
Contents
What is a HIDA scan
HIDA scan is also known as hepatobiliary hydroxy iminodiacetic acid (HIDA) scan, cholescintigraphy or hepatobiliary scan or hepatobiliary scintigraphy, is an imaging procedure that uses radiotracers to assess the anatomy and function of the biliary system (and the liver indirectly). HIDA scan is used to diagnose problems of the liver, gallbladder and bile ducts. Currently, HIDA scan is most commonly performed with Tc99m-iminodiacetic acid analogues. During a HIDA scan, a radioactive tracer is injected into a vein in your arm. The tracer travels through your bloodstream to your liver, where the bile-producing cells (hepatocytes) take it up. The tracer then travels with the bile into your gallbladder and through your bile ducts to your small intestine. A nuclear medicine scanner (gamma camera) tracks the flow of the tracer from your liver into your gallbladder and small intestine and creates computer images.
Most of the time, HIDA scan is done only if a person has sudden pain that may be from gallbladder disease or gallstones. For this reason, some people may need urgent treatment based on the test results.
HIDA scan is combined with other imaging (such as CT or ultrasound). After the gallbladder scan, the person may be prepared for surgery, if needed.
Indications for HIDA scan
- The HIDA scan should be done when ultrasound is not diagnostic and when there is a clinical diagnosis of acute cholecystitis.
- Usually, HIDA scans are ordered for patients who are suspected of having an obstruction in the biliary tract, most commonly those who are thought to have a stone blocking the cystic duct leading out of the gallbladder.
- Such a scenario is consistent with acute cholecystitis, which often requires surgical removal of the gallbladder.
- In cholecystitis, HIDA will appear in the bile ducts, but it will not enter the cystic duct or the gallbladder — a finding that indicates obstruction.
- If the HIDA enters the bile ducts but does not enter the small intestine, then an obstruction of the bile duct (usually due to stones or cancer) is suspected.
In a healthy person, HIDA will pass through the bile ducts and into the cystic duct to enter the gallbladder.
Limitation of HIDA scan
HIDA scans can be falsely positive when the gallbladder is not filling in the absence of cholecystitis. These situations include severe liver disease, patients on total parenteral nutrition, hyperbilirubinemia, inadequate fasting, and alcohol and opiate abuse.
In the presence of cystic duct obstruction the gallbladder does not fill with isotope.
Reasons for HIDA scan
A HIDA scan is most often done to evaluate your gallbladder. It’s also used to look at the bile-excreting function of your liver and to track the flow of bile from your liver into your small intestine. A HIDA scan is often used with X-ray and ultrasound.
A HIDA scan might help in the diagnosis of several diseases and conditions, such as:
- Gallbladder inflammation (cholecystitis)
- Bile duct obstruction
- Congenital abnormalities in the bile ducts, such as biliary atresia
- Postoperative complications, such as bile leaks and fistulas
- Assessment of liver transplant
Your doctor might use a HIDA scan as part of a test to measure the rate at which bile is released from your gallbladder (gallbladder ejection fraction).
HIDA scan can be used for evaluation of:
- Acute cholecystitis
- most common use is to confirm acute cholecystitis after an equivocal ultrasound study
- if the tracer does not enter the gallbladder after a sufficient length of time, then this is compatible with obstruction of the cystic duct
- Chronic cholecystitis
- diagnosed if an adequate % of bile mixed with radiotracer does not exit the gallbladder after administration of CCK
- Biliary atresia in neonates
- Bile leak
- if tracer spreads outside the biliary system, it provides direct evidence of a biliary leak
- Biliary obstruction
- tracer dose is held up before it can progress into the duodenum
- Confirmation of biliary dilatation
- may be useful in imaging choledochal cysts
With the exception of biliary atresia (and possibly chronic cholecystitis), cholescintigraphy is rarely a first line imaging modality but is often used as a problem-solving tool.
HIDA scan side effects
A HIDA scan carries only a few risks. They include:
- Allergic reaction to medications containing radioactive tracers used for the scan
- Bruising at the injection site
- Radiation exposure, which is small. The amount of radiation is small (less than that of a regular x-ray). It is almost all gone from the body within 1 or 2 days. Your risk from radiation may increase if you have a lot of scans.
- There is a small risk to pregnant or nursing mothers. Unless it is absolutely necessary, HIDA scan will be delayed until you are no longer pregnant or nursing.
Tell your doctor if there’s a chance you could be pregnant or if you’re breast-feeding. In most cases, nuclear medicine tests, such as the HIDA scan, aren’t performed in pregnant women because of potential harm to the fetus.
Is a HIDA scan painful?
No. There is normally no pain during the scan. You will feel a sharp prick from the needle when the tracer is injected into the vein. You might feel pressure or a cold sensation while the radioactive tracer is injected into the vein in your arm. The site may be sore after the injection.
How long does a HIDA scan take?
Images will be taken every 5 to 15 minutes. Most of the time, the HIDA scan test takes about 1 hour, but it can take up to 4 hours.
Liver anatomy
A fibrous capsule encloses the liver, and ligaments divide the organ into a large right lobe and a smaller left lobe (Figure 2).
The liver also has two minor lobes, the quadrate lobe and the caudate lobe. Each lobe is separated into many tiny hepatic lobules, the liver’s functional units (Figure 3). A lobule consists of many hepatic cells radiating outward from a central vein. Blood-filled channels called hepatic sinusoids separate platelike groups of these cells from each other. Blood from the digestive tract, carried in the hepatic portal vein, brings newly absorbed nutrients into the sinusoids and nourishes the hepatic cells.
Large phagocytic macrophages called Kupffer cells are fixed to the inner linings of the hepatic sinusoids. They remove bacteria or other foreign particles that enter the blood through the intestinal wall, and are brought to the liver via the hepatic portal vein. Blood passes from these sinusoids into the central veins of the hepatic lobules and exits the liver via the hepatic veins.
Within the hepatic lobules are many fine bile canaliculi, which carry secretions from hepatic cells to bile ductules. The ductules of neighboring lobules converge to ultimately form the hepatic ducts. These ducts merge, in turn, to form the common hepatic duct.
