Contents
What is fundoplication surgery
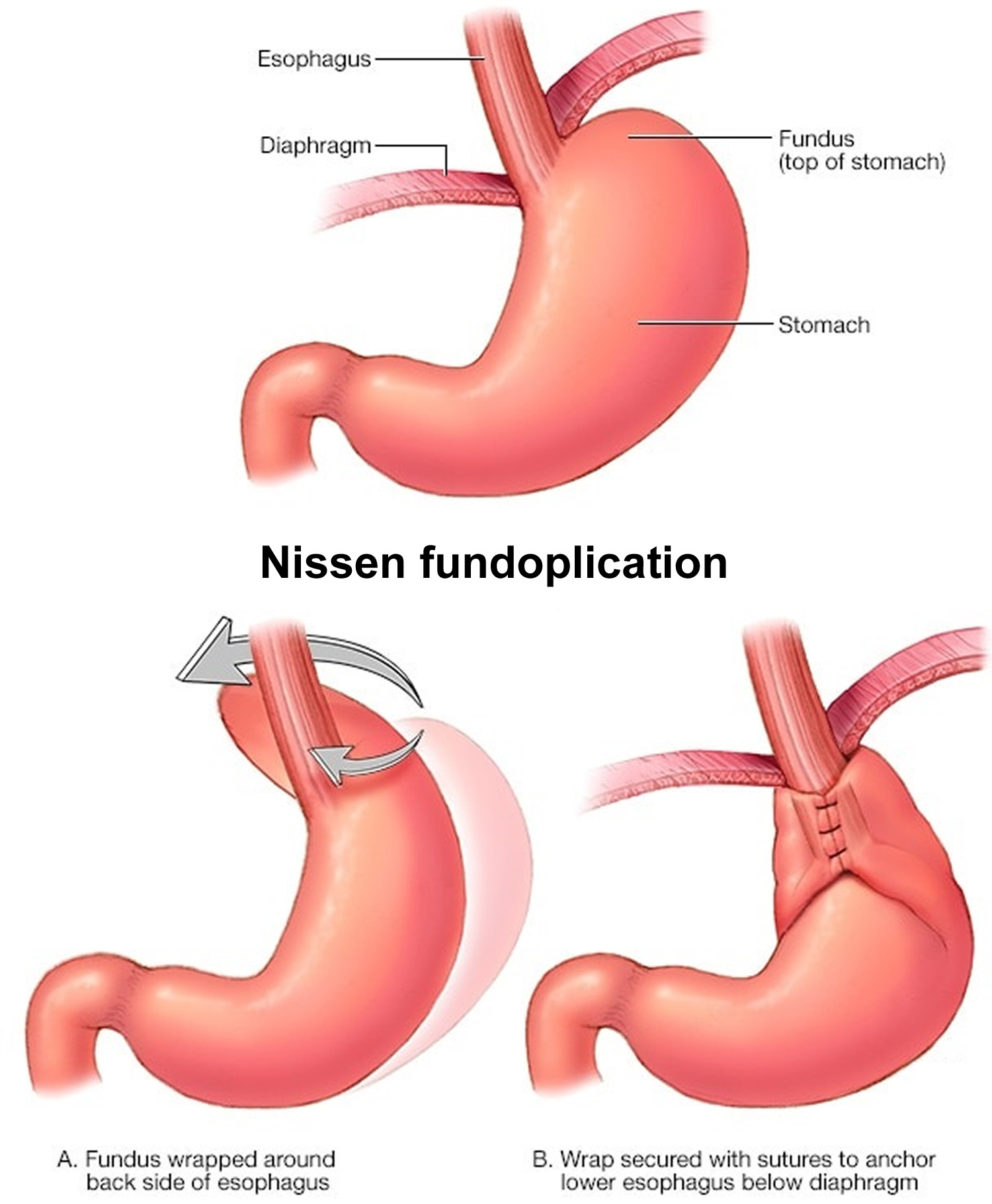
In a fundoplication is a surgery used to control problematic gastro-esophageal reflux or vomiting where the gastric fundus (upper part) of the stomach is wrapped around the lower end of the esophagus and stitched in place to reinforce the lower esophageal sphincter. The reinforced and tightened lower esophageal sphincter now provides a better “seal” and relieves the symptoms associated with GERD (gastroesophageal reflux disease) and achalasia. Fundoplication surgical procedure addresses the acid reflux–backflow of strong and irritating stomach acid into the lower esophagus–caused by gastroesophageal reflux disease (GERD). Constant exposure to the strong acids can damages the cells of your lower esophagus, where it joins the upper part of the stomach. In some cases, patients suffering from achalasia (a swallowing disorder) may need to undergo a fundoplication to reinforce the lower esophageal sphincter’s ability to close.
Fundoplication comes in a variety of forms such as Nissen, Dor, Toupet and Belsey. These surgical approaches differ in how much–and where–the lower esophagus is wrapped by the stomach. For example, in a Dor fundoplication, the top of the stomach is partially wrapped around the front of the esophagus’ lower end; while in a Toupet fundoplication, the top of the stomach is partially wrapped around the back of the lower esophagus. In Nissen fundoplication, the surgeon wraps the top of the stomach around the lower esophagus. This reinforces the lower esophageal sphincter, making it less likely that acid will back up in the esophagus (see Figure 4). Over the last decade and a half, the number of patients referred for antireflux surgery has increased eight fold. Approximately 70,000 operations are performed annually in the United States.
Gastro‐esophageal reflux disease (GERD) is a condition which develops when stomach contents regurgitate into the esophagus causing troublesome symptoms such as heartburn (burning sensation at the lower end of the breastbone) or regurgitation (perception of flow of stomach content into the throat or mouth) 1. Long‐term complications of GERD include reflux oesophagitis (injury to lining of esophagus), bleeding from the esophagus, narrowing of the esophagus, change in the nature of the lining of the esophagus which can sometimes give rise to esophageal cancer 2. Other researchers have hypothesized that there is a direct link between symptomatic GERD and esophageal cancer based on their observation of increased esophageal cancer irrespective of the presence of Barrett’s esophagus 3. While there has been significant controversy over the definition of GERD, the international consensus definition of GERD includes asymptomatic patients with complications, does not stipulate the method of diagnosis, and includes reflux which may be weakly acidic or gaseous 1.
There is global variation in the prevalence of GERD. The prevalence is higher in Europe, North and South America, and the Middle East, with a prevalence ranging between 9% and 33% of adults compared to a prevalence ranging between 3% and 8% in East Asia 4. The incidence of GERD is available from the UK and the USA and is about five cases of GERD per 1000 person-years 4. The risk factors for GERD include genetic factors such as a family history of reflux disease in immediate relatives; demographic factors such as pregnancy, older age and obesity; behavioral factors such as cigarette smoking, excessive alcohol consumption, drug treatments such as non-steroidal anti-inflammatory drugs (NSAIDs), oral steroids; and co-morbidities such as abdominal pain, irritable bowel syndrome, gallstone disease, asthma, chronic obstructive pulmonary disease, chest pain, and angina. Coffee consumption, oral contraceptive consumption, and hormonal replacement therapy are associated with lower prevalence of GERD 5. It should be noted that these are associations and no causal association can be shown for many of these factors. Apart from lifestyle changes (such as cessation of smoking) and diet changes (avoiding food that causes heartburn), the major forms of treatment for GERD are medical and surgical. The medical treatment is usually aimed at decreasing acidity in the stomach. Currently a group of drugs which suppress acid secretion, called proton pump inhibitors, are considered the best in decreasing acid secretion.
