
Contents
What is Cellulite
Cellulite is a multi-factorial condition that is present in 85–98 % of post-pubertal women worldwide 1. Cellulite is a cosmetic condition of subcutaneous fat herniation through fibrous connective tissue that results in a dimpled appearance of the skin 2. The first notion of cellulite was defined by French doctors in 1922 3. Khan et al. 4 noted that there are specific classic patterns of cellulite that affect women exclusively. White women tend to have somewhat higher rates of cellulite than Asian women 4. The authors also stated that lifestyle factors such as high carbohydrate diets may lead to an increase in total body fat content, which enhances the appearance of cellulite 4. Whether cellulite is a real medical disease or not is still a matter of controversy, however it remains an issue of cosmetic concern to a great number of women. Despite its high prevalence, there have been few scientific investigations into the physiology of cellulite. There have only been a few dozen peer‐reviewed articles devoted to cellulite in the medical literature in the past 30 years.
In normal skin, the hypodermal fat layer is divided into chambers by septae, separating the adipose cells into chambers resembling a quilt. The fibrous tissue strands extend from the dermal layer, through the hypodermal fat layer, and connect to the underlying muscle layer. However, in women with cellulite, the septae sclerose (hardening – a pathological condition in which a tissue has become hard and which is produced by overgrowth of fibrous tissue and other changes) contract, holding the skin at an inflexible length, while hypodermal fat lobules extend upward into the dermis 5. These structural changes cause a heterogeneous effect on the skin surface which is the visible sign of cellulite 6. With age, the integrity of the dermis is further compromised as skin thickness and elasticity decreases 7. Treating any or all of the anatomical features of cellulite restores the skin to a more homogenous state, reducing the appearance of cellulite.
In order to have a better understanding of the micro-anatomical changes of cellulite, Piérard and colleagues examined under a microscope 39 autopsy specimens from 4 women and 11 men who had no evidence of cellulite 8. What they found was the lumpy aspect of the dermohypodermal (dermis-epidermis) interface appeared to represent a gender-linked characteristic of the thighs and buttocks region without being a specific sign of cellulite. The developing cellulite as identified by the mattress phenomenon was related to the presence of focally enlarged fibrosclerotic strands partitioning the hypodermis (subcutis) see Figure 1. Skin Anatomy and Figure 2. Cellulite Formation below. Such strands possibly serve as a physiologic buttress against fat herniation limiting the outpouching of fat lobules on pinching the skin. These structures might represent a reactive process to sustained hypodermal pressure caused by fat accumulation. Concurrently, as the adipose (fat) cells expand with weight gain or water absorption, promoting herniation, or outpouching of fat into the dermis. This results in skin dimpling creating the characteristic cellulite appearance. Two distinct morphologies of cellulite may be identified, sometimes coexisting in the same patient: 1) diffuse rippling in patients with increased adiposity and/or increased skin laxity and 2) dimpling, with discrete ellipsoid or linear depressions, in patients with good skin tone 8.
Figure 1. Normal Skin Anatomy
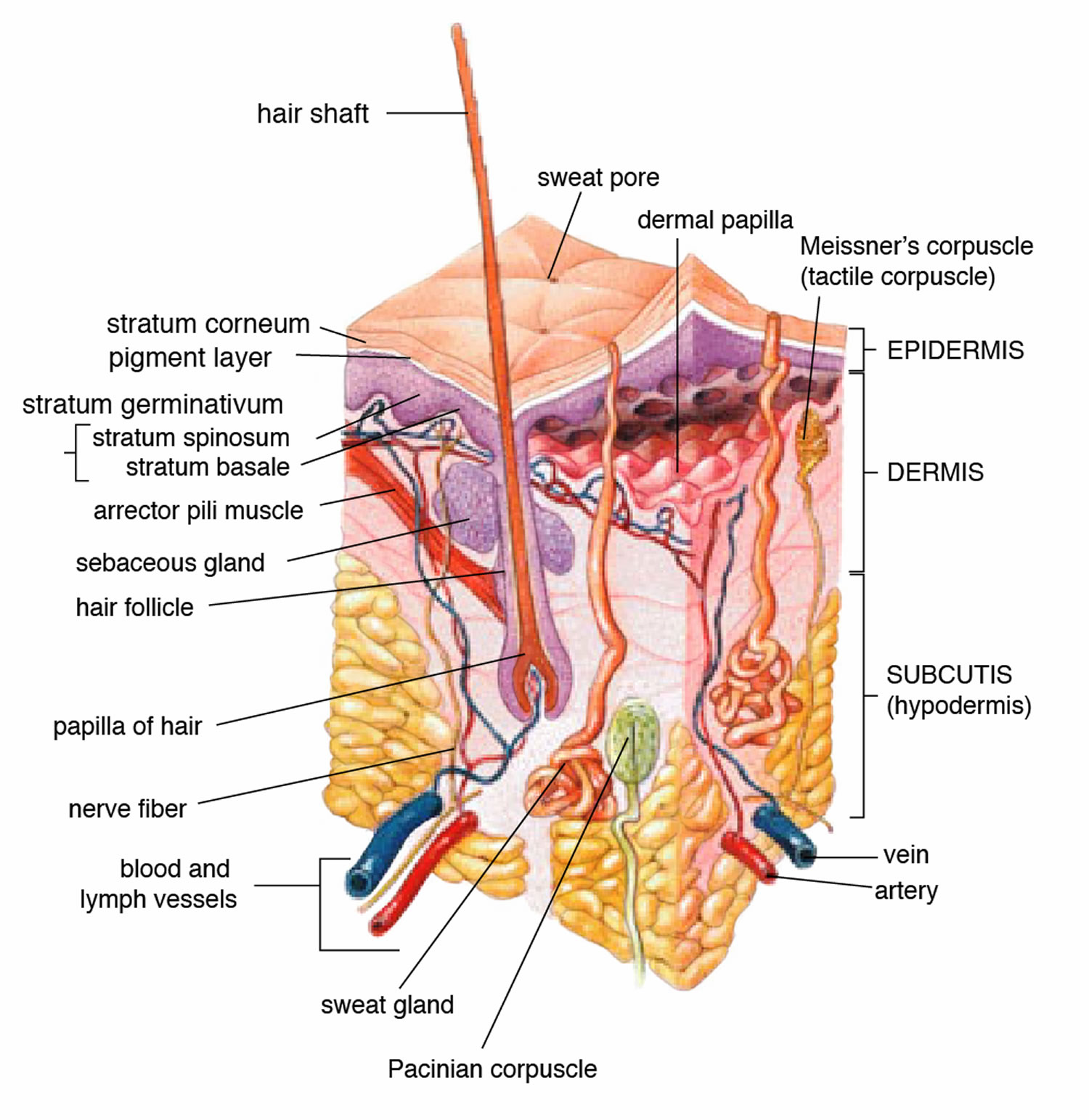
Figure 2. Cellulite Formation
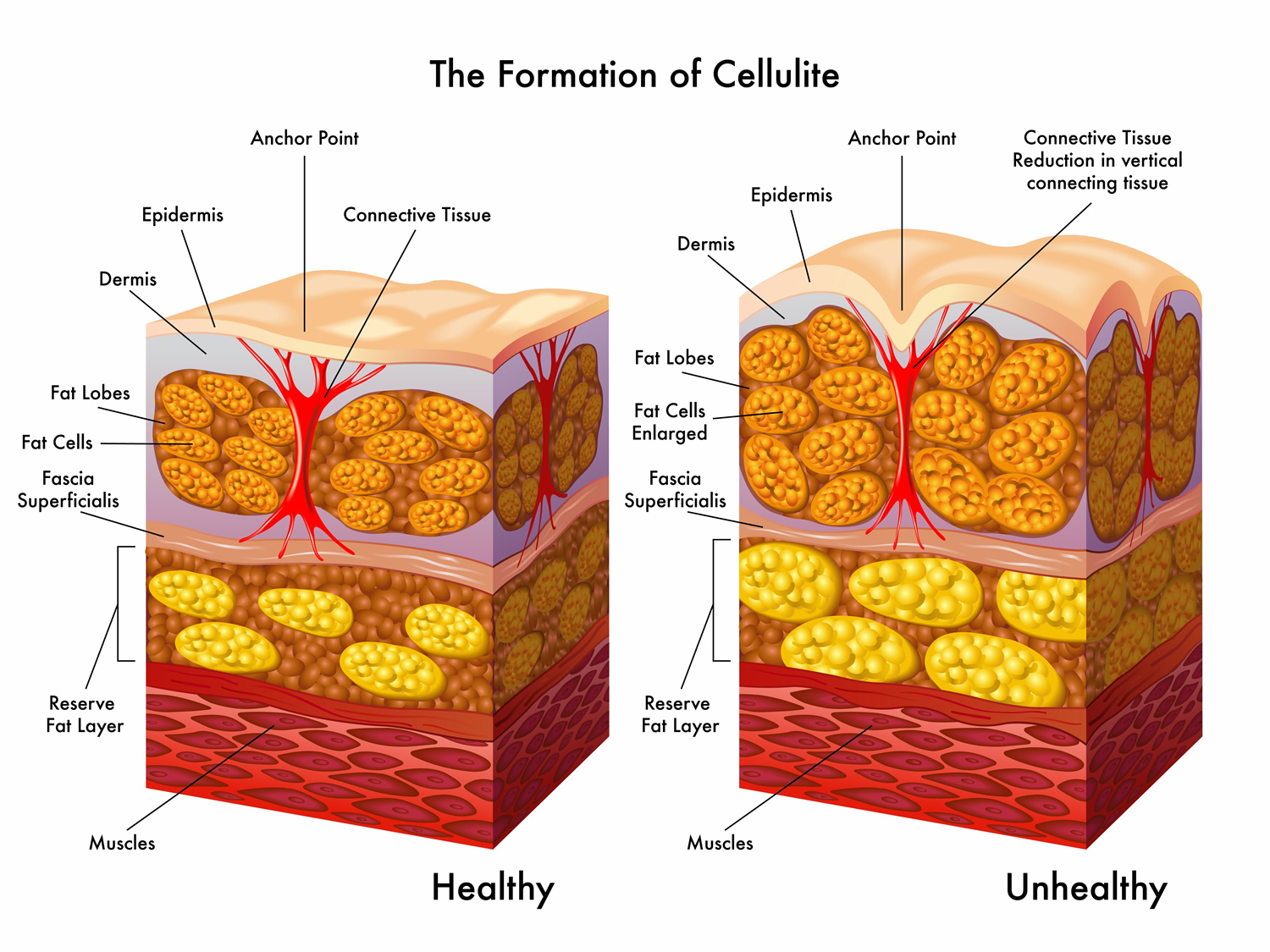
Note (Figure 2): Little is known about what causes cellulite. It is commonly accepted that dermal and subcutaneous connective tissue, which has been weakened by altered and disordered extracellular matrix, plays a key role in the pathophysiology of cellulite. It involves fibrous connective cords that tether the skin to the underlying muscle, with the fat lying between. As fat cells accumulate, they push up against the skin, while the long, tough cords pull down. This creates an uneven surface or dimpling. Consequently, therapies aiming to restore the normal structure of the dermis and subcutaneous tissue can be a meaningful approach to improving the cellulite condition.
