Contents
What is Hirschsprung disease
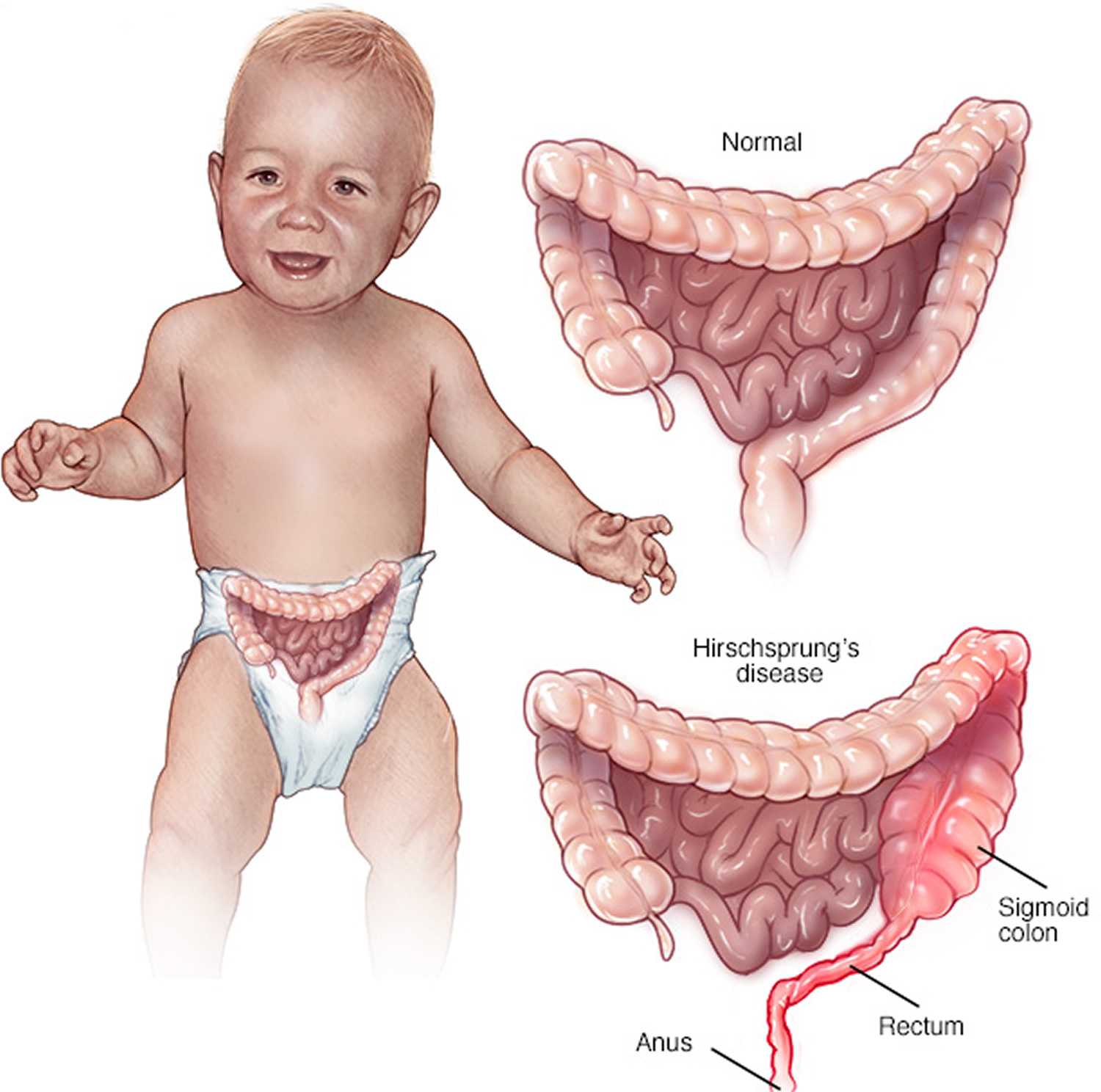
Hirschsprung disease is a birth defect in which nerve cells are missing at the end of a child’s bowel (small and large intestines). During normal embryonic development, neural crest cells migrate to the small and large intestines and establish the enteric nervous system. In Hirschsprung disease, however, they fail to supply the distal parts of the large intestine, leaving the sigmoid colon and rectum (see Figures 1, 2 and 6) without enteric ganglia. However, some children are missing the nerve cells for the entire colon or part of the small intestine.
- In short-segment Hirschsprung disease, nerve cells are missing from the last part of the large intestine.
- In long-segment Hirschsprung disease, nerve cells are missing from most or all of the large intestine and sometimes the last part of the small intestine.
- Rarely, nerve cells are missing in the entire large and small intestine.
In the absence of these ganglia, the sigmoidorectal region lacks motility, constricts permanently, and obstructs the passage of feces. In a child with Hirschsprung disease, stool moves through the bowel until it reaches the part lacking nerve cells. At that point, the stool moves slowly or stops. Feces accumulate and become impacted above the constriction, resulting in megacolon—a massive dilation of the bowel accompanied by abdominal distension and chronic constipation. The most life-threatening complications are colonic gangrene, perforation of the bowel, and bacterial infection of the peritoneum (peritonitis). The treatment of choice is surgical removal of the affected segment and attachment of the healthy colon directly to the anal canal.
Hirschsprung disease is usually evident even in the newborn, which fails to have its first expected bowel movement. Hirschsprung disease affects four times as many infant boys as girls, and although its incidence in the general population is about 1 in 5,000 live births. Children with Down syndrome and other medical problems, such as congenital heart defects, are at much greater risk. For example, about one in 100 children with Down syndrome also has Hirschsprung disease.
Hirschsprung disease is congenital, or present at birth; however, symptoms may or may not be obvious at birth. If you have a child with Hirschsprung disease, your chances of having more children with Hirschsprung disease are greater than people who don’t have a child with Hirschsprung disease. Also, if a parent has Hirschsprung disease, the chance of their child having Hirschsprung disease is higher. Talk with your doctor to learn more.