Figure 1. Location of the human liver
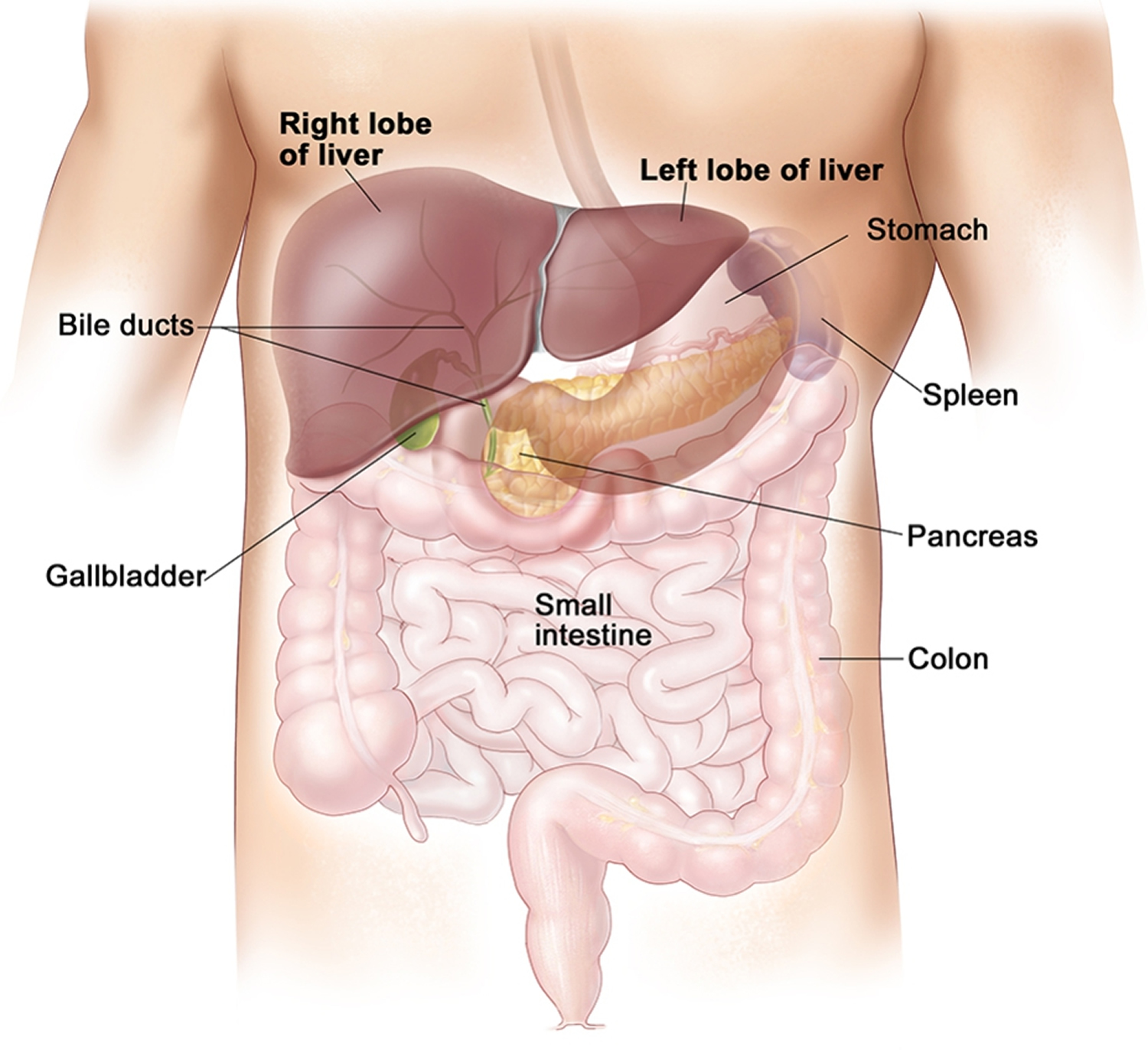
Figure 2. Liver anatomy
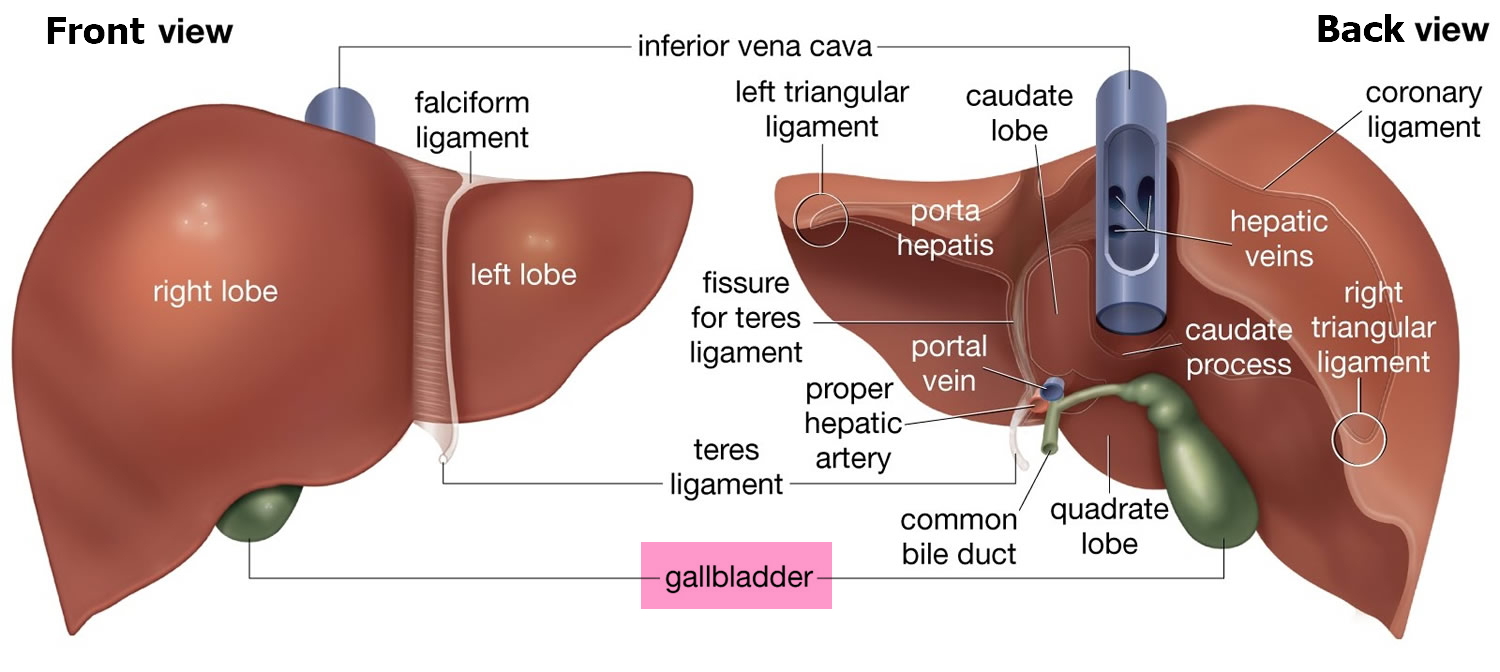
Figure 3. Liver lobule
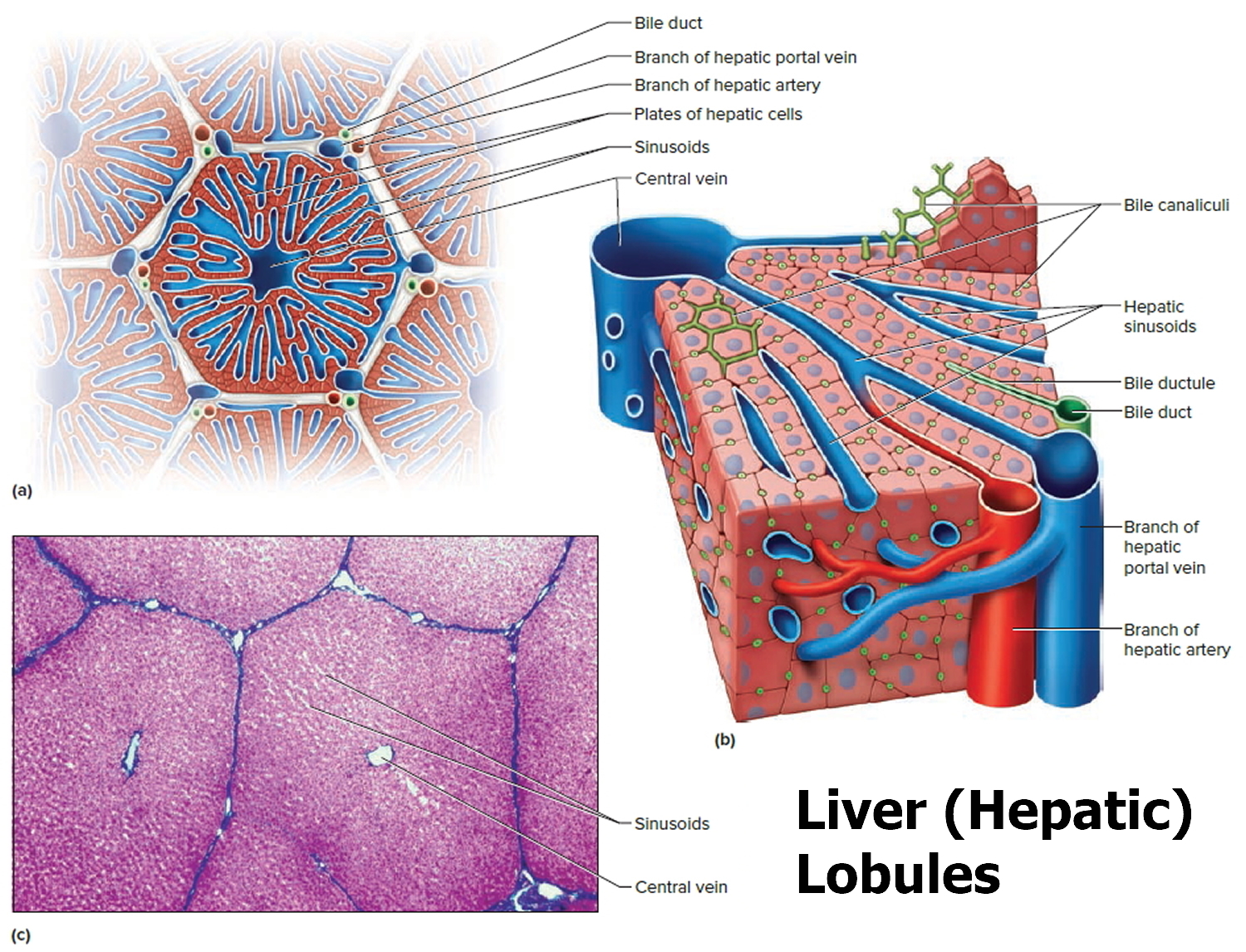
Note: (a) Cross section of a hepatic lobule. (b) Enlarged