The four leading hypotheses that purport to explain the physiology of cellulite include: 1) sexually dimorphic skin architecture; 2) altered connective tissue septae; 3) vascular changes and 4) inflammatory factors.
From a medical point of view, these are fibrous changes and an abnormal swelling involving the subcutaneous tissue layer, lipodystrophy (abnormal or degenerative conditions in which the body is unable to produce fat) or oedemetical (abnormal swelling), fibrosing (forming fibers) deviation of the connective tissue 10. In cellulite, because of disorders of the microcirculation, degenerative changes of the connective tissue occur. Cellulite is more and more often treated as illness, since as the definition of World Health Organization demonstrates, cellulite is more and more often negatively influencing the mental state of both women and men 11.
Despite its high prevalence, it remains a major cosmetic concern for women. From a clinical standpoint, cellulite is characterized by a cottage-cheese-like appearance of the skin, which can be most commonly found in certain areas of the body, especially on the thighs, buttocks and legs. Although cellulite is generally asymptomatic, the more severe stages can be accompanied by the appearance of painful nodules and increased local temperature, which are suggestive of an inflammatory reaction occurring in the dermis and in the underlying subcutaneous adipose (fatty) tissue. Whether cellulite is a real disease or only a disturbing aesthetic issue is still a matter of controversy. This debate notwithstanding, it seems clear from market trends that there is considerable commercial interest in developing effective treatments aimed at reducing the cottage-cheese-like appearance of cellulite areas. Quite disturbingly, the majority of treatment attempts to date have been conducted in an empirical manner and without the application of rigorous scientific methodology. This is likely due–at least in part–to the lack of major, evidence-based pathophysiological insights into the nature of this condition. More stringent regulatory control is needed over commercial products aiming at improving the appearance of cellulite 12.
What Causes Cellulite
Cellulite has a multifactorial etiology. Causes may be genetic, hormonal, or vascular in nature and may be related to the septa configuration in the subdermal tissue. Fibrosis at the dermal-subcutaneous junction as well as decreased vascular and lymphatic circulation also may be causative factors 13.
The subdermal anatomy affects the appearance of cellulite. Utilizing in vivo magnetic resonance imaging, Querleux et al. 14 showed that women with visible cellulite have dermal septa that are thinner and generally more perpendicular to the skin’s surface than women without cellulite. In women without cellulite, the orientation of the septa is more angled into a crisscross pattern. In women with a high percentage of perpendicular septa, the perpendicular septa allow for fat herniation with dimpling of the skin compared to the crisscross septa pattern 4. Other investigators have discussed the reduction of blood flow in specific areas of the body in women, particularly in cellulite-prone areas such as the buttocks and thighs, as another causative factor 4, 15, 16. Rossi and Vergnanini 17 showed that the blood flow was 35% lower in affected cellulite regions than in non-affected regions without cellulite, which can cause congestion of blood and lymphatic flow and increased subdermal pressure, thus increasing the appearance of cellulite.
Weight gain can make cellulite more noticeable, but some lean people have cellulite, as well. It tends to run in families, so genetics might play the biggest role in whether you develop cellulite. An inactive lifestyle also can increase your chances of having cellulite, as can pregnancy. But so far no one has managed to prove the connection between cellulite and obesity, since cellulite also appears in slim and active persons 18. Although there is some controversy regarding the effects of weight loss on the appearance of cellulite 4, 19, it appears that the subdermal septa and morphology have more of an effect on the appearance of cellulite 4, 14, 20.
Hormonal imbalances are regarded as the crucial cause of the cellulite and more precisely – too high concentration of oestrogens compared to the progesterone, that is relative hyperestrogenism 21. Such a hormone situation can appear physiologically in the period of pregnancy, puberty, menopause, as well as while taking the oral contraceptive pills (systemic hormone contraceptive) or in the course of the hormone replacement therapy. Development of cellulite is significantly influenced by two processes constantly occurring in fat cells – lipogenesis (formation of fat) and lipolysis (breakdown of fats) 18.
Mostly oestrogens are the hormones responsible for the development of cellulite, as they are responsible for arranging the fatty tissue. In women, the production of the fatty tissue is independent of the amount of food eaten. The development of the fatty tissue is subject to an adjustment of local hormone mechanisms. Aromatase, which is elevated in the period of the menopause activity, modifies the deficiency of ovarian oestrogens 22, as well as it influences the lipid and glucose metabolism. This process causes the increase in adipocytes, which under the influence of the pressure on blood vessels and lymphatic vessels causes the growth of the local pressure, burdening, and also microcirculation. Shortage of the sex hormone in the menopause exerts an adverse influence on the vasculature 23. It was proved that there is a close relationship between disorders of the venous circulation and pathological changes in the fatty tissue 11.
Progesterone has a relaxing effect on the fibres of smooth muscles and can cause the venostasis triggering disadvantageous morphological and functional changes 11. Disorders in the microcirculation may cause a local rise in pressure and support the increased permeability of veins which is supplying the slow blood flow and increases the viscosity, creating the leukocytary trap. In individual periods of the menopause, an impact of subtle interactions on development of the cellulite is also being considered, namely the impact of oestrogens and other hormones, such as progesterone, growth hormone, melatonin, dehydroepiandrosteron, androgens or insulin which can additionally entail changes associated with the wrong transformation of fats and carbohydrates.
Apart from the hormonal disorders mentioned above, there are other factors 18 that could make someone more susceptible to developing cellulite, here are some of those :
- Genetic Factors. Family tendencies exist for the abnormal deposition of the fatty tissue and its characteristic organization as simultaneously underdeveloped muscle mass 18.
- Bad Eating Habits. The increased supply of carbohydrates and fats supports hyperinsulinemia which, among others, intensifies the process of lipogenesis and is one of deciding causal factors 18.
- Poorly Diet with a lot of preservatives and salt in the food supports retention of liquids which results in swellings 18.
- Low physical activity and a sedentary lifestyle, which disturb correct functioning of the microcirculation and support the accumulation of fatty tissue 18.
- Smoking – Nicotine and many other substances contained in the cigarette smoke cause constriction of blood vessels which supports tissue hypoxia. After certain time, loosened vessels and the improvement in oxidation conditions result in allowing reactive oxygen species to act in the process of hypoxia – the reoxygenation 18.
- Dilators of the peripheral blood vessels applied in the arterial hypertension can affect the development of the cellulite: β-blocking agents, antihistamine and exogenous oestrogens 21.
- Improperly selected clothes and footwear, especially wearing too close-fitting clothes, can contribute to the disruption of the venous outflow 18.
