
Contents
- What is Bloating
- What are Functional Bowel Disorders
- Functional Bowel Disorders consist of:
- Irritable bowel syndrome
- What Causes Bloating
- Abnormal Gut Microbiota
- Small Intestinal Bacterial Overgrowth
- Intestinal Gas Accumulation
- Altered Gut Motility and Impaired Gas Handling
- Abnormal Abdominal-diaphragmatic Reflexes
- Visceral Hypersensitivity
- Food Intolerance and Carbohydrate Malabsorption
- Table 1. Foods High in Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs) and Suitable Alternatives
- Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs)
- Intraluminal Contents
- Hard stool/Constipation
- Psychological Aspects
- Gender and Sex Hormones
- How to get rid of bloating
- Summary
What is Bloating
Bloating is defined as subjective discomfort by patient’s sensation of intestinal gas; whereas, abdominal distension is a visible increase in abdominal girth and bloating is one of the most common gastrointestinal symptoms, which is a frequent complaint in the patients of all ages 1. This symptom is very common in patients with irritable bowel syndrome (IBS) and other functional gastrointestinal disorders as well as in patients with organic disorders (e.g. ovarian cancer, colon cancer), but bloating may appear alone 1, 2. Many clinicians encounter the patients’ complaints such as “too much gas in abdomen,” “heavy and uncomfortable feeling in abdomen” and “full belly.” Burping and belching, which are other common gastrointestinal complaints, reflect the expulsion of excess gas from the stomach. These complaints may or may not be related to bloating and abdominal distention. The severity of bloating is varied from mild discomfort to severe, and it is one of the bothersome symptoms of the patients, affecting their quality of life. Despite being one of the frequent and bothersome complaints, bloating remains incompletely understood of all the symptoms 2.
In the medical literature, the terms “bloating” and “distension” are largely used synonymously, relying more on patient descriptions rather than on any attempt to record an actual change in girth. However, it has recently been suggested that the term “bloating” should be reserved exclusively for the subjective symptom of abdominal enlargement, with the term “distension” being used only when there is an actual change in girth. The situation is further complicated by the fact that in some languages there is not necessarily an exact equivalent of the word “bloating” 3.
In the past, bloating had been considered to be related to abdominal distension directly, but recent studies have suggested that it is not always accompanied by abdominal distension 4. There have been many studies to evaluate the relationship between bloating and abdominal distension. One study has shown that actual abdominal distension only occurred in about half of the patients suffering from bloating 5. In addition, some patients with both visceral hypersensitivity and functional gastrointestinal disorders complained of bloating in the absence of visible distension 6, 7.
In summary, abdominal bloating is the subjective symptom and distension is the objective sign, so bloating and distension should be considered as separate disorders with different mechanisms. Although bloating has been considered as a supportive symptom for irritable bowel syndrome or functional bloating according to Rome classification, functional bloating is also included as an independent entity in Rome criteria 8, 9, 10. The diagnosis of functional bloating is made in patients who do not meet the diagnostic criteria of irritable bowel syndrome or other functional gastrointestinal disorders, but have recurrent symptoms of bloating. According to Rome III, the diagnostic criteria include recurrent feeling of bloating or visible distension at least 3 days a month in the last 3 months with symptom onset at least 6 months prior to diagnosis. Also it should exclude functional dyspepsia, IBS or other functional gastrointestinal disorders.
Bloating Not To Be Confused With Belching and Flatulence
- Belching: Getting rid of excess air
Belching, or burping, is your body’s way of expelling excess air from your upper digestive tract. Most belching is caused by swallowing excess air. This air most often never even reaches the stomach but accumulates in the esophagus.
You may swallow excess air if you eat or drink too fast, talk while you eat, chew gum or suck on hard candies, drink carbonated beverages, or smoke. Some people swallow air as a nervous habit — even when they’re not eating or drinking. This is called aerophagia.
Acid reflux or gastroesophageal reflux disease (GERD) can sometimes cause excessive belching by promoting increased swallowing. Chronic belching may be related to inflammation of the stomach lining (gastritis) or to an infection with Helicobacter pylori, the bacterium responsible for some stomach ulcers. In these cases, the belching is accompanied by other symptoms, such as heartburn or abdominal pain.
You can reduce belching if you:
- Eat and drink slowly. Taking your time can help you swallow less air. Try to make meals relaxed occasions; eating when you’re stressed or on the run increases the air you swallow.
- Avoid carbonated drinks and beer. They release carbon dioxide gas.
- Skip the gum and hard candy. When you chew gum or suck on hard candy, you swallow more often than normal. Part of what you’re swallowing is air.
- Don’t smoke. When you inhale smoke, you also inhale and swallow air.
- Check your dentures. Poorly fitting dentures can cause you to swallow excess air when you eat and drink.
- Get moving. It may help to take a short walk after eating.
- Treat heartburn. For occasional, mild heartburn, over-the-counter antacids or other remedies may be helpful. GERD may require prescription-strength medication or other treatments.
- Flatulence: Gas buildup in the intestines
Gas in the small intestine or colon is typically caused by the digestion or fermentation of undigested food, such as plant fiber or certain sugars (carbohydrates), by bacteria found in the colon. Gas can also form when your digestive system doesn’t completely break down certain components in foods, such as gluten or the sugar in dairy products and fruit.
Other sources of intestinal gas may include:
- Food residue in your colon
- A change in the bacteria in the small intestine
- Poor absorption of carbohydrates, which can upset the balance of helpful bacteria in your digestive system
- Constipation, since the longer food waste remains in your colon, the more time it has to ferment
- A digestive disorder, such as lactose or fructose intolerance or Celiac disease.
To prevent excess gas, it may help to:
- Eliminate certain foods. Common gas-causing offenders include beans, peas, lentils, cabbage, onions, broccoli, cauliflower, whole-grain foods, mushrooms, certain fruits, and beer and other carbonated drinks. Try removing one food at a time to see if your gas improves.
- Read labels. If dairy products seem to be a problem, you may have some degree of lactose intolerance. Pay attention to what you eat and try low-lactose or lactose-free varieties. Certain indigestible carbohydrates found in sugar-free foods (sorbitol, mannitol and xylitol) also may result in increased gas.
- Eat fewer fatty foods. Fat slows digestion, giving food more time to ferment.
- Temporarily cut back on high-fiber foods. Fiber has many benefits, but many high-fiber foods are also great gas producers. After a break, slowly add fiber back to your diet.
- Try an over-the-counter remedy. Some products such as Lactaid or Dairy Ease can help digest lactose. Products containing simethicone (Gas-X, Mylanta Gas) haven’t been proved to be helpful, but many people feel that these products work. Products such as Beano may decrease the gas produced during the breakdown of certain types of beans.
How Common is Bloating ?
In USA, 15-30% of general population has been reported to experience bloating 11, 12. Also in Asia, similar result has been shown (15-23%), suggesting that the prevalence of bloating is not interracially different 13. Though the data for functional bloating alone are relatively little, women typically have higher rates of bloating than men according to the reports of IBS 14. This relevance between female gender and bloating has long been suggested and the hormonal effect in connection with menstrual cycle is regarded as one of the possible explanation 15, 16. Besides, there are some reports of obese people experiencing more gastrointestinal symptoms such as abdominal pain or bloating 17, 18.
Bloating is the second most common reported symptom in patients with Irritable Bowel Syndrome (IBS) following abdominal pain 19. In a study from USA which assessed bloating in 542 Irritable Bowel Syndrome patients, 76% of the patients reported that they experienced bloating 20. Other study revealed that more than 90% of patients with IBS suffered from bloating 21. In addition, on comparing constipation dominant Irritable Bowel Syndrome (IBS-C) with diarrhea dominant Irritable Bowel Syndrome (IBS-D), the prevalence of bloating was higher in Irritable Bowel Syndrome-constipation 22.
A survey from the USA suggested that more than 65% of patients with bloating rated their symptom as moderate to severe, and 54% of patients complained of decreased daily activity due to bloating. Furthermore, 43% of patients took medication for bloating or needed medication 12.
What are Functional Bowel Disorders
A functional bowel disorder is a functional gastrointestinal disorder with symptoms attributable to the mid or lower gastrointestinal tract, including the irritable bowel syndrome (IBS), functional abdominal bloating, functional constipation, functional diarrhea, and unspecified functional bowel disorder 23. Subjects with a functional bowel disorder may be divided into the following groups:
- non-patients: those who have never sought health care for the functional bowel disorder;
- patients: those who have sought care for the functional bowel disorder.
Symptoms of a functional bowel disorder must have been present for 12 weeks or more within the past 12 months; the 12 weeks need not be consecutive. The diagnosis always presumes the absence of a structural or biochemical explanation for the symptoms 23.
Functional Bowel Disorders consist of:
- Irritable Bowel Syndrome (IBS)
- Functional Bloating
- Functional constipation
- Functional diarrhea
- Unspecified functional bowel disorder
- Functional abdominal pain
- Functional abdominal pain syndrome
- Unspecified functional abdominal pain
Irritable bowel syndrome
Irritable bowel syndrome (IBS) is a chronic, often disabling, functional bowel disorder characterized by abdominal discomfort or pain and changes in bowel habits and with features of disordered defecation 24. Surveys of Western populations have revealed irritable bowel syndrome (IBS) in 15–20% of adolescents and adults, with a higher prevalence in women; the prevalence is variable in other populations 25.
Irritable bowel syndrome (IBS) has a chronic relapsing course and overlaps with other functional gastrointestinal disorders 26. Irritable bowel syndrome (IBS) accounts for high direct medical expenses 27 and indirect costs, including absenteeism from work 26.
The pathophysiology of Irritable bowel syndrome (IBS) is incompletely understood and treatment options are limited, partly due to the heterogeneity of the IBS population 28. Nearly two thirds of IBS patients report that their symptoms are related to food 29. The pathogenic mechanism by which food induces IBS symptoms remains unclear, but it includes visceral hypersensitivity, altered motility, abnormal colonic fermentation, and sugar malabsorption, all of which lead to increased gas production and luminal distention 30. The use of elimination diets for the treatment of IBS has yielded conflicting results, although this treatment option has been slightly more successful in IBS patients who have diarrhea 31. However, elimination diets can result in dietary restrictions that can be burdensome to patients and can potentially compromise their nutritional health. In addition, there is a lack of randomized controlled data that show a symptomatic benefit with elimination diets 32.