Gastric contents are prevented from entering into the esophagus by the lower esophageal sphincter (LES). However, lower esophageal sphincter (LES) relaxes transiently resulting in the reflux of gastric contents into the esophagus, even in normal individuals 6. However, increased reflux of gastric contents into the esophagus and prolonged exposure of the lower esophagus to gastric contents are believed to contribute to the symptoms and complications of GERD 6. Hiatus hernia lowers the competence and pressure of the lower esophageal sphincter, reduces the length of the gastro-esophageal junction, and alters the opening characteristics of the gastro-oesophageal junction. This results in an increase in the exposure of the esophagus to acid 6. Hiatus hernia is associated with severe GERD symptoms and complications 6.
The main surgical treatment is fundoplication which involves wrapping around the lower part of the food pipe with stomach. This can be performed by traditional open surgery, keyhole surgery or surgery that is performed without making any cut from within the stomach with the help of an endoscope (in this context, a flexible tube introduced through the mouth to give a view of the food pipe and stomach). There are various modifications to original complete fundoplication suggested by Nissen, mainly with regards to the amount and area of the gastric fundus which is plicated and where the wrap is fixed 7. Fundoplication can be performed by open or laparoscopic surgery 7. Currently laparoscopic Nissen fundoplication is the most common surgical procedure for the management of GERD offering promising long-term outcomes 8 and has been recommended as a choice of surgical therapy by the European Study Group for Antireflux Surgery and the Society of American Gastrointestinal Endoscopic Surgeons 9. Nevertheless, laparoscopic Nissen fundoplication can induce functional disorders, such as dysphagia, gas-bloating and an inability to belch. Compared to laparoscopic Nissen fundoplication, several surgeons have stated that laparoscopic Toupet fundoplication has a lower prevalence of postoperative complications while obtaining a similar control of reflux 10, but, several studies have failed to show a significant difference between them 11. Also, whether preoperative esophageal motility should be considered when surgeons select a procedure has not been elucidated. Hence, the controversy regarding the optimal surgical method continues.
This report 12 demonstrated that the operating time of laparoscopic Toupet fundoplication was longer than that of laparoscopic Nissen fundoplication, which might be due to the fact that the gastric fundus and both sides of the esophagus should be secured, respectively. Prevalence of perioperative complications between the two groups was not significantly different. But it is notable that Strate et al. 13 and Booth et al. 14 reported a perforation in the fundal wrap and an episode of perioperative bleeding after laparoscopic Toupet fundoplication. And Guérin et al. 15 also observed in-hospital bleeding. This phenomenon may be because the esophagus does not have a serosal layer and gastric fundus and both sides of the esophagus wall need to be sutured together, which may increase the risk of perforation and bleeding.
Recently endoscopic endoluminal fundoplication, which involves fundoplication without any incision, has been proposed 16.
The short‐term gastro‐esophageal reflux disease (GERD)‐specific quality of life was better in the laparoscopic fundoplication group than in the medical treatment group 17. Research has shown that fundoplication surgery is more effective than medication, at least within the first year after surgery, fundoplication is better at relieving symptoms like heartburn and acid reflux, and can improve quality of life 18. However, it was not clear how much this improvement benefited the patient. Furthermore there is not enough good research to say whether these advantages of fundoplication surgery are sustained in the long term.
The proportion of people with serious adverse events, short‐term dysphagia, and medium‐term dysphagia was higher in the laparoscopic fundoplication group than in the medical treatment group. The proportion of people with heartburn at short term, medium term, and long term, and those with acid regurgitation at short term and medium term was less in the laparoscopic fundoplication group than in the medical treatment group 17. The severity of difficulty in swallowing, heartburn, or acid regurgitation was not reported. There is considerable uncertainty in the balance of benefits versus harms of laparoscopic fundoplication compared to long‐term medical treatment with proton pump inhibitors. Due to the poor quality of the trials, future high‐quality studies are needed in this field 17.
Fundoplication key points
- Fundoplication surgery works as well as only taking medicine to keep you from getting acid reflux and heartburn. However, you may still need medicine after fundoplication surgery to control your symptoms.
- People who have had fundoplication surgery usually take less medication than before, but they cannot always stop taking it altogether. One study showed the following 18:
- Without fundoplication surgery: 87 out of 100 people who didn’t have surgery were still taking medication after one year.
- With fundoplication surgery: 36 out of 100 people who had surgery were still taking proton pump inhibitors after one year.
- There are different ways to do fundoplication surgery (for example, with a laporascope or through a large cut in your belly), but they all work about the same.