- Wearing high-heeled shoes, through the adverse impact on muscles of calves, disturb the good posture and weaken the function of the muscle pump of shins in transferring the venous blood to the heart 18.
In the prevention of cellulite, it is very important to pay attention to all the causal factors that could potentially cause a person to the formation of celluite. Some factors having a significant influence on cellulite, as for example genetic factors, are outside your control. However, it is worthwhile for you to concentrate on the elimination of factors that are in your control, like changing your poor diet, quit smoking, reduce salt intake and have a more active lifestyle 18.
Hormonal Disorders of Cellulite
In the fatty tissue built from adipocytes (fat cells), synthesis and disintegration occur. Lipogenesis (formation of fat) is supporting the growth and the gradual accumulation of the fatty tissue, however lipolysis (breakdown of fats) is a metabolic process which causes the decomposition of the stored-up fat. Exogenous and endogenic factors affect both processes. In the prevention of cellulite, it is important to keep balance between both processes. Local therapy is aimed at a change of the adipocyte metabolism and should limit lipogenesis and activate lipolysis 18.
Lipolysis is a process of destruction, disintegration and the reduction of lipids stored up in cells of the fatty tissue and muscle occurring with the participation of lipases. Endogenic factors regulating the lipolysis include such hormones and neurotransmitters as adrenaline and noradrenaline (demonstrating poorer action than adrenaline), estradiol and testosterone, adrenocorticotropic hormone (ACTH), growth hormone (GH), thyrotropin (TSH, thyroid stimulating hormone) and leptine, antidiuretic hormone and glucagon 18. Adrenaline being connected with receptors on the surface of β3 adipocytes activates G protein which excites adenyl cyclase and in the end increases cyclical AMP (cAMP). Protein kinase activated by cAMP stimulates the hormone-sensitive lipase causing the disintegration of stored up lipids 18.
Neutral fat lipase (known as desnutrin) hydrolyzes triglycerides (TG) to diglycerides, and hormone-sensitive lipase decomposes diglycerides to monoglycerides. Glycerol and free fatty acids are final products of the lipolysis (free fatty acids), being energy sources for cells 18.
Insulin which is suppressing the initiative of cyklase is the hormone blocking the process of lipolysis and it stimulates activity of lipoprotein lipase, responsible for the synthesis of lipids and the capture of free fatty acids. The process of lipogenesis is also dependent on SREBP-1 transcripting factor whose expression is increased by insulin. For this reason, a low concentration of this hormone can support the lipolysis process 24.
According to the theory of adipocytary receptors, α receptors intensify lipogenesis, however β receptors support lipolysis. Adrenaline, belonging to catecholamines, comes mainly from adrenal medullae and fibres of the sympathetic nervous system, and the stimulation of fat cells is one of its roles with α- and β-adrenergic receptors. An influence on both kinds of receptors is an effect of its acting. The amount of β adrenergic receptors is reduced under the influence of such factors as age – increasing the amount of the fatty tissue which extorts the response of α receptors. It can be the reason for the accumulation of fatty tissue in menopausal women. This relation causes the potential undesirable effect of anti-cellulite therapies 25.
Catechol amines speed up the process of the metabolism via β receptors, affecting carbohydrates and fats economy 23. The consequence of hypoestrogenism is the upset in the balance between noradrenalin, dopamine, serotonin or endorphins in the menopause. Increased secretion of neuroendocrine can be a result of stress, affecting women in their menopause. Increasing the secretion of the noradrenalin shows the lack of the stability of the autonomous nervous system. In the period, the increased production of cortisol is connected with the climacteric and at the same time with a great concentration of adrenaline and noradrenalin 26.
PPAR nuclear receptor affects the metabolism of the fatty tissue. Receptors are one of three kinds of PPAR gamma receptors which influence the maturing and diversifying of adipocytes. They stimulate the accumulation of lipids and increase the synthesis of adiponectin 24. PPAR-α receptors are the second kind of units which influence β-oxidation of free fatty acids and serve as adjusters in lipogenesis 27. Activated receptors through peroxisome proliferators of PPAR – retinal acid and conjugated linoleic acid (CLA) influence the lipolysis process 10. Oestrogens activate the action of adrenergic receptors of the α type, and support the accumulation of fatty tissue in the region of thighs, hips and the pelvis, as well as influence the extension and increase the permeability of blood vessels. This results in the occurrence of microembolisms and microswellings. Oestrogens hinder the process of lipolysis and elevate lipogenesis. They influence the increased amount of glycosaminoglicans (Gag) which is contributing to impairment of the microcirculation (accumulating liquid in the intercellular space creates swelling which causes disorders in the microcirculation).
In the premenopause, in spite of lowering concentrations of the plasmatic estradiol, escalating luteal deficiency caused by more and more rare ovulations can translate into the state relative to hyperestrogenism, and this creates conditions for initiation of growth of the fatty cellulite along with the tendency of swellings.
Another issue is strongly expressed postmenopausal hypoestrogenism, as the maintained peripheral production of androgens, can cause relative hyperandrogenism in older women 28, which can influence the change of arranging of the fatty tissue which surrenders to reduction among others in places typical of women, and develops in the belly and torso regions as well as supports androidal (visceral) type of the build 29. With age, reduced stimulation of oestrogens worsens the blood supply to the skin, suppresses the initiative of fibroblasts, disadvantages normal synthesis of collagen fibres and reduces the number of elastin fibres. Under the skin there can occur perceptible palpable irregularities – conglomerations of the bruised connective tissue underlined with the lack of the skin elasticity. Such changes are characteristic of the slender figure of the cellulite.
Types of Cellulite
In women cellulite most often appears in regions of thighs, the belly and buttocks, in places, which have a lot of the receptors responsible for the lipogenesis 10.
Cellulite is much more common in women than in men. In fact, most women develop some cellulite after puberty. This is because women’s fat is typically distributed in the thighs, hips and buttocks — common areas for cellulite. Cellulite is also more common with aging, when the skin loses elasticity. Whereas in men, cellulite is exclusively seen in pathological states and while applying anti-androgen therapy, for example for the treatment of prostate cancer. Moreover, the cellulite in men is located within the neck and belly region of the body 25.
There are 3 main clinical types of the cellulite 18:
- Fatty – by the overdeveloped fatty tissue;
- Lymphatic – transitional, intensified mainly before the menstruation;
- Alleged – appearing because of weakened tension of the gluteus muscle, visible on the back of thighs; it is possible to improve this state through the right exercises 30.
And on the account of characteristic skin changes, it is possible to divide cellulite into:
- Tough type (in women practising sports where the great cohesion of the skin and the well-developed musculature are characteristic);
- Slender form (in women of the perimenopausal age, is also appearing after dieting; pliability of muscles is characteristic, the skin is poorly tense and loose);
- Hydropic form (the most severe form, appears in women with serious disorders of the cardiovascular system) 31.
Clinically, nodular, uneven forming of the surface of the skin is a sign of cellulite 18. From a medical point of view, the structure of the tissue with cellulite differs from the fatty tissue – all with the increased number and the hypertrophy of adipocytes and with disturbed proportion between saturated and unsaturated fatty acids included in these cells, with a higher the proportion of saturated fatty acids 25.
Rossi and Vergnanini 17 proposed a 4-grade system for evaluating the appearance of cellulite (grade I, no cellulite; grade II, skin that is smooth and without any pronounced dimpling upon standing or lying down but may show some dimpling upon pinching and strong muscle contraction; grade III, cellulite is present in upright positions but not when the patient is in a supine position; grade IV, cellulite can be seen when the patient is standing and in a supine position). Both grades III and IV can be exacerbated by maximal voluntary contraction and strong pinching of the skin because these actions cause the subcutaneous fat to move toward the surface of the skin between the septa. This grading system aligns with categories I through III described by Mirrashed et al. 32.
How Cellulite is Diagnosed and Graded
Cellulite is diagnosed by a cosmetologist or a dermatologist. A palpable medical examination and a visual evaluation are the basis of assessment of cellulite. There are many scales of the evaluation of cellulite. A scale that is universally used is the Doris Maria Hexsel’s photonumerical scale of cellulite intensification – is newer and regarded more exact 18.
