Contents
What is galactorrhea
Galactorrhea occurs when one or both breasts make milk or a milky discharge. Galactorrhea is not related to milk production in breastfeeding. The breasts may leak only when touched, or on their own. Galactorrhea can occur in women or in men, but is less common in men 1. Rarely, it can occur in newborns. The incidence is variable, but it can occur in up to 90 percent of women with hyperprolactinemia 2. The marked variability is likely a result of the difference in how the milk is expressed and how galactorrhea is defined.
Galactorrhea itself isn’t a disease, but it could be a sign of an underlying problem. Galactorrhea usually occurs in women, even those who have never had children or after menopause. But galactorrhea can happen in men and even in infants.
Excessive breast stimulation, medication side effects or disorders of the pituitary gland all may contribute to galactorrhea. Often, galactorrhea results from increased levels of prolactin, the hormone that stimulates milk production.
Sometimes, the cause of galactorrhea can’t be determined. The condition may resolve on its own.
If you have a persistent, spontaneous milky nipple discharge from one or both of your breasts and you’re not pregnant or breast-feeding, make an appointment to see your doctor.
If breast stimulation — such as excessive nipple manipulation during sexual activity — triggers nipple discharge from multiple ducts, you have little cause for worry. The discharge probably doesn’t signal anything abnormal, including breast cancer, but you should still see a doctor for evaluation.
- Nonmilky nipple discharge — particularly bloody, yellow or clear spontaneous discharge that comes from one duct or is associated with a lump you can feel — requires prompt medical attention, as it may be a sign of an underlying breast cancer.
The pituitary gland
The pituitary gland (hypophysis) is located at the base of the brain where it sits in the middle of the head in a bony box called the sella turcica, where a pituitary stalk (infundibulum) attaches it to the hypothalamus. The gland is about 1 centimeter in diameter and consists of an anterior pituitary or anterior lobe, and a posterior pituitary, or posterior lobe. The pituitary stalk (infundibulum) contains both blood vessels and nerves. The pituitary gland controls a system of hormones in the body that regulate growth, metabolism, the stress response, and functions of the sex organs via the thyroid gland, adrenal gland, ovaries, and testes. The optic nerves sit directly above the pituitary gland. Enlargement of the gland can cause symptoms such as headaches or visual disturbances. Pituitary tumors may also impair production of one or more pituitary hormones, causing reduced pituitary function, also called hypopituitarism.