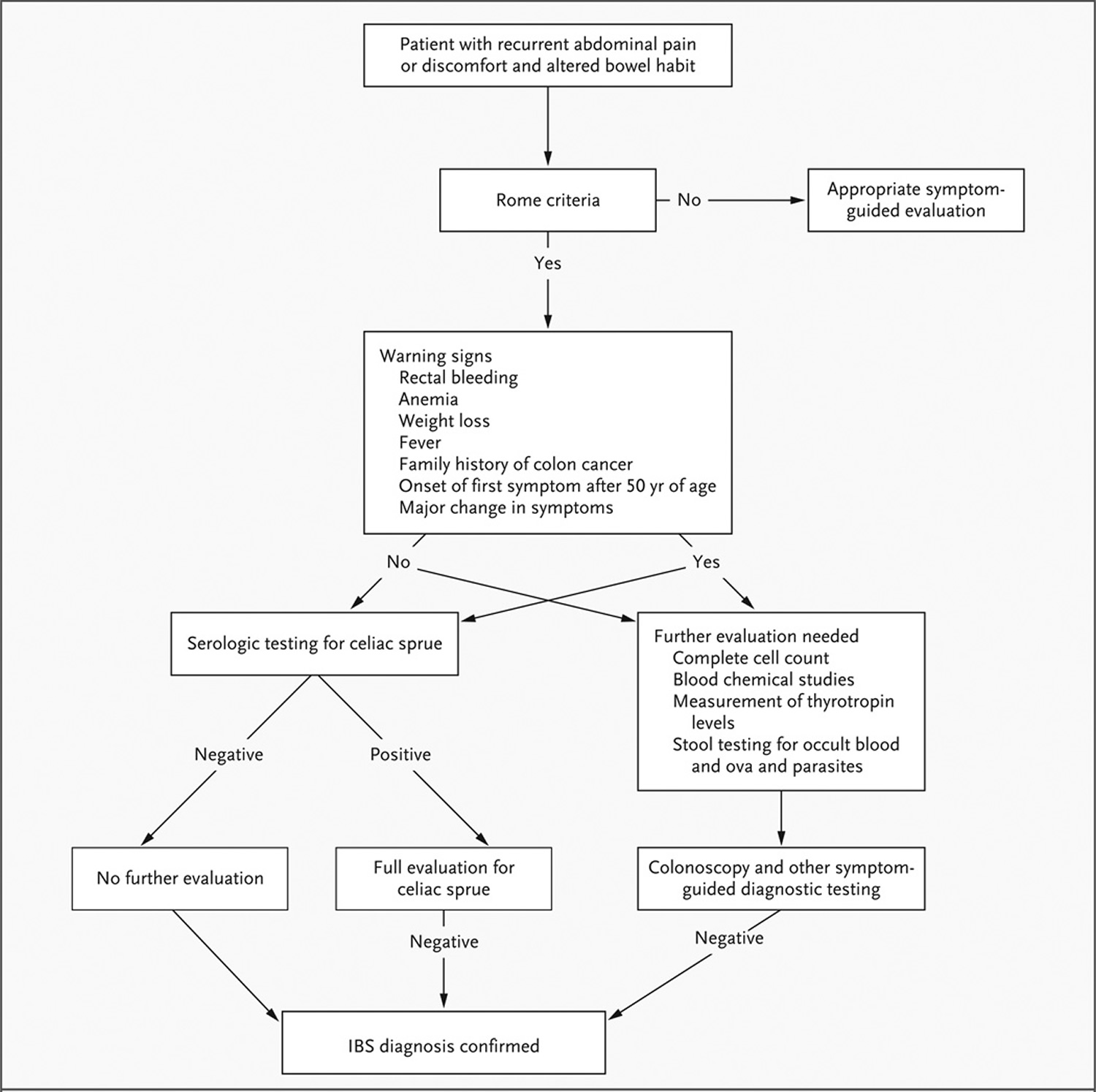
The Rome Diagnostic Criteria for Irritable Bowel Syndrome (IBS) 33:
- Recurrent abdominal pain or discomfort at least 3 days per month for the past 3 months, associated with two or more of the following:
- (1) Relieved with defecation; and/or
- (2) Onset associated with a change in frequency of stool; and/or
- (3) Onset associated with a change in form (appearance) of stool.
The following symptoms cumulatively support the diagnosis of IBS:
- abnormal stool frequency (for research purposes “abnormal” may be defined as >3/day and <3/week);
- abnormal stool form (lumpy/hard or loose/watery stool);
- abnormal stool passage (straining, urgency,or feeling of incomplete evacuation);
- passage of mucus;
- bloating or feeling of abdominal distension.
Figure 1. How To Diagnose Irritable bowel syndrome (IBS)
What Causes Bloating
The pathophysiology of bloating is complicated, incompletely understood and remains ambiguous, some evidences are emerging in support the potential mechanisms, including gut hypersensitivity, impaired gas handling, altered gut microbiota, and abnormal abdominal-phrenic reflexes 2. Abdominal bloating or abdominal distention may occur in isolation or along with other gastrointestinal symptoms in patients with functional disorders (eg, aerophagia, nonulcer dyspepsia, gastroparesis, irritable bowel syndrome) or organic disorders (eg, ovarian cancer, colon cancer) 1. Gastroparesis (and consequent bloating) also has many nonfunctional causes, the most important of which is autonomic visceral neuropathy due to diabetes; other causes include postviral infection, drugs with anticholinergic properties, and long-term opiate use 1. However, excessive intestinal gas is not clearly linked to these complaints. In most healthy people, 1 L/hour of gas can be infused into the gut with minimal symptoms. It is likely that many symptoms are incorrectly attributed to “too much gas” 1.
On the other hand, some patients with recurrent GI symptoms often cannot tolerate small quantities of gas: Retrograde colonic distention by balloon inflation or air instillation during colonoscopy often elicits severe discomfort in some patients (eg, those with irritable bowel syndrome) but minimal symptoms in others 1. Similarly, patients with eating disorders (eg, anorexia nervosa, bulimia) often misperceive and are particularly stressed by symptoms such as bloating. Thus, the basic abnormality in patients with gas-related symptoms may be a hypersensitive intestine. Altered motility may contribute further to symptoms 1.
Owing to the insufficient understanding of these mechanisms, the available therapeutic options are limited 2. However, medical treatment with some prokinetics, rifaximin, lubiprostone and linaclotide could be considered in the treatment of bloating. In addition, dietary intervention is important in relieving symptom in patients with bloating 2.
Abnormal Gut Microbiota
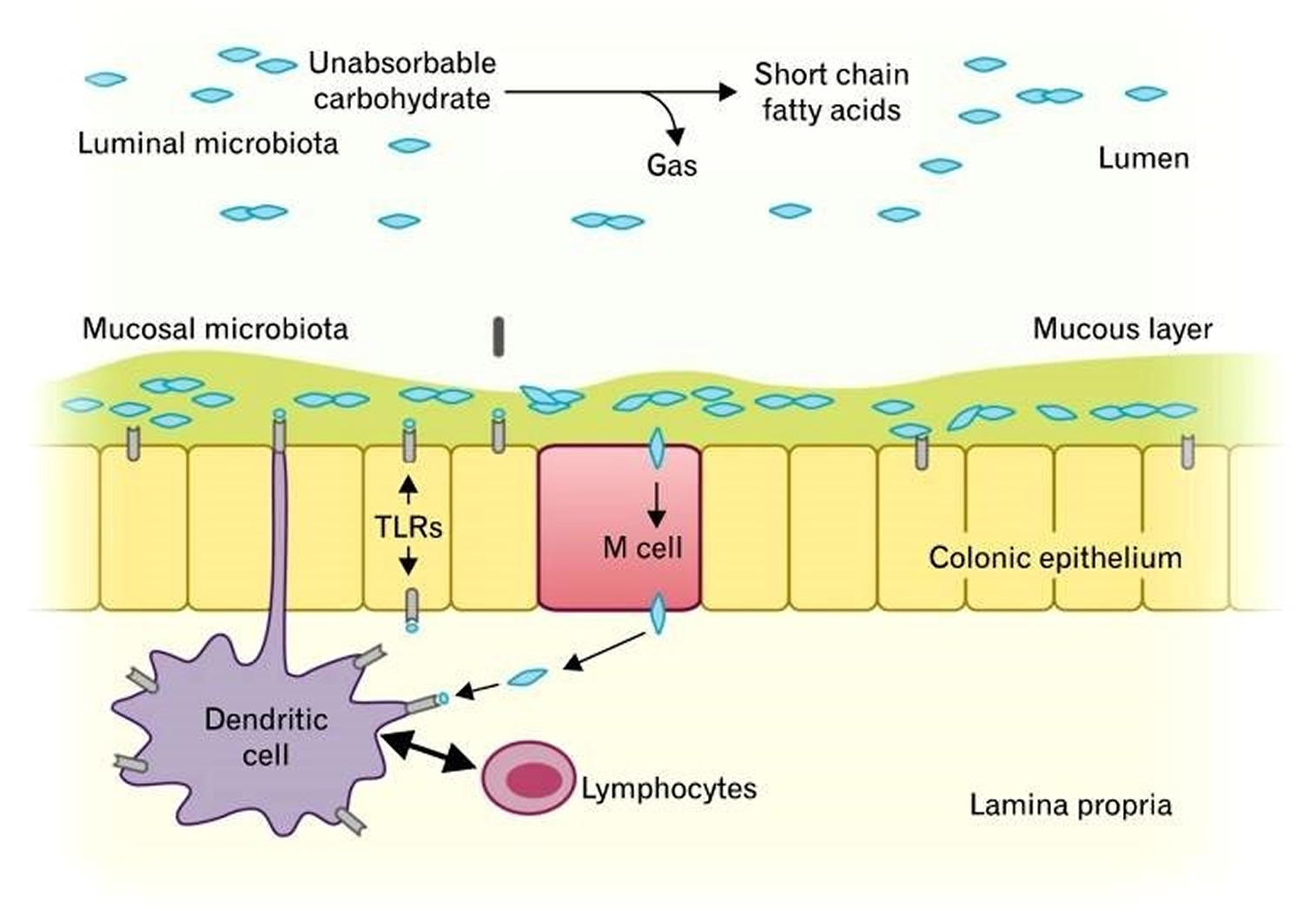
The GI tract microbiota play an important role in host immune system, and there are more than 500 different species of GI microbiota in adult, which mostly are obligate anaerobes 35. Only a fraction of these organisms can be cultured; therefore, the understanding of the functions of various microbes in the GI tract is still limited. However, researches over the past decades have shown that altered colonic flora were found in stool samples of patients with IBS 36, 37. Parkes et al. 38 suggested that the GI microbiota can be divided into 2 ecosystems; the luminal bacteria and the mucosa-associated bacteria (Figure 1). Luminal microbiota form the majority of the GI tract flora, and they play a key role in bloating and flatulence in IBS through carbohydrate fermentation and gas production 38. It has been shown that fecal microbiota are significantly altered in IBS. That is, some patients with IBS seem to have different patterns of colonization with coliforms, such as lactobacillus and bifidobacterium compared to the controls 39.
