
Contents
- What is hearing loss
- Hearing loss complications
- Overview of the ear
- Types of hearing loss
- Test your hearing questionnaire
- Hearing loss causes
- Hearing loss prevention
- Hearing loss signs and symptoms
- Hearing loss diagnosis
- Hearing loss treatment
What is hearing loss
Hearing loss or deafness can be temporary or permanent, partial or complete. Hearing loss often comes on gradually as you get older (presbycusis), but hearing loss can sometimes happen suddenly. You may also have other symptoms, such as earache, unusual noises in your ear (tinnitus) or a spinning sensation (vertigo).
It can be hard to tell if you’re losing your hearing. Other people may notice it before you do.
About 25 percent of people in the United States between the ages of 55 and 64 have some degree of hearing loss. For those older than 65, the number of people with some hearing loss is almost 1 in 2.
Early signs of hearing loss include:
- difficulty hearing other people clearly and misunderstanding what they say, especially in noisy places
- asking people to repeat themselves
- listening to music or watching TV with the volume higher than other people need
- difficulty hearing on the phone
- finding it hard to keep up with a conversation
- feeling tired or stressed from having to concentrate while listening
Aging and chronic exposure to loud noises are significant factors that contribute to hearing loss. Other factors, such as excessive earwax, can temporarily prevent your ears from conducting sounds as well as they should.
See your doctor if you notice any problems with your hearing so you can find out the cause and get advice on treatment.
If you have a sudden loss of hearing, particularly in one ear, seek immediate medical attention.
See your doctor if difficulty hearing is interfering with your daily life. Your hearing may have deteriorated if:
- You find that it’s harder to understand everything that’s said in conversation, especially when there’s background noise
- Sounds seem muffled
- You find yourself having to turn the volume higher when you listen to music, the radio or television
Sudden hearing loss in one ear
It’s not always easy to tell if you’ve lost hearing in one ear, as you may still be able to hear with your other ear.
Signs of a hearing problem in one ear include:
- your hearing is worse when sound comes from one side
- all sounds seem generally quieter than usual
- finding it hard to tell where sound is coming from
- difficulty ignoring background noise or telling different sounds apart
- finding speech unclear
- difficulty hearing in noisy places or over long distances
Hearing loss in one ear is often caused by sound temporarily being unable to pass through the ear – for example, because of earwax or an ear infection.
Hearing loss in children
Your child may have a problem with their hearing if they:
- are slow to learn to talk, or aren’t clear when they speak
- don’t reply when you call them
- talk very loudly
- ask you to repeat yourself or respond inappropriately to questions
- turn up the volume of the TV very high
See your doctor if you’re worried about your child’s hearing.
Hearing loss in children can be caused by a build-up of fluid in the ear (glue ear or middle ear effusion or otitis media), which tends to get better over time and can be treated.
Hearing loss in babies
Babies have a hearing check in the first few weeks after birth, but speak to your health visitor or see your doctor if you think they might have difficulty hearing.
They may have a problem with their hearing if they:
- aren’t startled by loud noises
- seem to hear some sounds but not others
- notice you when they see you, but not when you call their name
- don’t turn towards voices by four months of age
- haven’t started to say any recognizable words by around 15 months
Babies Reaction to Sounds Checklist
This list give pointers about what to look for as your baby grows to check if he/she can hear. Babies differ widely in what they can do at any given age. The ages presented here are an approximate guide only.
- Shortly after birth – a baby: Is startled by a sudden loud noise such as a hand clap or a door slamming. Blinks or opens eyes widely to such sounds or stops sucking or starts to cry.
- 1 month – a baby: Starts to notice sudden prolonged sounds like the noise of a vacuum cleaner and may turn towards the noise. Pauses and listens to the noises when they begin.
- 4 months – a baby: Quietens or smiles to the sounds of familiar voice even when unable to see speaker and turns eyes or head towards voice. Shows excitement at sounds (e.g. voices, footsteps etc).
- 7 months – a baby: Turns immediately to familiar voice across the room or to very quiet noises made on each side (if not too occupied with other things).
- 9 months – a baby: Listens attentively to familiar everyday sounds and searches for very quiet sounds made out of sight.
- 12 months – a baby: Shows some response to own name. May also respond to expressions like ‘no’ and ‘bye bye’ even when any accompanying gesture cannot be seen.
If at any stage in the baby or child’s development you think he/she may have difficulties hearing, contact your family doctor.
Babies Making Sounds Checklist
Babies Making Sounds Checklist and Babies Reaction to Sounds Checklist give pointers about what to look for as your baby grows to check if he/she can hear. Babies do differ in what they can do at any given age. The ages presented here are approximate only.
- 4 months – a baby: Makes soft sounds when awake. Gurgles and coos.
- 6 months – a baby: Makes laughter-like sounds. Starts to make sing-song vowel sounds (e.g., a-a, muh, goo, der, aroo, adah).
- 9 months – a baby: Makes sounds to communicate in friendliness or annoyance. Babbles (e.g., ‘dada da’, ‘ma ma ma’, ‘ba ba ba’). Shows pleasure in babbling loudly and tunefully. Starts to imitate other sounds like coughing or smacking lips.
- 12 months – a baby: Babbles loudly, often in a conversational-type rhythm. May start to use one or two recognizable words.
- 15 months – a baby: Makes lots of speech-like sounds. Uses 2-6 recognizable words meaningfully (e.g., ‘teddy’ when seeing or wanting the teddy bear).
- 18 months – a baby: Makes speech-like sounds with conversational-type rhythm when playing. Uses 6-20 recognizable words. Tries to join in nursery rhymes and songs.
- 24 months – a child: Uses 50 or more recognizable words appropriately. Puts 2 or more words together to make simple sentences (for example: more milk). Joins in nursery rhymes and songs. Talks to self during play (may be incomprehensible to others).
- 30 months – a child: Uses 200 or more recognisable words. Uses pronouns (e.g., I, me, you). Uses sentences but many will lack adult structure. Talks intelligibly to self during play. Asks questions. Says a few nursery rhymes.
- 36 months – a child: Has a large vocabulary intelligible to everyone.
Hearing loss complications
Hearing loss can have a significant effect on your quality of life. Among older adults with hearing loss, commonly reported problems include:
- Depression
- Anxiety
- An often false sense that others are angry with you
Unfortunately, most people affected by hearing loss live with these difficulties for years before seeking treatment — or never seek treatment at all. This may also cause lasting problems for those who love you, if you try to cope by denying your hearing loss or withdrawing from social interactions.
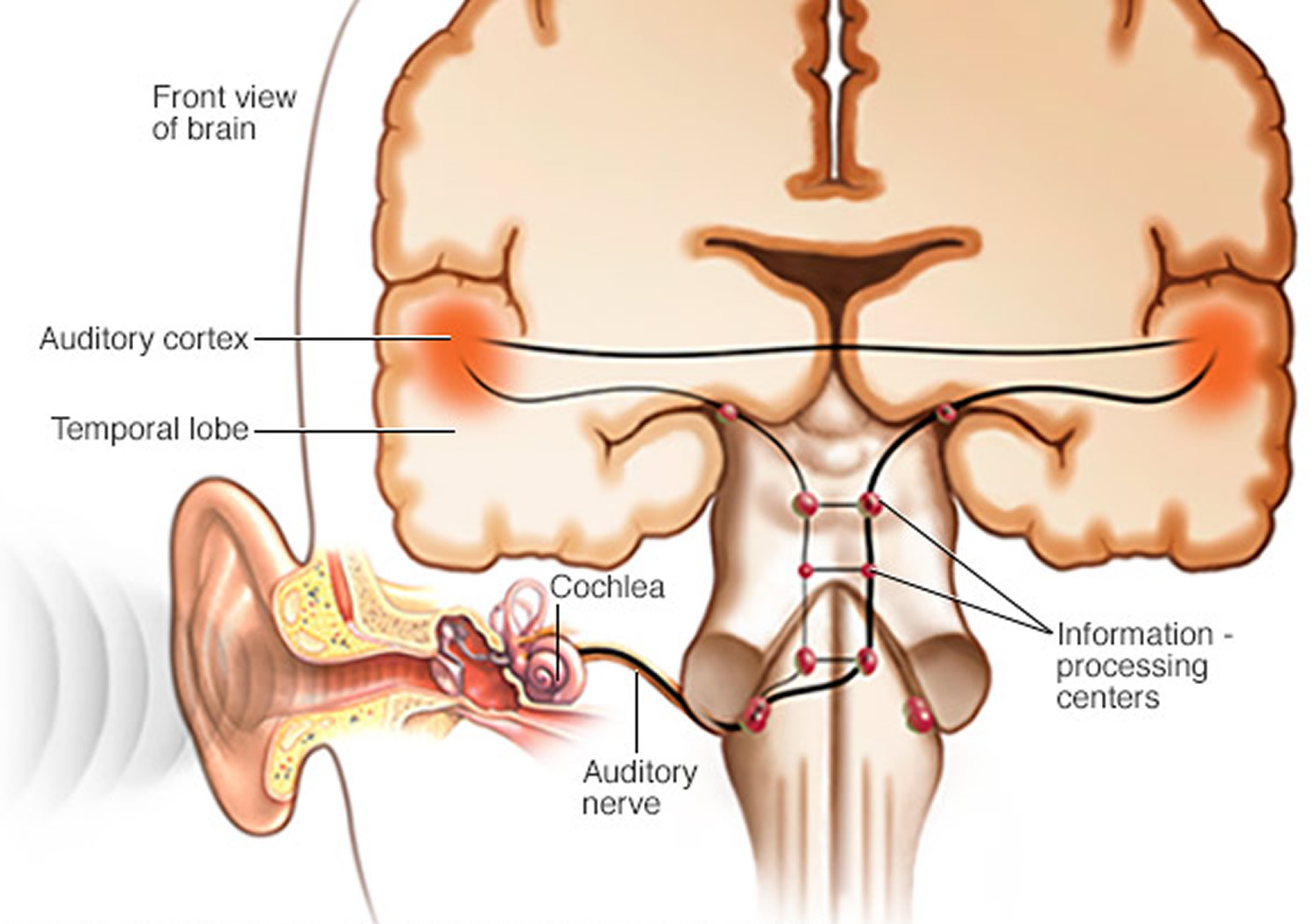
Overview of the ear
The ear is the sense organ that enables us to hear. Hearing can be defined as the perception of sound energy via the brain and central nervous system. Hearing consists of two components: identification of sounds (what the sound is) and localization of those sounds (where the sounds are coming from). The ear is divided into three main parts – the outer ear, the middle ear, and the inner ear (see Figures 1 to 5). The inner ear is filled with fluid (Figures 4 and 5). The inner ear also contains the receptors for sound which convert fluid motion into electrical signals known as action potentials that are sent to the brain to enable sound perception. The airborne sound waves must therefore be channelled toward and transferred into the inner ear for hearing to occur. The role of the outer and middle ear is to transmit sound to the inner ear (Figures 1 to 3). They also help compensate for the loss in sound energy that naturally occurs when the sound waves pass from air into water by amplifying the sound energy during the process of sound transmission. In addition to converting sound waves into nerve action potentials, the inner ear is also responsible for the sense of equilibrium, which relates to our general abilities for balance and coordination (Figure 4).