The pituitary gland, sometimes also called the master gland, because it plays a critical role in regulating growth and development, metabolism, and reproduction. The pituitary gland (hypophysis) produces prolactin and other key hormones including:
- Growth hormone (GH), which regulates growth
- Adrenocorticotropin (ACTH), which stimulates the adrenal glands to produce cortisol, a hormone important in metabolism and the body’s response to stress
- Thyrotropin (TSH or thyroid stimulating hormone), which signals the thyroid gland to produce thyroid hormone, also involved in metabolism and growth
- Luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which regulate ovulation and estrogen and progesterone production in women and sperm formation and testosterone production in men.
Prolactin production and release is mediated via tonic inhibition by dopamine secreted by the hypothalamus.
Figure 1. The pituitary gland location

Figure 2. Pituitary gland
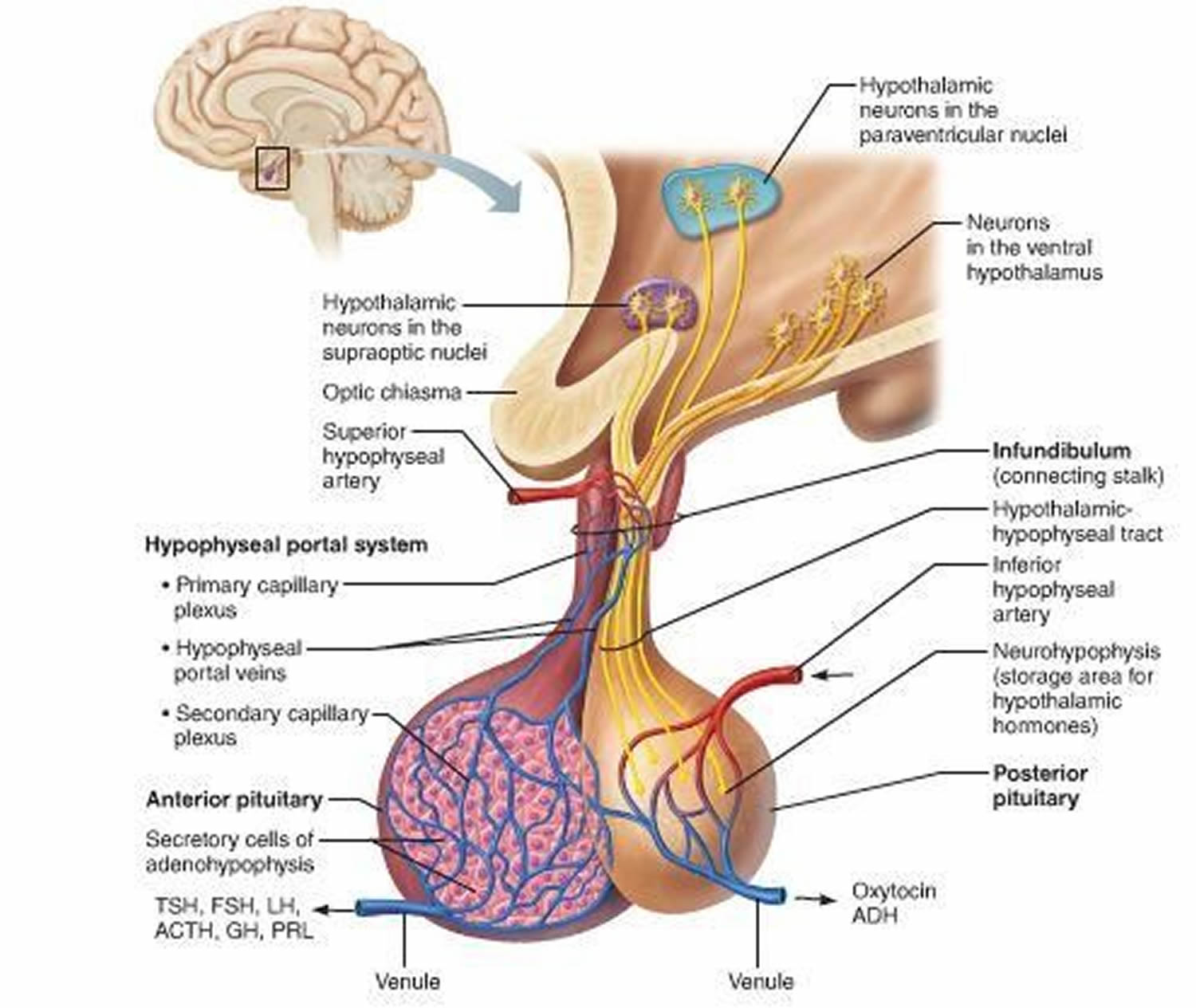
Figure 3. The hypothalamus and pituitary gland (anterior and posterior) endocrine pathways and target organs
 Prolactin
Prolactin
It is important to understand the mechanism underlying breast development and lactation. Breast development is affected by a number of factors, including estrogen, progesterone, and prolactin (PRL) levels. Prolactin (PRL) is essential for morphologic breast development and lactation, which includes synthesis of milk and maintenance of milk production 3.
Prolactin (PRL) is synthesized and secreted from the lactotrophs in the anterior pituitary gland. Hypothalamic dopamine inhibits prolactin secretion 4. There are several possible hypothalamic releasing factors for prolactin. Vasoactive intestinal polypeptide stimulates prolactin synthesis. Thyrotropin-releasing hormone can increase prolactin secretion in the short term, but plays only a minor role overall (Figure 4) 5.
The pituitary lactotroph and prolactin secretion are also directly stimulated by estrogen 6, which explains why pregnant women have elevated prolactin levels 7. Following delivery, prolactin increases with each suckling episode, stimulating milk production. Over the next several weeks, as breastfeeding gradually shifts from being on demand to a schedule, the increases in prolactin levels become less. By two to three months, prolactin levels no longer increase with each suckling episode, but milk production continues. Following cessation of breastfeeding, milk production rapidly decreases so that it is usually gone after a month.
