
Contents
What is a food allergy
A food allergy occurs when the immune system responds to an allergen (an ingredient that is usually harmless) in food. This triggers an immune reaction, which can range from mild to severe. Food allergy is an immune system reaction (antibody mediated food allergy) and can be immunoglobulin E (IgE)-mediated or non-IgE-mediated 1, 2, 3, 4, 5, 6. A food allergy is caused by an overreaction of the immune system due to your body mistaking an ingredient in food — usually a protein — as harmful and creates a defense system (antibodies) to fight it 7. An allergic reaction occurs when the antibodies are battling an “invading” food protein. Any food can cause allergy but overall only a few foods account for the vast majority of food allergies. Although any food can produce an allergy 8, the most common food allergies that trigger 90% of food allergic reactions are shellfish, peanuts, tree nuts, fish, eggs, wheat, soy, and milk 4. About 6% of children experience food allergic reactions in the first three years of life, including approximately 2.5% with cow’s milk allergy, 1.5% with egg allergy, and 1% with peanut allergy 1. Peanut allergy, the most common food allergy, is the leading cause of life-threatening anaphylaxis. Anaphylaxis is a very serious and potentially life-threatening allergic reaction that involves a sudden drop in blood pressure, swelling of the airways to the lungs, wheezing, shortness of breath, loss of consciousness and body system failure. If you’ve had allergic reactions to food or insect bites, your doctor will prescribe an epinephrine (adrenaline) injection (Adrenaclick, Auvi-Q, EpiPen) for emergency self-treatment.
Diagnosis of food allergy starts with a detailed, allergy-focused history addressing specific risk factors such as atopic dermatitis and a family history of atopic disease 9. Tests for food allergies include avoidance of the food, allergy skin prick testing, serum immunoglobulin E (IgE) testing, and an oral food challenge. In patients with suspected food allergy, the first step should be elimination of the suspected food to see if symptoms resolve. Immunoglobulin E (IgE) specific antibody and skin testing are helpful to confirm or exclude allergens. In patients with a history suggestive of anaphylaxis to a particular food, the response to specific IgE antibody levels and a skin test can confirm and predict the results of an oral food challenge 10, 11. An oral food challenge is used to confirm a negative or questionable test result. The only definitive diagnostic method for food allergy is the oral food challenge, in which increasing doses of a potential food allergen are ingested over fixed time intervals, until either an allergic reaction is observed or a maximum dose is reached 12. Oral food challenges are typically performed in an allergist’s office where the proper equipment and expertise are available in the event of severe anaphylactic reaction. To avoid this possibility, the oral food challenges test is reserved for patients with a low risk of severe reaction, and the tested food is administered using progressive dosing until a customary meal dose is met. A negative food allergy test results together with negative oral food challenge can help reassure the patient and family that no allergy is present and no further testing is necessary 11. Primary treatment of food allergy involves elimination of the offending food from your diet.
Figure 1. Food allergy diagnostic algorithm
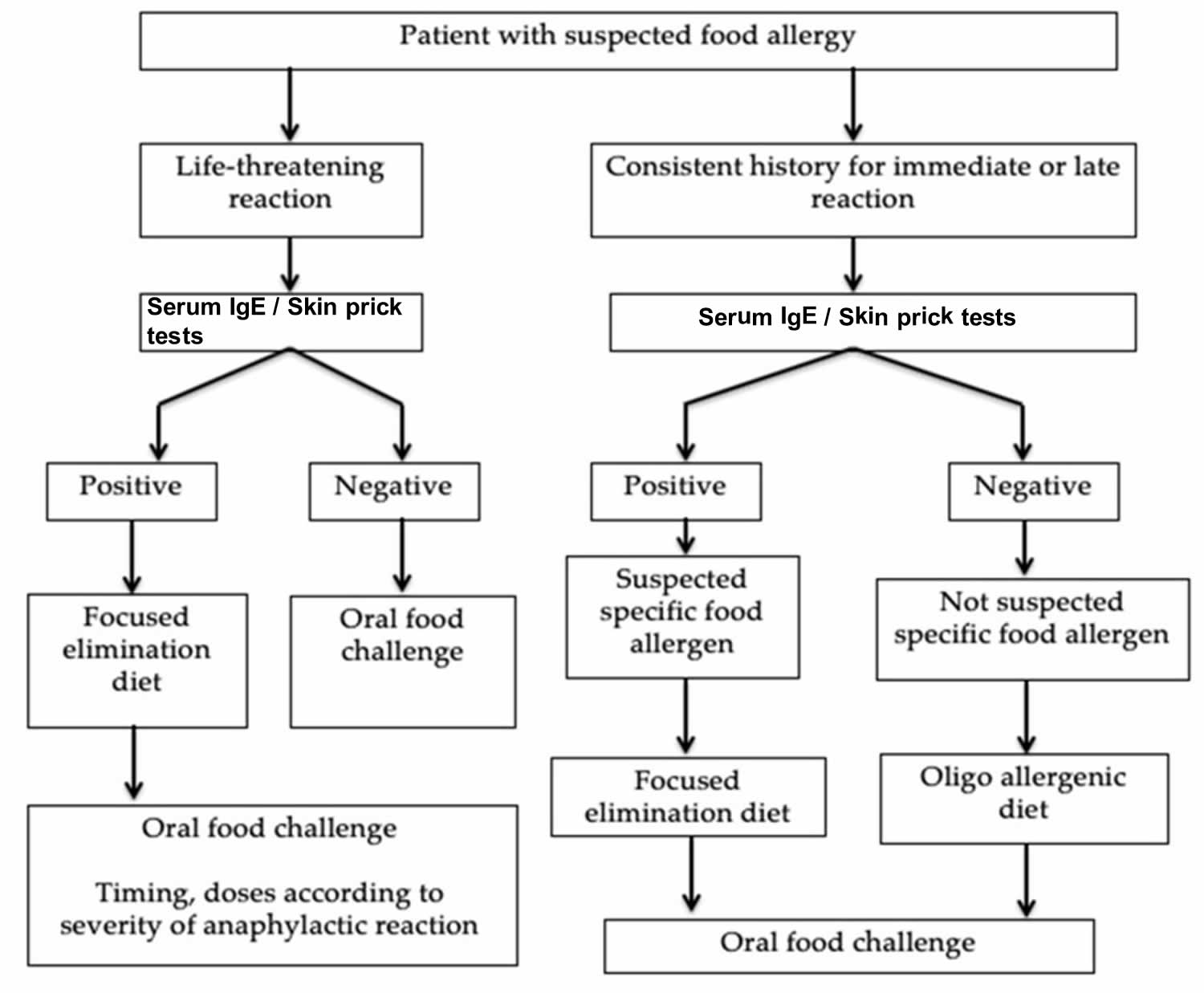
Footnotes: The only definitive diagnostic method for food allergy is the oral food challenge, in which increasing doses of a potential food allergen are ingested over fixed time intervals, until either an allergic reaction is observed or a maximum dose is reached 12. However, the oral food challenge method is infrequently used outside properly equipped and staffed specialist centers because it is resource-intensive and carries the risk of inducing a severe anaphylactic reaction.