In addition, these microbial changes altered protein and carbohydrate metabolism in the gut 40. A study from Japan also showed higher counts of Veillonella and Lactobacillus in IBS patients than in controls. Besides, they expressed significantly higher levels of acetic acid, propionic acid and total organic acids than controls, which is related to symptoms such as abdominal pain, bloating and changes in bowel habits 41. Another study demonstrated that the patients with IBS produced more Hydrogen gas but the total gas excretion was similar in both IBS patients and controls 42. This may be associated with alteration in colonic fermentation by hydrogen-consuming bacteria, which may be an important factor in the pathogenesis of IBS.
Collins et al. 43 have proposed that disruption of the balance between the host and intestinal microbiota produces changes in the mucosal immune system from microscopic to overt inflammation and this also results in changes in gut sensory-motor function and immune activity. Besides, these altered microflora may produce differences in fermented gas type and volume, which may be the causes of symptom in patients with bloating 43, 44.
There have been some reports to verify the relationship between the types of gas produced by colonic microflora and bloating. The low producers of methane reported significantly increased bloating and cramping after ingestion of sorbitol and fiber, and the high producers of methane revealed lower prevalence of severe lactulose intolerance than low producers. Hence, the role of methanogenic flora may be important in the pathogenesis of bloating 45, 46.
Figure 2. Luminal and mucosal colonic microbiota and their roles in gut homeostasis.
Small Intestinal Bacterial Overgrowth
The patients with IBS who specifically complain of bloating have been reported to have increased gas production from bacterial fermentation caused by small intestinal bacterial overgrowth. Pimentel and colleagues had established the concept thatsmall intestinal bacterial overgrowth might be a major pathogenesis of IBS 47, Moreover, several studies found significant improvement of symptoms such as abdominal pain or bloating, when they were treated with antibiotics 47, 48. These findings, however, have not been supported by other studies 49, 50, they found mildly increased counts of small intestinal bacteria by culture to be more common in IBS, but the breath Hydrogen gas concentration was not significantly different between IBS patients and controls 51. Also, there was no correlation between bacterial alteration and symptom pattern, and even lactulose breath test was considered as an unreliable method to detect an association between bacterial overgrowth and IBS 51. In another study, breath hydrogen concentration was similar in IBS group and control group, and did not correlate with pain ratings in IBS patients, owing to the lack of objective diagnostic measures and inconsistent data 52.
It is unclear whether changes in small bowel bacterial flora could contribute to bloating in IBS patients, thus further studies are required to confirm these observations.
Intestinal Gas Accumulation
In the fasting state, the healthy gastrointestinal tract contains only about 100 mL of gas distributed almost equally among 6 compartments – stomach, small intestine, ascending colon, transverse colon, descending colon and distal (pelvic) colon. Postprandial volume of gas increases by about 65%, primarily in the pelvic colon 53. The excessive volume of intestinal gas has been proposed as the likely cause of bloating and distension, and many researchers have attempted to determine this view. A few studies using plain abdominal radiography demonstrated that intestinal gas volume was greater in patients with IBS than in controls (54% vs. 118%), however, the correlation between intra-abdominal gas contents and bloating was poor 54, 55. The vast majority of studies do not support that excessive gas induces bloating or abdominal pain. Lasser et al. (The role of intestinal gas in functional abdominal pain. Lasser RB, Bond JH, Levitt MD. N Engl J Med. 1975 Sep 11; 293(11):524-6. https://www.ncbi.nlm.nih.gov/pubmed/1152877/()) conducted a study using argon washout technique, which demonstrated no differences in the accumulation of intestinal gas between patients with bloating and healthy subjects. More recent studies using CT scans combined with modern imaging analysis software have also shown that excess gas was not associated with abdominal bloating in most patients 56. Thus, these observations suggest that increased volume of gas may not be the main mechanism of bloating, but rather impaired gas transit or distribution are more often the sources of problem.
Altered Gut Motility and Impaired Gas Handling
Various abnormal motility patterns have been described in IBS patients, but none of those parameters can be used as diagnostic markers 57. Some authors have suggested that slow transit of food representing alteration in gut motility is related to bloating in IBS-Constipation patients 58. Also in a traditional experiment, normal volunteers being made constipated with loperamide, an agent known to slow transit, experienced bloating 59. Recently, IBS-Constipation patients with delayed orocecal and colonic transits have shown abdominal distension rather than bloating.15 Although delayed gastric emptying and slow intestinal transit in IBS-C patients were reported in many Asian studies, there are still controversies to define these motor disturbances as unique features in Asian IBS patients. Besides, the association between altered gut motility and IBS symptoms is pretty obscure. A recent study has also suggested that altered colon transit is of no or minor importance for IBS symptoms such as bloating or pain.
However, there are some different points with respect to the intestinal gas handling or transit. In a study by Serra et al. 60, they have shown that infused gas into the jejunum resulted in distension and abdominal bloating in most of the IBS patients (18 of 20), while only 20% (4 of 20) of control subjects developed symptoms like that. Another study using gas challenge technique has demonstrated that small intestinal gas transit (especially, jejunum) was more prolonged in patients with bloating than in controls, whereas colonic transit was normal. These data support that impaired small intestinal gas handling could be a mechanism of IBS or gas-bloating. Furthermore, a gas challenge test in healthy subjects during blocked rectal gas outflow showed that abdominal distension by girth measurement was similar in the jejunal and rectal infusion experiments, whereas abdominal symptoms including bloating were more significant in jejunal group. These data indicate that gas related symptom perception is determined by intraluminal gas distribution, whereas abdominal distension depends on the volume of intestinal gas. Besides, the patients with IBS or functional bloating are considered to evacuate intestinal gas less effectively, so that they are more likely to have symptoms of abdominal distension. This aspect of bloating’s mechanism has not been considered to be very relevant, but some researchers are interested in this view owing to the observations of anorectal function, especially in patients with constipation. Constipated patients with bloating plus distension exhibited a greater degree of anorectal dysfunction than those without distension. Moreover, self-restrained anal evacuation also increased symptom perception, while impaired gut propulsion caused by intravenous glucagon did not.
Taken together, ineffective anorectal evacuation as well as impaired gas handling may be possible mechanisms of abdominal distension and bloating. However, the data on the link between altered food transit of gut and bloating are not consistent, although they probably account for bloating in some of the IBS patients.
Abnormal Abdominal-diaphragmatic Reflexes
The abdominal cavity is determined by the placement of the walls of abdominal cavity including diaphragm, vertebral column and abdominal wall musculature. Even if there is no increase in intra-abdominal volume, a change of the position of abdominal cavity components may produce abdominal distension. Thus, there have been some efforts to evaluate the relationship between bloating and lumbar lordosis or weakened abdominal muscles. In one classic report, Sullivan suggested that the patients with bloating have weak abdominal muscles and frequently had recently gained weight than controls 61. But another study measuring upper and lower abdominal wall activities using surface electromyography has suggested that there were no differences in abdominal muscle activities between the patients and the controls. Moreover, in an early CT study, some IBS patients showed a tendency of lumbar lordosis but not consistent, and a change in lumbar lordosis did not correlate in any way with the changes in abdominal girth. Also, there were no noticeable changes in position of the diaphragm.
Tremolaterra et al. 62 reported that intestinal gas load was associated with a significant increment in abdominal wall muscle activity in healthy subjects. In contrast, the response to gas infusion was impaired in patients with bloating, and rather a paradoxical relaxation of the internal oblique muscles was noted. Further study using modern CT analysis with electromyography from Barcelona group has provided a novel concept of abnormal abdomino-phrenic reflexes for abdominal bloating and distension. Since then, several studies have demonstrated that abdomino-phrenic dyssynergia is one of main factors for abdominal distension and bloating. In healthy adults, colonic gas infusion increases anterior wall tone and relaxes the diaphragm at the same time. On the contrary, patients with bloating have shown diaphragmatic contraction (descent) and relaxation of the internal oblique muscle with the same gas load 63, 64.
Visceral Hypersensitivity
The sensation of bloating may originate from abdominal viscera in patients with functional gastrointestinal disorders, in whom normal stimuli or small variations of gas content within the gut may be perceived as bloating. Indeed, it has been well recognized that the patients with IBS have lower visceral perception threshold than healthy controls 65, 66 and it has been speculated that this process might be associated with the sensation of bloating. Kellow et al. 67 revealed that threshold for perception of small bowel contraction was lower than normal in some patients with IBS. Also, altered rectal perception assessed by phasic balloon distension has been reported in IBS patients. In addition, a gas challenge test proved a role of sensory disturbances in IBS patients, and recent clinical experiment has demonstrated that bloating without visible distension is associated with visceral hypersensitivity.