Large intestine
The large intestine extends from the distal end of the ileum to the anus, at birth the large intestine is about 2 feet long and in adults it’s approximately 1.5 m in adults (5 ft) long and 6.5 cm (2.5 in.) in diameter. The large intestine is named for its relatively large diameter, not its length. The large intestine absorbs fluids and salts from the gut contents, thus forming feces. The large intestine consists of the cecum, appendix, colon, rectum, and anal canal.
Beginning in the right groin as the cecum, with its associated appendix, the large intestine continues upward as the ascending colon through the right flank and into the right hypochondrium. The ascending colon begins at the ileocecal valve and passes up the right side of the abdominal cavity. It makes a 90° turn at the right colic (hepatic) flexure, near the right lobe of the liver, and crosses the abdomen as the transverse colon to the left hypochondrium. At this position, just below the spleen, the large intestine bends downward, forming the left colic flexure (splenic flexure) and continues as the descending colon through the left flank and into the left groin. Ascending, transverse, and descending colons thus form a squarish, three-sided frame around the small intestine.
The cecum is a blind pouch in the lower right abdominal quadrant inferior to the ileocecal valve. Attached to its lower end is the appendix, a blind tube 2 to 7 cm long. The appendix is densely populated with lymphocytes and is a significant source of immune cells.
Figure 1. Large intestine
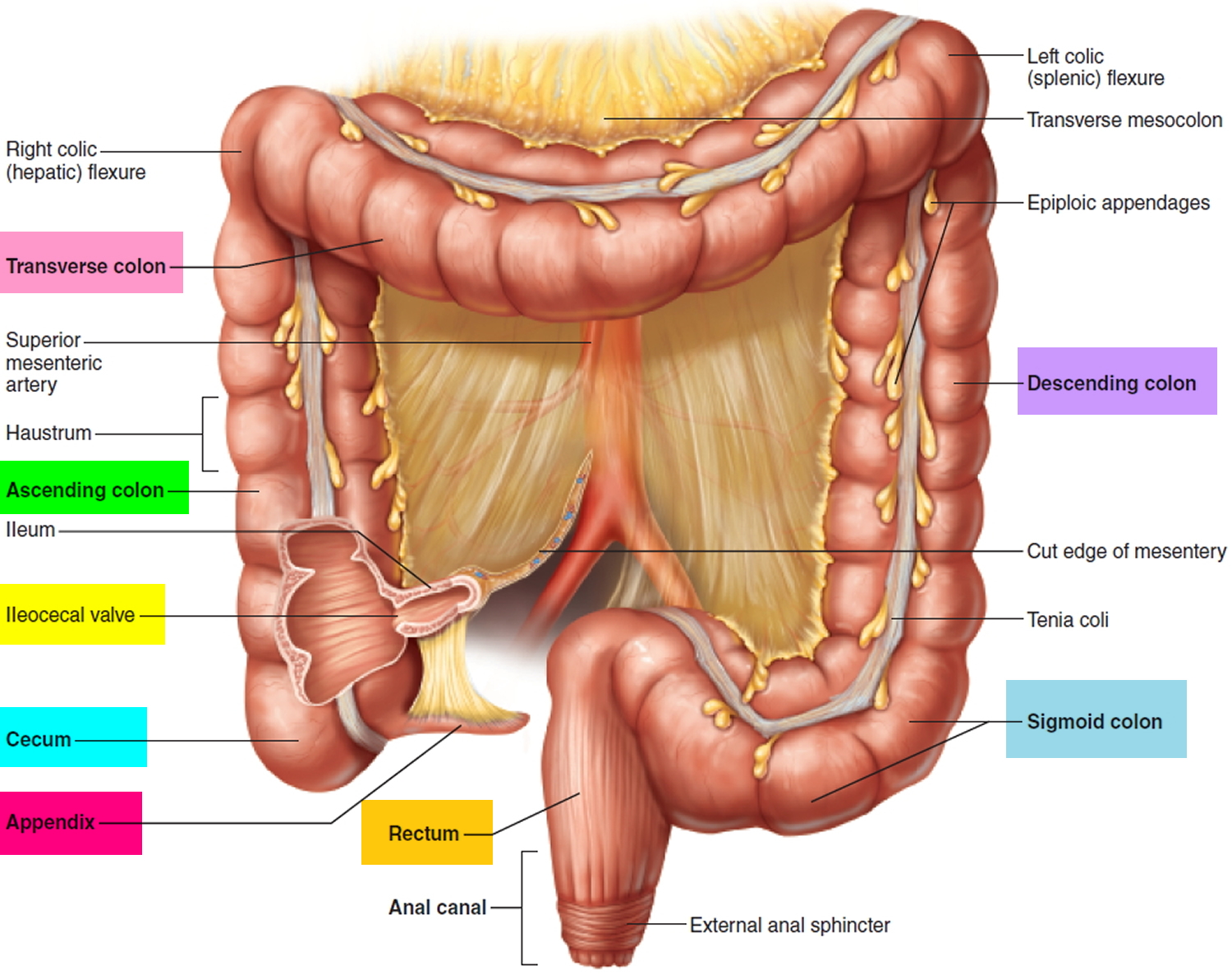 Figure 2. Rectum and Anal canal
Figure 2. Rectum and Anal canal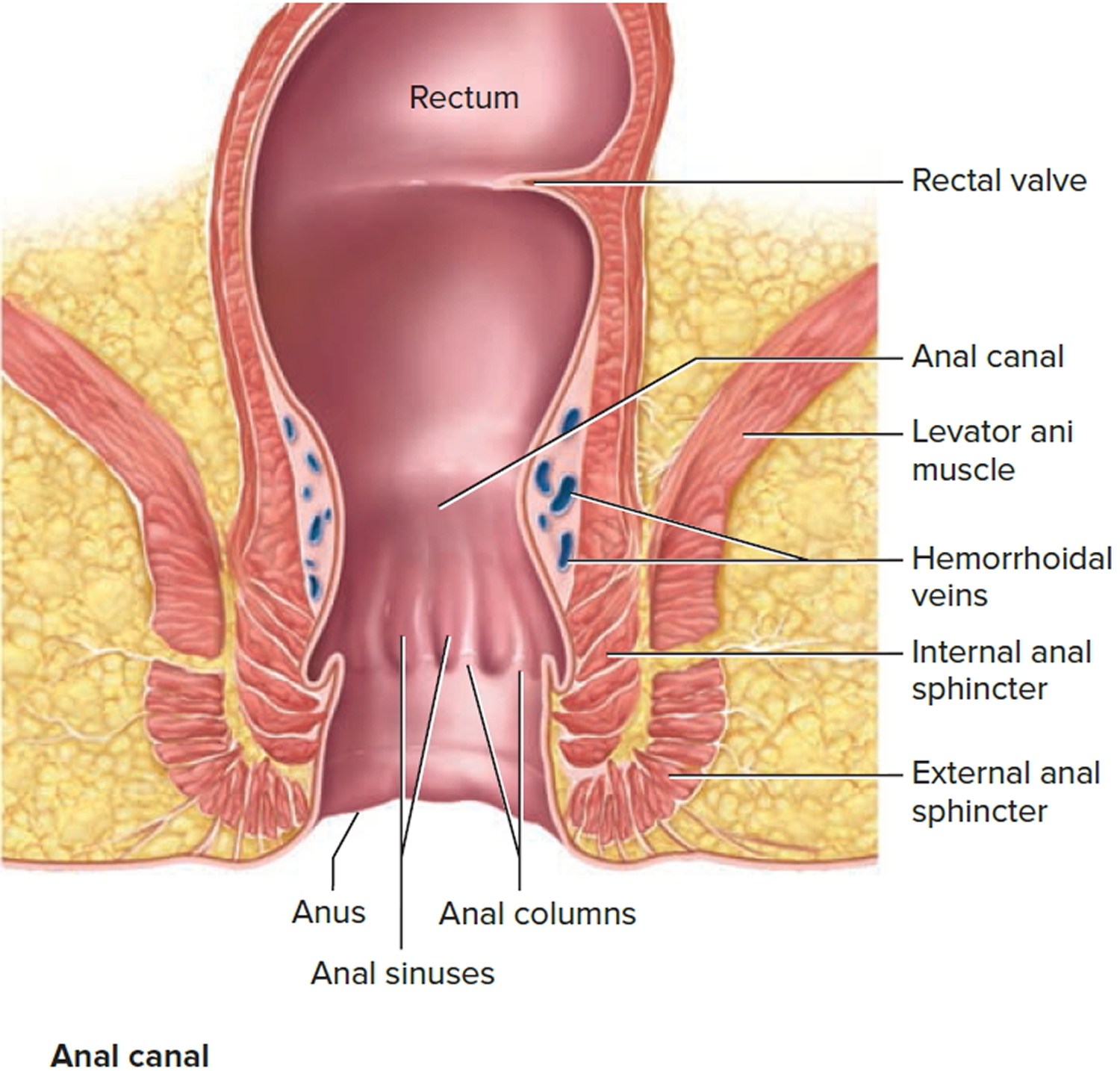
Figure 3. Large intestine location
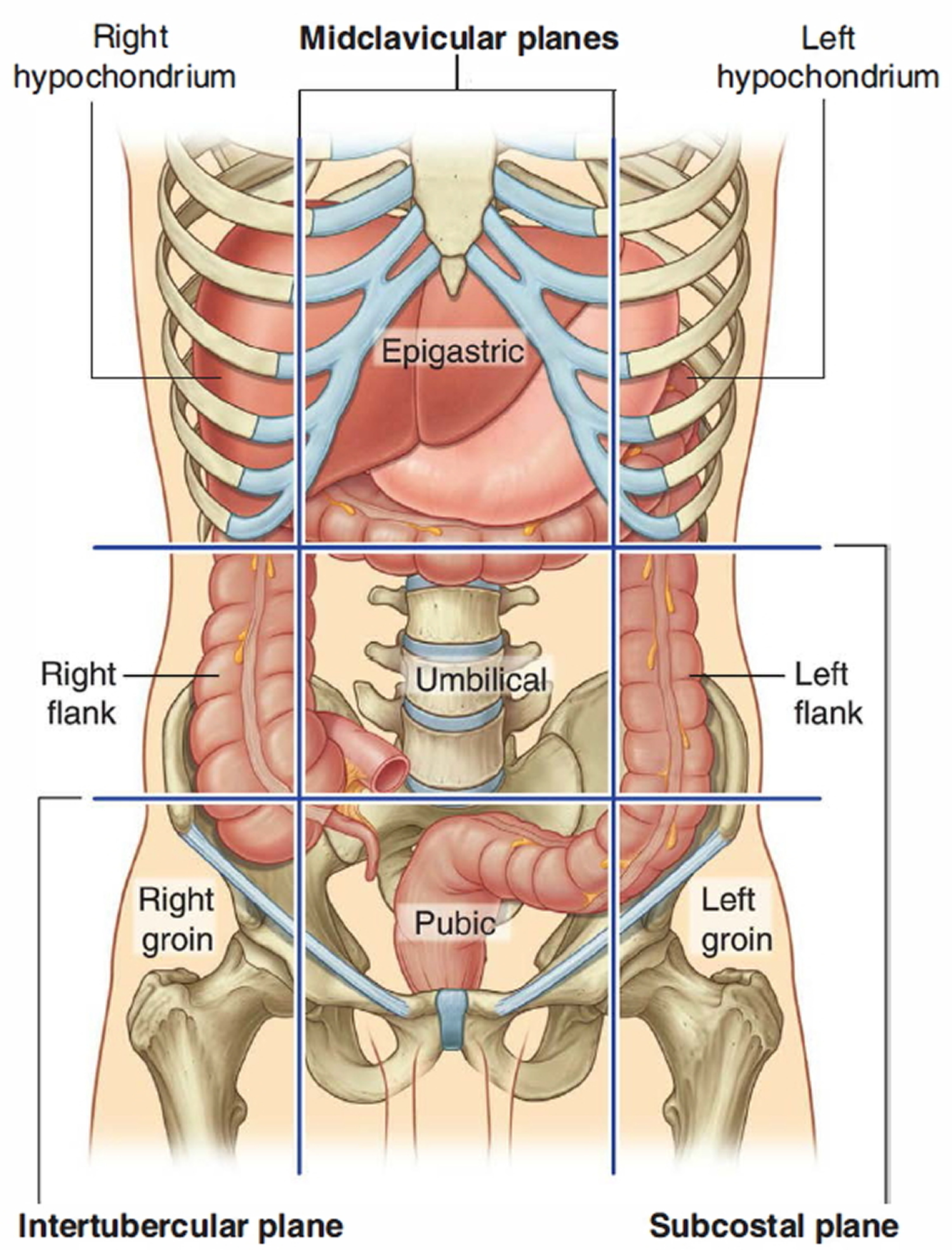
Figure 4. Large intestine and small intestine
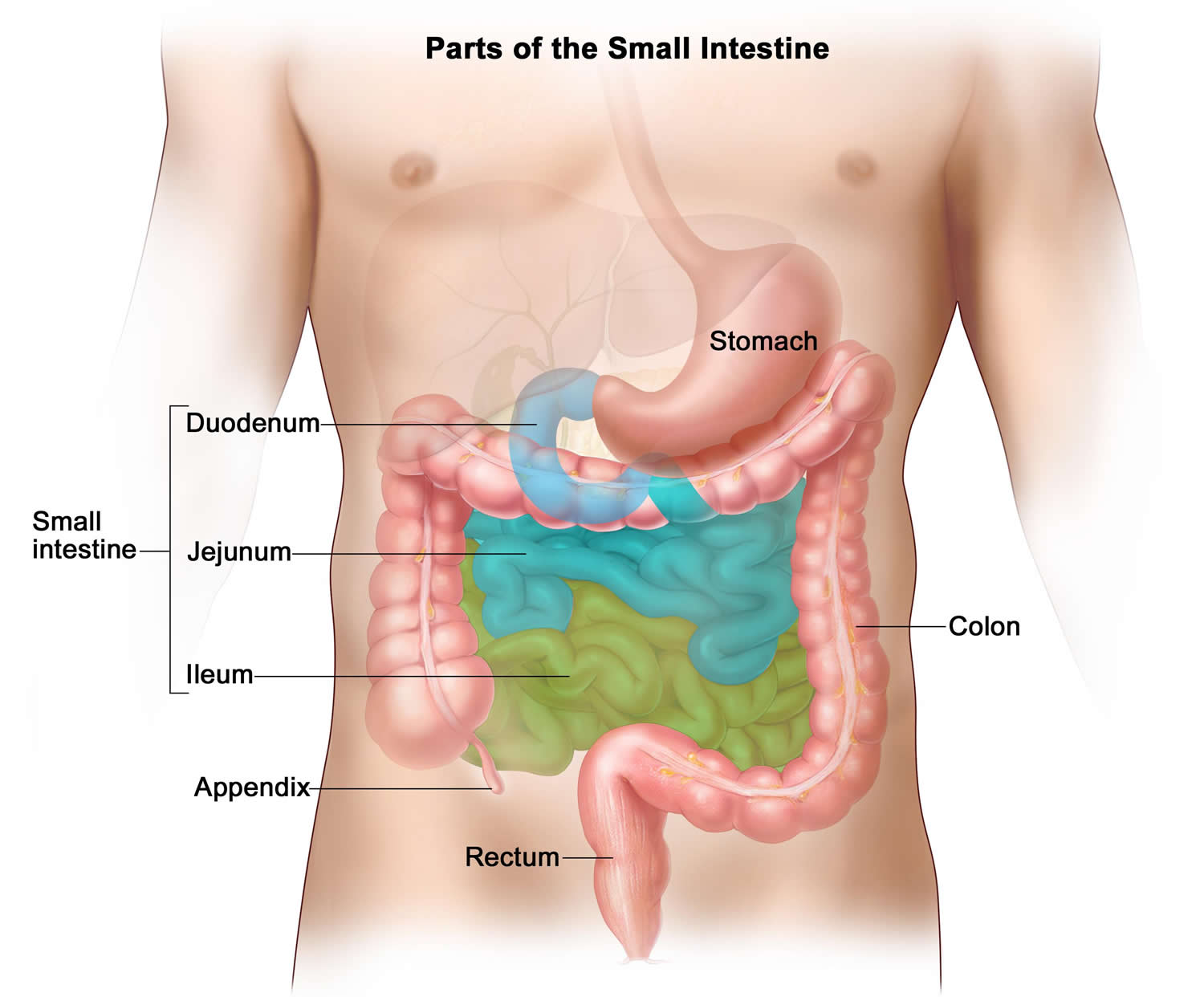
Figure 5. Large intestine anatomy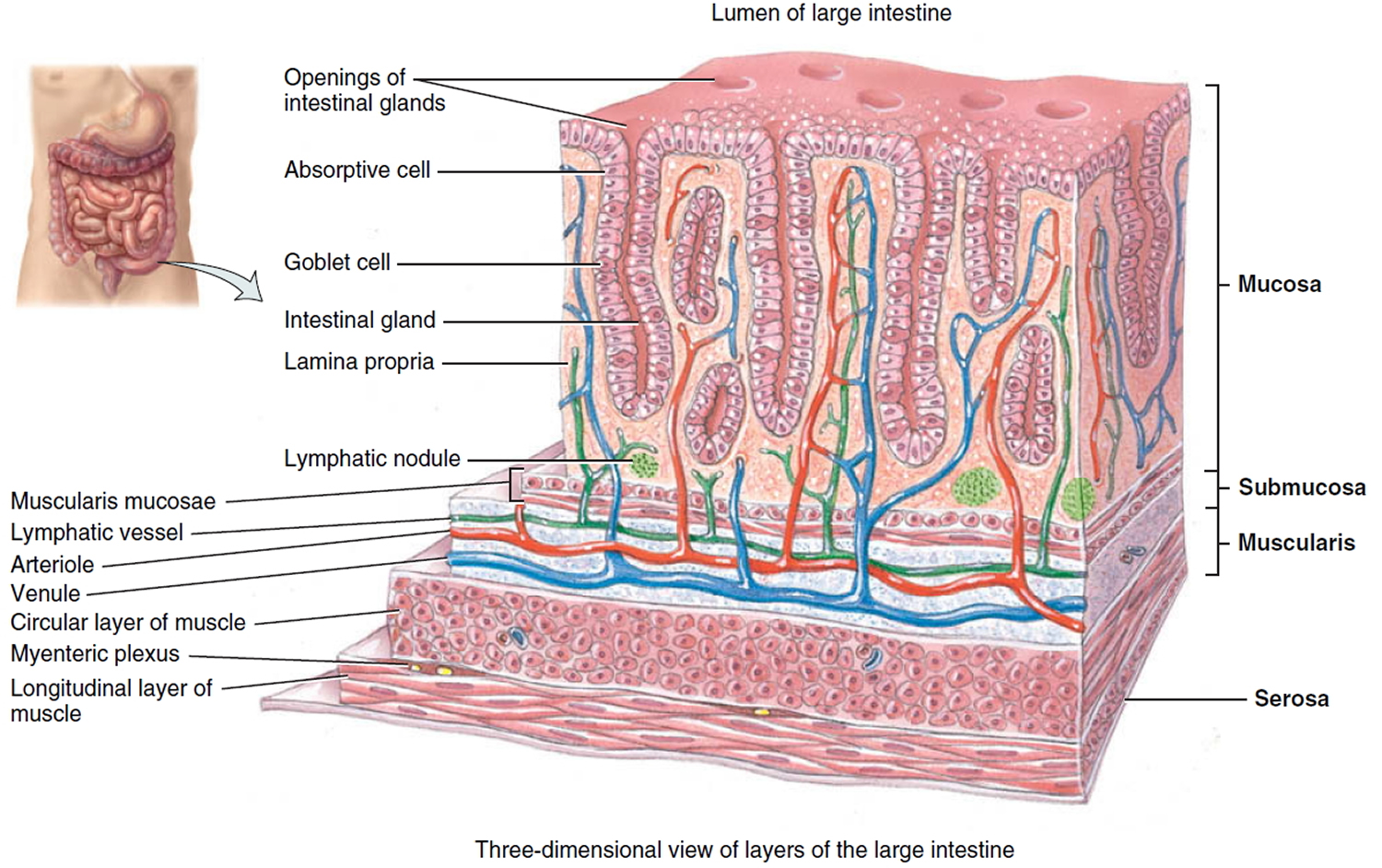 Figure 6. Hirschsprung’s disease
Figure 6. Hirschsprung’s disease
Hirschsprung disease causes
During early development of the baby in the mother’s womb, nerve cells stop growing toward the end of a child’s bowel causing Hirschsprung disease. Most of these cells start at the beginning of the bowel and grow toward the end. Hirschsprung disease occurs when these cells do not reach the end of a child’s bowel. Scientists know that genetic defects can increase the chance of a child developing Hirschsprung disease. However, no testing exists that