Contents
What is entropion
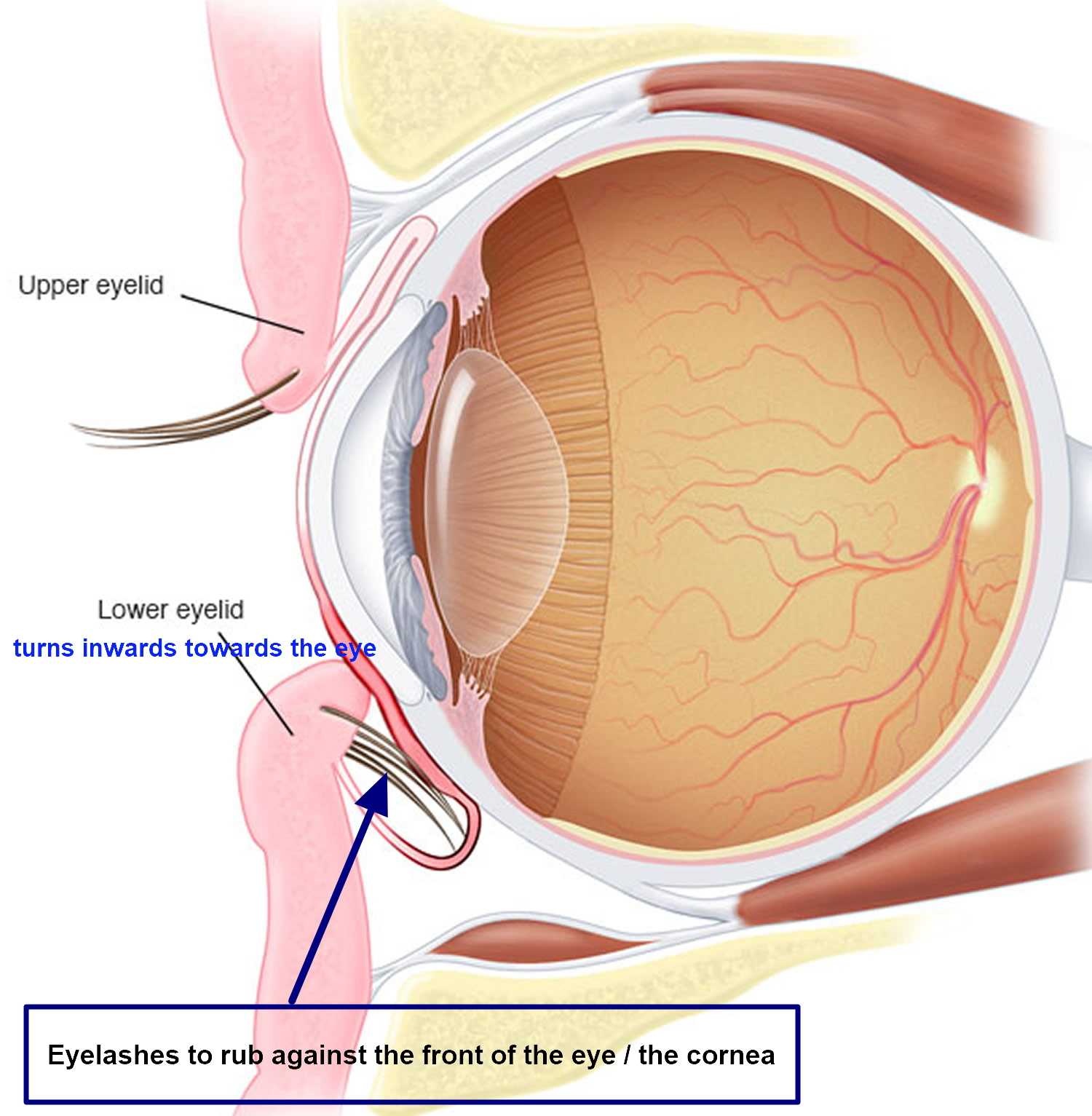
Entropion is the turning in of an edge of an eyelid. Entropion is most often is seen on the lower eyelid where the lower eyelid and eyelashes turn towards the eye (Figure 1). The eyelashes and skin of the eyelid rub against the cornea (the front part of the eye) and conjunctiva (the mucous membrane that protects the eye). This rubbing can lead to excessive tearing, crusting of the eyelid, mucous discharge, irritation of the cornea, impaired vision, and a feeling that something is in the eye.