Figure 1. Stomach
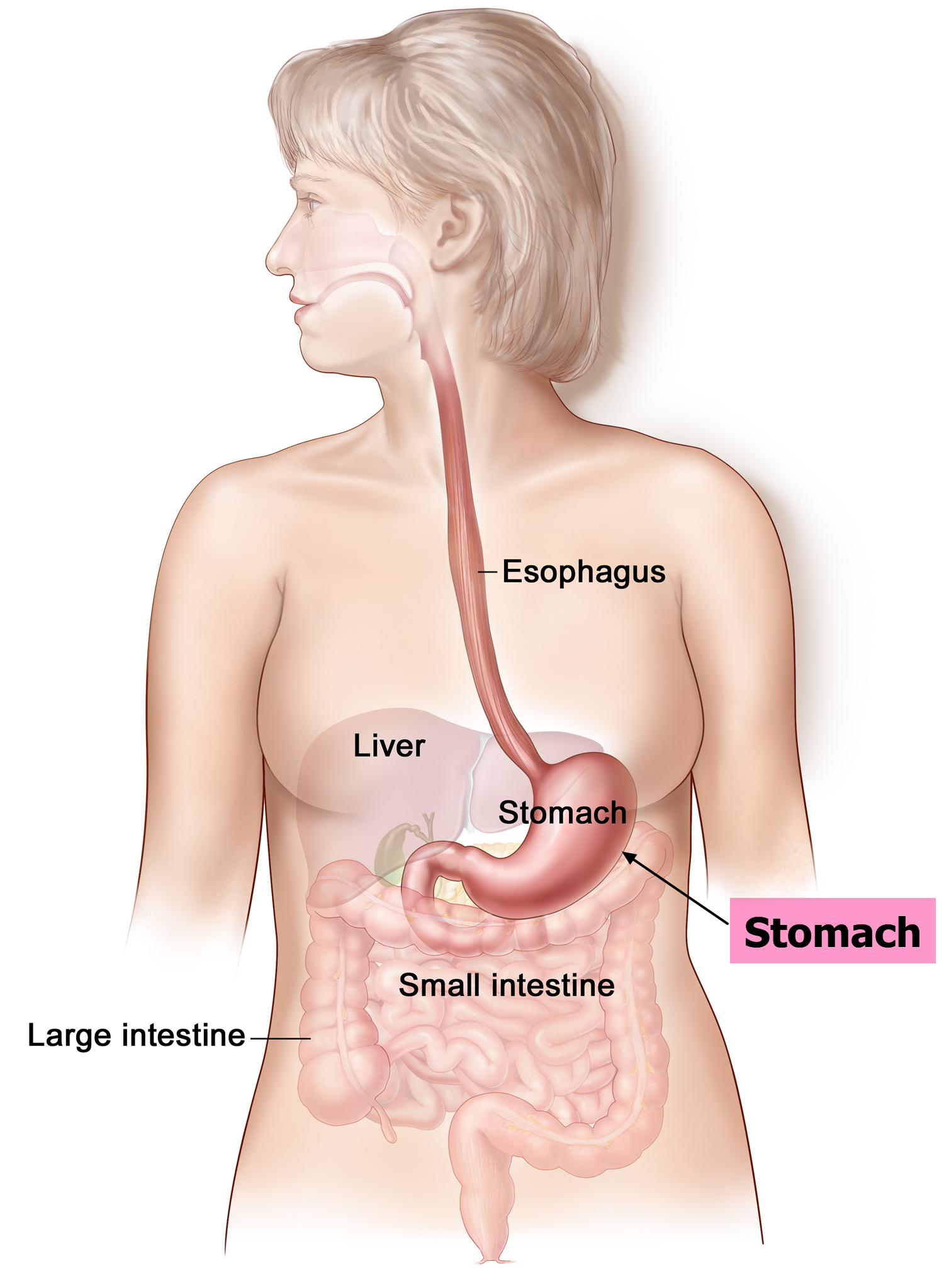
Figure 2. Parts of the stomach
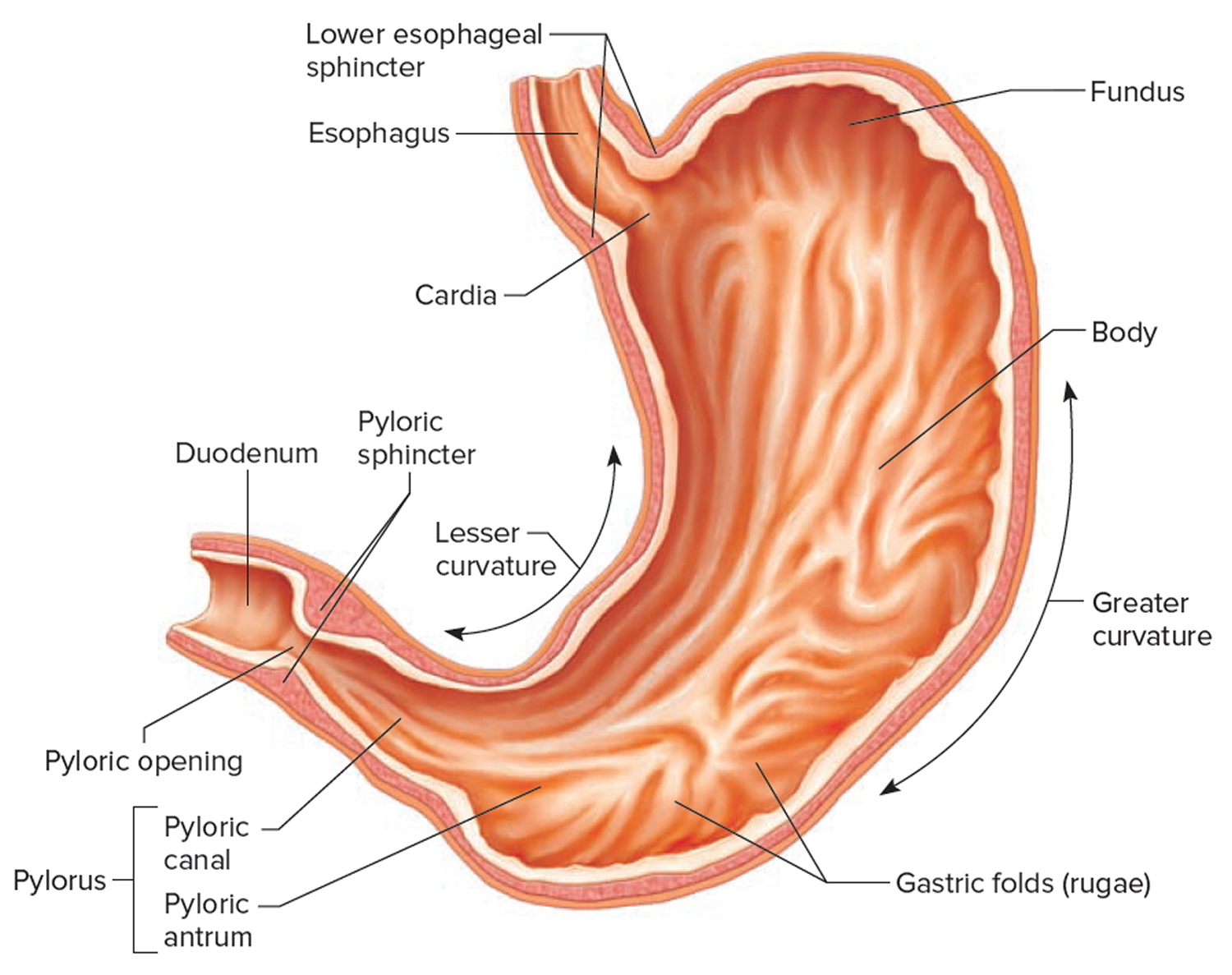
Figure 3. Gastroesophageal junction
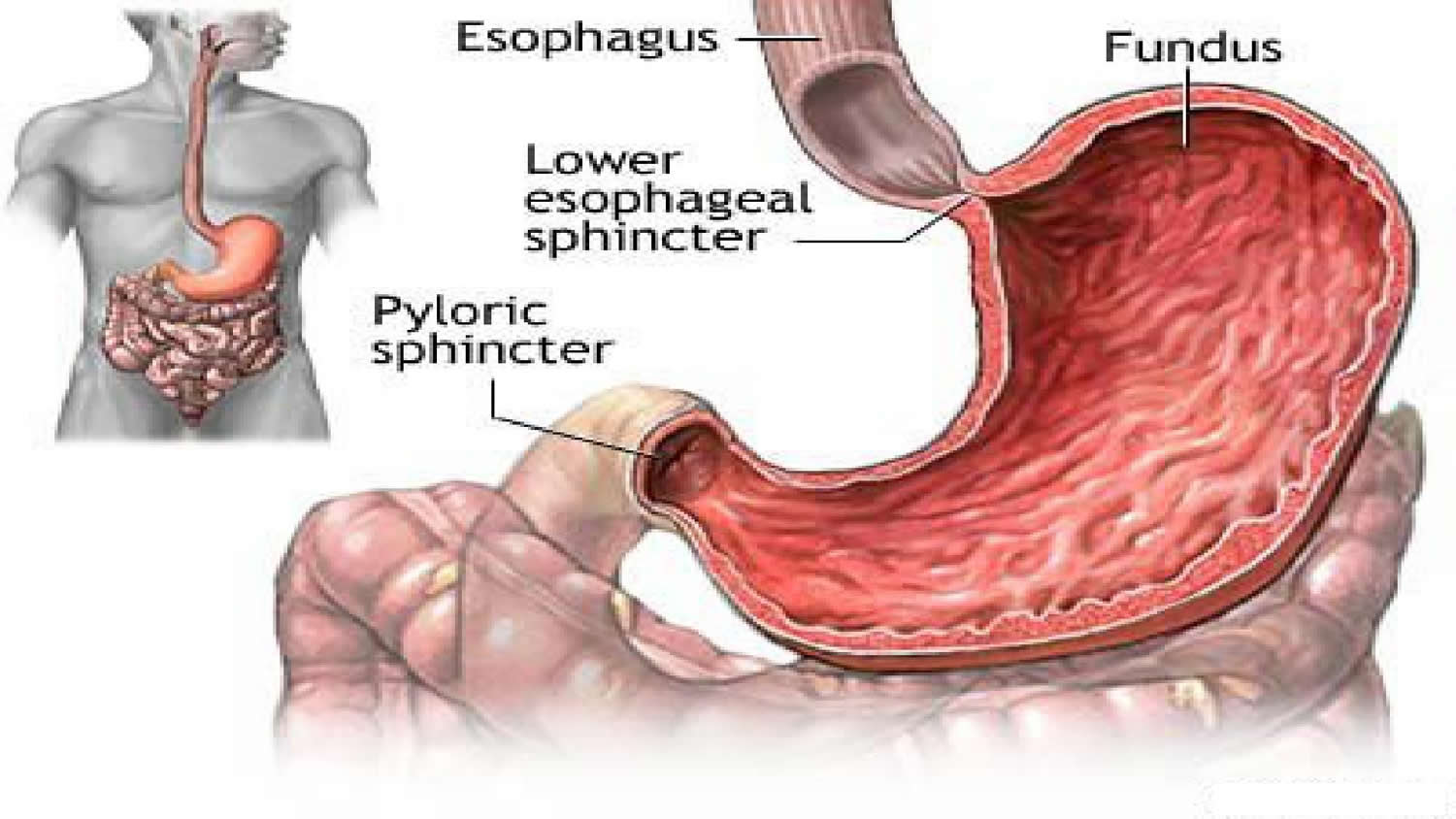
Figure 4. Gastroesophageal reflux disease (GERD)
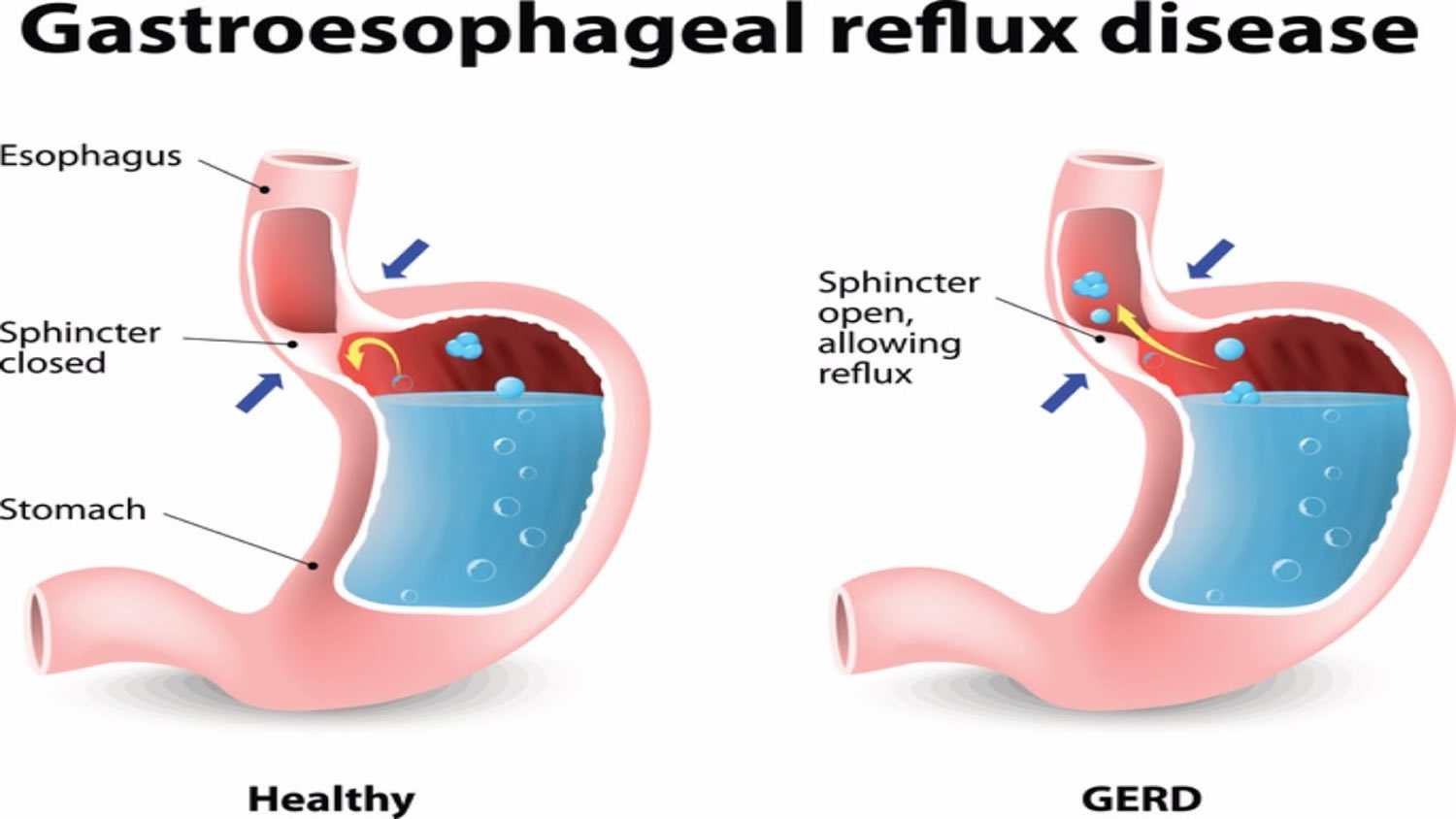
Figure 5. Fundoplication
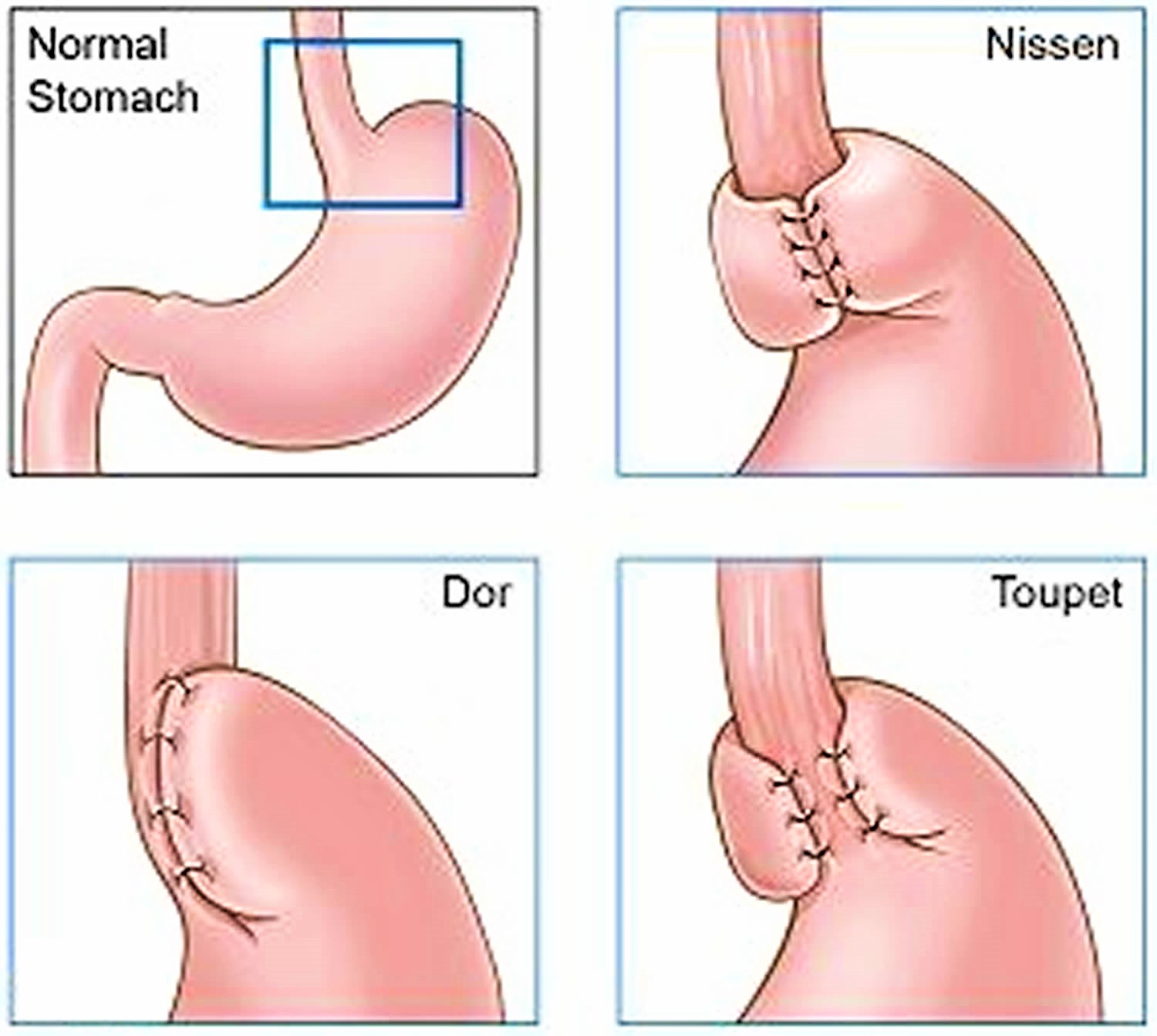
Figure 6. Nissen fundoplication
Fundoplication surgery
The lower esophageal sphincter (LES) plays an important role in the pathogenesis of gastroesophageal reflux disease (GERD) 19. In order to inhibit lower esophageal sphincter relaxation, fundoplication is considered to be an essential and important part of antireflux surgery. Fundoplication can be done in two ways, depending on whether a section of the stomach is wrapped all the way around the food pipe, or only part of the way around it. A complete fundoplication, where the stomach is wrapped all the way around the food pipe, is called Nissen fundoplication. In what is known as Toupet fundoplication, the stomach is only partially wrapped around the food pipe. This surgical technique is the method of choice if, for example, there is a problem with the movements of the food pipe (called a motility disorder).
Laparoscopic Nissen fundoplication, a total wrap that surrounds the esophagus 360°, is the most commonly used, gold standard technique worldwide for antireflux surgery 20. However, laparoscopic Nissen fundoplication is associated with a high incidence of postoperative dysphagia and gas-bloat syndrome 21. Laparoscopic Toupet fundoplication, a 270° partial wrap, was introduced to counteract these side effects.
