Contents
What is epiglottitis
Epiglottitis is a potentially life-threatening inflammation and swelling of the epiglottis with the potential risk of fatal airway obstruction – blocking the flow of air into your lungs (see Figures 1 and 2) 1. Acute epiglottitis is known to be potentially life-threatening because the special structure and anatomical location of the epiglottis (see Figures 1 and 2) make it prone to severe edema, which can lead to dyspnea and even suffocation, resulting in death 2. In most cases, epiglottitis is caused by infection. Effective management requires rapid diagnosis, airway management, and treatment of the causative agent.
The epiglottis is a flap of tissue that sits beneath the tongue at the back of the throat. Its main function is to close over the windpipe (trachea) while you’re eating, to prevent food entering your airways.
Acute epiglottitis can occur at any age. Epidemiological studies have shown that the number of acute epiglottitis cases has decreased in children due to proper vaccinations, while the number of adult cases has increased significantly 3. Previously, 75%–90% of cases of epiglottitis were caused by Haemophilus influenza type B (Hib), the same bacterium that causes pneumonia, meningitis and infections in the bloodstream. Haemophilus influenzae type b (Hib) bacteria spreads in the same way as the cold or flu virus; the bacteria are in the tiny droplets of saliva and mucus propelled into the air when an infected person coughs or sneezes. You catch the infection by breathing in these droplets or, if the droplets have landed on a surface or object, by touching this surface and then touching your face or mouth. Because of the success of the Hib vaccination programme, epiglottitis is rare in the US, and most cases now occur in adults. Deaths from epiglottitis are also rare, occurring in less than 1 in 100 cases. But infection with group A beta-hemolytic Streptococci has become more frequent after the widespread use of Hemophilus influenzae type B (Hib) vaccination. Hib vaccination, introduced in 1985, significantly reduced the incidence of epiglottitis 4. Routine Hemophilus influenzae type B (Hib) vaccination for infants has made epiglottitis rare, but epiglottitis remains a concern. Cases presenting today show a mixed microbial etiology (other bacteria as well as fungi and virus), with a relative increased incidence in older children 5. A number of other factors can cause the epiglottis to swell — burns from hot liquids, direct injury to your throat and various infections.
Less common causes of acute epiglottitis include:
- other bacterial infections – such as streptococcus pneumoniae (a common cause of pneumonia)
- fungal infections – people with a weakened immune system are most at risk from these types of infection
- viral infections – such as the varicella zoster virus (the virus responsible for chickenpox) and the herpes simplex virus (the virus responsible for cold sores)
- trauma to the throat – such as a blow to the throat, or burning the throat by drinking very hot liquids
- smoking – particularly illegal drugs, such as cannabis or crack cocaine
The clinical features of acute epiglottitis commonly include sore throat, odynophagia [painful swallowing], stridor [high-pitched, wheezing sound caused by obstructed airflow], fever, hoarseness, drooling, hyperpyrexia, and dyspnea [difficult or labored breathing or shortness of breath] 6.
The typical histopathological changes associated with this condition include extensive mucosal or submucosal edema accompanied by neutrophil infiltration and hemorrhage, which are frequently found microscopically. In addition, epiglottic abscess may be observed in some patients with acute epiglottitis (approximately 24% of the cases) 7.
There are differences in trends, occurrences and management of acute epiglottitis between children and adults. There is also more diversity in the cause of epiglottitis in adults 8.
In an 8-year retrospective (1998–2006) review of epiglottitis admissions, Shah et al. 9 found that epiglottitis continues to be a significant entity, with two uniquely vulnerable populations: infants (<1 year old) and the elderly (>85 years old). When examining the pediatric cohort of patients (patients <18 years of age), 34.4% were <1 year of age. This category of age <1 year seemed to have increased in frequency in representing 26.8% of pediatric patients in 1998 to 41.1% in 2006 9. A case of epiglottitis with negative cultures has been reported in a neonate within hours of birth 10.
Epiglottitis is a medical emergency. If you or someone you know suddenly has trouble breathing and swallowing, call your local emergency number for an ambulance or go to the nearest hospital emergency department. Try to keep the person quiet and upright, because this position may make it easier to breathe. Don’t try to examine the person’s throat yourself. This can make matters worse.
Epiglottitis in adults
Although epiglottitis is common in childhood, it has been recognized that its frequency has increased in adults in recent years. The incidence of acute epiglottitis in adults ranges from 0.97 to 3.1 per 100,000, with a mortality of approximately 7.1% 11. The mean annual incidence of acute epiglottitis per 100,000 adults significantly increased from 0.88 (from 1986 to 1990) to 2.1 (from 1991 to 1995) and to 3.1 (from 1996 to 2000) 11. This rise seems to be unrelated to Hemophilus influenzae type b infection, but related to miscellaneous pathogenic bacteria. The number of epiglottic abscesses increased concomitantly with a rise in the incidence of acute epiglottitis 11. In adults, a more diverse microbiological etiology is found with often negative sputum cultures and negative blood cultures to Hemophilus influenzae type B (Hib). Some cases of epiglottitis have been attributed to Candida spp.
Acute epiglottitis in adults, it is common in males between the age of 30 and 70 years 12. The upper airway is more rigid and wider in adults than in pediatric patients, so that adults have a lower risk of upper airway obstruction. However, the reported mortality rate is 18%–21% 13. In adults, epiglottitis can easily be overlooked due to its equivocal initial symptoms and rarity. Therefore, it can sometimes be life-threatening and lead rapidly to upper airway obstruction.
The most common symptoms of acute epiglottitis in adults are odynophagia, difficulty in swallowing secretions, increased oral saliva, sore throat, dyspnea, muffled voice, and stridor 14. Although epiglottitis is mainly caused by bacterial infections, noninfectious agents such as viral, caustic, and thermal injuries can also be causes 15. Diagnosis is best made by examination using direct, indirect, or flexible laryngoscopy.
Noninfectious causes of epiglottitis may include trauma by foreign objects, inhalation and chemical burns, or are associated with systemic disease or reactions to chemotherapy. The presence of dysphagia, drooling and stridor subsequent to thermal or caustic injury should alert the treating physician to the possibility of injury to the supraglottic structures with resultant epiglottitis. Epiglottic injuries of this type should be suspected in patients with mental disorders or communication difficulties 16. In young adults, acute epiglottitis has been described as being caused by inhalation of heated objects when smoking illicit drugs; the symptoms, signs, X-ray and laryngoscopic findings are similar to infectious epiglottitis 17. These adults present many of the features seen in acute infectious epiglottitis, and should be handled with the same consideration for potential upper airway obstruction.