Table 1. Doris Maria Hexsel’s photonumeric scale of cellulite intensification
| Clinical morphological features of cellulite advancement | Result |
|---|---|
| 1. Number of visible thickenings | 0 = absence of thickenings |
| 1 = small number; 1-4 visible thickenings | |
| 2 = average number; 5-9 visible thickenings | |
| 3 = high number; 10 and more visible thickenings | |
| 2. Depth of the thickenings | 0 – no changes |
| 1 – superficially deep changes | |
| 2 – mild deep changes | |
| 3 – deep changes | |
| 3. Various morphological models of superficial models of skin changes | 0 – no affected areas |
| 1 – ‘orange skin’ look | |
| 2 – ‘cottage cheese’ look | |
| 3 – ‘mattress’ look | |
| 4. Level of loosening and relaxation of the skin | 0 – absence of visible changes or skin creasings |
| 1 – light creasings | |
| 2 – mild creasings | |
| 3 – numerous creasings | |
| 5. Nürnberger and Müller’s classification scale – in the standing position subjected to ‘pinching test’ (at the relaxed buttock muscle there may not be visible creases; this allows to differentiate 0 from 1) | 0 – zero degree |
| 1 – first degree | |
| 2 – second degree | |
| 3 – third degree |
Photo 1. Doris Maria Hexsel’s photonumeric scale of cellulite intensification
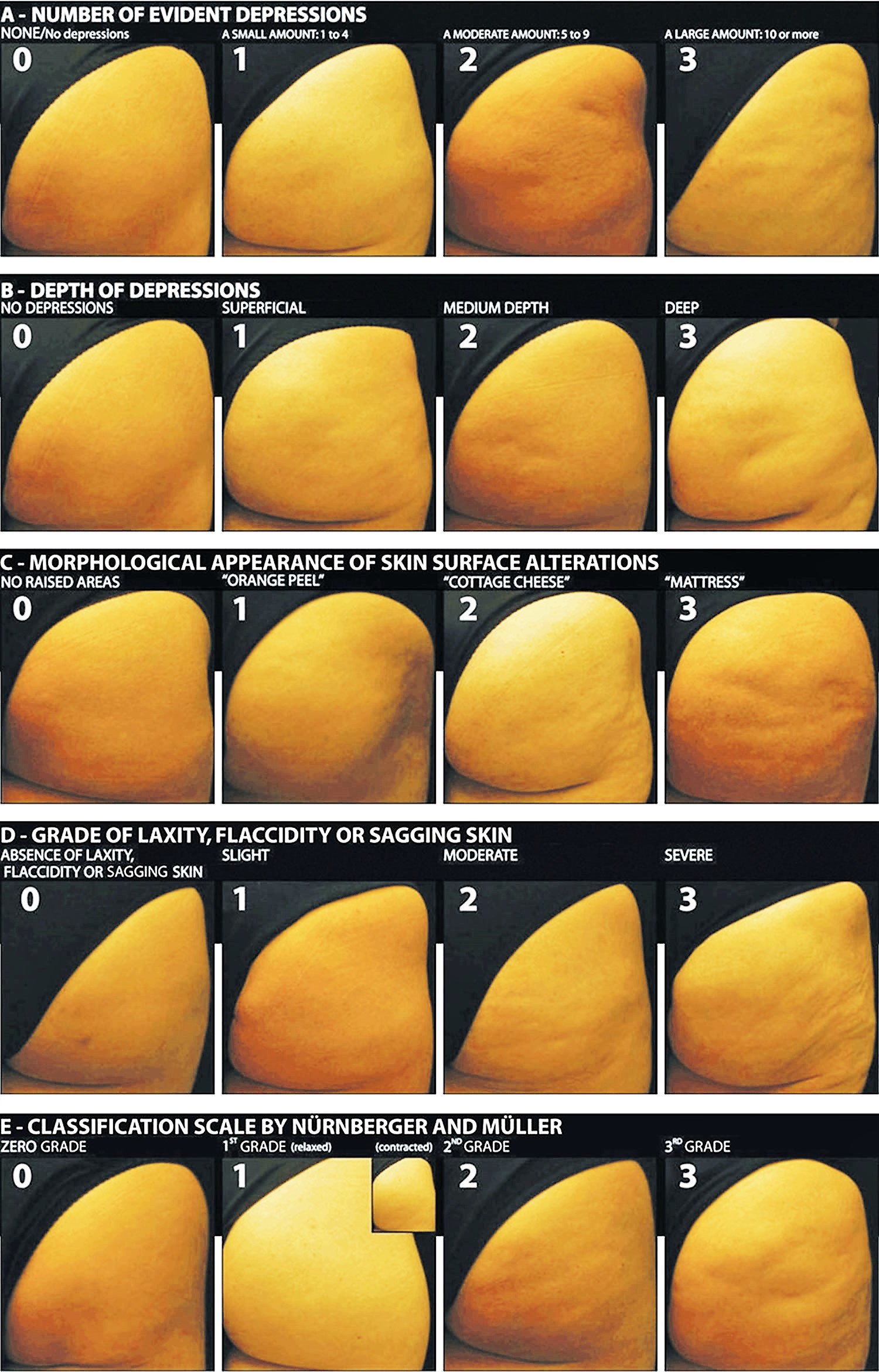
Note: Based on photographs of 55 patients with cellulite, five key morphological aspects of cellulite were identified and were distinguished in the assessment of cellulite problem. The proposed Doris Maria Hexsel’s photonumeric scale of cellulite intensification is a consistent, comprehensive, reliable, and reproducible tool for the standardized and objective assessment of the severity of cellulite 33.
A photonumeric scale of intensifying changes in cellulite is extremely valuable in monitoring therapeutic anti-cellulite methods and can be applied for examining affected patients 33.
It is also possible to assess cellulite basing on specialist examinations: thermography (it determines the temperature of the surface of the body, and colours are indicating the temperature of the tissue), macrography, TEWL determination (measurement of transcutaneous dehydration), the apparatus measurement of greasing or the skin elasticity, videocapillaroscopy (the examination assesses the state of the filling of capillaries: in the place of the advanced cellulite the tissue is poorly supplied with blood), electric bioimpedance (determines content of the fatty tissue and water in the body). However in the diagnosis of cellulite, computed axial tomography, magnetic resonance and ultrasonography turned out to be extremely useful 18.
But neither the computed axial tomography nor the magnetic resonance can be universally used on account of their costs and in the case of the computed axial tomography as for the radiation exposure to X-ray. Therefore, ultrasonography is more cost effective and more available and more objective than the palpable scale. The research on the evaluation of cellulite is performed using ultrasound scanners 18.
Classical ultrasonography assesses such parameters as fatness of the corium (the dermis. the deep inner layer of the skin, beneath the epidermis, containing connective tissue, blood vessels, and fat) and of the subcutaneous layer, echogenicity of both structures, and the border between the corium and subcutaneous layer 34. In the high frequency ultrasonography it is possible to assess the following parameters: the fatness of the cuticle and corium, presence of swellings, echogenicity of corium and what is most essential, the advanced process of forming the root of the corium in the subcutaneous layer 35.
Cellulite Treatment
Despite high incidence rate of cellulite and a wide range of products and many treatment methods are available to treat cellulite such as massage 36, low-level light energy therapy from laser light 37, intense pulse light, radiofrequency 38, diode laser, infrared light, and ultrasound with and without mechanical massage as well as injectables and topicals 39, 40, 41, 42, 43, 44, 45, 46, 47 and subcision, both mechanical and thermal 48, 49.
There are very little scientific systematic review has been performed so far to evaluate the effectiveness of the available treatment options for cellulite. Many methods for reducing cellulite involve cosmetic procedures, cosmetic surgery, pharmacology and surgical procedures 50.
There are many cellulite treatments available but few actually create a reduction in the visible appearance of cellulite. A number of these treatments were reviewed by Khan et al. 51 including massage; a noninvasive suction-assisted massage technique; and topical agents such as xanthine, retinols, and other botanicals 15, 52, 53, 54, 55. Mesotherapy, a modality that entails injecting substances into the subcutaneous fat layer, is another treatment of cellulite. Two of the most common agents purported to dissolve fat include phosphatidylcholine and sodium deoxycholate 13. The efficacy and safety of mesotherapy remains controversial and unproven. A July 2008 position statement from the American Society of Plastic Surgeons stated that “low levels of validity and quality of the literature does not allow [American Society of Plastic Surgeons] to support a recommendation for the use of mesotherapy/injection lipolysis for fat reduction” 56. Other modalities such as noninvasive dual-wavelength laser/suction devices; low-energy diode laser, contact cooling, suction, and massage devices; and infrared, bipolar radiofrequency, and suction with mechanical massage devices are available and show some small improvements in the visible appearance of cellulite, but no rating scales were used in any of these studies 57, 58. DiBernardo 59 utilized a 1440-nm pulsed laser to treat cellulite. It is an invasive treatment that works by breaking down some of the connective tissue septa responsible for the majority and greater severity of the dermal dimpling seen in cellulite, increasing the thickness of the dermis as well as its elasticity, reducing subcutaneous fat, and improving circulation and reducing general lymphatic congestion 59. The system showed promise but was an invasive treatment, and one session could cost $5000 to $7000 for bilateral areas and another $2500 for each additional area 60. Burns 61 expressed that the short-term results showed promise in reducing the appearance of cellulite. Noninvasive ultrasound 62, 63 as well as extracorporeal shock wave therapy 64, 65 also has shown some improvement in the firmness of collagen but generally not in the appearance of cellulite.
