your catheter so you can move around and do your normal activities. While the dialysis solution is inside your belly, it absorbs wastes and extra fluid from your body 2. You shouldn’t feel any pain. Most people look and feel normal despite a belly full of solution. After a few hours, the solution and the wastes are drained out of your belly into the empty bag. You can throw away the used solution in a toilet or tub. Then, you start over with a fresh bag of dialysis solution. When the solution is fresh, it absorbs wastes quickly. As time passes, filtering slows. For this reason, you need to repeat the process of emptying the used solution and refilling your belly with fresh solution four to six times every day. This process is called an exchange. You can do your exchanges during the day, or at night using a machine that pumps the fluid in and out. For the best results, it is important that you perform all of your exchanges as prescribed. Dialysis can help you feel better and live longer, but it is not a cure for kidney failure.
- Kidney transplant. Kidney transplant is surgery to place a healthy kidney from a person who has just died, or from a living person, into your body to filter your blood.
- Conservative management. Some people with kidney failure choose not to have dialysis or a transplant but continue to receive care from their health care team, take medicines, and monitor their diet and lifestyle choices to preserve your kidney function and quality of life as long as possible.
Dialysis
Dialysis does some of the work of your kidneys when your kidneys can’t do it themselves. This includes removing extra fluids and waste products from your blood, restoring electrolyte levels, and helping control your blood pressure. For most people, the need for dialysis comes on slowly. Symptoms, such as losing your desire to eat and losing muscle, may begin so slowly that you don’t notice them. Many people start dialysis when their kidney function (glomerular filtration rate [GFR]) is between 5 and 10. When kidney function is this low, you may have symptoms from kidney failure and starting dialysis may help relieve them. Starting dialysis can help you regain your appetite and maintain your strength, which is harder to rebuild than it is to retain. Your kidney doctor can help you decide the best time to begin treatment. For dialysis to be successful, you may need to make lifestyle changes, such as following certain dietary recommendations.
Dialysis options include peritoneal dialysis and hemodialysis.
Your doctor, nurse, or social worker can help you find a dialysis center that’s convenient for you. Under Medicare rules, you have the right to choose the dialysis center where you’ll receive treatment. You may want to use Dialysis Facility Compare, which rates all dialysis centers according to quality. Your doctor will give your medical information to the dialysis center you choose.
Most large cities have more than one dialysis center to choose from. You can visit the centers to see which one best fits your needs. For example, you can ask about a center’s rules for laptop and cellphone use, as well as for having visitors. You may want the center to be close to your home to save travel time. If you live in a rural area, the closest dialysis center may be far from your home. If you’d have a hard time getting to the dialysis center, you may want to consider home dialysis treatments such as home hemodialysis or peritoneal dialysis.
Peritoneal dialysis
During peritoneal dialysis, blood vessels in your abdominal lining (peritoneum) fill in for your kidneys with the help of a fluid that washes in and out of the peritoneal space. Peritoneal dialysis is done in your home.
You can choose the type of peritoneal dialysis that best fits your life:
- Continuous ambulatory peritoneal dialysis (CAPD). With continuous ambulatory peritoneal dialysis (CAPD) an exchange takes about 30 to 40 minutes, and most people need to do four exchanges per day. You sleep with solution in your belly at night.
- Automated peritoneal dialysis. Automated peritoneal dialysis uses a machine called a cycler to do three to five exchanges per night while you sleep. You may have to do one exchange during the day without the machine.
The main differences between the two types of peritoneal dialysis are:
- the schedule of exchanges
- one uses a machine and the other is done by hand
If one type of peritoneal dialysis doesn’t suit you, talk with your doctor about trying the other type.
You may need a combination of continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis if you weigh more than 175 pounds or if your peritoneum filters wastes slowly 5. For example, some people use a cycler (automated peritoneal dialysis machine) at night and perform one exchange during the day. Others do four exchanges during the day and use a minicycler to perform one or more exchanges during the night. You’ll work with your doctor to find the best schedule for you.
What are the pros and cons of peritoneal dialysis?
With either continuous ambulatory peritoneal dialysis (CAPD) or automated peritoneal dialysis, you gain a sense of control over your treatments and don’t need the help of a partner. After you’re trained, you can do continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis by yourself. With peritoneal dialysis, you’ll have boxes of dialysis solution taking up space in your home.
Continuous ambulatory peritoneal dialysis (CAPD) pros
- You don’t need a machine to do continuous ambulatory peritoneal dialysis (CAPD).