When you have entropion, your eyelid may be turned in all the time or only when you blink hard or squeeze your eyelids shut. Entropion is more common in older adults, and it generally affects only the lower eyelid.
Entropion can cause corneal and conjunctival damage leading to corneal stromal abrasion, scarring, corneal thinning and corneal neovascularization. In advanced cases, there can be risk of corneal ulcer and perforation 1.
Entropion can be present at birth (congenital).
In babies, it rarely causes problems because the lashes are very soft and do not easily damage the eye. In older people, the condition is most often caused by a spasm or weakening of the muscles surrounding the lower part of the eye.
Another cause can be trachoma infection, which can lead to scarring of the inner side of the lid. This is rare in North America and Europe. However, trachoma scarring is one of the three leading causes of blindness in the world.
Risk factors for entropion are:
- Aging
- Chemical burn
- Infection with trachoma
Entropion eye symptoms include:
- Decreased vision if the cornea is damaged
- Excessive tearing
- Eye discomfort or pain
- Eye irritation
- Redness
Artificial tears and lubricating ointments can help relieve symptoms of entropion. But usually surgery is needed to fully correct the condition. Left untreated, entropion can cause damage to the transparent covering in the front part of your eye (cornea), eye infections and vision loss.
Figure 1. Entropion eye

Seek immediate care if you have received a diagnosis of entropion and you experience:
- Rapidly increasing redness in your eyes
- Pain
- Sensitivity to light
- Decreasing vision
These are signs and symptoms of cornea injury, which can harm your vision.
Make an appointment to see your doctor if you feel like you constantly have something in your eye or you notice that some of your eyelashes seem to be turning in toward your eye. If you leave entropion untreated for too long, it can cause permanent damage to your eye. Start using artificial tears and eye-moisturizing ointments to protect your eye before your appointment.
Entropion complications
Dry eye and irritation may increase the risk for:
- Corneal abrasions
- Corneal ulcers
- Eye infections
Corneal irritation and injury are the most serious complications related to entropion because they can lead to permanent vision loss.
Entropion types
There are four main categories of entropion, each with a different pathophysiology: involutional, spastic, cicatricial and congenital. Treatments are aimed specifically at the particular causes for the condition.
Involutional Entropion
Involutional entropion is the most common type of entropion. Management should be directed at the specific mechanical failures of horizontal and vertical lid laxity, lower lid retractor weakness and orbicularis oculi override. Addressing more contributing factors has a greater chance at achieving resolution 2.
Management strategies range from conservative, noninvasive measures to more complex surgeries requiring tissue grafts. The approach depends on disease severity, patient comorbidities and goals of care. Numerous repair techniques are described in the literature, each with a slightly different approach to the mechanical issues underlying involutional entropion and various combinations of the strategies discussed below.
Figure 2. Involutional entropion

Noninvasive Treatment
Patients can achieve temporary relief with taping of the lower lid to the malar eminence 3 or with application of a cyanoacrylate liquid bandage to evert the lid margin 4. These treatments are beneficial as temporizing measures until the patient can have surgery for definitive repair, or if the patient is too ill to be a candidate for surgical intervention. Temporary relief from involutional entropion can also be achieved with botulinum toxin injections to the orbicularis, weakening the orbicularis to combat override 5.
Carbon dioxide laser skin resurfacing has been proposed as a conservative means of managing involutional entropion. This method was described with success in four of five patients followed for 21 months 6.