Figure 4. Prolactin regulation – production, release and inhibition
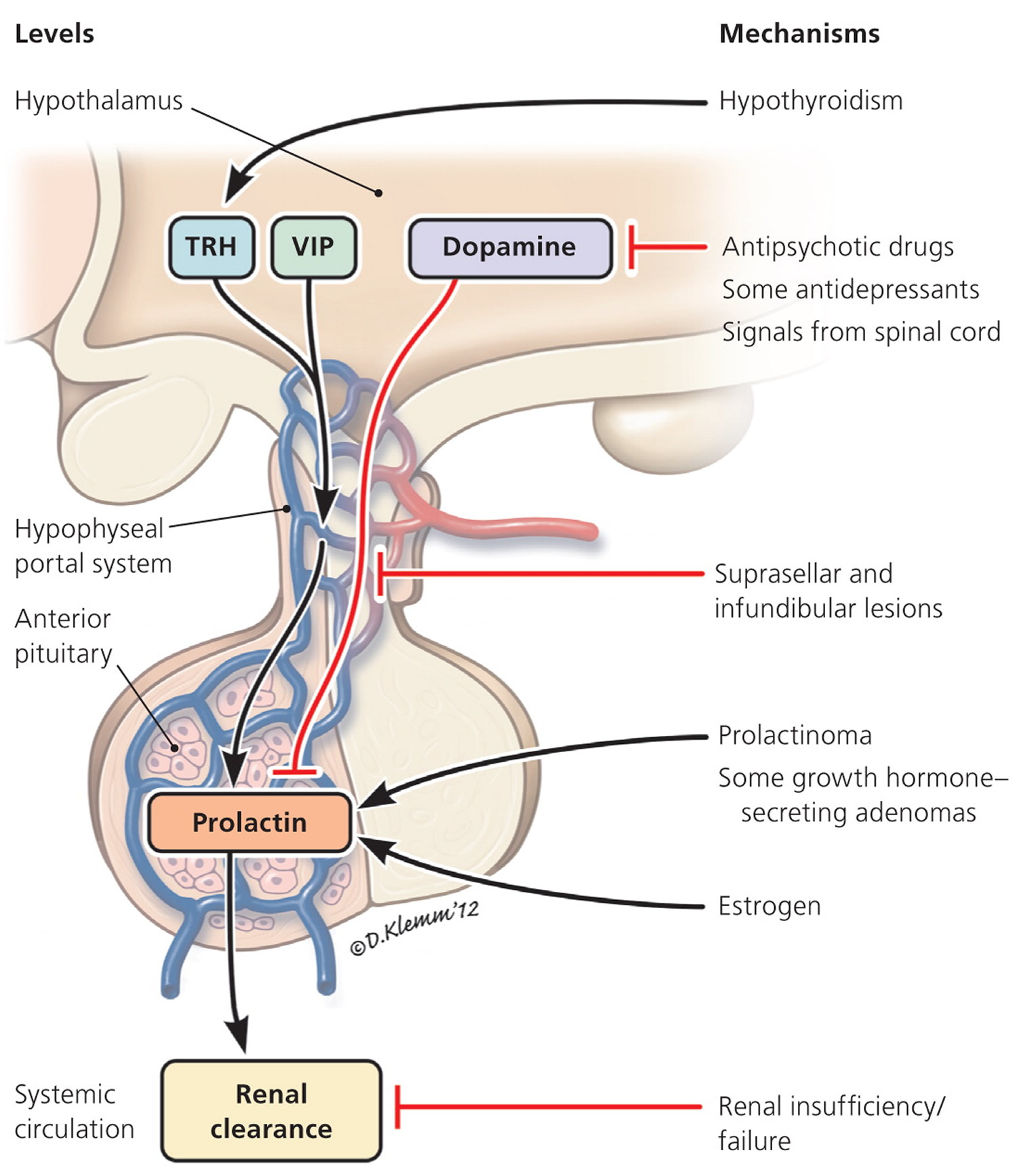
Note: Regulation of prolactin level under physiologic and pathologic conditions. Arrows indicate stimulation, whereas bars depict inhibition. The regulation of serum prolactin occurs at different levels, which is illustrated on the left. The right side lists the common causes of hyperprolactinemia and relevant mechanisms. (TRH = thyrotropin-releasing hormone; VIP = vasoactive intestinal polypeptide.)
Galactorrhea causes
There are many possible causes of galactorrhea. Someone who has it, most likely has an underlying condition.
Galactorrhea often results from too much prolactin — the hormone responsible for milk production (lactation) when you have a baby. Prolactin is produced by your pituitary gland, a marble-sized gland at the base of your brain that secretes and regulates several hormones.
Possible causes include:
Hyperprolactinemic galactorrhea
- Pregnancy
- Oral birth control pills
- Over stimulation of the breasts, such as during sexual activity
- Frequent (daily) breast self-exams
- Clothing that irritates the breasts (may include scratchy wool shirts or bras that don’t fit well)
- Often they are located in the pituitary gland in the brain. Most tumors are benign, or not cancerous.
- Certain medications. These can include hormones, antidepressants, blood pressure medicines, and sedatives.
- Herbal supplements. These can include nettle, fennel, blessed thistle, anise, and fenugreek seed.
- Drugs, such as marijuana, cocaine, and opiates
- Kidney disease
- An underactive thyroid (hypothyroidism). The thyroid is a gland that produces hormones.
- Nerve damage to the chest wall from chest surgery, breast surgery, burns, herpes zoster or other chest injuries
- Injury or trauma to your chest or spinal cord
- Hypothalamic or infundibular lesions:
- Tumors –
- Craniopharyngioma
- Germinoma
- Meningioma
- Infiltrative disorders –
- Histiocytosis
- Sarcoidosis
- Others –
- Rathke’s cleft cysts
- Tumors –
- Pituitary lesions:
- Prolactinoma
- Acromegaly
- Others
Galactorrhea in newborns
Galactorrhea sometimes occurs in newborns. High maternal estrogen levels cross the placenta into the baby’s blood. This can cause enlargement of the baby’s breast tissue, which may be associated with a milky nipple discharge.