Many surgeons advocate that the incidence of regurgitation and heartburn are similar in both laparoscopic Nissen fundoplication and laparoscopic Toupet fundoplication, while postoperative dysphagia may have a higher incidence following laparoscopic Nissen fundoplication 22. Besides fundoplication type, other variables such as the length of the wrap and impaired esophageal peristalsis may also be associated with postoperative dysphagia 23. The original laparoscopic Nissen fundoplication procedure, which purports a 6-cm wrap length, is associated with a higher dysphagia rate 24. Two studies on the length of the Nissen fundoplication showed that a loose wrap of 1–2 cm was sufficient to suppress reflux and reduce the incidence of postoperative bloating and dysphagia 25, 26. An early study showed that laparoscopic Toupet fundoplication was more effective when esophageal motility was abnormal (less than 50% peristaltic waveforms) 27. However, a previous study reported a similar incidence of dysphagia between laparoscopic Toupet fundoplication and laparoscopic Nissen fundoplication 1 year postoperatively 28. Whether laparoscopic Toupet fundoplication has a benefit on abnormal esophageal peristalsis remains controversial.
Several meta-analyses have been performed comparing outcomes between laparoscopic Nissen fundoplication and laparoscopic Toupet fundoplication until 2011 29, 30. However, a comprehensive study collecting randomized clinical trials has not been conducted to date. In recent years, several studies with large sample sizes and recent follow-up data have been published comparing long-term efficacy and adverse events of both total and partial fundoplication 31, 32. The results of this 2010 meta-analysis 33 suggested that laparoscopic Toupet fundoplication might be the current procedure of choice to treat GERD.
DOR fundoplication
Achalasia is a rare neurodegenerative disease of the esophagus and the lower esophageal sphincter that has generally been accepted as an autoimmune esophageal motility disorder resulting from the loss of inhibitory nerve endings in the myenteric plexus of the esophagus 34. Pathophysiologically esophageal achalasia is characterized by poor relaxation of lower esophageal sphincter (LES) and aperistalsis of the esophageal body, achalasia presents mainly relevant symptoms are dysphagia, regurgitation, heartburn, and chest pain 35. The commonly used treatment of achalasia involves medicine therapy, endoscopic pneumatic dilation, and surgical myotomy with the aim of eliminating the high lower esophageal sphincter (LES) pressure.
Current treatment of achalasia is directed at palliation of symptoms. Therapies include pharmacological therapy, endoscopic injection of botulinum toxin, endoscopic dilation, and surgery. Until the late 1980s, endoscopic dilation was the first line of therapy. The advent of safe and effective minimally invasive surgical techniques in the early 1990s paved the way for the introduction of laparoscopic myotomy.
