Contents
What is erythropoiesis
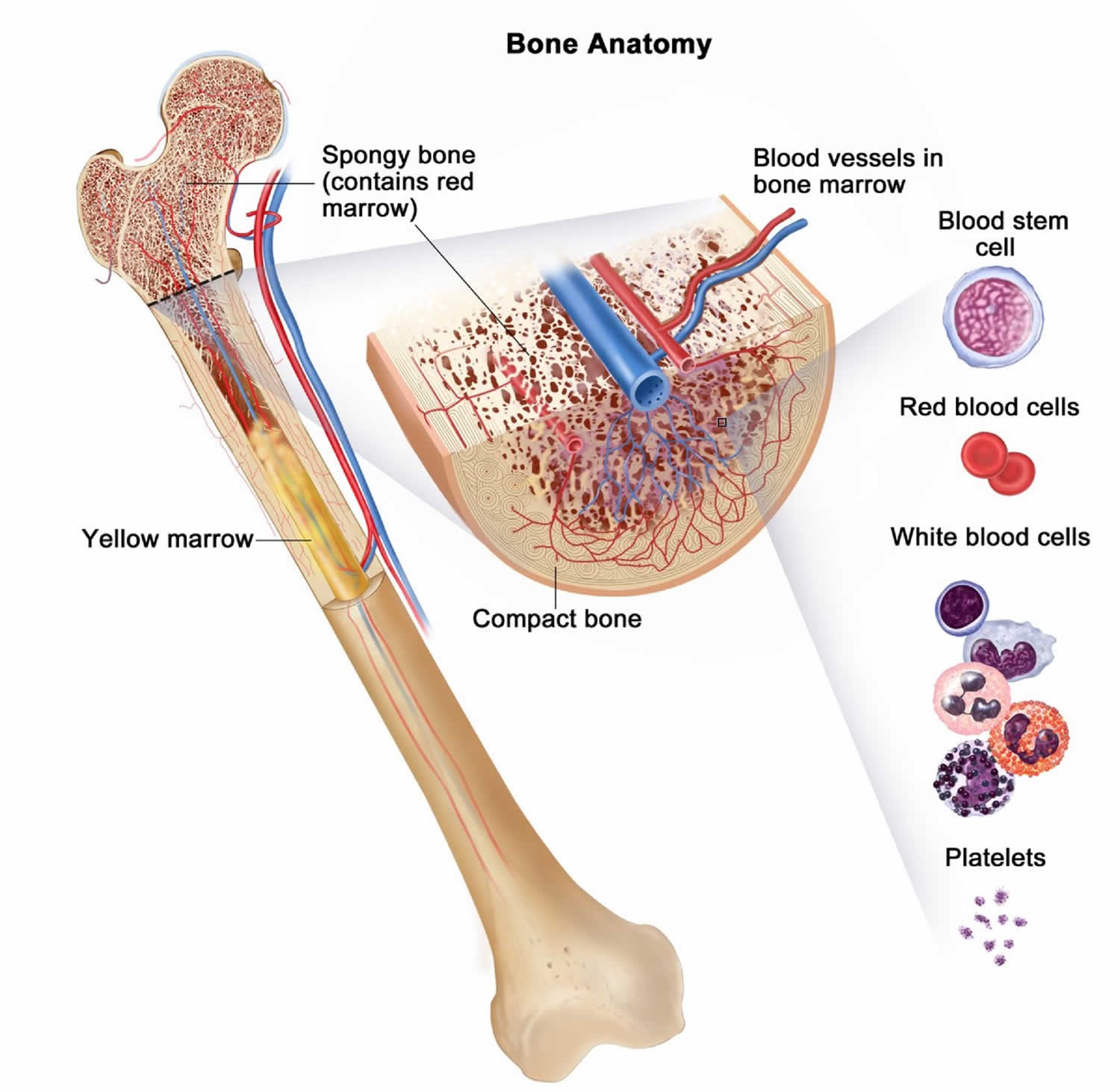
Erythropoiesis is the formation of red blood cells (RBCs) or erythrocytes in blood-forming tissue. A hormone called erythropoietin (EPO) triggers erythropoiesis. Red blood cell production or erythropoiesis requires adequate supplies of substrates, mainly iron, vitamin B12, folate, and heme (an iron-containing pigment). In the early development of a fetus, erythropoiesis takes place in the yolk sac, spleen, and liver. After birth, all erythropoiesis occurs in your bone marrow. Bone marrow is the spongy tissue inside of your bones. Once red blood cells (erythrocytes) are fully mature, they’re released into your bloodstream, where they transport oxygen throughout your body. Problems with erythropoiesis also called ineffective erythropoiesis can result in anemia, a condition that involves not having enough red blood cells.