Figure 1. Ear structure
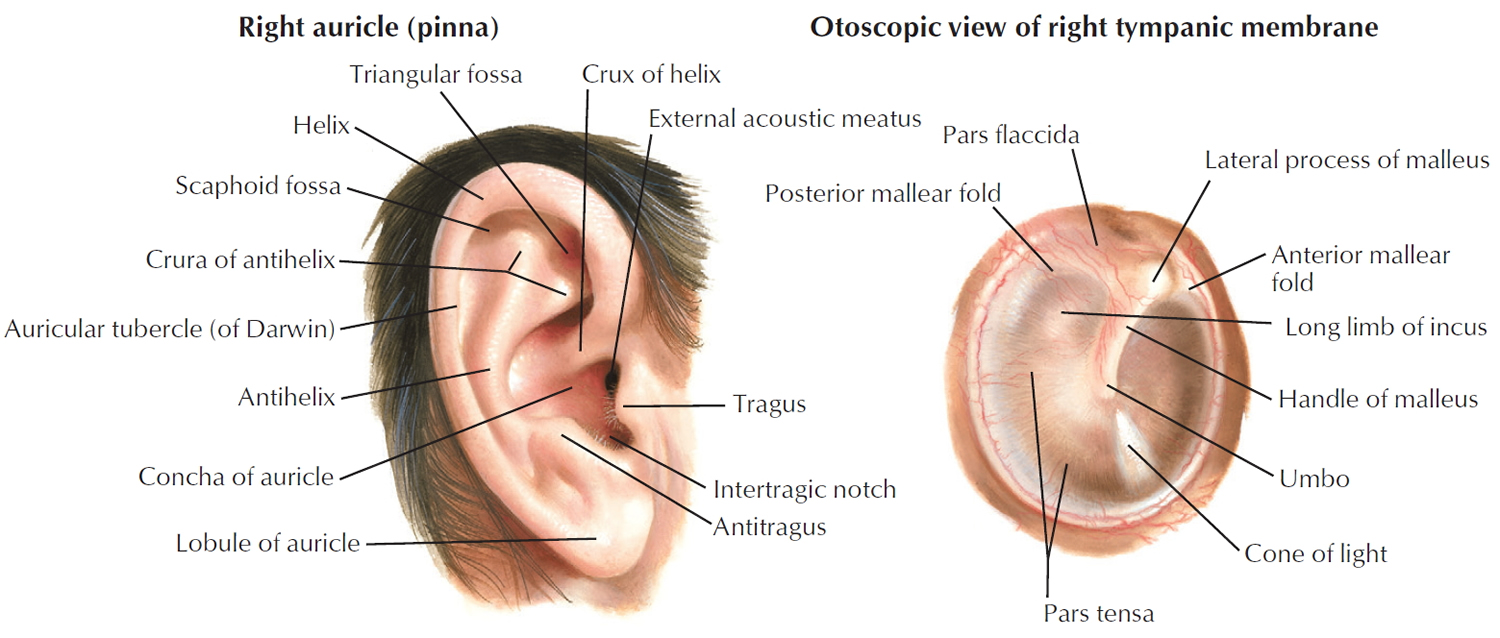
Figure 2. Ear anatomy

Figure 3. Middle ear and auditory ossicles
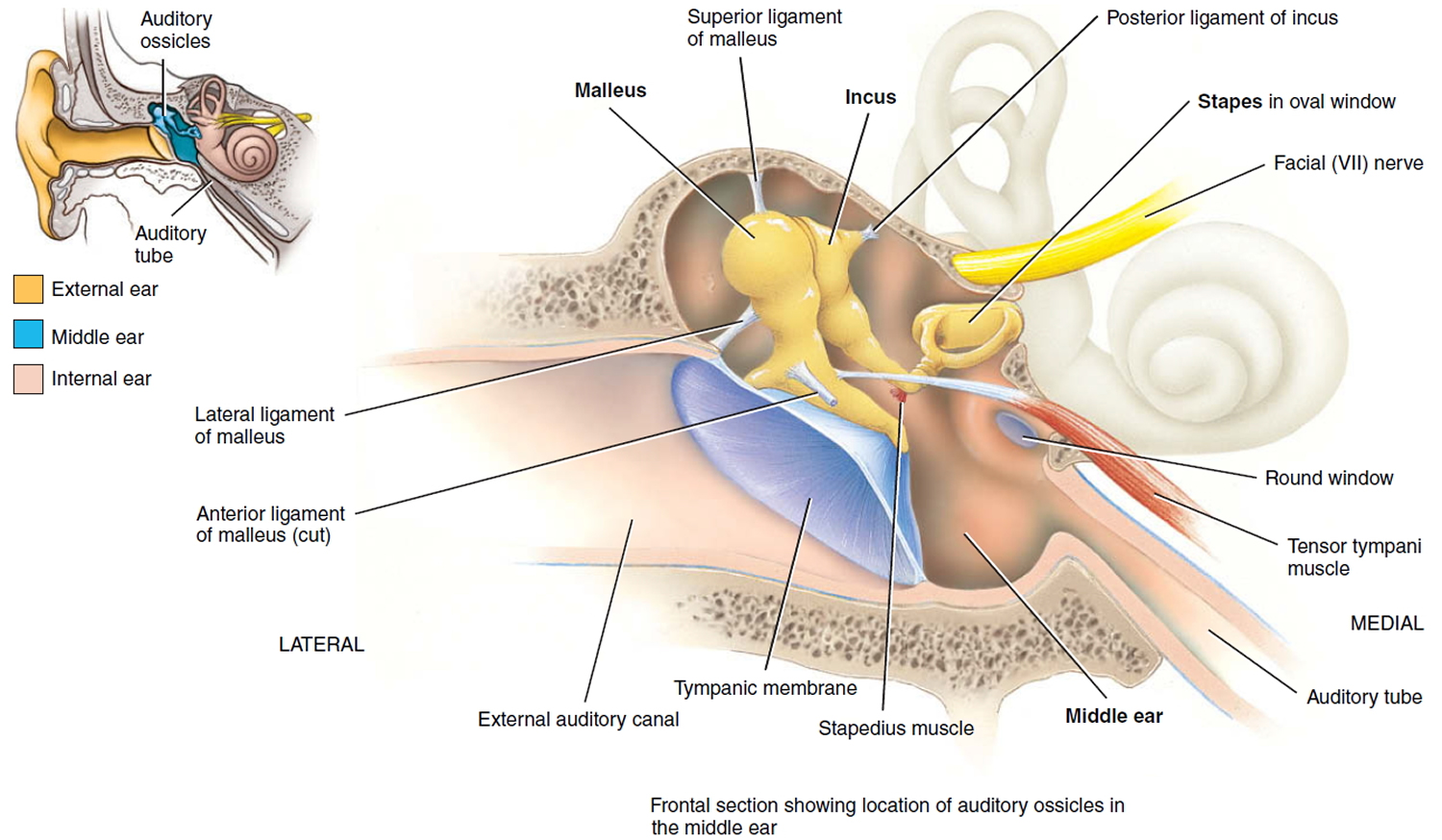
Figure 4. Parts of the inner ear
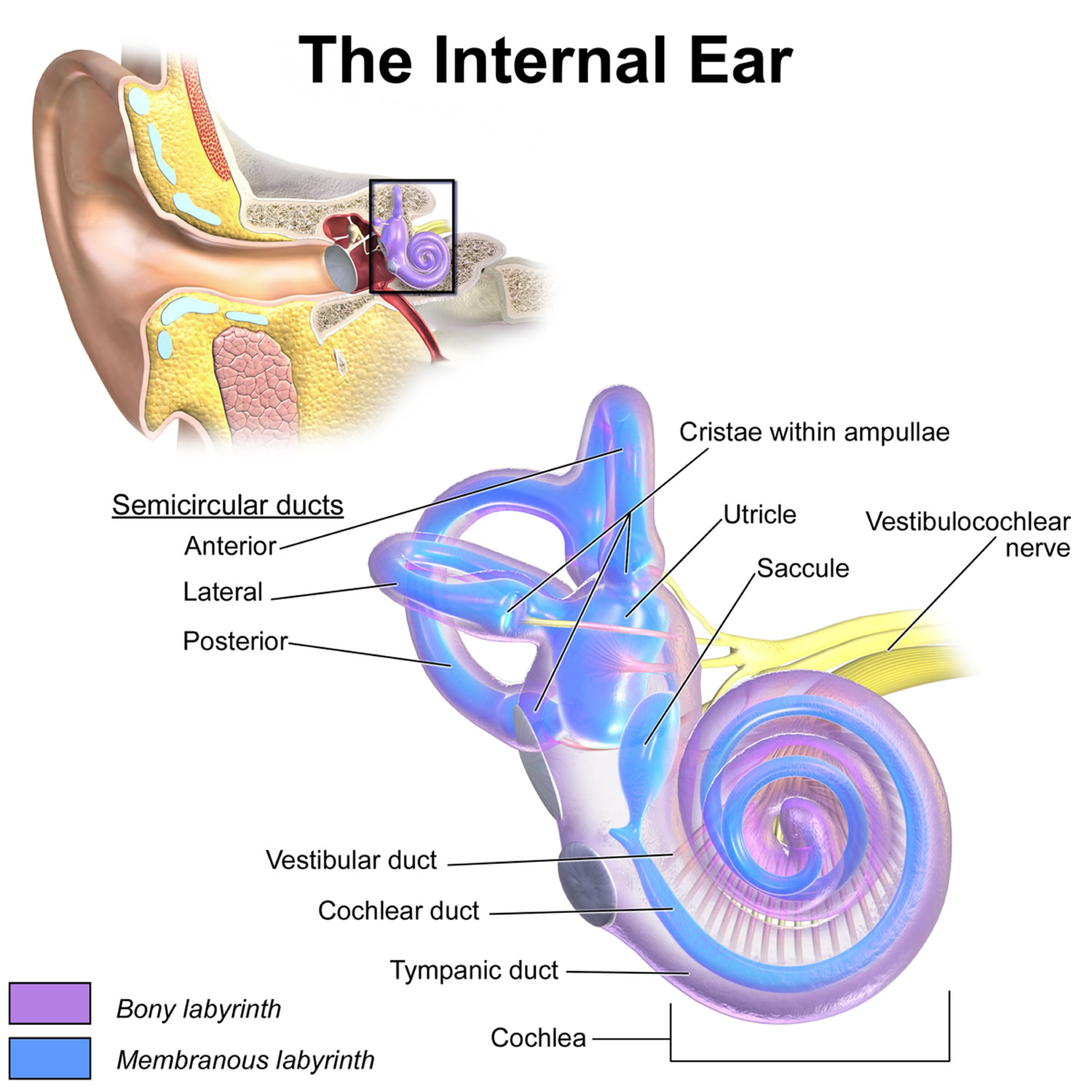
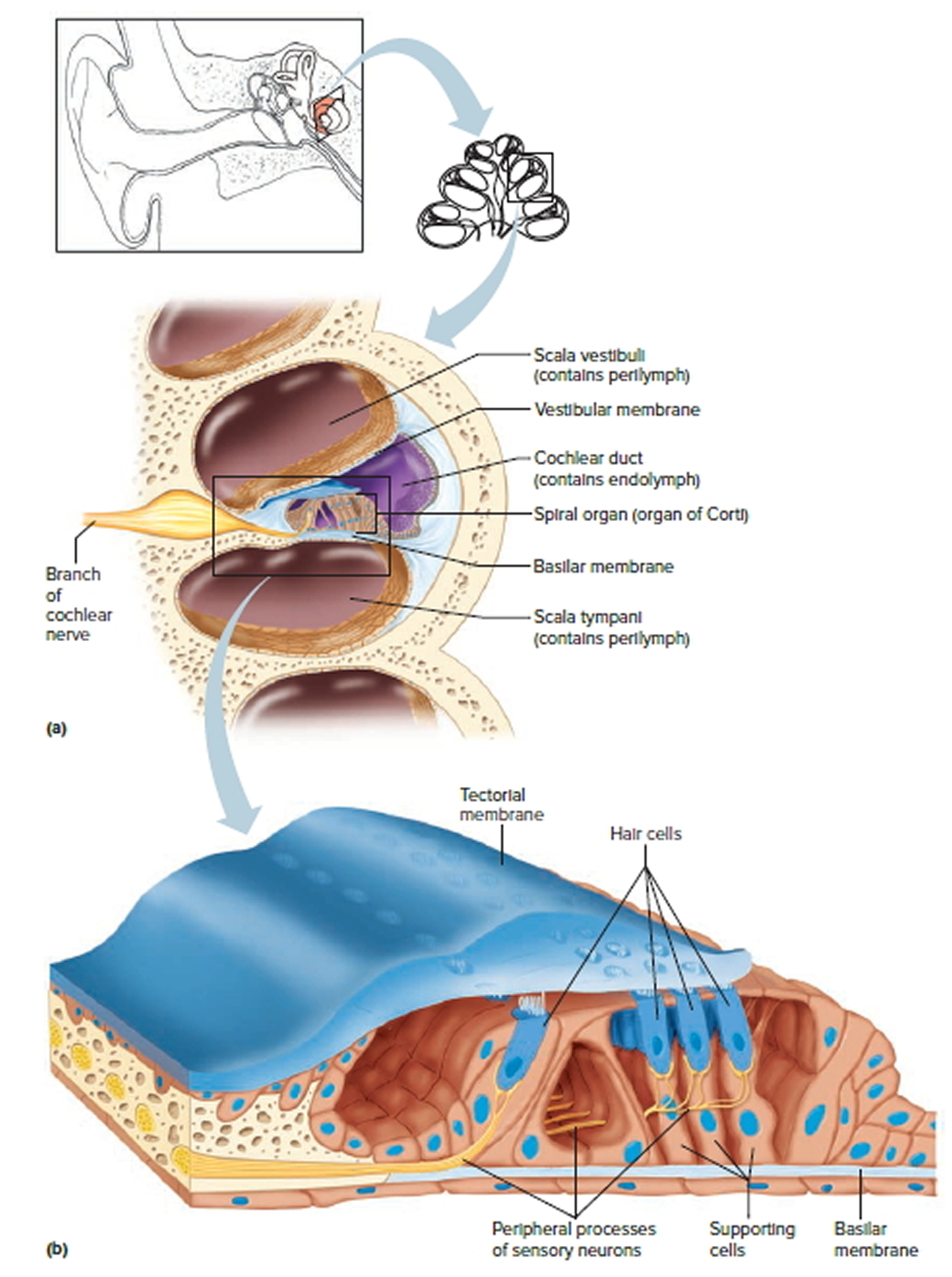
Figure 5. The Cochlea (cross section view)
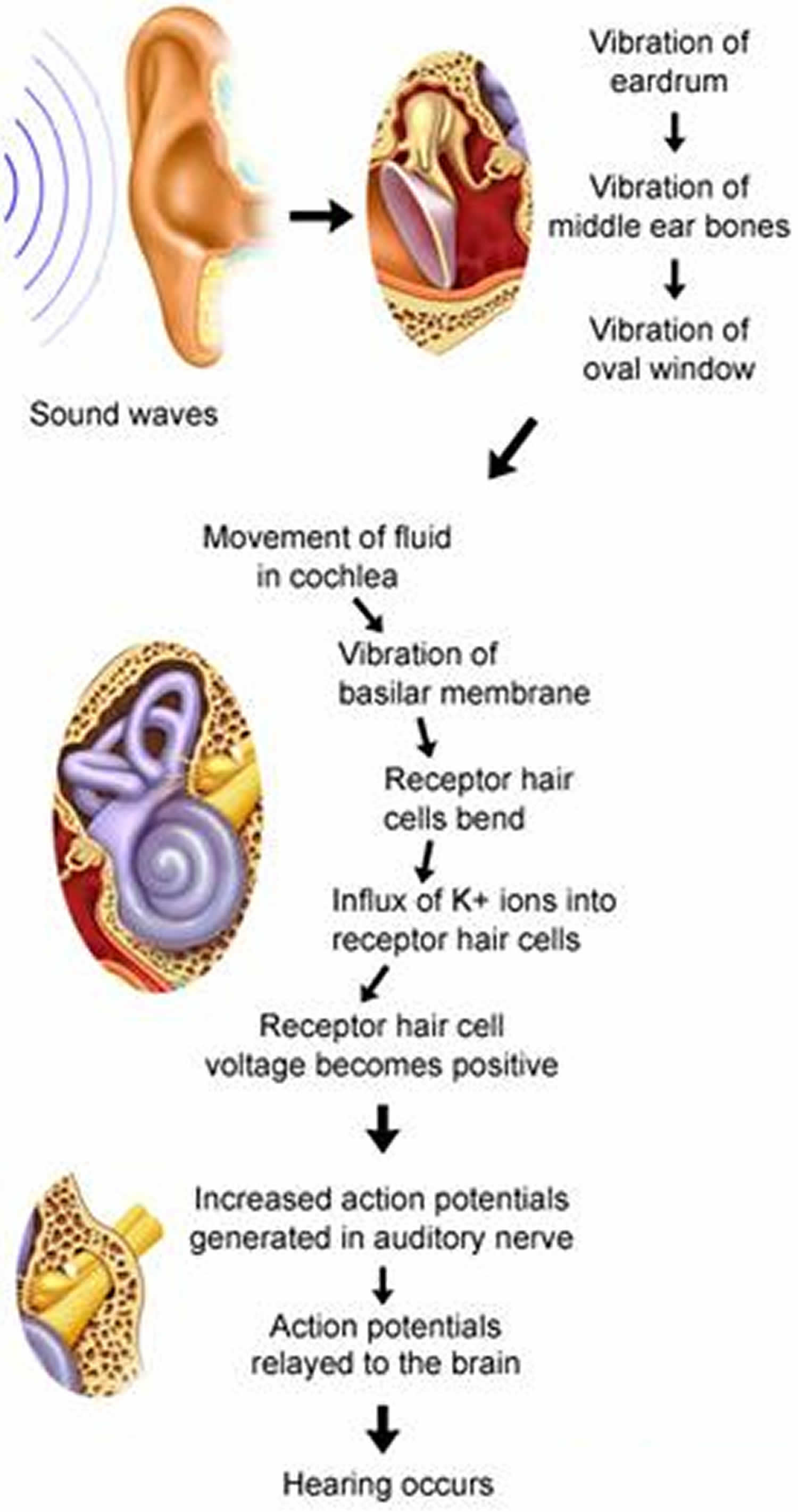
Converting sound wave vibrations into inner ear fluid movement
As the eardrum vibrates in response to air waves, the chain of inner ear bones are set into motion at the same frequency (see Figure 3). The frequency of movement is transmitted across from the eardrum to the oval window (another structure in the ear), resulting in a pressure being exerted on the oval window with each vibration. This produces wavelike movements of the inner ear fluid at the same frequency as the original sound wave. However, in order to set the fluid into motion, greater pressure is required, so that the pressure must be amplified. This amplification of the pressure of the airborne sound wave to set up fluid vibrations in the cochlea is related to two mechanisms. Firstly, the surface area of the tympanic membrane is much large than that of the oval window. In addition, the lever action of the ossicles greatly increases the force exerted on the oval window. The extra pressure generated through these mechanisms is sufficient to set the cochlea fluid in motion.
Physiology of the middle ear
Concentration of energy
The function of the auditory ossicles in the middle ear is to concentrate the energy of the vibrating eardrum so as to create a greater force per unit area at the oval window, as previously described.