[Source 13 ]An allergy is when the immune system reacts to a substance (allergen) in the environment which is usually harmless (e.g. food, pollen, animal dander and dust mite) or bites, stings and medications. This results in the production of allergy antibodies which are proteins in the immune system which identify and react with foreign substances.
An allergic reaction is when someone develops symptoms following exposure to an allergen, such as hives, swelling of the lips, eyes or face, vomiting or wheeze. It is important to note that only some people with allergy antibodies will develop symptoms following exposure to the allergen, hence confirmation of allergy by a clinical immunology/allergy specialist is required.
The majority of food allergies in children are not severe and usually children will outgrow many allergies with time. Most children tend to outgrow milk and egg allergies by school-age. In contrast, some allergies, particularly peanut, tree nut, seed and seafood allergies are less likely to decrease with age and tend to be lifelong allergies persisting in the majority (~ 75%) of children affected 14, 15. When food allergy develops for the first time in adults, it usually persists.
Some food allergies can be severe, causing life-threatening reactions known as anaphylaxis.
- Food allergy occurs in around 1 in 20 children and in about 2 in 100 adults.
- Studies have shown that food allergy affects 10% of children up to 1 year of age; between 4-8% of children aged up to 5 years of age and approximately 2% of adults.
- Hospital admissions for severe allergic reactions (anaphylaxis) have doubled over the last decade in Australia, USA and UK. In Australia, admissions for anaphylaxis due to food allergy in children aged 0 to 4 years are even higher, having increased five-fold over the same period.
Figure 2. Food allergy rash baby

Figure 3. Food allergy rash

When does food allergy develop?
Food allergy can develop at any age, but is most common in young children aged less than 5 years. Even young babies can develop symptoms of food allergy. Children with asthma, allergic rhinitis, atopic dermatitis, or an allergy to insect venom, medications, or latex are at an increased risk of developing food allergies 2.
Food allergy can sometimes be dangerous
Although mild, moderate and even severe allergic reactions (anaphylaxis) to foods are common. Deaths from anaphylaxis due to food allergy are rare in America. Most deaths can be prevented by careful allergen avoidance measures and immediate administration of an adrenaline auto-injector.
The most common foods causing life-threatening anaphylaxis are peanuts, tree nuts, shellfish, milk and egg. Symptoms of anaphylaxis affect your breathing and/or your heart.
Sometimes food allergy may be less obvious
Less common symptoms of food allergy include infantile colic, reflux of stomach contents, eczema, chronic diarrhea and failure to thrive in infants.
Not all adverse reactions to foods are due to allergy
The term allergy is often misused to describe any adverse reaction to foods which results in annoying (but ultimately harmless) symptoms such as headaches after overindulging in chocolate or red wine, or bloating after drinking a milkshake or eating too much pasta. While these reactions are not allergic, the result is a widespread impression that all adverse reactions to foods are trivial. Adverse reactions to foods that are not allergy include food intolerances, toxic reactions, food poisoning, enzyme deficiencies, food aversion or irritation from skin contact with certain foods. These adverse reactions are often mistaken for food allergy.
Why the rise in food allergy?
Scientists currently do not have clear information as to why food allergy seems to have increased so rapidly in recent years, particularly in young children. This area requires additional research studies, several of which are already underway.
Proposed explanations (which have not yet been proven in studies) include:
- Hygiene hypothesis, which proposes that less exposure to infections in early childhood, is associated with an increased risk of allergy. A more recent version of the hygiene hypothesis proposes that the make-up and type of the micro-organisms to which the mother, baby and infant is exposed and colonized with may alter allergic risk.
- Delayed introduction of allergenic foods such as egg, peanut or tree nuts.
- Methods of food processing, such as roasted versus boiled peanuts.
- Development of allergy to food by skin exposure such as the use of unrefined nut oil based moisturizers.
These areas require additional research studies, several of which are underway.
Food allergy does not run in the family
Most of the time, children with food allergy do not have parents with food allergy. However, if a family has one child with food allergy, their brothers and sisters are at a slightly higher risk of having food allergy themselves, although that risk is still relatively low.
Some parents want to have their other children screened for food allergy. If the test is negative, that may be reassuring, but does not mean that the other child will never develop an allergy in the future. If their screening test is positive, it is not always clear whether it definitely represents allergy. In this situation, a food challenge (under medical supervision) may be required to confirm the allergy.
Food Intolerance vs Food Allergy
Food intolerance also known as food sensitivity is a broad term that is used to describe a wide range of unwanted reactions (usually digestive system reactions) to certain foods, that cause symptoms after eating some foods 16. Food intolerance or food sensitivity occurs when something in food irritates a person’s digestive system or when a person is unable to properly digest, or break down, the food. The types of foods that trigger food sensitivity or food intolerance vary from individual to individual. Common foods that may cause food sensitivity include dairy products (e.g., cheddar cheese, cottage cheese, cow’s milk, mozzarella cheese, yogurt); egg white and egg yolk; grains (e.g., barley, bran, brown rice, gluten); fruits (e.g., apple, avocado, banana); meat (e.g., beef, chicken, lamb); and more. Consuming certain foods can cause various symptoms including stomach pain, cramps, nausea, diarrhea, bloating, gas/flatulence, diarrhea, vomiting, irritable bowel syndrome (IBS), rashes, hives (urticaria), recurrent mouth ulcers, heartburn, headaches and irritability or nervousness. Intolerance to lactose, which is found in milk and other dairy products, is the most common food sensitivity or food intolerance affecting about 10 percent of Americans. If food intolerances (food sensitivity) are not properly managed, these symptoms can adversely affect general health and wellbeing. Unfortunately, tests cannot easily identify most food sensitivities. While there are tests are available that look for dozens of types of antibodies called immunoglobulin-G (IgG) in the blood. Experts advise against this type of screening because it has not been shown to be accurate in identifying true food intolerance and sensitivities.
Many people who think they are allergic to a food may actually be intolerant to it. Some of the symptoms of food intolerance and food allergy are similar, but the differences between the two are very important. If you are allergic to a food, this allergen triggers a response in the immune system. Food allergy reactions can be life-threatening, so people with this type of allergy must be very careful to avoid their food triggers.