Erythropoesis starts with a hematopoietic stem cell (HSCs), which differentiates into a common myeloid progenitor and then into a megakaryocyte-erythroid progenitor (MEP) (Figures 1 and 3). Further differentiation results in commitment to the erythroid lineage. The proerythroblast is the earliest morphologically identifiable bone marrow red cell precursor, characterized by a large cell with high nuclear:cytoplasmic ratio, prominent nucleoli and blue cytoplasm (presence of RNA). As the erythroid cells mature, they become smaller, have more condensed chromatin, losing their nucleoli, and their cytoplasm changes from blue to pink. Eventually, the nucleus is extruded, resulting in a reticulocyte (immature red blood cell). Most of this process takes place in the bone marrow over three weeks. The resulting reticulocyte (immature red blood cell) retains some ribosomal RNA to make hemoglobin and after 1-2 days in the bone marrow, it enters the peripheral blood where the RNA is lost after 1-2 days resulting in a mature red blood cell.
Red blood cells survive about 120 days. Red blood cells then lose their cell membranes and are largely cleared from the circulation by the phagocytic cells of the spleen and liver. Hemoglobin is broken down primarily by the heme oxygenase system with conservation (and subsequent reutilization) of iron, degradation of heme to bilirubin through a series of enzymatic steps, and reutilization of amino acids. Maintenance of a steady number of red blood cells requires daily renewal of 1/120 of the cells; immature red blood cells (reticulocytes) are continually released and constitute 0.5 to 1.5% of the peripheral red blood cell population.
With aging, hemoglobin and hematocrit (Hct) decrease slightly, but not below normal values. In menstruating women, the most common cause of lower red blood cell levels is iron deficiency due to chronic blood loss resulting from menstruation.
Red blood cells (erythrocytes) are important because they:
- Transport oxygen you breathe in through your lungs to tissues throughout your body.
- Transport carbon dioxide from tissues throughout your body to your lungs so you can breathe it out.
Erythropoiesis is one type of hematopoiesis. Hematopoiesis is your body’s process of making all three types of blood cells: red blood cells (erythropoiesis), white blood cells (leukopoiesis) and platelets (thrombopoiesis).
Each of the three types of blood cells—all made in the bone marrow—performs an important job.
- Red blood cells or erythrocytes contain hemoglobin (Hb), which is a protein that carries oxygen from your lungs to all parts of your body. Having fewer red blood cells than normal is called anemia.
- White blood cells or leukocytes are an important part of your immune system, helping your body fight infections. Having fewer white blood cells than normal is called leukopenia.
- Platelets or thrombocytes are small blood cells that stick together to stop bleeding and help wounds heal. Having fewer platelets than normal is called thrombocytopenia.
