What is frostbite
Frostbite is damage to skin and tissue caused by exposure to freezing temperatures – typically any temperature below -0.55 °C (31 °F). Frostbite can affect any part of your body, but the extremities, such as the hands, feet, ears, nose and lips, are most likely to be affected.
Frostbite is freezing of the skin that occurs due to exposure to cold temperatures. Frostbite often starts out with mild symptoms and can progress and become quite severe and even limb-threatening.
Mild frostbite is considered skin that is either red and painful, or white and numb. Severe frostbite includes blistering skin, hard skin (due to frozen bone and blood vessels), and possibly gangrene (tissue that has died and turned black, after blood vessels became frozen).
Frostbite is often associated with hypothermia.
The symptoms of frostbite usually begin with the affected parts feeling cold and painful. Frostnip, the first stage of frostbite, doesn’t cause permanent skin damage. You can treat very mild frostbite with first-aid measures, including rewarming your skin. All other frostbite requires medical attention because it can damage skin, tissues, muscle and bones. Possible complications of severe frostbite include infection and nerve damage.
If exposure to the cold continues, you may feel pins and needles before the area becomes numb, as the tissues freeze.
- If you think you or someone else may have frostbite, see your doctor for advice.
- If the symptoms are more severe or there are signs of hypothermia.
Signs and symptoms of hypothermia include:
- Intense shivering
- Fast breathing (hyperventilation)
- Slurred speech
- Drowsiness and loss of coordination
- Cold and pale skin
- Tiredness
- Confusion
Hypothermia is a dangerous drop in body temperature below 35 °C (95 °F). Normal body temperature is around 37 °C (98.6 °F).
The symptoms above are for mild hypothermia, where someone’s body temperature is between 32 °C (89.6 °F) and 35 °C (95 °F).
If their temperature drops to 32 °C (89.6 °F) or lower, they’ll usually stop shivering completely and may pass out.
This is a sign that their condition is getting worse and emergency medical help is needed.
Hypothermia can be serious if not treated quickly. You should call your local emergency number and get emergency medical help if you suspect hypothermia.
Give first aid if you notice signs of hypothermia.
First aid for hypothermia
You need to warm the person up.
Follow these five steps:
- Move them indoors.
- Remove any wet clothing and dry them.
- Wrap them in blankets.
- Give them a warm non-alcoholic drink, but only if they can swallow normally.
- Give energy food that contains sugar, such as a chocolate bar, but only if they can swallow normally.
If the person can’t be moved indoors, find something for them to rest on to protect them from the cold ground, like a towel or a blanket.
If they don’t appear to be breathing – and you know how to do it – give them CPR (cardiopulmonary resuscitation), but you must continue this until professional help arrives in the form of the ambulance service or a medical team.
Things to avoid
Some things can make hypothermia worse:
- DON’T put the person into a hot bath.
- DON’T massage their limbs.
- DON’T use heating lamps.
- DON’T give them alcohol to drink.
These actions can cause the heart to suddenly stop beating (cardiac arrest).
Who’s at risk of frostbite?
Frostbite occurs most often to those exposed to extreme cold, so people who participate in cold-weather outdoor activities or live in or travel to cold climates are most at risk. Frostbite can also occur in those exposed to high winds, those with poor circulation, those in cramped positions who have tight-fitting clothing or boots, and those suffering from fatigue. Additionally, certain diseases and medications, alcohol consumption, and smoking increase risk for frostbite.
Frostbite stages
The symptoms of frostbite progress in three stages.
The colder the temperature and the longer the body is exposed to freezing conditions, the more advanced frostbite can become.
Figure 1. Frostbite stages

Early stage (frostnip)
During the early stage of frostbite, you’ll experience pins and needles, throbbing or aching in the affected area. Your skin will become cold, numb and white, and you may feel a tingling sensation.
This mild frostbite is known as frostnip, and it often affects people who live or work in cold climates. The extremities, such as the fingers, nose, ears and toes, are most commonly affected.
Frostnip doesn’t permanently damage the skin and can be treated with first-aid measures.
Intermediate stage (superficial frostbite)
After these early signs of frostbite, prolonged exposure to cold temperatures will cause more tissue damage. The affected area will feel hard and frozen.
When you’re out of the cold and the tissue has thawed out, the skin will turn red and blister, which can be painful. A fluid-filled blister may appear 24 to 36 hours after rewarming the skin. There may also be swelling and itching.