- You can do continuous ambulatory peritoneal dialysis (CAPD) at the times you choose, as long as you complete the required number of exchanges each day.
- You can do continuous ambulatory peritoneal dialysis (CAPD) in many locations.
- You can travel as long as you bring dialysis supplies with you or have them delivered to where you’re going.
Continuous ambulatory peritoneal dialysis (CAPD) cons
- Continuous ambulatory peritoneal dialysis (CAPD) can disrupt your daily routine.
- Continuous ambulatory peritoneal dialysis (CAPD) is a continuous treatment, and you need to do all exchanges 7 days a week.
Automated peritoneal dialysis pros
- You can do exchanges at night while you sleep.
- You may not have to perform exchanges during the day.
- You can travel as long as you bring dialysis supplies with you or have them delivered to where you’re going.
Automated peritoneal dialysis cons
- You need a machine. If you travel, you may have to carry your cycler with you.
- Your connection to the cycler limits your movement at night.
Hemodialysis
During hemodialysis, a machine does some of the work of the kidneys by filtering harmful wastes, salts and fluid from your blood. During hemodialysis, your blood goes through a filter, called a dialyzer, outside your body 1. A dialyzer is sometimes called an “artificial kidney”. Hemodialysis helps control blood pressure and balance important minerals, such as potassium, sodium, and calcium, in your blood. At the start of a hemodialysis treatment, a dialysis nurse or technician places two needles into your arm. You may prefer to put in your own needles after you’re trained by your health care team. A numbing cream or spray can be used if placing the needles bothers you. Each needle is attached to a soft tube connected to the dialysis machine. The dialysis machine pumps blood through the filter and returns the blood to your body. During the process, the dialysis machine checks your blood pressure and controls how quickly blood flows through the filter and fluid is removed from your body. You can receive hemodialysis at a dialysis center or at home. Each location has its pros and cons.
Pros and cons of having hemodialysis at home
Home hemodialysis lets you have longer or more frequent dialysis, which comes closer to replacing the work healthy kidneys do, usually three to seven times per week, and with treatment sessions that last between 2 and 10 hours 1. Machines for home use are small enough to sit on an end table 1. If you choose to have your hemodialysis at home, you’ll still see your doctor once per month.
Flexible schedule
You can choose a schedule that fits the way you live. You can use 1:
- Standard home hemodialysis: 3 times a week or every other day for 3 to 5 hours.
- Short daily hemodialysis: 5 to 7 days per week for 2 to 4 hours at a time.
- Nightly home hemodialysis: 3 to 6 times per week while you sleep.
Your doctor will decide how many treatments you need each week for daily or nightly home hemodialysis.
More dialysis filters your blood more thoroughly
Compared with a standard hemodialysis schedule, daily or nightly home hemodialysis will let you 1:
- Eat and drink more normally
- Take fewer blood pressure medicines
Healthy kidneys work 24 hours a day, 7 days a week. Getting more hemodialysis feels more like having healthy kidneys and lowers your chances for problems that are common with a standard hemodialysis schedule, such as 1:
- Painful muscle cramps from removing too much fluid too quickly.
- High blood pressure, which can cause a headache or, in rare cases, a stroke.
- Low blood pressure, which can make you faint, feel sick to your stomach, or be more likely to fall.
- High phosphate levels, which can weaken bones and make your skin itch.
Better quality of life
Standard hemodialysis can make you feel tired or washed out for several hours after each treatment. People who have switched from standard hemodialysis to longer or more frequent hemodialysis report they feel better, with more energy, less nausea, and better sleep. They also may report a better quality of life 4.
Training for home hemodialysis
Most dialysis centers require that you have a trained partner in your home during hemodialysis treatments, so you must ask a family member or friend to go through the training with you 1. The clinic’s home-training nurse will teach you important safety skills.
During training, you and your care partner will learn to 1:
- Set up the machine
- Take steps to prevent infection
- Place needles into the vascular access
- Respond to any alarms from the machine
- Check your weight, temperature, blood pressure, and pulse
- Record treatment details for the clinic
- Clean the machine
- Throw out used supplies safely
- Track used supplies and order new ones
Training may take 4½ to 6 hours, 5 days a week, for 3 to 8 weeks. If you already know how to place the needles into your access, training may take less time.
The home-training nurse will make sure that you and your partner feel confident and may visit your home to help with your first at-home treatment. In addition to providing training and a hemodialysis machine that stays in your home, the dialysis center also provides 24-hour support if you have a question or problem. Some programs also monitor treatments over the internet.
Disadvantages of home hemodialysis
- Not all dialysis centers offer home hemodialysis training and support.