longitudinal section of a hepatic lobule. (c) Light micrograph of hepatic lobules in cross section.
Figure 4. Gallbladder location
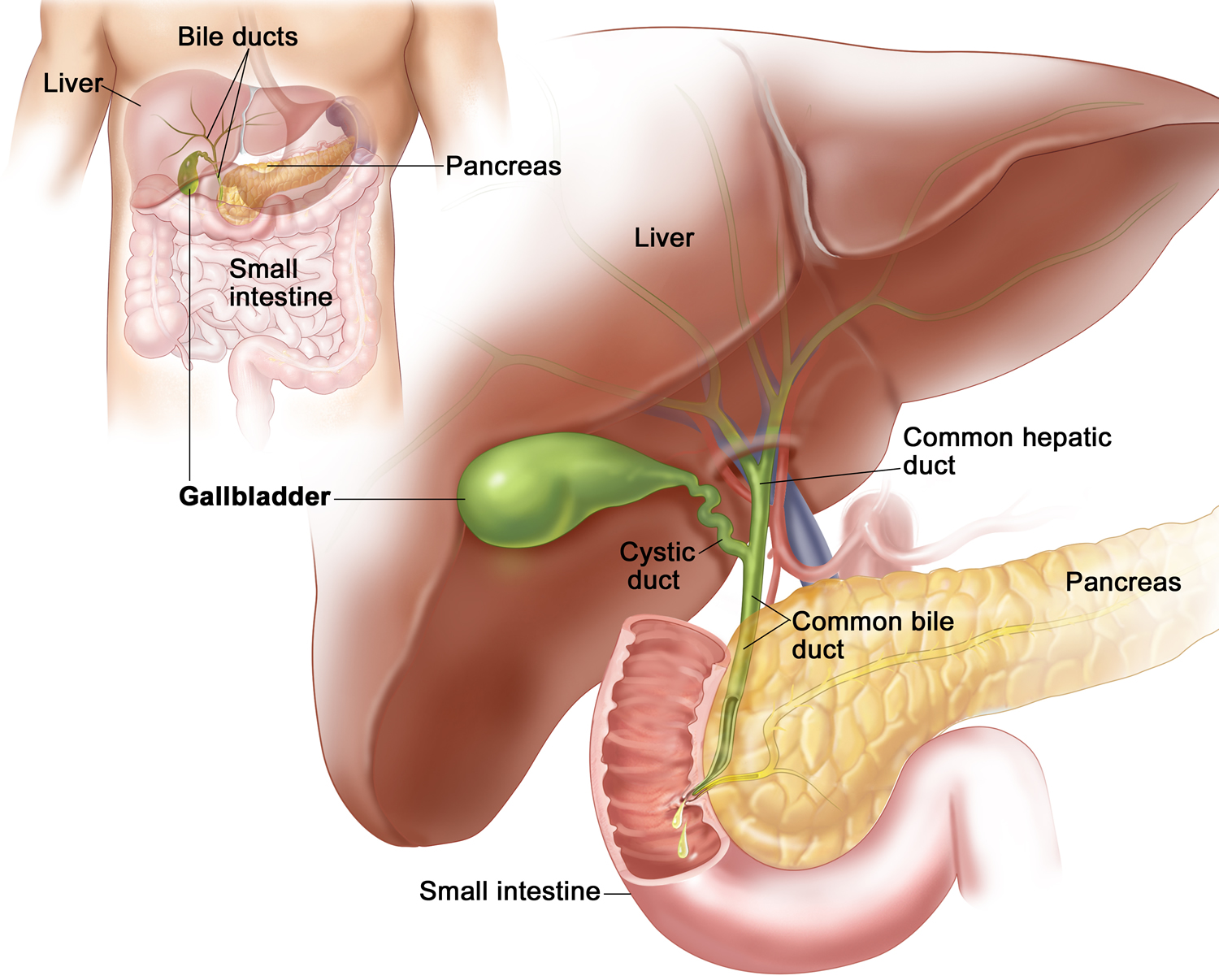
Figure 5. Gallbladder anatomy
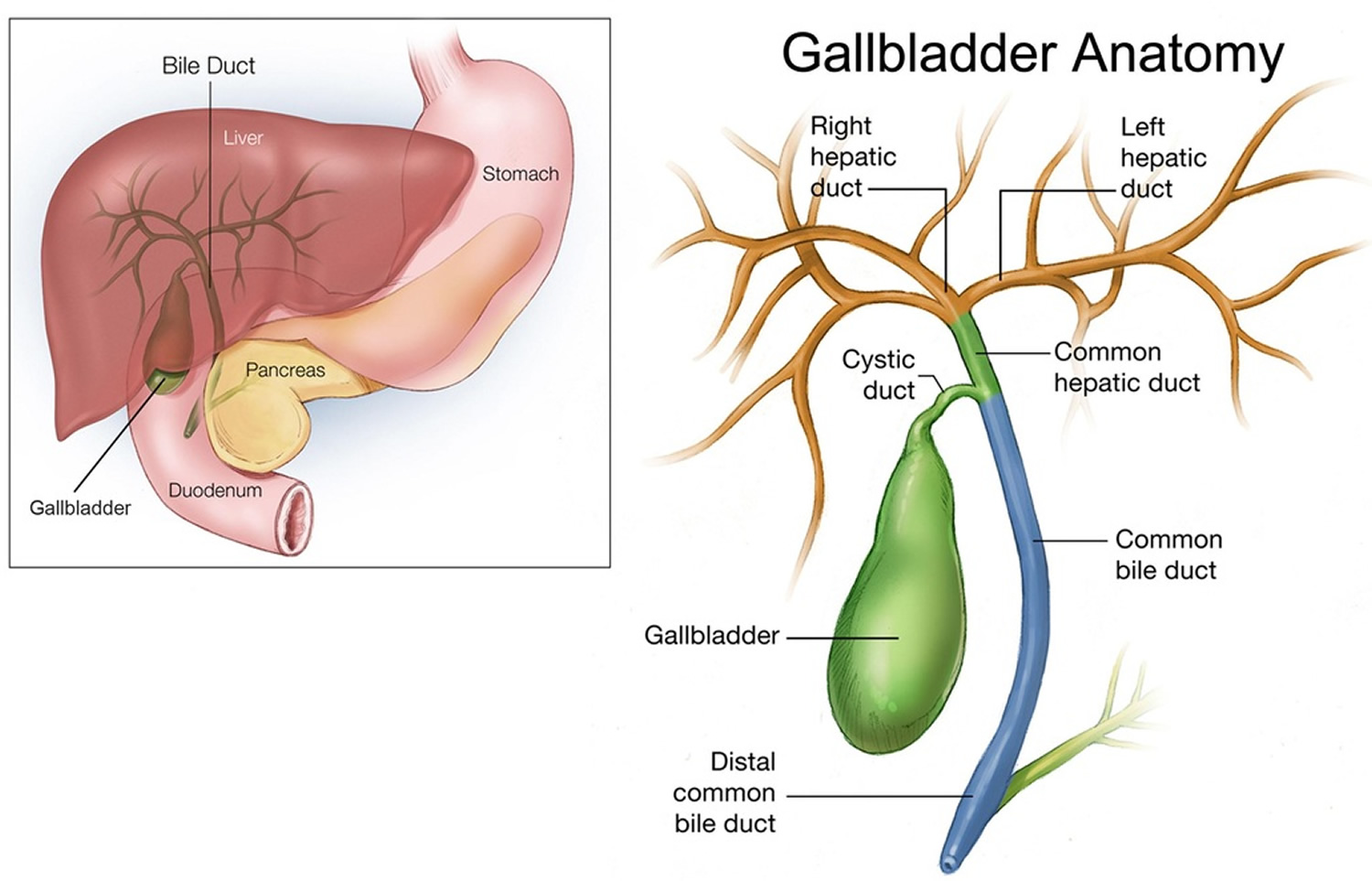