can diagnose a child while the mother is pregnant. Researchers are studying if the mother’s health history or lifestyle during pregnancy increases the chance of her baby developing Hirschsprung disease.
Hirschsprung disease signs and symptoms
The main signs and symptoms of Hirschsprung disease are constipation or intestinal obstruction, usually appearing shortly after birth. Typically, the most obvious sign is a newborn’s failure to have a bowel movement within 48 hours after birth. Many healthy infants and children have difficulty passing stool or infrequent bowel movements. However, unlike healthy children and infants, kids with Hirschsprung disease typically do not respond to constipation medicines given by mouth. Most often, an infant or a child with Hirschsprung disease will have other symptoms, including
- growth failure
- swelling of the abdomen, or belly
- unexplained fever
- vomiting
The symptoms can vary; however, how they vary does not depend on how much of the intestine is missing nerve cells. No matter where in the intestine the nerve cells are missing, once the stool reaches this area, the blockage forms and the child develops symptoms.
Symptoms in Newborns
An early symptom in some newborns is failure to have a first bowel movement within 48 hours after birth. Other symptoms may include:
- green or brown vomit
- explosive stools after a doctor inserts a finger into the newborn’s rectum
- swelling of the abdomen
- diarrhea, often with blood
Symptoms in Toddlers and Older Children
Symptoms of Hirschsprung disease in toddlers and older children may include:
- not being able to pass stools without enemas or suppositories. An enema involves flushing liquid into the child’s anus using a special wash bottle. A suppository is a pill placed into the child’s rectum.
- swelling of the abdomen.
- diarrhea, often with blood.
- slow growth.
Hirschsprung’s disease complications
Children who have Hirschsprung’s disease are prone to a serious intestinal infection called enterocolitis.
Enterocolitis can be life-threatening. It’s treated in the hospital with colon cleaning and antibiotics.
Hirschsprung disease diagnosis
A doctor will know if your child has Hirschsprung disease based on:
- a physical exam
- a medical and family history
- symptoms
- test results
If your doctor suspects Hirschsprung disease, he or she may refer your child to a pediatric gastroenterologist—a doctor who specializes in digestive diseases in children—for additional evaluation.