This is known as superficial frostbite as it affects the top layers of skin and tissue. The skin underneath the blisters is usually still intact, but treatment is needed to make sure there’s no lasting damage.
Advanced stage
When exposure to the cold continues, frostbite becomes increasingly severe. The skin becomes white, blue or blotchy, and the tissue underneath feels hard and cold to touch.
Further damage may occur beneath the skin to tendons, muscles, nerves and bones. With deep frostbite, you may experience numbness. Joints or muscles may no longer work. This is known as deep frostbite and requires urgent medical attention.
As the skin thaws, blood-filled blisters form and turn into thick black scabs. Large blisters form 24 to 48 hours after rewarming. Afterward, the area turns black and hard as the tissue dies. This is known as tissue necrosis, and the affected tissue may have to be removed to prevent infection.
Long-term effects
People with a history of severe frostbite often report further long-term effects of frostbite.
These can include:
- increased sensitivity to cold
- numbness in the affected body parts, most commonly the fingers
- reduced sense of touch in the affected body parts
- persistent pain in the affected body parts.
Frostbite long-term effects
After having frostbite, some people are left with permanent problems, such as increased sensitivity to cold, numbness, stiffness and pain in the affected area.
Unfortunately, not much can be done to treat sensitivity to cold, numbness or stiffness. A medication called amitriptyline can sometimes be effective at controlling the pain associated with the long-term effects of frostbite.
What does frostbite look like
Figure 2. Frostbite hands

Figure 3. Frostbite on face
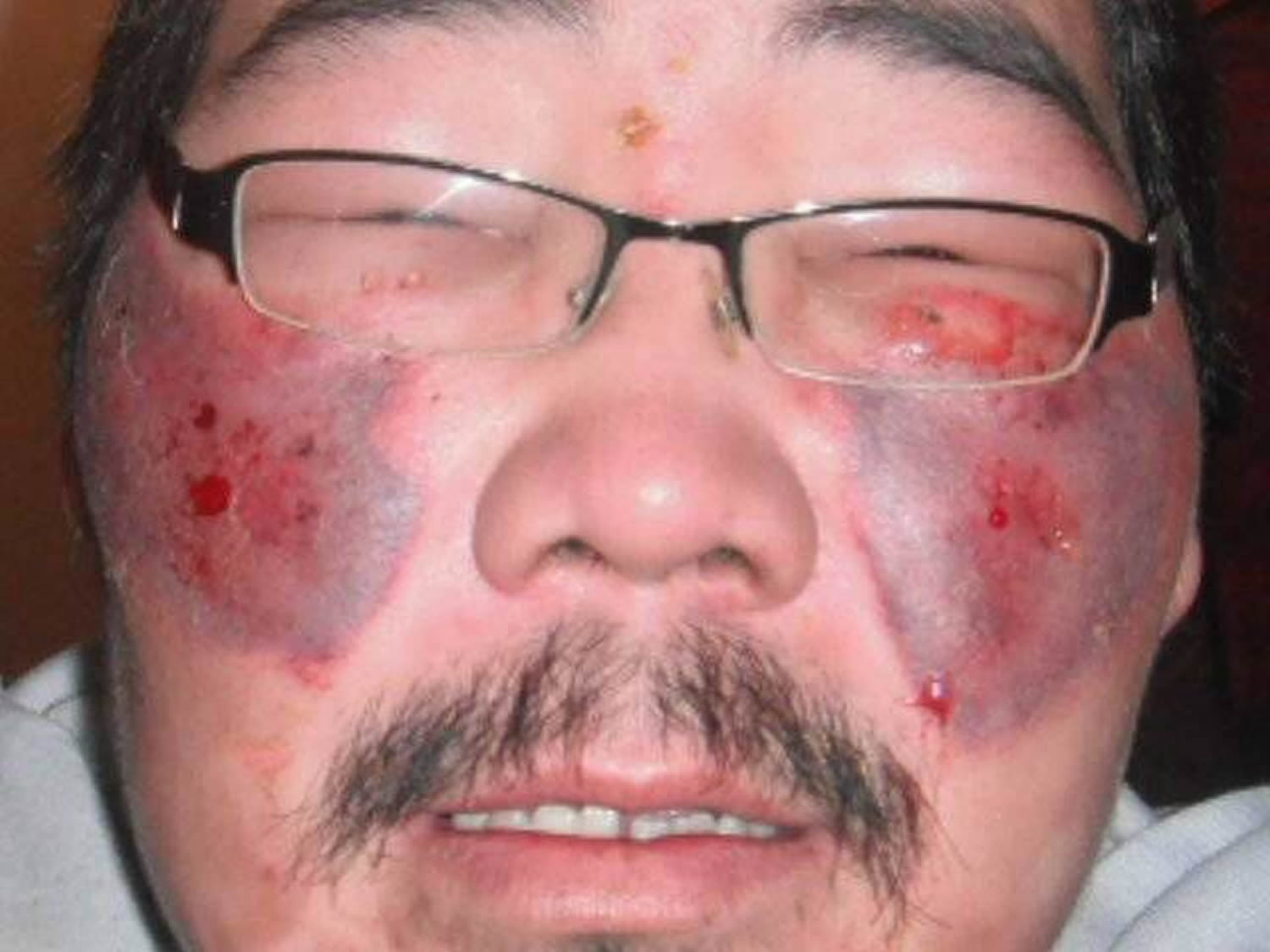
Figure 4. Frostbite foot

Frostbite complications
If some of your tissue dies, the dead tissue will no longer have a blood supply. This can make the affected body part very vulnerable to infection because your body relies on white blood cells to ward off infections.