Surgical Treatment
Rotational Sutures
Full-thickness eyelid sutures (Quickert sutures) can be placed at the bedside or in the office as a quick procedure to offer patients immediate relief from entropion symptoms 7. The procedure takes an average of 15 minutes to complete and requires only local anesthesia 8. A double-armed 4-0 chromic suture is placed from the deep inferior fornix below the inferior tarsal border, through the lower lid retractors, and exits through the skin superior to the level of insertion. Exiting more superiorly causes more lid eversion. This procedure indirectly tightens the lower lid retractors and forms scarring between the retractors, orbicularis and skin to prevent override 1. Recurrence is common, with Jand et al observing over 21% recurrence at 6 months and nearly 50% by two years 9. Tsang et al 8 encountered better results with 33% recurrence at 14-40 months.
Tarsal Strip
Horizontal lid laxity can be addressed surgically with a tarsal strip. A lateral canthotomy and inferior cantholysis is performed to release the lower lid. The mucocutaneous junction is removed from the lid margin, and the anterior lamella is excised off the tarsus. Conjunctiva is debrided from the posterior tarsus. A horizontal incision through the superior tarsal plate creates a strip that is trimmed to achieve the desired amount of tightening. The strip is attached to the internal aspect of the lateral orbital rim 10.
A small case series of 15 patients treated with tarsal strip only showed no recurrence of entropion at an average of 13 months follow-up 11. A series of 42 eyelids with involutional entropion without canthal tendon laxity used full-thickness excision and repair to treat entropion. This study reported 8% recurrence at 14 months, with average time to failure of 13 months 12. As an independent measure, addressing the horizontal dimension of the lower lid is more successful in correcting entropion than targeting lid rotation.
There is only one randomized control trial comparing entropion repair techniques 10, examining everting sutures against everting sutures with tarsal strip. This study found 21% recurrence of entropion by 18 months for patient’s with only everting sutures and no recurrences in the combined group 10.
Lower Lid Retractor Reinsertion
Lower lid retractor disinsertion can be reversed surgically with posterior advancement of the retractors. After lateral canthotomy and inferior cantholysis, an incision is made through the conjunctiva and lower lid retractors spanning from the lateral canthus to just lateral to the inferior punctum, taking advantage of the bloodless plane just below the inferior tarsal border. The conjunctiva and retractors are then separated from the anterior lamella to expose the orbital septum overlying orbital fat. A strip of orbicularis is excised or ablated inferior to the tarsus, reducing the effect of preseptal orbicularis override. The lower lid retractors are immediately posterior to the fat compartments and adherent to the conjunctiva. The patient can look up and down to assist in locating the retractors. The retractors are separated from the conjunctiva with cautery, and sharp dissection allows for exposure of the anterior surface of the inferior tarsal plate 2.
Using 6-0 vicryl, the retractors are reattached to the anterior inferior tarsus to evert the lid margin. Tarsal strip can be combined with this procedure after the retractors are attached, as adequate exposure is already obtained 2. Combining tarsal strip with retractor advancement takes an average of 13 minutes more than retractor advancement alone 13 and gives a 96.7% success rate 14. The dual procedure is more effective in treating involutional entropion with horizontal lid laxity than retractor advancement alone 13. External approach can be used if there is absent lid laxity, significant festoons or prominent lower lid dermatochalasis 2.
Everting sutures can also be placed along with tarsal strip and retractor reinsertion with recurrence rate of 2.2% at 22.6 months, much less than the rate of 29% for everting sutures alone 15.
Cicatricial Entropion
Cicatricial entropion results from chronic inflammation leading to fibrosis, scarring and shortening of the posterior lamella. These cases are associated with other stigmata of chronic inflammation such as symblepharon, forniceal shortening, keratinization, and loss of normal margin structures. This is unique from other causes of entropion because it is usually secondary to a systemic and progressive inflammatory condition such as ocular cicatricial pemphigoid, Stevens-Johnson syndrome, trachoma, and herpetic disease 2.
Cicatricial entropion may also be the result of trauma and can be iatrogenic from surgery or radiation therapy 2. Cicatricial entropion has also been noted to develop after treatment with glaucoma medications, especially miotic agents, and some chemotherapy drugs 16.