Physical Exam
During a physical exam, a doctor usually:
- reviews your child’s height and weight
- examines your child’s abdomen for swelling and examines his or her body for signs of poor nutrition
- uses a stethoscope to listen to sounds within abdomen
- taps on specific areas of your child’s body
- performs a rectal exam—explosive stool after a rectal exam may be a sign of Hirschsprung disease
Medical and Family History
A doctor will ask you to provide your child’s medical and family history to help diagnose Hirschsprung disease. The doctor will ask questions about your child’s bowel movements. The doctor will also ask about vomiting, swelling of the abdomen, and unexplained fever. The doctor is less likely to diagnose Hirschsprung disease if problems with bowel movements began after 1 year of age.
Medical Tests
A doctor who suspects Hirschsprung disease will do one or more of the following tests:
- Rectal biopsy. A rectal biopsy is a procedure that involves taking a small piece of tissue from the rectum for examination with a microscope. The doctor can perform two types of procedures:
- a rectal “suction” biopsy. During this biopsy, a pediatric gastroenterologist or a pediatric surgeon will insert a small instrument into the child’s anus and remove a small piece of tissue from the lining of his or her rectum. The biopsy is not painful and babies may even fall asleep during the procedure. In most cases, doctors do not use pain medicine or anesthesia. However, for older children doctors sometimes will use medicine to relieve anxiety or reduce the memory of the test.
- a “full thickness” rectal biopsy. A pediatric surgeon performs this procedure, in which he or she will remove a thicker piece of tissue. The child will receive anesthesia.
A doctor will examine the tissue under a microscope. The rectal biopsy is the best test to diagnose or rule out Hirschsprung disease.
- Abdominal x-ray. An x-ray is a picture created by using radiation and recorded on film or on a computer. The amount of radiation is small. An x-ray technician performs the x-ray at a hospital or an outpatient center, and a radiologist—a doctor who specializes in medical imaging—interprets the images. The child does not need anesthesia. The child will lie on a table or stand during the x-ray. The technician may ask the child to change positions for additional pictures. An x-ray of the abdomen may show intestinal obstruction.
- Anorectal Manometry. Anorectal manometry is a test that uses pressure sensors and balloons to measure how well the child’s rectum is working. A doctor performs anorectal manometry in a hospital. During the procedure, the doctor inflates a small balloon inside the child’s rectum. Normally, the child’s rectal muscles will relax. If his or her muscles don’t relax, the doctor may suspect Hirschsprung disease.
- Lower GI series. A lower GI series is an x-ray exam that doctors use to look at the large intestine. An x-ray technician and a radiologist perform the test at a hospital or an outpatient center, and a radiologist interprets the images. A child does not need anesthesia and does not need a bowel prep for the test.
For the test, the child will lie on a table while the radiologist inserts a flexible tube into the child’s anus. The radiologist fills the child’s large intestine with barium or another contrast material. A technician performs this test on newborns, toddlers, and older children. A lower GI series can show changes in the bowel and help doctors diagnose obstructions.
In most cases, doctors diagnose Hirschsprung disease in infancy; however, sometimes doctors diagnose Hirschsprung disease in older children.
Hirschsprung disease treatment
All children with Hirschsprung’s disease will need surgery.
As they wait for surgery, they may need to:
- stop having milk feeds and instead be given fluids directly into a vein
- have a tube passed through their nose and into their stomach to drain away any fluid and air collecting in it
- have regular bowel washouts, where a thin tube is inserted into their bottom and warm salt water is used to soften and flush out the trapped stools
- take antibiotics if they have enterocolitis
Your child may need to stay in hospital during this time, or you may be able to look after them at home. Your doctor will advise you about this.
Hirschsprung disease surgery
Hirschsprung disease is a life-threatening illness, and treatment requires surgery. Children who have surgery for Hirschsprung disease most often feel better after surgery. If growth was slow because of Hirschsprung disease, growth typically improves after surgery.
For treatment, a pediatric surgeon will perform a pull-through procedure or an ostomy surgery. During either procedure, the surgeon may remove all or part of the colon, called a colectomy.
Pull-through Procedure
During a pull-through procedure, a surgeon removes the part of the large intestine that is missing nerve cells and connects the healthy part to the anus. A surgeon most often does a pull-through procedure soon after diagnosis.
If your child isn’t well enough to have this procedure – for example, because they have enterocolitis or a severe blockage – they may have it in two stages.
A few days after birth, the surgeon will divert the bowel through a temporary opening (stoma) made in the tummy. This procedure is called a colostomy formation.
Stools will pass directly out of the opening into a pouch worn on your child’s body until they’re well enough to have another procedure to remove the affected section of bowel, close the opening, and join the healthy sections of bowel together. This is usually done at around three months of age.
These procedures can be done using either:
- laparoscopic (keyhole) surgery – this involves inserting surgical instruments through tiny cuts
- open surgery – where a larger cut is made in your child’s tummy
Speak to your surgeon about the best option for your child.
Risks of surgery
No surgery is risk-free. There’s a small chance of:
- bleeding during or after the operation
- the bowel becoming infected (enterocolitis)
- bowel contents leaking into the body, which could lead to serious infection (peritonitis) if not treated quickly
- the bowel becoming narrowed or blocked again, requiring further surgery
After the Pull-through Procedure
After surgery, your child will need time to adjust to the new structure of his or her large intestine.
Most children feel better after the pull-through procedure. However, some children can have complications or problems after surgery. Problems can include
- narrowing of the anus
- constipation
- diarrhea
- leaking stool from the anus
- delayed toilet training
- enterocolitis
Typically, these problems improve over time with guidance from your child’s doctors. Most children eventually have normal bowel movements.
Ostomy Surgery
Ostomy surgery is a surgical procedure that reroutes the normal movement of the stool out of the body when a part of the bowel is removed. Creating an ostomy means bringing part of the intestine through the abdominal wall so that stool can leave the body without passing through the anus. The opening in the abdomen through which stool leaves the body is called a stoma.
A removable external collection pouch, called an ostomy pouch or ostomy appliance, is attached to the stoma and worn outside the body to collect the stool. The child or caregiver will need to empty the pouch several times each day.