The autonomic nervous system may also contribute to modulation of the visceral sensitivity. Sympathetic activation is known to increase the perception of intestinal distention in functional dyspepsia patients; likewise, autonomic dysfunction could affect the visceral sensitivity in IBS patients. This mechanism may play a role in bloating. Moreover, it has been proposed that visceral perception may be influenced by cognitive mechanism. That is, IBS patients with bloating pay more attention to their abdominal symptoms, which is a kind of hyper-vigilance. Also, a report indicated that female patients with IBS had worsening of abdominal pain and bloating during their peri-menstrual phase, at which time heightened rectal sensitivity might have contributed to bloating, but not to distension. Taken together, altered sensory threshold combined with altered conscious perception may explain the mechanism of bloating.
Food Intolerance and Carbohydrate Malabsorption
It is well recognized that dietary habits may be responsible for abdominal symptoms, and there have been efforts to prove the relationship between diet and IBS symptoms. Fiber overload has long been regarded as worsening factor of IBS symptoms through decreased small bowel motility or intraluminal bulking 68, 69. In addition, lactose intolerance may contribute to symptom development in IBS patients. In the small intestine, disaccharides are split by intestinal enzymes into monosaccharides which are then absorbed. If this process is not carried out, the disaccharide reaches the colon, in turn is split by bacterial enzymes into short chain carbonic acids and gases. Hence, malabsorption of lactose may produce the symptom of bloating in patients with IBS or functional bloating. Additionally, a new hypothesis is proposed, by which excessive delivery of highly fermentable but poorly absorbed short chain carbohydrates and polyols (collectively termed FODMAPs; fermentable oligo-, di- and mono-saccharides and polyols) to the small intestine and colon may contribute to the development of GI symptoms. FODMAPs are small molecules that are osmotically active and very rapidly fermentable compared with long-chain carbohydrates. These molecules induce relatively selective bacterial proliferation, especially of bifidobacterium, and it has been demonstrated indirectly that these can lead to expansion of bacterial populations in distal small intestine 70, 71, 72. Thus, high FODMAP diet has demonstrated prolonged hydrogen production in the intestine, colonic distension by fermentation, increased colonic fluid delivery by osmotic load within the bowel lumen, and GI symptom generation 73, 74.
Table 1. Foods High in Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs) and Suitable Alternatives
| FODMAP | Foods high in FODMAPs | Suitable alternatives low in FODMAPs |
|---|---|---|
| Excess fructose | Fruits: apple, clingstone peach, mango, nashi pear, pear, sugar snap pea, tinned fruit in natural juice, watermelon | Fruits: banana, blueberry, cantaloupe, carambola, durian, grape, grapefruit, honeydew melon, kiwi, lemon, lime, orange, passion fruit, pawpaw, raspberry, strawberry, tangelo |
| Honey sweeteners: fructose, high-fructose corn syrup | Honey substitutes: golden syrup, maple syrup | |
| Large total fructose dose: concentrated fruit sources, large servings of fruit, dried fruit, fruit juice | Sweeteners: any sweeteners except polyols | |
| Lactose | Milk: regular and low-fat cow, goat, and sheep milk; ice cream | Milk: lactose-free milk, rice milk Ice cream substitutes: gelato, sorbet |
| Yogurts: regular and low-fat yogurts | Yogurts: lactose-free yogurts | |
| Cheeses: soft and fresh cheeses | Cheeses: hard cheeses | |
| Oligosaccharides (fructans and/or galactans) | Vegetables: artichoke, asparagus, beetroot, broccoli, Brussels sprout, cabbage, fennel, garlic, leek, okra, onion, pea, shallot | Vegetables: bamboo shoot, bok choy, capsicum, carrot, celery, chives, choko, choy sum, corn, eggplant, green bean, lettuce, parsnip, pumpkin, silverbeet, spring onion (green part only) |
| Cereals: rye and wheat cereals when eaten in large amounts (eg, biscuit, bread, couscous, cracker, pasta) | Onion/garlic substitutes: garlic-infused oil | |
| Legumes: baked bean, chickpea, lentil, red kidney bean | Cereals: gluten-free and spelt bread/cereal products | |
| Fruits: custard apple, persimmon, rambutan, watermelon, white peach | Fruit: tomato | |
| Polyols | Fruits: apple, apricot, avocado, cherry, longon, lychee, nashi pear, nectarine, peach, pear, plum, prune, watermelon | Fruits: banana, blueberry, cantaloupe, carambola, durian, grape, grapefruit, honeydew melon, kiwi, lemon, lime, orange, passion fruit, pawpaw, raspberry |
| Vegetables: cauliflower, mushroom, snow pea | ||
| Sweeteners: isomalt, maltitol, mannitol, sorbitol, xylitol, and other sweeteners ending in “-ol” | Sweeteners: glucose, sugar (sucrose), other artificial sweeteners not ending in “-ol” |
Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs)
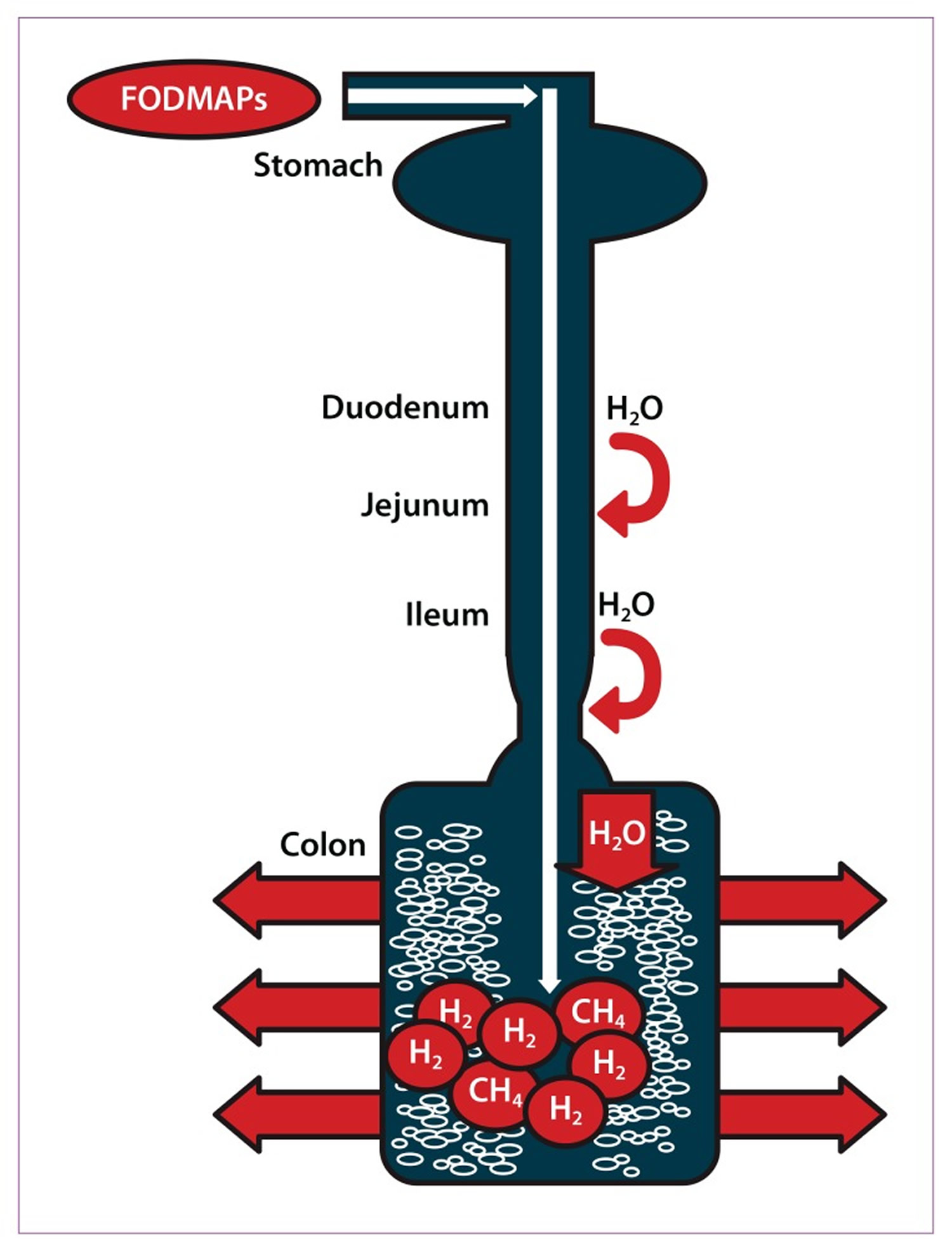
The acronym FODMAPs was created to describe poorly absorbed, short-chain carbohydrates that can lead to excessive fluid and gas accumulation, resulting in bloating, abdominal pain, and distention (Figure 3). FODMAPs are found in a wide variety of foods, including those containing lactose, fructose in excess of glucose, fructans, galacto-oligosaccharides, and polyols (sorbitol, mannitol, xylitol, and maltitol). All FODMAPs have poor absorption and rapid fermentation, and they are comprised of small, osmotically active molecules. FODMAPs are poorly absorbed for a number of reasons, including the absence of luminal enzymes capable of hydrolyzing the glycosidic bonds contained in carbohydrates, the absence or low activity of brush border enzymes (eg, lactase), or the presence of low-capacity epithelial transporters (fructose, glucose transporter 2 [GLUT-2], and glucose transporter 5 [GLUT-5]). Fructose, which is an important FODMAP in the Western diet, is absorbed across villous epithelium through low-capacity, carrier-mediated diffusion involving GLUT-5. The absorption of free fructose is markedly enhanced in the presence of glucose via GLUT-2. Therefore, if fructose is present in excess of glucose, the risk of fructose malabsorption is increased. In addition, some molecules, such as polyols, are too large for simple diffusion. The fermentation rate is determined by the chain length of the carbohydrate 76.
For example, oligosaccharides are rapidly fermented, compared to polysaccharides. Fermentation results in the production of carbon dioxide, hydrogen, and/or methane gas. Finally, small, osmotically active molecules draw more water and other liquid into the small bowel. Given these properties, a diet low in FODMAPs has become a potential therapy for IBS patients.
Figure 3. Ingested fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) are poorly absorbed in the small intestine. Their small molecular size results in an osmotic effect, drawing water (H20) through to the large intestine. FODMAPs are then fermented by colonic microflora, producing hydrogen (H2) and/or methane gas (CH4). The increase in fluid and gas leads to diarrhea, bloating, flatulence, abdominal pain, and distension.