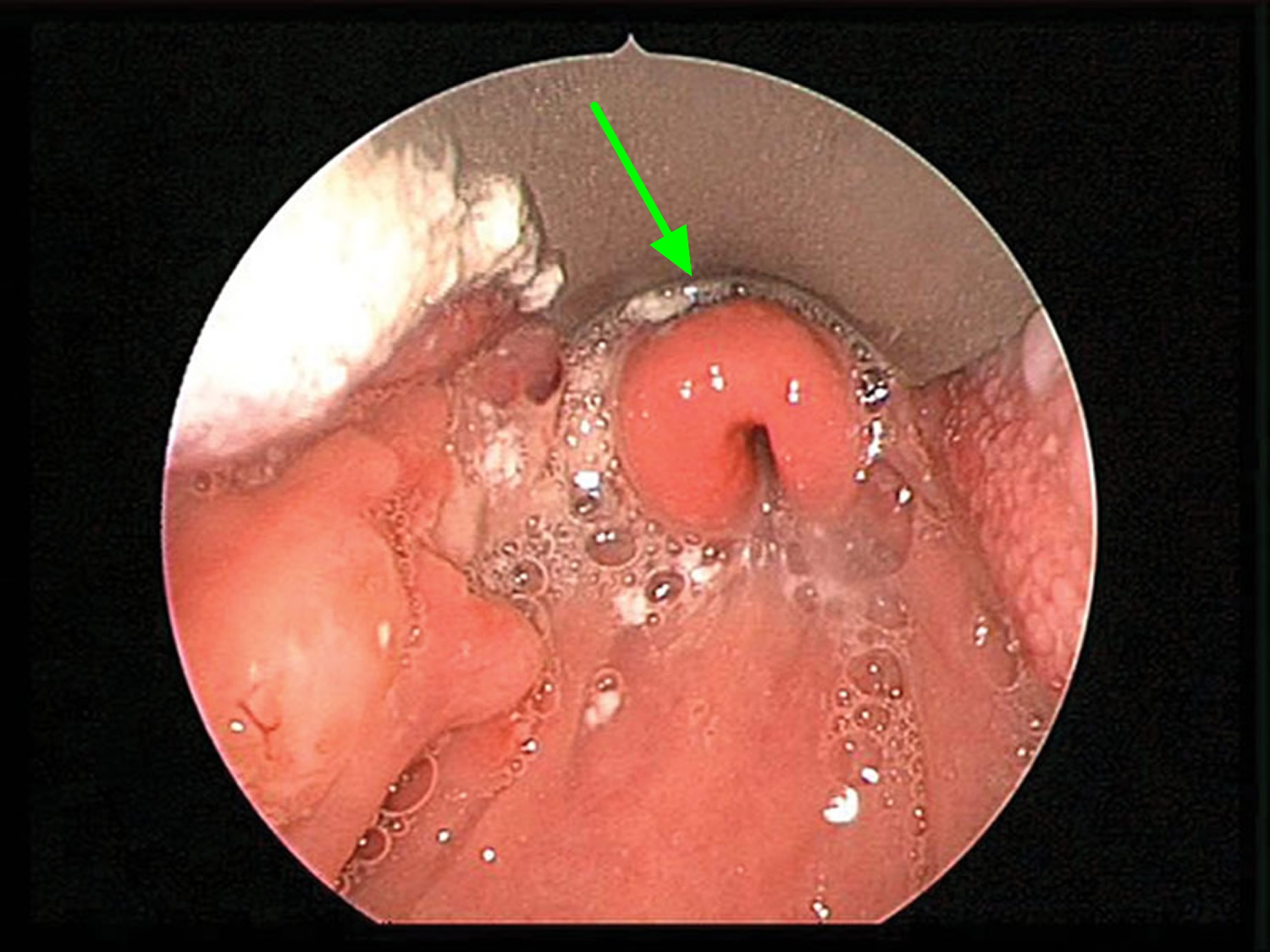
Figure 1. Larynx and pharynx anatomy
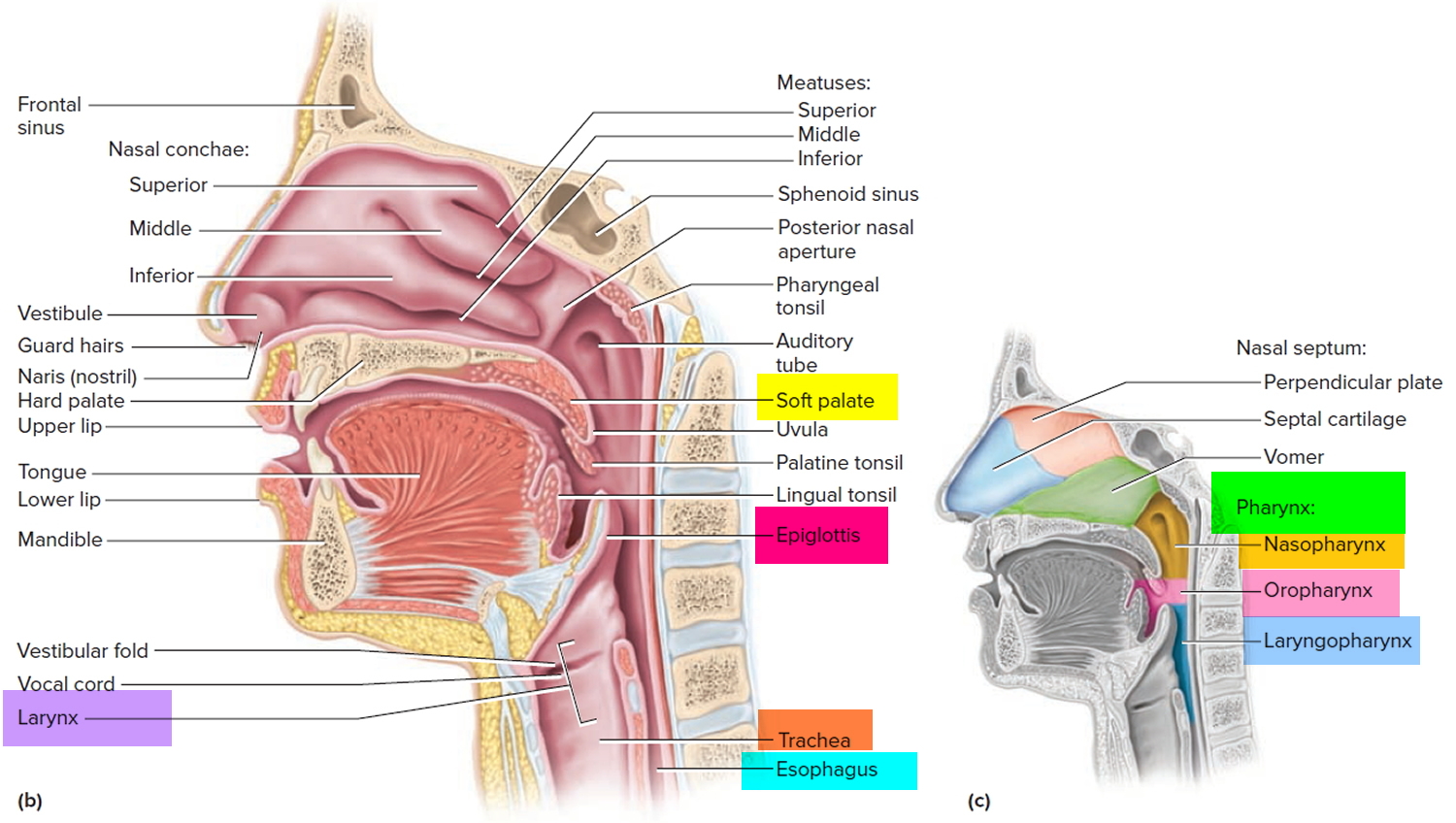
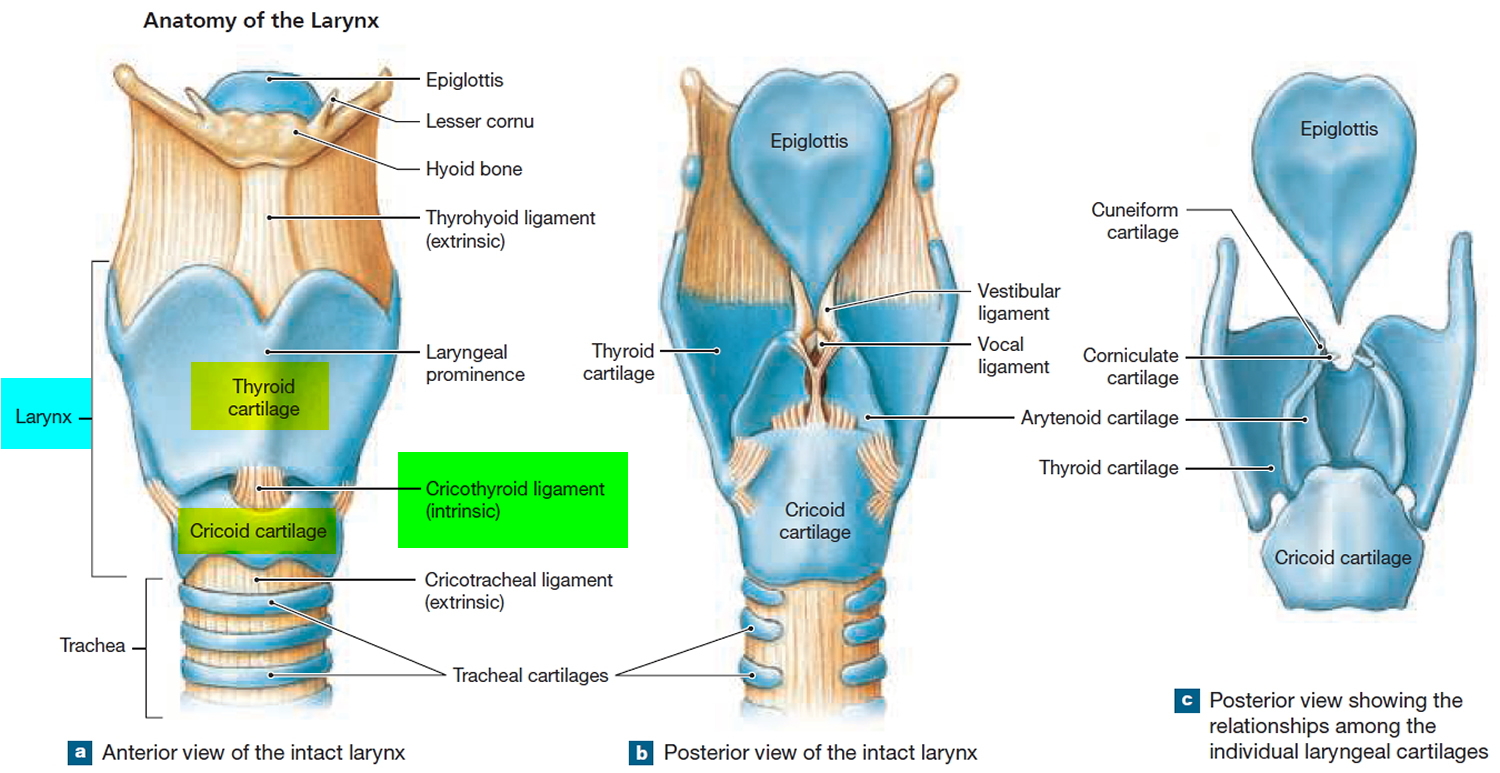
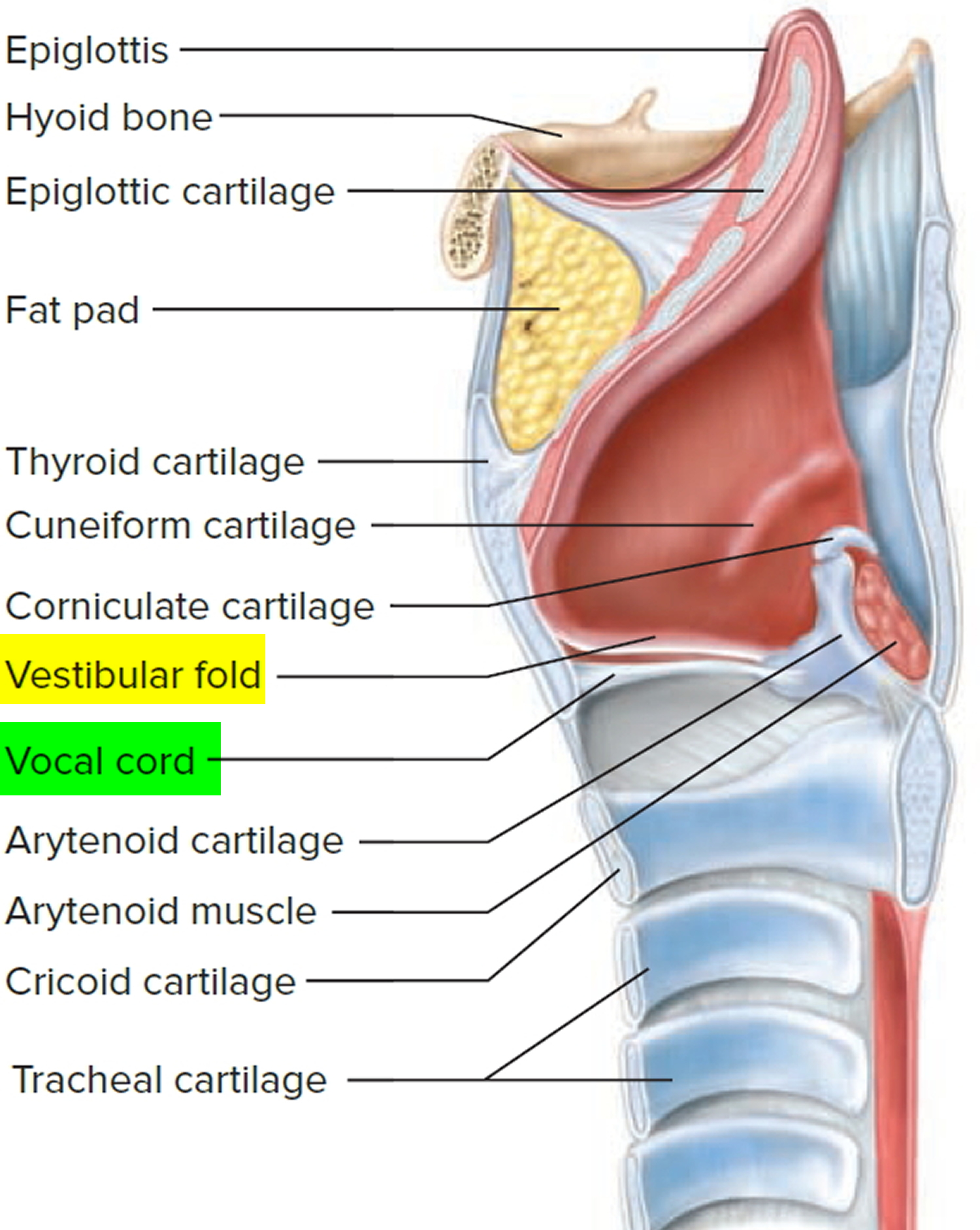
Figure 2. Larynx anatomy
Croup vs epiglottitis
Croup is a viral laryngotracheobronchitis (usually caused by the Hemophilus parainfluenzae virus) that causes swelling of the windpipe (trachea), the airways to the lungs (the bronchi) and the vocal cords (larynx or voice box). This swelling makes the airway narrower, so it is harder to breathe. Croup causes difficulty breathing, a seal barking cough, and a hoarse voice. The cause is usually a virus, often parainfluenza virus. Other causes include allergies and reflux. Treatment of croup includes oxygen, steroids (dexamethasone 0.6 mg/kg PO/IM) and epinephrine (to relieve airway edema and decrease airway resistance due to swelling).