People with frostbite are at risk of bacterial wound infections, such as tetanus. More seriously, this infection can spread into the blood (sepsis), which requires treatment with antibiotics. Both conditions require hospital admission.
Complications of frostbite include:
- Increased sensitivity to cold
- Increased risk of developing frostbite again
- Long-term numbness in the affected area
- Changes in the cartilage between the joints (frostbite arthritis)
- Growth defects in children, if frostbite damages a bone’s growth plate
- Infection
- Tetanus
- Gangrene — decay and death of tissue resulting from an interruption of blood flow to the affected area — which can result in amputation
Cold exposure that’s severe enough to cause frostbite also can cause hypothermia. When your body temperature drops, your heart, nervous system and other organs don’t work correctly. Left untreated, hypothermia eventually leads to complete failure of your heart and respiratory system and to death.
Hypothermia
Severe frostbite is often associated with hypothermia, which occurs when a person’s body temperature drops below 35 °C (95 °F).
Initial symptoms of hypothermia can include:
- constant shivering
- tiredness
- low energy
- cold or pale skin
- fast breathing (hyperventilation)
Someone with severe hypothermia may be unconscious and have shallow breathing and a weak pulse.
Frostbite causes
The body responds to cold temperatures by narrowing the blood vessels. Blood flow to the extremities slows down so flow to the vital organs can be increased.
As the blood is redirected away from the extremities, these parts of the body get colder, and fluid in the tissue can freeze into ice crystals.
The ice crystals can cause severe cell and tissue damage in the affected area. The low blood flow also deprives the tissues of oxygen. If blood flow can’t be restored, the tissue will eventually die.
Frostbite occurs when skin and underlying tissues freeze. The most common cause of frostbite is exposure to cold-weather conditions. But it can also be caused by direct contact with ice, freezing metals or very cold liquids.
Specific conditions that lead to frostbite include:
- Wearing clothing that isn’t suitable for the conditions you’re in — for example, it doesn’t protect against cold, windy or wet weather or it’s too tight.
- Staying out in the cold and wind too long. Risk increases as air temperature falls below 5 °F (minus 15 °C), even with low wind speeds. In wind chill of minus 16.6 °F (minus 27 °C), frostbite can occur on exposed skin in less than 30 minutes.
- Touching materials such as ice, cold packs or frozen metal.
At-risk groups
Certain groups of people are at greater risk of getting frostbite.
They include:
- people who take part in winter and high-altitude sports, such as mountaineers and skiers
- anyone stranded in extreme cold weather conditions
- anyone who works outdoors in harsh conditions for long periods of time, such as soldiers, sailors and rescue workers
- homeless people
- the very young and very old, as their bodies are less able to regulate body temperature
- people with conditions that cause blood vessel damage or circulation problems, such as diabetes and Raynaud’s phenomenon
- anyone taking medication that constricts the blood vessels, including beta-blockers – smoking can also constrict the blood vessels
Many cases of frostbite occur in people who have taken drugs or drunk alcohol. Taking drugs or being drunk can lead to risky behavior, not responding normally to cold, or falling asleep outside in cold weather.