Due to its progressive nature and difficulty in managing the underlying condition, cicatricial entropion is considered the most difficult type of entropion to treat 1. Recurrence rate following surgery ranges from 12-71% regardless of technique used, with higher rates in more severe cases 17.
Treatment of cicatricial entropion
Treatment of cicatricial entropion should always include medical control of the underlying pathologic condition when present. Surgical management poses a challenge of lysing the scar tissue responsible for margin malposition without the corrective surgery inciting additional inflammation. Surgical technique depends on the severity of disease and etiology of symptoms 2.
If there is mild disease with symptoms from lashes abrading the corneal surface, skin resection may be sufficient to rotate the margin. If offending lashes are arranged in a sectoral pattern, cryotherapy can be offered 2. If a large portion of the lid has offending lashes follicle excision can be performed. Follicle excision is achieved by splitting the lamella posterior to the lashes and excising the lashes with Westcott scissors. The base of the lash follicles is then cauterized to prevent regrowth 2. 90% of eyelids treated with this procedure had functional success with no return of trichiasis at 6-24 months 18.
In moderate disease affecting the upper lids, tarsal infracture is a viable surgical option that preserves the lashes and can deliver acceptable cosmesis. An external partial tarsectomy is performed through a lid crease incision. A double-armed 6-0 vicryl is placed partial thickness through the tarsus and externalized. A full-thickness tarsotomy is then performed to direct the lid margin away from the globe. Everting sutures are placed to keep the lid margin rotated anteriorly, and the skin is closed 2.
Transverse blepharotomy and marginal rotation has also been used to treat cicatricial entropion. In this procedure a full-thickness incision is made 4mm from the lid margin and 5-0 absorbable suture is passed partial-thickness through the anterior tarsus and lower lid retractors of the proximal lid and then through the orbicularis and skin of the distal lid. The suture is tied in horizontal mattress fashion over a bolster near the lash line, and skin is closed. The sutures and bolster remain in place for 10 days. This procedure has an 85% success rate for upper and lower lid cicatricial entropion repair 19.
For severe cicatricial disease, the posterior lamella must be lengthened while releasing scar tissue and lid retractors. In these instances the posterior lid retractors can be weakened by recession or lysis with a spacer 20. Hard palate graft, other mucous membrane graft or allograft can be used to support and bolster the posterior lamella. Graft choice is especially important when operating on the upper lid, as the graft will be in constant contact with the cornea, and free tarsoconjunctival grafts may provide good results 2.
Spastic Entropion
Spastic entropion is thought by some to be a subset of involutional entropion 1. Muscle spasm of the orbicularis can induced by local irritation or infection can unmask asymptomatic involutional changes that make the eyelid more susceptible to override, resulting in temporary entropion 21.
Treatment of spastic entropion
First line treatment is to relieve the instigating condition by treating any infection or local reaction present on the eyelid 21. Hubbard and Kanski in 1973 described injecting 80% alcohol into the orbicularis oculi to quell spasm with high rates of success 22. Presently, botulinum toxin injection to the orbicularis and full thickness eyelid sutures have been used to treat this entity 23.
Congenital Entropion
Congenital entropion is a rare condition in which the lower lid margin is rotated inward since birth. This results from disinserted lower lid retractors, posterior lamella vertical insufficiency or kinking of the tarsal plate 2. Children may also develop entropion following facial paralysis, a condition that typically leads to ectropion in adults. In pediatric patients, the orbicularis acts to counter the inturning force of the lower lid retractors, and facial paralysis results in unchecked retractor function rotating the eyelid margin toward the globe surface 24. Eyelid retraction may be confused with congenital entropion 25.
Treatment of congenital entropion
Treatments include lubrication to limit mechanical trauma, taping the lower lid to the malar prominence to correct lid margin position, or injecting low doses of botulinum toxin into the orbicularis to weaken the muscle and prevent override. Surgical therapy provides definitive treatment 5.
Entropion causes
Entropion can be caused by:
- Muscle weakness. As you age, the muscles under your eyes tend to weaken, and the tendons stretch out. This is the most common cause of entropion.