Being allergic to a food may also result in being allergic to a similar protein found in something else. For example, if you are allergic to ragweed, you may also develop reactions to bananas or melons. This is known as cross-reactivity. Cross-reactivity happens when the immune system thinks one protein is closely related to another. When foods are involved it is called oral allergy syndrome.
Food allergy can strike children and adults alike. While many children outgrow a food allergy, it is also possible for adults to develop allergies to particular foods.
Some foods are more likely to cause allergies than others. These include:
- dairy (including milk)
- peanuts
- walnuts, almonds, pine nuts, brazil nuts, pecans and other tree nuts
- soy
- grains that contain gluten (wheat, barley, rye and oats)
- fish and shellfish.
Most common food allergies
Nine foods are responsible for the majority of allergic reactions:
- Cow’s milk
- Eggs
- Fish
- Peanuts
- Sesame
- Shellfish
- Soy
- Tree nuts
- Wheat
Allergies to cow’s milk, eggs and peanuts are the most common in children.
Nine foods cause 90% of food allergic reactions, including cow’s milk, egg, peanut, tree nuts, sesame, soy, fish, shellfish and wheat. Peanut, tree nuts, shellfish, fish, sesame and egg are the most common food allergens in older children and adults. Other triggers such as herbal medicines, fruits and vegetables have been described and almost any food can cause an allergic reaction.
Complications of food allergy
Complications of food allergy can include:
- Anaphylaxis. This is a life-threatening allergic reaction.
- Atopic dermatitis (eczema). Food allergy may cause a skin reaction, such as eczema.
Food allergies signs and symptoms
Allergic reactions to food normally occur within minutes of eating the trigger food, though they can sometimes appear a few hours later. Symptoms of mild food allergy include:
- Hives (red circular weals on the skin) or red, itchy skin
- Stuffy or itchy nose, sneezing or itchy, teary eyes
- Vomiting, stomach cramps (discomfort or pain) or diarrhea
- Angioedema or swelling of the face or around the mouth
Allergic reactions may be mild, moderate or severe, and can be influenced by a number of factors
These factors include:
- the severity of the allergy
- the amount eaten
- the form of the food (liquid may sometimes be absorbed faster)
- whether it is eaten on its own or mixed in with other foods
- exercise around the same time as the meal, as this may worsen severity
- whether the food is cooked, as cooked food is sometimes better tolerated
- the presence or absence of asthma
- menstrual cycle in females
- intake of alcohol
Symptoms of severe allergy (anaphylaxis) may include:
- trouble breathing or noisy breathing
- difficulty talking more than a few words and/or hoarse voice
- wheeze
- cough
- swelling and tightness of the throat
- collapse
- light-headedness or dizziness
- diarrhea
- tingling in the hands, feet, lips or scalp
- swelling of tongue
- pale and floppy (in young children)
A severe allergic reaction (anaphylaxis) is a medical emergency. Call your local emergency immediately. Lay the person down. If they have an adrenaline injector and you are able to administer it, do so.
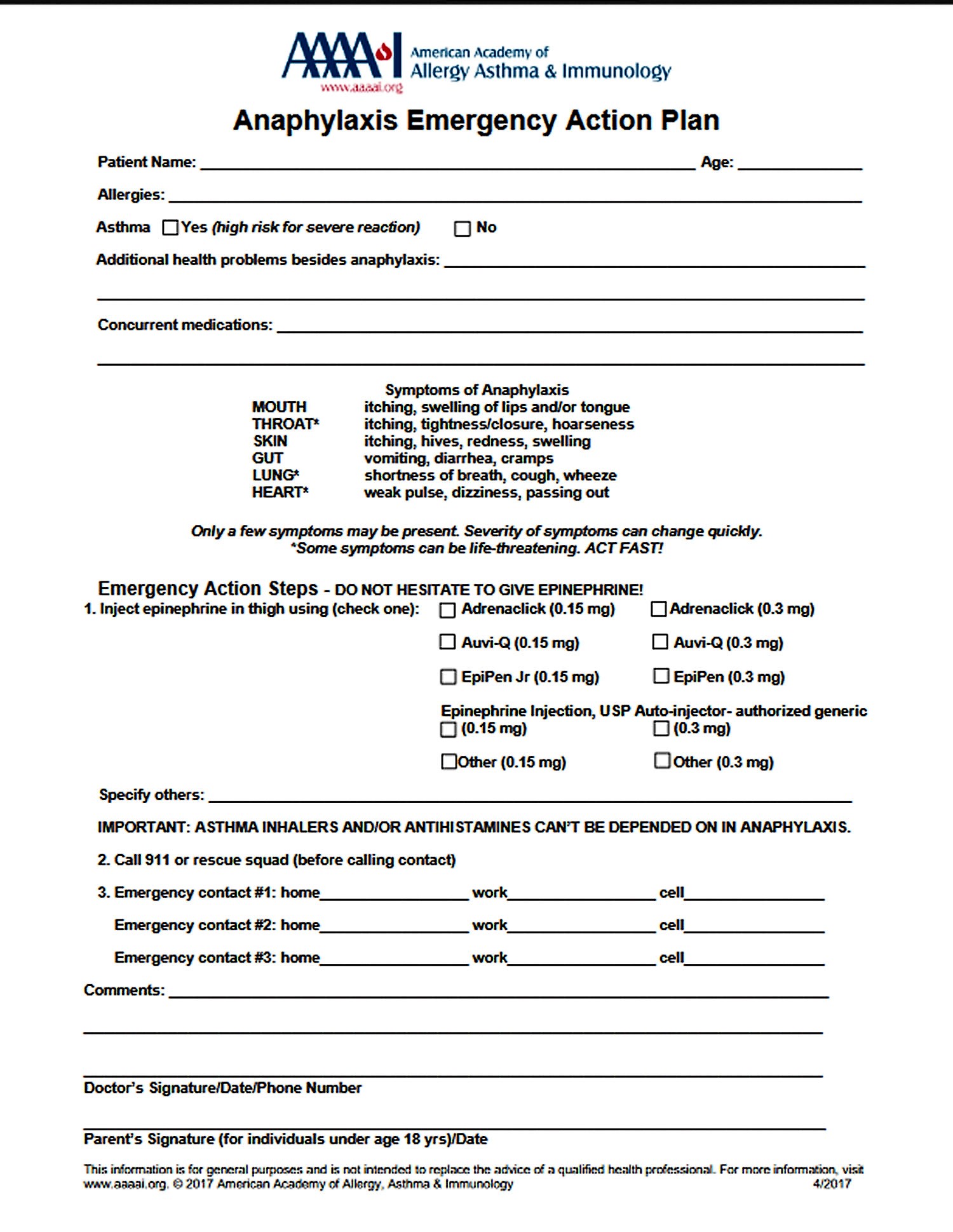
Figure 4. Anaphylaxis Emergency Action Plan
Causes of food allergies
When you have a food allergy, your immune system mistakenly identifies a specific food or a substance in food as something harmful. In response, your immune system triggers cells to release an antibody known as immunoglobulin E (IgE) to neutralize the allergy-causing food or food substance (the allergen).
