What is familial adenomatous polyposis
Familial adenomatous polyposis (FAP) is an inherited disorder characterized by cancer of the large intestine (colon) and rectum. People with the classic type of familial adenomatous polyposis may begin to develop hundreds to thousands of noncancerous (benign) growths (polyps) in the colon as early as their teenage years. Unless the colon is removed, these polyps will become malignant (cancerous). The average age at which an individual develops colon and/or rectum cancer with nearly 100 percent certainty in classic familial adenomatous polyposis is 39 years. Some people have a variant of the disorder, called attenuated familial adenomatous polyposis, in which polyp growth is delayed. The average age of colorectal cancer onset for attenuated familial adenomatous polyposis is 55 years.
Familial adenomatous polyposis can cause other complications:
- Duodenal polyps. These polyps grow in the upper part of your small intestine and may become cancerous. But with careful monitoring, duodenal polyps can often be detected and removed before cancer develops.
- Periampullary polyps. These polyps occur where the bile and pancreas ducts enter the duodenum (ampulla). Periampullary polyps might become cancerous but can often be detected and removed before cancer develops.
- Desmoid tumors. These noncancerous masses can arise anywhere in the body but often develop in the stomach area (abdomen). Desmoid tumors can cause serious problems if they grow into nerves or blood vessels or exert pressure on other organs in your body.
- Other cancers. Rarely, familial adenomatous polyposis can cause cancer to develop in your thyroid gland, central nervous system, adrenal glands, liver or other organs.
- Noncancerous skin tumors.
- Noncancerous bone tumors.
- Pigment changes in the retina of your eye.
- Dental abnormalities.
Familial adenomatous polyposis is inherited in an autosomal dominant manner and caused by abnormalities (mutations) in the adenomatous polyposis coli (APC) gene. Mutations in the adenomatous polyposis coli (APC) gene cause a group of polyposis conditions that have overlapping features: familial adenomatous polyposis, Gardner syndrome, Turcot syndrome and attenuated familial adenomatous polyposis. Most people inherit the APC genetic abnormality from a parent. But in about 25 percent of cases, the genetic mutation occurs spontaneously.
The reported incidence of familial adenomatous polyposis varies from 1 in 5,000 to 1 in 22,000 individuals in the United States. Familial adenomatous polyposis affects males and females in equal numbers. Familial adenomatous polyposis accounts for about 0.5% of all cases of colorectal cancer. One estimate suggests that familial adenomatous polyposis affects 50,000 American families. According to national registries, familial adenomatous polyposis occurs in 2.29-3.2 per 100,000 individuals.
In people with classic familial adenomatous polyposis, the number of polyps increases with age, and hundreds to thousands of polyps can develop in the colon. Also of particular significance are noncancerous growths called desmoid tumors. These fibrous tumors usually occur in the tissue covering the intestines and may be provoked by surgery to remove the colon. Desmoid tumors tend to recur after they are surgically removed. In both classic familial adenomatous polyposis and its attenuated variant, benign and malignant tumors are sometimes found in other places in the body, including the duodenum (a section of the small intestine), stomach, bones, skin, and other tissues. People who have colon polyps as well as growths outside the colon are sometimes described as having Gardner syndrome.
A milder type of familial adenomatous polyposis, called autosomal recessive familial adenomatous polyposis, has also been identified. People with the autosomal recessive type of this disorder have fewer polyps than those with the classic type. Fewer than 100 polyps typically develop, rather than hundreds or thousands. The autosomal recessive type of this disorder is caused by mutations in a different gene than the classic and attenuated types of familial adenomatous polyposis.