Protection of inner ear
In addition to this, the ossicles and their adjacent muscles also serve a protective function. In response to a loud noise, the tensor tympani pulls the eardrum inward and tenses it. At the same time, the stapedius reduces movement of the stapes. These actions of the muscles are known collectively as the tympanic reflex. This reflex muffles the transfer of vibrations from the eardrum to the oval window. It is thought that the tympanic reflex is an evolutionary adaptation for protection against loud but slowly building noises such as thunder. However, because it has a time delay of about 40 ms, it is not quick enough to protect the inner ear from sudden loud noises such as gunshots. It also does not adequately protect the ears from sustained loud noises such as factory noises or loud music. These noises can irreversibly damage the stereocilia of the hair cells in the inner ear, leading to hearing loss.
Coordinating speech with hearing
The muscles of the middle ear also assist in coordinating speech with hearing, so that the sound of our own speech is not so loud as to damage our inner ear and drown out soft or high-pitched sounds from other sources. Just as we are about to speak, the brain signals the middle ear muscles to contract, dampening the sense of hearing in coordination with the sound of our own voice. This makes it possible to hear other people while we are speaking ourselves.
Physiology of the inner ear
Cochlea
Arising from the vestibule is the cochlea, which is sometimes referred to as the organ of hearing, as it is the part of the whole ear that actually converts sound vibrations to the perception of hearing. The cochlea is in the form of a snail-like spiral, so that a longer cochlea is able to fit inside an enclosed space. It is about 9mm wide at the base and 5mm high, and winds around a section of spongy bone called the modiolus. The modiolus is shaped like a screw whose threads form a spiral platform that support the cochlea, which is fleshy and unable to support itself.
Chambers of the cochlea
The cochlea contains three fluid-filled chambers separated by membranes. The upper chamber, scala vestibule, and the bottom chamber, scala tympani, are filled with perilymph. The scala tympani is covered by a secondary tympanic membrane. The middle chamber is the scala media, or the cochlea duct. It is filled with endolymph, instead of perilymph.
Organ of corti
The organ of corti is supported by a membrane called the basilar membrane. It about the size of a pea, and acts as a transducer, converting vibration into nerve impulses. It has hair cells and supporting cells. Hair cells have long stiff microvilli called stereocilia on their apical surfaces. Microvilli are fine hair-like structures on cells that help to increase cell surface area. On top of these stereocilia is a jelly-like membrane called the tectorial membrane. Four rows of hair cells spiral along the length of the organ of Corti. Of these, there are about 3500 inner hair cells, each with a cluster of 50-60 stereocilia graded from short to tall. There are another 20 000 outer hair cells that are arranged in three rows opposite the inner hair cells. Each outer hair cell has about 100 stereocilia with their tips embedded in the tectorial membrane above them. These outer hair cells adjust the response of the cochlea to different sound frequencies so as to enable the inner hair cells to function more accurately. The physiological mechanisms, by which hair cells within the cochlea act to produce hearing, are discussed in more detail below.
Cochlea hair cells
As previously mentioned, the cochlea is the organ that enables sound perception. The physiology of the cochlea revolves around the functioning of the inner and outer cochlea hair cells. In addition to the cells themselves, there are several other components of the cochlea that contribute to the ability to hear.
Role of inner hair cells
The inner hair cells transform the mechanical force of sound (cochlea fluid vibration) into the electrical impulses of hearing (action potentials sending auditory messages to the brain). They communicate with nerve fibers that make up the auditory nerve leading to the brain. When the rate of neurotransmitter (chemicals released by cells in response to stimuli) release from these hair cells is increased, the rate of firing in the nerve fibers is also increased. This occurs when the voltage of the hair cells becomes more positive. Conversely, when the voltage of the hair cells becomes more negative, the hair cells release less neurotransmitter and the firing rate in nerve fibers decreases.
Role of outer hair cells
Unlike the inner hair cells, the outer hair cells do not signal the brain about incoming sounds. They instead actively and rapidly elongate in response to changes in the voltages of the cell membrane. This behavior is known as electromotility. When the outer hair cells elongate, the motion of the basilar membrane is amplified. This modification of the basilar membrane is believed to improve and tune the stimulation of the inner hair cells. The outer hair cells therefore enhance the receptors of the inner hair cells, increasing their sensitivity to sound intensity and rendering them highly discriminatory between various pitches of sound.
Other components of cochlear physiology
The activity of the inner and outer hair cells is possible through various other components within the cochlear. They key components are listed as follows:
Basilar membrane
The vibration of the auditory ossicles, as previously described, eventually leads to the vibration of the basilar membrane on which the hair cells rest through sequence of chain reactions. During the vibration of the auditory ossicles, the stapes vibrates rapidly in and out, leading to the basilar membrane vibrating down and up, and the secondary tympanic membrane vibrating out and in. This can occur as often as 20 000 times per second.
Endolymph
In order for inner hair cells to function properly, the tips of their stereocilia must be bathed in endolymph, which has an exceptionally high potassium ion (K+) concentration, creating a strong electrochemical gradient (large difference in voltage) from the tip to base of a hair cell. This electrochemical gradient provides the energy that allows the hair cell to function. The interaction between stereocilia and endolymph is further discussed below. (Stereocilia)
Tectorial membrane
The stereocilia of the outer hair cells have their tips embedded in the tectorial membrane, while the stereocilia of the inner hair cells come very close to the membrane. The tectorial membrane is anchored to a structure called the modiolus, which holds it relatively still as the basilar membrane and hair cells vibrate. Vibration of the basilar membrane therefore causes shearing of the hair cells against the tectorial membrane, bending the hair cell stereocilia back and forth.
Stereocilia
A protein functions as a mechanically gated ion channel on the top of each stereocilia of the inner hair cells. In addition, there is a fine stretchy protein filament known as a tip link that extends like a spring from the ion channel of one stereocilium to the side of the streocilium next to it. On each inner hair cell, the stereocilia progressively increase in height, so that all but the tallest ones have tip links leading to taller stereocilia beside them. When a taller stereocilium bends away from a shorter one, it pulls on the tip link, so that the ion channel of the short stereocilium is opened. The endolymph bathing the stereocilia has a very high concentration of K+ ions, so that when the channel is pulled open, there is a rapid flow of K+ into each hair cell. This makes the voltage of the hair cell become positive when the channel is open. When the stereocilium is bent the other way, the channel closes and the cell voltage becomes negative. When the cell voltage is positive, the inner hair cells release a neurotransmitter that stimulates the sensory nerves at the base of the hair cell. This leads to the generation of action potentials in the cochlea nerve.
Sound transduction
The conversion of sound energy into a neural signal that is interpreted by the brain as sound perception, as described above, is known as sound transduction. The following diagram summarises this process:
Figure 6. Sound transduction
Sensory coding
Loud vs soft sounds
The organ of Corti allows you to discriminate between different sound intensities. Loud sounds produce more vigorous vibrations of the organ of Corti, thereby exciting a greater number of hair cells over a greater area of basilar membrane. This leads to a high frequency of action potentials being initiated in the cochlea nerve. Intense activity in the cochlea nerve fibres from a broad region of the organ of Corti is therefore detected by the brain and interpreted as a loud sound. The reverse applies to detect soft sounds.
High-pitched vs low-pitched sounds
The basilar membrane enables us to differentiate between high and low pitched sounds. The membrane is spanned by short stiff fibres of various lengths. At its lower end, the basilar membrane is attached, narrow and stiff. At the top end, however, it is unattached, wider and more flexible. The vibration of one region of the basilar membrane causes a wave of vibration to travel down its length and back again. This is referred to as a standing wave, and is akin to plucking a string at one end, causing a wave vibration (like on a guitar). The peak amplitude of the standing wave is near the top end during low-frequency sounds and near the bottom end during higher-frequency sounds. When the brain receives signals mainly from inner hair cells at the top end, it interprets this sound as being low-pitched. Likewise, when the brain receives signals mainly from inner hair cells at the bottom end, the sound is interpreted as being high-pitched. In the reality of everyday life, speech, music and other everyday sounds are not pure tones. Instead, they create complex patterns of vibration in the basilar membrane that have to be decoded and interpreted by the brain.
Comparing loudness of common sounds
What kind of decibel levels are you exposed to during a typical day? To give you an idea, compare noises around you to these specific sounds and their corresponding decibel levels:
Table 1. Sound levels of common noises
| Decibels | Noise source |
| Sources: The National Institute on Deafness and other communication disorder. And the National Institute for Occupational Safety and Health. | |
| Safe range | |
| 30 | Whisper |
| 60 | Normal conversation |
| 78 | Washing machine |
| Risk range | |
| 80 to 90 | Heavy city traffic, power lawn mower |
| 90 | Motorcycle |
| 100 | Snowmobile, hand drill |
| 110 | Chain saw, rock concert |
| Injury range | |
| 120 | Ambulance siren |
| 140 (pain threshold) | Jet engine at takeoff |
| 165 | 12-gauge shotgun blast |
| 180 | Rocket launch |
Maximum sound-exposure durations
Below are the maximum noise levels on the job to which you may be exposed without hearing protection, and for how long.
Table 2. Maximum job-noise exposure allowed by law
| Sound level, decibels | Duration, daily |
| Source: The National Institute for Occupational Safety and Health | |
| 90 | 8 hours |
| 92 | 6 hours |
| 95 | 4 hours |
| 97 | 3 hours |
| 100 | 2 hours |
| 102 | 1.5 hours |
| 105 | 1 hour |
| 110 | 30 minutes |
| 115 | 15 minutes or less |
Research suggests the safe exposure limits is 85 decibels for 8 hours a day. Your hearing could be at risk of damage if you are continually exposed to high volume sounds.
The world in which you live can be a noisy place and there can be times when environmental sounds are dangerously loud to be exposed to; whether at work, in public events such as firework displays or music events.
Equally, with music becoming more portable, on your phones and MP3 players you are listening to music for much longer periods of the day, and potentially at high levels. Over time, risky listening habits can permanently damage hearing or cause tinnitus, affecting your ability to hear the music you love as well as conversation at home or at work.
- Evaluate where you are going and if there may be short intense bursts of noise (such as with a firework display and clay pigeon shooting) or longer exposures (for example in clubs and music concerts)
- Consider purchasing hearing protection such as ear plugs prior to the event
5 ways to protect hearing at work
The risk to hearing from noise at work is dependent on the sound levels (acoustic power). The safe exposure limit is calculated from a combination of exposure time and sound intensity (level). The noise level where employers must provide hearing protection is a daily or weekly average exposure of 85 decibels. Reducing the noise level by only three decibels would allow a doubling of the exposure time.