Epiglottitis is an inflammation of the epiglottis due to an infectious process. It can involve other structures such as the arytenoid, false cords and posterior tongue leading to airway obstruction. Most often epiglottitis is bacterial in origin due to Hemophilus influenzae type B (Hib), it affects children between 2 and 5, however the median age is increasing over the past decade. It presents acutely in otherwise healthy children with a fever as high as 104 °F (40 °C). Epiglottic inflammation occurs quickly with the child sitting forward to use the accessory muscles of respiration and pain in the throat. Salivation is prominent with difficulty swallowing. Treatment includes keeping a parent in attendance at all times to keep the child calm, oxygen, sitting position, immediate intubation. Diagnosis is confirmed through radiologic studies showing the steeple sign representing a uniform narrowing of the subglottic airway by inflammation.
Croup is more prevalent during the wintertime, while there is no seasonal predilection to epiglottitis. Croup also has a more gradual onset than acute epiglottitis, and is commonly associated with low-grade fever. Although both acute epiglottitis and croup share the same symptoms of inspiratory stridor, suprasternal, intercostal and substernal retractions and hoarseness, differentiation in early illness is possible by additional observation of seal barking cough and absence of drooling and dysphagia in croup and by the additional observation of drooling and dysphagia with absence of coughing in epiglottitis. Additional reliable signs of epiglottitis are a preference to sit, dysphagia and refusal to swallow 18. Unlike croup, where onset is insidious over a period of 2 to 3 days, epiglottitis patients tend to experience acute onset of symptoms. In one series, while both croup and epiglottitis were associated with acute stridor, croup was also associated with coughing and no drooling, while epiglottitis was associated with drooling and the lack of coughing 19.
Epiglottitis complications
Epiglottitis can cause a number of complications, including:
- Respiratory failure. The epiglottis is a small, movable “lid” just above the larynx that prevents food and drink from entering your windpipe. But if the epiglottis becomes swollen — either from infection or from injury — the airway narrows and may become completely blocked. This can lead to respiratory failure — a life-threatening condition in which the level of oxygen in the blood drops dangerously low or the level of carbon dioxide becomes excessively high.
- Spreading infection. Sometimes the bacteria that cause epiglottitis cause infections elsewhere in the body, such as pneumonia, meningitis or a blood infection (sepsis).
Epiglottitis can lead to airway loss and death. Epiglottic abscess has been found to occur in up to 24% of patients 20. The abscesses can often be detected using a computed tomography scan, while a magnetic resonance imaging shows obliteration of the surrounding fat planes. These scans require the patient to be in a supine position, and with this condition, respiratory distress can be greater when the patient is supine. If computed tomography or magnetic resonance imaging is felt to be necessary in a complicated patient, consideration should be given to securing the airway before placing these patients in the supine position in an imaging department. Likewise, naso-fiberoptic exam can also assess edema and abscesses even when performed on an intubated patient. Patients with epiglottic abscess often require drainage of the abscess in addition to intravenous antibiotics. Descending necrotizing mediastinitis has also been reported in cases of epiglottitis 21. These patients often require drainage of the mediastinum in addition to drainage of the primary abscess and airway management via tracheotomy. Immunocompromised patients are at a higher risk of these complications, and physicians must therefore use broad-spectrum antibiotics as well as debridement, as needed.
Epiglottitis causes
Epiglottitis is can be caused by an infection or an injury.
Infection
In the past, a common cause of swelling and inflammation of the epiglottis and surrounding tissues was infection with Haemophilus influenzae type b (Hib) bacteria. Haemophilus influenzae type b (Hib) is responsible for a number of serious conditions, the most common of which is meningitis. This is now much less common in developed countries due to Haemophilus influenzae type b (Hib) immunization in children.
Haemophilus influenzae type b (Hib) spreads through infected droplets coughed or sneezed into the air. It’s possible to harbor Hib in your nose and throat without becoming sick — though you still have the potential to spread the bacteria to others.
In adults, other bacteria and viruses also can cause inflammation of the epiglottis, including:
- Streptococcus pneumoniae (pneumococcus), another bacterium that can cause meningitis, pneumonia, ear infections and blood infection (septicemia)
- Streptococcus A, B and C, a group of bacteria that also can cause diseases ranging from strep throat to blood infections
- Staphylococcus aureus, a bacterium that causes skin infections and other diseases including pneumonia and toxic shock syndrome
Injury
Physical injury, such as a direct blow to the throat, can cause epiglottitis. So can burns from drinking very hot or caustic liquids.
You also may develop signs and symptoms similar to those of epiglottitis if you:
- Swallow a chemical that burns your throat
- Swallow a foreign object
- Smoke drugs, such as crack cocaine
Risk factors for epiglottitis
Certain factors increase the risk of developing epiglottitis, including:
- Being male. Epiglottitis affects more males than females.
- Having a weakened immune system. If your immune system has been weakened by illness or medication, you’re more susceptible to the bacterial infections that may cause epiglottitis.
- Lacking adequate vaccination. Delayed or skipped immunizations can leave a child vulnerable to Hib and increases the risk of epiglottitis.
Epiglottitis prevention
Haemophilus influenzae type b (Hib) vaccine
The most effective way to prevent your child getting epiglottitis is to make sure their vaccinations are up to date.
Children are particularly vulnerable to a Hib infection, because they have an underdeveloped immune system.
Children should receive their Hib as part of the 5 in 1 DTaP/IPV/Hib vaccine, which also protects against diphtheria, tetanus, whooping cough and polio.
Immunization with the Hib vaccine is an effective way to prevent epiglottitis caused by Hib. Children should receive three doses of the vaccine: one at two months, one when they are three months and one when they are four months old. This is followed by an additional Hib/Men C “booster” vaccine at 12 months.
In the United States, children usually receive the vaccine in three or four doses:
- At 2 months
- At 4 months
- At 6 months if your child is being given the four-dose vaccine
- At 12 to 15 months
The Hib vaccine is generally not given to children older than age 5 or to adults because they’re less likely to develop Hib infection. But the Centers for Disease Control and Prevention recommends the vaccine for older children and adults whose immune systems have been weakened by:
- Sickle cell disease
- HIV/AIDS
- Spleen removal
- Chemotherapy
- Medications to prevent rejection of organ or bone marrow transplants
Haemophilus influenzae type b (Hib) vaccine side effects
- Allergic reaction. Seek immediate medical help if you have an allergic reaction. Though rare, an allergic reaction may cause difficulty breathing, wheezing, hives, weakness, a rapid heartbeat or dizziness within minutes or a few hours after the shot.
- Possible mild side effects. These include redness, warmth, swelling or pain at the injection site, and a fever.
Commonsense precautions
Of course, the Hib vaccine doesn’t offer guarantees. Immunized children have been known to develop epiglottitis — and other germs can cause epiglottitis, too. That’s where commonsense precautions come in:
- Don’t share personal items.
- Wash your hands frequently.
- Use an alcohol-based hand sanitizer if soap and water aren’t available.
Epiglottitis symptoms
The symptoms of epiglottitis usually develop quickly and get rapidly worse, although they can develop over a few days in older children and adults.