Figure 1. Large intestine (colon)
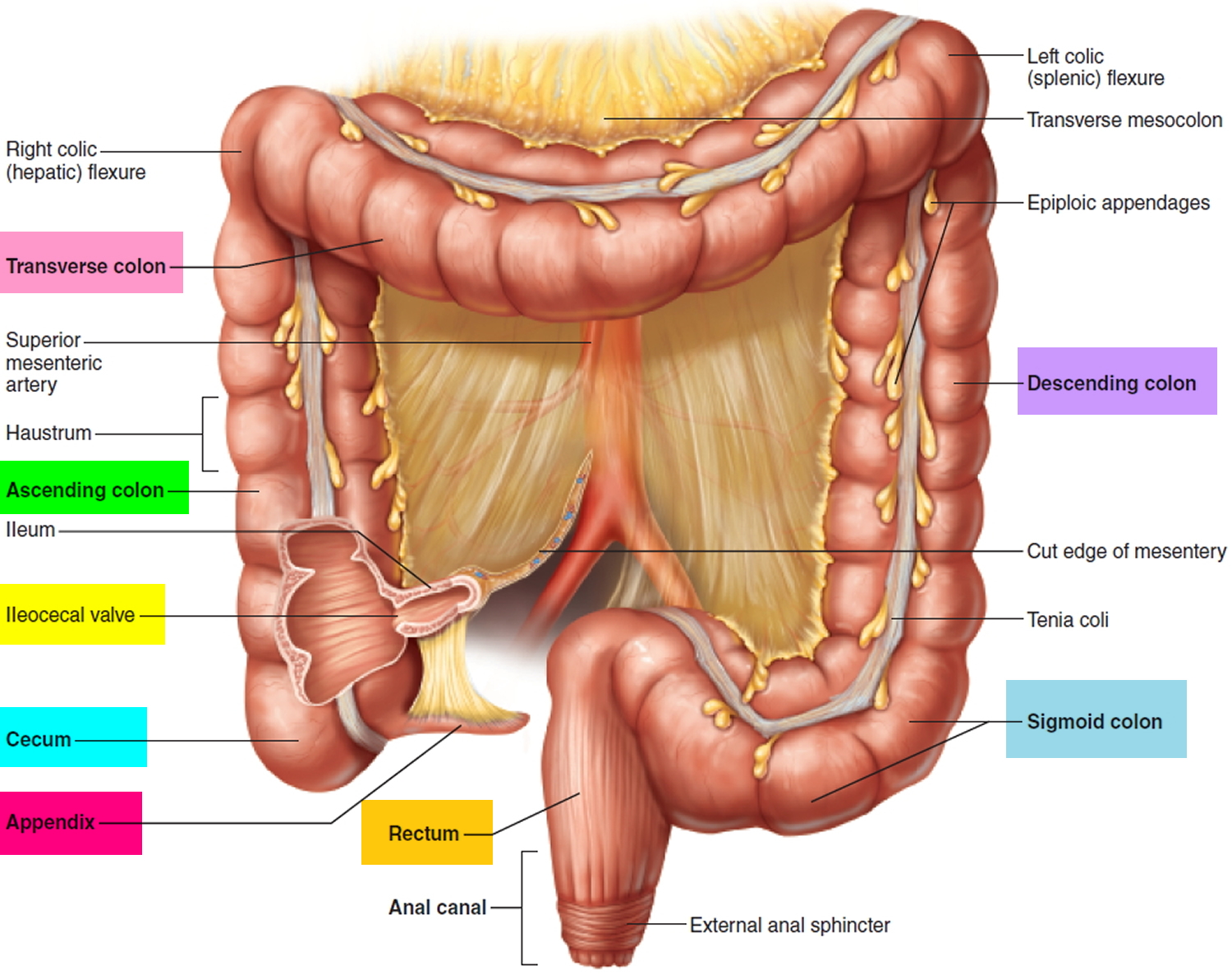
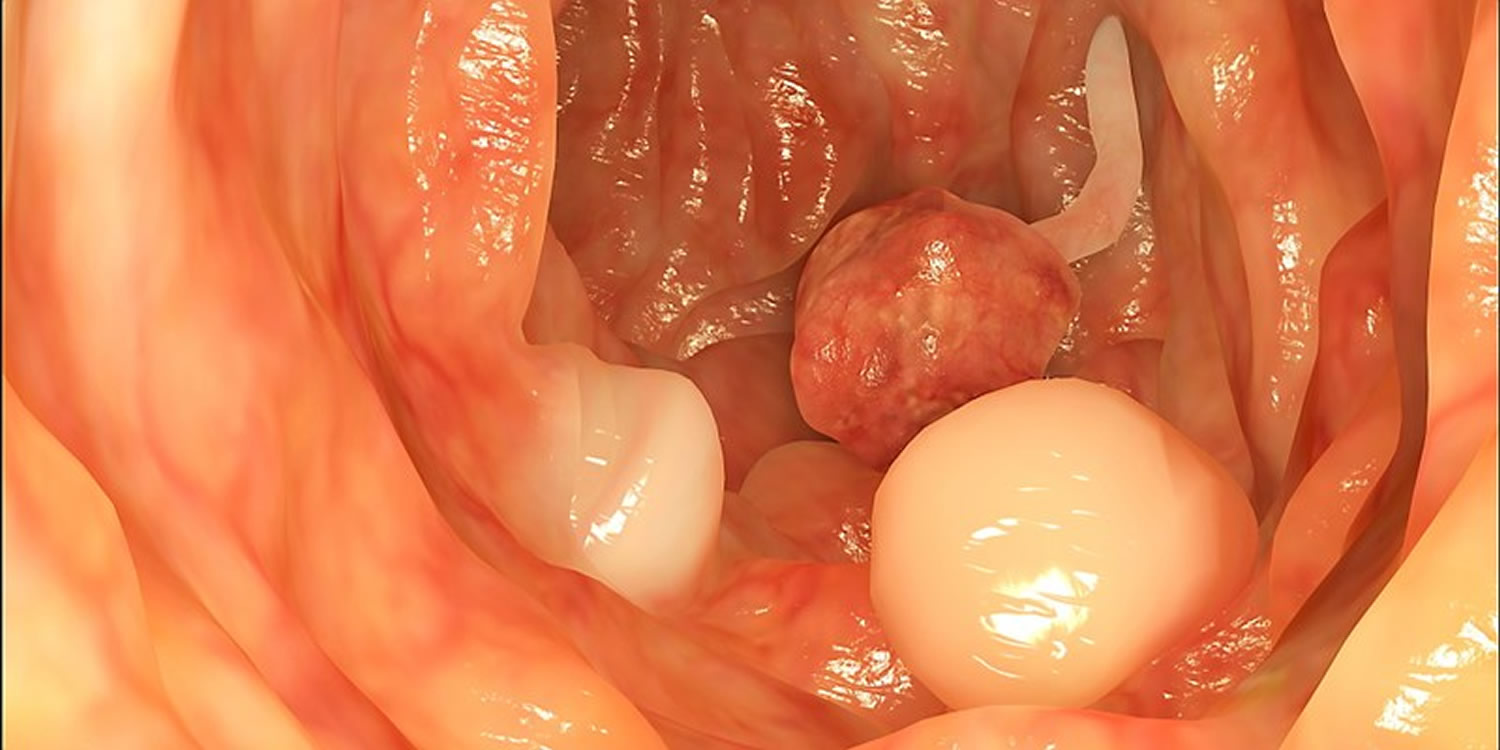
Figure 2. Colon polyps

Figure 3. Familial adenomatous polyposis (FAP)
Familial adenomatous polyposis life expectancy
As mentioned above, individuals with familial adenomatous polyposis who are not screened and treated early will develop colon cancer in their thirties, which can be fatal. However, with early screening and prophylactic removal of the colon (colectomy) in their twenties, many individuals are now able to live normal life spans. The prognosis for the other syndromes will depend on whether affected individuals do actually develop colon cancer (or another type) – otherwise there is no effect on prognosis.
Familial adenomatous polyposis causes
Mutations in the APC gene cause both classic and attenuated familial adenomatous polyposis. These mutations affect the ability of the cell to maintain normal growth and function. Cell overgrowth resulting from mutations in the APC gene leads to the colon polyps seen in familial adenomatous polyposis. Although most people with mutations in the APC gene will develop colorectal cancer, the number of polyps and the time frame in which they become malignant depend on the location of the mutation in the gene.
Mutations in the MUTYH gene cause autosomal recessive familial adenomatous polyposis (also called MYH-associated polyposis). Mutations in this gene prevent cells from correcting errors that are made when DNA is copied (DNA replication) in preparation for cell division. As these errors build up in a person’s DNA, the likelihood of cell overgrowth increases, leading to colon polyps and the possibility of colon cancer.