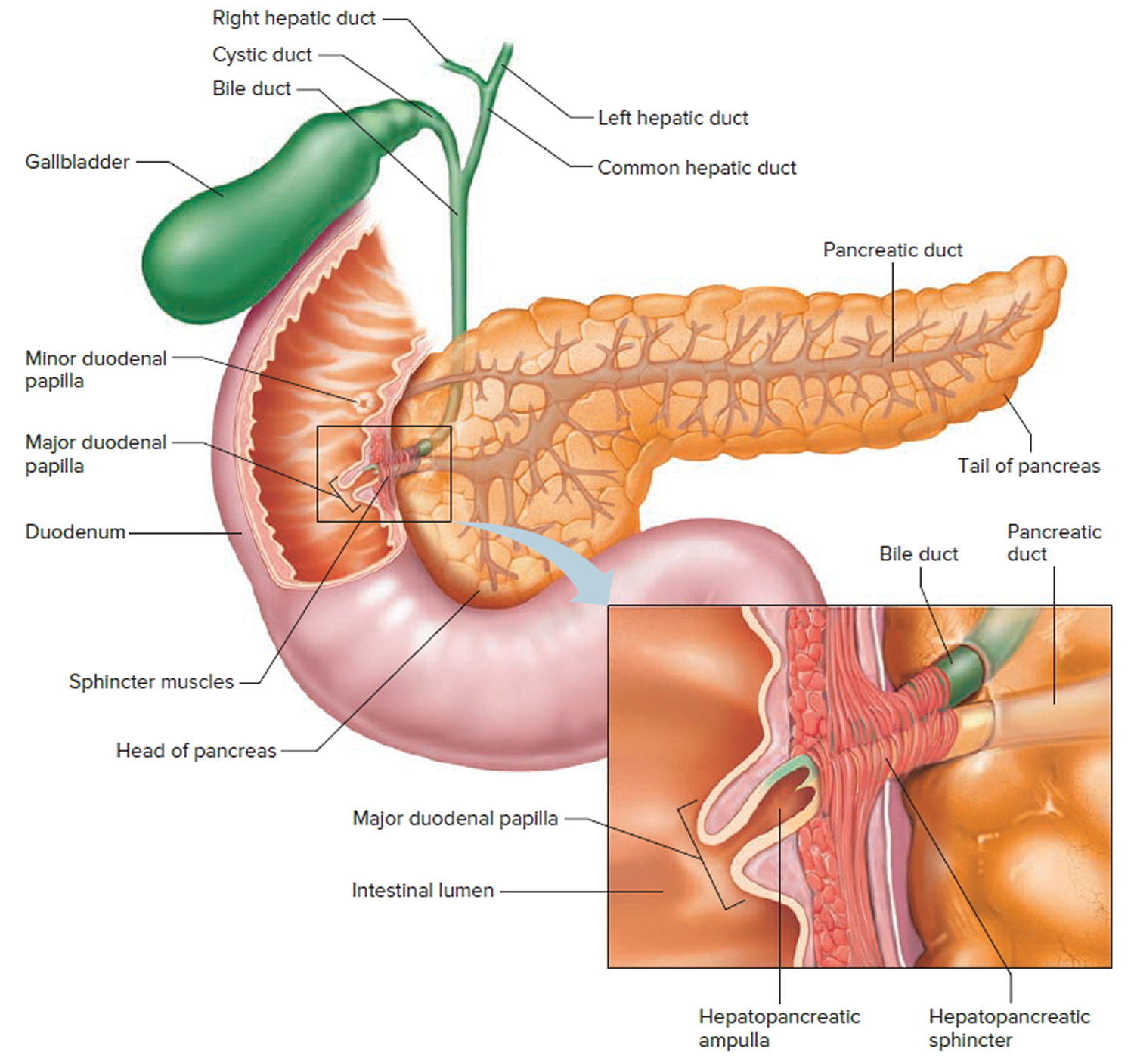
Figure 6. The common bile duct is closely associated with the pancreatic duct and the duodenum
HIDA scan Results
To make a diagnosis, your doctor will consider your signs and symptoms and other test results with the results of your HIDA scan.