Risk factors for frostbite
The following factors increase the risk of frostbite:
- Medical conditions that affect your ability to feel or respond to cold, such as dehydration, exhaustion, diabetes and poor blood flow in your limbs
- Alcohol or drug abuse
- Smoking
- Fear, panic or mental illness, if it inhibits good judgment or hampers your ability to respond to cold
- Previous frostbite or cold injury
- Being an infant or older adult, both of whom may have a harder time producing and retaining body heat
- Being at high altitude, which reduces the oxygen supply to your skin
What is the best prevention for frostbite
Preventing frostbite
Almost all frostbite cases can be prevented by taking precautions during cold weather.
Avoid unnecessary exposure to cold temperatures. The combination of wind and cold temperatures (wind chill) can also cause a rapid drop in temperature, so avoid going out when it’s cold and windy, if possible.
It’s also important to know what the early symptoms of frostbite are, particularly the tingling sensation of frostnip.
Wear appropriate clothing that protects your extremities, such as:
- Well-insulated boots and wear socks and sock liners that fit well, wick moisture and provide insulation. You might also try hand and foot warmers. Be sure the foot warmers don’t make your boots too tight, restricting blood flow.
- Wear mittens rather than gloves. Mittens provide better protection. Or try a thin pair of glove liners made of a wicking material (like polypropylene) under a pair of heavier gloves or mittens.
- Wear a hat or headband that fully covers your ears – it’s important to protect your head from the cold
- Dress in several layers of loose, warm clothing. Air trapped between the layers of clothing acts as insulation against the cold. Wear windproof and waterproof outer garments to protect against wind, snow and rain. Choose undergarments that wick moisture away from your skin. Change out of wet clothing — particularly gloves, hats and socks — as soon as possible.
You should also try to keep dry and remove any wet clothing as soon as you can.
Limit time you’re outdoors in cold, wet or windy weather. Pay attention to weather forecasts and wind chill readings. In very cold, windy weather, exposed skin can develop frostbite in a matter of minutes.
If you’re traveling during cold weather, plan for emergencies. For example, if you’re driving in icy conditions, make sure you keep a warm blanket and some spare clothes in the boot of your car in case you break down.
If you’re traveling by foot, always let others know where you’re going and what time you’ll be back. Take a fully charged mobile phone with you so you can call for help if you have an accident, such as a fall.
Be careful when drinking alcohol during very cold weather. Drinking too much increases your risk of falling asleep in the cold, a common cause of frostbite. Alcohol also causes you to lose heat at a faster rate.
Watch for signs of frostbite. Early signs of frostbite include red or pale skin, prickling, and numbness.
Plan to protect yourself. When traveling in cold weather, carry emergency supplies and warm clothing in case you become stranded. If you’ll be in remote territory, tell others your route and expected return date.
Eat well-balanced meals and stay hydrated. Doing this even before you go out in the cold will help you stay warm. And if you do become cold, drinking warm, sweet beverages, such as hot chocolate, will help you warm up.
Keep moving. Exercise can get the blood flowing and help you stay warm, but don’t do it to the point of exhaustion.
Smoking also makes you more vulnerable to the effects of the cold as nicotine can narrow your blood vessels.
Frostbite signs and symptoms
Signs and symptoms of frostbite include:
- At first, cold skin and a prickling feeling
- Numbness
- Red, white, bluish-white or grayish-yellow skin
- Hard or waxy-looking skin
- Clumsiness due to joint and muscle stiffness
- Blistering after rewarming, in severe cases
Frostbite is most common on the fingers, toes, nose, ears, cheeks and chin. Because of skin numbness, you may not realize you have frostbite until someone else points it out.
Frostbite occurs in several stages:
- Frostnip. The first stage of frostbite is frostnip. With this mild form of frostbite, your skin pales or turns red and feels very cold. Continued exposure leads to prickling and numbness in the affected area. As your skin warms, you may feel pain and tingling. Frostnip doesn’t permanently damage the skin.
- Superficial frostbite. The second stage of frostbite appears as reddened skin that turns white or pale. The skin may remain soft, but some ice crystals may form in the tissue. Your skin may begin to feel warm — a sign of serious skin involvement. If you treat frostbite with rewarming at this stage, the surface of your skin may appear mottled, blue or purple. And you may notice stinging, burning and swelling. A fluid-filled blister may appear 24 to 36 hours after rewarming the skin.
- Severe (deep) frostbite. As frostbite progresses, it affects all layers of the skin, including the tissues that lie below. You may experience numbness, losing all sensation of cold, pain or discomfort in the affected area. Joints or muscles may no longer work. Large blisters form 24 to 48 hours after rewarming. Afterward, the area turns black and hard as the tissue dies.