Laparoscopic Heller myotomy has gained world-wide popularity and is increasingly regarded as the standard treatment for achalasia by surgeons and gastroenterologists. However, laparoscopic Heller myotomy alone has been shown to increase gastroesophageal reflux disease (GERD) 36; hence, it is now common practice to include an antireflux procedure. A 360° (Nissen) fundoplication has been used. However, this patient population experienced a high rate of dysphagia. These patients have some degree of esophageal body dysmotility, and a 360° wrap can make esophageal emptying more difficult 37. Thus, although Nissen fundoplication is effective at controlling postoperative acid reflux, it is less favorable because of a high dysphagia recurrence rate 36.
A partial fundoplication has the benefits of less dissection, decreased operative time, and improvement in dysphagia symptoms, while showing improvement in reflux rates comparable with 360° fundoplication 38. Both Dor and Toupet fundoplications provide antireflux benefits with less risk for recurrent dysphagia in postmyotomy patients 39. Dor fundoplication which is a 180° anterior fundoplication, with the advantage of a simple procedure and covering of the mucosa, is being accepted as the first-line type of fundoplication for achalasia in most regions. Dor partial anterior fundoplication allows preservation of the posterior gastroesophageal junction as well as the potential advantage of protection of the exposed mucosa at the myotomy site. However, laparoscopic Heller myotomy alone or laparoscopic Heller myotomy plus other types of fundoplication (e.g., posterior 270° Toupet and total 360° Nissen fundoplication) have also been reported to have different benefits compared with laparoscopic Heller myotomy plus Dor fundoplication. Thus, there is no consensus on whether Dor fundoplication is the optimum procedure after laparoscopic Heller myotomy for the prevention of gastroesophageal reflux 35.
Toupet fundoplication
Toupet fundoplication is first described in 1963. Toupet fundoplication is described as a 270-degree posterior fundoplication, with crural closure and fixation of the wrap to the closure 40. The efficacy of Toupet fundoplication has been demonstrated and a partial wrap is believed to produce less postoperative side effects than the complete wrap. However, some studies have indicated that recurrence rate of reflux symptoms may be higher after Toupet fundoplication 41. Laparoscopic Toupet fundoplication is performed with five ports under general anesthesia. After dissecting the gastro-hepatic ligament with a harmonic scalpel, a window was created behind the lower esophagus. Then, the diaphragmatic crura were carefully dissected, and approximately 5 cm of the distal esophagus was mobilized, while the mediastinal structures, including the pleura, pericardium, vagus nerves, and aorta, were identified and preserved. In all cases, the gastric fundus was dissected by dividing the short gastric vessels. The diaphragmatic crura were sewed behind the esophagus with 1-2 non-absorbable sutures, and a posterior 270° and 2-cm-long fundoplication was constructed with 5-6 interrupted non-absorbable sutures.
Nissen fundoplication surgery
Laparoscopic Nissen Fundoplication is a minimally invasive surgery that has been very successful and replaces classical open operations for the treatment of GERD (gastroesophageal reflux disease). The Nissen fundoplication is performed under general anesthesia with 5 small (puncture hole) incisions placed on the abdomen. The stomach is wrapped around the lower esophagus, which then prevents the reflux of stomach contents into the esophagus and respiratory tract.
Patients typically spend one night in the hospital and go home the next day. After surgery, patients will no longer need “heartburn” medications, with a greater than 90% success rate in relieving symptoms of GERD (gastroesophageal reflux disease).
Nissen fundoplication complications
Every surgical procedure carries certain risks. The complications related to fundoplication include injury to nearby structures such as the liver, spleen, or esophagus; dysphagia (troublesome difficulty in swallowing) (5%); wrap migration (1%); recurrent regurgitation (1%); recurrent heartburn (1% to 10%); and chest complications (3%) 17. Overall, 1% to 14% of patients undergoing fundoplication develop complications 17.
Quite a lot of people have symptoms such as flatulence (“passing wind” or “farting”) and regurgitation after having anti-reflux surgery. But these symptoms could also be caused by the disease itself, and not by the surgery. Surgery causes swallowing problems in some people, or makes existing swallowing problems worse. Up to 23 out of 100 people in the studies had symptoms like these after fundoplication surgery.
Possible serious complications of surgery include severe bleeding, organ injury and infections. Up to 2 out of 100 people have severe bleeding, and the digestive tract is injured in about 1 out of 100 people.
Fundoplication side effects
- Fundoplication surgery can cause you to feel bloated and make it hard to swallow. These side effects may last for 30 days or longer, and some side effects may require a second surgery to fix.
- Serious side effects, such as infection and heart attack, may be more common with surgery than with medicine. These side effects are rare.
Nissen fundoplication recovery
You will need to be in hospital for about 5 days for the operation. You may need to be nursed in the intensive care unit after the operation for 1-2 days.
The major risks of the operation are bleeding, infection, leakage from oesophagus or stomach and chest infection.
Nissen fundoplication diet
There is not a lot of good research about post Nissen fundoplication diet and whether making changes in daily life helps relieve heartburn and acid reflux. But it can be worth changing certain habits. For instance, the symptoms might get better if you stop smoking or drink less alcohol.
If certain foods appear to make your gastroesophageal reflux symptoms worse, avoiding those foods could help. The problems are often caused by specific things, such as coffee, chocolate, very fatty or spicy foods, citrus fruits or fizzy drinks. It might take time and patience to find out which types of food you don’t tolerate well. Sometimes people also find that food hardly has any effect on their symptoms.
People who are overweight are often advised to lose weight because the extra pounds can put a strain on the digestive system and push against the food pipe and stomach. This could affect the function of the sphincter muscle at the lower end of the food pipe. Meals that have a lot of fat or calories in them, or large meals, can cause gastroesophageal reflux disease (GERD) symptoms too. But thin people who have low-fat diets can also have gastroesophageal reflux and heartburn. So there is no guarantee that your symptoms will get better if you lose weight or change your diet.
Many people wake up several times a night because of pain and burning in their food pipe. Some then decide to stop eating late in the evening, or only lie down at least three hours after a meal. Others sleep with their upper body raised. Lying on your left side can also help because then the entrance to your stomach is higher than your stomach itself.
If your symptoms do not improve despite making changes to your lifestyle, medication is a further treatment option. Various medications are available, some of which can relieve the symptoms very effectively – but the effect only lasts for as long as you take it.
Which medications can help?
Proton pump inhibitors (PPIs)
Proton pump inhibitors (PPIs) reduce the production of acidic stomach juices by inhibiting a certain enzyme. They can relieve typical symptoms like heartburn.
There are many names and brands of PPIs. Most work equally as well. Side effects may vary from drug to drug.
- Omeprazole (Prilosec), also available over-the-counter (without a prescription)
- Esomeprazole (Nexium), also available over-the-counter (without a prescription)
- Lansoprazole (Prevacid)
- Rabeprazole (AcipHex)
- Pantoprazole (Protonix)
- Dexlansoprazole (Dexilant)
- Zegerid (omeprazole with sodium bicarbonate), also available over-the-counter (without a prescription)
Studies have tested just how effective these medications are. It was found that:
- 25 out of 100 people who took a dummy drug (placebo) hardly had heartburn any more after two to eight weeks.