Results of a HIDA scan include:
- Normal. The radioactive tracer moved freely with the bile from your liver into your gallbladder and small intestine. A normal result means that the gallbladder is visualized within 1 hour of the injection and the tracer is in the small intestine.
- Slow movement of radioactive tracer. Slow movement of the tracer might indicate a blockage or obstruction, or a problem in liver function.
- No radioactive tracer seen in the gallbladder (gallbladder not visualized). Inability to see the radioactive tracer in your gallbladder might indicate acute inflammation (acute cholecystitis). If the gallbladder is not visualized within 4 hours after the injection it indicates that there is either cholecystitis or cystic duct obstruction. HIDA scan for acute cholecystitis has a sensitivity of 97%, Specificity of 94%.
- Abnormally low gallbladder ejection fraction. The amount of tracer leaving your gallbladder is low after you’ve been given a drug to make it empty, which might indicate chronic inflammation (chronic cholecystitis).
- Radioactive tracer detected in other areas. Radioactive tracer found outside of your biliary system might indicate a leak.
- Tracer not visualized in intestines means common bile duct obstruction. If the radioactive tracer moves through bile ducts very slowly, this may indicate a blockage or obstruction. Or it may indicate a problem in liver.
Figure 7. Normal HIDA scan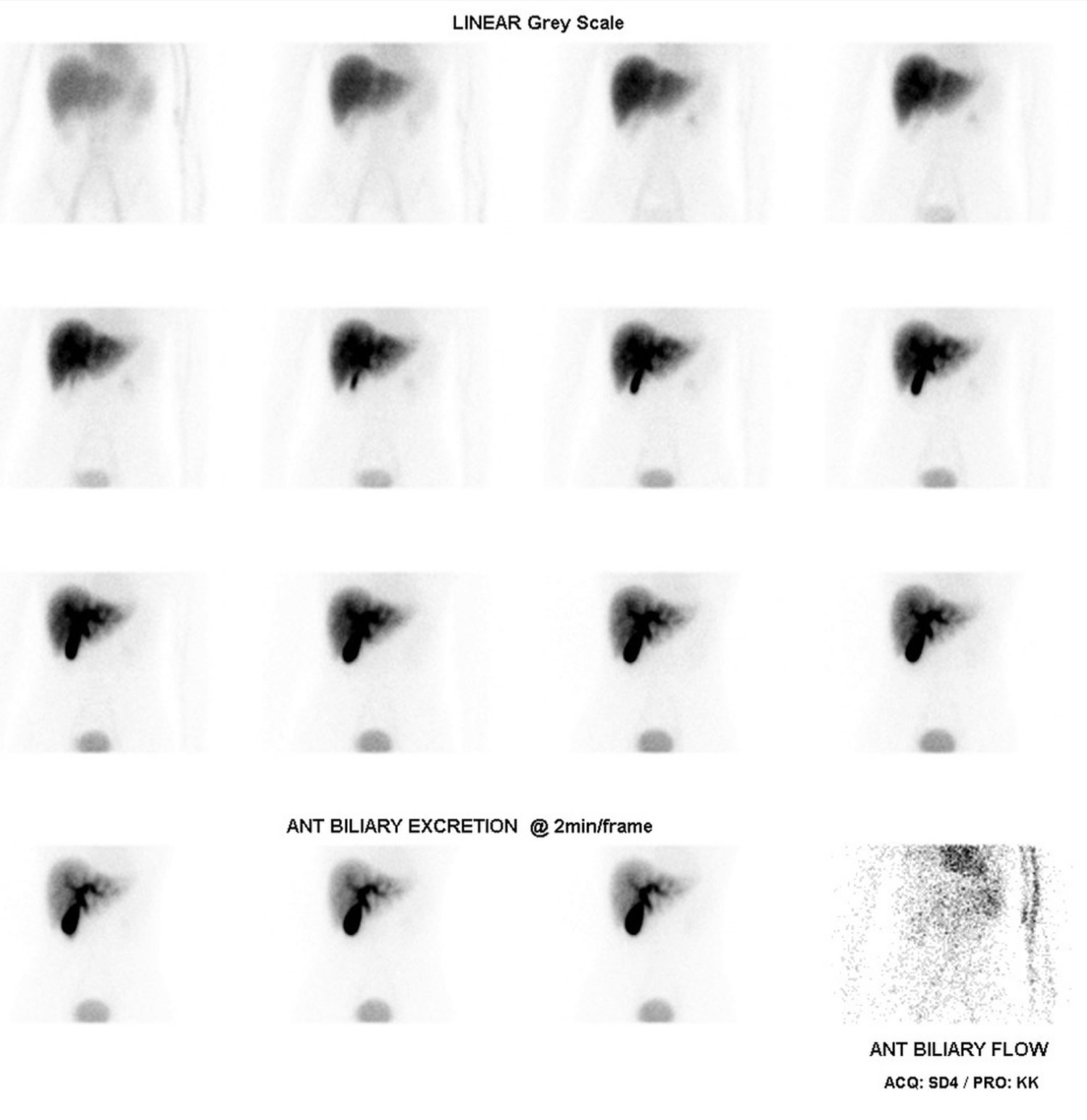 Footnotes: Normal HIDA scan performed with 200 mBq of Tc-99m DISIDA given IV and 30 minutes of imaging.