Most of the evaluated studies, including laser- and light-based methods, radio-frequency and others had important methodological flaws; some did not use cellulite severity as an endpoint or did not provide sufficient statistical analyses. Of the 67 studies analyzed in this review 50, only 19 were placebo-controlled studies with randomization. Some evidence for potential benefit was only seen for acoustic wave therapy and the 1440 nm Nd:YAG minimally invasive laser 50. However, the review authors concluded that there is no clear evidence of good efficacy (the ability to produce a desired or intended result) could be identified in any of the evaluated cellulite treatments.
How To Get Rid of Cellulite At Home
The basis of home remedy primarily involves the prevention and also elimination of risk factors (see causes of cellulite above). A preventive program containing information about factors affecting the development of cellulite and methods of its elimination (e.g. quit smoking, eat less sodium, healthy eating, etc). Because by preventing the development of the advanced stage of the cellulite, which is most resistant to therapy, you can have a better outcome for the home remedy.
You should be aware that home remedy will not eliminate cellulite completely and it will only slightly reduce the cellulite area and therefore will affect the temporary improvement in the appearance of the skin.
The basis of home therapy 18 is:
- Weight loss
If you’re overweight or obese, weight loss — through healthy eating and regular exercise — might improve the appearance of the dimpled skin. Weight loss and exercise won’t make it go away completely.
- Application of cosmeceutics, containing active ingredients:
Improving the tightness of blood and lymphatic vessels, e.g. flavonoids, antioxidants, saponins, tannins, which also help eliminate unnecessary products of metabolism. The above-mentioned group of substances appear in extracts from arnica and seeds and leaves of the horse chestnut.
Intake of compounds of plant origin increases the process of lipolysis, but suppresses lipogenesis such as caffeine, extracts from guarana, Garcinia gummigutta, theophylline, xanthine (come from coffee, the green tea and the Paraguayan tea).
Toning and moistening substances applied in anti-cellulite cosmetology: hyaluronic acid, vitamin A and E, urea, plant extracts, amino acids and hydroxyacids.
- Supplementation – is based on products containing caffeine and vitamin B1 (Thiamin), B5 (Pantothenic acid), B9 (Folate or Folic Acid) and B12 (Cobalamin).
- Physical activity and healthy diet.
Recently, an oral supplementation with polyphenol-rich chokeberry juice taken over a period of 90 days improved cellulite with a marked reduction in the subcutaneous tissue thickness and edema 66.
How to Get Rid of Cellulite Fast
The most popular treatments in the cosmetic and cosmetic surgery areas applied to reduce the cellulite are:
Cosmetic Procedures
- Cellulite creams. Creams that contain a variety of ingredients, such as vitamins, minerals, herbal extracts and antioxidants, are often marketed as the cure for cellulite. But no studies show that these creams alone offer improvement. Some of these products contain ingredients that can cause skin reactions or rashes.
- Lymphatic drainage – massage. works positively on lymphatic vessels, eliminates swellings, is also beneficial for deep layers of the skin 18.
- Endermology (also referred to as Lipomassage) – apparatus massage (massage therapy by vacuum suction). Endermologie was originally developed during the 1980s in France by Louis-Paul Guitay to treat burns and loosen scar tissue. However while using the procedure it became increasingly evident that it also improved the appearance of cellulite. In Endermology, subcutaneous tissue (dermis and some fat) is kneaded into a rolling device while negative pressure holds the skin in the rollers. The effect of endermology is to increase oxidation of tissues, improve skin elasticity, hasten the apoptosis of fat cells, however does not strengthen the corium 67, 68, 69. It may reduce bulk slightly but temporarily. It may smoothen uneven contour with cellulite, but again, it is a temporary effect. Most patients undergo Endermologie treatment two or three times per week for a month, and then may continue with once per month, or less, to maintain their result.
- 1440-nm Nd:YAG Wavelength Laser with side-firing fiber
In this study to treat cellulite using a 1440-nm YAG wavelength laser with side-firing fiber, DiBernardo et al. 5 treated 57 patients with a single, 3-step, minimally invasive laser treatment using a 1440-nm Nd:YAG laser, side-firing fiber and temperature-sensing cannula 5. The results were at 6 months, the average improvement score was 1.7 for dimples and 1.1 for contour irregularities. At 12 months, the average improvement score was 1.4 for dimples and 1.0 for contour irregularities. The average satisfaction score for the physician was 5.6 and the patient was 5.3 on a 6-point scale 5.
- Velasmooth™ is at present an effective appliance in the treatment of cellulite in a non-invasive method, in which three energy sources are used: infrared, bipolar electricity of high frequency (RF), the impulse suction and massage. Their cooperation considerably increases the effect in comparison to results obtained when using single energy sources. All three energies are being administered to the tissue simultaneously, using one therapeutic head. The treatment comprises 10-12 sessions which are taken twice a week for 5-6 weeks 69. In a study by Sadick and Mulholland on VelaSmooth 70, 35 female subjects with cellulite and/or skin irregularities on the thighs and/or buttocks were treated with the VelaSmooth device. Patients received from eight to 16 treatments twice weekly. All patients maintained their normal lifestyle and diet and fluid consumption. The circumference of the right and left medial thighs was measured at both baseline and approximately 4 weeks after the last treatment. All study patients showed some level of reduction in thigh circumference after 8 weeks of treatment; indeed, 70% of all patients showed such a reduction after 4 weeks of treatment. The mean decrease in circumference was 0.8 inches. Some patients demonstrated reductions of more than 2 inches. Also, 100% of all patients showed some level of improvement in skin texture and cellulite. There were minimal complications associated with treatment 70.
In a more recnt study on a new way method of getting rid of cellulite by combining radiofrequency and ultrasound device 71. Kapoor et al. treated two hundred seventy-five (235 women and 40 men) patients. Each patient received 3 treatment sessions, each session comprising Ultrasound and Radio-Frequency treatments, at two-week intervals. Some received treatment for the abdomen, some for the thighs and some for both. Efficacy was assessed accordingly by measuring changes in abdominal circumference, thigh circumference and appearance of cellulite. Any adverse effect was noted. The results just after 4 weeks after 3rd session was significant amongst all the groups, showing that most patients showed improvement in abdominal and/or thigh circumferences. No significant adverse effects were noted during or after the treatment. The study authors concluded that a combination of alternating hot and cold module Ultrasound and Radiofrequency technologies is a safe and effective modality for lipolysis and to treat skin laxity and cellulite 71.
- Triactive™ – three various methods are being used for the treatment: the diode laser, cryotherapy, deep massage and lymphatic drainage. The diode laser stimulates the reconstruction of vessels in the subcutaneous layer, cryotherapy reduces swelling and lymphatic drainage and massage stimulate blocked circulation of lymph expelling water and unnecessary products of metabolism from the organism. Series are usually applied in about 10-15 treatments 1-2 times a week 69.
- SmoothShapes™ – the device is using three technologies – connecting the laser, biostimulating light, massage with rolls and vacuum 69.
- Alma Accent™ RF system – the device is a source of high frequency waves for collagen remodelling, improving texture of the skin and cellulite reduction. It uses two types of radio frequency: unipolar and bipolar. By proper applying different heads for heating (of heat treatment), appropriate layers of the skin and the subcutaneous layer are treated 18.
- InfraRed Light – trigger thermogenesis after which the reduction in fat cells takes place 18.
- Ultrasound. This noninvasive procedure uses sound waves to reduce targeted fat in the abdomen and thighs. Results take two or three months, and include an improvement in the appearance of cellulite.
- Ultrasonic Band Device. In a novel and yet to be named device, the device consisted of a 10.16 cm belt with a layer of nonslip material wrapped around the belt. The belt was attached to a mechanical oscillator that move the dermis at that length of approximately 2 cm at approximately 1000 strokes per minute 72. Each participant was treated for a total treatment time of 18 to 24 minutes. The total treatment area included the top of the iliac crest to just above the top of the popliteal space. The width of the belt (10.16 cm) was equal to 1 individual treatment area. Each individual treatment area was treated for 2 minutes. First the buttocks and bilateral thighs were treated, followed by the right lateral thigh and the left lateral thigh. The belt was moved progressively down the total treatment area until all individual treatment areas were addressed. The average participant had 3 to 4 bilateral thigh and buttocks treatment areas and 3 to 4 lateral treatment areas on both the left and right sides of the body. Roubal et al. study enrolled 43 participants (age range, 21–67 years; average age, 37.6 years; weight range, 51–97 kg; mean weight, 64.95 kg) who resided in the Midwestern United States, who were interested in reducing their cellulite, and were willing to commit to treatment 2 times weekly for the duration of the 8-week study. Fourteen percent (6/43) of participants were smokers. However the results of band device was less convincing, of the 2 blinded board-certified plastic surgeons, one physician rated all participants in category III as significantly improved and rated the other categories as marginally insignificantly improved; the second physician rated all categories as marginally insignificantly improved 72.