The typical presentation in epiglottitis includes acute occurrence of high fever, severe sore throat and difficulty in swallowing with the sitting up and leaning forward position in order to enhance airflow. There is usually drooling because of difficulty and pain on swallowing. Acute epiglottitis usually leads to generalized toxemia. The most common differential diagnosis is croup and a foreign body in the airway. A late referral to an acute care setting with its serious consequences may result from difficulty in differentiation between acute epiglottitis and less urgent causes of a sore throat, shortness of breath and dysphagia. Antibiotic therapy is usually initiated without preceding bacterial culture, with the consequence of negative cultures at admission.
Epiglottitis symptoms include:
- a severe sore throat
- difficulty and pain when swallowing
- difficulty breathing, which may improve when leaning forwards
- breathing that sounds abnormal and high-pitched (stridor)
- a high temperature (fever) of 38 °C (100.4 °F) or above
- irritability and restlessness
- muffled or hoarse voice
- drooling
The main symptoms of epiglottitis in young children are breathing difficulties, stridor and a hoarse voice. In adults and older children, the main signs are a severe sore throat, swallowing difficulties and drooling.
Difficulty in breathing and stridor are common signs of epiglottitis in children, but are less frequent in adults. The most common presenting symptom in adults is odynophagia [painful swallowing] (100%), followed by dysphagia [difficulty in swallowing] (85%) and voice change (75%) 22. In adults, stridor is regarded as a warning sign for occlusion of the upper airway. Stridor, tachycardia, tachypnea, rapid onset of symptoms and a “thumb-sign” (see Figures 3 and 4 below) present in 79% of the cases on lateral X-rays of the neck are significant predictors for imminent airway compromise with rapid clinical deterioration 23.
Symptoms in children
In children, signs and symptoms of epiglottitis may develop within a matter of hours, including:
- Fever
- Severe sore throat
- Abnormal, high-pitched sound when breathing in (stridor)
- Difficult and painful swallowing
- Drooling
- Anxious, restless behavior
- Greater comfort when sitting up or leaning forward
Epiglottitis can cause a life-threatening airway emergency. Patients with epiglottitis usually present with a generalized toxemia, including high fevers, severe sore throat, and difficulty swallowing. Stridor, if present, is usually inspiratory. The patient may be sitting up and leaning forward in the sniffing position, breathing with an open mouth and a protruding tongue. The child frequently drools because of difficulty and pain on swallowing. This “tripod position” may not be present in the older child/adult presenting with epiglottitis. Findings may only include subtle signs of respiratory difficulties, such as the inability to lie flat, voice changes, and dysphagia. Epiglottitis patients tend to experience acute onset of symptoms. In one series, while both croup and epiglottitis were associated with acute stridor, croup was also associated with coughing and no drooling, while epiglottitis was associated with drooling and the lack of coughing.6
Symptoms in adults
For adults, signs and symptoms may develop more slowly, over days rather than hours. Signs and symptoms may include:
- Severe sore throat
- Fever
- A muffled or hoarse voice
- Abnormal, high-pitched sound when breathing in (stridor)
- Difficulty breathing
- Difficulty swallowing
- Drooling
Supraglottitis, or inflammation of the supraglottic larynx, seen in adults, has a different presentation than epiglottitis in children. Adults with supraglottitis have predominant symptoms of odynophagia, dysphagia, and voice changes out of proportion to pharyngeal inflammation. Childhood epiglottitis—muffled voice, drooling, dyspnea, stridor, and cough—occurs in less than 50% of adults 24. Adults may also experience fever, toxic appearance, cervical lymphadenopathy, and anterior neck and chest cellulitis. Guardiani et al. 25, based on a 10-yr study of 60 adults and 1 child, described odynophagia (painful swallowing) (100% of patients) as the most common symptom, followed by difficulty swallowing (85%) and voice changes (74%). The presentation of adult supraglottitis peaks at 42 to 48 yr of age, with a male predilection of 2.5:1 26. This “tripod position” may not be present in the older child/adult presenting with epiglottitis.
Epiglottitis diagnosis
If your doctor suspects epiglottitis, the first priority is to ensure that your or your child’s airway is open and that enough oxygen is getting through.
Initial test
A pulse oximeter is a device that estimates blood oxygen levels. This device:
- Clips onto a finger
- Measures an estimation of the saturation of oxygen in your blood
If oxygen saturation levels drop too low, you or your child may need help breathing.
Tests after stabilizing breathing
- Throat examination. Using a flexible fiber-optic-lighted tube, the doctor may look down your or your child’s throat to see what’s causing the symptoms. A local anesthetic can help relieve any discomfort. In case of the diagnosis of epiglottitis, a fibreoptic nasal intubation or rigid bronchoscopy using an endotracheal tube with substantially reduced diameter is preferred. Because of the risk of inducing laryngeal spasm and/or total airway obstruction, examination of the pharynx and larynx should be attempted only in an area with adequate equipment and staff prepared to intervene should upper airway obstruction develop, ideally, in the operating room.
- Chest or neck X-ray. Because of the danger of sudden breathing problems, children may have X-rays taken at their bedside rather than in the radiology department — but only after the airway is protected. With epiglottitis, the X-ray may reveal what looks like a thumbprint in the neck, an indication of an enlarged epiglottis.
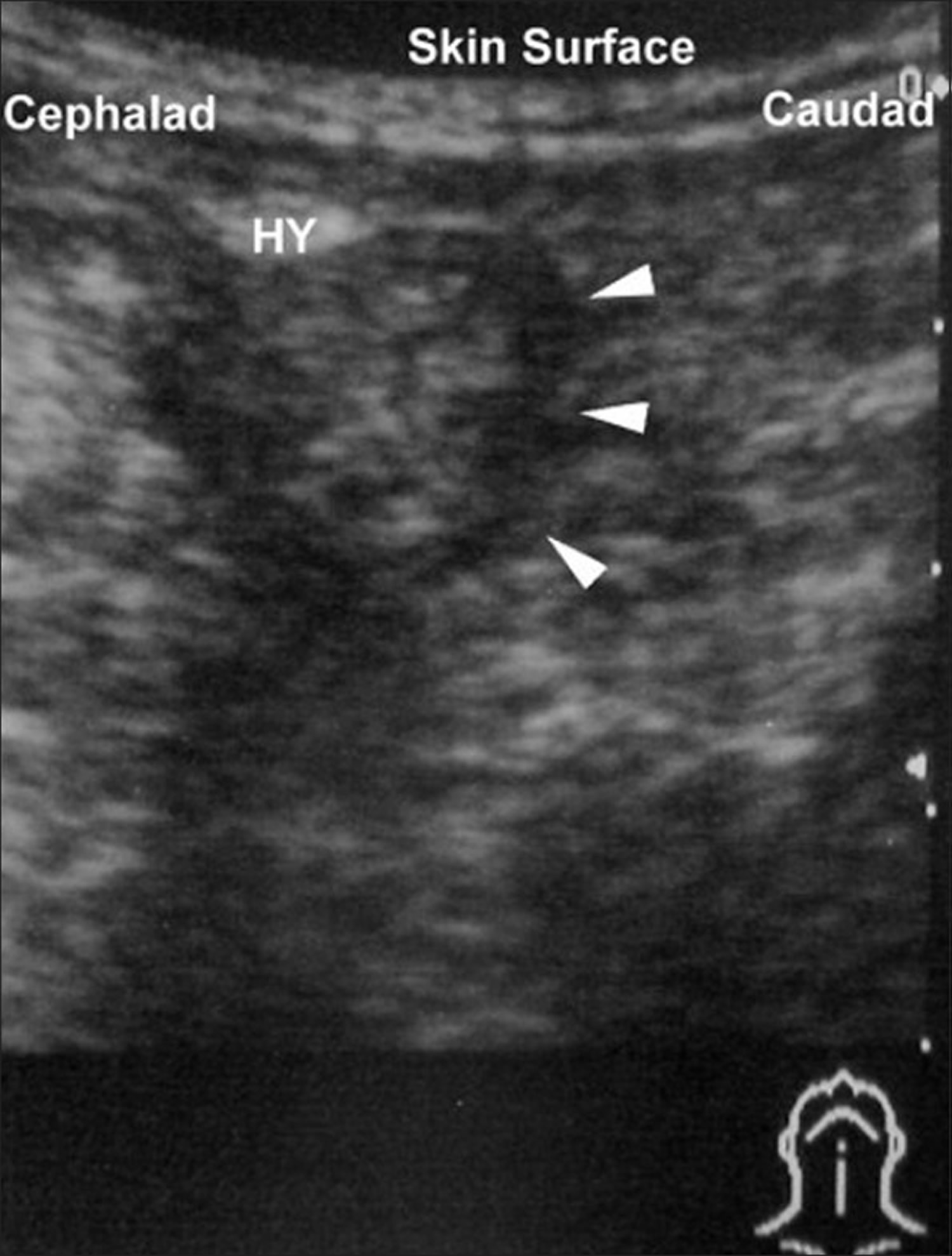
- Ultrasonography has been described as a way to investigate the epiglottis by visualization of the “alphabet P sign” in a longitudinal view through the thyrohyoid membrane (Figure 5) 27.