Intraluminal Contents
Levitt et al. 77 suggested that abdominal bloating might develop without gas retention, but by other gut contents. They had undertaken randomized, double-blind, crossover study of gaseous symptoms by observing the responses of healthy subjects to dietary supplement with lactulose or 2 types of fibers (psyllium or methylcellulose). In lactulose group, gas passages, subjective perception of rectal gas and breath hydrogen excretion were significantly increased, but not in fiber groups. However, the sensation of bloating was increased in all 3 groups. Thus, it has been proposed that increased intra-abdominal bulk, not gaseous filling, might be a cause of abdominal bloating. In another study, bran accelerated small bowel transit and ascending colon clearance without causing symptom in controls, but small bowel transit has not further been accelerated in IBS patients with bloating. Thus, they speculated that bran might cause increased bulking effect in the colon, which led to the exacerbation of bloating in IBS patients 78. Francis and Whorwell 68 even proposed that use of the bran in IBS should be reconsidered, because excessive consumption of bran might give rise to symptoms such as bloating in IBS patients. Although more studies are needed for further understanding of their relationship, it could be possible that intraluminal bulking aggravates the bloating in some IBS patients.
Hard stool/Constipation
Many constipated patients complain of bloating.14 Also there is a tendency of its being more common in IBS-Constipation patients than IBS-Diarrhea patients, though it is not statistically significant in some studies 79, 80. Distension of the rectum by retained feces slows small intestinal transit as well as colonic transit, probably explaining the aggravated bloating in constipated patients 81, 82. Thus it seems reasonable that constipation or hard/lumpy stool induces alteration of gut motility and thus maybe increases bacterial fermentation. In addition, constipation may accelerate bloating by intraluminal bulking effect in the same manner as bran.
Psychological Aspects
Bloating is a frequent complaint of women with IBS. Park et al. 83 proposed that there was a tendency to increase the index of psychological distress when the bloating was more severe. Also, patients with bloating revealed increased anxiety and depression, which allows the hypothesis that psychological distress may contribute to the perceived severity of bloating 84. Additionally, in large population surveys, bloating was significantly related with psychiatric dysfunction such as major depressive disorder, panic disorder and sleeping difficulties 85, 86. Nevertheless, other studies have failed to demonstrate the relationships between psychological distress and either bloating or distension 87. However, it is unclear whether or not there is an actual relationship between bloating and psychosocial distress, and further studies are needed to demonstrate it.
Gender and Sex Hormones
In a population based study in USA, female gender was significantly associated with increased symptoms of bloating and distension in IBS, and similar findings have been reported so far. Although the question of the gender role in IBS has been raised from many studies, the mechanisms of gender differences in bloating and distension are unclear. Some studies have suggested that bloating is one of the frequent symptoms of menstruation as aforementioned 88, 89. Hormonal effect has also been speculated, that is, the variation of reproductive hormones throughout the menstrual cycle and after the menopause may influence the gut motility and visceral perception. Additionally, difference in symptom expression by gender is presented as a potential explanation. Although more investigations regarding the underlying mechanisms for these disparities remain to be determined, it seems to be possible to speculate that the hormonal fluctuation may contribute to bloating in female IBS patients.
How to get rid of bloating
Antibiotics
There has been an increasing acceptance of the use of the antibiotics to treat IBS symptoms, and it is plausible based on the presumption that altered gut flora or Small Intestinal Bacterial Overgrowth may contribute to gaseous distension or bloating symptom.
Although some questions have been raised regarding the validity of the lactulose breath test in diagnosis of Small Intestinal Bacterial Overgrowth and the possibility of overdiagnosis,106 much more data support the clinical use of antibiotics in this condition. Specifically, rifaximin, a rifamycin derivative, has largely been studied, and it showed superiority to placebo in relieving bloating in IBS or in patients who were diagnosed as Small Intestinal Bacterial Overgrowth. As rifaximin is a non-absorbable antimicrobial agent, the risk of side effects or emergence of resistant organisms is expected to be low; therefore it is suitable for chronic administration. Recently, a phase 3 multicenter trial proved that rifaximin provided significant improvement of IBS symptoms including abdominal pain and bloating in non-constipated IBS patients. Pimentel et al. 90 also suggested that neomycin normalized lactulose breath test and it contributed to the reduction of bloating in IBS patients. Besides, there have been several retrospective or observational studies, which support the efficacy of rifaximin treatment in IBS patients. Specifically, rifaximin turned the lactulose breath test to negative and significantly reduced the overall symptom scores. Also, high dose rifaximin treatment (2,400 mg/day) was proved to be effective in patients who had incomplete response to usual dose of rifaximin. Another retrospective study has revealed that rifaximin is superior to other antibiotics, such as neomycin, doxycycline, amoxicillin/clavulanate and ciprofloxacin in patients with IBS. Therefore, antibiotics like rifaximin could be considered as a short course therapeutic regimen for bloating, mainly in IBS without constipation. Further studies are needed to determine how long these antibiotics should be given and whether drug resistance will be a problem.
Probiotics
Alteration in gut microbiota may produce or perpetuate the symptoms of bloating or distension, therefore many researchers postulated that modification of the gut microflora could improve gas related symptoms. One placebo-controlled study conducted in IBS patients revealed a beneficial effect of Bifidobacterium infantis and they suggested immune-modulating role of that organism. Another multicenter, clinical trial in women with IBS also showed that B. infantis relieved many of the symptoms of IBS, but just at a specific dosage (1 × 108 CFU/mL). In addition, more recent experiments have shown that some probiotic strains significantly alleviate the bloating as well as overall symptoms. One study from Korea has shown that multi-species probiotics given to IBS patients are effective in the relief of bloating, albeit not statistically significant over placebo. In the most recent meta-analysis of probiotics for lower GI symptoms, specific probiotics are recommended in the management of bloating in IBS patients as moderate grade of evidence along with 70% level of agreement.
On the contrary, many other studies have failed to prove favorable effects of the probiotics. Kim et al. 91 evaluated the effectiveness of VSL#3, a composite probiotic containing Bifidobacterium, Lactobacillus and Streptococcus in IBS patients. VSL#3 reduced flatulence scores and retarded colonic transit without altering bowel function, but there was no significant reduction in bloating score with VSL#3. Some experimental studies from Korea showed a trend towards amelioration of bloating, but failed to prove beneficial effect over placebo. In addition, several other studies using lactobacillus strains reported unfavorable effect on bloating in IBS. Most of the studies were relatively small and there have been inconsistent results regarding the efficacy of probiotics on bloating. Hence, larger and well-designed trials are needed to prove whether the probiotics are reasonable to treat patients with bloating.
Prokinetics
Prokinetics have been used in the treatment of bloating in functional dyspepsia traditionally, in spite of the weak evidence for correlation between symptoms and underlying pathophysiological mechanisms. A number of studies have shown the beneficial effect of prokinetics such as dopamine antagonist, muscarinic antagonist, and serotonergic agents in functional dyspepsia, but studies conducted in IBS patients are relatively rare. Several studies have suggested that cisapride, a 5-hydroxytryptamine 4 (5-HT4) receptor agonist, significantly improves postprandial bloating in functional dyspepsia patients. Levosulpiride turned out to be as effective as cisapride in the treatment of functional dyspepsia symptoms, such as bloating. Acotiamide, a novel prokinetic agent, also provided relief of bloating in functional dyspepsia patients in a small study. Although there are conflicting evidences regarding the effect of prokinetics on bloating, some of the prokinetics could be a treatment option for bloating.
Antispasmodics
Various types of antispasmodics have been commonly used to relieve the symptoms of IBS, given the presumption that altered GI motility and smooth muscle spasm may give rise to the IBS symptoms. Several studies have shown the efficacy of these drugs in IBS symptoms such as bloating, but some do not. Also data are limited since many of these agents (e.g., mebeverine, otilonium and trimebutine) are not licensed in the USA. There have been several reports that support the beneficial effect of otilonium. Besides, in a few studies, peppermint oil, considered as a natural spasmolytic agent due to its calcium influx blocking effect, was also superior to placebo in reduction of abdominal distension and bloating. One systematic review evaluated the efficacy and tolerability of mebeverine. In the meta-analysis, it was effective in the clinical improvement of abdominal pain or distension, but it did not reach a statistical significance. Taken together, antispasmodics have shown some efficacy in the treatment of bloating, but the study results were inconsistent and it is difficult to draw definite conclusion about these conflicting views. Thus, larger studies are needed.
Dietary Interventions
Food intake may play a key role in perpetuating symptoms in IBS patients, so a careful history taking for diet should be taken. Many retrospective observational studies have shown that the reduced intake of large amounts of highly fermentable, poorly absorbed short chain carbohydrates (FODMAPs) may reduce bloating in IBS patients. Finally, the low FODMAP diet was developed at Monash University in Melbourne and recently, the first prospective study confirming the efficacy of low FODMAP diet for IBS patients was reported. Besides, patients with IBS who had also fructose malabsorption were significantly more likely to respond to the low FODMAP diet than those without fructose malabsorption.
Gas Reducing Substances
One of the earliest pharmachological modalities used in treating distension and bloating was antifoaming agent (an agent that breaks up small gas bubbles), and a silicone derivative with surfactant, officially designated as “simethicone” is known as a traditional antifoaming agent, by which gases are evacuated and absorbed from the gut. As most of the studies which investigated the therapeutic benefit of those agents were carried out in the subset of patients who have functional dyspepsia, their efficacy in IBS patients seems questionable. Bernstein et al. 92 reported that simethicone significantly relieved the frequency and severity of gas-related symptoms in patients with FGID. Holtmann 93 also conducted a randomized, placebo-controlled trial of simethicone, and suggested that simethicone was significantly better than placebo for overall symptom control in functional dyspepsia patients, in spite of unfavorable effect for bloating. More recently, prospective, multicenter trial to demonstrate a favorable action of activated charcoal-simethicone combination therapy revealed that the severity of fullness and bloating was significantly decreased in the therapy group compared with placebo .