The Medical and Surgical Procedures as treatment for the cellulite:
- Liposuction – Some people turn to liposuction as a treatment for cellulite. During liposuction, a surgeon inserts a narrow tube under your skin through tiny incisions and suctions out local excess of fat cells. Though liposuction can shape the body, it won’t remove cellulite, and it might worsen the appearance of cellulite. Laser-assisted liposuction — a newer, less invasive form of this treatment that destroys fat cells while tightening the skin — might be more effective for cellulite. More study is needed. Liposuction can be made with the help of lasers and apparatuses producing airwaves. In medicine, applying high frequency waves causes effects of the overheating of tissues. Modern apparatuses are equipped with the cooling system that prevents burns of the skin (cryogenic liquid) and exchangeable treatment heads. The treatment consists in the proper dosage of airwaves, of which the energy is turned into the central heating, stimulating cells to produce collagen; waves work on the corium and the subcutaneous layer. The treatment improves firmness and density of the skin 69.
Liposuction has not been shown to be effective in the treatment of cellulite and in fact may increase the appearance of cellulite 32, 73.
- Mesotherapy – This procedure involves injecting a solution, which might contain aminophylline, healing agents (silica, caffeine, tiratricol), hormones, enzymes, herbal extracts, vitamins and minerals — under the skin. This treatment can cause several unwanted effects, including infection, rashes, and bumpy or uneven skin contours. It assists the lipolysis which reduces cellulite, but it does not directly affect the fat tissue causing cellulite 18.
In a recent clinical trial to assess the efficacy of intradermal mesotherapy in cellulite reduction involving 21 women who underwent a series of intradermal mesotherapy procedures 74. The the thigh circumference was measured; body mass index (BMI) and cellulite severity were assessed based on photographs using Nürnberger-Müller’s scale. The study showed intradermal mesotherapy reduced severity of cellulite. The surface area of serrated hypodermis-dermis junction and hypodermis thickness decreased significantly as compared to baseline. Cellulite reduction was also confirmed by palpation, decreased thigh circumference and the Nürnberger-Müller’s grade. There were no statistically significant changes in epidermis or dermis thickness, body weight and the BMI 74. The researchers concluded by saying intradermal mesotherapy is a simple, effective and safe treatment for getting rid of cellulite.
However, the efficacy and safety of mesotherapy remains controversial and unproven. A July 2008 position statement from the American Society of Plastic Surgeons stated that “low levels of validity and quality of the literature does not allow [American Society of Plastic Surgeons] to support a recommendation for the use of mesotherapy/injection lipolysis for fat reduction” 75. The American Society of Plastic Surgeons also stated that, “Currently, there is no known FDA-approved injectible solution or pharmaceutical preparation for mesotherapy or injection lipolysis. Thus, physicians who wish to perform this therapy for adipose reduction may be subject to some degree of liability as the FDA may review individual occurrences on a case-by-case basis for enforcement action.”
- Injection lipolysis – lipolysis can be applied to supplement liposuction, but cannot replace it; the treatment consists in the reduction in the local fatty tissue with the injection; phosphatidylcholine has most often been applied and sodium deoxycholate, but both are registered for this purpose. At present for the injection lipolysis surgery, one uses a new injection technique – intralipotherapy – which was registered in 2007 and popularised by Professor Motolese as Aqualyx preparation. Gel is also applicable in the ‘no-needle’ mesotherapy against defluvium – Dermaheal HR. Professor Maurizio Ceccarelli is using vitamin C and iron for the lipolysis which causes the apoptosis of fat cells 18.
- Cryolipolysis consists in exploiting cryotherapy and is applied for the reduction of the fatty tissue.This noninvasive procedure approved by the Food and Drug Administration shows promise in improving the appearance of cellulite. It removes abdominal fat and fat along the sides of the body by freezing the lipids in fat cells. It can take three treatments to dissolve an inch of fat and three or four months to see improvement. Under the influence of the low temperature, cell membranes of adipocytes are yielding to injury. Next, lipids undergo crystallization, what in the end leads to their apoptosis. Lipids from adipocytes are consumed by macrophages. During one treatment not always we can destroy all cells – treatment performed by dermatologists and surgeons 76.
- Carboxytherapy. Carbon dioxide therapy, better known as carboxytherapy, relates to percutaneous infusion of medical carbon dioxide in the treatment of localized fat 77. In a pilot study involving ten women (average age 35 years and body mass index (BMI) of 25.5 kg/m2) who received eight treatment sessions, with an interval of 7 days between sessions. At each selected points, 80 mL of CO2 gas with a flow rate of 80 mL/min was infused. The needle was positioned at 45° (inferior angle), and a subcutaneous puncture was made with a depth of ~10 mm. After the treatment, there was a significant reduction of the cellulite from degree III to degree II, and this improvement had correlation with the improvement in the organization of the fibrous lines and the disposal of adipose tissue lines of the treated regions observed through the panoramic ultrasound images diagnosis 77.
Pharmacological therapy is also popular for improving the appearance of the skin with the cellulite.
- Gestagenic hormone replacement therapy.
- Methyloxantines stimulate lipolysis.
- Pentoxifylline corrects the microcirculation and is advantageous for the immunological system 3.
- The primary topical therapies include retinoids and methylxanthines. Retinoids are known to increase neocollagenesis and are thought to decrease fat herniation by creating a thicker dermis 78. A twice-daily application of 0.3 percent retinol cream has been shown to improve the appearance of cellulite after six months.
How to Get Rid of Cellulite on Legs and Thighs
In a small study using Monopolar Dielectric Radio-Frequency 79 on the hips, buttocks and thighs region of 9 women. The women received 10 sessions of monopolar dielectric transmission radio frequency treatment. The researchers found that the application of Monopolar Dielectric Radio-Frequency seems to be effective in reducing not only the thickness of cellulite (panniculus adiposus), but also the circumference of the gluteal (buttocks) and posterior (behind) the thigh areas 79.
Summary on Cellulite Treatment
Currently there are no truly effective treatments for cellulite and no effective method of getting rid of cellulite permanently 1. Despite the lack of evidence to support efficacy, treatment options continue to proliferate. Treatment modalities can be divided into four main categories: attenuation of aggravating factors, physical and mechanical methods, pharmacological agents and laser. However, good effects, though short lived, can be obtained by using a combination of cellulite treatments. For example, cellulite treatment most often involve treatments using the cosmetic procedures, connected with applying cosmeceuticals and combining that with an increased physical activity and healthy diet. A special note for the beneficial effect of massage should be mentioned, and more precisely the fact that exerted pressure on adipocytes blocks their diversification, which makes the accumulation of fatty tissue impossible 80. Gentle massage with elements of aromatherapy is peculiarly recommended for women, since added oils not only work favourably on the state of the skin, but also improve the psychological condition. Although they will not get rid of the cellulite permanently, they will improve the general state of the skin, and hence improve self-image and wellbeing.