Based upon the Equal Energy Law:
80dB for 8 hours is the equivalent to 83dB for 4 hours, is the equivalent to 92dB(A) for 30 minutes, is the equivalent to 110dB(A) for 30 seconds. Meaning, the louder the noise, the less time you should be exposed.
- If hearing protection is recommended wear it correctly in all areas – for hearing protection to be effective you must wear it 100% of the time
- Find ear protection which is comfortable for you, whether ear plugs, ear muffs or a combination of the two
- Know your surroundings – what are the average levels of noise you are exposed to throughout your shift
- If the company you work for offers annual hearing checks, book yourself in and monitor your hearing.
- If you are worried about your hearing , get your hearing checked and inform the person testing your hearing when you were last exposed to noise and how long you were exposed for.
5 ways to listen safely to music on phones and portable devices
- Set your headphone volume levels when you’re in a quiet environment, not a place with lots of competing sounds
- Lower the volume if you can’t hear those around you speaking
- Avoid using a listening device where lack of attention to your surroundings could be dangerous, for example whilst driving or operating machinery
- Pay attention to how long you listen to music at high volume. Your ears adapt to higher volume settings over time meaning that you can damage your hearing even if the intensity doesn’t seem uncomfortable to your ears
- The louder the volume, the less time noise takes to affect your hearing. If you experience ringing in your ears or speech sounds muffled, stop listening and get your hearing checked
Types of hearing loss
Conductive Hearing loss
Conductive hearing loss occurs when sound waves are not properly conducted through the external and middle portions of the ear to set the fluid in the inner ear in motion.
Possible causes include:
- Physical blockage of the ear canal with earwax
- Foreign object that is stuck in the ear canal
- Eardrum rupture
- Scar on the eardrum from repeated infections
- Middle ear infection with accompanying fluid accumulation
- Restriction of the movement of the ossicles, due to bony adhesions between the stapes and oval window
- Damage to the very small bones (ossicles) that are right behind the eardrum
Sensorineural Hearing loss
In sensorineural hearing loss, the sound waves are transmitted to the inner ear, but they are not converted into nerve signals that are interpreted by the brain as sounds. The defect can lie in the organ of Corti or the auditory nerves, or rarely, in some pathways and parts of the brain.
Sensorineural hearing loss is caused by damage to these special cells, or to the nerve fibers in the inner ear. Sometimes, the hearing loss is caused by damage to the nerve that carries the signals to the brain.
Sensorineural deafness that is present at birth (congenital) is most often due to:
- Genetic syndromes
- Infections that the mother passes to her baby in the womb (toxoplasmosis, rubella, herpes)
Sensorineural hearing loss may develop in children or adults later in life (acquired) as a result of:
- Age-related hearing loss
- Disease of the blood vessels
- Immune disease
- Infections, such as meningitis, mumps, scarlet fever, and measles
- Injury
- Loud noises or sounds, or loud sounds that last for a long time
- Meniere disease
- Tumor, such as acoustic neuroma
- Use of certain medicines
- Working around loud noises every day
In some cases, the cause is unknown.
Neural presbycusis
Neural presbycusis is one of the most common causes of partial hearing loss. It is a progressive age-related process that occurs over time as the hair cells “wear out” with use. Even exposure to ordinary modern-day sounds can eventually damage hair cells over long periods of time. An adult loses on average more than 40% of their cochlea hair cells by the age of 65. Those hair cells that process high-frequency sounds are the most vulnerable to destruction.
Test your hearing questionnaire
To get an idea of how well you hear, answer the following questions and then calculate your score. To calculate your score, give yourself:
- 3 points for every ”almost always” answer
- 2 points for every ”half the time” answer
- 1 point for every “occasionally” answer
- 0 for every ”never” answer
Please note: If hearing loss runs in your family, add an additional 3 points to your overall score.
The American Academy of Otolaryngology–Head and Neck Surgery recommends the following:
- 0-5 points Your hearing is fine. No action is required.
- 6-9 points Suggest you see an ear, nose, and throat (ENT) specialist.
- 10+ points Strongly recommend you see an ear, nose, and throat (ENT) specialist.
1.I have a problem hearing over the telephone.
- Almost always
- Half the time
- Occasionally
- Never
2. I have trouble following the conversation when two or more people are talking at the same time.
- Almost always
- Half the time
- Occasionally
- Never
3. People complain that I turn the TV volume too high.
- Almost always
- Half the time
- Occasionally
- Never
4. I have to strain to understand conversations.
- Almost always
- Half the time
- Occasionally
- Never
5. I miss hearing some common sounds like the phone or doorbell ring.
- Almost always
- Half the time
- Occasionally
- Never
6. I have trouble hearing conversations in a noisy background, such as a party.
- Almost always
- Half the time
- Occasionally
- Never
7. I get confused about where sounds come from.
- Almost always
- Half the time
- Occasionally
- Never
8. I misunderstand some words in a sentence and need to ask people to repeat themselves.
- Almost always
- Half the time
- Occasionally
- Never
9. I especially have trouble understanding the speech of women and children.
- Almost always
- Half the time
- Occasionally
- Never
10. I have worked in noisy environments (such as assembly lines, construction sites, or near jet engines).
- Almost always
- Half the time
- Occasionally
- Never
11. Many people I talk to seem to mumble, or don’t speak clearly.
- Almost always
- Half the time
- Occasionally
- Never
12. People get annoyed because I misunderstand what they say.
- Almost always
- Half the time
- Occasionally
- Never
13. I misunderstand what others are saying and make inappropriate responses.
- Almost always
- Half the time
- Occasionally
- Never
14. I avoid social activities because I cannot hear well and fear I’ll make improper replies.
- Almost always
- Half the time
- Occasionally
- Never
15. Ask a family member or friend to answer this question: Do you think this person has a hearing loss?
- Almost always
- Half the time
- Occasionally
- Never
Hearing loss causes
Some causes of hearing loss include damage to the inner ear, a buildup of earwax, infections and a ruptured eardrum. To understand how hearing loss occurs, it can be helpful to understand how you hear. Please read the overview of the ear above.
How you hear
Hearing occurs when sound waves reach the structures inside your ear, where the sound wave vibrations are converted into nerve signals that your brain recognizes as sound.
Your ear consists of three major areas: outer ear, middle ear and inner ear. Sound waves pass through the outer ear and cause vibrations at the eardrum. The eardrum and three small bones of the middle ear amplify the vibrations as they travel to the inner ear. There, the vibrations pass through fluid in a snail-shaped structure in the inner ear (cochlea). Attached to nerve cells in the cochlea are thousands of tiny hairs that help translate sound vibrations into electrical signals that are transmitted to your brain. The vibrations of different sounds affect these tiny hairs in different ways, causing the nerve cells to send different signals to your brain. That’s how you distinguish one sound from another.
Causes of hearing loss include:
- Damage to the inner ear. Aging and exposure to loud noise may cause wear and tear on the hairs or nerve cells in the cochlea that send sound signals to the brain. When these hairs or nerve cells are damaged or missing, electrical signals aren’t transmitted as efficiently, and hearing loss occurs. Higher pitched tones may become muffled to you. It may become difficult for you to pick out words against background noise. Heredity may make you more prone to these changes. This type of hearing loss is known as sensorineural hearing loss, which is permanent.
- A gradual buildup of earwax. Earwax can block the ear canal and prevent conduction of sound waves. This can be restored with earwax removal.
- Ear infection and abnormal bone growths or tumors. In the outer or middle ear, any of these can cause hearing loss.
- Ruptured eardrum (tympanic membrane perforation). Loud blasts of noise, sudden changes in pressure, poking your eardrum with an object and infection can cause your eardrum to rupture and affect your hearing.
Risk factors for hearing loss
Factors that may damage or lead to loss of the hairs and nerve cells in your inner ear include:
- Aging. Degeneration of delicate inner ear structures occurs over time.
- Loud noise. Exposure to loud sounds can damage the cells of your inner ear. Damage can occur with long-term exposure to loud noises, or from a short blast of noise, such as from a gunshot.
- Heredity. Your genetic makeup may make you more susceptible to ear damage from sound or deterioration from aging.
- Occupational noises. Jobs where loud noise is a regular part of the working environment, such as farming, construction or factory work, can lead to damage inside your ear.
- Recreational noises. Exposure to explosive noises, such as from firearms and jet engines, can cause immediate, permanent hearing loss. Other recreational activities with dangerously high noise levels include snowmobiling, motorcycling or listening to loud music.
- Some medications. Drugs, such as the antibiotic gentamicin and certain chemotherapy drugs, can damage the inner ear. Temporary effects on your hearing — ringing in the ear (tinnitus) or hearing loss — can occur if you take very high doses of aspirin, other pain relievers, antimalarial drugs or loop diuretics.
- Some illnesses. Diseases or illnesses that result in high fever, such as meningitis, may damage the cochlea
Hearing loss prevention
Hearing loss prevention consists of steps you can take to help you prevent noise-induced hearing loss and avoid worsening of age-related hearing loss:
- Protect your ears in the workplace. Specially designed earmuffs that resemble earphones can protect your ears by bringing most loud sounds down to an acceptable level. Foam, pre-formed or custom-molded earplugs made of plastic or rubber also can help protect your ears from damaging noise.
- Have your hearing tested. Consider regular hearing tests if you work in a noisy environment. Regular testing of your hearing can provide early detection of hearing loss. Knowing you’ve lost some hearing means you’re in a position to take steps to prevent further hearing loss.
- Avoid recreational risks. Some activities, such as riding a snowmobile, hunting or listening to rock concerts for long periods of time, can damage your hearing. Wearing hearing protectors or taking breaks from the noise during loud recreational activities can protect your ears. Turning down the volume when listening to music can help you avoid damage to your hearing.
Tips to maintain hearing health
- If you work in noisy places or commute to work in noisy traffic or construction, choose quiet leisure activities instead of noisy ones.
- Develop the habit of wearing earplugs when you know you will be exposed to noise for a long time.
- Earplugs can reduce the volume of sound reaching the ear to a safer level.
- Try not to use several noisy machines at the same time.
- Try to keep television sets, stereos and headsets low in volume.
Ear protection
A wide range of technical hearing protection products are available. Quality ear plugs will reduce the overall level of sound while maintaining an even balance across the sound spectrum. This means that you can still hear everything clearly, although the overall sound level is reduced. The greater the number of decibels of attenuation by the ear plugs, the better overall protection they offer.