The next time you eat even the smallest amount of that food, IgE antibodies sense it and signal your immune system to release a chemical called histamine, as well as other chemicals, into your bloodstream. These chemicals cause allergy symptoms.
In adults, the majority of food allergies are triggered by certain proteins in:
- Shellfish, such as shrimp, lobster and crab
- Peanuts
- Tree nuts, such as walnuts and pecans
- Fish
In children, food allergies are commonly triggered by proteins in:
- Peanuts
- Tree nuts
- Eggs
- Cow’s milk
- Wheat
- Soy
Pollen-food allergy syndrome (Oral Allergy Syndrome)
Also known as oral allergy syndrome, pollen-food allergy syndrome affects many people who have hay fever. In this condition, certain fresh fruits and vegetables or nuts and spices can trigger an allergic reaction that causes the mouth to tingle or itch. In serious cases, the reaction results in swelling of the throat or even anaphylaxis.
Proteins in certain fruits, vegetables, nuts and spices cause the reaction because they’re similar to allergy-causing proteins found in certain pollens. This is an example of cross-reactivity. These proteins can confuse the immune system in people with food or outdoor allergies.
For instance, if you are allergic to birch tree pollen, a primary airborne allergen responsible for symptoms in the springtime, you may have reactions triggered by peach, apple, pear, kiwi, plum, coriander, fennel, parsley, celery, cherry and carrot.
The most frequent reaction involves itchiness or swelling of the mouth, face, lip, tongue and throat. Symptoms usually appear immediately after eating raw fruits or vegetables, although the reaction can occur more than an hour later.
Rarely, oral allergy syndrome can cause severe throat swelling or anaphylaxis in a person who is highly allergic.
When you cook foods that trigger pollen-food allergy syndrome, your symptoms may be less severe.
This following table shows the specific fruits, vegetables, nuts and spices that can cause pollen-food allergy syndrome in people who are allergic to different pollens.
| If you are allergic to: | Birch pollen | Ragweed pollen | Grasses | Mugwort pollen |
|---|---|---|---|---|
| You may also have a reaction to: | Almond Apple Apricot Carrot Celery Cherry Hazelnut Peach Peanut Pear Plum Raw potatoes Soybean Some herbs and spices (anise, caraway, coriander, fennel, parsley) | Bananas Cucumber Melons (cantaloupe, honeydew and watermelon) Zucchini | Cucumber Melons (cantaloupe, honeydew and watermelon) Orange Peanut Tomatoes White potato Zucchini | Apples Bell pepper Broccoli Cabbage Carrots Celery Cauliflower Garlic Onion Peach Some herbs and spices (anise, black pepper, caraway seed, coriander, fennel, mustard, parsley) |
Food Protein-Induced Enterocolitis Syndrome
Food Protein-Induced Enterocolitis Syndrome, sometimes referred to as a delayed food allergy, is a severe condition causing vomiting and diarrhea. In some cases, symptoms can progress to dehydration and shock brought on by low blood pressure and poor blood circulation.
Much like other food allergies, Food Protein-Induced Enterocolitis Syndrome allergic reactions are triggered by ingesting a food allergen. Although any food can be a trigger, the most common culprits include milk, soy and grains. Food Protein-Induced Enterocolitis Syndrome often develops in infancy, usually when a baby is introduced to solid food or formula.
Eosinophilic Esophagitis
Eosinophilic Esophagitis is an allergic condition causing inflammation of the esophagus. The esophagus is the tube that sends food from the throat to the stomach. Most research suggests that the leading cause of Eosinophilic Esophagitis is an allergy or a sensitivity to particular proteins found in foods. Many people with Eosinophilic Esophagitis have a family history of allergic disorders such as asthma, rhinitis, dermatitis or food allergy.
Exercise-induced food allergy
Eating certain foods may cause some people to feel itchy and lightheaded soon after starting to exercise. Serious cases may even involve hives or anaphylaxis. Not eating for a couple of hours before exercising and avoiding certain foods may help prevent this problem.
Food intolerance and other reactions
A food intolerance or a reaction to another substance you ate may cause the same signs and symptoms as a food allergy does — such as nausea, vomiting, cramping and diarrhea.
Depending on the type of food intolerance you have, you may be able to eat small amounts of problem foods without a reaction. By contrast, if you have a true food allergy, even a tiny amount of food may trigger an allergic reaction.
One of the tricky aspects of diagnosing food intolerance is that some people are sensitive not to the food itself but to a substance or ingredient used in the preparation of the food.
Common conditions that can cause symptoms mistaken for a food allergy include:
- Absence of an enzyme needed to fully digest a food. You may not have adequate amounts of some enzymes needed to digest certain foods. Insufficient quantities of the enzyme lactase, for example, reduce your ability to digest lactose, the main sugar in milk products. Lactose intolerance can cause bloating, cramping, diarrhea and excess gas.
- Food poisoning. Sometimes food poisoning can mimic an allergic reaction. Bacteria in spoiled tuna and other fish also can make a toxin that triggers harmful reactions.
- Sensitivity to food additives. Some people have digestive reactions and other symptoms after eating certain food additives. For example, sulfites used to preserve dried fruit, canned goods and wine can trigger asthma attacks in sensitive people.
- Histamine toxicity. Certain fish, such as tuna or mackerel, that are not refrigerated properly and that contain high amounts of bacteria may also contain high levels of histamine that trigger symptoms similar to those of food allergy. Rather than an allergic reaction, this is known as histamine toxicity or scombroid poisoning.
- Celiac disease. While celiac disease is sometimes referred to as a gluten allergy, it does not result in anaphylaxis. Like a food allergy, it does involve an immune system response, but it’s a unique reaction that’s more complex than a simple food allergy. This chronic digestive condition is triggered by eating gluten, a protein found in bread, pasta, cookies, and many other foods containing wheat, barley or rye. If you have celiac disease and eat foods containing gluten, an immune reaction occurs that causes damage to the surface of your small intestine, leading to an inability to absorb certain nutrients.