- 70 out of 100 people who took a proton pump inhibitors (PPI) hardly had heartburn any more after two to eight weeks.
In other words, the medications led to a noticeable improvement in symptoms in 45 out of 100 people.
Research has shown that proton pump inhibitors usually relieve the symptoms or reduce food pipe inflammations better than H2-receptor antagonists do. But proton pump inhibitors (PPIs) sometimes don’t reduce the production of stomach acid enough at night. If this happens, people may have reflux symptoms at night despite taking medication. In the US and other countries, proton pump inhibitors (PPIs) are available over the counter at low doses and in small pack sizes. A prescription is needed for higher doses.
H2-receptor antagonists (H2RAs)
H2-receptor antagonists (e.g., ranitidine, cimetidine, famotidine, nizatidine) prevent large amounts of stomach juices from being made, by blocking the action of the hormone histamine in the stomach. Studies have shown that these drugs can relieve the symptoms of reflux:
- 41 out of 100 people who took a dummy drug (placebo) hardly had heartburn any more after two to six weeks.
- 55 out of 100 people who took an H2-receptor antagonist hardly had heartburn any more after two to six weeks.
In other words, the medication relieved heartburn in 14 out of 100 people.
Antacids
Antacids used to be a commonly used treatment option in Germany. These drugs are meant to bind to stomach acid, thereby neutralizing acidic stomach juices in the food pipe and stomach. But no good-quality studies have shown that antacids help in people who have GERD. Antacids might be an option if someone only has mild heartburn or cannot tolerate the medications mentioned above. In Germany, they are available in pharmacies without a prescription.
Prokinetics
Prokinetics are meant to speed up the emptying of your stomach and help stop stomach contents from flowing back into the food pipe. However, it is not clear whether they help in people who have GERD. There has not been enough good-quality research in this area. For this reason, prokinetics are only rarely used in the treatment of GERD in the US.
Side effects does the medication
Overall, about 2 out of 100 people who take proton pump inhibitors have side effects like diarrhea, nausea or vomiting, pain in the upper stomach area, difficulty swallowing or headaches. Sometimes these side effects can be avoided by switching to a different proton pump inhibitors (PPI) or changing the dose.
The long-term use of Proton pump inhibitors (PPIs) can increase the risk of bone fractures, particularly if they are taken at high doses for more than a year. There is some debate as to whether these drugs might also make people more likely to develop a severe inflammation of the bowel or pneumonia.
Fewer than 1 out of 100 people who take H2-receptor antagonists have side effects such as nausea or headaches.
- Vakil N, Van Zanten SV, Kahrilas P, Dent J, Jones R, Global Consensus G. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. American Journal of Gastroenterology 2006;101(8):1900-20.[↩][↩]
- Solaymani-Dodaran M, Logan RF, West J, Card T, Coupland C. Risk of oesophageal cancer in Barrett’s oesophagus and gastro-oesophageal reflux. Gut 2004;53(8):1070-4.[↩]
- Cook MB, Corley DA, Murray LJ, Liao LM, Kamangar F, Ye W, et al. Gastroesophageal reflux in relation to adenocarcinomas of the esophagus: a pooled analysis from the Barrett’s and Esophageal Adenocarcinoma Consortium (BEACON). PloS One 2014;9(7):e103508.[↩]
- El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 2014;63(6):871-80.[↩][↩]
- Dent J, El-Serag HB, Wallander MA, Johansson S. Epidemiology of gastroesophageal reflux disease: a systematic review. Gut 2005;54:710-7.[↩]
- Boeckxstaens GE, Rohof WO. Pathophysiology of gastroesophageal reflux disease. Gastroenterology Clinics of North America 2014;43(1):15-25.[↩][↩][↩][↩]
- Watson A. Update: total versus partial laparoscopic fundoplication. Digestive Surgery 1998;15(2):172-80.[↩][↩]
- The impact of laparoscopic Nissen fundoplication on the long-term quality of life in patients with gastroesophageal reflux disease. Korkolis DP, Kapritsou M, Konstantinou EA, Giannakopoulou M, Chrysi MS, Tsakiridou M, Kouloura A, Flamourakis M, Maricosu M, Gontikakis E, Plataniotis G. Gastroenterol Nurs. 2015 Mar-Apr; 38(2):111-5. https://www.ncbi.nlm.nih.gov/pubmed/25831248/[↩]
- Guidelines for surgical treatment of gastroesophageal reflux disease (GERD). Society of American Gastrointestinal Endoscopic Surgeons (SAGES). Surg Endosc. 1998 Feb; 12(2):186-8. https://www.ncbi.nlm.nih.gov/pubmed/9479742/[↩]
- Owers C, Ackroyd R. Management of gastroesophageal reflux disease and hiatus hernia: Overview and authors’ perspective. J Surg. 2013;1:51–8.[↩]
- Influence of wrap length on the effectiveness of Nissen and Toupet fundoplication: a prospective randomized study. Mickevicius A, Endzinas Z, Kiudelis M, Jonaitis L, Kupcinskas L, Maleckas A, Pundzius J. Surg Endosc. 2008 Oct; 22(10):2269-76. https://www.ncbi.nlm.nih.gov/pubmed/18398651/[↩]
- Du X, Hu Z, Yan C, Zhang C, Wang Z, Wu J. A meta-analysis of long follow-up outcomes of laparoscopic Nissen (total) versus Toupet (270°) fundoplication for gastro-esophageal reflux disease based on randomized controlled trials in adults. BMC Gastroenterology. 2016;16:88. doi:10.1186/s12876-016-0502-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4969978/[↩]
- Strate U, Emmermann A, Fibbe C, Layer P, Zornig C. Laparoscopic fundoplication: Nissen versus Toupet two-year outcome of a prospective randomized study of 200 patients regarding preoperative esophageal motility. Surg Endosc. 2008;22:21–30. doi: 10.1007/s00464-007-9546-8.[↩]
- Booth MI, Stratford J, Jones L, Dehn TC. Randomized clinical trial of laparoscopic total (Nissen) versus posterior partial (Toupet) fundoplication for gastro-oesophageal reflux disease based on preoperative oesophageal manometry. Br J Surg. 2008;95(1):57–63. doi: 10.1002/bjs.6047[↩]
- Guérin E, Betroune K, Closset J, Mehdi A, Lefebvre JC, Houben JJ, Gelin M, Vaneukem P, El NI. Nissen versus Toupet fundoplication: results of a randomized and multicenter trial. Surg Endosc. 2007;21(11):1985–90. doi: 10.1007/s00464-007-9474-7[↩]