- Scars or previous surgeries. Skin scarred by chemical burns, trauma or surgery can distort the normal curve of the eyelid.
- Eye infection. An eye infection called trachoma is common in many developing countries of Africa, Asia, Latin America, the Middle East and Pacific Islands. It can cause scarring of the inner eyelid, leading to entropion and even blindness.
- Inflammation. An irritation of the eye caused from dryness or inflammation can lead to an effort to relieve the symptoms by rubbing the eyelids or squeezing them shut. This can lead to a spasm of the eyelid muscles and a rolling of the edge of the lid inward against the cornea (spastic entropion).
- Developmental complication. When entropion is present at birth (congenital), it may be caused by an extra fold of skin on the eyelid that causes turned-in eyelashes.
Risk factors for developing entropion
Factors that increase your risk of developing entropion include:
- Age. The older you are, the greater your chances of developing the condition.
- Previous burns or trauma. If you’ve had a burn or other injury on your face, the resulting scar tissue may put you at higher risk of developing entropion.
- Trachoma infection. Because trachoma can scar the inner eyelids, people who have had this infection are more likely to develop entropion.
Entropion prevention
Generally, entropion isn’t preventable. You may be able to prevent the type caused by trachoma infection. If your eyes become red and irritated after you visit an area where trachoma infection is common, seek evaluation and treatment immediately.
Entropion symptoms
The signs and symptoms of entropion result from the friction of your eyelashes and outer eyelid against the surface of your eye. You may experience:
- The feeling that something is in your eye
- Eye redness
- Eye irritation or pain
- Sensitivity to light and wind
- Watery eyes (excessive tearing)
- Mucous discharge and eyelid crusting
- Decreased vision
Entropion diagnosis
Entropion can usually be diagnosed with a routine eye exam and physical. Your doctor may pull on your eyelids during the exam or ask you to blink or close your eyes forcefully. This helps him or her assess your eyelid’s position on the eye, its muscle tone and its tightness.
If your entropion is caused by scar tissue, previous surgery or other conditions, your doctor will examine the surrounding tissue as well.
Entropion treatment
The treatment approach depends on what’s causing your entropion. Nonsurgical treatments are available to relieve symptoms and protect your eye from damage.
When active inflammation or infection causes entropion (spastic entropion), your eyelid may return to its normal alignment as you treat the inflamed or infected eye. But entropion may persist even after the other condition has been treated.
Surgery is generally required to fully correct entropion.
Temporary treatments
Short-term fixes can be useful if you can’t tolerate surgery or you have to delay it. Effective temporary treatments include:
- Soft contact lens. Your eye doctor may suggest you use a type of soft contact lens as a sort of corneal bandage to help ease symptoms. These are available with or without a prescription.
- Stitches that turn the eyelid outward. This procedure can be done in your doctor’s office with local anesthesia. After numbing the eyelid, your doctor places several stitches in specific locations along the affected eyelid. The stitches turn the eyelid outward, and resulting scar tissue keeps it in position even after the stitches are removed. After several months, your eyelid may turn itself back inward. So this technique isn’t a long-term solution.
- Botox. Small amounts of botulinum toxin (Botox) injected in the lower eyelid can turn the eyelid out. You may get a series of injections, with effects lasting up to six months.
- Skin tape. Special transparent skin tape can be applied to your eyelid to keep it from turning in.
Entropion surgery
The type of surgery you have depends on the condition of the tissue surrounding your eyelid and on the cause of your entropion.
If your entropion is age related, your surgeon will likely remove a small part of your lower eyelid. This helps tighten the affected tendons and muscles. You’ll have a few stitches on the outside corner of your eye or just below your lower eyelid.
If you have scar tissue on the inside of your lid or have had trauma or previous surgeries, your surgeon may use a mucous membrane graft using tissue from the roof of your mouth or nasal passages.
Before surgery you’ll receive a local anesthetic to numb your eyelid and the area around it. You may be lightly sedated to make you more comfortable, depending on the type of procedure you’re having and whether it’s done in an outpatient surgical clinic.