Tips for avoiding cellulite include:
- Eating a healthy diet rich in fruits, vegetables, and fiber
- Staying hydrated by drinking plenty of fluids
- Exercising regularly to keep muscles toned and bones strong
- Maintaining a healthy weight (no yo-yo dieting)
- Reduce salt in your diet
- Not smoking
- Avram MM. Cellulite: a review of its physiology and treatment. Journal of Cosmetics and Laser Therapy. 2004;6:181–185. https://www.ncbi.nlm.nih.gov/pubmed/16020201[↩][↩]
- Roubal PJ, Busuito MJ, Freeman DC, Placzek JD. Cutis. 2016 Dec;98(6):393-398. A noninvasive mechanical treatment to reduce the visible appearance of cellulite. https://www.ncbi.nlm.nih.gov/pubmed/28099534[↩]
- Haneke E. Cellulit – fakty i mity. Dermatologia Estetyczna. 2006;3:132–138.[↩][↩]
- Khan MH, Victor F, Rao B, et al. Treatment of cellulite: part I. pathophysiology. J Am Acad Dermatol. 2010;62:361-370, quiz 371-372.[↩][↩][↩][↩][↩][↩][↩]
- DiBernardo BE, Sasaki GH, Katz BE, Hunstad JP, Petti C, Burns AJ. A Multicenter Study for Cellulite Treatment Using a 1440-nm Nd:YAG Wavelength Laser with Side-Firing Fiber. Aesthetic Surgery Journal. 2016;36(3):335-343. doi:10.1093/asj/sjv203. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5127477/[↩][↩][↩][↩]
- DiBernardo BE. Treatment of cellulite using a 1440-nm pulsed laser with one-year follow-up. Aesthet Surg J. 2011;313:328-341. https://www.ncbi.nlm.nih.gov/pubmed/21385743[↩]
- Escoffier C, de Rigal J, Rochefort A, Vasselet R, Lévêque JL, Agache PG. Age-related mechanical properties of human skin: an in vivo study. J Invest Dermatol. 1989;933:353-357. https://www.ncbi.nlm.nih.gov/pubmed/2768836[↩]
- Piérard GE, Nizet JL, Piérard-Franchimont C. Am J Dermatopathol. 2000 Feb;22(1):34-7. Cellulite: from standing fat herniation to hypodermal stretch marks. https://www.ncbi.nlm.nih.gov/pubmed/10698214[↩][↩]
- Wikipedia. Subcutaneous tissue. https://en.wikipedia.org/wiki/Subcutaneous_tissue[↩]
- Ciupińska M, Noszczyk M. Kosmetologia pielęgnacyjna i lekarska. Warszawa: Wydawnictwo Lekarskie PZWL; 2010. Pielęgnacja ciała. Częste problemy estetyczne i zdrowotne sylwetki i skóry ciała; pp. 189–209.[↩][↩][↩]
- Pura-Rynasiewicz A. Dermatologia i Uroda. Wiosna-Lato; 2010. Cellulit – choroba czy defekt kosmetyczny? pp. 3–4.[↩][↩][↩]
- Emanuele E. Clin Dermatol. 2013 Nov-Dec;31(6):725-30. doi: 10.1016/j.clindermatol.2013.05.009. Cellulite: advances in treatment: facts and controversies. https://www.ncbi.nlm.nih.gov/pubmed/24160277?dopt=Abstract[↩]
- Roubal PJ, Busuito MJ, Freeman DC, Placzek JD. Cutis. 2016 Dec;98(6):393-398. A noninvasive mechanical treatment to reduce the visible appearance of cellulite. http://www.mdedge.com/cutis/article/119124/aesthetic-dermatology/noninvasive-mechanical-treatment-reduce-visible[↩][↩]
- Querleux B, Cornillon C, Jolivet O, et al. Anatomy and physiology of subcutaneous adipose tissue by in vivo magnetic resonance imaging and spectroscopy: relationships with sex and presence of cellulite. Skin Res Technol. 2002;8:118-124.[↩][↩]
- Rawlings A. Cellulite and its treatment. Int J Cos Sci. 2006;28:175-190.[↩][↩]
- Rosenbaum M, Prieto V, Hellmer J, et al. An exploratory investigation of the morphology and biochemistry of cellulite. Plast Reconstr Surg. 1998;101:1934-1939.[↩]
- Rossi AB, Vergnanini AL. Cellulite: a review. J Eur Acad Dermatol Venereol. 2000;14:251-262.[↩][↩]
- Leszko M. Cellulite in menopause. Przegla̜d Menopauzalny = Menopause Review. 2014;13(5):298-304. doi:10.5114/pm.2014.46472. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4520379/[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Smalls LK, Hicks M, Passeretti D, et al. Effect of weight loss on cellulite: gynoid lypodystrophy. Plast Reconstr Surg. 2006;118:510-516.[↩]
- Nürnberger F, Müller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol. 1978;4:221-229.[↩]
- Woźniak M, Zegarska B, Kaczmarek-Skamira E. Cellulit (III). Patogeneza. Dermatologia Estetyczna. 2011;3:149–150.[↩][↩]
- Wojnowska D, Juszkiewicz-Borowiec M, Chodorowska G. Wpływ menopauzy na starzenie się skóry. Post Dermatol Alergol. 2006;3:149–156.[↩]
- Skałba P. Receptory, hormony płciowe, leki stosowane w hormonalnej terapii. In: W: Skałba P, editor. Hormonalna terapia zastępcza. Wyd. II. Warszawa: Wydawnictwo Lekarskie PZWL; 2005. pp. 88–50.[↩][↩]
- Adipose tissue. Pathophysiology, distribution, sex differences and the role in inflammation and cancerogenesis. Siemińska L. Endokrynol Pol. 2007 Jul-Aug; 58(4):330-42. https://www.ncbi.nlm.nih.gov/pubmed/18058725/[↩][↩]
- Martini MC. Warszawa: Wydawnictwo Lekarskie PZWL; 2007. Kosmetologia i farmakologia skóry; pp. 300–309.[↩][↩][↩]
- Sobstyl M, Bednarek W, Tkaczuk-Włach J, et al. Objawy naczynioruchowe w menopauzie – diagnostyka i leczenie. Prz Menopauzalny. 2011;3:254–259.[↩]
- Warenik-Szymankiewicz A, Halerz-Nowakowska B. Diagnostyka w endokrynologii ginekologicznej. In: W: Pawlikowski M, editor. Zaburzenia hormonalne. Warszawa: Wydawnictwo Lekarskie PZWL; 2003. pp. 251–257.[↩]
- Pertyński T, Stachowiak G, Stetkiewicz T. Rola ginekologa w okresie pre-i okołomenopauzalnym. Prz Menopauzalny. 2007;2:251–254.[↩]
- Kos-Kudła B, Staszewicz P. Otyłość u kobiet w okresie około- i pomenopauzalnym. In: W: Skalba P, editor. Hormonalna terapia zastępcza. Wyd. II. Warszawa: Wydawnictwo Lekarskie PZWL; 2005. pp. 316–333[↩]
- Załęska-Żyłka I. Cellulit jako problem medyczny. Problemy Higieny i Epidemiologii. 2008;89:487–491.[↩]
- Ciupińska M, Noszczyk M. Kosmetologia pielęgnacyjna i lekarska. Warszawa: Wydawnictwo Lekarskie PZWL; 2010. Pielęgnacja ciała. Częste problemy estetyczne i zdrowotne sylwetki i skóry ciała; pp. 189–209[↩]
- Mirrashed F, Sharp JC, Krause V, et al. Pilot study of dermal and subcutaneous fat structures by MRI in individuals who differ in gender, BMI, and cellulite grading. Skin Res Technol. 2004;10:161-168.[↩][↩]
- A validated photonumeric cellulite severity scale. Hexsel DM, Dal’forno T, Hexsel CL. J Eur Acad Dermatol Venereol. 2009 May; 23(5):523-8. https://www.ncbi.nlm.nih.gov/pubmed/19220646/[↩][↩]
- Mlosek RK. Ultrasonograficzne badanie skóry. Ultrasonografia. 2011;47:58–62.[↩]
- Mlosek R, Dębowska R, Lewandowski M, et al. Zastosowanie badań ultrasonograficznych wysokiej częstotliwości w monitorowaniu terapii antycellulitowej – doświadczenia własne. Polish Journal of Cosmetology. 2008;11:283–294.[↩]
- Treatment of cellulite with LPG endermologie. Güleç AT. Int J Dermatol. 2009 Mar; 48(3):265-70. https://www.ncbi.nlm.nih.gov/pubmed/19261014/[↩]
- Sasaki GH. Scientific basis for the use of low level light energy on the treatment of cellulite. In: Cellulite. 2nd ed London, UK: Informa Healthcare; 2010:118-123.[↩]
- Clinical, laboratory, and MRI analysis of cellulite treatment with a unipolar radiofrequency device. Goldberg DJ, Fazeli A, Berlin AL. Dermatol Surg. 2008 Feb; 34(2):204-9; discussion 209. https://www.ncbi.nlm.nih.gov/pubmed/18093200/[↩]
- Alexiades-Armenakas M, Dover JS, Arndt KA. Unipolar radiofrequency treatment to improve the appearance of cellulite. J Cosmet Laser Ther. 2008;103:148-153. https://www.ncbi.nlm.nih.gov/pubmed/18788033[↩]
- Alster TS, Tanzi EL. Cellulite treatment using a novel combination radiofrequency, infrared light, and mechanical tissue manipulation device. J Cosmet Laser Ther. 2005;72:81-85. https://www.ncbi.nlm.nih.gov/pubmed/16537213[↩]
- Gold MH, Khatri KA, Hails K, Weiss RA, Fournier N. Reduction in thigh circumference and improvement in the appearance of cellulite with dual-wavelength, low-level laser energy and massage. J Cosmet Laser Ther. 2011;131:13-20. https://www.ncbi.nlm.nih.gov/pubmed/21275531[↩]
- Lach E. Reduction of subcutaneous fat and improvement in cellulite appearance by dual-wavelength, low-level laser energy combined with vacuum and massage. J Cosmet Laser Ther. 2008;104:202-209. https://www.ncbi.nlm.nih.gov/pubmed/19093288[↩]