Physiologic
Excessive nipple manipulation, including during sex or suckling, can cause hyperprolactinemia and galactorrhea.8,9 In the neonatal period, the high level of estrogen from the mother can cause transient galactorrhea in the newborn, called witch’s milk.10,11 During pregnancy, especially during the third trimester, women can have galactorrhea with prolactin levels up to 200 mcg per L 8. Other causes of transient hyperprolactinemia are vigorous exercise and physical stress 9.
Disorders involving the hypothalamus or pituitary stalk
Suprasellar or sellar lesions extending dorsally to involve the pituitary stalk can lead to hyperprolactinemia and galactorrhea. This is called the “stalk effect.” Such lesions cause impairment of dopamine secretion from the hypothalamus or its transport from the hypothalamus to the pituitary gland 10. These lesions include large nonfunctioning pituitary adenomas, germ cell tumors, craniopharyngiomas, Rathke’s cleft cysts, meningiomas, neural sarcoidosis, and Langerhans cell histiocytosis. Generally, prolactin levels are rarely higher than 100 mcg per L with these conditions 11.
Pituitary disorders
Pituitary adenomas are the most common cause of hyperprolactinemia, which results from either direct production by the adenoma (prolactinoma) or the stalk effect. Prolactinomas are the most common pituitary adenomas and are classified into two types based on size: microadenomas (less than 1 cm) and macroadenomas (1 cm or greater) 12. Circulating prolactin levels usually parallel tumor size, such that microadenomas rarely result in prolactin levels higher than 200 mcg per L and macroadenomas usually result in prolactin levels higher than 200 mcg per L. On the other hand, if a very large macroadenoma (greater than 3 cm) is found in a patient with a normal or only mildly elevated prolactin level, the “hook effect” must be suspected. The hook effect is an assay artifact caused by an extremely high level of prolactin, which saturates the detecting antibody used in the prolactin assay, thus resulting in a falsely low reported value 13.
About 20 to 50 percent of the pituitary adenomas in patients with acromegaly also secrete prolactin 14. In addition, growth hormone has a lactogenic effect, which explains why some patients with acromegaly have galactorrhea without hyperprolactinemia.
Thyroid disorders
Hypothyroidism has been associated with hyperprolactinemia and galactorrhea 3, likely because of elevated thyrotropin-releasing hormone levels resulting from less negative feedback from the thyroid hormone. This in turn stimulates prolactin secretion directly by activating thyrotropin-releasing hormone receptors in the lactotrophs4 or indirectly by regulating hypothalamic dopamine release 15.
Kidney disease
Hyperprolactinemia has also occurred in patients with renal insufficiency 16. Prolactin levels up to 1,000 mcg per L have been reported. The mechanism is likely a result of decreased clearance of prolactin, as well as continued secretion. After kidney transplantation, hyperprolactinemia and galactorrhea can usually be corrected or significantly improved, sometimes within days 17.
Hyperestrogenemia
Estrogen stimulates lactotroph proliferation and prolactin secretion directly 4 and indirectly by inhibiting the hypothalamic dopamine neurons 6. An ovarian hyperstimulation syndrome due to a follicle-stimulating hormone (FSH)–secreting tumor has been associated with hyperprolactinemia and galactorrhea, both of which resolved after tumor removal, indicating that the very high estrogen level contributes to the previously mentioned clinical features 18. Clinically, the effects of estrogen are most evident during pregnancy, when the high estrogen levels cause lactotroph hyperplasia, hyperprolactinemia, and even stimulation of growth of a preexisting prolactinoma 19. Despite the well-known stimulatory effect of estrogen on lactotrophs, the effect of oral contraceptives and hormone therapy, especially low-dose estrogen (30 mcg or less of ethinyl estradiol), on hyperprolactinemia and prolactinoma is not well established.
Lesions involving the chest wall
Various chest wall irritations have been reported to cause hyperprolactinemia and galactorrhea, such as mammoplasty, burns, herpes zoster, trauma, and spinal cord injury 20. The signal from the chest wall is postulated to be first transmitted to the spinal cord, then further relayed to the hypothalamus to reduce the dopamine signal, thereby inducing hyperprolactinemia 20.
Medication induced
Hyperprolactinemia and galactorrhea are often caused by medications 21, most commonly antipsychotics, gastrointestinal promotility agents, and verapamil. Antipsychotics and gastrointestinal promotility agents block the dopamine receptor on the pituitary lactotrophs, decreasing the normal inhibition of prolactin release and leading to hyperprolactinemia.
Medication classes and substances that can cause hyperprolactinemia:
- Antipsychotics
- Gastrointestinal motility medications: metoclopramide (Reglan)
- Antidepressants: rare
- Antihypertensive medications (not a class-specific effect): verapamil, methyldopa, reserpine
- Others: opioids, cocaine
Normoprolactinemic galactorrhea
In some cases, the cause of galactorrhea is unknown.
Idiopathic galactorrhea
Sometimes doctors can’t find a cause for galactorrhea. This is called idiopathic galactorrhea, and it may just mean that your breast tissue is particularly sensitive to the milk-producing hormone prolactin in your blood. If you have increased sensitivity to prolactin, even normal prolactin levels can lead to galactorrhea.