Figure 4. Autosomal dominant inheritance pattern of both classic and attenuated familial adenomatous polyposis (APC gene)
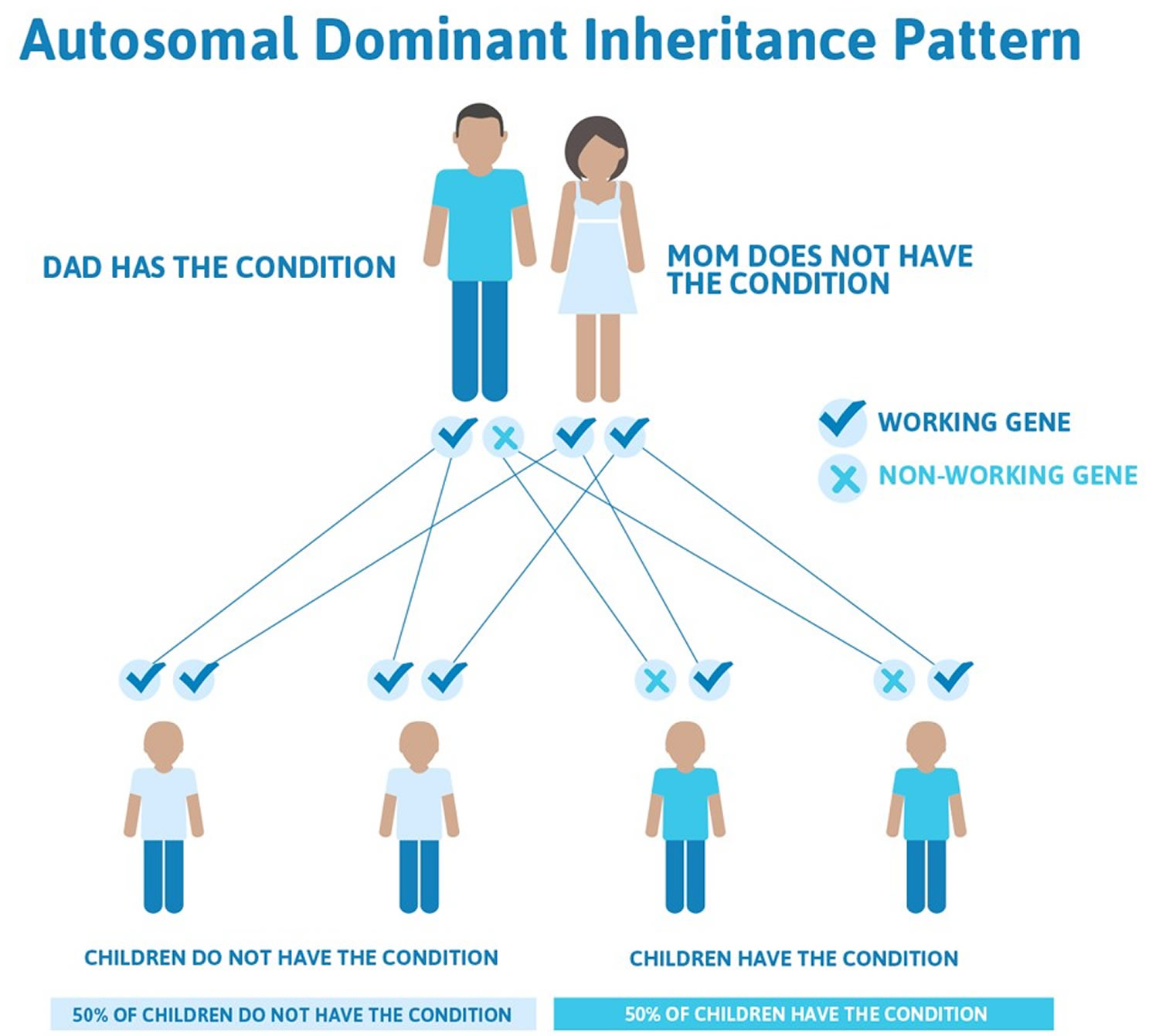
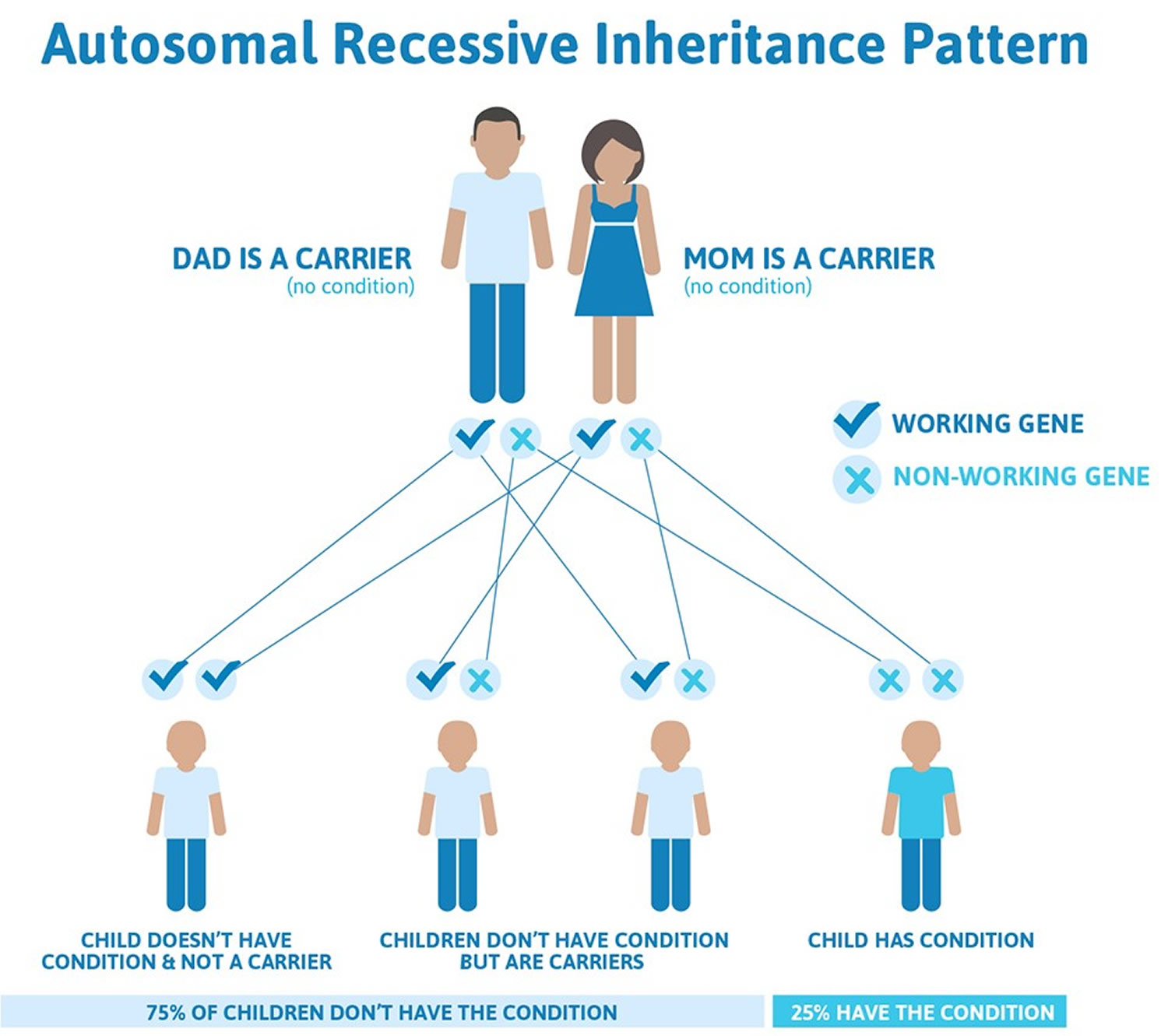
Figure 5. Autosomal recessive inheritance pattern of MYH gene associated with familial adenomatous polyposis
Familial adenomatous polyposis can have different inheritance patterns
- When familial adenomatous polyposis results from mutations in the APC gene, it is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases, an affected person has one parent with the condition.
- When familial adenomatous polyposis results from mutations in the MUTYH gene, it is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. Most often, the parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but do not show signs and symptoms of the condition.
Familial adenomatous polyposis symptoms
Classic familial adenomatous polyposis is characterized by hundreds to thousands of colorectal adenomatous polyps, with polyps appearing on average at age 16 years. Without colectomy, affected individuals usually develop colorectal cancer by the third or fourth decade of life. Familial adenomatous polyposis is also associated with an increased risk for cancer of the small intestine including the duodenum, and cancer of the thyroid, pancreas, liver (hepatoblatoma), central nervous system (CNS), and bile ducts, although these typically occur in less than 10% of affected individuals.