- Throat culture and blood tests. For the culture, the epiglottis is wiped with a cotton swab and the tissue sample is checked for Hib. Blood cultures are usually taken because bacteremia — a severe bloodstream infection — may accompany epiglottitis.
In acute epiglottitis, the radiological “thumb sign” (Figures 3 and 4) is indicative of severe inflammation of the epiglottis with potential for irrevocable loss of the airway. The thumb sign in epiglottitis is a manifestation of swelling and enlarged epiglottis which is seen on lateral soft-tissue radiograph of the neck, and it suggests a diagnosis of acute infectious epiglottitis. This is the radiographic corollary of the omega sign 28.
Figure 3. Thumb sign epiglottitis (adult)
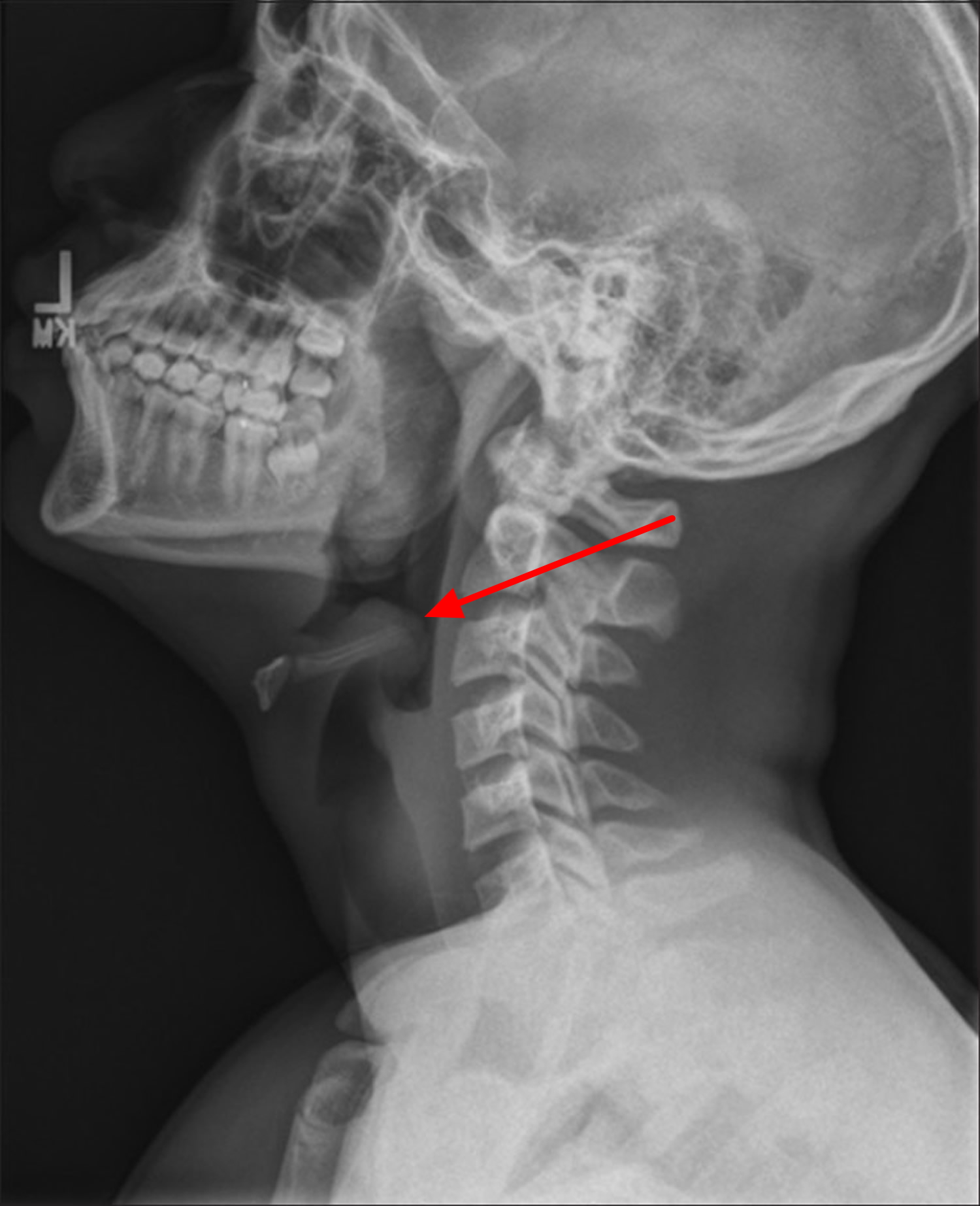
Figure 4. Thumb sign epiglottitis (child)
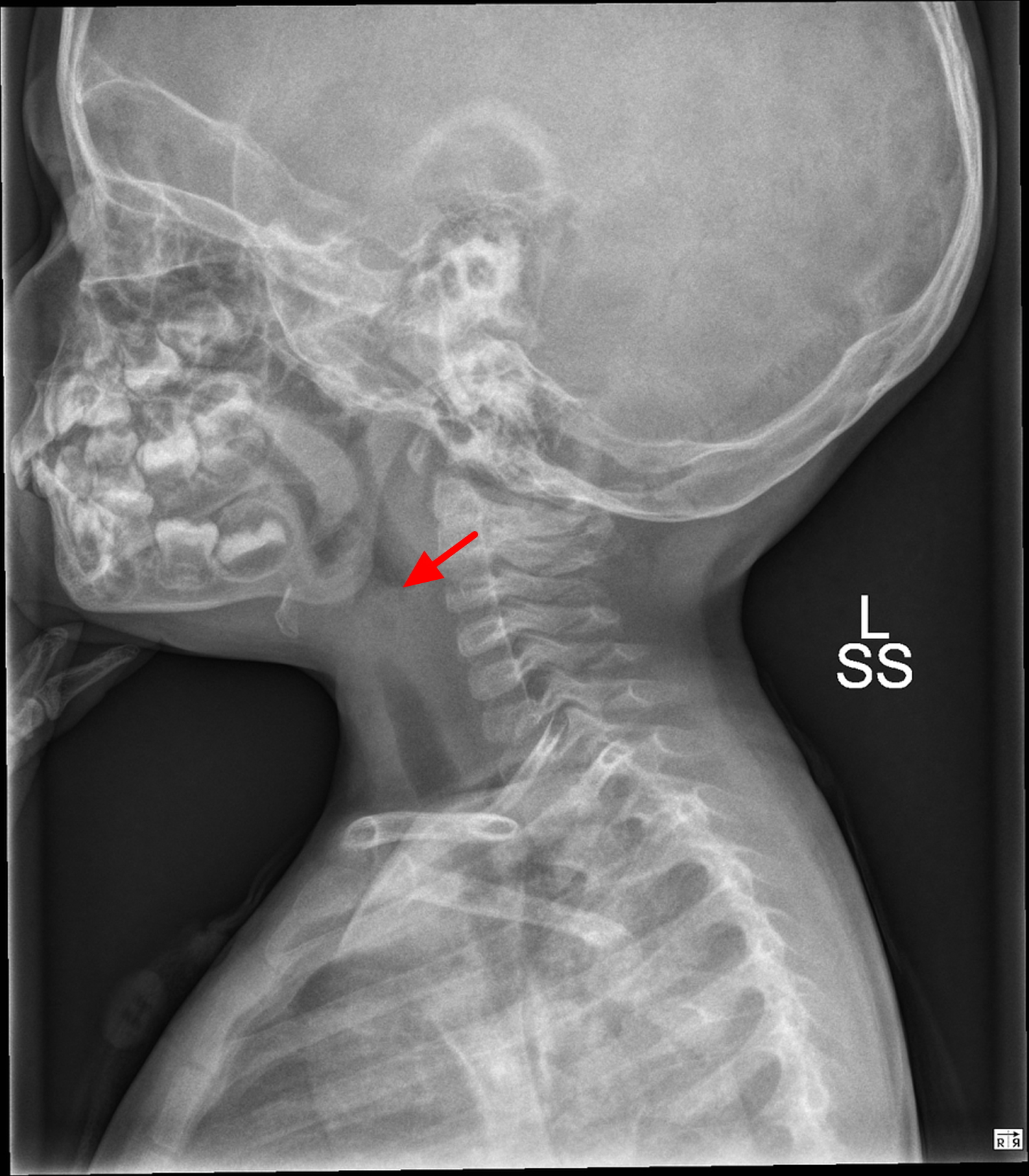
Figure 5. Epiglottitis ultrasonogram – note “Alphabet P sign” formed by acoustic shadow of hyoid bone (HY), swollen epiglottis (pointed by white arrows)
Epiglottitis treatment
Patients with signs of an advancing upper airway obstruction, consistent with an acute epiglottitis, should be treated as a medical and an airway emergency. In the presence of respiratory distress, diagnostic procedures and radiography are not indicated, and securing the airway should be prioritized.
Treatment of epiglottitis involves first making sure you or your child can breathe, and then treating any identified infection.
Helping you breathe
The first priority in treating epiglottitis is ensuring that you or your child is receiving enough air. This may mean:
- Wearing a mask. The mask delivers oxygen to the lungs.
- Having a breathing tube placed into the windpipe through the nose or mouth (tracheal intubation). The tube must remain in place until the swelling in your or your child’s throat has decreased — sometimes for several days.
- Inserting a needle into the trachea (needle tracheostomy). In extreme cases or if more conservative measures fail, the doctor may need to create an emergency airway by inserting a needle directly into an area of cartilage in your or your child’s trachea. This procedure allows air into your lungs while bypassing the larynx.
Tracheal intubation of a patient with epiglottitis must be regarded as a potentially difficult procedure 29. It should be done in strict monitored conditions, i.e. in the operating room, while maintaining spontaneous ventilation. The readiness of a team capable of performing an immediate tracheotomy should be verified. The patient should be transferred to the operating room under the supervision of an experienced anesthesiologist and surgeon 29. The induction may be performed with the patient sitting upright. Forcing the child/patient into a supine position may precipitate acute airway obstruction. Anesthesia induction with achievement of a deep level of