After surgery you might need to:
- Use an antibiotic ointment on your eye for one week
- Use cold compresses periodically to decrease bruising and swelling
After surgery you will likely experience:
- Temporary swelling
- Bruising on and around your eye
How long does entropion surgery take to heal
Your eyelid might feel tight after surgery. But as you heal it will become more comfortable. Stitches are usually removed about a week after surgery. You can expect the swelling and bruising to fade in about two weeks.
Entropion repair complications
The most common complication following entropion repair is recurrence. As mentioned prior, transconjunctival involutional entropion repair has a recurrence of 3.3% 14. Cicatricial entropion repair poses a more challenging treatment picture and has a higher rate of recurrence 19. Recurrence can be prevented by aiming for over-correction at time of surgery, but overly aggressive correction of lid rotation may lead to punctual eversion. Ectropion can also result from repairs that attach the inferior lid retractors to the anterior surface of the tarsus rather than the inferior aspect. Overly aggressive shortening of the lower lid retractors or excessive skin removal can produce lower lid retraction and inferior scleral show. Using local anesthesia allows the surgeon to assess lid height, motility and contour during the procedure and make any necessary adjustments promptly to prevent induction of ectropion. Simultaneous correction of horizontal lid laxity can also prevent postoperative ectropion 1. Erb et al 14, noted no incidences of retraction, inferior scleral show or ectropion in a series of 151 eyelid repairs for involutional entropion.
Lid-splitting surgical approaches risk fistula formation. If encountered, these should be excised and repaired 1.
The surgeon should be cognizant of the marginal arcade during entropion repair to prevent necrosis at the lid margin. Any full-thickness incisions through the lid should be made inferior to the inferior margin of the tarsus, at least 4mm inferior to the lid margin, to avoid vascular compromise 1.
Overall, transconjunctival entropion repair has a low rate of complications, with Erb et al 14 noting a 4% rate: stitch abscess and conjunctivochalasis 0.7% each and lateral tarsal strip dehiscence and lateral canthal dystopia.
Entropion home remedies
To relieve the symptoms of entropion until you have surgery, you can try:
- Eye lubricants. Artificial tears and eye ointments help protect your cornea and keep it lubricated.
- Skin tape. Special transparent skin tape can be applied to your eyelid to keep it from turning in. Place one end of the tape near your lower eyelashes, then pull down gently and attach the other end of the tape to your upper cheek. Ask your doctor to demonstrate proper technique and placement of the tape.
- Nowinski TS. 2011. Entropion. In: Tse DT, editor. Color Atlas of Oculoplastic Surgery. 2nd ed. Philadelphia (PA): Lippincott Williams & Wilkins. p 44-53.[↩][↩][↩][↩][↩][↩][↩]
- Iyengar SS, Dresner SC. 2012. Entropion. In: Black EH, Nesi FA, Calvano CJ, Gladstone GJ, Levine MR editors. Smith and Nesi’s Ophthalmic Plastic and Reconstructive Surgery. 3rd ed. New York (NY):Springer. p. 311-315.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Stevens S. Tape correction for lower eyelid entropion. Comm Eye Health. 2012;25(78):36.[↩]
- Osaki T, Osaki MH, Osaki TH. Temporary management of involutional entropion with octyl-2-cyanoacrylate liquid bandage application. Arg Bras Oftalmol. 2010 Mar-Apr;73(2):120-4.[↩]