Figure 1. Erythropoiesis
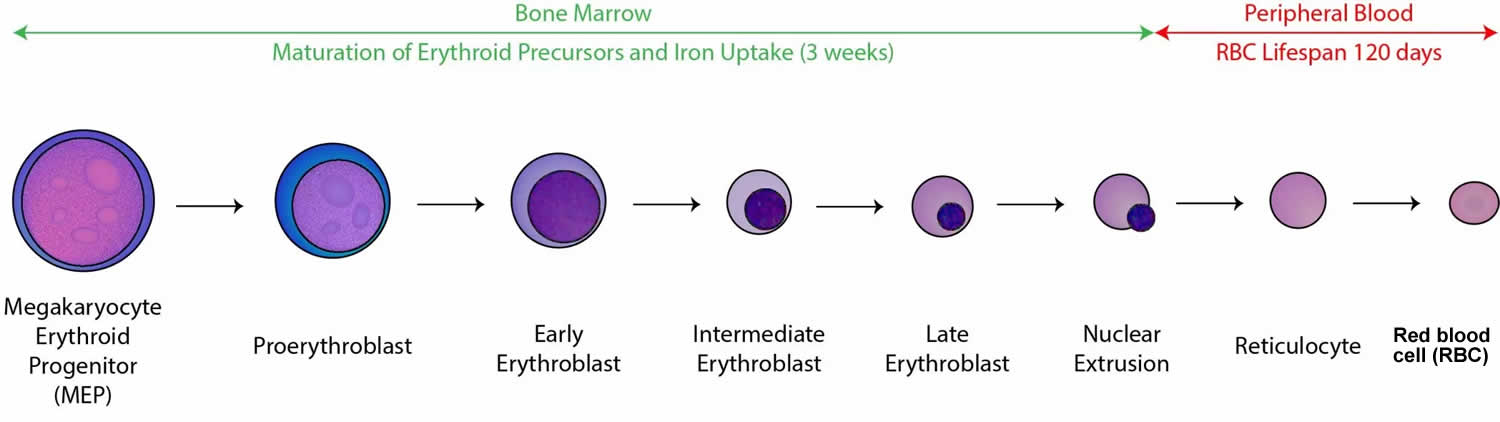
Figure 2. Vitamins and minerals influencing erythropoiesis
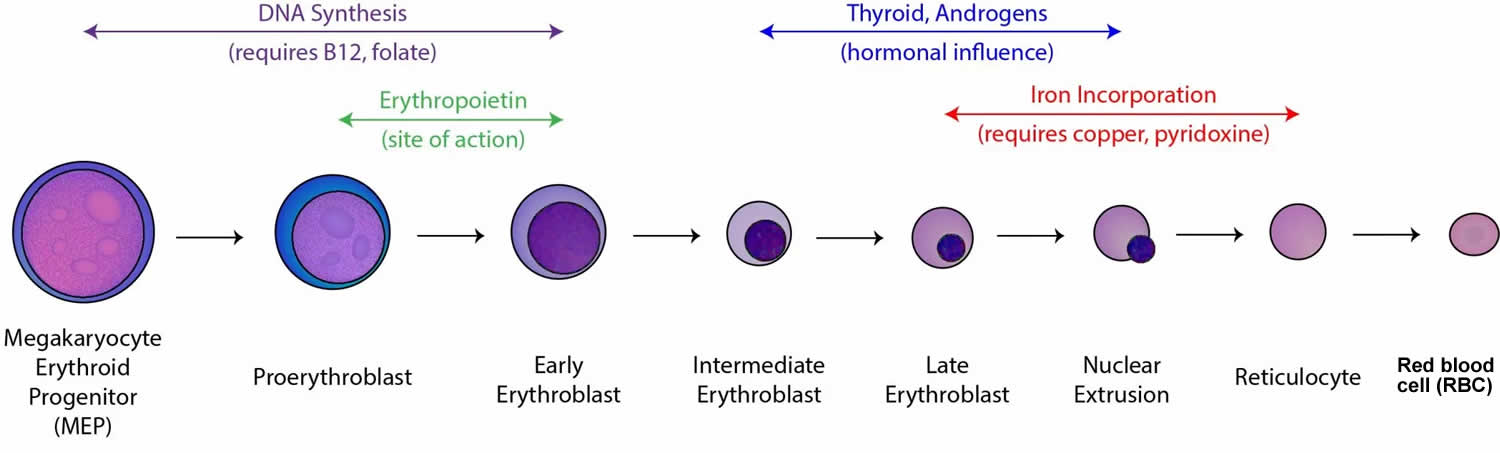
Footnote: Maturation factors such as vitamin B12 and folate are key components of DNA synthesis. Vitamin B12 and/or folate deficiency results in megaloblastic anemia, with inefficient DNA replication and selective death of more mature precursors. Androgens (male sex hormones) and thyroxine (thyroid hormone) also exert a stimulatory effect on erythropoiesis. Copper and pyridoxine (vitamin B6) are key components of iron incorporation into heme; deficiency of either can result in sideroblastic anemia.