Footnotes: Normal HIDA scan performed with 200 mBq of Tc-99m DISIDA given IV and 30 minutes of imaging.
- Uniform radiotracer activity throughout the liver
- Prompt excretion into the bile ducts
- Radioactivity tracer activity seen in the gallbladder after 10 min
- Ongoing accumulation of radiotracer over the 30 min study.
- Acute cholecystitis and/or cystic duct obstruction can effectively be excluded since there is radiotracer activity in the gallbladder after 10 min and ongoing accumulation over the 30 min study
Figure 8. Normal HIDA scan
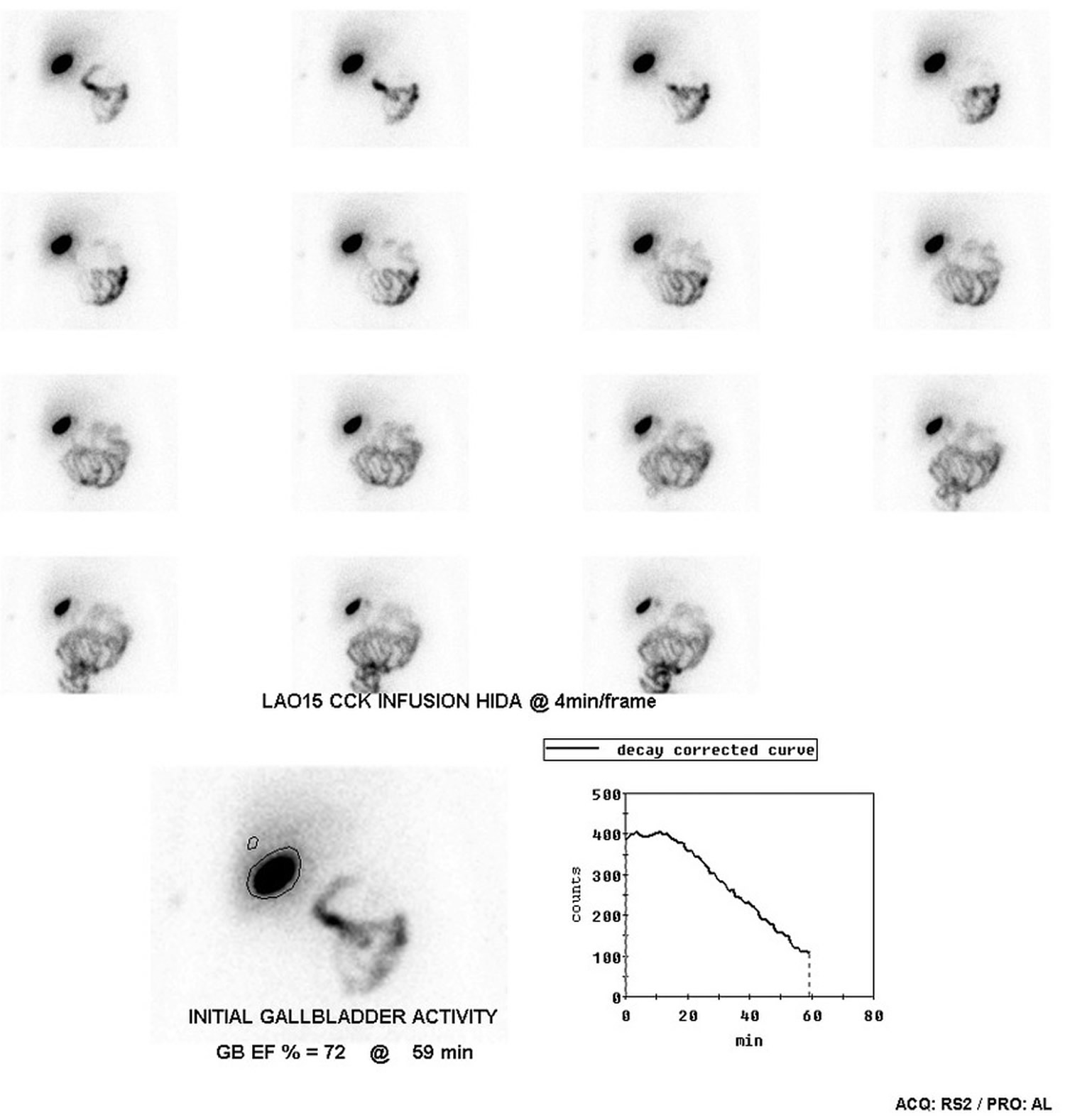
Footnotes: Normal HIDA scan performed with 75 MBq of Tc-99m DISIDA given intravenously, with imaging commenced at 1 hr and an oral fat-rich meal given to stimulate gallbladder contraction. Radiotracer activity in the gallbladder is measured over time as the gallbladder empties through the cystic duct, allowing gallbladder function to be assessed. A normal gallbladder ejection fraction under this protocol is > 33%.