anesthesia and maintenance of spontaneous ventilation has been described as the method of choice. The amount of time necessary to produce deep anesthesia using an inhalation induction may be increased secondary to airway obstruction and may necessitate increasing gas concentration. Capnography with exhaled gas analysis is useful in determining anesthetic depth. Muscle relaxants are avoided and spontaneous ventilation should be maintained. The patient should be transferred sedated to an intensive care unit (ICU) after securing the airway. Intravenous sedation should ideally allow spontaneous ventilation. Tracheal extubation should be preceded by a cuff leak test with a deflated cuff and, usually, a second look by direct laryngoscopy with deep sedation or general anesthesia. Complications of acute epiglottitis may include deep neck space infection, recurrent illness and vocal granuloma 30. Dexamethasone treatment or budesonide aerosols could be used in an attempt to limit pharyngeal edema and thereby reduce the obstruction. The use of corticosteroids has been associated with shorter ICU and overall length of stay, with an average overall length of stay of 3.8 days in adults 31.
Once the airways have been secured and the person is able to breathe unrestricted, a more comfortable and convenient way of assisting breathing may be found. This is usually achieved by threading a tube through the nose and into the windpipe.
Fluids will be supplied through a drip into one of your veins, until the person is able to swallow.
Once this has been achieved and the situation is thought to be safe, some tests may be carried out, such as:
- a fibre-optic laryngoscopy – a flexible tube with a camera attached to one end (laryngoscope) is used to examine the throat
- a throat swab – to test for any bacteria or viruses
- blood tests – to check the number of white blood cells (a high number indicates there may an infection) and to identify any traces of bacteria or viruses in the blood
- an X-ray or a computerised tomography (CT) scan – sometimes used to check the level of swelling
The underlying infection will then be treated with a course of antibiotics, and most people with epiglottitis are well enough to leave hospital after five to seven days.
With prompt treatment, most people recover from epiglottitis after about a week and are usually well enough to leave hospital after five to seven days.
Treating infection
If your epiglottitis is related to an infection, intravenous antibiotics will be given once you or your child is getting enough air.
- Broad-spectrum antibiotic. Because of the need for quick treatment, rather than wait for the results of the blood and tissue cultures, you or your child is likely to be treated with a broad-spectrum drug.
- More-targeted antibiotic. The drug may be changed later, depending on what’s causing the epiglottitis.