With long-term follow-up, some women with idiopathic hyperprolactinemia are found to have microprolactinomas that were too small to be detected originally 16. In one-third of patients with idiopathic hyperprolactinemia, the elevated prolactin level will resolve, and in one-half of patients, the prolactin level will remain stable 22. The prolactin levels are usually less than 100 mcg per L 23.
Male galactorrhea
In males, galactorrhea may be associated with testosterone deficiency (male hypogonadism) and usually occurs with breast enlargement or tenderness (gynecomastia). Erectile dysfunction and a lack of sexual desire also are associated with testosterone deficiency.
Galactorrhea prevention
You cannot prevent galactorrhea. However, once you know the cause, you may be able to avoid it.
Galactorrhea symptoms
The main symptom of galactorrhea is a milky white discharge from one of both nipples. Sometimes, the discharge is yellow or greenish in color. Your doctor may want to check you for cancer. Blood in the discharge is not a symptom of galactorrhea. Patients with nipple discharge that comes from a single duct, is bloody or serosanguineous, or is associated with a palpable or radiologically evident breast mass will need further evaluation for breast tumors 24.
Other related symptoms include:
- An absence of menstrual periods or periods that are not regular
- Headaches
- Vision loss
- Decreased sex drive
- Increase in hair growth on your chin or chest
- Acne
- Erectile dysfunction in men
Galactorrhea diagnosis
Your doctor will do a physical exam and review your symptoms. They will ask about your health history and lifestyle, and what medicines you take. The doctor may order blood tests to check your hormone levels. For women, they may order a pregnancy test. If the doctor suspects a tumor, they can order an MRI (magnetic resonance imaging). This test scans your head to see if you have a tumor or defect of the pituitary gland. To check for breast cancer, the doctor can order a mammogram and/or ultrasound.
Testing may involve:
- A physical exam, during which your doctor may try to express some of the fluid from your nipple by gently examining the area around your nipple. Your doctor may also check for breast lumps or other suspicious areas of thickened breast tissue.
- Analysis of fluid discharged from the nipple, to see if fat droplets are present in the fluid, which can help confirm the diagnosis of galactorrhea.
- A blood test, to check the level of prolactin in your system. If your prolactin level is elevated, your doctor will most likely check your thyroid-stimulating hormone (TSH) level, too.
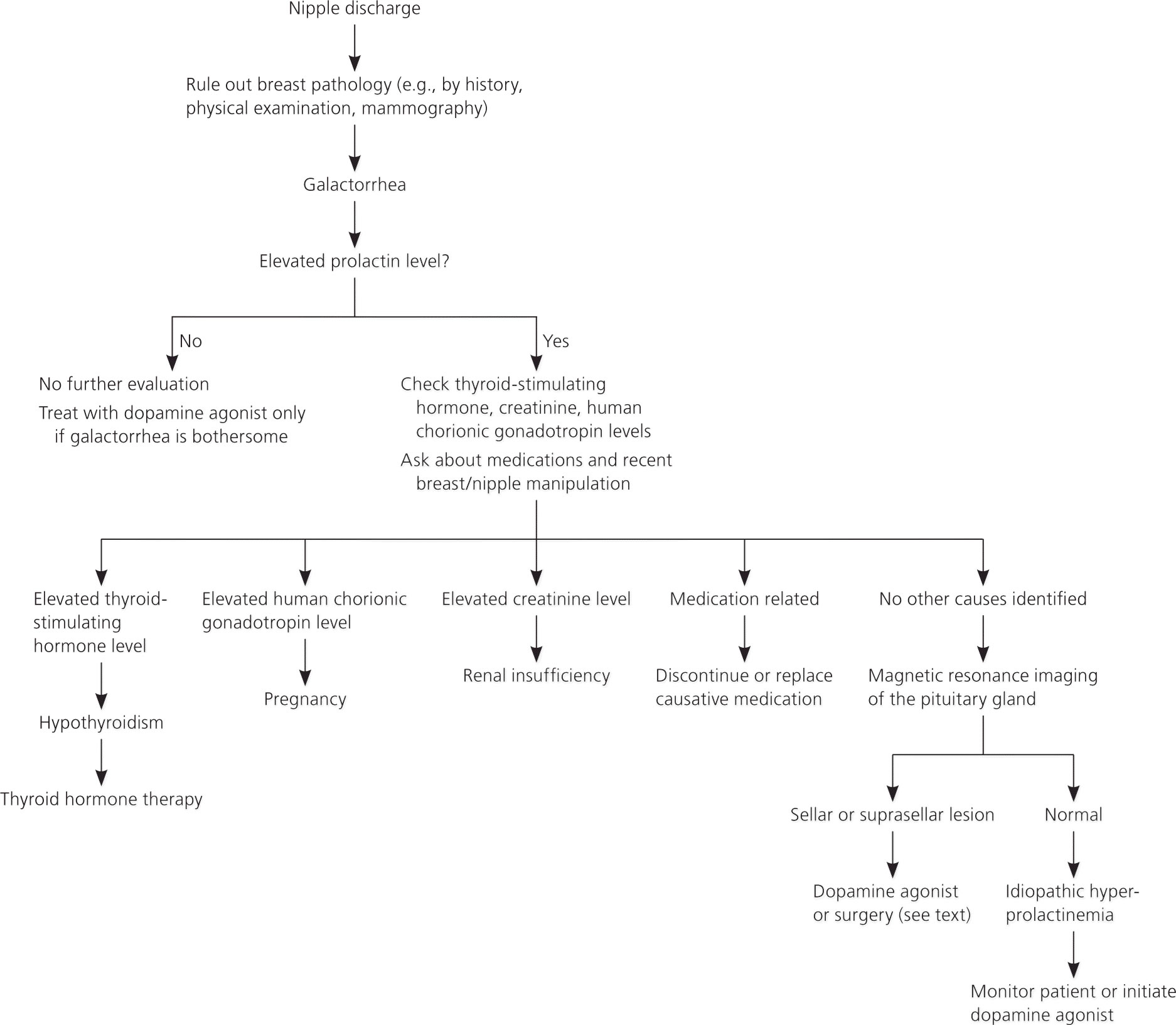
- Prolactin level evaluation: Vigorous exercise and nipple stimulation should be avoided for at least 30 minutes before checking prolactin levels 8. An elevated prolactin level should be confirmed at least once. If the hook effect is suspected, such as in a patient with a very large pituitary adenoma (greater than 3 cm) and a normal or only mildly elevated prolactin level, a 1:100 dilution of the original blood sample should be obtained to confirm the prolactin level 22. In addition, thyroid-stimulating hormone (TSH) and creatinine levels should be obtained to rule out secondary causes of hyperprolactinemia. If hypogonadism is suspected, reproductive hormones such as estrogen or testosterone, luteinizing hormone (LH) and follicle-stimulating hormone (FSH) should also be checked.