- You and a family member or friend will have to set aside several weeks for training.
- Helping with treatments may be stressful for your treatment partner.
- You need space at home to store the hemodialysis machine and supplies.
You’ll need to learn to put dialysis needles into your vascular access. - Medicare and private insurance companies may limit the number of home hemodialysis treatments they will pay for. Few people can afford the costs for additional treatments.
Pros and cons of having hemodialysis at dialysis center
Most people go to a dialysis center for treatment. At the dialysis center, doctors and nurses set up and help you connect to the dialysis machine. A team of health care workers will be available to help you. You will continue to see your doctor. Other team members may include nurses, health care technicians, a dietitian, and a social worker.
Set schedule
You’ll have a fixed time slot for your treatments, usually three times per week: Monday, Wednesday, and Friday; or Tuesday, Thursday, and Saturday. Each dialysis session lasts about 4 hours. When choosing a dialysis schedule, think about your work and child care or other caregiving duties.
Nighttime option
Some dialysis centers offer nighttime treatments. These treatments occur at the dialysis center 3 nights a week while you sleep, which takes longer. Getting longer overnight dialysis treatments means 1:
- Your days are free.
- You have fewer diet changes.
- Your liquid allowance (how much liquid you can drink) is closer to normal.
- You may have a better quality of life than with a standard hemodialysis schedule. Longer treatment sessions may reduce your symptoms.
Disadvantages of dialysis center
- The center arranges treatments, so your schedule is less flexible.
- You must travel to the center for treatment.
- A longer time between treatments means you will have the strictest limits on diet and liquids—because wastes and extra fluid can build up in your body. Having too much fluid in your blood can raise blood pressure and stress your heart. Removing too much fluid too fast during standard hemodialysis also can stress the heart.
- You may have more “ups and downs” in how you feel from day to day because of the longer time between treatments.
- Feeling better after a treatment may take a few hours.
Kidney transplant
A kidney transplant is a surgical procedure to place a healthy kidney from a live or deceased donor into a person whose kidneys no longer function properly. A kidney transplant is often the treatment of choice for end-stage renal disease, compared with a lifetime on dialysis. A working, transplanted kidney does a better job filtering wastes and keeping you healthy than dialysis, but it still isn’t a cure. When you have a kidney transplant, surgeons usually leave your old kidneys in place and connect the donated kidney to an artery and a vein in your groin. The surgeon also transplants the ureter from the donor to let urine flow from your new kidney into your bladder. After a successful kidney transplant, your new kidney filters your blood, and you no longer need dialysis.
The kidney transplant process takes time. It involves finding a donor, living or deceased, whose kidney best matches your own. A transplant center can place you on the waiting list for a donor kidney if you have permanent kidney damage and your kidney function is 20 or less. While you’re waiting for a kidney transplant, you may need to start dialysis.
You then have surgery to place the new kidney in your lower abdomen and attach the blood vessels and ureter — the tube that links the kidney to the bladder — that will allow the new kidney to function.
Your body normally attacks anything it sees as foreign, so to keep your body from attacking the donor kidney, you will need to take anti-rejection medicines to help keep your immune system from rejecting your new kidney and to reduce the risk of post-surgery complications, such as infection. Like all strong medicines, anti-rejection medicines have side effects.
You may need to spend several days to a week in the hospital. After leaving the hospital, you can expect frequent checkups to monitor your progress as your recovery continues.
Anti-rejection medicines side effects
Some anti-rejection medicines (immunosuppressants) may change your appearance. Your face may get fuller, you may gain weight, or you may develop acne or facial hair. Not all people have these side effects.
Anti-rejection medicines (immunosuppressants) weaken your immune system, which can lead to infections. In some people over long periods of time, a weakened immune system can increase their risk of developing cancer. Some anti-rejection medicines cause cataracts, diabetes, extra stomach acid, high blood pressure, and bone disease.
When used over time, anti-rejection medicines (immunosuppressants) may also cause liver or kidney damage in some people. Your transplant team will order regular tests to monitor the levels of anti-rejection medicines in your blood and to measure your liver and kidney function.
Palliative care
If you choose not to have a kidney transplant or dialysis, you can choose palliative or supportive care to help you manage your symptoms and feel better. You also can combine palliative care with kidney transplant or dialysis.
Without either dialysis or a transplant, kidney failure progresses, eventually leading to death. Death can occur quickly or take months or years. Supportive care might include management of symptoms, measures to keep you comfortable and end-of-life planning.