- Chen C, Natarajan M, Bianchi D, Aue G, Powers JH. Acute Epiglottitis in the Immunocompromised Host: Case Report and Review of the Literature. Open Forum Infectious Diseases. 2018;5(3):ofy038. doi:10.1093/ofid/ofy038. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5846294/[↩]
- Pathological characteristics of the epiglottis relevant to acute epiglottitis. Sato S, Kuratomi Y, Inokuchi A. Auris Nasus Larynx. 2012 Oct; 39(5):507-11. https://www.ncbi.nlm.nih.gov/pubmed/22113103/[↩]
- Acute epiglottitis: analysis of factors associated with airway intervention. Katori H, Tsukuda M. J Laryngol Otol. 2005 Dec; 119(12):967-72. https://www.ncbi.nlm.nih.gov/pubmed/16354360/[↩]
- Epiglottitis in the United States: national trends, variances, prognosis, and management. Shah RK, Stocks C. Laryngoscope. 2010 Jun; 120(6):1256-62. https://www.ncbi.nlm.nih.gov/pubmed/20513048/[↩]
- Changing patterns in pediatric supraglottitis: a multi-institutional review, 1980 to 1992. Laryngoscope. 1994 Nov;104(11 Pt 1):1314-22. https://www.ncbi.nlm.nih.gov/pubmed/7968159/[↩]
- Adult epiglottitis. Shepherd M, Kidney E. Accid Emerg Nurs. 2004 Jan; 12(1):28-30. https://www.ncbi.nlm.nih.gov/pubmed/14700569/[↩]
- Four cases of acute epiglottitis with a peritonsillar abscess. Ito K, Chitose H, Koganemaru M. Auris Nasus Larynx. 2011 Apr; 38(2):284-8. https://www.ncbi.nlm.nih.gov/pubmed/20800396/[↩]
- Mathoera RB, Wever PC, van Dorsten FR, Balter SG, de Jager CP. Epiglottitis in the adult patient. Neth J Med. 2008;66:373–7. https://www.ncbi.nlm.nih.gov/pubmed/18931398[↩]
- Shah RK, Stocks C. Epiglottitis in the United States: National Trends, Variances, Prognosis and Management. Laryngoscope. 2010;120:1256–62. https://www.ncbi.nlm.nih.gov/pubmed/20513048[↩][↩]
- Ducic Y, O’ Flaherty P, Walker CR, Bernard P. Epiglottitis diagnosed within hours of birth. Am J Otolaryngol. 1997;18:224–5 https://www.ncbi.nlm.nih.gov/pubmed/9164630[↩]
- Berger G, Landau T, Berger S, Finkelstein Y, Bernheim J, Ophir D. The rising incidence of adult acute epiglottitis and epiglottic abscess. Am J Otolaryngoscopy. 2003;24:374–83 https://www.ncbi.nlm.nih.gov/pubmed/14608569[↩][↩][↩]
- Acute epiglottitis in adults. Analysis of 129 cases. Frantz TD, Rasgon BM, Quesenberry CP Jr. JAMA. 1994 Nov 2; 272(17):1358-60.https://www.ncbi.nlm.nih.gov/pubmed/7933397/[↩]
- Al-Qudah M, Shetty S, Alomari M, Alqdah M. Acute adult supraglottitis: current management and treatment. South Med J. 2010;103:800–4. https://www.ncbi.nlm.nih.gov/pubmed/20622745[↩]
- Hafidh MA, Sheahan P, Keogh I, Walsh RM. Acute epiglottitis in adults: a recent experience with 10 cases. J Laryngol Otol. 2006;120:310–3 https://www.ncbi.nlm.nih.gov/pubmed/16623975[↩]
- Alpay HC, Keles E, Orhan I, Yalcın S. Chemical injury of larynx after organophosphate ingestion. Otolaryngol Head Neck Surg. 2009;140:604–5. https://www.ncbi.nlm.nih.gov/pubmed/19328356[↩]
- Kornak JM, Freije JE, Campbell BH. Caustic and thermal epiglottitis in the adult. Otolaryngol Head Neck Surg. 1996;114:310–2. https://www.ncbi.nlm.nih.gov/pubmed/8637759[↩]
- Mayo-Smith MF, Spinale J. Thermal epiglottitis in adults: A new complication of illicit drug use. J Emerg Med. 1997;15:483–5. https://www.ncbi.nlm.nih.gov/pubmed/9279700[↩]
- Tibballs J, Watson T. Symptoms and signs differentiating croup and epiglottitis. J Paediatr Child Health. 2011;47:77–82. https://www.ncbi.nlm.nih.gov/pubmed/21091577[↩]
- Tibballs, J, Watson, T Symptoms and signs differentiating croup and epiglottitis.. J Paediatr Child Health. (2011). 47 77–82 https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1440-1754.2010.01892.x[↩]
- Ozanne, A, Marsot-Dupuch, K, Ducreux, D, Meyer, B, Lasjaunias, P Acute epiglottitis: MRI.. Neuroradiology. (2004). 46 153–5 https://www.ncbi.nlm.nih.gov/pubmed/14726983[↩]
- Huopio, M, Kokkonen, J, Heino, S, Valtonen, M, Hakala, T [Epiglottitis and necrotizing mediastinitis in a middle-aged man].. Duodecim. (2014). 130 503–6 https://www.ncbi.nlm.nih.gov/pubmed/24730202[↩]
- Guardiani E, Bliss M, Harley E. Supraglottitis in the era following widespread immunization against Haemophilus influenzae type B: Evolving principles in diagnosis and management. Laryngoscope. 2010;120:2183–8 https://www.ncbi.nlm.nih.gov/pubmed/20925091[↩]
- Chan KO, Pang YT, Tan KK. Acute epiglottitis in the tropics: Is it an adult disease? J Laryngol Otol. 2001;115:715–8. https://www.ncbi.nlm.nih.gov/pubmed/11564297[↩]
- Mayo-Smith, MF, Spinale, JW, Donskey, CJ, Yukawa, M, Li, RH, Schiffman, FJ Acute epiglottitis. An 18-year experience in Rhode Island.. Chest. (1995). 108 1640–7 http://journal.chestnet.org/article/S0012-3692(15)45122-0/fulltext[↩]
- Guardiani, E, Bliss, M, Harley, E Supraglottitis in the era following widespread immunization against Haemophilus influenzae type B: Evolving principles in diagnosis and management.. Laryngoscope. (2010). 120 2183–8 https://www.ncbi.nlm.nih.gov/pubmed/20925091[↩]
- Al-Qudah, M, Shetty, S, Alomari, M, Alqdah, M Acute adult supraglottitis: Current management and treatment.. South Med J. (2010). 103 800–4 https://www.ncbi.nlm.nih.gov/pubmed/20622745[↩]
- Hung TY, Li S, Chen PS, Wu LT, Yang YJ, Tseng LM, et al. Bedside ultrasonography as a safe and effective tool to diagnose acute epiglottitis. Am J Emerg Med. 2011;29:359.e1–3. Epub 2010 Aug 1. https://www.ncbi.nlm.nih.gov/pubmed/20674236[↩]
- Grover C. Images in clinical medicine. “Thumb sign” of epiglottitis. N. Engl. J. Med. 2011;365 (5): 447. doi:10.1056/NEJMicm1009990 http://www.nejm.org/doi/full/10.1056/NEJMicm1009990[↩]
- Abdallah C. Acute epiglottitis: Trends, diagnosis and management. Saudi Journal of Anaesthesia. 2012;6(3):279-281. doi:10.4103/1658-354X.101222. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3498669/[↩][↩]
- Shah RK, Roberson DW, Jones DT. Epiglottitis in the Hemophilus influenzae type B vaccine era: Changing trends. Laryngoscope. 2004;114:557–60 https://www.ncbi.nlm.nih.gov/pubmed/15091234[↩]
- Guardiani E, Bliss M, Harley E. Supraglottitis in the era following widespread immunization against Haemophilus influenzae type B: Evolving principles in diagnosis and management. Laryngoscope. 2010;120:2183–8. https://www.ncbi.nlm.nih.gov/pubmed/20925091[↩]





{kind=link}