Non-custom ear plugs
This type of ear protection is seen as the most basic form. Plugs can be made out of:
- Memory foam (where the plug is rolled up and inserted into the ear canal)
- Silicone (which is rolled into a ball and pressed into the ear to mould over the ear canal)
- Flanged (where they achieve a seal down to their tapered shape)
- Tapered ear plugs inserted into the ear to obtain a seal against the noise
One of the advantages of non-custom ear plugs is that they are disposable and therefore more hygienic. Non-custom plugs are also available fitted with specific filters for use in a variety of situations including at work, on aeroplanes, at parties and whilst asleep. Buy earplugs for noise, earplugs for swimming, earplugs for flying.
Ear muffs or defenders
Ear muffs or defenders have cups lined with sound-deadening material. The protection usually comes from acoustic foam which absorbs sound waves by increasing air resistance, thus reducing the amplitude of the waves.
Custom hearing protection
Customised earplugs, which attenuate sounds across all frequencies rather than just low and mid-frequencies, can be of particular interest to musicians looking for ear protection. These ear plugs are designed to protect your hearing, while delivering clear and natural sound across all frequencies.
Depending upon the environment you are in, different levels of protection will be required. Before purchasing any ear plugs discuss you needs with an audiologist/private hearing aid dispenser/manufacturer who will be able to recommend an appropriate product. Impressions of your ears will be taken by an audiologist or private hearing aid dispenser and sent to a manufacturer to be turned into an ear plugs.
What you can do to improve your hearing
- Eliminate or lower unnecessary noises around you.
- Let friends and family know about your hearing loss and ask them to speak slowly and more clearly.
- Ask people to face you when they are speaking to you, so you can watch their faces and see their expressions.
- Utilize sound amplifying devices on phones.
- Use personal listening systems to reduce background noise.
Hearing loss signs and symptoms
It’s not always easy to tell if you’re losing your hearing.
Hearing loss is sometimes sudden, but more often it happens gradually and you may not notice it at first.
Signs and symptoms of hearing loss may include:
- Muffling of speech and other sounds
- Asking people to repeat themselves
- Difficulty understanding words, especially against background noise or in a crowd of people
- Having to concentrate hard to hear what other people are saying, which can be tiring or stressful
- Trouble hearing consonants
- Frequently asking others to speak more slowly, clearly and loudly
- Needing to turn up the volume of the television or radio
- Withdrawal from conversations
- Avoidance of some social settings
The signs can be slightly different if you only have hearing loss in one ear or if a young child has hearing loss.
Hearing loss diagnosis
Tests to diagnose hearing loss may include:
- Physical exam. Your doctor will look in your ear for possible causes of your hearing loss, such as earwax or inflammation from an infection. Your doctor will also look for any structural causes of your hearing problems.
- General screening tests. Your doctor may ask you to cover one ear at a time to see how well you hear words spoken at various volumes and how you respond to other sounds.
- Tuning fork tests. Tuning forks are two-pronged, metal instruments that produce sounds when struck. Simple tests with tuning forks can help your doctor detect hearing loss. A tuning fork evaluation may also reveal whether hearing loss is caused by damage to the vibrating parts of your middle ear (including your eardrum), damage to sensors or nerves of your inner ear, or damage to both.
- Audiometer tests. During these more-thorough tests conducted by an audiologist, you wear earphones and hear sounds directed to one ear at a time. The audiologist presents a range of sounds of various tones and asks you to indicate each time you hear the sound.Each tone is repeated at faint levels to find out when you can barely hear. The audiologist will also present various words to determine your hearing ability.
- CT or MRI scan of the head (if a tumor or fracture is suspected)
Hearing loss treatment
If you have hearing problems, help is available.
Getting treatment can improve your quality of life dramatically. People who use hearing aids report these benefits:
- Greater self-confidence
- Closer relationships with loved ones
- Improved outlook on life, overall
- Less depression
Treatment depends on the cause and severity of your hearing loss.
Options include:
- Removing wax blockage. Earwax blockage is a reversible cause of hearing loss. Your doctor may remove earwax by loosening it with oil and then flushing, scooping or suctioning out the softened wax.
- Surgical procedures. Surgery may be necessary if you’ve had a traumatic ear injury or repeated infections that require the insertion of small tubes that help the ears drain.
Hearing aids
Hearing aids can be useful in treating conductive deafness but are less beneficial for sensorineural hearing loss. They increase the intensity of airborne sounds and may modify the sound spectrum to suit the patient’s particular pattern of hearing loss at higher or lower frequencies. However, the receptor cell-neural pathway system must still be intact and functioning for the sound to be perceived, so hearing aids are useless in sensorineural hearing loss.
Hearing aids vary in price according to style, features, and local market prices. Price can range from hundreds of dollars to more than $2,500 for a programmable, digital hearing aid. Purchase price should not be the only consideration in buying a hearing aid. Product reliability and customer service can save repair costs and decrease frustration of a malfunctioning hearing aid.
There are many different types of hearing aid, including:
- Behind the ear hearing aids (the most common type) – hearing aids that go around the top and back of the ear
- In the ear hearing aids – small hearing aids that fit in the opening of the ear
- In the canal hearing aids – very small hearing aids that fit a bit further into the opening of the ear, so they’re just visible
- Completely in-the-canal – least visible hearing aids
- Open fit receiver-in-the-ear (RITE) hearing aids are a newer design, and while still placed over the ear, they are extremely small and nearly invisible.
The best hearing aid for you depends upon your particular hearing loss and listening needs, the size and shape of your ear and ear canal, and the dexterity of your hands. Many hearing aids have tele-coil “T” switches for telephone use and public sound systems.
Other options, such as FM systems and Bluetooth devices in conjunction with hearing aids, may provide the best benefit for some patients.
An audiologist can discuss with you the potential benefits of using a hearing aid, recommend a device and fit you with it.
Federal regulation prohibits any hearing aid sale unless the buyer has first received a physicians evaluation, so you will need to see your doctor before you purchase a hearing aid. However, the regulation also says that if you are over 18 and aware of the recommendation for a medical exam, you may sign a waiver to forego it.
An otolaryngologist, audiologist, or independent dispenser can dispense aids. Hearing aids should be custom-fit to your ear and hearing needs. Mail-order hearing aids typically cannot be custom-fit.
Will I need a hearing aid for each ear?
Usually, if you have hearing loss in both ears, using two hearing aids is best. Listening in a noisy environment is difficult with amplification in one ear only, and it is more difficult to distinguish where sounds are coming from.
Figure 7. Hearing aid styles

Note: Many choices of hearing aid styles are available, including the following: completely in the canal (A), in the canal (B), in the ear (C), behind the ear (D), receiver in canal or receiver in the ear (E), and open fit (F).
Bone anchored hearing aids
A bone anchored hearing aid may be an option if you have hearing loss caused by sound being unable to reach your inner ear.
This type of hearing aid is attached to your skull during a minor operation. It picks up sound and sends it to the inner ear by vibrating the bones near your ear.
It can be clipped on and off – for example, it’s removed at night and when you swim or take a shower. Some newer types are held onto the head with magnets instead of a connector through the skin.
Figure 8. Bone anchored hearing aid

Bone conduction hearing devices
Bone conduction hearing devices is becoming increasingly used instead of bone anchored hearing aids (BAHA) because of how the technology has improved over the years.
A bone conduction hearing device is an alternative to a regular hearing aid for those with problems in their outer or middle ears. It transfers sound by bone vibration directly to the cochlea, bypassing the outer and the middle ear. This means it is useful for conductive and mixed hearing losses. A bone conduction hearing device relies on a working cochlea to send sound to the brain.
A bone conduction hearing device may be considered when a conventional hearing aid cannot be worn, (for example due to irritated or collapsed ear canals), or when a hearing aid does not give effective benefit.
A bone conduction hearing device offers amplification without an ear mould in the ear. This makes them more comfortable if you experience discomfort or infections in your ear. Some people also report that they have a more natural sound than conventional hearing aids for the same reason. They do not restore your hearing to normal, but can make managing in everyday situations easier.
A bone conduction hearing device is compatible with hearing loop (telecoil) systems. You can select to pick up sound through the microphone, through the loop, or through a combination of both microphone and loop. This means you can take advantage of assistive listening devices, neckloops or switching to ‘T’ in places displaying the ‘T’ symbol. The bone conduction hearing device processor may have the telecoil feature integrated within it. Otherwise a telecoil accessory can be plugged into the processor when needed.
How does a bone conduction hearing device work?
A bone conduction hearing device has two parts: an external part (the ‘processor’) and a surgically implanted fixture placed in the bone behind the ear. There are two types of bone conduction implant. The first is a fixture that protrudes through the skin so that the processor can attach onto it. The second is fully implanted under the skin, with the processor attached using a small magnet inside the processor. The photo below shows the magnet version.
Figure 9. Bone conduction hearing device

Figure 10. How bone conduction hearing devices work
Middle ear implants
A middle ear implant may be an option if you can’t use a regular hearing aid – for example, because you’re allergic to the materials they’re made from or they don’t fit in your ear correctly.
Middle ear implants are suitable for those with a mild-moderate mixed or conductive hearing loss or a sensorineural hearing loss.
A middle ear implant is a more recent hearing implant, offering an alternative to conventional hearing aids. It may be considered for those who suffer with earmould allergies, skin problems in their ears, outer ear infections, narrow, collapsed or closed ear canals, or malformed ears.
It can also provide (for mixed or conductive hearing losses) an alternative to a bone anchored hearing aid for those with any of the above ear problems who also have healing issues, dexterity problems, or those who might find difficulty in keeping a bone anchored hearing aid clean.
An middle ear implant has two main parts:
- a device attached to the skin that picks up sound and turns it into an electrical signal
- a device under the skin that picks up these signals and sends them along a wire to the small hearing bones deep in the ear or attached near to the membrane window of the cochlea, which causes them to vibrate.
The implant works by directly moving the bones of the middle ear, or by vibrating the membrane window of the cochlea means that sound can travel into your inner ear and brain. This won’t fully restore your hearing, but it can help make sounds louder and clearer.
In either case, middle ear implant is designed to amplify sounds by adding extra movement into the natural hearing pathway. The middle ear implant relies on a working cochlea and hearing nerve.