Frostbite diagnosis
The diagnosis of frostbite is usually made based on your signs and symptoms, the appearance of your skin, and a review of recent activities in which you were exposed to cold.
Your doctor may conduct tests, such as an X-ray, bone scan or magnetic resonance imaging (MRI) test, to determine the severity of the frostbite and to check if bone or muscle is damaged. Your doctor may also run tests if he or she suspects you have hypothermia, a condition that often occurs with frostbite.
Frostbite treatment
Treatment for frostbite depends on the severity of your symptoms. Always seek medical attention if you think you or someone else has frostbite.
First aid for frostbite
If medical assistance isn’t available, the following steps can be taken to treat frostbite and hypothermia:
- Protect your skin from further exposure. If you’re outside, warm frostbitten hands by tucking them into your armpits. Protect your face, nose and ears by covering them with dry, gloved hands. Don’t rub the affected area and never rub snow on frostbitten skin.
- Move to a warmer place (if possible) – it’s best to avoid walking on frostbitten feet and toes as it can cause further damage, but in emergency situations this may not always be possible.
- Replace wet clothing with soft, dry clothing to stop further heat loss.
- Check for hypothermia. Get emergency medical help if you suspect hypothermia.
- Warm the body by wrapping it in blankets and protecting the frostbitten parts.
- Don’t rub the affected area or apply direct heat (such as from a fire or heater) as this can cause further injury.
- Don’t smoke if you have frostbite (or allow someone else with frostbite to smoke) because smoking can affect blood circulation.
- Gently rewarm frostbitten areas. Soak hands or feet in warm water — 99 to 108 °F (37 to 42 °C) — for 15 to 30 minutes. A bath of water at a temperature of 40-41 °C (104-105.8 °F) is recommended for rewarming. If a thermometer isn’t available, test the water by placing an uninjured hand or elbow in it — it should feel very warm, not hot. Don’t rewarm frostbitten skin with direct heat, such as a stove, heat lamp, fireplace or heating pad. These can cause burns. Rewarming can be a painful process requiring painkillers and expert medical assessment.
- If there’s any chance the affected areas will freeze again, don’t thaw them. If they’re already thawed, wrap them up so that they don’t refreeze – it can cause further irreversible damage.
- It’s important not to rewarm the affected area if there’s a chance of it freezing again as this can lead to further tissue damage.
- Take pain medicine. If you are in pain, take over-the-counter ibuprofen (Advil, Motrin IB, others) to reduce pain and inflammation.
- Don’t walk on frostbitten feet or toes if possible. This further damages the tissue.
- Know what to expect as skin thaws. If the skin turns red and you feel tingling and burning as it warms, normal blood flow is returning. But seek emergency medical attention if the numbness or pain remains during warming or if blisters develop.
- In severe cases of frostbite, the loss of blood supply to the tissue may cause it to die (gangrene). A type of surgery called debridement may be needed to remove the dead tissue. Amputation may be needed in very severe cases.
Rewarming the frostbitten areas
The frostbitten areas need to be rewarmed. Rewarming shouldn’t be attempted until you’re out of the cold.
If the warming process is started and the frozen parts are then re-exposed to the cold, it can cause further irreversible damage.
Rewarming should ideally be carried out under medical supervision – it can be a painful process requiring painkillers and expert medical assessment. Depending on the severity of pain, very strong painkillers, such as morphine, may be needed. Ibuprofen should also be taken as it has additional protective properties for frostbite. The best results are achieved using a whirlpool bath that contains a mild antiseptic.
- The affected area should be rewarmed slowly by immersing it in warm, but not hot, water. A bath of water at a temperature of 40-41 °C (104-105.8 °F) is recommended.
- Rewarming should last at least 30 minutes and only be stopped once the affected body part is a red-purple color and can be easily moved.
- If there is potential for refreezing of an area, do not attempt to thaw, as thawing followed by refreezing can cause even more extensive damage to the area.
This process can be repeated twice a day until there are clear signs that the affected body part is beginning to heal, such as the growth of new skin and the return of normal skin color.
- Do NOT use direct heat (hair dryers, heating pads, etc) to rewarm the affected area.
After rewarming
After the frostbitten area has been thawed, it should be gently wrapped in clean bandages, with the fingers and toes separated. It’s very important to keep the skin clean to avoid infection.