Although most children with Hirschsprung disease do not need ostomy surgery, a child sick from Hirschsprung disease may need ostomy surgery to get better before undergoing the pull-through procedure. This gives the inflamed areas of the intestine time to heal. In most cases, an ostomy is temporary and the child will have a second surgery to close the ostomy and reattach the intestine. However, sometimes children with Hirschsprung disease have a permanent ostomy, especially if a long segment of the bowel is missing nerve cells or the child has repeated episodes of bowel inflammation, which health care providers call enterocolitis.
Ostomy surgeries include the following:
- Ileostomy surgery is when the surgeon connects the small intestine to the stoma.
- Colostomy surgery is when the surgeon connects part of the large intestine to the stoma.
Stool leaves the body through the stoma into a bag.
Later, the doctor closes the stoma and connects the healthy portion of the intestine to the rectum or anus.
After Ostomy Surgery
After surgery, your child will need time to adjust to the new structure of his or her large intestine.
Infants will feel better after ostomy surgery because they will be able to pass gas and stool easily.
Older children will feel better as well, although they must adjust to living with an ostomy. They will need to learn how to take care of the stoma and how to change the ostomy pouch. With a few lifestyle changes, children with ostomies can lead normal lives. However, they may worry about being different from their friends. A special nurse, called an ostomy nurse, can answer questions and show your child how to care for an ostomy.
What are the complications of ostomy surgery of the bowel?
Complications of ostomy surgery of the bowel may include:
- skin irritation
- stoma problems
- blockage
- diarrhea
- bleeding
- electrolyte imbalance
- infection
- irritation of the internal pouch, or pouchitis
- vitamin B12 deficiency
- phantom rectum
- short bowel syndrome
- rectal discharge
Skin Irritation
Skin irritation is the most common complication for people with an ostomy. If the external ostomy pouch does not fit properly, stool or stool contents can leak out around the stoma and under the pouch. When irritated, a person’s skin will become itchy, red, and uncomfortable. When changing the pouch, a person can use an ostomy powder on the skin around the stoma to treat skin irritation. If the skin irritation does not improve, the person should talk with a wound, ostomy and continence nurse or an enterostomal therapist—who are specially trained in ostomy care and rehabilitation—or another health care provider about the symptoms. Skin irritation may occur around the stoma for people who have an ileostomy or a colostomy. People who have ileoanal reservoir surgery may have skin irritation around the anus. Sometimes, using a barrier ointment to protect the skin around the anus can help treat and prevent irritation.
Stoma Problems
Stoma problems include the following:
- Hernia. A stoma hernia, seen as a bulge in the skin around the stoma, is a weakening of the abdominal wall around the stoma site. As with all hernias, a stoma hernia continues to increase in size and may eventually need surgical repair when it becomes too large. Rarely, the intestine gets trapped or kinked within the hernia and becomes blocked. A blocked intestine that loses its blood supply requires emergency surgery.
- Prolapse. A stoma prolapse occurs when the bowel pushes itself through the stoma. A person may be able to push the bowel back through the stoma and keep it in place with a stoma shield. If not, the stoma prolapse may require special care and a larger ostomy pouch. A stoma prolapse that becomes blocked or loses its blood supply requires surgical repair.
- Narrowing of the stoma. Narrowing of the stoma makes it difficult for stool to pass through the stoma. A narrowed stoma may need surgical repair.
Blockage
Occasionally, an ileostomy or a colostomy does not function for a short time. If the stoma has not passed intestinal content or stool for 4 to 6 hours and the person is experiencing cramping or nausea, the ileum or colon may be blocked. Blockage may occur when foods that are hard to digest get stuck in the ileum or colon.
Abdominal adhesions in the ileum or colon may cause blockage as well. Abdominal adhesions are bands of fibrous tissue that form between abdominal tissues and organs, causing them to kink or narrow. Most blockages get better without additional surgery by not eating food and drinking only clear liquids to rest the bowel for a short time.
Diarrhea
Diarrhea is loose, watery stools. A person has diarrhea if he or she passes loose stools three or more times a day. Diarrhea occurs when intestinal contents pass through the small intestine too quickly for fluid and mineral absorption. When fluids and minerals such as sodium and potassium are not absorbed, they leave the body. Diarrhea can lead to dehydration, malnutrition, and weight loss. Diarrhea is common, even normal, with an ileostomy or ileoanal reservoir. In most cases of diarrhea, the only treatment necessary is replacing lost fluids and electrolytes to prevent dehydration. Electrolytes are minerals in body fluids that are part of salts, including sodium, potassium, magnesium, and chloride. People should maintain good daily hydration by drinking plenty of water and liquids, such as fruit juices, sports drinks, caffeine-free soft drinks, and broths. In some cases of diarrhea, a health care provider may recommend changes in diet and may prescribe medications to treat diarrhea.
Bleeding
As with any major surgery, ostomy surgery may cause internal bleeding. If too much blood is lost, the person may require a blood transfusion. Bleeding may also occur through the stoma or through the anus after surgery.
Electrolyte Imbalance
The main function of the large intestine is to absorb water, nutrients, and electrolytes from partially digested food that enters from the ileum. When a surgeon removes the large intestine, absorption of electrolytes does not occur to the same extent, making electrolyte imbalance more likely. Diarrhea, excessive sweating, and vomiting can increase the chance of developing electrolyte imbalance.
Symptoms of electrolyte imbalance may include:
- fatigue, or feeling tired
- weakness
- nausea
- muscle problems such as spasms, weakness, uncontrolled twitching, and cramps
- dizziness and confusion
People with these symptoms require medical care and should contact a health care provider.
People who have had their large intestine removed should talk with a health care provider or dietitian about diets that help maintain electrolyte balance.
Infection
The gastrointestinal (GI) tract is filled with bacteria that can leak out during ostomy surgery and infect areas inside the abdomen. Bacteria entering the body through the stoma or anus can also cause an infection. The person’s skin around the stoma may also become infected with bacteria or skin fungus. Health care providers treat infections with antibiotics.