Risk factors for food allergies
Food allergy risk factors include:
- Family history. You’re at increased risk of food allergies if asthma, eczema, hives or allergies such as hay fever are common in your family.
- Other allergies. If you’re already allergic to one food, you may be at increased risk of becoming allergic to another. Similarly, if you have other types of allergic reactions, such as hay fever or eczema, your risk of having a food allergy is greater.
- Age. Food allergies are more common in children, especially toddlers and infants. As children grow older, their digestive systems mature and their bodies are less likely to absorb food or food components that trigger allergies. Fortunately, children typically outgrow allergies to milk, soy, wheat and eggs. Severe allergies and allergies to nuts and shellfish are more likely to be lifelong.
- Asthma. Asthma and food allergy commonly occur together. When they do, both food allergy and asthma symptoms are more likely to be severe.
Factors that may increase your risk of developing an anaphylactic reaction include:
- Having a history of asthma
- Being a teenager or younger
- Delaying use of epinephrine to treat your food allergy symptoms
- Not having hives or other skin symptoms.
Prevention of food allergy
The best way to prevent an allergic reaction is to know and avoid foods that cause signs and symptoms. For some people, this is a mere inconvenience, but others find it a greater hardship. Also, some foods — when used as ingredients in certain dishes — may be well-hidden. This is especially true in restaurants and in other social settings.
If you know you have a food allergy, follow these steps:
- Know what you’re eating and drinking. Be sure to read food labels carefully.
- If you have already had a severe reaction, wear a medical alert bracelet or necklace that lets others know that you have a food allergy in case you have a reaction and you’re unable to communicate.
- Talk with your doctor about prescribing emergency epinephrine. You may need to carry an epinephrine autoinjector (Adrenaclick, EpiPen) if you’re at risk of a severe allergic reaction.
- Be careful at restaurants. Be certain your server or chef is aware that you absolutely can’t eat the food you’re allergic to, and you need to be completely certain that the meal you order doesn’t contain it. Also, make sure food isn’t prepared on surfaces or in pans that contained any of the food you’re allergic to. Don’t be reluctant to make your needs known. Restaurant staff members are usually more than happy to help when they clearly understand your request.
- Plan meals and snacks before leaving home. If necessary, take a cooler packed with allergen-free foods when you travel or go to an event. If you or your child can’t have the cake or dessert at a party, bring an approved special treat so no one feels left out of the celebration.
If your child has a food allergy, take these precautions to ensure his or her safety:
- Notify key people that your child has a food allergy. Talk with child care providers, school personnel, parents of your child’s friends and other adults who regularly interact with your child. Emphasize that an allergic reaction can be life-threatening and requires immediate action. Make sure that your child also knows to ask for help right away if he or she reacts to food.
- Explain food allergy symptoms. Teach the adults who spend time with your child how to recognize signs and symptoms of an allergic reaction.
- Write an action plan. Your plan should describe how to care for your child when he or she has an allergic reaction to food. Provide a copy of the plan to your child’s school nurse and others who care for and supervise your child.
- Have your child wear a medical alert bracelet or necklace. This alert lists your child’s allergy symptoms and explains how others can provide first aid in an emergency.
Early exposure
Currently, the recommendations are to introduce complementary solid foods, such as egg, peanut products, fish, wheat, and other allergenic foods one at a time after four to six months of age when breastfeeding, as there is no need to avoid or delay their introduction 1. However, before introducing allergenic foods, talk with your child’s doctor about the best time to offer them.
Early introduction of peanut products has been associated with a lower risk of peanut allergy 17, 18. In a recent study, high-risk infants — such as those with atopic dermatitis or egg allergy or both — were selected to either ingest or avoid peanut products from 4 to 6 months of age until 5 years of age 19, 20, 21, 22.
Researchers found that high-risk children who regularly consumed peanut protein, such as peanut butter or peanut-flavored snacks, were around 80% less likely to develop a peanut allergy 23.
Food allergy testing
There’s no perfect test used to confirm or rule out a food allergy. Your doctor will consider a number of factors before making a diagnosis. Proper diagnosis of food allergies is extremely important. Studies have shown that many suspected food allergies are actually caused by other conditions such as a food intolerance. Skin tests and blood tests are often ordered. A food challenge under the care of your allergist / immunologist may also be needed to confirm an allergy.
It is important to note that:
- Allergy test results cannot be used on their own and must be considered together with your clinical history.
- Medicare rebates are available for skin prick tests or blood tests for allergen specific IgE (formerly known as RAST).
- In some cases, you may be referred to a clinical immunology/allergy specialist for further detailed assessment.
Skin prick allergy tests or allergy blood tests help to confirm or exclude potential triggers. Sometimes a temporary elimination diet under close medical and dietetic supervision will be needed, followed by food challenges to identify the cause. Long term unsupervised restricted diets should not be undertaken, as this can lead to malnutrition and other complications such as food aversion.
While the results of allergy testing are a useful guide in determining whether the person is allergic, they do not provide a reliable guide to whether the reaction will be mild or severe.
Skin prick testing
Skin prick testing is the most convenient method of allergy testing and has been shown in clinical studies to improve the diagnosis of allergy. As results are available within 20 minutes, this allows you to discuss the outcome with your doctor at the time of testing.
Most commonly performed on the forearm or the back, the skin is first cleaned with alcohol. It may be marked with numbers corresponding to the allergens. Using a sterile lancet, a small prick is made through a drop of allergen extract. This allows a small amount of allergen to enter the skin.
To see if your skin is reacting normally, two additional substances are scratched into your skin’s surface:
- Histamine. In most people, this substance causes a skin response. If you don’t react to histamine, your allergy skin test may not reveal an allergy even if you have one.
- Glycerin or saline. In most people, these substances don’t cause any reaction. If you do react to glycerin or saline, you may have sensitive skin. Test results will need to be interpreted cautiously to avoid a false allergy diagnosis.
If you are allergic to the tested allergen, a small itchy lump (wheal) surrounded by a red flare will appear within 15-20 minutes.
Skin prick tests are slightly uncomfortable but are usually well tolerated, even by small children. Local itch and swelling normally subside within 1-2 hours. More prolonged or severe swelling may be treated with a non-sedating antihistamine, a painkiller tablet and/or a cool compress. Occasionally people will feel dizzy or light-headed and need to lie down. Severe allergic reactions from allergy testing for asthma or allergic rhinitis (hay fever) are very rare.
Skin prick testing should only be performed by a health professional who has been trained in the procedure and who knows how to select the allergens, interpret the results and deal with any generalized allergic reaction that might very rarely occur.