What Abnormal HIDA scan Results Mean
Abnormal HIDA scan results may be due to:
- Abnormal anatomy of the bile system (biliary anomalies)
- Bile duct obstruction
- Bile leaks or abnormal ducts
- Cancer of the hepatobiliary system
- Gallbladder infection (cholecystitis)
- Gallstones
- Infection of the gallbladder, ducts, or liver
- Liver disease
- Transplant rejection (after liver transplant)
Figure 9. HIDA scan of a patient with biliary atresia
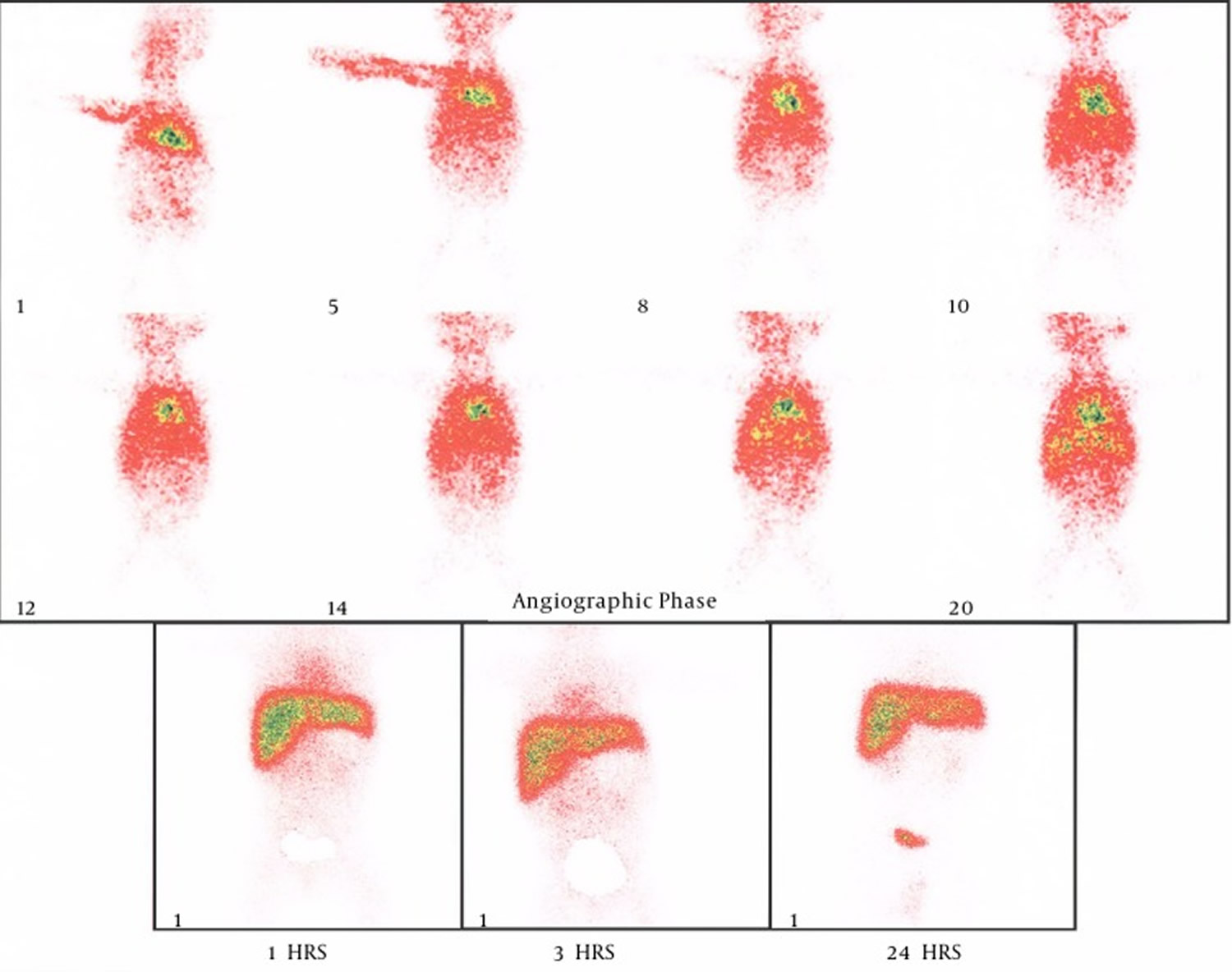
Figure 10. HIDA scan of a patient with acute acalculous cholecystitis – the gallbladder area which doesn’t light up with the radio-tracer.
Figure 11. HIDA scan of a patient with gallbladder agenesis

Figure 12. HIDA scan of a patient with bile leak
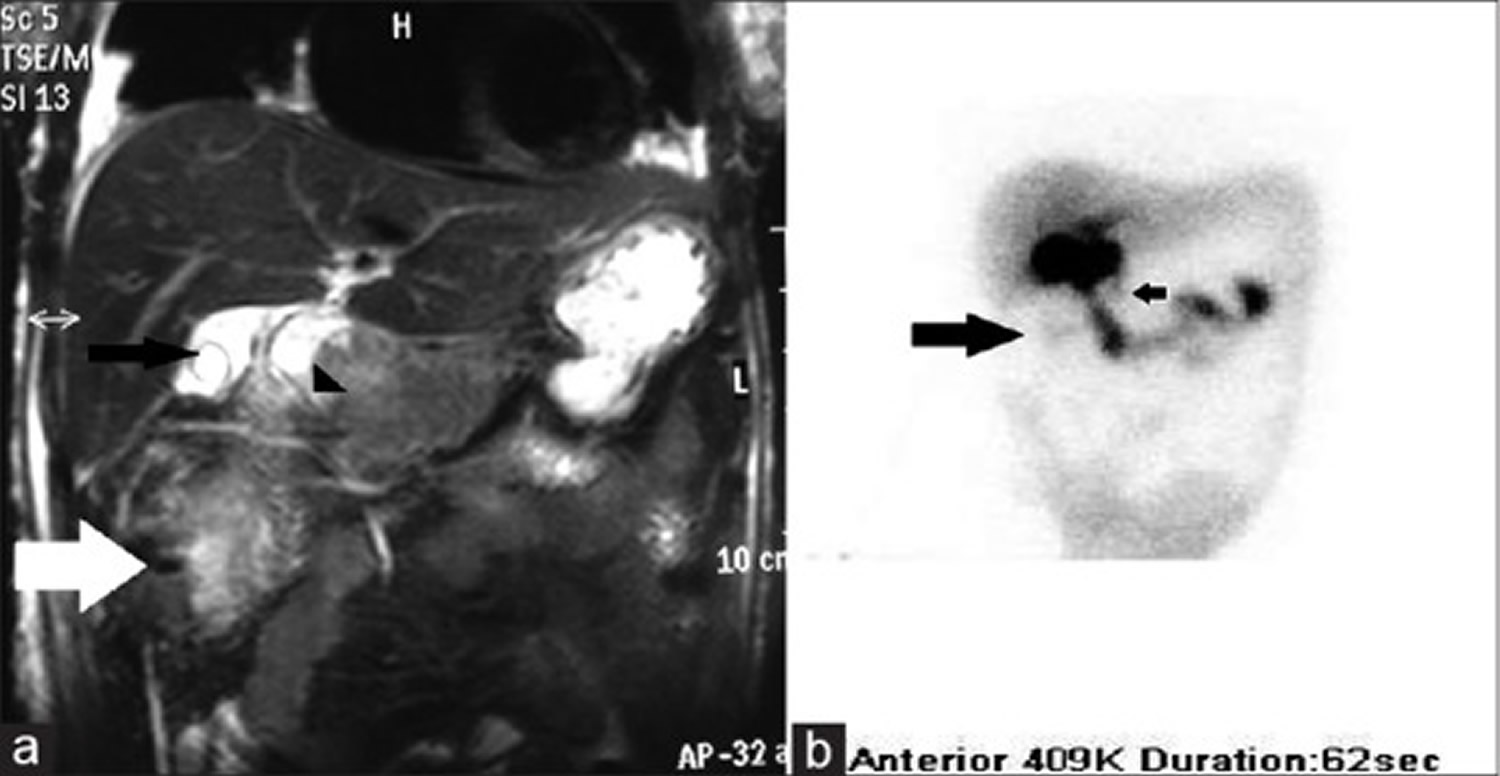
Footnotes: (a) Magnetic resonance cholangiopancreatography and (b) HIDA scan images depicting normal hepatobiliary pathway with unidentified site of leak. (a) Coronal magnetic resonance cholangiopancreatography image of the hepatobiliary system showing fluid collection in the subhepatic region (white arrow), gall bladder with pericholecystic fluid (black arrow) and duodenal cap (arrow head). (b) HIDA scan showing some leak in the subhepatic region (large black arrow) with normal hepatobiliary pathway (small black arrow)
Figure 13. HIDA scan of a patient with gallbladder dysfunction
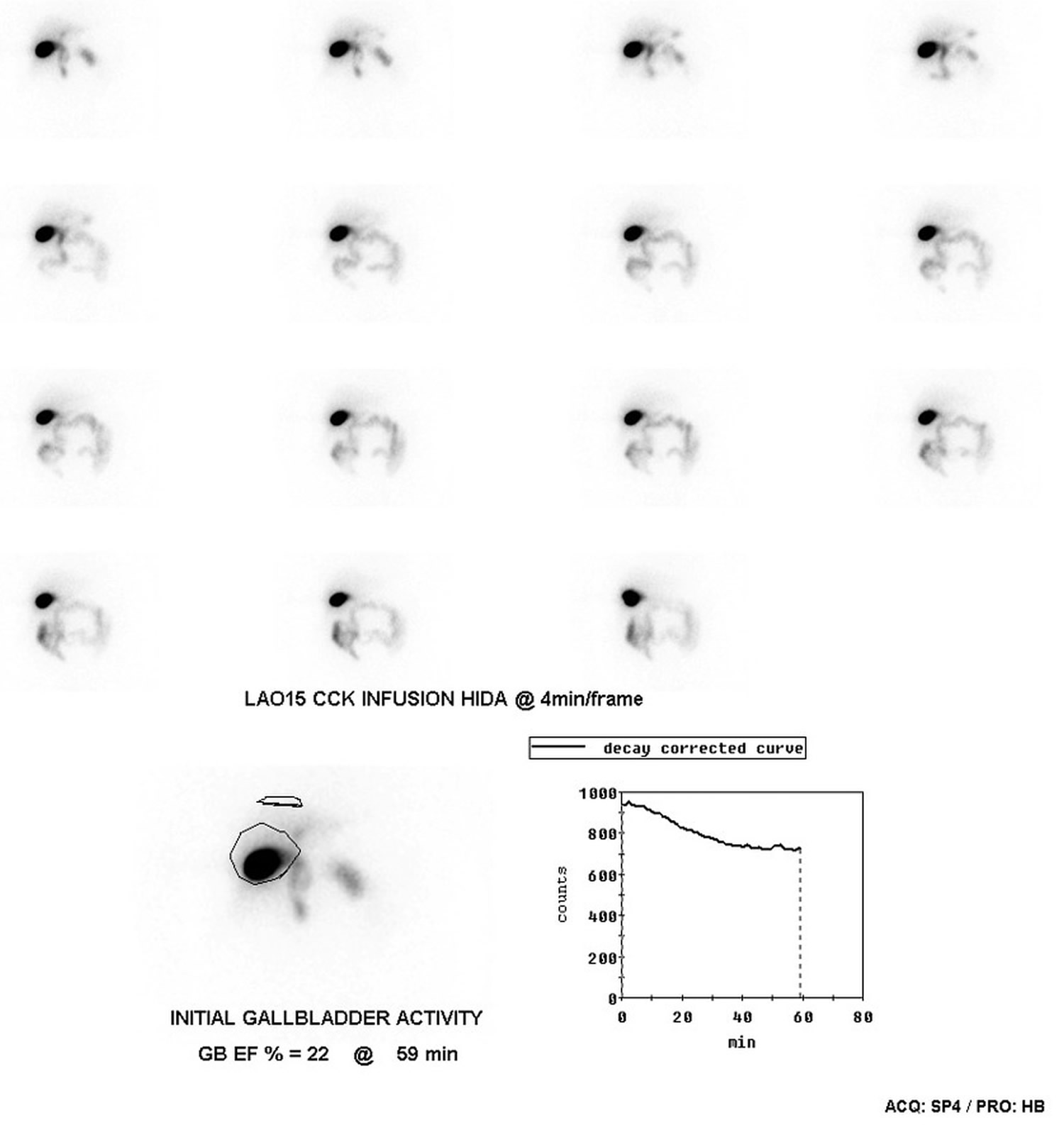
Footnotes: This cholescintigraphy (HIDA) scan was performed with 75 MBq of Tc-99m given IV, with imaging commenced at 1 hr and an oral fat-rich meal given to stimulate gallbladder contraction. Radiotracer activity in the gallbladder is measured over time as the gallbladder empties through the cystic duct, assessing gallbladder function. A normal gallbladder ejection fraction under this protocol is > 33%. The patient in this case proceeded to cholecystectomy. Histopathology revealed patchy, light chronic inflammation with Rokitansky-Aschoff sinus formation.
HIDA scan prep
How you prepare
Food and medications
Your doctor is likely to ask you:
- To fast for 4 hours before your HIDA scan. You might be allowed to drink clear liquids.