Individuals with central nervous system (CNS) tumors and colorectal polyposis have historically been defined as Turcot syndrome. Two-thirds of cases of Turcot syndrome develop from mutations in the APC gene. The remaining cases develop from mutations in the genes that cause hereditary non-polyposis colorectal cancer (HNPCC) also known as Lynch syndrome. Mutations in the APC gene are more commonly associated with medulloblastoma; mutations in the genes that cause hereditary non-polyposis colorectal cancer (HNPCC) are more commonly associated with glioblastoma. In addition, hereditary non-polyposis colon cancer (HNPCC) or Lynch syndrome is an autosomal dominant cancer that also causes endometrial cancer, cancers of the ovary, stomach, small intestine, hepatobiliary tract, upper urinary tract, brain, and skin.
Extracolonic manifestations are variably present in familial adenomatous polyposis, including polyps of the stomach, duodenum and small bowel; and osteomas (bony growths), dental abnormalities, congenital hypertrophy of the retinal pigment epithelium and soft tissue tumors including epidermoid cysts, fibromas and desmoid tumors. About 5% of individuals with familial adenomatous polyposis experience morbidity and/or mortality from desmoid tumors. The term Gardner syndrome is often used when colonic polyposis is accompanied by clinically obvious osteomas and soft tissue tumors.
Attenuated familial adenomatous polyposis is a variant of familial adenomatous polyposis. The disorder is characterized by an increased risk for colorectal cancer (although lower risk than classical familial adenomatous polyposis) but with fewer polyps (average of 30) and later age of onset of polyps and cancer than is typically seen in classic familial adenomatous polyposis. Extra-colonic manifestations are also associated with attenuated familial adenomatous polyposis.
Familial adenomatous polyposis diagnosis
You’re at risk of familial adenomatous polyposis if you have a parent, child, brother or sister with the condition.
If you’re at risk, it’s important to be screened frequently, starting in childhood. Annual exams can detect the growth of polyps before they become cancerous. At-risk children who have the defective gene or whose genetic status isn’t known are screened every year starting at age 10. At-risk children who don’t have the defective gene are screened periodically starting at age 15.
Screening tests for familial adenomatous polyposis and its complications:
- Sigmoidoscopy. A flexible tube is inserted into your rectum to inspect the rectum and sigmoid — the last two feet of the colon. Sigmoidoscopy is used to screen at-risk children who haven’t yet developed polyps.
- Colonoscopy. A flexible tube is inserted into your rectum to inspect the entire colon. Colonoscopy is used after polyps start growing and after age 18, and if attenuated familial adenomatous polyposis is suspected or already diagnosed.
- Esophagogastroduodenoscopy (EGD) and side-viewing duodenoscopy. Two types of scopes are used to inspect your esophagus, stomach and upper part of the small intestine (duodenum and ampulla). The doctor may remove a small tissue sample (biopsy) for further study.
- CT or MRI. Imaging of the abdomen and pelvis may be used, especially to evaluate desmoid tumors.
Classical familial adenomatous polyposis is diagnosed clinically when an individual has 100 or more adenomatous colorectal polyps (typically occurring by the third decade of life) or fewer than 100 polyps and a relative with familial adenomatous polyposis. Genetic testing for mutations in the APC gene is available to confirm the diagnosis of familial adenomatous polyposis and the associated conditions. Younger individuals may have fewer polyps. A diagnosis is made in younger people by the presence of the typical polyps and in immediate relative with familial adenomatous polyposis or by genetic testing.
Genetic testing
A simple blood test can determine if you carry the abnormal gene that causes familial adenomatous polyposis. Genetic testing may also detect whether you’re at risk of complications of familial adenomatous polyposis.
Genetic testing is recommended if:
- You have family members with familial adenomatous polyposis
- You have some, but not all, of the signs of familial adenomatous polyposis
Ruling out familial adenomatous polyposis spares at-risk children years of screening and emotional distress. For children who do carry the gene, appropriate screening and treatment greatly reduce the risk of cancer.