- In patients with macroadenomas, other pituitary hormones should also be checked to evaluate for hypopituitarism.
- A pregnancy test, to exclude pregnancy as a possible cause of nipple discharge.
- Mammography, ultrasound or both, to obtain images of your breast tissue, if your doctor finds a breast lump or observes other suspicious breast or nipple changes during your physical exam.
- Magnetic resonance imaging (MRI) of the brain to check for a tumor or other abnormality of your pituitary gland, if your blood test reveals an elevated prolactin level.
- A bone density scan should be performed in patients with hyperprolactinemia and hypogonadism who are at risk of osteoporosis or fracture.
If your doctor suspects a medicine you’re taking might be the cause of galactorrhea, he or she might instruct you to stop taking the medicine for a short time to assess this possible cause.
Figure 5. Evaluation of galactorrhea
 [Source 25]
[Source 25]
Galactorrhea treatment
Treatment depends on the cause of galactorrhea. Benign tumors can be treated with medicine or surgery. Medicine can help if your body is producing too much of a hormone, such as prolactin. It also helps treat problems, such as hypothyroidism. If a certain medicine causes galactorrhea, your doctor may prescribe a different medicine.
In many cases, no treatment is necessary. Over time, the condition may go away on its own. Until then, there are some things you can do to help.
- Avoid stimulating your breasts.
- Avoid touching your nipples during sexual activity.
- Don’t do breast self-exams more than once a month.
- Avoid clothes that are too tight or rub and irritate your skin.
- Wear pads in your bra, for women, to absorb the milky discharge.
Sometimes doctors can’t determine an exact cause of galactorrhea. Your doctor might recommend treatment anyway if you have bothersome or persistent nipple discharge. In such instances, you might be given a medication to block the effects of prolactin or to lower the amount of prolactin in your body. Reducing the prolactin level in your body may eliminate galactorrhea.
Treatment of the causes of hyperprolactinemia
Because most galactorrhea is associated with hyperprolactinemia, the treatment can be classified based on the underlying causes or effects of hyperprolactinemia 26.
- Medication use: Stop taking medication, change dose or switch to another medication. Make medication changes only if your doctor says it’s okay to do so.
- Underactive thyroid gland (hypothyroidism): Take a medication, such as levothyroxine, to counter insufficient hormone production by your thyroid gland (thyroid replacement therapy).
- Pituitary tumor (prolactinoma): Use a medication to shrink the tumor or have surgery to remove it.
- Unknown cause: Try a medication to lower your prolactin level, such as bromocriptine (Parlodel, Cycloset) or cabergoline, and minimize or stop milky nipple discharge. Side effects of these medications commonly include nausea, dizziness and headaches.