- About medications and supplements you take.
Clothing and personal items
You might be asked to:
- Change into a hospital gown
- Leave jewelry and other metal accessories at home or remove them before the procedure
HIDA scan procedure
Your health care team will position you on a table, usually on your back, and inject the radioactive tracer into a vein in your arm. You might feel pressure or a cold sensation while the radioactive tracer is injected. In some cases, you may be given a medicine during this test to see how well your gallbladder squeezes (contracts). The medicine may be injected into the vein.
If the provider cannot see the gallbladder after certain amount of time, you may get an intravenous injection of the drug sincalide (Kinevac), which makes your gallbladder contract and empty. Morphine is another drug sometimes given during a HIDA scan, this can help the radionuclide get into the gallbladder and makes the gallbladder easier to visualize. The morphine may cause you to feel tired after the exam. Otherwise, you may be asked to drink a high-density drink like Boost which will help your gallbladder contract.
A gamma camera is positioned over your abdomen to take pictures of the tracer as it moves through your body. The scanner detects the rays being emitted from the tracer. A computer displays images of where the tracer is found in the organs. Images will be taken every 5 to 15 minutes. This process takes about an hour, during which you’ll need to remain still.
Tell your team if you become uncomfortable. You might be able to lessen the discomfort by taking deep breaths.
On a computer, the radiologist will watch the progress of the radioactive tracer through your body. In some cases, you might need additional imaging within 24 hours if original images aren’t satisfactory.
After the HIDA scan procedure
In most cases, you can go about your day after your scan. The small amount of radioactive tracer will lose its reactivity or pass through your urine and stool over the next day or two. Drink plenty of water to help flush it out of your system.





{kind=link}