[Source 1 ]Figure 3. Hematopoiesis (the process of all three types of blood cells formation)
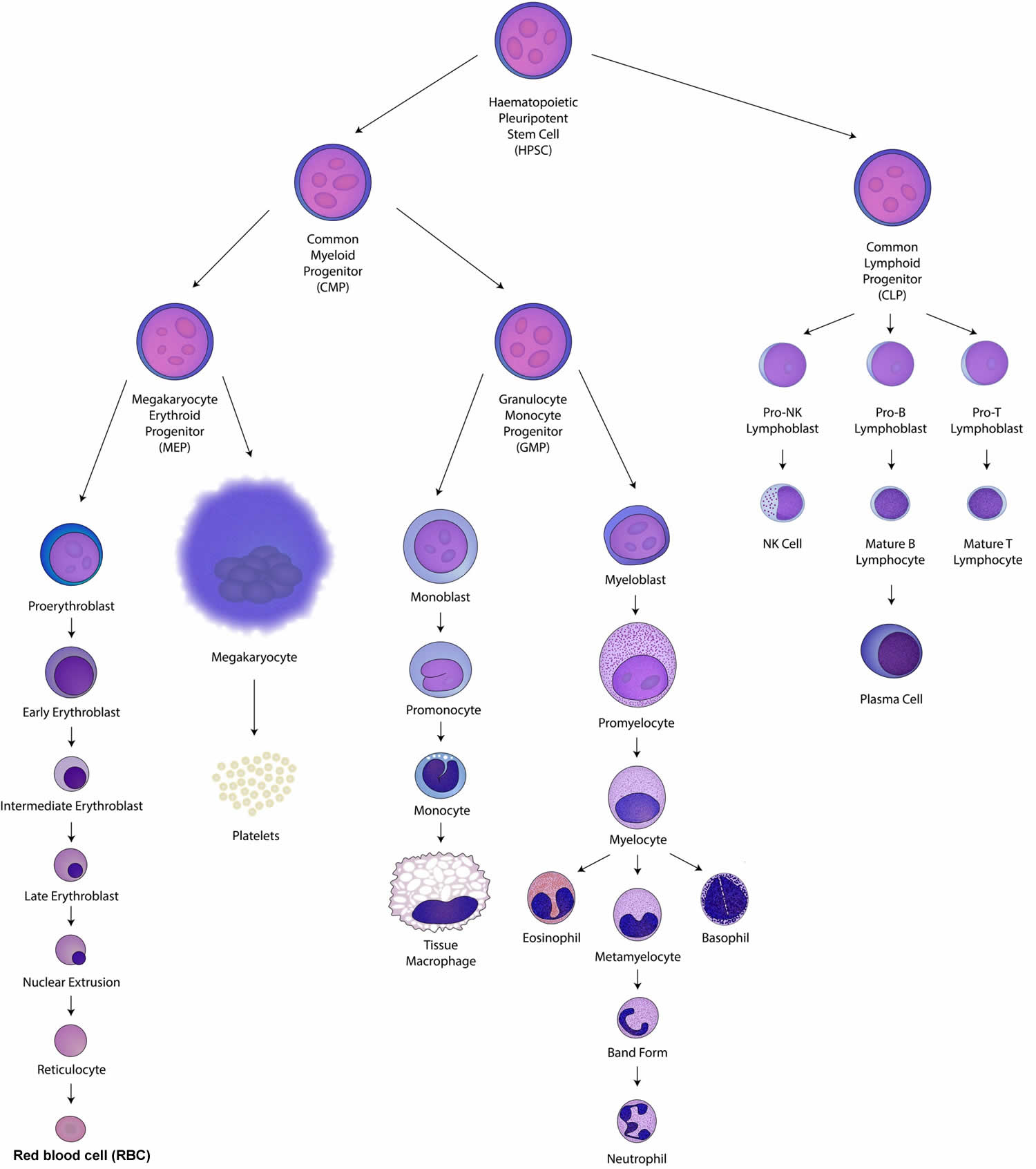
Footnotes: Hematopoietic stem cells (HSCs) also called hematopoietic plueripotent stem cell (HPSC) are the stem cells that give rise to both the common myeloid progenitor (CMP) and lymphoid progenitor (CLP) cells of blood cells through the process of hematopoiesis. Common myeloid progenitors (CMPs) can general all mature myeloid cells while granulocyte-monocyte progenitors (GMPs) or megakaryocyte-erythroid progenitors (MEPs) produce only myeloid or monocytic and megakaryocytic or erythroid lineage cells respectively. B and T lymphocytes and NK cells differentiate from the common lymphoid progenitor (CLP).