End-stage renal disease diet
Healthy kidneys balance the salts and minerals—such as calcium, phosphorus, sodium, and potassium—that circulate in your blood. When you have end-stage renal disease, what you eat and drink may help you maintain a healthy balance of salts and minerals in your body. You will need to keep track of what you eat and drink. Changes may need to be made based on your blood test results. Nutrients are substances found in food that your body needs to function and maintain health—for example, water, sodium, protein, phosphorus, potassium, vitamins, and other minerals. Your diet can supply nutrients that are lost through treatment, or you might need to limit certain nutrients you eat that can build up in your body. You may also need to keep track of how many calories are in what you eat and drink.
All dialysis and transplant centers have a dietitian who can help you plan your meals. A renal dietitian has special training in counseling people with kidney failure.
As part of your treatment for kidney disease, your doctor might recommend that you follow a special diet to help support your kidneys and limit the work they must do. Ask for a referral to a registered dietitian with expertise in kidney disease to learn ways to make your diet easier on your kidneys. You can find a registered dietitian online through the Academy of Nutrition and Dietetics or through your kidney care team. Work closely with your dietitian to develop a meal plan that includes foods and drinks you enjoy eating while maintaining your health.
The kind of kidney failure treatment you’ve chosen will also affect your eating plan. If you have a kidney transplant, you’ll have fewer limits to your diet.
Water
Water is in drinks such as coffee, tea, and soda; and in foods such as fruits, vegetables, ice cream, gelatin, soup, and popsicles. Your body needs water to function properly; however, in kidney failure, the kidneys can’t get rid of extra water. Taking in too much water can cause swelling, raise your blood pressure, and make your heart work harder.
Sodium
Sodium is a part of salt. You can find sodium in many canned, packaged, processed, and fast foods and in some seasonings. You need sodium to help control the amount of fluid in your body. However, too much sodium may cause high blood pressure. No matter what treatment you’re on, it’s likely you will need to limit sodium intake.
Protein
Protein provides the building blocks that help maintain and repair muscles, organs, and other parts of the body. Protein is in many foods you eat, including foods from animals and plants. Most diets include both types of protein. Too much protein can cause waste to build up in your blood, making your kidneys work harder.
Phosphorus
Phosphorus is balanced with calcium to keep your bones healthy. When you have kidney disease, phosphorus can build up in your blood. Too much phosphorus can weaken your bones.
Phosphorus is found naturally in foods rich in protein, such as meat, poultry, fish, nuts, beans, and dairy products. Phosphorus is also added to many processed foods, such as lunch meats. Phosphorus added to food may cause your blood levels to rise more than the phosphorus that is naturally found in food.
Your dietitian can help you find ways to get the protein you need without getting too much phosphorus.
Potassium
Potassium is a mineral that helps your nerves and muscles work. Potassium is found in fruits and vegetables such as oranges, bananas, tomatoes, and potatoes. Your nerve cells and brain will not work well if your potassium is too high or too low. If you have kidney failure, your potassium level may tend to be high. You may need to limit foods that are high in potassium.
Calories
You need energy to fuel your body. Energy is measured in calories. Taking in more calories than your body uses can cause weight gain and high blood sugar. Taking in fewer calories than your body uses will result in weight loss.
Supplements for people with kidney failure
Supplements help provide some of the vitamins and minerals you may be missing, either because you need to avoid certain foods or because your treatment removes some vitamins from your body. Your doctor may prescribe a supplement made for people with kidney failure. You should only take vitamin, mineral, or dietary supplements that your kidney doctor has recommended. Over-the-counter (no prescription needed) supplements not recommended by your kidney doctor may be harmful to you.
- Hemodialysis. https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/hemodialysis[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Peritoneal Dialysis. https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/peritoneal-dialysis[↩][↩][↩][↩]
- Choosing a Treatment for Kidney Failure. https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/choosing-treatment#conservative[↩][↩][↩][↩]
- Hall YN, Larive B, Painter P, et al. Effects of six versus three times per week hemodialysis on physical performance, health, and functioning: Frequent Hemodialysis Network (FHN) randomized trials. Clinical Journal of the American Society of Nephrology. 2012;7(5):782–794.[↩][↩]
- Choosing a Treatment for Kidney Failure. https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/choosing-treatment[↩][↩]
- Aeddula NR, Bardhan M, Baradhi KM. Sickle Cell Nephropathy. [Updated 2022 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526017[↩]
- http://nkdep.nih.gov/professionals/gfr_calculators/gfr_faq.htm[↩]





{kind=link}