- Steel DH, Hoh HB, Harrad RA, Collins CR. Botulinum toxin for the temporary treatment of involutional lower lid entropion: a clinical and morphological study. Eye. 1997;11(Pt 4):472-5.[↩][↩]
- Babuccu O. An alternative approach for involutional entropion: a preliminary study. Lasers Med Sci. 2012 Sep;27(5):1009-12.[↩]
- Quickert MH, Rathbun E. Suture repair of entropion. Arch Ophthalmol. 1971 Mar;85(3):304-5.[↩]
- Tsang S, Yau GS, Lee JW, Chu AT, Yuen CY. Surgical outcome of involutional lower eyelid entropion correction using transcutaneous everting sutures in Chines patients. Int Ophthalmol. 2014 Aug;34(4):865-8.[↩][↩]
- Jang SY, Choi SR, Jang JW, Kim SJ, Choi HS. Long-term surgical outcomes of Quickert sutures for involutional lower eyelid entropion. J Craniomaxillofac Surg. 2014 May 14.[↩]
- Scheepers MA, Singh R, Ng J, Zuercher D, Gibson A, Bunce C, Fong K, Michaelides M, Olver J. A randomized controlled trial comparing everting sutures and a lateral tarsal strip for involutional entropion. Ophthalmology. 2010 Feb;117(2):352-5.[↩][↩][↩]
- Balaji K, Balaji V, Kummararaj G. The correction of involutional entropion of eyelid by lateral strip procedure. J Surg Tech Case Rep. 2010 Jul;2(2):64-6.[↩]
- Roberts MA, Baddeley P, Sinclair N, Lane CM. The lower lid diamond: a simple entropion repair to correct both horizontal and lower-lid retractor laxity. Ophthal Plast Reconstr Surg. 2012 Jan-Feb;28(1):44-6.[↩]
- Lee H, Takahashi Y, Ichinose A, Kakizaki H. Comparison of surgical outcomes between simple posterior layer advancement of lower eyelid retractors and combinatin with a lateral tarsal strip procedure for involutional entropion in a Japanese population. Br J Ophthalmol. 2014 May 30.[↩][↩]
- Erb MH, Uzcategui N, Dresner SC. Efficacy and complications of the transconjunctival entropion repair for lower eyelid involutional entropion. Ophthalmology. 2006 Dec;113(12):2351-6.[↩][↩][↩][↩]
- Serin D, Buttanri IB, Karslioglu S, Sevim MS, Buttanri B, Akbaba M. The efficacy of the combined procedure in involutional entropion surgery; a comparative study. Korean J Ophthalmol. 2013 Dec;27(6):405-8.[↩]
- Hatton MP, Raizman M, Foster CS. Exacerbation of undiagnosed ocular cicatricial pemphigoid after repair of involutional entropion. Ophthal Plast Reconstr Surg. 2008 Mar-Apr;24(2):165-6.[↩]
- Milliman AL, Katzen LB, Putterman AM. Cicatricial entropion: an analysis of its treatment with transverse blepharotomy and marginal rotation. Ophthalmic Surg. 1989 Aug;20(8):575-9.[↩]
- Wu AY, Thakker MM, Wladis EJ, Weinberg DA. Eyelash resection procedure for severe, recurrent, or segmental cicatricial entropion. Ophthal Plast Reconstr Surg. 2010 Mar-Apr;26(2):112-6.[↩]
- Bleyen I, Dolman PJ. The Weis procedure for management of trichiasis or cicatricial entropion of either upper or lower eyelids. Br J Ophthalmol. 2009 Dec;93(12):1612-5.[↩][↩]
- Kakizaki H, Malhotra R, Madge SN, Selva D. Lower eyelid anatomy: an update. Ann Plast Surg. 2009 Sep;63(3):344-51.[↩]
- Faria-E-Sousa SJ, de Paula Gomes Vieira M, Silva JV. Uncovering intermittent entropion. Clin Ophthalmol. 2013;7:385-8.[↩][↩]
- Hubbard IH, Kanski JJ. A simple treatment for spastic entropion. Proc R Soc Med. 1973 Feb;66(2):173-4.[↩]
- Winterhoff J, Köhler S, Laskawi R. Botulinum toxin for the treatment of spastic entropion. Case report. HNO. 2013 Jul;61(7):665-7.[↩]
- Pasco NY, Kikkawa DO, Korn BS, Punja KG, Jones MC. Facial nerve paralysis: an unrecognized cause of lower eyelid entropion in the pediatric population. Ophthal Plast Reconstr Surg. 2007 Mar-Apr;23(2):126-9.[↩]
- Maman DY, Taub PJ. Congenital entropion. Ann Plast Surg. 2011 Apr;66(4):351-3.[↩]





{kind=link}