Symptoms of infection may include:
- fever
- back pain
- poor appetite
- nausea and vomiting
Irritation of the Internal Pouch, or Pouchitis
Pouchitis is an irritation or inflammation of the lining of an ileoanal reservoir or a continent ileostomy pouch. A health care provider treats pouchitis with antibiotics. For severe or chronic pouchitis, a health care provider may prescribe immunosuppressive medications, such as corticosteroids.
Symptoms of pouchitis include:
- frequent bowel movements with diarrhea
- an urgent need to have a bowel movement
- a feeling of pressure in the pouch
- abdominal pain
- cramping or bleeding
- dehydration
- low-grade fever
- a general unwell feeling
Vitamin B12 Deficiency
Ostomy surgery of the bowel may affect vitamin B12 absorption from food and result in a gradual drop in vitamin B12 levels in the body. Low levels of vitamin B12 can affect the body’s ability to use nutrients and may cause anemia. Anemia is a condition in which red blood cells are fewer or smaller than normal, which prevents the body’s cells from getting enough oxygen. Health care providers treat vitamin B12 deficiency with vitamin B12 supplements.
Phantom Rectum
Phantom rectum is the feeling of needing to have a bowel movement even though the rectum is not present. Phantom rectum is relatively common. Symptoms are usually mild and often go away without treatment. However, for some people, phantom rectum may occur for years after a surgeon removes the rectum. Some people with phantom rectum may feel pain. Health care providers treat rectal pain with medications such as pain relievers and sometimes antidepressants. To help control phantom rectum, a health care provider may recommend complementary therapies such as guided imagery and other relaxation techniques.
Short Bowel Syndrome
Short bowel syndrome is a group of problems related to inadequate absorption of nutrients after removal of part of the small intestine. People with short bowel syndrome cannot absorb enough water, vitamins, and other nutrients from food to sustain life. Diarrhea is the main symptom of short bowel syndrome. Other symptoms may include:
- cramping
- bloating
- heartburn
- weakness and fatigue
- vomiting
- excessive gas
- foul-smelling stool
Short bowel syndrome is uncommon and can occur with Crohn’s disease, trauma, or other conditions that lead to removal of a large amount of the small intestine.
A health care provider will recommend a treatment for short bowel syndrome based on a person’s nutritional needs. Treatment may include nutritional support, medications, and surgery.
Rectal Discharge
People with an ileostomy or a colostomy whose lower colon, rectum, and anus are still present may experience a discharge of mucus from their rectum. Mucus is a clear fluid made by the gastrointestinal (GI) tract that coats and protects the lining of the bowel. Mucus within the bypassed part of the colon may leak out of the rectum from time to time or gradually build up, forming a small, stool-like ball that passes out of the rectum. A person cannot control mucus production and rectal discharge. However, people who have rectal discharge can learn how to manage and cope with this problem.
Enterocolitis
Adults and children with Hirschsprung disease can suffer from enterocolitis (inflammation of both the small intestine and the colon) before or after surgery. Symptoms of enterocolitis may include:
- a swollen abdomen
- bleeding from the rectum
- diarrhea
- fever
- lack of energy
- vomiting
A child with enterocolitis needs to go to the hospital, because enterocolitis can be life threatening. Doctors can treat some children with enterocolitis with a special antibiotic by mouth, often in combination with rectal irrigation at home and in the doctor’s office. During rectal irrigation, a doctor inserts a small amount of mild salt water into the child’s rectum and allows it to come back out.
Doctors will admit children with more severe symptoms of enterocolitis to the hospital for monitoring, rectal irrigation, and intravenous (IV) antibiotics and IV fluid. Doctors give IV antibiotics and fluids through a tube inserted into a vein in the child’s arm. In severe or repeated cases of enterocolitis, a child may need a temporary ostomy to let the intestine heal or a revision of the pull-through surgery.
Hirschsprung disease diet
If a surgeon removes the child’s colon or bypasses it because of an ostomy, the child will need to drink more liquids to make up for water loss and prevent dehydration. They also need twice as much salt as a healthy child. A doctor can measure the sodium in a child’s urine and adjust his or her diet to ensure adequate salt replacement.
Some infants may need tube feedings for a while. A feeding tube is a passageway for the infant to receive infant formula or liquid food directly into his or her stomach or small intestine. The doctor will pass the feeding tube through the nose. In some cases the doctor will recommend a more permanent feeding tube that he or she puts in place surgically in the child’s abdomen.
Hirschsprung’s disease outlook (prognosis)
Most children are able to pass stools normally and have a normal functioning bowel after surgery, although they may take a bit longer to toilet train.
Some may experience persistent constipation and need to follow a high-fiber diet and take laxatives. Your doctor will advise about this treatment.
A small number of children have problems controlling their bowels (bowel incontinence), which can last until they’re a teenager and be very distressing.
Lifestyle and home remedies
If your child has constipation after surgery for Hirschsprung’s disease, discuss with your doctor whether to try any of the following:
- Serve high-fiber foods. If your child eats solid foods, include high-fiber foods. Offer whole grains, fruits and vegetables and limit white bread and other low-fiber foods. Because a sudden increase in high-fiber foods can worsen constipation at first, add high-fiber foods to your child’s diet slowly. If your child isn’t eating solid foods yet, ask the doctor about formulas that might help relieve constipation. Some infants might need a feeding tube for a while.
- Increase fluids. Encourage your child to drink more water. If a portion or all of your child’s colon was removed, your child may have trouble absorbing enough water. Drinking more water can help your child stay hydrated, which may help ease constipation.
- Encourage physical activity. Daily aerobic activity helps promote regular bowel movements.
- Laxatives. If your child does not respond to or can’t tolerate increased fiber, water or physical activity, certain laxatives — medications to encourage bowel movements — might help relieve constipation. Ask the doctor whether you should give your child laxatives and about the risks and benefits.





{kind=link}