- Zacherl J, Roy-Shapira A, Bonavina L, Bapaye A, Kiesslich R, Schoppmann SF, et al. Endoscopic anterior fundoplication with the Medigus Ultrasonic Surgical Endostapler (MUSE) for gastroesophageal reflux disease: 6-month results from a multi-center prospective trial. Surgical Endoscopy 2015;29(1):220-9.[↩]
- Garg SK, Gurusamy KS. Laparoscopic fundoplication surgery versus medical management for gastro-oesophageal reflux disease (GORD) in adults. Cochrane Database of Systematic Reviews 2015, Issue 11. Art. No.: CD003243. DOI: 10.1002/14651858.CD003243.pub3. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD003243.pub3/full[↩][↩][↩][↩][↩]
- Heartburn and GERD: Treatment options for GERD. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072436[↩][↩]
- GERD pathogenesis, pathophysiology, and clinical manifestations. Kahrilas PJ. Cleve Clin J Med. 2003 Nov; 70 Suppl 5():S4-19. https://www.ncbi.nlm.nih.gov/pubmed/14705378/[↩]
- Columnar mucosa and intestinal metaplasia of the esophagus: fifty years of controversy. DeMeester SR, DeMeester TR. Ann Surg. 2000 Mar; 231(3):303-21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1421001/[↩]
- Rantanen TK, Salo JA, Salminen JT, Kellokumpu IH. (1999) Functional outcome after laparoscopic or open Nissen fundoplication: a follow-up study. Archives of surgery. 134: 240–244 https://www.ncbi.nlm.nih.gov/pubmed/10088561[↩]
- Owers C, Ackroyd R. (2013) Management of gastroesophageal reflux disease and hiatus hernia: Overview and authors’ perspective. Journal of Surgery 1: 51–58.[↩]
- Mickevičius A, Endzinas Ž, Kiudelis M, Jonaitis L, Kupčinskas L, Pundzius J, et al. (2013) Influence of wrap length on the effectiveness of Nissen and Toupet fundoplications: 5-year results of prospective, randomized study[J]. Surgical endoscopy 27: 986–991. doi: 10.1007/s00464-012-2550-7 https://www.ncbi.nlm.nih.gov/pubmed/23052526[↩]
- Nissen R. (1956) Gastropexy as the lone procedure in the surgical repair of hiatus hernia. The American Journal of Surgery 92: 389–392. https://www.ncbi.nlm.nih.gov/pubmed/13354861[↩]
- DeMeester TR, Bonavina L, Albertucci M. (1986) Nissen fundoplication for gastroesophageal reflux disease. Evaluation of primary repair in 100 consecutive patients. Annals of surgery 204: 9–20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1251217/pdf/annsurg00089-0015.pdf[↩]
- del Pino Porres FJ, Sancho Fornos S, Benages Martinez A, Mora F. (2000) Manometric comprobation of esophagogastric junction competence after Nissen fundoplication and its relation to the length of fundic wrap. World journal of surgery 24: 870–873. https://www.ncbi.nlm.nih.gov/pubmed/10833257[↩]
- Worrell SG, Greene CL, DeMeester TR. (2014) The state of surgical treatment of gastroesophageal reflux disease after five decades. Journal of the American College of Surgeons 219: 819–830. doi: 10.1016/j.jamcollsurg.2014.05.018 https://www.ncbi.nlm.nih.gov/pubmed/25241236[↩]
- Chrysos E, Tsiaoussis J, Zoras OJ, Athanasakis E, Mantides A, Katsamouris A, et al. (2003) Laparoscopic surgery for gastroesophageal reflux disease patients with impaired esophageal peristalsis: total or partial fundoplication? Journal of the American College of Surgeons 197: 8–15. https://www.ncbi.nlm.nih.gov/pubmed/12831918[↩]
- Shan CX, Zhang W, Zheng XM, Jiang DZ, Liu S, Qiu M. (2010) Evidence-based appraisal in laparoscopic Nissen and Toupet fundoplications for gastroesophageal reflux disease. World journal of gastroenterology: WJG, 16: 3063–3071. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2890948/[↩]
- Tan G, Yang Z, Wang Z. (2011) Meta-analysis of laparoscopic total (Nissen) versus posterior (Toupet) fundoplication for gastro-oesophageal reflux disease based on randomized clinical trials. ANZ journal of surgery 81: 246–252. doi: 10.1111/j.1445-2197.2010.05481.x https://www.ncbi.nlm.nih.gov/pubmed/21418467[↩]
- Koch OO, Kaindlstorfer A, Antoniou SA, Luketina RR, Emmanuel K, Pointner R. (2013) Comparison of results from a randomized trial 1 year after laparoscopic Nissen and Toupet fundoplications[J]. Surgical endoscopy 27: 2383–2390. doi: 10.1007/s00464-013-2803-0 https://www.ncbi.nlm.nih.gov/pubmed/23361260[↩]
- Qin M, Ding G, Yang H. (2013) A clinical comparison of laparoscopic nissen and toupet fundoplication for gastroesophageal reflux disease. Journal of Laparoendoscopic & Advanced Surgical Techniques 23: 601–604. https://www.ncbi.nlm.nih.gov/pubmed/23614820[↩]
- Shan C-X, Zhang W, Zheng X-M, Jiang D-Z, Liu S, Qiu M. Evidence-based appraisal in laparoscopic Nissen and Toupet fundoplications for gastroesophageal reflux disease. World Journal of Gastroenterology : WJG. 2010;16(24):3063-3071. doi:10.3748/wjg.v16.i24.3063. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2890948/[↩]
- Zaninotto G, Rizzetto C. Endoscopic and surgical management of achalasia. Eur Surg. 2008;40:146–153.[↩]
- Wei M-T, He Y-Z, Deng X-B, et al. Is Dor fundoplication optimum after laparoscopic Heller myotomy for achalasia? A meta-analysis. World Journal of Gastroenterology : WJG. 2013;19(43):7804-7812. doi:10.3748/wjg.v19.i43.7804. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3837282/[↩][↩]
- Richards WO, Torquati A, Holzman MD, et al. Heller myotomy versus Heller myotomy with Dor fundoplication for achalasia: a prospective randomized double-blind clinical trial. Ann Surg. 2004;240(3):405–415 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1356431/[↩][↩]
- Topart P, Deschamps C, Taillefer R, Duranceau A. Long-term effect of total fundoplication on the myotomized esophagus. Ann Thorac Surg. 1992;54(6):1046–1051 https://www.ncbi.nlm.nih.gov/pubmed/1449285[↩]
- Rebecchi F, Giaccone C, Farinella E, Campaci R, Morino M. Randomized controlled trial of laparoscopic Heller myotomy plus Dor fundoplication versus Nissen fundoplication for achalasia: long term results. Ann Surg. 2008;248(6):1023–1030[↩]
- Williams VA, Peters JH. Achalasia of the esophagus: a surgical disease. J Am Coll Surg 2009;208(1):151–162[↩]
- Wykypiel H, Bonatti H, Hinder RA, Glaser K, Wetscher GJ. The laparoscopic fundoplications: Nissen and partialposterior (Toupet) fundoplication. Eur Surg. 2006;38:244–9.[↩]
- Cuschieri A, Hunter J, Wolfe B, Swanstrom LL, Hutson W. Multicentre evaluation of laparoscopic antireflux surgery. Preliminary report. Surg Endosc. 1993;7:505–10.[↩]





{kind=link}