Stimulants of Fluid Secretion
Lubiprostone and linaclotide are novel agents recently approved by the USA Food and Drug Administration, that enhance fluid secretion into the gut lumen and accelerate intestinal transit. These properties are considered to play a role in treatment of constipation, thus a number of clinical trials focusing in the chronic constipation or IBS-Constipation have been conducted. In 2 phase III trials, lubiprostone significantly improved the overall IBS symptoms including bloating in IBS-Constipation 94, 95. Several multicenter, randomized trials of linaclotide in chronic constipation or IBS-Constipation also demonstrated the beneficial effect in relieving abdominal bloating. Thus so far, these 2 novel drugs offer a reasonable therapeutic approach for bloating mainly in IBS-Constipation and functional constipation patients.
Antidepressants
Antidepressants such as selective serotonin reuptake inhibitor (SSRI) or tricyclic antidepressant (TCA) are believed to alleviate symptoms in functional gastrointestinal disorders on the basis of their visceral analgesic properties as well as psychological aspects. However, one small study conducted in IBS patients with visceral hypersensitivity revealed that fluoxetine, one of the SSRI, was effective only in abdominal pain, not in other symptoms such as bloating. Paroxetine was also evaluated in IBS patients who did not respond to high fiber diet. Overall well-being sensation was improved more with paroxetine than with placebo, but abdominal bloating was not. However, there were also some positive results. That is, the SSRI, citalopram significantly improved abdominal bloating compared with placebo, though the therapeutic effect was independent of the effect on anxiety, depression and colonic sensitivity. Taken together, the results for the treatment of bloating and distension with antidepressants are partly contradictory, and there were few studies which explained the effect of TCA on bloating. Hence, larger, well-designed trials with SSRIs and TCAs are warranted to identify the efficacy of these drugs on bloating and distension.
Opioid Agents
There have been a few reports that propose the usefulness of opioid agents in IBS patients. The kappa receptor agonist, fedotozine has been shown to increase the threshold of perception to colonic distension and reduce visceral sensation. It has also demonstrated its superiority to placebo in relieving postprandial fullness and bloating in functional dyspepsia patients. In a phase II trial, asimadoline, a novel kappa-opioid agonist, has yielded excellent efficacy results on pain and bloating in IBS-Diarrhea patients. A small study has suggested that naloxone is beneficial in reducing the bloating score in IBS-Constipation or IBS-Mixed patients, but there were no significant differences in the results with naloxone and placebo. Though a recent review also makes a suggestion of the use of opioid agonists in IBS-Diarrhea patients, their role in bloating is uncertain to date.
Summary
Abdominal bloating is a frequent and bothersome, but poorly understood clinical problem. The terms of bloating and distension are often confused, but these 2 symptoms should be considered to be separate, as they probably have different pathophysiological mechanisms. The possible mechanisms of bloating are complex and maybe various mechanisms are combined in symptom generation. Important mechanisms of bloating are impaired gas handling and hypersensitivity. Also, recent evidences are beginning to emphasize that patients with bloating may have an altered bacterial flora, Small Intestinal Bacterial Overgrowth, and abdomino-phrenic dyssynergia. Other less-established factors for bloating are food intolerance, intraluminal bulking and psychological factors.
Currently, there is no treatment which has indisputably proven to be effective for bloating. Treatment strategy for bloating may include pharmacologic approach, dietary modification, and psychological therapy. Taken together, 5-HT4 agonists, antibiotics such as rifaximin, some probiotics, and also novel agents, lubiprostone and linaclotide are substantiated to be effective in some degree in the treatment of bloating. Dietary intervention with low FODMAP is also newly qualified treatment option. Though the evidence is weak, antifoaming agents and antidepressants could be considered in some patients.
- Merck Sharp & Dohme Corp., Merck Manual. Gas-Related Complaints. https://www.merckmanuals.com/professional/gastrointestinal-disorders/symptoms-of-gi-disorders/gas-related-complaints[↩][↩][↩][↩][↩][↩][↩]
- Seo AY, Kim N, Oh DH. Abdominal Bloating: Pathophysiology and Treatment. Journal of Neurogastroenterology and Motility. 2013;19(4):433-453. doi:10.5056/jnm.2013.19.4.433. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3816178/[↩][↩][↩][↩][↩]
- Lea R, Whorwell PJ. Expert Commentary – Bloating, Distension, and the Irritable Bowel Syndrome. Medscape General Medicine. 2005;7(1):18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1681432/[↩]
- Páramo Hernández DB. Bloating and abdominal distention: Just gas? A look in the direction of physiology. Rev Col Gastroenterol. 2011;26:269–272.[↩]
- Relationship of abdominal bloating to distention in irritable bowel syndrome and effect of bowel habit. Houghton LA, Lea R, Agrawal A, Reilly B, Whorwell PJ. Gastroenterology. 2006 Oct; 131(4):1003-10. https://www.ncbi.nlm.nih.gov/pubmed/17030170/[↩]
- Bloating and distension in irritable bowel syndrome: the role of gastrointestinal transit. Agrawal A, Houghton LA, Reilly B, Morris J, Whorwell PJ. Am J Gastroenterol. 2009 Aug; 104(8):1998-2004. https://www.ncbi.nlm.nih.gov/pubmed/19491831/[↩]
- Prevalence and risk factors for abdominal bloating and visible distention: a population-based study. Jiang X, Locke GR 3rd, Choung RS, Zinsmeister AR, Schleck CD, Talley NJ. Gut. 2008 Jun; 57(6):756-63. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2581929/[↩]
- Functional bowel disorders and functional abdominal pain. Thompson WG, Longstreth GF, Drossman DA, Heaton KW, Irvine EJ, Müller-Lissner SA. Gut. 1999 Sep; 45 Suppl 2():II43-7. https://www.ncbi.nlm.nih.gov/pubmed/10457044/[↩]
- Drossman DA, Corazziari E, Tally NJ, Thompson W, Whitehead W. Rome II. The functional gastrointestinal disorders. Diagnosis, pathophysiology and treatment: amultinational consensus. 2nd ed. McLean, VA: Degnon Associates Inc; 2000.[↩]
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130:1480–1491. https://www.ncbi.nlm.nih.gov/pubmed/16678561[↩]
- Prevalence, characteristics, and impact of bloating symptoms in patients with irritable Bowel Syndrome (IBS). Ringel Y, Williams RE, Kalilani L, Cook SF. Clin Gastroenterol Hepatol. 2009 Jan; 7(1):68-72; quiz 3. https://www.ncbi.nlm.nih.gov/pubmed/19124113/[↩]
- Abdominal pain, bloating, and diarrhea in the United States: prevalence and impact. Sandler RS, Stewart WF, Liberman JN, Ricci JA, Zorich NL. Dig Dis Sci. 2000 Jun; 45(6):1166-71. https://www.ncbi.nlm.nih.gov/pubmed/10877233/[↩][↩]
- Prevalence of gastrointestinal symptoms in a multiracial Asian population, with particular reference to reflux-type symptoms. Ho KY, Kang JY, Seow A. Am J Gastroenterol. 1998 Oct; 93(10):1816-22. https://www.ncbi.nlm.nih.gov/pubmed/9772037/[↩]
- Prevalence, characteristics, and impact of bloating symptoms in patients with irritable bowel syndrome. Ringel Y, Williams RE, Kalilani L, Cook SF. Clin Gastroenterol Hepatol. 2009 Jan; 7(1):68-72; quiz 3. https://www.ncbi.nlm.nih.gov/pubmed/19124113/[↩]
- Symptoms across the menstrual cycle in women with irritable bowel syndrome. Heitkemper MM, Cain KC, Jarrett ME, Burr RL, Hertig V, Bond EF. Am J Gastroenterol. 2003 Feb; 98(2):420-30. https://www.ncbi.nlm.nih.gov/pubmed/12591063/[↩]
- Association of physical and emotional symptoms with the menstrual cycle and life-style. Huerta-Franco MR, Malacara JM. J Reprod Med. 1993 Jun; 38(6):448-54. https://www.ncbi.nlm.nih.gov/pubmed/8331624/[↩]
- Obesity is associated with increased risk of gastrointestinal symptoms: a population-based study. Delgado-Aros S, Locke GR 3rd, Camilleri M, Talley NJ, Fett S, Zinsmeister AR, Melton LJ 3rd. Am J Gastroenterol. 2004 Sep; 99(9):1801-6. https://www.ncbi.nlm.nih.gov/pubmed/15330922/[↩]
- Association of upper and lower gastrointestinal tract symptoms with body mass index in an Australian cohort. Talley NJ, Quan C, Jones MP, Horowitz M. Neurogastroenterol Motil. 2004 Aug; 16(4):413-9. https://www.ncbi.nlm.nih.gov/pubmed/15305996/[↩]
- Ranking of symptoms by patients with the irritable bowel syndrome. Maxton DG, Morris JA, Whorwell PJ. BMJ. 1989 Nov 4; 299(6708):1138. https://www.ncbi.nlm.nih.gov/pubmed/2513023/[↩]