For medication-induced hyperprolactinemia, ideally the causitive medication should be discontinued. If the underlying condition warrants continuation of such medications, switching to another medication in a similar class that has lower or no potential to cause hyperprolactinemia would be the most appropriate management option 27. For patients with symptomatic prolactinomas, medical therapy is the treatment of choice 28. Dopamine agonists have been shown to be effective in normalizing prolactin, restoring reproductive hormones, shrinking adenomas, and increasing bone density via normalization of estrogen/testosterone levels 29. Treatment is not recommended for patients with asymptomatic microprolactinoma 26.
Bromocriptine and cabergoline are available in the United States. Compared with bromocriptine, cabergoline is more effective and better tolerated (Table 1) 29. Both drugs are safe for the facilitation of ovulation and pregnancy, although the safety database for bromocriptine is about 10-fold larger 30. Surgery or radiation therapy is rarely needed for prolactinomas 12. Patients with hypothalamic or pituitary lesions other than prolactinomas should be referred to a neurosurgeon, especially if the lesions also present with mass effects 10.
Table 1. Medications to Treat Hyperprolactinemia and Prolactinoma
| Dopamine agonist | Common dosages | Common adverse effects | Comments | |
| Bromocriptine | 2.5 to 15 mg daily | Both medications have similar adverse effects, including gastrointestinal (nausea, vomiting), cardiovascular (postural hypotension, dizziness), and neurologic (drowsiness, headache); cardiac valvulopathy reported with high dose of cabergoline (more than 4 mg daily) | Compared with bromocriptine, the adverse effects of cabergoline are usually less frequent, of shorter duration, and less severe Bromocriptine is preferred by some women who are trying to conceive because of the larger safety database; it typically should be discontinued once pregnancy is confirmed | |
| Cabergoline | 0.25 to 1 mg twice weekly | |||
| or | ||||
| 0.5 to 2 mg once weekly | ||||
NA = not available.
[Source 29]Treatment of hyperprolactinemia or its effects
Sometimes it is not clinically appropriate or safe to treat the cause of hyperprolactinemia (e.g., a patient with a nonresectable brain tumor). Thus, treatment should focus on correcting the hyperprolactinemia with a dopamine agonist, or the resulting hypogonadism by simply replacing estrogen or testosterone in patients who do not have macroprolactinomas. Use of dopamine agonists is sometimes indicated in patients with antipsychotic-induced hyperprolactinemia; however, it is not always successful 31. In addition, such use carries a very small risk of exacerbation of the underlying psychiatric disorder because of activation of the dopamine receptors 32.
If the major concern is decreased reproductive hormones (e.g., estrogen), they can be replaced. Estrogen replacement is considered safe for the patient with a microadenoma or idiopathic hyperprolactinemia. However, its use should be individualized in patients with macroadenomas because estrogen has the potential to increase tumor growth in patients with macroadenomas, although this is generally limited to the very high levels of estrogen found in pregnancy and not with exogenous estrogen use. Because estrogen replacement does not correct the luteinizing hormone and follicle-stimulating hormone deficiencies, women should be advised that such replacement will not restore ovulation. Likewise, in men, replacement of testosterone may not help with spermatogenesis. If the patient has osteoporosis, a bisphosphonate can be added for bone protection.
Treatment of galactorrhea when prolactin levels are normal
If the galactorrhea is not associated with breast tenderness and swelling, and is not particularly bothersome, the patient can be reassured. He or she should also be advised to not check for persistence of the galactorrhea, because repeated milking of the breast will stimulate prolactin production and delay the resolution of the galactorrhea. If the galactorrhea is bothersome, treatment with a low-dose dopamine agonist, such as 0.5 mg of cabergoline once weekly, will generally cause the galactorrhea to resolve, usually within a couple of months. The drug should then be tapered off.