- Nootheti PK, Magpantay A, Yosowitz G, Calderon S, Goldman MP. A single center, randomized, comparative, prospective clinical study to determine the efficacy of the VelaSmooth system versus the Triactive system for the treatment of cellulite. Lasers Surg Med. 2006;3810:908-912. https://www.ncbi.nlm.nih.gov/pubmed/17163477[↩]
- Sadick NS, Mulholland RS. A prospective clinical study to evaluate the efficacy and safety of cellulite treatment using the combination of optical and RF energies for subcutaneous tissue heating. J Cosmet Laser Ther. 2004;64:187-190. https://www.ncbi.nlm.nih.gov/pubmed/16020202[↩]
- Trelles MA, Mordon SR. Adipocyte membrane lysis observed after cellulite treatment is performed with radiofrequency. Aesthetic Plast Surg. 2009;331:125-128. https://www.ncbi.nlm.nih.gov/pubmed/19037688[↩]
- Trelles MA, van der Lugt C, Mordon S, Ribé A, Al-Zarouni M. Histological findings in adipocytes when cellulite is treated with a variable-emission radiofrequency system. Lasers Med Sci. 2010;252:191-195. https://www.ncbi.nlm.nih.gov/pubmed/19322624[↩]
- Wanner M, Avram M. An evidence-based assessment of treatments for cellulite. J Drugs Dermatol. 2008;74:341-345. https://www.ncbi.nlm.nih.gov/pubmed/18459514[↩]
- Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Orentreich DS, Orentreich N. Dermatol Surg. 1995 Jun; 21(6):543-9. https://www.ncbi.nlm.nih.gov/pubmed/7773602/[↩]
- Subcision: a treatment for cellulite. Hexsel DM, Mazzuco R. Int J Dermatol. 2000 Jul; 39(7):539-44. https://www.ncbi.nlm.nih.gov/pubmed/10940122/[↩]
- Luebberding S, Krueger N, Sadick NS. Am J Clin Dermatol. 2015 Aug;16(4):243-56. doi: 10.1007/s40257-015-0129-5. Cellulite: an evidence-based review. https://www.ncbi.nlm.nih.gov/pubmed/25940753[↩][↩][↩]
- Khan M, Victor F, Rao B, et al. Treatment of cellulite, part II. advances and controversies. J Am Acad Dermatol. 2010;62:373-384.[↩]
- Collis N, Elliot L, Sharp C, et al. Cellulite treatment: a myth or reality: a prospective randomized, controlled trial of two therapies, endermologie and aminophylline cream. Plast Reconstr Surg. 1999;104:1110-1114.[↩]
- Adcock D, Paulsen S, Jabour K, et al. Analysis of the effects of deep mechanical massage in the porcine model. Plast Reconstr Surg. 2000;108:233-240.[↩]
- Güleç AT. Treatment of cellulite with LPG endermologie. Int J Dermatol. 2009;48:265-270.[↩]
- Piérard-Franchimont C, Piérard GE, Henry F, et al. A randomized, placebo-controlled trial of tropical retinol in the treatment of cellulite. Am J Clin Dermatol. 2000;1:369-374.[↩]
- ASPS guiding principles for mesotherapy/injection lipolysis. American Society of Plastic Surgeons website. https://www.plasticsurgery.org/Documents/medical-professionals/health-policy/guiding-principles/ASPS-Guiding-Principles-for-Mesotherapy-Injection-Lipolysis-7-08.pdf[↩]
- Kulick MI. Evaluation of a noninvasive, dual-wavelength laser-suction and massage device for the regional treatment of cellulite. Plast Reconstr Surg. 2010;125:1788-1796.[↩]
- Nootheti PK, Magpantay A, Yosowitz G, et al. A single center, randomized, comparative, prospective clinical study to determine the efficacy of the VelaSmooth system versus the TriActive system for the treatment of cellulite. Lasers Surg Med. 2006;38:908-912.[↩]
- DiBernardo BE. Treatment of cellulite using a 1440-nm pulsed laser with one-year follow up. Aesthet Surg J. 2011;31:328-341.[↩][↩]
- Johannes L. New laser aims to zap cellulite at the source. Wall Street Journal. July 3, 2012. https://www.wsj.com/articles/SB10001424052702303649504577496981754619546[↩]
- Burns AJ. Commentary on: treatment of cellulite using a 1440-nm pulsed laser with one-year follow up: preliminary report. Aesthet Surg J. 2011;31:342-343.[↩]
- Teitelbaum SA, Burns JL, Kubota J, et al. Noninvasive body contouring by focused ultrasound: safety efficacy of the contour I device in a multicenter, controlled, clinical study. Plast Reconstr Surg. 2007;120:779-789.[↩]
- Brown SA, Greenbaum L, Shtukmaster S, et al. Characterization of nonthermal focused ultrasound for noninvasive selective fat cell disruption (lysis): technical and preclinical assessment. Plast Reconstr Surg. 2009;124:92-101.[↩]
- Angehrn F, Kuhn C, Voss A. Can cellulite be treated with low energy extracorporeal shock wave therapy? Clin Interv Aging. 2007;2:623-630.[↩]
- Christ C, Brenke R, Sattler G, et al. Improvement in skin elasticity in the treatment of cellulite and connective tissue weakness by means of extracorporeal pulse activation therapy. Aesthet Surg J. 2008;28:538-544.[↩]
- Savikin K1, Menković N, Zdunić G, Pljevljakušić D, Spasić S, Kardum N, Konić-Ristić A. J Med Food. 2014 May;17(5):582-7. doi: 10.1089/jmf.2013.0102. Epub 2014 Jan 16. Dietary supplementation with polyphenol-rich chokeberry juice improves skin morphology in cellulite. https://www.ncbi.nlm.nih.gov/pubmed/24433076/[↩]
- Miękoś-Zydek B, Czyż P, Ograczyk A. Mezoterapia w dermatologii i dermatologii estetycznej. In: W: Adamski Z, Kaszuba A, editors. Dermatologia dla kosmetologów. Wrocław: Elsevier Urban & Partner; 2010. pp. 281–285.[↩]
- Wilk M, Dankowska S, Adamski Z. Gabinet kosmetyczny. In: W: Adamski Z, Kaszuba A, editors. Dermatologia dla kosmetologów. Wrocław: Elsevier Urban & Partner; 2010. pp. 424–429.[↩]
- Wassef C, Rao Babar K. The science of cellulite treatment and its long-term effectiveness. J Cosmet Laser Ther. 2012;14:50–58. https://www.ncbi.nlm.nih.gov/pubmed/22372471[↩][↩][↩][↩][↩]
- Sadick NS, Mulholland RS. J Cosmet Laser Ther. 2004 Dec;6(4):187-90. A prospective clinical study to evaluate the efficacy and safety of cellulite treatment using the combination of optical and RF energies for subcutaneous tissue heating. https://www.ncbi.nlm.nih.gov/pubmed/16020202[↩][↩]
- Kapoor R, Shome D, Ranjan A. J Cosmet Laser Ther. 2017 Mar 10:1-9. doi: 10.1080/14764172.2017.1303169. Use of a novel combined radiofrequency and ultrasound device for lipolysis, skin tightening and cellulite treatment. https://www.ncbi.nlm.nih.gov/pubmed/28281840[↩][↩]
- Roubal PJ, Busuito MJ, Freeman DC, Placzek JD. Cutis. 2016 Dec;98(6):393-398. A noninvasive mechanical treatment to reduce the visible appearance of cellulite.[↩][↩]
- Coleman WP. Liposuction. In: Coleman WP, Hanke CW, Alt TH, eds. Cosmetic Surgery of the Skin: Principles and Practice. Philadelphia, PA: BC Decker; 1991:213-238.[↩]
- Sylwia M, Krzysztof MR. J Cosmet Laser Ther. 2017 Jun 7:1-5. doi: 10.1080/14764172.2017.1334927. Efficacy of intradermal mesotherapy in cellulite reduction – Conventional and high-frequency ultrasound monitoring results. https://www.ncbi.nlm.nih.gov/pubmed/28590783[↩][↩]
- American Society of Plastic Surgeons. ASPS Guiding Principles for Mesotherapy/Injection Lipolysis. American Society of Plastic Surgeons website. https://www.plasticsurgery.org/Documents/medical-professionals/health-policy/guiding-principles/ASPS-Guiding-Principles-for-Mesotherapy-Injection-Lipolysis-7-08.pdf[↩]
- Hexsel D, Dal’Forno T, Hexsel C. A validated photonumeric cellulite severity scale. J Eur Acad Dermatol Venereol. 2009;23:523–528. https://www.ncbi.nlm.nih.gov/pubmed/19220646[↩]
- Pianez LR, Custódio FS, Guidi RM, de Freitas JN, Sant’Ana E. Effectiveness of carboxytherapy in the treatment of cellulite in healthy women: a pilot study. Clinical, Cosmetic and Investigational Dermatology. 2016;9:183-190. doi:10.2147/CCID.S102503. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5001663/[↩][↩]
- Christman MP, Belkin D, Geronemus RG, Brauer JA. J Drugs Dermatol. 2017 Jan 1;16(1):58-61. An Anatomical Approach to Evaluating and Treating Cellulite. https://www.ncbi.nlm.nih.gov/pubmed/28095534[↩]
- Albornoz-Cabello M, Ibáñez-Vera AJ, De la Cruz-Torres B. J Cosmet Laser Ther. 2017 Jul 5:1-5. doi: 10.1080/14764172.2017.1342041. Efficacy of monopolar dielectric transmission radio frequency in panniculus adiposus and cellulite reduction. https://www.ncbi.nlm.nih.gov/pubmed/28678582[↩][↩]
- Kasprzak W, Mańkowska A. Warszawa: Wydawnictwo Lekarskie PZWL; 2008. Fizykoterapia, medycyna uzdrowiskowa i SPA; pp. 332–339.[↩]





{kind=link}