- Sensation of bloating and visible abdominal distension in patients with irritable bowel syndrome. Chang L, Lee OY, Naliboff B, Schmulson M, Mayer EA. Am J Gastroenterol. 2001 Dec; 96(12):3341-7. https://www.ncbi.nlm.nih.gov/pubmed/11774947/[↩]
- Bloating in constipation: relevance of intraluminal gas handling. Houghton LA. Best Pract Res Clin Gastroenterol. 2011 Feb; 25(1):141-50. https://www.ncbi.nlm.nih.gov/pubmed/21382585/[↩]
- Overlapping upper and lower gastrointestinal symptoms in irritable bowel syndrome patients with constipation or diarrhea. Talley NJ, Dennis EH, Schettler-Duncan VA, Lacy BE, Olden KW, Crowell MD. Am J Gastroenterol. 2003 Nov; 98(11):2454-9. https://www.ncbi.nlm.nih.gov/pubmed/14638348/[↩]
- Thompson W, Longstreth G, Drossman D, Heaton K, Irvine E, Muller-Lissner S. Functional bowel disorders and functional abdominal pain. Gut. 1999;45(Suppl 2):II43-II47. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1766683/pdf/v045p0II43.pdf[↩][↩]
- Functional bowel disorders. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Gastroenterology. 2006 Apr; 130(5):1480-91. https://www.ncbi.nlm.nih.gov/pubmed/16678561/[↩]
- Drossman DA, Whitehead WE, Camilleri M. Irritable bowel syndrome. A technical review for practice guideline development. Gastroenterology 1997;112:2120–37.[↩]
- Drossman DA, Li Z, Andruzzi E, et al. U.S. householder survey of functional gastrointestinal disorders: prevalence, sociodemography and health impact. Dig Dis Sci 1993;38:1569–80. https://www.ncbi.nlm.nih.gov/pubmed/8359066[↩][↩]
- Talley NJ, Gabriel SE, Harmsen WS, Zinsmeister AR, Evans RW. Medical costs in community subjects with irritable bowel syndrome. Gastroenterology. 1995 Dec;109(6):1736–1741. https://www.ncbi.nlm.nih.gov/pubmed/7498636[↩]
- Clinical practice. Irritable bowel syndrome. Mayer EA. N Engl J Med. 2008 Apr 17; 358(16):1692-9. https://www.ncbi.nlm.nih.gov/pubmed/18420501/[↩]
- Food-related gastrointestinal symptoms in the irritable bowel syndrome. Simrén M, Månsson A, Langkilde AM, Svedlund J, Abrahamsson H, Bengtsson U, Björnsson ES. Digestion. 2001; 63(2):108-15. https://www.ncbi.nlm.nih.gov/pubmed/11244249/[↩]
- Prospective study of motor, sensory, psychologic, and autonomic functions in patients with irritable bowel syndrome. Camilleri M, McKinzie S, Busciglio I, Low PA, Sweetser S, Burton D, Baxter K, Ryks M, Zinsmeister AR. Clin Gastroenterol Hepatol. 2008 Jul; 6(7):772-81. https://www.ncbi.nlm.nih.gov/pubmed/18456567/[↩]
- Are adverse food reactions linked to irritable bowel syndrome? Niec AM, Frankum B, Talley NJ. Am J Gastroenterol. 1998 Nov; 93(11):2184-90. https://www.ncbi.nlm.nih.gov/pubmed/9820394/[↩]
- Food intolerance in functional bowel disorders. Gibson PR. J Gastroenterol Hepatol. 2011 Apr; 26 Suppl 3():128-31. https://www.ncbi.nlm.nih.gov/pubmed/21443725/[↩]
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. In: Drossman DA, Corazziari E, Delvaux M, et al., editors. Rome III: the functional gastrointestinal disorders. 3rd ed. McLean, VA: Degnon; 2006. pp. 487–555.[↩]
- Mayer EA. Irritable Bowel Syndrome. The New England journal of medicine. 2008;358(16):10.1056/NEJMcp0801447. doi:10.1056/NEJMcp0801447. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3816529/[↩]
- Pathophysiology, evaluation, and treatment of bloating: hope, hype, or hot air? Lacy BE, Gabbard SL, Crowell MD. Gastroenterol Hepatol (N Y). 2011 Nov; 7(11):729-39. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3264926/[↩]
- The fecal microbial population in the irritable bowel syndrome. Balsari A, Ceccarelli A, Dubini F, Fesce E, Poli G. Microbiologica. 1982 Jul; 5(3):185-94. https://www.ncbi.nlm.nih.gov/pubmed/7121297/[↩]
- Irritable bowel syndrome, gut microbiota and probiotics. Lee BJ, Bak YT. J Neurogastroenterol Motil. 2011 Jul; 17(3):252-66. https://www.ncbi.nlm.nih.gov/pubmed/21860817/[↩]
- Gastrointestinal microbiota in irritable bowel syndrome: their role in its pathogenesis and treatment. Parkes GC, Brostoff J, Whelan K, Sanderson JD. Am J Gastroenterol. 2008 Jun; 103(6):1557-67. https://www.ncbi.nlm.nih.gov/pubmed/18513268/[↩][↩][↩]
- The fecal microbiota of irritable bowel syndrome patients differs significantly from that of healthy subjects. Kassinen A, Krogius-Kurikka L, Mäkivuokko H, Rinttilä T, Paulin L, Corander J, Malinen E, Apajalahti J, Palva A. Gastroenterology. 2007 Jul; 133(1):24-33. https://www.ncbi.nlm.nih.gov/pubmed/17631127/[↩]
- Microbial community and metabolomic comparison of irritable bowel syndrome faeces. Ponnusamy K, Choi JN, Kim J, Lee SY, Lee CH. J Med Microbiol. 2011 Jun; 60(Pt 6):817-27. https://www.ncbi.nlm.nih.gov/pubmed/21330412/[↩]
- Altered profiles of intestinal microbiota and organic acids may be the origin of symptoms in irritable bowel syndrome. Tana C, Umesaki Y, Imaoka A, Handa T, Kanazawa M, Fukudo S. Neurogastroenterol Motil. 2010 May; 22(5):512-9, e114-5. https://www.ncbi.nlm.nih.gov/pubmed/19903265/[↩]
- Abnormal colonic fermentation in irritable bowel syndrome. King TS, Elia M, Hunter JO. Lancet. 1998 Oct 10; 352(9135):1187-9. https://www.ncbi.nlm.nih.gov/pubmed/9777836/[↩]
- The putative role of the intestinal microbiota in the irritable bowel syndrome. Collins SM, Denou E, Verdu EF, Bercik P. Dig Liver Dis. 2009 Dec; 41(12):850-3. https://www.ncbi.nlm.nih.gov/pubmed/19740713/[↩][↩]
- Alteration of intestinal microflora is associated with reduction in abdominal bloating and pain in patients with irritable bowel syndrome. Nobaek S, Johansson ML, Molin G, Ahrné S, Jeppsson B. Am J Gastroenterol. 2000 May; 95(5):1231-8. https://www.ncbi.nlm.nih.gov/pubmed/10811333/[↩]
- Influence of a methanogenic flora on the breath H2 and symptom response to ingestion of sorbitol or oat fiber. Kajs TM, Fitzgerald JA, Buckner RY, Coyle GA, Stinson BS, Morel JG, Levitt MD. Am J Gastroenterol. 1997 Jan; 92(1):89-94. https://www.ncbi.nlm.nih.gov/pubmed/8995944/[↩]
- Effect of predominant methanogenic flora on the outcome of lactose breath test in irritable bowel syndrome patients. Vernia P, Camillo MD, Marinaro V, Caprilli R. Eur J Clin Nutr. 2003 Sep; 57(9):1116-9. https://www.ncbi.nlm.nih.gov/pubmed/12947430/[↩]
- The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: a randomized trial. Pimentel M, Park S, Mirocha J, Kane SV, Kong Y. Ann Intern Med. 2006 Oct 17; 145(8):557-63. https://www.ncbi.nlm.nih.gov/pubmed/17043337/[↩][↩]
- Non-absorbable antibiotics for managing intestinal gas production and gas-related symptoms. Di Stefano M, Strocchi A, Malservisi S, Veneto G, Ferrieri A, Corazza GR. Aliment Pharmacol Ther. 2000 Aug; 14(8):1001-8. https://www.ncbi.nlm.nih.gov/pubmed/10930893/[↩]
- Detection of bacterial overgrowth in IBS using the lactulose H2 breath test: comparison with 14C-D-xylose and healthy controls. Walters B, Vanner SJ. Am J Gastroenterol. 2005 Jul; 100(7):1566-70. https://www.ncbi.nlm.nih.gov/pubmed/15984983/[↩]
- Small intestinal bacterial overgrowth and the irritable bowel syndrome. Riordan SM, McIver CJ, Duncombe VM, Thomas MC, Nagree A, Bolin TD. Am J Gastroenterol. 2001 Aug; 96(8):2506-8. https://www.ncbi.nlm.nih.gov/pubmed/11513204/[↩]
- Small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Posserud I, Stotzer PO, Björnsson ES, Abrahamsson H, Simrén M. Gut. 2007 Jun; 56(6):802-8. https://www.ncbi.nlm.nih.gov/pubmed/17148502/[↩][↩]
- Review article: small intestinal bacterial overgrowth–prevalence, clinical features, current and developing diagnostic tests, and treatment. Grace E, Shaw C, Whelan K, Andreyev HJ. Aliment Pharmacol Ther. 2013 Oct; 38(7):674-88. https://www.ncbi.nlm.nih.gov/pubmed/23957651/[↩]
- Azpiroz F, Levitt M. Intestinal Gas. In: Feldman M, Friedman LS, Brand LJ, editors. Sleisenger and Fordtran’s. Gastrointestinal and liver disease: pathophysiology, diagnosis, management. Philadelphia: Saunders; 2010. pp. 233–240.[↩]
- A simple radiologic method to estimate the quantity of bowel gas. Chami TN, Schuster MM, Bohlman ME, Pulliam TJ, Kamal N, Whitehead WE. Am J Gastroenterol. 1991 May; 86(5):599-602. https://www.ncbi.nlm.nih.gov/pubmed/2028951/[↩]
- Quantitative analysis of bowel gas using plain abdominal radiograph in patients with irritable bowel syndrome. Koide A, Yamaguchi T, Odaka T, Koyama H, Tsuyuguchi T, Kitahara H, Ohto M, Saisho H. Am J Gastroenterol. 2000 Jul; 95(7):1735-41. https://www.ncbi.nlm.nih.gov/pubmed/10925977/[↩]
- Intestinal gas and bloating: effect of prokinetic stimulation. Accarino A, Perez F, Azpiroz F, Quiroga S, Malagelada JR. Am J Gastroenterol. 2008 Aug; 103(8):2036-42. https://www.ncbi.nlm.nih.gov/pubmed/18802999/[↩]
- AGA technical review on irritable bowel syndrome. Drossman DA, Camilleri M, Mayer EA, Whitehead WE. Gastroenterology. 2002 Dec; 123(6):2108-31. https://www.ncbi.nlm.nih.gov/pubmed/12454866/[↩]