[Source 2 ]Figure 4. Bone marrow anatomy
How long does erythropoiesis take?
It takes about a week for a red blood cell to fully mature.
What is a red blood cell’s (erythrocyte’s) lifespan?
Red blood cells or erythrocytes live for approximately 120 days.
What causes erythropoiesis?
Your body’s sensitivity to oxygen levels regulates erythropoiesis. If your tissues don’t have enough oxygen (hypoxia), your body will ramp up red blood cell production. More red blood cells mean there’s more oxygen flowing to your tissues and cells. A hormone called erythropoietin (EPO) triggers erythropoiesis.
What is erythropoietin?
Your kidneys produce and secrete most of your body’s erythropoietin (EPO). Erythropoietin (EPO) is produced by liver in fetus 3. Erythropoietin is a hormone that is produced in your kidney and plays a major role in the control of erythropoiesis; iron is a key mineral required for hemoglobin production. A lack of erythropoeitin (EPO), which is seen most commonly in kidney failure, can result in profound reticulocytopenia (having fewer immature red blood cells) and anemia (having fewer mature red blood cells). In kidney failure, where the red blood cell (erythroid) precursors are preserved, exogenous erythropoeitin can correct anemia. Conversely, excessive erythropoietin (EPO), which is either a normal response to hypoxia or the result of pathological production (e.g. erythropoietin-secreting tumours), causes erythrocytosis.
Erythropoietin (EPO) production and control:
- Your tissues lack oxygen (hypoxia) because your red blood cells are low.
- Your kidneys secrete more erythropoietin (EPO) in response.
- The erythropoietin (EPO) stimulates your bone marrow to make more red blood cells.
- Your kidneys detect an increase in hemoglobin, a key protein in red blood cells, and secrete less erythropoietin (EPO) in response.
- Your body achieves a balance (homeostasis) where you have the right amount of red blood cells.
Your kidneys constantly secrete low levels of erythropoietin (EPO) to keep red blood cell production going. You lose about 1% of your red blood cells each day. Erythropoiesis replaces the red blood cells that have reached the end of their lifespan.
Your kidneys may secrete more or less erythropoietin (EPO) in response to conditions or injuries affecting your red blood cell levels.