- Frostbitten areas, once thawed, should be moved as little as possible.
- Do not massage the affected area to attempt to rewarm it.
Too much movement should be avoided, and the limbs should be raised if possible. Avoid walking on affected feet and toes that have been rewarmed as the tissues will be very delicate.
After rewarming, the skin will be discolored and blistered, and will eventually scab over. If the frostbite is superficial, new pink skin will form beneath the discolored skin and scabs. The area usually recovers within six months.
- Avoid disturbing any blisters or skin that has become gangrenous.
Severe frostbite
If you have severe frostbite, you’ll need to be admitted to a specialist unit where medical staff are experienced in treating these types of injuries.
This is often a specialist burns unit because exposure to very high temperatures can cause the same type of injury as exposure to very cold temperatures.
Medical treatment
- Rewarming of the skin. If it hasn’t been done already, your doctor will rewarm the area using a warm-water bath for 15 to 30 minutes. The skin may turn soft and look red or purple. You may be encouraged to gently move the affected area as it rewarms.
- Oral pain medicine. Because the rewarming process can be painful, your doctor will likely give you a drug to ease the pain.
- Protecting the injury. Once your skin thaws, your doctor may loosely wrap the area with sterile sheets, towels or dressings to protect the skin. You may need a brace or splint if the bone or muscle is involved. And you may need to elevate the affected area to reduce swelling.
- Removal of damaged tissue (debridement). To heal properly, frostbitten skin needs to be free of damaged, dead or infected tissue. To better distinguish between healthy and dead tissue, your doctor may wait one to three months before removing damaged tissue.
- Whirlpool therapy. Soaking in a whirlpool bath (hydrotherapy) can aid healing by keeping skin clean and naturally removing dead tissue. You’ll be encouraged to gently move the affected area while it is under water.
- Infection-fighting drugs. If your skin or blisters appear infected, your doctor may prescribe oral antibiotics.
- Clot-busting drugs. You may receive an intravenous injection (IV) of a drug that helps restore blood flow (thrombolytic), such as tissue plasminogen activator (TPA). Studies of people with severe frostbite show that TPA lowers the risk of amputation. But these drugs can cause serious bleeding and are typically used only in the most serious situations and within 24 hours of exposure.
- Wound therapy. If you have a complex wound, your doctor might suggest a technique called vacuum-assisted closure therapy to promote healing.
- Surgery. In severe cases, surgery or amputation may be necessary to remove the dead or decaying tissue.
- Hyperbaric oxygen therapy. Hyperbaric oxygen therapy involves breathing pure oxygen in a pressurized room. Some patients showed improved symptoms after this therapy. But more study is needed.
If there’s a very high risk of major damage, you may have thrombolytic therapy (tPA). Medication to help break up small clots in the frostbitten blood vessels will be given as injections or through a drip in your arm.
This should improve blood flow to the affected body part, which can stimulate healing and prevent further damage. You may also be given antibiotics to prevent the affected body part becoming infected.
Iloprost is sometimes used to treat very severe cases of frostbite. It works by widening the blood vessels that supply blood to the affected body part.
When severe frostbite threatens the loss of a limb, finger or toe, a person should be considered for treatment with tPA or iloprost within 24 hours of the injury occurring.
Experience has shown that treatment given within this timeframe has the best outcomes in terms of saving the affected body part.
But giving these treatments after 24 hours could still be considered to be an option at an experienced unit.
If some of the tissue of the affected body part has died (a condition known as gangrene), it’ll need to be removed. The procedure to remove dead tissue is called debridement.
In the most serious cases, an entire part of the body, such as the fingers or toes, may need to be removed (amputated).
A decision to perform debridement or amputation is usually delayed for several weeks, as often what appears to be dead tissue can heal and recover over time.
Lifestyle and home remedies
To care for your skin after frostbite:
- Take all medications — antibiotics or pain medicine — as prescribed by your doctor. For milder cases of frostbite, take over-the-counter ibuprofen (Advil, Motrin IB, others) to reduce pain and inflammation.
- For superficial frostbite that has been rewarmed, apply aloe vera gel or lotion to the affected area several times a day to reduce inflammation.
- Avoid further exposure to cold and wind.
- Don’t walk on frostbitten feet.
- Don’t apply direct heat or rub the area.
- Don’t break blisters that may develop. Blisters act like a bandage. Allow blisters to break on their own.





{kind=link}