Antihistamine tablets/syrups or medications with antihistamine-like actions (such as some cold remedies and antidepressants) should not be taken for 3-7 days before testing as these will interfere with the results. You may also be advised to avoid creams and moisturisers on your forearms on the day of the test to reduce the likelihood that allergen extracts will run into each other.
Skin prick testing has no value in the investigation of suspected reactions to aspirin, food additives, or respiratory irritants like smoke or perfumes.
Your doctor may advise against skin testing if you:
- Have ever had a severe allergic reaction. You may be so sensitive to certain substances that even the tiny amounts used in skin tests could trigger a life-threatening reaction (anaphylaxis).
- Take medications that could interfere with test results. These include antihistamines, many antidepressants and some heartburn medications. Your doctor may determine that it’s better for you to continue taking these medications than to temporarily discontinue them in preparation for a skin test.
- Have certain skin conditions. If severe eczema or psoriasis affects large areas of skin on your arms and back — the usual testing sites — there may not be enough clear, uninvolved skin to do an effective test. Other skin conditions, such as dermatographism, can cause unreliable test results.
Blood tests (in vitro immunoglobulin E antibody tests) can be useful for those who shouldn’t undergo skin tests. Blood tests aren’t done as often as skin tests because they can be less sensitive than skin tests and are more expensive.
In general, allergy skin tests are most reliable for diagnosing allergies to airborne substances, such as pollen, pet dander and dust mites. Skin testing may help diagnose food allergies. But because food allergies can be complex, you may need additional tests or procedures.
Allergy skin test preparation
Before recommending a skin test, your doctor will ask you detailed questions about your medical history, your signs and symptoms, and your usual way of treating them. Your answers can help your doctor determine if allergies run in your family and if an allergic reaction is most likely causing your symptoms. Your doctor may also perform a physical examination to search for additional clues about the cause of your signs and symptoms.
Medications can interfere with allergy skin test results
Before scheduling a skin test, bring your doctor a list of all of your prescription and over-the-counter medications. Some medications can suppress allergic reactions, preventing the skin testing from giving accurate results. Other medications may increase your risk of developing a severe allergic reaction during a test.
Because medications clear out of your system at different rates, your doctor may ask that you stop taking certain medications for up to 10 days.
Medications that can interfere with skin tests include:
- Prescription antihistamines, such as levocetirizine (Xyzal) and desloratadine (Clarinex).
- Over-the-counter antihistamines, such as loratadine (Claritin, Alavert), diphenhydramine (Benadryl, others), chlorpheniramine (Chlor-Trimeton), cetirizine (Zyrtec, others) and fexofenadine (Allegra).
- Tricyclic antidepressants, such as nortriptyline (Pamelor) and desipramine (Norpramin).
- Certain heartburn medications, such as cimetidine (Tagamet) and ranitidine (Zantac).
- The asthma medication omalizumab (Xolair). This medication can disrupt test results for six months or longer even after you quit using it (most medications affect results for days to weeks).
Other skin testing methods
Scratch testing was used in the past but it is less reliable than skin prick testing, and causes much greater discomfort. Intradermal skin testing may be used to test for allergies to antibiotic drugs or stinging insect venom, when greater sensitivity is needed. Intradermal testing should not be used to test for allergy to inhalants or foods.
A positive allergy test is not the same as being food allergic
It is important to know that a positive skin prick allergy test or allergy blood test means that the body’s immune system has produced a response to a food, but sometimes these are false positives. In other words, the test may be positive yet the person can actually eat the food without any symptoms. For this reason, it is important to confirm the significance of a positive allergy test (in some circumstances) with a supervised food challenge. In a child with a positive test of uncertain meaning, this is often done around school entry age under medical supervision. Interpretation of test results (and whether challenge should be undertaken) should be discussed with your doctor.
Food allergy blood test for allergen specific IgE (formerly known as RAST)
Immunoglobulin E (IgE) antibodies directed against specific allergens can be measured with a blood test, formerly referred to as RAST tests (RAST was the abbreviation for the original name of the technology – RadioAllergoSorbent Test). These tests are often performed when skin testing is not easily available, when skin conditions such as severe eczema preclude skin prick testing, or when a person is taking medications (such as antihistamines) that interfere with accurate skin prick testing.
Total IgE testing
Measurement of total IgE antibodies can be estimated from a blood sample. Total IgE may be raised in people with allergies. High total IgE antibody levels are also found in people with parasite infections, eczema and some rare medical conditions. High IgE levels do not prove that symptoms are due to allergy, and a normal IgE level does not exclude allergy. Therefore, measuring total IgE levels is not routinely recommended in allergy testing.
Eosinophil counts
Eosinophils are specialised white blood cells that are designed to kill worms and parasites. They can also cause tissue inflammation in allergy. High levels are sometimes seen in blood samples from people with allergic rhinitis (hay fever), asthma and eczema, as well as in a number of less common conditions. However, a high eosinophil count does not prove that symptoms are due to allergy, and a normal eosinophil count does not exclude allergy. Therefore measuring eosinophil counts has a limited role to play in allergy testing.
Patch testing
Patch testing is useful for testing for allergic contact dermatitis, such as that triggered by metal, cosmetic preservatives or various plants. Using hypoallergenic tape, commercial standardized allergen paste is applied to a rash-free area of skin, most commonly the individual’s back. The tapes are left in place for 48 hours and kept dry for the entire time. The test site is then read at different time intervals. An eczema-like rash can indicate sensitivity to a particular allergen.
Elimination diet
If you have a suspected food allergy, you may be advised to avoid eating a particular food to see if your symptoms improve.
After a few weeks, you may then be asked to eat the food again to check if you have another reaction.
Don’t attempt to do this yourself without discussing it with a qualified healthcare professional.
Oral food challenge testing
Oral food challenge testing may sometimes be required to confirm diagnosis when the cause of a severe allergic reaction has not been confirmed. This will normally only be performed using foods or medications under the supervision of a clinical immunology/allergy specialist with appropriate resuscitation facilities immediately available. If you don’t have a reaction during this test, you may be able to include this food in your diet again.
Unproven methods
There are several methods that claim to test for allergy. These include cytotoxic food testing, kinesiology, Vega testing, electrodermal testing, pulse testing, reflexology, hair analysis, allergy elimination techniques, iridology, Alcat testing, Rinkel’s intradermal skin testing, reflexology and IgG food antibody testing. These have no scientific basis, are unreliable and have no useful role in the assessment of allergy 24. These techniques have not been shown to be reliable or reproducible when subjected to formal study. Australasian Society of Clinical Immunology and Allergy advises against the use of these tests for diagnosis or to guide medical treatment. No Medicare rebate is available for these tests and their use is also not supported.