Figure 5. Erythropoietin production and function
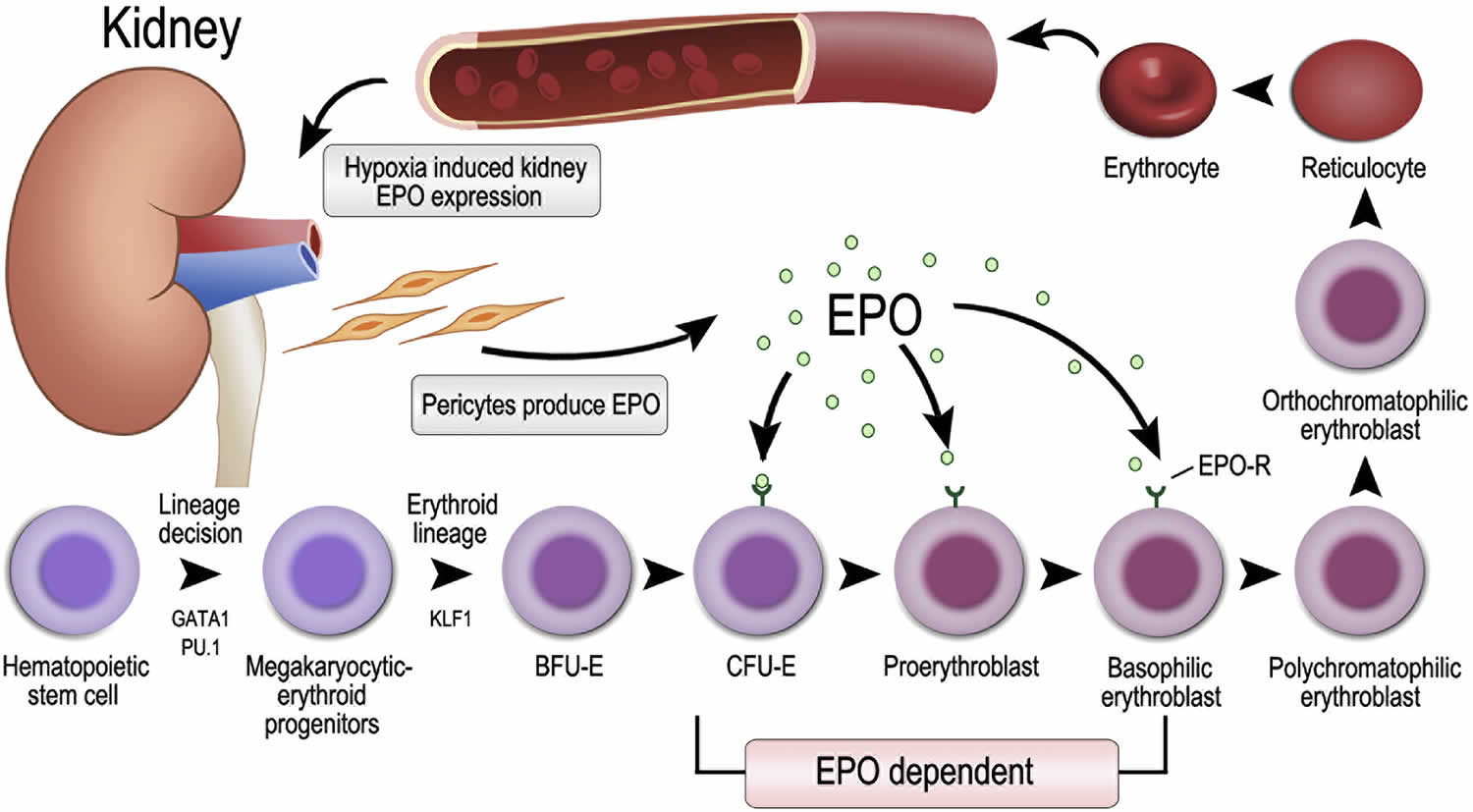
Footnotes: Erythropoietin (EPO) is produced in the kidney. Hypoxia, which may be caused by anemia, impaired gas exchange or increased tissue demand for oxygen, increases the production of hypoxia-inducible factor (HIF), which in turn stimulates kidney production of erythropoietin (EPO). Delivery of oxygen to kidney depends on hemoglobin (Hb) concentration. Once hemoglobin concentration decreases, pericytes sense hypoxia and produce erythropoietin (EPO). EPO binds to erythropoietin receptor (EPOR) which is expressed on colony-forming unit-erythroid (CFU-E), proerythroblasts and early basophilic erythroblasts, preventing these progenitor cells from apoptosis and upregulates their transferrin receptors to stimulate increased red blood cells (erythrocytes) production. Subsequently, increased red blood cells (erythrocytes) in circulation lead to improvement of tissue oxygenation relieving the hypoxia, down-regulating hypoxia-inducible factor (HIF) in a negative feedback loop and therefore decreased erythropoietin (EPO) production.
Abbreviations: EPO = erythropoietin; EPOR, erythropoietin receptor; KLF1 = Krüppel-like factor 1; BFU-E = burst-forming unit-erythroid; CFU-E = colony-forming unit-erythroid.
[Source 4 ]What is ineffective erythropoiesis?