- Kleinberg DL. Endocrinology of mammary development, lactation and galactorrhea. In: DeGroot LJ, Jameson JL, eds. Endocrinology. 4th ed. London, United Kingdom: W.B. Saunders; 2000:2464–2475.[↩]
- Colao A, Sarno AD, Cappabianca P, et al. Gender differences in the prevalence, clinical features and response to cabergoline in hyperprolactinemia. Eur J Endocrinol. 2003;148(3):325–331.[↩]
- Molitch ME. Disorders of prolactin secretion. Endocrinol Metab Clin North Am. 2001;30(3):585–610.[↩][↩]
- Freeman ME, Kanyicska B, Lerant A, Nagy G. Prolactin: structure, function, and regulation of secretion. Physiol Rev. 2000;80(4):1523–1631.[↩][↩]
- van den Pol AN. Excitatory neuromodulator reduces dopamine release, enhancing prolactin secretion. Neuron. 2010;65(2):147–149.[↩]
- Morel GR, Carón RW, Cónsole GM, et al. Estrogen inhibits tuberoinfundibular dopaminergic neurons but does not cause irreversible damage. Brain Res Bull. 2009;80(6):347–352.[↩][↩]
- Molitch ME. Pituitary disorders during pregnancy. Endocrinol Metab Clin North Am. 2006;35(1):99–116vi.[↩]
- Leung AK, Pacaud D. Diagnosis and management of galactorrhea. Am Fam Physician. 2004;70(3):543–550.[↩][↩]
- Peña KS, Rosenfeld JA. Evaluation and treatment of galactorrhea. Am Fam Physician. 2001;63(9):1763–1770.[↩]
- Melmed S, Kleinberg DL. Anterior pituitary. In: Kronenberg H, Williams RH, eds. Williams Textbook of Endocrinology. 11th ed. Philadelphia, Pa.: Elsevier Saunders; 2007:155–262.[↩][↩]
- Karavitaki N, Thanabalasingham G, Shore HC, et al. Do the limits of serum prolactin in disconnection hyperprolactinaemia need re-definition? A study of 226 patients with histologically verified non-functioning pituitary macroadenoma. Clin Endocrinol (Oxf). 2006;65(4):524–529.[↩]
- Klibanski A. Clinical practice. Prolactinomas [published correction appears in N Engl J Med. 2010;362(22): 2142]. N Engl J Med. 2010;362(13):1219–1226.[↩][↩]
- Barkan AL, Chandler WF. Giant pituitary prolactinoma with falsely low serum prolactin: the pitfall of the “high-dose hook effect”: case report. Neurosurgery. 1998;42(4):913–916.[↩]
- Katznelson L, Kleinberg D, Vance ML, et al. Hypogonadism in patients with acromegaly: data from the multi-centre acromegaly registry pilot study [published correction appears in Clin Endocrinol (Oxf). 2001;55(5):699]. Clin Endocrinol (Oxf). 2001;54(2):183–188.[↩]
- Lyons DJ, Horjales-Araujo E, Broberger C. Synchronized network oscillations in rat tuberoinfundibular dopamine neurons: switch to tonic discharge by thyrotropin-releasing hormone. Neuron. 2010;65(2):217–229.[↩]
- Verhelst J, Abs R. Hyperprolactinemia: pathophysiology and management. Treat Endocrinol. 2003;2(1):23–32.[↩][↩]
- Saha MT, Saha HH, Niskanen LK, Salmela KT, Pasternack AI. Time course of serum prolactin and sex hormones following successful renal transplantation. Nephron. 2002;92(3):735–737.[↩]
- Cooper O, Geller JL, Melmed S. Ovarian hyperstimulation syndrome caused by an FSH-secreting pituitary adenoma. Nat Clin Pract Endocrinol Metab. 2008;4(4):234–238.[↩]
- Christin-Maître S, Delemer B, Touraine P, Young J. Prolactinoma and estrogens: pregnancy, contraception and hormonal replacement therapy. Ann Endocrinol (Paris). 2007;68(2–3):106–112.[↩]
- Serri O, Chik CL, Ur E, Ezzat S. Diagnosis and management of hyperprolactinemia. CMAJ. 2003;169(6):575–581.[↩][↩]
- Coker F, Taylor D. Antidepressant-induced hyperprolactinaemia: incidence, mechanisms and management. CNS Drugs. 2010;24(7):563–574.[↩]
- Chahal J, Schlechte J. Hyperprolactinemia. Pituitary. 2008;11(2):141–146.[↩][↩]
- Berinder K, Stackenäs I, Akre O, Hirschberg AL, Hulting AL. Hyperprolactinaemia in 271 women: up to three decades of clinical follow-up. Clin Endocrinol (Oxf). 2005;63(4):450–455.[↩]
- Vaidyanathan L, Barnard K, Elnicki DM. Benign breast disease: when to treat, when to reassure, when to refer. Cleve Clin J Med. 2002;69(5):425–432.[↩]
- Evaluation and Management of Galactorrhea. Am Fam Physician. 2012 Jun 1;85(11):1073-1080. https://www.aafp.org/afp/2012/0601/p1073.html[↩]
- Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273–288.[↩][↩]
- Molitch ME. Medication-induced hyperprolactinemia. Mayo Clin Proc. 2005;80(8):1050–1057.[↩]
- Schlechte JA. Clinical practice. Prolactinoma. N Engl J Med. 2003;349(21):2035–2041.[↩]
- Gillam MP, Molitch ME, Lombardi G, Colao A. Advances in the treatment of prolactinomas. Endocr Rev. 2006;27(5):485–534.[↩][↩][↩]
- Molitch ME. Prolactinomas and pregnancy. Clin Endocrinol (Oxf). 2010;73(2):147–148.[↩]
- Cavallaro R, Cocchi F, Angelone SM, Lattuada E, Smeraldi E. Cabergoline treatment of risperidone-induced hyperprolactinemia: a pilot study. J Clin Psychiatry. 2004;65(2):187–190.[↩]
- Smith S. Neuroleptic-associated hyperprolactinemia. Can it be treated with bromocriptine? J Reprod Med. 1992;37(8):737–740.[↩]





{kind=link}