Adverse consequences may also arise from unorthodox testing and treatments. Treatment based on inaccurate, false positive or clinically irrelevant results is not only misleading, but can lead to ineffective and at times expensive treatments, and delay more effective therapy. Sometimes harmful therapy may result, such as dangerous avoidance strategies and risk of malnutrition, particularly in children.
When considering testing and treatment, advice needs to be evidence based. In other words, there needs to be evidence that a particular test or treatment is reliable, based on studies of other patients with the same condition.
Reliable tests need to be able to distinguish between those with illness and those without. Therapeutic trials are designed to show that any improvement seen is due to the treatment, and not just due to chance or coincidence. Such studies also examine whether a particular treatment may also cause harm as well as benefit.
These tests have not been scientifically validated and may lead to unnecessary, costly and (in the case of some changes in diet).
Food allergies treatments
The only way to avoid an allergic reaction is to avoid the foods that cause signs and symptoms. However, despite your best efforts, you may come into contact with a food that causes a reaction.
For a minor allergic reaction, over-the-counter or prescribed antihistamines may help reduce symptoms. These drugs can be taken after exposure to an allergy-causing food to help relieve itching or hives. However, antihistamines can’t treat a severe allergic reaction.
For a severe allergic reaction, you may need an emergency injection of epinephrine and a trip to the emergency room. Many people with allergies carry an epinephrine autoinjector (Adrenaclick, EpiPen). This device is a combined syringe and concealed needle that injects a single dose of medication when pressed against your thigh.
If your doctor has prescribed an epinephrine autoinjector:
- Be sure you know how to use the autoinjector. Also, make sure the people closest to you know how to administer the drug — if they’re with you in an anaphylactic emergency, they could save your life.
- Carry it with you at all times. It may be a good idea to keep an extra autoinjector in your car or in your desk at work.
Always be sure to replace epinephrine before its expiration date or it may not work properly.
Experimental treatments
While there’s ongoing research to find better treatments to reduce food allergy symptoms and prevent allergy attacks, there isn’t any proven treatment that can prevent or completely relieve symptoms.
Treatments being studied are:
Anti-IgE therapy. The medication omalizumab (Xolair) interferes with the body’s ability to use IgE. The drug is currently being studied for treatment of allergic asthma and food allergies.
This treatment is still considered experimental, and more research needs to be done on the drug’s long-term safety. It has been associated with a potential increased risk of anaphylaxis.
Oral immunotherapy. Researchers have been studying the use of oral immunotherapy as a treatment for food allergy. Small doses of the food you’re allergic to are swallowed or placed under your tongue (sublingual). The dose of the allergy-provoking food is gradually increased.
Initial results look promising, even in people with peanut, egg and milk allergies. But more research needs to be done to ensure that this treatment is safe.
Early exposure. In the past, it’s been generally recommended that children avoid allergenic foods to reduce the likelihood of developing allergies. But in a recent study, high-risk infants — such as those with atopic dermatitis or egg allergy or both — were selected to either ingest or avoid peanut products from 4 to 11 months of age until 5 years of age.
Researchers found that high-risk children who regularly consumed peanut protein, such as peanut butter or peanut-flavored snacks, were 70 to 86 percent less likely to develop a peanut allergy. These findings may impact food allergy guidelines in the future.
Living with your food allergy
As there is currently no cure for food allergy, strict avoidance is essential in the management of food allergy.
The good news is that people with food allergy can learn to live with their condition with the guidance of their clinical immunology/allergy specialist and a network of supportive contacts.
It is important for individuals with food allergy to:
- Carry their adrenaline (epinephrine) autoinjector (if prescribed) and Allergy Action Plan with them at all times;
- Know the signs and symptoms of mild to moderate and severe allergic reactions (anaphylaxis) and what to do when a reaction occurs;
- Read and understand food labels for food allergy;
- Tell wait staff that they have a food allergy when eating out;
- Be aware of cross contamination of food allergens when preparing food.
Don’t assume. Always read food labels to make sure they don’t contain an ingredient you’re allergic to. Even if you think you know what’s in a food, check the label. Ingredients sometimes change.
Food labels are required to clearly list whether they contain any common food allergens. Read food labels carefully to avoid the most common sources of food allergens: milk, eggs, peanuts, tree nuts, fish, shellfish, soy and wheat.
When in doubt, say no thanks. At restaurants and social gatherings, you’re always taking a risk that you might eat a food you’re allergic to. Many people don’t understand the seriousness of an allergic food reaction and may not realize that a tiny amount of a food can cause a severe reaction in some people.
If you have any suspicion at all that a food may contain something you’re allergic to, steer clear.
Involve caregivers. If your child has a food allergy, enlist the help of relatives, baby sitters, teachers and other caregivers. Make sure that they understand how important it is for your child to avoid the allergy-causing food and they know what to do in an emergency.
It’s also important to let caregivers know what steps they can take to prevent a reaction in the first place, such as careful hand-washing and cleaning any surfaces that might have come in contact with the allergy-causing food.
Food allergy prognosis
About 6% of children experience food allergic reactions in the first three years of life, including approximately 2.5% with cow’s milk allergy, 1.5% with egg allergy, and 1% with peanut allergy 1. Over time, most children outgrow or become tolerant of food allergens to eggs, milk, wheat, and soy 1. However, allergies to nuts and shellfish are more long-standing 14, 15. Close to 20% of children have a resolution of their food allergy by school age 1. The non-IgE mediated food allergies resolve within the first year of life. Unfortunately, sporadic cases of fatal anaphylactic reactions still continue to occur 1.