What you can expect from a middle ear implant
Middle ear implants offer amplification without an ear mould in the ear. This makes them more comfortable if you experience discomfort or infections in your ear. Some people also report that they have a more natural sound than conventional hearing aids for the same reason. They do not restore your hearing to normal, but can make managing in everyday situations easier.
The audio processor of a middle ear system can be connected to external devices via Bluetooth or telecoil. This enables the signal from your mobile phone, MP3 player, FM system or assistive listening device to be transmitted wirelessly to the audio processor with no loss of sound quality.
Figure 11. Middle ear implant

Figure 12. How middle ear implants work
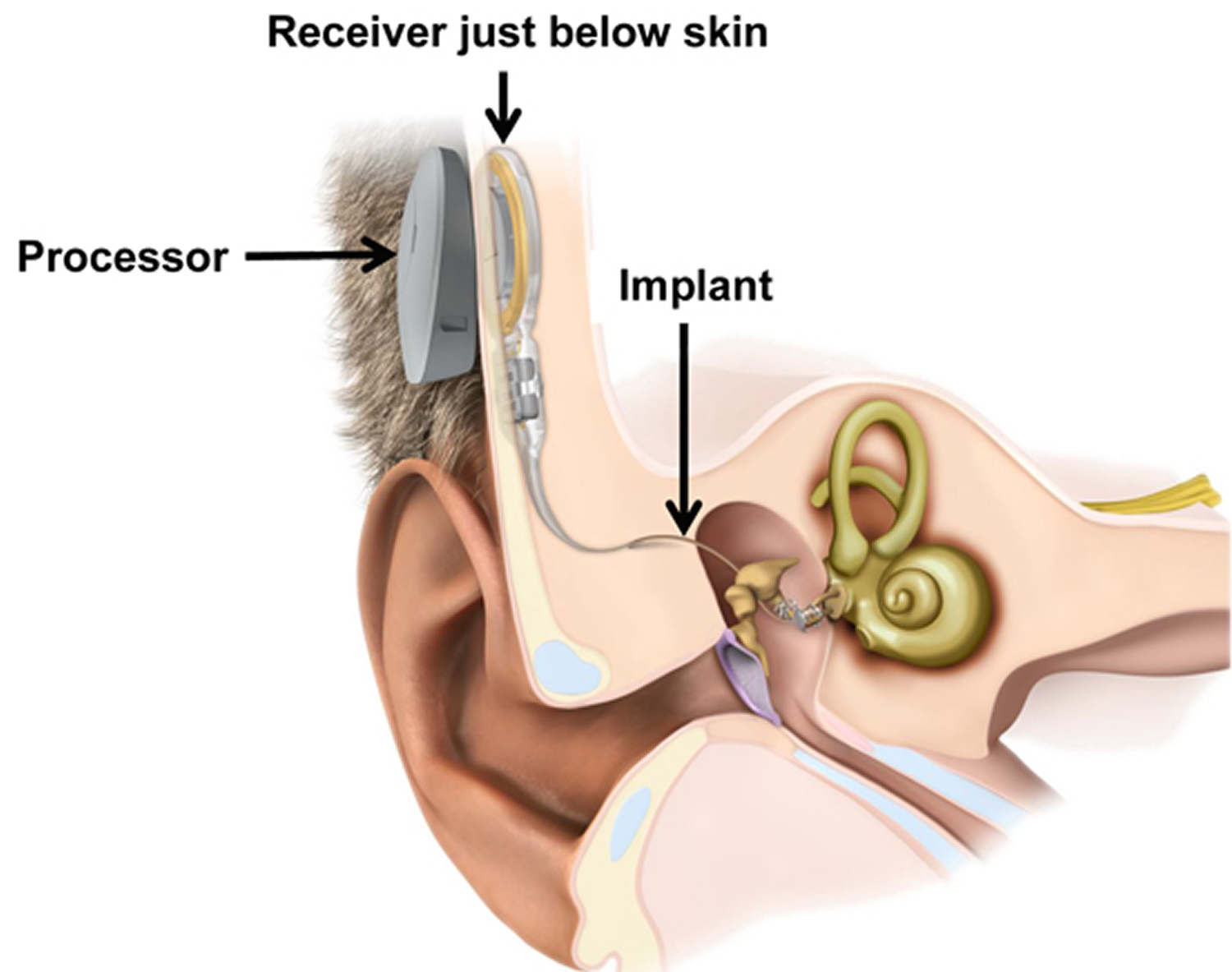
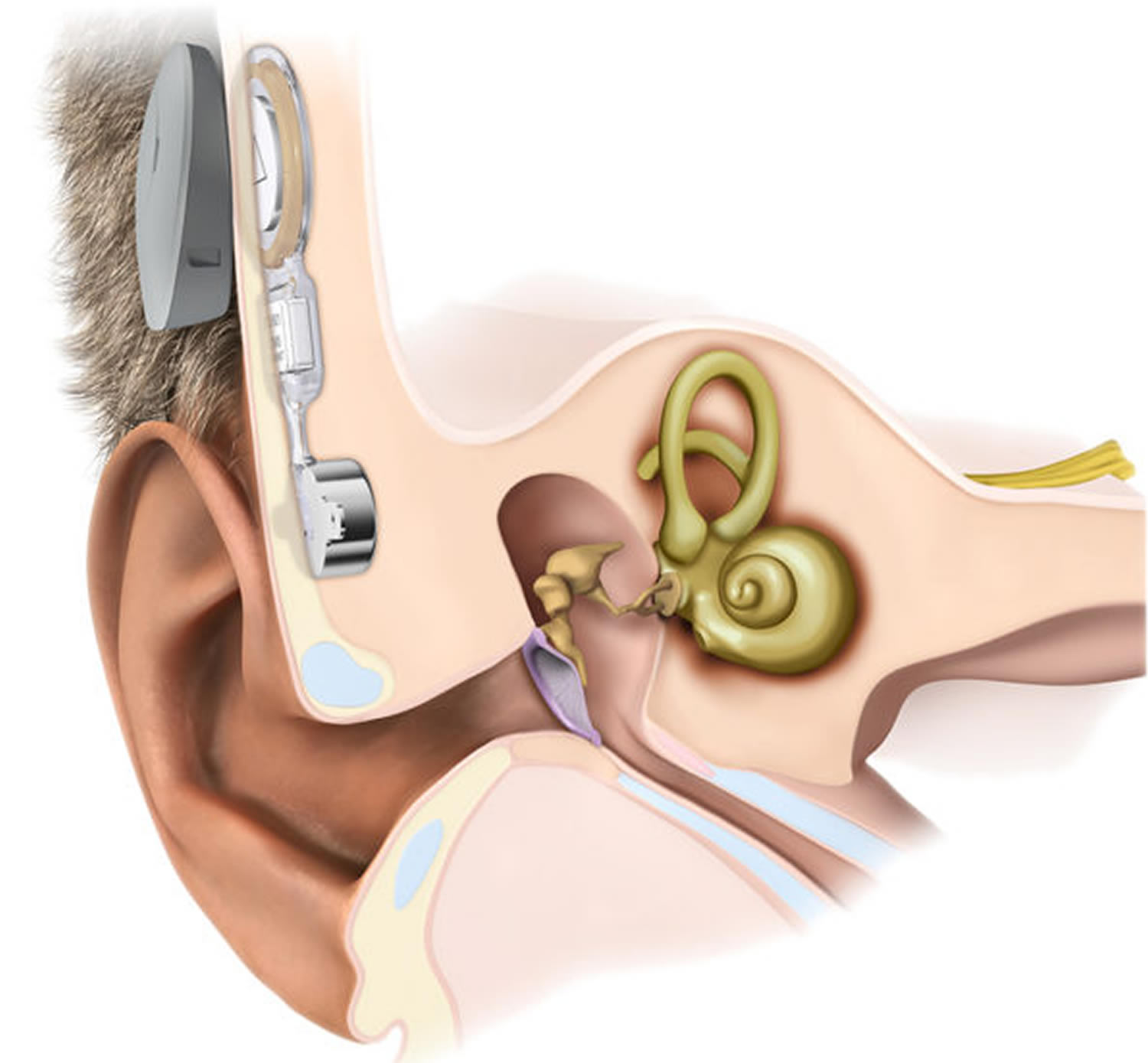
Cochlear implants
Recently, cochlear implants have become available. The implants are electronic devices which are surgically implanted. A cochlear implant may be an option if you have severe, permanent hearing loss that isn’t helped by hearing aids. They convert sound signals into electrical signals that can directly stimulate the auditory nerve, so as to bypass a defective cochlea system. Cochlear implants cannot restore normal hearing but they permit recipients to recognize sounds. Success can range from an ability to hear a phone ringing, to being able to carry on a conversation over the telephone.
The cochlear implant has two main parts:
- a microphone behind the ear that picks up sound and changes it into electrical signals, which are sent along a wire to a device on the skin
- a device placed inside the skull that picks up the electrical signals from the device on the skin and sends them along wires to the cochlea
The implant will only work if the nerve that sends sound to the brain (auditory nerve) is working properly.
If you’re considering a cochlear implant, your audiologist, along with a medical doctor who specializes in disorders of the ears, nose and throat (ENT), can discuss the risks and benefits with you.