Genetics counselors will discuss the pros and cons of testing with you, including the psychological and medical implications and confidentiality issues. If you choose genetic testing, your counselor and your doctor will discuss the results with you.
The genetics laboratory uses the latest techniques to detect specific mutations in the APC gene associated with familial adenomatous polyposis. If the initial genetic test is negative, scientists can sequence the MUTYH gene to determine if you have MUTYH-associated polyposis.
Additional tests
Your doctor may recommend thyroid exams and other testing to detect other medical problems that can occur if you have familial adenomatous polyposis.
Familial adenomatous polyposis treatment
If you have a few small polyps, your doctor can remove them during your colonoscopy exam. Eventually, though, polyps may become too numerous to remove individually. Prophylactic (preventive) removal of the colon is usually recommended for individuals with classical familial adenomatous polyposis at an appropriate age, usually between the late teens and late 30s. Surgery doesn’t cure familial adenomatous polyposis. Polyps can continue to form in the remaining or reconstructed parts of your colon, stomach and small intestine. But with careful monitoring, these polyps usually can be found and removed during colonoscopy before becoming cancerous.
Three surgical options are possible:
- The whole colon including the rectum and the anus can be removed (proctocolectomy) which means the patient needs a stoma (an ileostomy bag). In this procedure, your small intestine (ileum) is connected to the outside body through an opening (stoma) on your abdomen. An ileostomy provides a new path for waste material to leave your body after part of the intestine has been removed, but there is no chance of developing colon cancer.
- Ileal pouch-anal anastomosis (J-pouch) surgery. The colon and rectum are removed while preserving your anus, allowing you to have normal bowel movements. J-pouch surgery is the preferred treatment for familial adenomatous polyposis in some surgical centers. J-pouch surgery can affect fertility. Medical geneticists and reproductive gynecologists advise prospective parents about their options.
- Alternatively, the colon without the rectum can be removed (colectomy) which means the patient does not need a stoma, but the patient needs to be followed up (with proctoscopy) to make sure they do not develop rectal cancer. Surgeons will consider colectomy only if you don’t have polyps in your rectum.
Surgery is usually performed in the patient’s twenties. Regular follow-up with an upper endoscopy (a thin flexible instrument is advanced through the mouth to evaluate or treat problems of the esophagus, stomach, and beginning part of the small intestine) is recommended when an individual is in their fifties because of the risk of cancer in the upper gastrointestinal tract – mainly the duodenum. Removal of duodenal polyps is sometimes recommended if they cause symptoms, are large or contain large numbers of abnormal cells (dysplasia). This is to prevent them from becoming cancerous. The patient’s family members should be screened after the age of twelve.
Genetic counseling is recommended for individuals with familial adenomatous polyposis and their at-risk family members. This is very helpful to properly obtain and interpret genetic testing. Affected individuals should be screened clinically and endoscopically on a regular basis in order to identify cancerous and pre-cancerous tumors at an early stage. Colon cancer is virtually always prevented by screening and properly timed colectomy. This is similar for duodenal cancer. Other cancers are usually detected early, rather than prevented.
Sulindac is a nonsteroidal antiinflammatory drug (NSAID) usually used for arthritis, but is sometimes prescribed for individuals with familial adenomatous polyposis who have had a colectomy to treat polyps in the remaining rectum. Polyps will almost always regress, but it is uncertain if the cancer risk is changed, so surveillance must be continued.
Follow-up treatment
You are screened regularly and treated for complications of familial adenomatous polyposis that can develop after colorectal surgery, including:
- Duodenal polyps and periampullary polyps. Your doctor may recommend surgery in some cases to remove the entire duodenum because these types of polyps can progress to cancer.
- Desmoid tumors. Mayo specialists use a combination of medications, including nonsteroidal anti-inflammatory drugs, anti-estrogen, chemotherapy and, in some cases, surgery.
- Noncancerous bone tumors. Surgeons can remove these tumors for pain relief or cosmetic reasons.
Non-Adenomatous Polyposis Syndromes
Children of an affected individual may have a screening sigmoidoscopy (inspection of the rectum and lower colon using a thin lighted tube called a sigmoidoscope). If it is found to have hamartomatous polyps they are at increased risk for obstruction of bleeding. Polyps should be removed at the time of sigmoidoscopy.





{kind=link}