- Lopez CM, Yarrarapu SNS, Mendez MD. Food Allergies. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482187[↩][↩][↩][↩][↩][↩][↩]
- Bright DM, Stegall HL, Slawson DC. Food Allergies: Diagnosis, Treatment, and Prevention. Am Fam Physician. 2023 Aug;108(2):159-165. https://www.aafp.org/pubs/afp/issues/2023/0800/food-allergies.html[↩][↩]
- Barni S, Liccioli G, Sarti L, Giovannini M, Novembre E, Mori F. Immunoglobulin E (IgE)-Mediated Food Allergy in Children: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Management. Medicina (Kaunas). 2020 Mar 4;56(3):111. doi: 10.3390/medicina56030111[↩]
- Boyce JA, Assa’ad A, Burks AW, et al. NIAID-Sponsored Expert Panel. Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report. J Allergy Clin Immunol. 2010 Dec;126(6):1105-18. doi: 10.1016/j.jaci.2010.10.008[↩][↩]
- Chang KL, Guarderas JC. Allergy Testing: Common Questions and Answers. Am Fam Physician. 2018 Jul 1;98(1):34-39. https://www.aafp.org/pubs/afp/issues/2018/0701/p34.html[↩]
- Budimir J, Mravak-Stipetić M, Bulat V, Ferček I, Japundžić I, Lugović-Mihić L. Allergic reactions in oral and perioral diseases-what do allergy skin test results show? Oral Surg Oral Med Oral Pathol Oral Radiol. 2019 Jan;127(1):40-48. doi: 10.1016/j.oooo.2018.08.001[↩]
- Sicherer SH, Sampson HA. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol. 2018 Jan;141(1):41-58. doi: 10.1016/j.jaci.2017.11.003[↩]
- Burks AW, Tang M, Sicherer S, Muraro A, Eigenmann PA, Ebisawa M, Fiocchi A, Chiang W, Beyer K, Wood R, Hourihane J, Jones SM, Lack G, Sampson HA. ICON: food allergy. J Allergy Clin Immunol. 2012 Apr;129(4):906-20. doi: 10.1016/j.jaci.2012.02.001[↩]
- NIAID-Sponsored Expert Panel; Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, et al. Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010 Dec;126(6 Suppl):S1-58. doi: 10.1016/j.jaci.2010.10.007[↩]
- Sampson HA, Aceves S, Bock SA, James J, et al. Food allergy: a practice parameter update-2014. J Allergy Clin Immunol. 2014 Nov;134(5):1016-25.e43. doi: 10.1016/j.jaci.2014.05.013[↩]
- Sampson HA. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J Allergy Clin Immunol. 2001 May;107(5):891-6. doi: 10.1067/mai.2001.114708[↩][↩]
- Chinthrajah RS, Tupa D, Prince BT, Block WM, Rosa JS, Singh AM, Nadeau K. Diagnosis of Food Allergy. Pediatr Clin North Am. 2015 Dec;62(6):1393-408. doi: 10.1016/j.pcl.2015.07.009[↩][↩]
- Muraro A., Werfel T., Hoffmann-Sommergruber K., Roberts G., Beyer K., Bindslev-Jensen C., Cardona V., Dubois A., duToit G., Eigenmann P., et al. EAACI Food Allergy and Anaphylaxis Guidelines Group. EAACI food allergy and anaphylaxis guidelines: Diagnosis and management of food allergy. Allergy. 2014;69:1008–1025. doi: 10.1111/all.12429[↩]
- Rial MJ, Sastre J. Food Allergies Caused by Allergenic Lipid Transfer Proteins: What Is behind the Geographic Restriction? Curr Allergy Asthma Rep. 2018 Sep 11;18(11):56. doi: 10.1007/s11882-018-0810-x[↩][↩]
- Shroba J, Rath N, Barnes C. Possible Role of Environmental Factors in the Development of Food Allergies. Clin Rev Allergy Immunol. 2019 Dec;57(3):303-311. doi: 10.1007/s12016-018-8703-2[↩][↩]
- Food Intolerance. https://www.allergy.org.au/patients/food-other-adverse-reactions/food-intolerance[↩]
- Fleischer DM, Sicherer S, Greenhawt M, et al. American Academy of Allergy, Asthma & Immunology; American Academy of Pediatrics, American College of Allergy; Asthma & Immunology, Australasian Society of Clinical Immunology and Allergy; Canadian Society of Allergy and Clinical Immunology; European Academy of Allergy and Clinical Immunology; Israel Association of Allergy and Clinical Immunology; Japanese Society for Allergology; Society for Pediatric Dermatology; World Allergy Organization. Consensus communication on early peanut introduction and the prevention of peanut allergy in high-risk infants. J Allergy Clin Immunol. 2015 Aug;136(2):258-61. doi: 10.1016/j.jaci.2015.06.001. Epub 2015 Jun 20. Erratum in: J Allergy Clin Immunol. 2015 Dec;136(6):1710.[↩]
- Perkin MR, Logan K, Marrs T, Radulovic S, Craven J, Flohr C, Lack G; EAT Study Team. Enquiring About Tolerance (EAT) study: Feasibility of an early allergenic food introduction regimen. J Allergy Clin Immunol. 2016 May;137(5):1477-1486.e8. doi: 10.1016/j.jaci.2015.12.1322[↩]
- Du Toit G, Sayre PH, Roberts G, Sever ML, Lawson K, Bahnson HT, Brough HA, Santos AF, Harris KM, Radulovic S, Basting M, Turcanu V, Plaut M, Lack G; Immune Tolerance Network LEAP-On Study Team. Effect of Avoidance on Peanut Allergy after Early Peanut Consumption. N Engl J Med. 2016 Apr 14;374(15):1435-43. doi: 10.1056/NEJMoa1514209[↩]
- Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, Brough HA, Phippard D, Basting M, Feeney M, Turcanu V, Sever ML, Gomez Lorenzo M, Plaut M, Lack G; LEAP Study Team. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. 2015 Feb 26;372(9):803-13. doi: 10.1056/NEJMoa1414850. Epub 2015 Feb 23. Erratum in: N Engl J Med. 2016 Jul 28;375(4):398.[↩]
- Roduit C, Frei R, Depner M, Schaub B, Loss G, Genuneit J, Pfefferle P, Hyvärinen A, Karvonen AM, Riedler J, Dalphin JC, Pekkanen J, von Mutius E, Braun-Fahrländer C, Lauener R; PASTURE study group. Increased food diversity in the first year of life is inversely associated with allergic diseases. J Allergy Clin Immunol. 2014 Apr;133(4):1056-64. doi: 10.1016/j.jaci.2013.12.1044[↩]
- Bunyavanich S, Rifas-Shiman SL, Platts-Mills TA, Workman L, Sordillo JE, Camargo CA Jr, Gillman MW, Gold DR, Litonjua AA. Peanut, milk, and wheat intake during pregnancy is associated with reduced allergy and asthma in children. J Allergy Clin Immunol. 2014 May;133(5):1373-82. doi: 10.1016/j.jaci.2013.11.040[↩]
- Yu W, Freeland DMH, Nadeau KC. Food allergy: immune mechanisms, diagnosis and immunotherapy. Nat Rev Immunol. 2016 Dec;16(12):751-765. doi: 10.1038/nri.2016.111[↩]
- Unorthodox testing and treatment for allergic disorders. https://www.allergy.org.au/patients/allergy-testing/unorthodox-testing-and-treatment[↩]





{kind=link}