Figure 13. How Cochlear implants work
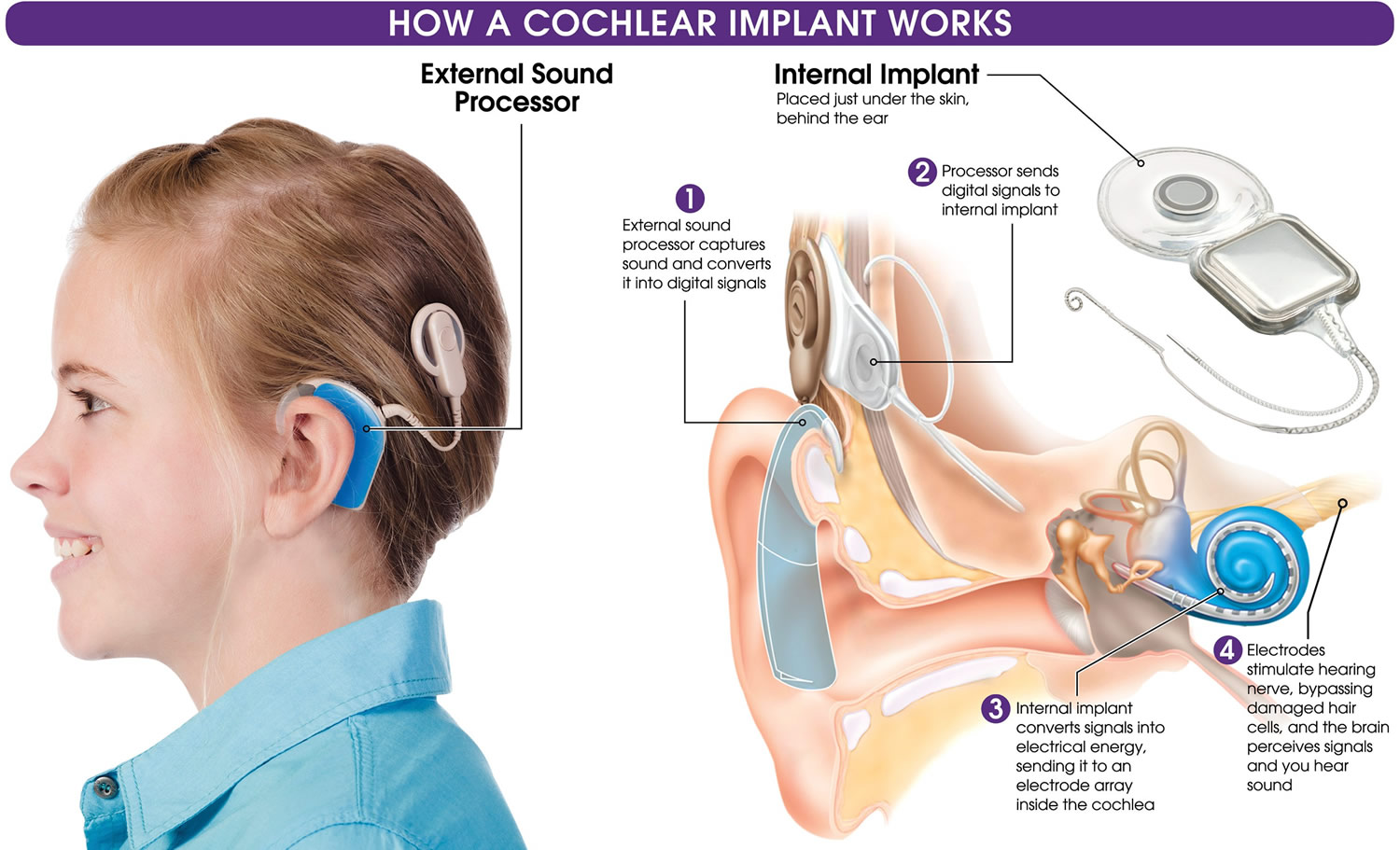
Note: Cochlear implants use an external sound processor that you generally wear behind your ear. A transmitter sends radiofrequency signals to a surgically implanted electronic chip, the receiver and stimulator unit, which stimulates the auditory nerve with electrodes that have been threaded through the cochlea.
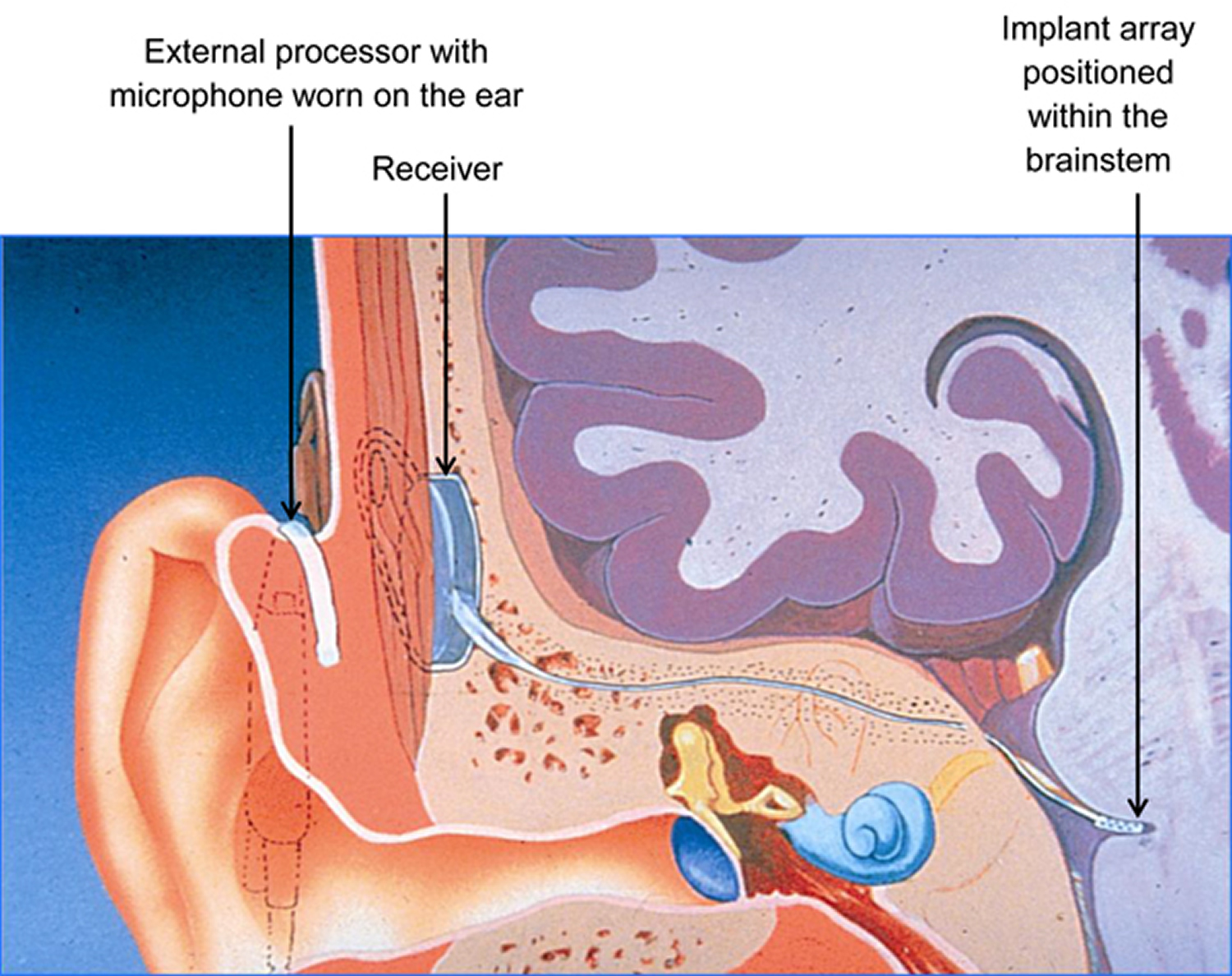
Auditory brainstem implants
An auditory brainstem implant may be an option if you have severe, permanent hearing loss and a problem with your auditory nerve. An auditory brainstem implant may provide a link to sounds when there would otherwise be no natural hearing at all. An auditory brainstem implant may help with lip-reading.
An auditory brainstem implant works in a similar way to a cochlear implant, but the electrical sound signals are sent directly to the brain along wires, instead of the cochlea.
An auditory brainstem implant won’t usually fully restore your hearing, but it can usually improve it to some degree.
An auditory brainstem implant has two parts:
- an external part (the ‘processor’, worn on the ear) and
- the surgically implanted internal part.
A microphone on the processor picks up the sound around it, and turns it from a sound wave into an electrical signal. The processor then transmits the sound signal to the internal part of the hearing implant. This consists of a receiver just below the skin, together with the implant array which is positioned within the brainstem.
This means that the implant is bypassing both the cochlea and the hearing nerve, taking a short cut to the brainstem. In this way the auditory brainstem implant aims to give a sense of sound when the hearing nerve is not working.
Who can be considered for an auditory brainstem implant?
One main use of the auditory brainstem implant is for those with the condition Neurofibromatosis type 2 (NF2). If you have Neurofibromatosis type 2 (NF2), you are likely to have a tumour on or near the hearing nerve. If this tumour is removed for medical reasons, the surgeons may well have to cut across the nerve of hearing. This brings about a complete breakdown of natural hearing in that ear. During the tumour removal surgery, the surgeon may consider placing an auditory brainstem implant as an alternative method of hearing.
Other uses of the auditory brainstem implant are for people who are born with no functioning nerve of hearing in either ear, or people who are deaf because of an unusually shaped cochlea. Sometimes meningitis leads to deafness but leaves the cochlea too damaged to take a cochlear implant. However, an auditory brainstem implant for one of these reasons is very rare, because the auditory brainstem implant requires neurosurgery.
Any drawbacks of an auditory brainstem implant?
An auditory brainstem implant involves complex neurosurgery to the brainstem. Your consultant would need to discuss all the risks with you.
The results of an auditory brainstem implant are extremely variable. It is a difficult task to position the auditory brainstem implant on the brainstem exactly to deliver sound. It is possible that there is no hearing sensation at all from the auditory brainstem implant.
In some cases the hearing sensation is within a narrow range so that sounds are not well differentiated. It takes time to adjust to the sound perceived through an auditory brainstem implant.
Figure 14. Auditory brainstem implant

Figure 15. How auditory brainstem implants work
Sign language and lip reading
If you’ve been deaf from birth or you develop severe hearing loss later in life, it can affect your ability to communicate with other people.
But you can learn different methods of communicating that can be used instead of, or as well as, spoken English.
Two of the main methods are:
- lip-reading – where you learn to watch a person’s mouth movements while they’re speaking to understand what they’re saying
- sign language – a visual way of communicating using hand gestures, facial expressions and body language
Coping and support
These tips can help you to communicate more easily despite your hearing loss:
- Position yourself to hear. Face the person with whom you’re having a conversation.
- Turn off background noise. For example, noise from a television may interfere with conversation.
- Ask others to speak clearly. Most people will be helpful if they know you’re having trouble hearing them.
- Choose quiet settings. In public, such as in a restaurant or at a social gathering, choose a place to talk that’s away from noisy areas.
- Consider using an assistive listening device. Hearing devices, such as TV-listening systems or telephone-amplifying devices, can help you hear better while decreasing other noises around you. Telephone service over the Internet — known as Voice Over Internet Protocol (VoIP) — transmits more frequencies from human speech than does standard telephone service, which may make it easier to hear during phone calls.





{kind=link}