Ineffective erythropoiesis is a term used to describe the imbalance of erythroid proliferation and differentiation and is characterized by an increase in erythroblast proliferation that fails to differentiate and give rise to enucleate red blood cells, a decreased output of red blood cells from the bone marrow, and, consequently resulting in anemia. Ineffective erythropoiesis is a condition characterized by the presence or abundance of dysfunctional progenitor cells. Ineffective erythropoiesis is prominent in disorders of nucleic acid, heme or globin synthesis 5. Ineffective erythropoiesis examples include folate deficiency, iron deficiency, vitamin B6 deficiency, lead poisoning, and thalassemia 6. Ineffective erythropoiesis also occurs in association with myeloproliferative and myelodysplastic syndromes and congenital dyserythropoiesis.
What conditions can impact erythropoiesis?
Many conditions can impact your body’s ability to make and regulate red blood cells.
Lung diseases
- Asthma. Asthma also called bronchial asthma, is a disease that affects your lungs. It’s a chronic (ongoing) condition, meaning it doesn’t go away and needs ongoing medical management.
- Chronic obstructive pulmonary disease (COPD). Chronic obstructive pulmonary disease (COPD) is an umbrella term for a range of progressive lung diseases. Chronic bronchitis and emphysema can both result in COPD. A COPD diagnosis means you may have one of these lung-damaging diseases or symptoms of both. COPD can progress gradually, making it harder to breathe over time.
Cancers affecting your blood or bone marrow
- Leukemia
- Lymphoma
- Myeloma
- Myeloproliferative disorders is now called myeloproliferative neoplasms. Myeloproliferative disorders are a group of conditions where your bone marrow makes too many blood cells. Main types of myeloproliferative disorder (myeloproliferative neoplasm) are chronic myeloid leukemia (CML), polycythemia vera (PV), essential thrombocythemia (ET) and primary myelofibrosis (PMF) 7. World Health Organization (WHO) classification also included chronic neutrophilic leukemia (CNL), chronic eosinophilic leukemia (CEL), and myeloproliferative neoplasm unclassifiable 8.
Other factors
- Vitamin and mineral deficiencies (iron deficiency, B12 deficiency, folate deficiency).
- High altitudes: Your body secretes more erythropoietin (EPO) in response to the decreased oxygen at high altitudes.
What are erythropoietin stimulating agents?
Erythropoietin (EPO) is a hormone, naturally produced by your kidneys, that stimulates erythropoiesis or red blood cell production. Erythropoietin stimulating agents are man-made versions of erythropoietin (EPO) produced pharmacologically via recombinant DNA technology in cell cultures 9. Examples of erythropoietin stimulating agents include epoetin alfa, darbepoetin, and methoxy polyethylene glycol-epoetin beta 10.
Thrombosis occurs when blood clots block your blood vessels. The most severe adverse effects of erythropoietin (EPO) are related to a significant risk of thrombotic events, particularly in surgical patients 11. Supplemental use of erythropoietin stimulating agents leads to an increase in blood viscosity because of a higher rate of red blood cell production. Given this, as well as the reduced vasodilatory effect due to a low baseline pO2, there is an associated increased risk of ischemic stroke and myocardial infarction 12. There is also an increased risk of venous thromboembolism, and some have proposed the use of antithrombotic prophylaxis in patients receiving erythropoietin stimulating agent therapy 11. Because of increased blood viscosity when using erythropoietin stimulating agent, doctors should exercise caution in patients with a history of deep vein thrombosis (DVT), pulmonary embolism, or hypercoagulability disorder. Likewise, caution is necessary for patients with a history of ischemic stroke or cardiovascular disease 12.
There has been concern regarding the potential progression of tumorigenesis in patients with certain forms of cancer, particularly breast cancer, non-small cell lung cancer, head and neck cancer, lymphoid cancer, and cervical cancer 13. The mechanism is through increased cell signaling and tumor angiogenesis.
Researchers reported nausea, vomiting, diarrhea, fatigue, insomnia, peripheral edema, thrombocytopenia (low platelet level in your blood), muscle aches and pain (myalgias), joint pain and stiffness (arthralgias), rashes, abdominal pain, headache, and burning or prickling sensation (paresthesias) as common adverse effects experienced by patients undergoing chemotherapy who received epoetin alfa in a multicenter study 14.