- Irritable bowel syndrome: relationship of disorders in the transit of a single solid meal to symptom patterns. Cann PA, Read NW, Brown C, Hobson N, Holdsworth CD. Gut. 1983 May; 24(5):405-11. https://www.ncbi.nlm.nih.gov/pubmed/6840614/[↩]
- Altered small bowel motility in irritable bowel syndrome is correlated with symptoms. Kellow JE, Phillips SF. Gastroenterology. 1987 Jun; 92(6):1885-93. https://www.ncbi.nlm.nih.gov/pubmed/3569764/[↩]
- Impaired transit and tolerance of intestinal gas in the irritable bowel syndrome. Serra J, Azpiroz F, Malagelada JR. Gut. 2001 Jan; 48(1):14-9. https://www.ncbi.nlm.nih.gov/pubmed/11115817/[↩]
- A prospective study of unexplained visible abdominal bloating. Sullivan SN. N Z Med J. 1994 Oct 26; 107(988):428-30. https://www.ncbi.nlm.nih.gov/pubmed/7970340/[↩]
- Impaired viscerosomatic reflexes and abdominal-wall dystony associated with bloating. Tremolaterra F, Villoria A, Azpiroz F, Serra J, Aguadé S, Malagelada JR. Gastroenterology. 2006 Apr; 130(4):1062-8. https://www.ncbi.nlm.nih.gov/pubmed/16618400/[↩]
- Abdomino-phrenic dyssynergia in patients with abdominal bloating and distension. Villoria A, Azpiroz F, Burri E, Cisternas D, Soldevilla A, Malagelada JR. Am J Gastroenterol. 2011 May; 106(5):815-9. https://www.ncbi.nlm.nih.gov/pubmed/21540894/[↩]
- Abdominal accommodation: a coordinated adaptation of the abdominal wall to its content. Villoria A, Azpiroz F, Soldevilla A, Perez F, Malagelada JR. Am J Gastroenterol. 2008 Nov; 103(11):2807-15. https://www.ncbi.nlm.nih.gov/pubmed/18786126/[↩]
- Bradette M, Delvaux M, Staumont G, Fioramonti J, Bueno L, Frexinos J. Evaluation of colonic sensory thresholds in IBS patients using a barostat. Definition of optimal conditions and comparison with healthy subjects. Dig Dis Sci. 1994;39:449–457. https://www.ncbi.nlm.nih.gov/pubmed/8131679[↩]
- Bouin M, Plourde V, Boivin M, et al. Rectal distention testing in patients with irritable bowel syndrome: sensitivity, specificity, and predictive values of pain sensory thresholds. Gastroenterology. 2002;122:1771–1777. https://www.ncbi.nlm.nih.gov/pubmed/12055583[↩]
- Kellow JE, Eckersley CM, Jones MP. Enhanced perception of physiological intestinal motility in the irritable bowel syndrome. Gastroenterology. 1991;101:1621–1627. https://www.ncbi.nlm.nih.gov/pubmed/1955127[↩]
- Francis CY, Whorwell PJ. Bran and irritable bowel syndrome: time for reappraisal. Lancet. 1994;344:39–40. https://www.ncbi.nlm.nih.gov/pubmed/7912305[↩][↩]
- Friedman G. Diet and the irritable bowel syndrome. Gastroenterol Clin North Am. 1991;20:313–324. https://www.ncbi.nlm.nih.gov/pubmed/2066155[↩]
- Roberfroid MB, Van Loo JA, Gibson GR. The bifidogenic nature of chicory inulin and its hydrolysis products. J Nutr. 1998;128:11–19. https://www.ncbi.nlm.nih.gov/pubmed/9430596[↩]
- O’Leary C, Quigley EM. Small bowel bacterial overgrowth, celiac disease, and IBS: what are the real associations? Am J Gastroenterol. 2003;98:720–722. https://www.ncbi.nlm.nih.gov/pubmed/12738446[↩]
- Tursi A, Brandimarte G, Giorgetti G. High prevalence of small intestinal bacterial overgrowth in celiac patients with persistence of gastrointestinal symptoms after gluten withdrawal. Am J Gastroenterol. 2003;98:839–843. https://www.ncbi.nlm.nih.gov/pubmed/12738465[↩]
- Barrett JS, Gearry RB, Muir JG, et al. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment Pharmacol Ther. 2010;31:874–882. https://www.ncbi.nlm.nih.gov/pubmed/20102355[↩]
- Ong DK, Mitchell SB, Barrett JS, et al. Manipulation of dietary short chain carbohydrates alters the pattern of gas production and genesis of symptoms in irritable bowel syndrome. J Gastroenterol Hepatol. 2010;25:1366–1373. https://www.ncbi.nlm.nih.gov/pubmed/20659225[↩]
- Magge S, Lembo A. Low-FODMAP Diet for Treatment of Irritable Bowel Syndrome. Gastroenterology & Hepatology. 2012;8(11):739-745. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3966170/[↩][↩]
- Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. Gibson PR, Shepherd SJ. J Gastroenterol Hepatol. 2010 Feb; 25(2):252-8. https://www.ncbi.nlm.nih.gov/pubmed/20136989/[↩]
- Levitt MD, Furne J, Olsson S. The relation of passage of gas an abdominal bloating to colonic gas production. Ann Intern Med. 1996;124:422–424. https://www.ncbi.nlm.nih.gov/pubmed/8554251[↩]
- Hebden JM, Blackshaw E, D’Amato M, Perkins AC, Spiller RC. Abnormalities of GI transit in bloated irritable bowel syndrome: effect of bran on transit and symptoms. Am J Gastroenterol. 2002;97:2315–2320. https://www.ncbi.nlm.nih.gov/pubmed/12358250[↩]
- Schmulson M, Chang L, Naliboff B, Lee OY, Mayer EA. Correlation of symptom criteria with perception thresholds during rectosigmoid distension in irritable bowel syndrome patients. Am J Gastroenterol. 2000;95:152–156. https://www.ncbi.nlm.nih.gov/pubmed/10638575[↩]
- Ringel Y, Williams RE, Kalilani L, Cook SF. Prevalence, characteristics, and impact of bloating symptoms in patients with irritable bowel syndrome. Clin Gastroenterol Hepatol. 2009;7:68–72. https://www.ncbi.nlm.nih.gov/pubmed/19124113[↩]
- Agrawal A, Houghton LA, Reilly B, Morris J, Whorwell PJ. Bloating and distension in irritable bowel syndrome: the role of gastrointestinal transit. Am J Gastroenterol. 2009;104:1998–2004. https://www.ncbi.nlm.nih.gov/pubmed/19491831[↩]
- Cann PA, Read NW, Brown C, Hobson N, Holdsworth CD. Irritable bowel syndrome: relationship of disorders in the transit of a single solid meal to symptom patterns. Gut. 1983;24:405–411. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1419989/[↩]
- Park HJ, Jarrett M, Cain K, Heitkemper M. Psychological distress and GI symptoms are related to severity of bloating in women with irritable bowel syndrome. Res Nurs Health. 2008;31:98–107. https://www.ncbi.nlm.nih.gov/pubmed/18181134[↩]
- Song JY, Merskey H, Sullivan S, Noh S. Anxiety and depression in patients with abdominal bloating. Can J Psychiatry. 1993;38:475–479. https://www.ncbi.nlm.nih.gov/pubmed/8242519[↩]
- Johnsen R, Jacobsen BK, Førde OH. Associations between symptoms of irritable colon and psychological and social conditions and lifestyle. Br Med J (Clin Res Ed) 1986;292:1633–1635. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1340703/[↩]
- Walker EA, Katon WJ, Jemelka RP, Roy-Bryne PP. Comorbidity of gastrointestinal complaints, depression, and anxiety in the Epidemiologic Catchment Area (ECA) Study. Am J Med. 1992;92:26S–30S. https://www.ncbi.nlm.nih.gov/pubmed/1531168[↩]
- Heitkemper MM, Cain KC, Jarrett ME, Burr RL, Crowell MD, Woods NF. Relationship of bloating to other GI and menstrual symptoms in women with irritable bowel syndrome. Dig Dis Sci. 2004;49:88–95. https://www.ncbi.nlm.nih.gov/pubmed/14992441[↩]
- Heitkemper MM, Cain KC, Jarrett ME, Burr RL, Hertig V, Bond EF. Symptoms across the menstrual cycle in women with irritable bowel syndrome. Am J Gastroenterol. 2003;98:420–430. https://www.ncbi.nlm.nih.gov/pubmed/12591063[↩]
- Huerta-Franco MR, Malacara JM. Association of physical and emotional symptoms with the menstrual cycle and life-style. J Reprod Med. 1993;38:448–454. https://www.ncbi.nlm.nih.gov/pubmed/8331624[↩]
- Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome. a double-blind, randomized, placebo-controlled study. Am J Gastroenterol. 2003;98:412–419. https://www.ncbi.nlm.nih.gov/pubmed/12591062[↩]
- Kim HJ, Vazquez Roque MI, Camilleri M, et al. A randomized controlled trial of a probiotic combination VSL# 3 and placebo in irritable bowel syndrome with bloating. Neurogastroenterol Motil. 2005;17:687–696. https://www.ncbi.nlm.nih.gov/pubmed/16185307[↩]
- Bernstein JE, Kasich AM. A double-blind trial of simethicone in functional disease of the upper gastrointestinal tract. J Clin Pharmacol. 1974;14:617–623. https://www.ncbi.nlm.nih.gov/pubmed/4612060[↩]
- Holtmann G, Gschossmann J, Mayr P, Talley NJ. A randomized placebo-controlled trial of simethicone and cisapride for the treatment of patients with functional dyspepsia. Aliment Pharmacol Ther. 2002;16:1641–1648. https://www.ncbi.nlm.nih.gov/pubmed/12197843[↩]
- Johanson JF, Ueno R. Lubiprostone, a locally acting chloride channel activator, in adult patients with chronic constipation: a double-blind, placebo-controlled, dose – ranging study to evaluate efficacy and safety. Aliment Pharmacol Ther. 2007;25:1351–1361. https://www.ncbi.nlm.nih.gov/pubmed/17509103[↩]
- Drossman DA, Chey WD, Johanson JF, et al. Clinical trial: lubiprostone in patients with constipation-associated irritable bowel syndrome-results of two randomized, placebo-controlled studies. Aliment Pharmacol Ther. 2009;29:329–341. https://www.ncbi.nlm.nih.gov/pubmed/19006537[↩]





{kind=link}