Erythropoietin stimulating agents are contraindicated in patients with hypersensitivity to non-human mammal-derived products because of erythropoietin stimulating agent production methods 11.
Erythropoietin stimulating agents containing benzyl alcohol are contraindicated in neonates, peripartum mothers, and breastfeeding mothers due to the risk for gasping syndrome. This syndrome causes gasping breathing, kidney failure, and neurological deterioration in neonates, resulting from severe metabolic acidosis 15.
- Normal Erythropoiesis. https://www.learnhaem.com/courses/anaemia/lessons/normal-haematopoiesis/topic/normal-erythropoiesis[↩][↩]
- Haematopoiesis. https://www.learnhaem.com/courses/anaemia/lessons/normal-haematopoiesis/topic/haematopoiesis[↩]
- Bondurant MC, Koury MJ. Anemia induces accumulation of erythropoietin mRNA in the kidney and liver. Mol Cell Biol. 1986 Jul;6(7):2731-3. doi: 10.1128/mcb.6.7.2731-2733.1986[↩]
- Shih HM, Wu CJ, Lin SL. Physiology and pathophysiology of renal erythropoietin-producing cells. J Formos Med Assoc. 2018 Nov;117(11):955-963. https://doi.org/10.1016/j.jfma.2018.03.017[↩]
- Clinical Biochemistry of Domestic Animals. Sixth Edition 2008. ISBN 978-0-12-370491-7 https://doi.org/10.1016/B978-0-12-370491-7.X0001-3[↩]
- JANDL JH. A SYMPOSIUM ON THE MECHANISMS OF DISORDERS OF ERYTHROPOIESIS. INTRODUCTION. Medicine (Baltimore). 1964 Nov;43:615-6.[↩]
- Thapa B, Rogers HJ. Cancer, Myeloproliferative Neoplasms. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531464[↩]
- Tefferi A, Thiele J, Vardiman JW. The 2008 World Health Organization classification system for myeloproliferative neoplasms: order out of chaos. Cancer. 2009 Sep 1;115(17):3842-7. doi: 10.1002/cncr.24440[↩]
- Schoener B, Borger J. Erythropoietin Stimulating Agents. [Updated 2023 Mar 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536997[↩]
- Wolfgang Jelkmann, 2016. “Erythropoietin”, Sports Endocrinology, F. Lanfranco, C.J. Strasburger. Front Horm Res. 2016;47:115-27. doi: 10.1159/000445174[↩]
- Jelkmann W. Physiology and pharmacology of erythropoietin. Transfus Med Hemother. 2013 Oct;40(5):302-9. doi: 10.1159/000356193[↩][↩][↩]
- McCullough PA, Barnhart HX, Inrig JK, Reddan D, Sapp S, Patel UD, Singh AK, Szczech LA, Califf RM. Cardiovascular toxicity of epoetin-alfa in patients with chronic kidney disease. Am J Nephrol. 2013;37(6):549-58. doi: 10.1159/000351175[↩][↩]
- Annese T, Tamma R, Ruggieri S, Ribatti D. Erythropoietin in tumor angiogenesis. Exp Cell Res. 2019 Jan 15;374(2):266-273. doi: 10.1016/j.yexcr.2018.12.013[↩]
- Glaspy JA, Charu V, Luo D, Moyo V, Kamin M, Wilhelm FE. Initiation of epoetin-alpha therapy at a starting dose of 120,000 units once every 3 weeks in patients with cancer receiving chemotherapy: an open-label, multicenter study with randomized and nonrandomized treatment arms. Cancer. 2009 Mar 1;115(5):1121-31. doi: 10.1002/cncr.24127[↩]
- Gershanik J, Boecler B, Ensley H, McCloskey S, George W. The gasping syndrome and benzyl alcohol poisoning. N Engl J Med. 1982 Nov 25;307(22):1384-8. doi: 10.1056/NEJM198211253072206[↩]




{kind=link}